pac,,l itation page a d-a 240 839ion o thik pac,,l itation page ia. ... regional heat flux increases...
TRANSCRIPT
UNLLbb I rIUSEUIYCLASSIFICAT'ION O THIK PAC,,l
ITATION PAGE
ia. REPORT SECURITY CLAS A D-A 240 839 RESTRICTIVE MARKINGS
l INCl ll IImiIIII2a. SECURITY CLASSIFICATI( )ISTRIBUTION/AVAJLABIUTY OF REPORT
1111111111111111111111111111111111111 11111 iiApproved for public release;
2b. OECLASSIFICATIONIDOWNGRADING SCHEDULE distribution is unlimited
4. PERFORMING ORGANIZATION REPORT NUMBER(S) S. MONITORING ORGANIZATION REPORT NUMBER(S)
NMRI 91-59.
6a. NAME OF PERFORMING ORGANIZATION 6b. OFFICE SYMBOL 7a. NAME OF MONITORING ORGANIZATION
Naval hedical Research (If applicable) Naval Medical CommandInstitute
6C. ADDRESS (Gty, State, and ZIP Code) 7b. ADDRESS (O-y, State, and ZIP Code)b90l Wisconsin Avenue Department of the Navy
Bethesda, MD 20889-5055 Washington, DC 20372-5120
8a. NAME OF FUNDING/SPONSORING I 8b. OFFICE SYMBOL 9. PROCUREMENT INSTRUMENT IDENTIFICATION NUMBER
ORGANIZATION Nava I Med i ca l (If appika ble)
Research & Development Commanj
8c. ADDRESS (Cty,State, and ZIP Code) 10. SOURCE OF FUNDING NUMBERS
8901 Wisconsin Avenue PROGRAM PROJECT ITASK WORK UNIT
Bethesda, MD 20889-5044 ELEMENT NO. NO. . NO. ACCESSION NO.
63713 M0099.01A 1003 DN377011
11. TITLE (Include Security Casication)
Physiology of exercise in the cold
12. PERSONAL AUTHOR(S) /
Doubt TJ
13a. TYPE OF REPORT 13b. TIME COVERED 114. DATE OF REPORT (YeareMonth¢Day) uS. PAGE COUNT
Jourl~al article' FROM TO lggl 15
16. SUPPLEMENTARY NOTATION
Reprinted from: Spor.ts Medicine 1991 Vol.11 No. 6 pp. 367-381
17. COSATI CODES 18. SUBJECT TERMS (Continue on reverse if necessary and identify by block number)
FIELD GROUP I SUB-GROUP Exercise physiology; Cold stress; Human; Review; Sports medicine
19. ABSTRACT (Continue on reverse if necessary and identify by block number)
OTICS EL ThEESEP26 1991
DU
20. DISTRIBUTIONAVAJLABIUTY OF ABSTRACT 21. ABSTRACT SECURITY CLASSIFICATION
UUNCASSIFIFIDAJNUMITED 0 SAME AS RPT. C DTIC USERS Unclassified22a. NAME OF RESPONSIBLE-INDIVIDUAL 22b.TELEPHONE (Include Area Code) 22c. OFFICE SYMBOL
Phyllis -.Blum.,-. "ibiarian. (5-O'). 295-2188 kIRL/NNP
D D FORM 1473, 84 MAR S3 APR eduon maybe used until exhausted. SECURITY CLASSIFICATION OF THIS PAGEAll other editions.are obsolete. UNCLASS I F I ED
Sports Medicine 11 (6). 367-381, 19910112-1642/91/0006-0367© Adis International Limited. t I rights reserved.SPO0 25
Physiology of Exercise in the ColdThomas J. DoubtHyperbaric Environmental Adaptation Program, Naval Medical Research Institute, Bethesda, Maryland, USA
Contents: Summary Accesion For
1 6 1. Metabolic Changes NTIS CRA&I,:369 , 1.1 Diet r iC 1Ar3 , 1.2 Lipid Metabolism
1.3 Carbohydrate Metabolism i.' - U;a ou: cW rj
3 1.4 Lactate Metabolism JusWfca o-#j37T,2hth i 2. Cardiopulmonary Changes ---
3?) 7 2.1 Ventilation I -
~ . 372 ~ 2.2 Oxygen Consumption . ..........3<37: .~ 2.3 Ventilatory Equivalent _ Dit ib,:tic /:374t'f " 2.4 Heart Rate _ -" 34 2.5 Cardiac Arrhythmias - AVubLY' .
VIP5~ 2.6 Cardiac Output ___Aw~Av,4 ,
, 75,'43 2.7 Peripheral Blood Flow __,,
.176', 3. Thermal Aspects Dist3.1 Respiratory Heat Loss3.2 Peripheral Thermoregulation
'376" 3.3 Skeletal Muscle Temperature3.4 Core Temperature Homeostasis
, . 4. Conclusion
Summary Recreational and job requirements have increased the incidence in which humans exercise incold environments. Understanding the physiological responses while exposed to cold entailsknowledge of how exercise and cold interact on metabolic, cardiopulmonary, muscle and thermalaspects of human performance. Where possible, distinctions ate made between responses in coldair and cold water.
While there is no consensus for diets most appropriate for working cold exposures, the evi-dence is strong that adequate amounts of carbohydrate are necessary. Carbohydrate loading ap-pears to be efficacious, as it is for other athletic endeavours.
Contrary to conventional wisdom, the combination of exercise and cold exposure does notact synergistically to enhance metabolism of fats. Free fatty acid (FFA) levels are not higher, andmay be lower, with exercise in cold air or water when compared to corresponding warmer con-ditions. Glycerol, a good indicator of lipid mobilisation, is likewise reduced in the cold, suggestingimpaired mobilisation from adipose tissue.
Catecholamines, which promote lipolysis, are higher during exercise in cold air and water,
91 !
368 Sports Medicine 11 (6) 1991
indicating that the reduced lipid metabolism is not due to a lack of adequate hormonal stimu-lation. It is proposed that cold-induced vasoconstriction of peripheral adipose tissue may account,in part, for the decrease in lipid mobilisation. The respiratory exchange ratio (RER) is oftensimilar for exercise conducted in warm and cold climates, suggesting FFA utilisation is equivalentbetween warm and cold exposures. The fractional portion of oxygen consumption ('O2) usedfor FFA combustion may decrease slightly during exercise in the cold. This decrease may berelated to a relative decrease in oxygen delivery (i.e. muscle blood flow) or to impaired lipidmobilisation.
Venous glucose is not substantially altered during exercise in the cold, but lactate levels aregenerally higher than with work in milder conditions. The time lag between production of lactatewithin the muscle and its release into the venous circulation may be increased by cold exposure.
Minute ventilation is substantially increased upon initial exposure to cold, and a relativehyperventilation may persist throughout exercise. With prolonged exercise, though, ventilationmay return to values comparable to exercise ;n warmer conditions. Exercise i'O2 is generallyhigher in the cold, but the difference between warm and cold environments becomes less asworkload increases. Increases in oxygen uptake may be due to persistence of shivering duringexercise, to an increase in muscle tonus in the absence of overshivering, or to nonshivering ther-mogenesis.
Heart rate is often, but not always, lower during exercise in the cold. The linear relationshipbetween heart rate and oxygen consumption is displaced such that at a given rate oxygen uptakeis higher. Cardiac arrhythmias are more frequent in the cold. Stroke volume tends to be higherthan under warmer control conditions, but may decline sooner or at a rate equivalent to m armcontrols at heavy workloads. Cardiac output is similar to the same work done in temperatureenvironments.
Cold-induced vasoconstriction occurs both in cutaneous and resting skeletal muscle beds, butinactive muscle provides most of the passive body insulation. With exercise insulation providedby muscle decreases as blood flow increases. Relative to warmer conditions, muscle blood flowat a given workload may be reduced if deep muscle temperature is below normal (i.e. 39"C op-timum).
Respiratory heat loss is often assumed to represent 8% of the total metabolic heat production.However, during exercise this value will increase as minute ventilation increases. Loss of sig-nificant amounts of heat from the distal extremities can limit performance, even though the areais not directly involved with exercise.
Cooled muscle has a decreased capacity to generate force expressed on cross-sectional area.As a consequence, it may be necessary to recruit more fast twitch motor units. Glycolysis ishigher in cooled muscle, which may account for higher lactate levels and greater rates of muscleglycogen depletion. Brief intense exercise will not raise cooled muscle temperature to normallimits, but mild exercise can maintain normal temperatures if exercise begins before the musclesbecome cooled.
Regional heat flux increases with exercise in the cold in direct proportion to the workload.Differing rates of heat loss can occur between active and inactive limbs, and individual rates arenot constant throughout steady-state exercise. Peak rates of heat flux for inactive limbs occurduring exercise, but peak flux for active limbs occurs in the postexercise period. At equal meta-bolic rates, more heat is lost with arm than with leg exercise.
