meniere's disease* - pmj.bmj.com · of meniere's disease. for this information we need...
TRANSCRIPT

330
MENIERE'S DISEASE*By C. S. HALLPIKE, F.R.C.P., F.R.C.S.
Aural Physician and Director, Otological Research Unit, Medical Research Council, National Hositali.Queen Square, London
The story of scientific enquiry into the problemsof human vertigo began, as we know, one hundredyears ago with the work of a citizen of Paris,Prosper Meniere. It is, therefore, fitting that Ishould begin with a few remarks on the history ofhis work and its remarkably true relationship tomodern views.
Meniere's first great achievement was hisrecognition that paroxysmal vertigo could becaused by a labyrinthine lesion. This may seema commonplace notion now, but it is necessary tobear in mind that in 186i, when Meniere publishedhis best known paper, the very possibility that alesion of the internal ear could cause such severesymptoms as vertigo and vomiting was still a mootpoint. Flourens' experimental work on pigeons,in which he demonstrated for the first time thatgross disorders of equilibrium could be producedby injury of the semi-circular canals, had only beenpublished some 30 years earlier, and its significanceas regards the problems of human disease had notyet been appreciated. It was Meniere's greatmerit that he knew of Flourens' work, understoodits meaning and applied it to human problems.
Meniere's second great achievement was madepossible by his remarkable powers of describingand analysing the symptoms and signs of disease.These enabled him to identify, with an accuracywhich has never been seriously questioned, theparticular disease of the labyrinth which has sincecome to bear his name. Of this the essentialfeature, as we now know, is a distension withoutevidence of infection or trauma of the endo-lymphatic vesicle, a finding remarkable in itselfand since reproduced with remarkable uniformityin a considerable number of further histologicalstudies of temporal bones carried out, some bymyself and also by a number of others.The present position is, therefore, this: That
we know the symptomatology and natural historyof Meniere's disease. For this information weneed not go far beyond Meniere's own writing.
*Lecture given at Cours International de Labyrin-thologie Clinique, Paris, January 15-21, 1955.
We know, also, the morbid anatomy of thelabyrinth which is associated with the disease,though to be sure the exact mechanism of theendolymphatic distension still escapes us.
But we have also at our disposal what Menierehad not, namely, a good deal of new knowledgederived from special tests of cochlear and vestibu-lar function, which enables us to identify thedisease and to assess its severity with greateraccuracy than Meniere could command.
I propose to begin my remarks with a brief out-line, in essentials a recapitulation of Meni6re'sown description, of the symptoms and naturalhistory of his disease.These I shall then endeavour to correlate with
the morbid anatomical findings in the labyrinthwhich have been fully established by recent patho-logical studies. Thereafter I shall discuss in somedetail the results of certain of the tests of cochlearand vestibular function and will again correlatethese with the morbid anatomical findings.
Finally, I shall discuss certain problems ofdifferential diagnosis.We will begin with the clinical features of
Meniere's disease. Its onset is usually in themiddle period of life, 40 to 60 years, and the sexesare equally affected. Its course is essentiallybenign in so far as it does not directly shorten thelife span and it exhibits no significant associationwith any other form of organic disease, includingallergy, outside the eighth nerve system.
Partial deafness of one ear, accompanied bytinnitus, provides the usual clinical background ofestablished Meniere's disease, upon which aresuperimposed its better known dramatic features,paroxysmal attacks of vertigo nearly always withnausea, vomiting and prostration. In a minorityof cases the vertigo comes on very rapidly, withina matter of seconds, and without any warning.More often, however, the vertigo is of sloweronset or may be heralded by some change in thecharacter or intensity of the tinnitus.The duration of the attacks seldom exceeds five
or six hours. They generally end with a state ofextreme prostration and are typically followed by
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from

July 1955 HALLPIKE: Meniere's Disease 331
a long, deep sleep from which the patient awakenswithout the vertigo, which troubles him no moreuntil the next attack.
In other patients, however, the severe attacksmay be interspersed with longer periods of minorunsteadiness which are noticeably aggravated byhead movements. In such patients the cochlearsymptoms, deafness and tinnitus, are usually over-shadowed by the vertigo and occupy a secondaryplace in the patient's impressions.One other cochlear symptom must not be for-
gotten: intolerance of loud sounds with distor-tion of voice sounds and music. This is commonand highly characteristic of Meniere's disease.We come next to the highly characteristic
FIG. I.
morbid anatomical changes in the labyrinth whichwere first described by Cairns and myself in I938.
In Fig. i is shown a transverse section of theunaffected temporal bone of a typical case ofMeniere's disease. In the vestibular area can beseen the macula of the saccule with the thinsaccular wall. Outside this, and underlying thestapes footplate, is the large perilymph space of
- --
FIG. 2.
the vestibule. In the cochlea are seen the twoperilymph scalae and between them the scalamedia filled with endolymph and containing thesensory cells of Corti's organ. It is separated fromthe scala vestibuli by the thin membrane ofReissner.
In Fig. 2 is shown, for comparison, a section ofthe opposite affected temporal bone. In thevestibule the saccule is distended, the membranebeing pushed back everywhere upon the bonyvestibular wall with obliteration of the perilymphspace which lies deep to the stapes footplate. Inthe cochlea the outstanding abnormality is theapparent disappearance of Reissner's membrane.In fact this appearance is brought about by a gross
FIG. 3.
distension of the scala media with displacement ofthe membrane on to the bony wall of the scalavestibuli.
