mechanical ventilation pos seminar series december 2010 dr. j. wassermann department of anesthesia...
TRANSCRIPT

Mechanical Ventilation
POS Seminar SeriesDecember 2010
Dr. J. Wassermann
Department of Anesthesia
St. Michael’s Hospital
University of Toronto

Outline
Definition – what is itIndications – when do you use itVentilator Settings – how do you use itModes of VentilationAdverse EffectsSummary

Mechanical Ventilation – Definition
Mechanical Ventilation =
– Use of a mechanical apparatus to provide (or augment) the requirements of a patient’s breathing (i.e. get O2 into and CO2 out of alveoli)

Mechanical Ventilation – Definition
Use of positive pressure to physically transport gases into and out of lungs
(earlier ventilators used negative pressure)
Usually performed via ETT but not always (noninvasive ventilation)

Mechanical Ventilation
A supportive measure – not a therapy
Must diagnose and treat underlying cause
Use ventilator to support patient until underlying disorder improved – and try not to cause harm in the process

Intubation - Indications
1. Airway patency (obstruction)
2. Airway protection (aspiration)
3. Oxygenation (pO2)*
4. Ventilation (pCO2)*
5. Tracheal Toilet (secretions)
* don’t necessarily need intubation for these

Mechanical Ventilation – Indications
Improve Oxygenation (pO2; SaO2)
Improve Ventilation (pCO2) - or hyperventilate pt
Reduce work of breathing (WOB)(i.e. asthma; COPD)____________________________________________
CHF
Hemodynamic Instability

Inadequate Oxygenation
1. Decreased FIO2/PIO2
2. A/W obstruction
3. Hypoventilation
4. V/Q mismatch*
5. Diffusion
6. Decreased mixed venous O2
7. RL shunt (i.e. intra-cardiac shunt)

Alveolar Gas Equation
PALVO2 = [(PATM – PH2O) × FIO2] – (PCO2 ) RQ
PALVO2 = [(760 – 47) × 0.21] − (40 ÷ 0.8)
PALVO2 = [ 713 × 0.21] − 50 = 100
NOTE: On 100% O2 , PALVO2 should be ~ 650

Inadequate OxygenationV/Q mismatch (low V/Q):
– Pneumonia– Aspiration– Pulmonary edema– Atelectasis/collapse (plug/PTX/HTX/effusions)– ARDS– Pulmonary contusion– Alveolar hemorrhage

Inadequate Ventilation
PaCO2 CO2 production Minute Ventilation (VE )
VE = RR x Vt
Any condition inadequate ventilation
increased pCO2 Altered LOC S. cord injuries/NM disorders weakness

Work of Breathing
WOB ~ ventilatory demands (CO2 prod’n)
~ airway resistance (i.e. severe asthma)
~ compliance (lung, c/w, abdo)
Increased WOB usually O2/CO2 problems;May need mech vent purely for WOB (i.e. asthma)
c/w = chest wall

Summary thus far
Mechanical ventilation indicated in situations with:
1. O2 problems (oxygenation)
2. CO2 problems (ventilation)
3. WOB (often assoc with 1 and/or 2)
Don’t always need an ETT

Mechanical Ventilators
How do you use them……

Ventilator Settings
ModeRateVolume (VT)PressureFIO2PEEPI:E (ratio of insp vs exp time)
Insp Flow rateFlow patternAlarms

Modes of Mechanical Ventilation
Controlled Mechanical Ventilation (CMV)Assist Control (AC)/Volume Control (VC)Intermittent Mandatory Ventilation (SIMV)Pressure Control (PCV)Pressure Support Ventilation (PSV)

Modes of Mechanical Ventilation
Trigger – what initiates a breath
Target – what the vent is trying to achieve
Cycle – what causes the breath to end

Continuous Mandatory Ventilation (CMV)
Trigger –Ventilator initiates all breaths
Patient can not initiate
Target – Volume
Cycle - Time

Continuous Mandatory Ventilation (CMV)
e.g. Settings - Mode: CMV
Rate 10; Vt 700cc
FIO2 0.5; PEEP 5.0vent gives 10 bpm @ 700cc each
pt gets zero extra breaths (even if tries)
very uncomfortable for pt
only used if pt paralyzed (i.e. in O.R.)

Assist Control (Volume Control)
Trigger – machine and patientTarget – volumeSettings-Mode: VC
Rate 10; Vt 700cc
FIO2 0.5; PEEP 5.0
e.g. vent gives 10 bpm @ 700cc each
pt initiates 6 bpm – vent provides 700cc

Synchronized Intermittent Mandatory Ventilation (SIMV)
Trigger – ventilator and patientTarget – ventilator breaths = set volume
patient breaths = patient effortSettings-Mode: SIMV
Rate 10; Vt 700cc
FIO2 0.5; PEEP 5.0e.g. vent gives 10 bpm @ 700cc each
patient takes 6 bpm @ 150 cc each

Pressure Control (PC)
Trigger – ventilator and patientTarget – Pressure (above PEEP)Settings – Mode: PC
Rate 10; Pressure 24 cm H2O
FIO2 0.5; PEEP 5
e.g. vent gives 10 bpm to a peak Paw = 29
pt takes 6 bpm targeted to peak Paw =29

Pressure Support Ventilation (PSV)
Trigger – patient onlyTarget - pressureCycle – patient flow decrease
Settings – Mode: PSV = 14 cm H2O FIO2 0.4; PEEP 5
e.g. pt takes 18 bpm @ Vt = 500ccmachine gives zero breaths

