neue antikoagulantien bei spontaner und tumor-assoziierter vte paul kyrle univ. klinik f. innere...
TRANSCRIPT
Neue Antikoagulantien bei spontaner
und Tumor-assoziierter VTE
Paul KyrleUniv. Klinik f. Innere Medizin I
AKH/Medizinische Universität Wien

Treatment of VTE: past, present and future
Heparin Vitamin K antagonists
Heparin Dabigatran/Edoxaban
Rivaroxaban/Apixaban

Treatment of VTE
acute subacute extended
up to 2 weeks up to 3 - 6 months > 6 months

Schulman, N Engl J Med 2009
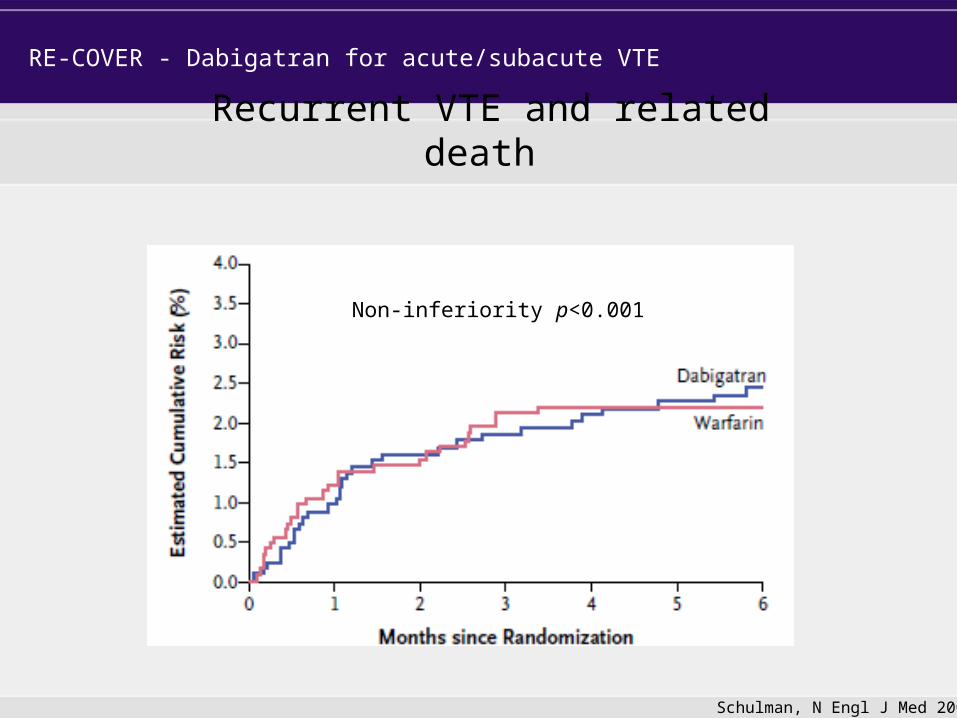
Recurrent VTE and related death
RE-COVER - Dabigatran for acute/subacute VTE
Non-inferiority p<0.001
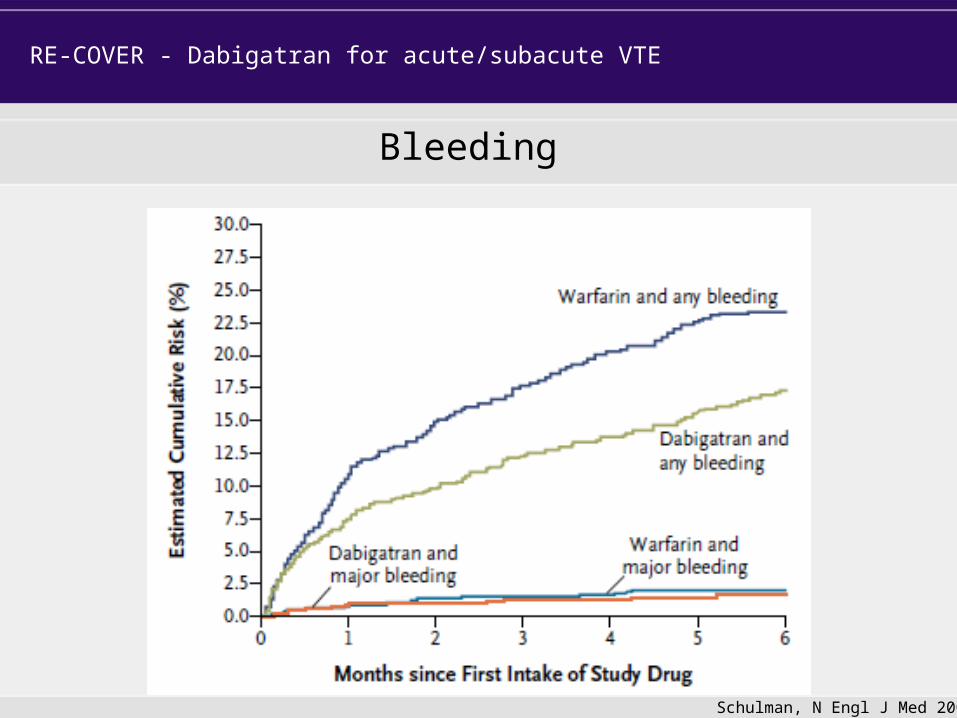
RE-COVER - Dabigatran for acute/subacute VTE
Schulman, N Engl J Med 2009
Bleeding

