nbs manual 28-6-2015
TRANSCRIPT

Newborn Screening Manual
� of �1 86
Newborn
Screening
Manual
A GUIDE FOR NEWBORN CARE PROVIDERS EDITION: 1 2015

Newborn Screening Manual
� of �2 86
Newborn Screening Manual:
A Guide for Newborn Care Providers
This manual was created by Kuwait National Newborn Screening Committee (KNNSC) as a comprehensive guide for newborn screening offices (NSO) and other health care providers to ensure that all infants born in Kuwait have a high quality newborn screen completed. This manual outlines recommended practices in newborn screening, along with common problems encountered in practical settings.
This manual is available free of charge to governmental and private hospitals that submit newborn screening samples to NSO. Revised or additional pages of the manual will be distributed periodically to ensure that the information contained is consistent with current practices.
If you have any questions about the information contained in this manual, or would like to order additional copies for your hospital, please e-mail [email protected] .

Newborn Screening Manual
� of �3 86
Table of contents
Background information
Introduction
Newborn screening history
Newborn screening system
Newborn screening timeline
Limitation of newborn screening
Scope on parts of screening program
Role of the screening team
Specimen collection Definition
Ensuring that the screen performed
Parental right for refusal
Time for specimens collection
Special consideration in sample collection
Recommendation for neonate in ICU
Specimens handling after collection
Transportation guidline for DBS
Unsatisfactory specimens
Identification of unsatisfactory specimens
Causes of unsatisfactory specimens
Privacy and confidentiality
Privacy and confidentiality health information
Storage of the dried blood spot samples
Use of dried blood spot samples
Destruction of the dried blood spot sample
Specific information
Overview of NSO process
Screening methodology
Factor causing of false positive and false negative
Special consideration that affect results of screen
Outline of 22 disorders included in the panel

Newborn Screening Manual
� of �4 86
Table of contents
Appendices Filter paper for dried –blood spot specimens APP1 Algorithm for Decreased
BIOTINIDASE APP20
Referral form for early discharged babies APP2 Algorithm for elevated C3
NBS report form for Tandem MS/MS APP3 Algorithm for elevated C5DC
NBS report form for DELFIAAPP4 Algorithm for elevated 17OH
progesterone
Transportation checklist APP5 Algorithm for elevated TSH
Laboratory refusal form APP6 Algorithm for Decreased GALT
Low birth weight and sick newborns guidline APP7 Algorithm for elevated C16OH
Newborns admitted to NICU APP8 Algorithm for elevated C8
Newborn screening flowchart APP9 Algorithm for elevated C14:1
Newborn screening order form (KMGC) APP10 Algorithm for elevated C5
Newborn screening order form (each hospital) APP11 Algorithm for elevated C5OH
List of disorders in the newborn screening APP12 Algorithm for elevated
CITRULLINE
Newborn screening card replacement form APP13 Algorithm for elevated
METHIONINE
Parental refusal for newborn screening APP14 Algorithm for MSUD
Newborn Screening sample collection procedure APP15 Algorithm for elevated
PHENYLALANINE
Diagram of invalid specimensAPP16 Algorithm for elevated
TYROSINE
Diseases screened by symptoms APP17 Kuwait NBSResults and
Confirmatory Testing APP21
Disease summary APP18
Brochure APP19

Newborn Screening Manual
� of �5 86
Introduction :
Newborn screening is a public health system made up of many different yet integral parts: screening, diagnosis, management, evaluation and education. The idea was born 1979 when Kuwait Medical Genetic Center constructed. Kuwait National Newborn Screening Program was based on screen two diseases in the governmental hospital of Kuwait (MOH). KNNSC coordinated the modernization of Kuwait newborn screening system over the last few years, both in the logistical aspects of how the program is run and in the ability to screen for an increasing number of diseases. To ensure that the newborn screening system runs smoothly, Newborn Screening Offices (NSO) is responsible for communicating with a multitude of newborn screening stakeholders including the families of infants screened, Newborn Screening labs, neonatal departments and the Ministry of Health. Expanded newborn screening began in October 2014, making Kuwait one of the most comprehensive newborn screening programs in Middle East. The primary goal of newborn screening is the early identification of affected infants in time to prevent serious health problems. To do so, every infant must be offered screening. Realizing this goal involves the combined efforts of health care providers across the state. The purpose of this guide is to ensure that all infants born in Kuwait have the opportunity to have a high quality newborn screen completed. This manual outlines: • recommended practices in newborn screening • common problems with screening practices • general information about NSO • diseases currently included in the newborn screening panel. While all of the diseases tested for are rare and not usually apparent at birth, a collectively large number of affected infants in Kuwait will be found to have these conditions every year but with low incidence. NSO can help these children to have the best start in life through timely newborn screening, early diagnosis and treatment. The cost of missing one of these conditions is immense, both in human suffering and in financial terms. Untreated infants can develop mental retardation, serious health problems, or even die, sometimes without a diagnosis being made.
Ensuring that every infant born in Kuwait is screened and that every affected infant receives appropriate treatment and follow-up requires the coordinated efforts of three main groups of Health care providers (HCPs):
• NSO in hospitals : They are responsible for the prompt follow up in the event of positive screen, unsatisfactory sample or a screen is missed. The NSO will release statistics with the confirmed cases and false positive screening results. They responsible for parent education about newborn screening, specimen collection, providing accurate and complete information for every screened infant, and for prompt follow-up in the event a sample is unsatisfactory or a screen is missed.
• Newborn Screening Laboratories at KMGC : NSL is responsible for testing, record keeping, quality assurance of testing, communication with NSOs about unsatisfactory or missed samples, referring screen positive infants to NSO in hospitals, obtaining follow-up information on screen positive infants, and providing education about newborn screening to parents, health care providers, and the general public.
• Metabolic and Endocrine clinics: Every screen positive infant is referred to metabolic specialist clinic . The metabolic specialist is responsible for ensuring confirmatory testing of screen positive infants, management of confirmed cases, providing NSO with follow-up information, and for education of local health care providers.
Newborn Screening History in Kuwait
1965 – Screening for Phenylketonuria (PKU) as a pilot study
1978 – Screening for congenital hypothyroidism (CH) as a pilot study
2005 – Screening of PKU and CH start in Kuwait medical genetic center after receiving DELFIA system
2007 – Screening of PKU, CH, 17OH progesterone, Galactosemia and biotindase start in Kuwait medical genetic center after receiving DELFIA system
2014 – Screening of 22 diseases in Kuwait started after receiving Tandem mass spectrometry system.

Newborn Screening Manual
� of �6 86
In addition, the Newborn Screening Committee includes most expert professionals in newborn screening to establish the policies of newborn screening program, for any information, contact [email protected]
Kuwait Newborn Screening system

Newborn Screening Manual
NSO contact information
� of �7 86
Up to date protocol: Kuwait National Newborn Screening Committee will add any new update of forms in the website . If you would like to be informed with any new update, please send an email with your name, institution, fax and phone number to: [email protected]
Newborn screening laboratories at Kuwait Medical Genetic Center Phone: 24814328 Fax: 24823242 e-mail:[email protected] Our lab hours are Sunday to Thursday 8:00am-16:00pm Holidays 8:00 – 01:00
10 important points to remember about newborn screening
1. Please use the term “Newborn Screen.” The term “Genetic test” is confusing to parents.
2. The incidence of all the newborn screening diseases very low and few cases are discovered per year
3. Screen every infant. Newborn screening detects rare diseases that are not apparent at birth. Most affected infants do not have a family history of the disease; therefore every infant is at risk.
4. Screen every infant prior to discharge from hospital. Infants discharged prior to 24 hrs of age should have a sample taken prior to discharge. Inform parents of the need and process for a repeat screen prior to five days of age. If an infant is transferred to another hospital, ensure there is communication between hospitals regarding the responsibility for obtaining the newborn screen.
5. Goal of Newborn Screening: Diagnose and treat in early life. If undetected and untreated these disorders may cause mental retardation, serious health problems, or even death. Early detection and treatment can greatly improve the outcome for these babies and sometimes even save their life. For example, infants with PKU and congenital hypothyroidism irretrievably lose significant cognitive function if phenylalanine and thyroid stimulating hormone (TSH) are not under control by three weeks of age.
NSO at Farwanyia Hospital Phone: 24888000 - ext.: 6319 Fax: 24805072 e-mail:[email protected] Office hours are Sunday to Thursday 8:00am-13:00pm
NSO at Al adan Hospital Phone: 23941628 Fax: 23966826 email:[email protected] Office hours are Sunday to Thursday 8:00am-13:00pm
NSO at Al jahra Hospital Phone: 24569418 Fax: 24577213 e-mail:[email protected] Office hours are Sunday to Thursday 8:00am-13:00pm
NSO at Maternity Hospital Phone: 24843100 ext. 7206 24842100 ext. 7206 Fax: e-mail:[email protected] Office hours are Sunday to Thursday 8:00am-13:00pm
Al- Sabah Hospital laboratories Phone: 24815000 ext. 3432- Dr.Rao(mob.99535228) / 3716-Dr.Jassim Abbas (mob . 66661580) 3713 – Dr.Ayman Salloum (mob. 66057790) Fax: 24840319 e-mail:[email protected] Office hours are Sunday to Thursday 8:00am-13:00pm
Dr. Mona Al-khawari Kuwait National Newborn Screening –Chair Phone: 97290055 Fax: 22436149 E-mail: [email protected]
Dr. Laila A.Bastaki Kuwait Medical Genetic Center –Director Phone: 99641572 Fax: 24814328 E-mail: [email protected]

Newborn Screening Manual
� of �8 86
6. A) A positive screen does not mean a baby is affected with a disease: • confirmatory tests must be done to confirm or rule out a disease
B) A negative screen does not rule out a disease: • Any infant symptomatic of a disease should have the appropriate diagnostic evaluation immediately.
7. Newborn screening is standard of care and is strongly recommended for all infants, but is not mandatory. Ensure that you have thoroughly explained newborn screening to all parents. If parents do not consent to testing, it is extremely important to document the refusal in the infant’s records.
8. Unsatisfactory samples require a repeat sample immediately. The NSO that took the initial sample is responsible for ensuring the repeat sample is done, even if the infant has been discharged. Delays in obtaining a repeat sample can lead to delayed diagnosis and serious health problems in affected infants.
9. Ensure that the newborn screening cards are filled out completely and accurately. All requested information is essential for accurate interpretation and follow-up of results. Incorrect or missing information can lead to false positive results and unnecessary testing for healthy infants.
10. For any additional information contact [email protected]
After delivery
A newborn screening blood spot collection card should be completed between one day (24 hours) and seven days after the birth of the infant, ideally, between two days (48 hours) and three days (72 hours) after birth. If tested before 24 hours of age, the test should be repeated within 5 days (eg. at the first postnatal checkup). Blood spots from infants are collected using the heel-prick method, which is detailed on the back of the specimen card. The parent should be given the education, pamphlets to orient with the program.
Newborn Screening offices in hospitals will fill out demographic information about the infant and the infant’s mother on the blood spot collection card. This information allows newborn screening laboratory to correctly interpret the infant’s results, and, in the event that the infant screens positive for a disease, it will allow the NSO coordinating follow-up to contact the parent quickly to retrieve the infant.
It is important that you emphasize to parents that newborn screening is part of their infant’s routine care and could save their infant’s life and/or prevent serious health problems. The vast majority of parents agree to have their infant screened. Parents may choose to decline newborn screening for their infant. You should discuss this decision with them, and you should document this decision in the infant’s medical record. NSOs will ask parents to sign a form indicating that they have refused newborn screening for their infant.
The newborn screening (NS) sample
Newborn screening timeline Before birth
As a provider of antenatal or newborn care, you should discuss newborn screening with your patient. Information about newborn screening should also be discussed with prospective parents in their prenatal education classes. To assist with parent education, pamphlets about newborn screening are available in many different languages (Arabic/English) and can be found in the NS offices in hospitals .
It is critical that newborn screening laboratories receive the newborn screening specimen card as soon as possible after the blood spots are collected. Therefore, the cards should be sent no later than 24 hours after collection and, ideally, as soon as the blood spots are dry (2-3 hours after collection). Infants with some of the diseases screened will start to become ill and may suffer irreversible damage soon after birth.
DO NOT BATCH SAMPLES FOR TRANSPORTATION.

Newborn Screening Manual
� of �9 86
When the sample is received, the blood spot is tested and the demographic information from the newborn screening card is entered into a database. This database links the infant’s information with the results of the screening tests, and also serves as a way to store the infant’s newborn screening result. The results of the screening tests are reviewed by a biochemistry consultant to determine if the infant has a lower risk of having a disease (“screen negative”) or a higher risk of having a disease (“screen positive”).
Newborn screening results
Screen negative results (low risk)
If the infant is “screen negative”, he or she has a low risk of having any the diseases included on the screening panel. In this case, a report is mailed to the hospital or health care provider that submitted the infant’s sample.
Unsatisfactory sample
If the infant’s sample is unsatisfactory (for example, if it was taken too early, or if there was not enough blood to do the testing), newborn screening laboratories will contact the hospital that sent in the sample and ask them for a new sample. The NSO who submitted the sample should send another if the baby still present in the neonatal department but if discharged they will need to call the parent to tell them that the infant’s test needs to be repeated and make arrangements for another sample to be taken as soon as possible.
Screen positive results (increased risk)
If the infant is screen positive, this does NOT mean that the infant has a disease; however, it does mean that the infant has an increased chance to have a disease. An NSO physician will refer the infant to metabolic specialist for follow-up diagnostic testing to determine if the infant truly has the disease. In some cases, NSO staff work directly with families to arrange testing. The metabolic specialist will provide the referring physician at NSO with follow-up information about the infant, as is the case for any medical referral. This includes medical information, which tests were done, the results of those tests, and whether or not the infant truly has the disease. This feedback allows NSO to make sure that screen positive infants receive appropriate and timely care. So ,can do monthly statistic of newborn screening program.
Screening limitations
As with all screening tests, false positive and false negative results occur in newborn screening. False positives may increase parental anxiety, while false negatives will give a misleading sense of reassurance. If an infant in your care displays symptoms of a particular disease, the child should be investigated and managed appropriately regardless of the results of the newborn screen. The relevant specialist should be contacted immediately for further advice.
There is wide variation in the clinical presentation of the diseases that the newborn screen detects. Therefore, some affected individuals – infants who have had diagnostic testing indicating that they have a par t icular d isease– wi l l remain asymptomatic or have very mild symptoms, even without treatment.

