peristomal skin photographs: results of a preliminary ... · tool and studio alterazioni cutanee...
TRANSCRIPT
12 ostomy wound management® march 2014 www.o-wm.com
Feature
the reliability and Validity of Color Indicators using digital Image analysis of Peristomal skin Photographs: results of a Preliminary Prospective Clinical study Shinji Iizaka, PhD; Mayumi Asada, MHS; Hiroe Koyanagi, MHS; Sanae Sasaki, BSN; Ayumi Naito, MHS; Chizuko Konya, PhD; and Hiromi Sanada, PhD
abstractAccurate assessment is necessary to evaluate peristomal skin condition, but objective methods are lacking. The purpose of this prospective, repeated-measures study was to evaluate the reliability and validity of color indica-tors using digital image analysis of peristomal skin photographs. The 6-month study was conducted among 21 patients (mean age 65.1 years old, 15 men) with ostomies (14 colostomies, six ileostomies, and one urostomy) at four outpatient clinics. Photographs taken by nurses of the peristomal area using point-and-shoot cameras were processed using digital image analysis, which involved color calibration, image processing, and indicator calcula-tion. An erythema index (EI), melanin index (MI), and hypopigmentation index were created to represent increased degrees of red, black, and white color, respectively, and their average values in the peristomal region of an image were calculated relative to values for intact skin. Reproducibility was evaluated using the interclass correlation co-efficient (ICC). ICCs of color indicators for intact skin were >0.7 between baseline and the end of follow-up for the 16 participants with two or more clinic visits. Differences in these indices between peristomal and intact regions were evaluated using a linear mixed model. The EI and MI of peristomal skin were significantly higher than those of intact skin (n = 42, P <0.001). All color indicators in adjacent regions and areas where adhesive was applied were associated with the discoloration severity score and visual analogue pain score (all P <0.05). This objective and simple method had adequate reproducibility and criterion-related validity and may be useful for peristomal skin as-sessment. Further research is warranted.
Keywords: ostomy, assessment, nursing, validity, reliability
Index: Ostomy Wound Management 2014;60(3):12–29
Potential Conflicts of Interest: This study was funded by a grant from the Japanese Society of Stoma and Con-tinence Rehabilitation, 2011. The funding organization had no role in the design, data collection, analysis, review, or approval of the manuscript.
Dr. Iizaka and Ms. Asada are nurses, Department of Gerontological Nursing/Wound Care Management, Division of Health Sciences and Nursing, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan. Ms. Koyanagi and Ms. Sasaki are wound, ostomy, and continence nurses, The University of Tokyo Hospital, Tokyo, Japan. Ms. Naito is a wound, ostomy, and continence nurse, Fujisawa City Hospital, Kanagawa, Japan. Dr. Konya is a professor and a wound, ostomy, and continence nurse, School of Nursing, Kanazawa Medical University, Ishikawa, Japan. Dr. Sanada is a professor and a wound, ostomy, and conti-nence nurse, Department of Gerontological Nursing/Wound Care Management, Division of Health Sciences and Nursing, Graduate School of Medicine, The University of Tokyo. Please address correspondence to: Shinji Iizaka, PhD, Department of Gerontological Nursing/Wound Care Management, Division of Health Sciences and Nursing, Graduate School of Medicine, The University of Tokyo Hospital, Faculty of Medicine Building No. 5-304, Bunkyo-ku, Tokyo 113-0033 email: [email protected].
DO NOT D
UPLICATE

march 2014 ostomy wound management® 13www.o-wm.com
dIgItal Image analysIs oF PerIstomal sKIn
Peristomal skin frequently is exposed to various negative stimuli, including mechanical stress secondary to repeat-
ed removal of adhesives, irritants associated with leakage of feces and urine, allergens in stoma care products, moisture from increased sweating under adhesives, and an increased biological burden from micro-organisms or fungi.1 These factors interdependently increase the risk of peristomal skin complications such as erosion, moisture-associated contact irritation, allergic dermatitis, folliculitis, and infection.1,2
Such complications are observed in 13% to 60% of people with a stoma depending on the stoma type and time since surgery.3-6 Peristomal skin complications often result in phys-ical symptoms such as pain and itching, compromised pouch attachment, increased medical costs, and decreased quality of life for patients.6-9 Therefore, prevention, early detection, and early treatment of peristomal skin complications are crucial issues in stoma care.
