miemss: mission/vision/key goals - msa.maryland.gov
TRANSCRIPT

MIEMSS: MISSION/VISION/KEY GOALS
The Maryland Institute for Emergency Medical Services Systems (MIEMSS) overseesand coordinates all components of the statewide EMS system (including planning,operations, evaluation, and research), provides leadership and medical direction, conductsand/or supports EMS educational programs, operates and maintains a statewidecommunications system, designates trauma and specialty centers, licenses and regulatescommercial ambulance services, and participates in EMS-related public education andprevention programs.
MIEMSS provides the executive support for the EMS Board in reviewing andapproving the budgets for agencies receiving funds from the EMS Operations Fund,developing and promulgating regulations and protocols, proposing EMS system legislation,licensing/certifying and disciplining EMS providers, and conducting other EMS Boardbusiness. MIEMSS also provides the administrative and staff support for the StatewideEMS Advisory Council (SEMSAC) and five EMS regional councils.
MISSIONConsistent with Maryland law and guided by the EMS Plan, to provide the resources
(communications, infrastructure, grants, and training), leadership (vision, expertise, andcoordination), and oversight (medical, regulatory, and administrative) necessary forMaryland’s statewide emergency medical services (EMS) system to function optimally andto provide effective care to patients by reducing preventable deaths, disability, anddiscomfort.
VISIONTo be a state EMS system acknowledged as a leader for providing the highest quality
patient care and that is sought out to help other EMS systems attain the same level ofquality care.
KEY GOALS• Provide high quality medical care to individuals receiving emergency medical
services.• Maintain a well-functioning emergency medical services system.

i
2002–2003 ANNUAL REPORTCONTENTS
MIEMSS Vision/Mission/Key Goals inside front cover
From the EMS Board Chairperson 1
MIEMSS From the Executive Director 2Administration 4Aeromedical Operations 4Attorney General’s Office 5Communications Engineering Services 6Compliance Office 7Emergency Health Services Department,
University of Maryland Baltimore County 7Emergency Medical Services for Children 8EMRC/SYSCOM 10Hospital Programs Office 11Information Technology 11Licensure and Certification 12Maryland Critical Incident Stress Management Program 13Medical Director’s Office 14Policy and Planning 15Public Information and Media Services 17Quality Management 18Regional Programs 19State Office of Commercial Ambulance Licensing and Regulation 25
Maryland Trauma and Specialty Referral CentersOverview 26Trauma Center Categorization 27Adult Trauma Centers
PARC: R Adams Cowley Shock Trauma Center 27Level I: Johns Hopkins Hospital 29Level II:
Johns Hopkins Bayview Medical Center 30Prince George’s Hospital Center 30Sinai Hospital 31Suburban Hospital 31
Level III:Peninsula Regional Medical Center 32Washington County Hospital Center 33Western Maryland Health System–Memorial Trauma Center 33
Specialty Referral CentersBaltimore Regional Burn Center, Johns Hopkins Bayview Medical Center 34Burn Center at the Washington Hospital Center 34The Curtis National Hand Center, Union Memorial Hospital 35Hyperbaric Medicine Center, R Adams Cowley Shock Trauma Center 36Maryland Eye Trauma System: The Johns Hopkins Wilmer Eye Institute 36Maryland Eye Trauma System: Suburban Hospital Eye Trauma Center 38Neurotrauma Center, R Adams Cowley Shock Trauma Center 38Pediatric Trauma Center, The Johns Hopkins Children’s Center 38Pediatric Trauma Center, Children’s National Medical Center 39Perinatal Referral Centers 40

ii
Poison Consultation Center, Maryland Poison Center 40
Rehabilitation 42
Maryland Trauma Statistics 43Combined Adult & Pediatric Trauma Statistics Report
Age Distribution of Adult & Pediatric Trauma 43Maryland Adult Trauma Statistics Report (Tables & Graphs)
Total Cases Reported by Trauma Centers (3-Year Comparison) 43Gender of Patients 43Occurrence of Injury by County 44Residence of Patients by County 44Patients with Protective Devices at Time of Trauma Incident 44Age Distribution of Patients 45Emergency Department Arrivals by Day of Week 45Emergency Department Arrivals by Time of Day 45Mode of Patient Transport to Trauma Centers 45Origin of Patient Transport to Trauma Centers 45Number of Deaths by Age 46Number of Injuries by Age 46Number of Injuries and Deaths by Age 46Etiology of Injuries to Patients 46Blood Alcohol Content of Patients by Injury Type 46Injury Type Distribution of Patients 47Etiology Distribution for Patients with Blunt Injuries 47Etiology Distribution for Patients with Penetrating Injuries 47Etiology of Injuries by Age of Patients 47Final Disposition of Patients 48Injury Severity Score by Injury Type 48Injury Severity Scores of Patients with Blunt Injuries 48Injury Severity Scores of Patients with Penetrating Injuries 48Injury Severity Scores of Patients with Either Blunt or Penetrating Injuries 48
Maryland Pediatric Trauma Statistics Report (Tables & Graphs)Total Cases Reported by Trauma Center 49Gender Profile 49Emergency Department Arrivals by Day of Week 49Emergency Department Arrivals by Time of Day 49Occurrence of Injury by County 49Mode of Transport 50Origin of Patient Transport 50Disposition of Patients 50Outcome Profile 50Etiology of Injuries by Ages of Patients 50Mechanism of Injury 51Injury Type 51Number of Injuries and Deaths by Age 51Number of Injuries by Age 51Number of Deaths by Age 51Children with Protective Devices at Time of Trauma Incident 52Residence of Injury by County 52
National Study Center for Trauma and EMS 53
Current Listing of EMS Board, Statewide EMS Advisory Council, and MIEMSS Executive Staff inside back cover

Donald L. DeVries, Jr., Esq.Chairperson, EMS Board
Tragedy has no zip code. Accidents strike any-where. Mother Nature is indiscriminant when sheis wreaking havoc. Emergency Medical Services(EMS), unlike Wal-Mart or McDonald’s, cannotselect demographics-driven locations for its base.Maryland’s EMS system is only as strong as it isin the most remote area of the state. EMS must beprepared to respond at a moment’s notice inBaltimore, Annapolis, Bel Air, Gaithersburg . . . orFinzel, Maryland.
Finzel, in Western Maryland, is so small that ithas no mayor, no local police, no public paidwork force, and no recognition in the U.S.Census. Yet, on top of fog-shrouded Big SavageMountain in Garrett County on May 23, 2003, itwas the scene of a mass collision involving 85vehicles that tested the responsiveness andresourcefulness of fire and EMS in Maryland.
Visibility was nearly zero on the Appalachianridge around 1:15 PM at marker 29 in the east-bound lane of I-68 when five cars were involvedin a crash. The Eastern Garrett Volunteer FireDepartment and the Frostburg Area AmbulanceService responded. At 2 PM, as patients werebeing treated and loaded into ambulances andvehicles were being moved out of the roadway,motorists in the westbound lane of I-68, slowingto see what was occurring at the wreck site, set offa second chain-reaction crash. The mass collisioninvolved 40 separate collisions, 80 vehicles, andultimately led to 70 injured patients and twodeaths. Over 12 excruciatingly long minutes, carsand trucks plowed into each other. A tangle ofdamaged cars, trucks, and tractor-trailers was leftin its wake. A 20-mile stretch of I-68 was closed inboth directions, from LaVale to Grantsville.
There are countless stories of personal kind-nesses, of a town too small to get even an honor-able mention in the census, taking on a gargantu-an task. Neighbors offered food and consolation tostrangers; stranded families were provided homesto stay in; school buses appeared out of the mistto ferry motorists to the Finzel town hall wherevolunteers served up food and comfort.
The incident was also remarkable for thebroad range of EMS services that melded seam-lessly in response. The system of care thatMIEMSS has developed over decades workedeffectively in one of the most rural areas of thestate. Lessons learned from drills and educationalprograms dealing with chain-reaction crashes thathave been offered to providers in recent yearswere implemented. Thirty ambulances, public andcommercial, paid and volunteer, from Maryland,Pennsylvania, and West Virginia responded. Theskills taught to first responders and emergencymedical services technicians were tested. TheMaryland State Police Crash Team reported to thescene. A Red Cross shelter was set up three milesfrom the incident. The extrication equipment usedto free victims, paid for by Highway Safety grantssecured through the Maryland State HighwayAdministration by MIEMSS and the Region I(Western Maryland) Advisory Council, workedflawlessly. Sacred Heart Hospital, CumberlandMemorial Hospital, and the R Adams CowleyShock Trauma Center, all members of Maryland’ssystem of hospital trauma care, received and treat-ed patients from the incident. The 9-1-1 centers in Garrett and Allegany counties provided the com-munications coordination. MIEMSS communica-
1
FROM THE EMS BOARD CHAIRPERSON
2
MIEMSStions channels linked those at the scene to the hos-pitals. The Critical Injury Stress ManagementTeam offered stress management to responders,some of whom witnessed deaths only a few feet infront of them as cars crashed in the fog.
The "System" worked. Was it flawless? Mostlikely not, and those driving our EMS systemalways strive to be better, to be on the cuttingedge. Representatives from responding fire, EMS,police, state highway, and the Red Cross havealready met to discuss the positive and negativeaspects of the response to the incident and willmeet again to address areas of concern.
But, the entire scene was cleared of more than70 patients within two hours. The Golden Hourwas met for all serious trauma patients. The spiritof cooperation between fire and EMS was excel-lent at the scene. Beyond skills, providers demon-strated the spirit that drives our system and makesit the best in the world. Lives were saved, injurieswere treated effectively and expeditiously. Thiswas truly an example of the "cooperative excel-lence" that is the hallmark of Maryland’s EMSsystem.
We are fortunate to have a system in place inMaryland that can respond to urban streets andalleys, to suburban malls and ball fields, to ruralseashores and mountain vistas. The topographyand demographics of Maryland offer a wide arrayof challenges to fire and EMS, and I am pleasedto report that these challenges are being met everyday by a cadre of dedicated people supported bya system steeped in tradition and success. Thanksto everyone involved in the delivery ofEmergency Medical Services in Maryland.
Robert R. Bass, MD, FACEPExecutive Director, MIEMSS
FROM THE EXECUTIVE DIRECTORThe past year has been a challenge and the
prospects for the near future are also challenging.The nationwide recession reached Maryland. Ourcountry has been engaged in war and is still reel-ing from terrorist acts that touched our shores.The challenges for the fire and EMS services aregreat. Yet, because of the efforts of many over thepast decade, I am confident we are better pre-pared to meet these challenges.
July marked the 10-year anniversary of theimplementation of Maryland’s EMS Law. Liketoday, the 1990s began with the nation at war andin the throes of a recession that threatened toclaim Maryland EMS as a victim. Draconian bud-get cuts were proposed to the State’s EMS agen-cies and to state support for local fire and EMS.Statewide, EMS was struggling with leadershipissues, its place in state government, and its rolewithin the EMS community. However, with thesupport of Maryland’s fire and EMS community,the executive and legislative leadership respond-ed, first creating the EMS Operations Fund in1992, and then enacting House Bill 1222, theEMS Law, in 1993.
The EMS Operations Fund was enacted toprovide a source of revenue dedicated solely tothe Maryland Fire and Rescue Institute, theMaryland Institute for Emergency Medical

3
Services Systems, the Aviation Division of theMaryland State Police, the Shock Trauma Center,and State Aid to Local Fire, Rescue, andAmbulance Services (now known as the AmossFund). The Fund was expected to provide a stablefunding resource for the state’s EMS and fire-relat-ed organizations. In fact, each of the entities sup-ported by the Fund has realized a modest growthover this decade that has strengthened fire andEMS services in Maryland.
The leadership structure created by the EMSLaw was equally important to MIEMSS and thefire and EMS communities. The law clarified thelegal authority and organizational framework forEMS in Maryland. The legislation establishedMIEMSS as an independent, executive-level stateagency and created an EMS Board and AdvisoryCouncil to provide oversight, communication, par-ticipation, and leadership for the system. The lawdetailed MIEMSS’ responsibilities and its role insupport of emergency medical services and theEMS Board. The Board and Advisory Council sitatop a pyramid of subcommittees that promoteeffective, broad-based participation from the fireand EMS community and a process of "consensusbuilding" that leads to "cooperative excellence."The Board and SEMSAC have been extremelyeffective advocates for EMS in Maryland, provid-ing direction to MIEMSS.
Despite our significant advances, we still faceboth old and new challenges. A principal focus ofMIEMSS is enhancing the use and value of theresources that we have to support local providersand the improvement of patient outcome. This isaccomplished by collecting data and evaluatingthe quality of the care. Quality improvement inte-grates planning and leadership with data utiliza-tion and analysis in cooperation with customersand stakeholders. Over the years, and in conjunc-tion with other EMS-related agencies, Marylandhas amassed a wide variety of data. This databasewill be enhanced within the next year by theintroduction of the Electronic MarylandAmbulance Information System (EMAIS). Ourchallenge is to utilize this database with an eyetoward improving the effectiveness of the EMSsystem.
MIEMSS’ responsibilities will continue toinclude the statewide EMS communications sys-tem, licensing or certifying over 30,000 EMSproviders, system medical oversight, regionaladministration, hospital designation, and injuryprevention and education. In the past decade, theEMS for Children Program, and more recently,Geriatric EMS, regulation of commercial ambu-lances, and participating in domestic preparednessefforts have increasingly become important priori-ties for MIEMSS.
Events of recent years have added new priori-ties for MIEMSS. The agency has an importantrole in the planning related to Weapons of MassDestruction. With the Department of Health andMental Hygiene, the agency developed the state’smedical response plan. MIEMSS supports thehealth function at the state’s EmergencyOperations Center and has a trained cadre ofRapid Response Teams with defined responsibili-ties for multi-casualty events. Through ourEMRC/SYSCOM communications center and theFacility Resource Emergency Database (FRED)that was created by MIEMSS staff, MIEMSS isthe information repository for these events, pro-viding statewide advisories of events, call-downsfor emergency department availability, resourcecataloging, syndromic surveillance, and patienttracking.
I invite you to read through our report to gainfurther, detailed insight into what we are accom-plishing and where we are going.
We have come a long way in the past tenyears. The laws that were enacted in the early1990s have been invaluable to us in our efforts tomeet our mission. But, more important are thepeople working within the framework of our sys-tem. I thank the fire and EMS community, bothvolunteer and career, for its partnership over thepast decade. Fire and Emergency Medical Servicesin Maryland are remarkable for their integratedapproach and dedicated personnel. The partner-ship between fire and EMS is strong, and its rootsare firmly planted in each and every jurisdiction.Your support has been vital, and will be as impor-tant in the future. I thank you and pledge our con-tinued efforts to strengthen and improve emer-gency medical services in the state of Maryland.

4
ADMINISTRATIONMission: To secure and effectively utilize financialand personnel resources that will enable MIEMSSto meet its goals and objectives in a manner that isconsistent with state regulations and policies.
The Administration Office is responsible forthe financial, purchasing, and human resourcesservices of MIEMSS.
The finance staff is responsible for accountingprocesses to ensure that expenditures are in com-pliance with applicable regulations. The staffdevelops the budget, tracks and monitors expendi-tures, and performs year-end closing. The stafftracks special funds, grant funds, and reimbursablefunds.
The purchasing staff procures all necessarysupplies, materials, and services for the MIEMSSstaff. It is also responsible for the timely paymentof invoices.
The human resources staff is responsible forrecruitment, timekeeping, payroll-related services,benefits and retirement coordination, personnelevaluation processes, and other traditional person-nel functions.
The Administration Office is also accountablefor inventory control, fleet management, travelservices, and building operations and mainte-nance.
Most administrative, fleet, meeting, and officecosts are centrally funded through theAdministration’s budget.
MIEMSS FY 2003 budget information is dis-played by state object code and department in thecharts on page 5.
AEROMEDICAL OPERATIONSMission: To provide the physician medical supportnecessary for the Maryland State Police AviationDivision to meet the emergency helicopter needs ofMaryland’s citizens. The State Aeromedical Directoris actively involved in the ongoing training and ver-ification of skill proficiency for the State Policeflight paramedics. He provides around the clock con-sultation support to SYSCOM for med-evac requestsand medical direction and is actively involved in thedevelopment of new patient care protocols and theoversight of ongoing care.
In FY 2003 there were 5,011 patients trans-ported by the Maryland State Police (MSP)Aviation Division. Of these patients, 4,759 (95%)were transported from the scene of injury at therequest of the local fire services, and 252 (5%)were transported between hospitals to a higherlevel of care.
Types of calls included the following:• Motor vehicle crashes 2,464• Falls 689• Pedestrians 211• Gunshot wounds 125• Assaults 104• Burns 96• Industrial accidents 80• Stabbings 66• Hand injuries 52• Hyperbaric patients 17• Eye injuries 10• Drownings 8• Electrocutions 6
Interfacility transports included the followingtypes of patients:
• Trauma 107• Medical 76• Neonatal 69
FY 2003($46,427,238)
EMS Operations Fund
MFRI = Maryland Fire & Rescue Institute • STC = R Adams Cowley Shock Trauma CenterMSP = Maryland State Police
FY 2004($54,182,241)
MIEMSS$9.7 m
MFRI$6.3 m
STC$3.4 m
AmossFund
$10.0 m
MSPAviation$12.6 m
VolunteerLoan Fund$1.0 m
STC Building/Equipment
Fund$3.5 m
MIEMSS$10.1 m
MFRI$5.9 m
STC$3.5 m
AmossFund
$10.0 m
MSPAviation
$14.8 m
VolunteerLoan Fund$6.4 m
STC Building/Equipment
Fund$3.5 m

5
In FY 2003, Maryland's EMS communitycommemorated the transport of the MSP AviationDivision's 100,000th patient. In continuous opera-tion since March 19, 1970, the MSP program is
the oldest existing med-evac program for thetransport of civilians in the country.
FY 2003 saw the Aviation Division initiateparticipation in the new Pediatric Rapid SequenceIntubation (RSI) pilot protocol, in addition tomaintaining participation in the current Adult RSIpilot. Designed to address the needs of patientswith severe head injuries, these RSI pilot proto-cols allow MSP flight paramedics to use neuro-muscular blocking agents in the field to provideendotracheal intubation for patients who are notbreathing adequately.
Advanced scenario-based training was againutilized for division flight paramedics in jointtraining exercises with the U.S. Secret Service atthe Secret Service training facility. These exercisesallowed life-like simulation of patient care situa-tions as would be faced by flight paramedics inthe course of their normal duties.
FY 2003 also saw the continuation of efforts tocomputerize the documentation of patient careinformation. Once complete, this process will bet-ter allow for linkage with patient outcome infor-mation, thereby giving greater ability to evaluatehow best to optimize patient care.
ATTORNEY GENERAL’S OFFICEMission: To provide legal advice to the EMS Board,the Statewide EMS Advisory Council, andMIEMSS in connection with all aspects of emer-gency medical services, the ongoing administrativefunctions of the agency, and the regulation of com-mercial ambulance services. The Attorney General’sOffice also serves as the administrative prosecutorfor cases involving allegations of prohibited acts byEMS providers before the EMS Provider ReviewPanel, the EMS Board, the Office of AdministrativeHearings, and the courts.
During the past fiscal year, the AttorneyGeneral’s Office continued to support MIEMSSin promulgating and implementing the agency’sregulations and procurement and contracts,including technology initiatives.
The Attorney General’s Office reviewed andprosecuted 37 cases of alleged prohibited acts byEMS providers and applicants, litigated a freedomof information act claim, and successfully defend-ed a procurement claim in connection with theElectronic Maryland Ambulance InformationSystem (EMAIS) RFP.
The Attorney General’s Office participated in
MIEMSS FY 2003 EXPENDITURE BY OBJECT CODE (INCLUDES SPECIAL,
REIMBURSEABLE AND FEDERAL FUNDS)
FY 2003Actual
Number of Positions 92.1Salaries and Wages $6,193,195Technical/Special Fees 402,382Communication 1,100,014Travel 117,477Fuel and Utilities 36,887Motor Vehicle Operation and Maintenance 170,815Contractual Services 1,295,409Supplies and Materials 201,465Equipment—Replacement 69,985Equipment—Additional 448,827Fixed Charges 68,466Grants 941,451
Total Salary and Wages $6,995,577Total Operating Expenses $4,450,796Total Expenditure $11,046,373
MIEMSS FY 2003 APPROPRIATION BY DEPARTMENT
Administrative OfficesExecutive Director, Legal Office $591,827Financial & Human Resources Administration 1,012,347Planning/Program Development/Total Quality Management 253,289
CommunicationsEquipment 972,745Maintenance 1,111,026EMRC/SYSCOM 1,006,338
Education/Public InformationLicensure, & Certification 1,239,994Public Information & Media Services 536,139Emergency Health Services Program 93,500
Information Technology 1,099,592
Medical ServicesOffice of Medical Director 558,669Office of Hospital Programs 105,339EMS-Children 154,888
Regional Administration 861,945
Commercial Ambulance Program 220,000
GrantsEMS-Children 100,000Perinatal Center Designation Program 75,000
TOTAL $9,992,648

a variety of committees, task forces, and workgroups. The Attorney General’s Office workedwith MIEMSS to implement changes to theEmergency Medical Services Do Not Resuscitateprogram. The Attorney General’s Office also par-ticipates in a work group of Assistant AttorneysGeneral representing several state agencies study-ing the state’s response to bioterrorism and othersecurity issues. In addition, the Attorney General’sOffice participated in task forces monitoring theAutomated External Defibrillator (AED) program,the Yellow Alert program, and developing EMAISto replace the current paper runsheet with a com-puter software application.
The Office also assisted in the interpretationand implementation of the Homeland Security Actof 2002 as it related to the smallpox vaccinationinitiative and the Smallpox Emergency PersonnelProtection Act of 2003.
The Attorney General’s Office presented sev-eral educational programs on the HIPAA Privacyregulations and data transaction set regulations. Apresentation by the Office was videotaped and dis-tributed, along with sample forms to be used inimplementing the HIPAA privacy regulations.These will assist EMS units in education and train-ing. Presentations were also made explaining thefederal ambulance restocking safe harbor regula-tions, and a state regulation was written to assist inimplementing the safe harbor regulation.
The Attorney’s General’s Office assisted in theadministration of state and federal grants, and inlicensing the MIEMSS Facility ResourceEmergency Database program to Pennsylvania.
COMMUNICATIONS ENGINEERINGSERVICES
Mission: To provide the equipment, support, andexpertise necessary to operate the statewide emer-gency medical services communications system.
The main highlight for MIEMSSCommunications for FY 2003 was the integrationof Frederick County EMS services into theBaltimore Emergency Medical Resource Center(EMRC). With this change, all Frederick EMSproviders now have access to the entire networkprovided by SYSCOM and EMRC. Thisenhances the services by allowing rapid conferenc-ing between the field provider and all of the fixedmedical resources in the Baltimore–Washington
region, as well as Frederick County’s hospital.MIEMSS Communications continued sup-
porting the statewide radio infrastructure projectwith the installation of new towers at Kingsville(Baltimore County), Stoney Forest (HarfordCounty), Hagerstown (Washington County), andFederalsburg (Caroline County). A new communi-cations shelter was installed at the DorchesterCounty Bucktown site. Dorchester County provid-ed the equipment to establish the last digital linkbetween Baltimore and Ocean City.
A new digital microwave link was installedbetween the MIEMSS backbone to the PikesvilleMaryland State Police (MSP) Headquarters. Thiswill permit access to the MIEMSS helicopter cadsystem over a private and secure network.
Three regular Central Alarm AdvisoryCouncil meetings were held around the state—onein Queen Anne’s County, one in WashingtonCounty, and one in Baltimore City.
A total of 120 mobile EMS radios were dis-tributed throughout the state at a cost of $83,400.Funding in the amount of $315,000 was suppliedfor grants for Cardiac Monitor/Defibrillators andAutomated External Defibrillators (AEDs).
A new wireless digital project was started toprovide data connectivity between the variouspublic safety entities in Maryland. The prototypesystem was deployed in Easton, Maryland (TalbotCounty). This system uses a small amount of thedigital microwave capacity to link MIEMSS, theMSP, and the State Highway Administration totheir respective facilities in Easton. Later, otherstate and local agencies will join this network.
MIEMSS Communications processed a totalof 752 service reports for FY 2003. In addition,staff performed 90 ambulance radio inspectionsunder the Volunteer Ambulance InspectionProgram.
6
7
COMPLIANCE OFFICEMission: To ensure the health, safety, and welfare ofthe public as it relates to the delivery of emergencymedical services by Emergency Medical ServicesProviders throughout Maryland. To that end, theCompliance Office is responsible for ensuring qualityof care by investigating complaints and allegationsof prohibited conduct.
The Compliance Office works closely with theProvider Review Panel (PRP) panel (the 13-mem-ber panel composed of all levels of EMSproviders; physicians representing the MarylandBoard of Physicians, the Maryland MedicalChirurgical Society, and the EMS OperationalProgram Medical Directors; the State EMSMedical Director; the MIEMSS ExecutiveDirector; the EMS Board; and the AttorneyGeneral’s Office). The PRP reviews complaints, aswell as the results of the investigations conductedby the Compliance Office, and recommends to theEMS Board any further action.
ACTIVITY REPORT OF THE INCIDENTREVIEW COMMITTEE (IRC), EMSPROVIDER REVIEW PANEL (PRP), ANDTHE EMS BOARD
• Incidents Reported to IRC 224• IRC Investigations Initiated 200• IRC Investigations Conducted 185• IRC Investigations Continued 24• IRC Complaints Forwarded to PRP 37• Complaints Dismissed by PRP 2• Complaints Forwarded to EMS Board 37
EMS Board Action• Reprimands 3• Probation 6• Suspensions 6• Revocations 6• Remedial training 5• Surrenders 0• Evaluation 2• Applications Denied 5• Case Resolution Conferences 5• Dismissed 2
EMERGENCY HEALTH SERVICESDEPARTMENT
UNIVERSITY OF MARYLAND, BALTIMORE COUNTY
Mission: To provide leadership in the field of emer-gency health services through excellence in education.This educational excellence is supported by an activeresearch agenda, service to the University and EMScommunities, and provision of professional continu-ing education. The EHS Department recognizes asconstituents the University of Maryland atBaltimore County, MIEMSS, and the Maryland,national, and international EMS communities.
The Emergency Health Services (EHS)Department received a continuation of its contractfor the third year with the U.S. Public HealthService to develop and provide training and edu-cation for over 8,000 members of the NationalDisaster Medical System (NDMS). This year'sbudget is a little over $ 2 million, with emphasison creating training for special response teams,including teams focused on surgical, veterinary,mortuary, and international responses to disasters.Headed by Rick Bissell, the EHS team now hasover 50 courses completed and available forNDMS members nationwide.
Demand has increased for our students upongraduation, with an increasing shortage of quali-fied paramedics nationwide and rapidly growingemployment for management and graduate stu-dents in the realm of homeland security.Numerous current students and recent graduatesare now working for the Department of HomelandSecurity, the National Disaster Medical System,the Centers for Disease Control and Prevention,and related contractors such as Titan/RPI andBooze-Allen-Hamilton.
Undergraduate enrollment continues toincrease, especially in the paramedic track. Onereason for this is the opening of the EHS LivingLearning Center, an academic residential commu-nity for EHS majors. The department alsoreceived Maryland accreditation from MIEMSSand continues to maintain national accreditationthrough CAAHEP.
To date, EHS has contracts with 26 education-al institutions nationwide to provide critical caretransport training utilizing the department’sCritical Care Transport Course. In 2001, 634 stu-dents, and in the first half of 2002, 240 students,