In Fig. 3 is shown the affected cochlea at ahigher magnification. No abnormality can beseen in the fibres of the cochlear nerve as they liein the spiral osseous lamina, while the cells of thespiral ganglion are also normal in number andstructure.We come finally to the cells of Corti's organ.
These are notoriously difficult to display in histo-logical preparations of the human temporal bone.Nevertheless, it is possible even at this magnifica-tion to detect certain obvious pathological changes,and these are better shown in Fig. 4. Above wesee Corti's organ of the affected ear with its haircells and Corti's rods enclosing a well-formedtunnel. Below, on the affected side, the cell massof Corti's organ is greatly compressed and its out-line irregular, while Corti's tunnel is occupied bya structureless coagulum.
Changes closely resembling these have beenfound both by myself and by others in the tem-poral bones of a considerable number of subjects
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from

332 POSTGRADUATE MEDICAL JOURNAL July 1955
-M
FIG.4.
... ...............:: ' :.·.:.. :::·.. :: ····..
.... .... ..i::i::iiiiiiiiiij j.il'
:i ::i:: I···. :~: ·~;iiii:FIG:: ;.:i ·il'- 4li:iIil::::.
with Meniere's disease, and it is now safe todescribe them as constituting its essential morbidanatomy.As to the cause of the endolymphatic distension,
little even now can be said. Some evidence,mainly histological, has been advanced for aprimary failure of the absorptive mechanism of theendolymphatic sac. The evidence, however, is farfrom strong and the alternative possibility of someabnormality, quantitative or qualitative, of theendolymph itself as secreted by the stria vascularis,remains to be investigated.Although in this sense the morbid anatomical
findings give us no full explanation of the disease,they do enable us to say this; that the essentialevents which underlie the characteristic paroxysmsconsist of recurrent bouts of endolymphatic dis-tension. As a result of the accompanying physico-chemical changes in the endolymph the sensorycells of hearing and equilibrium undergo acutestructural changes with resulting derangement ofhearing and equilibrium.These changes are incompletely reversible be-
tween the attacks, and this we expect to find
reflected in the results of functional tests appliedduring these periods. We can, in fact, return tothe subject of these tests enlivened by the assurancethat we can interpret their results in terms ofknown structural changes in particular anatomicalelements, namely the sensory end-organs ofhearing and equilibrium.We come now to the tests themselves. Of the
vestibular tests we have come to rely chiefly uponthe caloric tests practised according to a techniquefirst described in I942 in association with mycolleague, the late Dr. Gerald Fitzgerald. Thesubject of these tests is still, we find, looked uponas a matter of some difficulty, and I propose, there-fore, to begin with a brief description of the way inwhich we perform them and interpret their results.
TAPWATERAT
\ 30CC. 44 C.
\
\
FIG. 5.
The tests are carried out with the patient lyingsupine, as shown in Fig. 5, the head being raised30 degrees from the horizontal, thus bringing theexternal canal into its position of maximum sen-sitivity. The cold and hot stimuli, water at 30°and 44° C., are equidistant from body tempera-ture, and are applied for 40 seconds. Their effectsare substantially limited to the external canal andare calculated to bring about equal and oppositedeflections of the cupula.The subject is asked to fix his gaze upon a small
object in front of him, usually a mark upon theceiling. The observations of the resulting nystag-mus are, therefore, of second degree nystagmus.The subject's eyes are well illuminated, and theobserver inspects them from a distance of about30 cm. The observational conditions are thus verygood.What we measure is the time interval between
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from

July 1955 HALLPIKE: Meniere's Disease 333
,L----- -I- i--- --
30t I I - ' i_ iR----------
__/"| i
NORMAL.FIG. 6.
the application of the stimulus and the end of theresponse. In this, the latent period of the responseis included, and we make no attempt to measure itseparately. The results are graphically recordedin the manner shown in Fig. 6.The results shown are characteristic of an
average normal subject. The two continuous linesrepresent time, three minutes sub-divided intointervals of ten seconds. The interrupted linesrepresent the response durations. Above are thetwo cold responses for the left and right ears, andbelow the two hot responses. It is convenient forreference to number these responses i to 4 fromabove downwards. Responses i and 4 consist ofnystagmus to the right. Responses 2 and 3 con-sist of nystagmus to the left. The direction of thenystagmus is specified in accordance with con-vention in terms of its rapid component.
/L
L - - - -'
R/ -----*
RLeft canal paresis.
FIG. 7-
The commonest and most obvious type of
a'left canal paresis. Responses i and 3are reducedwith respect to responses 2and 4 which are normal.Below, a right canal paresis. Responses 2 and 4are reduced.The degree of paresis varies. The responses, as
shown, may be moderately reduced. It may beseverely reduced or totally extinguished. The
-<:R.' -'-.-
I? -,
ORMAIL.
oiRECTIOMAL PREPONMMRANCE' TO LEFT.
'"- --- -----
L_'- -
OIRECTIONAL PREPONIDeANCE TO RICr.
FIG. 8.
question which now arises is: Is it really necessaryto use both cold and hot stimuli? Does not theinformation derived from the hot responses merelyreduplicate that derived from the cold responses?
This would certainly be the case if the onlyabnormality which occurred were a loss of sen-sitivity of one or other external canal. In point offact it is not the only abnormality, and this bringsus to the interesting and important phenomenonfor which, since I942, we have used the term' directional preponderance.' The nature of thisis shown in Fig. 8.Above is shown the normal caloric pattern.
