medication error reduction plan (merp) - sfdph.org error reduction plan (merp) san francisco general...
TRANSCRIPT
(rev10_Dec09) page 1
Medication Error Reduction Plan (MERP) San Francisco General Hospital and Trauma Center
2009 SB 1875 Annual Report Health and Safety Code 1339.63: subdivision (d) Medication-related errors can occur in the following areas:
• Prescribing • Prescription order communication • Product labeling • Packaging and nomenclature • Compounding • Dispensing
• Distribution • Administration • Education • Monitoring • Use
Plan Elements
1. Evaluate, assess, and include a method to address each of the procedures and systems listed under subdivision (d) to identify weakness or deficiencies that could contribute to errors in the administration of medications.
2. Annual review to assess the effectiveness of the implementation of each of the procedures and systems listed under subdivision (d). 3. Modified as warranted when weaknesses or deficiencies are noted to achieve the reduction of medication errors. 4. Describe the technology to be implemented and how it is expected to reduce medication errors. 5. Include a system/process to proactively identify actual or potential errors. Shall include concurrent and retrospective review of clinical care. 6. Multidisciplinary process to regularly analyze all identified actual or potential errors and describe how the analysis will be utilized to change
current procedures and systems to reduce errors. 7. Include a process to incorporate external medication-related error alerts to modify current processes and systems as appropriate.
Note: Plan Elements #1-4 are defined within the grids on the following pages and #5-7 are located on page 25.
(rev10_Dec09) page 2
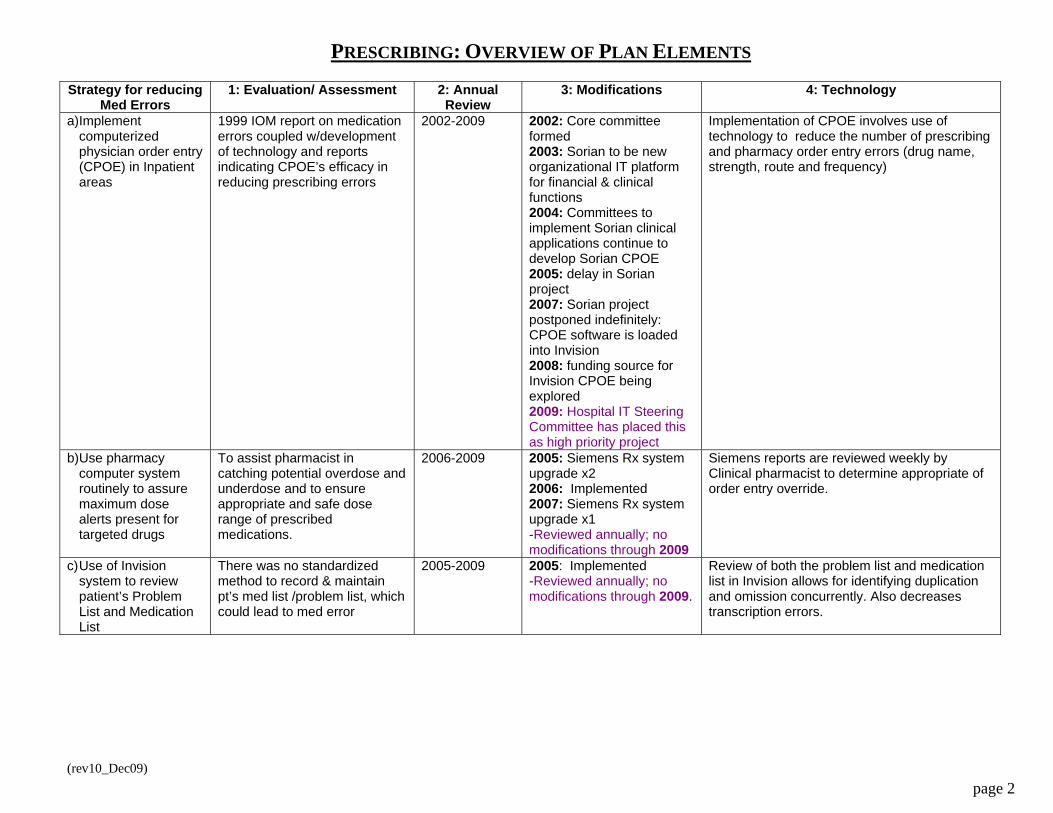
PRESCRIBING: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Implement computerized physician order entry (CPOE) in Inpatient areas
1999 IOM report on medication errors coupled w/development of technology and reports indicating CPOE’s efficacy in reducing prescribing errors
2002-2009
2002: Core committee formed 2003: Sorian to be new organizational IT platform for financial & clinical functions 2004: Committees to implement Sorian clinical applications continue to develop Sorian CPOE 2005: delay in Sorian project 2007: Sorian project postponed indefinitely: CPOE software is loaded into Invision 2008: funding source for Invision CPOE being explored 2009: Hospital IT Steering Committee has placed this as high priority project
Implementation of CPOE involves use of technology to reduce the number of prescribing and pharmacy order entry errors (drug name, strength, route and frequency)
b) Use pharmacy computer system routinely to assure maximum dose alerts present for targeted drugs
To assist pharmacist in catching potential overdose and underdose and to ensure appropriate and safe dose range of prescribed medications.
2006-2009
2005: Siemens Rx system upgrade x2 2006: Implemented 2007: Siemens Rx system upgrade x1 -Reviewed annually; no modifications through 2009
Siemens reports are reviewed weekly by Clinical pharmacist to determine appropriate of order entry override.
c) Use of Invision system to review patient’s Problem List and Medication List
There was no standardized method to record & maintain pt’s med list /problem list, which could lead to med error
2005-2009 2005: Implemented -Reviewed annually; no modifications through 2009.
Review of both the problem list and medication list in Invision allows for identifying duplication and omission concurrently. Also decreases transcription errors.

(rev10_Dec09) page 3
Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
d) Use of Invision system to establish Medication Reconciliation Process: Taskforce consists of physicians, nurses, IT and pharmacy meet bimonthly; training for MD by MDs
Patient Safety & Quality literature suggests medication reconciliation as one of many safe practices for better patient care. It is also one of The Joint Commission’s National Patient Safety Goals (TJC-NPSG #8) to improve communication of patient medication information throughout the continuum of care.
2005-2009 2005: Pilot implemented 2007: Full implementation completed. 2007: ED Med rec form created 2007: OR Med Rec process implemented 2008: Home Med List function in Nursing Admission Database 2008: Improved formatting & nomenclature changes to printed forms & Invision function buttons 2009: To address prescribing errors in SFBHC pts admitted to the hospital, new pop-up window implemented to alert prescribers to use the current hospital med list, not the outpatient med list which is normally used for a standard admission.
Invision system can be accessed by all disciplines. Orders are sent to Invision directly from Siemens Pharmacy system. Medication Reconciliation instructions are also posted on Invision for all disciplines to access as necessary.
e) Chemotherapy Manual installed electronically on the CHN Intranet
Decision made to post on Intranet for easier and consistent update and maintenance. Hard copy manuals were previously stored & referenced in multiple locations throughout the organization.
2005-2009 2005: Implemented 2008: Currently updated by newly hired Heme-Onc Clinical RPh 2009: Administrative policy revised & streamlined for easier reference; Chemo order form modified to eliminate ambiguity
Chemotherapy Manual posted on hospital intranet to provide same, legible information for all disciplines involved in chemotherapy.
f) Hire a clinical pharmacist to assist in dosing and selection of appropriate chemotherapy agent
To augment clinical expertise and support for safe use of these high alert medications.
2007-2009 2007: Clinical Pharmacist hired
N/A
(rev10_Dec09) page 4
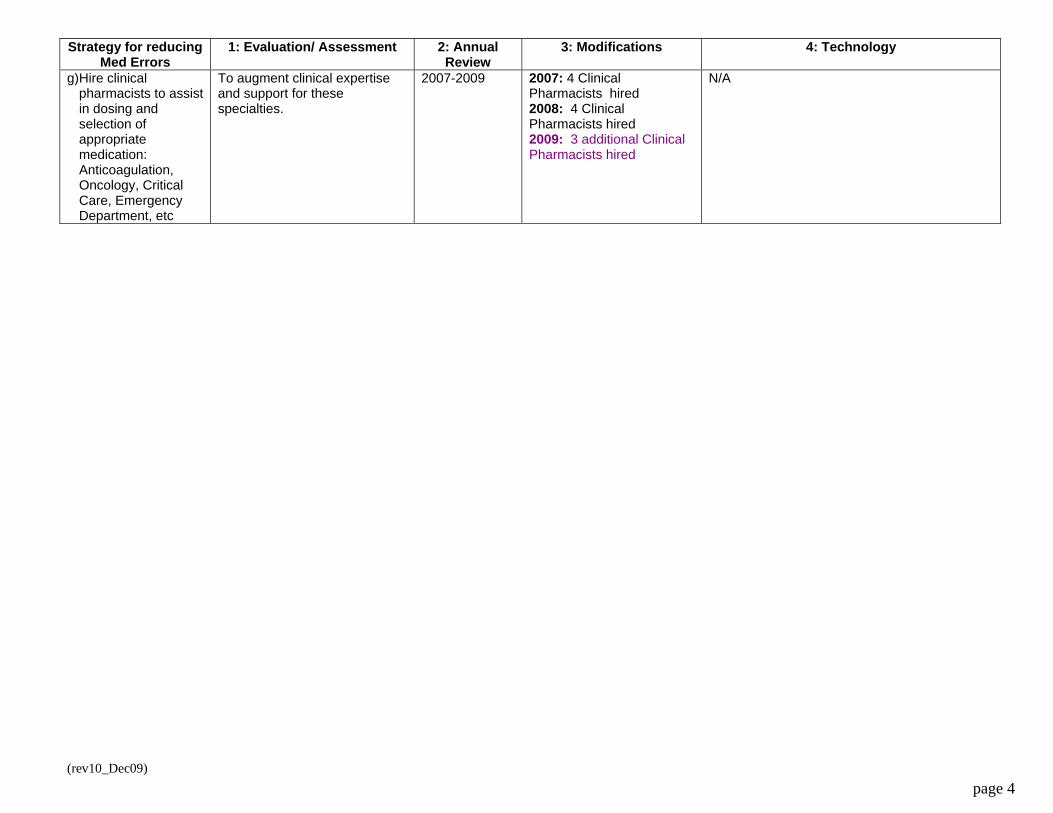
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
g) Hire clinical pharmacists to assist in dosing and selection of appropriate medication: Anticoagulation, Oncology, Critical Care, Emergency Department, etc
To augment clinical expertise and support for these specialties.