8
attended Critical Care Transport courses. Sixty-five students have completed the Pediatric andNeonatal Critical Care Transport Course since itsfirst offering in 2001.
EMERGENCY MEDICAL SERVICES FOR CHILDREN
Mission: To provide the leadership,direction, and expertise in the coor-dination of resources that focus onthe unique needs of children andtheir families in a manner that facilitates the effi-cient and effective delivery of prehospital, hospital,and restorative care throughout the state. Theseresources include injury and illness prevention, clini-cal protocols, standards of care and facility regula-tion, quality improvement initiatives, interagencycollaboration, and initial and continuing educationfor providers across the continuum of care that willpromote the health and well-being of children inMaryland.
The Emergency Medical Services for Children(EMSC) Program is responsible for the develop-ment of statewide guidelines and resources forpediatric care, the review of pediatric emergency
care and facility regulations, coordination of pedi-atric education programs, and collaboration withother agencies and organizations focused on child-hood health and illness and injury prevention. TheEMSC Program coordinates the state PediatricEmergency Medical Advisory Group (PEMAG),the state Pediatric Quality ImprovementCommittee, and the five Regional Pediatric EMSAdvisory Committees. Federal EMSC grants arecoordinated through the Maryland EMSCProgram Office, involving statewide projects, spe-cialized targeted issues, projects, and research ini-tiatives at academic universities.
MIEMSS has again been awarded an EMSCState Partnership Grant from the Maternal ChildHealth Bureau of the Department of Health andHuman Services in joint sponsorship with theNational Highway Traffic Safety Administration(NHTSA). The 2000-2004 EMSC PartnershipGrant has two major focus areas: (1) ABC’s ofKIDS: Preparing and Planning for the Needs ofChildren in Disasters and (2) Injury PreventionInitiatives for Children through the Introduction ofthe RISK WATCH® Curriculum from theNational Fire Protection Association. The 2003-2006 EMSC Partnership Grant continues to build
Applicant
Region IFrostburg Area Service
Region IGarrett County
Region IVShore Health Systems–Easton Maryland
Region VMontgomery County DFRS
Region VRegion V Education Council
Target Area
Children 0-12 in Frostburg areaand county
School-age children in GarrettCounty
Eastern Shore families
School-age children inMontgomery County
Prince George’s County Special School
Summary of Project
Child Safety Seat (CSS) Checks for Allegany Countyarea. Continue to support the CPS resource withinFrostburg with the purchase of CSS & materials for 2 seatchecks.
Pre-Incident Planning System (PIPS)Establish the technical resources and hardware to imple-ment the PIPS computer system for school preplanning.
Hunting: A Safety and Family TraditionDevelopment of a safety poster focused on safe huntingpractices for both land and water recreational/sport hunt-ing.
Children Should Be Seen and Not Hurt Bike helmet distribution in coordination with a safetyevent & new Boys & Girls Club in northern county inhigh-risk area.
Adapting RISK WATCH® for Preschool Childrenwith SHCN Adaptation of tools and toys for RISK WATCH atWheatley Special Center serving 700 children, ages 2-6with special needs.
EMS Based Injury Prevention Program for Children special projects were funded through the EMSCPartnership Grant for the fourth year. The following awards were made:

9
on the integration of EMSC with new interagencycollaborations with the Maryland chapter of theAmerican Academy of Pediatrics and theMaryland State Department of Education.
This grant will provide for further integrationof the Kids in Disasters initiatives with a review ofexisting programs, plans, and policies for inclusionof the needs of children and families and expand-ing the JUMPSTART triage training and disasterpreplanning with schools. The Kids in Disastersproject includes the following initiatives: 1. Pediatric Triage Training with JUMPSTART &START workshops with corresponding table-topexercises and scenarios focused on children.Educational opportunities will be expanded toinclude school and public health nurses, and sce-narios will include children with special learningand health needs.2. Moulage workshops have been developed to
recruit and maintain a team of volunteers to assistwith drills. The project has also established amoulage resource kit and moulage workshop-train-ing document and pictorial files.3. The Maryland Virtual Emergency Response
Systems (MVERS) joint project with the MarylandState Police, MIEMSS Rapid Response Team, andschool partners. The MVERS program providesworksheets for gathering information and thepage-builder software on CD-ROM to store andrecall the essential data in an organized format forall aspects of an emergency response. The pro-gram will improve and enhance the communica-tion and coordinated response of public safety,public health, and educational professionals to crit-ical incidents, both man-made and natural.
In October 2002, the Maryland EMSC pro-gram hosted the first Mid-Atlantic eight-stateEMSC Regional Symposium in Columbia,Maryland through an EMSC Supplemental Grantfrom MCHB and NHTSA. This two-day sympo-sium brought together interdisciplinary representa-tives from surrounding states to promote the dis-semination of knowledge and programs developedfrom federal grant awards and to increase commu-nication throughout the region. The Mid-AtlanticEMSC group grew from the existing AtlanticEMS Council that includes Virginia, WestVirginia, the District of Columbia, Maryland,Delaware, Pennsylvania, and New Jersey. TheEMSC group has recently expanded to includeNew York State. During June 2003, the MarylandEMSC and Public Information & Media Servicesoffices collaborated with the District of Columbia
EMSC Partnership Grant team for the secondMid-Atlantic EMSC Regional Symposium held inWashington, DC. The Maryland RISKWATCH®, Kids in Disasters, and School HealthFirst Aid Guidelines were presented at these twosymposiums.
The EMSC Program received a MarylandDepartment of Transportation Highway SafetyGrant to initiate an assessment of hospitalresources and knowledge on child passenger safe-ty. The focus for the second year of the HospitalChild Passenger Safety (CPS) Project grant was toincrease the educational opportunities for healthcare providers and to provide current and accuratechild passenger safety information. During the pastyear, the project has conducted five regional work-shops on CPS for Children with Special HealthCare Needs and held two conferences on SafeTransport for All Children offered to clinicians,public safety, and child health advocates through-out the state. CPS resource packets were devel-oped and delivered to every acute care hospital inthe state by Certified Child Passenger SafetyTechnicians. Promotional materials were devel-oped for occupant protection initiatives for all agesjointly with the MIEMSS Public Information &Media Services staff.
Maryland was awarded a RISK WATCH®Champion Award for 2003 from the National FireProtection Association (NFPA). The EmergencyMedical Services for Children (EMSC) program atMIEMSS is the lead agency coordinating this two-year initiative, along with other state partners fromthe Office of the Maryland State Fire Marshal, theMaryland State Police, and the MarylandDepartment of Education. Other partners in RISKWATCH® include Maryland SAFE KIDS, theFire Prevention Committee of the Maryland StateFiremen’s Association, the State HighwayAdministration, the Maryland & National CapitalPoison Centers, the Maryland Chapter of theAmerican Trauma Society (ATS), and theMaryland Department of Natural Resources. During the first year of the Champion Awardgiven to Maryland, five communities have com-mitted to place the RISK WATCH® program into20 classrooms during fall 2003. The five communi-ties are Howard, Montgomery, and PrinceGeorge’s counties, the special needs schools inMaryland, and parochial schools in CharlesCounty. During the second year of the Championproject, the RISK WATCH® program will expandinto 100 more classrooms in Maryland, with

10
implementation during the academic school year.The EMSC Program staff and medical direc-
tors from PEMAG continued to supportPrehospital Education for Prehospital Providers(PEPP) courses and coordinate the PEPPstatewide steering committee to facilitate sharingof faculty resources, plan for recertification, andidentify material that correlates with the MarylandEMS Medical Protocols. This steering committeemeets jointly with the state PEMAG and theMaryland chapter of the American Academy ofPediatrics’ (AAP) Committee on PediatricEmergency Medicine. Based upon the consensusprocess, the PEPP curriculum has been enhancedto include models that complement the MarylandEMS Medical Protocols and address those clinicalskills that the Pediatric QIC and Pediatric BaseStations have identified as high risk and low vol-ume. The Children with Special Health Care edu-cational modules and equipment have also beenintegrated in the PEPP courses offered and sup-ported by the EMSC Office and the MarylandAAP. Maryland Enhanced PEPP courses havebeen provided to more than 500 ALS and BLSproviders, and 12 pediatric medical directors havecompleted the course and been approved by thenational AAP. The first PEPP Refresher coursewas held at Winterfest 2003 in January for bothALS and BLS providers.
Prehospital continuing education programswere offered at several conferences throughout thestate. Pyramid 2002 included a Moulage workshopand JUMPSTART training stations. Winterfest2003 featured workshops on Child Abuse,Pediatric Respiratory Care, and JUMPSTART.The EMS Care 2003 state conference included aMaryland Enhanced BLS PEPP course, PediatricBurns, Crash Reconstruction, JUMPSTART, andPediatric Case Reviews. The Maryland Responseto School Bus Incidents with Special Emphasis onChildren with Special Needs was completed bythe Region V Office and is available on CD-ROMfor interdisciplinary training. The Moulage andSchool Bus programs were featured at the 2003National EMSC Grantees meeting in Washington,DC.
The EMSC Program staff actively participatesin national, state, and local SAFE KIDS coalitions;the Maryland division of the American TraumaSociety; the Maryland Occupant Task Force; andthe Child Passenger Safety Board coordinated bythe State Highway Administration. This collabora-
tion provides a consistent flow of information tothe five regional pediatric committees and thestate PEMAG on injury prevention resources andinitiatives.
EMRC/SYSCOMMission: To provide communication services to assistin the quality of care provided patients inMaryland’s EMS System and coordinate the trans-port of critically ill or injured patients by med-evachelicopter.
In FY 2003, the Emergency MedicalResources Center (EMRC) handled 142,291 tele-phone calls and 108,970 radio calls. Of these251,261 calls, 94,751 were communications involv-ing a patient or an incident with multiple patients.During the same time frame, the SystemsCommunications Center (SYSCOM) handled64,563 telephone calls and 4,529 radio calls. Ofthese 69,092 calls, 6,540 were related to requestsfor med-evac helicopters. However, not allrequests resulted in the transport of a patient.Some requests were canceled by the requestor orwere unable to be completed due to weather orother factors.
EMRC/SYSCOM continued participation inthe National Disaster Medical System (NDMS).Utilizing FRED, the Facility Resource EmergencyDatabase, EMRC/SYSCOM obtained bed statusinformation for routine quarterly reports and inresponse to specific requests related to the war inIraq.
FRED was also utilized by EMRC/SYSCOMin support of several drills, such as the REFLEXdrill, which was the first region-wide drill conduct-ed in Region III.
During the peak hospital alert season,December through March, the hospital alert poli-

11
cy/procedures were again modified. The EMRCscollected information on reasons for alerts andrequired specific names requesting the alerts.
EMS communications operations forFrederick County were incorporated into theEMRC. Access to EMRC for Frederick Countyunits is available both by conventional EMS radioand the Frederick County 800Mhz system.
HOSPITAL PROGRAMS OFFICEMission: To implement the designation and verifica-tion processes for trauma and specialty referral cen-ters, to provide continuing evaluation of these centersfor compliance with the regulations and standardsin COMAR 30.08 et seq., and to ensure ongoingquality monitoring of the trauma/specialty care sys-tem.
The Hospital Programs staff continued tomanage and coordinate quality monitoring activi-ties for the trauma/specialty care system. Keycomponents of the ongoing monitoring activitiesare the trauma registry data analysis, monthlymeetings with the Maryland Trauma and SpecialtyCare Quality Improvement Committee, and case-specific follow-up on consumer complaints.
The office staff coordinated the designationprocess for the Neurotrauma Center and the re-verification process for seven of the nine traumacenters. These processes involved accepting andreviewing trauma center applications, obtaining anout-of-state review team, site visits to each of thecenters, and writing the report of findings.
The office staff worked with several membersof the MIEMSS administrative staff to support thework of the Legislative Trauma Funding StudyPanel.
The Hospital Programs Office continued toprovide support to the Maryland Traumatic BrainInjury Demonstration Project. This grant project isbeing coordinated through the MarylandDepartment of Health and Mental Hygiene(DHMH), which is the lead agency for traumaticbrain injury in Maryland. DHMH is collaboratingwith the Mental Hygiene Administration and theBrain Injury Association of Maryland to imple-ment project activities for training and outreachacross the State.
The office was successful in obtaining a$40,000 grant from the Health Resources andServices Administration (HRSA) Trauma-EMSSystems State Planning Grant. The purpose of this
grant was to evaluate the use of the Severe HeadInjury Treatment Standards in the nine adult trau-ma centers in Maryland. An evaluation tool wasdesigned and tested, followed by a chart audit of asample of severely head-injured patients at each ofthe adult trauma centers. The chart audits wereconducted by an out-of-state team consisting of aneurosurgeon and trauma nurse. The data are cur-rently being collated and analyzed.
A second year planning grant was submittedto HRSA with a request of $40,000 to evaluateaccess to trauma centers statewide, along with theappropriate triage of trauma patients to traumacenters.
INFORMATION TECHNOLOGYMission: To provide leadership, expertise, and coor-dination in information systems, data management,networking, and application development relating toemergency medical services systems.
Work continued on EMAIS (ElectronicMaryland Ambulance Information System),designed to replace the current paper runsheetwith a computer software application. Currently,commercial, paid, and volunteer EMS providersfill out more than 700,000 paper MAIS runsheetseach year. EMAIS will save money, improve thequality of the data, and shorten the time to submitdata to MIEMSS. MIEMSS published a Requestfor Proposal for a web-based accessible system inFebruary 2002. The contract was awarded inOctober 2002. EMAIS is currently in beta testingand will be rolled out to the first of seven pilotprogram jurisdictions starting October 2003.
The County Hospital Alert Tracking System(CHATS) tracks six different alert types for thehospitals and jurisdictions of Region III andRegion V. Those data help identify emergencydepartment overcrowding as it occurs, so thatambulances may be redirected to less crowded

12
facilities, as needed. Participating hospitals and thepublic are able to view the status of the hospitalsat all times via the MIEMSS external web page.
MIEMSS continues to use its web-based sys-tem called FRED (Facility Resource EmergencyDatabase). This was developed in response to the9/11 tragedy. During any disaster or emergency,MIEMSS would contact hospitals for a status ofavailable beds. The time for the hospitals torespond would vary, depending on numerous fac-tors, but it could take many hours for all hospitalsto respond. FRED allows MIEMSS to send analert to all hospitals requesting an update on theircurrent status. This includes not only beds, butalso staffing and medications, as well as informa-tion from the local jurisdictions regarding EMSstaffing. FRED will reduce the time it takes to col-lect this data and make the process more efficient.
MIEMSS began actively pursuing itseGovernment goals in FY 2001 and continued tomake progress in FY 2003. Thus far, CHATS sys-tem status is accessible via the MIEMSS webpage. In addition, MIEMSS staff can access theiremail via the MIEMSS web page. EMS providerswill also find copies of the protocols on-line andcan access their individual continuing educationreports. Hospitals can update their status viaFRED. EMAIS will allow MIEMSS to beginmoving its current paper data tracking system toan electronic web-based system
The Information Technology Department con-tinued optical character recognition (OCR) scan-ning during FY 2003 to convert paper records toelectronic images. By scanning and capturingimages of prehospital care forms, it is possible tolink the electronic images of records to the MAISdatabase. Linking images to database records willmake available for review the text portions of theforms that are not otherwise captured electronical-ly. As of June 2003, MIEMSS has successfullyOCR-scanned over 1,550,000 MAIS forms.
MIEMSS continues to use its vast dataresources to answer many questions regardingEMS care in Maryland. The main access packageis a customer-defined system using MicrosoftOLAP (On-Line Analytical Processing). This givesMIEMSS staff the flexibility of looking at theMAIS database from numerous perspectives in auser-friendly environment. As its database contin-ues to grow with the addition of the EMAIS data,MIEMSS will be better prepared to answer evenmore questions about EMS in Maryland.
LICENSURE AND CERTIFICATIONMission: To coordinate a variety of services to protectthe public and to promote and facilitate the develop-ment of knowledgeable, skilled, and proficient pre-hospital professionals who deliver emergency care inthe Maryland EMS system.
During FY 2003, the number of career, volun-teer, and commercial prehospital providers inMaryland was 30,449, with the following break-down:
• First Responders 11,034• Emergency Medical
Technicians-Basic 15,548• Cardiac Rescue Technicians 490• Cardiac Rescue Technicians-(I) 136• Emergency Medical
Technicians-Paramedic 2,332• Emergency Medical Dispatchers 907
In cooperation with the Basic Life Support(BLS) Committee of the Statewide EMS AdvisoryCouncil (SEMSAC), the Office of Licensure &Certification designed, developed, and assistedwith the implementation of the new enhanced 24-hour EMT-Basic refresher course. Through analy-sis of data and educational trends, the BLSCommittee identified several topics to be coveredin the EMT refresher course. The modified con-tent includes specialized topics ranging from pedi-atrics to geriatrics, special medical devices, adultrespiratory emergencies, documentation, and oth-ers. The intent of the new content is to provideexisting EMTs with updates on current medicalinformation and applicable new information basedon the scope of practice for the Maryland EMT-Basic. The Maryland Fire & Rescue Institute(MFRI), in cooperation with MIEMSS, hostedseveral instructor rollouts of the new curriculumacross the state in 2002. Implementation of thenew curriculum took place in July 2002.
The Office of Licensure & Certification con-ducted several site visits for the advanced life sup-port (ALS) education program approval process.As of June 2003, eight education programs areapproved to offer ALS courses leading to licen-sure. Over 20 education programs are scheduledto complete the entire approval process byOctober 2004. The approval process, as outlinedin COMAR 30.04, requires a comprehensive self-study of the educational program and a site visit

13
by outside educators and medical directors. Thefindings of the self-study and site visit are thensubmitted to the EMS Board for approval.
In the fall of 2002, the Office of Licensure andCertification worked in conjunction with theCommercial Ambulance Office and theDepartment of Emergency Health Services at theUniversity of Maryland Baltimore County todesign and develop components of a curriculum toeducate existing paramedics with specialty caretransports. The proposed course is scheduled to bereviewed and approved by the EMS Board in thefall of 2003.
During May and June 2003, five first respon-der instructor update courses were held for lawenforcement instructors. The update courses, held
around the State, provided nearly 100 instructorswith the content and resources for including AEDin all first responder courses. Effective July 1,2003, all first responder basic and refresher cours-es include AED content. Given the prevalence ofAEDs in the public, as well as the inclusion ofAED content in all CPR courses since 2000, theaddition to the first responder curriculum was wellreceived.
In cooperation with MFRI and the MIEMSSPrehospital Education Quality ImprovementCommittee, the Office of Certification & Licensureanalyzed two years of data from the MarylandEmergency Services Student Application(MESSA) and Registry (MESSR). Informationobtained from the MESSR data includes studentoutcome, student demographics, State written andpractical examination results, and more. The infor-mation can be broken down and analyzed byinstructor, county, region, and course type.Information derived from the MESSR will beused to maximize the quality of EMS educationalprograms offered in Maryland. In addition, it willbe used to better meet the educational needs ofthe all learners.
MARYLAND CRITICAL INCIDENTSTRESS MANAGEMENT PROGRAM
Mission: To offer psychological support services tofirefighters, emergency medical technicians, police,and other emergency services personnel involved inemergency operations under extreme stress, to mini-mize the impact of job-related stress, and to helpaccelerate recovery of those persons exhibiting symp-toms of severe stress reaction.
The Maryland Critical Incident StressManagement (MCISM) program offers education,defusings, and debriefings conducted by astatewide team of trained volunteers. The teamconsists of volunteer doctoral or master-level psy-chosocial clinicians interested in working withemergency services personnel, and fire/rescue/lawenforcement peer-support persons trained in theprocess. Volunteer regional coordinators areresponsible for specific geographic areas of thestate and serve as the points of contact, throughlocal 9-1-1 centers and SYSCOM, for critical inci-dent stress management.

14
MEDICAL DIRECTOR’S OFFICEMission: To provide leadership and coordination forstate medical programs, protocols, and quality assur-ance, to liaison with the regional programs andclinical facilities, and to promote creative, respon-sive, and scientifically sound programs for the deliv-ery of medical care to all citizens.
Throughout FY 2002/03, the Office of theMedical Director has been working with theOffice of Information Technology on the develop-ment of the Electronic Maryland AmbulanceInformation System (EMAIS). The developmentprocess has included identifying data elements,designing screen layout, producing teaching mate-rials, and working with the vendor to ensure thesuccess of the program. Presentations providing anoverview of the system’s screen layouts and datapoints were conducted in jurisdictions across thestate.
In addition, the Office of the Medical Directorworked cooperatively with the MarylandDepartment of Health and Mental Hygiene(DHMH) to distribute funding through a ruralhealth grant to jurisdictions that qualify and agreeto participate in the EMAIS Pilot Program. Todate, seven jurisdictions have received $28,000 topurchase computer hardware for EMS stations,fire stations, and hospitals. Washington Countywill be the first pilot test for the new EMAIS soft-ware using the enhanced hardware for completionof the data set, as well as using the hardware foraccessing the Facility Resource EmergencyDatabase (FRED) and the County HospitalAlerting and Tracking System (CHATS). CecilCounty is anticipated to come online this fall asthe second pilot county.
In February 2003, an update to the MarylandMedical Protocols for EMS providers was distrib-uted to the jurisdictions. The new protocols weredeveloped after extensive review by the ProtocolReview Committee. Effective July 1, the new pro-tocols included:• A Chemical and Physical Restraint Protocol• A protocol for the administration of MARK IKits by BLS and ALS providers• A Stroke Protocol • An addition that would allow BLS providers touse glucometers• An addition to the AED protocol that addressesthe use of pediatric AED on patients from 1 to 8years of age
A PowerPoint presentation of the new protocolswas developed to assist the jurisdictions with theimplementation of the new protocols. The newprotocols and update materials are posted on theMIEMSS website.
In May a meeting was held with representa-tives from MIEMSS, the Maryland HospitalAssociation, and representatives from hospitalsacross the state to discuss the new Stroke Protocoland the designation of Acute Stroke CareFacilities. Consensus was reached and the Officeof the Medical Director was tasked with the devel-opment of guidelines for "levels" of Stroke CareFacilities. Three levels of stroke care facilities areto be identified, with a Level I Center providingcomprehensive care, a Level II Center providinginitial emergency management including screenand fibrinolytic therapy, and a Level III Centerthat will screen the patient and arrange immediatetransfer to a facility offering comprehensive or fib-rinolytic therapy. A draft of the guidelines is to bedeveloped for review by Fall 2003. In late June2003, a memo from the Office of the MedicalDirectors was distributed to all EMS providers sus-pending the transport guideline in the new proto-col until the designation process is completed.
The MIEMSS Rapid Response Team (RRT),coordinated in the Office of the Medical Director,was activated several times this year, primarily inresponse to severe weather. A tornado in CharlesCounty and record snowfall in many parts of thestate created several opportunities for the Team toutilize the agency’s new Facility ResourceEmergency Database. The increased threat of ter-rorism and subsequent war in Iraq prompted adeluge of preparation and planning forums. Inaddition to enhancements to the MIEMSSresponse plan, members of the RRT have assistedmany local, state, and federal agencies with thedevelopment of and revisions to their mass casual-ty response plans. The revisions of response plansresulted in a record number of drills and exercisesheld at the local, state, and federal levels. RapidResponse Team personnel participated in the plan-ning, executing, and evaluating of these exercisesat the local, state, and federal levels.
The Office of the Medical Director has beenworking with the Region III Quality ImprovementCommittee to establish a mechanism to reduce thenumber of unrecognized esophageal intubationsand to establish a mechanism for evaluating the"refusal of care" patients. The committee has