Below is a typical directional preponderance to theleft. Reactions i and 4, which consist of nystag-mus to the right, are inhibited. Reactions 2 and3, which consist of nystagmus to the left, areincreased.
Below is seen an example of directional pre-ponderance to the right. In this, reactions 2 and3, which consist of nystagmus to the left, are in-hibited. It is easy to understand that this type ofabnormality could not possibly be demonstrated bymeans of cold stimuli alone. Thus in this caseresponses i and 2 would indicate a loss of sen-sitivity of the right labyrinth. Responses 3 and 4,however, would indicate a loss of sensitivity of theleft labyrinth.
It is only when all four responses are known thatthe directional nature of the derangement is madeapparent.
It is necessary at this point to ask and answer apractical question. What is the clinical importanceof directional preponderance which makes it worthwhile demonstrating? The answer is found in thefact, established by observation, that in a signifi-cant proportion of cases of unilateral vestibular
Bl
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from
POSTGRADUATE MEDICAL JOURNAL
disease, affecting either the labyrinth or the eighthnerve, it occurs as the sole abnormality of thecaloric responses: Thus we have found it in some20 per cent. of our series, extending to severalhundreds of cases of unilateral Meniere's disease.The direction of the preponderance is always tothe side opposite to the lesion; its presence canbe accepted as evidence of that lesion, and this isthe fact which gives it its clinical importance.What now of its cause? This will best be under-stood if we consider the neurological mechanismsto which it is usual to attribute certain well-knowndisturbances which follow experimental destruc-tion of one labyrinth. These it is customary toexplain in the following way:Each labyrinth, in addition to responding in a
phasic manner to angular accelerations by meansof its semicircular canals, is also the source oftonic impulses which exercise an assymmetricalinfluence upon the limbs and eyes. Thus theright labyrinth alone causes a rotation of the headto the right, together with a sustained nystagmuswith its rapid component to the right; effectswhich in the intact animal are cancelled by theopposing influence of the left labyrinth.
If now the right labyrinth be destroyed, then theunopposed tonic impulses from the left labyrinthwill cause rotation of the head to the left withnystagmus to the left. As we know, this nystag-mus, severe at first, gradually disappears in thecourse of a few weeks, its abolition being broughtabout by a process of central compensation. Thusthe right vestibular nuclei, being deprived of in-coming tonic impulses, set up a rhythm of theirown and in this way the output of the two sets ofvestibular nuclei are once more brought intobalance and the nystagmus ceases.
Let us now take the case in which the rightlabyrinth, instead of being completely destroyed,is, as in Meniere's disease, the seat of a partiallesion which has brought about no more than apartial loss oi its tonic discharge. In this case weassume that the resulting minor imbalance of thetonic discharges would be insufficient to cause anyspontaneous nystagmus to the left. Nevertheless,its tendency to occur will still be present and willmanifest itself as a directional preponderance tothe left of the caloric responses.Thus we see that in the absence of spontaneous
nystagmus, and in the absence also of any altera-tions in sensitivity of the external semi-circularcanal, a unilateral loss of labyrinth tonus may stillbe made evident by means of the cold and hotcaloric tests.Thus in Fig. 8 the upper pattern, preponderance
to the left, is indicative of a tonus defect of theright labyrinth. The lower, preponderance to the
right, is indicative of a tonus defect of the leftlabyrinth.Whether or not this is the true explanation of the
directional preponderance of the caloric responseswhich we have encountered in unilateral labyrin-thine lesions, such as occur in Meniere's disease,cannot yet be stated with certainty. We can onlysay that the circumstantial evidence in its favouris very strong.What we can state as matters of fact are: That
it does occur in association with such lesions; thatit can be accepted as evidence of their presence;that its demonstration requires both cold and hotcaloric stimuli and that for this reason their use isessential.To complete this exposition of the caloric test
abnormalities encountered in Meniere's disease, Imust explain that while these two primary abnor-malities, canal paresis and directional preponder-ance, usually occur separately, they are notinfrequently combined. The resulting abnor-malities in the patterns of the caloric responses,though they may be very confusing, are neverthe-less readily recognizable as algebraic summationsof the primary abnormalities.The results of the caloric tests obtained in a
series of 50 cases of Meniere's disease were pub-lished in I942 by my colleague, Mr. Cawthorne,and myself, and the figures therein given continueto accord very well with our subsequent findingswhich cover several hundred subjects and areshown in Table i.We may now turn to the tests of cochlear func-
tion; in particular to two which are especiallydeserving of our attention. These are the in-telligibility test for amplified speech and theloudness recruitment test.
Otologists have been aware for many years thatthe capacity of deaf patients to derive benefit fromhearing aids depends very much upon the patho-logical basis of their deafness. Knowledge of thissubject has been greatly advanced by the numerous.and searching enquiries into the problems ofhearing aid design which have been carried out inthe last ten years by investigators upon both sidesof the Atlantic, in particular the Harvard Groupin the U.S.A. and the Electro-Acoustics Com-mittee of the Medical Research Council in Britain.In the course of this work great advances havebeen made in the principles and practice of speechaudiometry and as a result this valuable test pro-cedure has now been put upon an accuratequantitative basis.By its means otologists are now able to answer
with rapidity and precision one of the most im-portant practical questions that can arise in con-nection with any deaf subject. To what extentcan his social disability, loss of speech intelligi-
July 1955334
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from

July I955 HALLPIKE: Meniere's Disease 335
CALORIC TEST RESULTS IN100 CASES 'OF MENIERE'S DISEASE.
