multivariate analysis of prognostic factors in patients with rapidly progressive alopecia areata
TRANSCRIPT
Multivariate analysis of prognostic factors in patientswith rapidly progressive alopecia areata
Masaki Uchiyama, MD, Chizu Egusa, Ayako Hobo, MD, Ryokichi Irisawa, MD, Masashi Yamazaki, MD, PhD,and Ryoji Tsuboi, MD, PhD
Tokyo, Japan
From
Fund
Conf
Acce
Repr
D
Background: Alopecia areata (AA) is a common acquired hair disorder showing variable hair loss.Although various prognostic factors have been reported, no evident factors for determining prognosis andappropriate treatment are known.
Objective: To identify prognostic factors in AA patients, especially those with positive results for the hair-pull test on the first visit or with a history of rapidly progressive AA (RPAA) within 6 months prior to the firstvisit.
Methods: One thousand thirty (1030) patients diagnosed with AA at Tokyo Medical University Hospitalwere retrospectively examined for 3 years, and their prognosis was assessed on the basis of various indicesusing multivariate analysis.
Results: Patients with regenerated vellus hairs showed a significantly higher improvement or cure rateregardless of severity. Early onset and lengthy duration were significantly associated with lower cure, andhigher relapse, rates. RPAA patients tended to show a good prognosis regardless of the treatment employed.
Limitations: The present study is retrospective, and treatment modalities were chosen according toclinical and social circumstances.
Conclusion: RPAA patients tend to show a favorable prognosis regardless of treatment modality.Furthermore, the presence of regenerated vellus hairs may indicate a good prognosis. ( J Am AcadDermatol 2012;67:1163-73.)
Key words: acute diffuse and total alopecia; alopecia areata; hair-pull test; multivariate analysis; prognosticfactor; rapidly progressive alopecia areata.
Abbreviations used:
AA: alopecia areataADTA: acute diffuse and total alopecia areataAT: alopecia totalisAU: alopecia universalis
INTRODUCTIONAlopecia areata (AA), the most common form of
acquired alopecia, shows variable hair loss1 andaffects infants and elderly patients alike.2 The extentand pattern of hair loss can be classified by clinicaltypes, such as the patchy type, ophiasis type, alope-cia totalis (AT), and alopecia universalis (AU)3,4 or bygrade (percent) of scalp hair loss (S1-S5).4
Prognosis of AA is influenced by various factors,including age,5,6 severity of hair loss,6 and acuteprogression.7,8 Identification of prognostic factorssolely by means of univariate analysis is difficult. In
the Department of Dermatology, Tokyo Medical University.
ing sources: None.
licts of interest: None declared.
pted for publication June 5, 2012.
int requests: Masaki Uchiyama, MD, Department of
ermatology, Tokyo Medical University, 6-7-1 Nishi-Shinjuku,
the present study, 1030 patients diagnosed with AAat our clinic were retrospectively examined for 3years, and the prognosis of 311 AA patients wasassessed using multivariate analysis to identify prog-nostic factors as independent factors.
Shinjuku-ku, Tokyo 160-0023, Japan. E-mail: sky777xyz@yahoo.
co.jp.
Published online September 24, 2012.
0190-9622/$36.00
� 2012 by the American Academy of Dermatology, Inc.
http://dx.doi.org/10.1016/j.jaad.2012.06.006
1163

J AM ACAD DERMATOL
DECEMBER 20121164 Uchiyama et al
The main purpose of this study was twofold: first,to compare the prognosis of patients with rapidlyprogressive AA (RPAA), defined as those with pos-itive hair-pull test results across the entire scalp onthe first visit or with a history of onset or rapidworsening of hair loss across the entire scalp within 6months prior to first visit, with that of other types of
CAPSULE SUMMARY
d Alopecia areata (AA) shows variableextent of hair loss and prognosis. Somepatients present a form of rapidlyprogressive AA (RPAA).
d Regenerated vellus hairs and RPAA arefavorable prognostic factors regardlessof severity. Early onset and lengthyduration are poor prognostic factors.
AA (non-RPAA) patients and,second, to examine the prog-nostic factors among RPAApatients.
METHODSPatients
The profiles and progno-ses of patients diagnosedwith AA at Tokyo MedicalUniversity Hospital betweenJanuary 2005 and December2007 were assessed retro-spectively by using the pa-
tients’ medical records. Other types of alopeciawhich should be differentiated from AA, such asfemale-pattern hair loss, telogen effluvium, cicatri-cial alopecia, or trichotillomania9 were excluded.Written informed consent was obtained from all 1030patients. The study was conducted according to theDeclaration of Helsinki principles.The types of hair loss were classified as follows:(1) single (single patch of hair loss), (2) multiple(multiple patches of hair loss), (3) ophiasis (band-like hair loss in parieto-temporo-occipital area), (4)AT (extensive hair loss involving the entire scalp),and (5) AU (100% loss of scalp and body hair). Theseverity of hair loss on the first visit was assessed inaccordance with the Alopecia Areata InvestigationalAssessment Guideline criteria4: S0 (no hair loss),S1 (\25%), S2 (25%-49%), S3 (50%-74%), S4a(75%-95%), S4b (96%-99%), and S5 (100%) hairloss. Severity of hair loss was evaluated by macro-scopic observation of the amount of terminal hairsremaining on the scalp. The hair-pull test wasperformed not only around the patches of hair lossbut also over the entire scalp and judged positiveonly when hairs across the entire scalp were easilydetached. Patients with RPAA were defined as thosewith positive hair-pull test results across the entirescalp on the first visit regardless of hair loss areas, orthose with history of onset or rapid worsening of hairloss, resulting in extensive hair loss over the entirescalp, within 6 months prior to the first visit.Regenerated vellus hair was defined as vellus orintermediate hair shorter in length or smaller indiameter than terminal hair. Clumps of regeneratedvellus hairs in the hair loss areas were recorded on
the first visit. Patients’ family history was investigatedto the first or second degree of kinship for evidenceof AA. A previous history of AA was defined asprevious occurrences of hair loss not including thepresent instance. Themale-female ratio, age at onset,age at first visit, and duration as measured from thefirst episode of AA were also recorded. Any of the
following complications sup-posedly associated with AAand other forms of alopeciawere noted when they oc-curred: (1) atopic dermatitis,(2) atopic diseases includingatopic dermatitis, allergic rhi-nitis, allergic conjunctivitis,and asthma, (3) thyroid dis-ease, (4) iron deficiency ane-mia, (5) collagen disease,and (6) vitiligo.