2007-2009 2007: 4 Clinical Pharmacists hired 2008: 4 Clinical Pharmacists hired 2009: 3 additional Clinical Pharmacists hired
N/A
(rev10_Dec09) page 5
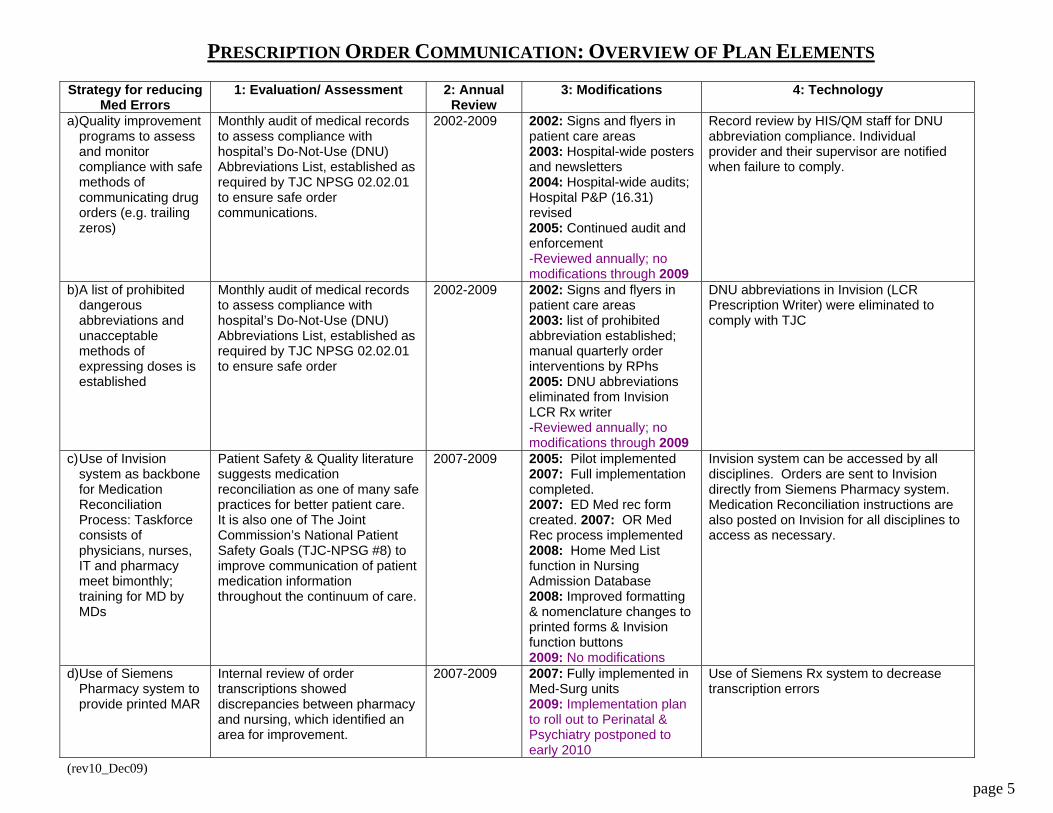
PRESCRIPTION ORDER COMMUNICATION: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Quality improvement programs to assess and monitor compliance with safe methods of communicating drug orders (e.g. trailing zeros)
Monthly audit of medical records to assess compliance with hospital’s Do-Not-Use (DNU) Abbreviations List, established as required by TJC NPSG 02.02.01 to ensure safe order communications.
2002-2009
2002: Signs and flyers in patient care areas 2003: Hospital-wide posters and newsletters 2004: Hospital-wide audits; Hospital P&P (16.31) revised 2005: Continued audit and enforcement -Reviewed annually; no modifications through 2009
Record review by HIS/QM staff for DNU abbreviation compliance. Individual provider and their supervisor are notified when failure to comply.
b) A list of prohibited dangerous abbreviations and unacceptable methods of expressing doses is established
Monthly audit of medical records to assess compliance with hospital’s Do-Not-Use (DNU) Abbreviations List, established as required by TJC NPSG 02.02.01 to ensure safe order
2002-2009
2002: Signs and flyers in patient care areas 2003: list of prohibited abbreviation established; manual quarterly order interventions by RPhs 2005: DNU abbreviations eliminated from Invision LCR Rx writer -Reviewed annually; no modifications through 2009
DNU abbreviations in Invision (LCR Prescription Writer) were eliminated to comply with TJC
c) Use of Invision system as backbone for Medication Reconciliation Process: Taskforce consists of physicians, nurses, IT and pharmacy meet bimonthly; training for MD by MDs
Patient Safety & Quality literature suggests medication reconciliation as one of many safe practices for better patient care. It is also one of The Joint Commission’s National Patient Safety Goals (TJC-NPSG #8) to improve communication of patient medication information throughout the continuum of care.
2007-2009 2005: Pilot implemented 2007: Full implementation completed. 2007: ED Med rec form created. 2007: OR Med Rec process implemented 2008: Home Med List function in Nursing Admission Database 2008: Improved formatting & nomenclature changes to printed forms & Invision function buttons 2009: No modifications
Invision system can be accessed by all disciplines. Orders are sent to Invision directly from Siemens Pharmacy system. Medication Reconciliation instructions are also posted on Invision for all disciplines to access as necessary.
d) Use of Siemens Pharmacy system to provide printed MAR
Internal review of order transcriptions showed discrepancies between pharmacy and nursing, which identified an area for improvement.
2007-2009 2007: Fully implemented in Med-Surg units 2009: Implementation plan to roll out to Perinatal & Psychiatry postponed to early 2010
Use of Siemens Rx system to decrease transcription errors
(rev10_Dec09) page 6
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
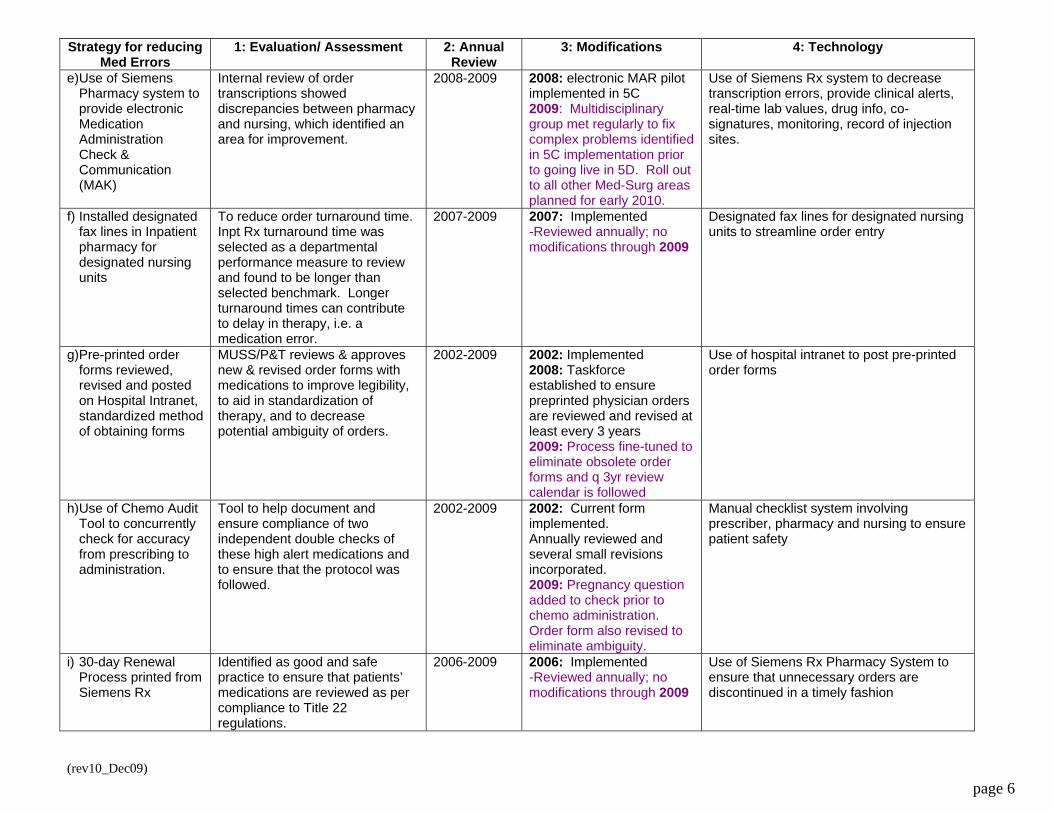
e) Use of Siemens Pharmacy system to provide electronic Medication Administration Check & Communication (MAK)
Internal review of order transcriptions showed discrepancies between pharmacy and nursing, which identified an area for improvement.
2008-2009 2008: electronic MAR pilot implemented in 5C 2009: Multidisciplinary group met regularly to fix complex problems identified in 5C implementation prior to going live in 5D. Roll out to all other Med-Surg areas planned for early 2010.
Use of Siemens Rx system to decrease transcription errors, provide clinical alerts, real-time lab values, drug info, co-signatures, monitoring, record of injection sites.
f) Installed designated fax lines in Inpatient pharmacy for designated nursing units
To reduce order turnaround time. Inpt Rx turnaround time was selected as a departmental performance measure to review and found to be longer than selected benchmark. Longer turnaround times can contribute to delay in therapy, i.e. a medication error.
2007-2009 2007: Implemented -Reviewed annually; no modifications through 2009
Designated fax lines for designated nursing units to streamline order entry
g) Pre-printed order forms reviewed, revised and posted on Hospital Intranet, standardized method of obtaining forms
MUSS/P&T reviews & approves new & revised order forms with medications to improve legibility, to aid in standardization of therapy, and to decrease potential ambiguity of orders.
2002-2009 2002: Implemented 2008: Taskforce established to ensure preprinted physician orders are reviewed and revised at least every 3 years 2009: Process fine-tuned to eliminate obsolete order forms and q 3yr review calendar is followed
Use of hospital intranet to post pre-printed order forms
h) Use of Chemo Audit Tool to concurrently check for accuracy from prescribing to administration.
Tool to help document and ensure compliance of two independent double checks of these high alert medications and to ensure that the protocol was followed.
2002-2009 2002: Current form implemented. Annually reviewed and several small revisions incorporated. 2009: Pregnancy question added to check prior to chemo administration. Order form also revised to eliminate ambiguity.
Manual checklist system involving prescriber, pharmacy and nursing to ensure patient safety
i) 30-day Renewal Process printed from Siemens Rx
Identified as good and safe practice to ensure that patients’ medications are reviewed as per compliance to Title 22 regulations.
2006-2009 2006: Implemented -Reviewed annually; no modifications through 2009
Use of Siemens Rx Pharmacy System to ensure that unnecessary orders are discontinued in a timely fashion
(rev10_Dec09) page 7
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
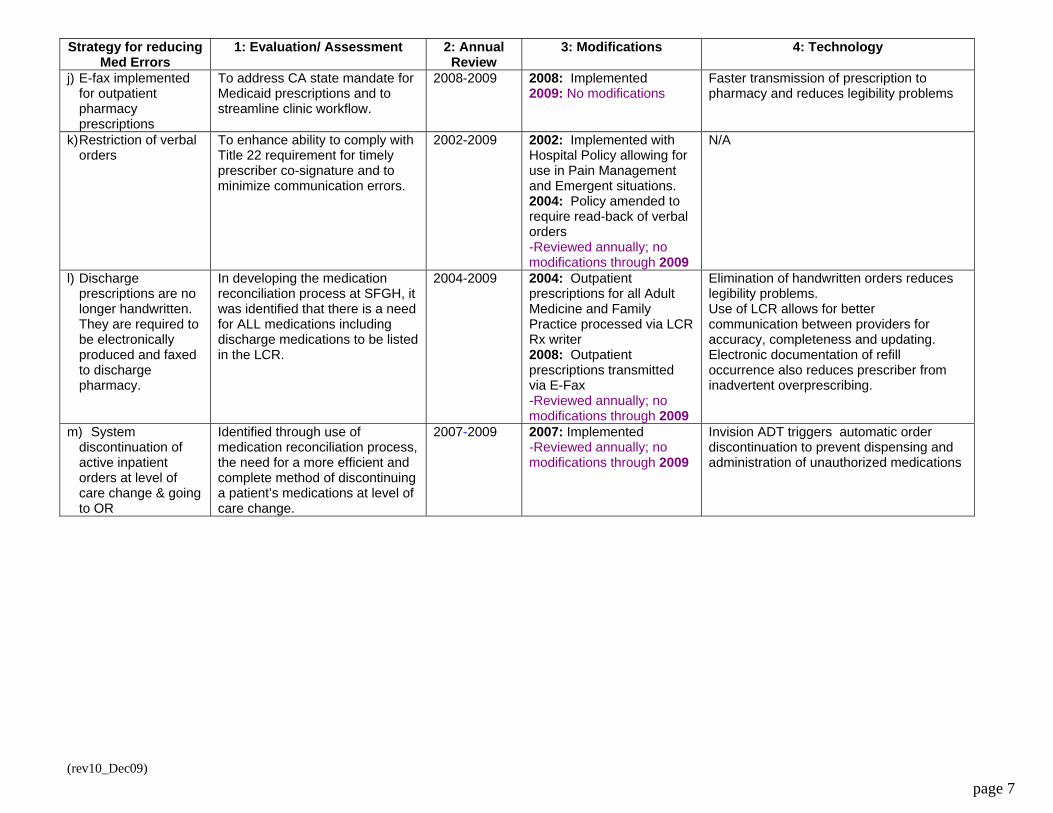
j) E-fax implemented for outpatient pharmacy prescriptions
To address CA state mandate for Medicaid prescriptions and to streamline clinic workflow.