DIRECTIONAL PREPONDERANCE 21 CASES
CANAL PARESIS 49 CASES
DIRECTIONAL PREPONDERANCE+ CANAL PARESIS 18 CASES
NORMAL 12 CASESTABLTE I.
bility, be corrected by means of amplification.This criterion, applied by means of speech audio-metry, makes it possible to divide deaf subjectsinto two groups.
In the first group the deafness is generally dueto conductive lesions and restoration of speechintelligibility by amplification can be satisfactorilyaccomplished. It would seem that in these sub-jects, if the sounds of speech can be made to reachthe cochlea at all, then they are well understood.
In the second group the deafness is of the so-called perceptive type and restoration of intelligi-bility by amplification cannot be achieved. Thereactions to amplification of four subjects belong-ing to these two groups is shown in Fig. 9.
Curv.s for Noreme.
--$weea-°t
40-----lrtn- - -----4or( .
t~ ._L:ptso - - - - 0 /
f To1_ j I. '' '---- 70*"'oot/.0" ----.10 0 Jo$ 0s O0 s0 0o0 100
AM:LFICArIO I Ce m»/'lfll(Lot»f)(0£CIBLS) I Conrer«ftlon. (Orlmr V .I ft)
C*rc* vl. l.
FIG. 9.
The tests are carried out with the patient seatedin an anechoic soundproof room with the ear undertest at a fixed distance from a loudspeaker. Re-corded lists of monosyllabic words are reproducedon the speaker by means of an amplifier system.The amplification can be adjusted over a range
of Ioo db. and this intensity scale is set along thebase line. The percentage of words understood
are recorded upon the ordinates. The amplifiersetting of 50 db. gives an intensity at the ear ofthe subject which corresponds to that of anordinary conversational voice at a distance of onemetre. Other useful amplifier settings specifiedon the chart are at 64 db., which correspondsroughly to a loud conversational voice at 3 ft., andat 36 db. This we call 'church level' since itcorresponds roughly to the speech intensity levelswhich reach the ears of listeners in churches andother auditoria. The response curves of a normalsubject are shown on the left. At an amplificationof 30 db., well below church level, the score wouldbe go per cent., which corresponds to a sentenceintelligibility of Ioo per cent. Curves A and Bwere obtained from two subjects with conductivedeafness.
Subject 'A' at church level can only under-stand an occasional word. With increasing am-plification, however, his score steadily increasesand reaches 90 per cent. level when the intensityis raised to the level of ordinary conversation at3 ft. With this degree of deafness the patientwould, of course, experience no difficulty with atete-a-tete conversation. ' B's deafness is moresevere. He understands a few words at 50 db.Nevertheless he reaches the score of 90 per cent.when amplification is raised to 80 db. We see thatin both these cases it is possible by means ofamplification to restore full intelligibility ofspeech.
In Fig. 9 are also shown for contrast the verydifferent results that are obtained in the type ofperceptive deafness which we encountered inMeniere's disease. Both curves C and D begin atpoints which correspond closely to those of the
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from

336 POSTGRADUATE MEDICAL JOURNAL July 1955;
two cases of conductive deafness. As the amplifica-tion is increased, however, intelligibility, after aninitial slight increase, falls off again and at no pointis any serviceable restoration of intelligibilityachieved. These results are highly characteristicof Meniere's disease, at any rate in its active phases.We come now to the Loudness Recruitment
Test. Most of our work has been carried out withpatients suffering from unilateral Meniere's diseaseand in these we have found it best to use theso-called ' alternate binaural loudness balancingprocedure' with which Fowler first demonstratedthe phenomenon.
AUDIOGRAMS
CONOUCTING DEAFNESS NORMAL NERVE DEAFNESSLEFT EAR LEFT EAP
0__-__-.-.---- -2o20-
m60- 1 1 1 61 60-T11 I
I125 0000 125 8000 1?5 8000--LEFT ..) R-GTr FPEOIUEACY CPS --LEFT -- RGrT
R L P LL L0 f00- .00 /00- .f00
Bo. 80 8 * 80
40g Th40 40f th 40s
LOUDNESS BALACE DC,A,MSF,CO'(ENCY' KOOCR.
FIG. 0.
The way the test is carried out is shown in Fig.lo. The subject wears a telephone receiver oneach ear, each supplied by a separate pure tonegenerator. The frequency of the stimulus is thesame for each ear but the intensity.can be variedindependently. With the switch the stimulus isapplied alternatively to each ear, the intensitybeing adjusted to give equality of the loudnesssensations in the two ears. The two intensityscales are marked in decibels above the normalthreshold, one for the right ear and one for theleft. The test procedure is designed to identifyand connect, as shown, points on the two scaleswhich give equal sensations of loudness. Theladder diagram was derived from a normal subject
and the rungs of the ladder, as would be expected,.run horizontally from top to bottom.On the left is shown the result obtained with a
case of unilateral deafness due to middle eardisease. The hearing loss at threshold is 30 db.at ,000ooo c.p.s. This is shown by the lowest rungof the ladder. The intensity is then increased bysome 20 db. at the normal ear and the matchingintensity at the affected ear is found to lie at 50 db.In the same way the sensitivity difference betweenthe two ears, 30 db. at threshold, is maintained allthe way up the intensity scale.On the right, by contrast, is shown the result
obtained with a case of unilateral deafness due toMeniere's disease. The hearing loss at thresholdis also 30 db. at I,ooo cycles, and this too is shownby the lowest rung of the ladder. As the intensityscale is mounted, however, the difference in sen-sitivity between the two ears, 30 db. at threshold,diminishes until at 60 db., equal intensities giveequal loudness sensation, and this in brief con-stitutes the Loudness Recruitment phenomenon.