Treatment modalities
Treatment for AAwas generally chosen accordingto clinical typology and severity, and the patient’swishes. AA patients were classified by the initialtreatment modalities at our clinic: (1) topical corti-costeroids alone (0.05% clobetasol propionate or0.05% betamethasone butyrate propionate); (2) in-tralesional corticosteroids (triamcinolone acetonide(10 mg/mL) alone every 4 to 6 weeks, or in combi-nation with topical corticosteroids); (3) oral cortico-steroids (oral prednisolone, alone or in combinationwith topical corticosteroids, mainly applied to RPAApatients or severe AA cases with extensive hair loss.Dosage of daily oral prednisolone ranged from 10 to30mg/day); (4) topical immunotherapy alone (eitherSADBE [squaric acid dibutylester] or DPCP [diphe-nylcyclopropenone] repeated once every 2 weeksafter sensitization). In this study, the effects of theinitial treatment modalities on the prognosis of AAwere compared. Treatment modalities were changedin some patients during the follow-up according tothe clinical manifestations and the patient’s wishes.
Assessment of prognosisThe patients were followed up for 24 months
or more at our clinic or by questionnaire.Questionnaires regarding the current status of hairloss were given only to RPAA patients to assess long-term prognosis. The extent of improvement wasmeasured by comparing the extent of hair loss asseen on the first visit and the final report. Thefollowing indices of prognosis were used: (1) im-provement (improvement in hair regrowth [25%based on the amount of terminal hair found acrossthe entire scalp [eg, improved from S3 to S1]);

J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Uchiyama et al 1165
(2) complete or temporary cure (no hair loss [S0] atleast at one time point during the follow-up period[eg, improved from S1 to S0]); and (3) relapse(recurrence of hair loss regardless of severity follow-ing a temporary cure [S0]).
Statistical evaluationStatistical analyses were performed by using SPSS
(version 17.0.2), with P \ .05 being statisticallysignificant for all results.
To identify prognostic factors, patient and treat-ment variables were analyzed by means of thechi-square test, Fisher’s exact probability, or m 3 nchi-square test. The variables with P\ .25 in theseanalyses were further analyzed as independent var-iables using multiple logistic regression analysis.Background characteristics on the first visit werealso compared using the chi-square test and Mann-Whitney U test.
RESULTSThe duration of the follow-up and the number of
patients assessed at each point in time are shown inFig 1, and the demographics of all 1030 AA patientsare shown in Table I. Comparison of backgroundcharacteristics between RPAA and non-RPAA groupson the first visit in all of the AA patients (n = 1030)and patients with severe AA (n = 145) is shown inTables II and III, respectively. Results of multivariateanalysis for the prognosis of all AA patients (n = 311),RPAA patients (n = 128) and severe AA patients with50% hair loss or greater (n = 60), followed up for 24months or longer, are shown in Tables IV, V, and VI,respectively. Only variables shown to be significant(P \ .05) in either the univariate or multivariateanalysis are shown in Tables IV, V, and VI.
As shown in Fig 1, the average (6 standarddeviation [SD]) duration of the follow-up atour clinic was 12.76 17.1 months, while the average(6 SD) duration of the follow-up including use ofquestionnaires was 15.4 6 17.1 months. Three hun-dred eleven patients (30.2%) were followed up for 24months or longer. Of all AA patients (n = 1030), 199(19.3%) had been diagnosed with RPAA, and 831patients (80.7%) had been diagnosed with non-RPAA, including single-type AA with mild hair lossand AU with severe hair loss. Among the 199 RPAApatients, the hair-pull test results on the first visitwere positive in 178 RPAA patients. Twenty-oneRPAA patients showed negative results on the firstvisit but reported onset or rapid worsening of hairloss across the entire scalp within 6 months. Of the199 RPAA patients, 100 (50.3%) were also assessedfor final severity using questionnaires. Twenty-ninepatients in the RPAA group and 116 patients in the
non-RPAA group presented severe AA with 50% hairloss or greater (S4 - S5) on the first visit (Fig 1).
As shown in Table I, age at onset of AA and at thefirst visit ranged from infancy to the eighties. Onset ofAA (average age 6 SD, 30.6 6 16.5 years) wasobserved most frequently in both males and femalesin their twenties. At the first visit, most males were intheir thirties and most females were in their twenties(average age 6 SD, 35.4 6 14.9 years). Average(6 SD) duration from the first episode of AA was59.5 6 97.0 months. The multiple type of hair losswith 4 areas of hair loss or more was the mostcommon. With respect to severity, S1 (\25%),followed by S2 (25%-49%), was most common.Regenerated vellus hairs were observed in 624 of878 patients (71.1%) on the first visit. Fifty-threepatients (5.1%) had a family history of AA, and 296patients (28.7%) reported a previous occurrence ofAA. With regard to complications, 209 patients(20.3%) had atopic dermatitis, 411 (39.9%) hadsome form of atopic disease, 35 (3.4%) had a formof thyroid disease, 35 (3.4%) had iron deficiencyanemia, 7 (0.7%) had some form of collagen disease,and 6 (0.6%) had vitiligo. With respect to the initialtreatment modalities at our clinic, 412 patients(40.0%) were treated with topical corticosteroidsalone, 246 (23.9%) with intralesional corticosteroids,86 (8.3%) with oral prednisolone, and 210 (20.4%)with topical immunotherapy alone.
