managing acute medical problems in pregnancy - rcp london
TRANSCRIPT

Managing acute medical problems in pregnancyCathy Nelson-Piercy
Consultant Obstetric Physician Guyrsquos amp St Thomasrsquo Foundation Trust
and Imperial College Healthcare Trust
Professor of Obstetric Medicine
Kingrsquos Health Partners
KCL Division of Womenrsquos Health
nelson_piercy
bull Pregnant women are more predisposed to certain acute
medical problems
bull Those with chronic medical conditions can worsen
flare
bull Pregnant women can suffer pregnancy specific medical
problems
bull Pregnant and postpartum women deserve the same
attention to diagnosis and treatment and appropriate
management plans as the non-pregnant patient
bull Most drugs do not have a licence for use in pregnancy
bull Errors of omission are common
General Principles Page 1
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 1
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 1 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
Paroxysmal supra-ventricular tachycardia (SVT)
self terminate
vagal manoevres
adenosine
Prevention
Beta blockers
Verapamil
Flecainide
Arrhythmias Page 12
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 2
Which of the following are true
1 Chest MRI is preferable to Chest CT
2 IV labetalol is first choice antihypertensive
3 Echocardiogram should be urgently requested
4 Abdo US is essential to exclude fetal death from aortic dissection
affecting descending aorta and uterine arteries
5 The baby should be delivered vaginally before surgery for a type A
aortic dissection
For interactive MCQ Page 14
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

bull Pregnant women are more predisposed to certain acute
medical problems
bull Those with chronic medical conditions can worsen
flare
bull Pregnant women can suffer pregnancy specific medical
problems
bull Pregnant and postpartum women deserve the same
attention to diagnosis and treatment and appropriate
management plans as the non-pregnant patient
bull Most drugs do not have a licence for use in pregnancy
bull Errors of omission are common
General Principles Page 1
bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 1
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 1 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
Paroxysmal supra-ventricular tachycardia (SVT)
self terminate
vagal manoevres
adenosine
Prevention
Beta blockers
Verapamil
Flecainide
Arrhythmias Page 12
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 2
Which of the following are true
1 Chest MRI is preferable to Chest CT
2 IV labetalol is first choice antihypertensive
3 Echocardiogram should be urgently requested
4 Abdo US is essential to exclude fetal death from aortic dissection
affecting descending aorta and uterine arteries
5 The baby should be delivered vaginally before surgery for a type A
aortic dissection
For interactive MCQ Page 14
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

bull39 yr old asian 37 weeks pregnant
bullco dizziness and epigastric pain
bulloe sweaty BP 9468 HR 84
Case 1
A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 1 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
Paroxysmal supra-ventricular tachycardia (SVT)
self terminate
vagal manoevres
adenosine
Prevention
Beta blockers
Verapamil
Flecainide
Arrhythmias Page 12
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 2
Which of the following are true
1 Chest MRI is preferable to Chest CT
2 IV labetalol is first choice antihypertensive
3 Echocardiogram should be urgently requested
4 Abdo US is essential to exclude fetal death from aortic dissection
affecting descending aorta and uterine arteries
5 The baby should be delivered vaginally before surgery for a type A
aortic dissection
For interactive MCQ Page 14
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

A Troponin
B Thrombolysis
C Transfer to catheter lab
D Primary angioplasty
E Aspirin
F Clopidogrel
Case 1 which of the following are appropriate
If normal coronaries consider CMRI
Bubble test also safe in pregnancy
Paroxysmal supra-ventricular tachycardia (SVT)
self terminate
vagal manoevres
adenosine
Prevention
Beta blockers
Verapamil
Flecainide
Arrhythmias Page 12
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 2
Which of the following are true
1 Chest MRI is preferable to Chest CT
2 IV labetalol is first choice antihypertensive
3 Echocardiogram should be urgently requested
4 Abdo US is essential to exclude fetal death from aortic dissection
affecting descending aorta and uterine arteries
5 The baby should be delivered vaginally before surgery for a type A
aortic dissection
For interactive MCQ Page 14
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Paroxysmal supra-ventricular tachycardia (SVT)
self terminate
vagal manoevres
adenosine
Prevention
Beta blockers
Verapamil
Flecainide
Arrhythmias Page 12
bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 2
Which of the following are true
1 Chest MRI is preferable to Chest CT
2 IV labetalol is first choice antihypertensive
3 Echocardiogram should be urgently requested
4 Abdo US is essential to exclude fetal death from aortic dissection
affecting descending aorta and uterine arteries
5 The baby should be delivered vaginally before surgery for a type A
aortic dissection
For interactive MCQ Page 14
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