2008-2009 2008: Implemented 2009: No modifications
Faster transmission of prescription to pharmacy and reduces legibility problems
k) Restriction of verbal orders
To enhance ability to comply with Title 22 requirement for timely prescriber co-signature and to minimize communication errors.
2002-2009 2002: Implemented with Hospital Policy allowing for use in Pain Management and Emergent situations. 2004: Policy amended to require read-back of verbal orders -Reviewed annually; no modifications through 2009
N/A
l) Discharge prescriptions are no longer handwritten. They are required to be electronically produced and faxed to discharge pharmacy.
In developing the medication reconciliation process at SFGH, it was identified that there is a need for ALL medications including discharge medications to be listed in the LCR.
2004-2009 2004: Outpatient prescriptions for all Adult Medicine and Family Practice processed via LCR Rx writer 2008: Outpatient prescriptions transmitted via E-Fax -Reviewed annually; no modifications through 2009
Elimination of handwritten orders reduces legibility problems. Use of LCR allows for better communication between providers for accuracy, completeness and updating. Electronic documentation of refill occurrence also reduces prescriber from inadvertent overprescribing.
m) System discontinuation of active inpatient orders at level of care change & going to OR
Identified through use of medication reconciliation process, the need for a more efficient and complete method of discontinuing a patient’s medications at level of care change.
2007-2009 2007: Implemented -Reviewed annually; no modifications through 2009
Invision ADT triggers automatic order discontinuation to prevent dispensing and administration of unauthorized medications
(rev10_Dec09) page 8
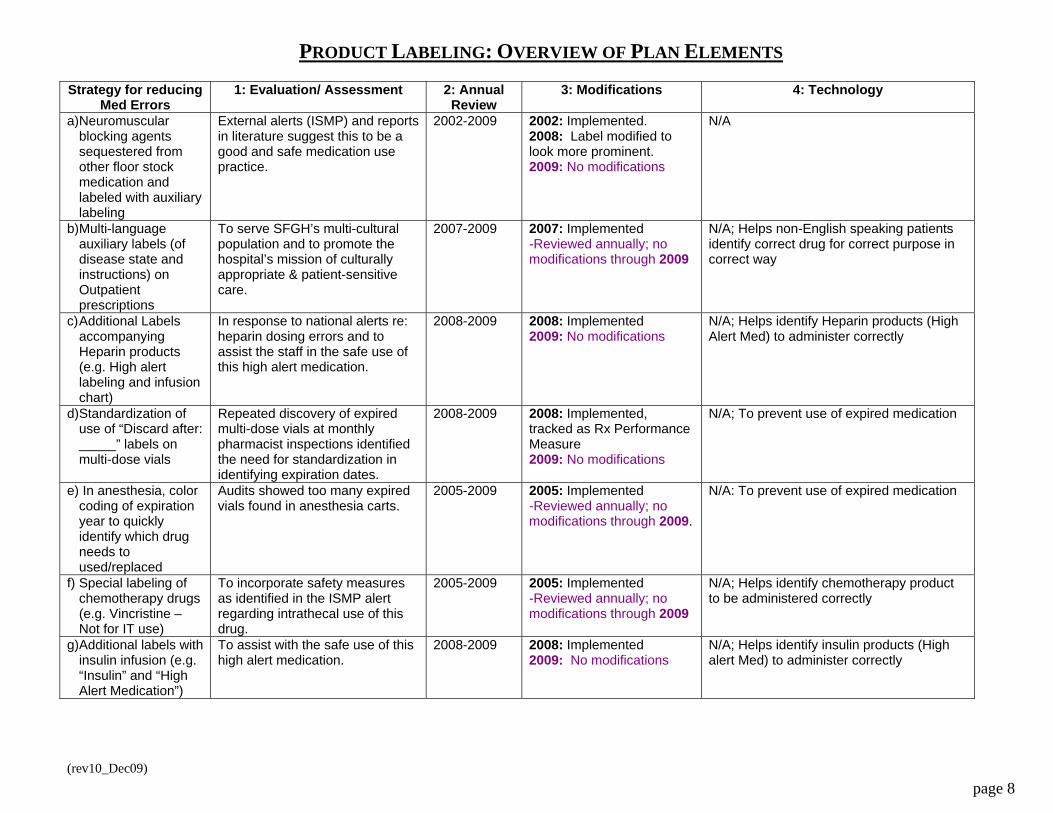
PRODUCT LABELING: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Neuromuscular blocking agents sequestered from other floor stock medication and labeled with auxiliary labeling
External alerts (ISMP) and reports in literature suggest this to be a good and safe medication use practice.
2002-2009 2002: Implemented. 2008: Label modified to look more prominent. 2009: No modifications
N/A
b) Multi-language auxiliary labels (of disease state and instructions) on Outpatient prescriptions
To serve SFGH’s multi-cultural population and to promote the hospital’s mission of culturally appropriate & patient-sensitive care.
2007-2009 2007: Implemented -Reviewed annually; no modifications through 2009
N/A; Helps non-English speaking patients identify correct drug for correct purpose in correct way
c) Additional Labels accompanying Heparin products (e.g. High alert labeling and infusion chart)
In response to national alerts re: heparin dosing errors and to assist the staff in the safe use of this high alert medication.
2008-2009 2008: Implemented 2009: No modifications
N/A; Helps identify Heparin products (High Alert Med) to administer correctly
d) Standardization of use of “Discard after: _____” labels on multi-dose vials
Repeated discovery of expired multi-dose vials at monthly pharmacist inspections identified the need for standardization in identifying expiration dates.
2008-2009 2008: Implemented, tracked as Rx Performance Measure 2009: No modifications
N/A; To prevent use of expired medication
e) In anesthesia, color coding of expiration year to quickly identify which drug needs to used/replaced
Audits showed too many expired vials found in anesthesia carts.
2005-2009 2005: Implemented -Reviewed annually; no modifications through 2009.
N/A: To prevent use of expired medication
f) Special labeling of chemotherapy drugs (e.g. Vincristine – Not for IT use)
To incorporate safety measures as identified in the ISMP alert regarding intrathecal use of this drug.
2005-2009 2005: Implemented -Reviewed annually; no modifications through 2009
N/A; Helps identify chemotherapy product to be administered correctly
g) Additional labels with insulin infusion (e.g. “Insulin” and “High Alert Medication”)
To assist with the safe use of this high alert medication.
2008-2009 2008: Implemented 2009: No modifications
N/A; Helps identify insulin products (High alert Med) to administer correctly
(rev10_Dec09) page 9
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
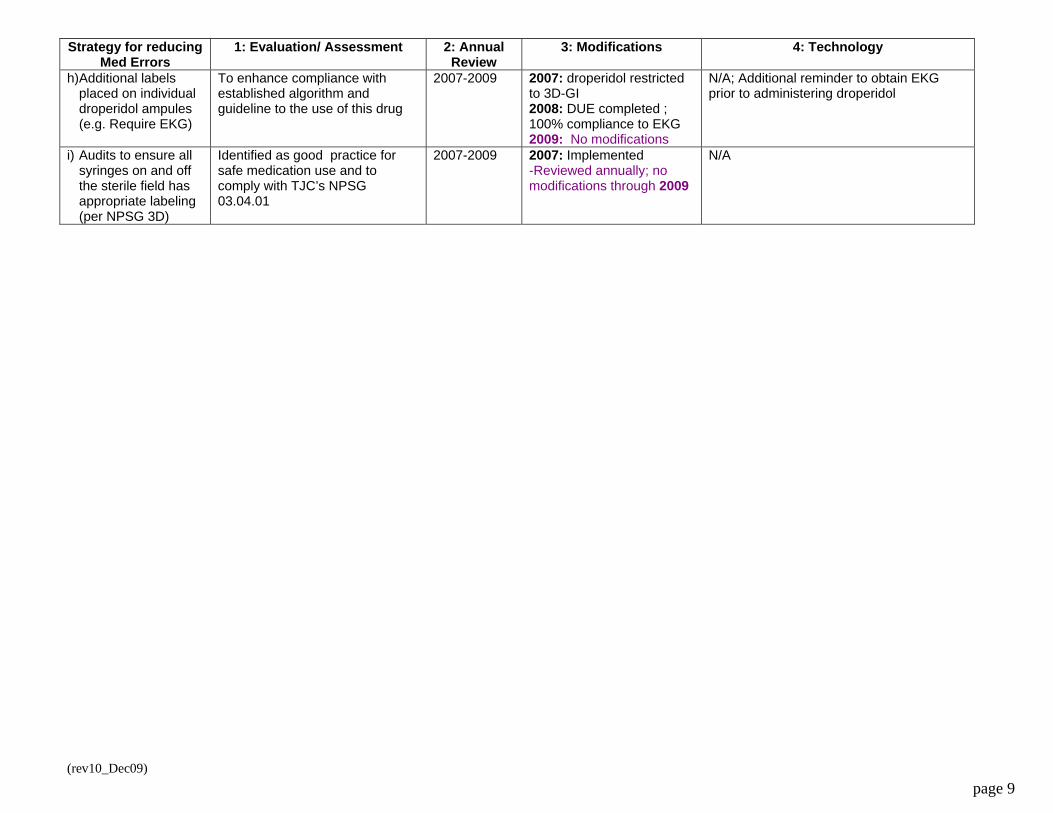
h) Additional labels placed on individual droperidol ampules (e.g. Require EKG)
To enhance compliance with established algorithm and guideline to the use of this drug
2007-2009 2007: droperidol restricted to 3D-GI 2008: DUE completed ; 100% compliance to EKG 2009: No modifications
N/A; Additional reminder to obtain EKG prior to administering droperidol
i) Audits to ensure all syringes on and off the sterile field has appropriate labeling (per NPSG 3D)
Identified as good practice for safe medication use and to comply with TJC’s NPSG 03.04.01
2007-2009 2007: Implemented -Reviewed annually; no modifications through 2009
N/A
(rev10_Dec09) page 10
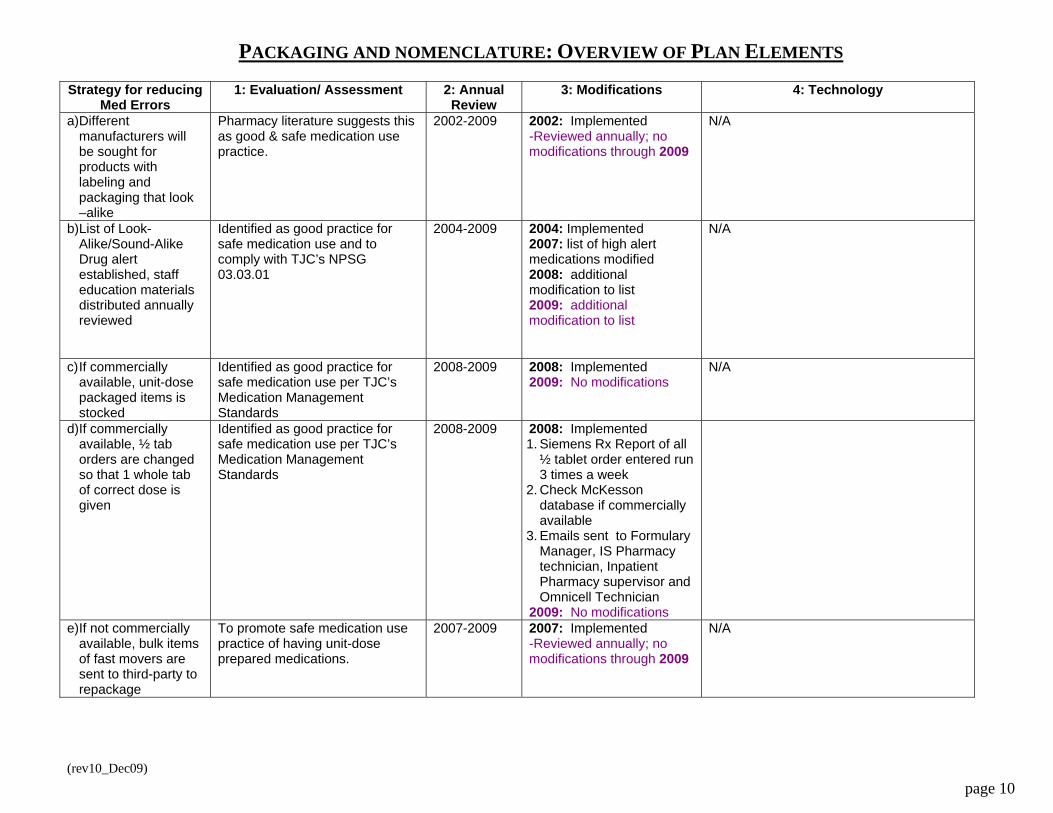
PACKAGING AND NOMENCLATURE: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Different manufacturers will be sought for products with labeling and packaging that look –alike
Pharmacy literature suggests this as good & safe medication use practice.