Oral Rivaroxaban for the Treatment of Symptomatic Venous Thromboembolism: A Pooled Analysis of the EINSTEIN DVT and EINSTEIN PE Studies
Harry R Büller on behalf of the EINSTEIN Investigators

EINSTEIN DVT and EINSTEIN PE studies
Randomized, open-label, event-driven, non-inferiority studies of identical design with a priori specified combined analyses
Primary efficacy outcome: first recurrent VTE Principal safety outcome: first major or non -major clinically relevant bleeding
1. The EINSTEIN Investigators. N Engl J Med 2010;363:2499–510; 2. The EINSTEIN–PE Investigators. N Engl J Med 2012;366:1287–97
15 mg bid
Confirmed DVT without symptomatic
PE1
N=3449 N=8282Rivaroxaban
Day 1 Day 21
Enoxaparin bid for at least 5 days +
VKA, INR 2.0–3.0
Confirmed PE with or
without symptomatic
DVT2
N=4833
Predefined treatment period of 3, 6, or 12 months
20 mg od
30
-da
y p
os
t-s
tud
y
tre
atm
en
t p
eri
odRivaroxaban
R

Rivaroxaban(N=4150)
Enoxaparin/VKA(N=4131)
Males, % 55 54Age, mean, years ± SD 57±17 57±17Weight, n (%)
≤50 kg 75 (1.8) 92 (2.2)>50–100 kg 3477 (84) 3432 (83)≥100 kg 590 (14) 605 (15)
Creatinine clearance, ml/min (%)<30 10 (0.2) 11 (0.3)30–49 322 (8) 311 (8)50–79 1030 (25) 992 (24)≥80 2748 (66) 2787 (67)
Index VTE, n (%)DVT 1699 (41) 1690 (41)PE 1793 (43) 1804 (44)DVT and PE 615 (15) 597 (15)
Unprovoked VTE, n (%) 2003 (48) 2048 (50)Previous VTE, n (%) 791 (19) 819 (20)Active cancer, n (%) 232 (6) 198 (5)
EINSTEIN DVT and EINSTEIN PE pooled analysis: patient characteristics
ITT population

EINSTEIN DVT and EINSTEIN PE pooled analysis: primary efficacy outcome
Number of patients at risk
Rivaroxaban 4150 4018 3969 3924 3604 3579 3283 1237 1163 1148 1102 1034 938
Enoxaparin/VKA 4131 3932 3876 3826 3523 3504 3236 1215 1149 1109 1071 1019 939
0.5
3.0
2.5
2.0
1.5
1.0
0.0
RivaroxabanN=4150
Enoxaparin/VKAN=4131
0 30 60 90 120 150 180 210 240 270 300 330 360
Time to event (days)
Cu
mu
lati
ve e
ven
t ra
te (
%)
HR=0.89; p non-inferiority <0.0001
Mean time in therapeutic range = 61.7%
ITT population

EINSTEIN DVT and EINSTEIN PE pooled analysis: principal safety outcome
Number of patients at risk
Rivaroxaban 4130 3768 3671 3406 3270 3210 1928 1051 1009 936 878 853 453
Enoxaparin/VKA 4116 3738 3618 3330 3186 3125 1711 1025 981 907 857 823 369
Cu
mu
lati
ve e
ven
t ra
te (
%)
RivaroxabanN=4130
Enoxaparin/VKAN=4116
0 30 60 90 120 150 180 210 240 270 300 330 360
14
10
12
8
6
4
2
0
Time to event (days)
First major or clinically relevant non-major bleeding
Rivaroxabann/N (%)
Enoxaparin/VKAn/N (%)
HR (95% CI)p-value
388/4130 (9.4)
412/4116(10.0)
0.93 (0.81–1.06) p=0.27
Safety population