15
developed several recommendations for improvedairway assessment and real-time evaluation of suc-cess. Several recommendations on refusal of careare already making their way into the protocolcommittee discussions.
Seven of the EMS operational programs haveupdated their current Quality Assurance andQuality Improvement plans. These updates werereviewed by the Regional Quality ImprovementCommittee and the State EMS Medical Director.These programs demonstrated great improvementin the delivery of quality medical care and over-sight. Several EMS operational programs are cur-rently pursuing extensive quality improvementprojects.
The Medical Director’s Office was integrallyinvolved with the development of the newChemical Stockpile Emergency PreparednessProgram’s (CSEPP) nationally recognized "AllHazards Training Program." This is a 368-slidePowerPoint presentation designed to educatephysicians and EMS providers in the preparation,evaluation, and treatment of chemically/radiologi-cally contaminated or biologically exposed indi-viduals who may access the EMS/ healthcare sys-tem.
POLICY AND PLANNINGMission: To develop effective policies and innovativestrategies to enhance and improve the statewideemergency medical services system.
Yellow Alerts/Emergency DepartmentOvercrowding
MIEMSS continues to monitor statewide alertactivity via the County Hospital Alert TrackingSystem (CHATS) and provides monthly summaryreports containing individual facility alert activityto all hospitals. Overall alert activity continues toincrease annually and is particularly high duringthe flu and respiratory season. The 2002-2003 sea-son was a relatively light season in comparison toprevious years. Continuous online availability ofhospital alert activity status is available atwww.miemss.org/chats.
Lay Person Automated ExternalDefibrillator Program
The Lay Person Automated ExternalDefibrillator (AED) Program has continued togrow throughout Maryland. Under the program,non-health care facilities that meet certain require-
ments are permitted to have an AED on site to beused by trained lay persons in the event of a sud-den cardiac arrest until EMS arrives. Currently,there are more than 300 approved facilities in thestate. A list of AED facilities and program infor-mation can be viewed at www.miemss.org/AED.
The AED Task Force dealt with issues relatedto regulation revisions, as well as strategies forenhanced statewide placement of AEDs. The TaskForce was also provided with progress reportsfrom the Office of Epidemiology on the CardiacArrest Defibrillation Study.
MIEMSS, in partnership with EMS servicesin nine rural jurisdictions in Maryland, includingGarrett, St. Mary’s, Caroline, Dorchester, Kent,Somerset, Talbot, Wicomico, and Worcester coun-ties, obtained funds through the federal Office ofRural Health Policy’s FY 2002 Rural Access toEmergency Devices Grant Program that allowedplacement of AEDs and training in CPR and AEDuse in federally designated rural communities.More than 80 AEDs were placed in EMS, publicsafety, and layperson sites. MIEMSS has receivednotice that funds will again be awarded from theRural Access to Emergency Devices GrantProgram in FY 2003. The FY 2003 partnershipincludes the following five additional partial coun-ties by federally designated zip codes: Calvert,Washington, Frederick, Carroll, and Harford coun-ties.
MIEMSS partnered with several agencies andthe State Advisory Council on Heart Disease andStroke in a public awareness campaign designed toeducate citizens on the Chain of Survival. Thecampaign encourages learning CPR, how to usean AED, and developing public access defibrilla-tion programs when appropriate. The awarenesseffort was kicked off at a meeting of the StateAdvisory Council on Heart Disease and Strokewith a proclamation from Governor RobertEhrlich, Jr. that declared September 2003 "Partnerwith Us: Create a Heart Safe Community Month."
Geriatric Emergency Medical ServicesAdvisory Committee
As part of an ongoing effort to maintain high-quality emergency medical care, MIEMSS hasidentified a need for geriatric-specific EMS educa-tional programs, evaluation of geriatric emergencyassessment guidelines and treatment protocols,and other relevant geriatric emergency manage-

16
ment issues. In order to incorporate a geriatric-specific component into the Maryland EMSSystem, MIEMSS has established the GeriatricEmergency Medical Services AdvisoryCommittee (GEMSAC), consisting of memberswith clinical knowledge and expertise in geriatricpatient care. The committee’s primary responsi-bilities include the evaluation of current geriatricassessment guidelines, recommendations for geri-atric-specific protocol changes, and advisement onEMS geriatric educational curricula in the future.
The committee meets on a quarterly basisand includes representation from physicians andnurses specializing in geriatrics and emergencymedicine, EMS providers with geriatric clinicalexpertise and knowledge, and the MarylandDepartment of Aging.
Do Not Resuscitate ProgramMIEMSS continues studying various aspects of
the EMS/Do Not Resuscitate (DNR) program. Aspart of a working group that was convened by theAttorney General as a result of Chapter 152 (HouseBill 770) of the Laws of Maryland 2000, the groupdevised a comprehensively revised EMS/DNR andmedical care order form. Use of the new, simplerform will become effective July 1, 2003. This newform will be easier for patients and their caregiversto read and use. The new form will be available onthe MIEMSS web site and also available in printedform from MIEMSS. An updated educational pro-gram is also being developed.
Maryland Cardiac Arrest PublicDefibrillation Study
The Maryland Cardiac Arrest PublicDefibrillation Study (M-CAPD) was begun inJanuary 2001 by the Office of Epidemiology. Thisstudy has two main objectives: (1) to determinethe impact of the Facility AED Program; and (2)to identify whether there is a need for the State torequire that AEDs be placed in certain publiclocations. This study is ongoing.
Additional information about the study can befound on the M-CAPD website http://www.miemss.org/m-capd.htm.
Maryland Cardiac Arrest SurveillanceSystem (M-CASS)
MIEMSS Office of Epidemiology establishedthe Maryland Cardiac Arrest Surveillance System(M-CASS) in January 2001.The surveillance sys-tem has two main objectives: (1) to identify the
epidemiology of out-of-hospital sudden cardiacarrest in Maryland; and (2) to evaluate the effec-tiveness of the Maryland EMS System in respond-ing to cardiac arrests. The surveillance system cap-tures all out-of-hospital sudden cardiac arrests thatcontact the 9-1-1 emergency medical system inMaryland. The Utstein Style templates (Adult andPediatric) are applied to the data to evaluate theMaryland System (see algorithm on this page).State annual reports for statewide data are avail-able upon request.
Weapons of Mass DestructionThe overall strategic approach by MIEMSS to
Weapons of Mass Destruction (WMD) planningand preparedness has continued: by working toenhance and improve general disaster prepared-ness and response, an "all hazards" approach, thestate will be better prepared for both a WMD inci-dent and more routine disasters. In addition, plan-ning and preparedness activities are based ineveryday processes and routines to help ensurethat those systems needed to respond to WMDwill be better able to perform their tasks and func-tions should such an incident occur. Preparednessactivities also continued inclusive of the major
POPULATION SERVED BY EMS SYSTEMN = 5,296,486
CONFIRMED CARDIAC ARRESTS CONSIDERED FOR RESUSCITATION
N = 3,189 (60.2 PER 100,00 POPULATION) Exclude Children
< 21 years of age andefforts terminated in
the fieldN = 370 (11.6%)
Non-Cardiac EtiologyN =503 (17.8%)
Note: Incidentswhere the Pt. isconsidered deadon arrival and noresuscitativeefforts areattempted orpatients that havevalid EMS DoNot ResuscitateOrders are notcaptured in thisnumber.
RESUSCITATIONS ATTEMPTEDN = 2,819(88.4%)
CARDIAC / UNKNOWN ETIOLOGYN =2,316 (82.2%)
ARREST WITNESSED(Bystanders n = 886; EMS n =220)
N =1,106 (47.8%)
Arrests Not WitnessedN =1,210 (52.2%)
INITIALRHYTHM VFN =186 (16.8%)
INITIALRHYTHM VTN = 9 (0.8%)
INITIAL RHYTHMAED SHOCKABLE
N =129 (11.7%)
Initial RhythmAsystole
N = 203 (18.4%)
Other InitialRhythm
N = 579 (52.4%)
RETURN OF SPONTANEOUSCIRCULATION (ROSC) AT ED
ARRIVALN = 78(24.1%)
No Return ofSpontaneous Circulation(ROSC) at ED Arrival
N = 888(80.3%)
Return of SpontaneousCirculation (ROSC) at
ED ArrivalN = 140(17.9%)
Maryland Out-of-Hospital Cardiac Arrests for Adults 21 years and older,Utstein Style Template (M-CASS 2001)
Notes: (1) Percentages are calculated by the latest figure derived at each level of the algorithm rather thanthe total number of confirmed cardiac arrests. (2) Children less then 21 years of age were excluded early inthe algorithm because of the different underlying etiology of sudden cardiac arrests in the pediatric popula-tion. The pediatric Utstein Style Template is applied to this population.

17
agent categories: chemical, biological, radiological,and explosives/incendiaries.
MIEMSS’ WMD preparedness activities focuson three complementary strategic directions: plan-ning, coordination, and operational preparedness.
In planning, refinements to the "MarylandHealth and Medical WMD Response Plan" contin-ued to be developed, with a major revision to bereleased in the fall of 2003. The Plan covers thehealth and medical response spectrum, identifiesbest practices and responses, and enables coordi-nation among the various public and private com-ponents of the health care system. Highlightsinclude decontamination practices, personal pro-tective equipment, incident management systems,and communications capabilities. The "2003Maryland Hospital Disaster Preparedness Survey"was completed with the assistance of the MIEMSSRegional Offices with a 100% response rate. TheSurvey was first done in the fall of 2001, allows acomparison of hospital preparedness between2001 and 2003, and incorporates additions tocoordinate between Maryland, Virginia, and theDistrict of Columbia.
In coordination, MIEMSS continued as anactive participant in the Maryland TerrorismForum, the Terrorism Forum ExecutiveCommittee, and the Terrorism Forum SteeringCommittee under the leadership of the MarylandEmergency Management Agency. In addition topolicy issues, these groups determine funding pri-orities and distribution formulas for federal fundsbased on assessments of preparedness and needs.MIEMSS continued active participation inNational Capital Region preparedness activities inbioterrorism, completed Strategic NationalStockpile planning for hospitals, and worked withsmallpox and Severe Acute Respiratory Syndrome(SARS) preparations.
In operational preparedness, activities includecontinuity of operations and response planning forMIEMSS through the establishment of an internalemergency operations group, continuing improve-ments to the Facility Resource EmergencyDatabase (FRED), and implementing EMAIS(Electronic Maryland Ambulance InformationSystem) enhancements. Technical assistance con-tinues to be provided to individual Maryland hos-pitals to improve disaster preparedness. Finally,MIEMSS prepares and distributes advisories tohospitals and EMS through FRED andEMRC/SYSCOM when threat conditions change.
PUBLIC INFORMATION ANDMEDIA SERVICES
Mission: To contribute to MIEMSS’ vision of elimi-nating preventable death and disability by providingto the public essential information on how to recog-nize an emergency, summon an EMS response, andincorporate injury prevention methods in their dailylives, as well as designing and developing education-al programs for EMS providers through state-of-the-art technology.
The Public Information and Media ServicesDepartment provides education and informationto Maryland’s Emergency Medical Servicesproviders and the general public through trainingmodules and informative programs. The depart-ment develops, designs, and produces programsthat are distributed statewide.
The department is responsible for the designand editorial content of the MIEMSS AnnualReport, MIEMSS web page, and the MarylandEMS News. The newsletter is sent to 32,000 hospi-tal and prehospital EMS personnel six times ayear. This keeps emergency medical services per-sonnel in touch with local, state, and nationalEMS issues. Recent topics include updates oninfectious diseases and geriatric medical issues.These documents are also available on theMIEMSS web page. The annual EMS Week andStars of Life Awards Ceremony were organizedand planned. Press releases were distributedstatewide and media coverage obtained on theaward winners.
The department provides technical and audio-visual support to MIEMSS-sponsored continuingeducation programs. These regional and statewideconferences allow providers to update their certifi-cation and licensure by attending programs.Design and production of printed, photographic,computer-assisted programs, and video materialsassist the learning process.
Several training modules were produced dur-ing the past year. These included "The PrehospitalProtocol Update," "Hospital Base Station,""Facility Resource Emergency Database (FRED)Training," and the update to the MoulageProgram. These modules were produced on com-pact disc and include printed materials. Thedepartment provided satellite down-linking andtaping of many informational programs on infec-tion control and WMD/Bioterrorism issues. Videoprojects included the documentation of variousdisaster drill videos and several Public Service

18
Announcements (PSAs), including the PoisonCenter and Maryland’s new Booster Seat law. Amajor video project on the dangers of impaireddriving for high-school aged drivers was producedwith the R Adams Cowley Shock Trauma Center.Working with the Maryland State Firemen’sAssociation and the Governor’s Office, the staffproduced a PSA for volunteer recruitment;Governor Ehrlich delivered the message of theneed for emergency personnel and the benefits ofvolunteering in Maryland’s emergency services.
Statewide prevention initiatives were devel-oped through partnerships with other state andlocal government agencies. Participation on theOccupant Protection Task Force, the MotorcycleSafety Task Force, the Pedestrian Safety TaskForce, and the Impaired Drivers Coalition allowedthese coalition teams to work collaboratively onmultiple projects. Membership on the StateHighway’s Diversity in Traffic Safety Programraised the need for diversity in our public educa-tion efforts. Print and broadcast projects were pro-duced in both Spanish and English. Projects werecompleted with representation of Maryland’sgrowing diverse population.
QUALITY MANAGEMENTMission: To support MIEMSS and the EMS com-munity in their continuous quality improvement ini-tiatives and commitment to a customer-based way ofdoing business. Successfully accomplishing this is notsimply dependent upon recognizing that the ultimatecustomer is a patient in need of timely, proficient,and compassionate care, but understanding andimproving the processes that maintain a well func-tioning EMS system for the delivery of quality med-ical care.
MIEMSS initiated its quality managementimplementation through the development of aJuran-based program. Over the years MIEMSShas taken advantage of state supported resources,particularly those offered through the ContinuousQuality Improvement and Managing for Resultsprograms, in its efforts to improve upon its ser-vices and customer interactions.
Managing for Results (MFR)Each state agency is required to submit a
Managing for Results plan, along with its FY 2004budget requests, to the Maryland Department ofBudget and Management. This phased-in planningprocess was initiated in 1997 with the submissionof MIEMSS Vision, Mission, and Principles state-ment through a customer-focus strategic planningprocess. MIEMSS has again met all requirementsfor state agencies; these include re-evaluation ofkey goals, subsequent objectives and strategies,development of associated action plans, and theestablishment and monitoring of performanceindicators.
MIEMSS has identified two strategic goalsand seven associated objectives. Three objectivesare outcome oriented, while the remaining fourare quality-based indicators. Each objective includ-ed performance indicators, which will help bothsystem and jurisdictional quality management ini-tiatives in establishing benchmarks for future quali-ty control and quality improvement efforts.
Goal 1. Provide high quality medical care to indi-viduals receiving emergency medical services.
Objective 1.1 Maryland will maintain its trau-ma patient care performance above the nationalnorm at a 95% or higher statistical level of confi-dence.
Performance Measures/Performance Indicators2002 2003 2004 2005
Actual Actual Estimated Estimated_______________________________________________________________________________________________________________
Outcome:
1.1 Maintaining >95% statistical level of confidence yes yes yes yes
1.2 Statewide trauma center complication rate 11.9 12.3 11.0 10.0
1.3 % jurisdictions achieving % resuscitation rate 52 65 70 75
Quality:
2.1 % jurisdictions with uniform EMD indicator * * 100 100
2.2 % jurisdictions with ≥90% protocol compliance * * 100 100
2.2 % EMS radio communications successfully 98 98 98 98completed
2.4 % seriously injured patients transported 86 86 87 88_______________________________________________________________________________________________________________
* New measures for which data are not available.

19
Objective 1.2 By 2005, maintain an overallinpatient complication rate of 10% or less forMaryland trauma centers.
Objective 1.3 Achieve 20% witnessed suddenV Fib / V Tach cardiac arrest resuscitation uponemergency department arrival in 80% of jurisdic-tions by 2003.
Goal 2. Maintain a well-functioning emergencymedical services system.
Objective 2.1 By 2003, all jurisdictions willuse a uniform set of quality indicators for priori-tized EMD services.
Objective 2.2 Before 2003, x% of jurisdictionswill achieve or exceed 90% compliance with pre-hospital provider standards of care per the"Maryland Medical Protocols."
Objective 2.3 Maintain an EMS responseincident location to hospital base station communi-cation at a successful completion rate of 95% orbetter.
Objective 2.4 Maintain at least an 85% ratefor transporting seriously injured patients to a des-ignated trauma center in Maryland.
Team EMSAn innovative approach to Quality
Management education and application in the realworld of EMS management was developed in con-junction with the MIEMSS Region V administra-tion. Implemented in 1996 and updated to presentstandards, MIEMSS staff and a cadre of volunteerpresenters from the EMS community offer waysfor company and jurisdictional managers to planfor, measure, maintain, and improve quality ser-vices. Techniques taught range from brainstormingto data analysis interpretation and include topicsfrom quality improvement team creation to meet-ing quality assurance standards established understate law. Regional councils have utilized this train-ing for planning purposes and over 50 providershave attended workshops at Pyramid and EMSCare during the year. Emphasis this year was onthe implementation and continued support of indi-vidual jurisdictional Quality Assurance/QualityImprovement plans.
EMS Surveillance MeasuresYellow Alert Demand: To assist hospitals
statewide in planning and preparation for acuteincreases in emergency department servicesdemand, MIEMSS maintains two tracking provi-sions on its web page. The first is concurrent infor-mation on all hospitals’ alert status. This includesavailability of cardiac monitor beds (red alert),emergency department beds (yellow alert), andtrauma beds at designated centers (trauma by-pass). Second, weekly updates to regional graphsare available. These graphs provide a daily per-cent of yellow alert demand. Trends are monitoredbefore voluntary actions are taken on a regionalbasis.
Data ConfidentialityMIEMSS maintains or has access to eight
confidential databases used in ensuring qualityEMS care delivery. The Data Access Committee(DAC) was formed to ensure that all data andinformation requests were expedited efficientlyand accurately, while ensuring patient andprovider confidentiality at all times. Since January2000, over 1000 requests have been tracked andfacilitated.
REGIONAL PROGRAMSMission: To provide a liaison between theMIEMSS Central Office and the local EMSagencies, manage MIEMSS programs at thelocal level, work closely with the local govern-mental entities, training centers, emergencymedical services/fire providers, and staff theRegional EMS Advisory Councils.
Region IThis past fiscal year the Region I Office
worked on numerous grant proposals and theimplementation of various projects. Working withthe EMS Council’s Transportation Committee, theRegion I Office applied for four Highway SafetyGrants. They were approved, with the award total-ing $40,000. The monies were used for auto extri-cation, medical response equipment, paramedictraining equipment, and scene safety equipment. Itshould be noted that previous Highway SafetyGrant funding was used in purchasing the extrica-tion equipment utilized in a multi-vehicle crash onMemorial Day 2003 that involved 85 vehicles.EMS and fire providers reported that the equip-

20
ment purchased with these grants was critical intheir successful response to this disaster.
Other grant projects included the Rural AEDGrant. This program placed 11 automated externaldefibrillators (AEDs) with fire, EMS, police, andcommunity centers with the goal of improvedaccess to defibrillation during cardiac arrest in therural areas. The Region I Office also continued towork on the Rural Access Grant, which will pro-vide computers for all EMS services in Alleganyand Garrett counties.
The Region I Office was instrumental in thepassage of the new Seal of Excellence VoluntaryAmbulance Inspection Program Standards for thestate. Activities involved formulation of the Seal ofExcellence Committee’s recommendations andpresentations to the EMS Committee of theMaryland State Firemen’s Association, theStatewide EMS Advisory Council (SEMSAC), andthe EMS Executive Board. In Region I, the newSeal of Excellence standards were used for theinspection of Garrett County ambulance servicesduring EMS Week.
Quality Assurance/Quality Improvement pro-jects were a major emphasis for the RegionalOffice. The Region I Administrator staffed theMIEMSS Jurisdictional Quality ImprovementCommittee and the Region I QualityImprovement Committee. At the state level, effortswere centered on the first QualityAssurance/Quality Improvement Officers Summit.This was held during EMS Care and attracted 17of the 22 jurisdictions in the state. At the Region Ilevel, work continued on the endotrachial intuba-tion study and response time studies for ambu-lance services. The response time study inAllegany County has resulted in a special taskforce organized by the Allegany County Fire andRescue Board.
Training activities in Region I were highlight-ed with the first Miltenberger Emergency ServicesSeminar. This day-long program presented onMay 31 was highly successful and offered trainingfor fire, EMS, and nursing personnel. It is antici-pated in FY 2004 that a Miltenberger lectureseries, as well as a second seminar, will be con-ducted. Other training activities in Region I were aDisaster Planning Seminar conducted by RickMeighen and a Moulage Workshop sponsored bythe MIEMSS EMS for Children Program. Therewas also training on utilization of the CountyHospital Alert Tracking System (CHATS) andFacility Resource Emergency Database (FRED)programs by John Donohue.
The Region I Office worked to resolve inter-state response issues with West Virginia. As aresult of the intervention, leaders from Marylandand West Virginia were able to resolve the possi-ble duplication of Tri-Towns Ambulance Servicehaving to meet multiple training operational stan-dards.
The Region I Office continued to work onpreparations for weapons of mass destruction(WMD) response. The office participates withAllegany and Garrett counties’ WMD Committeesand assisted in the completion of hospital disasterresponse surveys.
A new ambulance service was added inRegion I during this reporting period. District 16initiated service in July of 2002. Also during thisperiod, the McCoole ambulance service steppedback to an ALS Engine designation.
Region IIThe Region II Office continues to be very
active in the region’s Quality Assurance andQuality Improvement programs and participatesin all of the Jurisdictional Medical ReviewCommittee meetings. Significant progress has beenmade in the development of quality review at thestation level. A Regional Medical ReviewCommittee has been established within theRegional EMS Council to discuss issues or initia-tives that could affect or benefit the entire region.
The Region II Office coordinated and partici-pated in the inspection of 84 EMS response vehi-cles, including both ALS and BLS ambulances,EMS, engines and special units, and ALS "chasecars." Both jurisdictions in Region II have adoptedthe MIEMSS/Maryland State Firemen’sAssociation’s Voluntary Ambulance InspectionProgram as the standard for their annual inspec-tion of vehicles providing EMS services.
This office remains active in participating withthe local jurisdictions in the planning and conduct-ing of mass casualty drills and events. Support wasprovided to the Hagerstown Community Collegefor a multi-discipline drill involving their EMT-Paramedic students, their nursing students, andtheir Administration of Justice students. A mockemergency department overseen by Dr. SteveKotch, the Washington County JurisdictionalMedical Director, utilized the nursing students toevaluate/treat the "patients" who received prehos-pital care from the EMT-P students. The justicestudents investigated the "crime scene," which wasa simulated weapons of mass destruction explo-sion.
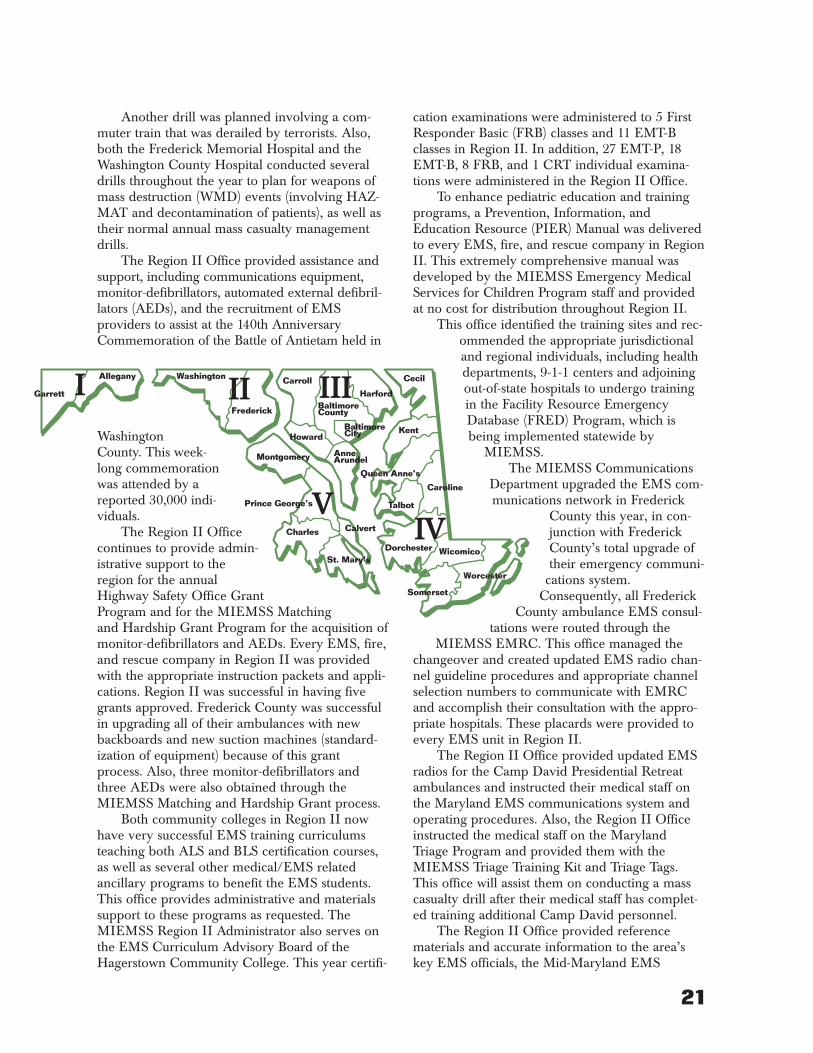
21
Another drill was planned involving a com-muter train that was derailed by terrorists. Also,both the Frederick Memorial Hospital and theWashington County Hospital conducted severaldrills throughout the year to plan for weapons ofmass destruction (WMD) events (involving HAZ-MAT and decontamination of patients), as well astheir normal annual mass casualty managementdrills.
The Region II Office provided assistance andsupport, including communications equipment,monitor-defibrillators, automated external defibril-lators (AEDs), and the recruitment of EMSproviders to assist at the 140th AnniversaryCommemoration of the Battle of Antietam held in
WashingtonCounty. This week-long commemorationwas attended by areported 30,000 indi-viduals.
The Region II Officecontinues to provide admin-istrative support to theregion for the annualHighway Safety Office GrantProgram and for the MIEMSS Matchingand Hardship Grant Program for the acquisition ofmonitor-defibrillators and AEDs. Every EMS, fire,and rescue company in Region II was providedwith the appropriate instruction packets and appli-cations. Region II was successful in having fivegrants approved. Frederick County was successfulin upgrading all of their ambulances with newbackboards and new suction machines (standard-ization of equipment) because of this grantprocess. Also, three monitor-defibrillators andthree AEDs were also obtained through theMIEMSS Matching and Hardship Grant process.
Both community colleges in Region II nowhave very successful EMS training curriculumsteaching both ALS and BLS certification courses,as well as several other medical/EMS relatedancillary programs to benefit the EMS students.This office provides administrative and materialssupport to these programs as requested. TheMIEMSS Region II Administrator also serves onthe EMS Curriculum Advisory Board of theHagerstown Community College. This year certifi-
cation examinations were administered to 5 FirstResponder Basic (FRB) classes and 11 EMT-Bclasses in Region II. In addition, 27 EMT-P, 18EMT-B, 8 FRB, and 1 CRT individual examina-tions were administered in the Region II Office.
To enhance pediatric education and trainingprograms, a Prevention, Information, andEducation Resource (PIER) Manual was deliveredto every EMS, fire, and rescue company in RegionII. This extremely comprehensive manual wasdeveloped by the MIEMSS Emergency MedicalServices for Children Program staff and providedat no cost for distribution throughout Region II.
This office identified the training sites and rec-ommended the appropriate jurisdictionaland regional individuals, including healthdepartments, 9-1-1 centers and adjoiningout-of-state hospitals to undergo trainingin the Facility Resource EmergencyDatabase (FRED) Program, which isbeing implemented statewide by
MIEMSS.The MIEMSS Communications
Department upgraded the EMS com-munications network in Frederick
County this year, in con-junction with FrederickCounty’s total upgrade oftheir emergency communi-
cations system.Consequently, all Frederick
County ambulance EMS consul-tations were routed through the
MIEMSS EMRC. This office managed thechangeover and created updated EMS radio chan-nel guideline procedures and appropriate channelselection numbers to communicate with EMRCand accomplish their consultation with the appro-priate hospitals. These placards were provided toevery EMS unit in Region II.
The Region II Office provided updated EMSradios for the Camp David Presidential Retreatambulances and instructed their medical staff onthe Maryland EMS communications system andoperating procedures. Also, the Region II Officeinstructed the medical staff on the MarylandTriage Program and provided them with theMIEMSS Triage Training Kit and Triage Tags.This office will assist them on conducting a masscasualty drill after their medical staff has complet-ed training additional Camp David personnel.
The Region II Office provided referencematerials and accurate information to the area’skey EMS officials, the Mid-Maryland EMS
Garrett II III
IVV
I Allegany Washington
Frederick
Montgomery
CarrollHarford
BaltimoreCounty
BaltimoreCity
Cecil
KentHoward
AnneArundel
Queen Anne’s
Caroline
Talbot
Calvert
Prince George’s
Charles
DorchesterSt. Mary’s
Wicomico
Worcester
Somerset