Newborn Screening Manual
List of disorders included in the Newborn Screening panel
� of �10 86
Test
Amino Acidemias :
Phenylketonuria (PKU)
Maple syrup urine disease (MSUD)
Homocystinuria (Cystathionine synthase def.)
Citrullinemia (ASA synthase deficiency )
Tyrosinemia (Type 1)
Argininosuccinic Aciduria (ASA Lyase deficiency)
Organic Acidemias :
Propionic Acidemia (PA)
Methylmalonic Acidemia (MMA)
Isovaleric Acidemia (IVA)
Glutaric Acidemia Type I (GA-I)
3-methylcrotonyl-CoA Carboxylase deficiency (3MCC)
Beta Ketothiolase deficiency (Mitochondrial Acetoacetyl CoA Thiolase deficiency)
Multiple CoA Carboxylase deficiency (MCD)
Fatty Acid Oxidation Defect :
Medium Chain Acyl CoA Dehydrogenase Deficiency (MCAD)
Very Long Chain Acyl CoA Dehydrogenase Deficiency (VLCAD)
Long Chain Hydroxy Acyl Dehydrogenase Deficiency (LCHAD)
Trifunctional Protein Deficiency (TFP)
3-Hydroxy-3-methylglutaryl-CoA Lyase Deficiency (3HMG)
Galactosemia
Biotinidase Deficiency
Endocrine Disorders :
Congenital Hypothyrodism
Congenital Adrenal Hyperplasia

Newborn Screening Manual
� of �11 86
g. Working hours for Clinical Biochemistry doctors:" Will follow MOH regulation" 4. Data registry: a. Site; KMGC b. In-charge personnel; i. NBS Coordinator ii. Data entry personnel iii.MOH Informatics Directorate c. Method; Newborn Screening Software
Equipment: 1. Tandem mass spectrometry 2. Fluoroimmunoassay analyzer (DELFIA system) 3. Hardware and Software for data registry 4. Newborn screening website 5. Consumables (a) Blood spot punctures (b) Filter papers for dried–blood spot specimens (c) CD rack, paper envelope (A5) (d) Referral form for early discharged babies (e) Transport checklist (f) NBS resources order form (g) Parental refusal for newborn screening (h) Newborn screening card replacement form (i) Brochures (j) Posters: collecting samples, valid samples, newborn screening flowchart.
Scope:
1. Kuwait Medical Genetics Center (KMGC) is the place for processing the collected filter papers from all newborn babies in Kuwait
2. Newborn Screening Office (NSO): a. Located in hospitals with maternity services (Farwanyia, Adan, Al-Jahra, and Sabah Maternity hospitals). b. Manned with one neonatologist ,one nurse , phlebotomist and data entry personnel per shift. c. Working hours: i. Working days :Open from 7:00-14:00 hours ii. Saturdays and public holidays: Open from 8:00-13:00 hours
3. Newborn screening unit (NSU)in Kuwait Medical Genetics Centre: a. Senior Clinical Biochemistry doctors b. Two Clinical Biochemistry registrars c. Medical laboratory technologists d. Two NBS coordinators e. Administrative staff f. Working hours Medical laboratory technologists: i. Working days :Open from 7:00-19:00 hours ii. Saturdays and public holidays: Open from 8:00-13:00 hours
References : 1. Clinical Laboratory and Standards Institute. Blood collection on filter paper for newborn screening programs; Approved standard–Fifth edition. CLSI document LA4-A6. Wayne, PA: Clinical and Laboratory Standards Institute; 2012. " 2. De Jesús VR, Mei JV, Bell CJ, Hannon WH. Improving and assuring newborn screening laboratory quality worldwide: 30-year experience at the Centers for Disease Control and Prevention. Seminars in Perinatalology 2010; 34:125–33. " 3. Federal Register. 39 CFR part 111 New Mailing Standards for Division 6.2 Infectious Substances. 2006; Section 10.17.9(b). Available at: www.gpo.gov/fdsys/pkg/FR" 4. Federal Register. 49 CFR part 173 Shippers General Requirements for Shipments and packaging. 2010; Section 173.134(b). Available at: http://ecfr.gpoaccess.gov/cgi" 5. World Health Organization. Guidance on regulations for the transport of infectious substances 2011 2012 .Geneva: WHO /HSE/IHR/2010.8.Available at: http:// www.biosafety.moh.gov.sg/home/uploadedFiles/Common/ WHO_Guidance_on_regulations_for_transport_of_Infectious_Substances." 6. Centers for Disease Control and Prevention. Guide to infection prevention for Outpatient settings: minimum expectations for safe care. Available at:" http://www.cdc.gov/HAI/settings/outpatient/outpatient-care-gl-standared-precautions" 7. Michigan Department of Community Health,Newborn screening guideline,October 2013" 8.newborn screening manual guideline of ontario

Newborn Screening Manual
Specimen collection
� of �12 86
Newborn Screening office:
A newborn Screening office is located in each of the 4 governmental hospitals and is concerned with newborn screening activities in the draining areas covered by these hospitals. Staff working in each office include: • Newborn Screening Coordinator • Nursing staff • Phlebotomist
Role of the Newborn Screening Coordinator:
(Responsible doctor at Newborn Screening office)" The hospital NBS coordinator plays a crucial role in assuring that the NBS process is both effective and efficient. " The coordinator fulfils this role by arranging, assisting and following up of different steps of screening process assuring proper interaction between nursing, and NSO staff and assisting NSO staff in resolving problems." The responsibilities of the NBS coordinator are:" 1. Clinical assessment of cases of positive screen results" 2. Initiating confirmatory testing for positive screen" 3. Referral of confirmed cases to specialist" 4. Reporting of confirmed cases and monthly statistics of Newborn Screening (NBS) to Kuwait Medical Genetics Center." 5. Serving as a contact person and facilitator between the NBS program and hospital staff involved in the NBS process " 6. Assuring that there is an adequate supply of NBS brochures and a mechanism for distribution to all mothers." 7. Working with obstetric department staff member to incorporate NBS educational information is existing and future prenatal classes offered to parents." 8. Performing quality assurance activities:" a. Assuring that there is a NBS policy in place describing the hospital’s NBS procedures. " b. Assuring that a log is maintained to track NBS specimens, transport personnel, and receipt of screening results." c. Assuring adequate inventory of NBS cards." d. Providing guidance/information to nurses and laboratory staff on the importance of accurately filling out all demographic fields on the NBS card." e. Assisting NSO staff in resolving problems of missing/incorrect demographic information on the NBS card and in obtaining retests when specimens were unsatisfactory for testing."
f. Assuring that hospital NBS policies and procedures include a protocol for notifying the NBS program if parents refuse NBS testing or if a newborn death occurs after a specimen was sent to the NBS laboratory." 9. Perform educational activities" a. Informing and educating hospital staff about new program guidelines and protocol changes e.g. new disorders added to test panel, changes in specimen collection requirements, and other NBS information, as necessary." b. Educating parents about importance of newborn screening and explanation of screening results."
Role of the Newborn Screening Office Nurses :
1. Gathering of Newborn Screening Samples from labour room, postnatal wards, NICU, SCU and Newborn Screening Office" 2. Assuring validity of samples for testing before delivery of samples to transportation personnel 3. Collecting samples in the specified envelope." 4. Delivery of samples to newborn screening transportation personnel with registration in registration book of data of each sample and total no.of valid samples delivered with date and time." 5. Recall of positive screen
Role of the Newborn Screening Office phlebotomy personnel : Collecting newborn Screening samples according to standard protocol of sample collection
Role of the Newborn Screening Office Data entry personnel :
1. Registration of Newborn screening data in registration book and electronically." 2. Monthly statistics of NBS cases."recall of positive screen."

Newborn Screening Manual
� of �13 86
Definition NSO, as a submitter, are integral to the newborn screening process and responsible for parent education, specimen collection, and following up on unsatisfactory samples and missed newborn screens. In following the recommended newborn screening practices.
Sample collection at Postnatal wards, NICU, SCU and Labor rooms: 1. Kuwait Medical Genetics Centre will supply the NSO in different hospitals in the state of Kuwait with the filter papers and brochures, ect."
2. Inventory of supply is the responsibility of NBS coordinator through the Head of the neonate departments using the NBS resources order form.
3. It is the responsibility of the nurse in-charge of the baby at the postnatal wards, NICU, SCU and labor room to collect the blood sample following the instructions on back of the filter paper .
4. The ideal sample should be collected between (48-72 hour) of age; 24 hours at a minimum. "
5. If the baby discharged home before 24 hour of age, the first sample should be collected before discharge and a clear instructions has to be given to the parents by the neonatologist regarding the importance of repeating the test up to one week and provide them with a referral form to the Newborn Screening office to collect another sample of filter paper.
6. The nurse in-charge should write the baby’s data on the filter paper including the contact numbers of the parents (It has to be 2 contact telephone numbers one of them should be a land line)
7. The nurse in-charge of the baby in any location should register the baby’s data including the barcode of the filter paper in the screening registry book, as well as in the nursing notes of the baby’s/ mother’s medical record, which should be available in any location for collecting samples."
8. The nurse in-charge of the baby in any location should allow the collected filter papers to dry in the assigned racks for a minimum 3 hours. "
9. The in-charge nurse at the Newborn Screening Office should collect the samples from postnatal ward; NICU, SCU and Labor room and communicate with the
in-charge nurse in the ward regarding improper sampling. "
10.The in-charge nurse at the Newborn Screening Office should store the samples in the office at room temperature."
11. The coordinator at the Newborn Screening Office has to guarantee safe transport of the filter papers to the newborn screening unit at KMGC.
Ensuring that the screening test is performed? Test is performed for all infants born in Kuwait hospitals, ensuring the test has been offered/ performed should be part of the pre-discharge check list. For infants born at home ensuring that the test has been offered / performed should be part of the first or second postpartum visit. If an infant is being transferred between hospitals, when possible, the newborn screen should be performed prior to the transfer and clearly documented in the discharge summary. If the newborn screen was not performed prior to transfer, the plan for the newborn screen should be part of the discharge summary. Clear communication between the two hospitals involved is essential to ensure the newborn screen is offered/ performed
Information for parents It is important that antenatal and prenatal educators discuss newborn screening with prospective parents. Pamphlets in multiple languages are available through the NSO.
Parental right of refusal Newborn screening is not currently mandated by law, however, it is considered standard of care. The vast majority of parents agree to have their infant screened. As with many standard medical practices, there is no formal province-wide mechanism to document consent. However ,members of KNNSC have taken many steps to provide education to ensure information is available to parents to make informed decisions for their infants. It is important that parents are made aware that newborn screening could save their infant’s life and/or prevent serious health problems. Parents may decline screening, and NSO should discuss this decision with them to ensure they are making an informed decision. Hospitals should document this decision in the infant’s medical record and/or have the parents sign a form indicating they have refused this testing for their infant.

Newborn Screening Manual
� of �14 86
Completing the Newborn Screening Card:
It is extremely important to fill out the NBS card completely and accurately. The specimen submitter is legally responsible for the accuracy and completeness of the information on the NBS card. The card will be scanned into the NBS database so legibility is critical. Press firmly using a black or blue pen and record the following information in the spaces provided:"
Infant information:
• INFANT'S NAME: Record the mother in capital letters. You should put before mother name” baby of …” . In multiple parity state the baby as twin I,II, ect." • GENDER: Completely shade in the appropriate oval to designate newborn's gender as male or female or unknown." • BIRTH DATE: Use a six-digit number (dd / mm /yy) for date of birth. For example, a birth on 4th of January 2012 would be recorded as 040112." • BIRTH TIME: Record time of birth. For example, a birth at 4:30 p.m. " • BIRTH WEIGHT in GRAMS: Record the exact birth weight in grams (1520 gram) in the boxes provided. Do not use pounds and ounces. " • CURRENT WEIGHT in GRAMS for 2nd and 3rd samples: Record the current weight in grams in the boxes provided do not use pounds and ounces. " • GESTATIONAL WEEKS: Record weeks of gestation at time of birth. " • MULTIPLE BIRTH ORDER: Completely record birth order by "I”, “II”,“III" for twins, triplets, etc." • SPECIMEN DATE: Use a six-digit number (dd/mm/ yy) representing the date on which the specimen was obtained." • COLLECTION TIME: Record time of specimen collection." • COLLECTED BY: Record initials or employee hospital identification number of person collecting the specimen." • MEDICAL RECORD NUMBER BABY: Record the birth/mother hospital's identification or medical record number." • NATIONALITY: Record Nationality of Newborn." • RBC TRANSFUSION: Record if the newborn was ever transfused with red blood cells prior to specimen collection. If yes,record the date (dd / mm /yy) and the time of the most recent transfusion. " • ANY TPN FEEDING: Completely shade in oval “yes” if the newborn is receiving total parenteral nutrition (TPN) at the time the specimen is obtained -OR- received TPN within 24 hrs of specimen collection."
Received TPN within 24 hrs of specimen collection." • OTHER FEEDING: Check all that apply. For instance, if a mother is both breast and bottle feeding, mark both and indicate the type of formula." • ANTIBIOTICS: " o For the 24-36 hour specimen; " ▪ State in the box “special things” if the newborn is currently receiving antibiotics or the mother was receiving ongoing antibiotics at the time of birth. " • TYPE OF COLLECTION: The preferred collection method is by heel prick with a single drop of blood applied directly to each circle on the filter paper. Check both “heel” and “capillary” if the blood was collected from the heel using a capillary tube. Note that the use of a capillary tube can result in layered, serum, clotted and damaged specimens. If the heel was not used, indicate the alternate collection method."
Mother information:
• MOTHER'S NAME: Record last name followed by first name. If the newborn is going to be released at birth to adoptive or foster parents, provide contact information of adoptive or foster mother."
• MOTHER'S ADDRESS: Record mother's current address.Information about the mother is needed to locate newborns in need of clinical evaluation or retesting."
• MOTHER'S PHONE: Record mother's mobile and home telephone number."
• MEDICAL RECORD NUMBER-MOTHER: Record the hospital identification or• medical record number
•BIOHAZARD CONDITIONS: Record in the special things box if the mother is having HEPATITIS, AIDS OR OTHER INFECTIOUS DISORDER to deal with the sample according to the approved standard protocol"
• BIRTH HOSPITAL: Record name of the birth hospital here only if different from the submitter."
Note: It is extremely important to fill out the screening card completely and accurately"

Newborn Screening Manual
� of �15 86
Timing of specimen collection
Full term infants
A newborn screening sample should be collected between one day (24 hours) and seven days after the birth of the infant. The ideal time to obtain the newborn screen is between two days (48 hours) and three days (72 hours) after birth.
Infants discharged early (<24hrs)
A newborn screening sample should be taken on every infant prior to discharge from hospital. If this happens before 24 hours, parents should be informed that a repeat newborn screen after 24 hours must be done and be informed how to obtain a repeat screen for their infant. The repeat should be performed within 5 days of the initial sample.
Not all diseases are reliably detected using blood samples taken before 24 hours of age. Samples obtained at less than 24 hours of age are considered unsatisfactory and a repeat sample will be requested. The NSO who submitted the initial sample is responsible for making arrangements for the repeat sample to be obtained.
Premature or low birth weight infants
Premature and/or low birth weight infants who are being screened should have their gestational age at birth and/or birth weight clearly indicated on the newborn screening specimen card. Premature or low birth weight (LBW) babies may have a delayed rise in TSH even if they have Congenital Hypothyroidism (CH). As NS laboratory uses elevation of TSH as the screening marker for CH, there is an increased risk of a false negative result (missed case) if these babies are screened only once in the early neonatal period. Premature or LBW infants also have a higher false positive rate for Severe Combined Immune Deficiency (SCID) screening. It is therefore important that screening samples are taken as outlined below and in the flow chart at the appendix .
Premature (less than 33.0 weeks gestational age) or low birth weight (less than 1800g) babies should have:
1. A first Newborn Screening specimen collected between 24 and 72 hours of age.
2. A second specimen collected at 2 weeks of age or when the baby is being discharged home from the hospital, which ever comes first . • If the baby is discharged home prior to 2 weeks of age from a hospital blood draw prior to discharge.
• If the baby is discharged home with the second specimen collected before 2 weeks of age consideration should be given to having a third specimen arranged as an outpatient at 4 weeks of age.
3. If the baby is being transferred to another hospital after 2 weeks of age, the hospital receiving the baby should confirm that the second sample was taken prior to transfer. If it was not taken, the receiving hospital should take the second sample as soon as possible after the baby arrives.

Newborn Screening Manual
� of �16 86
The following exceptions to the above policy apply:
1. A specimen should be collected prior to the baby receiving a packed red blood cell (PRBC) transfusion, even if this is prior to 24 hours of age.
This will ensure a satisfactory screen for:
• Galactosemia since the test relies on measurement of the Galactose-1-Phosphate Uridyltransferase enzyme activity in red blood cells.
If the first sample is taken at less than 24 hours of age, a second sample should be taken between 24 hours and 7 days of age.
2. Total Parenteral Nutrition (TPN). Amino acid solutions administered as part of TPN are a common reason for false
positive screening results for amino acid diseases in premature / LBW babies. Ideally, a specimen should be collected at a time when the baby is receiving lower amounts of TPN.
For example, if the baby is receiving 1.5 g/kg/d of amino acids at 24 hours of age, it is preferable to take the screening sample before this amount is increased. Please note that there is no increased risk of a false negative result if a sample is taken when the baby is receiving higher amounts of amino acid solutions; screening should not be delayed beyond 72 hours of age for this reason.
Premature infants ≥33 WGA and ≥1500g should NOT be treated differently than term babies.
Samples collected from infants greater than 7 days of age Samples taken from infants who are greater than 7 days of age are analyzed. As the levels of many screening markers drop over the first week of life, these lab results are checked manually to minimize the risk of missing an affected child (false negative results).
Transfused infants For the purpose of newborn screening, a transfusion is defined as receipt of packed red blood cells (PRBC). You may indicate “no” for transfusion status on the newborn screening requisition if an infant has only received fresh frozen plasma (FFP) and/or platelets. If possible, it is best to take the newborn screen prior to a blood transfusion. If the sample is not obtained before transfusion, the health care provider should wait 48-72 hours hours before a first screening specimen is collected. Blood transfusions are known to affect the results of screening for galactosemia. Infants who are affected with one of these disorders may be missed if they have a transfusion prior to their screen because the donor blood interferes with the screen. If an infant has a blood transfusion prior to their newborn screen, a repeat sample should be obtained 4 to 6 months after their most recent transfusion . The NSO who submitted the initial sample is responsible for making arrangements for the repeat sample to be obtained. All correspondence with parents should be documented.
Total Parental Nutrition (TPN)
If the infant is on TPN, the TPN circle on the blood spot collection card should be checked. This helps NS laboratory to interpret the infant’s results.
Infants transferred to another hospital
A newborn screening sample should be taken prior to discharge from the birth hospital. If transfer occurs <24 hours or a newborn screening sample was not taken at the birth hospital, this information should be included in the discharge summary and the receiving hospital should collect the newborn screening sample. Clear communication between the two hospitals involved is essential to ensure the newborn screen is not missed.
Expiration date
Check the expiration date of the blood spot collection card located in the upper right hand corner of the card next to the image of an hourglass, under the circles for the blood. The expiration date is in a year-month format (i.e. 2014-05). If the blood spot collection card has expired, use another card for specimen collection.