Accurate assessment of the peristomal skin condition is indispensable in selecting the most appropriate treatments among the various options available in stoma care.2 In addi-tion, clinicians should monitor skin conditions to determine the effects of the care provided. For these objectives, a stan-dardized indicator to evaluate, diagnose, and classify peristo-mal skin is required.10
Color is regarded as an important indicator in peristomal skin assessment, because peristomal skin complications are frequently accompanied by color changes such as erythema or hyperpigmentation.1,2,11 Clinicians assess color in the peri-stomal region to determine the severity of skin complications, evaluate the extent of discoloration and the areas involved, and monitor improvements as abnormal color disappears. Although several standardized tools such as the Ostomy Skin Tool and Studio Alterazioni Cutanee Stomali instrument include items related to discoloration,12,13 these evaluations depend solely on subjective classification of discoloration, possibly resulting in inadequate inter-rater agreement.14 Fur-thermore, these tools may have insensitive responsiveness in the monitoring of longitudinal peristomal skin changes such as decreased erythema and increased hyperpigmentation. An objective method would contribute to more accurate, precise, and continuous assessment of peristomal skin discoloration.
Digital image analysis recently emerged in dermatology and wound care as a novel method to evaluate color objec-tively.15-17 This method is also available for peristomal assess-ment, because peristomal photography is a common proto-col in stoma care for accurate documentation of the stoma condition.13 Digital image analysis of color has several advan-tages in stoma care: it uses a noncontact device, objective and quantitative measures, and two-dimensional assessment, all of which facilitate evaluation of both the severity and area of discoloration. Therefore, digital image analysis may be more suitable than reflectance spectrophotometers and tristimulus colorimeters that have been generally used to evaluate a lim-ited area of skin or wound.18
Considering the increased interest in wound care in home care settings using telemedicine or assessment via the inter-net, photograph and image analysis of peristomal skin will become essential techniques.19 In such situations, nurses in outpatient clinics must depend on visual assessment because they cannot directly assess peristomal burning, swelling, or abnormal smells, which usually are detected by palpation or olfaction. It is crucial that visual assessment maintains accu-racy across descriptions and personnel. Color indicators in digital image analysis of peristomal skin may be one solution to increase inter- and intra-rater reliability. The reliability and validity of this method have not been studied.
It was hypothesized that erythema, hyperpigmentation, and hypopigmentation are key parameters in the assessment of skin complications and that the degree of peristomal skin color can be evaluated using digital image analysis.11 The purpose of this study was to: 1) develop color indicators using digital image analysis of photographs of peristomal skin, and 2) evaluate the reliability, criterion-related valid-ity, and responsiveness — ie, confirmation of the change of indicators according to longitudinal color changes — in the clinical setting.
materials and methodsStudy design. A prospective, repeated-measures study
was conducted between October 2011 and March 2012. Pa-tients with a stoma who visited outpatient clinics for regular follow-up were recruited from four institutions. The outpa-tient clinics were recruited by snowball sampling (additional populations — ie, clinics — were introduced by those already included in the study) and comprised one university hospital and three community hospitals. Patients with 1) any type of stoma, including colostomy, ileostomy, and urostomy; and 2) any purpose for and type of stoma construction, includ-ing permanent or temporary stomas, were eligible. Patients
Key Points• Peristomalskinproblemsarecommon,andoptimal
assessment will help prevent serious complications and guide care.
• Theauthorsdevelopedandtestedcolorindicatorsusing digital image analysis of photographs of peris-tomal skin.
• Twenty-one(21)patientsparticipatedinthisvalidityand reliability study; of those, 16 had more than one assessment.
• Themethodusedhadadequatereproducibilityandcriterion-related validity.
• Thistechniqueispromisingforregularclinicandtele-medicine use, and additional research is warranted.
ostomy wound management 2014;60(3):12–29
DO NOT D
UPLICATE

14 ostomy wound management® march 2014 www.o-wm.com
Feature
who did not provide consent to participate were excluded. Patients were repeatedly evaluated based on their individual regular care plan during the study period; therefore, the in-terval of visits varied (range 1 week to 3 months). All repeat-ed data for a given patient at any time point were analyzed to evaluate the reproducibility and the responsiveness of image analysis to clinical changes in the peristomal skin condition. The study protocol was approved by the Ethics Committee of the Graduate School of Medicine, The University of Tokyo (#2634) and each clinic. Written informed consent was ob-tained from all patients.