22
Advisory Council (MMEMSAC), and to the emer-gency services community pertaining to the con-struction of two controversial emergency commu-nications towers that the state proposed to be con-structed in Washington County. The Region IIOffice also coordinated several meetings held inthe region between state communications person-nel and regional/jurisdictional EMS officials andcounty government officials. As a result of thesemeetings, the Region II EMS Advisory Council(MMEMSAC) was able to develop a positionpaper that was sent to the Governor and officialson his staff and to appropriate legislators in theGeneral Assembly.
The Region II Office arranged for free train-ing for the staff of three Maryland WelcomeCenters in its region on proper use of the AED.These staff members received appropriate certifi-cation through the American Heart Association.Each of these Welcome Centers was provided withan AED through the grant program sponsored andprocessed through MIEMSS.
This office worked with our Region II EMSjurisdictions to qualify appropriate areas and com-munities in this region to receive AEDs at no costunder the Rural Access to Emergency Devices(RAED) Federal Grant Program being managedvia MIEMSS.
The Region II Office disseminated urgentSevere Acute Respiratory Syndrome (SARS) infor-mation and advisories to its health departments,hospitals, 9-1-1 centers, and jurisdictional EMSofficials as it was received from MIEMSS head-quarters. Critical advisories, such as the "GroundEmergency Transport Instructions andPrecautions" that were developed by MIEMSS,were issued to every EMS, fire, and rescue compa-ny in Region II, as well as to the health depart-ments, hospitals, and 9-1-1 centers.
Region IIIThe Region III Office continued its efforts to
ensure the region is prepared for large-scale inci-dents. This year the staff concentrated on enhanc-ing multiple jurisdiction response. A region-wideexercise named REFLEX (Regional Fall Exercise),originally scheduled for the fall but rescheduleddue to sniper activity in the area, was conducted inJune. Three scenarios were conducted, one each inHarford, Howard, and Carroll counties. Two otherscenarios were also scheduled to be conducted inconjunction with the regional effort, but theBaltimore-Washington International Airport’sEmergency Plan Exercise (EPLEX) proceeded asscheduled in October, and the Baltimore CountyMass Transit subway exercise was rescheduled forMay due to regulatory requirements and con-straints from other partners. The Region III Officesupported all five scenarios. Each scenariorevealed that more effort is required on utilizationof incident management systems, communicationand resource notification, and triage systems oper-ation. Region III staff also assisted in an exercisehosted by the University of Maryland MedicalSystem with the US Air Force and the MarylandStadium Authority.
Partially in response to the urging of theRegion III Emergency Medical Advisory Council,the Fire Chiefs in the Baltimore area, in conjunc-tion with the Baltimore Metropolitan Council,have begun meeting to address some of the issuesthat were brought to light in planning for theREFLEX exercise. An Incident ManagementCommittee was established to standardize emer-gency operations plans with the national standardsas the model and to automate notification andresponse of support resources. The Region IIIOffice is a member of that committee. The workdone by the fire departments is being tied into thework of other disciplines through the BaltimoreMetropolitan Council through their BaltimoreRegional Operations Committee and theirTransportation Emergency PreparednessCommittee. Region III staff are also involved withboth those committees.
The Baltimore City Health Departmentrequested assistance with conducting a multipleday exercise responding to the release of a biologi-cal agent. Region III staff served on the executivecommittee and several subcommittees for theplanning of the exercise. A tabletop exercise wasconducted in March to prepare hospitals for theexercise. The actual exercise was planned for

23
April but was postponed to July because of thestart of the Iraqi War.
Dr. Bass appointed an Emergency OperationsGroup to coordinate many of the activities associ-ated with emergency operations. John Donohue,Region III Administrator, was assigned to coordi-nate that group. The Emergency Operations Planwas updated, as were plans for "building evacua-tion" and "shelter in place." Additional communi-cation resources were acquired and assigned tokey individuals. The group is now acting as aclearinghouse for all emergency response andplanning activities to ensure coordination betweenall individuals involved in various aspects of thoseefforts.
The Facility Resource Emergency Database(FRED) became operational in October 2002.Participation in FRED at the beginning of 2003was minimal, but as training exercises occurred,more participants registered. FRED is an internet-based communication system to alert all compo-nents of the State’s EMS system and catalogresources available for response to a large-scaleincident. Several requests for the use of FRED byorganizations outside of Maryland have beenreceived. A memorandum of understanding wassigned by MIEMSS and the PennsylvaniaDepartment of Health to establish a back-up serverfor FRED in Harrisburg. They are also assisting incontracting with the software development compa-ny to reprogram FRED to include several com-ments on operation received to date. Theseenhancements will include regional alerting capa-bilities, text paging of key individuals, more flexi-bility of databases, and more organized informa-tion pages. Revisions are due in September 2003.
Additional funding was received through theEMS for Children Program to enhance efforts toestablish a patient triage and tracking program.This computer program was used to track patientsduring a rock concert in Prince George’s Countyin the past. These funds were planned to help net-work computers to improve operations and torevise the program. A request for support at anoth-er concert at Fed-EX Field is pending for earlynext fiscal year.
The Region III Office’s commitment to educa-tion continues. The many educational institutionsand academies in the region were beginning toexperience a decrease in attendance in many ofthe upper level EMS courses and a duplication ofefforts in responding to the educational needs of
the EMS system. Representatives from these pro-grams gathered to revitalize the EmergencyEducation Council of Region III. Here they hopeto standardize skills verification processes, estab-lish a regional training calendar, and share trainingresources. This cooperation will also play a leadrole in planning for and coordinating EMS Careand other educational conferences. Battalion ChiefMichael Robinson is the President of theEmergency Education Council of Region III,which now meets quarterly.
Title 30 requires that each EMS operationalprogram establish a Quality Assurance Plan and aMedical Review Committee. The Regional EMSAdvisory Council also hosted a TEAM EMS con-ference in which they identified their priorities ofissues to be investigated in a quality improvementformat. To organize all of these efforts, the Councilidentified a Quality Improvement ManagersCommittee, which consists of all the qualityimprovement managers from the EMSOperational Programs. Their two priorities are toinvestigate patterns of refusals of care and unrec-ognized esophageal intubations. They are meetingmonthly and are supported by the Region IIIOffice. Dr. Christina Johns is the Chairperson.
A program to improve the readiness of thosein the Maryland Welcome Centers was completedthis year. Money received from the Department ofTransportation’s Highway Safety Office was usedto place automated external defibrillators (AEDs)at all the Welcome Centers around the state.Twelve centers, including highway rest stops andinformation booths, had no means to respond tovictims of heart attacks who stopped there forassistance. Now all the welcome centers haveAEDs, and each shift supervisor is trained in AEDuse and CPR. The Welcome Centers are now allregistered public access defibrillation facilities.
Testing and ambulance inspections also con-tinued throughout the year with the Region IIIOffice conducting 110 written exams and 150 vehi-cle inspections.
Region IVThe Region IV Office coordinated with the
region’s nine counties in the development of emer-gency medical services quality assurance and qual-ity improvement programs. The medical directors,jurisdictional representatives, and EMS organiza-tions have been actively supporting this initiativeto include intubation audits, continuous positive

24
airway pressure, and cardiac arrests and interven-tion. Dr. Deborah Davis, Regional MedicalDirector, hosted two jurisdictional medical direc-tors meetings. This forum assists in the distributionof information between regional programs.
Wor-Wic Community College formallyreceived provisional advanced life support (ALS)training center designation by MIEMSS after anon-site visitation was completed on December 16,2002. The first Emergency Medical TechnicianParamedic course application was submitted andapproved by MIEMSS, with course completionbeing scheduled in 2003. The college is currentlyoffering two ALS program choices—an Associate ofApplied Sciences and a Certificate of Proficiency.Both programs follow the national certificationand state protocol standards, which allow gradu-ates to take the national and State of Marylandcertification examinations.
The Region IV Office has actively partneredwith the MIEMSS Communications Departmentby coordinating regional hospital visitations rele-vant to the expansion of the state’s infrastructureproject currently being developed and the RuralQuality Assurance Project. Cecil, Dorchester, andSomerset counties are all participating in this pro-ject.
The Region IV EMS Advisory Council priori-tized and received funding for MarylandDepartment of Transportation Highway SafetyGrants. In addition, matching grants fromMIEMSS assisted with the placement of moni-tor/defibrillators and automated external defibril-lators (AEDs) in EMS departments throughout theregion. Seven counties within the region were eli-gible for funding and participated in the RuralAccess AED program which placed additionalAEDs in the region.
The Education Committee of the Region IVEMS Advisory Council prioritized and coordinat-ed the distribution of training funds for initialtraining of ALS providers, as well as recertificationtraining for ALS and BLS providers.
The Region IV Office worked closely with theregion’s health departments, hospitals, and officesof emergency management in the education andtraining of designated managers relevant to theimplementation of the Facility ResourceEmergency Database (FRED) project.
Chester River Hospital Center (formerlyknown as the Kent and Queen Anne’s Hospital) atChestertown opened a new emergency depart-
ment. This has allowed the hospital to expand itsservices to the community.
The MIEMSS Region IV administratorsinspected 29 prehospital emergency response vehi-cles, including advanced and basic life supportambulance, chase cars, and first responder units.
The Region IV Office staff assisted in plan-ning and staffing two regional conferences. TheWinterfest 2003 EMS Seminar was held January25-26, 2003, at Tilghman Island, and thePeninsula Regional Medical Center TraumaConference was held at the Ocean CityConvention Center on September 20, 2002.
Region VPyramid 2002, the thirteenth annual Tri-
County EMS Conference, was conducted in con-junction with the Emergency Education Council ofRegion V, Inc. Held at the Holiday Inn andConference Center, Solomon’s, Maryland, theOctober conference had 230 registrants. Amongthe skill workshops were EMS incident command,mass casualty tabletop exercises, and an interac-tive program on the changes to sensory and physi-cal capabilities that come with aging. Plenary ses-sions were presented on the LaPlata Tornado, inci-dent command for EMS, managing violentpatients, and domestic violence. Pediatric offeringsincluded case reviews and management of asthma.
In April 2003, 250 attended EMS CARE atthe Greenbelt Marriott Hotel. The theme was"EMS for Every Season of Life" and focused onissues in both pediatric and geriatric emergencycare. "Understanding Aging," "Altered MentalStatus in the Elderly," "Geriatric Trauma" and"Legal Issues" all focused on the special needs ofelderly patients. The new Geriatric EmergencyMedical Services (GEMS) program was presentedfor the first time as a pre-conference program.
Following the events of September 11, 2001,Region V staff continue to be heavily involved indisaster preparation across the state. The office hasprovided assistance on mass casualty exerciseplanning and implementation through both pre-sentations and guidance. Data collected from theexercises are used to improve the drills themselvesand, more importantly, actual mass casualtyresponse. Working in conjunction with theEmergency Education Council of Region V, Inc.and the Emergency Medical Services for Children(EMSC) Program, Region V staff have continuedto train and support the Moulage Technician

25
Program. The Region V Associate RegionalAdministrator has also been active in the develop-ment and implementation of the Maryland VirtualEmergency Resource System, working with theOffice of the Medical Director, the MarylandEMS for Children Program, the Maryland StatePolice, the Maryland Emergency ManagementAgency, and the Maryland Department ofEducation. The Region V Office worked closelywith the Health Departments of Montgomery andPrince George’s counties in coordinating weaponsof mass destruction and bioterrorism planning forhospitals and health care facilities.
Region V continues to support a variety ofeducation and prevention activities through theRegion V EMS Advisory Council, county fire andrescue associations, the Prince George’s CountySafe Kids Coalition, and the EMSC RISKWATCH initiative. Charles County parochialschools, public schools in Prince George’s andMontgomery counties (including special needsschools in Prince George’s County), will partici-pate in the National Fire Protection AssociationRisk Watch Programs as part of the StateChampion Grant.
Shock Trauma mini-grants distributed by theRegion V EMS Advisory Council provided pedi-atric training equipment for use in SouthernMaryland, as well as an Officers QualityImprovement Seminar in Montgomery County.
The Region V EMS Advisory Council hasstrongly supported the development of QualityCouncils in each county and supported qualitymanagement education and implementation. Eachcounty has an operational Quality Assurance/Quality Improvement Plan, and the EMSAdvisory Council seeks input from these groups indeveloping new initiatives. For example, thisyear’s emphasis on geriatric issues in EMS Caregrew out of this process.
STATE OFFICE OF COMMERCIALAMBULANCE LICENSING AND REGULATION
Mission: To provide leadership and direction regard-ing the commercial (private) ambulance industry inMaryland to protect the health, safety, and welfareof persons utilizing these services. This includes thedevelopment and modification of statewide require-ments for commercial ambulance services and vehi-cles and the uniform and equitable regulation of thecommercial ambulance industry throughoutMaryland.
Operating statistics:144 BLS vehicles licensed112 ALS vehicles licensed8 neonatal vehicles licensed33 ground ambulance services licensed3 air ambulance services licensed13 temporary upgrades authorized18 complaints received and investigated127 routine compliance inspections performed
Number of commercial ambulance transports:Total ground ambulance transports: 217,100
BLS 189,007ALS 27,256Neonatal 837
Total commercial air transports: 2,810
The State Office of Commercial AmbulanceLicensing and Regulation (SOCALR) faced signifi-cant challenges in FY 2003, its 10th year of opera-tion. While the number of transports performed inthe state increased 4% (from 210,837 in FY 2002to 219,910 in FY 2003), the number of ambulancesincreased less than 1%. Therefore, the licensingrevenue upon which SOCALR depends remainedessentially flat.
Furthermore, SOCALR itself underwent a sig-nificant leadership change. Cheryl Bowen, RN,retired from the Director’s position after ably guid-ing SOCALR through the critical industry contrac-tion between FY 1999 and FY 2001. Her influencecontinued to be felt, however, as her two staffmembers organized and carried on SOCALR’smission in exemplary form. Despite the dual chal-lenges of reduced staffing and budgetary con-straints, the SOCALR team performed more than50% the number of previous years’ compliancechecks. Of these, 31% (n=39) resulted in notices ofnon-compliance and 9% (n=12) resulted in vehiclelicense suspensions. Importantly, SOCALR’s coreservices continued unabated as evidenced by theoperating statistics presented above.
The fiscal year concluded with a newDirector, John Young, RN, joining the team. Nowfully staffed at three FTEs and with the keyinvolvement of several part-time inspectors,SOCALR is poised to focus on a tripartite para-digm of leadership, education, and regulation.Challenges to be met in the coming year includeimproving the effectiveness of core licensing oper-ations, implementing air ambulance and specialtycare transport regulations, and integrating com-mercial services into disaster planning.

Injured patients need treatment at the hospitalbest staffed and equipped to meet their specialneeds. Maryland's system of care ensures thatpatients promptly get to the most appropriate hos-pital in an effort to decrease morbidity and mortali-ty. (For differences in standards in the levels of trau-ma centers, see the Trauma Center Categorizationchart on the next page.)
The trauma and specialty referral centers withinthe Maryland EMS System are:
TRAUMA CENTERSPrimary Adult Resource Center
R Adams Cowley Shock Trauma Center/University of Maryland Medical System, Baltimore City
Level I Trauma CenterThe Johns Hopkins Hospital Adult Trauma
Center, Baltimore City
Level II Trauma CentersThe Johns Hopkins Bayview Medical Center,
Baltimore CityPrince George's Hospital Center, CheverlySinai Hospital of Baltimore, Baltimore CitySuburban Hospital, Bethesda
Level III Trauma CentersWashington County Hospital, HagerstownWestern Maryland Health System,
Memorial Hospital, CumberlandPeninsula Regional Medical Center, Salisbury
SPECIALTY REFERRAL CENTERSBurns
Baltimore Regional Burn Center/The Johns Hopkins Bayview Medical Center, Baltimore City
Burn Center/Washington Hospital Center, Washington, DC
Eye TraumaWilmer Eye Institute’s Emergency Service/The
Johns Hopkins Hospital, Baltimore City
Eye Trauma Center, Suburban Hospital, Bethesda
Hand/Upper Extremity TraumaThe Curtis National Hand Center /UnionMemorial Hospital, Baltimore City
Hyperbaric MedicineHyperbaric Medicine Center/R Adams Cowley
Shock Trauma Center/University of Maryland Medical System, Baltimore City
Neurotrauma (Head and Spinal Cord Injuries)Neurotrauma Center/R Adams Cowley Shock
Trauma Center/University of Maryland Medical System, Baltimore City
Pediatric TraumaPediatric Trauma Center/The Johns Hopkins
Children’s Center, Baltimore CityPediatric Trauma Center/Children's National
Medical Center, Washington, DCPerinatal Referral Centers
Anne Arundel Medical CenterFranklin Square Hospital CenterGreater Baltimore Medical CenterHoly Cross HospitalHoward County General HospitalJohns Hopkins Bayview Medical CenterJohns Hopkins HospitalMercy Medical CenterPrince George’s Hospital CenterSt. Agnes Health CareSt. Joseph Medical CenterShady Grove Adventist HospitalSinai Hospital of BaltimoreUniversity of Maryland Medical System
Poison Consultation CenterMaryland Poison Center/University of
Maryland School of Pharmacy, Baltimore City
MARYLAND TRAUMA & SPECIALTY REFERRAL CENTERS
26

27
Primary Adult Resource CenterR Adams Cowley Shock Trauma CenterUniversity of Maryland Medical System
Located in Baltimore City, the R Adams CowleyShock Trauma Center, which serves as the state’sPrimary Adult Resource Center (PARC), reportedreceiving 6,025 trauma patients from June 2002 toMay 2003, according to the Maryland TraumaRegistry. (See pages 43 to 48 for patient data invarious categories.) Thomas M. Scalea, MD, FACS,FCCM, serves as the Physician-in-Chief for theProgram in Trauma, and Robbi Hartsock, RN,MSN, CRNP, as the Trauma Nurse Coordinator.
Shock Trauma Center staff were very active inprehospital EMS educational activities. Tours weregiven to 50 groups. Case reviews open to prehos-pital care providers were held quarterly. One hun-dred and ten EMS providers participated in ALSSkills Labs that were offered 10 times. In theObservation Program, 208 EMS providersobserved in the Trauma Resuscitation Unit, and 82EMS providers in Critical Care. In addition, 97on-site clinical programs were held at firehouses,training academies, and EMS conferences.The Research Program at the Shock TraumaCenter is an integrated multi-disciplinary programthat seeks to answer important questions concern-
ing issues that affect trauma patients. The RAdams Cowley Shock Trauma Center researchersparticipate in large national and internationalmulti-institutional projects, and are conductingprojects funded by the National Institutes ofHealth. A Research Education Program continuesfor residents and fellows who rotate through ShockTrauma.
In the area of clinical research, the R AdamsCowley Shock Trauma Center:
• Actively investigated the use of intravenousfluid and ideal target blood pressure during theevaluation of seriously injured patients
• Collaborated with diagnostic and interven-tional radiology to define optimal strategy for non-operative management of solid visceral injuries
• Actively investigated optimal resuscitationstrategy and alternative therapies in geriatricpatients
• Collaborated with orthopedic surgeons tofind optimal timing for fracture fixation thatinvolves multiple injuries
• Conducted ongoing investigations of meth-ods for providing organ support in patients whoseorgans had failed
• Used airway pressure release ventilation inpatients with respiratory failure
• Collaborated with neurosurgeons to developa noninvasive monitor to assess head injuries intrauma patients
Trauma Center Categorization
Differences in Standards Based on Physician Availability and Dedicated Resources PARC Level I Level II Level IIIAttending surgeon who is fellowship-trained and is in the hospital at all times X
Dedicated facilities (Resuscitation Unit, Operating Room, and Intensive Care Unit) 24 hours X
Facilities (Resuscitation Unit, Operating Room, and Intensive Care Unit) available at all times X X X X
Trauma Surgeon available in the hospital at all times X X
On-call Trauma Surgeon available within 30 minutes of call X
Anesthesiologist in the hospital at all times and dedicated to trauma care X
Anesthesiologist in the hospital at all times but shared with other services X X
On-call Anesthesiologist with CRNA who is in the hospital X
Orthopedic Surgeon in the hospital at all times and dedicated to trauma care X
Orthopedic Surgeon in the hospital at all times but shared with other services X
On-call Orthopedic Surgeon available within 30 minutes of call X X
Neurosurgeon in the hospital at all times and dedicated to trauma care X
Neurosurgeon in the hospital at all times but shared with other services X
On-call Neurosurgeon available within 30 minutes of call X X
Fellowship-trained/board-certified surgical director of the Intensive Care Unit X X
Physician with privileges in critical care on duty in the Intensive Care Unit 24 hrs/day X X X
Comprehensive Trauma Research Program X X
Education—Fellowship Training in Trauma X
Surgical Residency Program X X
Outreach Professional Education X X X