In our study, 194 patients (18.8%) of all of the AApatients (n = 1030) showed a complete or temporarycure within 1 year during the follow-up. On the otherhand, 37 patients (11.9%) followed up for 24 monthsor longer (n = 311) remained unchanged or pro-gressed to severe hair loss (S4-S5) as their final status(data not shown).
The results of multivariate analysis for the prog-nosis of all AA patients (n = 311) are shown in TableIV. The prognostic factors are given below with theindices for evaluating the prognosis: regeneratedvellus hairs indicated a significantly higher rate ofimprovement (odds ratio [OR] = 2.71; 95% confidenceinterval [CI] = 1.35-5.43;P= .005) and cure (OR = 3.46;95% CI = 1.86-6.43; P \ .001); the long diseaseduration group ($ 6 months) showed a significantlyhigher rate of relapse (OR = 0.37; 95% CI = 0.14-0.94;P = .036); RPAA showed a significantly higher im-provement (OR = 5.81; 95% CI = 2.87-11.77; P\.001)and cure rate (OR = 4.90; 95%CI = 2.82-8.52;P\.001)and lower relapse rate (OR = 0.37; 95%CI = 0.15-0.95;P = .039); the early-onset group (\16 years of age)had a significantly lower cure rate (OR = 3.45; 95%CI = 1.52-7.81; P = .003); among initial treatmentmodalities, the topical corticosteroid monotherapygroup had a significantly lower improvement rate
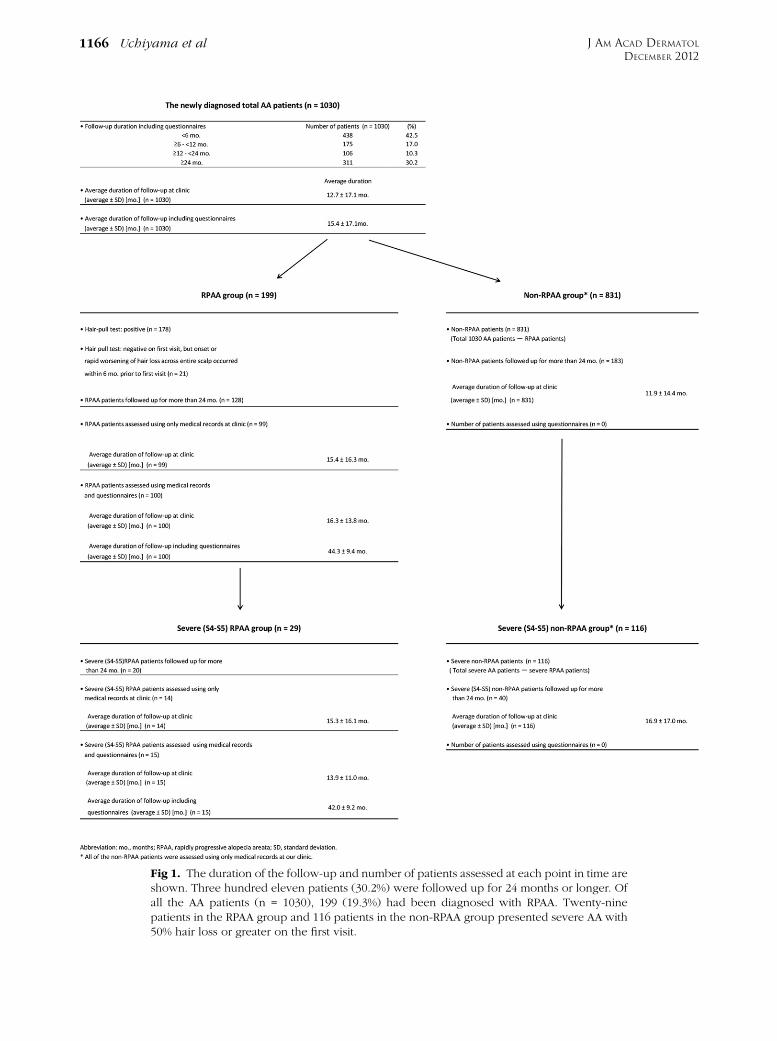
Fig 1. The duration of the follow-up and number of patients assessed at each point in time areshown. Three hundred eleven patients (30.2%) were followed up for 24 months or longer. Ofall the AA patients (n = 1030), 199 (19.3%) had been diagnosed with RPAA. Twenty-ninepatients in the RPAA group and 116 patients in the non-RPAA group presented severe AA with50% hair loss or greater on the first visit.