Data collection. Patient demographics including age, gender, stoma type, underlying disease associated with stoma construction, and type of pouching system used were col-lected from the medical charts. In order to evaluate validity, visual peristomal skin condition and self-perception by pa-tients including pain and itching were selected as parameters. For visual peristomal skin assessment, wound, ostomy, and continence (WOC) nurses at each institution evaluated the Discoloration, Erosion, and Tissue overgrowth (DET) score of the Ostomy Skin Tool.12,14 This tool has been translated into Japanese, and the inter- and intrarater reliability among WOC nurses were confirmed for the Japanese version.20 The severity score and the area score for discoloration, erosion, and tissue overgrowth were evaluated, and the total score (range 0–15, where 0 = none and 15 = most severe) then was calculated. In addition, patients were asked to express the de-gree of pain and itching of peristomal skin on a 0- to 100-mm visual analogue scale (VAS) (0 mm = none, 100 mm = most severe).
Each WOC nurse photographed the peristomal skin using a digital point-and-shoot camera. Patients sat on a chair for stoma care, and the skin/stoma photograph was taken after removal of the pouching system and following skin cleans-ing. The nurses followed the written manual of photography and received explanations and training from the primary au-thor before the study. Skin was photographed approximately 10 minutes after pouch removal and cleansing.
The camera types were not strictly standardized in the data collection phase; WOC nurses used their own cameras for daily practice. Color settings were standardized by a color-calibration process (description to follow) during the image-processing phase so the difference in camera types was not anticipated to influence the result. A commercially available reference color chart with nine calibrated colors (Casmatch; Bear Medic Co, Tokyo, Japan) was placed on the surrounding skin. Photographs were taken to include the intact surround-ing skin, such as that on the opposite side of the stoma. A flash was not used except in an environment that would re-sult in extreme underexposure. The photographs were stored in JPEG format.
The photographs were processed by digital image analy-sis, which comprised color calibration, image processing, and indicator calculation.15 Color calibration was conducted
according to the standard protocol of the color chart by image-editing software (Photoshop 6; Adobe Systems Inc, San Jose, CA, USA). The detailed protocol is described else-where.15 Three images reflecting different colors were ob-tained from a calibrated photograph using ImageJ software (National Institutes of Health, Bethesda, MD, USA); these images were the erythema index (EI), melanin index (MI), and hypopigmentation index (HI) (see Figure 1). It was hypothesized that higher EI, MI, and HI values represent increased degrees of erythema, hyperpigmentation, and hy-popigmentation, respectively. The EI image was obtained from the formula logR – logG by the image calculator tool, indicating the result of subtraction of the R and G channels of the digital color images after they were logarithmically transformed.15,16 The MI image was obtained from the in-verted image of the logarithm of the R channels. The HI image was obtained by transforming the original RGB im-age into a 16-bit gray image that represented the degree of brightness. The image intensity was arbitrarily calibrated to standardize the intensity of the reference color (red for EI, black for MI, and white for HI) at 200. The intensity of each image ranged from 0 to 255, and a higher intensity indi-cated a brighter color.
To calculate the color indicators, a researcher manually selected the peristomal skin region including the stoma, the stoma region itself, and the intact skin region using a free-hand tool. The inter- and intra-rater reliability of this tech-nique have been reported previously.15 The peristomal skin region excluding the stoma — ie, the region covered by the pouch — was obtained by subtracting the stoma region from the peristomal skin region including the stoma. The peristo-mal skin region then was separated into the regions adjacent to the stoma and under the adhesive, because skin conditions supposedly differ between peristomal regions. The border of these regions was determined by the original image and ad-hesive sizes. The intact skin was determined as that on the opposite side of the stoma or that uncovered by adhesives without an operative incision on the abdomen. A histogram of the selected region was obtained. Because whiteout and blackout areas will exist in an image as noise caused by ele-ments such as light reflectance or shadow, the intensities 0–5 and 251–255 were deleted for the purpose of noise reduction. The mean intensity of each color in the region of interest was calculated as an indicator. All indicators in the peristomal regions were expressed as relative values for those on intact skin, because relative values may be helpful in assessing the effect of skin complications independent from a patient’s in-herent skin type. The representative values of each indicator for a specific patient are shown in Figure 2. In this patient, both the EI and MI ratios were increased in the region ad-jacent to the stoma, while only the MI ratio was high in the region under the adhesives with a slightly increased EI ratio secondary to erosion. These features corresponded to the vi-sual features.
DO NOT D
UPLICATE

16 ostomy wound management® march 2014 www.o-wm.com
Feature
Figure 1. A representative case: a) calibrated photograph; b) erythema index (EI) image; c) melanin index (MI) im-age; d) hypopigmentation (HI) index. Brighter colors indicate greater degrees of erythema in the EI image, hyperpig-mentation in the MI image, and hypopigmentation in the HI image.