Most of the heat generated by exercising muscle is transferred convectively to the core viathe venous circulation. The amount of heat lost conductively to the environment through tissuedepends upon factors such as subcutaneous fat. Thus, individuals with higher levels of fat (e.g.ski nfold thickness) generally are better able to maintain their core temperature in cold environ-ments.
Steady-state exercise V 0 2 values of approximately 2.0 L/min have been shown to preventfalls in core temperature in water as low as 15"C. Warmer temperatures are required in order tomaintain core homeostasis during intermittent exercise,
Predicting an individual's response to exercise in the cold is quite difficult because of theinterplay of many factors. Using existing data, responses to some forms of exercise and environ-mental stress can be estimated with reasonable accuracy. However, the number of these type
I

Exercise in the Cold 369
responses is small compared to the total number of possible permutations, showing that muchis yet to be learned.
Interest in exercise in cold environments is no tive effects on tolerance and endurance (see Askewlonger limited to wintertime sporting events. There 1989). It is difficult to define a single effect of diet-is increasing participation in sports like scuba div- ary manipulation since increasing one nutrienting, long distance swimming, triathlons, running must, as a consequence, reduce another, unless totaland cycling that occur on a year-round basis. In caloric intake is also changed. Thus, an observedaddition, there are greater numbers of men and effect may be due to the higher intake of one nu-women working in environmental extremes where trient, a corresponding reduction in another orcold temperatures may limit performance. As a simply an alteration in caloric intake.consequence, there is more than an occasional con- simplne c alorc tae.cern about the interaction between cold stress and For prolonged cold exposure, there does not ap-human performance. Understanding the physio- pear to be an increase in the resting energy re-logical limits of endurance in the cold presents a quirement, provided adequate thermal protectionchallenge to exercise scientists that will likely con- is available (Askew 1989). However, the energy cost
tinue into the next century. of performing work will increase as a consequenceThis review presents an update on human ex- of the added resistance imposed by the thermal
ercise in the cold, using selected physiological top- protective gear. For example, there is about a 10%ics that relate to performance. The intent is to pro- increase in the oxygen cost of walking while wear-vide both the expert and nonexper with a sufficient ing Arctic clothing (Nunneley 1989).overview to permit visualisation of the human re- The amount of dietary carbohydrate intake maysponse to cold stress. It is evident that there is no not be essential at rest, but has added importancesingle response that covers every type of exposure, during exercise. Young et al. (1989) found similarexercise protocol, or individual; although a generic rates of decline in rectal temperature at rest in 18°Cexample is offeree-i the conclusion to further aid water after either a 3-day high carbohydrate dietthe nonexpert. It is hoped that readers will also (65% of calorie) or a high fat diet (65% of calories).note those areas where additional research is needed The high fat diet was coupled with exercise to pro-to fill gaps in our present understanding.to fll apsin or peset unersandng.duce low muscle glycogen levels, but the net change
Cold exposure is defined herein as any environ- dc low e cogen ls bt the higemental condition where the potential exists to lose in glycogen content was comparable to the higha significant amount of heat from any region of the carbohydrate diet.body. This distinction is necessary since certain as- High carbohydrate diets, used to increase muscle
pects of exercise performance may be influenced glycogen, are well known to increase exercise en-by heat loss from one or more areas of the body. durance conducted in milder environments (e.g.
Sherman et al. 1981). A similar benefit of a high
1. Metabolic Changes carbohydrate diet may also occur during cold ex-
1.1 Diet posure. Using intermittent exercise at 80% '4 O2maxfor 4 hours in 25°C water, significantly more work
At present, there is no consensus as to what the was achieved after a 3-day high carbohydrate diet
most appropriate diet should be for cold exposure. (600 g/day) than after a 3-day normal diet (300 g/Both high carbohydrate and high fat diets have been day) [Thorp et al. 1990]. It would thus appear thatreported to increase tolerance to cold and physical carbohydrate intake is an important prede' ,rmi-endurance, but high protein diets may have nega- nant of exercise performance in the cold.

370 Sports Medicine 11 (6) 1991
1.2 Lipid Metabolism ferences in steady-state RER between warm andcold conditions, indicating co.d stress does not in-
Either cold exposure or exercise alone will in- crease FFA use (Doubt & Hsieh 1991; Jacobs et al.crease lipid mobilisation and venous free fatty acid 1985; Moore et al. 1970; Sink et al. 1989; Ther-(FFA) concentration. The combination of cold plus minarias et al. 1989). Others have noted RER toexercise does not, however, act synergistically on be lower by 0.02 to 0.03 in cold air, suggestinglipid metabolism. Leg exercise at 50 to 60% 102max greater FFA oxidation (Dolny & Lemon 1988;in 0°C air resulted in smaller increases in venous Timmons et al. 1985).triglyceride than for the same exercise in 22°C air Such disparate findings in RER are not easy to(Sink et al. 1989). Exercise at 65% N4 O2max in 18°C reconcile. Reported changes in RER are small, andwater also produced a smaller increase in FFA than minor differences in technical approach or subjectthe same exercise in 28°C water (Doubt & Hsieh variability may complicate interpretation of data.1991). Small changes in RER can relate to larger estimates
Increases in circulating catecholamines stimu- in fractional substrate utilisation. For example, anlate lipolysis from adipose tissue and enhance the RER of 1.00 and 0.71 will occur for oxidation ofintravascular breakdown of triglycerides, with ad- 100% carbohydrate and fat, respectively (Mc-renaline (epinephrine) being more potent than nor- Gilvery 1970). The fractional utilisation of fat, Ffat,adrenaline (norepinephrine). Both adrenaline and can be estimated by:noradrenaline are higher with exercise in cold water(Doubt & Hsieh 1991) or air (Dolny & Lemon 1988; Ffat = 1.00 - [(RER - 0.71)/0.29] (Eq. 1)Therminarias et al. 1989) than in warmer trials,suggesting that any relative decrease in FFA in the The term in parentheses represents the frac-cold cannot be ascribed to a reduction in the hor- tional utilisation of carbohydrate. Analysis ofmonal stimulus. Glycerol, which is a better indi- equation 1 reveals that Ffat will change by 3.4% forcator of lipid mobilisation than FFA, is also re- eh 0.01 cn in RER. roduced during exercise in cold water (Doubt & Hsieh in ither i r40 of o 1 mI/m chlle1991) and air (Sink et al. 1989). Thus, the simul- sult in a change in RER of 0.01, or a 3.4% changetaneous reductions in FFA and glycerol may be due, in Fat. Thus, while RER may be a useful meansin part, to a perfusion limitation of peripheral adi- to estimate nonprotein fractional substrate utilis-pose tissue. It is known, for example, that cold ex- ation it clearly must be used with caution when
posure directly induces vasoconstriction in adipose calculating total energy expenditures during exer-
tissue and potentiates adrenergic vasoconstriction cise.(Hjemdahl & Sollevi 1978), thereby reducing blood Protein degradation during exercise further
flow. This cold effect would be less pronounced in complicates estimates of fat (or carbohydrate) util-fat depots within the core since local temperature isation since RER is about 0.82 for protein oxi-would be higher. dation. Urea nitrogen excretion, measured over 3
The respiratory exchange ratio (RER = CO2/ days including 90 minutes of cycle exercise, was
402) is often used to estimate nonprotein sub- higher when exercise was conducted in 5C air thanstrate utilisation. Use of RER is confined to steady- in 30°C air (Dolny & Lemon 1988), indicatingstate conditions. Initial exposure to cold or the start greater protein degradation occurred in the cold.of exercise will transiently increase and decrease This finding does not segregate thc portion of pro-RER, respectively, due to changes in body CO2 tein breakdown actually used directly in support ofstores that are not related to any alteration in sub- muscle contraction (oxidation and gluconeogene-strate metabolism. RER will decline during steady- sis) from other metabolic pathways or muscle dam-state exercise, reflecting an increase in fat metab- age. It does, nonetheless, illustrate the need to con-olism. Many studies have found no significant dif- sider protein metabolism when attempting to
Exercise in the Cold 371
quantify energy expenditure and substrate utilisa- higher, and postexercise content lower, in subjectstion during exercise. who performed the cold exposure. When a higher
workload was used (85 to 120W) this study found1.3 Carbohydrate Metabolism equivalent decreases in muscle glycogen in both air
temperatures. At the lighter workload muscle tern-There is little doubt that circulating glucose plays perature may have been lower than at the higher
an important role in tolerance to cold and in ex- workload, thereby increasing the reliance on muscleercise endurance. Exogenous manipulation of yen- glycolysis. This postulate is supported by the find-ous glucose concentration with insulin infusion has ing that glycolysis is higher in vastus lateralis muscleshown that hypoglycaemia will suppress shivering cooled to 28 to 29°C prior to exercise than in muscle(Gale et al. 1981) and significantly reduce rectal at 35°C (Blomstrand et al. 1986; Blomstrand &temperature (Mager & Francesconi 1983). In the Essen-Gustavsson 1987).absnce of exogenous manipulation, Jacobs et al.(1984) found no significant change in plasma glu- 1.4 Lactate Metabolismcose following a resting immersion in 10°C waterthat resulted in a 1l°C drop in core temperature.thatresltedin VCdropin oretempratre. Since there is an inverse relation between mnuscleThere was a significant decrease in insulin and a Sincerthre an ie ratio n beteen uenonsignificant increase in glucagon. Likewise, no temperature and the rate ofglycolysis, it is not sur-significant change occurred in glucose concentra- prising that many studies have reported venous
tion after thermally protected subjects had been lactate concentrations to be higher with exercise in
immersed in 5C water for 6 hours, performing 9 the cold than under warmer conditions (Doubt &
minutes of moderate work each hour (Smith et al. Hsieh 1991; Jacobs et al. 1984, 1985). Absolute
1990). values of lactate appear to be higher in cold water
It is readily appreciated that exercise generally (Goodman et al. 1985) than in cold air (Jacobs et
can not be sustained if glucose concentrations fall al. 1985; Therminarias et al. 1989), but the reason
below 3.5 to 4.0 mmol/L. Glucose concentrations is not obvious.
