oncothermia: a new paradigm in cancer therapies
DESCRIPTION
In oncology, the term “hyperthermia” refers to the treatment of malignant diseases by administering heat in various ways. Hyperthermia is usually applied as an adjunct to an already established treatment modality, where tumor temperatures in the range ofTRANSCRIPT

1
Oncothermia: a new paradigm in cancer therapies
Gabriella Hegyi*, Andras Szasz, Oliver Szasz
*Department of Complementary and Alternative Medicine, University of Pecs, Hungary Department of Biotechnics, St.Istvan University, Godollo, Hungary
Historical background
Hyperthermia means overheating of the living object completely (systemic) or partly (regionally or locally). The “overheating” in simple and popular understanding means “higher temperature than normal”. The use of hyperthermia for cancer therapy was first documented by Hippocrates for the treatment of breast tumor [1]. It is in fact the oldest oncology treatment in medicine [2]. The ancient applications of hyperthermia were mainly supported by sacral, philosophical ideas, where the fire (heat, Sun) had the highest level of abilities and freedom. Hyperthermia was also mentioned throughout the Middle Ages [3], but due to the strict Galenus’ school and the inadequate heating techniques, the treatment has never become a standard in the oncology practice. Contrary of this it is not generally accepted as conventional therapy. The problem is its controversial performance. The controversy is originated from the complications of the deep heating and the selection (focusing) of the heat-effect. These challenges are based on bio-physical and engineering problems. This was the reason why the oncotherm development was made by biophysical origins. Oncothermia is a further development of the traditional, more than two thousand years old [4] oncological hyperthermia method. It solves such technical problems, which were blocking the stable applications. The idea of oncothermia solves the selective deep action on nearly cellular resolution [5].
We would like to demonstrate the force and perspectives of oncothermia, as a highly specialized hyperthermia in clinical oncology. Our aim is to prove the ability of oncothermia to be a candidate to become a widely accepted modality of the standard cancer-care. We would like to show the proofs and the challenges of the oncothermia applications, to provide the presently available data and summarize the knowledge in the topic. We concentrate mainly on local/regional hyperthermia with its non-invasive electro-magnetic applications, so whole-body hyperthermia or the RF-ablation techniques will not get much attention and neither will the ultrasound and other heating techniques. The state of oncological hyperthermia today is similar to that of radiology at its infancy. Like many early-stage therapies, it lacks adequate treatment experience and long-range, comprehensive statistics that can help us optimize its use for all indications.
Change of paradigm
The traditional hyperthermia is controlled the only single thermodynamic intensive parameter, with the temperature. Oncothermia is based on the paradigm of the energy-dose control, replacing the single temperature concept [6], [7], [8]. With this approach oncothermia returned to the gold standards of the dose concepts in medicine: instead of the parameter, which can not regarded as dose (the temperature

2
does not depend on the volume or mass), oncothermia uses the energy (kJ/kg [=Gy]), like the radiation oncology uses the same (Gy) to characterize the dosing of the treatment. The requested job is to kill the malignant cells, for what a definite energy dose is necessary [9]. The historical energy-dose-like control (temperature multiplied by its application time), is physically incorrect, and operates with an overall energy average in the area, instead of a directed and well measurable energy-dose (measured in kJ). The high energy application could cause controversies: the high temperature burns the malignant cells but because it’s missing selectivity it damages the healthy cells and starts unwanted physiological reactions as well as enlarged dissemination possibility. These conditions make the hyperthermia effect not controlled, irrespective that the temperature could be kept on a certain level in the tumor or not. In reality the selectivity which would be necessary for the actions is missing, and the heating attacks all the cells in the target, and also unselectively provokes the psychological control and regulation. The original idea of the hyperthermia was the “fire by fire” concept: set a controlled contra-fire depleting the possible fire-supply, blocking the coming large bush-fire endangering a house. The heated tumor is forced to higher metabolism; high metabolic rate of the cancer lesion is gained by elevated temperature. However, when the surrounding is intact, it delivers the same amount of nutrients than before, does not deliver more glucose for the forced metabolism Figure 1. The tumor very quickly deflates from nutrients, empties all its energies, suffers and burns away. However, by the large heating energy heats up the healthy surrounding us well, see Figure 2., the blood-flow will be enhanced, the nutrients supply will be higher, we make opposite than our aim was to do. The situation became even worst by continuing the high-energy heating: the high blood-flow helps the dissemination [10] and could gain the metastases Figure 3. With this we can definitely worsen the survival and the quality of life of the patient.
heated tumorforced metabolic rate without extra supply
unheated healthy surroundingsproviding only regular supply to cancer
Figure 1. The focused local heating situation, expecting the locality for longer time
heated tumor forced metabolic rate with extra supply by extended blood-flow
heated healthy surroundingssupplying the cancer by nutrients
Figure 2. The real situation heats up the surroundings, the local heating does not remain locally
focused

3
larger heated volume by heat-flow, out of control, high dissemination of malignant cells
Figure 3. The large heated volume is not controlled from the focusing, and makes possibility of the
malignant dissemination by the high blood-flow in the healthy surroundings
The blood-flow is an important thermodynamic modification factor, which makes the dominant addition to the temperature development in the tumor. According to the fits of measurements, [11], actually the blood-flow for tumor - and the healthy tissues are both definitely temperature dependent, and in general there is a threshold when the blood-flow of the tumor became lower than the blood-flow of the healthy surroundings. Below this threshold the efficacy of radiotherapy (which is propositional with the oxygenation of the tissue) and the chemotherapy, which is proportional with the drug-concentration in the tissue) is growing by the increasing of the temperature, due to both of these properties are delivered by the increasing blood-flow. However, the complementary therapies over the threshold are suppressed by the decreasing of the blood-flow in the tumor, Figure 4.
<40 C >40 oChealthy tumor healthy tumor
Radio-efficacy;(pO2)
Chemo-efficacy (drug-penetration)
Blood-flow
Possible cell-dissemination( ! )
_ _
Abs
olut
e bl
ood-
flow
37 38 39 40 41 420
0.5
1
1.5
2
2.52.5
0
ymiyfi
yti
QmT( )iQ0
4237 Ti
tumormuscle
fat
Metabolic rate/3000
37 38 39 40 41 420
0.5
1
1.5
2
2.52.5
0
ymiyfi
yti
QmT( )iQ0
4237 Ti
tumormuscle
fat
Metabolic rate/3000
37 38 39 40 41 420
0.5
1
1.5
2
2.52.5
0
ymiyfi
yti
QmT( )iQ0
4237 Ti37 38 39 40 41 420
0.5
1
1.5
2
2.52.5
0
ymiyfi
yti
QmT( )iQ0
4237 Ti
tumormuscle
fat
Metabolic rate/3000
37 38 39 40 41 420
0.5
1
1.5
2
2.52.5
0
ymiyfi
yti
QmT( )iQ0
4237 Ti37 38 39 40 41 420
0.5
1
1.5
2
2.52.5
0
ymiyfi
yti
QmT( )iQ0
4237 Ti
tumormuscle
fat
Metabolic rate/3000
Temperature
Below Threshold → Above
Figure 4. Blood-flow changes and its consequences below and above 42 ºC for healthy and tumorous
tissues
4
Oncothermia technology heats non-equally; concentrating the absorbed energy to the intercellular electrolytes [12]. This method creates inhomogeneous heating, microscopic temperature differences far from thermal equilibrium. The definitely large temperature gradient between the intra- and extracellular liquids changes the membrane processes, ignites signal pathways for natural programmed cell-death, avoiding the toxic effects of the simple necrosis. The synergy of electric field with the thermal effects potently and selectively makes the job [13]. The clue to find the mechanisms, which could create the requested optimization, selection and control of the energy intake based on the clear biophysical differences between healthy and cancerous cells, finding the biophysical property to focus the energy on the desired cellular membranes.
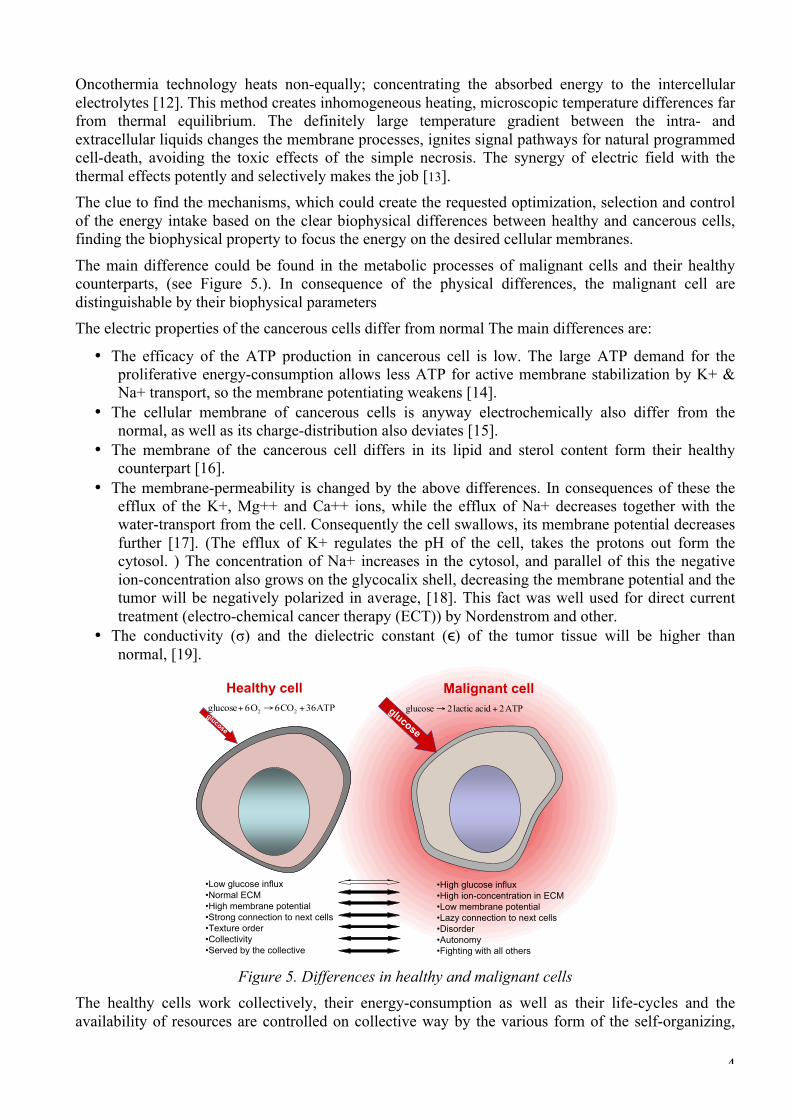
The main difference could be found in the metabolic processes of malignant cells and their healthy counterparts, (see Figure 5.). In consequence of the physical differences, the malignant cell are distinguishable by their biophysical parameters The electric properties of the cancerous cells differ from normal The main differences are:
• The efficacy of the ATP production in cancerous cell is low. The large ATP demand for the proliferative energy-consumption allows less ATP for active membrane stabilization by K+ & Na+ transport, so the membrane potentiating weakens [14].
• The cellular membrane of cancerous cells is anyway electrochemically also differ from the normal, as well as its charge-distribution also deviates [15].
• The membrane of the cancerous cell differs in its lipid and sterol content form their healthy counterpart [16].
• The membrane-permeability is changed by the above differences. In consequences of these the efflux of the K+, Mg++ and Ca++ ions, while the efflux of Na+ decreases together with the water-transport from the cell. Consequently the cell swallows, its membrane potential decreases further [17]. (The efflux of K+ regulates the pH of the cell, takes the protons out form the cytosol. ) The concentration of Na+ increases in the cytosol, and parallel of this the negative ion-concentration also grows on the glycocalix shell, decreasing the membrane potential and the tumor will be negatively polarized in average, [18]. This fact was well used for direct current treatment (electro-chemical cancer therapy (ECT)) by Nordenstrom and other.
• The conductivity (σ) and the dielectric constant (ϵ) of the tumor tissue will be higher than normal, [19].
Healthy cell Malignant cellATP2acidlactic2glucose +→ATP36CO6O6glucose 22 +→+
glucose
glucose
•Low glucose influx•Normal ECM•High membrane potential •Strong connection to next cells•Texture order•Collectivity •Served by the collective
•High glucose influx •High ion-concentration in ECM•Low membrane potential•Lazy connection to next cells•Disorder•Autonomy•Fighting with all others
Figure 5. Differences in healthy and malignant cells The healthy cells work collectively, their energy-consumption as well as their life-cycles and the availability of resources are controlled on collective way by the various form of the self-organizing,