A
C
B
D
Figure 2. Color indicators of a representative case; a) calibrated photograph; b) borders of regions; c) color indica-tors of the EI, MI, and HI in each region. Color indicators are expressed as relative values to those of intact skin. In this case, the EI and MI ratios are high in areas adjacent (within the yellow line) to the stoma and are as high as four times that of intact skin. In the adhesive region (within the blue line), the MI is higher than the EI, indicating chronic pigmentation dominates this region. These features correspond to the original photograph.
A B
C
DO NOT D
UPLICATE

18 ostomy wound management® march 2014 www.o-wm.com
Feature
Statistical analysis. Descriptive data at baseline were ex-pressed as mean (SD) for continuous variables and n (%) for categorical variables. The reproducibility or test-retest reli-ability of the color indicators in each patient was evaluated by an intraclass correlation coefficient (ICC) on intact skin between baseline and the end of follow-up, with the assump-tion that intact skin color will undergo little change. The ICC was interpreted according to common criteria; values of 0.21 to 0.40 indicate a “fair” correlation, 0.41 to 0.60 a “moderate” correlation, 0.61 to 0.80 a “substantial” correla-tion, and >0.81 an “almost perfect” correlation.21 To show the
descriptive statistics of the color indicators, the least square means were calculated by a linear mixed model that included all time pe-riods of evaluation for the same patients as a repeated variable (SAS PROC MIXED). Because the color indicators were expressed as relative values and were skewed, their logarithm values were used to make the distribution similar to the normal distribution. The same analytical procedure was applied to evaluate associations between the color indicators and DET and VAS scores, indicating criterion-related validity, and to assess the responsiveness of the color indicators against changes in the DET scores. All analyses were conducted using SAS version 9.3 (SAS Institute Inc, Cary, NC, USA). The statistical significance level was set at a P value of <0.05.
resultsA total of 21 patients with a sto-
ma was enrolled during the study period. The mean age (SD) was 65.1 (14.1) years, and 15 patients (71.4%) were male (see Table 1). One patient used a one-piece and all others used a two-piece pouch-
ing system. The median (range) duration since stoma con-struction was 14 (range 0–111) months. Sixteen (16) patients (76.2%) were evaluated twice or more. The most frequent stoma type was a colostomy (71.4%). The mean (SD) of the total DET score was 4.1 (2.9).
The reproducibility of the color indicators on intact skin was evaluated for the 16 patients who were evaluated twice or more (see Table 2). All ICCs for the EI, MI, and HI were >0.7, indicating substantial or almost perfect agreement between baseline and the end of follow-up.20 In total, 42 data parameters, including repeated data parameters in a patient, were available during the study period. As descrip-tive statistics of peristomal skin color (see Figure 3), the EI and MI ratios were significantly higher than 1 (P <0.001), indicating a higher EI and MI in the peristomal region, the region adjacent to the stoma, and the adhesive region than in intact skin. However, the HI ratio was significantly lower than 1 in each region, respectively (All P values <0.001). The EI and MI were significantly higher in the region adja-cent to the stoma than in the region under adhesives within a given patient (P <0.001).
table 1. Patients’ demographic characteristics (n = 21)
Variables Category Mean (SD) or n (%)
Age (years), mean (SD) 65.1 (14.1)
Gender, n (%) Female 6 (28.6)
Male 15 (71.4)
Evaluation time, n (%) 1 5 (23.8)
2 14 (66.7)
≥3 2 (9.5)
Stoma type, n (%) Colostomy 14 (66.6)
Ileostomy 6 (28.6)
Urostomy 1 (4.8)
Diseasea, n (%) Colon cancer 15 (71.4)
Crohn’s disease 2 (9.5)
Bladder cancer 1 (4.8)
Others 6 (28.6)
Discoloration, Erosion, Tissue overgrowth score, mean (SD)
Discoloration area 1.4 (0.9)
Discoloration severity 1.2 (0.6)
Erosion area 0.5 (0.5)
Erosion severity 0.7 (0.9)
Tissue overgrowth area 0.2 (0.4)
Tissue overgrowth severity 0.1 (0.4)
Total score 4.1 (2.9)
Pain scoreb, mean (SD) 1.1 (2.5)
Itching scoreb, mean (SD) 2.1 (2.6)amultiple responses; bincludes the values at every time point (n = 25)
table 2. reproducibility of color indicators on intact skin between two time points (n = 16)
Variables Mean (SD) ICC
Erythema index 30.87 (9.68) 0.760
Melanin index 35.64 (15.72) 0.841
Hypopigmentation index 120.57 (29.57) 0.889
ICC = intraclass correlation coefficient
DO NOT D
UPLICATE

20 ostomy wound management® march 2014 www.o-wm.com
Feature
For assessment of criterion-related validity, associations between color indicators and DET scores were evaluated (see Table 3). All color indicators in each region were signif-icantly associated with the DET discoloration severity score and total score (all P <0.05). The EI and MI ratios showed positive relationships and the HI ratio showed a negative relationship, indicating that clinically more severe peris-tomal skin discoloration was accompanied by increased erythema and hyperpigmentation. For assessment of the responsiveness of the color indicators, the data at baseline and at the end of the study duration were analyzed in the 16
patients who were evaluated twice or more (see Table 4). Changes in some color indicators in each region tended to be associated with changes in the DET discoloration se-verity score and total score, showing the color indicators changed according to the clinical condition. Not all asso-ciations reached statistical significance, possibly because of the lack of statistical power.