In describing the technical features of this testin such detail I have had a special point in mind.As has been clearly shown by my colleagues, Drs.Dix and Hood, and myself, the Loudness Recruit-ment phenomenon is characteristic of hair celldisease. It depends, in fact, upon the capacity ofdiseased hair cells to give responses of normalmagnitude to stimuli of high intensity. Theycannot, however, sustain such responses and,indeed, if the stimuli are at all prolonged theresponses rapidly relapse to sub-normal level.Hence we insist upon using a test procedure which,as in the one that I have described, short interruptedstimuli are used.
In all that I have so far told you of MLeniere'sdisease, I have endeavoured to include none butwell attested facts. The information, although notcomplete, is impressive both in character andamount. It enables us to say of the disease that ithas a highly characteristic symptomatology andnatural history, matched by an equally character-istic morbid anatomy. Further, the tests ofvestibular and cochlear function all give results ina uniform and, we should like to think, distinctivecharacter.Now, finally, comes the practical question of
diagnosis. To what extent do these clear-cutclinical features enable us, in practice, to dis-tinguish it from other organic disorders of theeighth nerve system? What, in fact, are theseother disorders and in what way do their clinicalfeatures and pathology differ from those ofMeniere's disease?The subject is a large one and was dealt with in
some detail by Dr. Dix and myself in a paper com-municated in March I952 to the Otological
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from

HALLPIKE: Meniere's Disease
Section of the Royal Society of Medicine ofLondon. In the time at my disposal it will benecessary to confine myself to a brief review ofthe salient points of that paper.We stated that by far the greater part of the
patients seen by us at Queen Square, with symp-toms indicative of organic derangement of theeighth nerve system, could be divided into fourdistinct clinico-pathological groups:
I. Meniere's disease.2. Vestibular neuronitis.3. Positional vertigo of the benign paroxysmal
type.4. Tumours of the cerebello-pontine angle in-
cluding neurofibromata of the eighth nerve.I. On the subject of Mdniere's disease I need
say no more.
2. Vestibular neuronitis is chiefly distinguishableon clinical grounds from Meniere's disease by theconspicuous absence of cochlear signs and symp-toms. It affects adults without preference for sexand is relatively more common than Meniere'sdisease under the age of 30.Apart from the absence of cochlear signs and
symptoms the condition is sometimes, though notalways, distinguishable from Meniire's disease bythe character of the vertigo. This may consist ofsudden and transient seizures accompanied bysensations of blackout. On the other hand theremay be no severe paroxysms and the disequilibriummay take the form of feeling ' top heavy' or offbalance when walking.
In a fairly high proportion of the subjects theonset of the symptoms is associated with some kindof febrile illness or with some evidence of infectionin the nose or throat. Infective ear disease, as inMeniere's disease, does not seem to be a factor.As stated, tinnitus or deafness are conspicuous
by their absence, and the most searching tests ofcochlear function yield normal results. Tests ofvestibular function, however, tell a different story.In particular the caloric tests constantly showsevere and often bilateral derangement, while thegalvanic responses, too, are often much reduced.The condition is essentially a benign one and thesymptoms usually respond well to treatment ofinfective foci when these are present. Under thesecircumstances a restoration of the caloric responseshas also been observed. The evidence of vestibulardisease, taken in conjunction with the absence ofcochlear symptoms or signs, makes it necessary tolocate the lesion in the vestibular pathways at somepoint central to the labyrinth. It was, however,impossible to go further and specify the particularelements of the neurones, nerve cells or nerve fibres,which were involved. When, therefore, it came tonaming the condition, we required a term compre-hensive enough to encompass this ambiguity. We
chose the name ' vestibular neuronitis' and havesince continued to use it.
3. Positional nystagmus of the benign paroxysmaltype. Since Barany's original paper published in1921, otologists and neurologists alike have shareda growing interest in a group of patients in whomnystagmus and vertigo are precipitated by certaincritical orientation of the head. As Nylen hasshown in his well-known monograph, a particularvariety of this condition tends to occur in associa-tion with space-occupying lesions in the posteriorfossa. In addition, however, positional nystagmusmay occur in patients without any evidence what-soever of any serious intracranial disease and anincreasing body of evidence has accumulated tosupport Barainy's original thesis that in thesesubjects the lesion is situated in the otolith organsthemselves.
In our paper in I952, Dr. Dix and I analysedour findings in Ioo such subjects and came toconclusions which were in striking agreement withthose of Barany. Our findings and conclusionscan be stated quite briefly. The condition chieflyaffects adults of the age group 30 to 60 yearswithout preference for sex. In none was there anyevidence of disease of the central nervous systemoutside the eighth nerve system.
FIG. II.
The method of eliciting the nystagmus, and alsoits highly characteristic features, are depicted inFig. i. In this the critical head position is alsoindicated with the head turned either to the left or,as shown, to the right. In taking up this positionthe patient is first seated upon the couch with thehead turned to one side and the gaze fixed uponthe examiner's forehead. The examiner thengrasps the patient's head firmly between his handsand briskly pushes the patient back into the criticalposition. The reaction which results calls for somedetailed description.
