meghana doreswamy md neurology and sleep medicine september 6, 2015 management of migraine headaches...
TRANSCRIPT

MEGHANA DORESWAMY MDNEUROLOGY AND SLEEP
MEDICINESEPTEMBER 6, 2015
Management of migraine headaches in adults for primary care physician

Objectives
Diagnostic criteria and pathophysiology of migraine headache.
Epidemiology and impact of migraine headacheTreatment of acute migraine headache.Preventive therapy for migraine headaches.
.

A 32-year-old male presents with worsening headache
He has had headaches since 23, they have always been under and around eyes
He has a history of sinus trouble Headaches are associated with
photophobia/osmophobia/occasional loss of appetite
Pain is a dull pulsing pain, better with sleeping.
Diagnosis???
What type of headache is this?

Migraine vs. Sinus headache
Studies show that about 85% of people with self described sinus headaches actually have migraine headaches.
Sinus problems, like many other things trigger migraine headaches
Bottom line– the majority of headaches severe enough to cause a person to seek medical attention are Migraines
45% of migraine patients report sinus symptoms including rhinorrhea, nasal congestion and lacrimation.

Case 2
A 36 yr female presents with worsening headaches.
Started 2 years ago, occurred 2x per month, associated with N/V/photophobia/phonophobia
She has constant, background, holocephalic headache associated with continuous photophobia for three months, rated 6/10
Exacerbations- 4x /week, severe throbbing with worsened photophobia, phonophobia and nausea, last up to 24 hrs
Sumatriptan 100 mg has not been effective

Diagnosis?
Cluster headacheRebound headacheChronic migraine headacheChronic tension headache

Tension-Type Migraine
Mild
Moderate
Severe
Unilateral
Bilateral
Photophobia
Nausea
Throbbing
Pressure
Aura
Vomiting
Aggravated by Activity
© 2002 Primary Care Network
Tension-type Headache or Migraine

Dilemma in diagnosis of migraine headaches
Visual aura only 15-20% of migraineurs
Head pain can be non-throbbing in ~40% of patients
Head pain can be bilateral in ~ 43% of patients
Sinus pain and pressure, stuffiness, rhinorrhea & weather association is often present in up to 97% of migraine attacks
Neck pain is often present in up to 75% of migraine attacks

Migraine without aura
Diagnostic criteria:A. At least 5 attacks fulfilling criteria B-D B. Headache attacks lasting 4-72 hours (untreated or unsuccessfully treated) C. Headache has at least two of the following characteristics:
unilateral location pulsating quality moderate or severe pain intensity aggravation by or causing avoidance of routine physical activity (eg,
walking or climbing stairs) D. During headache at least one of the following:
nausea and/or vomiting photophobia and phonophobia
Not attributed to another disorder ICHS classification

Migraine with Aura
Diagnostic criteria:A. At least 2 attacks fulfilling criterion BB. Migraine aura fulfilling criteria B and C for one of the subforms 1.2.1-1.2.6C. Not attributed to another disorder.
Note:History and physical and neurological examinations do not suggest any of secondary disorders , or history and/or physical and/or neurological examinations do suggest such disorder but it is ruled out by appropriate investigations, or such disorder is present but attacks do not occur for the first time in close temporal relation to the disorder.

Migraine aura subforms
1.2.1 Typical aura with migraine headache1.2.2 Typical aura with non-migraine headache1.2.3 Typical aura without headache1.2.4 Familial hemiplegic migraine1.2.5 Sporadic hemiplegic migraine1.2.6 Basilar migraine

Retinal migraine
Diagnostic criteria:A. At least 2 attacks fulfilling criteria B and CB. Fully reversible monocular positive and/or negative visual phenomena (eg, scintillations, scotomata or blindness) confirmed by examination during an attack or (after proper instruction) by the patient's drawing of a monocular field defect during an attackC. Headache fulfilling criteria B-D for 1.1 .Migraine without aura begins during the visual symptoms or follows them within 60 minutesD. Normal ophthalmological examination between attacksE. Not attributed to another disorder.
Comment:Some patients who complain of monocular visual disturbance in fact have hemianopia. Other causes of transient monocular blindness (amaurosis fugax), such as optic neuropathy or carotid dissection, must be excluded.

Negative scotoma. Loss of local awareness of local structure
Positive Scotoma. Additional structures One side loss of perception.
Zigzag structure

Phases of migraine

Chronic migraine headaches
Migraine headache occurring on 15 or more days per month for more than 3 months in the absence of medication overuse.
Diagnostic criteria:Headache fulfilling criteria C and D for Migraine
without aura on ≥15 days/month for >3 monthsNot attributed to another disorder.

