part a treatment adherence site visit reviews kinga cieloszyk, md,mph deputy medical director of...
TRANSCRIPT

Part A Treatment Adherence Site Visit reviews
Kinga Cieloszyk, MD,MPH Deputy Medical Director of Clinical Care , NYCDOHMH,
HIV Care, Treatment, and Housing Program
Jacqueline P. Colon, MHAPart A Program Manager, NYSDOH, AIDS Institute
Quality Management Program

Purpose of Site Visit
Joint effort by the NYC and NYS Department of Health in support of quality improvement efforts across all Part A programs
Unexpectedly low service performance scores in several quality indicators
Address questions related to program scores Assessment of service provision and gaps that
may have impacted program’s ability to meet each quality indicator
Address program's ongoing service performance needs through quality improvement activities

Part A Programs Reviewed
Six Part A Treatment Adherence Programs reviewed:
Two Community Based Organizations (CBO’s)
Two clinic based programs Two hospital based providers

Overview of Treatment Adherence Indicators
Indicators are established with the involvement of various key stakeholders:
Part A service providers Clinical consultants, educators Treatment Adherence Quality Learning
network committee members NYSDOH Part A Quality Management staff NYCDOHMH, HIV Care, Treatment, and
Housing Program staff other representatives as deemed appropriate.

Overview of Treatment Adherence Indicators
Once indicators are chosen, a statistician assists with developing a method for the sampling of records.
The sampling plan ensures that enough records are reviewed to provide reliable, meaningful data, without requiring the review of more records than necessary.

Barriers with Treatment Adherence Indicators
Program staff at the various facilities reviewed identified indicators were too rigid
Too many indicators for initial review Difficulty to assess all indicators Different standards addressed by AI and
NYCDOHMH versus the program’s current contractor

Barriers with Treatment Adherence Indicators
Indicators are too clinical in nature for the various programs
Providers identified based on level of importance i.e. standard of care such as VL and CD 4 values) was most important to collect) and other support services were not relevant to integrating TAS

Barriers with Treatment Adherence Indicators
Documentation of the TA indicators was time consuming and did not occur at every intervention (i.e. due to the onset of client needs)
Unable to meet minimum requirements (i.e. adherence to ARV therapy has been quantified and documented every 4 months) versus various provider’s collecting information from PCP at 6 month intervals
Barriers with Treatment Adherence Indicators
Inability to obtain indicator information in a timely manner (CD 4 and VL values) since most programs are not co-located
Some indicators are not very important and do not accurately reflect what occurs at all facilities

Indicator Compliance
Not meeting initial documentation standards
Documentation activities do not reflect treatment adherence activities
Information was difficult to find Staff retention issues affected some
programs

Indicator Compliance
Counseling activities and other interventions offered did not support treatment adherence activities
The integration of treatment adherence services was not clear
Evidence does not suggest effective integration of care for some programs

Review of Program Models
Elements of a Treatment Adherence Program Target population/enrollment
criteria/intake process Barrier identification/treatment
readiness assessment How, when and how often services will
be delivered ART assessment & Quantification of
adherence

Review of Program Models
Treatment adherence support tools (curriculum-based education, individual and/or group counseling, peer support, pillboxes, DOT, etc.)
Link to non-medical case management (includes advice and assistance in obtaining social, community, legal, financial, and other needed services)

Review of Program Models
Staff training/supervision Multidisciplinary team
communication/rounds Strategies to engage, re-engage and
maintain clients in care Criteria for service
intensity/step-down/program completion

Responses from Part A Treatment Adherence Questionnaire
Barriers to Program Implementation
Frequently missed appointments/ lost-to-follow-up
Patient fails to obtained ordered labsPatient barriers: mental health,
substance use, legal issues, housing needs

