nutrition dr. sarita mangukiya assistant professor biochemistry, gmcs
TRANSCRIPT

NUTRITION
Dr. Sarita MangukiyaASSISTANT PROFESSORBIOCHEMISTRY, GMCS


NUTRITION
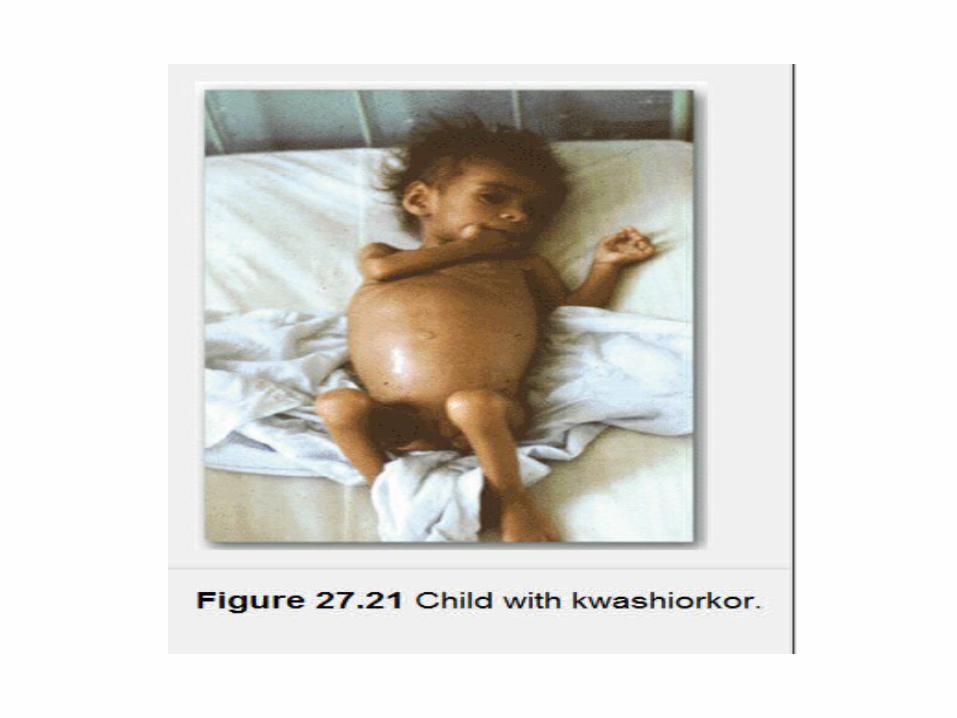
• Protein Energy Malnutrition:– Predominantly in children– Developing & underdeveloped countries– 20 – 50% prevalence– Marasmus kwarshiorkar
To waste sickness of older child when the next child is born.

Kwarshiorkar Marasmus
< 5 yr < 1 yrs
Weaning with intake of low protein high CHO diet
Premature weaning with low CHO/protein food
Milder atrophy & thining of muscles. Less emaciated look due to oedema
Severe atrophy of limb, abdominal muscles with emaciation.growth failure
Patchy hyperpigmentation, exfoliation, ulceration
Dry, thin wrinkled skin devoid of subcutaneus fat
Atrophy of int. mucosa, pancreatic acini. Failure of digestion. Diarrhoea & flatlulence.
Atrophy of int. mucosa, pancreatic acini. Failure of digestion. Diarrhoea & flatlulence.
Marked Hypoabuminemia Hypoalbuminemia

Kwarshiorkar Marasmus
Enlarged & fatty Liver. Decreased chol, Trig, -lipoproteins
Sometimes hepatic cirrhosis without fatty infiltration
Anemia, hypoglycemia low BMR, low body temp
Anemia, hypoglycemia low BMR, low body temp
poor brain dev. Low IQ Lower brain dev.
Normal / high insulin, normal / low cortisol, adrenaline
Low blood insulin, high cortisol, adrenaline



• Deficiency of the amino acid methionine, a precursor of cysteine, may also contribute.
• Cysteine is one of the three amino acids present in glutathione, the body's major antioxidant.
• If the tissues levels of glutathione decline, this could result in free radicals damaging various molecules and tissues and perhaps damaging cell membranes, increasing their permeability.