J AM ACAD DERMATOL
DECEMBER 20121166 Uchiyama et al

Table I. Demographics of 1030 patients with AA
Characteristics Average 6 SD (Range) Median
No. of patients
All patients (N = 1030) %
Age at onset of AA (years)Total 30.6 6 16.5 (0-84) 29.0Male 30.0 6 15.8 (0-75) 29.0Female 31.1 6 16.9 (0-84) 29.0
Age at first visit (years)Total 35.4 6 14.9 (0-89) 33.0Male 34.6 6 13.8 (1-75) 33.0Female 36.0 6 15.6 (0-89) 34.0
Duration from first episode of AA(months)
Total 59.5 6 97.0 (0.5 mo-50 yr) 7.0Male 57.7 6 92.2 (0.5 mo-50 yr) 8.0Female 60.7 6 100.1 (0.5 mo-50 yr) 6.0
Gender: male; female; (male-femaleratio)
411; 619 (1:1.5) —
Type of hair lossSingle 199 19.3Multiple (\4 patches) 91 8.8Multiple ($ 4 patches) 380 36.9Ophiasis 95 9.2Totalis (AT) 169 16.4Universalis (AU) 96 9.3
Severity (extent of hair loss)S1 (\25%) 630 61.2S2 (25%-49%) 174 16.9S3 (50%-74%) 81 7.9S4a (75%-95%) 67 6.5S4b (96%-99%) 17 1.7S5 (100%) 61 5.9
Regenerated vellus hairs 624* 71.1Family history of AA (1) 53 5.1Previous history of AA (1) 296 28.7Complications or past historiesAtopic dermatitis (1) 209 20.3Atopic diseases (1)y 411 39.9Thyroid diseases (1) 35 3.4Iron deficiency anemia (1) 35 3.4Collagen diseases (1) 7 0.7Vitiligo (1) 6 0.6
Initial treatments at our clinicTopical corticosteroids alone 412 40.0Intralesional corticosteroids 246 23.9Oral prednisolone 86 8.3Topical immunotherapy alone 210 20.4
AA, Alopecia areata; AT, alopecia totalis; AU, alopecia universalis; mo, months; yr, years; SD, standard deviation.
*Total number: 878.yAtopic diseases include atopic dermatitis, allergic rhinitis, allergic conjunctivitis, and asthma.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Uchiyama et al 1167
(OR = 0.32; 95% CI = 0.13-0.79; P = .014). There wasno statistically significant difference in the cure andrelapse rates among the initial treatment modalities,as shown by multivariate analysis.
The results of the comparison of the backgroundcharacteristics of the RPAA (n = 199) and non-RPAA(n = 831) groups obtained on the first visit are shown
in Table II, and the results of the multivariate analysisfor the prognosis of RPAA patients (n = 128) areshown in Table V. Duration from the first episode ofAA was significantly shorter in the RPAA group thanin the non-RPAA group (P\ .0001). The proportionof patients with greater than 50% hair loss wassignificantly lower in the RPAA group than in the
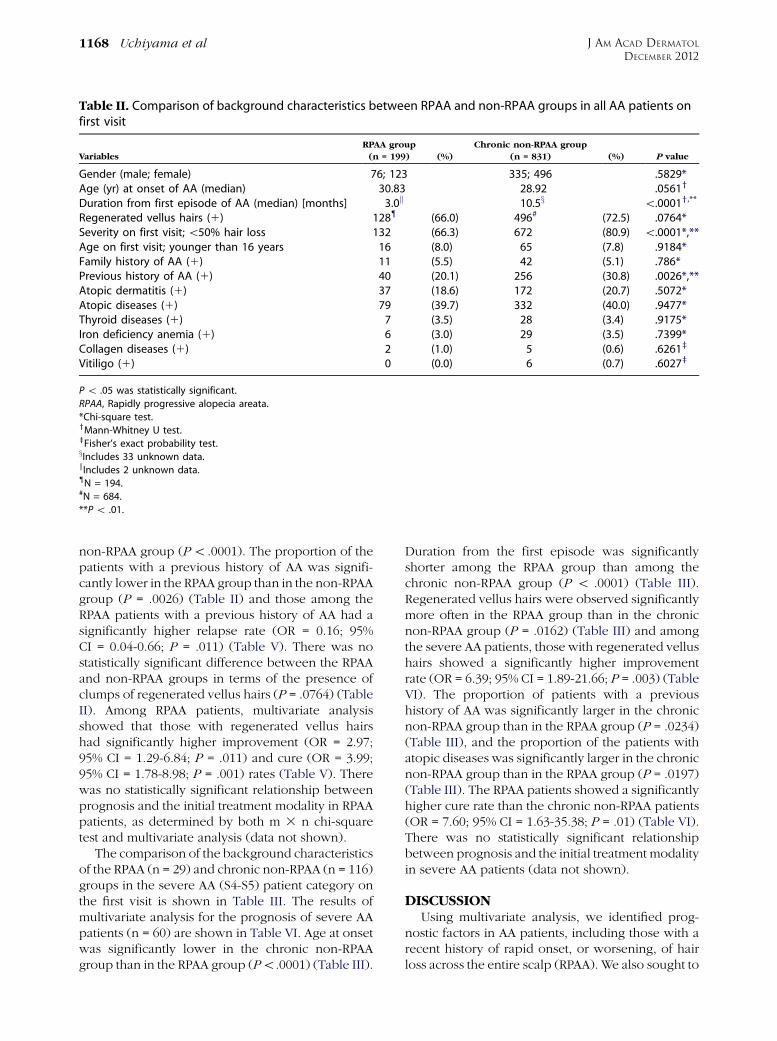
Table II. Comparison of background characteristics between RPAA and non-RPAA groups in all AA patients onfirst visit
Variables
RPAA group
(n = 199) (%)
Chronic non-RPAA group
(n = 831) (%) P value
Gender (male; female) 76; 123 335; 496 .5829*Age (yr) at onset of AA (median) 30.83 28.92 .0561y
Duration from first episode of AA (median) [months] 3.0k 10.5x \.0001y,**
Regenerated vellus hairs (1) 128{ (66.0) 496# (72.5) .0764*Severity on first visit;\50% hair loss 132 (66.3) 672 (80.9) \.0001*,**Age on first visit; younger than 16 years 16 (8.0) 65 (7.8) .9184*Family history of AA (1) 11 (5.5) 42 (5.1) .786*Previous history of AA (1) 40 (20.1) 256 (30.8) .0026*,**Atopic dermatitis (1) 37 (18.6) 172 (20.7) .5072*Atopic diseases (1) 79 (39.7) 332 (40.0) .9477*Thyroid diseases (1) 7 (3.5) 28 (3.4) .9175*Iron deficiency anemia (1) 6 (3.0) 29 (3.5) .7399*Collagen diseases (1) 2 (1.0) 5 (0.6) .6261z
Vitiligo (1) 0 (0.0) 6 (0.7) .6027z
P\ .05 was statistically significant.