28
• Investigated the etiology of and the idealtherapy for soft tissue infectionIn addition, Shock Trauma serves as a test-bed fornew technology. Most recently, a new full-body x-ray technology Statscan is being evaluated. It iscurrently the only Statscan in the U.S.
The Shock Trauma Center provides the lead-ership for the American Trauma Society,Maryland Division through its president, RobbiHartsock, RN. Active in all regions in Maryland,the American Trauma Society has sponsored andparticipated in 100 safety fairs, fire department andhospital open houses, conferences, and conven-tions and has distributed safety literature to thou-sands of Maryland’s adults and children over thelast year.
The Shock Trauma Center ViolenceIntervention Program (VIP) is designed to identifyprofiles of patients who are repeat victims of vio-lence in an effort to intervene and disrupt thecycle of violence. The program includes a multi-disciplinary approach that combines parole andprobation, surgeons, social workers, psychiatrists,nurses, epidemiologists, and physicians who plancare for these patients.
The Shock Trauma Center also hosted in the"Mentoring Male Teens in the Hood" program.Forty males, ages 8-18 years old, visited ShockTrauma to interact with role models from theSTC/VIP staff, tour the facility, and participate insmall group sessions to reinforce the importance ofstaying away from a life of crime. The purpose ofthis program is to teach young boys to be honest,respectful, and to model positive behavior.
The Shock Trauma Center took part in aProgressive Life Program geared for youths whoare court-ordered by the juvenile justice system toparticipate in the program to help them reframetheir behavior.
As part of the community outreach initiative,Shock Trauma also held a "Minds of the Future"program four times this year with 600 high-schoolstudents participating.
The High Risk Adolescent Trauma PreventionProgram (HRATPP) is an educational programdesigned to provide information on the conse-quences of drinking, taking drugs, and driving sothat the participants can make informed decisionsabout these high-risk behaviors. During FY 2003,500 high-risk adolescents attended 62 on-siteHRATPP programs. In addition, 7 groups fromStudents Against Destructive Decisions (SADD)brought participants from the metropolitan andEastern Shore high schools to attend HRATPPprograms at the Shock Trauma Center.
HRATPP staff participated in 36 classes andcountywide school-related summits. HRATPP con-ducted related tour programs and taught 42 classesin the community for 1,000 extremely high-riskadolescents. The HRATPP provided educationaldisplays at various community sites, includingschools, community fairs, and conferences reach-ing thousands of people. The Trauma Preventionstaff participated in 20 school-wide assemblies andhealth classes reaching thousands of students.They also participated in the Candlelight Vigil for3-D Month (National Drinking, Driving, DruggedCampaign) and developed a 3-D event held at theUniversity of Maryland Baltimore CampusStudent Union, reaching more than 500 people. Inaddition, they are involved in many of the activi-ties of Baltimore County SADD groups in the ele-mentary, middle, and high schools.
In conjunction with Anne Arundel andHarford county courts and the Office of Paroleand Probation, the HRATPP staff conducted 11on-site educational programs for over 400 adultoffenders who have driven while intoxicated dur-ing this fiscal year.
Positive Alternatives to Dangerous andDestructive Decisions (PADDD) is a not-for-profitcorporation founded by STC nurses Debbie Yohnand Laurel Stiff in 1997. The company servesMaryland by providing adult education for court-ordered clients who were involved in drunk dri-ving, speeding, distracted driving, and/or red lightrunning. An ongoing relationship with the RAdams Cowley Shock Trauma Center providesaccess to speakers, slides, and new content for thepresentations.
During FY 2002, PADDD provided six class-es in Harford County and expanded into HowardCounty. In FY 2003 PADDD provided nine edu-cational programs to more than 400 participants

29
and 80 guests. PADDD also gathers research infor-mation for the National Study Center and workswith MIEMSS on videos for trauma prevention.PADDD has been awarded a grant by theMaryland Highway Safety Office of the StateHighway Administration for FY 2004.
Level IThe Johns Hopkins Hospital, AdultTrauma Center
Located in Baltimore City, the Johns HopkinsHospital Adult Trauma Center reported receiving2,101 trauma patients from June 2002 to May2003, according to the Maryland Trauma Registry.(See pages 43 to 48 for patient data in various cat-egories.) Edward Cornwell, MD, serves as theDirector of the Johns Hopkins Adult Trauma Centerand Judy Phillips, RN, BS, as its Trauma NurseCoordinator.
The Johns Hopkins Adult Trauma Center,housed in the "#1 Hospital in America" accordingto the U.S. News & World Report, receives morethan 2000 adult trauma patients per year. In 1998the Adult Trauma Center implemented a 24-houra day in-house trauma attending surgeon commit-ment and has quickly demonstrated improved sur-vival, triage time, and length of stay among criti-cally injured patients (Archives of Surgery, 2003).
The Johns Hopkins Hospital’s Division ofAdult Trauma has a strong commitment to traumaprevention, particularly in the area of youth vio-lence. During the past fiscal year, the AdultTrauma Center continued its involvement in sever-al important trauma prevention endeavors. TheHopkins Injury Prevention and CommunityOutreach Collaborative (HIPCOC), which wasestablished by Dr. Edward Cornwell, the directorof the Adult Trauma Center, in 2000, is a multi-disciplinary group of clinicians, hospital, and com-munity affairs professionals, public health profes-sionals, and members of the community who areinterested in pursuing violence prevention througheducational and outreach activities. During thispast fiscal year, HIPCOC continued to conductseveral ongoing prevention programs, including:the dissemination of videos aimed at adolescentsdepicting the true consequences of gun violence;hospital tours to visit the survivors of interpersonalviolence; and slide presentations by health careprofessionals graphically demonstrating theanatomic damage that results from interpersonalviolence. In addition, as part of the HIPCOC ini-tiative and with a grant from the American
Trauma Society, the Division of Adult Traumacompleted a "readiness to change" study forinjured patients ages 15 to 24 who have positivetoxicology screens for drugs or alcohol. The resultsof this study will be presented as a poster at theannual meeting of the American Association forthe Surgery of Trauma (AAST) in September 2003.
As part of his many trauma prevention activi-ties, Dr. Cornwell continued his membership onthe Board of Directors of the Police AthleticLeague (PAL), the American Trauma Society, andthe New Song Community Learning Center in theSandtown neighborhood of West Baltimore. Dr.Cornwell also continued to serve as the sponsor ofthe Fort Worthington PAL center.
In the area of clinical research, the Division ofAdult Trauma:
• Studied the impact of an enhanced traumaprogram commitment on the process and outcomeof care. The results of this study were published inthe Archives of Surgery (2003).
– Retrospectively studied the significance ofearly leukocytosis in trauma patients. The resultsof this study were accepted for publication byCurrent Surgery (2003).
– Studied the demographics and communitycharacteristics of the trauma patients as determi-nants for an injury prevention outreach program.The results of this study were presented as a posterat annual meeting of the Pacific Coast SurgicalAssociation, February 2002, and were accepted forpublication in the Archives of Surgery (2003).
During the past fiscal year, the Division ofAdult Trauma continued to be actively involvedwithin the trauma community at both the state andnational levels. Dr. Cornwell assumed the positionof president of TraumaNet in November 2002.Judy Phillips, the trauma nurse coordinator,became the secretary of TraumaNet. Both Dr.Cornwell and Ms. Phillips were active participantsin TraumaNet’s legislative initiatives.
The Division of Adult Trauma continued toprovide educational and community outreachactivities within and outside of the hospital setting.During the past year, Dr. Cornwell participated innumerous grand rounds presentations throughoutthe state. He also presented educational offeringsto diverse groups, including area school children,college students, EMS personnel, trauma clini-cians, church congregations, and rotary clubs.Within the hospital, the Adult Trauma EducationCommittee continued to present quarterly traumacontinuing education seminars for nurses, techni-cians, ancillary staff, and EMS personnel.

30
Level IIJohns Hopkins Bayview Medical CenterTrauma Center
Located in Baltimore City, the Trauma Center atthe Johns Hopkins Bayview Medical Center reportedreceiving 1,144 trauma patients from June 2002 toMay 2003, according to the Maryland TraumaRegistry. (See pages 43 to 48 for patient data invarious categories.) Paul Freeswick, MD, FACS,serves as the center’s Trauma Director, Myra JoBeach, RN, MBA, as its Director of SurgicalNursing, and Robert Dice, RN, MS, as its TraumaCoordinator.
Paul Freeswick, MD, FACS continues as theDirector of Trauma. Dr. Freeswick has been anattending trauma surgeon at Bayview for fouryears. He previously was on staff in the traumadivision at the University of Pittsburgh MedicalCenter—Presbyterian in Pittsburgh, Pennsylvania.
During FY 2003, the adult trauma service atthe Johns Hopkins Bayview Medical Center( JHBMC) treated 1,144 patients, with a survivalrate of 98 percent.
In addition, the adult trauma service atJHBMC strives to minimize the use of traumabypass, remaining open for all critically or serious-ly injured trauma patients. It is experiencing rapidinternal growth in the areas of surgery, orthope-dics, and geriatric medicine.
An institutional member of the AmericanTrauma Society, the JHBMC trauma service sup-ports the functions of the local Maryland Division.
This past December, the trauma center heldits first Emergency Medical Services Reception,serving as host to members of the EMS communi-ty that serve Bayview as well as to representativesof agencies such as the Maryland State PoliceAviation Section, the Office of the State FireMarshal, and the Maryland Institute forEmergency Medical Services Systems. The recep-tion is planned as an annual event. In addition,"Trauma/EMS/Burn Grand Rounds" seminars arebeing planned to begin in Fall 2003.
The Trauma Center, the Baltimore RegionalBurn Center at JHBMC, and the EmergencyDepartment/Department of Emergency Medicinecontinue to support the local EMS jurisdictions bydistributing the pocket version of the MarylandEMS Protocols. Several EMS providers havevoiced their appreciation about this program—nowin its fourth year.
In preparation for the periodic trauma designa-tion survey, the leadership team revised and expand-ed the trauma center’s trauma team and patientreception protocols to enhance delivery of care totrauma and burn patients received by JHBMC.
Level IIPrince George’s Hospital Center
Located in Cheverly, the Trauma Center at PrinceGeorge’s Hospital Center reported receiving 2,356trauma patients from June 2002 to May 2003,according to the Maryland Trauma Registry. (Seepages 43 to 48 for patient data in various cate-gories.) Philip R. Militello, MD, served as theTrauma Director during this time. Sandra WaakRN, CEN, served as the Assistant Nurse Managerfor the Trauma Service and has also been filling infor the Trauma Services Manager position, vacatedin November.
The Prince George’s Hospital Center (PGHC)continues to serve as the primary adult traumacenter for the counties of Prince George’s, Calvert,Charles, St. Mary’s, southern Anne Arundel, aswell as parts of Montgomery and Howard countiesand the eastern part of Washington, DC.Approximately 30 percent of last year’s traumapatients arrived via helicopter. Three flight agen-cies routinely use the rooftop helipad: theMaryland State Police, United States Park Police,and MedStar.
Because of its unique proximity toWashington, DC, PGHC is also a designated trau-ma center for the White House Medical Team, aswell as Operation Capitol. Renovations to theground-level helipad have been made in order toaccommodate the larger helicopters from the mili-tary, should the need arise.
Prince George’s Hospital Center continuestheir affiliation with the R Adams Cowley ShockTrauma Center in Baltimore and regularly rotatesa team of senior trauma fellows through PGHC aspart of their fellowship training. This serves toenhance their clinical experiences and providesPGHC with additional resources for its growingtrauma program. One of the trauma fellows pre-pared a presentation on "The Non-OperativeManagement of Penetrating Torso Trauma" for aCanadian Medical Conference.
PGHC continues to host its award-winningtrauma prevention experience— the Shock MentorProgram—which provides a unique educational

31
experience to students within the Prince George’sCounty high schools in cooperation with theConcerned Black Men Organization. The TraumaCenter also actively participates in hosting the"Reality" program with the Prince George’sCounty Juvenile Justice System. In addition,PGHC has provided interventions for troubledteenagers for the past two years on the JudgeHatchett television program.
Nursing leadership in the Trauma Center hastransitioned from Connie Stone, Director ofEmergency/Trauma Services and Mike Walls,Trauma Services Manager, to Jackie Anderson,Director Emergency/Trauma Services and SandraWaak as Acting Department Manager, TraumaServices. In addition, the Trauma Services Officestaffing has increased to include a Trauma RegistryAssociate and an Assistant Nurse Manager position.
Level IISinai Hospital Trauma Center
Located in Baltimore City, Sinai Hospital TraumaCenter reported receiving 1,060 trauma patientsfrom June 2002 to May 2003, according to theMaryland Trauma Registry. (See pages 43 to 48 forpatient data in various categories.) Adrian Barbul,MD, FACS serves as the Trauma Director, andJocelyn Farrar, RN, MS, CCRN, ACNP, as theTrauma Coordinator.
The Trauma Division’s ongoing commitmentto injury prevention was demonstrated by activeinvolvement in community outreach and traumaprevention endeavors. Continued efforts to reducegeriatric injury resulted in the presentation ofongoing fall and injury prevention activities. Inconjunction with the Lifebridge CommunityHealth Education Department, the TraumaDivision presented the American Trauma Society’sTraumaroo injury prevention programs to childrenat local elementary schools and health fairs. Sinai’sFamily Violence Program continued its efforts tobreak the cycle of violence by providing counsel-ing, resources, referrals, and training of health careproviders.
Performance Improvement activities enhancedthe care provided to the trauma patient. Focusedmulti-disciplinary performance improvement ini-tiatives resulted in the reduction in complicationrates, enhancement of triage and transfer process-es, and development of improved trauma docu-mentation records.
Emergency medicine and trauma staff wereactively engaged in EMS educational activities.Continuing education courses and case reviewswere offered to the EMS community. In addition,preceptorship of paramedics was provided inSinai’s ER7.
During FY 2003, the Trauma Division contin-ued to be actively involved at the state level. Ms.Farrar and Dr. Barbul continued the leadership ofthe TraumaNet Research Committee. This multi-disciplinary committee is exploring outcomes ofgeriatric trauma patients cared for at trauma cen-ters versus those cared for in community hospitalsettings. Ms. Farrar assumed the role of theChairperson of the MIEMSS QualityImprovement Committee for Trauma. In addition,Dr. Barbul continues his research in nutrition andwound healing.
Level IISuburban Hospital
Located in Bethesda, the Suburban Hospital TraumaCenter received 1,370 trauma patients from June2002 to May 2003, according to the MarylandTrauma Registry. (See pages 43 to 48 for patientdata in various categories.) Daniel Powers, MD,FACS, serves as the Medical Director of SuburbanHospital’s Trauma Services and Anne Kuzas, RN, asits Trauma Nurse Coordinator/Program Manager.
During FY 2003, Suburban Hospital treatedan increasing number of trauma patients. Initiallythis increase was related to the temporary closureof the Washington County Hospital TraumaService; however, an increase in the number oftrauma service patients has continued even afterWashington County’s trauma program wasreopened. Suburban Hospital welcomed a traumacenter survey team in June to review the traumaprogram.
Last fiscal year Suburban Hospital implement-ed a Picture Archiving and CommunicationSystem (PACS) to bring its physician community"radiology at e-speed." The goal of the cost-effec-tive technology was to speed diagnoses, reducetime to treatment, and improve patient care. In FY2003, PACS was expanded to include additionaldepartments within the hospital, as well as remoteaccess for authorized users. Suburban’s traumastaff is adept at utilizing the system and is pleasedwith its ability to view patient images with suchease and speed in multiple locations throughout

32
the hospital. Ongoing enhancements are beingapplied to this system as further technologicaladvances continue to be made.
The trauma center’s bypass hours have contin-ued to remain within the thresholds that were setwhen the trauma bypass policy was developed andimplemented. Each event continues to be evaluat-ed on a daily basis for policy compliance as wellas the identification of additional opportunities forimprovement. The ability to maintain ongoingimprovement enables Suburban’s Trauma Centerto be more available to serve the trauma careneeds of citizens within its immediate communityand serve as a backup trauma center as neededwithin the statewide trauma system.
The Medical Director of Trauma Services andthe Trauma Nurse Coordinator/Program Managercontinue to actively participate in the MarylandEMS System through memberships in theTraumaNet, the MIEMSS Quality ImprovementCommittee for Trauma, the Region V EMSAdvisory Council, the Statewide EMS AdvisoryCouncil, and the Maryland Division of theAmerican Trauma Society. Suburban is an institu-tional member of the American Trauma Society.Its staff have also participated in local public ser-vice partnerships at media events to educate thepublic in the surrounding community about"pedestrian safety" and "drinking, drug, and dri-ving" awareness.
Two four-hour seminars, "Update on CriticalIssues in Trauma," were held in the fall and spring.These seminars were offered free of charge to thetrauma care community within the regional area,including medical and hospital staff and the EMScommunity. Emergency department nurses provid-ed an injury prevention program, ENCARE(Emergency Nurses Cancel Alcohol-RelatedEmergencies), as well as alcohol poisoning lecturesin community high schools.
Level IIIPeninsula Regional Medical CenterTrauma Center
Located in Salisbury, the Peninsula RegionalMedical Center (PRMC) Trauma Center reportedreceiving 846 trauma patients from June 2002 toMay 2003, according to the Maryland TraumaRegistry. (See pages 43 to 48 for patient data invarious categories.) Un Y. Chin, MD, serves as theTrauma Director, and Lisa Hohl, RN, BSN,CCRN, as the Trauma Nurse Coordinator.Under the direction of Dr. Un Y. Chin,
Peninsula Regional Medical Center successfully
applied for re-designation as a Level III traumacenter. The application was submitted in January2003, and a site visit completed in May 2003;results of the re-designation survey are pending.
Peninsula Regional Medical Center continuesto coordinate and participate in community-basedinjury prevention initiatives. Peninsula RegionalMedical Center was awarded a child passengersafety inspection site grant from the Society forHealthcare Strategy and Market Development.With this grant, Peninsula will sponsor five childpassenger safety check-point events throughout theLower Shore. A child passenger safety seat give-away program has been implemented for anyonereceiving services at the medical center who mayneed a safety seat for transporting a child homesafely. Additional injury prevention efforts contin-ue with the Maryland Division of the AmericanTrauma Society, the Lower Shore Safe KidsCoalition, the Worcester County Injury PreventionCommittees, and the Ocean City Pedestrian TaskForce.
Peninsula Regional Medical Center continuedto assist in planning, coordinating, and sponsoringseveral educational conferences:• It coordinated and sponsored the 13th annual"Topics in Trauma" conference, with topics rang-ing from prehospital care to advanced inpatienttrauma care. The EMS track continues to grow,with participation from local as well as regionalEMS providers. • It collaboratively worked with the Brain InjuryAssociation of Maryland and HealthsouthChesapeake Rehabilitation Center to plan andimplement a seminar "Living with Brain Injury:Challenges and Creative Solutions." This one-daycourse was geared to professionals who work withsurvivors of brain injury to increase awareness ofbrain injury and its aftermath and to identifyappropriate brain injury treatments, services, andsupport systems.
Peninsula Regional Medical Center hasimproved radiographic capability with the pur-chase of a GE Light Speed CT scanner. The scan-ner is a 16-slicer, making the timeframe for com-pleting scans 4 times faster than the other onsitescanner. The new scanner is capable of scanningan unenhanced CT of the brain in 30 seconds andan abdominal CT in 3 minutes. This capabilityimproves the throughput and quality for diagnos-ing injuries in the trauma patient.
Peninsula Regional continues to work collabo-ratively with Wor-Wic Community College in pro-viding continuing education for prehospital

33
providers, as well as curriculum management andcoordination of the EMT-B to the EMT-P pro-grams. • Survival Spanish Class for Paramedics and EMTswas held for EMS providers so they would be ableto communicate better with the vastly growingHispanic population. • Wor-Wic continues to coordinate the didacticportion of the EMT-P program, while Peninsulacontinues to be one of the sites for the clinical por-tion of the program. Peninsula’s EMS NurseLiaison functions as the clinical instructor andsupervisor. This gives the EMT the opportunity topractice needed skills in an acute care setting.• Numerous skills classes are offered for area EMSproviders by paramedic instructors. This instructorgroup consists of 12 local NREMT-Ps who cur-rently serve as career paramedics in different EMScompanies/Maryland State Police AviationDivision throughout the Lower Shore.
Level IIIWashington County Health SystemsTrauma Center
Located in Hagerstown, the Washington CountyHealth Systems Trauma Center reported receiving486 trauma patients from October 2002 throughMay 2003, according to the Maryland TraumaRegistry. (See pages 43 to 48 for patient data invarious categories.) Karl P. Riggle, MD, FACS isthe Director of Trauma Services, Marc E. Kross,MD, PhD, FACS is Surgeon-in-Chief of TraumaServices, and Joan Fortney, RN, BSN is theManager of Trauma Services.
Washington County Hospital closed itsTrauma Service on June 1, 2002. After lengthynegotiations, the Trauma Service was opened onOctober 2, 2002 as a Level III Center. As in thepast, the Trauma Center has provided trauma ser-vices to residents of Washington and Frederickcounties, Southern Pennsylvania, and the EasternPanhandle of West Virginia.
Throughout the year, the Trauma Center staffhave been active in community education events.They have participated in community health fairs,served as speakers about safety issues, and partici-pated in the Stop Red Light Running initiative.Trauma Center representatives have also beenworking with community members to plan thesecond Citizen’s Emergency Preparedness Dayand a Bike Safety Rodeo for later in the year.
The trauma staff continue to provide trauma-related education to physicians and other staffmembers on a regular basis. Extensive planning isunderway for the annual Trauma Seminar, in coor-dination with Hagerstown Community College forOctober 2003. Trauma Center representativeshave also presented case studies to area EMSproviders.
To celebrate the outstanding contributions anddedication of the trauma center staff throughoutthe hospital, the Trauma Service organized TraumaTeam Recognition Day. Members of the traumateam were invited to a reception. Displays abouttrauma services and water safety were set up in thehospital lobby. Employees and staff learned aboutthe multi-disciplinary approach to providing trau-ma services.
In May 2003, the Trauma Center underwentLevel III re-designation by the Maryland Institutefor Emergency Medical Services Systems. Whilethe official report is pending, the Trauma Centerlooks forward to continuing to provide traumacare to residents of the tri-state area.
Level IIIWestern Maryland Health System—Memorial Trauma Center
Located in Cumberland, the Western MarylandHealth System—Memorial Trauma Center reportedreceiving 515 patients from June 2002 until May2003, according to the Maryland Trauma Registry.(See pages 43 to 48 for patient data in various cat-egories.) Juan Arrisueno, MD, serves as the TraumaDirector, and Melissa Meyers, RN, was the TraumaNurse Coordinator during the FY 2003 annualreport period.
Emergency medical services in WesternMaryland were in the national spotlight onMemorial Day weekend when 85 cars crashed infog and rain on Interstate-68 at Big SavageMountain in Garrett County. Local EMS person-nel transported nearly 70 patients to the twoCumberland hospitals for treatment within a two-hour period. The Western Maryland HealthSystem (WMHS)—Memorial Trauma Centerreceived 22 Priority 1 patients, and the less seri-ously injured patients were taken to Sacred HeartHospital for treatment. Thanks to years of emer-gency preparedness drills and a tremendousresponse from WMHS staff and physicians,

34
patients were assessed and treated quickly and effi-ciently.
Vehicle crashes account for the major sourceof trauma in Western Maryland, and the WMHS—Memorial Trauma Center continues to focus ontraffic safety and other injury prevention programsin the community. WMHS works cooperativelywith the Allegany County Health Department,local law enforcement agencies, and other organi-zations to promote child passenger safety issuesand to host child safety seat checks in the commu-nity. Radio ads promoting traffic safety are usedaround national holidays as a reminder for thosewho are traveling.
Physicians, nurses, EMS personnel, and otherhealthcare providers take advantage of thetelemedicine link between the WMHS—MemorialTrauma Center and the University of MarylandShock Trauma Center to hone their skills by par-ticipating in Shock Trauma’s Grand Rounds.Nearly 100 Cumberland healthcare professionalsattended a case study involving an organ donationpatient from WMHS whose organs were placed intwo individuals with positive outcomes.Trauma patients also benefit from the technologi-cal enhancements made through this year’s acqui-sition of a spiral CT scanner, which is faster, pro-vides arterial studies, and has 3-D capabilities.
Baltimore Regional Burn CenterJohns Hopkins Bayview Medical Center
The Baltimore Regional Burn Center manages morethan 300 patients a year. For every inpatient, thereare approximately 4 patients seen as outpatientsthroughout the state. The outpatient burn clinicaverages about 1300 visits a year. Cleon Goodwin,MD, FACS was the Medical Director.
During FY 2003, the Baltimore Region BurnCenter (BRBC) treated 341 inpatients. Follow-upwas in the outpatient burn clinic. This resulted inmore than 1300 outpatient visits. As the trendtoward greater outpatient management continues,these statistics will probably change. Patients wereadmitted from all 22 counties in Maryland, as wellas the surrounding states of Virginia, WestVirginia, Delaware, and Washington, DC. Thisyear the BRBC had an outpatient from Bermuda,which was arranged through the Office ofInternational Relations. (See charts on pages 34-35for other statistics.)
This has been en exciting year for the BRBC.The effects of community education and preven-tion are now being seen, and the Center has been
able to "right size" into a very busy 10-bed, com-bined intensive care and step-down unit. It stillmaintains its assignment of 5 beds in the pediatricsunit for children with burns.
The Center has also managed to add anotheroutpatient clinic session to aid with the increasingdemands for outpatient care. The BRBC continuesto use home care services, which are providedthrough the Hopkins Home Health Care Group asneeded.
The BRBC has incorporated a wound careteam to provide continuity for the essential dailydressings needed in burn care management.
The BRBC maintains its commitment to bothprofessional and community education. The BurnFoundation concentrates its many efforts in pre-vention education in the school systems. TheCenter commits many hours to lecturing andspeaking to the professional community as well.The Center maintains its practice of providingeducational opportunities for nurses, physicians,medical students, nurse practitioners, physicianassistants, burn technicians, and paramedic stu-dents. It is a well respected clinical site for EMT-Iand EMT-P students. During FY 2003, more than170 paramedic students were at the BRBC for clin-ical rotations. The Metropolitan Fire Fighters Fundcontinues its special relationship with the BRBC.
The Burn Center at the WashingtonHospital Center
The Burn Center at the Washington HospitalCenter is located in the District of Columbia andserves as the adult regional burn center for theDistrict, southern Maryland, and northern Virginia.Marion Jordan, MD, is the Director.The Burn Center features a 7-bed intensive
care unit with a dedicated operating room andrecovery room, a 13-bed intermediate/rehab careunit, and the Skin Bank for Burn Injuries. Between275 and 300 adult burn patients are admitted eachyear.
ADMISSIONS TO BALTIMORE REGIONAL BURNCENTER BY MODE OF TRANSPORT (FY 2003)
_______________________________________________________________________Arrival Mode Patients Percentage_______________________________________________________________________
EMS ground 177 51.9%
EMS aeromedical 43 12.6%
Commercial, ground 59 17.3%
Commercial, aeromedical 9 2.6%
POV/walk-in 48 14.1%
Other 5 1.5%_______________________________________________________________________
Total 341 100%

