acute respiratory distress syndrome - rcp london
TRANSCRIPT

Acute Respiratory Distress Syndrome
Mark Griffiths
St Bartholomew’s Hospital
Imperial College London

ARDS for Physicians
What is ARDS?
Why should you care?
Should you change?

Date of download: 2/9/2016 Copyright © 2016 American Medical
Association. All rights reserved.
From: Acute Respiratory Distress Syndrome: The Berlin Definition
JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669
Acute non-cardiac pulmonary oedema with respiratory failure

Pulmonary oedema
↓
Surfactant dysfunction
↓
Collapse
Loss of Hypoxic Pulmonary
Vasoconstriction
Hypoxic respiratory
failure + =
Acute Inflammation

Pneumonia Aspiration
Noxious inhalation
Sepsis Embolisation
TRALI
Alcoholism Diabetes Smoking Obesity

ARDS for Respiratory Physicians
Diagnosis

ARF & diffuse pulmonary infiltrates
Not ARDS
Cardiac Respiratory
ARDS
Causes of ARDS

Cardiac
Acute LV failure
Right to left shunts
P. Vascular
PE, Sickle lung, Veno-Occl dz
Diffuse alveolar haemorrhage
Malignancy
BA Carcinoma, Lymphangitis
Acute leukaemia, lymphoma
Cryptogenic
Acute Interstitial Pneum
Cryptogenic Organising Pneum
Acute eosinophilic pneum
Differentials – non-ARDS / DAD

Imaging Echo
Bronchoscopy Micro
Immunology Cytology

ARDS for Physicians
“Not my problem”

Lung SAFE Bellani, G., et al. JAMA, 2016. 315(8): 788-800
• 459 ICUs, 50 countries, 5 continents
• 29,144 ICU admissions
• 10.4% developed ARDS
• 25% patients supported with IMV
• Unrecognised, diagnosis made in 50%
mild ARDS
• High mortality (35-40%)

Clinical risk conditions for ALI in ICU and hospital ward: a prospective observational study
Ferguson ND et al. Critical Care 2007;11(5):R96
28%

Clinical risk conditions for ALI in ICU and hospital ward: a prospective observational study
Ferguson ND et al. Critical Care 2007;11(5):R96

Eight-year trend of ARDS: a population-based study in Olmsted County, Minnesota
Li et al. Am J Respir Crit Care Med 2011;183:59-66
• ↓ ARDS incidence from 82.4 to 38.9 per 100,000 – incr severity of acute illness,
– more comorbidities,
– incr prevalence of predisposing conditions
• ↓Mortality, hospital and ICU los
• Resulting from changes in practice?

Predisposing conditions LIPS
points
Shock 2
Aspiration 2
Sepsis 1
Pneumonia 1.5
High-risk surgery
• Orthopedic spine 1
• Acute abdomen 2
• Cardiac 2.5
• Aortic vascular 3.5
High-risk trauma
• Traumatic brain injury 2
• Smoke inhalation 2
• Near drowning 2
• Lung contusion 1.5
• Multiple fractures 1.5
Risk modifiers LIPS
points
Alcohol abuse 1
Obesity (BMI > 30) 1
Hypoalbuminaemia 1
Diabetes mellitus -1
Chemotherapy 1
FiO2 > 0.35 or > 4
litres/minute
2
Tachypnoea RR > 30 1.5
SpO2 < 95% 1
Acidosis (pH < 7.35) 1.5
Score >4 points sensitivity for ALI 0.69 (95% CI 0.64-0.74),
specificity 0.78 (95% CI 0.77-0.79),

Can ARDS be prevented?
• Identifying a pre-ARDS population
– Where are they? >25% aren’t in AICU
• Time to intervene median lag 2-4 days
• Identifying at risk populations
– Epidemiology i.d. at risk groups - LIPS
– Biomarkers