Responses from Part A Treatment Adherence Questionnaire
Barriers to Program Implementation
Lack of co-location with limited record access
Working with multiple providers Limited staff (case managers, outreach
workers, data entry)
Review of the Evaluation Process
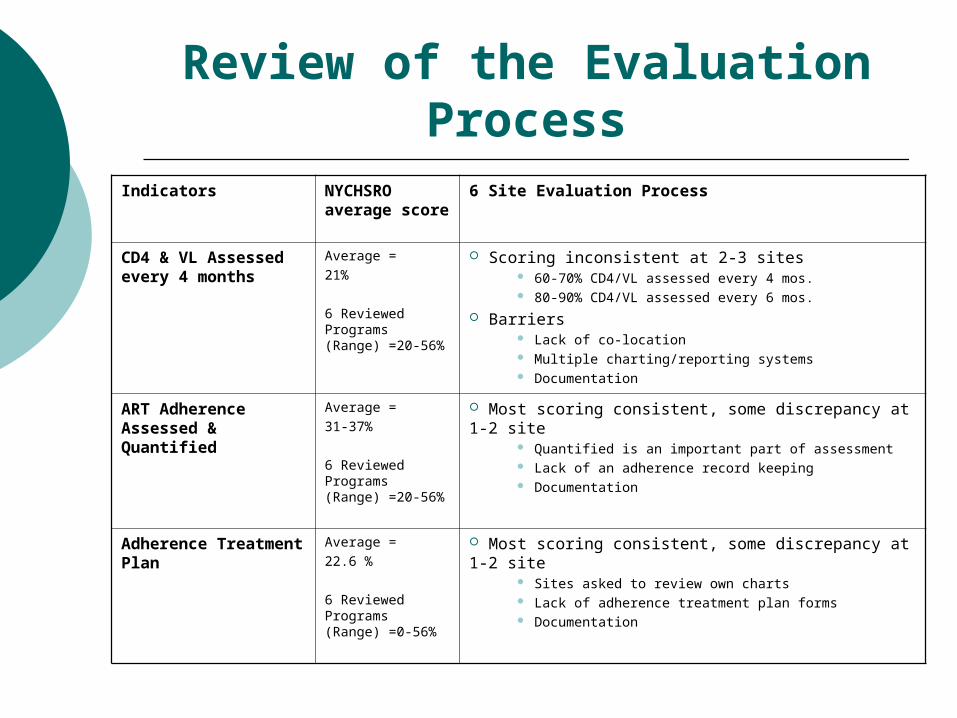
Indicators NYCHSRO average score
6 Site Evaluation Process
CD4 & VL Assessed every 4 months
Average =21%
6 Reviewed Programs (Range) =20-56%
Scoring inconsistent at 2-3 sites 60-70% CD4/VL assessed every 4 mos. 80-90% CD4/VL assessed every 6 mos.
Barriers Lack of co-location Multiple charting/reporting systems Documentation
ART Adherence Assessed & Quantified
Average =31-37%
6 Reviewed Programs (Range) =20-56%
Most scoring consistent, some discrepancy at 1-2 site Quantified is an important part of assessment Lack of an adherence record keeping Documentation
Adherence Treatment Plan
Average =22.6 %
6 Reviewed Programs (Range) =0-56%
Most scoring consistent, some discrepancy at 1-2 site Sites asked to review own charts Lack of adherence treatment plan forms Documentation

Documentation
Documentation Improvement
Proper documentation is critical Chronological record of patient care that
contributes to high quality Allows treatment to be planned and
monitored over time Effective ‘communication’ between staff
and improves hand-offs
Documentation
Documentation Improvement
Appropriate utilization review and quality of care evaluations
Assists in the defense of staff in the event of legal cases
Service reimbursements Collection of data that may be useful in
data evaluation and research

Documentation
Documentation Improvement Programs
Part of a site’s ‘Quality Improvement Project in HIV Care
Comprehensive and well-designed program focused at developing a well-documented adherence record system

Key components of documentation
Adherence record should be complete and legible (date and legible identity of staff)
Best practice: Adherence section
Treatment Plan (date, reason for enrollment/referral, barrier assessment, ART treatment review, service intensity (e.g. frequency of follow-up), use of supportive tools (e.g. pillbox) , assessment/service plan, follow-up/next appointment, communication with PCP/team)
Progress notes (date, reason for encounter, medication review, adherence quantification, labs, assessment/plan, next follow-up)
Flow sheet Trend: labs, ART, adherence rate
(quantified), etc.
Date CD4/ %
VL % of doses missed
HAART (regimen & dose, start date, date end, reason for change)
Treatment Plan Developed
Barrier Assessment
SAMPLE FLOW SHEET

Summary of Finding & Recommendations
Identified Challenges Improving the Process
Indicators Too manyDifficult to measureChanging standardsSome not very relevant
Re-evaluate & re-consider some chosen indicators (relevance, measurability, accuracy, improvability)Run an ‘indicator pilot test’
Treatment Adherence Program Models
Range of program models – from weak to strong Lacking ‘Treatment Adherence Program’ elements
Present ‘Best Practice’ Program ModelsTreatment Adherence Learning Networks – share experiencesStandardize ‘best practice’ program elements
Documentation Varied across programs – missing treatment adherence forms, plan updates, dedicated adherence sections, flow sheets
QI- Documentation Improvement Projects!
Review process
Multiple reviewers (NYSDOH/ PHS/ DOHMH)Weak collaboration and information sharing
Review findings to validate resultsFeedback from providers –what worked well and what posed challengesAnalyze and share resultsDOHMH/NYSDOH/PHS improve measurement process & work together!

Questions & Comments

Thank you

Contact Information
Kinga Cieloszyk, M.D., MPH Deputy Medical Director of Clinical Care , NYCDOHMH,
HIV Care, Treatment, and Housing Program
Tel: (212) -788-4660
Email: [email protected]
Jacqueline Colon, MHAProgram Manager, Part A Quality Management Program
Tel: (212) 417-4615
Email: [email protected]