EINSTEIN DVT and EINSTEIN PE pooled analysis: major bleeding
Number of patients at risk
Rivaroxaban 4130 3921 3862 3611 3479 3433 2074 1135 1095 1025 969 947 499
Enoxaparin/VKA 4116 3868 3784 3525 3394 3348 1835 1109 1065 990 950 916 409
0.5
3.0
2.5
2.0
1.5
1.0
0.0
RivaroxabanN=4130
Enoxaparin/VKAN=4116
0 30 60 90 120 150 180 210 240 270 300 330 360
Time to event (days)
Cu
mu
lati
ve e
ven
t ra
te (
%)
First major bleeding
Rivaroxabann/N (%)
Enoxaparin/VKAn/N (%)
HR (95% CI)p-value
40/4130 (1.0)
72/4116(1.7)
0.54 (0.37–0.79) p=0.002
Safety population

Treatment of VTE - conclusion
acute subacute extended
up to 2 weeks up to 3 - 6 months > 6 months
NOACS as safe and effective
NOACS as effective, but safer

Risk of recurrence after unprovoked VTE
Kyrle, Rosendaal & Eichinger, Lancet 2010

Confirmed symptomatic DVT or PE completing 6 or 12 months of
rivaroxaban or VKA in EINSTEIN VTE
program
Rivaroxaban 20 mg od
PlaceboDay 1
R
N=1,197
Treatment period of 6 or 12 months
30-d
ay o
bse
rvat
ion
al p
erio
d
Confirmed symptomatic DVT or PE completing
6 or 12 months of VKA
~53%
~47%
Randomized, double-blind, placebo-controlled, event-driven (n=30), superiority study
EINSTEINext - Rivaroxaban for extended thromboprophylaxis after VTE
Study design
EINSTEIN Investigators, NEJM 2011

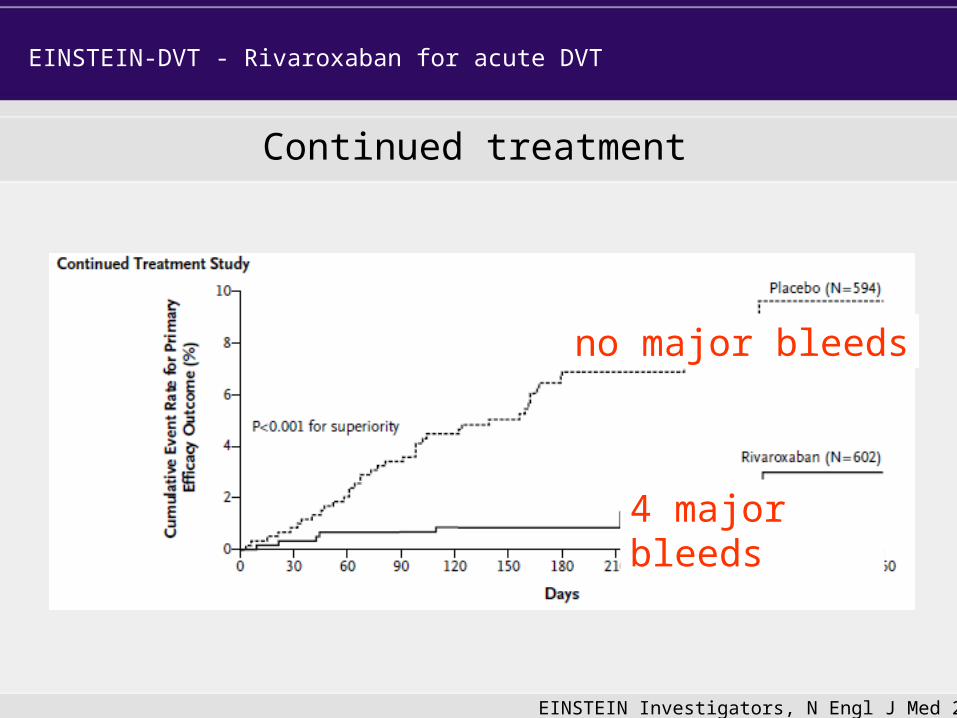
Continued treatment
EINSTEIN-DVT - Rivaroxaban for acute DVT
EINSTEIN Investigators, N Engl J Med 2010
Continued treatment
EINSTEIN-DVT - Rivaroxaban for acute DVT
EINSTEIN Investigators, N Engl J Med 2010
4 major bleeds
no major bleeds