Newborn Screening Manual
� of �17 86
Methods of collection : - Heelstick (method of choice) - Capillary tube - Dorsal hand vein - Umbilical Venous Catheter (UVC) - Umbilical Arterial Catheter (UAC)
If you only have expired cards, order new cards immediately. In the meantime, collect newborn screening samples on the expired cards. NS laboratory tests all samples received on expired cards ; however, the sample is considered unsatisfactory and a repeat sample will be required. If you identify newborn screening cards as expired, please remove them from circulation. To avoid wasting these cards, please return them to KMGC where they will be used for other purposes, such as educational initiatives. Please send the expired card(s) to KMGC via the same transportation system used to send the newborn screening samples.
Preliminary steps
Ensure that the expiration date of the blood spot collection card has not passed.
Complete the required demographic information on the requisition portion of the blood spot collection card either manually or electronically. In manual applications a ballpoint pen should be used; soft-tip pens will not copy through to the other sheets of paper. Address imprint devices (or adhesive labels) should never be used unless the handling process ensures that patient information is not obscured and the blood collection area is not compromised. Do not use printers that might compress the paper.
Collect the required number of uniform blood spots (currently 5). Failure to collect the appropriate number of blood spots may result in the sample being unsatisfactory for analysis due to insufficient blood. It is preferable not to reapply blood in a partially filled circle as this may result in layering. Each of the five 11 mm circles on the DBS card requires approximately 75 ul to 100 uL of blood to fill.
All fields on the newborn screening card should be filled in as completely as possible. A complete newborn screening report cannot be issued if certain critical fields are not completed.
Procedure for blood spot specimen collection Specimen quality The primary goal of this standard is to ensure the quality of blood spots collected from newborns. Unacceptable and poor quality specimens place a burden on the screening system, and cause unnecessary trauma to the infant and anxiety to the infant’s parents. Poor quality specimens can potentially delay the detection and treatment of an affected infant, and could contribute to a missed or late diagnosed case. When NS laboratory receives an unacceptable specimen, it requests another specimen from the NSO in hospital . The turnaround time for analytic results is critical if treatment to prevent the adverse consequences of the condition (such as irreversible mental retardation or death) is to begin on time.
Specimen acceptability The only justification for refusing to analyze a specimen and declaring it unacceptable is that its analysis might yield unreliable, misleading, values for one or more analytes. For this reason, such specimens are not analyzed, and those responsible for collecting the original sample are notified immediately so that a new sample can be collected as soon as possible. When a specimen is analyzed, NSO is acknowledging that the specimen is suitable for testing and is assuming responsibility for the reliability of the analytic values
Avoid touching the area within the circles on the filter paper section of the blood spot collection card before, during, and after collection (blood spots) of the specimen. Do not allow water, feeding formulas, antiseptic solutions, glove powder, hand lotion, or other materials to come into contact with the specimen card before or after use.
Unacceptable sites for NBS blood collection:
• Arch or central area of an infant’s foot.
• Fingers of a newborn
• Earlobe
• A swollen or previously punctured site as accumulated tissue fluid may contaminate the specimen
• Uncleared intravenous lines

Newborn Screening Manual
� of �18 86
Cleaning the site
The skin in the area of the puncture site should be disinfected with alcohol (isopropanol/water: 70/30 by volume, “70%”). Allow the skin to air dry.
Puncture
To obtain sufficient blood flow, puncture the lateral aspect of the infant’s heel on the plantar surface with a sterile lancet or with a heel incision device. The incision device provides excellent blood flow by making a standardized incision 1.0mm deep by 2.5 mm long. Any puncture device used should be selected so that the puncture does not exceed 2.0 mm in depth. For infant safety, scalpel blades or needles must not be used to puncture the skin for blood collection. Disposable skin puncture lancets of different designs are commercially available for performing the heel stick on infants. For worker safety, disposable skin puncture devices that protect the user from unintentional self-inflicted skin punctures are preferable.
Direct application
After the heel has been punctured, wipe away the first drop of blood with a sterile gauze pad or cotton ball. Allow a second large blood drop to form by intermittently applying gentle pressure as the drop of blood forms. Touch the filter paper gently against the large blood drop and, in one step, allow a sufficient quantity of blood to soak through and completely fill a preprinted circle on the filter paper. Do not press the filter paper against the puncture site on the heel. Blood should be applied only to one side of the filter paper. Both sides of the filter paper should be examined to assure that the blood has uniformly penetrated and saturated the paper to the other side. After blood has been collected from the heel of the newborn, the foot should be elevated above the body, and a sterile gauze pad or cotton swab pressed against the puncture site until the bleeding stop
Precautions
Confirm the identity of the infant and ensure accuracy of the demographic data on the card.
Wash hands vigorously before proceeding. All appropriate precautions, including wearing powder-free gloves and changing gloves between infants, should be employed. Dispose used lancets in a biohazard container for sharp objects.
Follow recommendations of infection control
Heelstick ( method of choice)
Site preparation
Warming the newborn’s heel, the skin-puncture site, can help increase blood flow. A warm, moist towel or commercial heel warming device at a temperature no higher than 42oC may be used to cover the site for three minutes. This technique increases the blood flow sufficiently and will not burn the skin. In addition, positioning the infant’s leg lower than the heart will increase venous pressure.
Caution: Topical anesthetic creams should not be used as they may cause vasoconstriction and may also produce analytic interferences.

Newborn Screening Manual
� of �19 86
circles requires approximately 75-100 uL) required for the newborn screen. Touch the tip of the capillary tube to the blood drop formed at the heel puncture site. Allow blood to flow into the tube by capillary action. Fill rates might be improved by holding the tube in a near-horizontal position when touching to the blood drop. Collect enough blood to fill all the circles.
After filling the capillary tube, immediately apply the contents of that tube to the center of a single, preprinted circle on the filter paper, completely filling the circle. Waiting too long before application will allow cells and plasma to separate or the blood to clot. To avoid damaging the filter paper fibers, do not allow the capillary tube to touch the filter paper. Actions such as “colouring in” the circle, repeated dabbing around the circle, or any technique that might scratch, abrade, compress, or indent the paper should not be used. These actions may lead to compression of the filter paper and inaccurate blood volume collection.
In small, premature infants: the heel bone (calcaneus) might be no more than 2.0 mm beneath the plantar heel skin surface and half this depth at the posterior curvature of the heel. Studies indicate that for some infants (including full-term infants) a puncturing depth beyond 2.0 mm might be excessive and might cause bone damage. Puncture site depth should not exceed 2.0 mm.
Milking Excessive milking or squeezing the puncture site may cause hemolysis of the blood or result in a mixture of tissue fluids with the specimen that can adversely affect the test result.
Layering
Do not apply layers of successive blood drops to the same printed circle. Applying successive drops of blood to already partially dried spots causes “layering” and inaccurate blood volume collection, which results in non-uniform analyte concentrations and invalidates the specimens.
Capillary tube method:
Although not the method of choice, specimens can be obtained by applying blood to the blood spot collection card, which has been collected in sterile, anticoagulant-free capillary tubes. The use of anticoagulants should be avoided during the collection of the newborn screening sample. As it may cause interference with some laboratory tests. Using a fresh sterile, plain capillary tube for each circle to be filled on the blood spot collection card, collect the appropriate volume of blood (each of the five 11 mm
Do not reuse capillary tubes. Apply blood to only one side of the filter paper. Do not apply multiple capillary specimens to the same circle, since caking or heterogeneous spreading will occur and might adversely affect test results. Collect the required number of uniform blood spots. Failure to collect the appropriate number of blood spots might result in the sample being unsatisfactory for analysis due to insufficient blood. After blood has been collected from the heel of the newborn, the foot should be elevated above the body, and a sterile gauze pad or cotton swab pressed against the puncture site until the bleeding stops.
Dorsal hand vein Although not the method of choice, blood collected from needle puncture of the dorsal hand vein and its application directly onto the preprinted circles of the filter paper is possible. Blood should not be drawn from an extremity into which IV fluids have been infused unless appropriate precautions are taken. Select the appropriate sized winged blood collection set (butterfly). Remove or shorten catheter length so blood can flow freely onto the circle on the filter paper. Use standard pediatric venous collection procedures. Collect the required number of uniform blood spots. Failure to collect the appropriate number of blood spots might result in the sample being unsatisfactory for analysis due to insufficient blood.
Syringe collection of blood for application onto a blood spot collection card is not recommended because time delays may allow for clot formation and settling of cells producing heterogeneous specimens since anticoagulants are not used.

Newborn Screening Manual
� of �20 86
3. All transferred infants must be screened at any age after admission to NICU/SCU. "
4. Screen all infants at least twice if hospitalised more than 7 days. Order another screen prior to discharge or at 28 days, whichever comes first. "
5. The assigned neonatologist at NICU/SCU should check with the NSO co-ordinator for newborn screen results at 7 days and prior to discharge. Make sure screening was done, report(s) received, and no repeats are needed."
6. The NSO neonatologist should communicate the positive result to the assigned neonatologist at NICU/SCU."
7. The assigned neonatologist at NICU/SCU should watch for signs of conditions, even if screening results are normal. "
Specimen handling after collection:
After application to the blood spot collection card, avoid touching or smearing the blood spots. Allow the blood specimen to air dry at an ambient temperature of 15°C to 22°C, on a horizontally level, non-absorbent, open surface for at least three hours. Keep the specimen away from direct sunlight (indirect room light is not usually detrimental unless accompanied by heat). Blood spots on the filter paper should not be heated, stacked, or allowed to touch other surfaces during the drying process.
Since cross-contamination between specimens might occur, specimen-to-specimen contact is not appropriate. Once the blood is fully dried, Specimens should be sent to NS laboratory by the appropriate delivery method .
Dorsal hand vein collection (not the method of choice) • Test results might be affected by blood from different vessel sources • Hand veins might be needed for IV fluids • Venous sampling is more invasive than a heel stick.
Umbilical Venous Catheter (UVC) or Umbilical Arterial Catheter (UA C)
Although not the method of choice, blood collected from umbilical catheters is acceptable in certain situations (e.g., sick infants or in very low birth weight infants). Although unknown, it is reasonable to expect that there might be some difference in analytic test results between blood taken from the heel and that collected by umbilical catheters. Drawn 2cc blood from the line in order to clean it before the blood is collected for testing purposes. After cleaning the line, collect blood in an anticoagulant-free syringe and immediately apply appropriate volumes to the printed circles on the blood spot collection card. It is important that the blood transfer be as quick as possible to avoid blood clotting that might invalidate the specimen for testing. Collect the required number of uniform blood spots.
Recommendations apply to all neonates receiving intensive care: 1. The Nurse in-charge in NICU/SCU should collect the newborn screen by heel-prick. "
2. Time of collection: Collect the initial newborn screen" a. Collect before treatment (antibiotics, steroids, parenteral nutrition) is started or transfusion given, even if less than 24 hours, unless medically indicated. Otherwise, collect at 24-48 hours. " b. If the initial screen was collected at less than 24 hours, order another newborn screen collection at 48 hours to 7 days at the latest. " c. Arrange for additional collection if infant was transfused prior to initial screen."
It is critical that NSO receives the newborn screening specimen card as soon as possible after the blood spots are collected. Therefore, the cards should be sent no later than 24 hours after collection, and ideally, as soon as the blood spots are dry (4-6 hours after collection). DO NOT BATCH NEWBORN SCREENING SAMPLES.

Newborn Screening Manual
� of �21 86
Common Errors in the completion of the newborn screening blood spot collection card:
1. Missing critical data fields (e.g. missing date of collection or date of birth) • Please ensure all fields on the card are completed prior to sending the sample to NS laboratory
2. Entering in the incorrect date of collection when a sample is collected close to midnight
3 Using expired blood cards
• Prior to obtaining the sample, please check that the blood spot collection card is not expired. The expiry date is located in the upper right hand corner of the card next to the image of an hourglass, under the circles for the blood. The expiry date is in a year month format (i.e. 2012-05).
2. Assuring adequate transport of newborn screening samples according to Transport Guidelines.
3. Delivering newborn screening samples to the assigned newborn screening laboratory staff at Kuwait Medical Genetics Centre with registration of details of each received samples, total number of sample received and time of receiving of samples in registration book.
Proper packing of dried-blood spot specimens:
1. Proper packaging and labelling notifies employees and transportation personnel of package’s contents. Once DBS are completely dry, fix them on alternating sides so that blood spot cards from different patients are not touching each other. Pack 10-15 blood spot cards in recommended paper envelope.
2. Avoid packaging of DBS specimens in plastic, foil bags, or other airtight, leak-proof sealed containers. Lack of air exchange in the inner environment of a sealed container causes heat to buildup and moisture accumulation. Heat, direct sunlight, humidity, and moisture are also detrimental to the stability of DBS specimens and to analyte recovery. The inclusion of desiccant packs with the primary cold (ice bag) container will aid in preventing moisture accumulation.
Checking validity of dried-blood spot specimens for testing:
Dried-blood spot specimens arrived at Newborn Screening Unit. Kuwait Medical Genetics Centre, first examined for validity of testing according to the standards protocol. Each blood card should be examined for collection quality and possible damage and a note should be made of any poor quality samples. Specimens invalid for testing are returned back to the sender."
Data registration for dried-blood spot specimens:
Dried-blood spot specimens arrived at Newborn Screening lab. Kuwait Medical Genetics Centre should be registered in delivery book for each hospital with signature of the receiving technician with time and date of delivery." All arrived DBS specimens are registered in Newborn Screening database system"
Transportation of the positive screen results:
All results should reach NSCTL at Sabah hospital from Newborn Screening lab at KMGC for further discussion with the whole biochemistry team.
Note : Samples received at NSO. laboratory greater than 14 days after collection are unsatisfactory, however, they will be analyzed. If the results are “screen positive” for any disease, this will be reported. The quality of the results cannot be assured due to possible sample degradation resulting from the length of time since collection and a repeat sample will be requested.
Transport Guidelines for Dried-Blood Spot Specimens! Role of the Newborn Screening Specimens transport personnel : 1. Receiving newborn screening samples from the assigned nursing staff at NSO with registration of details of each of received samples, total number of sample received and time of receiving of samples in registration book.
Newborn Screening Manual
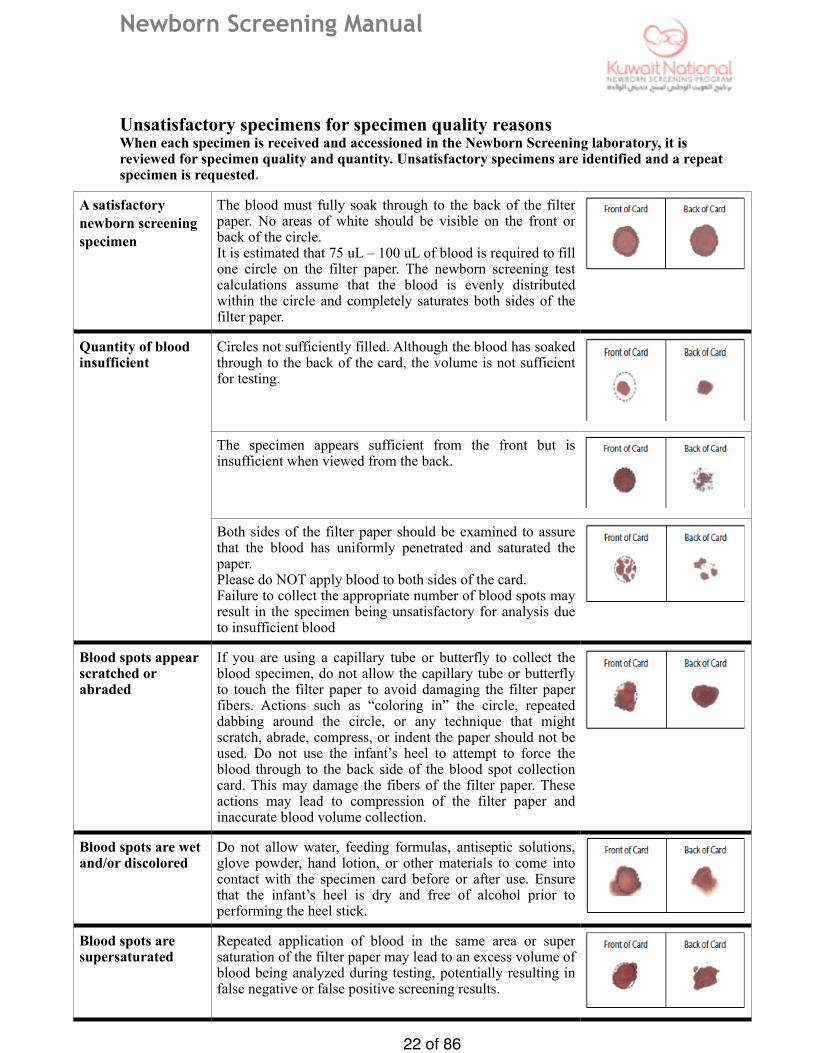
Unsatisfactory specimens for specimen quality reasons When each specimen is received and accessioned in the Newborn Screening laboratory, it is reviewed for specimen quality and quantity. Unsatisfactory specimens are identified and a repeat specimen is requested.
� of �22 86
A satisfactory newborn screening specimen
The blood must fully soak through to the back of the filter paper. No areas of white should be visible on the front or back of the circle. It is estimated that 75 uL – 100 uL of blood is required to fill one circle on the filter paper. The newborn screening test calculations assume that the blood is evenly distributed within the circle and completely saturates both sides of the filter paper.
Quantity of blood insufficient
Circles not sufficiently filled. Although the blood has soaked through to the back of the card, the volume is not sufficient for testing.
The specimen appears sufficient from the front but is insufficient when viewed from the back.
Both sides of the filter paper should be examined to assure that the blood has uniformly penetrated and saturated the paper. Please do NOT apply blood to both sides of the card. Failure to collect the appropriate number of blood spots may result in the specimen being unsatisfactory for analysis due to insufficient blood
Blood spots appear scratched or abraded
If you are using a capillary tube or butterfly to collect the blood specimen, do not allow the capillary tube or butterfly to touch the filter paper to avoid damaging the filter paper fibers. Actions such as “coloring in” the circle, repeated dabbing around the circle, or any technique that might scratch, abrade, compress, or indent the paper should not be used. Do not use the infant’s heel to attempt to force the blood through to the back side of the blood spot collection card. This may damage the fibers of the filter paper. These actions may lead to compression of the filter paper and inaccurate blood volume collection.
Blood spots are wet and/or discolored
Do not allow water, feeding formulas, antiseptic solutions, glove powder, hand lotion, or other materials to come into contact with the specimen card before or after use. Ensure that the infant’s heel is dry and free of alcohol prior to performing the heel stick.
Blood spots are supersaturated
Repeated application of blood in the same area or super saturation of the filter paper may lead to an excess volume of blood being analyzed during testing, potentially resulting in false negative or false positive screening results.
#
#
#
#
#
#
#