RPAA, Rapidly progressive alopecia areata.
*Chi-square test.yMann-Whitney U test.zFisher’s exact probability test.xIncludes 33 unknown data.kIncludes 2 unknown data.{N = 194.#N = 684.
**P\ .01.
J AM ACAD DERMATOL
DECEMBER 20121168 Uchiyama et al
non-RPAA group (P\ .0001). The proportion of thepatients with a previous history of AA was signifi-cantly lower in the RPAA group than in the non-RPAAgroup (P = .0026) (Table II) and those among theRPAA patients with a previous history of AA had asignificantly higher relapse rate (OR = 0.16; 95%CI = 0.04-0.66; P = .011) (Table V). There was nostatistically significant difference between the RPAAand non-RPAA groups in terms of the presence ofclumps of regenerated vellus hairs (P = .0764) (TableII). Among RPAA patients, multivariate analysisshowed that those with regenerated vellus hairshad significantly higher improvement (OR = 2.97;95% CI = 1.29-6.84; P = .011) and cure (OR = 3.99;95% CI = 1.78-8.98; P = .001) rates (Table V). Therewas no statistically significant relationship betweenprognosis and the initial treatment modality in RPAApatients, as determined by both m 3 n chi-squaretest and multivariate analysis (data not shown).
The comparison of the background characteristicsof the RPAA (n = 29) and chronic non-RPAA (n = 116)groups in the severe AA (S4-S5) patient category onthe first visit is shown in Table III. The results ofmultivariate analysis for the prognosis of severe AApatients (n = 60) are shown in Table VI. Age at onsetwas significantly lower in the chronic non-RPAAgroup than in the RPAA group (P\.0001) (Table III).
Duration from the first episode was significantlyshorter among the RPAA group than among thechronic non-RPAA group (P \ .0001) (Table III).Regenerated vellus hairs were observed significantlymore often in the RPAA group than in the chronicnon-RPAA group (P = .0162) (Table III) and amongthe severe AA patients, those with regenerated vellushairs showed a significantly higher improvementrate (OR = 6.39; 95% CI = 1.89-21.66; P = .003) (TableVI). The proportion of patients with a previoushistory of AA was significantly larger in the chronicnon-RPAA group than in the RPAA group (P = .0234)(Table III), and the proportion of the patients withatopic diseases was significantly larger in the chronicnon-RPAA group than in the RPAA group (P = .0197)(Table III). The RPAA patients showed a significantlyhigher cure rate than the chronic non-RPAA patients(OR = 7.60; 95% CI = 1.63-35.38; P = .01) (Table VI).There was no statistically significant relationshipbetween prognosis and the initial treatment modalityin severe AA patients (data not shown).
DISCUSSIONUsing multivariate analysis, we identified prog-
nostic factors in AA patients, including those with arecent history of rapid onset, or worsening, of hairloss across the entire scalp (RPAA). We also sought to

Table III. Comparison of background characteristics between RPAA and chronic non-RPAA groups in patientswith severe AA (S4-S5) on first visit
RPAA group
(n = 29) (%)
Chronic non-RPAA group
(n = 116) (%) P value
Gender (male; female) 13; 16 54; 62 (n = 116) .8677*Age at onset of AA (median) [years] 35.75 16.21 (n = 116) \.0001y,z
Duration from first episode of AA (median) [months] 3k 108{ \.0001y,z
Regenerated vellus hairs (1) 18 (62.1) 39# (37.1) .0162*,**Age on first visit; younger than 16 years 2 (6.9) 12 (10.3) .7364x
Family history of AA (1) 3 (10.3) 6 (5.2) .3837x
Previous history of AA (1) 7 (24.1) 55 (47.4) .0234*,**Atopic dermatitis (1) 6 (20.7) 45 (38.8) .0678*Atopic diseaseyy (1) 10 (34.5) 68 (58.6) .0197*,**Thyroid disease (1) 2 (6.9) 7 (6.0) [.99x
Iron deficiency anemia (1) 2 (6.9) 4 (3.4) .3446x
Collagen disease (1) 0 (0.0) 0 (0.0) —Vitiligo (1) 0 (0.0) 1 (0.9) [.99x
1, Positive.
*Chi-square test.yMann-Whitney U test.zP\ .01.xFisher’s exact probability test.kIncludes one unknown datum.{Includes one unknown datum.#N = 105.
**P\ .05.yyAtopic disease includes atopic dermatitis, allergic rhinitis, allergic conjunctivitis, and asthma.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Uchiyama et al 1169
clarify the features of RPAA by comparing the back-ground characteristics and prognosis of RPAA withthose of non-RPAA or severe, chronic AA patients.RPAA patients tended to show a good prognosisregardless of treatment modality or the severity onthe first visit. Early-onset and long disease durationwere significantly associated with a poor prognosisin all AA patients, whereas a previous history of AAwas significantly associated with a poor prognosis inRPAA patients. Furthermore, regenerated vellus hairswere a good prognostic factor regardless of the typeor severity of AA, including RPAA.
Concerning the correlation between the severityof the initially observed hair loss and prognosis,previous reports have indicated that mild AA showedcomplete resolutionmore often than severe AA,6 andspontaneous remission within 1 year occurred in80% of patients who presented only a few areas ofhair loss,10 suggesting that the type and extent of hairloss initially observed are important prognostic fac-tors. However, our study showed that RPAA tends tohave a favorable prognosis regardless of the extent ofhair loss on the first visit, suggesting that the severehair loss seen on the first visit may be a factorassociated with a poor prognosis among AA patientsin general, but possibly not among RPAA patients.