during steady-state submaximal ex.ercise usually do Increases in blood lactate are generally consid-
not fall below this range, and cold exposure per se ered to reflect a higher anaerobic contribution to
does not appear to significantly modify the rate of the work effort (Pendergast 1988).decline. For example. gluco.e concentration and it- The appearance of lactate in the venous circu-rate of decline were similar during 60 minutes of lation has, however, a time lag that may be tem-
exercise at 1.5 W/kg in 18 and 28°C water (Doubt perature dependent. Brief high intensity exercise& Hsieh 1991). Whether longer exercise periods or resulted in no difference in venous lactate duringgieater thermal stress alter control of circulating exercise using cooled vs notmothermic muscle, al-glucose remains to be determined, though intramuscular and postexercise venous lac-
The rate of muscle glycogen utilisation during tate values were higher in the cooled musclecold exposure depends on the interaction between (Blomstrand et al. 1986).cold and exercise intensity. At rest, muscle glyco- Therminarias et al. (1989) obtained venous lac-gen content has little effect on the change in core tate samples at the end of each incremental in-temperature during cold water immersion (Young crease in workload conducted at -2 and +24°C airet al. 1989). The combination of cold and light ex- temperatures. Lactate values were higher in the coldercise decreased glycogen by 23% in vastus lateraiis air at workloads from 30 to 90W, and increased atmuscle following 30 minutes of exercise at 50 to a slower rate than in 240C air. The rate was also65W in 9°C air, whereas the same workload in 21°C slower at workloads >120W, leading to lower lac-air resulted in minimal glycogen depletion (Jacobs tate levels in the -2°C air. A cold-induced delayet al. 1985). Pre-exercise glycogen content was in lactate release from muscle may have contrib-

372 Sports ?fedicine 11 (6) 1991
uted, in part. to the observed lower lactate values higher VE than when a similar workload was per-as work intensity increased, formed in the laboratory at a similar water tem-
Decreases in the aerobic utilisation of lactate perature (Cooper et al. 1976).within muscle (i.e. lactate shuttle) or decreases inits hepatic clearance could also contribute to higher 2.2 Oxygen Consumptionvenous concentrE.tions during exercise in the cold.A recent review addresses the difficulties in eval- Oxygen consumption (402) will depend on theuating lactate metabolism solely on the basis of interplay of exercise intensity and duration withvenous concentrations (Stainsby & Brooks 1990). the overall thermogenic requirements. In general,
thermogenesis at rest will increase 4 02 to a max-2. Cardiopulmonary Changes imum value of about 1.5 L/min. Exercise is the
only effective means to increase heat production2.1 Ventilation (e.g. 402) above this level. Given the wide range
of rest and exercise paradigms, and environmentalA relative increase in minute ventilation (VE) temperatures, it is not entirely surprising to find
occurs upon initial exposure to a cold environment studies where exercise "O2 in the cold increased(Doubt & Francis 1989; Mekjavic & Bligh 1989). (Doubt & Hsieh 1991; McArdle et al. 1976; Ther-A higher VE, compared to the same workload un- minarias et al. 1989; Timmons et al. 1985) or didder warmer conditions, can persist during light ex- not change (Doubt & Smith 1990; Jacobs et al.ercise (Cooper et al. 1976), during continuous in- 1985; McArdle et al. 1976) relative to warmer con-creases in workload (Therminarias et al. 1989), or ditions or time of exposure. Leaner subjects tendduring discontinuous incremental increases in to have a higher exercise 402 during cold expos-workload (Moore et al. 1970). Differences between ures than subjects with more body fat (McArdle etVE in warm and cold trials diminish as workload al. 1984).increases (Therminarias et al. 1989). During steady- Studies employing incremental increases instate exercise VE eventually becomes equivalent to workload have noted a convergence of the 402 vswork done under warmer conditions (Doubt & workload curves for warm and cold trials, sug-Hsieh 1991; McMurray & Horvath 1979. gesting that the absolute temperature-related dif-
Increases in VE may reduce end-tidal CO2 ference in '02 decreases as work intensity in-(ETc 0 2). At rest or with light to moderate exercise, creases (McArdle et al. 1976; Moore et al. 1970;the reduction in ETCo 2 can result in mental con- Therminarias et al. 1989).fusion in persons working in cold environments Two mechanisms (apart from percentage body(Cooper et al. 1976), probably secondary to cere- fat) can account for higher exercise '02 values inbral vasoconstriction induced by a low arterial the cold. First, total body heat flux increases during
PCO2. This effect may, in fact, be a contributing exercise in the cold (Nadel 1984; Park et al. 1984;factor in fatal or near-fatal accidents in cold water Rennie 1988; Sagawa et al. 1988). If the rate of heat(Doubt & Francis 1989). loss is sufficiently large then one would anticipate