Newborn Screening Manual
� of �23 86
Unsatisfactory specimens due to missing demographics
All fields on the blood spot collection card should be filled in as completely as possible. A complete newborn screening report cannot be issued if certain critical fields are not completed.
Critical fields: Please ensure that the following fields on the newborn screening requisition are completed:
• Mother information, • The infant’s date of birth, • The date of specimen collection, • Birth weight, • The Submitting NSO, • Gestational age.
To identify samples which to reject NS laboratory use check list to confirm acceptability of samples :
Failure to provide all information on the card may result in delays in retrieving an infant who screens positive or may make interpretation of the results more difficult.
Once notified of an unsatisfactory specimen. The NS laboratory should attempt to communicate the need for a repeat specimen to NSOs .
S p o t s a p p e a r diluted
Ensure that the puncture site is clean and dry before collecting the specimen. Protect the specimen during the drying process.
Blood spots exhibit serum rings
Excessive milking or squeezing the puncture may cause hemolysis of the specimen or result in a mixture of tissue fluids with the specimen which can adversely affect the test result.
Blood spots clotted or layered
Applying successive drops of blood to already partially dried spots causes “layering” and inaccurate blood volume collection, which results in non-uniform analyte concentrations.
Blood spots delayed in transit
The blood spot collection cards arrived in a wet or damaged envelope.
#
#
#

Newborn Screening Manual
� of �24 86
10. Confirmatory report will be sent from NSCTL at Sabah hospital to NSO at the KMGC
11. NSO laboratory at the KMGC will send the final report to co-coordinator at NSO hospitals by telephone, email, fax and a hard copy to be attached to medical record.
12. The data entry personnel in newborn screening unit at KMGC should receive and enter the data into the software data registry system for newborn screening.
13. Annual report should be submitted by the newborn screening unit at KMGC to Newborn Screening Committee and a copy to the Pediatric Council.
Missed newborn screens
We hope to have network system that link to registry system of the newborn in Kuwait which make us alert with any infants exceed 14 days without screen, also can give data about newborn screen declined by family , incorrect date of birth entered at birth , missed infant by human mistake
Newborn screening education for health care providers
Education about newborn screening is vital to the success of the program. It is recommended to provide orientation about newborn screening to all new employees, including review of this manual.
Newborn screening education for parents
Parent education is essential to successful newborn screening. Informed parents are better able to understand screen positive results and the next steps in the process. In addition, informed parents may experience less anxiety associated with a repeat test request for an unsatisfactory sample.
Notification of positive screens:
1. If the result is normal do not contact the parents and no further intervention is required.
2. If the result is positive or equivocal, the coordinator at the newborn screening unit at KMGC should contact the co-coordinator at Newborn Screening Office (NSO) by phone, email and to send the result by fax, after senior clinical biochemist authorization uses NBS Report form. 3. The coordinator at the NSO should contact the parents bringing their baby for assessment and to initiate the confirmatory tests.
4. For positive DELFIA screen the coordinator of NS lab. at KMGC should :
i. Retest the same sample if the result is borderline. If the retested sample is borderline inform the NSO coordinator. ii. Inform the NSO coordinator to take a confirmatory testing, if the result is significantly high
5. For positive Tandem MS screen the coordinator of NBS lab at KMGC should: i. Retest the same sample for all the positive in
duplicate at KMGC lab. ii. Inform the NSO coordinator, according to the protocol of retesting.
6. The co-coordinator at (NSO) should contact the responsible specialist (Inborn error of metabolism (IEM)/ Endocrinologist) to inform about the baby’s clinical status and to initiate the required confirmatory tests.
7. The nurse of NSO should collect the confirmatory tests (second filter paper, urine or plasma) (Appendix 5)
8.The confirmatory sample should be accompanied with a request form clearly showing the positive screening result and with the official stamp for confirmatory testing.
9. The coordinator at the NSO should send the confirmatory samples to NSCTL at Sabah hospital or relevant confirmatory labs.
Education materials available
- Arabic brochure for parents
- English brochure for parents

Newborn Screening Manual
� of �25 86
Privacy and confidentiality
Kuwait National Newborn Screening Committee maintains the privacy and confidentiality of the health information and dried blood spot samples it receives. Some parents may have concerns about the use of their children’s health information or secondary uses of the dried blood spot samples. Accordingly, health information provided to NSO (including screening results) may be used for the following purposes:
• To provide care. Personal health information is used by care providers and trainees who are part of a child’s health care team.
• To teach. A child’s information may be used to support our partnership with the Kuwait Board of biochemistry and pediatric medicine , while adequately protecting their privacy.
• To conduct research and compile statistics. Researchers may use health information while working on a study approved by the Kuwait Ministry Of Health Research Ethics Board.
• To improve the care we provide by conducting quality improvement and risk management activities.
Storage of the dried blood spot samples
Dried blood spot samples are stored in a secure facility for 6 months, as they are a part of a child’s medical record. After 6 months, the samples are destroyed. NSO laboratory regularly checks the screening cutoffs and the stored samples assist NSO laboratory in performing this task. If a infant with a negative newborn screen is diagnosed with one of the diseases screened, the infant’s stored sample can be re-tested. This helps NS laboratory assess why the infant was missed in the newborn period, and potentially stops the same thing from happening again in the future.
Use of the dried blood spot samples
Occasionally, the dried blood spot samples may be used for other purposes after testing is finished. These include:
• Quality control and quality assurance within the NBS laboratory;
• Retesting the sample to help make a diagnosis when requested by NSO
• After a legal warrant if the infant has died unexpectedly
• For other testing at the parent written request;
• Samples may be used for research approved by a research ethics board if all identifying information has been removed so it is impossible to link an individual with the research results and written consent taken from the parents
Therefore storing samples for this length of time would allow investigation and possible re-testing if a child was diagnosed with one of the conditions on our panel following a negative newborn screen. It would also allow confirmation of whether or not a screening sample was obtained on the child.

Newborn Screening Manual
� of �26 86
Overview of NSO process
It is a responsibility of NSO to ensure that all infants born in Kuwait are offered the newborn screening test . A small sample of blood from the newborn is collected on a special paper card and then sent to the NSO laboratory for testing. Parents may decline screening, and NSO should discuss this decision with parents and document dissent by parents. While, as with many standard medical practices, there is no formal document for consent, NSO provide education to ensure information is available to parents to make informed decisions for their infants. It is important that antenatal health care provider and prenatal educators discuss newborn screening with prospective parents. Pamphlets in multiple languages Arabic/English are provided by KNNSC to NSO.
KNNSC provides the transportation system for samples to be submitted from NSO for analysis in the laboratory. Data from the submitted card is entered into the screening information system. The screening tests are performed and the results are interpreted by biochemistry consultant in Sabah laboratory to determine whether the risk that an infant has a targeted disorder is high or screen negative
Newborn screening laboratory are separate from any other laboratories and are located in Kuwait Medical Genetic Center at Ghanima Ahmed Alghanim center in Maternity hospital of Sabah health region.
Sample are received daily in NSO laboratory at KMGC from 08:00 am to 02:00 pm and in holidays from 08:00 to 01:00 pm All specimens received are assessed for quality and quantity for subsequent entry into the NS database Blood cards suitable for analysis are bundled into groups of 78 and passed on to the technicians in charge of punching on the multi-puncher.
Re-punched samples:
Specimens may be unsuitable for several reasons: • Machine malfunction • QC issues • Instrumental flags • Equivocal results of unknown reason In these situations, the sample will typically be re-punched singly and processed for the specific analyte • Specimens flagged as an initial positive are re-punched in duplicate for confirmation and reported out the following day. Exceptions where an abnormal result will be re-evaluated for confirmation on the same day of initial analysis include very provocative results for disorders where the delay in diagnosis may have catastrophic consequences
Data entry Data entry clerks are responsible for entering demographic information into the NSO database on every infant whose sample we receive. In order to ensure accuracy. This information includes the infant and mother’s name the submitting hospital/ doctor/ and contact information for the infant’s mother. In the event that an infant screens positive, this information allows the NSO to contact the family immediately to arrange further testing. If any critical information is missing, a data entry clerk contacts the submitter to obtain the missing information. The NSO data entry team aims to enter all information on the same day that a specimen is received , this can be up to 400 specimens daily.
Screening methodology Procedure for amino acid and acylcarnitine analysis
by Tandem Mass Spectrometry Scope or principle: There are a variety of metabolic inherited diseases that result in changes in the metabolism and transformation of amino acids. A large number of amino acids are quantitatively analysed using Tandem Mass Spectrometry (TMS) without the need for chromatographic separation. By forming butylated derivatives of the free carboxylic acid group(s) using positive electrospray (ESI+), charged specimen are created allowing the analyte to be detected in the mass spectrometer. TMS offers an efficient method that has proven to be relatively fast, simple and specific for amino acids.
Blood spot punching: A “punch” is an excised circle of blood which is subsequently used for sample analysis. All samples are punched into Microplates that are designated for a specific method/procedure. The minimum number of punches required for a collection to be of sufficient quantity is currently 7. This may increase as the newborn screening panel expands. NSO uses 3.2 mm punches, which are taken from the blood spot collection card.

Newborn Screening Manual
� of �27 86
DELFIA :
Dissociat ion-Enhanced Lanthanide Fluorescent Immunoassay) i s a robus t , h igh-performance immunodetection platform that provides a combination of benefits that make it the superior alternative to conventional ELISA. DELFIA utilizes the unique chemical properties of lanthanide chelates in concert with time-resolved fluorescence (TRF) detection to create an assay that offers high sensitivity, wide dynamic range, superior stability, and excellent flexibility. Given the robust nature of DELFIA technology and the advantages it holds over traditional ELISA.
There are a variety of metabolic disorders characterized by organic aciduria. Some disorders involving fatty acid oxidation defects may present with non-specific organic aciduria or an uninformative profile when the patients are asymptomatic, especially in the newborn period. Difficulty in identifying asymptomatic children necessitates the identification of specific metabolites characteristic of these inherited diseases. Acylcarnitines have been identified as being specific indicators for some of these metabolic disorders. Since acylcarnitines are highly polar non volatile compounds, GC-MS, which depends on sample volatilization, is an inefficient technique for the analysis of such compounds. Therefore a method for acylcarnitine profiling and quantitation using ESI+ with TMS has been developed.For example Hepatorenal tyrosinemia (HT) is an inborn error of metabolism that affects a number of organs including liver, kidney and bone. The clinical presentation is variable.
Neonatal by DELFIA system • 17α-OH-Progesterone • Thyroid stimulating hormone • Biotinidase enzyme • Galactose transferase enzyme
Clinical note
Abnormal TSH results at <24 hrs of age
TSH is commonly elevated in infants less than 24 hours of age. If an infant has an elevated TSH on a sample taken at less than 24 hours of age, newborn screening laboratory informs the NSO immediately and requests a repeat newborn screen. If a normal repeat screen is received and is screen negative for congenital hypothyroidism, the infant does not need to be referred as screen positive

Newborn Screening Manual
� of �28 86
Disorders Appearance of symptoms
Risk of crisis
Screening time
Factors causing false positive results
Factors causing false negative results
Congenital hypothyroidism
first year of life, early treatment prevents mental retardation, developmental delays
12 - 72 hr and 2 - 6 weeks
• TSH surge in first 12-24 hours
• topical iodine on baby or breastfeeding mother
• maternal hyperthyroidism treated with propylthiouracil,
• acute illness until recovered
• iodine deficiency
• delayed rise of TSH in affected
• infants, particularly if preterm (immature hypothalamic-pituitary-thyroid axis)
• dopamine therapy (suppresses
• TSH) • steroid treatment
(suppresses TSH & T4)
Congenital adrenal hyperplasia
first week of lifeyes
12 - 48 hr and 2 - 4 weeks
• preterm birth or LBW • sick or stressed infant • mother with CAH and
elevated • 17-OHP • early collection (<24 hr
of age)
• maternal steroid treatment steroid (dexamethasone) treatment in infant
Biotindase 1 week – 10 years of age (most show Symptoms between 3 – 6 months of age)
birth - 72 hr• heat with humidity
damage to specimen • prematurity • liver disease • , jaundice
• transfusion of plasma or other blood products
Galactosemia first week of lifeyes
birth - 48 hours
• heat damage to specimen,
• age of specimen (received by lab more than 4 – 5 days after collection)
• red blood cell transfusion
PKU6 - 8 months of age (irreversible brain damage happens if treatment is not started in first weeks of life)
24 - 48 hours
• parenteral nutrition • liver dysfunction or
immaturity • maternal PKU or
hyperphe uncontrolled by diet or medication
• early collection (<24 hours of age) or collection only a few hours after transfusion or discontinuation of ECMO
Newborn Screening Manual
� of �29 86
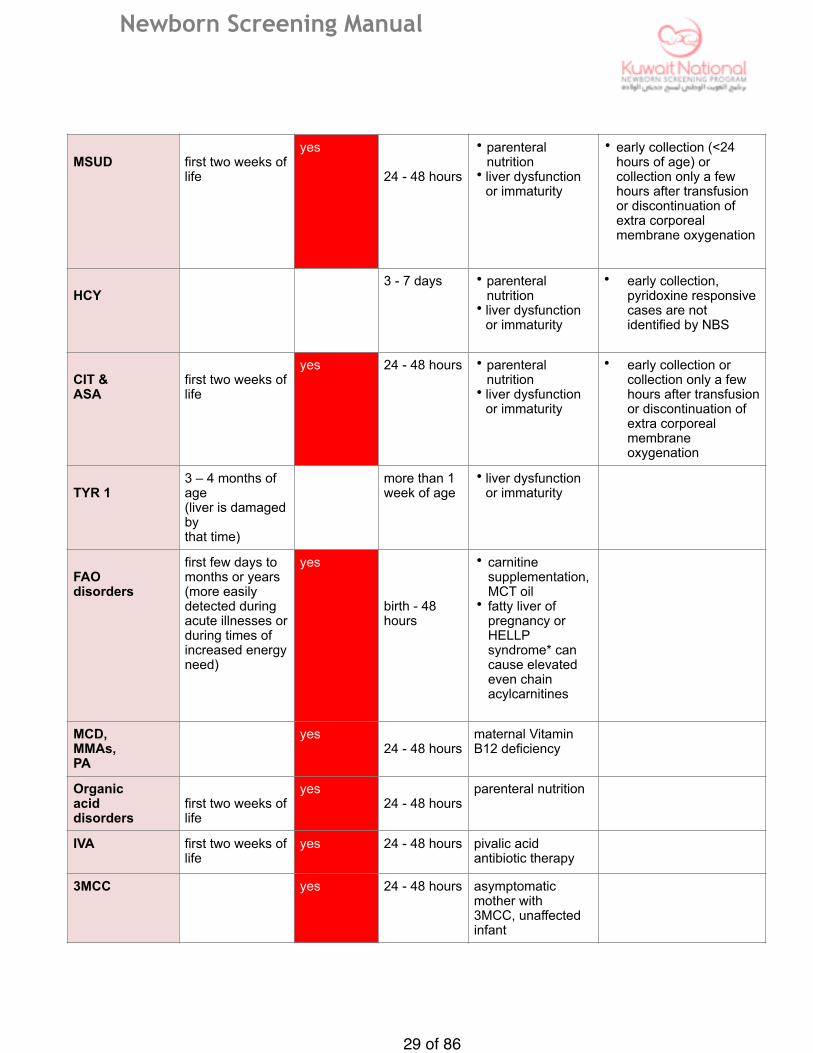
MSUD first two weeks of life
yes
24 - 48 hours
• parenteral nutrition
• liver dysfunction or immaturity
• early collection (<24 hours of age) or collection only a few hours after transfusion or discontinuation of extra corporeal membrane oxygenation
HCY3 - 7 days • parenteral
nutrition • liver dysfunction
or immaturity
• early collection, pyridoxine responsive cases are not identified by NBS
CIT & ASA
first two weeks of life
yes 24 - 48 hours • parenteral nutrition
• liver dysfunction or immaturity
• early collection or collection only a few hours after transfusion or discontinuation of extra corporeal membrane oxygenation
TYR 13 – 4 months of age (liver is damaged by that time)
more than 1 week of age
• liver dysfunction or immaturity
FAO disorders
first few days to months or years (more easily detected during acute illnesses or during times of increased energy need)
yes
birth - 48 hours
• carnitine supplementation, MCT oil
• fatty liver of pregnancy or HELLP syndrome* can cause elevated even chain acylcarnitines
MCD, MMAs, PA
yes24 - 48 hours
maternal Vitamin B12 deficiency
Organic acid disorders
first two weeks of life
yes24 - 48 hours
parenteral nutrition
IVA first two weeks of life
yes 24 - 48 hours pivalic acid antibiotic therapy
3MCC yes 24 - 48 hours asymptomatic mother with 3MCC, unaffected infant

