neil shah, md phd edward s. ageno distinguished professor in hematology/oncology ucsf school of...
TRANSCRIPT
Neil Shah, MD PhDEdward S. Ageno Distinguished Professor in
Hematology/OncologyUCSF School of MedicineSan Francisco, California
Chronic Myeloid Leukemia - Hematology Highlights -
Chronic Phase CML Treatment Landscape Evolution
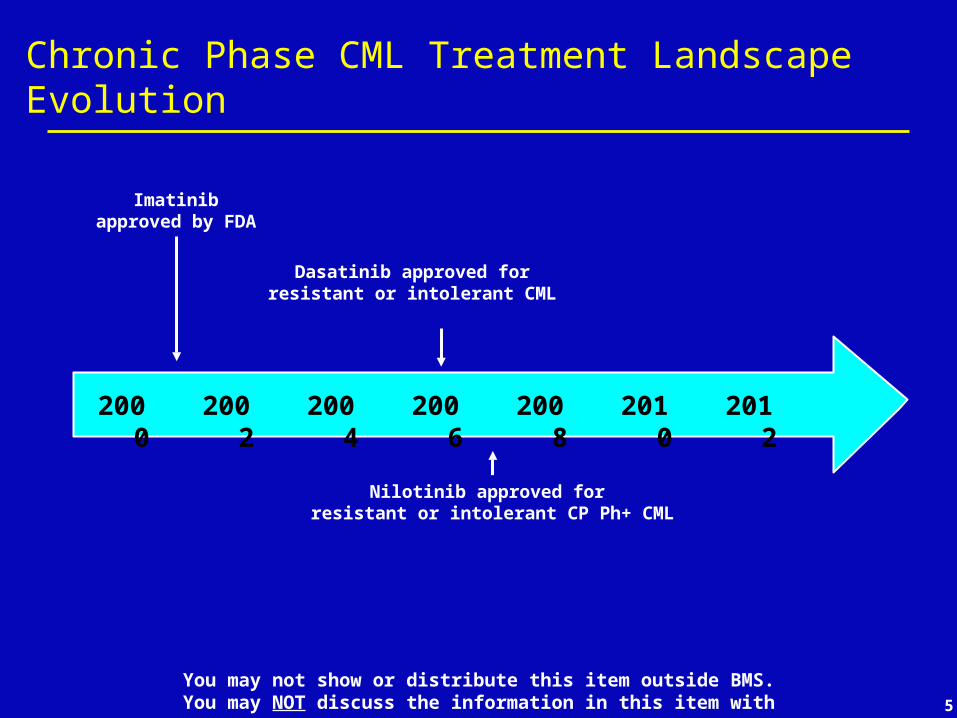
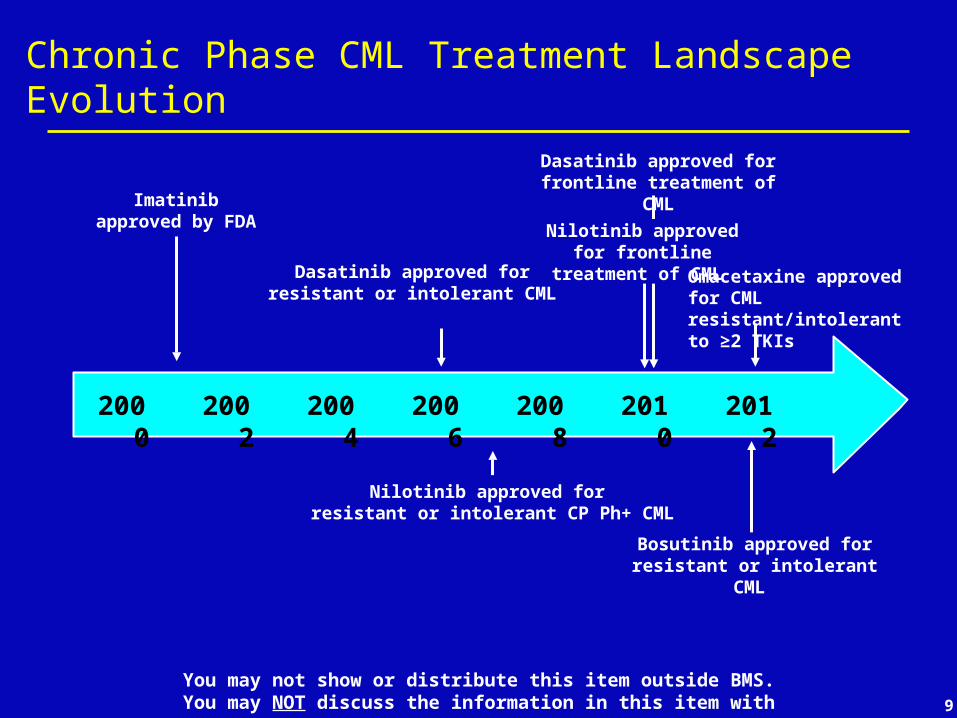
Chronic Phase CML Treatment Landscape Evolution
Imatinibapproved by FDA
2000 2010 20122008200620042002
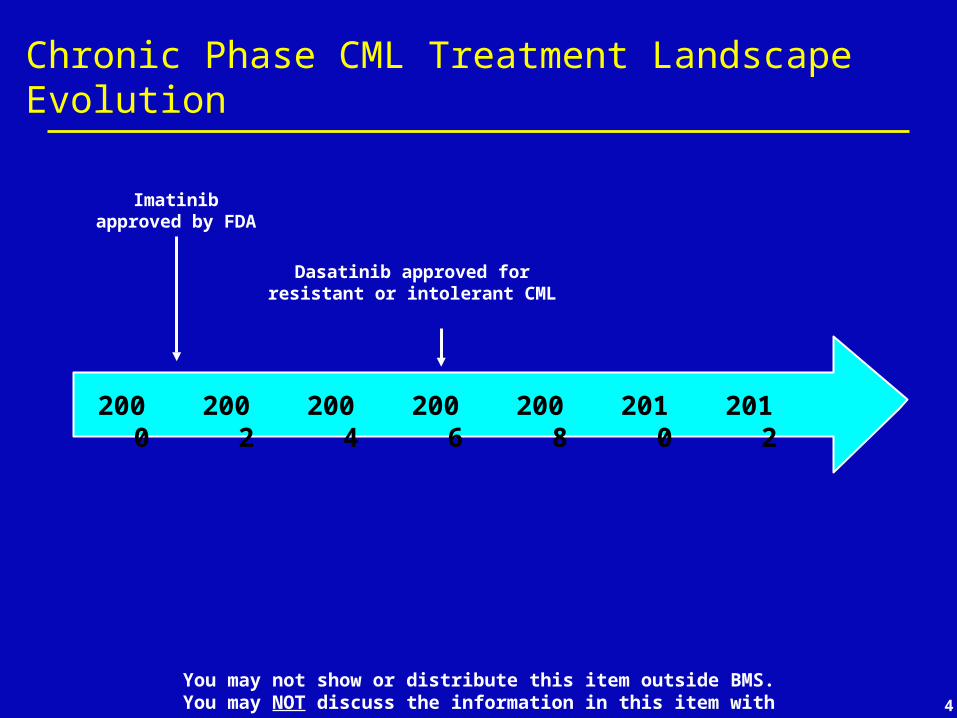
Chronic Phase CML Treatment Landscape Evolution
Imatinibapproved by FDA
Dasatinib approved for resistant or intolerant CML
2000 2010 20122008200620042002
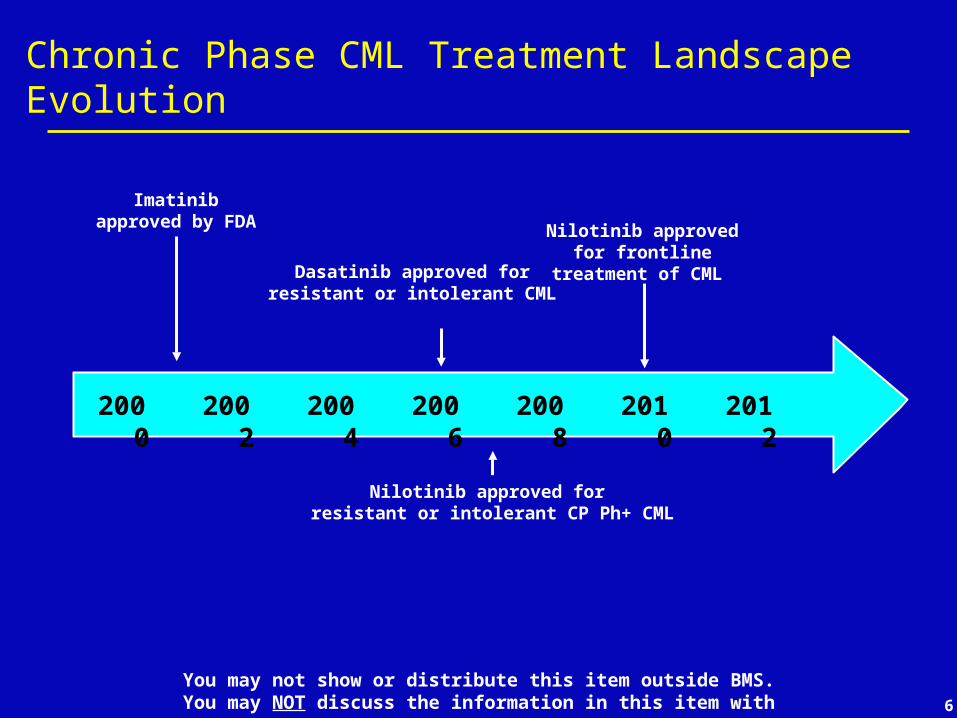
Chronic Phase CML Treatment Landscape Evolution
Imatinibapproved by FDA
Nilotinib approved for resistant or intolerant CP Ph+ CML
Dasatinib approved for resistant or intolerant CML
2000 2010 20122008200620042002
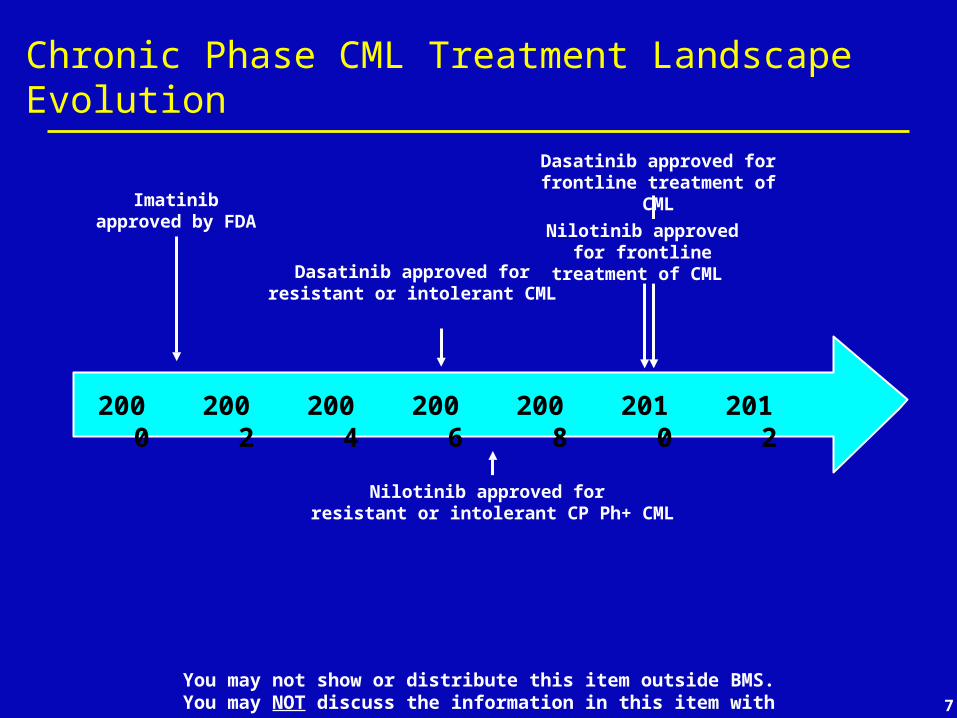
Chronic Phase CML Treatment Landscape Evolution
Imatinibapproved by FDA
Nilotinib approved for resistant or intolerant CP Ph+ CML
Nilotinib approved for frontline treatment of CML
Dasatinib approved for resistant or intolerant CML
2000 2010 20122008200620042002
Chronic Phase CML Treatment Landscape Evolution
Imatinibapproved by FDA
Nilotinib approved for resistant or intolerant CP Ph+ CML
Nilotinib approved for frontline treatment of CML
Dasatinib approved for resistant or intolerant CML
Dasatinib approved for frontline treatment of CML
2000 2010 20122008200620042002
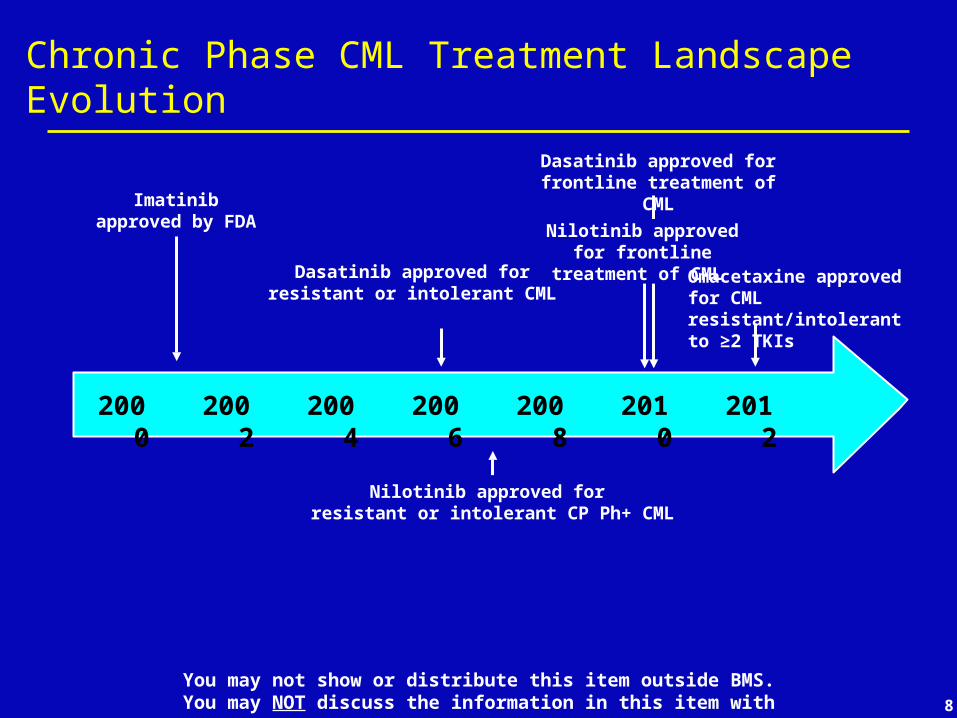
Chronic Phase CML Treatment Landscape Evolution
Imatinibapproved by FDA
Nilotinib approved for resistant or intolerant CP Ph+ CML
Nilotinib approved for frontline treatment of CML
Dasatinib approved for resistant or intolerant CML
Dasatinib approved for frontline treatment of CML
2000 2010 20122008200620042002
Omacetaxine approved for CML resistant/intolerant to ≥2 TKIs
Chronic Phase CML Treatment Landscape Evolution
Imatinibapproved by FDA
Nilotinib approved for resistant or intolerant CP Ph+ CML
Nilotinib approved for frontline treatment of CML
Dasatinib approved for resistant or intolerant CML
Dasatinib approved for frontline treatment of CML
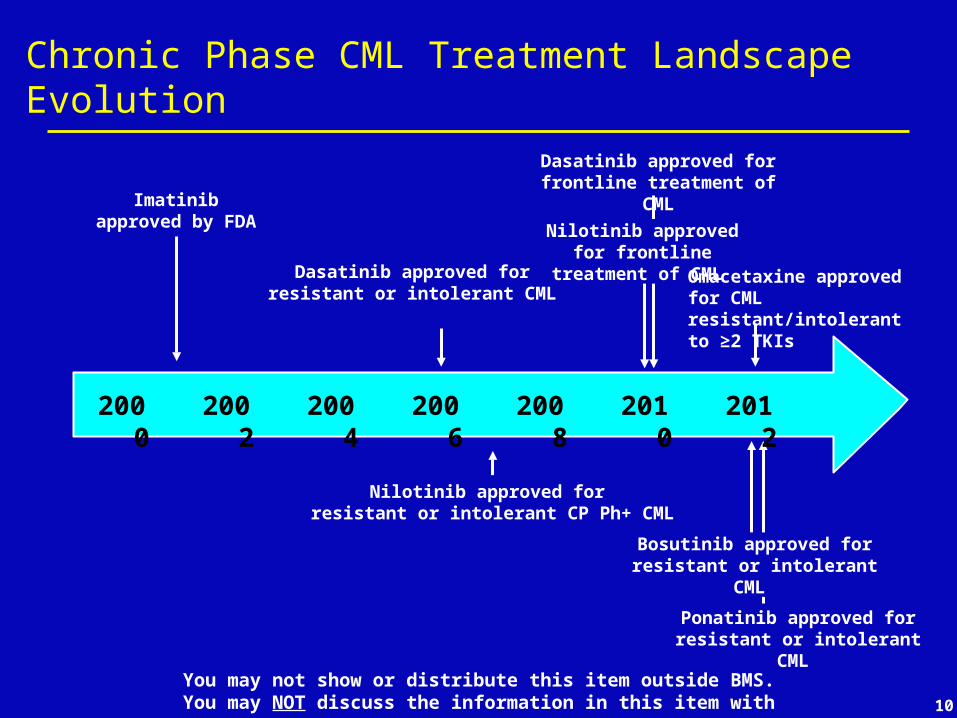
Bosutinib approved for resistant or intolerant CML
2000 2010 20122008200620042002
Omacetaxine approved for CML resistant/intolerant to ≥2 TKIs
Chronic Phase CML Treatment Landscape Evolution
Imatinibapproved by FDA
Nilotinib approved for resistant or intolerant CP Ph+ CML
Nilotinib approved for frontline treatment of CML
Dasatinib approved for resistant or intolerant CML
Ponatinib approved for resistant or intolerant CML
Dasatinib approved for frontline treatment of CML
Bosutinib approved for resistant or intolerant CML
2000 2010 20122008200620042002
Omacetaxine approved for CML resistant/intolerant to ≥2 TKIs
Chronic Phase CML - Goals of Therapy
Chronic Phase CML - Goals of Therapy
• Prevention of disease transformation to blast phase Chronic phase CML is not immediately life-threatening, so if
blast phase can be prevented indefinitely, patients will be “functionally” cured
May require lifelong therapy• Chronically administered therapies should ideally be well-
tolerated and minimally intrusive to everyday life
Chronic Phase CML - Goals of Therapy
• Prevention of disease transformation to blast phase Chronic phase CML is not immediately life-threatening, so if
blast phase can be prevented indefinitely, patients will be “functionally” cured
May require lifelong therapy• Chronically administered therapies should ideally be well-
tolerated and minimally intrusive to everyday life
• True disease cure - enabling patients to be off all therapies Allogeneic stem cell transplantation – best established
curative therapy (~70% cure rate)• ~20% risk of short-term death (1-2 years)• ~50-60% risk of chronic graft vs host disease
• “trading one disease for another”

MONITORING DISEASE IN PATIENTS WITH CML
MONITORING DISEASE IN PATIENTS WITH CML
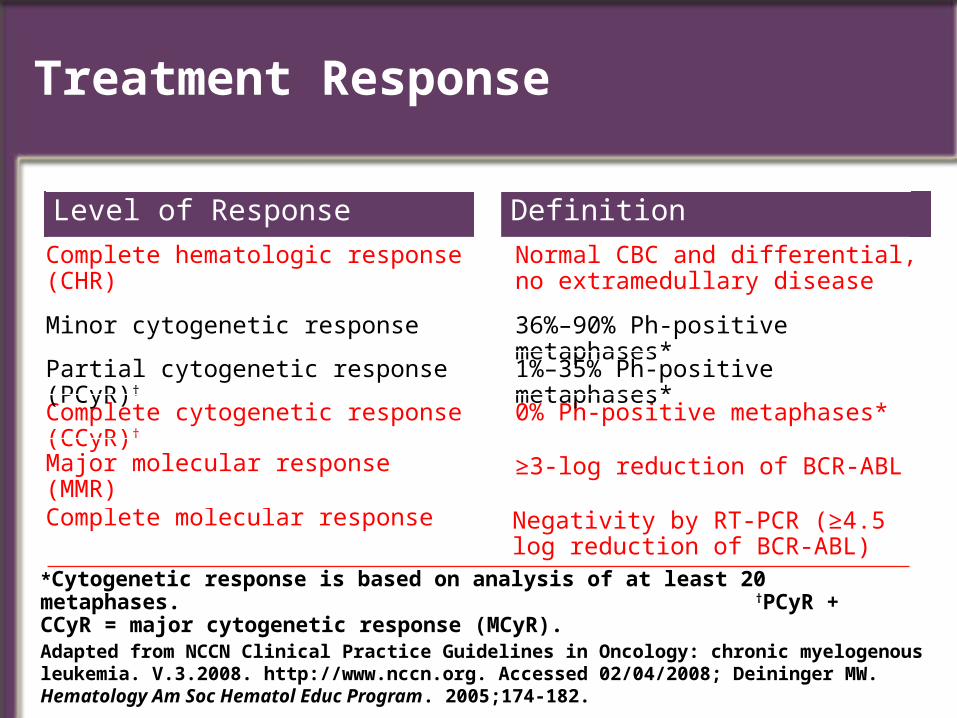
Normal CBC and differential, no extramedullary disease
Complete hematologic response (CHR)
DefinitionLevel of Response
Negativity by RT-PCR (≥4.5 log reduction of BCR-ABL)
Complete molecular response
≥3-log reduction of BCR-ABLMajor molecular response (MMR)
0% Ph-positive metaphases*Complete cytogenetic response (CCyR)†
1%–35% Ph-positive metaphases*Partial cytogenetic response (PCyR)†
36%–90% Ph-positive metaphases*Minor cytogenetic response
Treatment Response
Adapted from NCCN Clinical Practice Guidelines in Oncology: chronic myelogenous leukemia. V.3.2008. http://www.nccn.org. Accessed 02/04/2008; Deininger MW. Hematology Am Soc Hematol Educ Program. 2005;174-182.