It is likely that the increase in VE upon initial activation of nonexercising thermogenic mechan-cold exposure is due, in large measure, to afferent isms. For example, overt shivering can persist dur-input from cutaneous thermal receptors (Mekjavic ing dynamic exercise in cold water (Hoar et al. 1976;& Bligh 1989). Gradual reductions in VE at rest or McArdle et al. 1976). While shivering does notduring exercise in cold environments may reflect contribute to the dynamic work effort, its presencehabituation of the peripheral thermal receptors. A will result in a higher exercise 402. On the otherpsychogenic component to the relative hyperven- hand, overt shivering was absent in one of Mc-tilation may also occur under some circumstances. Ardle's subjects during exercise, and in other stud-For example, open water swimming resulted in a ies was noted to be diminished or absent during

Exercise in thc.Cold 373
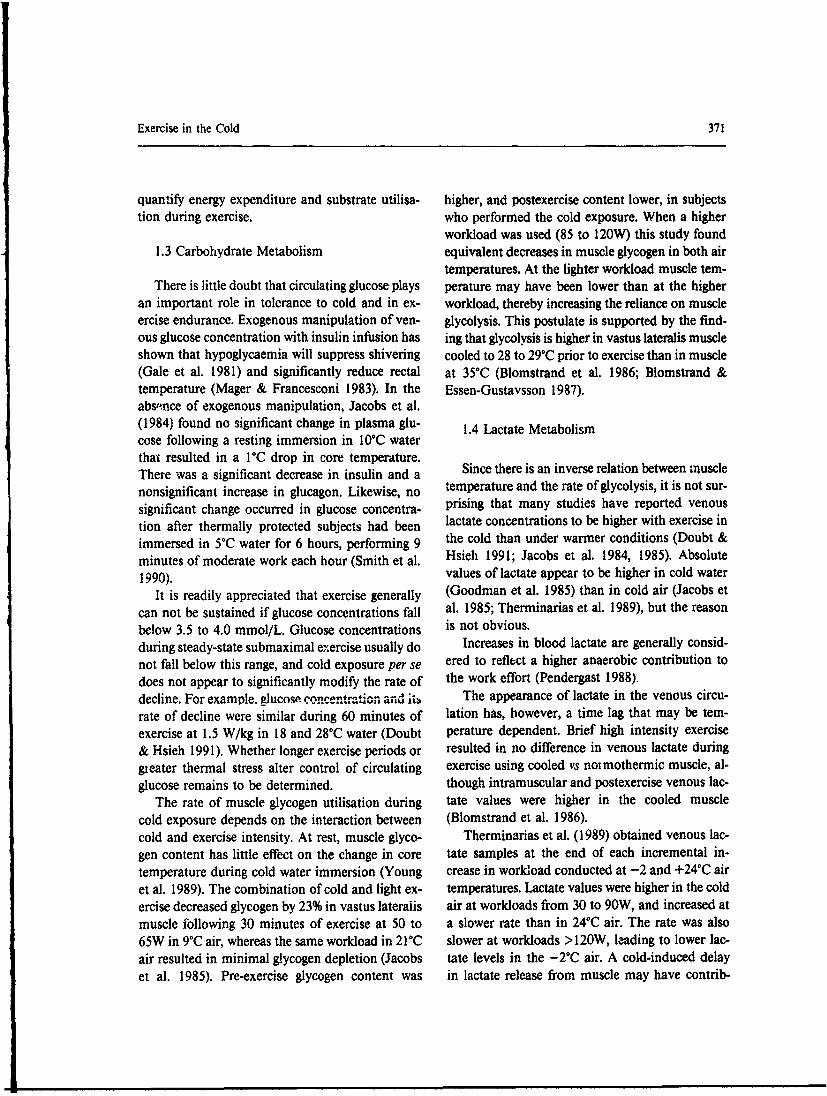
exercise (Craig & Dvorak 1968; Jacobs et al. 1985). 150 / o0We also did not observe shivering during exercise 125. 0 Dry * HOI + Peak 0. oin 18°C water, although exercise 402 was higher 0
100. 'zthan in 28°C water (Doubt & Hsieh 1991). The ab- . 0o.,/sence of overt shivering in the presence of a higher ' 75 4/
4r02 may reflect either nonshivering thermogene- 50 + 0sis or a subtle persistence of muscular shivering. 2
The second mechanism to consider relating a > 25higher exercise 402 to cold exposure is that net 0mechanical efficiency may be decreased (Pender- 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
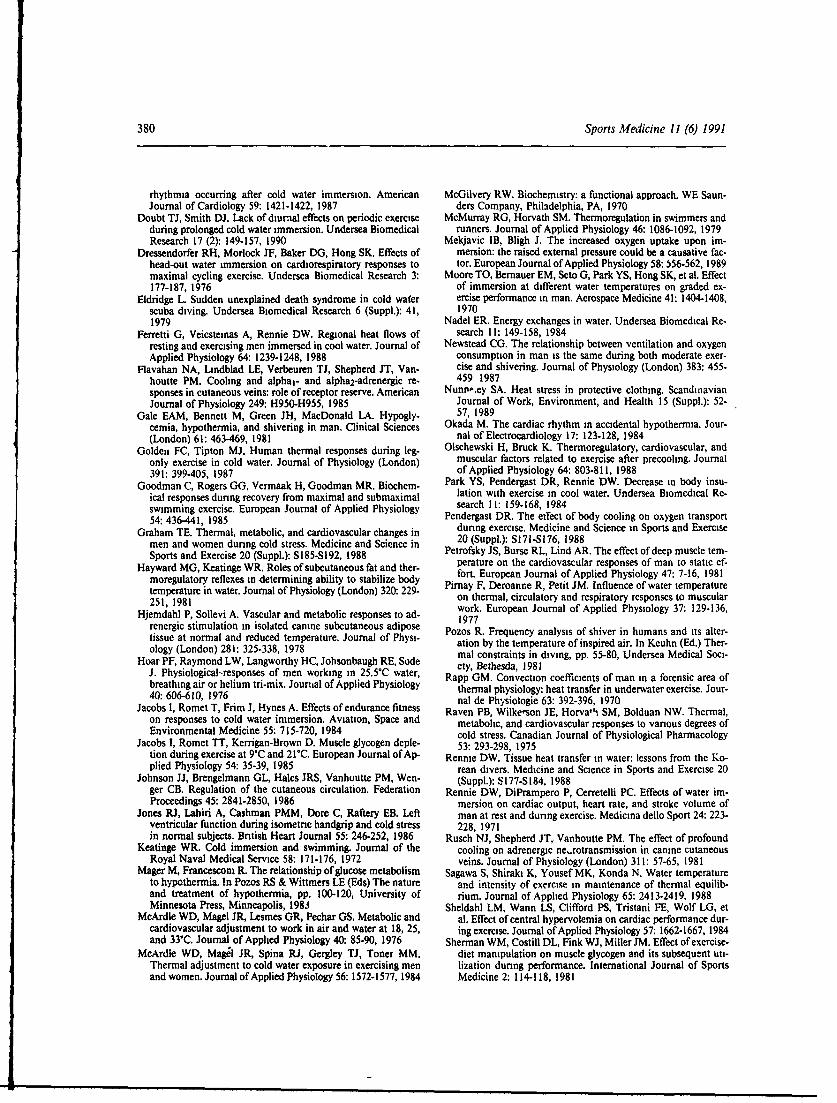
gast 1988). The kinetic energy required to perform oxyen uptake (1min)external work should not change as a function oftemperature (e.g. bike workload or running speed). Fig. 1. Relationship of minute ventilation to oxygen con-Therefore, the oxygen cost for this work should re- sumption obtained in dry and head-out immersion (HOI) in
18 to 31°C water, from rest to exhaustive workloads. HOImain independent of environmental temperature. resulted in significant shift in iE to 402 ratio at oxygen con-However, since cooled muscle has a reduced con- sumptions higher than 2.0 L/min. Crosses are resting data
tractile force per cross-sectional area, it has been from Meijavic & Bligh (1989) 1 minute after immersion in
proposed that more motor units might be recruited 10 to 40"C water, with 10 and 20"C data points appreciably
in order to meet the required work output (Blom- above the standard regression curve.
strand et al. 1986), potentially raising 402. In ad-dition, if shivering were present, it might involveboth agonist and antagonist muscle groups, in- tilatory equivalent when compared to exercise increasing the effort to conduct dynamic exercise. the dry (Doubt & Hsieh 1991; Moore et al. 1970;Even in the absence of overt shivering, muscle McArdle et al. 1976; Newstead 1987). Data from
agonist and antagonist groups could have increased thes e s t al s a te dncy 7fo t v i o r
activity that opposes movement and raises theequivalent to be higher during immersion when
oxygen cost of work. Support for this latter notion NO2 exceeds 2.0 L/min, but not in a temperature-comes from the study of Pozos (1981) where syn- dependent manner. Figure 1 illustrates this pointchronised EMG activity increased during cold ex- using data from several of our laboratory studies.posures in the absence of cvert shivering. The exponential fit of the immersed data begins to
Ventilatory Equivalent increase faster than the fit of the dry data at 402values greater than 2.0 L/min, such that V¢E ex-
The ratio of IE to 402 (ventilatory equivalent) ceeds '02. This mismatch of ventilation may be
provides a measure of how well ventilation can be due to immersion effects on alveolar-arterial 02
matched to the oxygen uptake requirement. Ther- gradients or ventilation-perfusion matching that
minarias et al. (1989) found this ratio to be higher become apparent at high work intensities.
in -2°C air than in 24°C air up to workloads of Figure 1 also contains peak resting values of150W with no temperature-related differences noted VE Vs 102 obtained during the first minute of im-
at higher intensities, suggesting that ventilation is mersion in water from 10 to 400C (Mckjavic &mismatched with oxygen demand at lower work- Bligh 1989). At temperatures below 20°C there isloads. Nearly the opposite effect is found during an obvious mismatch in E/ 4N02, since ventilationimmersion, although thermal stress does not exert is markedly higher than oxygen consumption. Ifa significant influence. At rest and during exercise exercise were to begin at this point it would likelyup to a 'M2 of about 2.0 L/min immersion in water require some time for the ventilatory equivalent tofrom 5 to 350C does not substantially alter the ven- return to the expected range.