First of all there is nearly always a marked latentperiod. Sometimes this is as long as five or sixseconds. Occasionally it is very short and indeedthe reaction may seem to come on at once. This,however, is uncommon. The onset of the nystag-mus is nearly always preceded by an appearance of
July 1955 337
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from
338 POSTGRADUATE MEDICAL JOURNAL July 1955
distress. The colour may change; the patientsmay close their eyes, cry out in alarm and makeactive efforts to sit up again. At this point it isnecessary to reassure the patient and maintain theposition of the head. The nystagmus is chieflyrotatory, the direction of the rotation being towardsthe undermost ear. (Note-In specifying thedirection of the rotation, reference is made to thedisplacement of the I2 o'clock point of the cornealcircumference.) In addition to the rotatoryelement there is generally a horizontal componentwhich is again directed towards the undermost ear.The nystagmus increases in a rapid crescendo in aperiod which may be as short as two to threeseconds or as long as ten seconds. Thereafter itrapidly declines and the patient's distress is re-lieved. If the patient is then allowed to sit up, arecurrence of the vertigo in a slighter form isgenerally noted, and if the eyes are examined atthis point nystagmus can be seen, the direction ofwhich is, on the whole, reversed. If this is allowedto disappear and the critical supine position is againassumed, the nystagmus again makes its appear-ance, but generally in slighter form and disappearsmore rapidly than before. After two or threerepetitions of this test it is generally found that thereaction has been eliminated altogether and cannotbe elicited except, as Barasny pointed out, after aperiod of rest.Now the evidence put forward by Miss Dix and
myself led us to conclude that the symptoms weredue to an irritative lesion of the otolith apparatusof the labyrinth towards which, when undermost,the nystagmus was directed. Thus in Fig. i thesubject's right labyrinth would be the affected one.This conclusion was derived from the followingchain of evidence:
I. The benign course of the disease and theabsence of evidence of any involvement of the cen-tral nervous system indicated a labyrinthine lesiondue to infection, trauma or some vascular lesion.
2. A labyrinthine lesion was also indicated bythe fact that in 55 of our Ioo cases substantial evi-dence of ear disease was present, usually in the formofgross middle ear infection or labyrinthine trauma.
3. In many of these 55 cases with ear diseasethis disease was unilateral and in practically all ofthese latter the nystagmus was directed towards theaffected ear when this was placed undermost.
4. In one typical case we were able to carry outa histological examination of the affectedlabyrinth and this revealed chronic changes in theotolith apparatus.The case was that of a woman of 40 who ex-
hibited before death a characteristic positionalnystagmus of the benign paroxysmal type with theright ear undermost. Her death was due to an un-related disorder. Histological examination of the
lt
I
I
'a·
Fic iz*.a...8.
FIG. I2.
left temporal bone showed a normal vestibularapparatus. In the right temporal bone, however,gross changes were found in the maculae of theotoliths.
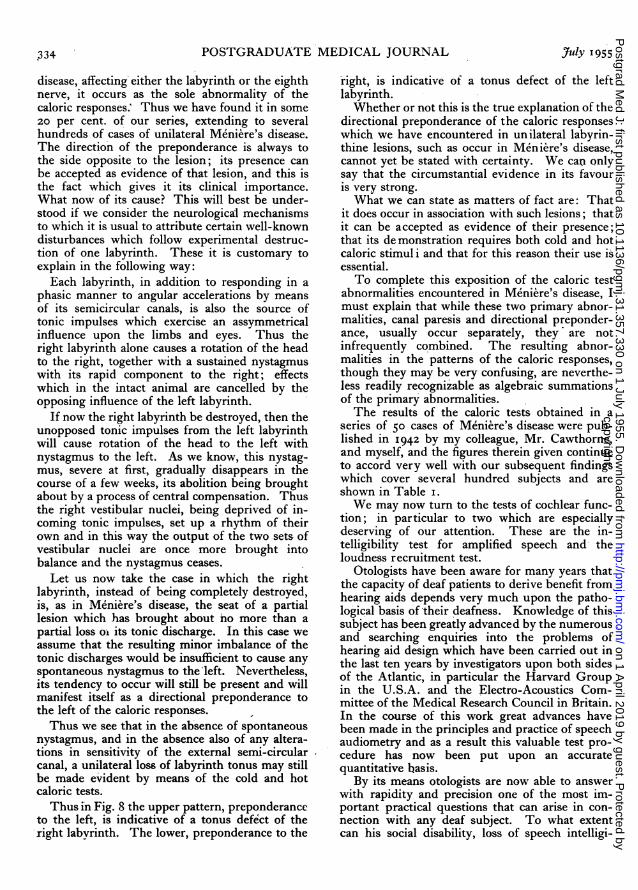
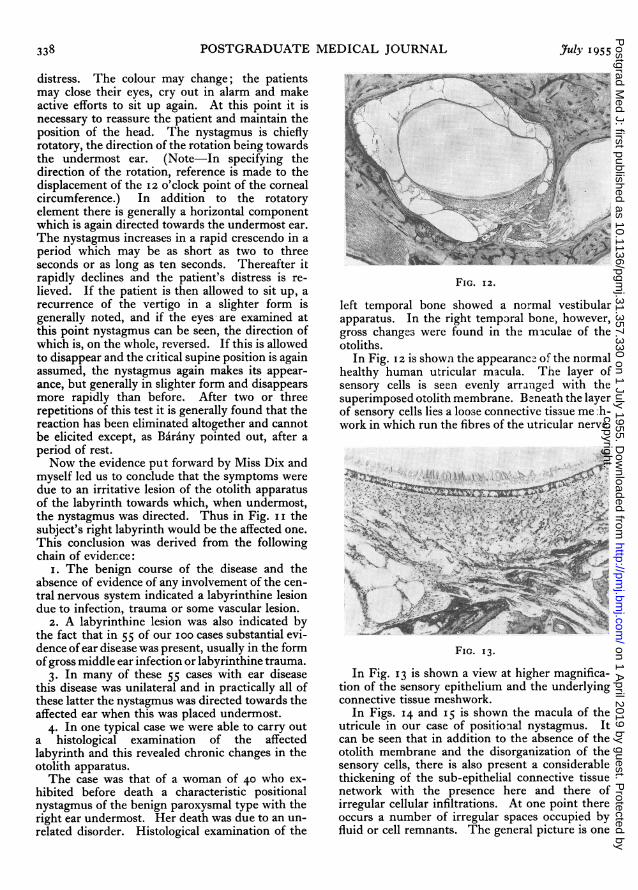
In Fig. 12 is shown the appearance of the normalhealthy human utricular macula. The layer ofsensory cells is seen evenly arranged with thesuperimposed otolith membrane. Beneath the layerof sensory cells lies a loose connective tissue me h-work in which run the fibres of the utricular nerve.