bull 38 year old primip 39 weeks pregnant
bull Co chest and back pain
bull Oe BP 16585 HR 124 O2 sats 97
bull Urinalysis NAD
bull lsquoWrithing around the bedrsquo lsquowonrsquot lie down to be examinedrsquo
bull Not in labour
Case 2
Which of the following are true
1 Chest MRI is preferable to Chest CT
2 IV labetalol is first choice antihypertensive
3 Echocardiogram should be urgently requested
4 Abdo US is essential to exclude fetal death from aortic dissection
affecting descending aorta and uterine arteries
5 The baby should be delivered vaginally before surgery for a type A
aortic dissection
For interactive MCQ Page 14
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Which of the following are true
1 Chest MRI is preferable to Chest CT
2 IV labetalol is first choice antihypertensive
3 Echocardiogram should be urgently requested
4 Abdo US is essential to exclude fetal death from aortic dissection
affecting descending aorta and uterine arteries
5 The baby should be delivered vaginally before surgery for a type A
aortic dissection
For interactive MCQ Page 14
bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

bull Not all chest pain and breathlessness = PE
bull Beware the hypertensive (systolic) woman with chest pain
bull CXR
bull Echo
Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Case 3
35 year old
1 day post first normal vaginal delivery
CO chest pain
Obstetric SHO requests CTPA
Medical registrar asked to review - told CXR normal
139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

139 per 100000 maternities
Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Maternal mortality from venous
thromboembolism
3 year rolling rates UK 2009-16
p=0664
Same rate as in 1985-87
bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

bull Treatment
bull Prevention
The RCOG guidelines
bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

bull 88 on left (vs 55 in non pregnant)
bull 71 proximal (vs 9 in non pregnant)
bull 64 were restricted to the iliac andor femoral vein
Chan WS et al CMAJ 2010 182657-60
Diagnosis of DVT in Pregnancy
Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Diagnosis
DVT
Doppler US
PE
CXR
VQ Lung scan
CTPA
D dimers are useless
Clinical prediction rules are also useless
Goodacre S Horspool K Nelson-Piercy C et alDiPEP research group BJOG 2018 May 21Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

ROC curves for D dimers Page 24
Hunt BJ Parmar K Horspool K Shephard N Nelson-Piercy C Goodacre S DiPEP research group Br J Haematol 2018 Mar180(5)694-704
Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Annals Page 25
Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Page 26
Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Righini et al Annals Internal Medicine 2018 Page 27
46 women (12) had PE ruled out by clinical probability and D-dimer
Most women required CT or VQ scanning suggesting that clinical probability and D-dimer add little to the diagnostic strategy
11 centres recruited for 8 years Thus the use of clinical probability and D-dimer only avoided scanning for one women every two years at each centre
Using clinical probability and D-dimer to rule out PE in pregnant women will not result in any meaningful reduction in the use of scanning
Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Rads mGy
bull CXR lt0001 lt001
bull Perfusion scan lt008 lt08
bull Ventilation scan lt001 lt01
bull CTPA Helical CT lt0013 lt013
bull Max recommended lt05 5
Radiation exposure
Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Radiation in pregnancy
Page 29
Pahade JK et al Radiographics 639-654 2009Mammogram is associated with 3-44 mSv
bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