374 Sports Medicine 11 (6) 1991
2.4 Heart Rate workload is largely unaffected by cold .,posureswhere ,ypothermna is absent.
Exposure to cold air or water causes a signifi- The oxygen pu!se (amount of 02 delivered percant peripheral vasoconstriction that results in an beat of the heart = "0 2/HR) may or may notelevation of blood pressure. In theory, barorecep- change with exercise in the cold. Relative to warmtor reflexes would attempt to lower pressure through control conditions, the oxygen pulse has been ob-a parasympathetically mediated reduction in heart served to increase in studies where exerciserate. However, it is far from universally observed 'O2 increased with no change in heart rate (Doubtthat resting or exercise heart rate will be lower with & Hsieh 1991), no change in 402 with decreasescold exposure. in heart rate (Sink et al. 1989), or where exercise
Males exposed to 5"C air had lower heart rates 402 increased and heart rate decreased (McArdleat rest and during exercise than in 22"C air, but no et al. 1976; Moore et al. 1970; Therminarias et al.significant changes were observed in females dur- 1989). A decrease in the oxygen pulse can occuring exercise (Stevens et al. 1987). Other studies, where there is no change in 4 02 coupled with anusing males, have noted heart rate to be relatively increase in heart rate, as observed in thermallylower duiing submaximal exercise in cold air (Sink protected subjects immersed for long periods in coldet al. 1989; Therminarias et al. 1989); while others water (Doubt & Smith 1990). McArdle et al. (1976)have found no difference between warm and cold have shown that the relationship of " 02 to heartair exposures (Jacobs et al. 1985). rate is shifted leftward in cold water, such that at
Decreases in heart rate upon head-out immer- a given heart rate the XO2 is higher. The varia-sion have often been noted, with a relative brady- bility of the oxygen pulse data obtained during coldcardia persisting throughout exercise compared to exposures also illustrates the difficulty of reliablydry conditions (Craig & Dvorak 1968; Dressen- predicting 1 02 from measures of heart rate alone.dorfer et al. 1976). Although these type studies haveused water temeratures below thermoneutral, a 2.5 Cardiac Arrhythmiaslower heart rate during immersion is not a priorievidence of a cold effect. We have, for example, Cardiac arrhythmias appear to be more fre-found no difference in exercise heart rzte for the quent with exercise in colder environments thansame workloads in 28 vs 18"C water (Doubt & in warmer environments (Doubt & Francis 1989).Hsieh 1991) or in 31 vs 20"C water (unpublished We have noted, for example, that cold water im-data). Dissimilar studies comparing warm with cold mersion increases the incidence of sinus dysrhyth-water have noted that exercise heart rate is reduced mias in healthy males; probably as a consequence(Craig & Dvorak 1968; Dressendorfer et al. 1976; of altered autonomic tone (Doubt et al. 1987). TheMcArdle et al. 1976; McMurray & Horvath 1979), incidence of ventricular extrasystoles is also notedunchanged (Pirnay et al. 1977) or even increased to be higher in colder environments (Keatinge 1972;(Cooper et al. 1976) in cold water. Such disparate Okada 1984); possibly related to increases in yen-results may reflect differences in level of fitness, tricular preload or afterload, or to increased sen-relative workload, sympathetic nervous system sitivity to higher catecholamine levels.arousal, psychogenic awareness of stress, shivering, The possibility exists that exercise in cold waterincreased muscle tonus or immersion times. may produce fatal cardiac arrhythmias. Eldridge
The slope of the linear relationship between (1979) did a retrospective study of scuba divingheart rate and exercise workload is little changed accidents and found a higher incidence of cardiacas a function of environmental temperature deaths occurred in cold water. Furthermore, she(McArdle et al. 1976; Moore et al. 1970) or dura- noted a positive correlation between the age of thetion of exposure (Doubt & Smith 1990). This in- diver and the occurrence of fatalities due to cardiacdicates that cardiac responsiveness to increases in events. Although aging and incidence of cardio-

Exercise in the Cold 375
vascular disease Eve positively correlated for the ever, stroke volume has been found to decline suchgeneral population, there is no definitive predictor that it may not differ significantly from controlas to how much an -udividual's risk of a serious conditions (Graham 1988; McArdle et al. 1976). Inarrhythmia might increase with exercise in the cold. these studies heart rate concurrently increasedFactors such as level of aerobic fitness will mod- (McArdle et al. 1976) or did not change (Grahamulate any age-related risk. 1988). Interestingly, Graham (1983) found that
women show little or no difference in stroke vol-2.6 Cardiac Output ume or heart rate during exercise in 5 vs 22"C air.
There are several factors that can influenceExposure to cold air increases intrathoracic changes in stroke volume in the cold. First, any
blood volume secondary to peripheral vasocon- increase in ventricular end-diastolic volume wouldstriction. Immersion in thermoneutral water in- result in a rightward shift in the Starling curve, po-creases thoracic blood volume by a hydrostatic ef- tentially to the point where stroke volume mightfect (Pendergast 1988). Cold water induces subsequently decline as the exercise demand in-peripheral vasoconstriction that further increases creased. Second, increases in myocardial oxygenthe thoracic volume, as implied by larger increases demand mentioned above may exceed cardiac re-in stroke volume (McArdle et al. 1976) or total body serve at high workloads, thereby reducing strokeinsulation (Rennie 1988). volume. Third, the positive inotropic or chrono-
The increase in thoracic blood volume resulting tropic effects of higher catecholamine levels mayfrom immersion has been shown to increase both support cardiac output.left ventricular end-diastolic and end-systolic di- Mild decreases in core temperature do not ad-mensions at rest and during exercise (Sheldahl et versely affect cardiac performance in healthy in-al. 1984). Such increases in cardiac dimensions are dividuals. Olschewski and Bruck (1988) reportedpresumptive evidence that wall tension increases, that a 15-minute exposure to 5 to 10°C air prior toboosting myocardial oxygen demand. Elevations in exercise lowered core temperature by 0.2°C. Dur-afterload can also alter cardiac function independ- ing light exercise stroke volume increased with noently of other physiological changes. For example, change in cardiac output relative to trials withoutimmersing a forearm in ice water raised blood precooling. During e.ercise at 80% 1O2max de-pressure 20 to 25% (i.e. afterload), and resulted in creases in stroke volume were comparable to con-a 7% decrease in left ventricular ejection fraction trol values although core temperature was aboutduring an isometric handgrip test (Jones et al. 1986). 0.50C lower with precooling. If this mild drop inThus, myocardial oxygen demand would be ex- core temperature had a negative influence on card-pected to increase during exercise in the cold as iac performance, one would have expected to seefunctions of increased preload (i.e. increased filling more of a decrease in stroke volume. Larger de-pressure, increased wall tension) and increased af- creases in core temperature, though, may result interload (i.e. increased blood pressure). a relative decline in cardiac output during exercise
Although absolute values may vary from la- (Pendergast 1988).boratory to laboratory, stroke volume will increaseon exposure to either cold air (Graham 1988; Raven 2.7 Peripheral Blood Flowet al. 1975) or cold water (McArdle et al. 1976;Pendergast 1988; Rennie et al. 1971). During light At rest, skeletal muscle blood flow is low. Con-to moderate exercise, stroke volume will generally sequently, muscle mass accounts for the major por-remain higher than equivalent dry or warm con- tion of passive body insulation at rest during coldditions, and heart rate will be lower, thereby re- exposures (Hayward & Keatinge 1981; Rennie 1988;suiting in little change in cardiac output compared Toner et al. 1986). With the onset of exercise,to control conditions. At higher workloads, how- muscle blood flow increases and reiuces insulation
376 Sports Medicine 11 (6) 1991
in direct proportion to workload. Blood flow to ac- in the exercise. However, thermal balance in thesetive muscle may be lower in cold environments, regions often will play a significant indirect role inhowever, at subnormal muscle temperatures overall performance. As an example, 14 of 63 ex-(Blomstrand et al. 1986; Pendergast 1988), posures of thermally protected subjects in 5°C water
The effects of cold on peripheral circulation are were terminated prematurely because low finger orsomewhat more complex than usually thought. toe temperatures produced undue discomfort evenThere is unanimous agreement that cold exposures though total body heat flux averaged only 125 W/result in peripheral vasoconstriction. Exercise pro- m2 and rectal temperature declined only 1.3°C induces a neurally mediated vasoconstriction that will 6 hours (Doubt & Smith 1990). In like fashion, onepersist up to maximal workloads (Johnson et al. can envision how athletic performance would be1986). Cold exposure magnifies the neurally and impaired if severe cold exposure of the digits re-humorally induced constriction of superficial cu- duced dexterity, or if heat loss through the headtaneous veins, while the opposite effect occurs in exacerbated body cooling.deep limb veins (Johnson et al. 1986). It has also Distal extremities depend on blood flow tobeen noted that cold exposures appear to primarily maintain suitable local temperature in the cold sinceinfluence the a2-adrenoreceptor constrictor re- their intrinsic capacity to generate heat is limited.sponse to noradrenaline (Flavahan et al. 1983). Cold induced vasoconstriction dramatically re-Data are currently lacking on how cold and exer- duces flow of warm arterial blood into the regioncise might modify the various types of adrenore- and local temperature falls. Prolonged low tem-ceptor responses in each of the peripheral circu- peratures in local regions can result in nonfreezinglatory beds, including skeletal muscle, cold injury or frostbite (Doubt & Francis 1989).