35
Reconstructive surgery and rehabilitation areavailable for patients in the post-acute and conva-lescent phases, regardless of where they receivedtreatment for their acute burns.
Patients with minor burns that do not requirehospitalization are provided with outpatientwound care and rehabilitation through the BurnCenter Clinic.
The Curtis National Hand CenterAt Union Memorial Hospital
The Curtis National Hand Center at UnionMemorial Hospital serves as the state’s referral cen-ter for specialized care of injuries to the hand, wrist,and elbow, including significant elbow trauma andinjuries requiring microsurgical reconstruction.Thomas J. Graham, MD, is the Director.
The Curtis National Hand Center is known asone of the country’s most advanced resources forthe care of patients with elbow, forearm, wrist, andhand trauma. Having received the congressionaldesignation as The National Hand Center in 1994,the Center remains one of the world’s premierfacilities for the study of hand surgery and thetraining of orthopaedic, plastic, and general sur-geons in the field of upper extremity surgery.Thomas J. Graham, MD is the Director of the
Curtis National Hand Center and the Chief of theUnion Memorial Hospital Division of HandSurgery, as well as the Vice-Chairman ofOrthopaedics at Union Memorial, and is anAssociate Professor of both Orthopaedic andPlastic Surgery at Johns Hopkins University.
The Curtis National Hand Center remainscommitted to handling acute injuries and provid-ing reconstructive surgery after trauma. The focuson complex hand, wrist, and elbow injuries haslong been part of the well-developed Marylandtrauma care system, since the Center’s founder,Dr. Raymond M. Curtis, collaborated with Dr. RAdams Cowley and others during the inception ofShock Trauma and the Maryland EMS System.
The Center’s expertise in complex bone andsoft tissue trauma is supplemented by advancedmicrosurgery skills. The handling of fractures,challenging soft tissue coverage problems, andamputations continues to be the major focus of theHand Surgery Service at Union Memorial.
The Curtis National Hand Center is one of thelargest training centers for hand surgery. TheCenter’s relationships with Johns HopkinsHospital, Georgetown University, Walter ReedArmy Medical Center, and Union MemorialHospital continue to provide extraordinary train-ing because of the volume and variety of thepathology. The surgeons of the National HandCenter have contributed some of the most impor-tant publications concerning the care of theinjured hand and upper extremity, and continue tolecture worldwide about the topic of hand trauma.
Continuing research projects, funded by bothinternal and external sources, look at a wide rangeof pertinent questions, including those in micro-surgery, surgery of the peripheral nerve, bone, softtissue problems, and reconstruction after signifi-cant trauma. Collaborations with the region’s sci-entists and other investigators promote currentthinking and new development in this vital area.
Among other upcoming projects is the physi-cal reorganization of the trauma intake facility tointroduce even better processes for the injuredpatient. The value of the association of The CurtisNational Hand Center and MIEMSS is clear andstrong. Maryland maintains the nation’s premiernetwork of institutions and physicians for traumacare in part because of the unique capabilities andavailability of the specialty trauma centers. One ofthe country’s most important resources in the careof hand and upper extremity trauma is also one ofthe critical components in Maryland’s strong net-work of advanced trauma centers.
ADMISSIONS TO BALTIMORE REGIONAL BURNCENTER BY INJURY TYPE (FY 2003)
_______________________________________________________________________Injury Type Patients Percentage_______________________________________________________________________
Flame 158 46.3%
Scald 98 28.7%
Electrical 14 4.1%
Contact w/hot surface 4 1.2%
Chemical 15 4.4%
Skin disease/TENS 22 6.5%
Frostbite 1 0.3%
Inhalation (smoke/chemicals) 9 2.6%
Late effects 18 5.3%
Other/unknown 2 0.6% _______________________________________________________________________
Total 341 100.00%
BALTIMORE REGIONAL BURN CENTERSTATISTICAL SUMMARY (FY 2003)
__________________________________________________________
Admissions 341
• Adults 290 (85%)
• Children 51 (15%)
Average Age 39.35 years
Average Total Burn Surface Area 13.67%
Average Length of Stay 11.34 days
Mortality 28 (8.2%)__________________________________________________________

36
Hyperbaric Medicine CenterR Adams Cowley Shock Trauma Center
The Hyperbaric Medicine Center of the R AdamsCowley Shock Trauma Center of the University ofMaryland Medical Systems is the statewide referralcenter for victims of diving accidents, carbon monox-ide poisoning, smoke inhalation, and gas gangrene.It is the only multi-place chamber in Maryland, andis capable of accommodating 10 stretcher patients or23 seated patients simultaneously. The center is ableto provide treatment around the clock, 365 days ayear. Robert Rosenthal, MD, is the Director of theHyperbaric Medicine Center.
During FY 2003, the types of emergent casestreated included: carbon monoxidepoisoning/smoke inhalation; arterial gasembolism; decompression sickness (the bends),clostridial myonecrosis; group A beta hemolyticstrep fasciitis/myositis; necrotizing fasciitis; com-promised skin grafts and flaps; crush injuries; andexceptional blood loss anemia.
The types of non-emergent cases treatedincluded: non-healing diabetic extremity wounds;refractory osteomyelitis; osteoradionecrosis; andradiation cystitis/enteritis.
All treatments are supervised by speciallytrained hyperbaric physicians; direct patient con-tact is administered by critical care nurse "tenders"who provide patient care in the chamber duringall "dives." Because of the chamber’s uniquedesign and staffing, even the most critically illpatients can receive hyperbaric treatments withoutany interruption of care.
Physician and nursing members of theHyperbaric Medicine Center actively lecture onhyperbaric medical education at regional andnational levels and to local and regional EMSproviders.
Researchers from the Department ofHyperbaric Medicine, in collaboration with theDepartment of Anesthesiology, are actively contin-uing pre-clinical investigations exploring the neu-roprotective effects of hyperbaric oxygen followingcardiac arrest and brain injury. Additionally,departmental researchers, in collaboration with theDivision of Plastic Surgery, are exploring the abili-ty of hyperbaric oxygen to promote the "accep-tance" of tissue flaps following surgery or trauma.
Maryland Eye Trauma SystemThe Wilmer Eye Institute at JohnsHopkins
The Eye Trauma Center at the Wilmer EyeInstitute, Johns Hopkins Hospital is the firststatewide eye trauma center in the nation. The mainobjectives of the eye trauma center are to provideoptimal clinical management of severe ocularinjuries, to conduct research into the natural historyof eye trauma, to develop new treatments for oculartrauma, and to initiate and support eye trauma pre-vention activities. Joseph B. Harlan, MD, is theDirector of the Center; the Associate Director for FY2004 is Albert S. Jun, MD, PhD. Amy Liu, RN,BSN, is Nurse Manager (Acting) of the WilmerEmergency Room/Wilmer Eye Care Pavilion.
During FY 2003, Dr. Peter J. McDonnell suc-ceeded Dr. Morton F. Goldberg as the sixthFunctional Unit Director of the Wilmer EyeInstitute and Chairman of the Department ofOphthalmology, Johns Hopkins Medicine. Bothserved as Assistant Chief of Service/Director ofOcular Trauma (Goldberg, 1967; McDonnell,1987). Dr. McDonnell also spent his internship inEmergency Medicine at Johns Hopkins Hospitaland has authored several publications on cornealwound healing.
The Wilmer Emergency Room (WER) logged5,832 patient visits in FY 2003. Serious eyeinjuries are reported to the US Eye Injury Registry(USEIR). (See tables and graphic for the USEIRdata analysis of Maryland serious eye injuries,from 1999-2002.)
In 2001, Baltimore City passed the first legisla-tion in the country mandating protective gear,which includes face guards on batting helmets andsoft-core baseballs to reduce facial fractures (inparticular, fractures of the orbit), for youth base-ball. From 1999-2001, WEI reported to theUSEIR 41.2 % (n=7) serious eye injuries frombaseball; these types of injuries dropped to 0% in2002. A similar bill on approved gear and equip-ment in youth baseball was introduced to the 2003Maryland General Assembly. USEIR data onbaseball eye injury were presented by Dr. StuartR. Dankner, pediatric ophthalmologist, facultymember of the WEI and Chairman of the EyeSafety Committee, Maryland Society for Sight, inhis testimony to support this bill which will be re-introduced to the Assembly in 2004.
The WER physicians and nurses are activeparticipants in the Johns Hopkins Disaster Plan,

37
Operation Red: Chemical Plan. The nursing staffassembled an eye irrigation cart to initiate treat-ment for victims of chemical eye burns. The cartincludes the recommended PPE (protective per-sonal equipment) to protect staff from chemicalagent contamination.
WEI collaborated with the Johns HopkinsOffice of Compliance on how the WER is meetingregulatory requirements of EMTALA or theEmergency Medical Treatment and Active LaborAct (anti-dumping law). An ocular triage levelingsystem (believed to be the first of its kind national-ly) was developed. Triage level 1 with zero waittime consists of three eye conditions, two of whichare eye trauma: chemical eye injury and protrud-ing object from the eye (possible intra-ocular for-eign body). It was also defined that for a specialtyeye emergency room, an ocular screening examby the ophthalmic nurse, a QMP (qualified med-ical personnel), determines if an emergency ocularcondition exists. Definitive ophthalmic diagnosis ismade by the physician.
WEI developed the MIEMSS QualityImprovement Indicators of Care for OcularTrauma, which was reviewed by Mary Beachley,RN, MSN, MIEMSS Director of HospitalPrograms. Both the Ocular Triage Leveling Systemand Ocular Trauma Indicators of Care will bepublished in the web site of the US Eye InjuryRegistry.
Victoria B. Navarro, RN, MAS, MSN,Director of Nursing, was appointed as a memberof the Funding Sources Research Committee,American Society of Ocular Trauma (ASOT) andUS Eye Injury Registry (USEIR).
During FY 2003, the WEI faculty made 12presentations on ocular trauma.
Statistics for Serious Eye Injuries
Note: Selected Data 1999-2002 from Maryland via the UnitedStates Eye Injury Registry (N=286) which contains reports ofserious eye injuries according to the USEIR criteria. Data pro-vided by the United States Eye Injury Registry, through fundingby the Helen Keller Foundation, Birmingham, Alabama, USA.
The above Note applies to statistics for Age, Eye Protection,Work Related Injuries, Sports Injuries, Source and Place of Injuries.
AGERange 2-93 yearsMean: 29.09 years. Median: 30 years.48% were less than 30 years old.
Age Percentage0-9 9.2%10-19 23.6%20-29 16.2%30-39 20.4%40-49 15.5%50-59 4.9%60-69 3.2%≥70 7%
EYE PROTECTION
None 85.1%Regular 2.2%Safety 3%Sun 0%
WORK RELATED INJURIES = 11.89%
Leading Reported Occupation:Construction/Contractor
Leading Reported Injury Source:Blunt Object
SPORTS INJURIES = 3.58%
Baseball 41.2%Basketball 14.7%Soccer 14.7%Softball 14.7%Other 14.7%
PLACE OF INJURY
Home 35.3%Street and Highway 27.0%Place for Recreation or Sport 7.9%Industrial Premises 7.6%School 4.0%Public Building 2.2%Other 5.8%Unknown 10.4%
SOURCE OF INJURY

38
Maryland Eye Trauma SystemSuburban Hospital Eye Trauma Center
Suburban Hospital has served as a state-designatedEye Trauma Center since July 2001 with a dedicat-ed, fully equipped eye trauma room for the evalua-tion and treatment of eye trauma patients. LeonardParver, MD, serves as the Medical Director andAnne Kuzas, as its Trauma NurseCoordinator/Program Manager. Dr. BenjaminRubin, who is affiliated with the National EyeInstitute, serves as the Clinical Director of the EyeTrauma Research Program.The Suburban Hospital Eye Trauma Center
treated 62 eye trauma patients during FY 2003. Ofthese 62 cases, 87% were due to blunt injuries, 8%were due to penetrating injuries, and 5% were dueto other causes such as chemical exposures.
The Eye Trauma Center continued to beactive with the community outreach programthrough participation in multiple educational andcommunity outreach activities through schoolevents, after-school programs, health fairs, semi-nars, and work sites. Prevention measures, eyesafety, and visual assessment are program compo-nents.
Eye Trauma Patient Statistics
GENDER FY 01 FY 02 FY 03Male 61% 71% 85%Female 39% 29% 15%
Neurotrauma CenterR Adams Cowley Shock Trauma Center
The Neurotrauma Center at the R Adams CowleyShock Trauma Center, University of MarylandMedical System, provides comprehensive manage-ment for patients with brain, spinal cord, andspinal-column-related injuries. Bizhan Aarabi, MD,is the Director of the Neurotrauma Center.
More than 500 neurosurgical procedures wereperformed for a variety of acute complex headand spinal cord injuries. Patients with epiduralhematomas, intracerebral hematomas, subduralhematomas, and subarachnoid hemorrhagesreceived care based on the latest treatment proto-cols. The Neurotrauma Center also provided state-of-the-art care for patients with complex spinal col-umn injuries.
Pediatric Trauma Center at the JohnsHopkins Children’s Center
In FY 2003, 978 children (ages newborn to 14years) were treated at the Pediatric Trauma Centerat the Johns Hopkins Children’s Center, located inBaltimore City. Charles N. Paidas, MD, is theDirector, and Susan Ziegfeld, MSN, CCRN,CPNP, serves as the Trauma Nurse Coordinator.
The Pediatric Trauma Service (PTS) at theJohns Hopkins Children’s Center is the Level 1pediatric trauma facility for the state of Maryland.The PTS is an advocate in the care of critically illand injured children and is actively involved inthe prevention of pediatric injuries at the local,state, and national levels. The PTS integratespatient care with ongoing National Institutes ofHealth (NIH)-funded laboratory and clinicalresearch and collaborates with other departmentsand the community to provide childhood injuryprevention activities. Charles N. Paidas, MD,Director of the Pediatric Trauma Center, serves asthe American College of Surgeons State Chair forthe Committee on Trauma. In addition, he is avoting member of the Maryland PediatricEmergency Medical Advisory Group (PEMAG).Moreover, Dr. Paidas is co-chairman of thePediatric Advanced Life Support Course (PALS)and has brought this course to Greece to assist intraining physicians and health care providersabroad.
Susan Ziegfeld, MSN, CCRN, CPNP, TraumaNurse Coordinator, serves on the MarylandTrauma and Specialty Care Quality ImprovementCommittee and on the Maryland Trauma Registry,Education and Injury Prevention Committee. Sheis serving as Course Director, in collaboration withthe Air Force and R Adams Cowley Shock TraumaCenter, to train nurses in Advanced Trauma LifeSupport.
Vinita Misra Knight, MPH, Pediatric TraumaProgram Coordinator, serves on the MarylandTrauma and Specialty Care Quality ImprovementCommittee, the Maryland Trauma Registry,Education and Injury Prevention Committee, andthe Pediatric Quality Improvement Committee ofthe Maryland EMS Quality Leadership Council.Mary Pasquariello, Pediatric Trauma Registrar,oversees all aspects of data collection and manage-ment. Both Ms. Knight and Ms. Pasquariello arecertified as car safety seat technicians and certifiedby the American Trauma Society as Specialists inTrauma Registry.

39
All members of the Pediatric Trauma Serviceactively participate in prehospital provider follow-up and education. Elizabeth Berg, RN, BSN,Nursing Outreach Coordinator for the HopkinsOutreach for Pediatric Education (HOPE), hasserved in numerous capacities throughout theEMS system to enhance the care of critically illand injured children. HOPE has continued to pro-vide quality educational programs for all prehospi-tal providers. More than 340 participants havecompleted the PALS course during the past year.
The Pediatric Trauma Service is involved inseveral other research initiatives, including a trau-matic brain injury study funded by the Centers forDisease Control, pelvic fractures, child physicalabuse, spinal injury, motor vehicle crashes, andincidents involving all-terrain vehicles. In addition,the Pediatric Trauma Service of the Children’sCenter received funding from the Robert WoodJohnson Foundation, in November 2002, forHopkins to become the 27th local site, of theInjury Free Coalition for Kids (IFCK). IFCK is anational network of community-based hospitalsand community advocates, focused on the preven-tion and reduction of injuries to children. InMarch 2003, the IFCK of Baltimore appointedMahseeyahu Ben Selassie, MSW, MPH, as theProject Administrator. The Baltimore Coalition’sprogram will gather information and input fromcommunity residents on injuries to children intheir neighborhoods. Combined with the datafrom pediatric trauma records, IFCK will trainparents, residents, neighbors, and caregivers tobecome safety leaders and teachers in their com-munities. The coalition has been meeting on a reg-ular basis for program planning and held its firstsuccessful focus group session in July.
Pediatric Trauma CenterChildren’s National Medical Center
In FY 2003, Children’s National Medical Center,as a pediatric specialty referral center, treated 919children with multiple trauma and burns who wereresidents of Maryland or who were injured inMaryland. Martin R. Eichelberger, MD, is theDirector of Emergency Trauma-Burn Services andKim Rogoza, RN, MSN, CPNP is the Trauma-Burn Coordinator.
The Children’s National Medical Center(CNMC) was re-verified by the American Collegeof Surgeons in June 2000 as a Level I PediatricTrauma Center. CNMC serves the pediatric com-munity of Region V, which includes Montgomery,Prince George’s, Calvert, Charles, and St. Mary’s
counties, by caring for children with multiple trau-ma and burns.
CNMC provides pediatric emergency andtrauma education to physicians, nurses, and pre-hospital providers. The EMT-B course is offeredtwice a year. Ten courses in Pediatric AdvancedLife Support (PALS) are offered annually. Fourcourses in the Pediatric Education for PrehospitalProfessionals (PEPP) were taught in 2003. TheCenter for Prehospital Pediatrics has produced amodel protocol for EMS to care for children withspecial needs. The Trauma Nurse CoreCurriculum (TNCC) is offered annually. Advancesin Pediatric Emergency Medicine is also offeredannually to community physicians.
Since its inception in 1987, the National SAFEKIDS Campaign (NSKC), a subsidiary of CNMC,has contributed to the decrease of childhood fatali-ties by: 10% from motor crashes, 34% fromdrowning, 53% from non-helmeted bike riders,and 56% from residential fires. The campaigninteracts with more than 300 state and local SAFEKIDS coalitions in 50 states and 2 jurisdictionsand 16 foreign countries to bring the prevention ofunintentional injury to the grass roots level. Inaddition, the NSKC provides critical safetydevices to those who cannot afford them, advo-cates for new and stronger safety legislation, andconducts primary research to identify who is mostaffected by injury and why (see www.safekids.org).
CNMC houses the Emergency MedicalServices for Children (EMSC) National ResourceCenter and supports programs that enhance thequality of medical and trauma care those childrenreceive. Since 1984, EMSC has provided 82 newand continuing grantees with technical assistanceand support for 14 Partnerships for ChildrenConsortium members. EMSC joined theAmerican College of Emergency Physicians foranother successful and highly visible nationalobservance of EMS week (May19-25). Duringthese challenging times, the EMSC initiative isfocused on an increasing national awareness of the

40
need to have an emergency response system thatis fully prepared for catastrophic emergencies (seewww.ems-c.org).
CNMC is part of the Crash Injury Researchand Engineering Network (CIREN), funded bythe National Highway Traffic SafetyAdministration/USDOT. It is the only pediatriccenter of seven centers nationwide investigatingthe bio-mechanics of vehicle crashes and theanatomic and physiologic impact on children. Thisinformation is used by pediatric professional orga-nizations, child restraint manufacturers, and otherchild passenger safety groups to design preventionprograms, make technological improvements torestraints and vehicles, and develop advocacy andpolicy recommendations (see www-nrd.nhtsa.dot.gov/departments/nrd-50/ciren/CIREN.html).
CNMC is one of 40 pediatric centers partici-pating in the Partnership for Development andDissemination of Outcome Measures for InjuredChildren: A Multi-Center Study of Burn InjuryAssessment and Outcomes, coordinated by theAmerican Pediatric Surgical Association (APSA).The objective is to obtain patient-based clinicaldata that allow for a comparison among burntreatments used in current practice. The datainclude clinical assessment and management;patient parameters of pain and anxiety, appear-ance, behavior, and parental issues such as expec-tations and stress. The data will be analyzed todetermine which clinical management strategiesappear to optimize outcome. Currently, Children'sis the leading pediatric user of TransCyteTM, abio-engineered skin equivalent, on partial thick-ness burns, which has reduced inpatient length ofstay from 2 weeks to 2 days (www.eapsa.org).
Perinatal Referral CentersThis year MIEMSS completed the designa-
tion process for the perinatal referral centers, byconducting on-site reviews of four Level III+
applicants. All received full designation as LevelIII+ Perinatal Referral Centers. To date, MIEMSShas designated a total of 12 Level III+ PerinatalReferral Centers. (See page 26 for a complete listof perinatal centers.)
MIEMSS has worked closely with theDepartment of Health and Mental Hygiene(DHMH) regarding perinatal centers in Maryland.DHMH provides grant funds to support a full-time staff member to coordinate the perinatal pro-grams at MIEMSS.
Poison Consultation Center MarylandPoison Center
The Maryland Poison Center (MPC) is a certifiedregional poison center that provides emergency poi-son information by telephone 24 hours a day to thegeneral public and health professionals in the state.A division of the University of Maryland School ofPharmacy, MPC is designated by the MarylandDepartment of Health and Mental Hygiene as thestate’s regional poison center. MPC also serves as aconsultation center for MIEMSS. Bruce D.Anderson, PharmD, DABAT, is Director ofOperations, and Suzanne Doyon, MD, ACMT, isMedical Director.
In Calendar Year 2002, the Maryland PoisonCenter (MPC) received 59,056 calls. While 34,942of these calls involved a human exposure, 2,187involved animal exposures, and the remaining21,927 were requests for information where noexposure occurred. The majority of poison expo-sures (54.6%) involved children under the age ofsix. Although the incidence of poisoning is greaterin children, most severe poisonings and poisoningdeaths occur in adolescents and adults.
Seventy-five percent of the cases reported tothe MPC were managed at a non-health care facil-ity site, such as the home, school, or workplace.Safely managing these patients at the site of theexposure saves millions of dollars in unnecessaryhealth care costs. It also allows more efficient andeffective use of limited health care resources.
All of the poison specialists who work in theMPC are pharmacists, and nurses are required tobe certified as specialists in poison information bythe American Association of Poison ControlCenters. Managing at least 2,000 human-exposure-poisoning cases and passing a national certificationexamination are required to become a certifiedspecialist. Specialists must re-test every seven yearsto maintain their status.