*Cytogenetic response is based on analysis of at least 20 metaphases. †PCyR + CCyR = major cytogenetic response (MCyR).
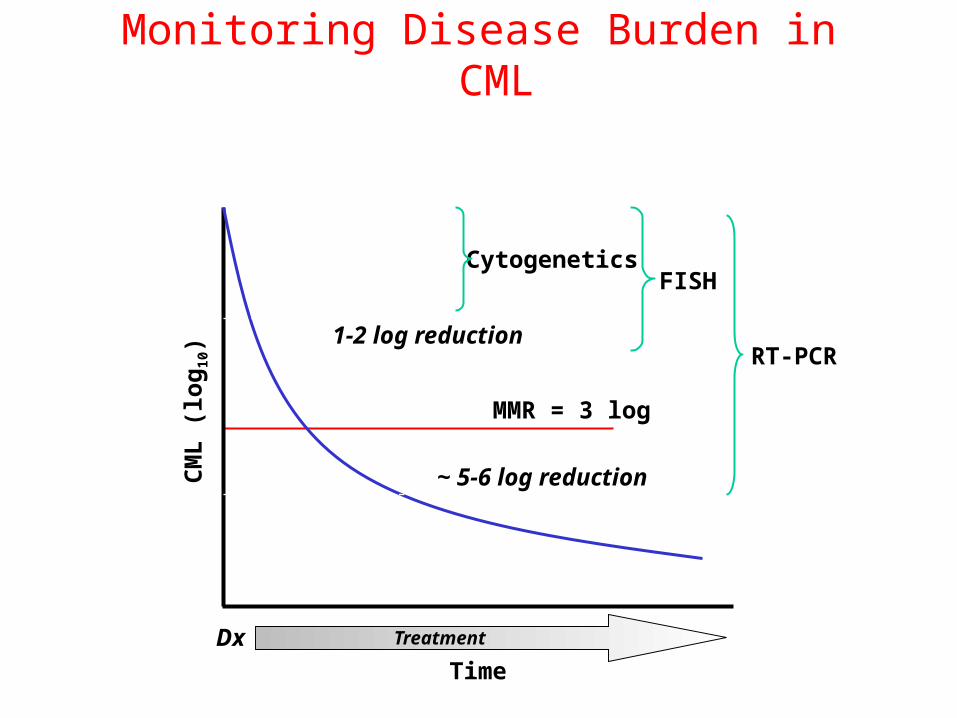
Monitoring Disease Burden in CML
Time
Dx
CytogeneticsFISH
RT-PCR
Treatment
CM
L (
log
10) 1-2 log reduction
~ 5-6 log reduction
MMR = 3 log
IMATINIB AS FRONTLINE THERAPY FOR CML
IMATINIB AS FRONTLINE THERAPY FOR CML
IMATINIB AS FRONTLINE THERAPY FOR CML
IMATINIB AS FRONTLINE THERAPY FOR CML
7-8 year update of newly-diagnosed Chronic Phase CML patients treated
with 400 mg daily imatinib
O’Brien et al. ASH 2008, Abstract 186
19
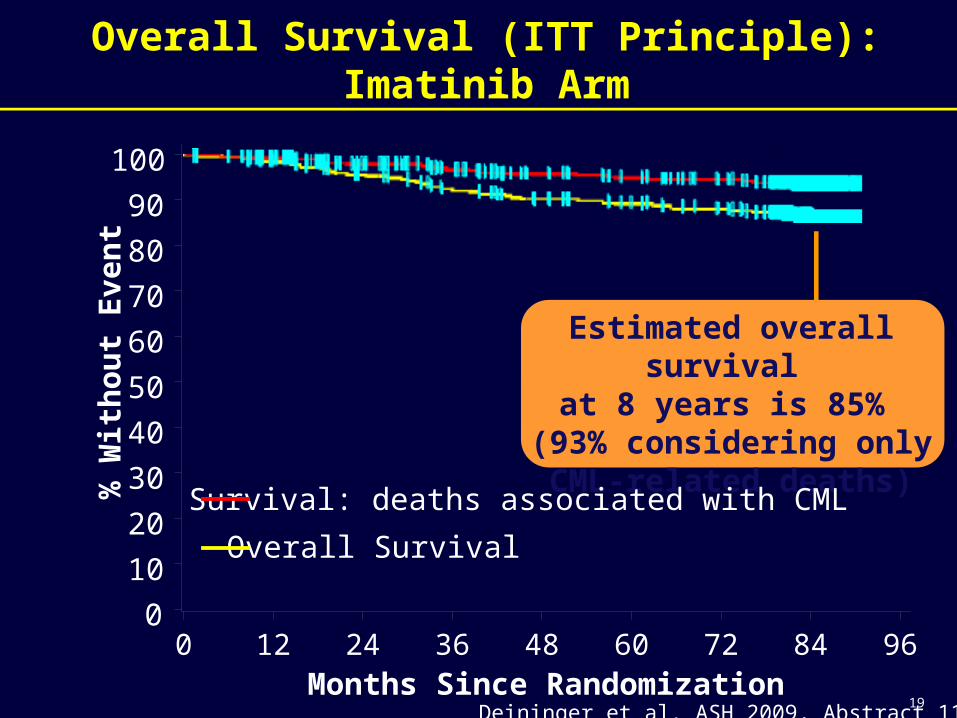
Overall Survival (ITT Principle): Imatinib Arm
Estimated overall survival at 8 years is 85%
(93% considering only CML-related deaths)
Survival: deaths associated with CML
Overall Survival
% W
ith
ou
t E
ve
nt
0
10
20
30
40
50
60
70
80
90
100
Months Since Randomization0 12 24 36 48 60 72 84 96
Deininger et al. ASH 2009, Abstract 1126
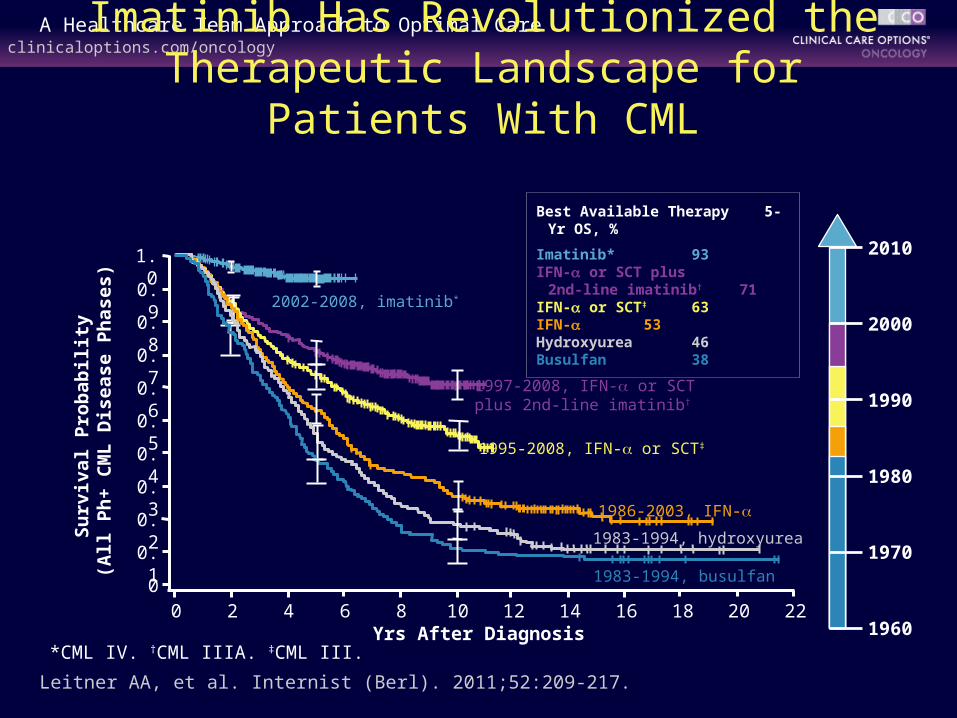
Leitner AA, et al. Internist (Berl). 2011;52:209-217.
Yrs After Diagnosis
Su
rviv
al P
rob
abil
ity
(All
Ph
+ C
ML
Dis
ease
Ph
ases
)
0 2 64 8 10 16 18 20 2212 140
0.2
0.1
0.5
0.6
0.7
0.8
0.9
1.0
0.3
0.4 1995-2008, IFN- or SCT‡
1986-2003, IFN-
1983-1994, busulfan
1983-1994, hydroxyurea
1997-2008, IFN- or SCT plus 2nd-line imatinib†
2002-2008, imatinib*
Best Available Therapy 5-Yr OS, %
Imatinib* 93IFN- or SCT plus
2nd-line imatinib† 71IFN- or SCT‡ 63IFN- 53Hydroxyurea 46Busulfan 38
1970
2000
1990
1980
1960
2010
Imatinib Has Revolutionized the Therapeutic Landscape for Patients With CML
*CML IV. †CML IIIA. ‡CML III.
IMATINIB DISCONTINUATION STUDIESIMATINIB DISCONTINUATION STUDIES
Can imatinib be safely stopped in patients with deep molecular
responses?
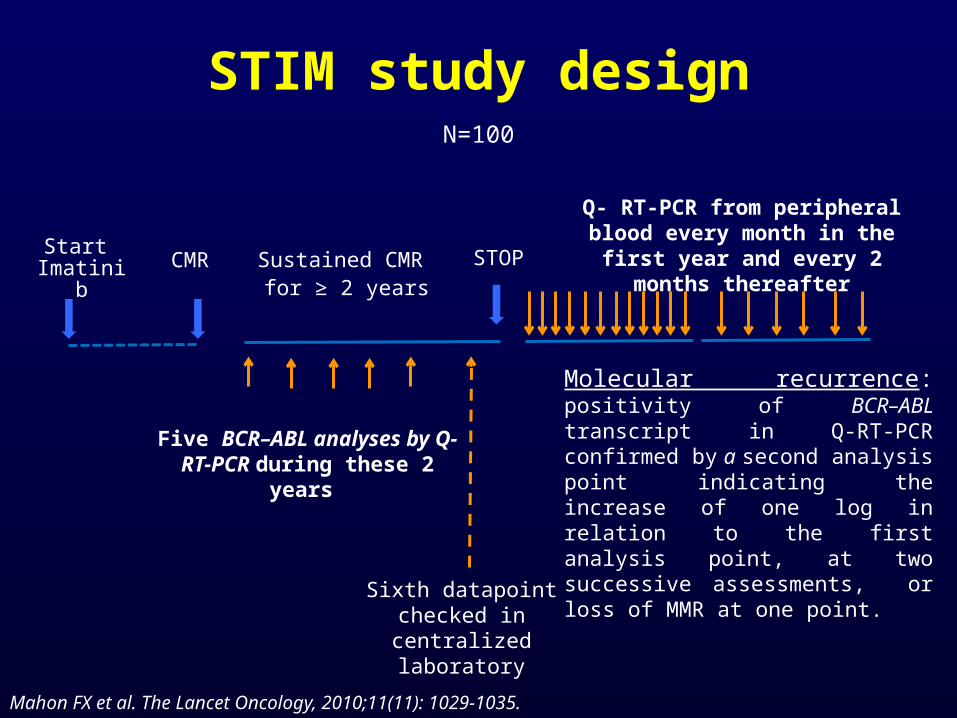
STIM study designN=100
STOPSustained CMR for ≥ 2 years
Start Imatinib
CMR
Q- RT-PCR from peripheral blood every month in the first year and
every 2 months thereafter
Five BCR–ABL analyses by Q- RT-PCR during these 2 years
Sixth datapoint checked in centralized laboratory
Mahon FX et al. The Lancet Oncology, 2010;11(11): 1029-1035.
Molecular recurrence: positivity of BCR–ABL transcript in Q-RT-PCR confirmed by a second analysis point indicating the increase of one log in relation to the first analysis point, at two successive assessments, or loss of MMR at one point.
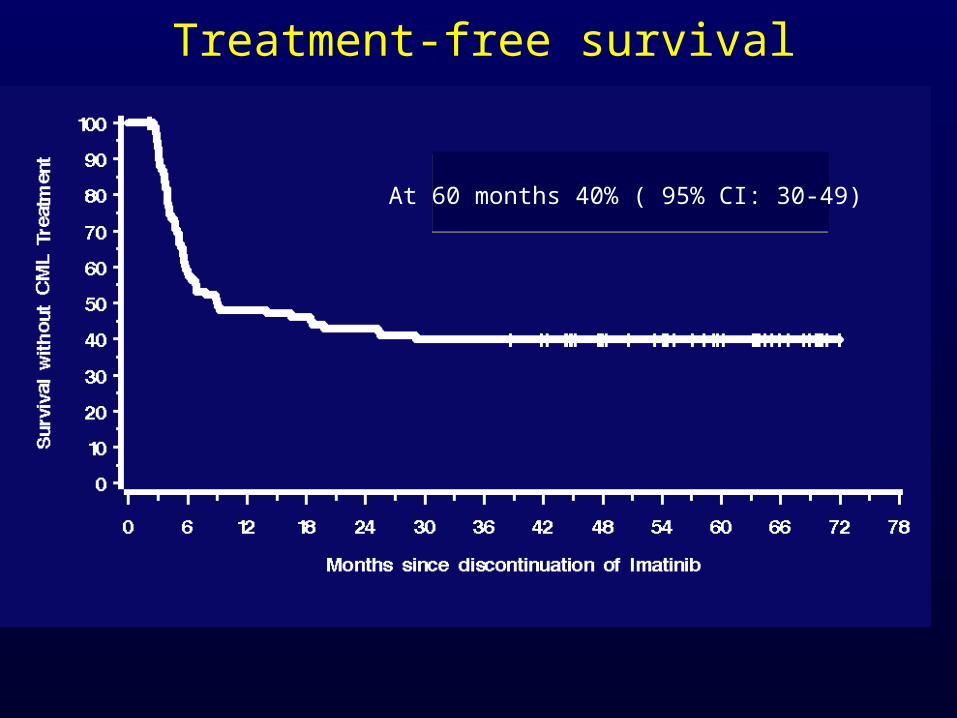
Treatment-free survival
At 60 months 40% ( 95% CI: 30-49)
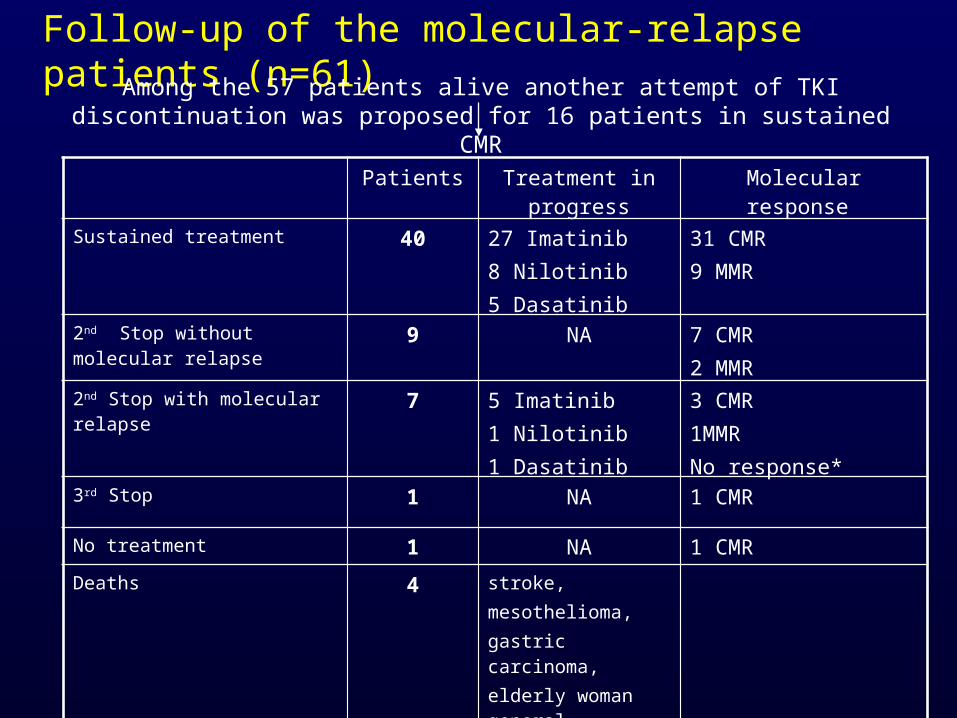
Follow-up of the molecular-relapse patients (n=61)
Among the 57 patients alive another attempt of TKI discontinuation was proposed for 16 patients in sustained CMR
Patients Treatment in progress
Molecular response
Sustained treatment 40 27 Imatinib 8 Nilotinib5 Dasatinib
31 CMR 9 MMR
2nd Stop without molecular relapse
9 NA 7 CMR 2 MMR
2nd Stop with molecular relapse 7 5 Imatinib1 Nilotinib1 Dasatinib
3 CMR 1MMR No response*
3rd Stop 1 NA 1 CMR
No treatment 1 NA 1 CMR
Deaths 4 stroke, mesothelioma, gastric carcinoma, elderly woman general deterioration
• With longer follow-up:• Approximately 40 percent of patients in CMR are able to
discontinue imatinib without suffering molecular relapse• Second and third attempts at treatment discontinuation in
patients who have suffered molecular relapse are ongoing
• Discontinuation should only be performed in the context of a clinical trial with strict molecular monitoring and plans for careful long-term follow up.