ARDS for Physicians
Effective interventions

Study Patients Mean Tidal
Volume Vt ml/kg
Mean Plateau Pressure
cmH2O
PEEP cmH2O
Mortality %
P C P C P C P C p
Stewart 120 6.8 10.1 20 28.6 9.6 8.0 50 47 NS
Brower 52 7.3 10.2 24.9 30.6 Not given 50 46 NS
Brochard 116 7.4 10.7 24.5 30.5 9.6 8.5 47 38 NS
ARMA ARDS Network
861 6.5 11.4 26 37 8.1 9.1 31 40 0.007
Ventilator Associated Lung Injury
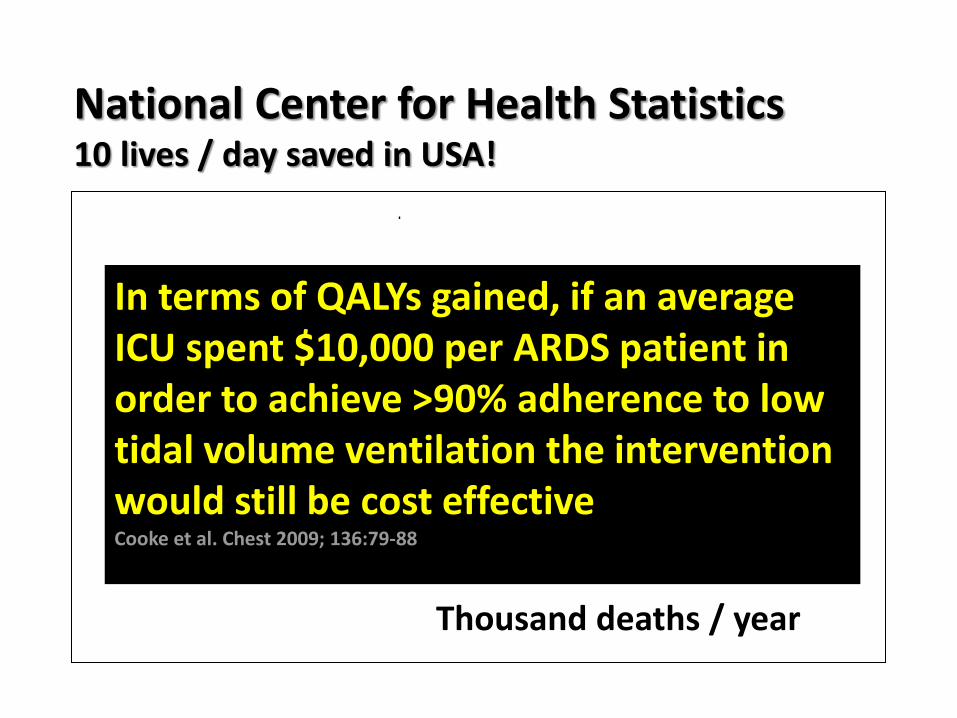
National Center for Health Statistics 10 lives / day saved in USA!
0 5 10 15 20
Thousand deaths / year
Asthma
AIDS
Emphysema
ARDS
In terms of QALYs gained, if an average ICU spent $10,000 per ARDS patient in order to achieve >90% adherence to low tidal volume ventilation the intervention would still be cost effective Cooke et al. Chest 2009; 136:79-88
Fluid And Catheter Treatment Trial (FACTT) ARDS Network N Engl J Med 2006;354:2564-75
• 1000 ALI pts within 48hrs of ALI diagnosis
• Protocolised fluid Mx in for 7 days
• Protective ventilation strategy
• Factorial design - CVC vs PAC
• Cumulative 7 day fluid balance
o Liberal 6992 ± 502 ml
o Conservative -136 ± 491 ml

Outcome Conservative Liberal P value
Death @ d60 25.5 28.4 0.30
Ventilator-free days from d1-28
14.6 + 0.5 12.1 + 0.5 <0.001
Lung injury score 2.03 + 0.07 2.27 + 0.06 0.001
ICU free days: Days 1-7 0.9 + 0.1 0.6 + 0.1 <0.001
Days 1-28 13.4 + 0.4 11.2 + 0.4 <0.001
Renal RT: Prevalence 10% 14% 0.06
Days of RRT 11.0 + 1.7 10.9 + 1.4 0.96

Transfusing ARDS patients
• Western Europe (ABC ‘02) & US (CRIT ‘04) trial 35-45% ICU pts transfused ~5u RBC
• Dose-dependent relationship between RBC utilization & ARDS incidence Gong et al CCM ’04
• Transfusion incr mortality, leukocyte depleted blood less injurious Netzer et al. Chest ’07
• Nosocomial infection: bacteraemia & VAP – TRIM
• Post SHOT, 2/3 decrease in TRALI

Mind the 2nd translational gap!
Young et al. Crit Care Med. 2004 Jun;32(6):1260-5.