3. Thermal Aspects Neurally mediated vasoconstriction is inhibited
3.1 Respiratory Heat Loss at very low local temperatures, leading to vasodi-lation (Rusch et al. 1981). The resulting influx of
Measurements of net thermal balance usually warm arterial blood establishes a negative feedbackassume that respiratory heat loss represents about loop (often termed 'hunting relfex') where alter-8% of total body heat production (Ferretti et al. nating vasoconstriction and vasodilation results in1988; Rennie 1988; Sagawa et al. 1988; Toner et corresponding decreases and increases in local skinal. 1986). Estimates of respiratory heat loss have temperature. During exercise, heat flux from handsused measures of V'E and assumed values for in- and feet will increase (Ferretti et al. 1988), indi-spired and expired gas temperatures (Hayward & cating an increase in blood flow. Finger and toeKeatinge 1981). Respiratory heat loss during ex- temperatures commonly rise and the magnitude ofercise can be higher than at rest. For example, dry the 'hunting reflex' will diminish with exercise.and evaporative respiratory heat loss represented8% of total heat production at rest in 22°C water, 3.3 Skeletal Muscle Temperaturebut increased to 11 to 14% (concomitant with in-creases in VE) while swimming at speeds of 0.3 to Skin and subcutaneous fat account for <30% of0.5 m/sec (Rapp 1970). This finding indicates that total body insulation at rest in cold water (Hay-assuming a strict 8% value for respiratory heat loss ward & Keatinge 1981; Nadel 1984; Rennie 1988).may underestimate net thermal balance during ex- Muscle provides most of the insulation at rest.ercise in cold environments. Toner et al. (1986), comparing males of similar
3.2 Peripheral Thermoregulation body fat resting in 22°C water, measured higherbody insulation values in individuals with a higher
The head, hands, feet, external genitalia and skin muscle mass. With the onset of exercise, insilationare often not considered when discussing exercise values were similar for low and high muscle massin the cold, since they do not participate directly groups as would be expected if increased blood flow
Exercise in the Cold 377
decreased the passive insulation value of skeletal of environmental temperature and exercise proto-muscle (Park et al. 1984; Rennie 1988; Sagawa et col will result in lower than optimal temperaturesal. 1988). that could limit performance. One might also ex-
A number of studies have shown that body in- pect intramuscular temperature gradients to existsulation decreases as workload increases (Rennie during cold exposures, the magnitude of which1988; Sagawa' et al. 1988; Toner et al. 1984; Veic- could influence local muscle blood flow, motor unitsteinas et al. 1982). In water colder than about 25"C recruitment or endurance.cutaneous vasoconstriction is near maximum, andany exercise-related decreases in insulation would 3.4 Core Temperature Homeostasispresumably reflect an increase in muscle blood flow.Total body insulation for a given workload will be Preservaticn of core temperature in cold en-higher at lower water temperatures which suggests vironments depends on the ability to generatea relative underperfusion of muscle at colder tem- enough heat to offset avenues of heat loss. Thereperatures. is no doubt that exercise, while increasing meta-
Cooling of skeletal muscle will reduce contrac- bolic heat production, also increases the rate of heattile force and increase the rate of fatigue. Petrofsky loss. Not only is the rate of heat loss proportionalet al. (1981) found that maximum voluntary con- to workload (Ferretti et a!. 1988; Rapp 1970; Tonertractions and isometric endurance time 'a forearm et al. 1985) but the ratio of limb to trunk heat lossmuscles decreased at water temperatures below also increases directly with exercise intensity (Sa-20"C. In order to perform dynamic exercise in gawa et al. 1988).muscle cooled from 35 to 29"C, Blomstrand et al. Regional heat flux is not necessarily constant(1986) speculated that more fast twitch fibres might with exercise time, and varies considerably be-be recruited. The greater participation of fast twitch tween active and inactive limbs. Toner et al. (1985),glycolytic fibres could contribute to the higher rates for example, reported arm heat flux decreased fromof lactate production and shorter endurance times 65 to 60 W/m 2 during 60 minutes of leg exerciseoften noted with exercise in the cold. in 30"C water, whereas in 18"C water the flux de-
It is evident that deep muscle temperature de- creased from 205 to 75 W/m 2 . Leg heat flux in thispends both on environmental temperature and the study increased from 50 to 74 W/m 2 and decreasedintensity and duration of exercise. In vastus later- from 158 io 114 W/m 2 for 30 and 18"C, respec-alis muscle cooled to 29"C exercise at 370W for 1.5 tively. Peak values for active and inactive limb heatminutes increasea muscle temperature to only 33°C, fluxes may not occur simultaneously. During in-compared to 36°C for muscle starting exercise at termittent leg exercise in 25"C water, peak values35"C (Blomstrand et al. 1986). Thus, brief intense for arm heat flux occurred during exercise whileexercise will not raise precooled muscle to normal leg flux peaked during the subsequent postexerciseoperating temperatures. rest period (Thorp et al. 1990). The high peak fluxes
If exercise begins before muscles become cooled in the postexercise period might explain why in-it appears that muscle temperature can increase to termittent exercise in cool water often results innear normal levels. As an example, subjects who declines in core temperature (Hoar et al. 1976).began exercising shortly after immersion in 20*C At equivalent metabolic rates, arm exercise orwater had deep quadriceps muscle temperatures of a combination of arm-leg exercise resulted in greater38"C after 15 minutes of work at 'M2 values of decreases in core temperature than leg-only exer-1.0 to 2.0 L/min (Pirnay et al. 1977). This study cise in 20 and 26"C water (Toner et al. 1984). Sincealso confirmed that 1O2max occurs at a deep arm muscle mass is less than the leg, the equivalentmuscle temperature around 39"C. One can con- metabolic rate was presumably achieved at a greaterdude, therefore, that although exercise will :n- arm muscle blood flow. This would decrease in-crease muscle temperature, certain combinations sulation and promote greater heat loss, as was ev-

378 Sports Medicine 11 (6) 1991
ident from higher rates of total heat flux when arm could modify the amount of heat transferred to theexercise was employed, core for a given metabolic rate.
It has been a longstanding concern as to whetherthere is a crucial water (or air) temperature, below 4. Conclusionwhich exercise will be detrimental to the mainten-ance of core temperature (Keatinge 1972; Sagawa No single set of physiological responses can de-et al. 1988). However, since factors such as skin- scribe exercise responses in cold environments.fold thickness (Rennie 1988; Veicsteinas et al. 1982) There are simply too many circumstances to yieldcan modify responses to cold water exposure, it is one discrete result. However, a useful conclusiondifficult to define a discrete water temperature. An can be offered using a generic example that mayexercise v0 2 of 1.6 to 1.7 L/min for 60 minutes be useful to many readers. Table I will be used aswas more effective than rest in maintaining core a guide, employing one rest: work protocol. Thetemperature in 18 to 30"C water (McArdle et al. generic subject is not classified by age, gender or1984; Toner et al. 1985). We noted no significant dietary history. The cold exposure is also unclas-change in rectal temperature during 60 minutes of sified with respect to water or air.exercise at a N402 of 2.0 to 2.2 L/min in 18"C water After a brief resting exposure, the subject begins(Doubt & Hsieh 1991). Golden and Tipton (1987) to exercise. Vasoconstriction results in a relativereported that an exercise 402 of about 1.8 L/min reduction in blood flow that, coupled with slightlyprevented significant changes in rectal temperature cooled muscle, increases the reliance on glycolysis
during 40 minutes in 15°C water. For continuous to provide energy. As a consequence, lactate ac-
exercise, it would appear that core temperature can cumulates 'n the muscle at a higher rate and sub-
be maintained in water as cold as 15C with an sequently raises venous lactate levels.
exercise 02 around 2.0 L/min. The crucial water Increased muscle tonus and shivering raise oxy-temperature for intermittent exercise is likely higher gen consumption above that of a warmer climate.tieete forC inritt irexcti s i hhe Increases in cardiac preload and afterload increasesince even 25'C can result in reductions in core moada xgndmn.Srk ouei
tempratue (oar t a. 196).myocardial oxygen demand. Stroke volume isItemraurde reaily 1976).iad tlarger, but heart rate is reflexly reduced and cardiac
It soul bereadly pprciaed tat keltal output is near normal. Circulating catecholaminesmuscle is the heat generator during exercise, and ouptineroma.Ccltngaehlmnsactiemuscle stemeratr edr eperad provide positive inotropic support to the heart, al-active muscle temperatures exceed core tempera- though an occasional irregular beat occurs.ture by at least 0.5 to l.0°C (Pirnay et al. 1977). As exercise continues the muscle temperatureSince the generator is located in the periphery, any increases towards normal and blood flow increases.heat transferred to the core occurs convectively Anaerobic metabolism declines. Lipid mobilisa-through venous return. It is equally obvious that tion increases, but due to cold induced vasocon-not all heat generated within the muscle will be striction in peripheral adipose tissue, the rate is lesstransferred to the core, since a certain amount will than in warmer conditions. Utilisation of fat is re-be lost to the environment by conductive heat duced somewhat, but blood glucose levels remaintransfer through the tissue (Rennie 1988). For ex- within normal limits.ample, Ferretti et al. (1988) estimated that the heat Peripheral thermoreceptors, initially stimulatedproduction of thigh muscles working at 79W in by the cold, become adapted. The relative hyper-30°C water was 49% greater than the measured heat ventilation decreases. The rate of heat loss in-flux from the thigh. A majority of this difference creases with the start of exercise, but enough meta-between local production and loss represents heat bolic heat is generated by muscle to prevent a droptransferred convectively to the core. Different in core temperature. Skin blood flow remains low.muscle to environment temperature gradients, cir- The subject stops exercising momentarily. Largeculatory responses and cutaneous insulation values amounts of heat are lost and core temperature falls.