• Many ongoing trials are assessing TKI cessation in patients with sustained CMR.
• A very long-term follow-up of various cessation studies necessary to affirm CML cure.
Conclusions

Imatinib: the gold medal winner?
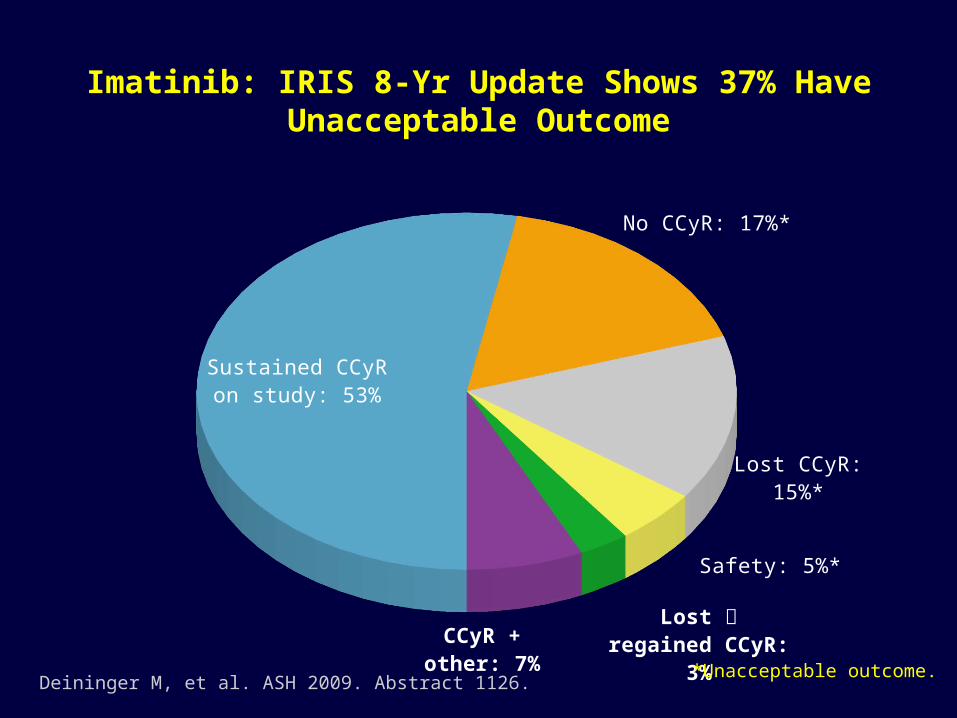
Sustained CCyR on study: 53%
No CCyR: 17%*
Lost CCyR: 15%*
Safety: 5%*
Lost regained CCyR: 3%CCyR +
other: 7%
Imatinib: IRIS 8-Yr Update Shows 37% Have Unacceptable Outcome
*Unacceptable outcome.Deininger M, et al. ASH 2009. Abstract 1126.
28
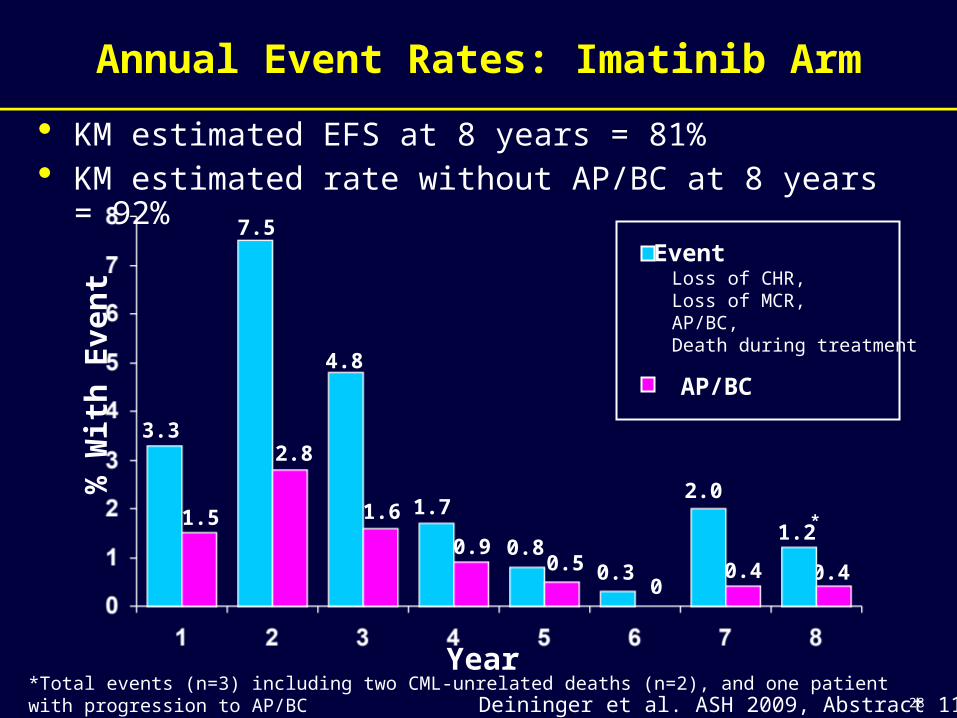
Annual Event Rates: Imatinib Arm
Year
% W
ith
Ev
en
t
EventLoss of CHR,Loss of MCR,AP/BC,Death during treatment
AP/BC
3.3
7.5
4.8
1.71.5
2.8
1.6
0.9 0.80.30.5
0
2.0
0.4
• KM estimated EFS at 8 years = 81%• KM estimated rate without AP/BC at 8 years = 92%
*Total events (n=3) including two CML-unrelated deaths (n=2), and one patient with progression to AP/BC
*
Deininger et al. ASH 2009, Abstract 1126
0.4
1.2
29
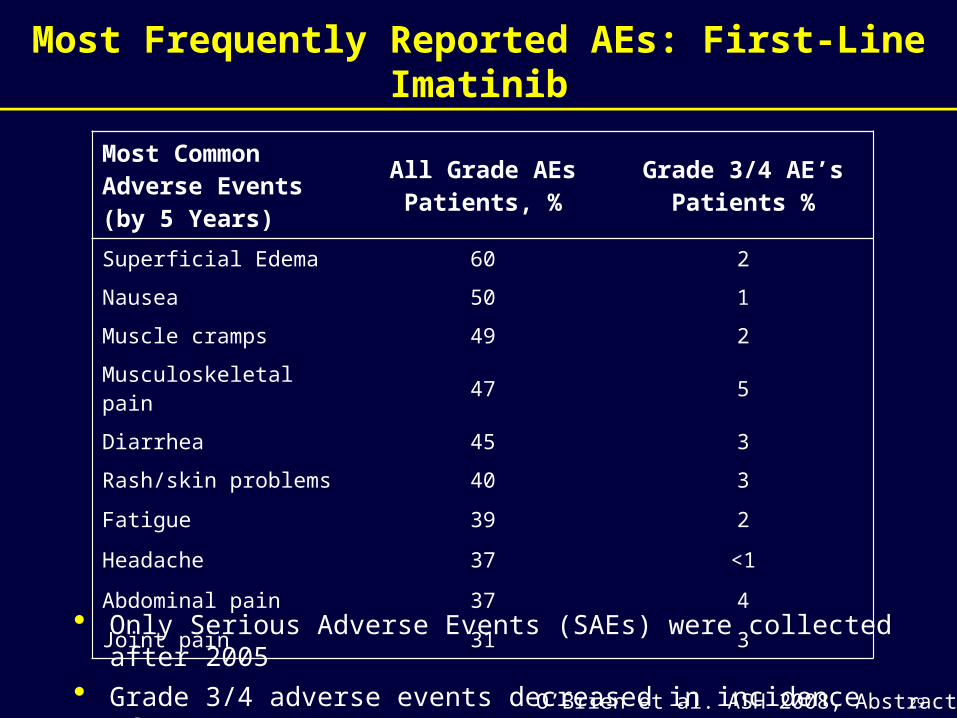
Most Frequently Reported AEs: First-Line Imatinib
Most Common Adverse Events (by 5 Years)
All Grade AEs Patients, %
Grade 3/4 AE’s Patients %
Superficial Edema 60 2
Nausea 50 1
Muscle cramps 49 2
Musculoskeletal pain 47 5
Diarrhea 45 3
Rash/skin problems 40 3
Fatigue 39 2
Headache 37 <1
Abdominal pain 37 4
Joint pain 31 3
• Only Serious Adverse Events (SAEs) were collected after 2005
• Grade 3/4 adverse events decreased in incidence after years 1-2O’Brien et al. ASH 2008, Abstract 186
Imatinib - Conclusions
• Imatinib (400 mg daily) remains the standard dose for chronic phase CML patients
• 85% overall survival with imatinib exceeds that of all other CML therapies, with 7% patients dying from CML after eight years
• 82% of patients treated with imatinib achieved a CCyR 55% of all imatinib randomized patients are still on study
treatment, and nearly all of these are in CCyR
• Responses are typically durable, and the annual risk of progression generally decreases with time
• Some patients appear to be able to have prolonged treatment-free molecular remissions
• No new safety findings seen with long term follow-up
Imatinib: maybe the silver medal winner?
IMATINIB-RESISTANT DISEASEIMATINIB-RESISTANT DISEASE
How is it defined?
Imatinib Resistance in Chronic Phase CML Definitions
• Primary resistance: lack of an acceptable initial response Primary hematologic resistance – rare Primary cytogenetic resistance – ~35% of patients
• lack of PCyR (≤35% Ph) by 3 months
• lack of CCyR (0% Ph) by 12 - 18 months
Imatinib Resistance in Chronic Phase CML Definitions
• Primary resistance: lack of an acceptable initial response Primary hematologic resistance – rare Primary cytogenetic resistance – ~35% of patients
• lack of PCyR (≤35% Ph) by 3 months
• lack of CCyR (0% Ph) by 12 - 18 months
• Secondary resistance: loss of an established initial response (relapse despite tx) Hematologic Relapse – WBC >nl and increasing) Cytogenetic Relapse – ≥30% increase in Ph+ metaphases Molecular Relapse – confirmed 1-log increase in BCR-ABL transcript level with
lack/loss of MMR
Primary resistance is a risk factor for the development of secondary resistance
Imatinib Resistance in Chronic Phase CML Definitions
• Primary resistance: lack of an acceptable initial response Primary hematologic resistance – rare Primary cytogenetic resistance – ~35% of patients
• lack of PCyR (≤35% Ph) by 3 months
• lack of CCyR (0% Ph) by 12 - 18 months
• Secondary resistance: loss of an established initial response (relapse despite tx) Hematologic Relapse – WBC >nl and increasing) Cytogenetic Relapse – ≥30% increase in Ph+ metaphases Molecular Relapse – confirmed 1-log increase in BCR-ABL transcript level with
lack/loss of MMR
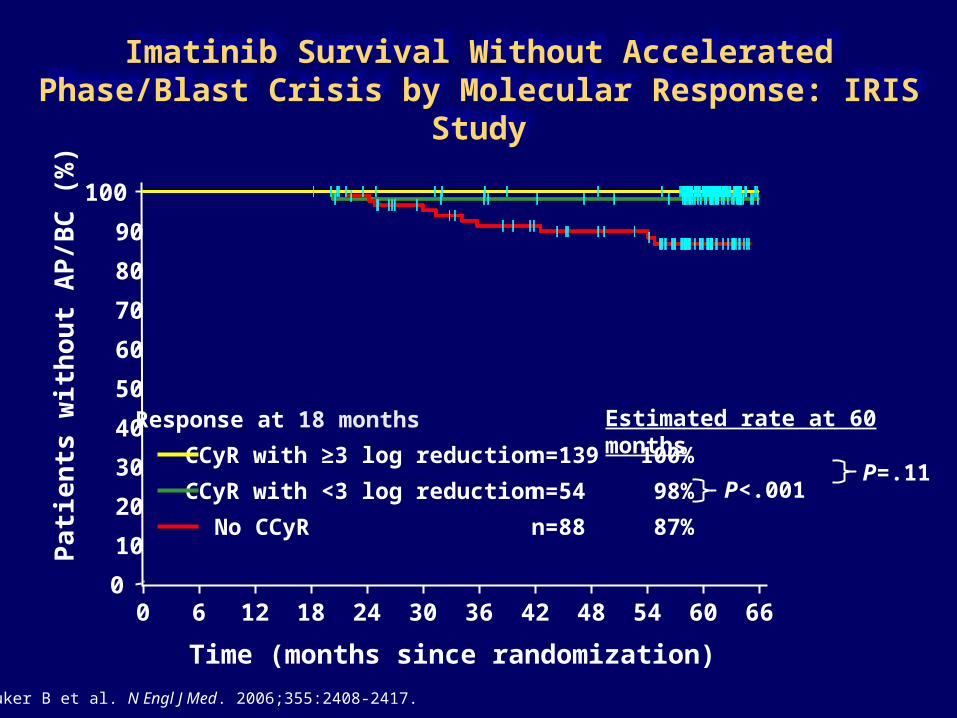
Imatinib Survival Without Accelerated Phase/Blast Crisis by Molecular Response: IRIS Study
Druker B et al. N Engl J Med. 2006;355:2408-2417.
Time (months since randomization)
n=54 98%
Estimated rate at 60 months
P<.001 P=.11
Response at 18 months
CCyR with ≥3 log reduction
CCyR with <3 log reduction
No CCyR
Pati
en
ts w
ith
ou
t A
P/B
C (
%)
0
10
20
30
40
50
60
70
80
90
100
0 6 12 18 24 30 36 42 48 54 60 66
n=88 87%
n=139 100%
IMATINIB-RESISTANT DISEASEIMATINIB-RESISTANT DISEASE
Can it be identified earlier than six months, ideally by less invasive
methods than bone marrow aspiration?
Pro
bab
ility
of
Su
rviv
al
Time From Onset of Imatinib Therapy (Yrs)
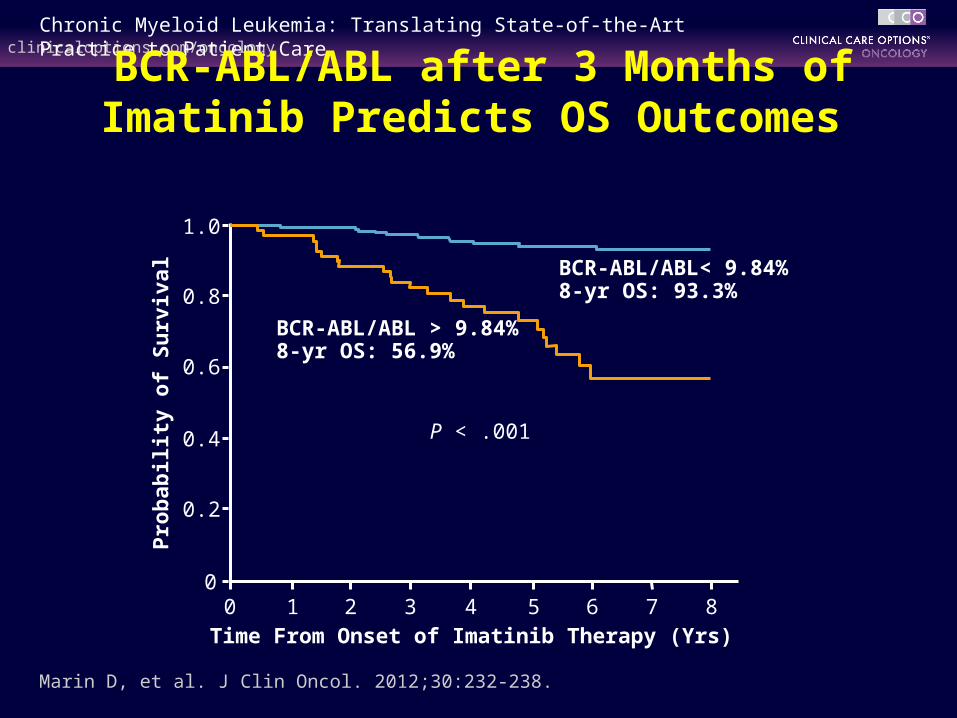
BCR-ABL/ABL< 9.84% 8-yr OS: 93.3%
BCR-ABL/ABL > 9.84% 8-yr OS: 56.9%
Marin D, et al. J Clin Oncol. 2012;30:232-238.
P < .001
BCR-ABL/ABL after 3 Months of Imatinib Predicts OS Outcomes
1.0
0.8
0.6
0.4
0.2
00 1 3 4 5 8762
Individual 3-month decline of BCR-ABL transcript levels as an
optimized predictor of survival in CML
B. Hanfstein, V. Shlyakhto, R. Hehlmann, M. Lauseker, S. Saussele, P. Erben, A. Fabarius, U. Proetel,
S. Schnittger, H.J. Kolb, S.W. Krause, J.E.A. Schubert, H. Einsele, M. Hänel, J. Dengler, C. Falge, L. Kanz, A. Neubauer,
M. Kneba, F. Stegelmann, M. Pfreundschuh, C.F. Waller, K. Spiekermann, G.M. Baerlocher, M. Pfirrmann, J. Hasford,
W.-K. Hofmann, A. Hochhaus and M.C. Müllerfor the SAKK and the German CML Study Group
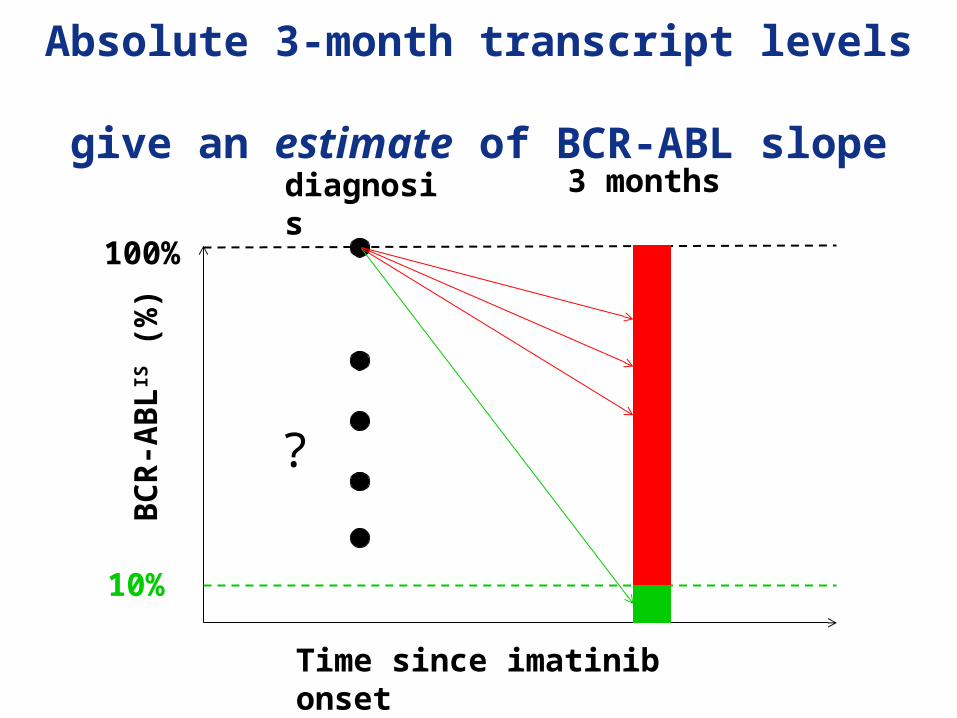
3 monthsdiagnosisB
CR
-AB
LIS (
%)
10%
100%
Time since imatinib onset
?
