nutritional modulation of the efficacy and toxicity of ... document… · cisplatin, carboplatin,...
TRANSCRIPT

Nutritional modulation of the
efficacy and toxicity of
chemotherapyVickie E Baracos, PhD
Department of Oncology
University of Alberta, Canada

Outline
• Therapeutic index - definition
• Types of chemotherapy
• Chemotherapy toxicity
• Nutritional modulation of therapeutic index
– Fish oil, glutamine, Vitamin E
• Interpretations

Cancer treatment, toxicity & efficacy
• cancer treatment approaches combine surgery,
cytotoxic or targeted chemotherapy and
radiation, multiplying nutritional risk.
• systemic antineoplastic agents have characteristic
toxicities, limiting the dose and duration of
cancer therapy
• Specific nutrients are proposed to improve the
therapeutic index of cancer treatments by
increasing their efficacy, reducing toxicity or both.

Efficacy and Toxicity:Therapeutic index

Efficacy and Toxicity
• Treatment at Maximum Tolerated Dose (MTD)
• Narrow therapeutic index of most cancer tx

Toxicity outcomes
• Patients experience limitations in their
chemotherapy treatment:
– dose reductions
– delays in therapy
– discontinuation of therapy.
• Toxicities also worsen malnutrition and
wasting

Types of chemotherapy
• Grouped into different classes based on mechanism of action.
• Drugs of different classes are combined to increase antitumor effects.
• Drugs in different classes have different side effect profiles
– Combination therapy often based on avoiding overlapping toxicities.

•act on rapidly dividing
cancer and normal cells
•Alkylating agents
interfere with DNA base
pairing, leading to strand
breaks.
•Topoisomerase inhibitors
prevent DNA uncoiling.
•Taxanes and vinca
alkaloids interfere with
microtubule function
required for mitosis.
•Antimetabolites block the
formation and use of
nucleic acids.
Mechanisms of cytotoxic
chemotherapy

•Receptor tyrosine kinases and
downstream RAS/RAF/MAPK and
PI3K/AKT/mTOR signaling pathways
are activated for proliferation and
invasion by tumor cells
•Molecular cancer therapeutics target
these pathways
•Some drugs (e.g., sorafenib [Nexavar],
sunitinib [Sutent], imatinib [Gleevec])
have multiple targets
EGFR = epithelial growth factor
receptor; VEGF = vascular endothelial
growth factor.)
Mechanisms of targeted
therapies

Chemotherapy side
effects and toxicities

Target of rapamycin (TOR) is a kinase
that integrates signals from nutrients
(amino acids and energy) and growth
factors to regulate cell growth, cell
cycle progression and protein
synthesis in tissues such as skeletal
muscle.
Nutrient utilization and the pathways
affected by targeted therapies
Glass DJ. PI3 kinase regulation of skeletal muscle hypertrophy and atrophy.
Curr Top Microbiol Immunol. 2010;346:267-78. Review.

Sorafenib causes muscle
wasting independent of disease
progression
Mean loss ~ 2.1 kg muscle
during 1 y on sorafenib

Cisplatin, carboplatin, oxaliplatin
• Binds to guanine residues in DNA, inhibits replication
• Cell-cycle nonspecific, kills all dividing cells
• Common uses
– Gastrointestinal tumors, Lung, Germ Cell, Ovarian cancer
Toxicities:
• Severe nausea/vomiting
• Nephropathy
• Chronic, cumulative sensory neuropathy
• Ototoxicity, high-frequency hearing loss
• Alopecia
• Myelosuppression
• Dysgeusia

Irinotecan
• DNA Topoisomerase inhibitor
• Used in metastatic colorectal cancer, pancreatic, gastric cancers
Toxicities:
• Diarrhea as major side effect
• Late diarrhea (>24 hours) may be insensitive to loperamide
• Incidence of severe diarrhea: 31-39%
• Life-threatening for 8% of patients

Can diet make a difference? Nutritional
modulation of therapeutic index
Glutamine,
Vitamin E
Reduced
toxic effect ?
N-3 fatty
acid
increase
therapeutic
effect ?
Widening the
therapeutic
index

Quantity and quality of evidence for dietary
alteration of therapeutic index
• Animal studies
• Small number of studies
• Heterogeneous design
• Low ability to translate to clinical setting
• Human studies
• Small number of studies
• Low n
• Non-randomized
• Heterogeneous design and outcomes
• Lack of dose-finding studies
• Contamination between treatment arms (patients self-treat)