2002-2009 2002: Implemented -Reviewed annually; no modifications through 2009
N/A
b) List of Look-Alike/Sound-Alike Drug alert established, staff education materials distributed annually reviewed
Identified as good practice for safe medication use and to comply with TJC’s NPSG 03.03.01
2004-2009 2004: Implemented 2007: list of high alert medications modified 2008: additional modification to list 2009: additional modification to list
N/A
c) If commercially available, unit-dose packaged items is stocked
Identified as good practice for safe medication use per TJC’s Medication Management Standards
2008-2009 2008: Implemented 2009: No modifications
N/A
d) If commercially available, ½ tab orders are changed so that 1 whole tab of correct dose is given
Identified as good practice for safe medication use per TJC’s Medication Management Standards
2008-2009 2008: Implemented 1. Siemens Rx Report of all
½ tablet order entered run 3 times a week
2. Check McKesson database if commercially available
3. Emails sent to Formulary Manager, IS Pharmacy technician, Inpatient Pharmacy supervisor and Omnicell Technician
2009: No modifications
e) If not commercially available, bulk items of fast movers are sent to third-party to repackage
To promote safe medication use practice of having unit-dose prepared medications.
2007-2009 2007: Implemented -Reviewed annually; no modifications through 2009
N/A

(rev10_Dec09) page 11
COMPOUNDING: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Triage phone calls to pharmacy IV preparation area and forward only when necessary
Interruption is known to increase potential for medication errors. Practice changed to minimize interruption.
2002-2009 2002: Implemented -Reviewed annually; no modifications through 2009
N/A
b) Install direct fax line to IVAC area for IVAC orders
To streamline workflow in IV preparation and to improve turnaround time.
2004-2009 2004: Implemented -Reviewed annually; no modifications through 2009
Direct Fax line to IVAC eliminates potential for missed orders or delay in orders; allows for IVAC pharmacist to follow critically ill patient’s parenteral needs
c) Compliance to USP 797 Regulations
USP 797 gap analysis performed to identify areas for improvement.
2005-2009 2005: Implemented 2006: Installation of MIC 2007: P&P’s changed to comply with USP regulations 2008: Additional changes to P&Ps 2009: Hospital Rebuild plan incorporates automated compounding & clean room
N/A
d) Concentrations are standardized for Adults/Neonates
Identified as good practice for safe medication use per TJC’s Medication Management Standards and other patient safety literature.
2002-2009 2002: Implemented prior to 2002 2008: Implemented in neonates 2009: Weight-based std concentration worksheet for neonates for Rx and Nursing to double check orders & calculations; All neonate IV orders (except emergency & drugs w/short stability) are mixed by Pharmacy
Posted on Hospital Intranet
e) In Anesthesia, intubation syringes for the medication module of their intubation kits are no longer made in advance by their residents.
Identified as good practice for safe medication use per TJC’s Medication Management Standards and USP 797.
2007-2009 2007: Inpatient IVAC Pharmacy prepares syringes for anesthesia 2008: Switched to commercially available premixed syringes 2009: No modifications
N/A
(rev10_Dec09) page 12
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
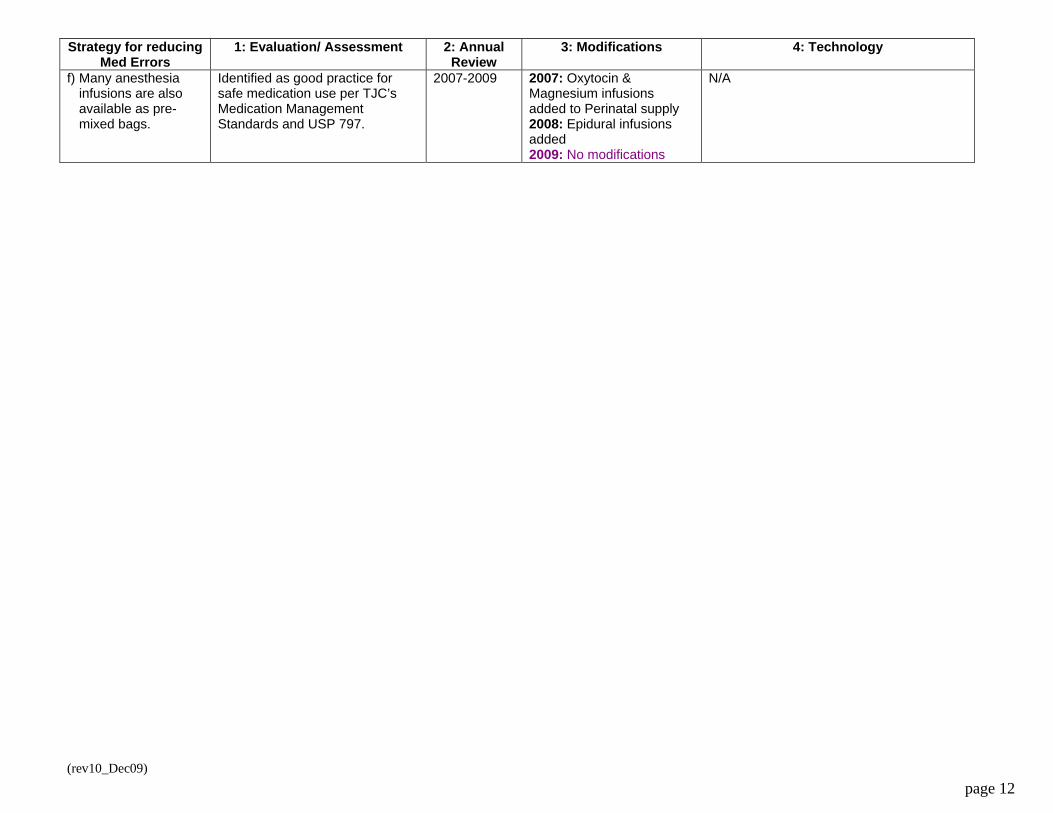
f) Many anesthesia infusions are also available as pre-mixed bags.
Identified as good practice for safe medication use per TJC’s Medication Management Standards and USP 797.
2007-2009 2007: Oxytocin & Magnesium infusions added to Perinatal supply 2008: Epidural infusions added 2009: No modifications
N/A
(rev10_Dec09) page 13
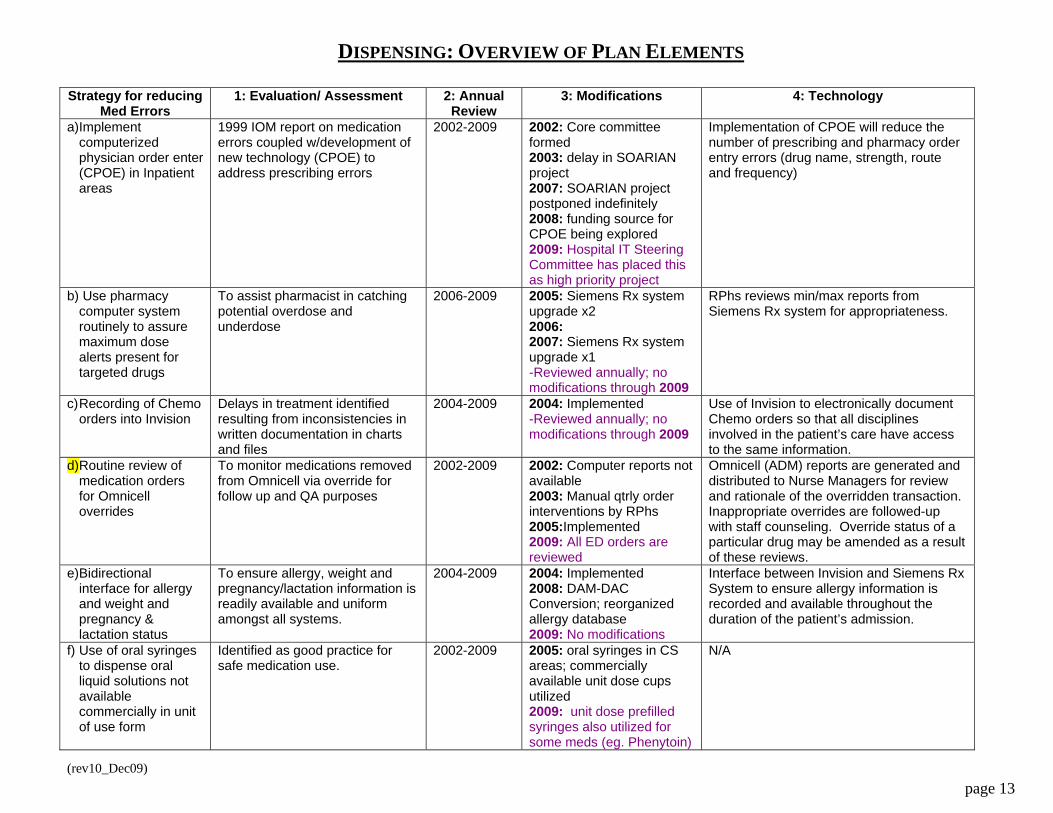
DISPENSING: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Implement computerized physician order enter (CPOE) in Inpatient areas
1999 IOM report on medication errors coupled w/development of new technology (CPOE) to address prescribing errors
2002-2009 2002: Core committee formed 2003: delay in SOARIAN project 2007: SOARIAN project postponed indefinitely 2008: funding source for CPOE being explored 2009: Hospital IT Steering Committee has placed this as high priority project
Implementation of CPOE will reduce the number of prescribing and pharmacy order entry errors (drug name, strength, route and frequency)
b) Use pharmacy computer system routinely to assure maximum dose alerts present for targeted drugs
To assist pharmacist in catching potential overdose and underdose
2006-2009 2005: Siemens Rx system upgrade x2 2006: 2007: Siemens Rx system upgrade x1 -Reviewed annually; no modifications through 2009
RPhs reviews min/max reports from Siemens Rx system for appropriateness.
c) Recording of Chemo orders into Invision
Delays in treatment identified resulting from inconsistencies in written documentation in charts and files
2004-2009 2004: Implemented -Reviewed annually; no modifications through 2009
Use of Invision to electronically document Chemo orders so that all disciplines involved in the patient’s care have access to the same information.
d) Routine review of medication orders for Omnicell overrides
To monitor medications removed from Omnicell via override for follow up and QA purposes
2002-2009 2002: Computer reports not available 2003: Manual qtrly order interventions by RPhs 2005:Implemented 2009: All ED orders are reviewed
Omnicell (ADM) reports are generated and distributed to Nurse Managers for review and rationale of the overridden transaction. Inappropriate overrides are followed-up with staff counseling. Override status of a particular drug may be amended as a result of these reviews.
e) Bidirectional interface for allergy and weight and pregnancy & lactation status
To ensure allergy, weight and pregnancy/lactation information is readily available and uniform amongst all systems.