For assessment of pain and itching, 25 data parame-ters were available in total during the study duration. All color indicators in all regions were significantly associated with the pain score (all P <0.05) (see Table 5). The EI and MI ratios showed positive relationships and the HI ratio showed a negative relationship, indicating increased ery-thema or hyperpigmentation in patients who complained of a greater degree of pain in the peristomal region. How-ever, no color indicators were significantly associated with the itching score.
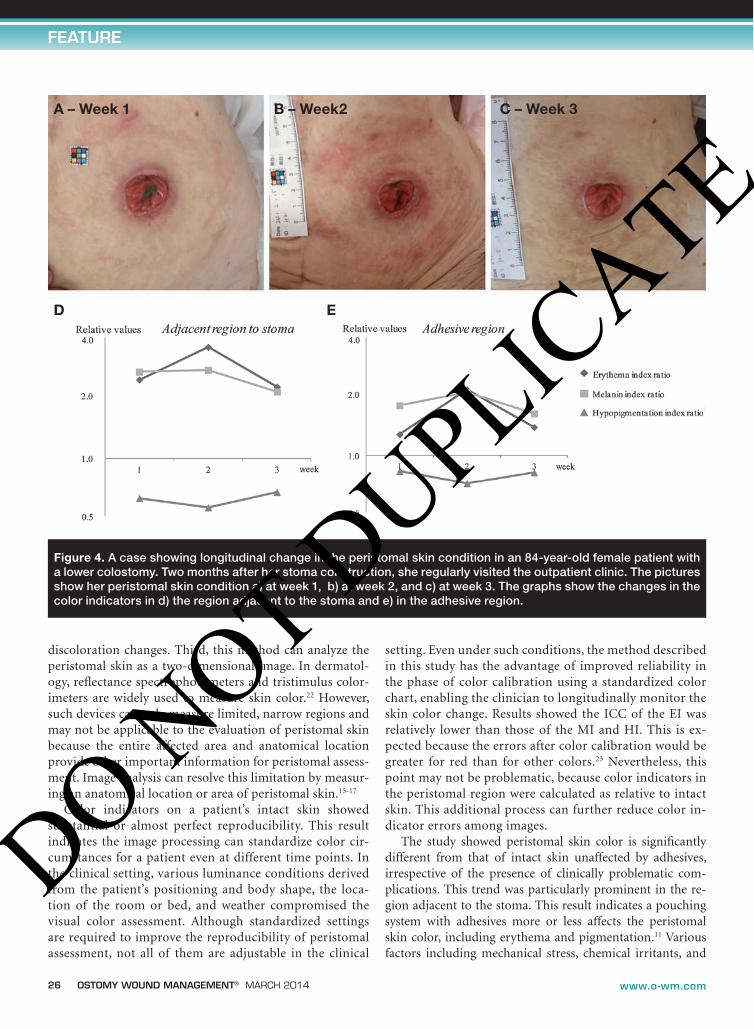
Longitudinal changes in the peristomal skin condition were monitored by the color indicators; a typical case is shown in Figure 4. The patient was an 84-year-old woman who had undergone surgical construction of a descending colostomy 2 months previously. At week 1 in the outpatient clinic, the peristomal skin in the region adjacent to the sto-ma showed increased EI and MI ratios; whereas, the skin under the adhesive showed slight pigmentation with an in-creased MI ratio. At week 2, irritant contact dermatitis, pos-sibly caused by mechanical stress, was apparent in the entire peristomal skin region with painful erythema, leading to a rapid increase in the EI ratio in both regions; the MI ratio remained constant. At this time, the types of adhesive and intervals between pouch changes were altered, and the use of moisturizing lotion was begun. After 1 week, the contact dermatitis was improved with color indicator values similar to those of the first week.
