multivisceral resection in colorectal carcinoma
TRANSCRIPT

Multivisceral en-bloc resection and metastasectomy for colorectal malignancy
Happykumar Kagathara, Shailendra Lalwani, Vivek Mangla, Naimish Mehta,
Amitabh Yadav, Samiran Nundy
Department of Surgical Gastroenterology and Liver Transplantation
Sir Ganga Ram Hospital, New Delhi

Background
• Long term survival in primary and recurrent colorectal tumors– Complete resection of all macroscopic disease
• The decision to embark on an extensive operation– Multivisceral en-bloc organ resection and metastasectomy
– Weigh the risks against the potential benefits of such procedures

Aim
• Evaluation of outcomes from complete extirpative operations in selected patients with locally advanced and advanced colorectal cancers
• Outcome measures– Survival
– Surgery related complications

Patients and Methods
• Retrospective study from prospectively maintained database
Colorectal carcinoma(n= 675 patients)
Conventional curative resectionn= 604 patients
Extended resectionn= 35 patients
Multivisceral en-bloc resectionn= 19 patients
Metastasectomyn= 8 patients
MVR + Metastasectomyn= 8 patients
Study cohort
August, 1996 to December, 2012

• Common symptoms– Abdominal pain, weight loss, bleeding P/R,
constipation, anorexia, diarrhoea
• Rare presentation– P/V discharge, lump, fever, anaemia, vomitting
• Preoperative evaluation of tumor– CEA level, Colonoscopy, CT scan
– PET-CT scan in selected group of patients presented with recurrence or metastasis

• Clinicopathological analysis, operative findings– Hospital records
• Follow up information– Out patient visit
– Telephonic survey
• Kaplan-Meier analysis for survival

Results
• Age : 53 ± 13.6 yrs
• M:F: 1 : 1.1
• BMI: 23.2 ± 5
• Recurrent tumor – 6 pts (17.6%)– Surgery – 6 pts
– Chemotherapy – 4 pts
– Radiotherapy – 1 pts
• Length of stay: 10 ± 5.5 days
• Follow up: 53%– 15 ± 9.4 months (7 – 48 months)
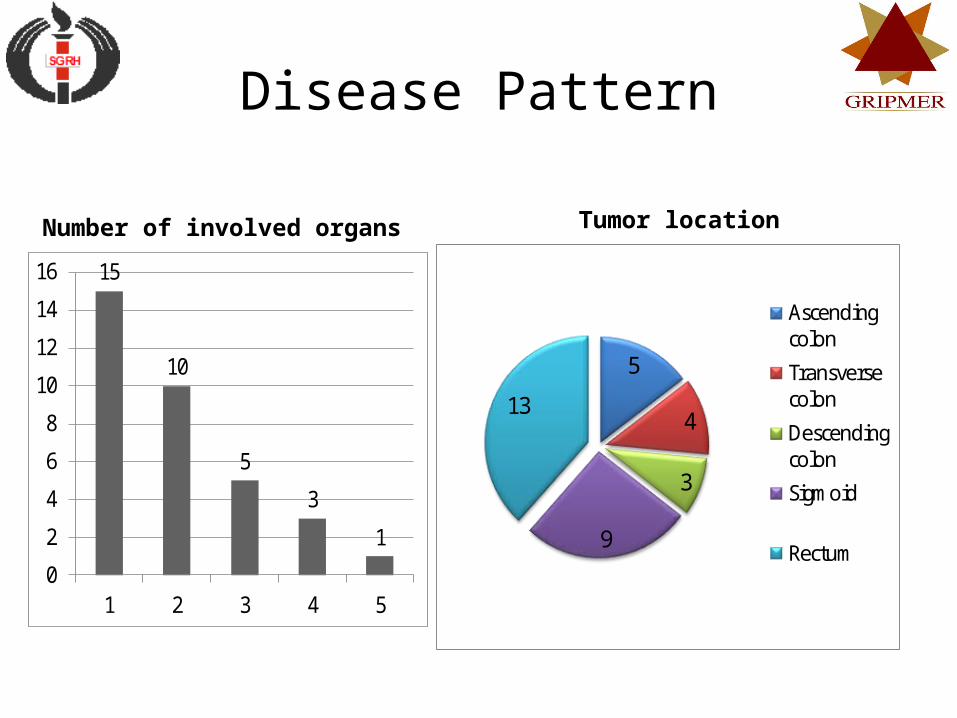
Disease Pattern
15
10
5
3
1
0
2
4
6
8
10
12
14
16
1 2 3 4 5
Number of involved organs
5
4
3
9
13
Ascending colon
Transverse colon
Descending colon
Sigmoid
Rectum
Tumor location

Organ Involvement
Organ involvement by local invasion
Pancreas 7 (27%)
Uterus 6 (23%)
Urinary bladder 5 (19%)
Small bowel 5 (19%)
Spleen 3 (11%)
Ureter 3 (11%)
Duodenum 3 (11%)
Vagina 3 (11%)
Ovary 3 (11%)
Liver 2 (7.6%)
Stomach 1 (3.8%)
Kidney 1 (3.8%)
Omentum 1 (3.8%)
Organ involvement by distant metastasis
Liver 10 (67%)
Peritoneum 5 (33%)
Omentum 3 (20%)
Small bowel 2 (13%)
Stomach 1 (6.6%)
Diaphragm 1 (6.6%)

Histology
• Adenocarcinoma – 68%
• Microscopic tumor infiltration (pT4) – 44%– Stage I and II: 50%
– Stage III: 17%
– Stage IV: 32%
• Positive lymph nodes – Mean – 2
– Median – 0 (0-29)
• Lymphovascular permeation – 9 (26%)

Postoperative Outcome
• Morbidity– Overall incidence – 60%
– Complications treated with intervention – 31.2% (n=13)• Anastomotic leaks – 14.2% (n=3)
• In hospital mortality: 0%
• Recurrence rate: 25.7%

Survival
• Overall 2-year survival rate: 80%
Literature Review
• Actual pathological infiltration - 50-85%Sokmen S, Terzi C et al. Int J Colorectal Dis 1999;14:282-5
• Complications after a multivisceral resection and metastasectomy
– 11% to 44%Nakafusa Y, Tanaka T et al. Rectum 2004;47:2055– 63
• Mortality – 0-7.5%Lehnert T, Methner M et al. Ann Surg 2002;235:217–25
Kruschewski M, Pohlen U et al. Zentralbl Chir 2006;131:217–22
• Overall 5-year survival rate – 51-53%Gebhardt C, Meyer W et al Langenbecks Arch Surg 384(2): 194-199, 1999

Conclusion
• Multivisceral en-bloc resection and metastasectomy in advanced colorectal carcinoma– Safe procedure
– May achieve 2-year survival rate up to 80%