Newborn Screening Manual
Special consideration that affect the results of screening:
1. Transfusions The first newborn screening test should be collected prior to any transfusion, This is necessary to avoid false negative results for many disorders. Any transfusion of red blood cells (whole blood, packed RBCs or ECMO) can cause false negative results for galactosemia and this effect lasts until the donor red blood cells have been replaced (3 – 4 months after the last transfusion). Re-screening then would be necessary unless a previous screen had been collected prior to transfusion. Note that for galactosemia a specimen collected prior to 24 hours of age is valid and yields reliable results. Transfusions of whole blood (or plasma,) can cause false negative results for all screened disorders for 4 – 72 hours after the transfusion (except for galactosemia the effect lasts for 3 – 4 months).
2. Parenteral Nutrition (PN) Parenteral nutrition can cause false positives for amino acids and fatty acids. Multiple amino acid abnormal results can be an indication of excess free amino acids from the parenteral nutrition solution or liver problems (immature enzymes or illness so that liver enzymes can’t handle the amino acids fast enough to prevent a rise in amino acid concentration in the blood). Medium chain fatty acids are also added to parenteral nutrition solutions and can be present in higher amounts in the blood. Prolonged PN can lead to carnitine depletion. A false positive result for IVA (elevated C5) is also possible. A repeat screen should be collected 24 – 72 hours after PN is stopped, if a previous screen had abnormal results.
3. Maternal Conditions • A mother with hyperthyroidism treated with antithyroid agent can deliver a baby with transient
hypothyroidism (elevated TSH on the newborn screen). Positive results will occur until the drug clears the newborn’s system - between 7-14 days after birth. A repeat screen or other thyroid testing should be done around two weeks of age.
• A mother with CAH can deliver a baby with a false positive result for 17-OHP. The newborn should be re-screened between 3 and 7 days after birth.
• Transient hyperphenylalaninemia in the newborn is a result of a mother with uncontrolled PKU (high phenylalanine levels). This effect will normalize within 12 – 24 hours, unless the baby also has PKU.
• A mother treated with steroids during pregnancy can deliver a baby with a false negative result for CAH since steroids can suppress fetal adrenal function. The length of the effect depends on the class of steroid and the dose, and is unknown but estimated at 1 – 2 weeks after birth. A repeat screen done later than 2 weeks of age would be needed.
• Maternal carnitine or Vitamin B12 deficiencies can cause false positive results for C0 (carnitine) and C3 (Vitamin B12). The effects can last several days depending on the nutrition provided to the newborn (for B12 deficiency) – the duration of the effect of carnitine deficiency is unknown).
• Carnitine supplementation can cause false negative results for C0 during supplementation and for some weeks afterwards. It can also cause false positives for other acylcarnitines. This effect lasts approximately 4 days.
• A mother with 3MCC can have an unaffected baby with elevated C5OH. The duration of this false positive effect is unknown.
� of �30 86

Newborn Screening Manual
4. Sick or stressed infant A sick or stressed newborn can have elevated 17-OHP (false positives for CAH) until recovered. Liver disease and jaundice can cause false positives for many disorders ( tyrosinemia, homocystinuria, PKU, biotinidase deficiency )
5. Preterm or low birth weight infant • Elevated tyrosine and 17-OHP and low biotinidase are common results for preterm or low birth
weight babies (false positives for tyrosinemia, CAH and biotinidase deficiency). • False positives for amino acids disorders are a result of immature liver enzymes. • A false negative result for hypothyroidism caused by an immature hypothalamic/ pituitary/thyroid
axis where TSH does not rise in response to low T4 levels can last for more than a month after birth. Since the newborn screen now measures only TSH, this possibility should be considered for all preterm and low birth weight babies, even though the hypothyroidism is usually transient.
6. Steroid or antibiotic treatment • Dopamine therapy suppresses TSH and can cause false negative results for hypothyroidism until
the drug is discontinued. • Steroid therapy (including dexamethasone) suppresses TSH and can cause false negative results
for hypothyroidism as well as false negative results for CAH. This effect can last for 1 to 2 weeks after therapy has been stopped.
• Antibiotics conjugated with pivalic acid (for example, pivampicillin) can elevate C5 (false positives for IVA). This effect lasts until the drug clears the baby’s system (at least 24 hours after discontinuing therapy).
7. Early collection (prior to 24 hours of age) • False positives for hypothyroidism and CAH are possible because of the normal hormone surge
after birth. • False negatives for amino acidopathies and organic acid disorders are possible with early
collection but specimens collected shortly after 24 hours of age are reliable.
8. Late collection • Collection of a first screen after 48 hours of age can show false negative results for fatty acid
oxidation disorders. A well fed state can mask indications of a FAOD so it is important that a first screen be collected between 24 and 36 hours if at all possible.
• If a baby has an abnormal result for any FAOD on a first screen and then has a normal result on the second, that second result cannot be taken to mean that the baby had a false positive on the first screen. All babies with abnormal results on first screens should have diagnostic testing done to confirm or rule out the possibility of a disorder even though their second screen is “normal.” Very few false positive results for fatty acid oxidation disorders ever occur.
• Late collection is also not helpful in identifying disorders that have early crises since results will not be available when symptoms start to appear. Disorders which can have serious consequences if not diagnosed early include galactosemia, MSUD, salt-wasting CAH, urea cycle disorders, organic acid disorders and some fatty acid oxidation disorders.
� of �31 86
Newborn Screening Manual
Kuwait National Newborn Screening Panel of 22 Disorders
These are the original core disorders of the recommended by Kuwait National Newborn Screening Committee (KNNSC). Early identification and lifelong treatment of these disorders can help to prevent many of the harmful consequences of the disorders and in many cases affected babies can grow and develop normally.
Endocrine Disorders (2 disorders)
Endocrine disorders occur when one or more of the body’s hormones cannot be produced while others are overproduced. Hormones regulate metabolism and are necessary for the normal function of the body’s organs.
Congenital hypothyroidism (CH) • A common*, endocrine condition resulting from deficient thyroid hormone secretion. It is not often an inherited condition and is most commonly caused by a failure of the thyroid gland to develop properly. • If undetected, developmental delays, poor growth and mental retardation develop before diagnosis is made and most of this damage is not reversible with treatment. A newborn with CH may have feeding problems, lethargy, hypotonia, jaundice and constipation. • Treated with daily oral doses of thyroid hormone. If treatment begins by two weeks of age a baby can develop normally. • Risk of this disorder is detected by an immunoassay for elevated thyroid stimulation hormone (TSH).
Congenital adrenal hyperplasia -21-hydroxylase deficiency (CAH) • A relatively common*, inherited group of disorders (autosomal recessive) marked by deficiency or absence of one or more enzymes essential to the production of adrenal cortex hormones. The enzyme involved most commonly is steroid 21-hydroxylase. This results in the inability to synthesize cortisol, aldosterone or both and also results in an overproduction of adrenal androgens. • Symptoms include ambiguous genitalia in girls and in the salt-wasting form of the disorder, vomiting, dehydration, electrolyte imbalances (hyponatremia and hypokalemia), hypotension, shock and even death within 2 weeks of birth. • Treated with hormone and electrolyte replacement with possible surgery for virilized females. Early treatment can prevent salt-wasting crises and growth and development problems. • Risk of this disorder is detected by an immunoassay for elevated 17α- hydroxyprogesterone (17-OHP).
� of �32 86

Newborn Screening Manual
Amino Acid Disorders (6 disorders) Amino acidopathies are disorders of amino acid metabolism that occur when enzymes needed to break down specific amino acids or eliminate nitrogen from the body are deficient or absent. Toxic levels of amino acids or ammonia accumulate and cause brain damage and even death.
Phenylketonuria (PKU) • A relatively common*, inherited disorder (autosomal recessive) that occurs when the enzyme, phenylalanine hydroxylase, necessary to break down phenylalanine, is missing or not working properly. • Without early detection and treatment, permanent mental retardation, behavioral problems and eczema develop after a few months. Newborns with PKU seem healthy and symptoms do not appear until irreversible damage has been done. • Treatment is a low protein diet with most protein provided in a phenylalaninerestricted formula. If treatment is started early, babies develop normally and have normal IQ. • Risk of this disorder is detected with elevated phenylalanine by MS/MS.
Maple syrup urine disease (MSUD) • A very rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, branched chain ketoacid dehydrogenase, necessary to break down ketoacid derivatives of leucine, isoleucine and valine, is missing or not working properly. • Symptoms develop within the first week of life - feeding intolerance, vomiting, lethargy and progress to irreversible mental retardation, seizures, coma and death. • Treatment is a low protein diet with most protein provided in a formula restricted in branched-chain amino acids and dietary monitoring to prevent metabolic crises. • Risk of this disorder is detected with elevated leucine by MS/MS.
Classical Homocystinuria (CHCY) • Also called cystathionine β-synthase deficiency or CBS deficiency. • A very rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, cystathionine β-synthase, necessary to break down methionine, is missing or not working properly. • Symptoms develop slowly and include developmental delay, mental retardation, skeletal abnormalities (marfanoid appearance), osteoporosis, blood clots and dislocated lens in the eye. • Treatment is a low protein diet with most protein provided in a methionine restricted formula. Vitamin B6 may be given along with other vitamin supplements. • Risk of this disorder is detected with elevated methionine by MS/MS.
� of �33 86

Newborn Screening Manual
Citrullinemia (CIT 1) • A rare*, inherited urea cycle disorder (autosomal recessive) that occurs when the enzyme, argininosuccinic acid synthetase, necessary to excrete the nitrogen from amino acids as urea, is missing or not working properly. • Crisis symptoms of hyperammonemia, which can appear in the first week of life, start with loss of appetite, lethargy, hypotonia and vomiting and progress to seizures and coma. Prolonged periods of hyperammonemia can cause brain damage (intellectual disability). • Treatment is a low protein diet and special formula, supplementary arginine and other medications along with avoiding going without eating for very long. • Risk of this disorder is detected with elevated citrulline by MS/MS.
Argininosuccinic acidemia (ASA) • Also called argininosuccinic aciduria or argininosuccinyl-CoA lyase deficiency. • A rare*, inherited urea cycle disorder (autosomal recessive) that occurs when the enzyme, argininosuccinyl-CoA lyase, necessary to excrete the nitrogen from amino acids as urea, is missing or not working properly. • Crisis symptoms of hyperammonemia, which can appear in the first week of life, start with loss of appetite, lethargy, poorly controlled breathing rate or body temperature, hypotonia and vomiting and progress to seizures and coma. Prolonged periods of hyperammonemia can cause brain damage (intellectual disability) and developmental delay. • Treatment is a low protein diet and special formula, supplementary arginine and other
medications along with avoiding going without eating for very long. • Risk of this disorder is detected with elevated citrulline by MS/MS.
Tyrosinemia Type 1 (TYR 1) • A very rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, fumarylacetoacetate hydrolase, necessary to break down tyrosine, is missing or not working properly. • Symptoms develop in the first months of life but are not present immediately after birth. Untreated, a baby with tyrosinemia will develop liver disease (enlarged liver, jaundice, cirrhosis) and kidney damage leading to death. Early symptoms include lethargy, vomiting, diarrhea, irritability and failure to thrive. • Treatment includes medication, a diet low in tyrosine and phenylalanine and possibly a liver transplant. • Risk of this disorder is detected with elevated tyrosine by MS/MS.
� of �34 86

Newborn Screening Manual
Fatty Acid Oxidation Disorders (4 disorders) Fatty acid oxidation disorders (FAODs or FODs) occur when fatty acids cannot be completely metabolized to produce energy because of defects in enzymes needed for this conversion. When the body’s supply of glucose and glycogen are expended, fatty acids are broken down to supply energy during periods of fasting or increased energy demands (fever, stress). Different defects in the fatty acid oxidation pathway prevent the complete breakdown of fatty acids to produce energy and a sudden crisis occurs which can leave an affected infant or child dead or with brain damage. These conditions can yield false negative results if screening occurs after a baby is well fed.
Medium-chain acyl-CoA dehydrogenase deficiency (MCAD) • A relatively common*, inherited disorder (autosomal recessive) that occurs when the enzyme, medium chain acyl-CoA dehydrogenase, necessary to break down fatty acids of medium chain length (4 to 12 carbons long), is missing or not working properly. • Symptoms present acutely with fasting and include hypoketotic hypoglycemia, vomiting, lethargy, seizures, metabolic acidosis, hyperammonemia, hepatomegaly and death. • Avoiding fasting (frequent feedings) and a low-fat diet can prevent metabolic crises. • Risk of this disorder is detected with elevated C8 by MS/MS.
Very long-chain acyl-CoA dehydrogenase deficiency (VLCAD) • A rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, very long chain acyl-CoA dehydrogenase, necessary to break down long chain fatty acids (12 to 18 carbons long), is missing or not working properly. • Symptoms present acutely with fasting and include hypoketotic hypoglycemia, cardiomyopathy in many cases, vomiting, lethargy, seizures, metabolic acidosis, hyperammonemia, hepatomegaly and death. • Avoiding fasting (frequent feedings) and a low-fat diet (supplemented with MCT oil and
cornstarch), can prevent metabolic crises. • Risk of this disorder is detected with elevated C14:1 by MS/MS.
Long-chain 3-OH acyl-CoA dehydrogenase deficiency (LCHAD) • A very rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, long chain L-3-hydroxyacyl-CoA dehydrogenase, necessary to break down certain fatty acids (between 12 and 18 carbons long), is missing or not working properly. • Symptoms include hepatomegaly, cardiomyopathy, lethargy, hypoketotic hypoglycemia. • Avoiding fasting (frequent feedings) and a low-fat diet (low in long chain fatty acids and supplemented with MCT oil and cornstarch), can prevent metabolic crises. • Risk of this disorder is detected with elevated C16OH by MS/MS.
� of �35 86

Newborn Screening Manual
Trifunctional protein deficiency (TFP) • Also called mitochondrial trifunctional protein deficiency. • A very rare*, inherited disorder (autosomal recessive) that occurs when a protein containing three enzymes (long chain 3-hydroxyacyl-CoA dehydrogenase, long chain enoyl-CoA hydratase and long chain thiolase) necessary to break down long-chain fatty acids is missing or not working properly. • Avoiding fasting (frequent feedings) and a low-fat diet (low in long chain fatty acids and supplemented with MCT oil and cornstarch), can prevent metabolic crises. • Risk of this disorder is detected with elevated C16OH by MS/MS.
Organic Acid Disorders (8 disorders) Organic acidemias (OAs) are a group of inherited metabolic disorders that occur when certain enzymes involved in the breakdown of amino acids and other substances are not functioning properly. Toxic acids build up in the blood and spill into the urine (metabolic acidemia). Without treatment and prevention of acute episodes, these disorders can lead to coma and death during the first days or weeks of life.
Isovaleric acidemia (IVA) • A very rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, isovaleryl-CoA dehydrogenase, necessary to break down leucine, is missing or not working properly. • Symptoms include metabolic ketoacidosis, poor feeding, vomiting, dehydration, lethargy, rapid shallow breathing, “sweaty feet” odor, hyperammonemia, coma and death. • Avoiding fasting (frequent feedings) and a low-protein diet can prevent metabolic crises. • Risk of this disorder is detected with elevated C5 by MS/MS.
Glutaric acidemia type 1 (GA-1) • A relatively rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, glutaryl-CoA dehydrogenase, necessary to break down lysine, hydroxylysine and tryptophan, is missing or not working properly. • Affected infant is usually macrocephalic with later signs of metabolic ketoacidosis (during
periods of fasting or illness, which can progress to coma and death), failure to thrive, irritability, hypotonia, poor balance and coordination and neurological problems.
• Avoiding fasting (frequent feedings) and a low-protein diet can prevent metabolic crises. • Risk of this disorder is detected with elevated C5DC by MS/MS.
� of �36 86