Other indicators reportedly associatedwith a poorprognosis include onychodystrophy,5 atopy,11,12
autoimmune diseases,11,13 early onset,5,6,14 andlong disease duration.10,15 Our study, as well asprevious reports, demonstrated that early onset wasassociated with a significantly lower cure rate, andlong disease duration was associated with a signifi-cantly higher risk of relapse among all AA patients. Aprevious history of AA is an indicator of recurrence ofhair loss and may be particularly associated with ahigher risk of relapse among RPAA patients. In ourstudy, complication by, or a history of, atopicdiseases was noted significantly more often inchronic non-RPAA patients with severe hair lossthan in RPAA patients with severe hair loss.
Regenerated vellus hairs observed macroscopi-cally or dermoscopically in hair loss areas were alsoexamined. Inui et al reported that short vellus hairsobserved dermoscopically constitute a diagnosticmarker for AA and are negatively correlated withdisease activity and severity in AA patients.16 Theseregenerated vellus hairs indicate the possibility ofnormal hair regrowth, although not all vellus hairseventually mature into terminal hairs. Our resultssuggest that regenerated vellus hairs initially ob-served on hair loss areas are associated with a goodprognosis regardless of the type or severity of AAassessed on the first visit. Significantly, the presenceof regenerated vellus hairs on the first visit tended toshow a good prognosis even in severe cases of AA,

Table IV. Multivariate analysis for prognosis in patients with all forms of AA
Variables Rate %
Chi-square test
P value OR 95% CI P value
ImprovementRegenerated vellus hairsPositive 56/190 29.5 .0369* 2.71 1.35-5.43 .005y
Negativez 18/99 18.2Duration from first episode of AAShorter than 6 months 44/131 33.6 .0017y — — —6 months or longerz 31/173 17.9
RPAA/non-RPAARPAA 54/128 42.2 \.0001y 5.81 2.87-11.77 \.001y
Non-RPAAz 21/183 11.5Initial treatmentsTopical corticosteroids alone 10/73 13.7 \.0001y,x 0.32 0.13-0.79 .014*Intralesional corticosteroids 10/78 12.8 — — —Oral prednisolone 22/52 42.3 — — —Topical immunotherapy alonez 33/104 31.7 — — —
Complete or temporary cureRegenerated vellus hairsPositive 96/190 50.5 \.0001y 3.46 1.86-6.43 \.001y
Negativez 22/99 22.2Duration from first episode of AAShorter than 6 months 74/131 56.5 \.0001y — — —6 months or longerz 45/173 26.0 — — —
RPAA/non-RPAARPAA 79/128 61.7 \.0001y 4.90 2.82-8.52 \.001y
Non-RPAAz 43/183 23.5Severity on first visitS1-S3 110/251 43.8 \.0007y 2.02 0.90-4.51 .088S4-S5z 12/60 20.0
Age on first visitYounger than 6 yearsz 6/25 24.0 \.0007y — — —16 years or older 116/286 40.6
Age at onsetYounger than 6 yearsz 11/63 17.5 \.0001y 3.45 1.52-7.81 .003y
16 years or older 111/248 44.8Previous history of AAYesx 20/85 23.5 \.0005y — — —No 102/226 45.1
Initial treatmentsTopical corticosteroids alone 32/73 43.8 \.00053y,x — — —Intralesional corticosteroids 30/78 38.5 — — —Oral prednisolone 30/52 57.7 — — —Topical immunotherapy alonez 30/104 28.8 — — —
RelapseDuration from first episode of AAShorter than 6 months 10/74 13.5 .0101* .37 0.14-0.94 .036*6 months or longerz 15/45 33.3
RPAA/non-RPAARPAA 11/79 13.9 .0069y .37 0.15-0.95 .039*Non-RPAAz 15/43 34.9
Patient and treatment variables were analyzed by using chi-square test, Fisher’s exact probability test, or m 3 n chi-square test. Variables
with P\ .25 in these analyses were also analyzed using a multiple logistic regression analysis. Only significant variables (P\ .05) in either of
these analyses are shown.
*P\ .05.yP\ .01.zRepresents reference value (odds ratio [OR] 1.00). ORs are indicated against the reference values.xm 3 n chi-square test.
J AM ACAD DERMATOL
DECEMBER 20121170 Uchiyama et al
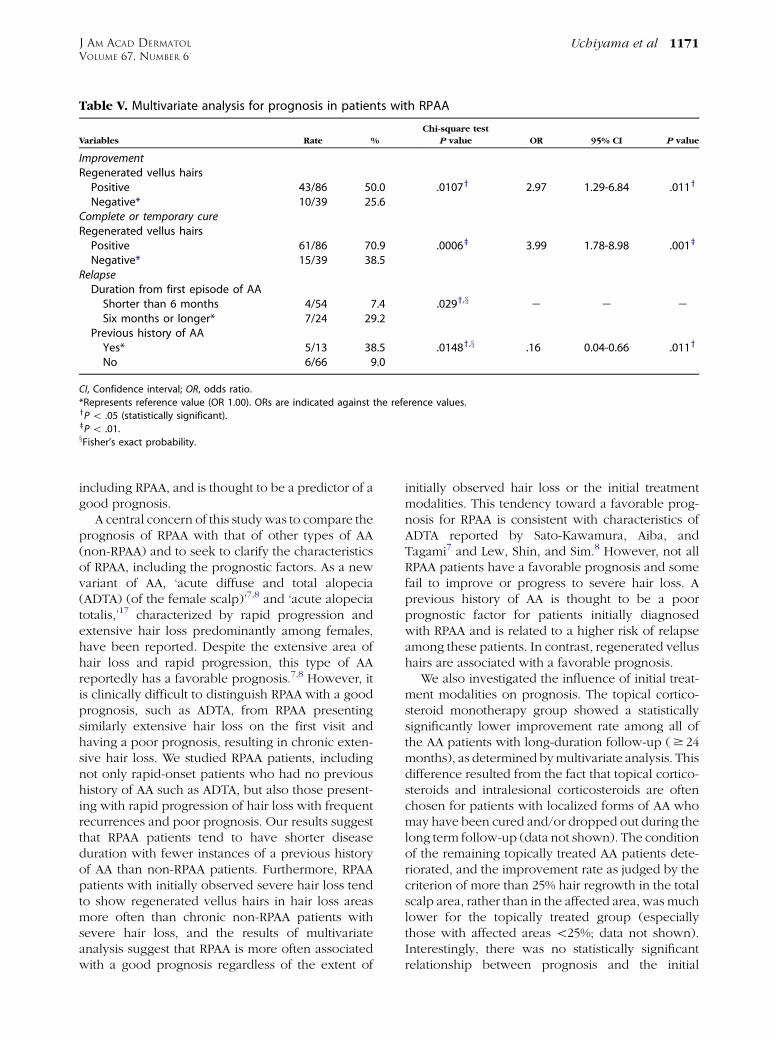
Table V. Multivariate analysis for prognosis in patients with RPAA
Variables Rate %
Chi-square test
P value OR 95% CI P value
ImprovementRegenerated vellus hairsPositive 43/86 50.0 .0107y 2.97 1.29-6.84 .011y
Negative* 10/39 25.6Complete or temporary cureRegenerated vellus hairsPositive 61/86 70.9 .0006z 3.99 1.78-8.98 .001z
Negative* 15/39 38.5RelapseDuration from first episode of AAShorter than 6 months 4/54 7.4 .029y,x e e eSix months or longer* 7/24 29.2