AMPLIFY - Extended
Agnelli, NEJM 2012

AMPLIFY - Extended
Agnelli, NEJM 2012


RESONATE

RESONATE

Time to first VTE or VTE-related death

Risk of first onset of any bleeding

0
0,5
1
1,5
2
2,5
3
Dabigatran 150 mg bid Warfarin13/1430
Major bleeding
0.9%
1.8%
HR 0.52 (95% CI: 0.27–1.02)
25/1426
Per
cen
tag
e
p = 0.058
On treatment
48% RRR
RRR, relative risk reduction.
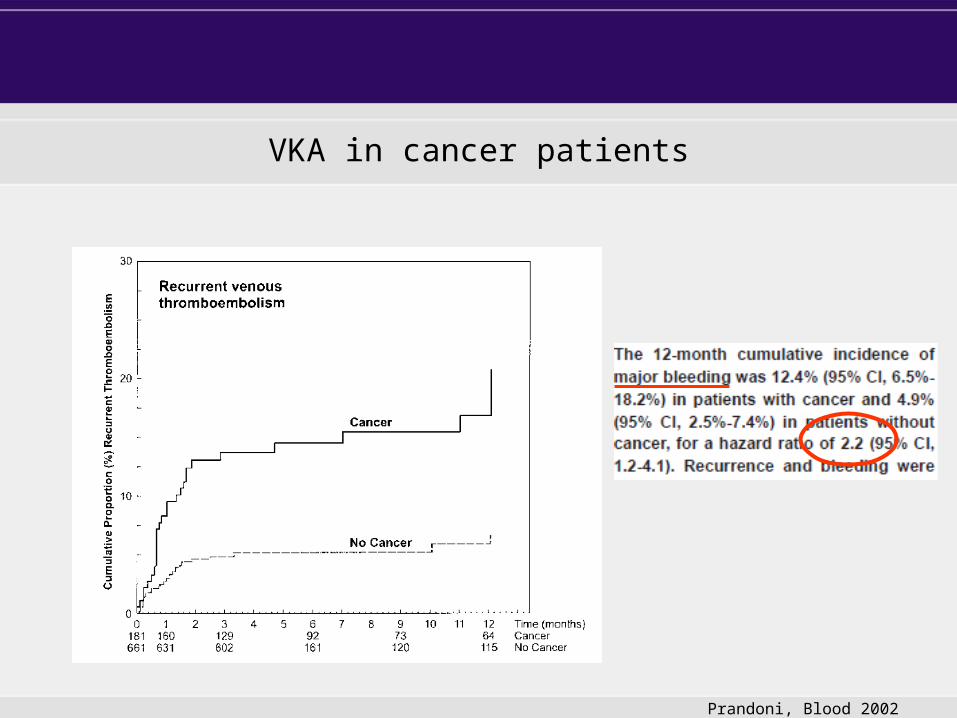
VKA in cancer patients
Prandoni, Blood 2002

Prandoni, Blood 2002
VKA in cancer patients

CLOT (Lee, NEJM 2003)
Major bleeding:Dalteparin 19/338 (6%)VKA 12/335 (4%)p = 0.3

VTE and cancer ACCP 2012
• LMWH over VKA (2B)• VKA over NOACs (2C)
• Dalteparin– once daily 200 IU/kg body weight s.c.– dose reduction to 75 - 85% of therapeutic dose after 4 weeks

EINSTEIN DVT and EINSTEIN PE pooled analysis: outcomes in patients with cancer
Outcome
Rivaroxaban Enoxaparin/VKAHR
(95% CI)n/N % n/N %
Recurrent VTE
Cancer 6/232 2.6 8/198 4.00.62
(0.22–1.80)
No cancer 80/3918 2.0 87/3933 2.2 0.91(0.67–1.24)
Major bleeding
Cancer 6/232 2.6 8/196 4.1 0.61(0.21–1.77)
No cancer 34/3898 0.9 64/3920 1.60.53
(0.35–0.80)

RE-COVER
Dabigatran in VTE cancer patients
D W

Advantages of NOACs in cancer patients with VTE
• oral route better quality of life/adherence• short half-life better flexibility• at least as effective and safe as VKA

Caveats für using NOACs in cancer patients with VTE
• Small patient numbers in clinical trials • Generalizability of trial data (low-risk pts)• Oral route in pts with nausea, vomiting and
diarrhea• Interaction with chemotherapy
• No on-going trials, neither with LMWH nor with NOACs
Summary
• as effective as LMWH/VKA• less (major) bleeding• single drug approach (rivaroxaban, apixaban)• effective in VTE long-term prevention (up to 1
year)• suitable for selected cancer patients
NOACs for treatment of VTE