5
[20], [21]. The healthy cells are organized in this way, their standard cycles, reactions and structures are complexly regulated in both internal and external areas. The malignant cells behave completely different way. This process is the “ancient” chemical reaction, which was characteristic at the beginning of the evolution of the life, when the oxygen, the general electron acceptor was available only in a small amount in the atmosphere. It is the fermentative way to utilize the energy of glucose converts it into lactic acid (CH3CHOHCOOH), producing 2 ATPs in one cycle, while the healthy cycle (Krebs cycle) produces 36 ATPs.
The enormously large demand of malignant cells for nutrients not only the ionic density in the surrounding makes the malignant cells distinguishable, but their structure is also very different. Their demand for the huge energy-production pushes them for the permanent competition for the sufficient amount of nutrition. The cells became independent competitors instead of the normal cooperation, and the harmony had been replaced by autonomy. The intercellular contacts which was in healthy network are broken in cancer, the order of the tissue had been lost, the “social signal” [22] between the cells vanish. The malignant cells become disordered, non-connected and isolated [23], [24]. The malignancy has definitely different structure that its healthy counterpart, its dielectric constant and optical refractive index deviates from normal. The lost intercellular contacts block the natural control over the structural changes, and the disordered structure changes the optical properties also.
Advantage of oncothermia, that while the classical artificially focused hyperthermia has to heat up in case of the multiple lesions overlapping all the volume, which contains these lesions; contrary, oncothermia automatically focuses on the lesions in their multiple places, without treating the healthy tissue between, see Figure 6.
(a) (b) Figure 6. The overall heating of a volume of course needs more energy, and much more waste (a),
than the targeting microscopic heating (b)
Oncothermia has a simple technical setup. The modulated radiofrequency current (RF) flows through the lesion, see Figure 7.
RF-current flows through
the target
RF-generator
Water-bolus
Water-bolus
Figure 7. Oncothermia setup. The cell-culture/animal/human is a part of the electric circuit. Energy is
carried by 13.56 MHz RF-current, (fractal-modulated)

6
The RF-current which flows through the cancerous lesion automatically focused by its lower impedance, will flow mainly in the extracellular electrolyte (see Figure 8.), because the cells are electronically capsulated (isolated) by their membrane by more than one-million V/m field-strength. (The membrane is a good isolating lipid (fatty) layer). The membrane disruption is one of the targeted aims [25], [26], [27], as well as many research groups are dealing with the electric field action on the cellular divisions [28], [29], [30], [31]. The main advantage of the electric field application is the missing control of the organism, physiology control over this effect; no physiology feedback is directly limiting the electric field only its consequences could be regulated. The process made by oncothermia has its main energy delivery into the extracellular liquid, heating it up, and creating a little (1/1000 oC) difference between the inner and outer temperature of the cell. This looks only a small difference, but regarding of the very tiny membrane layer (5 nm), the small difference in standard conditions is pretty high: ~200,000 oC/m! This starts a prompt heat-flow from outside to the cell through the membrane, and permanently acts till the temperature difference exists. Despite of the quick heat-flow through this tiny membrane, the heat-current is long-lasting, till the full cellular interior is not heated up to the same temperature than outside.
Figure 8. Oncothermia delivers its energy mainly into the extracellular electrolyte, creating a
temeperature gradient through the cellular membrane Oncothermia does not require high temperature for the treatment, the energy used for distortion of the selected malignant cells is that of thermodynamic effects (heat-flows are applied instead of the general average isotherms), [32]. Oncothermia is based on the modulated electric field effect, which works in synergy of the classical temperature-based hyperthermia concept. In preclinical conditions (in vivo and in vitro) many measurements were done in animals and there are many interested users who tried up till now the temperature development by the method, which is a complex, invasive measurement approach. A well-controlled clinical temperature measurement [33] by the CT-guided fluoroptic sensor shown the temperature increase facility of oncothermia also. The patient (suffering with advanced sarcoma) was treated with the medium applicator. The result is shown on the Figure 9. The maximal temperature in the tumor was 44 ºC, while the surface temperature remained around 32 ºC.

7
Figure 9. The intratumoral temperature in advanced sarcoma
However, the main advantage of oncothermia is the non-equilibrium heating creates a heat-flow through the membrane into the cytosol, which is active till the equilibrium is reached. This gains the efficacy and the reliability of the treatment. The membrane effect by electric field was expected having a thermal limit [34]. It was questioned [35], and later it was rigorously shown, that the effect of oncothermia is not limited in this issue, [36]. To enhance the selection for membrane distortion, and enhance the collective (apoptotic) control on the cell-death [37], [38]; a special modulation is built in the oncothermia process.
The not so high radiofrequency (13.56 MHz) absorbed in all the electrolytes, but the main energy absorption is in the membrane and the extracellular electrolyte [39]. This creates an extreme SAR between the cells, which makes temperature gradient through the membrane [32]. The treated tissue will be inhomogenicly heated, heat flows from extracellular to cytosol through the membrane, accompanying with definite other thermodynamical and chemical changes [32]. These definite thermal currents will be continued till the extra- and intracellular temperature reaches equilibrium, so the intracellular electrolyte had been heated up to the equal level (see Figure 10.).
Elapsed time [arb.units]
Tem
pera
ture
[arb
.uni
ts]
Temperature difference(driving force of heat-flow)
Figure 10. The thermal gradient action due to the inhomogenous heating
Oncothermia is microscopic heating The general idea of microscopic heating is simple: the heating energy is not liberated in a sudden single step, but regulated and multiple small energy liberation makes the same job, see Figure 11. In our case the forwarded energy targets the most influential areas selectively. Instead of the high, general energy pumping into the lesion, the energy is liberated at the membranes of the malignant cells.

8
regu
latin
g m
embr
ane
Figure 11. The difference of macro- and micro-liberation of energy. The efficacy of the last one is
much better
Anyway, the microscopic effects, instead of the large energy liberation, is one of the most update thinking in energy source developments. In the modern technologies, the relatively low efficacy combusting engines are intended to replace by the fuel-cell energy-sources and electric motors, which are based on the membrane regulated microscopic reactions of gases.
The efficacy of the energy depletion intended to pump into the tumor is limited by the energy loss outside of the malignant target. The main factors of the useless energy absorptions are:
• The absorbed energy by the tissues transfers the effect to the deep-seated tumor.
• The heat-exchange by the blood-flow
• The heat exchange by the heat-conduction from the tumor to the surroundings
• These heat-sinks are modifying the overall performance of the treatment and make uncontrolled the full heating process for the malignancy. The real effect which used for the intended treatment is be less than the losses, and the efficacy is usually less than 25%, which is very low. The problem of this is not only that the large part of energy is wasted, but also the useless energy part could be dangerous by overheating the healthy tissues as well as increasing the metabolic rate and also making physiology answer on this effect which tries to break the homeostasis. The massively heated tumor volume intensifies the control of physiology, and weakens the expected effect.
The adequate corrective actions for these challenges would be the more precise targeting, decreasing the losses in the surrounding and avoid the physiological corrections to suppress the desired effect. Construction the solution some new effects have been used increasing the efficacy:
• Apply the electric field as carrier of the energy, and that field cannot be compensated by homeostatic control
• Apply a correct microscopic targeting, using the energy-absorption cell-by-cell efficiently.
• Apply such mechanisms, which initializes natural effects kill the malignant cells
• Apply mechanism, which carries info for disseminated cells to be blocked According to the calculations [40], [41], [42] a relatively small amount of energy can heat up the average-sized tumors to the appropriate temperature, if it targets the tumor accurately enough [43]. The relatively low bio-impedance of malignant lesions makes possible the automatic focusing: the applied RF-current will choose the “easiest” way to flow, automatically loading the tumor with highest current density.

9
The approach using electric impedance for quality assurance is partly comparable with the ion- concentration concept of ionizing-radiation characterization: the old unit measured the ion-pair production, 1 R (roentgen) = 2.58*10-4 C/kg. Note, interestingly, that an electric field application without an increase in temperature (using less than 5W power) has also been found effective against cancer [44], [45], [46], [47], [48], [49], by using galvanic (DC) current applications. This electric tumor treatment measures and controls the tissue-resistance and the quality parameter is the applied charge load (in Coulombs, C), [50], [51], [52], with results reported in several peer-reviewed journals [53], [54], [55], [56], [57] and conferences organized on the subject [58]. Yet few studies discuss the biological mechanisms involved in electromagnetic field induced hyperthermia [59], [6]. However, the effect of electric field remains to be a hot topic in science, [60], [61]. Oncothermia works with much less forwarded energy, by focusing energy directly on the malignant tissue using its impedance selectivity even by cellular resolution, [12]. This effect is based on the low impedance of the tumor, due to its metabolism which is higher than that of its healthy counterpart’s, [62]. This special focusing in fact makes the treatment safer and really non-toxic. (For comparison see the picture of the artificial focusing process: it covers the actually shown malignancies, but also hits the healthy tissue in between.) The higher ionic concentration in the more active cellular environments and different physiological conditions (see PET, [positron tomography]), allows even spatial resolution by this effect (EIT [electric impedance tomography] and CDI [current density image]). The real focusing could be measured by RF-current density image, [63], [64], which spectacularly shows the focusing of the current in the tumor [65]. The focusing effect in this meaning is very similar to the PET picture, which shows the enhanced metabolic activity of the tumor.
Model of oncothermia method producing higher efficacy could be demonstrated with a simple parallelism with the solutions of modern energy sources. The conventional engines in vehicles use the energy of explosion of different chemicals (e.g. petrol, diesel, kerosene). The explosion by a spark or heating over their activation energy, liberates large energy in a short time, and only a small fraction of this could be applied beneficially, most of the energy are radiated conducted or lost in various other ways. One of the largest loss is the heat-exchange by the high temperature, which somehow has to be used again (e.g. intercooler, turbo). The most modern solution however is the set of microscopic explosions, promoting the chemical reactions individually by a membrane control (i.e. fuel cell solution) and using the energy step-by-step as a sum of the micro-reactions (see Figure 12.). This model is anyway learned from the living organisms, when the energy is liberated gradually in a “ladder” of multistep processes, and also moderated by surface reactions.
a.)
2000 µm
20 µm

10
b.)
2000 µm
20 µm
Figure 12. The schematics of macroscopic and microscopic heating of tumor
In this case, the lost energy is minimal; the efficacy of the energy utilization and its control is maximal. The energy is concentrated in this case directly to the chemical reactions and does not involve the above listed losses. The energy liberated by the micro reactions are used for the desired job in full, while the explosion-like, huge energy-supply in short time cannot be optimally used, due to the intensity of the immediate offer for the available energy is too much for prompt use. This causes a large demand of waste and a low efficacy of the desired effect. The problem of the heating however shows a false, specious effect of applications in biology. When the liberated energy is not used as active biochemical or biophysical driving-force than the waste appears as a simple growth of the temperature in the target. This deceptive illusion looks as higher efficacy. This process is of course a better heating, wasting the energy and not used for the actually necessary processes, distribution the excess energy in the neighborhood and gaining the average energy of all the particles in the target. This is a typical loose of aims by illusions: the temperature makes only conditions that are implements and not the aim. The question “Tool or goal?” became relevant to study the temperature alone. By a simple example of mixing the tool and the goal in our everyday life: the graduation is a tool fro our professional life, however when somebody makes regards the certificate of studies as a goal, its application, the aim of the study looses.
Mixing the tool with the action creates false goal in hyperthermia application: increase the temperature alone. This “auto-suggestion” creates such situation that magnetic resonant imaging (MRI) is applied to control the temperature during the treatment, instead using this capable imaginary method to see what is happening in the tumor indeed.
The non-temperature dependent cell destruction is studied by ultrasound [66] and widely by electric fields [67], [68], which is a hot topic in science [36], [60], [61]. Other line of the development of energy-absorption in depth for killing the malignant cells was parallel: the electromagnetic treatments to cure cancer. The first famous name was D’Arsonval. His method had fantastic popularity at the turn of the 19th-20th centuries. Numerous devices were developed and applied widely, but the expected breakthrough result was missing. Entirely new line was started with Professors Rudolf Pekar, [69], [70], [71], Bjorn Nordenstrom [48], [49] and Xin You Ling [72], [73], [50]; and continued by others [74], [75], [76], [54], [55], [56], [57]; and the first conference was organized in 1992 in Beijing [58]. They used the galvanic electric current to treat cancer. This method had delivered remarkable results; and the biological mechanisms involved in electromagnetic field are intensively investigated [6], [59] and the effect of electric field is studied on various side of its complex behavior, [60], [61]. Some special treatments are established to direct electric treatment of the tumor (mainly with DC-current), controlling the tissue-resistance and the quality parameter is the applied charge load, [50], [51], [52].

11
Several good surprising results reported [53], [54], [55], [56], [57] and conferences organized on the subject [77], [58]. Yet few studies discuss the biological mechanisms involved in electromagnetic field induced hyperthermia [6], [59].
Based on microscopic effects, there not only the heating makes the effect, but the electric field itself has a strong synergy with this (see Figure 13. [78]), having significantly larger cell killing in malignancy at 38 oC, than the conventional hyperthermia has on 42 oC [79].
Figure 13. The cell-destruction ability of oncothermia is three-times higher than of hyperthermia at
the same 42 oC temperature. Pumping the same energy as for temperature 42 oC, but cooling the lesion by outside water-bolus (to 38 oC temperature), the efficacy of the cell-destruction remained
much higher in oncothermia than in hyperthermia at 42 oC temperature The process is selective. The RF current is choosing the “easiest” path to flow, and due to the high ionic concentration of the near-neighborhood of malignant cells, the current will be densest at the tumor cells. The experimental results well support this idea (see Figure 14.) In the case of healthy cells the load is equal for all the cells, no difference between the treated and control samples. When we gain the metabolism (immortalized cells) but not yet malignant acceleration, the effect is selectively higher but not significant. However, when the malignancy is present, the cellular growth is aggressive, the selection became effective, and kills the tumor cells without affecting the healthy ones in the coculture. This electric field effect well demonstrates, that the average kinetic energy (temperature) has not decisional effect. The main action is the targeted energy-delivery, which could be done on such low average energy as the standard healthy body temperature.