2004-2009 2004: Implemented 2008: DAM-DAC Conversion; reorganized allergy database 2009: No modifications
Interface between Invision and Siemens Rx System to ensure allergy information is recorded and available throughout the duration of the patient’s admission.
f) Use of oral syringes to dispense oral liquid solutions not available commercially in unit of use form
Identified as good practice for safe medication use.
2002-2009 2005: oral syringes in CS areas; commercially available unit dose cups utilized 2009: unit dose prefilled syringes also utilized for some meds (eg. Phenytoin)
N/A
(rev10_Dec09) page 14
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
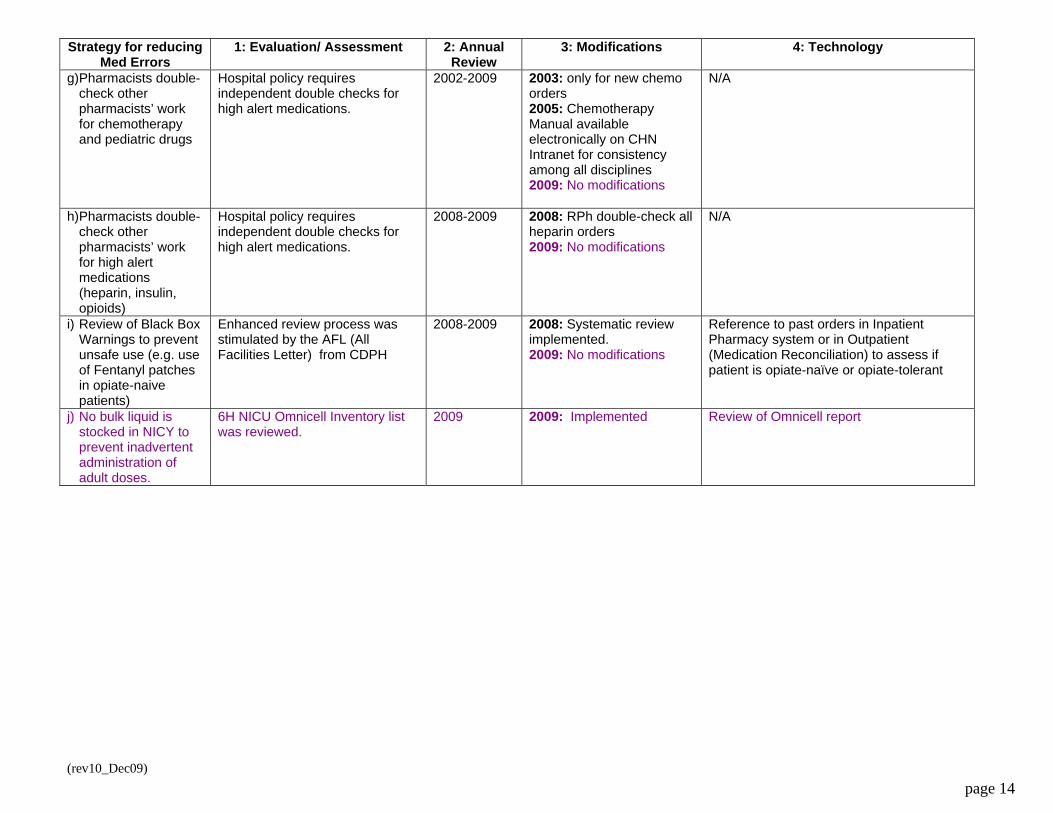
g) Pharmacists double-check other pharmacists’ work for chemotherapy and pediatric drugs
Hospital policy requires independent double checks for high alert medications.
2002-2009 2003: only for new chemo orders 2005: Chemotherapy Manual available electronically on CHN Intranet for consistency among all disciplines 2009: No modifications
N/A
h) Pharmacists double-check other pharmacists’ work for high alert medications (heparin, insulin, opioids)
Hospital policy requires independent double checks for high alert medications.
2008-2009 2008: RPh double-check all heparin orders 2009: No modifications
N/A
i) Review of Black Box Warnings to prevent unsafe use (e.g. use of Fentanyl patches in opiate-naive patients)
Enhanced review process was stimulated by the AFL (All Facilities Letter) from CDPH
2008-2009 2008: Systematic review implemented. 2009: No modifications
Reference to past orders in Inpatient Pharmacy system or in Outpatient (Medication Reconciliation) to assess if patient is opiate-naïve or opiate-tolerant
j) No bulk liquid is stocked in NICY to prevent inadvertent administration of adult doses.
6H NICU Omnicell Inventory list was reviewed.
2009 2009: Implemented Review of Omnicell report
(re 9) page 15
v10_Dec0
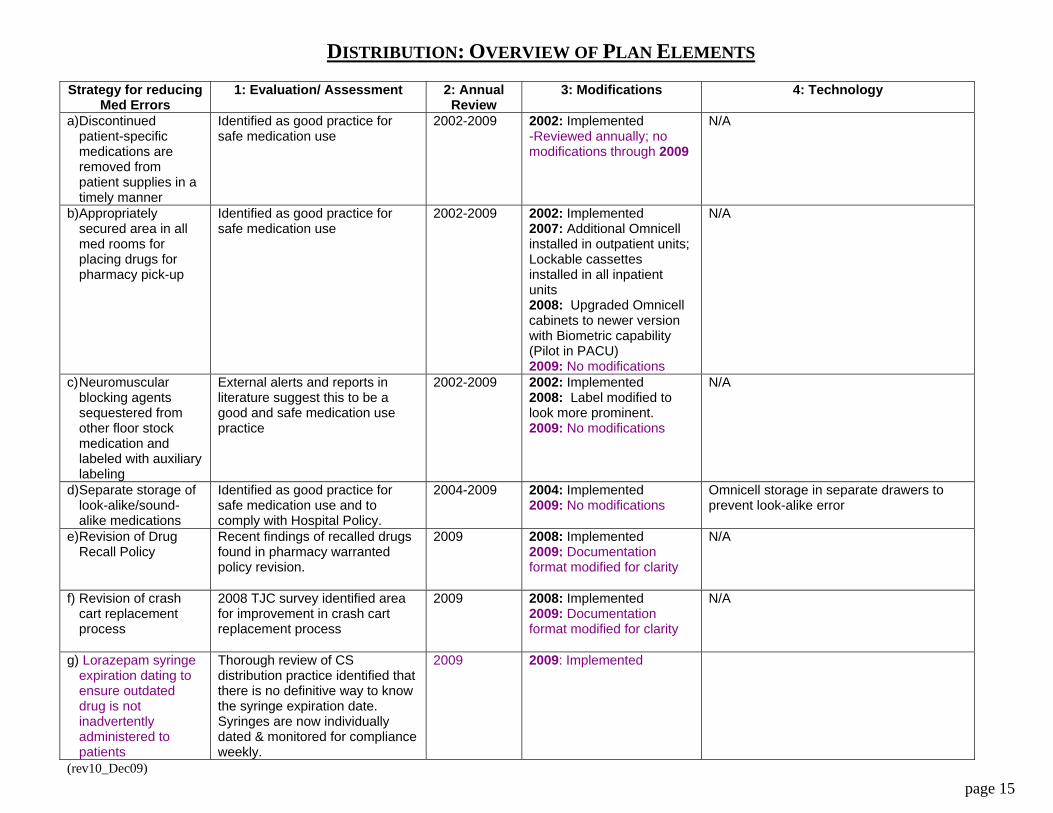
DISTRIBUTION: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Discontinued patient-specific medications are removed from patient supplies in a timely manner
Identified as good practice for safe medication use
2002-2009 2002: Implemented -Reviewed annually; no modifications through 2009
N/A
b) Appropriately secured area in all med rooms for placing drugs for pharmacy pick-up
Identified as good practice for safe medication use
2002-2009 2002: Implemented 2007: Additional Omnicell installed in outpatient units; Lockable cassettes installed in all inpatient units 2008: Upgraded Omnicell cabinets to newer version with Biometric capability (Pilot in PACU) 2009: No modifications
N/A
c) Neuromuscular blocking agents sequestered from other floor stock medication and labeled with auxiliary labeling
External alerts and reports in literature suggest this to be a good and safe medication use practice
2002-2009 2002: Implemented 2008: Label modified to look more prominent. 2009: No modifications
N/A
d) Separate storage of look-alike/sound-alike medications
Identified as good practice for safe medication use and to comply with Hospital Policy.
2004-2009 2004: Implemented 2009: No modifications
Omnicell storage in separate drawers to prevent look-alike error
e) Revision of Drug Recall Policy
Recent findings of recalled drugs found in pharmacy warranted policy revision.
2009 2008: Implemented 2009: Documentation format modified for clarity
N/A
f) Revision of crash cart replacement process
2008 TJC survey identified area for improvement in crash cart replacement process
2009 2008: Implemented 2009: Documentation format modified for clarity
N/A
g) Lorazepam syringe expiration dating to ensure outdated drug is not inadvertently administered to patients
Thorough review of CS distribution practice identified that there is no definitive way to know the syringe expiration date. Syringes are now individually dated & monitored for compliance weekly.