Limiting ventilator-induced lung injury through individual electronic medical record surveillance
Herasevich V et al. Critical Care Medicine 2011;39:34-39

ARDS for Respiratory Physicians
After you have failed….

Neutral fluid balance Transfusion @ 7 g/dL Antimicrobials Nutrition Rehab Psychology Out-patient services
Management of ARDS
Summary • Overall
Diagnose & treat the disease!
Avoid iatrogenic injury
Drugs (don’t hold your breath)
• Opportunity for prevention Your patients
Scoring - LIPS
Effective interventions
• Quality improvement Education, cohesive practice and audit
IT/ automated surveillance - “sniffer”

Challenge! 60 yr publican in HDU, d1 after
type B thoracic aneurysm repair
• Hypotensive, oliguric, T 37.8o
• Extubated requiring NIV, fiO2 0.5, CXR fluffy
• Confused
• Hb 80

According to AECC 1994
In the United States, there are estimated to be 190,000 cases and 74,000 deaths annually from ARDS.

Strong +ve Weak +ve Equipoise Weak -ve Strong -ve
Steroids X
NMB X
Inh vasod X
Low Vt X
Proning X
ECCOR X
APRV X
Recrtmt M
HFOV X
High PEEP X
-ve FB X
ECMO X
Analysis of Evidence

Strong +ve Weak +ve Equipoise Weak -ve Strong -ve
Steroids RCT required
NMB Cisatr, 48hr, mod/severe
Inh vasod iNO
Low Vt X
Proning >16hr, mod/severe
ECCOR RCT required
APRV X
Recrtmt M
HFOV X
High PEEP mod/severe
-ve FB X
ECMO X
ICS GDG Recommendations
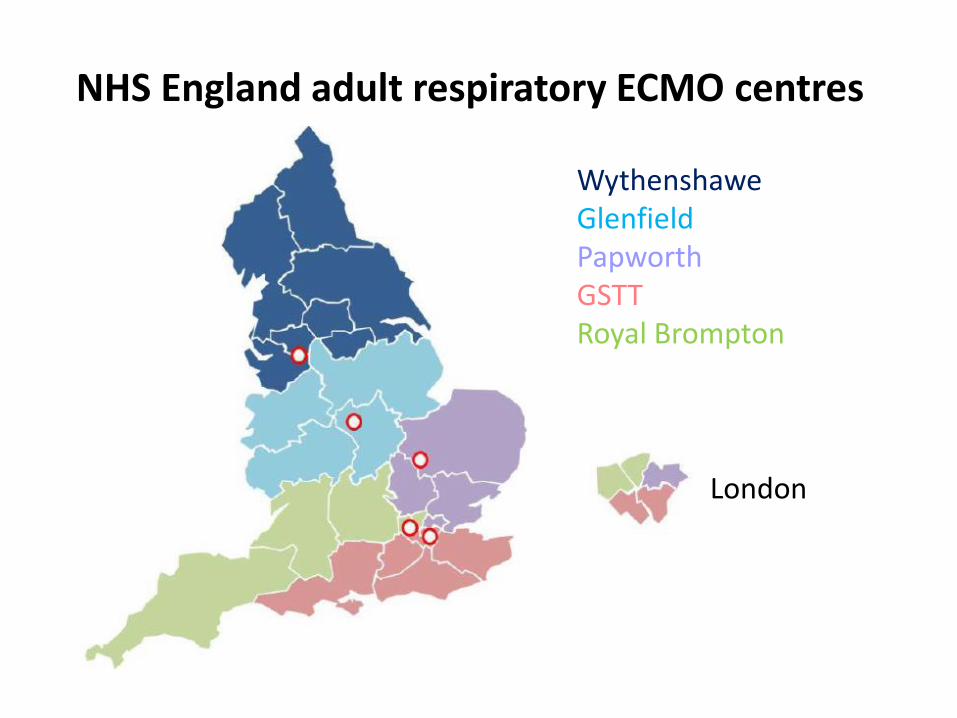
Wythenshawe Glenfield Papworth GSTT Royal Brompton
London
NHS England adult respiratory ECMO centres

Indications

Activity
Parameter N
Referrals 105
Admissions ECMO 29 AV-ECCO2R 1 HFOV 2
37
Patients not admitted Futility 44 “Too well” 13 Lack of capacity 9 Wrong area 1 Referrer wants to keep 1 Referral for cardiac ECMO 0
68