12
Untreated
Healthy human skin fibroblasts
Treated(oncothermia, 42 oC)(100.000 cell/ml, 37 oC)
Human keratinocytes[primary] (HCK)
HaCaT, controlHuman immortalized keratinocytes [non-tumorigenic], (HaCaT)
Human epidermoidcarcinoma cells [tumorigenic],(A431)
HaCaT, oncothermia
A431, control A431, oncothermia
HCK, control HCK, oncothermia
Malig
nicity
Healthy human skin fibroblasts
Healthy human skin fibroblasts
Figure 14. Co-culture with normal human skin fibroblasts as a model of a squamous carcinoma
growing within connective tissue cells (100.000/ml) were exposed to oncothermia, incubated for 24 h at 37oC, fixed and stained with crystal violet. Cellular metabolic activity was measured using the MTT assay (standard colorimetric test) and quantitated at 630 nm. Data represent the mean value ± S.E.M. of 4-6 separate experiments assayed in triplicate, but some experiments were repeated up to 12 times
to obtain reliable data. (a) Healthy tissue is unaffected. (b) Highly proliferating tissue is slightly affected, but the healthy cells are intact. (c) Malignant tissue is selectively treated, the malignance is
destroyed, the healthy cells are intact. [80] The cell killing needs energy, and afterwards the overall energy of the system would be decreased from a well ordered (bounded) state (which was in the case of the living cell) to a disordered chemical state with some broken chemical bonds. The transition from the ordered (chemically higher energy) state to the disordered (chemically lower state) arrangement the well known gap energy must be pumped. This gap-energy has different components. For hyperthermia the heat energy gives the full energy-consumption, however, in oncothermia a significant field effect takes part in the distortion mechanism [32]. This simple allows easier cell-destruction by oncothermia, (see Figure 15.); similar to the well known catalytic reactions.
Ene
rgy
[kJ/
mol
]
Reaction coordinate
Energy of damaged cell
Energy of cellular integrity
Original thermal energy to destroy(> 42.5 oC) Necessary thermal
energy to destroy
Oncothermia “catalysis”
Hyp
erth
erm
iaO
ncot
herm
ia
Ene
rgy
[kJ/
mol
]
Reaction coordinate
Ene
rgy
[kJ/
mol
]
Reaction coordinate
Energy of damaged cell
Energy of cellular integrity
Original thermal energy to destroy(> 42.5 oC) Necessary thermal
energy to destroy
Oncothermia “catalysis”
Hyp
erth
erm
iaO
ncot
herm
ia
Figure 15. Oncothermia needs less thermal energy to make the same distortion than the classical
hyperthermia does

13
The large extracellular SAR makes not only thermal, but also electric inhomogenity in the tissue; the extracellular matrix has higher current density than the other electrolytes. The current density gradient is accompanied with the gradient of the electric field, which could reorient the high-dielectric constant proteins in the extracellular liquid. The orientation of these protein molecules would be constrained perpendicular on the membrane surface. By this effect the lost adherent connections could be rebuilt in between the malignant cells, which were indeed shown experimentally, [81]. This effect helps to suppress the metastatic dissemination as well as promotes the intercellular signals to activate the natural cell-killing mechanisms.
Oncothermia promotes the programmed cell-deaths of tumor The selection and the tumor destruction of oncothermia became trivial hours later of the treatment (see Figure 16., [82])
Figure 16. Morphological observations show extended cell-destruction in the large volume of the
tumor (field effect is active, temperature doesn’t change, self-focusing). The destruction has a time-delay, hours are requested for the natural processes to be well active to fight. The numbers indicated on the mice are the hours after the single shoot 30 min oncothermia treatment, (HE Staining). (a) full
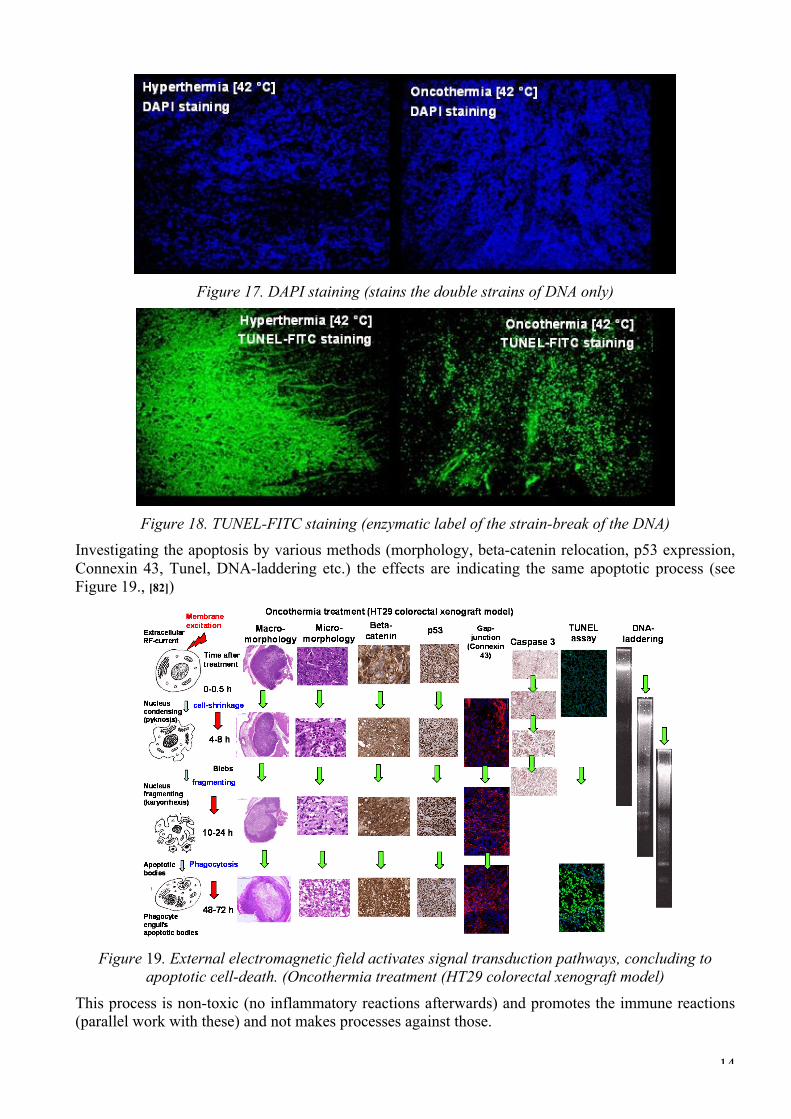
cross section of the tumor, (b) magnification of the tissue by 100x The time delay indicates the long-duration processes, which were identified as programmed cell-death (apoptosis). Detecting the double strains of DNA (DAPI staining, see Figure 17.) and measuring the enzymatic labeled strain-breaks of DNA (TUNEL-FICT, see Figure 18. ) the apoptosis is highly likely in oncothermia, while at identical temperature in classical hyperthermia the necrosis is preferred. Consequently the main effect in oncothermia is the apoptosis contrary to the conventional hyperthermia, which operates mainly by necrosis.
14
Figure 17. DAPI staining (stains the double strains of DNA only)
Figure 18. TUNEL-FITC staining (enzymatic label of the strain-break of the DNA)
Investigating the apoptosis by various methods (morphology, beta-catenin relocation, p53 expression, Connexin 43, Tunel, DNA-laddering etc.) the effects are indicating the same apoptotic process (see Figure 19., [82])
Figure 19. External electromagnetic field activates signal transduction pathways, concluding to
apoptotic cell-death. (Oncothermia treatment (HT29 colorectal xenograft model)
This process is non-toxic (no inflammatory reactions afterwards) and promotes the immune reactions (parallel work with these) and not makes processes against those.
15
Oncothermia limits the dissemination of malignant cell • Dissemination is blocked by the sticking of the cells to each other. The adherent connections
and the junctions between the malignant cells are reestablished, the cells are connected again, their autonomy is limited, the possibility of the dissemination decreases.
• The immune system (with presently not clear mechanism) acts against the metastatic lesions (abscopal, bystander effect), and the local treatment of the primary tumor decreases the distant metastases as well.
• These effects are the most important for the survival and quality of life.
The main threat of life by tumorous diseases is the distortion of the organs which are essential for the life of the organism. When the tumor grows somewhere without endanger the important systems like the respiratory system, central nervous system, cardiovascular system, etc., it has no life-threatening. These tumors are local (benign or early malignant), their elimination is possible. The real life-threatening is the malignancy, when the cells are disseminated from the tumor-lesion by the various transport systems (lymph, blood), or their effect become systemic by one of the general mechanisms of the organism. The problem of the classical hyperthermia is that sometimes it promotes the dissemination of the malignant cells [83], [84], [85].
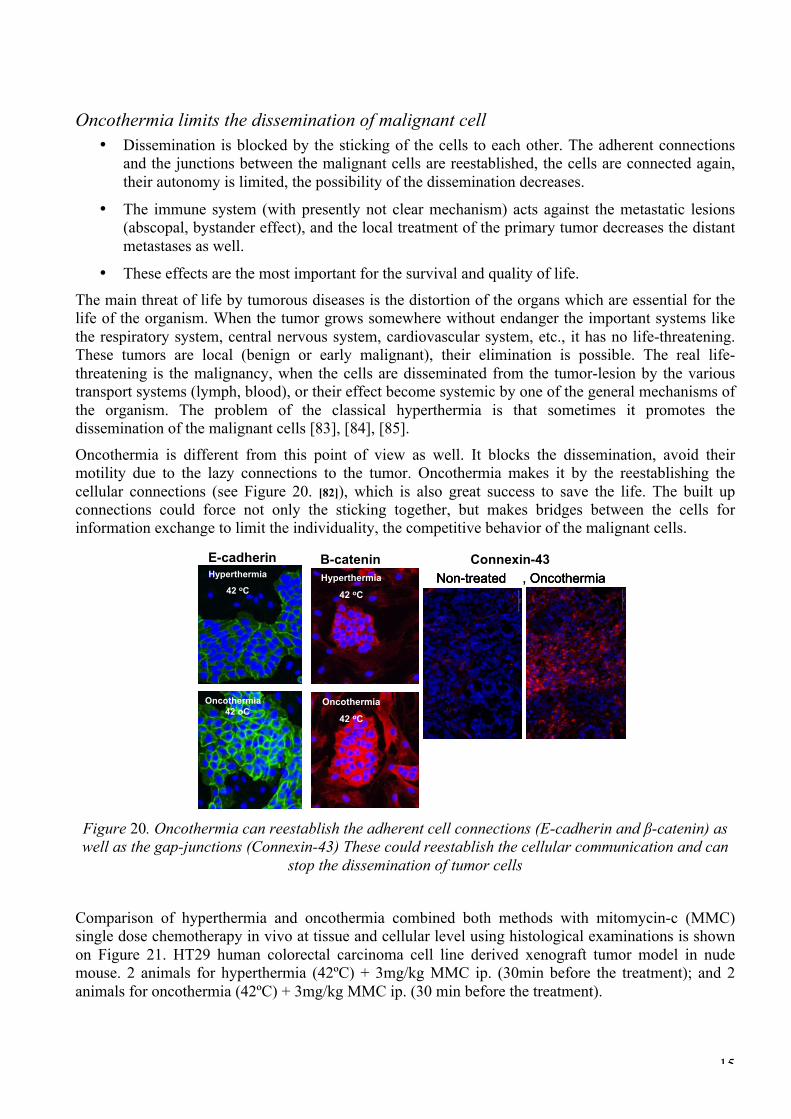
Oncothermia is different from this point of view as well. It blocks the dissemination, avoid their motility due to the lazy connections to the tumor. Oncothermia makes it by the reestablishing the cellular connections (see Figure 20. [82]), which is also great success to save the life. The built up connections could force not only the sticking together, but makes bridges between the cells for information exchange to limit the individuality, the competitive behavior of the malignant cells.
E-cadherin Β-catenin, OncothermiaNon-treated , Oncothermia, OncothermiaNon-treatedNon-treated
Connexin-43Hyperthermia
42 oC
Hyperthermia
42 oC
Oncothermia
42 oC
Oncothermia
42 oC
Hyperthermia
42 oC
Hyperthermia
42 oC
Oncothermia42 oC
Oncothermia42 oC
Figure 20. Oncothermia can reestablish the adherent cell connections (E-cadherin and β-catenin) as well as the gap-junctions (Connexin-43) These could reestablish the cellular communication and can
stop the dissemination of tumor cells
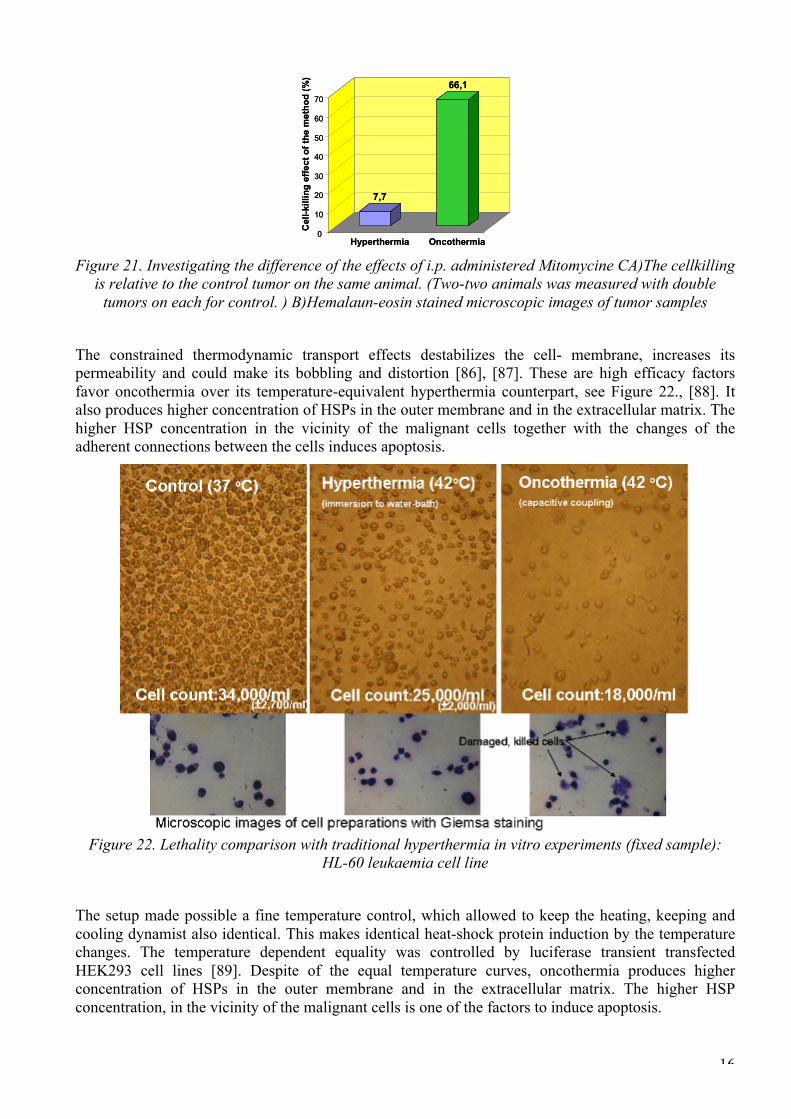
Comparison of hyperthermia and oncothermia combined both methods with mitomycin-c (MMC) single dose chemotherapy in vivo at tissue and cellular level using histological examinations is shown on Figure 21. HT29 human colorectal carcinoma cell line derived xenograft tumor model in nude mouse. 2 animals for hyperthermia (42ºC) + 3mg/kg MMC ip. (30min before the treatment); and 2 animals for oncothermia (42ºC) + 3mg/kg MMC ip. (30 min before the treatment).
16
0
10
20
30
40
50
60
70
Cel
l-kill
ing
effe
ct o
f the
met
hod
(%)
0
10
20
30
40
50
60
70
Cel
l-kill
ing
effe
ct o
f the
met
hod
(%)
7,7
Hyperthermia
7,7
Hyperthermia
66,1
Oncothermia
66,1
Oncothermia Figure 21. Investigating the difference of the effects of i.p. administered Mitomycine CA)The cellkilling
is relative to the control tumor on the same animal. (Two-two animals was measured with double tumors on each for control. ) B)Hemalaun-eosin stained microscopic images of tumor samples
The constrained thermodynamic transport effects destabilizes the cell- membrane, increases its permeability and could make its bobbling and distortion [86], [87]. These are high efficacy factors favor oncothermia over its temperature-equivalent hyperthermia counterpart, see Figure 22., [88]. It also produces higher concentration of HSPs in the outer membrane and in the extracellular matrix. The higher HSP concentration in the vicinity of the malignant cells together with the changes of the adherent connections between the cells induces apoptosis.
Figure 22. Lethality comparison with traditional hyperthermia in vitro experiments (fixed sample): HL-60 leukaemia cell line
The setup made possible a fine temperature control, which allowed to keep the heating, keeping and cooling dynamist also identical. This makes identical heat-shock protein induction by the temperature changes. The temperature dependent equality was controlled by luciferase transient transfected HEK293 cell lines [89]. Despite of the equal temperature curves, oncothermia produces higher concentration of HSPs in the outer membrane and in the extracellular matrix. The higher HSP concentration, in the vicinity of the malignant cells is one of the factors to induce apoptosis.