41
The MPC continues to provide educationalprograms and materials to the public and healthprofessionals. Programs for schools, parent groups,workplaces, and other community organizationswere conducted throughout Maryland in 2002.Over 1000 paramedics, nurses, physicians, andpharmacists attended professional education pro-grams provided by the MPC. The MPC alsoserves as a training site for a variety of health pro-fessionals.
The Poison Control Center Enhancement andAwareness Act was signed into federal law inFebruary 2000 to help stabilize the funding of poi-son centers and to assist in poison prevention edu-cation. This law also mandated the establishmentof a nationwide toll-free phone number 1-800-222-1222 that will automatically direct callers to theirregional poison center no matter where they are inthe U.S. The MPC implemented this national tele-phone number in June 2001.
During the past year, education and outreachremained a strong focus for the MPC. It receiveda federal grant award of $179,150 to help supportits education and outreach programs. New educa-tional materials were developed and distributedthroughout the state in 2002. These materials areimportant tools to assist in teaching people aboutpoison prevention and increasing awareness of theservices of the MPC. In addition, Angel Bivensjoined the MPC education team as a full-time pub-lic health educator. Previously she was a certifiedspecialist in poison information at the MPC forseven years. The MPC also contracted with a localadvertising and public relations firm, MGH, toassist with outreach and awareness.
The faculty of the MPC worked with theDepartment of Health and Mental Hygiene andthe Maryland State Board of Pharmacy to developand implement bioterrorism response training pro-grams for pharmacists throughout the state. Fivetraining sessions were conducted to help pharma-cists to be able to respond should there be anotherbiologic agent release.
Research and professional education on themanagement of poisoning patients is critical toimproving patient care and not only in Maryland.During the past calendar year, the faculty of theMPC have been engaged in several research pro-jects and have published eight journal articles andthree book chapters to increase awareness of themost appropriate management of poisoningpatients.
In addition, the MPC implemented a newdata collection system. With the new system, theMPC can submit data in near real-time to anationwide poison center surveillance system. Thegoal is to assist with nationwide monitoring forpossible biologic or chemical weapons exposuresor other toxic outbreaks.
Cause of Poisoning (CY 2002)Circumstance Number of Patients Percentage__________________________________________________________
Unintentional 28,800 82.43Intentional 5,293 15.15Other & Unknown 845 2.42
__________________________________________________________TOTAL 34,938 100.00
Medical Outcome (CY 2002)Medical Outcome Number of Patients Percentage__________________________________________________________
No Effect/Minor Effect 32,294 92.55Moderate Effect 1,295 3.71Major Effect 128 0.37Death 41 0.12Other & Unknown 1,134 3.25__________________________________________________________
TOTAL 34,892 100.00NOTE: The medical outcome is assessed, based on the inherent toxicity ofthe agent and the severity of the clinical manifestations.
Location of Exposure by Region (CY 2002)Region Number of Exposures Percentage__________________________________________________________
Region I (Garrett, Allegany) 716 2.05
Region II (Washington, Frederick) 2,547 7.29
Region III (Carroll, Howard, Harford,Anne Arundel, Baltimore County, Baltimore City) 21,701 62.10
Region IV (Cecil, Kent, Queen Anne’s, Talbot, Caroline, Dorchester,Wicomico, Worcester) 3,226 9.23
Region V (Montgomery, Prince George’sCharles, Calvert, St. Mary’s) 5,661 16.20
UnknownCounty/Other state 1,092 3.13
__________________________________________________________TOTAL 34,942 100.0

42
REHABILITATION
The vision of MIEMSS is the elimination ofpreventable deaths and disabilities due to suddenillness or injury though an integrated system ofprevention, intervention, and rehabilitation. Thisintegrated system is known as the trauma carecontinuum. Rehabilitation is the cornerstone of"post-trauma" care. It is the phase of emergencycare that enables the individual to return to a max-imum level of function and, in most cases, toreturn as a productive member of society.
In Maryland we are fortunate to have anextensive number of rehabilitation providers totreat patients who have experienced neurotrauma,multi-trauma, and orthopedic injuries in varioustreatment settings. The trauma centers providetransitional (subacute) care or have transfer agree-ments with rehabilitation hospitals to provide this
specialized care. Rehabilitation services are pro-vided in hospitals, acute inpatient rehabilitationhospitals, long-term care facilities, home care, out-patient services, and community-based rehabilita-tion programs. During FY 2003, trauma centers inMaryland referred 1,099 trauma patients ages 15and over to inpatient rehabilitation services. Theeleven rehabilitation facilities receiving the mostpatients are listed on this page.
TOP ELEVEN DESTINATIONS OF TRAUMAPATIENTS WHO WENT TO INPATIENT
REHABILITATION FACILITIES:(JUNE 2002 TO MAY 2003)
Source: Maryland Adult Trauma Registry____________________________________________________________________Rehabilitation Center Number
of patients ____________________________________________________________________
Deaton Hospital and Medical Center ofChrist Lutheran Church 37
Genesis Long—Term Care Facilities 17
Good Samaritan Hospital of Maryland 14
Health South Chesapeake Rehabilitation Center,Salisbury, Maryland 22
Kernan Hospital 356
Kessler Adventist Rehabilitation Facilities 18
Maryland General Hospital 57
NRH Regional Rehabilitation @ Irving Street, DC 29
Peninsula Regional Medical Center, Transitional Care Unit 15
Sinai Rehabilitation Center 15
Washington County Health System, ComprehensiveInpatient Rehab Services 31
____________________________________________________________________
Note: Total patients ages 15 and over who went to a rehabilitation center = 1099
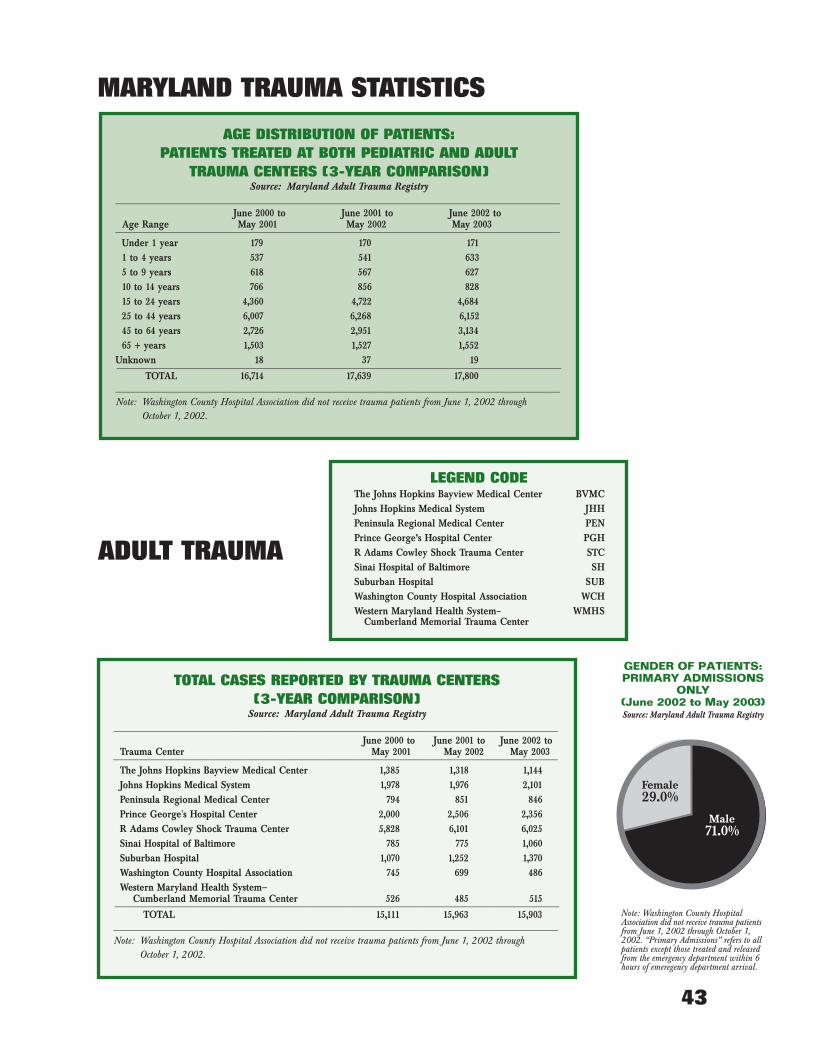
43
MARYLAND TRAUMA STATISTICS
ADULT TRAUMA
GENDER OF PATIENTS:PRIMARY ADMISSIONS
ONLY(June 2002 to May 2003)Source: Maryland Adult Trauma Registry
Male71.0%
Female29.0%
Note: Washington County HospitalAssociation did not receive trauma patientsfrom June 1, 2002 through October 1,2002. “Primary Admissions” refers to allpatients except those treated and releasedfrom the emergency department within 6hours of emeregency department arrival.
LEGEND CODEThe Johns Hopkins Bayview Medical Center BVMCJohns Hopkins Medical System JHHPeninsula Regional Medical Center PENPrince George’s Hospital Center PGHR Adams Cowley Shock Trauma Center STCSinai Hospital of Baltimore SHSuburban Hospital SUBWashington County Hospital Association WCHWestern Maryland Health System– WMHS
Cumberland Memorial Trauma Center
TOTAL CASES REPORTED BY TRAUMA CENTERS(3-YEAR COMPARISON)
Source: Maryland Adult Trauma Registry___________________________________________________________________________________________________
June 2000 to June 2001 to June 2002 toTrauma Center May 2001 May 2002 May 2003 ___________________________________________________________________________________________________The Johns Hopkins Bayview Medical Center 1,385 1,318 1,144Johns Hopkins Medical System 1,978 1,976 2,101 Peninsula Regional Medical Center 794 851 846Prince George's Hospital Center 2,000 2,506 2,356R Adams Cowley Shock Trauma Center 5,828 6,101 6,025Sinai Hospital of Baltimore 785 775 1,060Suburban Hospital 1,070 1,252 1,370 Washington County Hospital Association 745 699 486Western Maryland Health System—
Cumberland Memorial Trauma Center 526 485 515___________________________________________________________________________________________________TOTAL 15,111 15,963 15,903
___________________________________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from June 1, 2002 through
October 1, 2002.
AGE DISTRIBUTION OF PATIENTS:PATIENTS TREATED AT BOTH PEDIATRIC AND ADULT
TRAUMA CENTERS (3-YEAR COMPARISON)Source: Maryland Adult Trauma Registry
___________________________________________________________________________________________________ June 2000 to June 2001 to June 2002 to
Age Range May 2001 May 2002 May 2003 ___________________________________________________________________________________________________Under 1 year 179 170 1711 to 4 years 537 541 633 5 to 9 years 618 567 62710 to 14 years 766 856 82815 to 24 years 4,360 4,722 4,68425 to 44 years 6,007 6,268 6,15245 to 64 years 2,726 2,951 3,134 65 + years 1,503 1,527 1,552
Unknown 18 37 19___________________________________________________________________________________________________TOTAL 16,714 17,639 17,800
___________________________________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from June 1, 2002 through
October 1, 2002.

44
RESIDENCE OF PATIENTS BY COUNTY:SCENE ORIGIN CASES ONLY (JUNE 2002 TO MAY 2003)
Source: Maryland Adult Trauma Registry______________________________________________________________County of Residence Number______________________________________________________________
Allegany County 182Anne Arundel County 829Baltimore County 1,762Calvert County 118Caroline County 76Carroll County 348Cecil County 166Charles County 157Dorchester County 84Frederick County 208Garrett County 37Harford County 433Howard County 273Kent County 49Montgomery County 1,172Prince George's County 1,536Queen Anne's County 94St. Mary’s County 112Somerset County 56Talbot County 45Washington County 280Wicomico County 253Worcester County 108Baltimore City 4,044Virginia 316West Virginia 226Pennsylvania 275Washington, DC 301Delaware 178Other 380Not Indicated 97______________________________________________________________
TOTAL 14,195______________________________________________________________Note: Washington County Hospital Association did not receive trauma
patients from June 1, 2002 through October 1, 2002. Scene origincases represent 89.3% of the total trauma cases treated statewide.
OCCURRENCE OF INJURY BY COUNTY:SCENE ORIGIN CASES ONLY (JUNE 2002 TO MAY 2003)
Source: Maryland Adult Trauma Registry_________________________________________________________________County of Injury Number_________________________________________________________________
Allegany County 227Anne Arundel County 817Baltimore County 1,726Calvert County 109Caroline County 74Carroll County 350Cecil County 225Charles County 144Dorchester County 88Frederick County 242Garrett County 46Harford County 406Howard County 393Kent County 55Montgomery County 1,372Prince George's County 1,675Queen Anne's County 134St. Mary's County 93Somerset County 51Talbot County 50Washington County 365Wicomico County 283Worcester County 166Baltimore City 4,191Virginia 46West Virginia 184Pennsylvania 79Washington, DC 142Delaware 110Other 1Not Indicated 351
TOTAL 14,195_________________________________________________________________Note: Washington County Hospital Association did not receive trauma
patients from June 1, 2002 through October 1, 2002. Scene originrepresents 89.3% ot the total trauma cases treated statewide.
PATIENTS WITH PROTECTIVE DEVICES AT TIMEOF TRAUMA INCIDENT:
PRIMARY ADMISSIONS ONLY (3-YEAR COMPARISON)
Source: Maryland Adult Trauma Registry________________________________________________________________________Protective Device June 2000 to June 2001 to June 2002 to
May 2001 May 2002 May 2003________________________________________________________________________None 29.3% 31.1% 28.1%Seatbelt 40.6% 37.6% 38.3%Airbag & Seatbelt 10.9% 11.4% 14.3%Airbag Only 2.9% 3.0% 2.8%Infant/Child Seat 0.2% 0.2% 0.1%Protective Helmet 7.5% 8.3% 8.0%Padding/Protective Clothing 0.0% 0.1% 0.0%Other Protective Device 0.2% 0.4% 0.2%Unknown 8.4% 7.9% 8.2%________________________________________________________________________TOTAL 100.0% 100.0% 100.0%________________________________________________________________________
Note: Washington County Hosptial Association did not receive trauma patientsfrom June 1, 2002 through October 1, 2002. Patients were involved in motorvehicle, motorcycle, bicycle and sports-related incidents only. “PrimaryAdmissions” refers to all patients except those treated and released from theemergency department within 6 hours of emergency department arrival.

45
EMERGENCY DEPARTMENTARRIVALS BY DAY OF WEEK:PRIMARY ADMISSIONS ONLY
(June 2002 to May 2003)Source: Maryland Adult Trauma Registry
Sunday 16.0%
Monday 13.7%
Tuesday 12.6%
Wednesday 13.5%
Thursday 13.2%
Friday13.9%
Saturday 17.1%
Note: Washington County HospitalAssociation did not receive trauma patientsfrom June 1, 2002 through October 1,2002. “Primary Admissions” refers to allpatients except those treated and releasedfrom the emergency department within 6hours of emeregency department arrival.
AGE DISTRIBUTION OFPATIENTS: PRIMARYADMISSIONS ONLY
(June 2002 to May 2003)Source: Maryland Adult Trauma Registry
Unknown0.1%
1– 4 Yrs.0.3%
25-44 Yrs.
38.4%
15-24 Yrs.
27.3%45-64 Yrs.
20.8%
65+Yrs.11.3%
5–14 Yrs.1.7%
Notes: Washington County HospitalAssociation did not receive trauma patientsfrom June 1, 2002 through October 1,2002. “Primary Admissions” refers to allpatients except those treated and releasedfrom the emergency department within 6hours of emergency department arrival.Only pediatric patients that were treatedat adult trauma centers are included inthis table. For patients treated at pediatrictrauma centers, see pediatric trauma centertables and graphs.
Under 1-Yr.0.1%
EMERGENCY DEPARTMENTARRIVALS BY TIME OF DAY:
PRIMARY ADMISSIONS ONLY(June 2002 to May 2003)Source: Maryland Adult Trauma Registry
0:00–5:5923.1%
6:00–11:5916.1%
12:00–17:5929.0%
18:00–23:5931.8%
Note: Washington County HospitalAssociation did not receive trauma patientsfrom June 1, 2002 through October 1,2002. “Primary Admissions” refers to allpatients except those treated and releasedfrom the emergency department within 6hours of emeregency department arrival.
MODE OF PATIENT TRANSPORT TO TRAUMA CENTERS (JUNE 2002 TO MAY 2003)Source: Maryland Adult Trauma Registry
______________________________________________________________________________________________________________________________________________________Modality Type BVMC JHH PEN PGH SH STC SUB WCH WMHS TOTAL______________________________________________________________________________________________________________________________________________________
Gound Ambulance 86.5% 81.2% 61.0% 63.4% 92.4% 55.8% 75.8% 73.6% 58.5% 67.6%
Helicopter 0.2% 1.9% 30.9% 30.6% 0.0% 43.0% 21.7% 14.3% 29.2% 26.0%
Other 13.3% 16.9% 8.1% 6.0% 7.6% 1.2% 2.5% 12.1% 12.3% 6.4%______________________________________________________________________________________________________________________________________________________
TOTAL 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%______________________________________________________________________________________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from June 1, 2002 through October 1, 2002.
ORIGIN OF PATIENT TRANSPORT TO TRAUMA CENTERS (JUNE 2002 TO MAY 2003)Source: Maryland Adult Trauma Registry
_______________________________________________________________________________________________________________________________________________________Origin Type BVMC JHH PEN PGH SH STC SUB WCH WMHS TOTAL_______________________________________________________________________________________________________________________________________________________
Scene of Injury 94.9% 81.5% 97.3% 97.2% 99.3% 84.3% 96.0% 90.6% 93.4% 89.7%
Hospital Transfer 0.1% 2.6% 2.6% 1.1% 0.6% 15.7% 2.8% 5.6% 5.8% 7.3%
Other 5.0% 15.9% 0.1% 1.7% 0.1% 0.0% 1.2% 3.8% 0.8% 3.0%______________________________________________________________________________________________________________________________________________________
TOTAL 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%_______________________________________________________________________________________________________________________________________________________ Note: Washington County Hospital Association did not receive trauma patients from June 1, 2002 through October 1, 2002.

46
NUMBER OF INJURIES BY AGE(3-YEAR COMPARISON)
Source: Maryland Adult Trauma Registry__________________________________________________________________________
June 2000 to June 2001 to June 2002 toAge May 2001 May 2002 May 2003__________________________________________________________________________Under 1 year 37 24 181 to 4 years 108 88 605 to 14 years 407 404 34415 to 24 years 4,305 4,667 4,62525 to 44 years 6,007 6,268 6,15145 to 64 years 2,726 2,951 3,13465+ years 1,503 1,527 1,552Unknown 18 34 19 __________________________________________________________________________
TOTAL 15,111 15,963 15,903__________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from
June 1, 2002 through October 1, 2002. Only pediatric patients that weretreated at adult trauma centers are included in this table. For patients treatedat the pediatric trauma centers, see pediatric trauma center tables and graphs.
NUMBER OF DEATHS BY AGE (3-YEAR COMPARISON)
Source: Maryland Adult Trauma Registry__________________________________________________________________________
June 2000 to June 2001 to June 2002 toAge May 2001 May 2002 May 2003__________________________________________________________________________Under 1 year 0 2 11 to 4 years 4 4 05 to 14 years 12 8 1115 to 24 years 152 153 15825 to 44 years 177 192 17445 to 64 years 98 103 11065+ years 162 155 173Unknown 9 16 8 __________________________________________________________________________
TOTAL 614 633 635__________________________________________________________________________Deaths Overall as a Percentage of the TotalInjuries Treated 4.1% 4.0% 4.0%__________________________________________________________________________
Note: Washington County Hospital Association did not receive trauma patients fromJune 1, 2002 through October 1, 2002. Only pediatric patients that weretreated at adult trauma centers are included in this table. For patients treatedat the pediatric trauma centers, see pediatric trauma center tables and graphs.
NUMBER OF INJURIES AND DEATHS BY AGE(JUNE 2002 TO MAY 2003)
Source: Maryland Adult Trauma Registry______________________________________________________________________________
Number of Injured Patients Number of DeathsMaryland Maryland
Age Total Residents Total Residents______________________________________________________________________________
Under 1 year 18 16 1 11 to 4 years 60 46 0 05 to 14 years 344 291 11 9 15 to 24 years 4,625 4,099 158 13925 to 44 years 6,151 5,339 174 14545 to 64 years 3,134 2,714 110 9565+ years 1,552 1,362 173 149Unknown 19 14 8 8 ______________________________________________________________________________
TOTAL 15,903 13,881 635 546______________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from June 1,
2002 through October 1, 2002. Only pediatric patients that were treated at adulttrauma centers are included in this table. For patients treated at the pediatric traumacenters, see pediatric trauma center tables and graphs.
ETIOLOGY OF INJURIES TO PATIENTS:PRIMARY ADMISSIONS ONLY
(3-YEAR COMPARISON)Source: Maryland Adult Trauma Registry
__________________________________________________________________________ June 2000 to June 2001 to June 2002 to
Etiology May 2001 May 2002 May 2003 __________________________________________________________________________Motor Vehicle Crash 41.7% 42.1% 40.9%Motorcycle Crash 4.0% 4.6% 4.4%Pedestrian Incident 6.0% 5.9% 5.7%Fall 17.3% 17.6% 17.9%Gunshot Wound 7.7% 7.7% 8.0%Stab Wound 6.6% 7.3% 8.1%Other 16.7% 14.8% 15.0%__________________________________________________________________________
TOTAL 100.0% 100.0% 100.0%__________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from
June 1, 2002 through October 1, 2002. “Primary Admissions” refers to allpatients except those treated and released from the emergency department within6 hours of emergency department arrival.
BLOOD ALCOHOL CONTENT OF PATIENTS BY INJURY TYPE: PRIMARY ADMISSIONS ONLY (JUNE 2002 TO MAY 2003)
Source: Maryland Adult Trauma Registry__________________________________________________________________________________________________
Motor Vehicle Blood Alcohol Content Crash Assault Fall Other Total __________________________________________________________________________________________________ Negative 52.4% 36.8% 43.3% 46.0% 46.7%Positive 22.1% 34.4% 15.7% 10.4% 22.9%Undetermined 25.5% 28.8% 41.0% 43.6% 30.4%__________________________________________________________________________________________________
TOTAL 100.0% 100.0% 100.0% 100.0% 100.0%__________________________________________________________________________________________________ Note: Washington County Hospital Association did not receive trauma patients from June 1, 2002 through
October 1, 2002. “Primary Admissions” refers to all patients except those treated and released from theemergency department within 6 hours of emergency department arrival.

47
INJURY TYPE DISTRIBUTIONOF PATIENTS: PRIMARY
ADMISSIONS ONLY(June 2002 to May 2003)Source: Maryland Adult Trauma Registry
Penetrating Injuries 17.2%
BluntInjuries 82.8%
Note: Washington County HospitalAssociation did not receive trauma patientsfrom June 1, 2002 through October 1,2002. “Primary Admissions” refers to allpatients except those treated and releasedfrom the emergency department within 6hours of emeregency department arrival.
ETIOLOGY DISTRIBUTION FOR PATIENTSWITH BLUNT INJURIES:
PRIMARY ADMISSIONS ONLY (JUNE 2002 TO MAY 2003)
Source: Maryland Adult Trauma Registry_____________________________________________________________________Etiology Percentage_____________________________________________________________________
Motor Vehicle Crash 49.6%Motorcycle Crash 5.3%Pedestrian Incident 6.9%Fall 21.6%Other 15.9%Unknown 0.7%_____________________________________________________________________
TOTAL 100.0%_____________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients
from June 1, 2002 through October 1, 2002. “Primary Admissions” refersto all patients except those treated and released from the emergencydepartment within 6 hours of emergency department arrival.
ETIOLOGY DISTRIBUTION FOR PATIENTSWITH PENETRATING INJURIES:PRIMARY ADMISSIONS ONLY (JUNE 2002 TO MAY 2003)
Source: Maryland Adult Trauma Registry_________________________________________________________________Etiology Percentage_________________________________________________________________
Motor Vehicle Crash 0.6%Pedestrian Incident 0.1%Gunshot Wound 46.8%Stabbing 47.3%Fall 0.6%Other 4.0%Unknown 0.6%_________________________________________________________________
TOTAL 100.0%_________________________________________________________________Note: Washington County Hospital Association did not receive trauma
patients from June 1, 2002 through October 1, 2002. “PrimaryAdmissions” refers to all patients except those treated and releasedfrom the emergency department within 6 hours of emergencydepartment arrival.
ETIOLOGY OF INJURIES BY AGES OF PATIENTS: PRIMARY ADMISSIONS ONLY (JUNE 2002 TO MAY 2003)
Source: Maryland Adult Trauma Registry_______________________________________________________________________________________________________________________________________________________
Motor Vehicle Gunshot StabAge Crash Motorcycle Pedestrian Fall Wound Wound Other Total_______________________________________________________________________________________________________________________________________________________Under 1 year 0.0% 0.0% 0.0% 0.4% 0.0% 0.0% 0.3% 0.1%1 to 4 years 0.2% 0.0% 0.5% 0.5% 0.0% 0.0% 0.6% 0.3%5 to 14 years 1.4% 0.4% 5.9% 1.4% 0.9% 0.7% 2.9% 1.7%15 to 24 years 30.1% 26.7% 20.6% 11.1% 49.3% 38.4% 24.1% 27.4%25 to 44 years 37.0% 48.2% 38.5% 28.3% 39.5% 46.5% 45.1% 38.2%45 to 64 years 20.4% 22.7% 25.5% 27.7% 8.4% 13.0% 22.5% 20.9%65+ years 10.8% 2.0% 8.8% 30.6% 1.2% 1.2% 4.4% 11.3%Unknown 0.1% 0.0% 0.2% 0.0% 0.7% 0.2% 0.1% 0.1%_______________________________________________________________________________________________________________________________________________________
TOTAL 100.0% 100.0% 100.0% 100.0 100.0% 100.0% 100.0% 100.0%_______________________________________________________________________________________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from June 1, 2002 through October 1, 2002. “Primary Admissions” refers to all patients except
those treated and released from the emergency department within 6 hours of emergency department arrival. Only pediatric patients that were treated at adult traumacenters are included in this table. For patients treated at the pediatric trauma centers, see pediatric trauma center tables and graphs.

48
FINAL DISPOSITION OF PATIENTS:PRIMARY ADMISSIONS ONLY
(3-YEAR COMPARISON)Source: Maryland Adult Trauma Registry
_________________________________________________________________Final Disposition June 2000 to June 2001 to June 2002 to
May 2001 May 2002 May 2003_________________________________________________________________Inpatient Rehab Facility 9.6% 9.3% 9.3%Skilled Nursing Facility 2.0% 1.9% 1.6%Residential Facility 1.0% 1.2% 1.3%Specialty Referral Center 2.5% 2.8% 3.4%Home with Services 5.6% 4.3% 4.3%Home 69.3% 70.6% 70.1%Acute Care Hospital 2.5% 2.4% 2.5%Against Medical Advice 1.8% 1.7% 1.6%Morgue/Died 5.4% 5.3% 5.4%Other 0.3% 0.5% 0.5%_________________________________________________________________
TOTAL 100.0% 100.0% 100.0%_________________________________________________________________
Note: Washington County Hospital Association did not receive traumapatients from June 1, 2002 through October 1, 2002. “PrimaryAdmissions” refers to all patients except those treated and releasedfrom the emergency department within 6 hours of emergencydepartment arrival.
INJURY SEVERITY SCORES OF PATIENTS WITHPENETRATING INJURIES: PRIMARY
ADMISSIONS ONLY (3-YEAR COMPARISON)Source: Maryland Adult Trauma Registry
__________________________________________________________________________ June 2000 to June 2001 to June 2002 to
ISS May 2001 May 2002 May 2003__________________________________________________________________________1 to 12 73.7% 73.7% 72.0%13 to 19 10.9% 10.5% 12.3%20 to 35 11.9% 11.5% 12.6%36 to 75 3.5% 4.3% 3.1%__________________________________________________________________________
TOTAL 100.0% 100.0% 100.0%__________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from
June 1, 2002 through October 1, 2002. “Primary Admissions” refers to allpatients except those treated and released from the emergency department within6 hours of emergency department arrival.
INJURY SEVERITY SCORE (ISS) BY INJURY TYPE: PRIMARY ADMISSIONS
ONLY (JUNE 2002 TO MAY 2003)Source: Maryland Adult Trauma Registry
________________________________________________________________________ISS Blunt Penetrating Total ________________________________________________________________________1 to 12 70.1% 72.0% 70.4%
13 to 19 15.6% 12.3% 15.1%20 to 35 11.9% 12.6% 12.0%36 to 75 2.4% 3.1% 2.5%________________________________________________________________________
TOTAL 100.0% 100.0% 100.0%________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients
from June 1, 2002 through October 1, 2002. “Primary Admissions” refers toall patients except those treated and released from the emergency departmentwithin 6 hours of emergency department arrival.
INJURY SEVERITY SCORES OF PATIENTS WITHBLUNT INJURIES: PRIMARY ADMISSIONS ONLY
(3-YEAR COMPARISON)Source: Maryland Adult Trauma Registry
__________________________________________________________________________ June 2000 to June 2001 to June 2002 to
ISS May 2001 May 2002 May 2003__________________________________________________________________________1 to 12 71.3% 70.0% 70.1%13 to 19 15.7% 15.7% 15.6%20 to 35 10.4% 11.7% 11.9%36 to 75 2.6% 2.6% 2.4%__________________________________________________________________________
TOTAL 100.0% 100.0% 100.0%__________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from
June 1, 2002 through October 1, 2002. “Primary Admissions” refers to allpatients except those treated and released from the emergency department within6 hours of emergency department arrival.
INJURY SEVERITY SCORES OF PATIENTS WITHEITHER BLUNT OR PENETRATING INJURIES:
PRIMARY ADMISSIONS ONLY (3-YEAR COMPARISON)
Source: Maryland Adult Trauma Registry__________________________________________________________________________
June 2000 to June 2001 to June 2002 toISS May 2001 May 2002 May 2003__________________________________________________________________________1 to 12 71.6% 70.6% 70.4%13 to 19 14.9% 14.9% 15.1%20 to 35 10.7% 11.6% 12.0%36 to 75 2.8% 2.9% 2.5%__________________________________________________________________________
TOTAL 100.0% 100.0% 100.0%__________________________________________________________________________Note: Washington County Hospital Association did not receive trauma patients from
June 1, 2002 through October 1, 2002. “Primary Admissions” refers to allpatients except those treated and released from the emergency department within6 hours of emergency department arrival.