'ki
C :
FIG. 13.
In Fig. 13 is shown a view at higher magnifica-tion of the sensory epithelium and the underlyingconnective tissue meshwork.
In Figs. I4 and 15 is shown the macula of theutricule in our case of positional nystagmus. Itcan be seen that in addition to the absence of theotolith membrane and the disorganization of thesensory cells, there is also present a considerablethickening of the sub-epithelial connective tissuenetwork with the presence here and there ofirregular cellular infiltrations. At one point thereoccurs a number of irregular spaces occupied byfluid or cell remnants. The general picture is one
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from

July 1955 HALLPIKE: Meniere's Disease 339
cr.~......... ..... ........
... ... ....
.:: ...... .. ... ... ..
- *>-lii~3·iiji:eii~r
-.... ... .. .. ... .. .... .... .. ...
... .. ........ ......
...''.. ..
.... .. .-
..........~e~;
li 00
FIG. I4.
'.::
ri .ii
}>3;|~.*i;2 :} XM-^
:4,'....f-:i. r 9*:.twiSs i
FIG. IS.
of chronic tissue changes resulting either frominfection or trauma, and it accords very well withour conception of the responsible lesion which wehave reconstructed from our clinical evidence.Changes very similar in character but lesser indegree were present in the macula of the saccule.
4. Tumours of the cerebello-pontine angle. Thebest known and commonest of these tumours arethe acoustic neurofibromata. From what Croweand Hardy have told us of their early developmentthey seem to have their starting point in the regionof Scarpa's ganglion of the vestibular nerve as itlies in the internal auditory canal.The course of such a tumour falls typically into
two distinct stages, each with its own clinicalfeatures.
In the first or otological stage there is a slow andprogressive destruction of both cochlear andvestibular nerve fibres. Clinically, the condition isextremely insidious. Thus, the deafness beingunilateral, causes little social disability and is not asa rule accompanied by severe tinnitus. For thesereasons it seldom attracts serious attention. As to
the vestibular destruction its progress, being slowand steady, causes no paroxysmal disturbance, andwith it keep pace the processes of central com-pensation. As a result, the tumour may progressto complete unilateral destruction of vestibularfunction without causing any vestibular symptomsapart from slight unsteadiness and momentaryvertigo on walking.
In the second, or neurological stage, the tumourexpands from the internal auditory meatus andbegins to press at first upon the brain stem in theregion of the vestibular nuclei, thereby causingtrigeminal disturbances and spontaneous nystag-mus to the opposite side. Later interference withthe cerebellum develops with cerebellar ataxia ofthe homolateral limbs. It is with regret that wehave to admit that in most cases of eighth nervetumour the diagnosis is not made until they havepassed from the otological stage in which their re-moval is relatively easy, into the neurological stagewhen the brain stem changes add greatly to thehazards of the operation. The morbid anatomicalchanges in the labyrinth are well known. Thevestibular and cochlear neurones, including thespiral ganglion, degenerate completely, usuallywith preservation of the cells of Corti's organ.Sometimes, however, the tumour interferes withthe blood supply of the labyrinth and changes inthe hair cells then do occur. Distension of theScala media of the kind found in Meniere's diseaseis not found.
~*P*
-3 - .i ,
FIG ::.
FIG. I6.
In Fig. 16 is shown a transverse section of thetemporal bone from an early case of eighth nerveneurofibroma. The tumour has been removed.There is a characteristic funnel enlargement of theinternal auditory meatus. Remains of the tumourare still present in the fundus of the meatus at thispoint. Extensive degeneration of the cochlearneurones, including the cells of the spiral ganglion,have taken place within the labyrinth. The hair
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from

340 POSTGRADUATE MEDICAL JOURNAL .uly 1955CHARACTER COURSE RELATIONSHIP CALORIC DEAFNESS. TINNITUS. CHARACTER RESPONSE LOUDNESS PATHOLOGY.
OF OF OF VERTIGO OF TOVERTIGO. VERTIGO TO HEAD RESPONSES. DEAFNESS AMPLIFICATION. RECRUITMENT.
POSITION
ATTACKSOFTEN ALWAYS DISTENSION OF ENDOLYMPH
PAROXYSMAL. SEVERE ABNORMAL ALWAYS VARIABLE. PRESENT. SYSTEM.AT ONSET.
WITH RESPONSES ALWAYS PRESENT DEGENERATIVE CHANGESSENT O VER-M N E NAUSEA LONG ASENT OCCUR PRESENT POOR OVER- PRESENT IN END ORGANS.