Newborn Screening Manual
3-Hydroxy-3-methylglutaric aciduria (HMG) • Also known as 3-hydroxy-3-methylglutaryl-CoA lyase deficiency or HMG-CoA lyase deficiency. • A very rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, 3-hydroxy-3-methylglutaryl-CoA lyase, necessary to break down leucine, is missing or not working properly. • Symptoms usually appear during the first year of life and include vomiting, diarrhea, lethargy, hypotonia and metabolic acidosis (during a period of fasting or illness) which can lead to coma and death. • Treatment includes avoidance of fasting and a low protein diet to prevent metabolic crises. • Risk of this disorder is detected with elevated C5OH and C6DC by MS/MS.
3-Methylcrotonyl-CoA carboxylase deficiency (3MCC) • A rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, 3-methylcrotonyl-CoA carboxylase, necessary to break down leucine is missing or not working properly. • Symptoms usually appear during the first year of life and include lethargy, vomiting, hypotonia, seizures, developmental delay and metabolic acidosis (during a period of fasting or illness) which can lead to coma and death. • Treatment includes avoidance of fasting and a low protein diet to prevent metabolic crises. • Risk of this disorder is detected with elevated C5OH by MS/MS.
Multiple carboxylase deficiency (MCD) • Also known as holocarboxylase synthetase deficiency. • A rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, holocarboxylase synthetase, necessary to attach biotin as a cofactor to certain carboxylase enzymes, is missing or not working properly. • Symptoms can appear during the first week of life and include poor feeding, lethargy, vomiting, hypotonia, skin rash and metabolic acidosis which can lead to coma and death. • Treatment consists of biotin supplementation. • Risk of this disorder is detected with elevated C5OH and C3 by MS/MS.
� of �37 86
Newborn Screening Manual
Methylmalonic acidemia
mutase deficiency (MUT) • Also known as methylmalonic acidemia, Vitamin B12
• A rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, methylmalonyl-CoA mutase, necessary to break down certain lipids, amino acids and cholesterol is missing or not working properly. unresponsive. • Symptoms include lethargy, dehydration, vomiting, hypotonia, seizures and metabolic ketoacidosis which can lead to coma and death. • Treatment includes avoiding fasting and a low protein diet to prevent metabolic crises. • Risk of this disorder is detected with elevated C3 by MS/MS. cobalamin disorders (Cbl A,B) • Also known as methylmalonic acidemia, Vitamin B12
• Rare*, inherited disorders (autosomal recessive) that occur with a defect in the synthesis of adenosylcobalamin, one of the active forms of Vitamin B responsive. • Symptoms include lethargy, dehydration, vomiting, hypotonia, seizures and metabolic ketoacidosis which can lead to coma and death which is needed as a cofactor for methylmalonyl-CoA mutase, necessary to break down certain lipids, amino acids and cholesterol. • Treatment includes Vitamin B12 , injections and a low protein diet. • Risk of this disorder is detected with elevated C3 by MS/MS.
Propionic acidemia (PROP) • A very rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, propionyl-CoA carboxylase, necessary to break down a product of protein and fat metabolism is missing or not working properly. • Symptoms usually appear during the first week of life and include poor feeding, lethargy, vomiting, dehydration, hypotonia and metabolic ketoacidosis which can lead to coma and death. • Treatment includes avoidance of fasting and a protein-restricted diet to prevent metabolic crises. • Risk of this disorder is detected with elevated C3 by MS/MS.
Beta-ketothiolase deficiency (BKT) • A very rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, β -ketothiolase, necessary to break down isoleucine, is missing or not working properly. This disorder also impairs the body’s ability to process ketones, which are produced during the breakdown of fats. • Symptoms usually appear during the first year of life and include lethargy, vomiting, seizures, and metabolic acidosis (during a period of fasting or illness) which can lead to coma and death. Long term complications include developmental delay, cardiomyopathy and hypotonia. • Treatment includes avoidance of fasting and a low protein diet to prevent metabolic crises. • Risk of this disorder is detected with elevated C5OH and C5:1 by MS/MS.
� of �38 86

Newborn Screening Manual
Other Enzyme Deficiencies (2 disorders)
Biotinidase deficiency (BIO) • A rare*, inherited disorder (autosomal recessive) that occurs when the enzyme, biotinidase, necessary to recycle the vitamin biotin is missing or not working properly. Free biotin is needed as a cofactor for carboxylase enzymes and if it cannot be freed from its bound form by biotinidase it is not available to be used as a cofactor. • Symptoms which usually appear in a few months of age include seizures, hypotonia, hair loss and skin rashes. Untreated, developmental delays, speech problems, hearing loss and ataxia develop. • Treatment is daily supplementation with biotin. • Risk of this disorder is detected by DELFIA system for biotinidase enzyme (BIO) .
Galactosemia (GALT) • Also called galactosemia type 1 or classic galactosemia. • A rare*, inherited disorder (autosomal recessive) marked by the inability to metabolize galactose because of a deficiency of the enzyme, galactose-1- phosphate uridyl transferase (Gal-1-PUT), which is needed to convert galactose to glucose. • Symptoms which start in the first week of life include jaundice, vomiting and feeding problems leading to failure to thrive or even death. Even with treatment (a diet without any galactose), many affected children have some development delay or mental deficit, speech or language problems, cataracts or enlarged liver. • Risk of this disorder is detected by an enzyme assay for Gal-1-PUT (GALT) and total Galactose (T.GAL) by DELFIA .
Other Disorders and Incidental Findings Some of the secondary disorders that have been detected Newborn Screening Program along with incidental findings (carrier states) include: • Non-classical CAH • Hyperphenylalaninemia • Hypermethioninemia • Partial biotinidase deficiency • Galactosemia carrier or Duarte variant galactosemia • Carnitine palmitoyl transferase deficiency type II (CPT-2)
� of �39 86

Newborn Screening Manual
� of �40 86
Appendix 1
Filter paper for dried –blood spot specimens

Newborn Screening Manual
� of �41 86
Appendix 2
Referral form for early discharged babies

Newborn Screening Manual
� of �42 86
Appendix 3
NBS report form for Tandem MS/MS
Newborn Screening Manual
� of �43 86
Appendix 4
NBS report form for DELFIA

Newborn Screening Manual
� of �44 86
Appendix 5
Hospital Name Date:
Complete data on collection cards Valid Collection cards
• Not expired
• Not torn
• Newborn or mother details • Birth date • Collection date • Birth weight • Gestational age • Sex • Parent’s phone • Hospital informations (use the mailing address and post code
box)
Specimen Quantity sufficient for testing
Specimen Quality valid for testing• Dry Specimen
• Specimen not scratched or abraded or torn
• No clotting , super saturation or uneven saturation
• No contamination or serum rings
Specimen < 14 days after date of collection
Sender Newborn Screening Office StaffTotal No. Of Valid specimen sent:Signature : Date: / / Time:
KMGC Laboratory StaffTotal No. Of Valid specimen received:Signature : Date: / / Time:
�
�
�
�
�
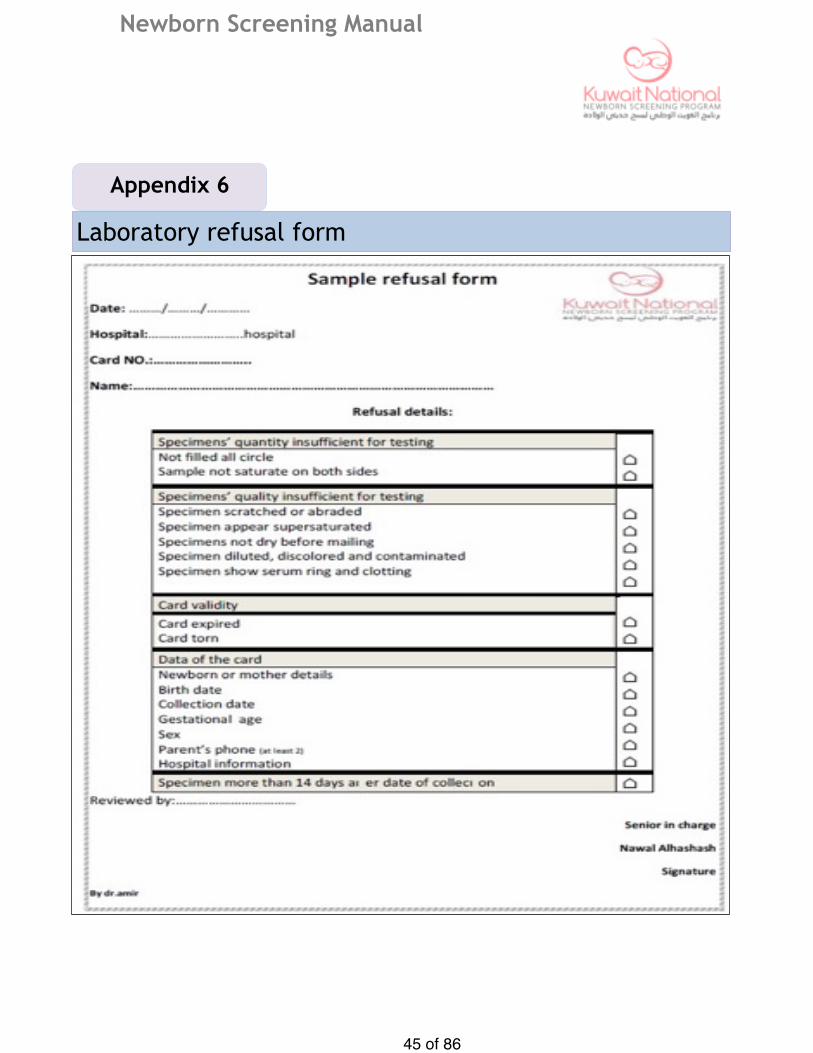
Newborn Screening Manual
� of �45 86
Appendix 6
Laboratory refusal form
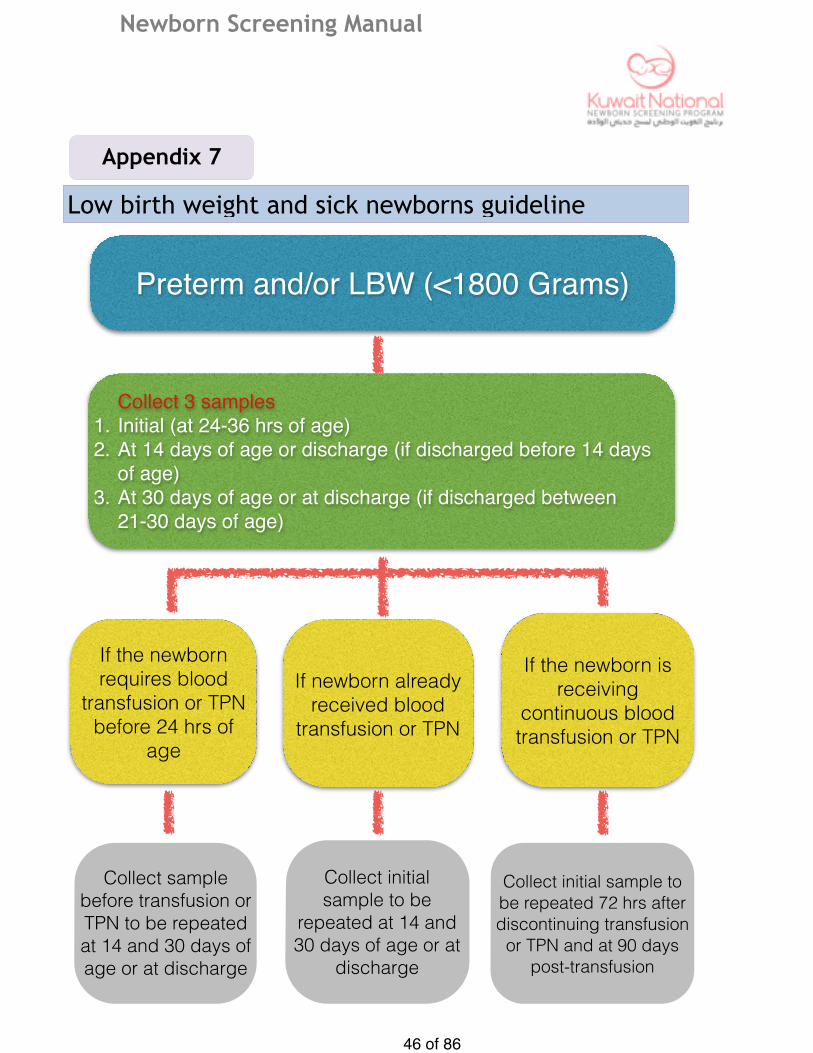
Newborn Screening Manual
� of �46 86
Appendix 7
Low birth weight and sick newborns guideline
Preterm and/or LBW (<1800 Grams)
Collect 3 samples1. Initial (at 24-36 hrs of age)2. At 14 days of age or discharge (if discharged before 14 days
of age)3. At 30 days of age or at discharge (if discharged between
21-30 days of age)
If the newborn requires blood
transfusion or TPN before 24 hrs of
age
If newborn already received blood
transfusion or TPN
If the newborn is receiving
continuous blood transfusion or TPN
Collect sample before transfusion or TPN to be repeated at 14 and 30 days of age or at discharge
Collect initial sample to be
repeated at 14 and 30 days of age or at
discharge
Collect initial sample to be repeated 72 hrs after discontinuing transfusion
or TPN and at 90 days post-transfusion

Newborn Screening Manual
� of �47 86
Appendix 8
Newborn admitted to NICU
Collect prior to treatment, if possible
Prior to 24hrsAbnormal resultNormal result
Follow Standard Protocol
Collect another specimen at 2-7 days Discharged
within 7 daysAbnormal resultNormal result
Verify prior to discharge
Follow standard Protocol
Normal result
Verify prior to discharge
Abnormal result
Follow standard Protocol
Not discharged within 7 days
Collect another specimen at discharge or at 28 days whichever
is soonest

Newborn Screening Manual
� of �48 86
At each hospital included in the newborn screening program
Collection and gathering of Newborn Screening Samples from labor room, postnatal wards and Newborn Screening Office by the responsible nursing staff
according to the standard protocol for sample collection
Checking the validity of collected samples by the responsible nursing NBS staff according to the standard check list
Registration of collected Newborn screening samples in standard registration book by the responsible NBS staff with a copy of list of collected samples
delivered to the Newborn screening co-ordinator
Delivery of samples to the Newborn screening transportation personnel by the responsible nursing staff with registration in delivery book with list of collected
samples and date and time of delivery
Newborn screening flow chart

Newborn Screening Manual
� of �49 86
Abnormal Screening Results
Confirmatory testing in NSCTL at Sabah Hospital
Consult Specialist
Retesting the same filter paper at KMGC
Newborn screening flowchart

Newborn Screening Manual
� of �50 86
At Newborn Screening Office
Recall of positive screen by the responsible nursing staff
Explanation of importance of newborn screening and screening results to parents by the responsible neonatologist
Clinical assessment of cases of positive screen
Initiation of confirmatory testing
Referral of confirmed cases to responsible specialist by
Reporting of confirmed cases to KMGC
Newborn screening flow chart

Newborn Screening Manual
� of �51 86
At Newborn Screening Flow Chart at KMGC Unit
Delivery of newborn screening samples by transportation personnel to the responsible Newborn screening laboratory staff with signing in delivery
book with date and time after ensuring the validity of received samples for testing
Processing of sample for testing
Result of Screening (notified to Newborn screening Co-ordinator at KMGC)
Normal Result Abnormal or Borderline Result
Highly Abnormal Result Unsatisfactory Specimen
Notification the NSO co-ordinator at the hospital ordered screening by phone call email and fax to collect another sample
Phone call ,email and fax the NSO co-ordinator at the hospital ordered screening
Notification the NSO co-ordinator at the hospital ordered screening
*Available through Newborn screening electronic database at KMGC
Recall the patient and, do clinical assessment, further testing and consultation with specialist if needed
If no repeat screen reminder to responsible doctor if no response, to further follow-up
Recall the patient Hospital admission if required following clinical assessment, immediate further testing and consultation with specialist