17
Temperature measurment
32
33
34
35
36
37
38
39
40
41
42
43
44
0 5 10 15 20 25 30 35 40 45 50
Time (min)
Tem
pera
ture
(oC
)
Oncothermia Hyperthermia
Hyperthermia Oncothermia
Figure 23. The dynamism of the heating and cooling is also well controlled for comparison of the two
heating methods
Change of adherent connections (E-cadherin and β-catenin) are also indicators of the gain of the social signals promoting the apoptosis [90], [91]. Remarkable change could be observed on beta-catenin dynamic development by time after the treatment, see Figure 24. on HepG2 human hepatocellular carcinoma cell-line. This considerable change after 24 hours of the treatment is sharply different from hyperthermia on the same temperature, and supports the other observations of the non-temperature dependent processes [92]. The sudden regrouping the beta-catenin and its enrichment at the cell-nuclei could be an indicator of apoptosis [93].
Figure 24. Development of β-catenin by time elapsed after the treatment in comparison of untreated and hyperthermia as well as oncothermia treated samples. Sampling: 1h, 3h, 24h after the treatment; (Immuno-fluorescent microscopic images, red: β-catenin, blue: cell nuclei)
Many in vitro and in vivo preclinical studies as well as twenty years entirely positive practice and huge number of retrospective clinical studies are behind of oncothermia.
Remarkable amount of retrospective clinical studies are available to indicate the oncothermia effect in humans. It is commonly used for such a complex and very frequent tumors like lung, liver, pancreas, brain, gastrointestinal, gynecological, etc. Prospective evidence based clinical trial was not performed till now with oncothermia. The reasons are:
(1) it is applied over the second line of treatments (far advancer cases). No evidence based trials exists in this treatment line for pharmaceutical products also.
(2) The evidence based studies are too expensive compared to the facilities of the company. (3) Most of the users run a private clinic, having no interest to make such studies.

18
Retrospective studies and case reports on huge number of patients show amazingly good results in all the registered localizations. The best enhancements are in the brain-gliomas (n=, %). The retrospective analyses in independent clinics show coherence in the success, and definitely and significantly higher survival time than the large databases (SEER [94], Eurocare [95]). The oncothermia challenge is its small fraction only of the overall survival. Oncothermia is applied when other treatments fall, consequently the patients with long overall survival could have not observable life-elongation, even if oncothermia was effective. The aggressive disease with short survival is a chance to indicate the efficacy. For these reasons we compare the 1st year survivals rate only (see Figure 25.). In this sense oncothermia is indicated as a feasible, effective method [96]; [97], [98], [99].
SEER Eurocare Oncothermia 1st year 2nd year
1 Brain glioma 28970 14452 140 90.63 50.382 Colo-rectal 242920 127406 218 20.5 53 Esophagus 18302 18231 12 34 67.74 Ovary 39383 22929 27 51.1 40.75 Corpus uteri 68271 22509 9 15 06 Kidney 38270 23683 39 22.2 15.37 Liver 12696 9041 25 250.9 221.78 Lung 268106 127487 258 96.7 98.19 Pancreas 47368 24988 99 230.53 336.71
10 Prostate 243451 82190 18 5.4 0.811 Soft-tissue 11256 5011 16 29.5 37.512 Stomach 42813 43082 68 47.3 14
# Localization
Patient number Oncothermia (+%)
40
7176
17 16
36
89
68
45
59
8287
72
51
65
97
85 83
68
114
92
25
99
258
103
39
24
0
20
40
60
80
100
120
0
20
40
60
80
100
120
Stomach Colon Rectum Liver Pancreas Lung andbronchus
Breast Kidney andrenal pelvis
Brain GBMStomach Colon Rectum Liver Pancreas Lung andbronchus
Breast Kidney andrenal pelvis
Brain GBM0
50
100
150
200
250
300
0
50
100
150
200
250
300Oncothermia dataOncothermia dataOncothermia patient’s numberOncothermia patient’s number
# pa
tient
s (n
)
SEERSEER
1st y
ear
surv
ival
(%)
Figure 25. Comparison of the first-year survival rates of various cancers with the large databases Improvement of the first-year survival percentages of oncothermia (advanced patients) compare to
SEER and Eurocare data weighted average On brain-gliomas, the Groenemeyer Institute (Bochum Germany) was active [100], [101], [102], [103], [104], [105], [106], together with the BioMed Clinic (Bad Bergzabern, Germany), [107], [108]. [109], [110], as well as the Empoli University had publication, [111]. Presently two German Universities (Regensburg [Prof. Bogdahn] and Heidelberg [Prof. Wick] are working on prospective clinical study on brain gliomas with hyperthermia. To see more evidences we show the retrospective data of independent clinics, having the same oncothermia protocol (see Figure 26.). The data are well correspond to each other and significantly higher than the data of the large international databases.
Brain glioma median survival [month]
11.49 11.3
23.63 23
19.8
n=140n=28970 n=35n=29n=1578
5
15
25
SEER RTOG HTT Clinic BioMed Clinic GroenemeyerClinic
Brain glioma median survival [month]
11.49 11.3
23.63 23
19.8
n=140n=28970 n=35n=29n=1578
5
15
25
SEER RTOG HTT Clinic BioMed Clinic GroenemeyerClinic
Brain glioma 1y survival [%]
45.437.8
86.2
73.8 71.7
n=140n=28970 n=35n=29n=14452
20
40
60
80
100
SEER Eurocare HTT Clinic BioMed Clinic GroenemeyerClinic
first
yea
r sur
viva
l [%
]
Figure 26. The median survival and the first year survival in comparison with different clics, having
the same oncothermia treatment protocol The metastatic liver tumor is a very complicated issue due to the effective cooling of the large blood flow and the sensitivity of the organ due to the chemo-toxicity from previous treatments. Our results are also exceptionally good for that organ. The colorectal liver metastasis was the topic of four different studies on liver [112], [113], [114], [115]. The sensitivity of the liver on the chemotherapy in