ASEA L BSEN NERVE FIBRES [, GANGLIOND/SEASE AND PERIODS IN 95% OFTEN VOICES MA N GANGLIONVOMITING REEDOM SEVERE DSTORTD OCCU CELLS NOT AFFECTED
COMMON
TUMOURS PAROXYSMS SLIGHT ALWAYS DEGENERATION OF FIBRESOF RARE. IN ABNORMAL PRESENT. USUALLY OF VIltkNERVE 6 ASSOCIATED
EARLY RESPONSES ALWAYS MAY ABSENT GANGLION CELLS.CEREBELLO- PERSISTENT STAGE S. RARE OCCUR PRESENT NOT PROGRESSIVE BE OR DEGENERATION OF END ORGANSPONT/NE IMBALANCE IN 100% OFTEN GOOD INCOMPLETE NOT USUAL BUT MAY RESULTANGLE USUAL THEREAFTER SEVERE FROM DERANGEMENT OF
POGRESSIVE VASCULAR SUPPLY
BLACK OUTS ATTACKSOR FREOUENTDOR RUN
ANORMAL C C H L E A R S Y M P T O M S UNKNOWN.DURING ABNORMAL
VESTIBULAP SEIZURES. ACTIVE RESPONSESSTAGES. ABSENT' OCCUR ? TOXIC DEGENERATION OF
NEURON S SOMETIMES RECOVERY IN 100% A N D S G N S A B S E N TNEURONITIS SOMETIMES RECOVERYPERSISTENT OR LONG OFTEN VESTIBULAR NEURONESIMBALANCE REMISSIONS BILATERAL
USUAL
POSITIONAL ATTACKS DEGENERATIONOStO FREQUENTK COCHLEA SYM P TOM S AN D SIGNS CEETONNYSAGMUS RING OF MACULAE OF OTOLITHNYSTAGMUS DURING
OF POXSMA ACTIVE PRESASENP NT ONLY WHEN CON DI TION C ORNSPAROXYSMAL STAGES. ALWAYS OFTEN CHARACTER OF TISSUE CHANGESBENIGN PRESENT NORMAL SUGGESTIVE OF TRAUMA,
PAROXYSA RECOVERY IS ASSO C I ATED WI TH EAR DISEASE. INECTIONOR VASCULARPAROXYSMAL INFECTION OR VASCULAROR LONGr)~' DE REMISSIONS UPSET.rTYPE RS USUALLY MIDDLE EAR INFECTION
UPSET
USUAL
TABLE 2.
cells, however, appear to be unaffected, while nodistension of the Scala media can be seen.The otological symptoms and signs are usually
quite characteristic. Paroxysmal attacks of vertigomay occur but are rare. The deafness may be ofany degree. It arises chiefly from destruction ofthe nerve fibres and not, as in Meniere's disease,from hair cell disease. Hence Loudness Recruit-ment, so typical of Meniere's disease, is character-istically absent in eighth nerve tumours, a diag-nostic point of great practical importance. In aproportion of cases, however, amounting in ourown series to 12 per cent., Loudness Recruitmentis present, and in these we have ascribed it to haircell changes resulting from interference by thetumour with the labyrinthine blood supply.
Tests of vestibular function invariably yieldabnormal results. Spontaneous nystagmus ispresent in cases which have reached the neuro-logical stage and all without exception showchanges in the caloric responses on the affected side.
In Table 2 the essential features of the path-ology, symptoms and physical signs of these fourorganic disorders of the eighth nerve system areseen assembled in a simplified form.Taken together, these disorders make up much of
that ill-defined assortment which has in the pastcarried that undiscriminating label Meniere'ssyndrome.
It is, of course, the longstanding task of oto-neurology to resolve this assortment into its com-ponent parts, and that by the methods in whichMeniere himself so excelled, of clinico-pathologicalanalysis. It is, therefore, the hope of myself andmy colleagues at Queen Square that the informa-tion assembled in this table will encourage you tobelieve that progress with this task is not at astandstill.
BIBLIOGRAPHYCAIRNS, H., and HALLPIKE, C. S. (1938), J. Laryng. & Otol.,
53, 625.CAWTHORNE, T. E., FITZGERALD, G., and HALLPIKE,
C. S. (1942), Brain, 65, i 8.CAWTHORNE, T. E., and HALLPIKE, C. S. (1943), Proc. Roy.
Soc. Med., 36, 533.CROWE, S. J., and HARDY, M. (1936), Arch. Surg. (Chicago),
32, 292.DAVIS, H., et al. (1946), Laryngoscope, 56, 85.DIX, M. R., HALLPIKE, C. S., and HOOD, J. D. (1948), Proc.
Roy. Soc. Med., 41, 516.DIX, M. R., HALLPIKE, C. S., and HOOD, J. D. (1949), Ibid..
42, 527.DIX, M. R., and HALLPIKE, C. S. (1952), Ann. Otol., 6i, 987.FITZGERALD, G., and HALLPIKE, C. S. (1942), Brain, 65, II5.HALLPIKE, C. S., and WRIGHT, A. J. (1939), Proc. Roy. Soc.
Med., 32, 1646.HALLPIKE, C S. (1949), Proc. IVth Internat. Cong. Otolaryng.MEDICAL RESEARCH COUNCIL (1947), Spec. Report Series
No. 261, 'Hearing Aids and Audiometers' (H.M. StationeryOffice).
copyright. on 1 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.357.330 on 1 July 1955. D
ownloaded from