2009 2009: Implemented
(rev10_Dec09) page 16
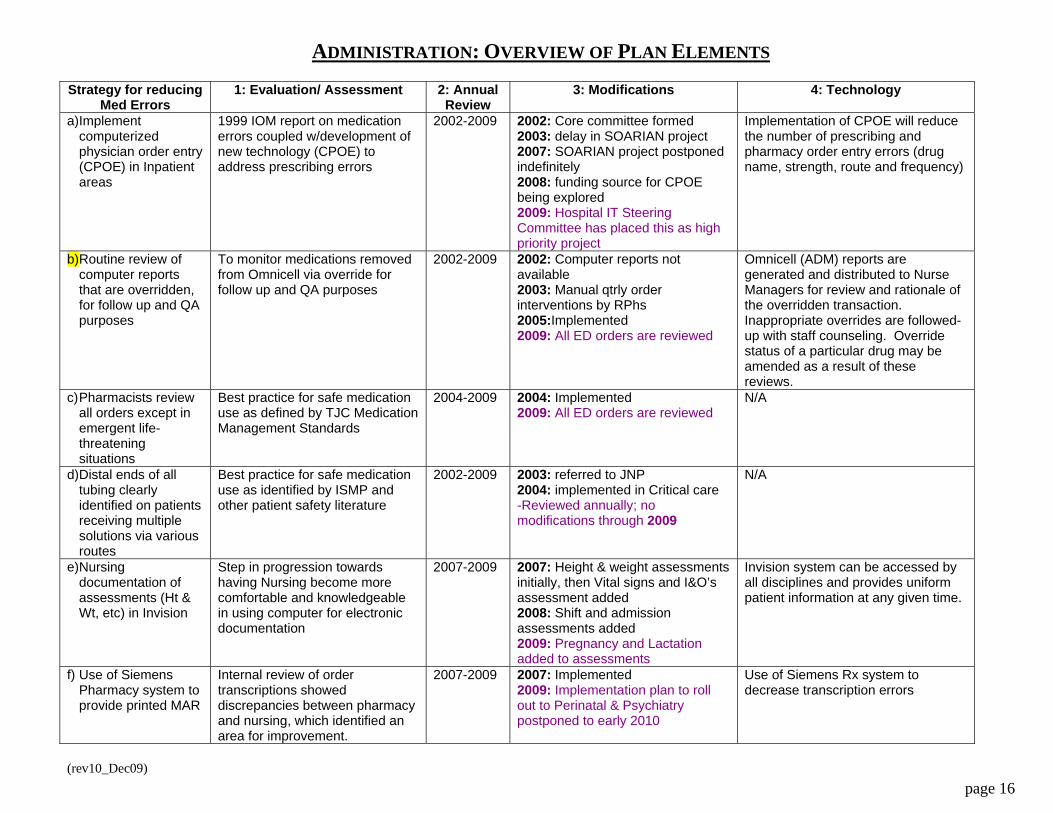
ADMINISTRATION: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Implement computerized physician order entry (CPOE) in Inpatient areas
1999 IOM report on medication errors coupled w/development of new technology (CPOE) to address prescribing errors
2002-2009 2002: Core committee formed 2003: delay in SOARIAN project 2007: SOARIAN project postponed indefinitely 2008: funding source for CPOE being explored 2009: Hospital IT Steering Committee has placed this as high priority project
Implementation of CPOE will reduce the number of prescribing and pharmacy order entry errors (drug name, strength, route and frequency)
b) Routine review of computer reports that are overridden, for follow up and QA purposes
To monitor medications removed from Omnicell via override for follow up and QA purposes
2002-2009 2002: Computer reports not available 2003: Manual qtrly order interventions by RPhs 2005:Implemented 2009: All ED orders are reviewed
Omnicell (ADM) reports are generated and distributed to Nurse Managers for review and rationale of the overridden transaction. Inappropriate overrides are followed-up with staff counseling. Override status of a particular drug may be amended as a result of these reviews.
c) Pharmacists review all orders except in emergent life-threatening situations
Best practice for safe medication use as defined by TJC Medication Management Standards
2004-2009 2004: Implemented 2009: All ED orders are reviewed
N/A
d) Distal ends of all tubing clearly identified on patients receiving multiple solutions via various routes
Best practice for safe medication use as identified by ISMP and other patient safety literature
2002-2009 2003: referred to JNP 2004: implemented in Critical care -Reviewed annually; no modifications through 2009
N/A
e) Nursing documentation of assessments (Ht & Wt, etc) in Invision
Step in progression towards having Nursing become more comfortable and knowledgeable in using computer for electronic documentation
2007-2009 2007: Height & weight assessments initially, then Vital signs and I&O’s assessment added 2008: Shift and admission assessments added 2009: Pregnancy and Lactation added to assessments
Invision system can be accessed by all disciplines and provides uniform patient information at any given time.
f) Use of Siemens Pharmacy system to provide printed MAR
Internal review of order transcriptions showed discrepancies between pharmacy and nursing, which identified an area for improvement.
2007-2009 2007: Implemented 2009: Implementation plan to roll out to Perinatal & Psychiatry postponed to early 2010
Use of Siemens Rx system to decrease transcription errors
(rev10_Dec09) page 17
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
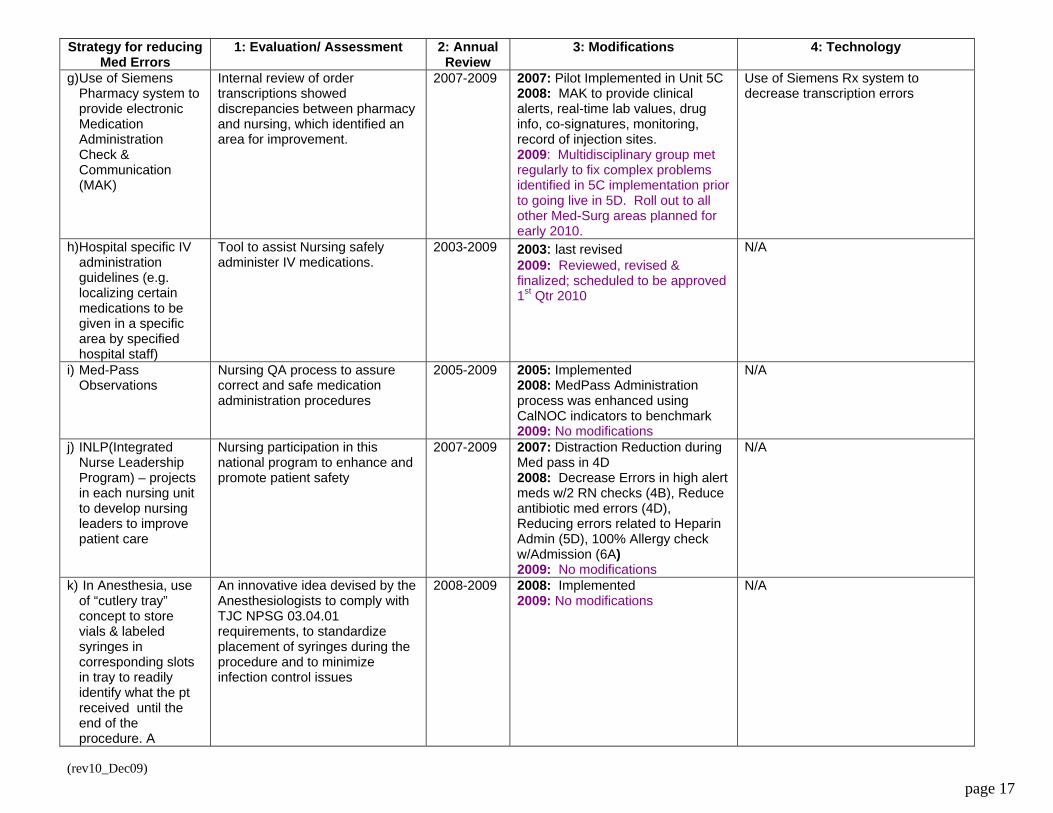
g) Use of Siemens Pharmacy system to provide electronic Medication Administration Check & Communication (MAK)
Internal review of order transcriptions showed discrepancies between pharmacy and nursing, which identified an area for improvement.
2007-2009 2007: Pilot Implemented in Unit 5C 2008: MAK to provide clinical alerts, real-time lab values, drug info, co-signatures, monitoring, record of injection sites. 2009: Multidisciplinary group met regularly to fix complex problems identified in 5C implementation prior to going live in 5D. Roll out to all other Med-Surg areas planned for early 2010.
Use of Siemens Rx system to decrease transcription errors
h) Hospital specific IV administration guidelines (e.g. localizing certain medications to be given in a specific area by specified hospital staff)
Tool to assist Nursing safely administer IV medications.
2003-2009 2003: last revised 2009: Reviewed, revised & finalized; scheduled to be approved 1st Qtr 2010
N/A
i) Med-Pass Observations
Nursing QA process to assure correct and safe medication administration procedures
2005-2009 2005: Implemented 2008: MedPass Administration process was enhanced using CalNOC indicators to benchmark 2009: No modifications
N/A
j) INLP(Integrated Nurse Leadership Program) – projects in each nursing unit to develop nursing leaders to improve patient care
Nursing participation in this national program to enhance and promote patient safety
2007-2009 2007: Distraction Reduction during Med pass in 4D 2008: Decrease Errors in high alert meds w/2 RN checks (4B), Reduce antibiotic med errors (4D), Reducing errors related to Heparin Admin (5D), 100% Allergy check w/Admission (6A) 2009: No modifications
N/A
k) In Anesthesia, use of “cutlery tray” concept to store vials & labeled syringes in corresponding slots in tray to readily identify what the pt received until the end of the procedure. A
An innovative idea devised by the Anesthesiologists to comply with TJC NPSG 03.04.01 requirements, to standardize placement of syringes during the procedure and to minimize infection control issues
2008-2009 2008: Implemented 2009: No modifications
N/A
(rev10_Dec09) page 18
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
separate tray was also instituted to separate “in use” from”used” syringes.
(rev10_Dec09) page 19
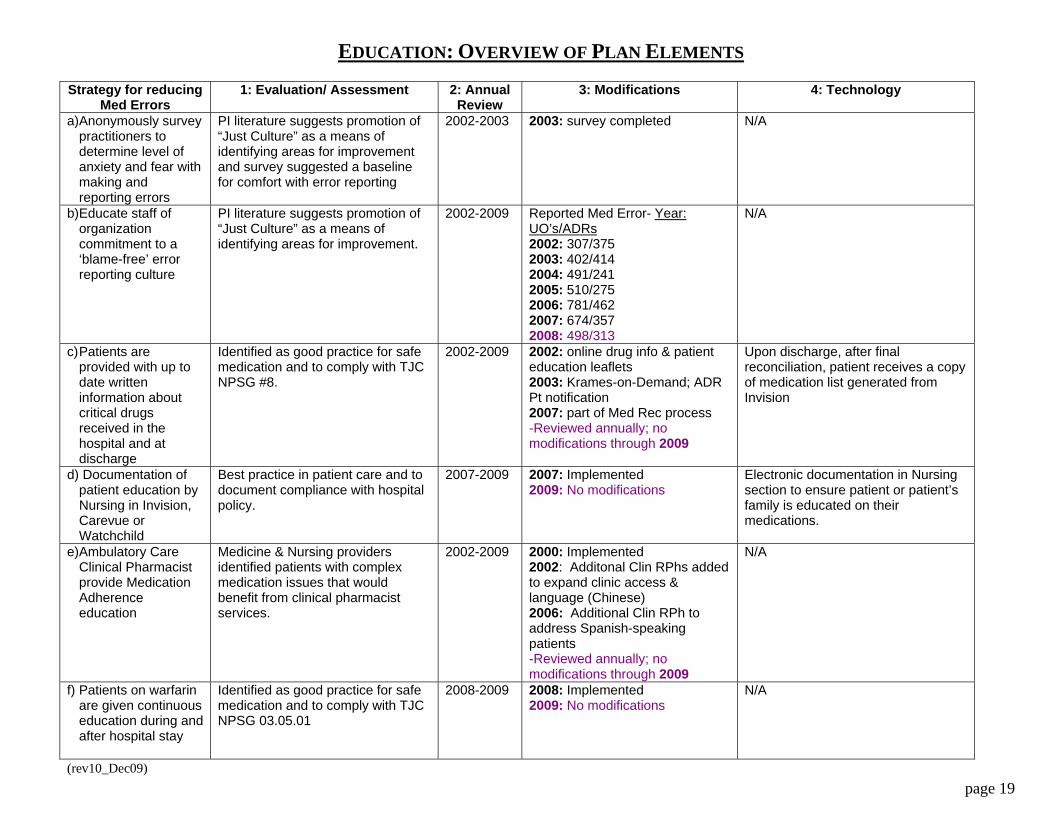
EDUCATION: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Anonymously survey practitioners to determine level of anxiety and fear with making and reporting errors
PI literature suggests promotion of “Just Culture” as a means of identifying areas for improvement and survey suggested a baseline for comfort with error reporting
2002-2003 2003: survey completed N/A
b) Educate staff of organization commitment to a ‘blame-free’ error reporting culture
PI literature suggests promotion of “Just Culture” as a means of identifying areas for improvement.