Absolute 3-month transcript levels give an estimate of BCR-ABL slope
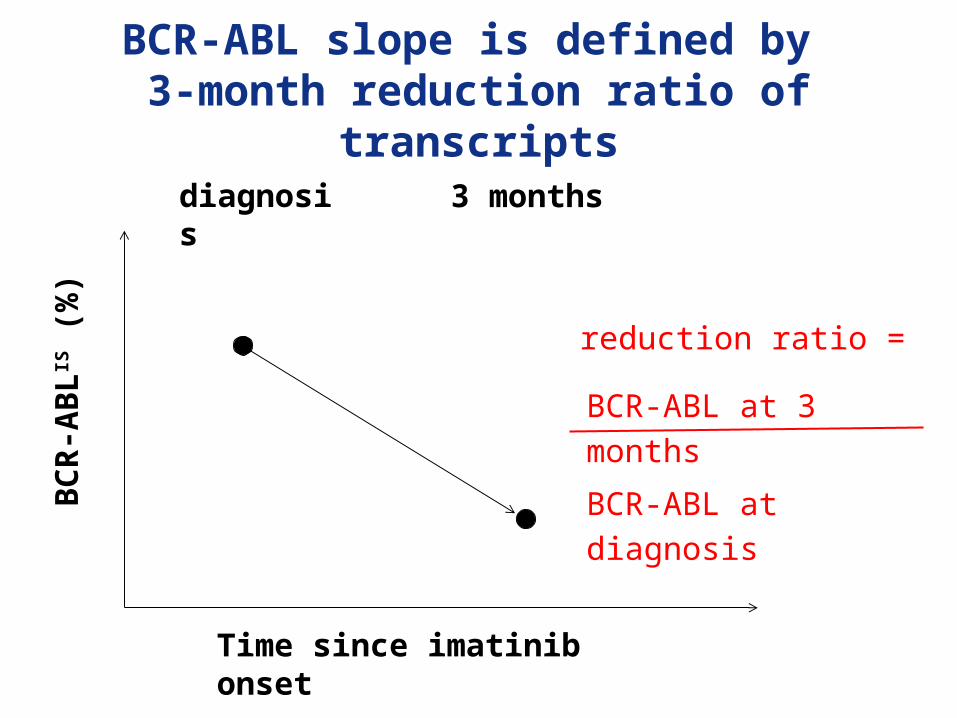
3 monthsdiagnosis
BC
R-A
BL
IS (
%)
Time since imatinib onset
BCR-ABL slope is defined by 3-month reduction ratio of
transcripts
BCR-ABL at 3 months
BCR-ABL at diagnosis
reduction ratio =
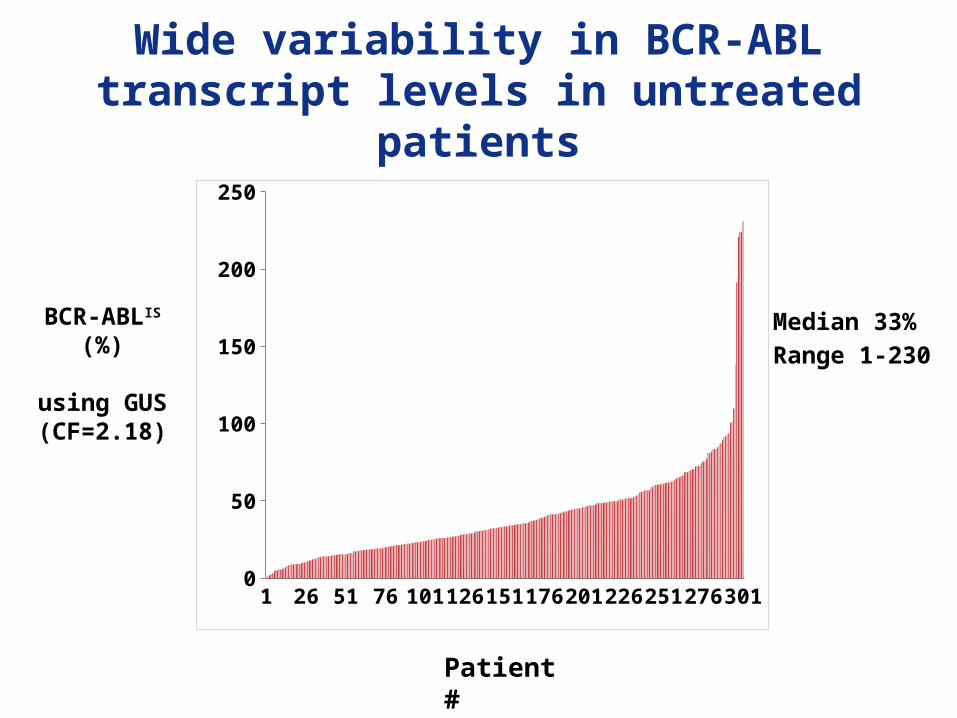
Wide variability in BCR-ABL transcript levels in untreated
patients
1 24 47 70 93 1161391621852082312542773000
50
100
150
200
250
BCR-ABLIS (%)
using GUS(CF=2.18)
Patient #
Median 33%
Range 1-230
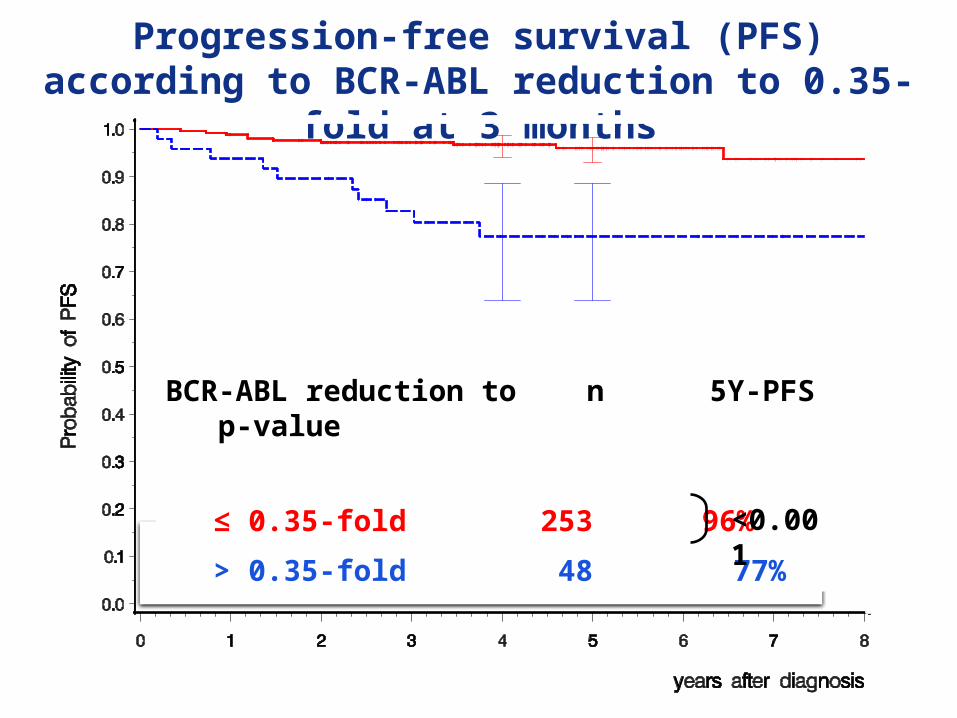
BCR-ABL reduction to n 5Y-PFS p-value
≤ 0.35-fold 253 96%
> 0.35-fold 48 77% <0.001
Progression-free survival (PFS) according to BCR-ABL reduction to 0.35-fold at 3
months
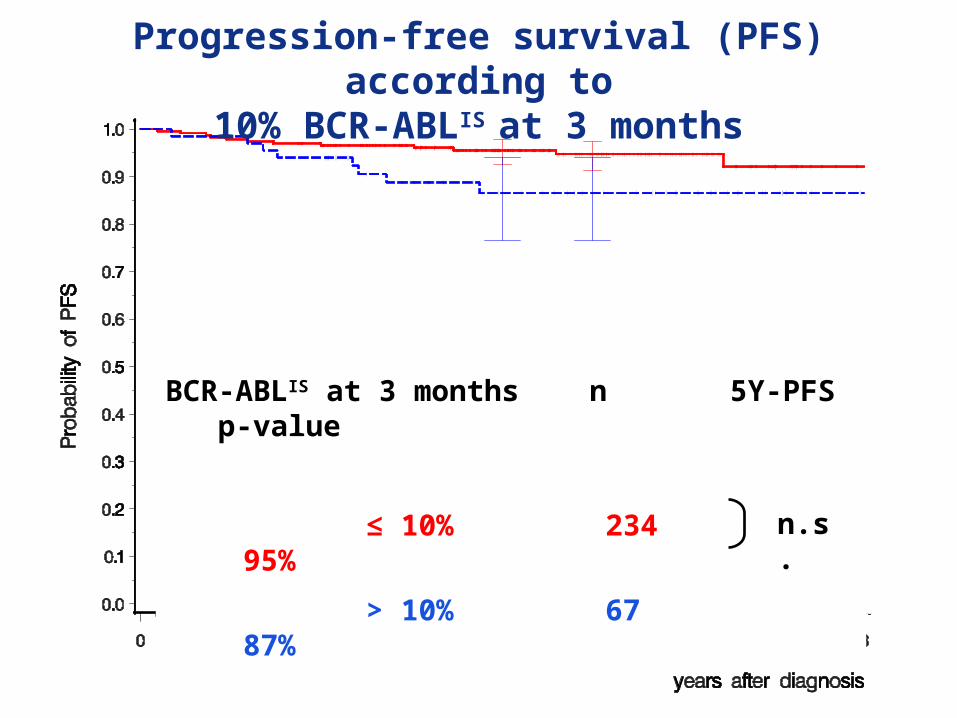
BCR-ABLIS at 3 months n 5Y-PFS p-value
≤ 10% 234 95%
> 10% 67 87% n.s.
Progression-free survival (PFS) according to
10% BCR-ABLIS at 3 months
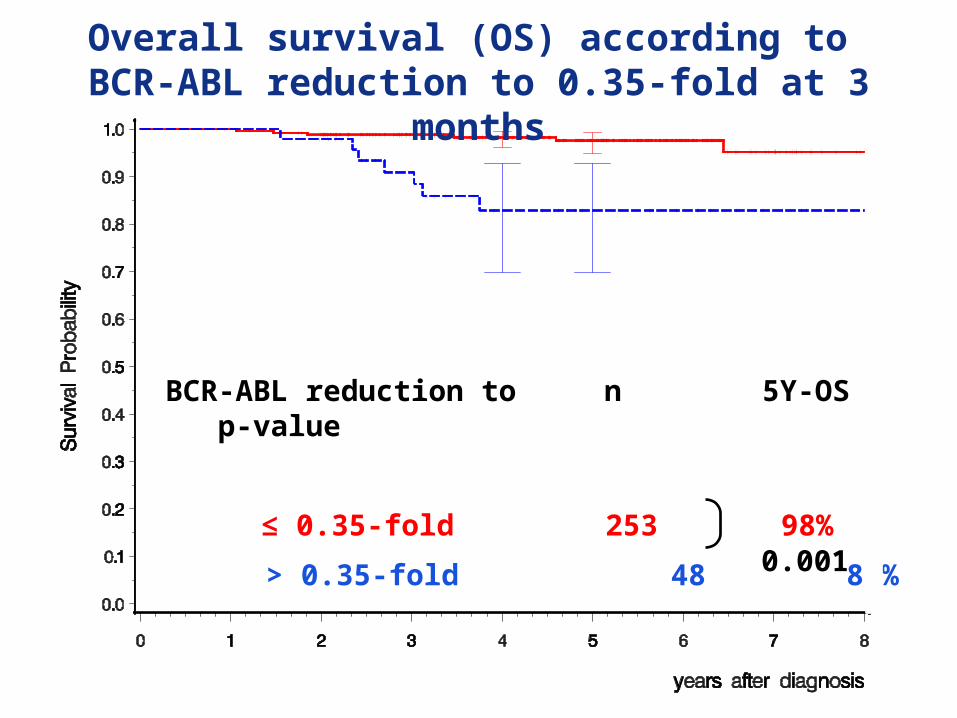
BCR-ABL reduction to n 5Y-OS p-value
≤ 0.35-fold 253 98%
> 0.35-fold 48 83%
Overall survival (OS) according to BCR-ABL reduction to 0.35-fold at 3
months
0.001
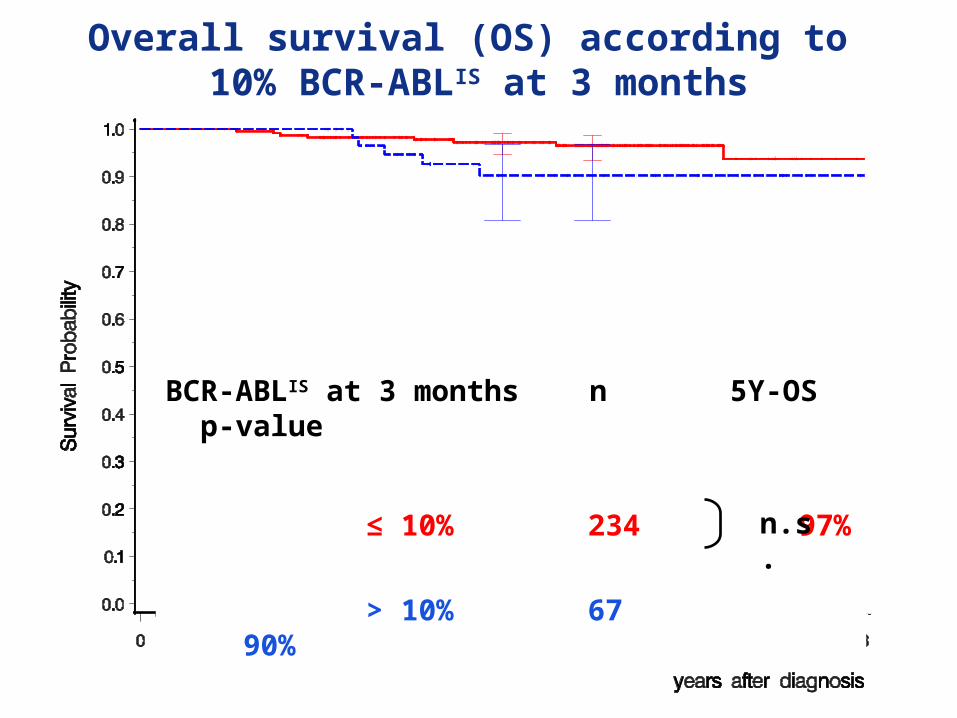
Overall survival (OS) according to 10% BCR-ABLIS at 3 months
BCR-ABLIS at 3 months n 5Y-OS p-value
≤ 10% 234 97%
> 10% 67 90%n.s.
Conclusions
BCR-ABLIS ratios at diagnosis vary in a wide range (1-230%).
The assumption of 100% BCR-ABLIS at diagnosis does not reflect the real-life situation.
Individual baseline levels have to be taken into account, when 3-month levels are interpreted.
No prognostic impact can be derived from baseline BCR-ABL.
The individual decline to the 0.35-fold of baseline levels within 3 months yielded a better discrimination with regard to PFS and OS than the 10% BCR-ABLIS cut-off.
High-risk patients in need of treatment escalation might be identified more precisely by the individual decline of BCR-ABL transcripts at 3 months of treatment.
FRONTLINE THERAPY FOR CMLFRONTLINE THERAPY FOR CML
How active are newer agents in the frontline management of CP-CML?
ENESTnd Update: Nilotinib vs Imatinib in Patients With Newly
Diagnosed CML-CP and the Impact of Early Molecular Response and Sokal
Risk at Diagnosis on Long-Term Outcomes
G. Saglio, A. Hochhaus, T. P. Hughes, R. E. Clark, H. Nakamae,
D.-W. Kim, S. Jootar, G. Etienne, I. W. Flinn, J. H. Lipton,
R. Pasquini, B. Moiraghi, C. Kemp, X. Fan, H. D. Menssen,
H. M. Kantarjian, and R. A. Larson,
on behalf of the ENESTnd Investigators
49
ENESTnd 5-Year Update
ENESTnd 5-Year Update
Data cutoff: May 22, 2013
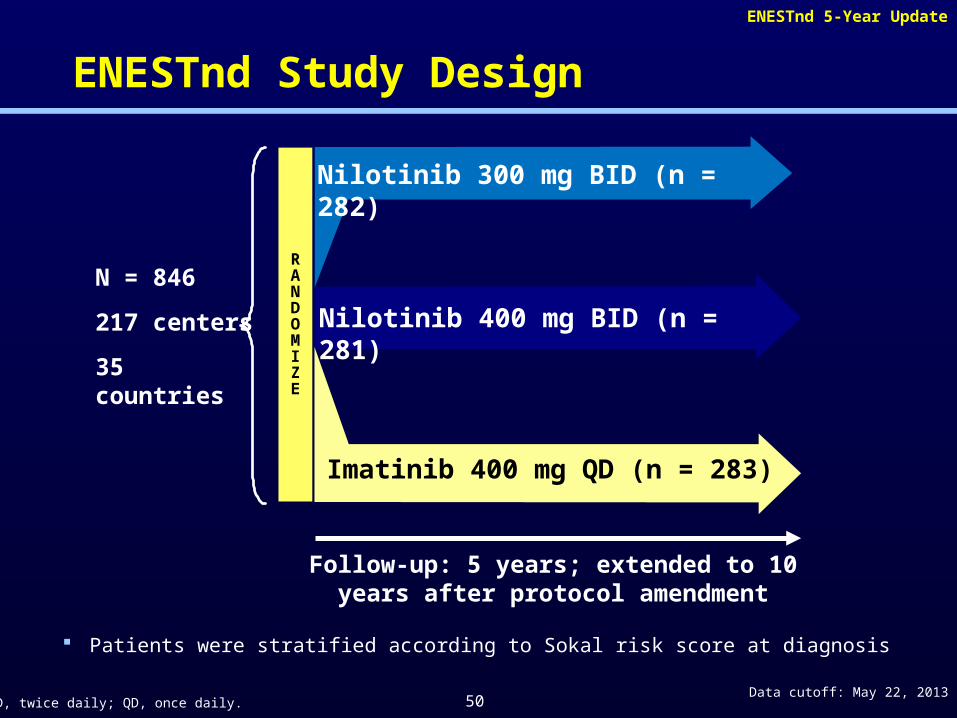
ENESTnd Study Design
50
N = 846
217 centers
35 countries
Imatinib 400 mg QD (n = 283)
Nilotinib 300 mg BID (n = 282)
RANDOMIZE
Nilotinib 400 mg BID (n = 281)
Follow-up: 5 years; extended to 10 years after protocol amendment
Patients were stratified according to Sokal risk score at diagnosis
BID, twice daily; QD, once daily.
ENESTnd 5-Year Update
Data cutoff: May 22, 2013
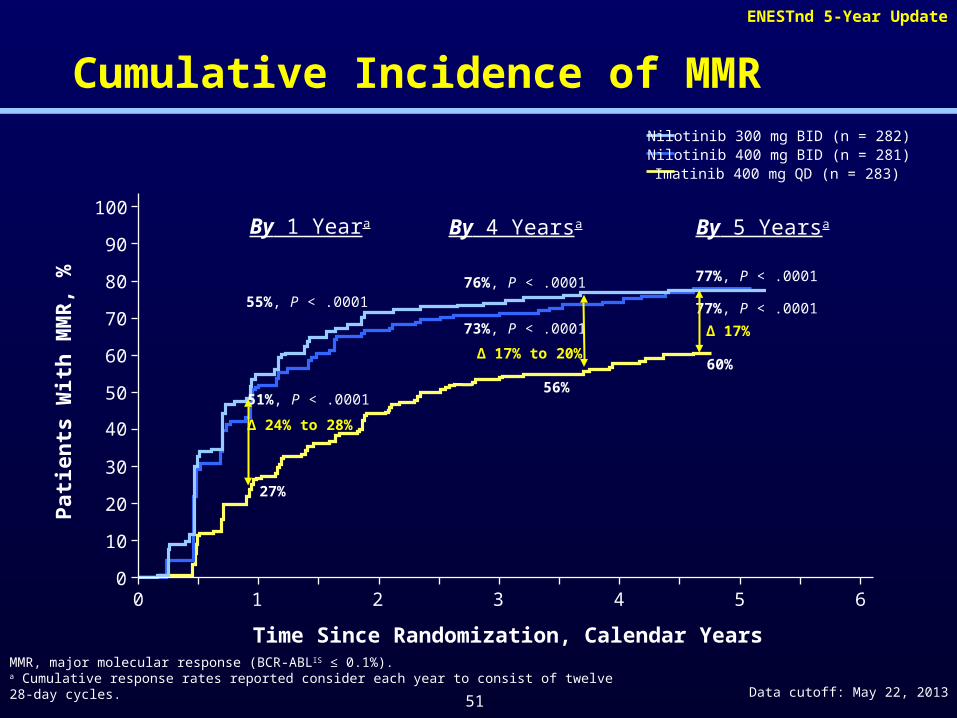
Cumulative Incidence of MMR
MMR, major molecular response (BCR-ABLIS ≤ 0.1%).a Cumulative response rates reported consider each year to consist of twelve 28-day cycles.