Clinical studies n-3 polyunsaturated fatty acids

Bougnoux P, et al. Improving outcome of chemotherapy of metastatic breast cancer
by docosahexaenoic acid: a phase II trial Br J Cancer. 2009 ;101(12):1978-85
•Metastatic breast cancer
•FEC 75 chemotherapy regimen (5-fluorouracil, epirubicin,
cyclophosphamide) , the standard first-line chemotherapy in
a metastatic setting
•Prospective open-label phase II trial
•1.8g/day of purified DHA

Differential incorporation of DHA

Time to tumor progression by DHA incorporation

Overall survival by DHA incorporation

Murphy RA et al. Supplementation with fish oil increases first-line
chemotherapy efficacy in patients with advanced nonsmall cell lung cancer.
Cancer 2011 , 117: 3774–3780
•Non-small cell lung cancer patients stage IIIB/IV
receiving 1st line platinum-based chemotherapy
•Matched fish oil supplemented (n=14) patients
compared with standard of care controls (n=31).
•Patient’s choice of supplementation with:
1) 4 capsules/d (2.5 g EPA + DHA) OR
2) 1.5 tsp/d fish oil liquid (2.5 g EPA +DHA)

Median 2.75%
High EPA incorporators
N=9
Low EPA incorporators N=7
Incorporation of EPA into plasma phospholipid was variable

0
10
20
30
40
50
60
Fish Oil
Std Care
%
Chemotherapy outcomes
Fish oil favoring
Increase partial
response
Decreased progressive
disease, p= 0.008

Witte TR et al RBC and WBC fatty acid composition following consumption of
an omega 3 supplement: lessons for future clinical trials. Lipids Health Dis.
2010 Mar 22;9:31

Interpretation
• Potentially interesting findings
• Still needed:
– Essential fatty acid status of patients throughout
the cancer trajectory
– A basis for dose; target levels in plasma? Cells?
– Purified DHA or EPA versus fish oil unclear
– Randomized designs needed
– Individual drug or regimen interaction with diet

Clinical studies glutamine
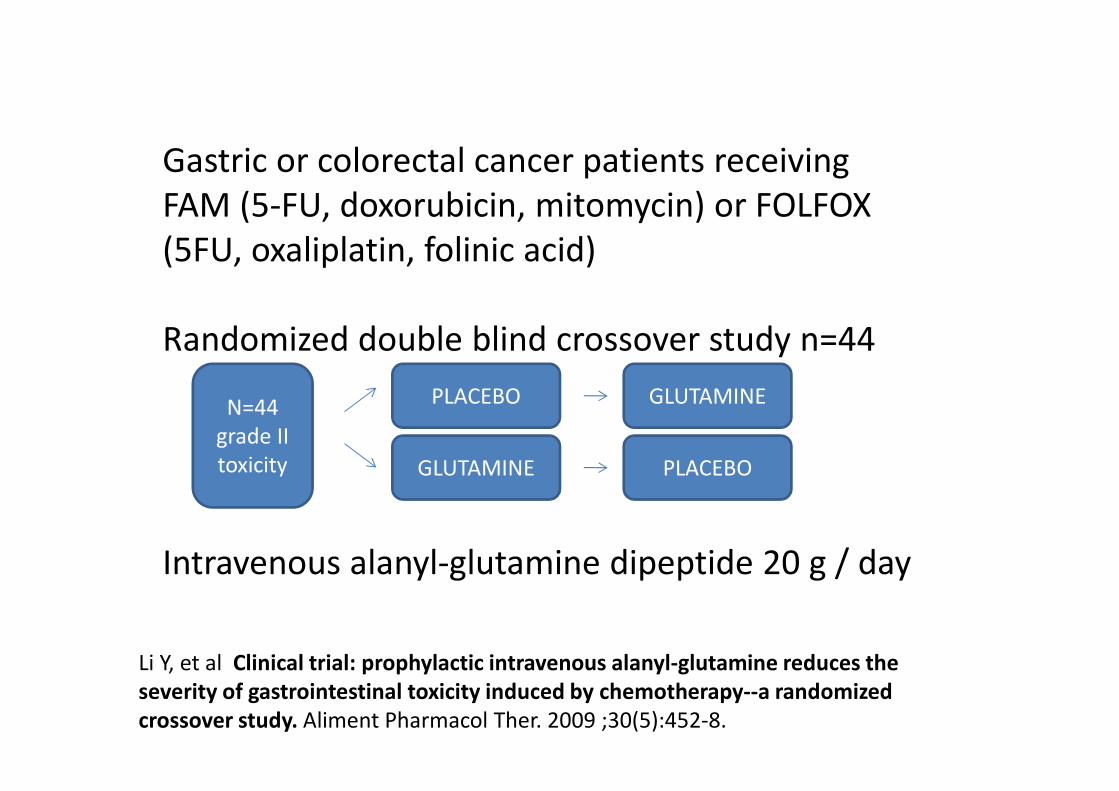
Li Y, et al Clinical trial: prophylactic intravenous alanyl-glutamine reduces the
severity of gastrointestinal toxicity induced by chemotherapy--a randomized
crossover study. Aliment Pharmacol Ther. 2009 ;30(5):452-8.
Gastric or colorectal cancer patients receiving
FAM (5-FU, doxorubicin, mitomycin) or FOLFOX
(5FU, oxaliplatin, folinic acid)
Randomized double blind crossover study n=44
Intravenous alanyl-glutamine dipeptide 20 g / day
N=44
grade II
toxicity
PLACEBO
GLUTAMINE PLACEBO
GLUTAMINE