2002-2009 Reported Med Error- Year: UO’s/ADRs2002: 307/375 2003: 402/414 2004: 491/241 2005: 510/275 2006: 781/462 2007: 674/357 2008: 498/313
N/A
c) Patients are provided with up to date written information about critical drugs received in the hospital and at discharge
Identified as good practice for safe medication and to comply with TJC NPSG #8.
2002-2009 2002: online drug info & patient education leaflets 2003: Krames-on-Demand; ADR Pt notification 2007: part of Med Rec process -Reviewed annually; no modifications through 2009
Upon discharge, after final reconciliation, patient receives a copy of medication list generated from Invision
d) Documentation of patient education by Nursing in Invision, Carevue or Watchchild
Best practice in patient care and to document compliance with hospital policy.
2007-2009 2007: Implemented 2009: No modifications
Electronic documentation in Nursing section to ensure patient or patient’s family is educated on their medications.
e) Ambulatory Care Clinical Pharmacist provide Medication Adherence education
Medicine & Nursing providers identified patients with complex medication issues that would benefit from clinical pharmacist services.
2002-2009 2000: Implemented 2002: Additonal Clin RPhs added to expand clinic access & language (Chinese) 2006: Additional Clin RPh to address Spanish-speaking patients -Reviewed annually; no modifications through 2009
N/A
f) Patients on warfarin are given continuous education during and after hospital stay
Identified as good practice for safe medication and to comply with TJC NPSG 03.05.01
2008-2009 2008: Implemented 2009: No modifications
N/A
(rev10_Dec09) page 20
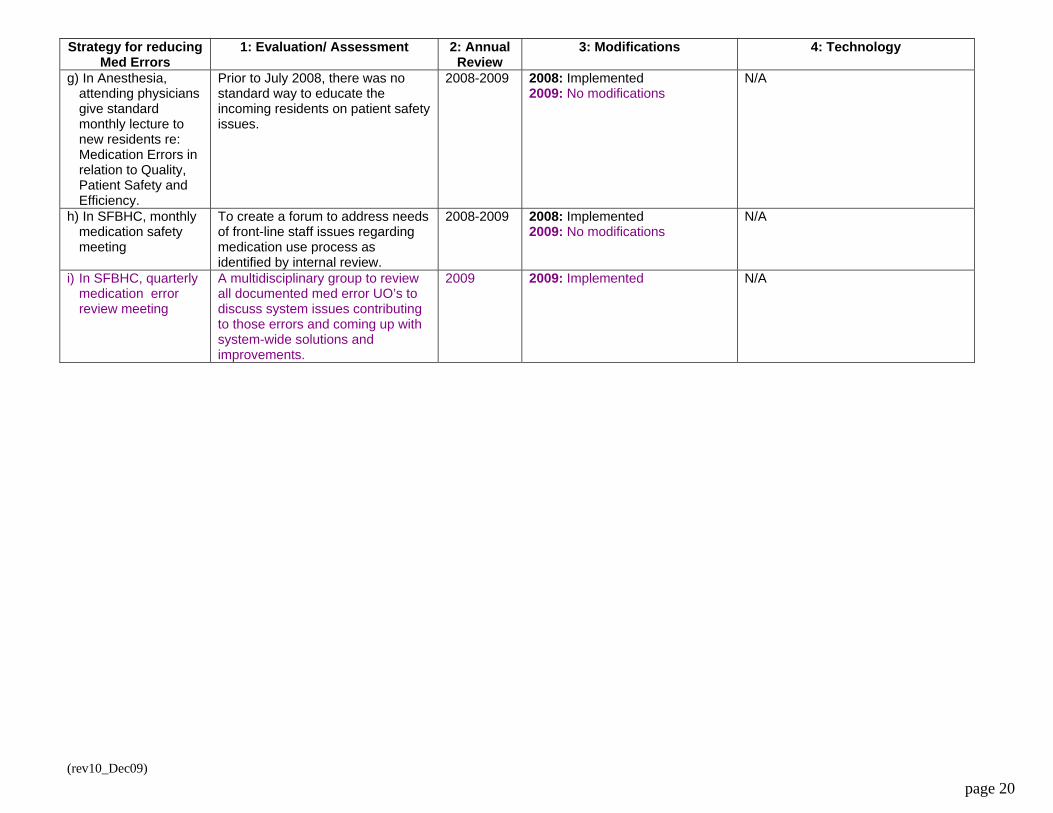
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
g) In Anesthesia, attending physicians give standard monthly lecture to new residents re: Medication Errors in relation to Quality, Patient Safety and Efficiency.
Prior to July 2008, there was no standard way to educate the incoming residents on patient safety issues.
2008-2009 2008: Implemented 2009: No modifications
N/A
h) In SFBHC, monthly medication safety meeting
To create a forum to address needs of front-line staff issues regarding medication use process as identified by internal review.
2008-2009 2008: Implemented 2009: No modifications
N/A
i) In SFBHC, quarterly medication error review meeting
A multidisciplinary group to review all documented med error UO’s to discuss system issues contributing to those errors and coming up with system-wide solutions and improvements.
2009 2009: Implemented N/A

(rev10_Dec09) page 21
MONITORING: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Medication Reconciliation process to prevent Adverse Events and to include patients whenever possible: Taskforce consists of physicians, nurses, IT and pharmacy meet bimonthly; training for MD by MDs
Patient Safety & Quality literature suggests medication reconciliation as one of many safe practices for better patient care. It is also one of The Joint Commission’s National Patient Safety Goals (TJC-NPSG #8) to improve communication of patient medication information throughout the continuum of care
2005-2009 2005: Pilot implemented 2007: Full implementation completed. 2007: ED Med rec form created 2007: OR Med Rec process implemented 2008: Home Med List function in Nursing Admission Database 2008: Improved formatting & nomenclature changes to printed forms & Invision function buttons 2009: No modifications
Invision system can be accessed by all disciplines. Orders are sent to Invision directly from Siemens Pharmacy system. Medication Reconciliation instructions are also posted on Invision for all disciplines to access as necessary.
b) The Medication Use and Safety Subcommittee, a multi-disciplinary group, analyzes and uses error experiences from other organizations to target improvements.
Hospital’s established body to review and evaluate all aspects of the medication use process to assure safety and compliance to all regulatory standards.
2002-2009 In existence before 2002. 2009: Committee charge and goal redefined to focus on MERP directives and membership expanded to ensure all areas w/medication use are represented.
N/A
c) A drug use evaluation study is initiated immediately after adding a drug identified as having high error potential to the formulary
Good practice for safe medication use and augments drug safety review portion of the formulary review process.
2002-2009 2002: Implemented 2009: Expectation of One DUE per clinical pharmacist per fiscal year established.
N/A
d) Review Black Box Warnings to ensure safe use (e.g. monitoring Hgb levels when patient is receiving epogen)
Enhanced review process was stimulated by the AFL (All Facilities Letter) from CDPH
2008-2009 2008: Systematic review implemented. 2009: No modifications
Lab values interface into Siemens Pharmacy system to ensure safe use
(rev10_Dec09) page 22
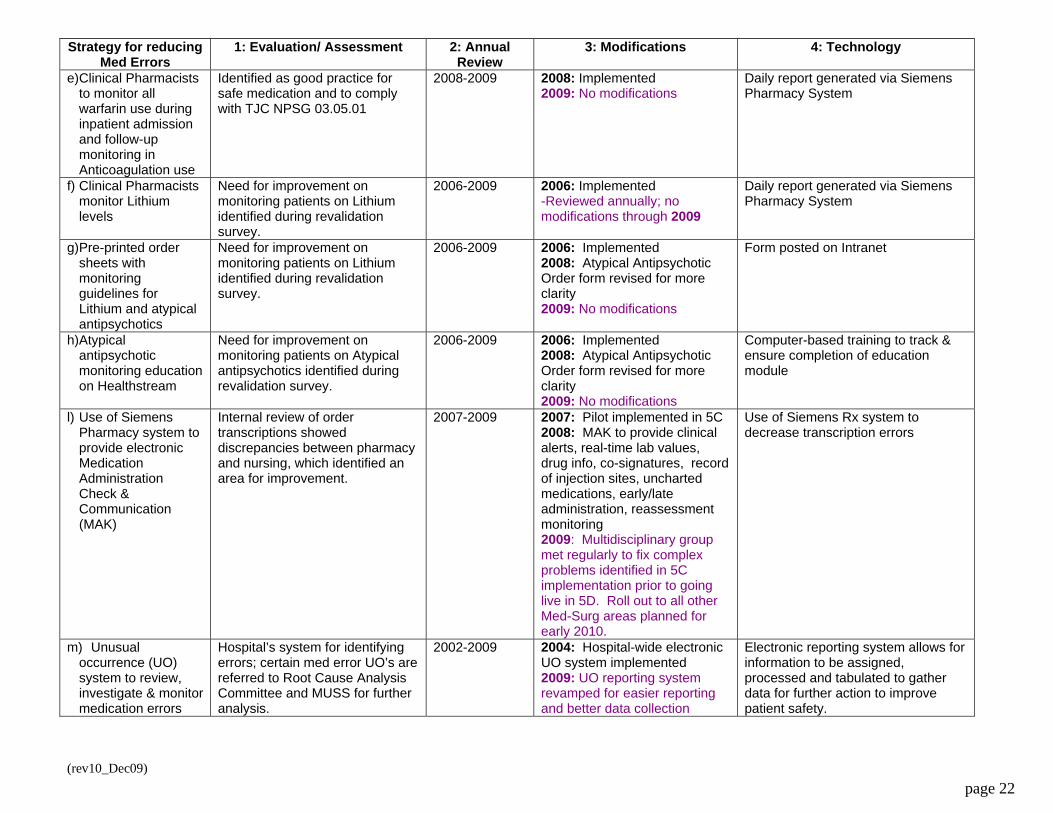
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
e) Clinical Pharmacists to monitor all warfarin use during inpatient admission and follow-up monitoring in Anticoagulation use
Identified as good practice for safe medication and to comply with TJC NPSG 03.05.01
2008-2009 2008: Implemented 2009: No modifications
Daily report generated via Siemens Pharmacy System
f) Clinical Pharmacists monitor Lithium levels
Need for improvement on monitoring patients on Lithium identified during revalidation survey.
2006-2009 2006: Implemented -Reviewed annually; no modifications through 2009
Daily report generated via Siemens Pharmacy System
g) Pre-printed order sheets with monitoring guidelines for Lithium and atypical antipsychotics
Need for improvement on monitoring patients on Lithium identified during revalidation survey.
2006-2009 2006: Implemented 2008: Atypical Antipsychotic Order form revised for more clarity 2009: No modifications
Form posted on Intranet
h) Atypical antipsychotic monitoring education on Healthstream
Need for improvement on monitoring patients on Atypical antipsychotics identified during revalidation survey.
2006-2009 2006: Implemented 2008: Atypical Antipsychotic Order form revised for more clarity 2009: No modifications
Computer-based training to track & ensure completion of education module
l) Use of Siemens Pharmacy system to provide electronic Medication Administration Check & Communication (MAK)
Internal review of order transcriptions showed discrepancies between pharmacy and nursing, which identified an area for improvement.
2007-2009 2007: Pilot implemented in 5C 2008: MAK to provide clinical alerts, real-time lab values, drug info, co-signatures, record of injection sites, uncharted medications, early/late administration, reassessment monitoring 2009: Multidisciplinary group met regularly to fix complex problems identified in 5C implementation prior to going live in 5D. Roll out to all other Med-Surg areas planned for early 2010.
Use of Siemens Rx system to decrease transcription errors
m) Unusual occurrence (UO) system to review, investigate & monitor medication errors
Hospital’s system for identifying errors; certain med error UO’s are referred to Root Cause Analysis Committee and MUSS for further analysis.