19
advanced cases (when the other chemo-treatments were unsuccessful) is well observable on the combined treatment compared to the oncothermia monotherapy, see Figure 27. [112].
Figure 27. Colorectal cancer liver metastases retrospective clinical study, (n=80)
The pancreas carcinoma is a rapid and aggressive disease, and not too many conventional hyperthermia results can be found in this location, [116]. Oncothermia results presented on ASCO, [117], and other conferences [118], [119] are significantly improving the achievements of the conventional treatments [120]. Results were repeated in six different clinics in two countries (see Figure 28), and so the gain definitely made on statistical evidences. pancreas
16.2 14.416.2 14.4
n=24988n=47368
1 y
surv
ival
[%]
10
20
30
40
50
60
1 y
surv
ival
[%]
10
20
30
40
50
60
Origin of the data
SEER Eurocare
n=73
HTTClinic
52.1n=73
HTTClinic
52.146.2
n=26
PeterfyHospital
46.2
n=26
PeterfyHospital
n=4252.4
VeramedClinic
n=4252.4
VeramedClinic
n=13
46.2
Nurnberg Clinic
n=13
46.2
Nurnberg Clinic
BioMedClinic
41
n=46
BioMedClinic
41
n=46
St.GeorgClinic
31
n=30
St.GeorgClinic
31
n=30
Figure 28. Comparison of six independent clinics treating with the same oncothermia protocol to the
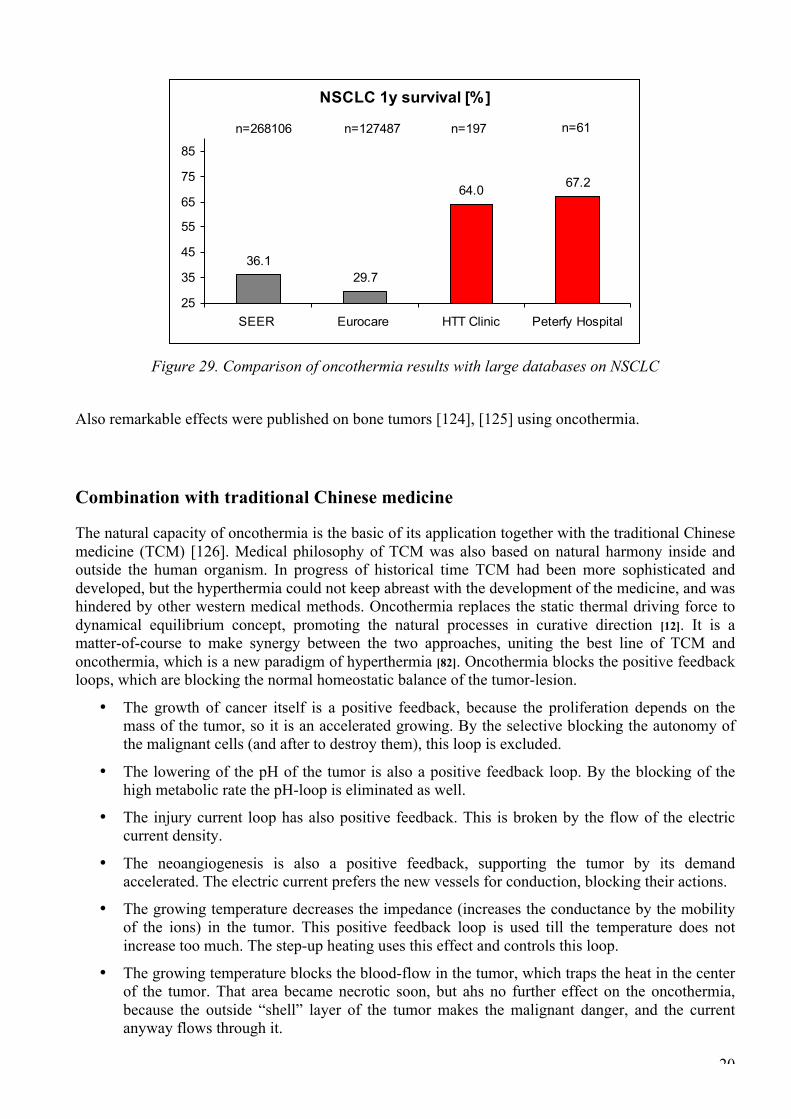
SEER and Eurocare databases The lung is also a complicated organ for hyperthermia because of the permanent cooling-ventilation of the breathing. Oncothermia, due to the non-equilibrium approach, is an excellent treatment for that as well, [121], [122], [123], see Figure 29.
20
NSCLC 1y survival [%]
36.129.7
64.0 67.2
n=268106 n=61n=197n=127487
25
35
45
55
65
75
85
SEER Eurocare HTT Clinic Peterfy Hospital
Figure 29. Comparison of oncothermia results with large databases on NSCLC
Also remarkable effects were published on bone tumors [124], [125] using oncothermia.
Combination with traditional Chinese medicine
The natural capacity of oncothermia is the basic of its application together with the traditional Chinese medicine (TCM) [126]. Medical philosophy of TCM was also based on natural harmony inside and outside the human organism. In progress of historical time TCM had been more sophisticated and developed, but the hyperthermia could not keep abreast with the development of the medicine, and was hindered by other western medical methods. Oncothermia replaces the static thermal driving force to dynamical equilibrium concept, promoting the natural processes in curative direction [12]. It is a matter-of-course to make synergy between the two approaches, uniting the best line of TCM and oncothermia, which is a new paradigm of hyperthermia [82]. Oncothermia blocks the positive feedback loops, which are blocking the normal homeostatic balance of the tumor-lesion.
• The growth of cancer itself is a positive feedback, because the proliferation depends on the mass of the tumor, so it is an accelerated growing. By the selective blocking the autonomy of the malignant cells (and after to destroy them), this loop is excluded.
• The lowering of the pH of the tumor is also a positive feedback loop. By the blocking of the high metabolic rate the pH-loop is eliminated as well.
• The injury current loop has also positive feedback. This is broken by the flow of the electric current density.
• The neoangiogenesis is also a positive feedback, supporting the tumor by its demand accelerated. The electric current prefers the new vessels for conduction, blocking their actions.
• The growing temperature decreases the impedance (increases the conductance by the mobility of the ions) in the tumor. This positive feedback loop is used till the temperature does not increase too much. The step-up heating uses this effect and controls this loop.
• The growing temperature blocks the blood-flow in the tumor, which traps the heat in the center of the tumor. That area became necrotic soon, but ahs no further effect on the oncothermia, because the outside “shell” layer of the tumor makes the malignant danger, and the current anyway flows through it.

21
Oncothermia is natural Oncothermia is a new, scientifically, medically and clinically well supported complementary method in oncology. The philosophy of oncothermia follows simple the line of Hypocrates: “Nil Nocere” (“Do not harm”) Of course this has to be understood on the way as “be natural as more as possible”. Oncothermia supports the natural processes of living organisms, applying the normal physiological and biophysical reactions of the body, using these to fight against the malignancy on standard way. The normal homeostasis works with negative feedback control, keeping the full system is harmonic complex balance (see Figure 30.).
Figure 30. The healthy homeostatic loop
When any disturbance (disease) interacts with the system, the feedback tries to compensate it and reestablish the normal homeostatic state (see Figure 31.).
Figure 31. The loop changes by disease, trying to reestablish the original state
When we make a constrained treatment, the controlling mechanism start to compensate that one too, and the physiological events will “fight” against of the healing-process also (see Figure 32.).
Figure 32. The constrained treatment enhances the physiological opposition, the control works against
the treatment as well
22
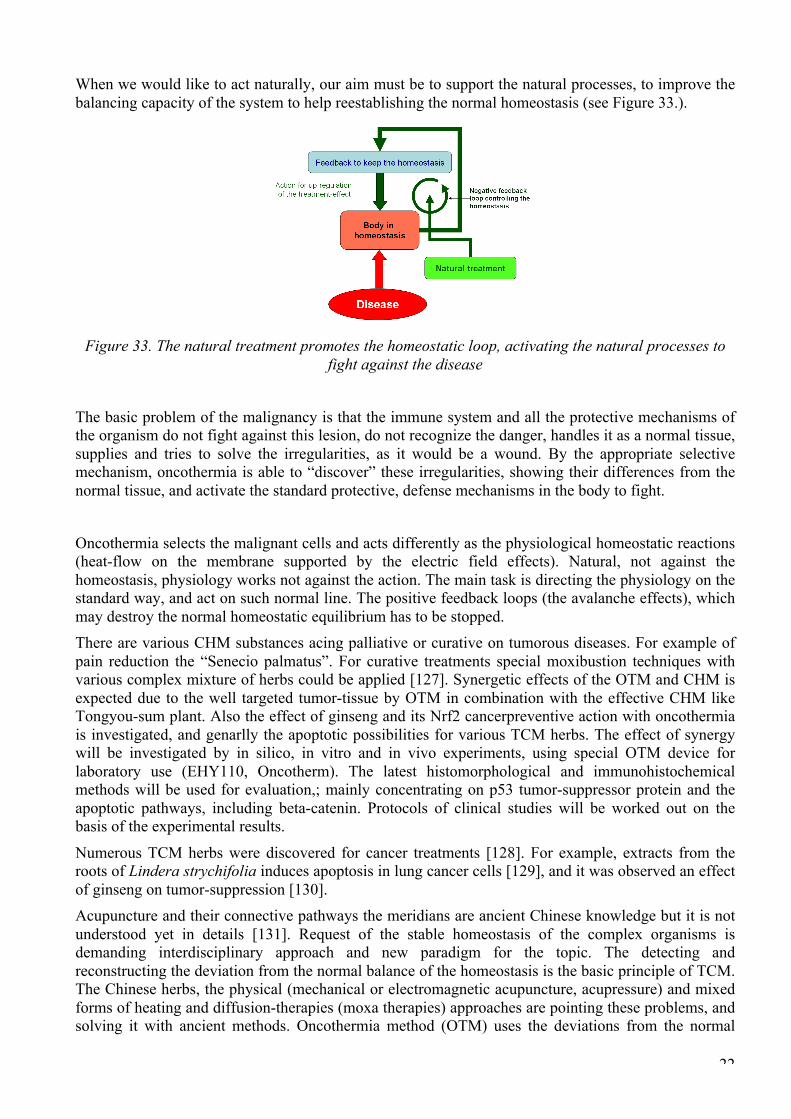
When we would like to act naturally, our aim must be to support the natural processes, to improve the balancing capacity of the system to help reestablishing the normal homeostasis (see Figure 33.).
Figure 33. The natural treatment promotes the homeostatic loop, activating the natural processes to
fight against the disease
The basic problem of the malignancy is that the immune system and all the protective mechanisms of the organism do not fight against this lesion, do not recognize the danger, handles it as a normal tissue, supplies and tries to solve the irregularities, as it would be a wound. By the appropriate selective mechanism, oncothermia is able to “discover” these irregularities, showing their differences from the normal tissue, and activate the standard protective, defense mechanisms in the body to fight.
Oncothermia selects the malignant cells and acts differently as the physiological homeostatic reactions (heat-flow on the membrane supported by the electric field effects). Natural, not against the homeostasis, physiology works not against the action. The main task is directing the physiology on the standard way, and act on such normal line. The positive feedback loops (the avalanche effects), which may destroy the normal homeostatic equilibrium has to be stopped. There are various CHM substances acing palliative or curative on tumorous diseases. For example of pain reduction the “Senecio palmatus”. For curative treatments special moxibustion techniques with various complex mixture of herbs could be applied [127]. Synergetic effects of the OTM and CHM is expected due to the well targeted tumor-tissue by OTM in combination with the effective CHM like Tongyou-sum plant. Also the effect of ginseng and its Nrf2 cancerpreventive action with oncothermia is investigated, and genarlly the apoptotic possibilities for various TCM herbs. The effect of synergy will be investigated by in silico, in vitro and in vivo experiments, using special OTM device for laboratory use (EHY110, Oncotherm). The latest histomorphological and immunohistochemical methods will be used for evaluation,; mainly concentrating on p53 tumor-suppressor protein and the apoptotic pathways, including beta-catenin. Protocols of clinical studies will be worked out on the basis of the experimental results.
Numerous TCM herbs were discovered for cancer treatments [128]. For example, extracts from the roots of Lindera strychifolia induces apoptosis in lung cancer cells [129], and it was observed an effect of ginseng on tumor-suppression [130]. Acupuncture and their connective pathways the meridians are ancient Chinese knowledge but it is not understood yet in details [131]. Request of the stable homeostasis of the complex organisms is demanding interdisciplinary approach and new paradigm for the topic. The detecting and reconstructing the deviation from the normal balance of the homeostasis is the basic principle of TCM. The Chinese herbs, the physical (mechanical or electromagnetic acupuncture, acupressure) and mixed forms of heating and diffusion-therapies (moxa therapies) approaches are pointing these problems, and solving it with ancient methods. Oncothermia method (OTM) uses the deviations from the normal

23
homeostasis for selecting the tumor cells and on this basis ignite natural processes to eliminate them from the system, reestablishing the communication harmony between the cells [12]. This technique [5] is well proven from the laboratory level to the clinical applications [82].
An extended network approach was presented in the topic [132], and we would like to continue our research on this basis. The in silico studies will have their roots from the network analysis together with the modern fluctuation theory for complex living organisms (fractal-physiology) was developed in the last decades to study this complexity: like self-organization ([133], [134], [135], [136]), fractal physiology ([137], [138], [139], [140]), and the bioscaling ([141], [142], [143]). Oncothermia widely using these new scientific results [144], [145] as well as the resonance phenomenon is studied and used in the light of a new theory [38], and special vector-potential theory [146], [147], [148] helps to complete the method. The problems of the thermal limit in the deep-seated tissues is theoretically [36] and experimentally [13] solved, so it has no any barrier for the wide investigations in synergy experiments. TCM involves electro-acupuncture and laser acupuncture, which are similar in their electromagnetic (conductive) approach to oncothermia effects. We studied the network control in acupuncture and connected it with the fractal physiology approach, used essentially in oncothermia applications. The network is recognized as scale independent and so well generalized for all the living structures.
Oncothermia promotes the natural processes and in this meaning has coherent aims with TCM philosophy and especially with the acupuncture [149]. The healthy balance (see Figure 34/a) lost by the disease (see Figure 34/b), and a curative therapy rebalances it (see Figure 34/c), which at the end will be normalized (see Figure 34/d).
Figure 34. The normal balance (a) disturbed by the disease (b), which is forced to be balanced again (c) and later reestablished the normal state (d)
The main proven effects of acupuncture are the pain-reduction and general analgesia, and reduction of the side effects of cytotoxic drugs and other side effects of the aggressive therapies. These factors

24
could be good complementary facilities of the TCM and oncothermia methods. The best, hypothetical cooperation of the methods however is on the field of immune-reactions. Numerous published data show the immune-effect of acupuncture & many evidences we have in oncothermia on the natural apoptosis and abscopal effect (immune assisted hypothesis) (see Tables below). Acupuncture - humans Immuno-action References Effect/action Macrophages [150], [151] promoter Neutrophils [152], [153], [150] promoter Neutrophils [154] no effect NK-cells [155], [156], [150] , [151] promoter Lymphocytes [150], [151] promoter Lymphocytes [157] suppressor Immunoglobulins [158], [159] suppressor Immunoglobulins [160] promoter Immunoglobulins [161], [162] no effect
Acupuncture - animals Immuno-action References Effect/action Macrophages [163] promoter Neutrophils [164] promoter NK-cells [165] promoter Lymphocytes [165] promoter Immunoglobulins [166] promoter
Electro-acupuncture - humans Immuno-action References Effect/action NK-cells [167] no effect
Electro-acupuncture - animals Immuno-action References Effect/action Macrophages [168], [169] suppressor Macrophages [170] no effect NK-cells [171], [172], [173], [174], [175] promoter Lymphocytes [176], [177] suppressor Lymphocytes [178] promoter Immunoglobulins [176] suppressor
Conclusion Recognition of the distortions in the healthy tissue have some common principles and possibilities in TCM and OTM. Potential of the synergy of high-tech OTM and TCM is extremely huge. We are ready to work out the European alternative of the “East meets West in cancer care collaboration” [179] based on the widely applied TCM evidences [180]. Asian governments hope that high-volume screening and rigorous clinical trials will unlock the secrets of ancient herbal remedies and that the results will pass muster with Western scientists [181]. The synergy of the ancient knowledge and the high-tech state-of-art of the medical knowledge could be established with this research. Further research is necessary to unite….