By 1 Yeara By 5 Yearsa
55%, P < .0001
51%, P < .0001
27%
Δ 24% to 28%
60%
77%, P < .0001
77%, P < .0001
Δ 17%
By 4 Yearsa
76%, P < .0001
73%, P < .0001
56%
Δ 17% to 20%
100
0 2 6
90
80
70
60
50
40
30
20
10
0
Pat
ien
ts W
ith
MM
R, %
Time Since Randomization, Calendar Years
31
Nilotinib 300 mg BID (n = 282)Nilotinib 400 mg BID (n = 281)Imatinib 400 mg QD (n = 283)
4 5
51
ENESTnd 5-Year Update
Data cutoff: May 22, 2013
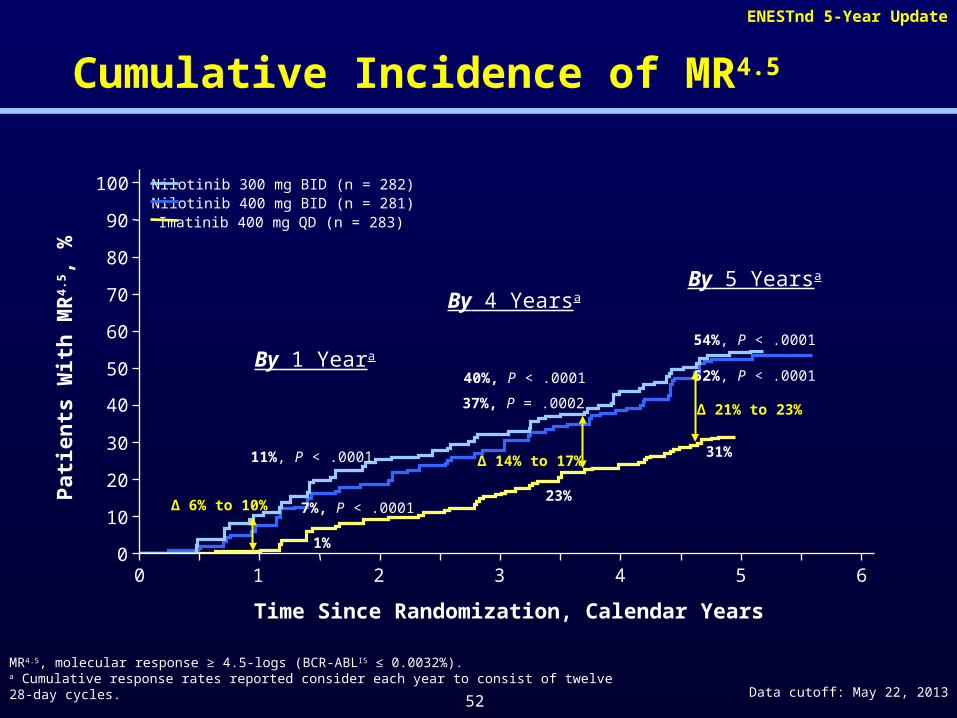
Cumulative Incidence of MR4.5
MR4.5, molecular response ≥ 4.5-logs (BCR-ABLIS ≤ 0.0032%).a Cumulative response rates reported consider each year to consist of twelve 28-day cycles.
By 5 Yearsa
11%, P < .0001
7%, P < .0001
1%
Δ 6% to 10%
31%
52%, P < .0001
54%, P < .0001
Δ 21% to 23%
By 4 Yearsa
40%, P < .0001
37%, P = .0002
23%
Δ 14% to 17%
100
0 2 6
90
80
70
60
50
40
30
20
10
0
Pat
ien
ts W
ith
MR
4.5 ,
%
Time Since Randomization, Calendar Years
31
Nilotinib 300 mg BID (n = 282)Nilotinib 400 mg BID (n = 281)Imatinib 400 mg QD (n = 283)
4 5
By 1 Yeara
52
ENESTnd 5-Year Update
Data cutoff: May 22, 2013
Progressions on Study0
5
10
15
20
25
20
10
Pat
ien
ts,
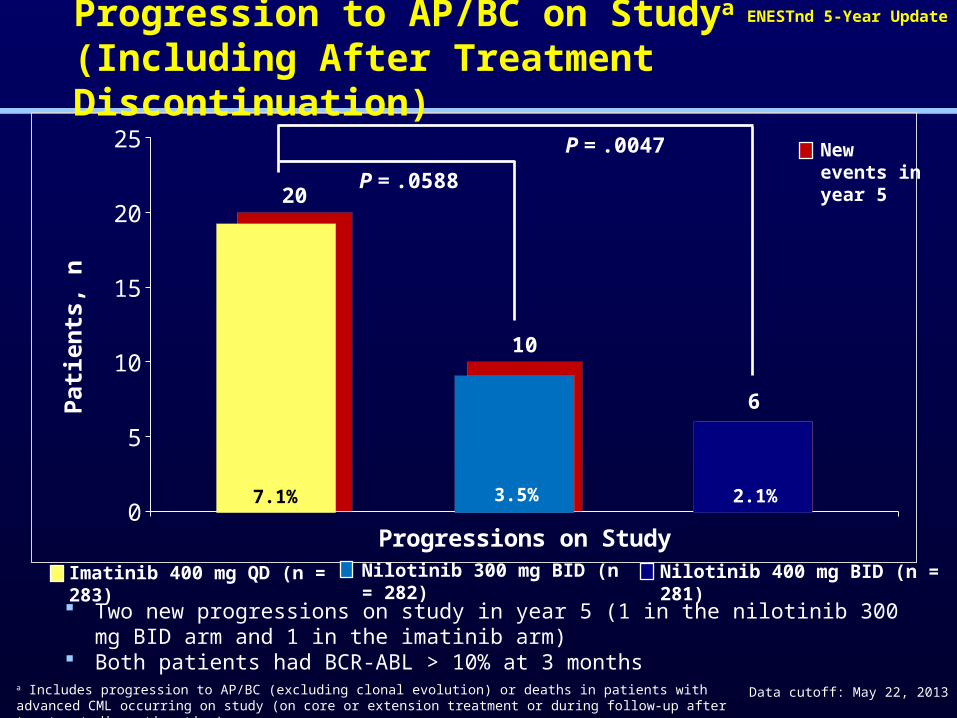
nProgression to AP/BC on Studya
(Including After Treatment Discontinuation)
a Includes progression to AP/BC (excluding clonal evolution) or deaths in patients with advanced CML occurring on study (on core or extension treatment or during follow-up after treatment discontinuation).
P = .0588
P = .0047
6
Nilotinib 300 mg BID (n = 282) Nilotinib 400 mg BID (n = 281)
Two new progressions on study in year 5 (1 in the nilotinib 300 mg BID arm and 1 in the imatinib arm)
Both patients had BCR-ABL > 10% at 3 months
New events in year 5
7.1% 3.5% 2.1%
Imatinib 400 mg QD (n = 283)
ENESTnd 5-Year Update
Data cutoff: May 22, 2013
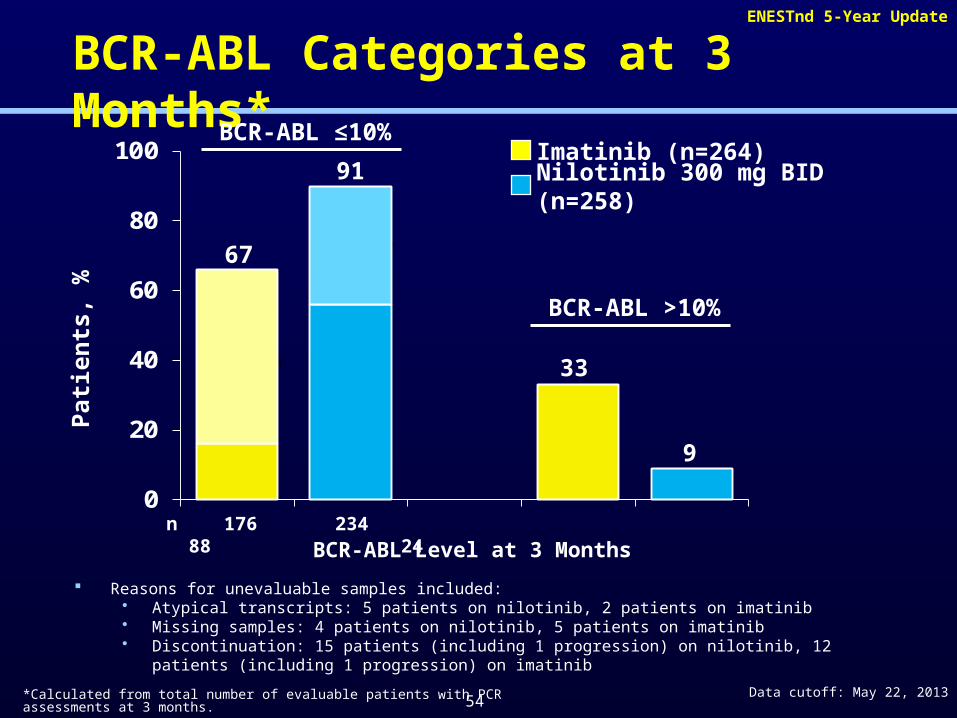
BCR-ABL Categories at 3 Months*
0
20
40
60
80
100
Pat
ien
ts,
%
BCR-ABL Level at 3 Monthsn 176 234 88 24
BCR-ABL >10%
91
67
9
33 >1- ≤10%
≤1%
Nilotinib 300 mg BID (n=258)
Imatinib (n=264)
Reasons for unevaluable samples included: • Atypical transcripts: 5 patients on nilotinib, 2 patients on imatinib• Missing samples: 4 patients on nilotinib, 5 patients on imatinib• Discontinuation: 15 patients (including 1 progression) on nilotinib, 12 patients (including 1 progression) on
imatinib
*Calculated from total number of evaluable patients with PCR assessments at 3 months.
BCR-ABL ≤10%
>1- ≤10%
≤1%
54
ENESTnd 5-Year Update
Data cutoff: May 22, 2013
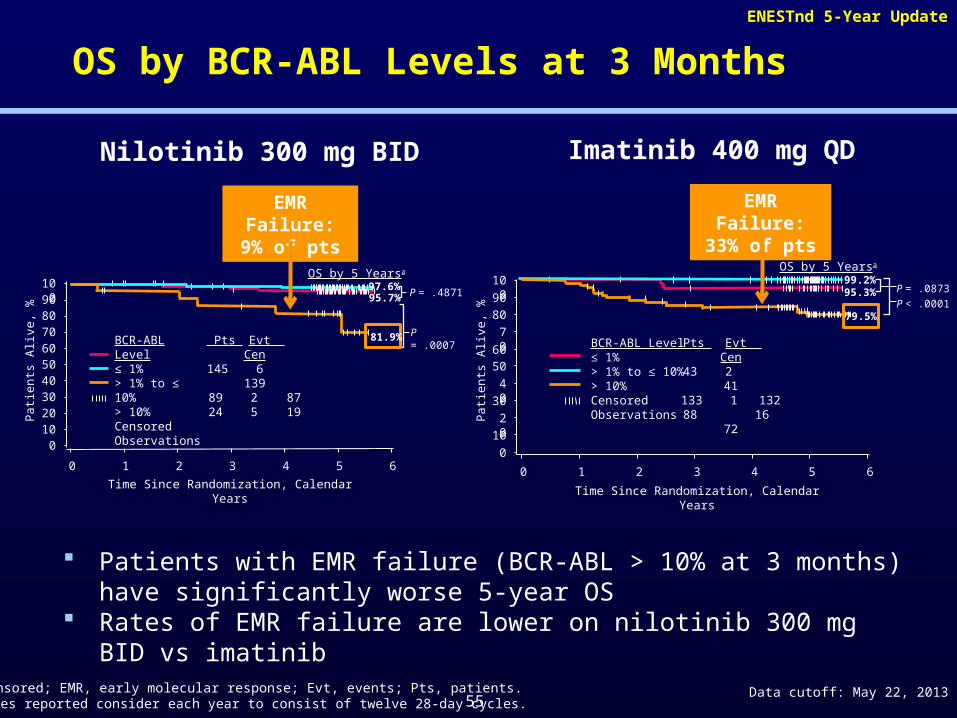
OS by BCR-ABL Levels at 3 Months
Nilotinib 300 mg BID Imatinib 400 mg QD
P = .4871
P = .0007
OS by 5 Yearsa
BCR-ABL Level≤ 1%> 1% to ≤ 10%> 10%Censored Observations
Pts Evt Cen145 6 13989 2 8724 5 19
100908070605040302010
0
0 1 2 3 4 5 6
Pat
ien
ts A
live
, %
Time Since Randomization, Calendar Years
100
90
80
70
6050
40
30
20
10
0
0 1 2 3 4 5 6
Time Since Randomization, Calendar Years
OS by 5 Yearsa
P < .0001
P = .087399.2%95.3%
BCR-ABL Level≤ 1%> 1% to ≤ 10%> 10%Censored Observations
Pts Evt Cen43 2 41133 1 13288 16 72
Cen, censored; EMR, early molecular response; Evt, events; Pts, patients.a OS rates reported consider each year to consist of twelve 28-day cycles.
Patients with EMR failure (BCR-ABL > 10% at 3 months) have significantly worse 5-year OS
Rates of EMR failure are lower on nilotinib 300 mg BID vs imatinib
79.5%
95.7%97.6%
81.9%
Pat
ien
ts A
live
, %
EMR Failure: 9% of pts
EMR Failure: 33% of pts
55
ENESTnd 5-Year Update
Data cutoff: May 22, 2013
Conclusions
At 5 years of follow-up, rates of event-free survival, progression-free survival, and overall survival were higher in patients treated with nilotinib than imatinib
Nilotinib demonstrated higher rates of early and deeper molecular response, including MR4.5, and a reduced risk of progression
By 5 years, more than half of nilotinib-treated patients had achieved MR4.5, a key eligibility criterion for many treatment-free remission studies
Side effects that appear unique to nilotinib include pancreatitis, hyperglycemia, EKG changes and peripheral arterial occlusive events.
56
57
DASISION 4-Year Follow-up
Four-Year (Yr) Follow-Up of Patients (Pts) With Newly Diagnosed Chronic Myeloid Leukemia in Chronic Phase (CML-CP) Receiving Dasatinib or Imatinib:
Efficacy Based on Early Response
J. Cortes,1 A. Hochhaus,2 D.-W. Kim,3 N.P. Shah,4 J. Mayer,5 P. Rowlings,6 H. Nakamae,7 M.B. Bradley-Garelik,8 H. Mohamed,9
H. Kantarjian,1 G. Saglio10
1University of Texas M.D. Anderson Cancer Center, Houston, TX, USA; 2Universitätsklinikum Jena, Jena, Germany; 3Seoul St. Mary's Hospital, Seoul,
Republic of Korea; 4UCSF School of Medicine, San Francisco, CA, USA; 5Department of Internal Medicine, Hematology and Oncology, University Hospital Brno, Brno,
Czech Republic; 6Calvary Mater Newcastle Hospital, University of Newcastle, Australia; 7Osaka City University Hospital, Osaka, Japan; 8Bristol-Myers Squibb, Wallingford, CT, USA; 9Bristol-Myers Squibb, Plainsboro, NJ, USA; 10University of
Turin, Turin, Italy
58
DASISION 4-Year Follow-up
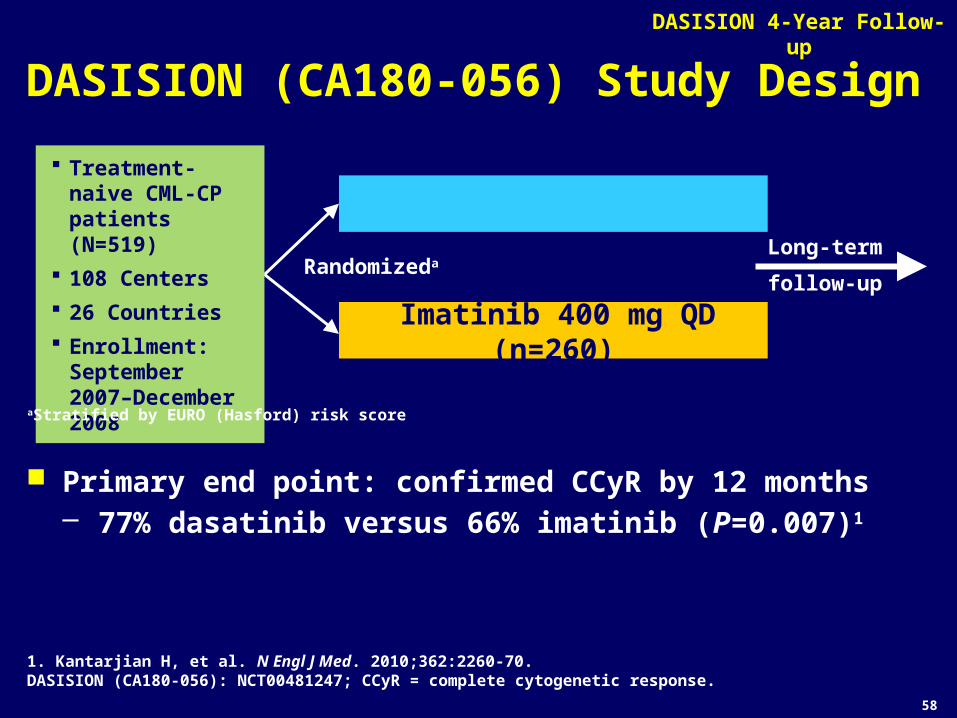
DASISION (CA180-056) Study Design
1. Kantarjian H, et al. N Engl J Med. 2010;362:2260-70.DASISION (CA180-056): NCT00481247; CCyR = complete cytogenetic response.