Exercise in the Cold 379
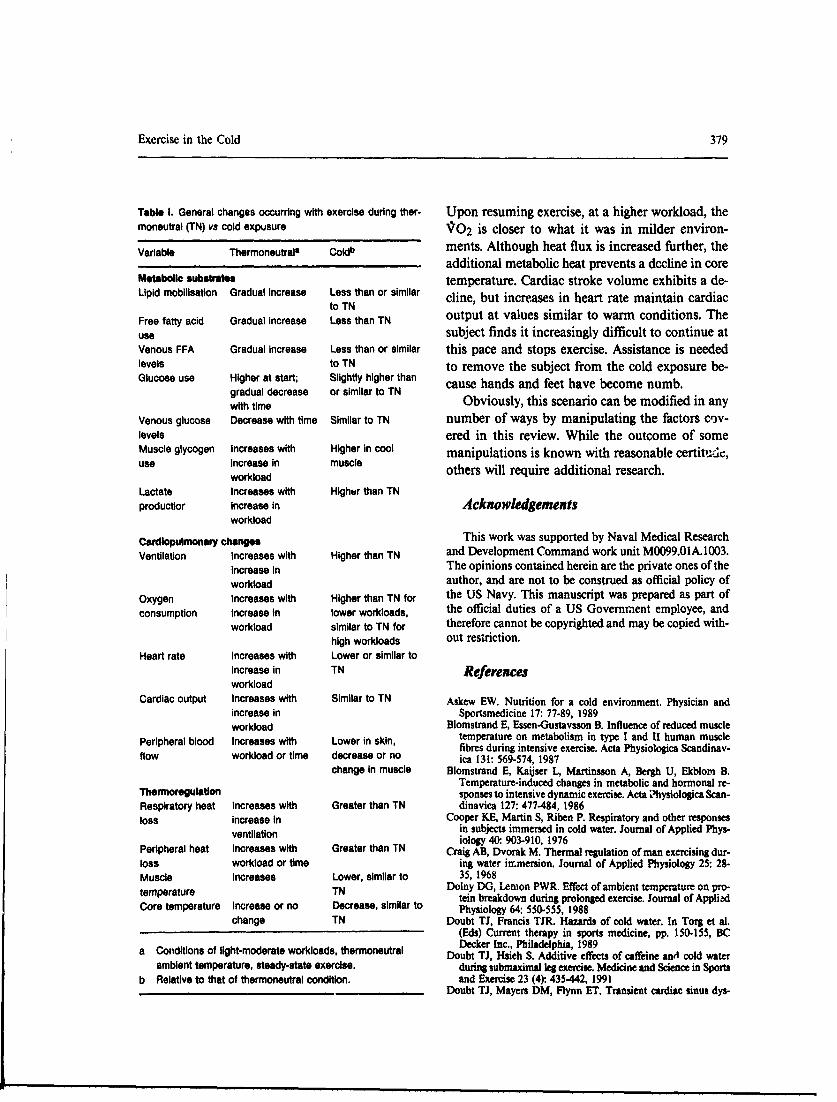
Table I. General changes occurring with exercise during ther- Upon resuming exercise, at a higher workload, themoneutral (TN) vs cold expusure 402 is closer to what it was in milder environ-
Variable Thermoneutrals Coldb ments. Although heat flux is increased further, theadditional metabolic heat prevents a decline in core
Metabolic substrates temperature. Cardiac stroke volume exhibits a de-Lipid mobilisation Gradual increase Less than or similar cline, but increases in heart rate maintain cardiac
to TNFree fatty acid Gradual increase Less than TN output at values similar to warm conditions. Theuse subject finds it increasingly difficult to continue atVenous FFA Gradual increase Less than or similar this pace and stops exercise. Assistance is neededlevels to TN to remove the subject from the cold exposure be-Glucose use Higher at start; Slightly higher thangradal ecrase or smilr t TN cause hands and feet have become numb.gradual decrease or similar to TN
with time Obviously, this scenario can be modified in anyVenous glucose Decrease with time Similar to TN number of ways by manipulating the factors c,)v-levels ered in this review. While the outcome of someMuscle glycogen Increases with Higher in cool manipulations is known with reasonable certitt-de,use increase in muscle others will require additional research.
workloadLactate Increases with Higher than TNproductior Increase in Acknowledgements
workload
Cardlopulmonary changes This work was supported by Naval Medical Research
Ventilation Increases with Higher than TN and Development Command work unit M0099.01A.1003.increase in The opinions contained herein are the private ones of theworkload author, and are not to be construed as official policy of
Oxygen Increases with Higher than TN for the US Navy. This manuscript was prepared as part ofconsumption increase in lower workloads, the official duties of a US Government employee, and
workload similar to TN for therefore cannot be copyrighted and may be copied with-
high workloads out restriction.Heart rate Increases with Lower or similar to
increase in TN Referencesworkload
Cardiac output Increases with Similar to TN Askew EW. Nutrition for a cold environment. Physician andincrease in Sportsmedicine 17: 77-89, 1989workload Blomstrand E, Essen-Gustavsson B. Influence of reduced muscle
Peripheral blood Increases with Lower in skin, temperature on metabolism in type I and II human musclefibres during intensive exercise. Acta Physiologica Scandinav-
flow workload or time decrease or no ica 131: 569-574, 1987change in muscle Blomstrand E, Kaijser L, Martinsson A, Bergh U, Ekblom B.
Temperature-induced changes in metabolic and hormonal re-Thermoregulation sponses to intensive dynamic exercise. Acta 11hysiologica Scan-Respiratory heat Increases with Greater than TN dinavica 127: 477-484, 1986loss increase in Cooper KE, Martin S, Riben P. Respiratory and other responses
ventilation in subjects immersed in cold water. Journal of Applied Phys-iology 40: 903-910, 1976Peripheral heat Increases with Greater than TN Craig AB, Dvorak M. Thermal regulation of man exercising dur-loss workload or time ing water immersion. Journal of Applied Physiology 25: 28-Muscle Increases Lower, similar to 35, 1968temperature TN Dolny DG, Lemon PWR. Effect of ambient temperature on pro-
tein breakdown during prolonged exercise. Journal of AppliedCore temperature Increase or no Decrease, similar to Physiology 64: 550-555, 1988
change TN Doubt TJ, Francis TJR. Hazards of cold water. In Torg et al.(Eds) Current therapy in sports medicine, pp. 150-155, BC
a Conditions of light-moderate workloads, thermoneutral Decker Inc., Philadelphia, 1989Doubt TJ, Hsieh S. Additive effects of caffeine and cold water
ambient temperature, steady-state exercise, during submaximal leg exercise. Medicine and Science in Sportsb Relative to that of thermoneutral condition, and Exercise 23 (4): 435-442, 1991
Doubt TJ, Mayers DM, Flynn ET. Transient cardiac sinus dys-
380 Sports Medicine 11 (6) 1991
rhythmia occurring after cold water immersion. American McGilvery RW. Biochemistry: a functional approach. WE Saun-Journal of Cardiology 59: 1421-1422, 1987 ders Company, Philadelphia, PA, 1970
Doubt TJ, Smith DJ. Lack of diurnal effects on periodic exercise McMurray RG, Horvath SM. Thermoregulation in swimmers andduring prolonged cold water immersion. Undersea Biomedical runners. Journal of Applied Physiology 46: 1086-1092, 1979Research 17 (2): 149-157, 1990 Mekjavic IB, Bligh J. The increased oxygen uptake upon im-
Dressendorfer RH, Morlock JF, Baker DO, Hong SK. Effects of mersion: the raised external pressure could be a causative fac-head-out water immersion on cardiorespiratory responses to tor. European Journal of Applied Physiology 58: 556-562, 1989maximal cycling exercise. Undersea Biomedical Research 3: Moore TO, Bernauer EM, Seto G, Park YS, Hong SK, et al. Effect177-187, 1976 of immersion at different water temperatures on graded ex-
Eldridge L. Sudden unexplained death syndrome in cold water ercise performance in man. Aerospace Medicine 41: 1404-1408,scuba diving. Undersea Biomedical Research 6 (Suppl.): 41, 19701979 Nadel ER. Energy exchanges in water. Undersea Biomedical Re-
Ferretti G, Veicstetnas A, Rennie DW. Regional heat flows of search 11: 149-158, 1984resting and exercising men immersed in cool water. Journal of Newstead CG. The relationship between ventilation and oxygenApplied Physiology 64: 1239-1248, 1988 consumption in man is the same during both moderate exer-
Flavahan NA, Lindblad LE, Verbeuren TJ, Shepherd JT, Van- cise and shivering. Journal of Physiology (London) 383: 455-houtte PM. Cooling and alpha,- and alpha2-adrenergic re- 459 1987sponses in cutaneous veins: role of receptor reserve. American Nunti,,ey SA. Heat stress in protective clothing. ScandinavianJournal of Physiology 249: H950-H955, 1985 Journal of Work, Environment, and Health 15 (Suppl.): 52-
Gale EAM, Bennett M, Green JH, MacDonald LA. Hypogly- 57, 1989cemia, hypothermia, and shivering in man. Clinical Sciences Okada M. The cardiac rhythm in accidental hypothermia. Jour-(London) 61: 463-469, 1981 nal of Electrocardiology 17: 123-128, 1984
Golden FC, Tipton MJ. Human thermal responses during leg- Olschewski H, Bruck K. Thermoregulatory, cardiovascular, andonly exercise in cold water. Journal of Physiology (London) muscular factors related to exercise after precooling. Journal391: 399-405, 1987 of Applied Physiology 64: 803-811, 1988