Newborn Screening Manual
� of �52 86
Newborn screening order form (KMGC)
Appendix 10
Newborn Screening Specimen collection
Cards
Amount of Collection
Cards
Newborn Screening Educational Brochures
Amount of Arabic copies
#
Amount of English copies
#
FAX OR E-MAIL YOUR ORDER TO
Kuwait Medical Genetic Center-Biochemical Screening LaboratoryAt Ghanema Al GhanemCenter for Prematures and Genetics, 2nd floorTel.: 24814328-24810563 Fax:24842073email:[email protected]
Hospital Name: ____________________________________________________Address:__________________________________________________________Contact Personnel Name: ___________________Telephone No___________
�
�

Newborn Screening Manual
� of �53 86
Please provide the number of item you are requesting
Sterile Lancet with tip (2.0-2.4 mm)
Amount Needed
Powderless GlovesAmount Needed
Sterile alcohol PrepAmount Needed
Sterile Gauze PadAmount Needed
Paper Envelops (7×10 inches Brown colour
Amount Needed
Referral form for early discharged babies
Amount of copies Needed
Parental refusal form
Amount of copies Needed
�
�
�
!
�
�
�
Newborn screening order form (each
Appendix 11

Newborn Screening Manual
� of �54 86
Test
Amino Acidemias :
Phenylketonuria (PKU)
Maple syrup urine disease (MSUD)
Homocystinuria (Cystathionine synthase def.)
Citrullinemias (ASA synthetase deficiency )
Tyrosinemias (Type 1)
Argininosuccinic Aciduria (ASA Lyase deficiency)
Organic Acidemias :
Propionic Acidemia (PA)
Methyl Malonic Acidemia (MMA)
Isovaleric Acidemia (IVA)
Glutaric Acidemia Type I (GA-I)
3-methylcrotonyl-CoA Carboxylase deficiency (3MCC)
Beta Ketothiolase deficiency (Mitochondrial Acetoacetyl CoA Thiolase deficiency)
Multiple CoA Carboxylase deficiency (MCD)
Fatty Acid Oxidation Defect :
Medium Chain Acyl Co-A Dehydrogenase Deficiency (MCAD)
Very Long Chain Acyl CoA-Dehydrogenase Deficiency (VLCAD)
Long Chain Hydroxy Acyl Dehydrogenase Deficiency (LCHAD)
Trifunctional Protein Deficiency (TEP)
3-Hydroxy-3-methylglutaryl-CoA Lyase Deiciency (3HMG)
Galactosemia
Biotinidase Deiciency
Endocrine Disorders :
Congenital Hypthyrodism
Congenital Adrenal Hyperplasia
Appendix 12
List of disorders in the newborn screening
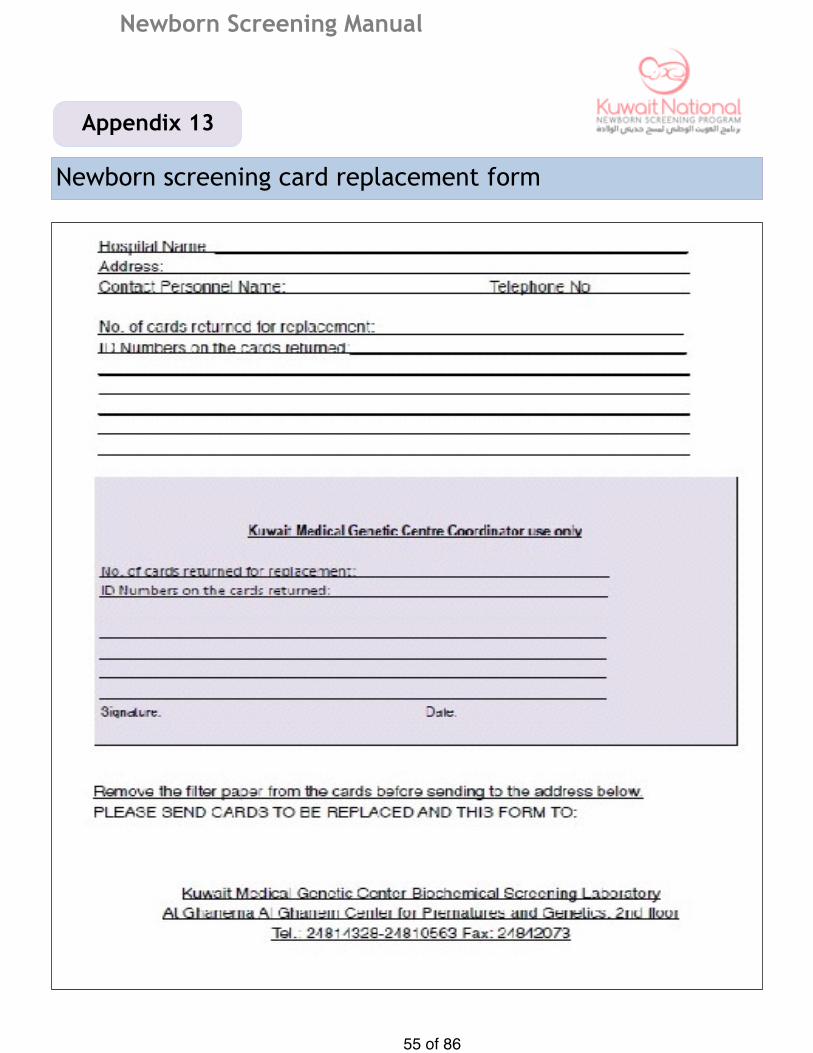
Newborn Screening Manual
� of �55 86
Newborn screening card replacement form
Appendix 13

Newborn Screening Manual
� of �56 86
Parental refusal for newborn screening
Appendix 14
إقرار برفض عمل مسح حديثي الوالدة
اقر أنا املوقع أدناه ولى أمر الطفل/ على رفضي لعمل فحص
مسح حديثي الوالدة للطفل املذكور علي مسئوليتي الخاصة وذلك رغم نصح األطباء لي بضرورة وأهمية عمل
مسح حديثي الوالدة.
املقر بما فيه
االسم:
التوقيع:
الرقم املدني:
56الطبيب املسئول:

Newborn Screening Manual
� of �57 86
Newborn Screening sample collection
Appendix 15

Newborn Screening Manual
� of �58 86
Diagram of invalid specimens
Appendix 16

Newborn Screening Manual
� of �59 86
Symptoms of screened Diseases
Appendix 17

Newborn Screening Manual
� of �60 86
Disease summary
Appendix 18
Disease Primary Analyte
Measured
Screening Can Prevent…
Treatment
Argininosuccinic Acidemia (ASA)
ASA & Citrulline …developmental delay , seizures , coma
, death
Avoid fasting , low protein diet , medication
Β-Ketothiolase (BKT) Deficency
C5OH & C5:1 … brain damage , developmental delay ,
coma , death
Avoid fasting , low protein and fat diet ,
medication
Biiotindase Deficency Biotindase … developmental delay , hypotonia , seizures , skin rash , hair loss ,
death
Biotin (vitamin) supplementation
Citrullinemia Cirtulline … developmental delay , seizures , coma ,
death
Low protein diet , avoid fasting , medication
Congenital Adrenal Hyperplasia (CAH)
17-OH progesterone
… salt-wasting crises , death
Hormone and mineral replacement
Congenital Hypothyroidism Thyroid hormones
… severe and irreversible
developmental delay , failure to thrive
Hormone replacement
Galactosemia Galactose -1-phosphate uridyl
transferase (GALT)
… failure to thrive , liver damage , sepsis,
death
Galactose restricted diet
Glutaric Acidemia Type I (GAI)
C5DC … developmental delay , spasticity ,
encephalopathy , coma , death
Avoid fasting , low protein diet , medication
Homocystinuria Methionine … developmental delay , lens dislocation ,
thrombosis
Low methionine diet , medication , dietary
supplementation
3-Hydroxy-3-methylglutaryl CoA Lyase
Deficiency
C5OH & C6DC … brain damage , developmental delay ,
death
Avoid fasting , low protein and fat diet ,
carnitine supplementation

Newborn Screening Manual
� of �61 86
Disease summary
Disease Primary Analyte
Measured
Screening Can Prevent…
Treatment
Isovaleric Acidemia (IVA) C5 … encephalopathy , neurological damage,
coma , death
Avoid fasting , low protein diet , medication
LCHAD Deficiency C16OH … cardiomyopathy , seizures ,
developmental delay , coma , death
Avoid fasting , diet low in long –chain fats
Maple Syrup Urine Disease (MSUD)
Leucine & isoleucine
.. failure to thrive , seizures ,
developmental delay , coma , death
Low protein diet , avoid fasting ,
MCAD Deficiency C8 … seizures , coma , dudden death
Avoid fasting , aggressive treatment of illness
3-Methylcrotonyl-CoA Carboxylase Deficiency
C5OH …failure to thrive , seizure , coma , death
Avoid fasting , medications , low
protein diet , supplementation
Methylmalonic Acidemia (mutase deficiency and
cobalamin defects)
C3 … failure to thrive , encephalopathy ,
coma , death
Low protein diet , avoid fasting ,, vitamin B12
supplementation
Multiiple Carbosylase Deficency
C3 & C5OH … failure to thrive , encephalopathy ,
coma , death
Biotin supplementation
Phenylketonuria Phenylalanine …severe and irreversible
developmental delay
Phenylalanine restricted diet , supplementation
Proprioic Acidemia C3 …encephalopathy , developmental delay,
coma, death
Avoid fasting , low protein diet , medication
Trifunctional protein Deficiency
C16OH ..developmental delay , failure to thrive , cardiomyopathy ,
coma , sudden death
Avoid fasting , diet low in long chain fats

Newborn Screening Manual
� of �62 86
Disease summary
Tyrosinemia Type I Tyrosine and Succinylacetone
… liver and kidney damage and sequelae ,
failure to thrive , cpagulopathy
Special diet , medication
VLCAD Deficiency C14:1 … developmental delay and failure to thrive ,
hepatomegaly , cardiomyopathy ,
coma , sudden death
Avoid fasting , special diet
Legand
Organic acid disorders
Immune deficiencies
Fatty acid oxidation disorders
Endocrine disorders
Amion acid disorders

Newborn Screening Manual
� of �63 86
General Information Brochure
Appendix 19

Newborn Screening Manual
� of �64 86

Newborn Screening Manual
� of �65 86
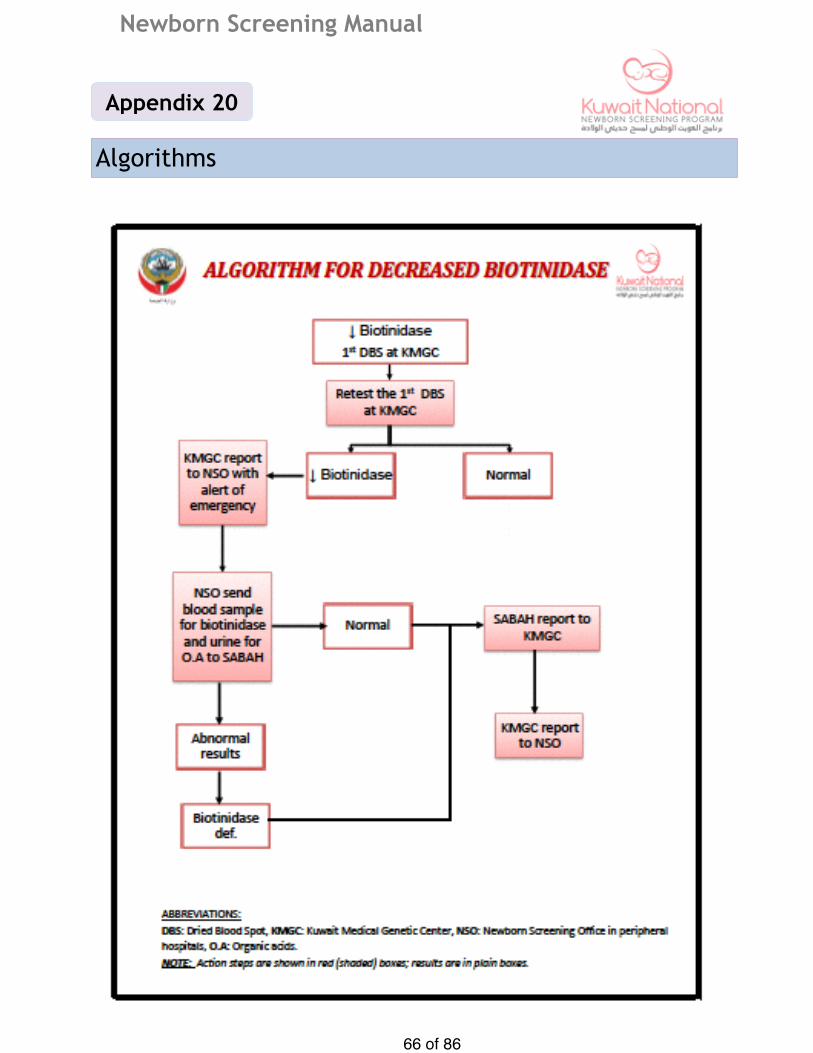
Newborn Screening Manual
� of �66 86
Algorithms
Appendix 20
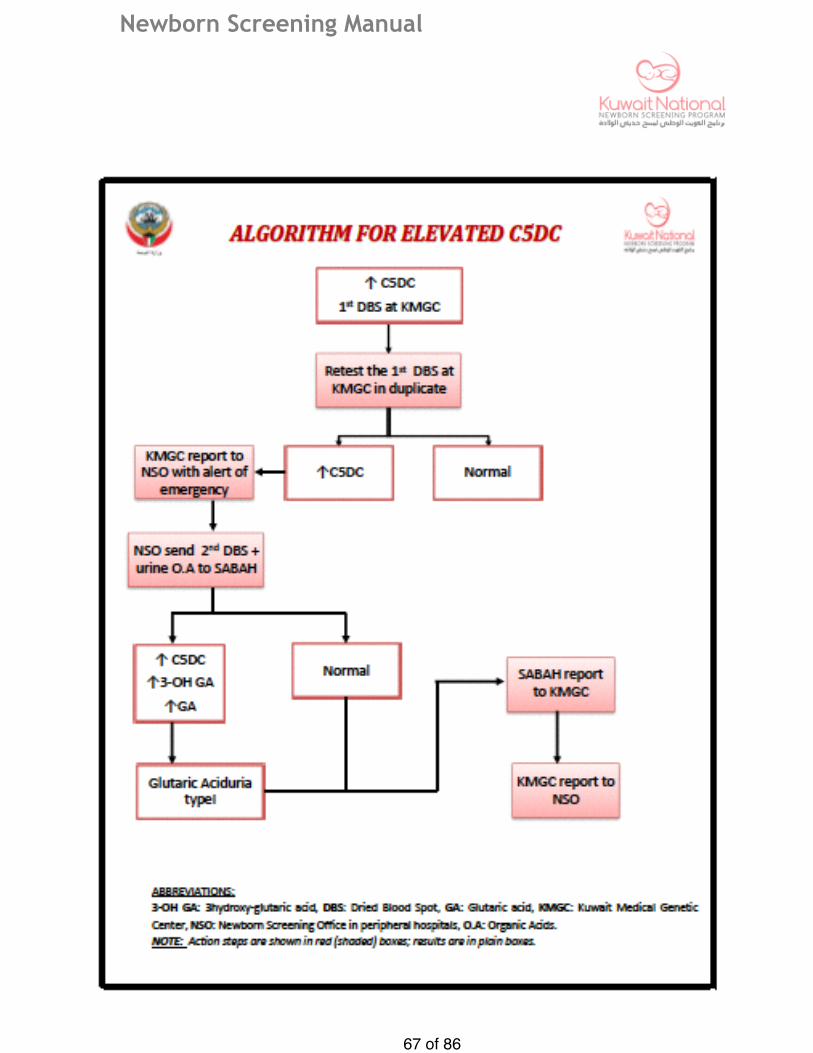
Newborn Screening Manual
� of �67 86
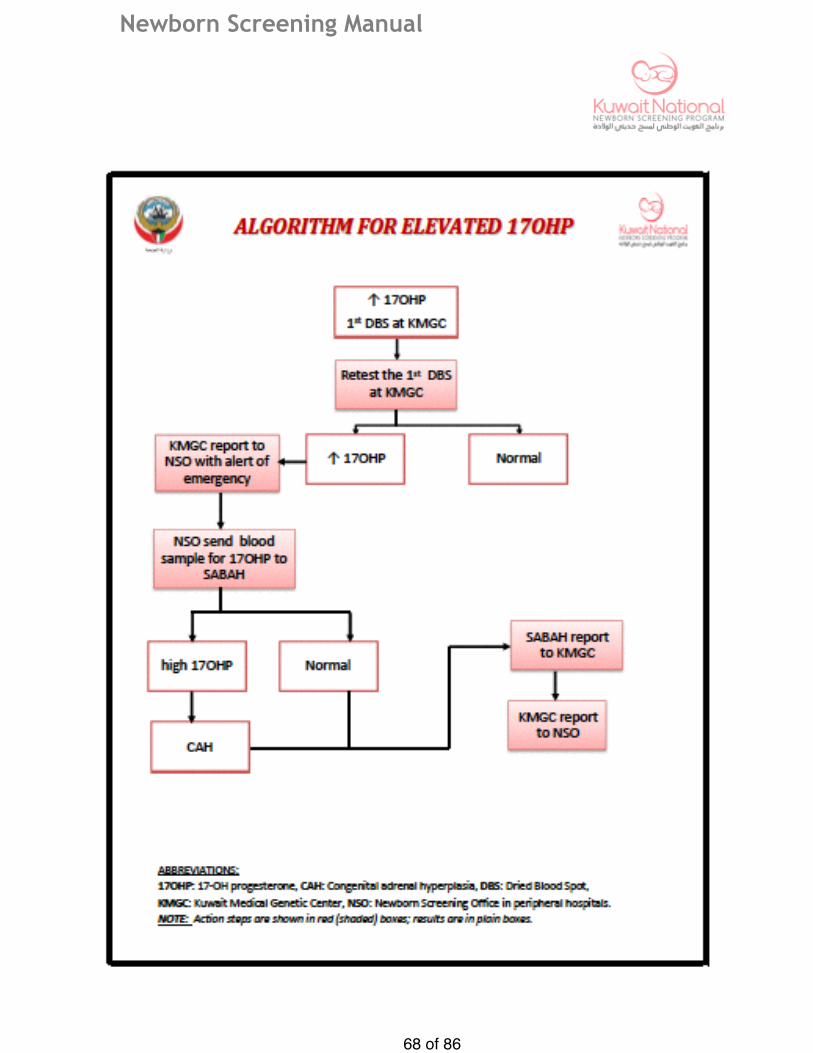
Newborn Screening Manual
� of �68 86