25
Legal note
According to European Medical Device Directive (MDD) oncothermia is certified by TUV, Munich. All the devices are manufactured according to the ISO9001 and ISO 13458. Safety and efficacy are certified also by TÜV Product Service München. The devices work over 150 places actively, and the oncothermia is twenty years on the market. No serious toxicity or side effects were reported. Minor adipose burns were happen in about 3% of all the large number of treatments. Anecdotal benefit: patients report less side effects from the conventional treatment if oncothermia is complementary applied. They report furthermore better quality of life and improved well-being.
References [1] Seegenschmiedt MH, Vernon CCA (1995) Historical Perspective on Hyperthermia in Oncology. Seegenschmiedt
MH, Fessenden P, Vernon CC (eds): Thermoradiotherapy and thermochemotherapy Vol 1, Springer/Verlag Berlin Heidelberg
[2] Szasz A, Szasz N, Szasz O: Hyperthermie in der Onkologie mit einem historischen uberblick, Deutsche Zeitschrift fur Onnkologie, 35:140-154, 2003 http://www.thieme-connect.com/ejournals/abstract/dzo/doi/10.1055/s-2003-43178;jsessionid=5AD5FBEED4E58569059A9097780E35D0.jvm5
[3] Medieval literature – 1. Medieval Turkish Surgical manuscript from Charaf ed-Din, 1465 (Paris, Bibliotheque Nationale), 2. Armamentarium chirurgicum of Johann Schultes, Amsterdam 1672 (Paris, Bibliotheque de Faculte Medicine), cited by: Seegenschmiedt MH, Vernon CC:A Historical Perspective on Hyperthermia in Oncology, In: Seegenschmiedt MH, Fessenden P, Vernon CC (eds): Thermoradiotherapy and thermochemotherapy Vol 1, Springer/Verlag Berlin Heidelberg 1995
[4] Seegenschmiedt MH, Vernon CC (1996) A historical perspective on hyperthermia in oncology, In: Seegenschmiedt MH., Fessenden P., Vernon CC. (Eds.) Thermo-radiotherapy and Thermo-chemiotherapy, Springer, Berlin Heidelberg, 1:3-46
[5] Szasz A (2006) Physical background and technical realization of hyperthermia, in: Locoregional Radiofrequency-Perfusional- and Wholebody- Hyperthermia in Cancer Treatment: New clinical aspects, (Eds: Baronzio GF, Hager ED), Springer Science Eurekah.com, Ch.3. pp. 27-59, http://www.springer.com/west/home/biomed/cancer?SGWID=4-125-22-150459762-0&detailsPage=ppmmedia%7CotherBooks&seqNo=0&CIPageCounter=CI_MORE_BOOKS_BY_AUTHOR0
[6] Szasz A, Szasz O, Szasz N (2001) Electrohyperthermia: a new paradigm in cancer therapy, Wissenschaft & Forschung, Deutsche Zeitschrift für Onkologie, 33:91-99. http://www.thieme-connect.com/ejournals/abstract/dzo/doi/10.1055/s-2001-19447
[7] Szasz A (2008) Oncothermie, OM & Ernährung, Fachinformation, Nr.123, F22-F23 [8] Szasz A (2008) Oncotherm, Traditionen und Reformen in der onkologischen Hyperthermie, Forum Hyperthermie,
Forum Medizine, 1:22-23 [9] Szasz A, Vincze Gy (2007) Dose concept of oncological hyperthermia: heat-equation considering the cell
destruction, Journal of Cancer Research and Therapeutics, 2:171-181, http://www.cancerjournal.net/article.asp?issn=0973-1482;year=2006;volume=2;issue=4;spage=171;epage=181;aulast=Szasz
[10] Oliveira RS, Bevilacqua FRG, Chammas R (1997) Hyperthermia increases the metastatic potential of murine melanoma. Braz J Med Biol Res, 30:941-945
[11] Erdmann B, Lang J, Seebass M (1998) Optimization of temperature distributions for regional hyperthermia based on a nonlinear heat transfer model. Annals of NYAS, 858:36-46
[12] Szasz A, Szasz N, Szasz O (2010) Oncothermia – Principles and Practices. Springer, http://www.amazon.co.uk/Oncothermia-Principles-Practices-Szasz/dp/9048194970
[13] Andocs G et al (2009) Strong synergy of heat and modulated electromagnetic field in tumor cell killing, Study of HT29 xenograft tumors in a nude mice model. Radiology and Oncology (Strahlentherapie und Onkologie) 185:120-126
[14] Marino AA, Iliev IG, Schwalke MA, Gonzalez E, Marler KC, Flanagan CA (1994) Association between cell membrane potential and breast cancer. Tumour Biol, 15:82-89
[15] Cure JC (1995) Ont he electrical charateristics of cacer. II> International Congress of Electrochemical Treatment of Cancer. Jupiter, Florida
[16] Revici E (1961) Research in Pathophysiology as Basis Guided Chemotherapy, with Special Application to Cancer. Princeton, NJ> D. Van Nostrand Compani
[17] Seeger PG, Wolz S (1990) Succesful Biological Contol of Cancer. Neuwieder Verlagsgesellschaft Gmbh [18] Cure JC. (1991) Cancer an electrical phenomenon. Resonant 1(1) [19] Foster KR, Schepps JL (1981) Dielectric properties of tumor and normal tissues at radio through microwave
frequencies. J. Microwave Power 16:107-119 [20] Camazine S, Deneubourg JL, Franks NR et al (2003) Self-organization in biological systems. Princeton Studies in
Complexity, Princeton Univ. Press, Princeton, Oxford
26
[21] Bak P, Tang C, Wieserfeld K (1988) Self-organized criticality. Phys. Rev. A. 38:364-373 [22] Raff MC (1992) Social controls on cell survival and death. Nature 356(6368):397-400 [23] Loewenstein WR, Kanno Y (1967) Intercellular Communications and Tissue Growth, I. Cancerous Growth. The
Journal of Cell Biology 33: 225-234 [24] Loewenstein WR (1999) The touchstone of life, Molecular information, cell communication and the foundations of
the life. Oxford University Press, Oxford, New York, pp 298-304 [25] Barnes F, Kwon Y (2005) A theoretical Study of the Effects of RF Fields in the vicinity of membranes.
Bioelectromagnetics 26: 118-124 [26] Groves JT, Boxer SG, McConnell MH (1997) Electric field-induced reorganization of two-component supported
bilayer membranes. Proc. Natl. Acad. Sci. USA 94:13390-13395 [27] Groves JT, Boxer SG, McConnell HM (1998) Electric field-induced critical demixing in lipid bilayer membranes.
Proc. Natl. Acad. Sci. USA 95:935-938 [28] de Pomerai DI et al (2002) Growth and maturation of the nematode Caenorhabditis elegans following exposure to
weak microwave fields. Enzyme and Microbial Technology 30:73-79 [29] de Pomerai DI et al (2003) Microwave radiation can alter protein conformation without bulk heating. FEBS Letters
543:93-97 [30] Zhao M, Forrester JV, McCaig CD (1999) A small, physiological electric field orients cell division. Proc. Natl.
Acad. Sci. USA 96:4942-4946 [31] Kirson ED et al (2004) Disruption of cancer cell replication by alternating electric fields. Cancer Research 64:3288-
3295 [32] Szasz A, Vincze Gy, Szasz O, Szasz N (2003) An energy analysis of extracellular hyperthermia. Magneto- and electro-biology
22:103-115 [33] Renner H (2008) Klinikum Nord, Nuernberg, (Prof.Dr.Renner’s Office). [34] Weaver JC, Astumian RD (1990) The response of living cells to very week electric fields: The thermal noise limit.
Science 247:459-462 [35] Kaune WT (2002) Thermal Noises Limit on the Sensitivity of Cellular Membranes to Power Frequency Electric and
Magnetic Fields. Bioelectromagnetics 23:622-628 [36] Vincze Gy, Szász A, Szasz N (2005) On the thermal noise limit of cellular membranes. Bioelectromagnetics, 26:28-
35, http://www3.interscience.wiley.com/journal/109857817/abstract?CRETRY=1&SRETRY=0 [37] Szasz A, Szendro P, Vincze Gy (2001) Pink-noise behaviour of biosystems. Eur.Biophysics J. 30:227-231 [38] Szendrő P, Vincze G, Szász A (2001) Bio-response to White Noise Excitation. Electro- and Magnetobiology
20:215-229 [39] Kotnik T, Miklavcic D (2000) Theoretical evaluation of the distributed power dissipation in biological cells exposed
to electric field. Bioelectromagnetics, 21:385-394 [40] Weinbaum S, Jiji LM (1985) A new simplified bioheat equation for the effect of blood-flow on local average tissue
temperature. J. Biomech. Eng. 107:131-139 [41] Pennes HH (1948) Analysis of tissue and arterial blood temperatures in the resting human forearm. J. Appl. Phys.
1:93-122 [42] Wren J, Karlsson M, Loyd D (2001) A hybrid equation for simulation of perfused tissue during thermal treatment.
Int J Hyp 17(6):483-498 [43] Szász A: Hyperthermia a Modality in the Wings, Journal of Cancer Research and Therapeutics, 3:56-66, 2007.
http://www.cancerjournal.net/article.asp?issn=0973-1482;year=2007;volume=3;issue=1;spage=56;epage=66;aulast=Szasz [44] Watson BW (1991) Reappraisal: The treatment of tumors with direct electric current. Med. Sci. Res., 19:103-105 [45] Samuelsson L, Jonsson L, Stahl E (1983) Percutaneous treatment of pulmonary tumors by electrolysis. Radiologie
23:284-287 [46] Miklavcic D, Sersa G, Kryzanowski M (1993) Tumor treatment by direct electric current, tumor temperature and
pH, electrode materials and configuration, Bioelectr. Bioeng. 30:209-211 [47] Katzberg AA (1974) The induction of cellular orientation by low-level electrical currents. Ann. New York Acad Sci.
238:445-450 [48] Nordenstrom BWE (1983) Biologically Closed Electric Circuits: Clinical experimental and theoretical evidence for
an additional circulatory system. Nordic Medical Publications, Stockholm, Sweden [49] Nordenstrom BWE (1998) Exploring BCEC-systems, (Biologically Closed Electric Circuits), Nordic Medical
Publications. Stockholm, Sweden [50] Xin Y-L (1994) Organization and Spread electrochemical therapy (ECT) in China, Eur. J. Surg. S-574:25-30, 1994,
and Xin Y-L: Advances in the treatment of malignant tumors by electrochemical therapy (ECT). Eur. J. Surg. S-574:31-36
[51] Matsushima Y, Takahashi E, Hagiwara K et al (1994) Clinical and experimental studies of anti-tumoral effects of electrochemical therapy (ECT) alone or in combination with chemotherapy. Eur. J. Surg. S-574:59-67
[52] Chou CK, Vora N, Li JR et al (1999) Development of Electrochemical treatment at he City of Hope (USA), Electricity and Magnetism in Biology and Medicine, Ed. Bersani, Kluwer Acad. Press/Plenum Publ., pp. 927-930,
[53] Xin Y-L, Xue F-Z, Ge B-S et al (1997) Electrochemical Treatment of Lung Cancer, Bioelectromagnetics, 18:8-13