Figure 2. One-year period prevalence of migraine by age and sex adjusted for demographics.
R. B. Lipton et al. Neurology 2007;68:343-349
©2007 by Lippincott Williams & Wilkins

Figure 3. One-year period prevalence of migraine by sex and household income.
R. B. Lipton et al. Neurology 2007;68:343-349
©2007 by Lippincott Williams & Wilkins

Prevalence of primary headache types in waiting room

Migraine Burden in U.S.
Migraineur in one in four households28 million migraineurs in the USEstimated annual cost of labor lost to migraine
greater than $ 13 billion per yearPeak prevalence ages 25-55 Often ineffectively treated.

Migraine Pain Intensity and Disability
0
10
20
30
40
50
Mild ModeratelySevere
Severe ExtremelySevere
>75% Report Severe to Extremely Severe Pain
Lipton RB et al. Headache. 2001;41:638-645.
Patients
(%)
39%
Some Impairment
9% Function Normally
53%
Severe Impairment or Bed Rest
Required

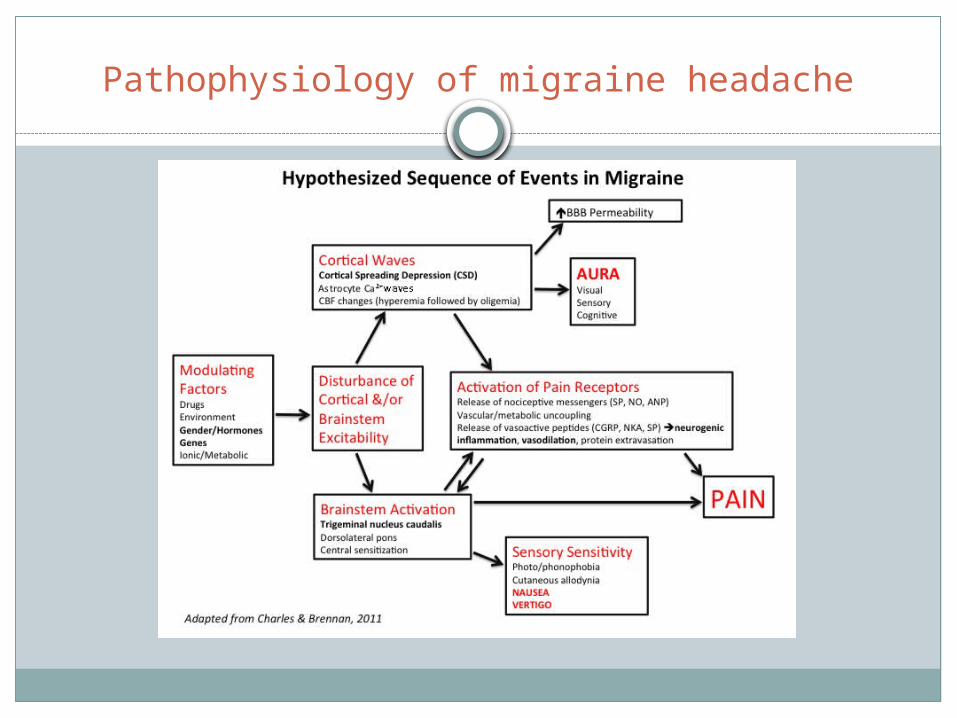
Pathophysiology of migraine headache
Harold G Wolff, a pioneer of the vascular theory of migraine, proposed that the neurological symptoms of the migraine aura were caused by cerebral vasoconstriction, and the headache by vasodilatation.
This had been replaced by cortical spreading depression theory of Leao(neural theory)
Most recent theory- migraine neurovascular phenomenon
Pathophysiology of migraine headache

Pathophysiology of migraine headache

Genetic predisposition to migraine headaches
The concordance for migraines is higher in monozygotic than dizygotic twins.
The first three types of familial hemiplegic migraine (FHM) are channelopathies. FHM1 is caused by mutations in the CACNA1A gene, FHM2 by mutations in the ATP1A2 gene, and FHM3 by mutations in the SCN1A gene. Mutations in the PRRT2 gene also cause some cases of familial hemiplegic migraine
Genetic basis is more complex- and increases individuals susceptibility to migraine headaches

Environmental factors

Principles of migraine management
Life style management- with patient educationAvoid medication rebound headacheAbortive therapyPreventive therapy.

Lifestyle Management
Sleep 8 hours consistent schedule Eat 3 regular meals (or more) per day Drink lots of fluids Get Aerobic exercise regularly Limit caffeine (or better yet avoid completely) Identify your triggers Keep a headache diary Manage stress Use correct posture and pause during repetitive
activities

Acute (abortive) migraine treatment principles
Treat early, while headache is building, within 15-30 minutes of onset.
Use correct dose and formulationLimit to 3 days per week (with exceptions)Try drug with at least 2 headaches to see if it
works before moving on to another agentUse drug combinations often work when a single
agent won’t work

Acute treatment options
Nonspecific NSAIDs simple analgesics combination analgesics Anti-Nausea meds
Promethazine,metoclopramide, prochloroperazine.
Ondansetron
Specific Triptans
- Faster onsetSumatriptan, Zolmitriptan,eletriptan, rizatriptan and almotriptanTriptans Slower Onset Naratriptan and Frovatriptan
-Ergotamine/DHE; Migranol

Triptan therapy
As a class triptan in relation to non specific medicationsRapid onset of reliefHave higher efficacy .Favorable side effect
Adverse effects- flushing, chest pain.Contraindicated in patients with coronary artery disease, angina, patients with hemiplegic or basilar migraines, severe uncontrolled hypertension.