Figure 3. Descriptive statistics of color indicators. All color indicators are expressed as relative values to those of intact skin. Least square means were calcu-lated by a linear mixed model including all data for a pa-tient as a repeated variable. All values were significantly higher (EI and MI ratios) or lower (HI ratio) than 1 (all P < 0.001). Boxes: mean values. Bars: the upper and lower limits of the 95% confidence interval.
table 3. associations between relative color indicators and discoloration, erosion, and tissue overgrowth (det) score (n = 42)
DET discoloration severity DET total score
Regions Variables Bb P Bb P
Peristomal skina EI ratio 0.18 0.013 0.050 <0.001
MI ratio 0.21 0.019 0.050 0.008
HI ratio −0.09 0.030 −0.026 0.002
Adjacent region EI ratio 0.27 0.003 0.050 0.009
MI ratio 0.29 0.007 0.056 0.013
HI ratio −0.16 0.007 −0.031 0.008
Adhesive regiona EI ratio 0.14 0.038 0.046 0.002
MI ratio 0.19 0.027 0.048 0.007
HI ratio −0.08 0.033 −0.024 0.001
EI=erythema index; MI= melanin index; HI= hypopigmentation indexa One data parameter was excluded because an image was not available owing to shadingb Coefficients of regression (beta) were calculated from the linear mixed model including evaluation time as repeated variables
DO NOT D
UPLICATE

22 ostomy wound management® march 2014 www.o-wm.com
Feature
discussionTo the authors’ knowledge, this is the first study involving
objective digital image analysis of color for the evaluation of peristomal skin conditions in the clinical setting. This meth-od had adequate reproducibility for intact skin color and cri-terion-related validity of scores for a clinical assessment tool and patient’s perceived pain. In addition, responsiveness of the color change over time was partly confirmed. The color indicators (EI, MI, and HI) showed adequate features of reli-ability and validity in this study.
This image analysis using the EI, MI, and HI has sev-eral advantages. First, this is a noninvasive and quantitative method that uses routinely available photographs. Although
visual assessment by clinicians is the most important meth-od in clinical practice to assess peristomal skin complica-tions and select appropriate care,2 objective tools to support visual assessment are lacking. This simple method can be useful to quantitatively monitor changes in peristomal skin conditions. Second, three colors (red, black, and white) can be evaluated separately. A previous report11 retrospectively investigated peristomal skin conditions for patients using skin-barrier products for 1 to 10 years. Results showed in-flammatory changes gradually disappeared and pigmentary changes, including hyper- and hypopigmentation, became prominent at later periods over 5 years. Using multiple colors in combination may help evaluate complex skin
table 4. responsiveness of color indicators for changes in discoloration, erosion, and tissue (det) overgrowth score score (n = 16)
Change of DETa scoreDiscoloration severity
Change ofDETa total score
Regions Variable changes rb P rb P
Peristomal skina EI ratio −0.54 0.035 −0.65 0.008
MI ratio −0.37 0.169 −0.53 0.043
HI ratio 0.34 0.219 0.55 0.032
Adjacent region EI ratio −0.64 0.008 −0.46 0.075
MI ratio −0.44 0.089 −0.45 0.083
HI ratio 0.47 0.065 0.43 0.095
Adhesive regiona EI ratio −0.47 0.075 −0.64 0.010
MI ratio −0.39 0.145 −0.57 0.026
HI ratio 0.33 0.223 0.59 0.022
EI= erythema index; MI= melanin index; HI= hypopigmentation index a One data parameter was excluded because an image was not available owing to shadingb Positive coefficients indicate increased values of color indicators when the clinical status as evaluated by the DET score was improved and negative coefficients indicated the opposite
table 5. associations between relative color indicators and pain and itching scores by the visual analog scale (n = 21)
Pain score Itching score
Regions Variable changes Bb P Bb P
Peristomal skina EI ratio 7.12 0.007 −0.55 0.687
MI ratio 5.02 0.008 0.38 0.764
HI ratio −11.08 0.008 0.38 0.897
Adjacent region EI ratio 4.41 0.006 −0.12 0.939
MI ratio 3.50 0.002 −0.08 0.957
HI ratio −6.44 0.008 0.50 0.857
Adhesive regiona EI ratio 7.33 0.006 −0.88 0.509
MI ratio 5.17 <0.001 0.29 0.818
HI ratio −11.46 0.008 0.55 0.858
EI= erythema index; MI= melanin index; HI= hypopigmentation indexa One data parameter was excluded because an image was not available owing to shadingb Coefficients of beta were calculated from the linear mixed model including evaluation time as repeated variables
DO NOT D
UPLICATE
26 ostomy wound management® march 2014 www.o-wm.com
Feature
discoloration changes. Third, this method can analyze the peristomal skin as a two-dimensional image. In dermatol-ogy, reflectance spectrophotometers and tristimulus color-imeters are widely used to measure skin color.22 However, such devices can only measure limited, narrow regions and may not be applicable to the evaluation of peristomal skin because the entire affected area and anatomical location provide other important information for peristomal assess-ment. Image analysis can resolve this limitation by measur-ing an anatomical location or area of peristomal skin.15-17