Primary end point: confirmed CCyR by 12 months– 77% dasatinib versus 66% imatinib (P=0.007)1
Long-term
follow-upRandomizeda
Imatinib 400 mg QD (n=260)
Dasatinib 100 mg QD (n=259)
Treatment-naive CML-CP patients (N=519)
108 Centers
26 Countries
Enrollment: September 2007–December 2008
aStratified by EURO (Hasford) risk score
59
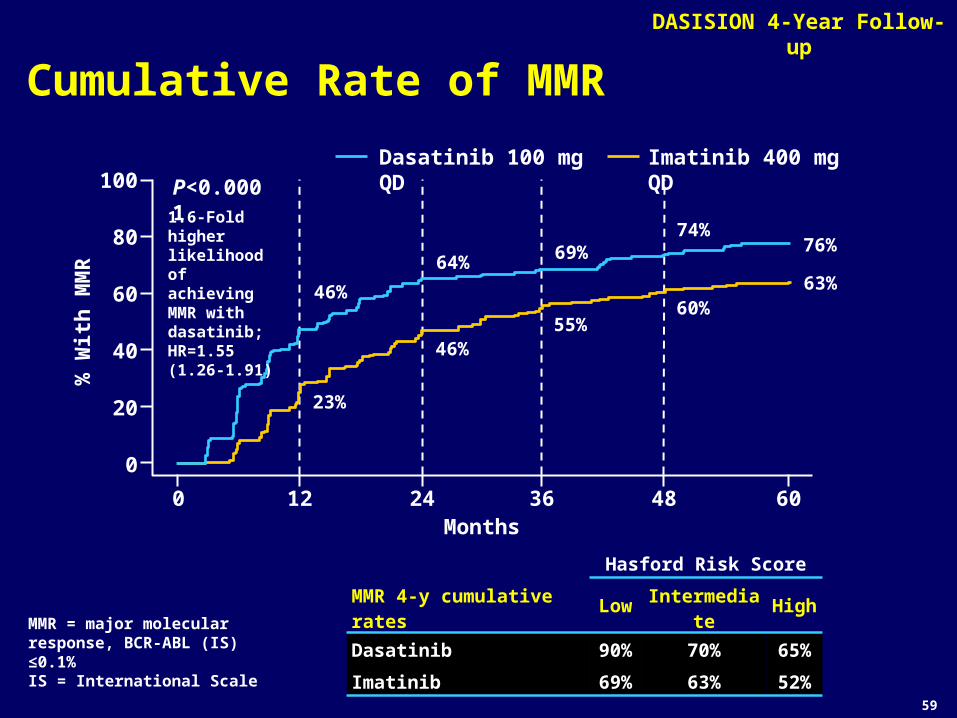
DASISION 4-Year Follow-up
Cumulative Rate of MMR
Dasatinib 100 mg QD Imatinib 400 mg QD
0 12Months
24 36 48 60
0
20
40
60
80
100 P<0.0001
% W
ith
MM
R
Hasford Risk Score
MMR 4-y cumulative rates Low Intermediate High
Dasatinib 90% 70% 65%
Imatinib 69% 63% 52%
46%
23%
64%
46%
69%
55%
74%
60%
76%
63%
1.6-Fold higher likelihood ofachieving MMR withdasatinib; HR=1.55(1.26-1.91)
MMR = major molecular response, BCR-ABL (IS) ≤0.1%IS = International Scale
60
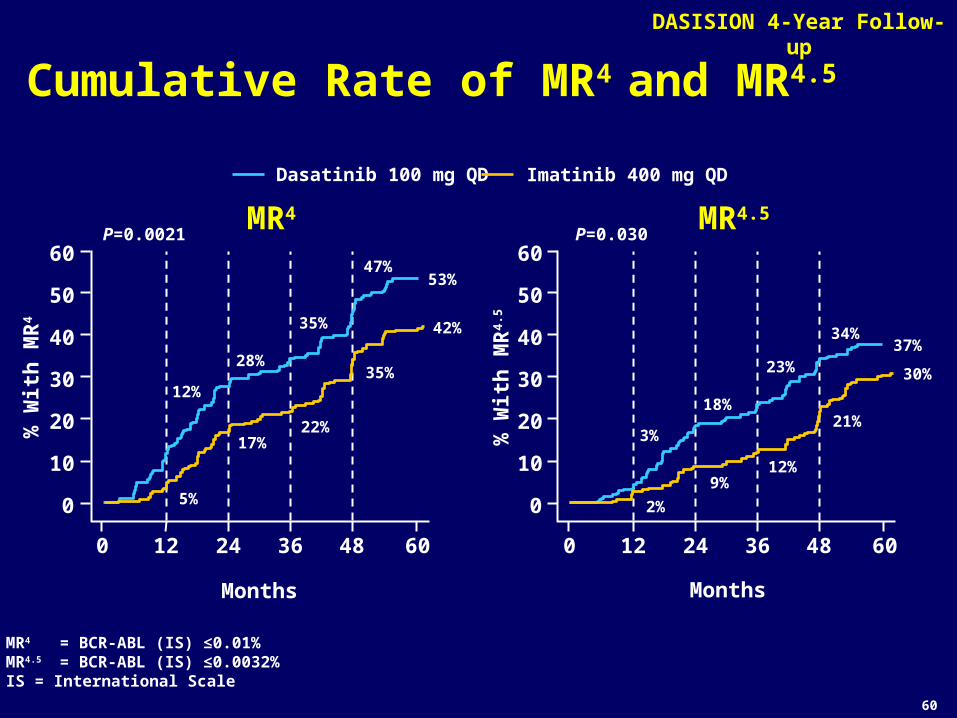
DASISION 4-Year Follow-up
Cumulative Rate of MR4 and MR4.5
% W
ith
MR
4.5
Months
P=0.030
0 12 24 36 48 60
Dasatinib 100 mg QD Imatinib 400 mg QD
MR4 = BCR-ABL (IS) ≤0.01%MR4.5 = BCR-ABL (IS) ≤0.0032%IS = International Scale
0
20
10
30
40
50
60
3%
2%
18%
9%
23%
12%
34%
21%
37%
30%
% W
ith
MR
4
Months
P=0.0021
0
20
10
30
40
50
60
12%
5%
28%
17%
35%
22%
47%
35%
0 12 24 36 48 60
53%
42%
MR4 MR4.5
61
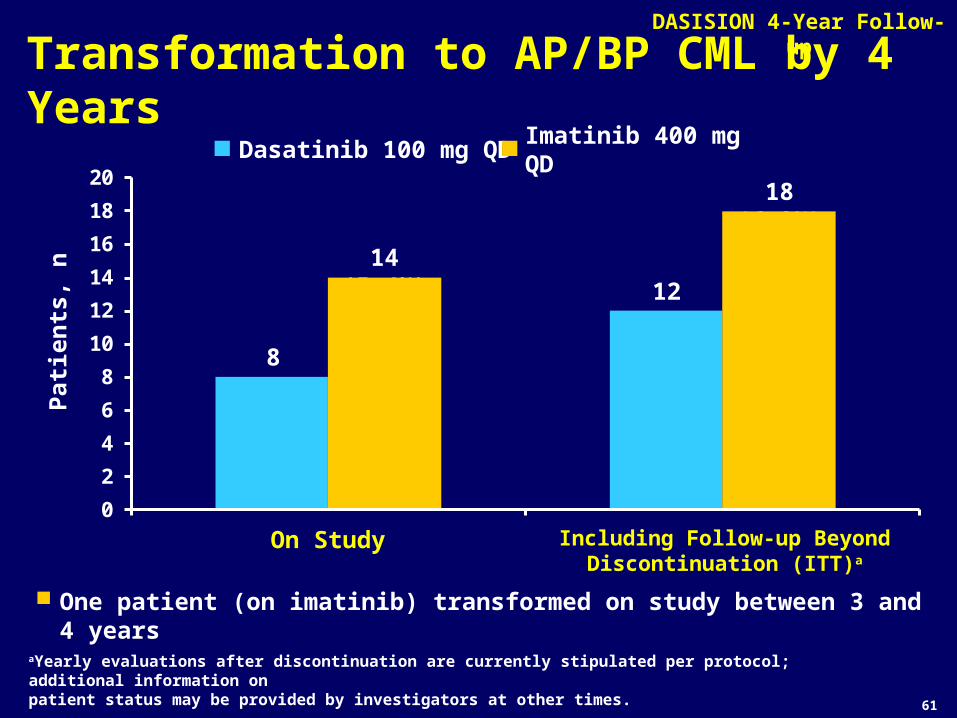
DASISION 4-Year Follow-up
Transformation to AP/BP CML by 4 Years
0
2
4
6
8
10
12
14
16
18
20
Pat
ien
ts,
n
On Study Including Follow-up Beyond Discontinuation (ITT)a
Dasatinib 100 mg QD Imatinib 400 mg QD
One patient (on imatinib) transformed on study between 3 and 4 years
8 (3.1%)
14 (5.4%)
12 (4.6%)
18 (6.9%)
aYearly evaluations after discontinuation are currently stipulated per protocol; additional information onpatient status may be provided by investigators at other times.
ASCO 2012 62
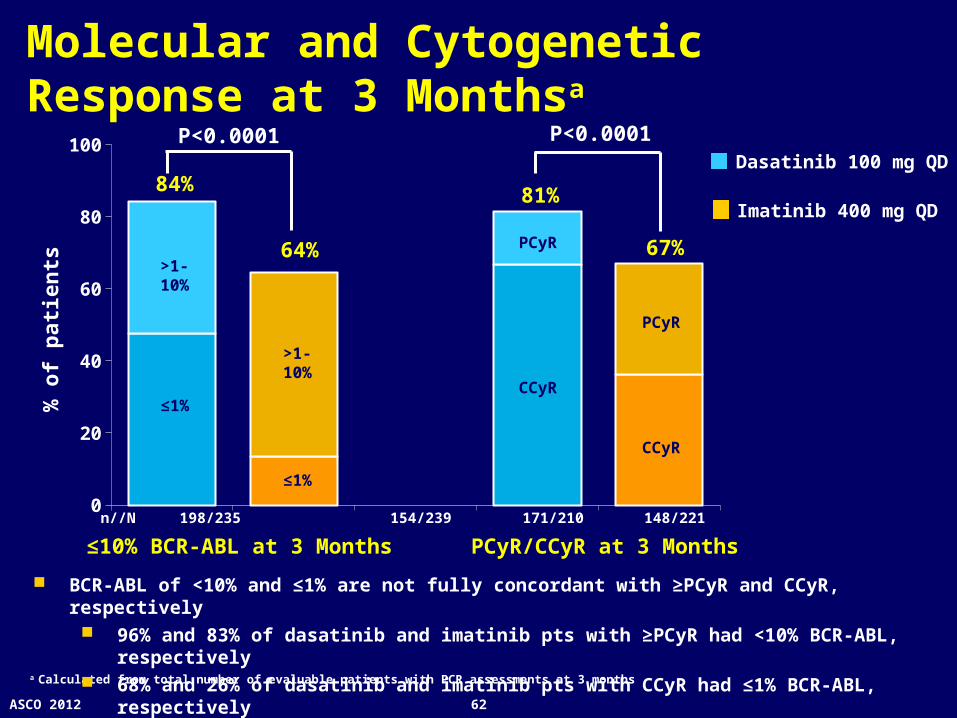
Molecular and Cytogenetic Response at 3 Monthsa
0
20
40
60
80
100
84%
64%
% o
f p
atie
nts
≤10% BCR-ABL at 3 Months
n//N 198/235 154/239 171/210 148/221
a Calculated from total number of evaluable patients with PCR assessments at 3 months
>1-10%
≤1%
>1-10%
≤1%
P<0.0001
CCyR
CCyR
PCyR
PCyR
PCyR/CCyR at 3 Months
81%
67%
P<0.0001Dasatinib 100 mg QD
Imatinib 400 mg QD
BCR-ABL of <10% and ≤1% are not fully concordant with ≥PCyR and CCyR, respectively 96% and 83% of dasatinib and imatinib pts with ≥PCyR had <10% BCR-ABL, respectively 68% and 26% of dasatinib and imatinib pts with CCyR had ≤1% BCR-ABL, respectively
63
DASISION 4-Year Follow-up
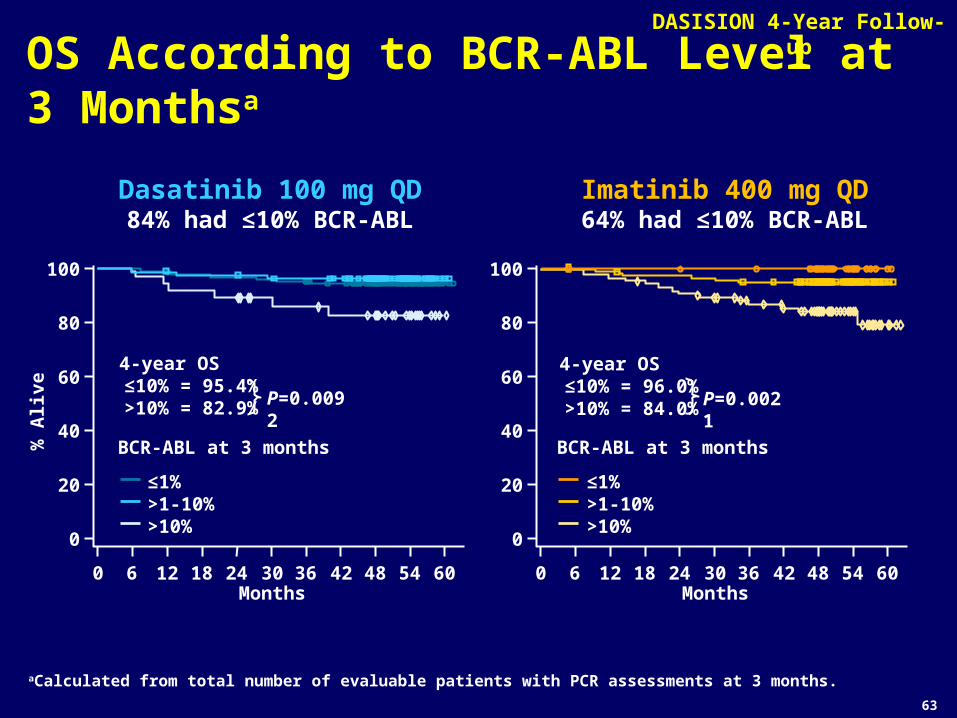
OS According to BCR-ABL Level at 3 Monthsa
aCalculated from total number of evaluable patients with PCR assessments at 3 months.
% A
live
Months
≤1%>1-10%>10%
BCR-ABL at 3 months
4-year OS ≤10% = 95.4% >10% = 82.9% P=0.0092
Dasatinib 100 mg QD84% had ≤10% BCR-ABL
0
20
40
60
80
100
0 18 36 546 12 24 30 42 48 60
Imatinib 400 mg QD64% had ≤10% BCR-ABL
Months
≤1%>1-10%>10%
BCR-ABL at 3 months
4-year OS ≤10% = 96.0% >10% = 84.0% P=0.0021
0
20
40
60
80
100
0 18 36 546 12 24 30 42 48 60
64
DASISION 4-Year Follow-up
Conclusions 4-Year follow-up demonstrates:
– Deeper molecular responses with dasatinib versus imatinib– More optimal molecular responses with dasatinib versus
imatinib– Fewer transformations to AP/BP
Achievement of BCR-ABL ≤10% at 3 months is associated with significantly higher PFS and OS by 4 years
- BCR-ABL ≤10% at 3 months: dasatinib 84% versus imatinib 64%
By 4 years, 37% of dasatinib-treated patients had achieved MR4.5, a key eligibility criterion for many treatment-free remission studies
Side effects that appear unique to dasatinib include pleural effusion and pulmonary arterial hypertension.
Nilotinib and Dasatinib in Previously Untreated Chronic Phase CML PatientsConcluding Thoughts
• Nilotinib and dasatinib are superior to imatinib at achieving deep responses and are associated with a lower likelihood of transformation to accelerated/blast phase disease
• The tolerability of nilotinib and dasatinib appears generally comparable to or slightly better than imatinib
• Patients and physicians have three approved TKI treatment options for newly diagnosed chronic phase CML
• Of these, imatinib has the longest and most convincing safety record
Should We Be Excited About Starting Patients on Imatinib?
While Some are Ecstatic with Silver…
…Others are Not So Impressed
IMATINIB-RESISTANT DISEASEIMATINIB-RESISTANT DISEASE
What are its causes?
Clinical Resistance to Imatinib Mechanisms
• Primary resistance Insufficient inhibition of BCR-ABL
• Can be due to low plasma levels, activity of drug pumps, etc Individual variation in normal bone marrow reserve (low levels of
normal hematopoietic stem cells in some patients)
• Secondary resistance Outgrowth of one or more clones harboring an imatinib-resistant
BCR-ABL kinase domain mutation (most common) Overproduction of BCR-ABL (e.g. via genomic amplification) BCR-ABL-independent mechanisms (poorly understood)
Efficacy and Safety of Bosutinib (SKI-606) Among Patients with
Chronic Phase Ph+ Chronic Myelogenous Leukemia (CML)
J. Cortes, T.H. Brümmendorf, H. Kantarjian, J. Khoury, G. Rosti, T. Fischer, L. Tornaghi, B.
Hewes, E.C. Martin, C. Gambacorti-Passerini
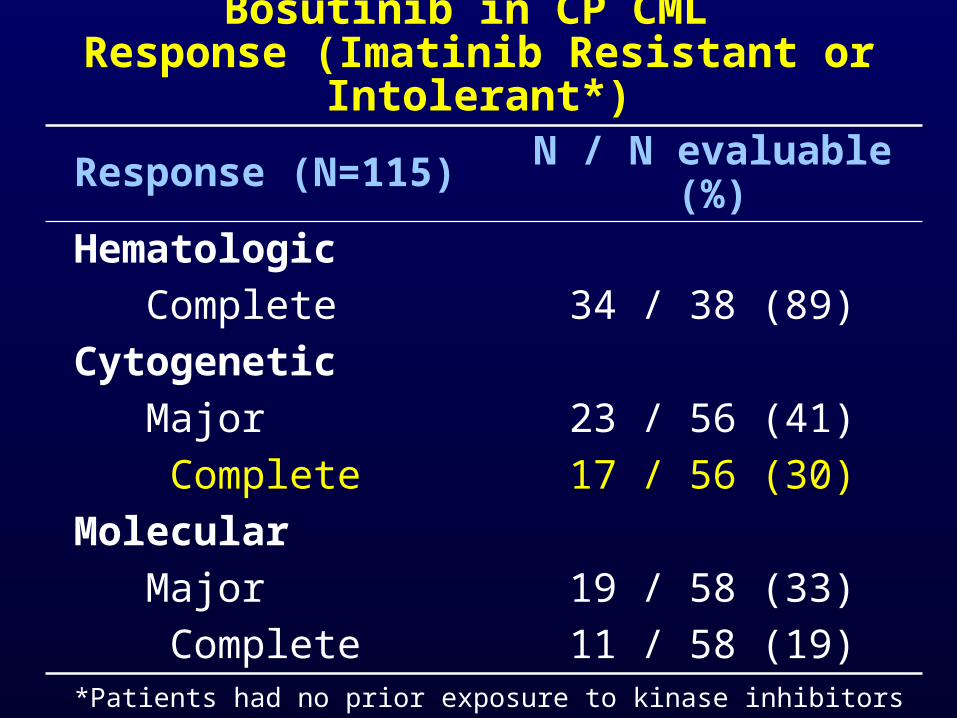
Bosutinib in CP CML Response (Imatinib Resistant or Intolerant*)
Response (N=115) N / N evaluable (%)
Hematologic
Complete 34 / 38 (89)
Cytogenetic
Major 23 / 56 (41)
Complete 17 / 56 (30)
Molecular
Major 19 / 58 (33)
Complete 11 / 58 (19)*Patients had no prior exposure to kinase inhibitors other than imatinib.