27
[54] Robertson GSM, Wemys-Holden SA, Dennisson AR, Hall PM, Baxter P, Maddern GJ (1998) Experimental study of
electrolysis-induced hepatic necrosis, British J. Surgery, 85:1212-1216 [55] Jaroszeski MJ, Coppola D, Pottinger C et al (2001) Treatment of hepatocellular carcinoma in a rat model, using
electrochemotherapy. Eur. J. Cancer, 37:422-430 [56] Holandino C, Veiga VF, Rodrigues ML et al (2001) Direct current decreases cell viability but not P-glucoprotein
expression and function in human multidrug resistant leukemic cells. Bioelectromagnetics 22:470/478 [57] Susil R, Semrov D, Miklavcic D (1998) Electric field-induced transmembrane potential depends on cell density and
organization, Electro- and Magnetobiology, 17:391-399 [58] The first international conference on the topic was in Beijing, China October 20-22, 1992 (200 Chinese and 30
foreign participants, one-hundred-thirty-six papers were presented), from that time in every second year regularly held, special international organization (IABC) organized with the center in USA.
[59] Holt JAG (1988) Microwaves are not hyperthermia. The Radiographer, 35:151-162 [60] McCaig CD, Rajnicek AM, Song B, Zhao M (2005) Controlling cell behaviour electrically: current views and future
potential. Physiol. Rev. 85:943-978 [61] Szasz N (2003) Electric field regulation of chondrocyte proliferation, biosynthesis and cellular signalling. PhD
theses, MIT, Cambridge, USA [62] Scholz B, Anderson R (2000) On Electrical Impedance Scanning – Principles and Simulations. Erectromedica
68:35-44
[63] Sersa I, Beravs K, Dodd NJF et al (1997) Electric current density imaging of mice tumors. MRM 37:404-409 [64] Scott GC, Joy MLG, Armstrong RL, Henkelman RM (1995) Electromagnetic considerations for RF current density
imaging. IEEE Trans. Med. Imaging 14:515-524 [65] Mikac U, Demsar F, Beravs K, Sersa I (2001) Magnetic Resonance Imaging of alternating electric currents.
Magnetic Resonance Imaging 19:845-856 [66] Johns L.D (2002) Nonthermal effects of therapeutic ultrasound: the frequency resonance hypothesis. Journal of
Athletic Training 37(3):293-299 [67] Szent-Györgyi A (1960) Introduction to a submolecular biology. Academic Press, New York and London [68] Schwan HP (1982) Nonthermal cellular effects of electromagnetic fields: AC-field induced ponderomotoric forces.
Br. J. Cancer 45:220 [69] Pekar R, Korpan NN (2002) Krebs - Die medizinische und die biologische Tragödie. Vienna, Munich, Berne [70] Pekar R (1996) Die Perkutane Galvano-Therapie bei Tumoren- Schwachstrombehandlung von zugänglichen
Neoplasmen und ihre vitale Hybridisation in Theorie und Praxis. Verlag W. Maudrich, Vienna, Munich, Berlin [71] Pekar R (2002) Die perkutane Bio-Elektrotherapie bei Tumoren (The percutaneous bio electrical therapy for
tumors). Verlag W. Maudrich; Vienna – Munich - Berlin [72] Ling X-Y (1994) Advances in the treatment of malignant tumors by Electrochemical Therapy (ECT). Eur.J.Surgery,
Suppl. 574:S31-36 [73] Xin Y, Xue F, Ge B et al (1997) Electrochemical treatment of lung cancer. Bioelectromagnetics 18(1):8-13 [74] Quan K (1994) Analysis of the Clinical Effectiveness of 144 Cases of Soft Tissue and Superficial Maligniant
Tumors Treated with Electrochemical Therapy The European Journal of Surgery Suppl. 574:S45-49, Scandinavian University Press
[75] Song Y (1994) Electrochemical Therapy in the Treatment of Malignant Tumors on the Body Surface. The European Journal of Surgery Suppl. 574:S41-43, Scandinavian University Press
[76] Senn E (1990) Elektrotherapie. Thieme Verlag, Stuttgart [77] IABC Public Symposium and Professional Seminar, Palm Beach, FL, USA, November 6-8, 2008 [78] Andocs G, Szasz O, Renner H, Patonay L, Balogh L, Fonyad L, Jakab Cs, Szasz A (2008) Synergy of temperature-
dependent and field-dependent effects at HT29 xenograft study in nude mice. Electromagnetic Biology and Medicine, (submitted, 2008)
[79] Andocs G, Renner H, Balogh L, Fonyad L, Jakab Cs, Szasz A (2009) Strong synergy of heat and modulated electromagnetic field in tumor cell killing, Study of HT29 xenograft tumors in a nude mice model, Accepted for publication in Radiology and Oncology [Strahlentherapie und Onkologie], 185:120-126
[80] Brunner G (2006) Klinik Hornheide, Munster Univ., Germany, Hyperthermia Symposium, Cologne [81] Andocs G, Meggyeshazy N (2010) Experimental oncothermia in nude mice xenograft tumor models 1t International
Oncothermia Symposium, Cologne, November 22-23 [82] Andocs G, Szasz O, Szasz A (2009) Oncothermia treatment of cancer: from the laboratory to clinic. Electromagn.
Biol. Med. 28(2):148-165 [83] Oliveira-Filho RS, Bevilacqua RG, Chammas R, (1997) Hyperthermia increases the metastatic potential of murine
melanoma, Brazilian Journal of Medical and Biological Research, 30:941-945 [84] Shah SA, Jain RK, Finney PL (1983) Enhanced metastasis formation by combined hyperthermia and hyperglycemia
in rats bearing Walker 256 carcinosarcoma. Cancer Lett. 19(3):317-23 [85] Nathanson SD, Nelson L, Anaya P, Havstad S, Hetzel FW (1991) Development of lymph node and pulmonary
metastases after local irradiation and hyperthermia of footpad melanomas, Clinical and Experimental Metastasis 9:377-392
28
[86] Brunner G (2006) Zellulare Hyperthermie-effecte in vitro in einem progressionsmodell des plattenepithelkarzinoms.
Hyperhermia Seminar, Sept 22-23, 2006, Cologne, Germany [87] Brunner G, Erkell L (2008) Cellular and molecular effects of electrohyperthermia in a cell model of skin cancer
progression. 10th International Congress on Hyperthermic Oncology, ICHO’2008, 9-12 April, Munich [88] Andocs G (2008) Forum hyperthermia, (Forum Medizine), Front page, 1/10/2008 [89] Andocs G, Kampinga HH (2008). Private communication.Unpublished results made at Department of Radiation and
Stress Cell Biology, Faculty of Medical Sciences, University of Groningen [90] Szasz O, Andocs G, Szasz A (2008) Thermally induced effects in oncothermia treatment, Symposium on
Biophysical Aspects of Cancer, Electromagnetic mechanisms, (in memoriam H. Froelich), Prague, 1-3. July, 2008, submitted to Electrom. Bio. Med.
[91] Bremnes RM, Veve R, Hirsch FR, Franklin WA (2002) The E-cadherin cell–cell adhesion complex and lung cancer invasion, metastasis, and prognosis, Lung Cancer 36:115–124
[92] Andocs G, Szasz O, Szasz A (2008) Oncothermia treatment of cancer: from the laboratory to clinic, Symposium on Biophysical Aspects of Cancer, Electromagnetic mechanisms, (in memoriam H. Froelich), Prague, 1-3. July, 2008, submitted to Electrom. Bio. Med. (2008).
[93] Gijn van ME, Snel F, Cleutjens JPM, Smits JFM, Blankesteijn WM. (2001) Overexpression of Components of the Frizzled-Dishevelled Cascade Results in Apoptotic Cell Death, Mediated by b-Catenin. Exp. Cell Res. 265:46–53
[94] Surveillance, Epidemiology, and End Results (SEER), National Cancer Institute. www.seer.cancer.gov. April, 2000 [95] EUROCARE-3, European Cancer Database. www.eurocare.org/profiles/index.html [96] Szasz A, Dani A, et al (2005) Retrospective analysis of 1180 oncological patients treated by electro-hyperthermia in
Hungary, DEGRO 11. Jahreskongress der Deutschen Gesellschaft für Radioonkologie, 26-29 Mai 2005, Kongresszentrum, Karlsruhe
[97] Sahinbas H, Grönemeyer D (2002) Local and regional deep-hyperthermia in combination with radiation- and chemotherapy for advanced tumors, 20th European Society for hyperthermic oncology, Bergen, Norway, May 23-25
[98] Kleef R, et al (2004) Locoregional hyperthermia in advanced cancer – case reports and research perspectives, ICHS Conference, Shenzhen, China
[99] Szasz A, Dani A, Varkonyi A (2004) Az elektro-hipertermia eredményei nagyszámú beteg retrospektív kiértékelésének tükrében Magyarországon, Magyar Klinikai Onkológiai Társaság III. Kongresszusa, 2004. November 17-20, Hilton Budapest Hotel WestEnd
[100] Sahinbas H, Baier JE, Groenemeyer DHW, Boecher E, Szasz A (2006) Retrospective clinical study for advanced brain-gliomas by adjuvant oncothermia (electro-hyperthermia) treatment. www.gimt-online.de/uploads/media/Therapieergebnisse_Giloma_Studie_01.pdf
[101] Sahinbas H, Groenemeyer DHW, Boecher E, Szasz A (2006) Retrospective clinical study of adjuvant electro-hyperthermia treatment for advanced brain-gliomas. Deutche Zeitschrifts fuer Onkologie, 39:154-160 http://www.thieme-connect.com/ejournals/abstract/dzo/doi/10.1055/s-2007-986020
[102] Szasz A, Sahinbas H, Dani A (2004) Electro- hyperthermia for anaplastic astrocytoma and gliobastoma multiforme ICACT 2004, Paris, 9-12. February
[103] Sahinbas H (2004) EHT bei Kindern mit Hirntumoren und nicht-invasive Messverfahren am beispiel von Hirntumoren, Symposium Hyperthermie, Cologne, 15-16 Oktober 2004
[104] Sahinbas H, Grönemeyer D (2005) Oncothermia: An effective treatment for advanced gliomas, Deutsche Kongress im Komplementare Medizine, Schortens
[105] Sahinbas H (2004) Deep RF hyperthermia treatment of advanced gliomas, Oncology Conference, Basel [106] Sahinbas H, Grönemeyer DHW, Böcher E, Lange S (2004) Hyperthermia treatment of advanced relapsed gliomas
and astrocytoma. The 9th International Congress on hyperthermic oncology, St. Louis, Missuri, ICHO, April 24-27, 2004
[107] Hager ED, Dziambor H, App EM, Popa C, Popa O, Hertlein M (2003) The treatment of patients with high-grade malignant gliomas with RF-hyperthermia. Proc ASCO 2003; 22:118, #47, Proc Am Soc Clin Oncol 22 http://www.asco.org/portal/site/ASCO/menuitem.34d60f5624ba07fd506fe310ee37a01d/? vgnextoid=76f8201eb61a7010VgnVCM100000ed730ad1RCRD&vmview=abst_detail_view&confID=23&abstractID=102803
[108] Hager ED, Sahinbas H, Groenemeyer DH, Migeod F (2008) Prospective phase II trial for recurrent high-grade malignant gliomas with capacitive coupled low radiofrequency (LRF) deep hyperthermia. ASCO 2008, Journal of Clinical Oncology, 2008 ASCO Annual Meeting Proceedings (Post-Meeting Edition). 26:2047 http://meeting.ascopubs.org/cgi/content/abstract/26/15_suppl/2047?maxtoshow=&HITS=10&hits=10&RESULTFORMAT=&fulltext=Hager&searchid=1&FIRSTINDEX=0&volume=26&issue=15_suppl&resourcetype=HWCIT
[109] Hager ED (2004) Response and survival of patients with gliomas grade III/IV treated with RF capacitive-coupled hyperthermia, ICHO Congress, St. Louis USA
[110] Hager ED (2004) Clinical Response and Overall Survival of Patients with Recurrent Gliomas Grade III/IV Treated with RF Deep Hyperthermia – An Update, ICHS Conference, Shenzhen, China
[111] Fiorentini G, Giovanis P, Rossi S, Dentico P, Paola R, Turrisi G, Bernardeschi P (2006) A phase II clinical study on relapsed malignant gliomas treated with electro-hyperthermia. In Vivo. 20:721-724 http://www.ncbi.nlm.nih.gov/sites/entrez?cmd=Retrieve&db=PubMed&list_uids=17203754&dopt=Citation
[112] Hager ED, Dziambor H, Hohmann D, Gallenbeck D, Stephan M, Popa C et al (1999) Deep hyperthermia with radiofrequencies in patients with liver metastases from colorectal cancer. Anticancer Res. 19(4C):3403-3408
29
http://www.ncbi.nlm.nih.gov/sites/entrez?cmd=Retrieve&db=PubMed&list_uids=10629627&dopt=Citation
[113] Ferrari VD, De Ponti S, Valcamonico F et al (2007) Deep electro-hyperthermia (EHY) with or without thermo-active agents in patients with advanced hepatic cell carcinoma: phase II study. Journal of Clinical Oncology, 25:18S, 15168
[114] Fiorentini G, deGiorgi U, Turrisi G, Rossi S, Dentice P, Bernardeschi P (2006) Deep electro-hyperthermia with radiofrequencies combined with thermoactive drugs in patients with liver metastases from colorectal cancer (CRC): a Phase II clinical study, ICACT 17th, Jan30-Feb2, Paris, France
[115] Panagiotou P, Sosada M, Schering S, Kirchner H (2005) Siloah Clinic, Hannover, ESHO, Graz [116] Hager ED, Süße B, Popa C, Schrittwieser G, Heise A, Kleef R (1994) Complex therapy of the not in sano
respectable carcinoma of the pancreas – a pilot study. J Cancer Res Clin Oncol, 120(Suppl.):R47,P1.04.15 [117] Hager ED, Dziambor H, Hoehmann D (2002) Survival and quality of life patients with advanced pancreatic cancer.
Proc ASCO 2002; 21:136b, No.2357; Proc Am Soc Clin Oncol 21. http://www.asco.org/portal/site/ASCO/menuitem.34d60f5624ba07fd506fe310ee37a01d/?vgnextoid=76f8201eb61a7010VgnVCM100000ed730ad1RCRD&vmview=abst_detail_view&confID=16&index=y&abstractID=2359
[118] Dani A, Varkonyi A, Nyiro I, Osvath M (2003) Clinical experience of electro-hyperthermia for advanced pancreatic tumors. ESHO Conference, Munich, June
[119] Dani A (2004) Electro-hyperthermia for advanced pancreas tumors, Deutscher Kongress für Radioonkologie, Strahlenbiologie und Medizinische Physik , Erfurt 10-13 June 2004
[120] Dani A, Varkonyi A, Magyar T, Szasz A (2008) Clinical study for advanced pancreas cancer treated by oncothermia. Forum Hyperthermia, Forum Medizine, 2:13-19
[121] Hager ED, Krautgartner I, Popa C, Höhmann D, Dziambor H (1999) Deep Hyperthermia with short waves of patients with advanced stage lung cancer. Hyperthermia in clinical practice. XXII Meeting of the International Clinical Hyperthermia Society
[122] Dani A (2003) Clinical experience of electro-hyperthermia for advanced lung tumors. ESHO Conference, Munich, June 2003
[123] Dani A et al (2004) Treatment of non-small-cell lung cancer by electro-hyperthermia. Strahlenbiologie und Medizinische Physik Deutscher Kongress für Radioonkologie (DEGRO) Erfurt 10-13 June 2004
[124] Aydin H (2003) Radiotherapy for liver-metastases and therapy-resistant bone-metastases. Hyperthermia Seminaries, 24-25. October 2003, Cologne
[125] Bogovic J, Douwes F, Muravjov G, Istomin Jet al (2001) Posttreatment histology and microcirculation status of osteogenic sarcoma after a neoadjuvant chemo- and radiotherapy in combination with local electromagnetic hyperthermia. Onkologie, 24:55-58 http://content.karger.com/ProdukteDB/produkte.asp?Aktion=ShowPDF&ProduktNr=224106&Ausgabe=227705&ArtikelNr=50283&filename=50283.pdf
[126] Unschuld, Paul Ulrich (1985). Medicine in China: A History of Ideas. University of California Press [127] Longo F (2007) “Traditional Chinese Medicine in Oncology”, in “Proceedings of the 56th S.C.I.V.A.C. National
Congress”; Rimini, June 1/3, pp. 230 - 232 [128] Szasz A, Hegyi G, Andocs G, Szasz O (2010) Oncothermia combination with traditional Chinese medicine: network
approach. First International Oncothermia Symposium, 22-23 November, Cologne, Germany [129] Yun-Mo Li et al (2003) Extracts from the Roots of Lindera strychifolia Induces Apoptosis in Lung Cancer Cells and
Prolongs Survival of Tumor-bearing Mice. The American Journal of Chinese Medicine, 31(6):857–869 [130] Saw CL-L, Qing Wu, Ah-Ng Tony Kong (2010) Anti-cancer and potential chemopreventive actions of ginseng by
activating Nrf2 anti-oxidative stress/anti-inflammatory pathways. Chinese Medicine 5:37 [131] Ernst E, Pittler MH, Wider B, Boddy K (2007) "Acupuncture: its evidence-base is changing". Am J Chin Med.
35(1):21-25 [132] Szasz A (2008) Electromagnetic considerations of meridian network (A network approach). International Council of
Medical Acupuncture and Related Techniques, (ICMART), XIII World Congress, Oct.10-12, Budapest [133] Haken H (1987) Self-Organization and Information. Phys. Script. 35(3):247-254 [134] Sornette D (2000) Chaos, Fractals, Self-Organization and Disorder: Concepts and Tools. Springer Verlag, Berlin-
Los Angeles [135] Walleczek J (ed) (2000) Self-organized biological dynamics & nonlinear control. Cambridge Univ. Press,
Cambridge [136] Mar’Yan MI, Szasz A (2000) Self-organizing processes in non-crystalline materials: from lifeless to living objects.
Oncotherm GmbH, Neubeuern, Germany [137] Deering W, West BJ (1992) Fractal physiology. IEEE Engineering in Medicine and Biology 11(2):40-46 [138] West BJ (1990) Fractal Physiology and Chaos in Medicine. World Scientific, Singapore, London [139] Bassingthwaighte JB, Leibovitch LS, West BJ (1994) Fractal Physiology. Oxford Univ. Press, New York, Oxford [140] Musha T, Sawada Y (eds.) (1994) Physics of the living state. IOS Press, Amsterdam [141] Brown JH, West GB (eds) (2000) Scaling in Biology. Oxford University Press, Oxford [142] Brown JH, West GB, Enquis BJ (2005) Yes, West, Brown and Enquist’s model of allometric scaling is both
mathematically correct and biologically relevant. Functional Ecology 19(4):735 –738 [143] West GB, Brown JH (2005) The origin of allometric scaling laws in biology from genomes to ecosystems: towards a
quantitative unifying theory of biological structure and organization. Journal of Experimental Biology 208:1575-
30
1592
[144] Szendrő P, Vincze G, Szász A (2001) Pink-noise behaviour of biosystems. Eur.Biophysics J. 30:227-231 [145] Vincze G, Szasz A, Liboff A (2008) New theoretical treatment of inon resonance phenomena. Bioelectromagnetics,
29:380-386 [146] Szász A, Vincze Gy, Andocs G, Szasz O (2009) Do Field-Free Electromagnetic Potentials Play a Role in Biology?
Electromagnetic Biology and Medicine, 28:135-147 [147] Szász A, Vincze Gy, Andocs G, Szasz O (2009) Effect of Curl-Free Potentials on Water. Electromagnetic Biology
and Medicine, 28:166-181 [148] Hegyi G, Vincze G, Szasz A (2007) Axial-vector interaction with bio-systems. Electromagnetic Biology and
Medicine, 26:107-118 [149] Hegyi G, Ji’an L, Bingsheng H, Andocs G, Szasz O, Szasz A (2010) Oncothermia combination with traditional
Chinese medicine: proposal on Chinese herbal medicine approach. First International Oncothermia Symposium, 22-23 November, Cologne, Germany
[150] Yamaguchi N, Takahashi T, Sakuma M, Sugita T, Ichikawa K,, Sakaihara S, Kanda T et al (2007) Acupuncture regulates leukocyte, and lymphocyte subpopulations in human peripheral blood: a, quantitative and qualitative discussion. Evid Based Complement, Alternat Med 4:447–453
[151] Petti F, Bangrazi A, Liguori A, Reale G, Ippoliti F (1998) Effects of acupuncture, on immune response related to opioid-like peptides. J Tradit Chin Med 18:55–63
[152] Karst M, Scheinichen D, Rueckert T, Wagner T, Wiese B,, Piepenbrock S, Fink M (2003) Effect of acupuncture on the neutrophil, respiratory burst: a placebo-controlled single-blinded study. Complement Ther Med 11:4–10
[153] Lu W, Matulonis UA, Doherty-Gilman A, Lee H, Dean-Clower E, Rosulek A, Gibson C et al (2009) Acupuncture for chemotherapyinduced, neutropenia in patients with gynecologic malignancies:, a pilot randomized, sham-controlled clinical trial. J Altern, Complement Med 15:745–753
[154] Karst M, Scheinichen D, Rueckert T, Wagner T, Wiese B, Fink M (2002) Acupuncture has no immediate treatment effect on the neutrophil, respiratory burst: a randomized single-blinded twoperiod, crossover study. Brain Behav Immun 16:813–6
[155] Wu B, Zhou RX, Zhou MS (1994) Effect of acupuncture on interleukin-, 2 level and NK cell immunoactivity of peripheral blood of malignant, tumor patients. Zhongguo Zhong Xi Yi Jie He Za Zhi 14:537–539
[156] Liu X, Sun L, Xiao J, Yin S, Liu C, Li Q, Li H et al (1993) Effect of acupuncture, and point-injection treatment on immunologic function, in rheumatoid arthritis. J Tradit Chin Med 13:174–178
[157] Petti FB, Liguori A, Ippoliti F (2002) Study on cytokines IL-2, IL-6, IL-10, in patients of chronic allergic rhinitis treated with acupuncture. J Tradit Chin Med 22:104–111
[158] Yu P, Bai H, Chen L, Zhang W, Xia Y, Wu G (2003) Clinical study on therapeutic, effect of acupuncture on Behcet’s disease. J Tradit Chin, Med 23:271–273
[159] Wozniak PR, Stachowiak GP, Pieta-Dolinska AK, Oszukowski PJ (2003) Anti-phlogistic and immunocompetent effects of acupuncture, treatment in women suffering from chronic pelvic inflammatory, diseases. Am J Chin Med 31:315–320
[160] Akimoto T, Nakahori C, Aizawa K, Kimura F, Fukubayashi T, Kono, I (2003) Acupuncture and responses of immunologic and endocrine, markers during competition. Med Sci Sports Exerc 35:1296–302
[161] Kho HG, Van Egmond J, Eijk RJ, Kapteyns WM (1991) Lack of influence, of acupuncture and transcutaneous stimulation on the immunoglobulin, levels and leucocyte counts following upperabdominal, surgery. Eur J Anaesthesiol 8:39-45
[162] Zhang BR, Li S, Yuan PY, Zhang XB, Cheng LX, Zhou HH, Zhou CY et al (2006) Effects of injection of Huangqi injectio into Zusanli (ST 36), on immune function in the patient of schizophrenia. Zhongguo, Zhen Jiu 26:625-628
[163] Zhao R, Ma C, Tan L, Zhao X, Zhuang D (1994) The effect of acupuncture, on the function of macrophages in rats of immunodepression. Zhen Ci Yan Jiu 19:66–68
[164] Scognamillo-Szabo MV, Bechara GH, Ferreira SH, Cunha FQ (2004) Effect of various acupuncture treatment protocols upon sepsis, in Wistar rats. Ann N Y Acad Sci 1026:251-256
[165] Okumura M, Toriizuka K, Iijima K, Haruyama K, Ishino S, Cyong JC (1999) Effects of acupuncture on peripheral T lymphocyte subpopulation, and amounts of cerebral catecholamines in mice. Acupunct, Electrother Res 24:127-139
[166] Sato T, Yu Y, Guo SY, Kasahara T, Hisamitsu T (1996) Acupuncture stimulation, enhances splenic natural killer cell cytotoxicity in rats. Jpn J Physiol 46:131–136
[167] Ye F, Liu D, Wang S, Xu L (2007) Effects of electro-acupuncture on T cell, subpopulations, NK activity, humoral immunity and leukocyte, count in patients undergoing chemotherapy. J Tradit Chin Med 27:19–21
[168] Aoki E, Kasahara T, Hagiwara H, Sunaga M, Hisamitsu N, Hisamitsu T (2005) Electroacupuncture and moxibustion influence, the lipopolysaccharide-induced TNF-alpha production by macrophages. In Vivo 19:495-500
[169] Fang JQ, Aoki E, Yu Y, Sohma T, Kasahara T, Hisamitsu T (1999) Inhibitory, effect of electroacupuncture on murine collagen arthritis and, its possible mechanisms. In Vivo 13:311–318
[170] Kavoussi B, Ross BE (2007) The neuroimmune basis of anti-inflammatory, acupuncture. Integr Cancer Ther 6:251-257
[171] Yu Y, Kasahara T, Sato T, Asano K, Yu G, Fang J, Guo S et al (1998) Role, of endogenous interferon-gamma on