2002-2009 2004: Hospital-wide electronic UO system implemented 2009: UO reporting system revamped for easier reporting and better data collection
Electronic reporting system allows for information to be assigned, processed and tabulated to gather data for further action to improve patient safety.
(rev10_Dec09) page 23
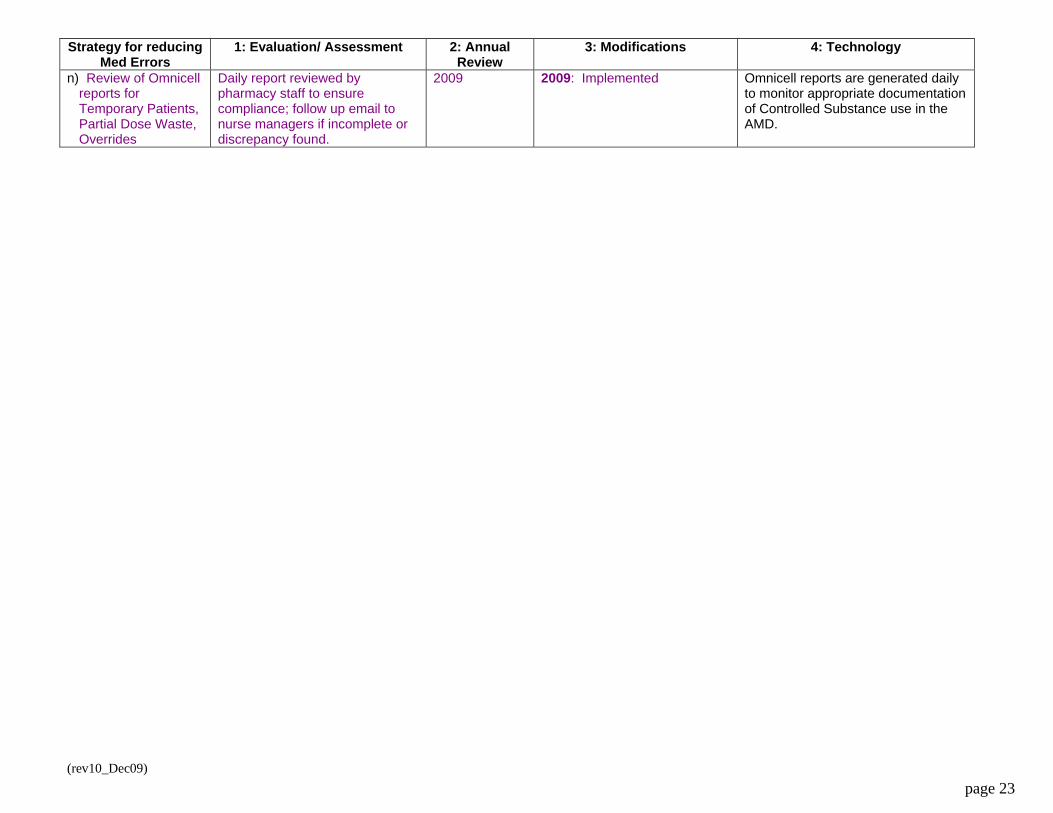
Strategy for reducing Med Errors
1: Evaluation/ Assessment 2: Annual Review
3: Modifications 4: Technology
n) Review of Omnicell reports for Temporary Patients, Partial Dose Waste, Overrides
Daily report reviewed by pharmacy staff to ensure compliance; follow up email to nurse managers if incomplete or discrepancy found.
2009 2009: Implemented Omnicell reports are generated daily to monitor appropriate documentation of Controlled Substance use in the AMD.
(rev10_Dec09) page 24
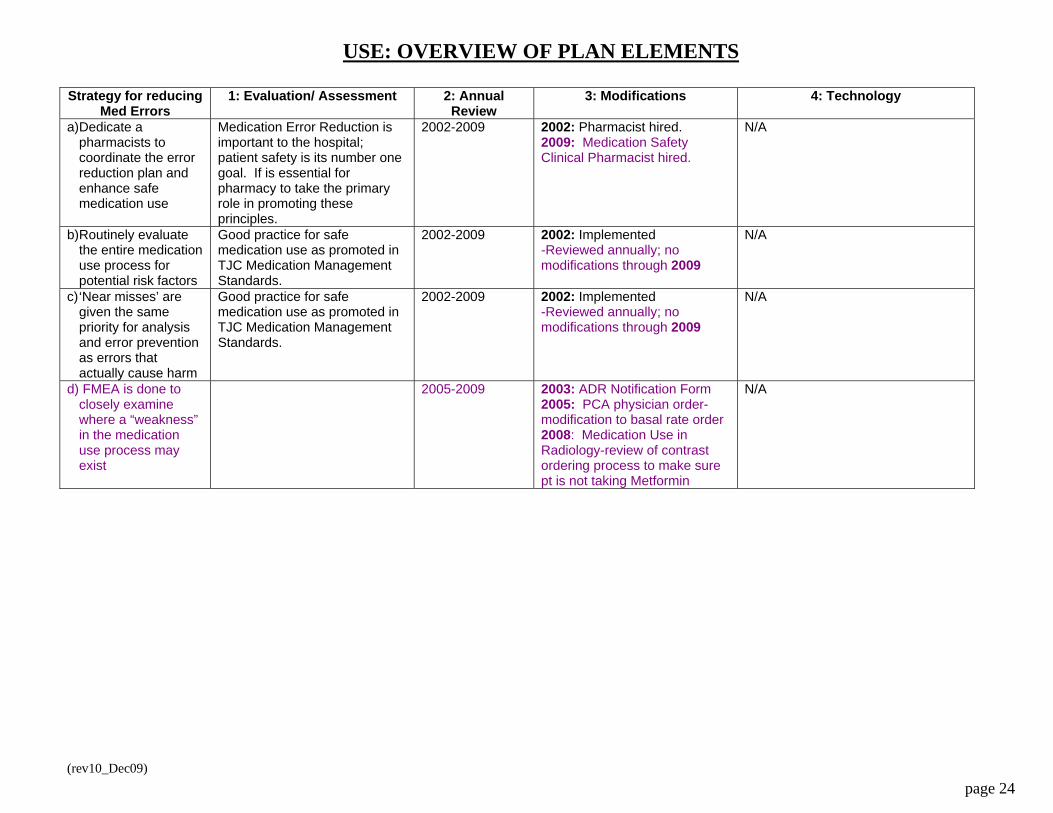
USE: OVERVIEW OF PLAN ELEMENTS Strategy for reducing
Med Errors 1: Evaluation/ Assessment 2: Annual
Review 3: Modifications 4: Technology
a) Dedicate a pharmacists to coordinate the error reduction plan and enhance safe medication use
Medication Error Reduction is important to the hospital; patient safety is its number one goal. If is essential for pharmacy to take the primary role in promoting these principles.
2002-2009 2002: Pharmacist hired. 2009: Medication Safety Clinical Pharmacist hired.
N/A
b) Routinely evaluate the entire medication use process for potential risk factors
Good practice for safe medication use as promoted in TJC Medication Management Standards.
2002-2009 2002: Implemented -Reviewed annually; no modifications through 2009
N/A
c) ‘Near misses’ are given the same priority for analysis and error prevention as errors that actually cause harm
Good practice for safe medication use as promoted in TJC Medication Management Standards.
2002-2009 2002: Implemented -Reviewed annually; no modifications through 2009
N/A
d) FMEA is done to closely examine where a “weakness” in the medication use process may exist
2005-2009 2003: ADR Notification Form 2005: PCA physician order-modification to basal rate order 2008: Medication Use in Radiology-review of contrast ordering process to make sure pt is not taking Metformin
N/A
(rev10_Dec09) page 25
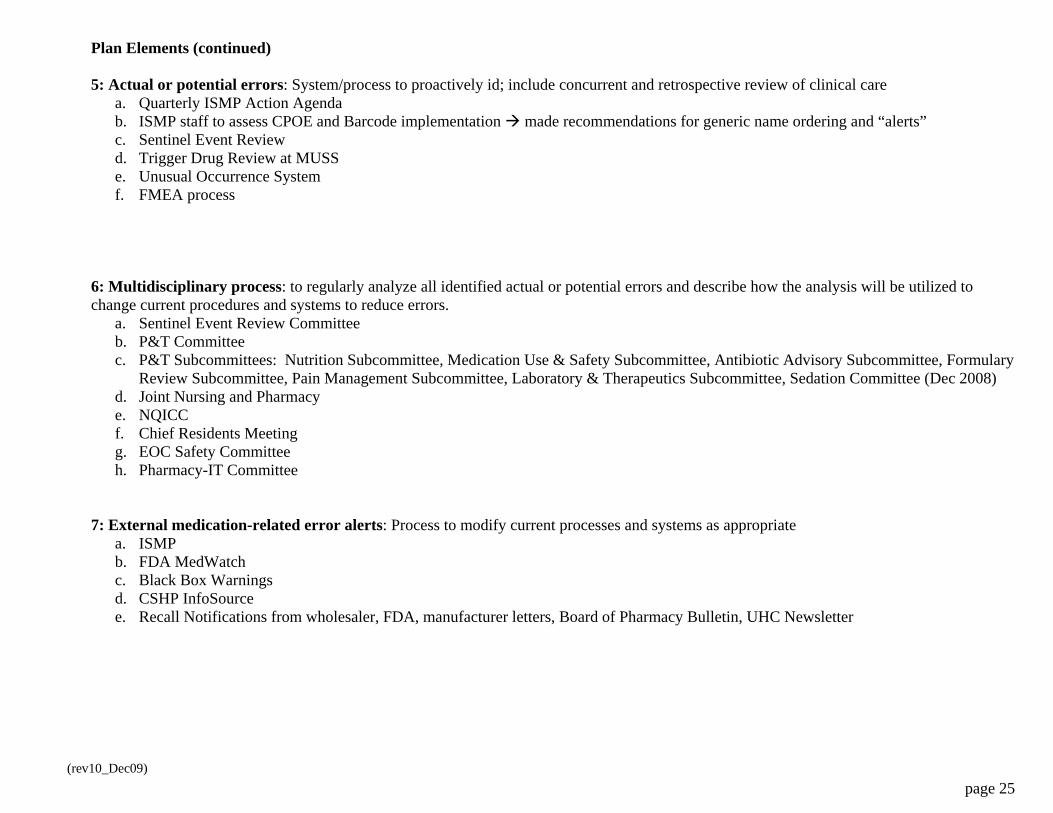
Plan Elements (continued) 5: Actual or potential errors: System/process to proactively id; include concurrent and retrospective review of clinical care
a. Quarterly ISMP Action Agenda b. ISMP staff to assess CPOE and Barcode implementation made recommendations for generic name ordering and “alerts” c. Sentinel Event Review d. Trigger Drug Review at MUSS e. Unusual Occurrence System f. FMEA process
6: Multidisciplinary process: to regularly analyze all identified actual or potential errors and describe how the analysis will be utilized to change current procedures and systems to reduce errors.
a. Sentinel Event Review Committee b. P&T Committee c. P&T Subcommittees: Nutrition Subcommittee, Medication Use & Safety Subcommittee, Antibiotic Advisory Subcommittee, Formulary
Review Subcommittee, Pain Management Subcommittee, Laboratory & Therapeutics Subcommittee, Sedation Committee (Dec 2008) d. Joint Nursing and Pharmacy e. NQICC f. Chief Residents Meeting g. EOC Safety Committee h. Pharmacy-IT Committee
7: External medication-related error alerts: Process to modify current processes and systems as appropriate a. ISMP b. FDA MedWatch c. Black Box Warnings d. CSHP InfoSource e. Recall Notifications from wholesaler, FDA, manufacturer letters, Board of Pharmacy Bulletin, UHC Newsletter