Previous history of AAYes* 5/13 38.5 .0148y,x .16 0.04-0.66 .011y
No 6/66 9.0
CI, Confidence interval; OR, odds ratio.
*Represents reference value (OR 1.00). ORs are indicated against the reference values.yP\ .05 (statistically significant).zP\ .01.xFisher’s exact probability.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Uchiyama et al 1171
including RPAA, and is thought to be a predictor of agood prognosis.
A central concern of this study was to compare theprognosis of RPAA with that of other types of AA(non-RPAA) and to seek to clarify the characteristicsof RPAA, including the prognostic factors. As a newvariant of AA, ‘acute diffuse and total alopecia(ADTA) (of the female scalp)’7,8 and ‘acute alopeciatotalis,’17 characterized by rapid progression andextensive hair loss predominantly among females,have been reported. Despite the extensive area ofhair loss and rapid progression, this type of AAreportedly has a favorable prognosis.7,8 However, itis clinically difficult to distinguish RPAA with a goodprognosis, such as ADTA, from RPAA presentingsimilarly extensive hair loss on the first visit andhaving a poor prognosis, resulting in chronic exten-sive hair loss. We studied RPAA patients, includingnot only rapid-onset patients who had no previoushistory of AA such as ADTA, but also those present-ing with rapid progression of hair loss with frequentrecurrences and poor prognosis. Our results suggestthat RPAA patients tend to have shorter diseaseduration with fewer instances of a previous historyof AA than non-RPAA patients. Furthermore, RPAApatients with initially observed severe hair loss tendto show regenerated vellus hairs in hair loss areasmore often than chronic non-RPAA patients withsevere hair loss, and the results of multivariateanalysis suggest that RPAA is more often associatedwith a good prognosis regardless of the extent of
initially observed hair loss or the initial treatmentmodalities. This tendency toward a favorable prog-nosis for RPAA is consistent with characteristics ofADTA reported by Sato-Kawamura, Aiba, andTagami7 and Lew, Shin, and Sim.8 However, not allRPAA patients have a favorable prognosis and somefail to improve or progress to severe hair loss. Aprevious history of AA is thought to be a poorprognostic factor for patients initially diagnosedwith RPAA and is related to a higher risk of relapseamong these patients. In contrast, regenerated vellushairs are associated with a favorable prognosis.
We also investigated the influence of initial treat-ment modalities on prognosis. The topical cortico-steroid monotherapy group showed a statisticallysignificantly lower improvement rate among all ofthe AA patients with long-duration follow-up ($ 24months), as determined bymultivariate analysis. Thisdifference resulted from the fact that topical cortico-steroids and intralesional corticosteroids are oftenchosen for patients with localized forms of AA whomay have been cured and/or dropped out during thelong term follow-up (data not shown). The conditionof the remaining topically treated AA patients dete-riorated, and the improvement rate as judged by thecriterion of more than 25% hair regrowth in the totalscalp area, rather than in the affected area, was muchlower for the topically treated group (especiallythose with affected areas \25%; data not shown).Interestingly, there was no statistically significantrelationship between prognosis and the initial

Table VI. Multivariate analysis for prognosis in patients with severe (S4-S5) AA
Variables Rate %
Chi-square test
P value OR 95% CI P value
ImprovementRegenerated vellus hairsPositive 16/25 64.0 .0054y 1.89-21.66 .003y
Negative* 8/30 26.7Duration from first episode of AAShorter than 6 months 9/14 64.3 .0341z — — —6 months or longer* 15/46 32.6
Atopic dermatitisPositive* 5/23 21.7 .0228z — — —Negative 19/37 51.4
Complete or temporary cureDuration from first episode of AAShorter than 6 months 7/14 50.0 .0337z — — —6 months or longer* 5/46 10.9
RPAA/Chronic non-RPAARPAA 9/20 45.0 .0013y,x 7.60 1.63-35.38 .01z
Chronic non-RPAA* 3/40 7.5Age at onsetYounger than 6 years* 1/21 4.8 .0304z — — —16 years of age or older 11/39 28.2
Previous history of AAYes* 1/23 4.3 .0169z 7.96 0.87-72.85 .066No 11/37 29.7
Relapse— — — — — — —
P\ .05 was statistically significant.