Color indicators on a patient’s intact skin showed substantial or almost perfect reproducibility. This result indicates the image processing can standardize color cir-cumstances for a patient even at different time points. In the clinical setting, various luminance conditions derived from the patient’s positioning and body shape, the loca-tion of the room or bed, and weather compromised the visual color assessment. Although standardized settings are required to improve the reproducibility of peristomal assessment, not all of them are adjustable in the clinical
setting. Even under such conditions, the method described in this study has the advantage of improved reliability in the phase of color calibration using a standardized color chart, enabling the clinician to longitudinally monitor the skin color change. Results showed the ICC of the EI was relatively lower than those of the MI and HI. This is ex-pected because the errors after color calibration would be greater for red than for other colors.23 Nevertheless, this point may not be problematic, because color indicators in the peristomal region were calculated as relative to intact skin. This additional process can further reduce color in-dicator errors among images.
The study showed peristomal skin color is significantly different from that of intact skin unaffected by adhesives, irrespective of the presence of clinically problematic com-plications. This trend was particularly prominent in the re-gion adjacent to the stoma. This result indicates a pouching system with adhesives more or less affects the peristomal skin color, including erythema and pigmentation.11 Various factors including mechanical stress, chemical irritants, and
Figure 4. A case showing longitudinal change in the peristomal skin condition in an 84-year-old female patient with a lower colostomy. Two months after her stoma construction, she regularly visited the outpatient clinic. The pictures show her peristomal skin condition a) at week 1, b) at week 2, and c) at week 3. The graphs show the changes in the color indicators in d) the region adjacent to the stoma and e) in the adhesive region.
A – Week 1 B – Week2 C – Week 3
ED
DO NOT D
UPLICATE

28 ostomy wound management® march 2014 www.o-wm.com
Feature
ongoing occlusion may lead to altered peristomal skin bar-rier function.24 This alteration can appear as clinically visible discoloration, although it does not necessarily represent a pathological condition. Digital image analysis may be helpful for early detection of such peristomal skin changes. Further studies using this digital image analysis will be required to quantify and understand the objective longitudinal discol-oration changes after stoma construction and the detailed relationships with potential factors. The color change cutoff points to predict clinically problematic skin complications are also important to determine.
The significant correlation between the severity of dis-coloration score and color indicators in this study indicated the image analysis had criterion-related validity for visual color classification. Although visual assessment of peristo-mal skin color is recommended in clinical practice, it only can evaluate the presence or absence of skin complications. Even a DET discoloration score includes only three catego-ries: none, slight, or severe.12 In addition, the strict defini-tion of color, such as “deep red,” is complicated and requires assessment expertise. This new method has the advantage of evaluating skin color quantitatively and continuously. Furthermore, results showed the color indicators in the region adjacent to the stoma had relatively stronger asso-ciations with the discoloration score than with those in the adhesive region. This result is in agreement with clinical ex-perience showing peristomal skin complications, especially moisture-associated skin damage, frequently occur in the region adjacent to stoma at high risk for direct contact with feces or urine.8 In addition, responsiveness to skin color changes was partly confirmed. These results can support the construct validity for color indicators. These color indica-tors enable clinicians to perform accurate and sophisticated assessment of peristomal color conditions.
Color indicators were associated with the degree of pain. In particular, the association between the EI and pain is of importance, because the EI reflects the degree of erythema. It is hypothesized that peristomal pain is strongly associated with erythema because of acute inflammation under condi-tions of irritant dermatitis or infection.7 The results support the criterion-related validity of digital image analysis. The reason why the MI and HI were associated with pain remains unclear, because hyper- and hypopigmentation may develop after acute inflammation has disappeared; a possible expla-nation may be that these observations reflect postinflamma-tory pigmentation secondary to repeated mechanical stress and perceived pain during adhesive changes.