Completely Unassisted Breaths
Trigger – patientCycle – patient effort ceases
Settings: CPAP 5; FIO2 0.4
e.g. patient takes 24 bpm @ 250 cc each

Mechanical Ventilator Settings
Mode (usually VC or PC to start)RateTidal Volume (VC) [or Pressure (PC)]FIO2
PEEP I:E

Choosing a Ventilatory Mode
No proven benefit of any mode of another
Keys are to:
– Support pt to allow time for underlying process to improve
– Avoid/minimize adverse effects of mech ventilation

Adverse Effects of Mechanical Ventilation
Pulmonary:
– Intubation effects– Air leaks (pneumothorax/BPF)
–Ventilator-associated lung injury– Ventilator-associated pneumonia– Dynamic hyperinflation/Auto-PEEP

Adverse Effects of Mechanical Ventilation
Cardiovascular:– Increased CVP (↑intrathoracic pressure)– Decreased venous return– Hypotension– Increased RV afterload
GI:– Stress ulcers/GI bleeding

Adverse Effects of Mechanical Ventilation
Neuro/muscular:
– ↑ ICP– Prolonged sedation– Myopathies/Neuropathies

Ventilator-Associated Lung Injury (VALI)
1. Volutrauma
2. Barotrauma
3. Atelectotrauma
4. Biotrauma

Ventilator-Associated Lung Injury (VALI)
1. Volutrauma – overdistension of alveoli
2. Barotrauma – high alveolar pressures
3. Atelectotrauma – repetitive opening and closing of alveoli
4. Biotrauma – release of infl mediators into systemic circulation organ dysfunction
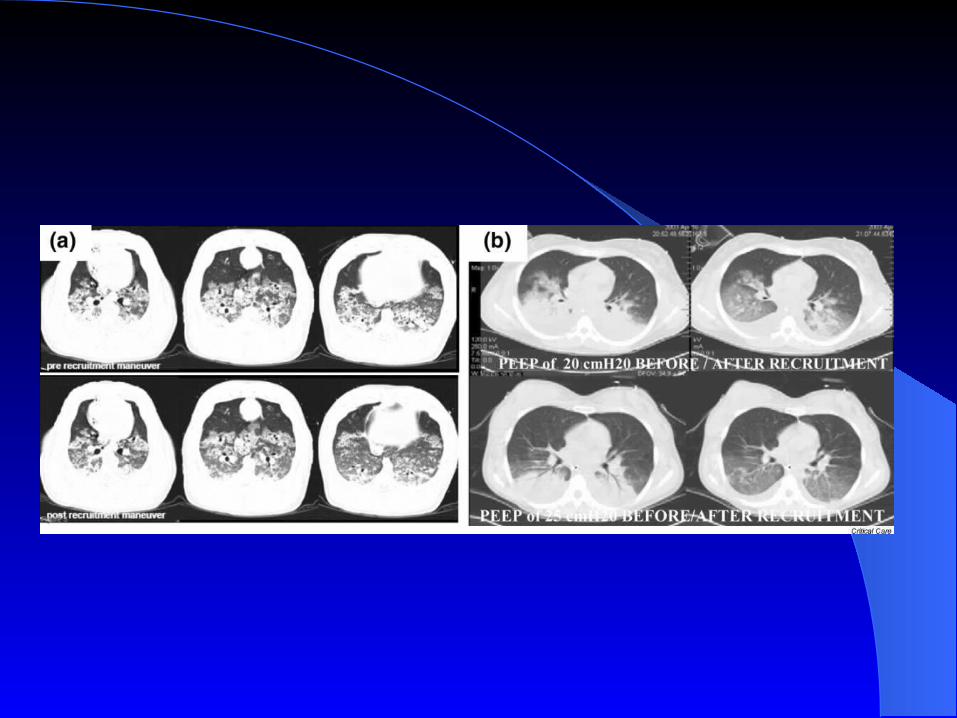

Ventilation of ARDS (baby lung)
Moderate PEEP (to keep alveoli open)• 10 – 15 cm H20
Small Vt’s (to avoid overdistension)• < 6 cc/kg
Plateau pressure < 30 cm H2OPermissive hypercapnia & hypoxemia

Summary
Mechanical ventilation used to:1. Improve oxygenation
2. Improve ventilation (CO2 removal)
3. Unload respiratory muscles
A support until patients condition improves

Summary
Different modes for ventilation– differ in how breaths are initiated, ended and
assisted– differ in independent and dependant variables
(i.e. what machine controls and what it doesn’t)– no proven advantage of one mode– use ventilator strategies to avoid lung injury
and other adverse effects

Questions?

Weaning from Mechanical Ventilation
Once underlying pathology improves
Need to ensure:– Adequate respiratory muscle strength– WOB not excessive
Ventilatory demands Resistance Compliance

Weaning from Mechanical Ventilation
Volume overload and myocardial ischemia
common causes of failure to wean
RR/Vt = good predictor if <80-100
SIMV inferior to SV trials or CPAP/PSV

Noninvasive Ventilation
Indications for intubation:
1. Airway patency*
2. Airway protection (aspiration)*
3. Oxygenation
4. Ventilation
5. Tracheal suctioning (toilet)*

Noninvasive Ventilation
Avoids intubation and complicationsCan deliver various modes of ventilation
– CPAP/CPAP + PSV most common
Indications:– hypercapneic respiratory failure (COPD exac)– cardiogenic p. edema

Noninvasive Ventilation
Contraindications:– Inability to cooperate (i.e. confusion)– Altered LOC– Inability to clear secretions– Hemodynamic instability

Ventilation Strategies in Specific Situations
ARDSAsthmaIncreased intraabdominal pressure