Variables with P \ .25 by chi-square test and Fisher’s exact probability were analyzed using a multiple logistic regression analysis. Only
significant variables (P\ .05) were shown.
CI, Confidence interval; OR, odds ratio; RPAA, rapidly progressive alopecia areata.
*Represents reference value (OR 1.00). ORs are indicated against the reference values.yP\ .01.zP\ .05.xFisher’s exact probability.
J AM ACAD DERMATOL
DECEMBER 20121172 Uchiyama et al
treatment modalities on the first visit in RPAA patientsand severe AA patients with a long-duration follow-up. A number of therapeutic agents have beendescribed for the treatment of AA, but none arecurative or preventive.18,19 Our study suggested thatthere was no statistically significant influence of theinitial treatment modalities on the prognosis of AApatients with severe hair loss including both RPAAand chronic persistent AA, although the limitations ofthe retrospective study should be considered. Recentstudies have demonstrated that AA is associated withautoimmunity.1,11,20,21 However, RPAA patients tendto have a favorable prognosis, and the pathogenesisof curable RPAA is thought to be less associated withthe autoimmune system than chronic forms of AA.RPAA is thought to include both the rapidly pro-gressing, recurrent, persistent form associated withautoimmune activity and the rapidly progressing butcurable form, which is less so. Our study suggeststhat regenerated vellus hairs and a previous history of
AA can aid in predicting prognosis among RPAApatients.
Some of the limitations of the study protocolshould be borne in mind: tracking by questionnaireswas performed only for RPAA patients, the durationof the follow-up was different depending on thecases, and the cure and relapse rates of only thepatients followed up for 24 months or more wereassessed.
Furthermore, our choice of initial treatment mo-dalities was not randomized, therefore admitting thepossibility of severity bias, and treatment modalitieswere changed in some patients during the follow-upperiod.
REFERENCES
1. Price VH. Therapy of alopecia areata: On the cusp and in the
future. J Investig Dermatol Symp Proc 2003;8:207-11.
2. Safavi KH, Muller SA, Suman VJ, Moshell AN, Melton LJ.
Incidence of alopecia areata in Olmsted County, Minnesota,
1975 through 1989. Mayo Clin Proc 1995;70:628-33.

J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Uchiyama et al 1173
3. Alkhalifah A, Alsantali A, Wang E, McElwee KJ, Shapiro J.
Alopecia areata update: Part I: Clinical picture, histopathology,
and pathogenesis. J Am Acad Dermatol 2010;62:177-88.
4. Olsen EA, Hordinsky MK, Price VH, Roberts JL, Shapiro J,
Canfield D, et al. Alopecia areata investigational assess-
ment guideline Part II. J Am Acad Dermatol 2004;51:
440-7.
5. De Waard-Van der Spek FB, Oranje AP, De Raeymaecker DM,
Peereboom-Wynia JDR. Juvenile versusmaturity-onset alopecia
areata: Comparative retrospective clinical study. Clin Exp
Dermatol 1989;14:429-33.
6. Tosti A, Bellavista S, Iorizzo M. Alopecia areata: A long term
follow-up study of 191 patients. J Am Acad Dermatol 2006;55:
438-41.
7. Sato-Kawamura M, Aiba S, Tagami H. Acute diffuse and total
alopecia of the female scalp. A new subtype of diffuse
alopecia areata that has a favorable prognosis. Dermatology
2002;205:367-73.
8. Lew BL, Shin MK, Sim WY. Acute diffuse and total alopecia: A
new subtype of alopecia areata with a favorable prognosis.
J Am Acad Dermatol 2009;60:85-93.
9. Shapiro J. Hair loss in women. N Engl J Med 2007;357:1620-30.
10. Ikeda T. A new classification of alopecia areata. Dermatologica
1965;131:421-45.
11. Barahmani N, Schabath MB, Duvic M. History of atopy or
autoimmunity increases risk of alopecia areata. J Am Acad
Dermatol 2009;61:581-91.
12. Hordinsky M, Ericson M. Autoimmunity: Alopecia areata.
J Investig Dermatol Symp Proc 2004;9:73-8.
13. Chu SY, Chen YJ, Tseng WC, Lin MW, Chen TJ, Hwang CY, et al.
Comorbidity profiles among patients with alopecia areata: The
importance of onset age, a nationwide population-based
study. J Am Acad Dermatol 2011;65:949-56.
14. Yang S, Yang J, Liu JB, Wang HY, Yang Q, Gao M, et al. The
genetic epidemiology of alopecia areata in China. Br J
Dermatol 2004;151:16-23.
15. NakajimaT, Inui S, ItamiS.Pulse corticosteroid therapy for alopecia
areata: Study of 139 patients. Dermatology 2007;215:320-4.
16. Inui S, Nakajima T, Nakagawa K, Itami S. Clinical significance of
dermoscopy in alopecia areata: Analysis of 300 cases. Int J
Dermatol 2008;47:688-93.
17. Choi HJ, Ihm CW. Acute alopecia totalis. Acta Dermatovenerol
Alp Panonica Adriat 2006;15:27-34.
18. MacDonald Hull SP, Wood ML, Hutchinson PE, Sladden M,
Messenger AG. Guidelines for the management of alopecia
areata. Br J Dermatol 2003;149:692-9.
19. Madani S, Shapiro J. Alopecia areata update. J Am Acad
Dermatol 2000;42:549-66.
20. Gilhar A, Ullmann Y, Berkutzki T, Assy B, Kalish RS. Autoimmune
hair loss (alopecia areata) transferred by T lymphocytes to
human scalp explants on SCIDmice. J Clin Invest 1998;101:62-7.
21. McElwee KJ, Tobin DJ, Bystryn JC, King LE Jr, Sundberg JP.
Alopecia areata: An autoimmune disease? Exp Dermatol 1999;
8:371-9.