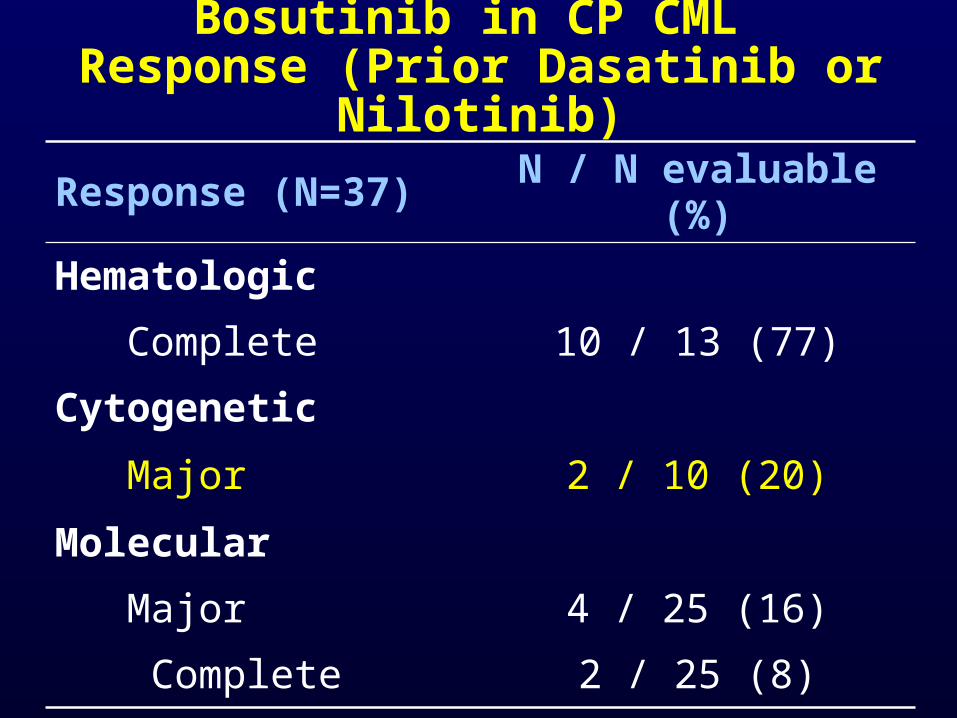
Bosutinib in CP CML Response (Prior Dasatinib or Nilotinib)
Response (N=37) N / N evaluable (%)
Hematologic
Complete 10 / 13 (77)
Cytogenetic
Major 2 / 10 (20)
Molecular
Major 4 / 25 (16)
Complete 2 / 25 (8)
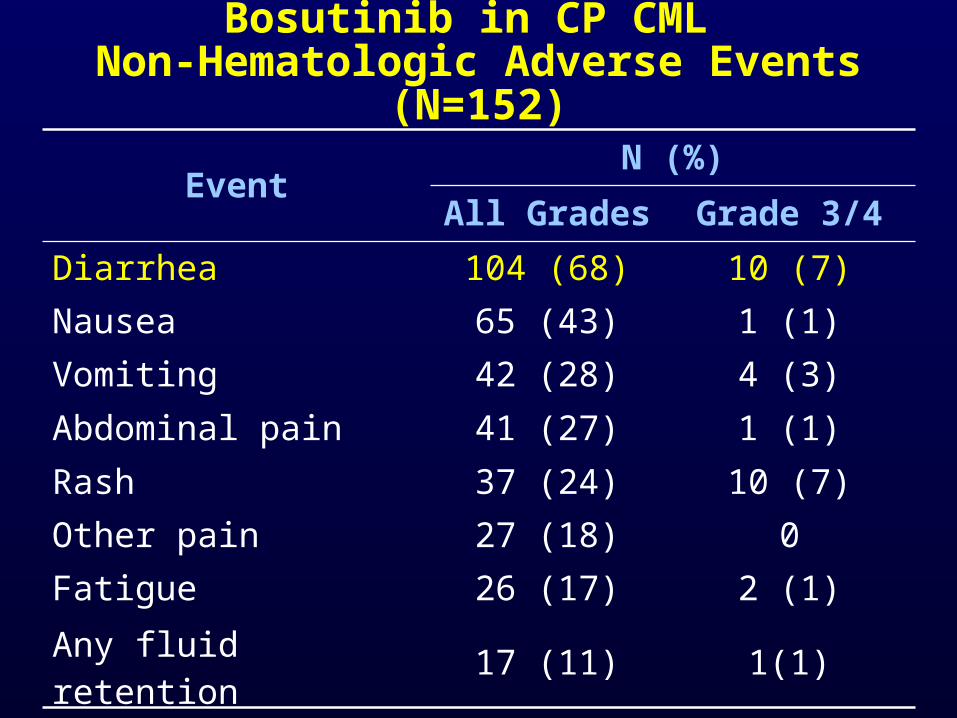
EventN (%)
All Grades Grade 3/4
Diarrhea 104 (68) 10 (7)
Nausea 65 (43) 1 (1)
Vomiting 42 (28) 4 (3)
Abdominal pain 41 (27) 1 (1)
Rash 37 (24) 10 (7)
Other pain 27 (18) 0
Fatigue 26 (17) 2 (1)
Any fluid retention 17 (11) 1(1)
Bosutinib in CP CML Non-Hematologic Adverse Events (N=152)
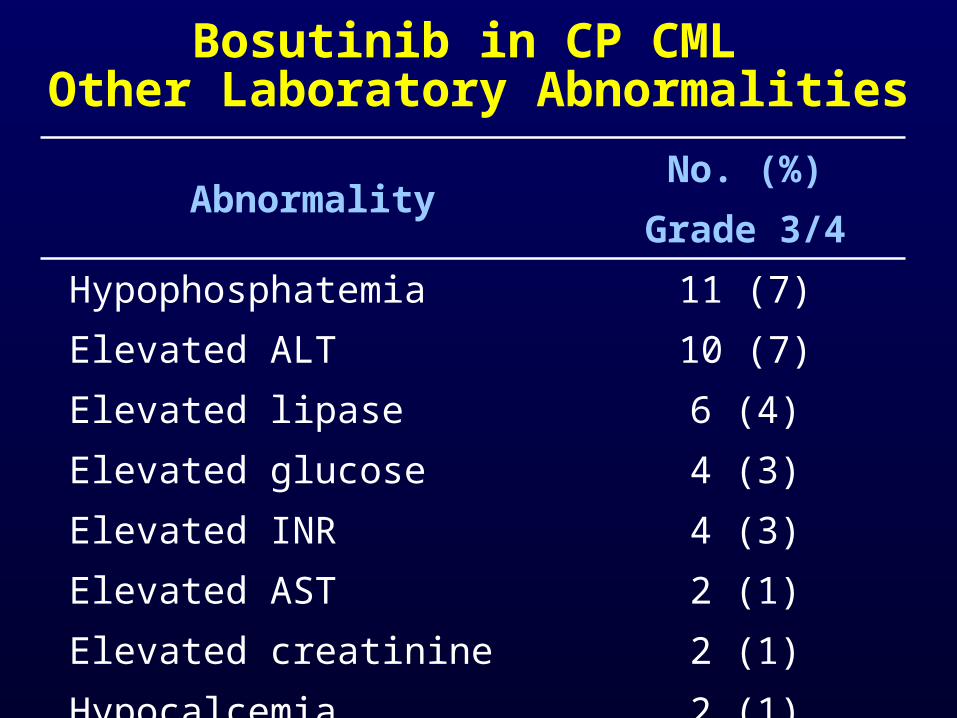
Bosutinib in CP CML Other Laboratory Abnormalities
AbnormalityNo. (%)
Grade 3/4Hypophosphatemia 11 (7)Elevated ALT 10 (7)Elevated lipase 6 (4)Elevated glucose 4 (3)Elevated INR 4 (3)Elevated AST 2 (1)Elevated creatinine 2 (1)
Hypocalcemia 2 (1)
Bosutinib in CP CML Conclusions
• Clinical efficacy in CP CML resistant or intolerant to imatinib (and other TKIs)
• Responses across a wide range of mutations, but not T315I
• Acceptable toxicity profile–Self-limiting diarrhea, liver function test
abnormalities–Low hematologic toxicity
Ponatinib in Patients with CML and Ph+ ALL Resistant or Intolerant to
Dasatinib or Nilotinib, or with the T315I BCR‐ABL Mutation: 2-Year Follow‐up of the
PACE Trial
ASH 2013 Abstract 650
JE Cortes, D-W Kim, J Pinilla-Ibarz, PD le Coutre, R Paquette, C Chuah,
FE Nicolini, JF Apperley, HJ Khoury, M Talpaz, JF DiPersio,
DJ DeAngelo, E Abruzzese, D Rea, M Baccarani,
MC Müller, C Gambacorti-Passerini, S Lustgarten, VM Rivera, T Clackson,
CD Turner, FG Haluska, F Guilhot, MW Deininger, A Hochhaus, TP Hughes,
JM Goldman, NP Shah, and HM Kantarjian
On behalf of the PACE Study Group
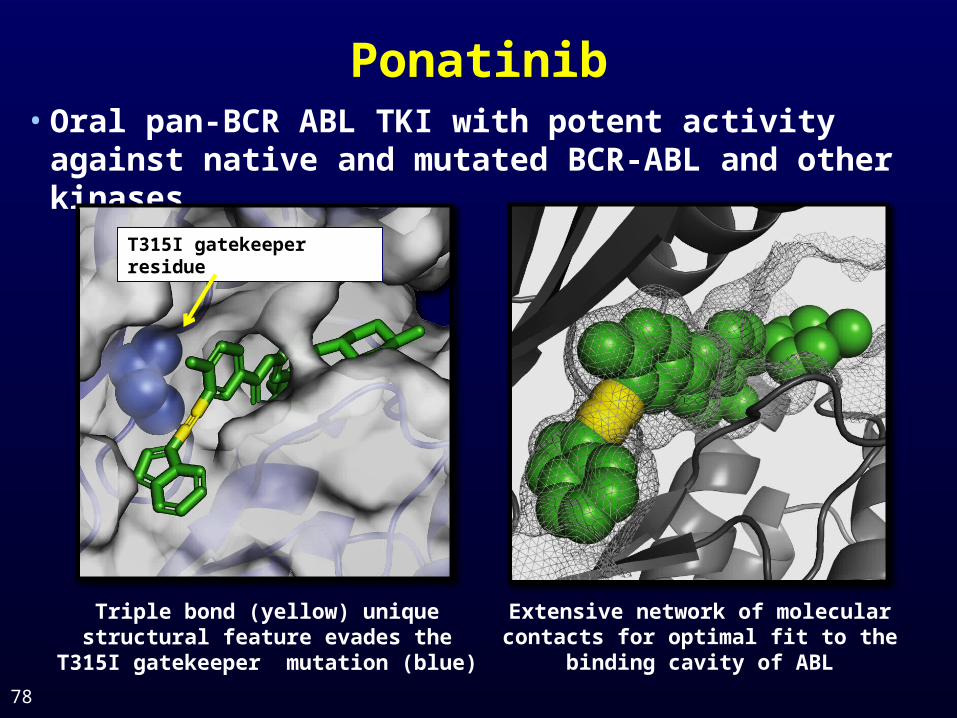
Ponatinib
78
• Oral pan-BCR ABL TKI with potent activity against native and mutated BCR-ABL and other kinases
Extensive network of molecular contacts for optimal fit to the binding
cavity of ABL
Triple bond (yellow) unique structural feature evades the T315I gatekeeper
mutation (blue)
T315I gatekeeper residue
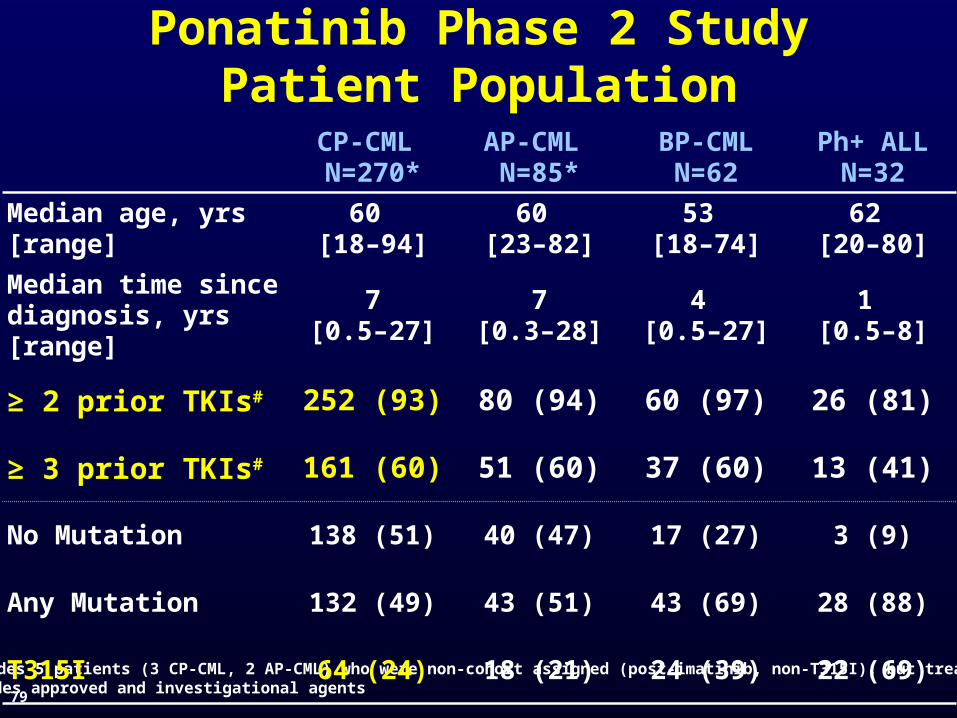
*Includes 5 patients (3 CP-CML, 2 AP-CML) who were non-cohort assigned (post-imatinib, non-T315I), but treated #Includes approved and investigational agents
Ponatinib Phase 2 StudyPatient Population
CP-CML N=270*
AP-CML N=85*
BP-CMLN=62
Ph+ ALLN=32
Median age, yrs [range]
60 [18–94]
60 [23–82]
53 [18–74]
62 [20–80]
Median time since diagnosis, yrs [range]
7[0.5–27]
7[0.3–28]
4 [0.5–27]
1 [0.5–8]
≥ 2 prior TKIs# 252 (93) 80 (94) 60 (97) 26 (81)
≥ 3 prior TKIs# 161 (60) 51 (60) 37 (60) 13 (41)
No Mutation 138 (51) 40 (47) 17 (27) 3 (9)
Any Mutation 132 (49) 43 (51) 43 (69) 28 (88)
T315I 64 (24) 18 (21) 24 (39) 22 (69)
79
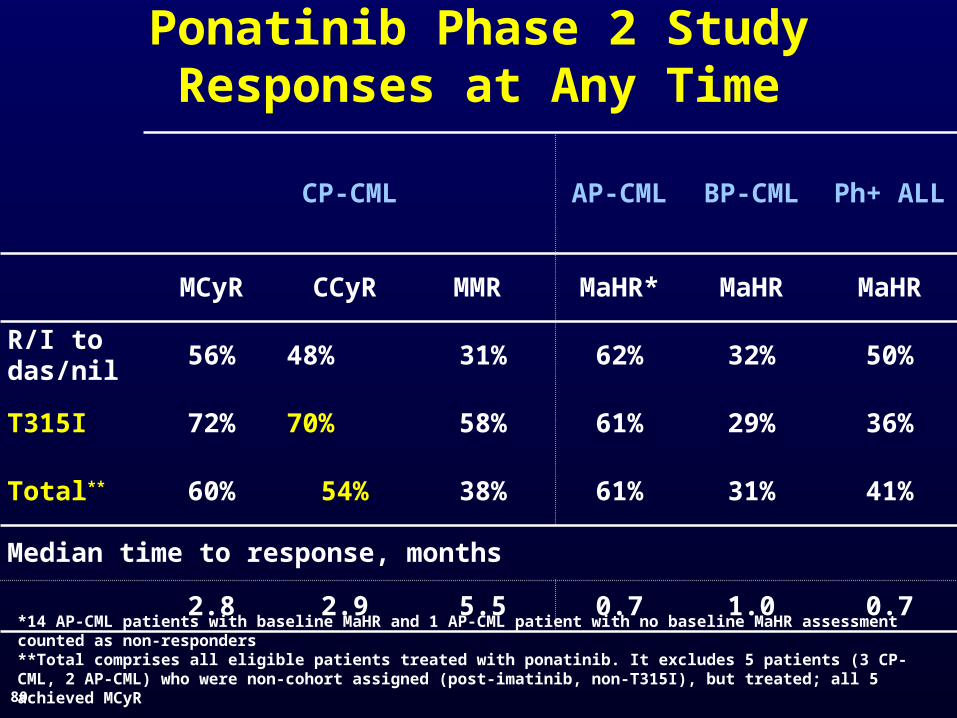
Ponatinib Phase 2 StudyResponses at Any Time
CP-CML AP-CML BP-CML Ph+ ALL
MCyR CCyR MMR MaHR* MaHR MaHR
R/I to das/nil 56% 48% 31% 62% 32% 50%
T315I 72% 70% 58% 61% 29% 36%
Total** 60% 54% 38% 61% 31% 41%
Median time to response, months
2.8 2.9 5.5 0.7 1.0 0.7*14 AP-CML patients with baseline MaHR and 1 AP-CML patient with no baseline MaHR assessment counted as non-responders **Total comprises all eligible patients treated with ponatinib. It excludes 5 patients (3 CP-CML, 2 AP-CML) who were non-cohort assigned (post-imatinib, non-T315I), but treated; all 5 achieved MCyR
80
Months
Pro
ba
bil
ity
of
PF
S (
%)
0 6 12 18 24 30 360
10
20
30
40
50
60
70
80
90
100
R/I (N=203)
T315I (N=64)
Total (N=267)
No. at riskTotal
267 204 170 139 73 3 0
MonthsP
rob
ab
ilit
y o
f O
S (
%)
0 6 12 18 24 30 360
10
20
30
40
50
60
70
80
90
100
R/I (N=203)
T315I (N=64)
Total (N=267)
No. at riskTotal
267 242 225 210 162 29 0
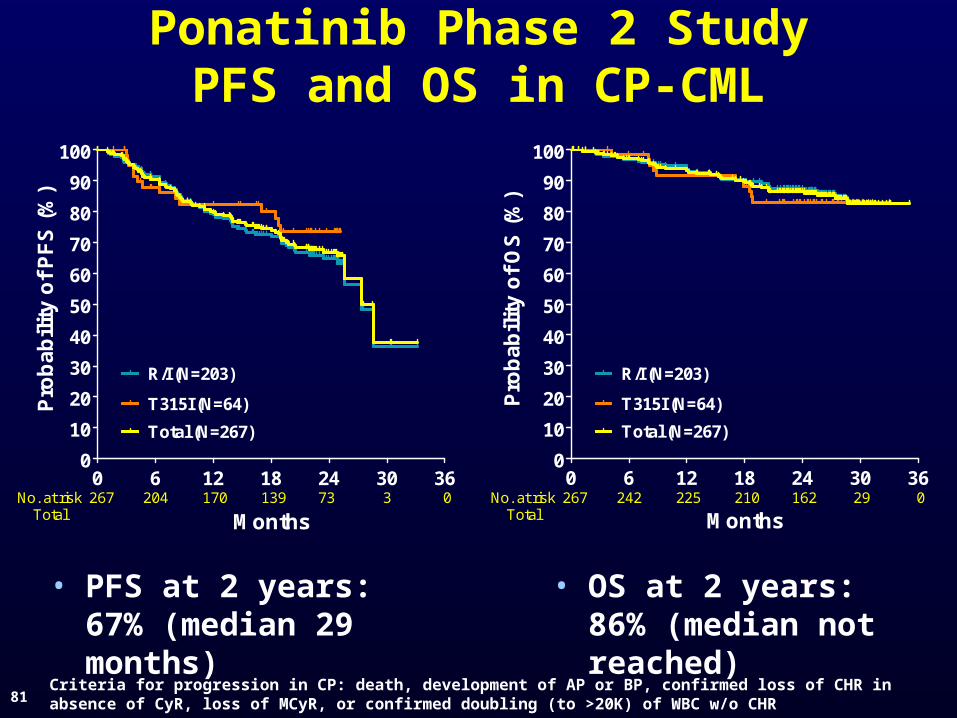
Ponatinib Phase 2 StudyPFS and OS in CP-CML
Criteria for progression in CP: death, development of AP or BP, confirmed loss of CHR in absence of CyR, loss of MCyR, or confirmed doubling (to >20K) of WBC w/o CHR
• PFS at 2 years: 67% (median 29 months)
• OS at 2 years: 86% (median not reached)
81
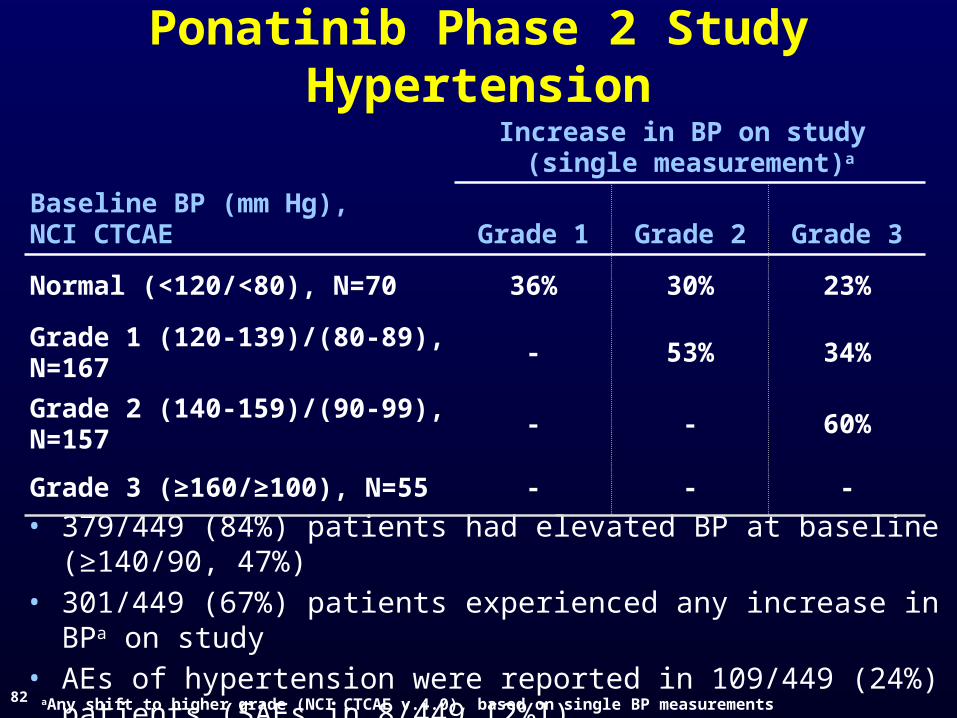
Ponatinib Phase 2 StudyHypertension
• 379/449 (84%) patients had elevated BP at baseline (≥140/90, 47%)• 301/449 (67%) patients experienced any increase in BPa on study• AEs of hypertension were reported in 109/449 (24%) patients (SAEs
in 8/449 [2%])
82
Baseline BP (mm Hg),NCI CTCAE
Increase in BP on study (single measurement)a
Grade 1 Grade 2 Grade 3
Normal (<120/<80), N=70 36% 30% 23%
Grade 1 (120-139)/(80-89), N=167 - 53% 34%
Grade 2 (140-159)/(90-99), N=157 - - 60%
Grade 3 (≥160/≥100), N=55 - - -
aAny shift to higher grade (NCI CTCAE v.4.0), based on single BP measurements
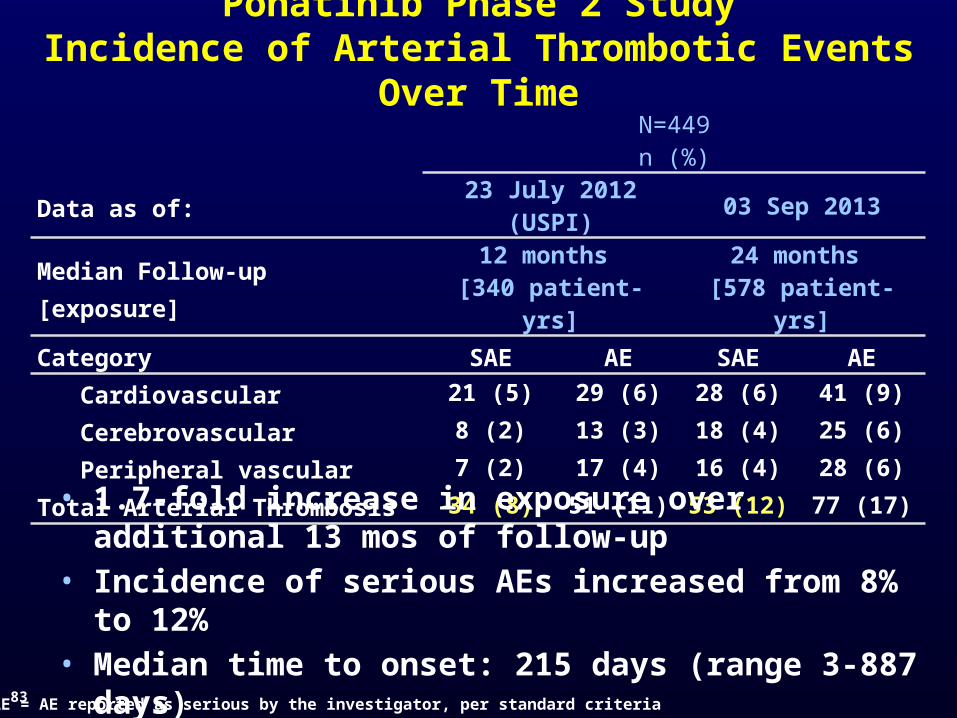
N=449n (%)
Data as of: 23 July 2012 (USPI) 03 Sep 2013
Median Follow-up [exposure]12 months
[340 patient-yrs]24 months
[578 patient-yrs]
Category SAE AE SAE AE Cardiovascular 21 (5) 29 (6) 28 (6) 41 (9)
Cerebrovascular 8 (2) 13 (3) 18 (4) 25 (6)
Peripheral vascular 7 (2) 17 (4) 16 (4) 28 (6)
Total Arterial Thrombosis 34 (8) 51 (11) 53 (12) 77 (17)
Ponatinib Phase 2 StudyIncidence of Arterial Thrombotic Events Over Time
83
• 1.7-fold increase in exposure over additional 13 mos of follow-up
• Incidence of serious AEs increased from 8% to 12%• Median time to onset: 215 days (range 3-887 days)