Also noted reduced plasma endotoxin levels in glutamine – treatment
period.

Vahdat L et al. Reduction of paclitaxel-induced peripheral neuropathy with
glutamine. Clin Cancer Res. 2001 May;7(5):1192-7.
•Metastatic breast cancer
•High dose paclitaxel as part of a regimen to ablate bone
marrow (followed by haematopoetic stem cell replacement)
•Successive cohorts without (n=33) and with (n=12)
glutamine treatment
•30 g/ d glutamine orally

Also improved by glutamine: motor weakness (p=0.04), gait
(p=0.0016), activities of daily living (p=0.001). No difference in nerve
conduction studies (amplitude and conduction velocity of motor or
sensory nerves)

Wang WS et al. Oral glutamine is effective for preventing oxaliplatin-induced
neuropathy in colorectal cancer patients Oncologist. 2007 Mar;12(3):312-9.
•Metastatic colorectal cancer
•FOLFOX regimen (5Fluorouracil, oxaliplatin, folinic acid)
•Randomized but not blinded or placebo controlled n=42
glutamine, 44 control
•30 g/ d glutamine orally

Incidence of neuropathy assessed according to Common Toxicity Criteria

Clinical outcomes of oral glutamine supplementation
Interpretation
• Potentially interesting findings suggesting
clinical benefit for GI toxicity and neuropathy
• Requires randomized, placebo controlled
designs
• Reproducible / objective quantification of
peripheral neuropathy is a challenge

Clinical studies Vitamin E and
chemotherapy – induced neuropathy

• Solid tumors, cumulative dose of cisplatin > 300
mg/m2
• Randomized, blinded and placebo controlled
n=17 supplemented, n=24 placebo
• Alpha tocopherol 400 mg/d
Pace A et al Vitamin E neuroprotection for cisplatin neuropathy: a randomized,
placebo-controlled trial. Neurology. 2010;74(9):762-6

Improved by Vitamin E 400 mg/ d
• Incidence and severity of
neurotoxicity (p<0.01)
• % grade 3 sensory
neuropathy (p<0.01)
• Vitamin E prevented fall in
sensory median nerve
amplitude (p<0.01)
0
10
20
30
40
50
Vit E Placebo
5,9
41,7

• Mixed patients on neurotoxic chemotherapy
(taxanes, cisplatin, carboplatin, oxaliplatin or
combination)
• Phase III Randomized, blinded and placebo
controlled n=96 supplemented, n=93 placebo
• Alpha tocopherol 600 mg/d
Kottschade LA The use of vitamin E for the prevention of chemotherapy-induced
peripheral neuropathy: results of a randomized phase III clinical trial. Support Care
Cancer. 2010 Oct 9. [Epub ahead of print] PMID: 20936417

• No significant effects : % grade 2 or greater
sensory neuropathy
• No significant effects: Time to onset or duration of
neuropathy
• No significant effects: Numbness, tingling, pain,
difficulty walking, working
No significant findings

Interpretation
• Randomized placebo controlled
• Single agent cisplatin vs mostly taxanes;
• ? glutamine is effective for taxane – neuropathy and Vitamin E is effective for cisplatin neuropathy
• Further discussion regarding objective and subjective assessment of neuropathy interventions: Albers JW et al Interventions for
preventing neuropathy caused by cisplatin and
related compounds Cochrane Database Syst Rev. 2011 Feb 16;(2):CD005228

Nutritional modulation of therapeutic index
• N-3 fatty acids may left-shift therapeutic effect
• Glutamine and Vitamin E may right-shift toxic effect
Glutamine,
Vitamin E
Reduced
toxic effect
N-3 fatty
acid
increase
therapeutic
effect
Widening the
therapeutic
index

Conclusions
• Specific individual nutrients are proposed to improve the therapeutic index of cancer treatments by increasing their efficacy, reducing toxicity or both
• Nutrition intervention might need to be specific to chemotherapy type / regimen
• Promising candidates include n-3 fatty acids (increased therapeutic efficacy), Vitamin E and glutamine (decreased toxicity)