Goodman C, Rogers GG, Vermaak H, Goodman MR. Biochem- Park YS, Pendergast DR, Rennie DW. Decrease in body insu-ical responses during recovery from maximal and submaximal lation with exercise in cool water. Undersea Biomedical Re-swimming exercise. European Journal of Applied Physiology search 11: 159-168, 198454: 436-441, 1985 Pendergast DR. The efTect of body cooling on oxygen transport
Graham TE. Thermal, metabolic, and cardiovascular changes in during exercise. Medicine and Science in Sports and Exercisemen and women during cold stress. Medicine and Science in 20 (Suppl.): S171-S 176, 1988Sports and Exercise 20 (Suppl.): S185-S192, 1988 Petrofsky JS, Burse RL, Lind AR. The effect of deep muscle tem-
Hayward MG, Keatinge WR. Roles of subcutaneous fat and ther- perature on the cardiovascular responses of man to static ef-moregulatory reflexes in determining ability to stabilize body fort. European Journal of Applied Physiology 47: 7-16, 1981temperature in water. Journal of Physiology (London) 320: 229- Pirnay F, Deroanne R, Petit JM. Influence of water temperature251, 1981 on thermal, circulatory and respiratory responses to muscular
Hjemdahl P, Sollevi A. Vascular and metabolic responses to ad- work. European Journal of Applied Physiology 37: 129-136,H edah stimulation in isolated canine subcutaneous adipose 1977renervc nomlan reisolatemeueaoua ios Pozos R. Frequency analysis of shiver in humans and its alter-tissue at normal and reduced temperature. Journal of Physi- ation by the temperature of inspired air. In Keuhn (Ed.) Ther-
Hoarlog ayond LW,: Lngwory H, omal constraints in diving, pp. 55-80, Undersea Medical Soci-Hoar PF, Raymond LW, Langworthy HC, Johsonbaugh RE, Sode ety, Bethesda, 1981J. Physiological-responses of men working i 25.5"C water, Rapp GM. Convection coefficients of man in a forensic area ofbreathing air or helium tri-mix. Jourial of Applied Physiology thermal physiology: heat transfer in underwater exercise. Jour-40: 606-610, 1976 nal de Physiologic 63: 392-396, 1970
Jacobs I, Romet T, Frim J, Hynes A. Effects of endurance fitness Raven PB, Wilkeson JE, Horva63 SM, Bolduan NW. Thermal,on responses to cold water immersion. Aviation, Space and metabolic, and cardiovascular responses to various degrees ofEnvironmental Medicine 55: 715-720, 1984 cold stress. Canadian Journal of Physiological Pharmacology
Jacobs I, Romet TT, Kerrigan-Brown D. Muscle glycogen deple- 53: 293-298, 1975tion during exercise at 9'C and 21"C. European Journal of Ap- Rennie DW. Tissue heat transfer in water: lessons from the Ko-plied Physiology 54: 35-39, 1985 rean divers. Medicine and Science in Sports and Exercise 20
Johnson JJ, Brengelmann GL, Hales JRS, Vanhoutte PM, Wen- (Suppl.): S177-S184, 1988ger CB. Regulation of the cutaneous circulation. Federation Rennie DW, DiPrampero P, Cerretelli PC. Effects of water im-Proceedings 45: 2841-2850, 1986 mersion on cardiac output, heart rate, and stroke volume of
Jones RJ, Lahiri A, Cashman PMM, Dore C, Raftery EB. Left man at rest and during exercise. Medicina dello Sport 24: 223-ventricular function during isometric handgrip and cold stress 228, 1971in normal subjects. British Heart Journal 55: 246-252, 1986 Rusch NJ, Shepherd JT, Vanhoutte PM. The effect of profound
Keatinge WR. Cold immersion and swimming. Journal of the cooling on adrenergic nerotransmission in canine cutaneousRoyal Naval Medical Service 58: 171-176, 1972 veins. Journal of Physiology (London) 311: 57-65, 1981
Mager M, Francesconi R. The relationship of glucose metabolism Sagawa S, Shiraki K, Yousef MK, Konda N. Water temperatureto hypothermia. In Pozos RS & Wittmers LE (Eds) The nature and intensity of exercise in maintenance of thermal equilib-and treatment of hypothermia, pp. 100-120, University of rium. Journal of Applied Physiology 65: 2413-2419, 1988Minnesota Press, Minneapolis, 1983 Sheldahl LM, Wann LS, Clifford PS, Tristani FE, Wolf LG, et
McArdle WD, Magel JR, Lesmes GR, Pechar GS. Metabolic and al. Effect of central hypervolemia on cardiac performance dur-cardiovascular adjustment to work in air and water at 18, 25, ing exercise. Journal of Applied Physiology 57: 1662-1667, 1984and 33"C. Journal of Applied Physiology 40: 85-90, 1976 Sherman WM, Costill DL, Fink WJ, Miller JM. Effect of exercise-
McArdle WD, Magil JR, Spina RJ, Gergley TJ, Toner MM. diet manipulation on muscle glycogen and its subsequent uti-Thermal adjustment to cold water exposure in exercising men lization during performance. International Journal of Sportsand women. Journal of Applied Physiology 56: 1572-1577, 1984 Medicine 2: 114-118, 1981

Exercise in the Cold 381
Sink KR, Thomas TR, Araujo J, Hill SF. Fat energy use and by exercise in a cold environment. Medicine and Science inplasma lipid changes associated with exercise intensity and Sports and Exercise 17: 673-678, 1985temperature. European Journal of Applied Physiology 58: 508- Toner MM, Sawka MN, Foley ME, Pandolf KB, Effect of body513, 1989 mass and morphology on thermal responses in water. Journal
of Applied Physiology 60: 521-525, 1986Smith DJ, Deuster PA, Ryan CJ, Doubt TJ. Prolonged whole Toner MM, Sawka MN, Holden WL, Pandolf KB. Compansonbody immersion in cold water: hormonal and metabolic of thermal responses between rest and leg exercise in water.changes. Undersea Biomedical Research 17 (2): 139-147, 1990 Journal of Applied Physiology 59: 248-253, 1985
Stainsby WN, Brooks GA. Control of lactic acid metabolism in Toner MM, S~awka MN, Pandolf KB. Thermal responses duringcontracting muscles during exercise. Exercise and Sports Sci- arm and leg and combined arm-leg exercise in water. Journalences Revicw 18: 29-64, 1990 of Applied Physiology 56: 1355-1360, 1984
Stevens GHJ, Graham TE, Wilson BA. Gender differences in car- Veicsteinas A, Ferretti G, Rennie DW. Superficial shell insulationdiovascular and metabolic responses to cold and exercise. Ca- in resting and exercising men in cold water. Journal of Appliednadian Journal of Physiological Pharmacology65: 165-171, 1987 Physiology 52: 1557-1564, 1982
Therminarias A, Flore P, Oddou-Chirpaz MF, Pellerei E, Quinon Young AJ, Sawka MN, Neufer PD, Muza SR, Askew EW, Pan-A. Influence of cold exposure on blood lactate response dunng dolf KB. Thermoregulation during cold water immersion isincremental exercise. European Journal of Applied Physiology unimpaired by low muscle glycogen levels. Journal of Applied58: 411-418, 1989 Physiology 66: 1809-1816, 1989
Thorp JW, Mittleman KD, Haberman KJ, House JF, Doubt TJ.Work enhancement and thermal changes during intermittentwork in cool water after carbohydrate loading, Technical Re- Correspondence and reprnts: Dr Thomas J Doubt, Hyperbancport 90-14, Naval Medical Research Institute, Bethesda, 1990 Environmental Adaptation Program, Naval Medical Research
Timmons BA, Araujo J, Thomas TR. Fat utilization enhanced Institute, Bethesda, MD 20814, USA