Formulations
Oral therapies- Most medicationsNasal sprays- Sumatriptan, Zolmitriptan, DHE ButarphanolInjectables(IM/SC/IV)- Sumatriptan, DHE,
neuroleptics, injectable NSAIDsTransdermal Patch- Sumatriptan 6.5 mgSuppositories- antiemetics,ergots, opioids.

Adapted -Marmura et al, Headache 2015;55:3-20
Proven effective with more than 1 randomized control trial

Resistant acute migraine therapy
If acute treatment is still inadequate
Change formulation or dosage.Use adjunctive therapyConsider addition of preventive agentEvaluate for medication overuse, excessive caffeine
use.Reconsider diagnosis.
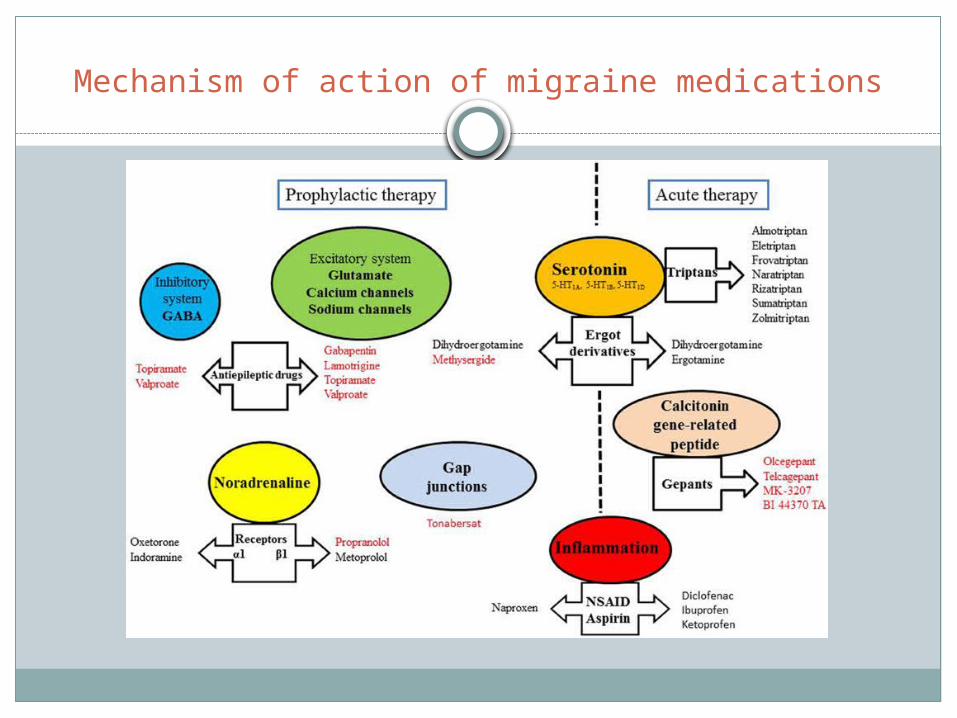
Mechanism of action of migraine medications

When to start migraine preventive therapy
Migraine significantly interferes with patient’s routine despite acute Rx
Frequent headaches> or = 2/ week.Acute therapy is ineffective, contraindicated or
ineffective.Patient preference.

Principles of preventive therapy
In order for preventive meds to be most effective, limit acute meds to 3 days per week
Make sure to use an appropriate dose At least a 2 month trial at a proper dose is required Goal is to decrease headache freq by 50% Evaluate headache therapy(use headache log), attempt to
lower and discontinue therapy when well controlled. Assess for coexisting conditions.

AAN/AHS guideline for migraine prophylaxis

AAN/AHS guideline for migraine prophylaxis

Nonpharmacologic Treatments
Biofeedback Relaxation therapy Cognitive Behavioral Therapy Acupressure Acupuncture Physical Therapy Chiropractic treatment

Additional Treatment Measures
Occipital Nerve Stimulators
TENS units
Transcranial Magnetic Stimulator
Special Diets
Botox Injections- Approved by FDA in Oct 2010. Approved for chronic migraine (migraine headaches more than 15 days/ month)31 injection sites in forehead, temples, shoulders and neck

Emerging therapy in migraine management
Monoclonal antibodies (mAbs) targeting calcitonin gene-related peptide (CGRP) and its receptor.
5-HT1F receptor agonist lasmiditan and glial cell modulator ibudilast.
Neuro-modulation for migraine headache- sphenopalatine ganglion stimulation, trigeminal nerve stimulation and transcutaneous vagus nerve stimulation.

Questions?