SAE = AE reported as serious by the investigator, per standard criteria
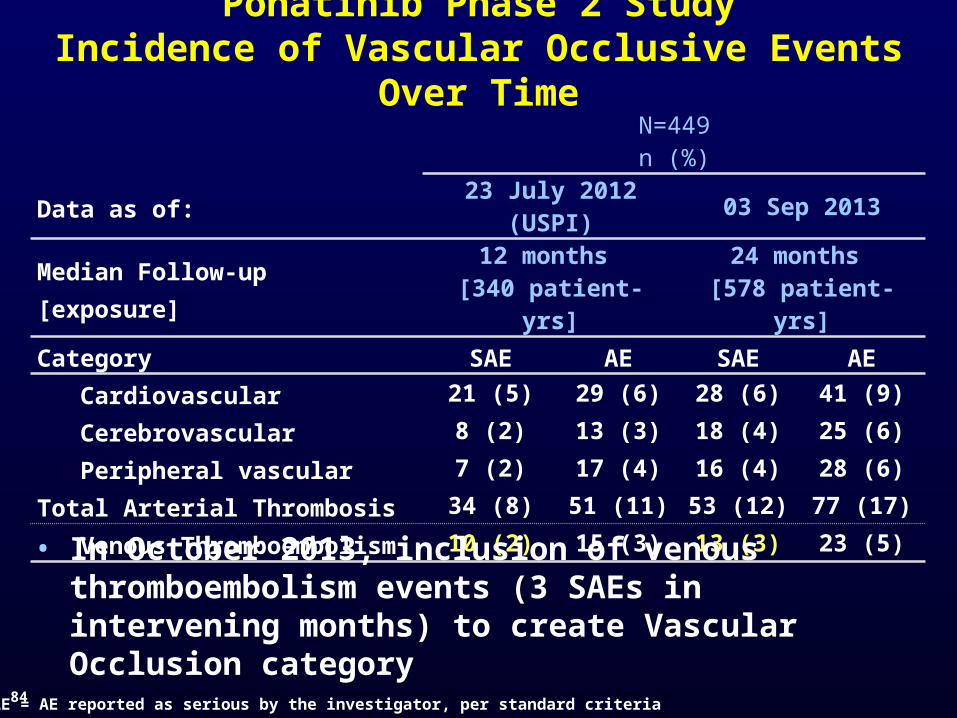
N=449n (%)
Data as of: 23 July 2012 (USPI) 03 Sep 2013
Median Follow-up [exposure]12 months
[340 patient-yrs]24 months
[578 patient-yrs]
Category SAE AE SAE AE Cardiovascular 21 (5) 29 (6) 28 (6) 41 (9)
Cerebrovascular 8 (2) 13 (3) 18 (4) 25 (6)
Peripheral vascular 7 (2) 17 (4) 16 (4) 28 (6)
Total Arterial Thrombosis 34 (8) 51 (11) 53 (12) 77 (17)
Venous Thromboembolism 10 (2) 15 (3) 13 (3) 23 (5)
84
• In October 2013, inclusion of venous thromboembolism events (3 SAEs in intervening months) to create Vascular Occlusion category
Ponatinib Phase 2 StudyIncidence of Vascular Occlusive Events Over Time
SAE = AE reported as serious by the investigator, per standard criteria
Ponatinib Phase 2 Study Impact of Dose Modification on
Response
85
• 149 CP-CML patients achieved MCyR by 12 mos
• Among patients who dose reduced after achieving response– 97% (62/64) maintained MCyR– 96% (51/53) maintained CCyR– 92% (34/37) maintained MMR
For additional information, see Poster 4007, Monday Dec. 9, 6-8pm
Ponatinib Phase 2 Study - PACE2 Year Follow-up Summary
• Confirmed substantial clinical activity in heavily pretreated patients with BCR-ABL+ leukemias
• Early, deep, and durable responses were observed; 89% maintained MCyR for at least 2 yrs in CP-CML
• Arterial thrombotic events occurred; higher dose intensity, older age, presence of other risk factors at baseline associated with higher likelihood of event
• Ponatinib is an important treatment for patients in whom the need and potential benefit outweigh the potential risk
86
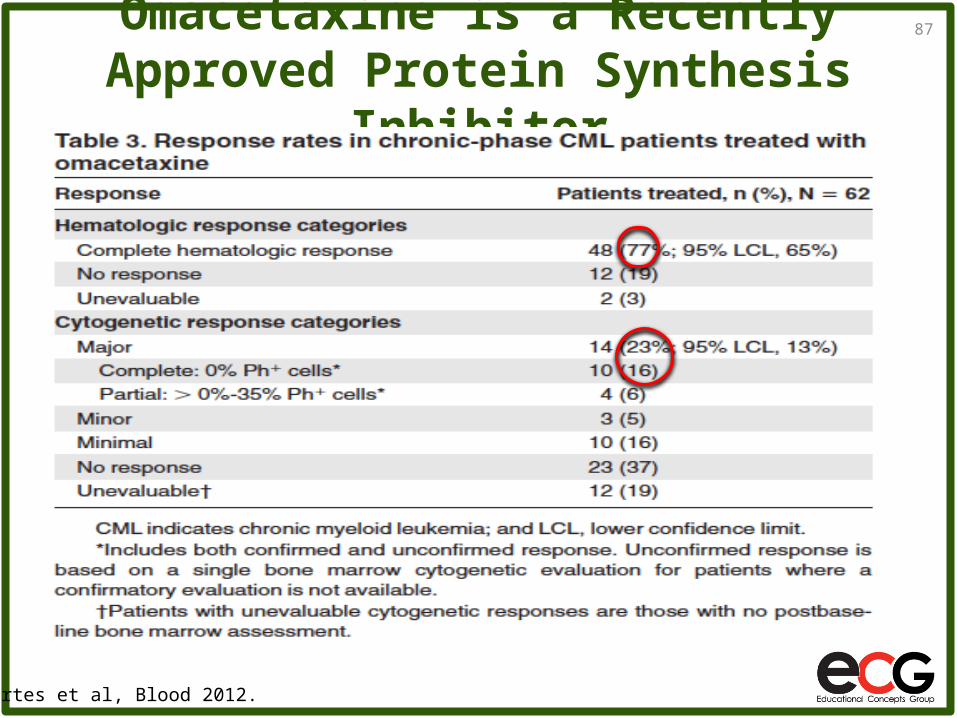
Omacetaxine is a Recently Approved Protein Synthesis Inhibitor
87
Cortes et al, Blood 2012.
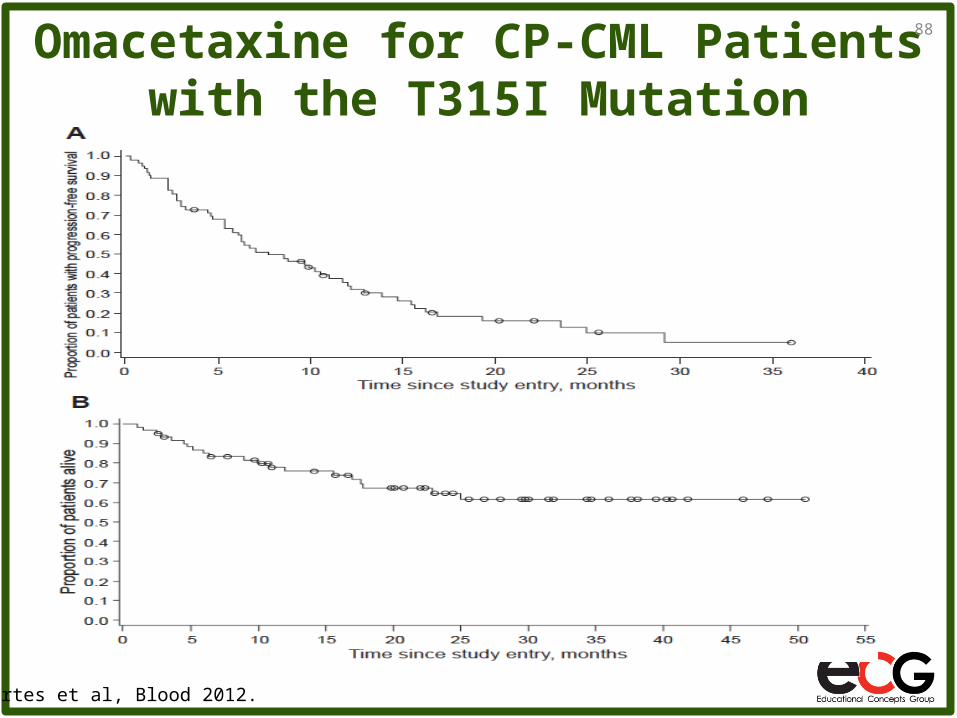
Omacetaxine for CP-CML Patients with the T315I Mutation
88
Cortes et al, Blood 2012.
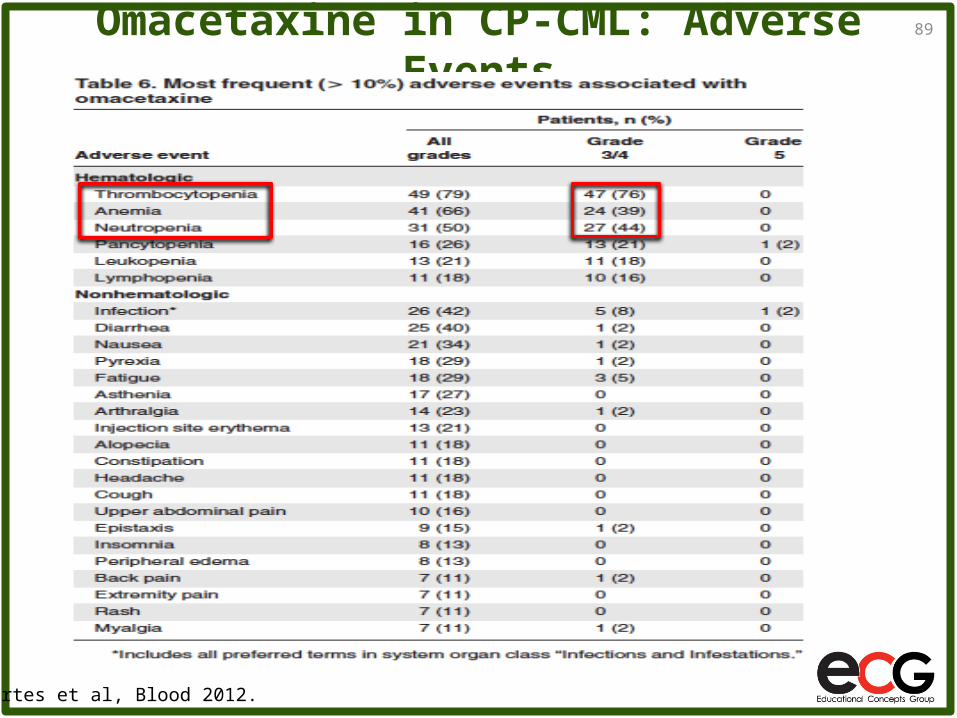
Omacetaxine in CP-CML: Adverse Events89
Cortes et al, Blood 2012.
Omacetaxine Conclusions
Omacetaxine is a first-in-class protein synthesis inhibitor with modest activity in highly pretreated CP-CML and accelerated phase patients, including those with the BCR-ABL T315I mutation
Response duration appears to be modest• Nine of 108 patients remain on treatment after ~5 years
Grade 3/4 myelosuppression is common Non-hematologic grade 3/4 toxicities are uncommon Omacetaxine was approved by the US FDA in
October 2012 for the treatment of imatinib-resistant (≥2 prior TKIs) chronic and accelerated phase CML
90
TKI-specific resistant mutations
• Dasatinib is inactive against V299L, T315A/I, F317I/L/V
• Nilotinib is inactive against Y253H, E255K/V, T315I, F359C/I/V
• Bosutinib is inactive against V299L, T315I
• Ponatinib is believed to be active against all single mutations, but should be used with caution due to its cardiovascular profile
• Omacetaxine is approved for patients with disease that is resistant or intolerant to two or more TKIs, irrespective of mutation status
• There is now an effective tyrosine kinase inhibitor option for every known imatinib-resistant BCR-ABL kinase domain mutation
Conclusions - I • Imatinib is favorably impacting survival in patients with chronic
phase CML
~65% are estimated to be on imatinib in CCyR after 7 years
~25% of patients meet the definitions of resistance within the first 18 months of therapy
• Dasatinib, nilotinib, bosutinib and ponatinib are effective in cases of imatinib -resistant and -intolerant chronic and accelerated phase of CML
• Nilotinib and dasatinib are approved for the treatment of newly diagnosed chronic phase CML patients
• Achieving a reduction in BCR-ABL transcript level to ≤10% after 3 months of TKI treatment is associated with superior outcomes. The slope of decline may be particularly important
Conclusions - II • Loss of response to the second generation TKIs dasatinib, nilotinib
and bosutinib is most often due to a small number of BCR-ABL kinase domain mutations (~5), commonly the T315I mutation
In cases where the T315I mutation is not the cause of resistance to one of these drugs, it is reasonable to try treatment with an alternate second-generation TKI (certain mutations excepted)
Ponatinib may be effective against all single BCR-ABL mutants, but due to safety concerns, it should only be used in patients who have no other acceptable TKI options
• In a subset of patients with the T315I mutation, deep cytogenetic responses have been observed in clinical studies of ponatinib, omacetaxine, MK-0457 and PHA-739358
• Adequate monitoring of disease burden in CML patients is essential, and CML patients are encouraged to consult with a CML expert to ensure their disease is being optimally managed
Challenges• In 2014, the remaining frontiers for the management of
CML are
Improving outcomes in advanced phase CML patients
Understanding and treating mechanisms of BCR-ABL-independent resistance to TKIs
Eliminating the small proportion of CML cells that remain in most patients with deep responses so that they may be able to discontinue therapy altogether (“true cure”)
• Studies with investigational agents are currently ongoing
• The continued participation of CML patients in clinical trials is essential to further improve treatment outcomes