49
EMERGENCY DEPARTMENTARRIVALS BY DAY OF WEEK:
CHILDREN TREATED ATPEDIATRIC TRAUMA CENTERS
(June 2002 to May 2003)
Sunday 16.8%
Monday 12.8%
Tuesday 15.0%
Wednesday 12.3%
Thursday 12.3%
Friday13.3%
Saturday 17.5
Note: For children who were treatedat adult trauma centers, see MarylandAdult Trauma Report. Children’sNational Medical Center data includepatients residing in Maryland and/orinjured in Maryland.
EMERGENCY DEPARTMENTARRIVALS BY TIME OF DAY:
CHILDREN TREATED ATPEDIATRIC TRAUMA CENTERS
(June 2002 to May 2003)
Note: For children that were treated atadult trauma centers, see MarylandAdult Trauma Report. Children’sNational Medical Center data includepatients residing in Maryland and/orinjured in Maryland.
12:00–17:5934.9%
18:00–23:5942.1%
06:00–11:599.7%
00:00–5:5913.3%
MARYLAND PEDIATRIC TRAUMA STATISTICS
OCCURRENCE OF INJURY BY COUNTY:SCENE ORIGIN CASES ONLY Children Treated at Pediatric Trauma
Centers ( June 2002 to May 2003)_________________________________________________________________County of Injury Number_________________________________________________________________
Anne Arundel County 78Baltimore County 97Calvert County 12Caroline County 5Carroll County 37Cecil County 31Charles County 27Dorchester County 2Frederick County 19Harford County 55Howard County 32Kent County 5Montgomery County 114Prince George's County 215Queen Anne's County 15St. Mary's County 30Somerset County 1Talbot County 6Washington County 8Baltimore City 172Virginia 0Pennsylvania 2Washington, DC 24Delaware 0Other 1Not Indicated 168_________________________________________________________________
TOTAL 1,156_________________________________________________________________Notes: For children who were treated at adult trauma centers, see
Maryland Adult Trauma Report. Children’s National Medical Center data include patients residing in Maryland and/orinjured in Maryland. Scene origin cases represent 60.9% of thetotal cases treated at pediatric trauma centers.
LEGEND CODEChildren’s National Medical Center CNMCJohns Hopkins Pediatric Trauma Center JHP
CHILDREN TREATED AT PEDIATRIC TRAUMA CENTERS (3-YEAR COMPARISON)
_______________________________________________________________________________ June 2000 to June 2001 to June 2002 to
Trauma Center May 2001 May 2002 May 2003 _______________________________________________________________________________CNMC 833 864 919 JHP 770 812 978 _______________________________________________________________________________
TOTAL 1,603 1,676 1,892 _______________________________________________________________________________Note: For children that were treated at adult trauma centers, see Maryland Adult Trauma
Report. Children’s National Medical Center data include patients residing in Marylandand/or injured in Maryland.
GENDER PROFILE:CHILDREN TREATED AT
PEDIATRIC TRAUMA CENTERS(June 2002 to May 2003)
Male64.7%
Female35.3%
Note: For children who were treatedat adult trauma centers, see MarylandAdult Trauma Report. Children’sNational Medical Center data includepatients residing in Maryland and/orinjured in Maryland.

50
OUTCOME PROFILE:CHILDREN TREATED AT
PEDIATRIC TRAUMA CENTERS(June 2002 to May 2003)
Died 1.7%
Lived98.3%
Note: For children who were treatedat adult trauma centers, see MarylandAdult Trauma Report. Children’sNational Medical Center data includepatients residing in Maryland and/orinjured in Maryland.
MODE OF PATIENT TRANSPORT BY CENTERChildren Treated at Pediatric Trauma
Centers (June 2002 to May 2003)___________________________________________________________________Modality Type CNMC JHP Total___________________________________________________________________
Ground Ambulance 29.8% 49.6% 40.3%
Helicopter 28.5% 33.0% 30.9%
Other 41.7% 17.4% 28.8%___________________________________________________________________TOTAL 100.0% 100.0% 100.0%___________________________________________________________________
Note: For children who were treated at adult trauma centers, see MarylandAdult Trauma Report. Children’s National Medical Center data includepatients residing in Maryland and/or injured in Maryland.
ORIGIN OF PATIENT TRANSPORT BY CENTERChildren Treated at Pediatric Trauma
Centers (June 2002 to May 2003)_____________________________________________________________________Origin CNMC JHP Total_____________________________________________________________________
Scene of Injury 55.8% 65.9% 61.0%
Hospital Transfer 40.8% 25.7% 33.0%
Other 3.4% 8.4% 6.0%_____________________________________________________________________TOTAL 100.0% 100.0% 100.0%_____________________________________________________________________
Note: For children who were treated at adult trauma centers, see Maryland AdultTrauma Report. Children’s National Medical Center data include patientsresiding in Maryland and/or injured in Maryland.
ETIOLOGY OF INJURIES BY AGES Children Treated at Pediatric Trauma Centers (June 2002 to May 2003)
_______________________________________________________________________________________________________________________________________________________Motor Vehicle Gunshot Stab
Age Crash Motorcycle Pedestrian Fall Wound Wound* Other Total_______________________________________________________________________________________________________________________________________________________Under 1 year 4.0% 0.0% 0.6% 11.8% 0.0% 0.0% 9.9% 8.1%1 to 4 years 22.1% 5.6% 16.9% 36.6% 12.0% 25.8% 34.3% 30.4%5 to 9 years 38.7% 33.3% 44.5% 26.6% 12.0% 16.1% 21.3% 28.3%10 to 14 years 33.9% 61.1% 38.0% 23.1% 68.0% 54.9% 28.8% 30.1%15+ years 1.3% 0.0% 0.0% 1.9% 8.0% 3.2% 5.7% 3.1%_______________________________________________________________________________________________________________________________________________________
TOTAL 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%_______________________________________________________________________________________________________________________________________________________Notes: For children who were treated at adult trauma centers, see Maryland Adult Trauma Report. Children’s National Medical Center data include patients
residing in Maryland and/or injured in Maryland.*Stab wounds include both intentional and unintentional piercing and punctures.
FINAL DISPOSITION OF PATIENTS:Children Treated at Pediatric Trauma
Centers (3-Year Comparison)_________________________________________________________________Final Disposition June 2000 to June 2001 to June 2002 to
May 2001 May 2002 May 2003_________________________________________________________________Inpatient Rehab Facility 2.3% 1.7% 1.7%Skilled Nursing Facility 0.1% 0.0% 0.1%Residential Facility 0.1% 0.1% 0.2%Specialty Referral Center 0.3% 0.6% 0.6%Home with Services 2.3% 2.5% 1.4%Home 92.3% 92.1% 92.2%Acute Care Hospital 0.2% 0.4% 1.1%Against Medical Advice 0.2% 0.1% 0.1%Morgue/Died 1.9% 2.0% 1.7%Foster Care 0.1% 0.3% 0.7%Other 0.2% 0.2% 0.2%_________________________________________________________________
TOTAL 100.0% 100.0% 100.0%_________________________________________________________________
Note: For children who were treated at adult trauma centers, see MarylandAdult Trauma Report. Children’s National Medical Center datainclude patients residing in Maryland and/or injured in Maryland.

51
INJURY TYPEChildren Treated at Pediatric Trauma Centers
(3-Year Comparison)__________________________________________________________________________
June 2000 to June 2001 to June 2002 toInjury Type May 2001 May 2002 May 2003__________________________________________________________________________Blunt 78.5% 80.3% 77.8%Penetrating 2.8% 2.8% 3.0%Burn 8.5% 6.0% 6.6%Near Drowning 1.6% 1.6% 1.5%Hanging 0.3% 0.1% 0.2%Inhalation 0.4% 0.7% 1.0% Ingestion 6.8% 7.2% 7.9%Crush 0.0% 0.1% 0.0%Snake Bite/Spider Bite 0.1% 0.1% 0.3% Animal Bite/Human Bite 0.7% 1.0% 1.4% Other 0.3% 0.1% 0.3% __________________________________________________________________________
TOTAL 100.0% 100.0% 100.0%__________________________________________________________________________Note: For children who were treated at adult trauma centers, see Maryland Adult
Trauma Report. Children’s National Medical Center data include patientsresiding in Maryland and/or injured in Maryland.
NUMBER OF INJURIES BY AGEChildren Treated at Pediatric Trauma Centers
(3-Year Comparison)__________________________________________________________________________
June 2000 to June 2001 to June 2002 toAge May 2001 May 2002 May 2003__________________________________________________________________________Under 1 year 142 146 1531 to 4 years 429 453 5735 to 9 years 491 450 54010 to 14 years 486 569 57115+ years 55 55 60Unknown 0 3 0 __________________________________________________________________________
TOTAL 1,603 1,676 1,897__________________________________________________________________________Note: For children that were treated at adult trauma centers, see Maryland Adult
Trauma Report. Children’s National Medical Center data include patientsresiding in Maryland and/or injured in Maryland.
NUMBER OF DEATHS BY AGEChildren Treated at Pediatric Trauma Centers
(3-Year Comparison)__________________________________________________________________________
June 2000 to June 2001 to June 2002 toAge May 2001 May 2002 May 2003__________________________________________________________________________Under 1 year 3 3 61 to 4 years 11 15 115 to 9 years 10 6 910 to 14 years 5 9 615+ years 2 0 1Unknown 0 1 0 __________________________________________________________________________
TOTAL 31 34 33__________________________________________________________________________Note: For children that were treated at adult trauma centers, see Maryland Adult
Trauma Report. Children’s National Medical Center data include patientsresiding in Maryland and/or injured in Maryland.
MECHANISM OF INJURYChildren Treated at Pediatric Trauma Centers
(3-Year Comparison)__________________________________________________________________________
June 2000 to June 2001 to June 2002 toMechanism May 2001 May 2002 May 2003__________________________________________________________________________Motor Vehicle Crash 18.7% 21.6% 19.7%Motorcycle Crash 1.4% 1.5% 1.0%Pedestrian Incident 13.7% 10.7% 8.8%Gunshot Wound 1.0% 1.4% 1.3%Stabbing* 1.6% 1.5% 1.6%Fall 27.1% 28.7% 30.5%Other 36.5% 34.6% 37.1% __________________________________________________________________________
TOTAL 100.0% 100.0% 100.0%__________________________________________________________________________Note: For children who were treated at adult trauma centers, see Maryland Adult
Trauma Report. Children’s National Medical Center data include patientsresiding in Maryland and/or injured in Maryland.
*Stab wounds include both intentional and unintentional piercing and punctures.
NUMBER OF INJURIES AND DEATHS BY AGEChildren Treated at Pediatric Trauma Centers
(June 2002 to May 2003)__________________________________________________________________________
Number of Injured Patients Number of DeathsMaryland Maryland
Age Total Residents Total Residents__________________________________________________________________________
Under 1 year 153 147 6 41 to 4 years 573 547 11 105 to 9 years 540 503 9 9 10 to 14 years 571 544 6 515+ years 60 59 1 1__________________________________________________________________________
TOTAL 1,897 1,800 33 29__________________________________________________________________________Note: For children who were treated at adult trauma centers, see Maryland Adult
Trauma Report. Children’s National Medical Center data include patientsresiding in Maryland and/or injured in Maryland.

52
RESIDENCE OF INJURY BY COUNTY:SCENE ORIGIN CASES ONLY Children Treated at Pediatric Trauma
Centers ( June 2002 to May 2003)_________________________________________________________________County of Injury Number_________________________________________________________________
Anne Arundel County 92Baltimore County 117Calvert County 15Caroline County 5Carroll County 43Cecil County 33Charles County 33Dorchester County 3Frederick County 26Harford County 50Howard County 19Kent County 0Montgomery County 129Prince George's County 248Queen Anne's County 16St. Mary's County 32Somerset County 1Talbot County 2Washington County 5Baltimore City 219Virginia 5Pennsylvania 9Washington, DC 9Delaware 4Other 41Not Indicated 0_________________________________________________________________
TOTAL 1,156_________________________________________________________________Notes: For children who were treated at adult trauma centers, see
Maryland Adult Trauma Report. Children’s National Medical Center data include patients residing in Maryland and/orinjured in Maryland. Scene origin cases represent 60.9% of thetotal cases treated at pediatric trauma centers.
CHILDREN WITH PROTECTIVE DEVICES AT TIMEOF TRAUMA INCIDENT: CHILDREN TREATED AT
PEDIATRIC TRAUMA CENTERS (3-YEAR COMPARISON)
________________________________________________________________________Protective Device June 2000 to June 2001 to June 2002 to
May 2001 May 2002 May 2003________________________________________________________________________None 33.1% 33.6% 36.1%Seatbelt 17.6% 18.9% 18.6%Airbag & Seatbelt 1.3% 1.7% 0.8%Airbag Only 0.2% 0.4% 0.6%Infant/Child Seat 8.5% 11.3% 9.7%Protective Helmet 8.5% 6.9% 7.9%Padding/Protective Clothing 0.0% 0.2% 0.2%Other Protective Device 0.2% 0.0% 0.2%Unknown 30.6% 27.0% 25.9%________________________________________________________________________TOTAL 100.0% 100.0% 100.0%________________________________________________________________________
Note: Children were involved in motor vehicle, motorcycle, bicycle, and sports-relatedincidents only. For children that were treated at adult trauma centers, seeMaryland Adult Trauma Report. Children’s National Medical Center datainclude patients residing in Maryland and/or injured in Maryland.

53
The National Study Center for Trauma andEmergency Medical Systems (NSC), at theUniversity of Maryland School of Medicine, is theprimary research center of the Maryland EMSSystem. The NSC collaborates with federal agencies,academic institutes, and governmental groups inprojects focused on injury epidemiology, injury pre-vention, and improvements in the prehospital andinhospital delivery and coordination of trauma care.Colin F. Mackenzie, MD, is the Director.
The National Study Center for Trauma andEmergency Medical Systems (NSC) is a leadingparticipant in two multi-center studies of injuriessustained in vehicular crashes, the Crash InjuryResearch and Engineering Network (CIREN) andthe Crash Outcomes Data Evaluation System(CODES) Data Network. To date, 293 patientshave been enrolled into the CIREN study, amulti-center collaboration of nine trauma centers.Recent presentations about this research havebeen made to the National Highway Traffic SafetyAdministration (NHTSA) addressing injuriesincurred in "vehicle mismatch" collisions. In addi-tion, patient interview data collected at six monthsand one year post-injury were presented at the46th annual meeting of the Association for theAdvancement of Automotive Medicine in Tempe,Arizona.
As part of the CIREN project, the NSC hasalso been funded by NHTSA to ascertain econom-ic costs and long-term outcomes associated withlower extremity injuries.
The NSC is also part of the CODES data net-work that provides data to NHTSA and other par-ties with an interest in highway safety. During FY2003, CODES data were used in projects thatwere presented at several national and internation-al conferences. Two such projects—an evaluation ofthe graduated licensing law in Maryland and adescription of the police perception of alcohol useamong Maryland drivers—were presented at themeeting of the American Public HealthAssociation in Philadelphia. The NSC was recent-ly awarded a five-year extension to continue itsrole in the CODES data network.
In April 2003, the NSC was awarded a three-year contract from the US Army to study mildtraumatic brain injury and long-term outcomes inShock Trauma patients with blunt trauma injuries.Patients will be given a battery of tests, includingan electronic balance test and various neuropsy-chological and cognitive measures, by a multi-dis-ciplinary team. Follow-up tests will be adminis-
tered and analyses conducted to determine which,if any, baseline measures predict those with persis-tent physical, cognitive, and behavioral problems.Such measures, if identified, may be useful to theArmy in field settings where decisions related topost-injury deployment must be made.
NSC investigators are focusing on motorcyclesafety as well. NHTSA has awarded funding tocharacterize the population of motorcycle opera-tors and to distinguish factors unique to those whohave experienced motorcycle crashes.Approximately 300 motorcyclists admitted to theShock Trauma Center will be interviewed withregard to their riding training and experiences,with a special focus on those over 40 years of age.Other federal funds will support an investigationof the impact of the motorcycle safety classesoffered by the Motor Vehicle Administration. TheNSC is also participating in a StatewideMotorcycle Safety Coalition in an effort to reducemotorcycle injuries and fatalities through an inter-disciplinary approach.
In August 2002, the NSC received excellentscores from the National Institute for OccupationalSafety and Health for its proposal to conduct athree-year surveillance of work-related injuries inMaryland. Funding is anticipated by mid-summer2003.
A study funded by Robert Wood JohnsonFoundation’s Substance Abuse Policy ResearchProgram in support of an assessment of motorvehicle crash culpability relative to alcohol andother drug use by injured drivers is in its secondyear.
Approximately 500 patients have beenenrolled in a four-year clinical trial of brief inter-vention of trauma patients identified as alcoholdependent. This trial is funded by the NationalInstitute of Alcohol and Alcohol Abuse. The studyhypothesis is that a personalized brief intervention
CHARLES McC.MATHIAS, JR., NATIONALSTUDYCENTERFOR TRAUMA AND EMERGENCY MEDICAL SYSTEMS

54
will result in decreased drinking and consequences(including injury episodes) from alcohol abuse.Enrollment into the trial has ended, but follow-upinterviews at six months have been completed andinterviews at twelve months post-discharge are stillunderway.
The results of a study describing factors thatinfluence hospital admission among children withtraumatic brain injury were published in AcademicEmergency Medicine. Data from another NSC study("Autopsy Study of Motorcyclist Fatalities: TheEffect of the 1992 Maryland Motorcycle HelmetUse Law") of motorcycle fatalities were publishedin the August 2002 American Journal of PublicHealth. These findings were also presented to theMaryland State Legislature in support of non-repeal of the motorcycle helmet law, and present-ed at the Lifesavers Conference for highway safetyprofessionals in Chicago.
During FY 2003, NSC researchers publishedthe third annual "Crash and Injury Fact Book,"which has been developed with support from theMaryland Department of Transportation. As partof this effort, the incidence and severity of motorvehicle-related injuries are being documentedstatewide. These data are available on the NSCweb site (http://nsc.umaryland.edu).
The Human Factors & Technology (HF&T)Group of the Department of Anesthesiology isworking collaboratively with NSC on several pro-jects funded by the National Institutes of Health,the Department of Defense, and the NationalScience Foundation. These collaborating projectsinvestigate potential uses of several types oftelecommunication technologies in field and trans-port care. For example, one project is the integra-tion of wireless mobile communication compo-nents into a system that provides reliable androbust transmission of multimedia diagnostic infor-mation from ambulance crews to receiving physi-cians, logistical control centers, and other experts.In another project, digital ambulances in theExpressCare ambulance system are being used toautomate the transmission of global positioningsystem data and the arrival time of the ambulancesat the University of Maryland Hospital. These dig-ital ambulances are also utilized for cardiacpatients transferred for cardiac catheterization.The potential benefits for this proof of concepttrial are that drug therapy can be initiated oradjusted en route. The catheterization team,whether it is at night or daytime, can be better
coordinated and prepared for patient arrival.Several applications of such field- and transport-based audio, video, and data access are being con-sidered, including mass casualty scene command,en-route diagnosis of acute stroke, and decisionsregarding transport of trauma and seizure patients.Currently, the HF&T researchers are developingvideo-based protocols in collaboration with NASAto assist in space-based medical emergencyresponse.
The NSC is leading a collaborative effortfunded by the US Army (TATRC) between theUniversity of Maryland campus, Baltimore City,State, and military groups to develop a model forLocal Area Defense (LAD) that will result in aDemonstration Exercise in 2004. During the LADDemonstration, inter-operability of communica-tion technologies, psychological and trauma "casu-alty" triage will be tested.
In three clinical projects, the NSC is the leadorganization in conjunction with the ShockTrauma Center in investigation of respectively,Best Practices or Chest Tube Insertion (Agency forHealthcare Research and Quality (AHRQ) fund-ed), Comparison of Succinylcholine andRocuronium for rapid sequence intubation(Organon funded), and a randomized trial of ahemoglobin-based O2 carrier ("blood substitute")in comparison to red cells for major orthopedicsurgery (Biopure funded).
The NSC and AHRQ co-sponsored a sympo-sium, "Video as Research Data" in September2002. The conference summarized research in theuse of video recording and analysis as a tool fordata gathering for topics related to patient safety,improved outcomes, and as a medium for captur-ing behavioral and other data in multiple domains.Participants included invited researchers fromdiverse backgrounds including medicine, educa-tion, psychology, human factors, medical informa-tion, mechanical and industrial engineering, avia-tion and space systems, safety research, legal, cog-nitive engineering, and applied cognitive psychol-ogy.
The NSC Board of Advisors met twice thisyear to review current programs and provide guid-ance to the NSC Director about current and futureinitiatives of mutual interest, such as collaborationwith State, Baltimore City, and University ofMaryland initiatives in homeland defense andpublic health including injury surveillance.

55
GOVERNOR OF MARYLANDRobert L. Ehrlich, Jr.
LIEUTENANT GOVERNORMichael S. Steele
MARYLAND EMS BOARD
Donald L. DeVries, Jr., Esq.ChairpersonPartner, Goodell, DeVries, Leech and Gray Attorneys at Law
Willie C. Blair, MD, FACSAssociate Professor of Surgery, Prince George’s CountyHospital Center
Victor A. BroccolinoPresident and CEO, Howard County General Hospital, Inc.
Dorothy W. Dyott, RNDigestive Health Associates, Easton
John R. FrazierStaff Chief, Baltimore City Fire Department
John M. MurphyPublic at Large (county population less than 175,000)
Nelson SabatiniSecretary of Maryland Department of Health & MentalHygiene
Roger C. Simonds, Sr.Chief, Anne Arundel County Fire DepartmentEx officio (SEMSAC Chairperson)
J. Andrew Sumner, MDEmergency Medical Services Physician
Donald E. Wilson, MDDean and Professor of Medicine, University of MarylandSchool of Medicine
Richard L. YingerPast President, Maryland State Firemen’s Association
STATEWIDE EMS ADVISORY COUNCIL
Roger C. Simonds, Sr.ChairpersonRepresenting EMS Region III Advisory CouncilChief, Anne Arundel County Fire Department
John W. Ashworth IIIRepresenting R Adams Cowley Shock Trauma Center
Wendell G. BaxterRepresenting Volunteer Field Providers
Capt. Barry A. ConteeRepresenting Maryland Metropolitan Fire Chiefs
George B. Delaplaine, Jr.Representing EMS Region II Advisory Council
Steven T. EdwardsRepresenting Maryland Fire & Rescue Institute
Jeffrey L. Fillmore, MDRepresenting EMS Regional Medical Directors
Richard P. Franklin, MDRepresenting American College of Surgeons, MarylandChapter
Wade Gaasch, MDRepresenting Medical and Chirurgical Faculty of Maryland
Kathleen D. GroteRepresenting MD/DC International Association of Firefighters
Murray A. Kalish, MDRepresenting MD/DC Society of Anesthesiologists
Steven J. KesnerRepresenting General Public (County population of less than 175,000)
Bernard KomanRepresenting Maryland Commercial Ambulance Services
Anne Marie Kuzas, RNRepresenting Maryland Trauma Network
Maj. Donald G. LewisRepresenting Maryland State Police Aviation Division
Ronald D. LippsRepresenting Highway Safety Division, Maryland Departmentof Transportation
Colin F. Mackenzie, MDRepresenting National Study Center for Trauma andEmergency Medical Systems
Paul A. Matera, MDRepresenting American College of Emergency Physicians,Maryland Chapter
Kenneth MayRepresenting EMS Region I Advisory Council
Robert SchoonoverRepresenting EMS Region IV Advisory Council
James SchuelenRepresenting the Maryland Hospital Association
Mary Alice Vanhoy, RNRepresenting Maryland Emergency Nurses Association
Allen R. Walker, MDRepresenting American Academy of Pediatrics, MarylandChapter
Charles W. WillsRepresenting Maryland State Firemen’s Association
Craig ColemanMIEMSS SEMSAC Liaison
VacantRepresenting American Association of Critical Care Nurses,Maryland Chapter (Chesapeake Bay)Representing Board of Physician Quality AssuranceRepresenting EMS Region V Advisory CouncilRepresenting the General PublicRepresenting State Emergency Numbers Board (9-1-1)
MARYLAND INSTITUTE FOR EMERGENCY MEDICALSERVICES SYSTEMS
Robert R. Bass, MD, FACEPExecutive Director
653 W. Pratt StreetBaltimore, MD 21201-1536410-706-5074Website: http://www.miemss.org