Newborn Screening Manual
� of �69 86

Newborn Screening Manual
� of �70 86

Newborn Screening Manual
� of �71 86
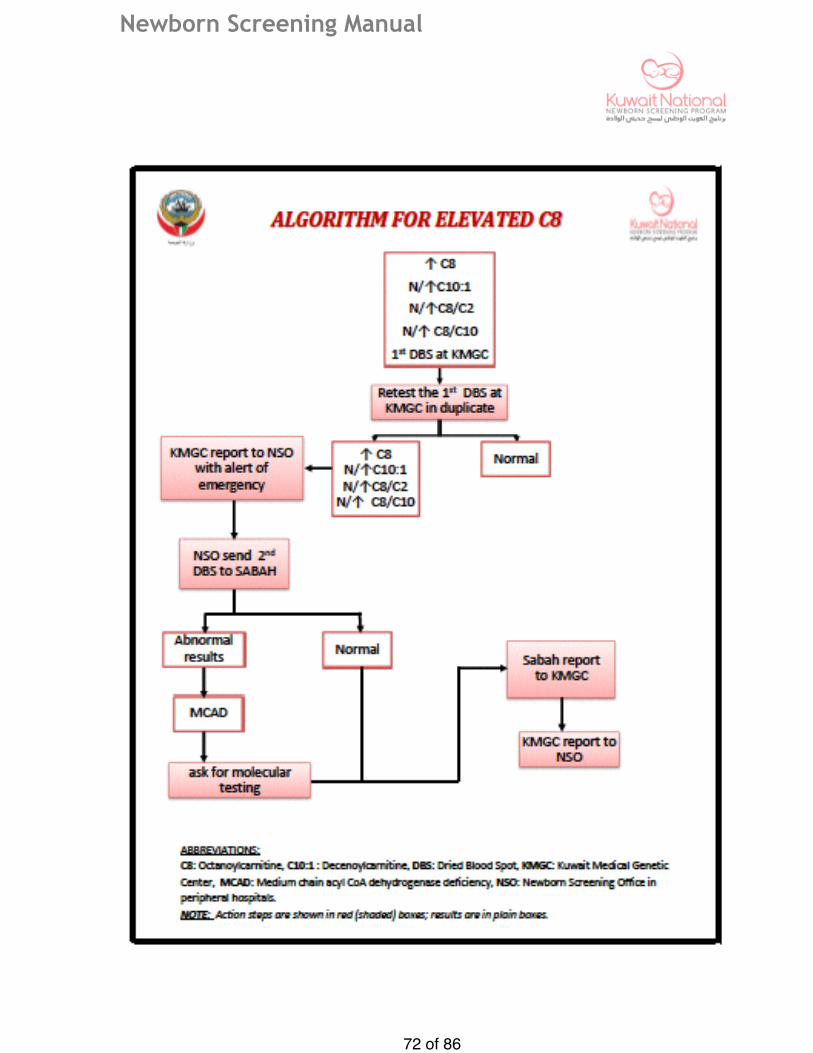
Newborn Screening Manual
� of �72 86

Newborn Screening Manual
� of �73 86

Newborn Screening Manual
� of �74 86
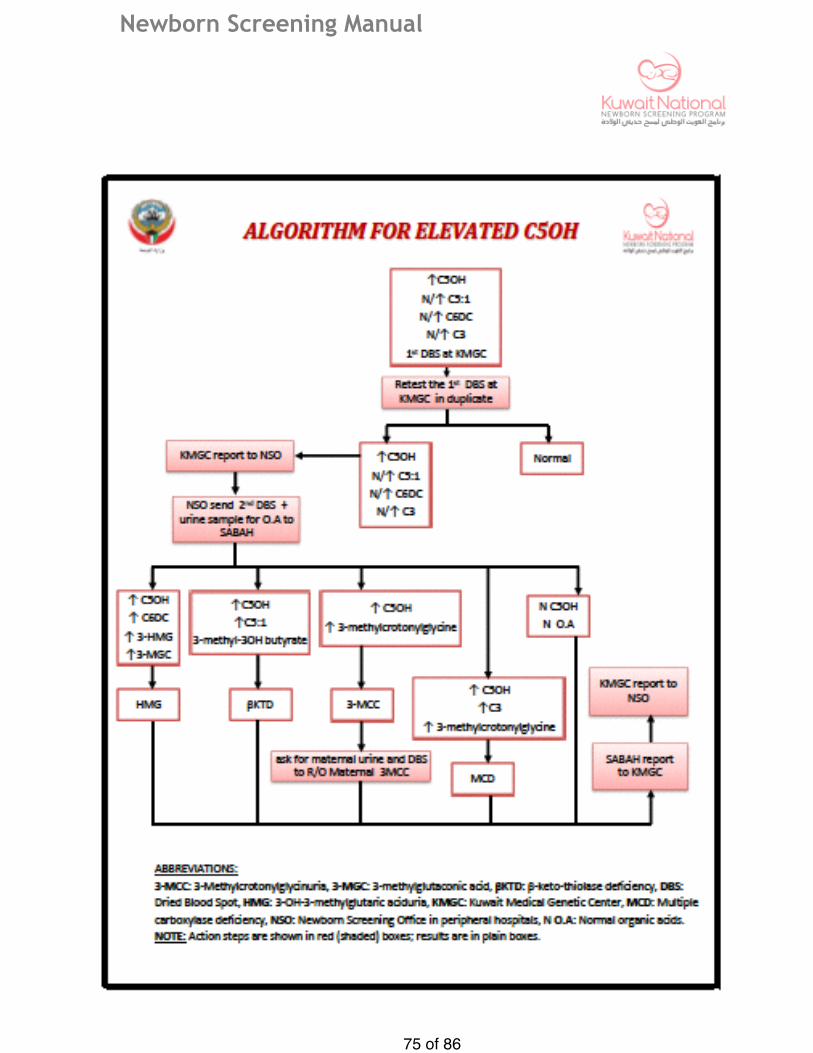
Newborn Screening Manual
� of �75 86

Newborn Screening Manual
� of �76 86

Newborn Screening Manual
� of �77 86

Newborn Screening Manual
� of �78 86
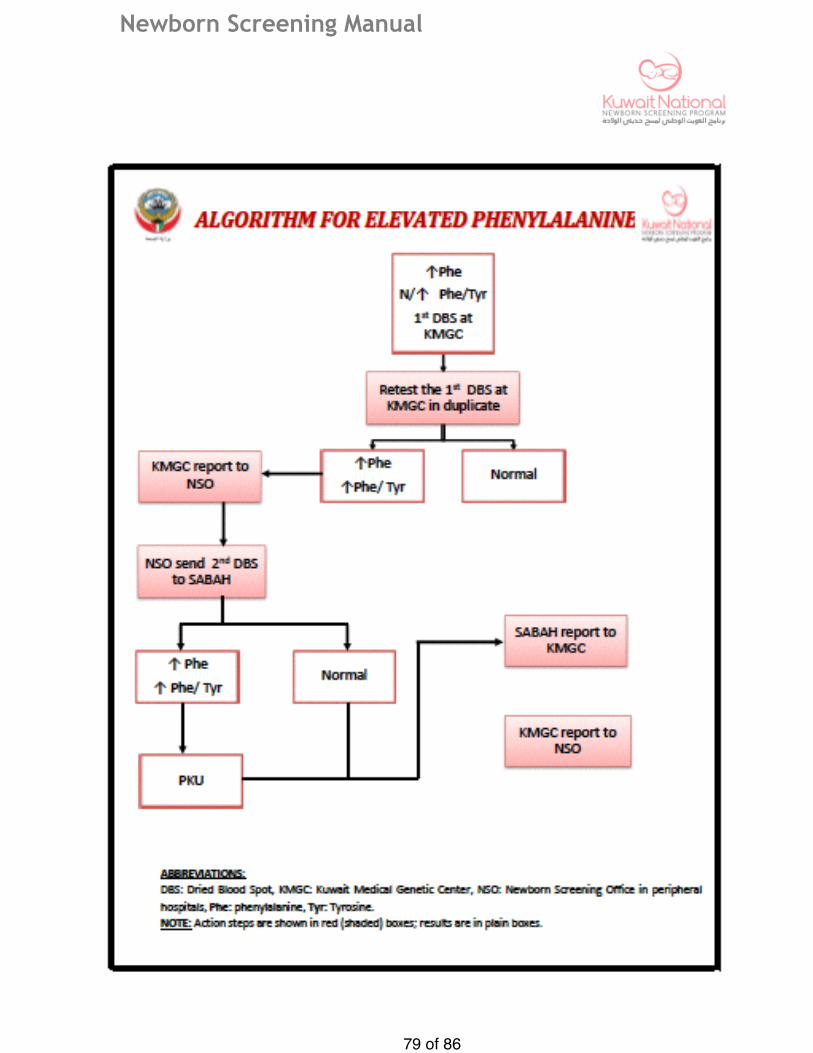
Newborn Screening Manual
� of �79 86
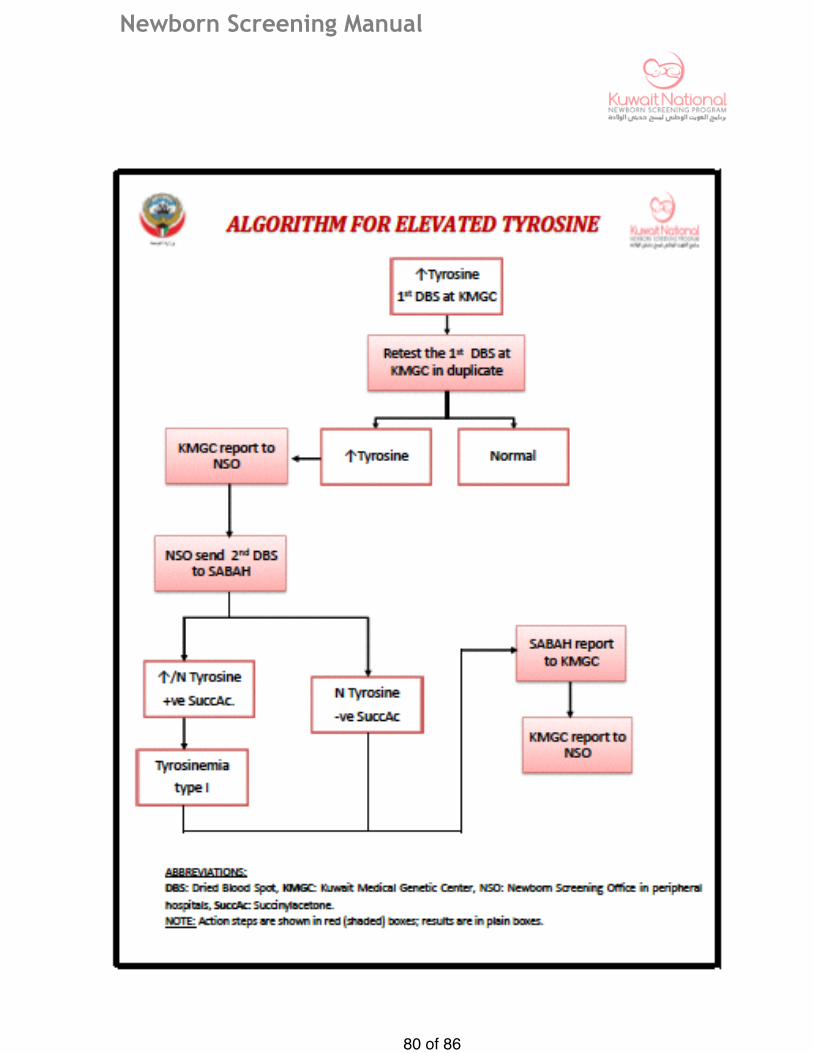
Newborn Screening Manual
� of �80 86

Newborn Screening Manual
� of �81 86
Appendix 21

Newborn Screening Manual
� of �82 86

Newborn Screening Manual
OwnershipTitle:
Newborn Screening Operational Policies & Procedures
Policy owner: Kuwait National Newborn Screening Committee
Policy Code C-NN*-01
Written by: Kuwait National Newborn Screening Committee
Effective Date:
Applies to: Staff in neonatal Unit, PNW**, LR*** and Newborn Screening Office Staff in different locations, General Paediatrician ,Nutritionist,Inborn error of metabolise specialists and Endocrinologist
Revision Date:
Approval: Kuwait National Newborn Screening Committee-Chair
Signature
Date
Approvals: The Under-Secretary of Ministry of Health
Signature
Date
� of �83 86

Newborn Screening Manual
Kuwait National Screening Committee
� of �84 86
Name Signutures
Dr Mona Abdullah Al-Khawari Pediatric and Neonate Council-Chair, Committee-Chair
Dr Laila Bastaki Director of Kuwait Genetics centre , Committe-Co-chair
Eng. Farah Dashti Director of Equipment Directoriate
Dr Ibraheem Al-Muzairi Director of Central Laboratory Services
Mr. Ashraf Alghout Head of Accounting-MOH
Dr Neran Al-Naqeeb Pediatric and Neonate Chair-Adan Hospital
Dr Rima Al-Sawan Neonate Chair-Farwanyia Hospital
Dr Nawal Al-Kazimi Consultant Neonatologist-Maternity Hospital
Dr Nawal Makhseed Consultant Inborn Error of metabolism -Jahra Hospital
Dr Jassem Khalefa Abbas Senior Specialist, Sabah Hospital Laboratory
Dr Ahmad Al-Saraf Head of Kuwait Cancer Center Laboratories

Newborn Screening Manual
This Policy published and edited by :
� of �85 86
Name Signutures
Dr Mona Abdullah Al-Khawari Pediatric and Neonate Council-Chair Committee-Chair
Dr Laila Bastaki Director of Kuwait Genetics centre Committe-Co-chair
Dr Neran Al-Naqeeb Pediatric and Neonate Chair-Adan Hospital
Dr Rima Al-Sawan Neonate Chair-Farwanyia Hospital
Dr Nawal Al-Kazimi Consultant Neonatologist-Maternity Hospital
Dr Nawal Makhseed Consultant Inborn Error of metabolism -Jahra Hospital
Dr Jassem Khalefa Abbas Senior Specialist, Sabah Hospital Laboratory
Dr Ahmad Al-Saraf Head of Kuwait Cancer Center Laboratories

Newborn Screening Manual
Abbreviations:
� of �86 86
CLSI: Clinical and Laboratory standard Institute
DBS: Dried Blood Spots
KMGC: Kuwait Medical Genetics Center
LR: Labor Room
MOH: Ministry Of Health
NBS: Newborn Screening
NICU: Newborn Intense Care Unit
NNSP: National Newborn Screening Program
NSL: Newborn Screening Laboratory
NSO: Newborn Screening Office
NSU: Newborn Screening Unit
PNW: Post Natal Wards
TPN: Total Parenteral Nutrition
NSCTL Newborn screening Confirmatory Testing Laboratory at Sabah hospital