Survival for patients admitted
Time point N 2014 2013-4
End of NSCT pathway 42 37 (88.1 %) 74.3%
Discharge from RBH ICU 42 32 (76.2 %) 68.8%
VA ECMO 4 3 (75 %)

Deaths
G. 33 year old male, pulmonary tuberculosis • IF drug user • Diagnosed with pulmonary TB two weeks previously • Directly observed therapy but defaulted after 1 week • Represented with 2 day history of breathlessness, Pseudomonas identified from
sputum • Ventilated and referred on day 2 (pH 7.10; pO2 7.9 kPa) • 25 min cardiac arrest due to tension pneumothorax whilst ECMO team en route
• Mobile VV-ECMO
• Acute liver dysfunction (hypoxic and Hepatitis E) • Acute kidney injury • Very significant sedation issues

Deaths
G. 33 year old male, pulmonary tuberculosis
• Recurrent pneumothoraces, torrential air leak • Relentless clinical decline • ECMO withdrawn day 16 • Referred but unsuitable for donation after cardiac death

Deaths
C. 67y male, community acquired pneumonia • Severe hypoxaemic respiratory failure • Left lower lobe consolidation • Empirical thrombolysis for PE • Transferred for consideration of ECMO
• Unequal pupils noted • CT head –no neurosurgical option • CT pulmonary angiogram – no PE • Not for escalation of therapy, died on day 2
• Hospital post-mortem

Intracranial haemorrhage
Last three years data
Non-ECMO • 3/39 (7.7%) ECMO patients • 7/49 (14.3%) No difference (p=0.506, Fisher’s Exact) 4 out of 10 patients survived to discharge home Prediction of outcome difficult
ELSO
~ 3.9 %
Australia
~ 8.8 %
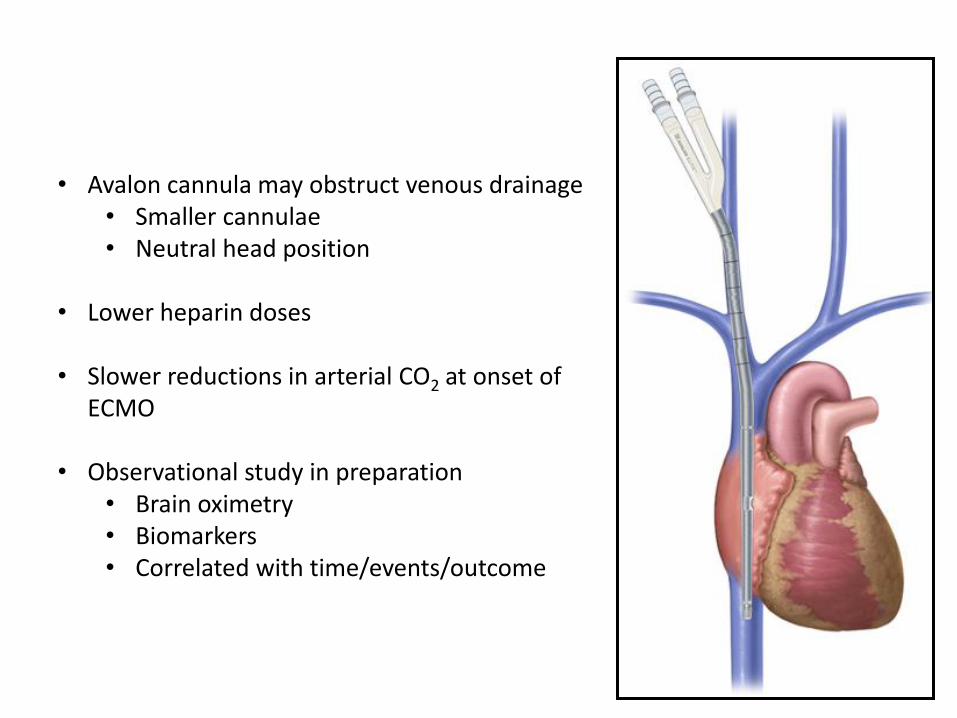
• Avalon cannula may obstruct venous drainage • Smaller cannulae • Neutral head position
• Lower heparin doses
• Slower reductions in arterial CO2 at onset of
ECMO
• Observational study in preparation • Brain oximetry • Biomarkers • Correlated with time/events/outcome