31
the enhancement of, splenic NK cell activity by electroacupuncture stimulation in, mice. J Neuroimmunol 90:176-186
[172] Yu Y, Kasahara T, Sato T, Guo SY, Liu Y, Asano K, Hisamitsu T (1997) Enhancement of splenic interferon-gamma, interleukin-2, and, NK cytotoxicity by S36 acupoint acupuncture in F344 rats. Jpn J Physiol 47:173178
[173] Hahm ET, Lee JJ, Lee WK, Bae HS, Min BI, Cho YW (2004) Electroacupuncture, enhancement of natural killer cell activity suppressed by, anterior hypothalamic lesions in rats. Neuroimmunomodulation 11:268-272
[174] Choi GS, Oha SD, Han JB, Bae HS, Cho YW, Yun YS, Lee WK et al (2002) Modulation of natural killer cell activity affected by electroacupuncture, through lateral hypothalamic area in rats. Neurosci Lett 329:1–4
[175] Kim CK, Choi GS, Oh SD, Han JB, Kim SK, Ahn HJ, Bae H et al (2005) Electroacupuncture up-regulates natural killer cell activity: identification, of genes altering their expressions in electroacupuncture, induced up-regulation of natural killer cell activity. J Neuroimmuno 168:144–153
[176] Park MB, Ko E, Ahn C, Choi H, Rho S, Shin MK, Hong MC et al (2004) Suppression of IgE production and modulation of Th1/Th2, cell response by electroacupuncture in DNP-KLH immunized mice. J Neuroimmunol 151:40–44
[177] Zhang Y, Wu GC, He QZ, Cao XD (2000) Effect of morphine and electroacupuncture, (EA) on apoptosis of thymocytes. Acupunct, Electrother Res 25:17-26
[178] Cheng XD, Wu GC, He QZ, Cao XD (1998) Effect of electroacupuncture, on the activities of tyrosine protein kinase in subcellular fractions, of activated T lymphocytes from the traumatized rats. Acupunct Electrother Res 23:161-170
[179] McMaster university Explores Evidence-based Chinese medicine, http://www.integrativeonc.org/mcmaster-university-explores-evidence-based-chinese-medicine
[180] Jin-Ling Tang, Bao-Yan Liu, Kan-Wen Ma (2008) Traditional Chinese Medicine, The Lancet, 373:1938-1940 [181] Normile D (2003) The New Face of Traditional Chinese Medicine. Science, 299, www.sciencemag.org