bull Increased risk of fatal childhood cancer to the age of 15 following in utero radiation exposure = 0006 per mGy (1 in 17 000 per mGy)
bull The fetal radiation exposure associated with CTPA = 01 mGy
VQ = 05 mGy
bull CTPA Radiation to motherrsquos breasts = 65-250 (70-100) x greater than VQ 10-20 times greater than 2 view mammogram
bull 10 mGy radiation (CTPA) to a womanrsquos breast increases lifetime risk of developing breast cancer by 136 above her background risk
bull VQ investigation of first choice for young women especially if FH of breast CA or patient has had previous chest CT scan
bull Higher rate of nondiagnostic scans in pregnancy with CTPA (375)
VQ (4)
(may be related to the imaging protocol employed)
Ridge CA et al Am J Roentgenol 20091931223ndash7
VQ versus CTPA
Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Page 31
Aug 2018
13 studies diagnostic efficiency false ndashve = 0 for CTPA(837) and VQ(1270)
30 for non-diagnostic results 12 CTPA(1774) 14 VQ(2535)
22 for radiation exposure analysis ndash no direct comparisons old protocols
Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Diagnosis of PE in pregnancySuspected PE
ABG ECG CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWHThrombolysisiv heparin thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
VQ scan
+ve
-ve
+ve-ve
Stop anticoagulation
Still suspicious of PE
ABG arterial blood gas ECG electrocardiogram CXR Chest X-ray USS ultrasound sonography CTPA computerised tomography pulmonary angiography
Modified from Scarsbrook et al Clin Radiol 2006611ndash12
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy
bull High dose LMWHeg Enoxaparin 1mgkgbd (= ACS dose)
NOT 15 mgkg od (= non-pregnant dose)
RCOG Green Top Guideline no 37b
bull ThrombolysisSHOULD NOT BE WITHELD in massive PE with haemodynamic
instability or submassive
Ahearn et al 2002
Leonhardt G et al J Thromb Thrombolysis 200621271-6
bull 56 articles 231 patients Gartman EJ Obstetric medicine 2013
Treatment of acute PE in pregnancy
Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Deaths in first trimesterbull Two women with risk factors presented to the emergency department
one with leg pain
bull D dimers over 20 fold upper limit of normal
bull A negative leg Doppler was assumed to exclude a DVT despite clinical suspicion and a very high D dimer
bull Further presentations to the GP with leg pain did not prompt a re-evaluation of the possibility of DVT
bull When a DVT was finally diagnosed an inadequate treatment dose of LMWH was prescribed
one woman referred by the GP with suspected PE
bull Diagnosis of chest infection was made despite a clear chest on examination and very abnormal D dimer
bull chest x-ray was not performed with a comment that unless necessary it should be withheld because of the pregnancy
bull Obstetric team were not informed despite the GP having alerted them to the womanrsquos referral and the suspected diagnosis
Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Acute asthma
Cydulka et al Am J Resp Crit Care Med 1999160887-892
bull 51 pregnant 500 non-pregnant presenting to ED with acute asthma
bull No difference in severity or duration of symptoms initial PEFR (51 vs 53 predicted)
bull 40 using inhaled steroids month prior to admission
bull Less likely to be given systemic steroids (44 vs 66)
bull Equally likely to be admitted (24 vs 21)
bull Steroids if sent home (38 vs 64)
bull x3 Ongoing exacerbation 2weeks later
Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Tata et al Thorax 2008
Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Hviid A Molgaard-Nielsen D CMAJ 2011183(7)796-804
bull Cohort study of all live births in Denmark 1996 to 2008
bull 832 636 live births
bull 51 973 exposures to corticosteroids during the first trimester
bull 1232 isolated orofacial clefts (ie cleft lip cleft palate or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester
Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Hviid A Molgaard-Nielsen D Corticosteroid use during pregnancy and risk of orofacialclefts CMAJ 2011183(7)796-804
Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Transfer of steroids across the placenta
Maternal concentration
Cord blood concentration
Prednisolone 10 1
Hydrocortisone 6 1
Betamethasone 3 1
All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

All antiemetics
All H2 blockers
All PPIs
NSAIDs lt 32 weeks if good indication
Beta blockers for heart disease thyrotoxicosis
Antihistamines cetirazine and loratidine
Metformin
lsquoOKrsquo drugs in pregnancy
Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Epilepsy
bull The death rate from
epilepsy in pregnancy
(040 per 100 000) is now
higher than the death rate
from hypertensive
disorders in pregnancy
(038 per 100 000)
Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Ischaemic Stroke
Rare
003 per 100 000 maternities
Neither pregnancy caesarean
section delivery nor the
immediate post-partum state
are absolute contraindications
to thrombolysis (intravenous
or intra-arterial) clot retrieval
or craniectomy
Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Eclampsia
Epilepsy
Cerebral venous thrombosis
CVA ICH SAH SOL
Thrombotic Thrombocytopenic Purpura
Meningitis
Drug ETOH withdrawal
Hypoglycaemia hypercalcaemia
Related to dural puncture
Differential diagnosis of seizures in pregnancy
A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