Treatment
• Treat secondary infection• Oral supplement of nutrition• Parenteral or enteral nutrition

Obesity
• Obesity is a disorder of body weight regulatory systems characterized by an accumulation of excess body fat.
• As adiposity has increased so has the risk of developing associated diseases, such as diabetes, hypertension, and cardiovascular disease

Assessment of Obesity
• body mass index (BMI) -The BMI gives a measure of relative weight, adjusted for height.
• BMI = (weight in kg)/(height in meters)2• Healthy range for the BMI- 19.5 to 25.0. • Overweight -25 and 29.9• Obese- equal to or greater than 30.

Anatomic differences in fat deposition
Biochemical differences in regional fat depots
• Abdominal subcutaneous fat and Visceral fat- Metabolically active than lower body subcutaneous fat.
• Endocrine function of adipocyte• Importance of Portal circulation
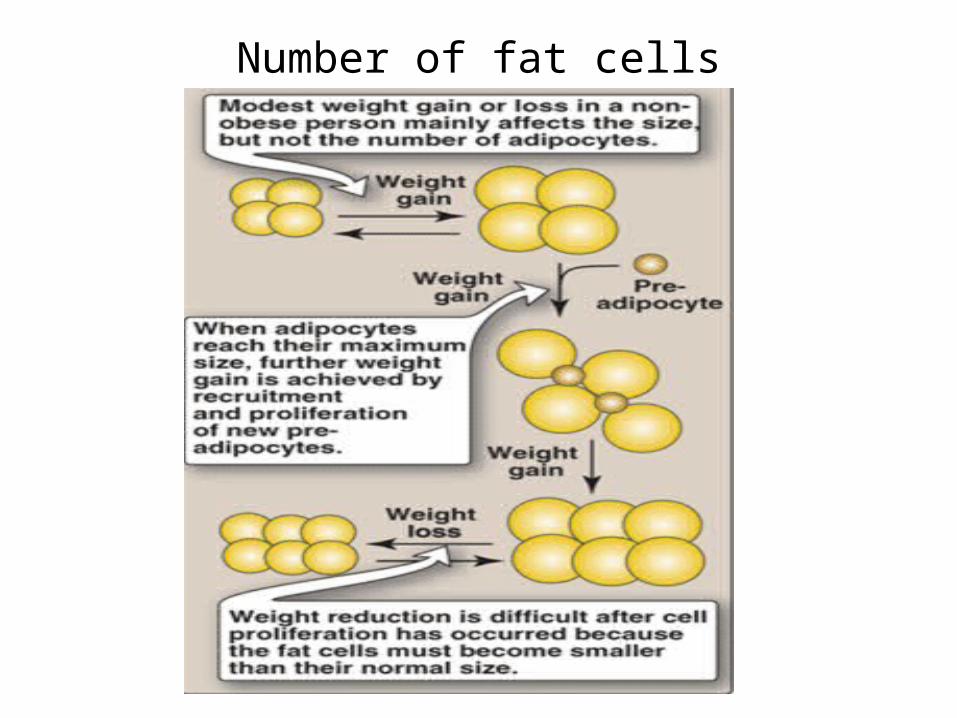
Number of fat cells

Body Weight Regulation
• Genetic contributions to obesity- identical twins , Families
• Environmental and behavioral contributions– ready availability of palatable, energy-dense
foods,– sedentary lifestyles, encouraged by TV watching,
automobiles, computer usage, and energy-sparing devices in the workplace and at home, decrease physical activity and enhance the tendency to gain weight.


Molecules that Influence Obesity
• Long term signals- Leptin, Insulin

• Short term Signals-– GIT- Ghrelin (Appetite stimulating hormone)– CCK, Peptides- action on gastric empyting and
neural signals to hypothalamus. (Satiety)– Hypothalamus- Neuropeptides(NPY, α- MSH) and
neurotransmitter (serotonine and dopamine)

Metabolic Changes Observed in Obesity
• Dyslipidemias, • Glucose intolerance, and • Insulin resistance• Hypertension

Weight Reduction
• Physical activity• Caloric restriction• Pharmacologic and surgical treatment