A first seizure in pregnancy that cannot readily be attributed
to eclampsia or epilepsy warrants investigation with CT or
MRI scan of brain
Seizures in Pregnancy
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy
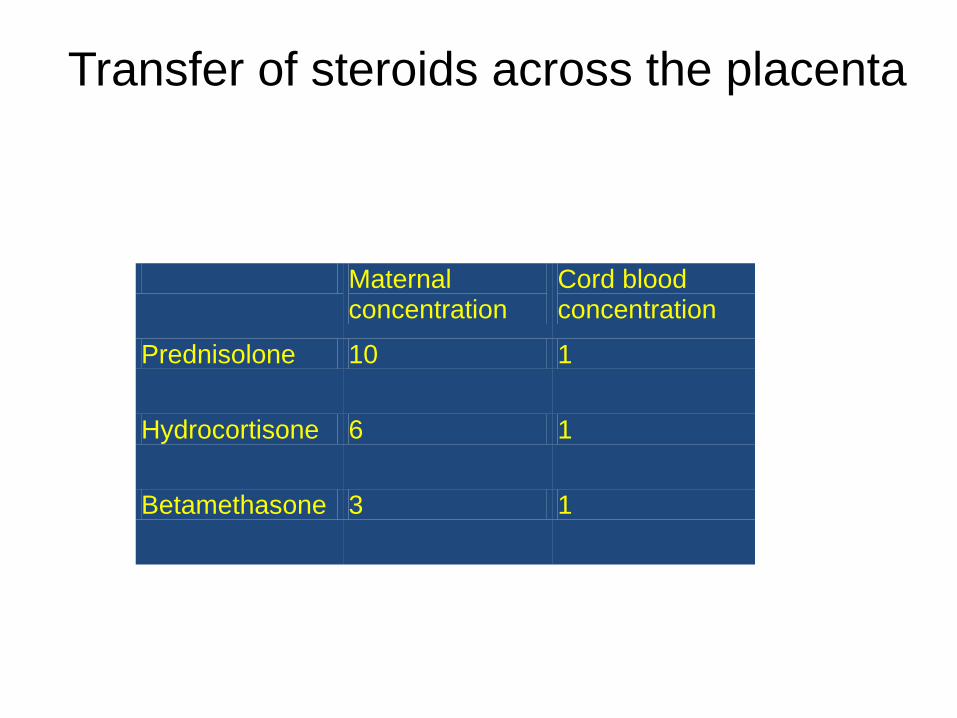
Headache Who to scan
Signs
Severe persistent (CVT)
Sudden onset thunderclap (SAH)
Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

Pressure (blood pressure for pre-eclampsiaeclampsia)
Anaesthetic (post-dural puncture headache)
Reversible (vasoconstriction syndrome [RCVS])
Thrombosis (cerebral venous sinus thrombosis ischaemic
stroke)
Use your brain (there are so many other causes of headache)
Migraine
Post partum Headache Page 48
Lim S Y et al Pract Neurol 20141492-99
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy
Medical problems in pregnancy are common and potentially fatal
Medical conditions are responsible for two thirds of all maternal deaths and much maternal morbidity in the UK
Cardiac disease is the leading cause of maternal mortality in the UK
ACS aortic dissection cardiomyopathy
VTE is the commonest direct cause of maternal death
Control of medical disease is important and improves pregnancy outcomes
Most drugs do not have a licence for use in pregnancy but much harm can result if they are omitted
Summary
sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy

sympregimperialacuk
RCP course
Nov 13-15th 2019
httpwwwsymposiaorguk
E-learning
httpwwwe-lfhorgukprogrammesmedical-problems-in-pregnancy
nelson_piercy