Color indicators did not show an association with the itching score. In fact, studies of factors and assessment meth-ods for peristomal itching are lacking, even though itching is a frequent complaint among people with a stoma.25 Further studies are required to reveal the relationships between peri-stomal skin conditions and itching.
limitationsAlthough the photograph method has clinically ad-
equate validity and reliability, study limitations exist. Selection bias may have been present because the study population was Japanese with a particular skin type that is easily pigmented. Although this population characteristic improved the feasibility of color assessment of peristomal skin in this study, the results should be cautiously inter-preted in terms of whether this method will apply to other populations, especially those with dark skin. The second limitation is the low statistical power due to the small sample size. One reason for this small sample is the differ-ent intervals of visiting outpatient clinics; some patients visited only once during the study period. Another rea-son is the exclusion of several photographs in which the color was difficult to accurately evaluate, such as pictures without the opposite side being visible or those affected by shade. To disseminate this method into broader settings, increased feasibility will be required in the form of easier-to-operate photography systems and supportive settings, such as optimal room illumination. Finally, the color in-dicators were evaluated over peristomal skin by a radial method, whereas the DET score only evaluates the propor-tion of the discolored area irrespective of location.12 An-other popular tool divides the peristomal region into four sites.13 If skin problems exist only in a part of a peristo-mal region but do not cover the entire region, this method may underestimate the severity because color indicators around the peristomal region are averaged. Further study will be required to compare the usefulness of various ana-tomical assessment techniques. Nevertheless, this method has an advantage even with respect to this point, because various indicators, such as area and morphology, can be created from image analysis using color.
ConclusionThis is the first study to apply digital image analysis to
peristomal skin color assessment in the clinical setting. All color indicators, including the EI, MI, and HI, had good to almost perfect reproducibility in terms of the intact skin color. In addition, criterion-related validity was evident in both the region adjacent to the stoma and under the adhe-sive for the clinical discoloration scores and patients’ per-ceived pain scores when color indicators were used in the form of relative values for the intact skin. Responsiveness to color changes over time was partly confirmed.
This novel, objective method can support clinicians in their decision-making when they evaluate peristomal skin complications, select appropriate care options, and moni-tor the effect of care. It also should contribute to improve-ment of the quality of stoma care and the assessment skill of specialized nurses in daily practice. n
DO NOT D
UPLICATE

www.o-wm.com
dIgItal Image analysIs oF PerIstomal sKIn
references1. Woo KY, Sibbald RG, Ayello EA, Coutts PM, Garde DE. Peristomal skin complications
and management. Adv Skin Wound Care. 2009;22(11):522–532.2. Gray M, Colwell JC, Doughty D, Goldberg M, Hoeflok J, Manson A, et al. Peristomal
moisture-associated skin damage in adults with fecal ostomies: a comprehensive re-view and consensus. J Wound Ostomy Continence Nurs. 2013;40(4):389–399.
3. Ratliff CR, Scarano KA, Donovan AM, Colwell JC. Descriptive study of peristomal complications. J Wound Ostomy Continence Nurs. 2005;32(1):33–37.
4. Richbourg L, Thorpe JM, Rapp CG. Difficulties experienced by the ostomate after hospital discharge. J Wound Ostomy Continence Nurs. 2007;34(1):70–79.
5. Kalashnikova I, Achkasov S, Fadeeva S, Vorobiev G. The development and use of algorithms for diagnosing and choosing treatment of ostomy complications: results of a prospective evaluation. Ostomy Wound Manage. 2011;57(1):20–27.
6. Meisner S, Lehur PA, Moran B, Martins L, Jemec GB. Peristomal skin complications are common, expensive, and difficult to manage: a population based cost modeling study. PLoS One. 2012;7(5):e37813.
7. Boland J, Brooks D. Topical application of a beclometasone steroid inhaler for treat-ment of stoma inflammation. Palliat Med. 2012;26(8):1055¬1056.
8. Pittman J, Rawl SM, Schmidt CM, Grant M, Ko CY, Wendel C, et al. Demographic and clinical factors related to ostomy complications and quality of life in veterans with an ostomy. J Wound Ostomy Continence Nurs. 2008;35(5):493–503.
9. Chambers SK, Meng X, Youl P, Aitken J, Dunn J, Baade P. A five-year prospective study of quality of life after colorectal cancer. Qual Life Res. 2012;21(9):1551–1564.
10. Haugen V, Ratliff CR. Tools for assessing peristomal skin complications. J Wound Os-tomy Continence Nurs. 2013;40(2):131–134.
11. Omura Y, Anazawa S. Outcome of peristomal skin management by long-term use of skin barrier. J Wound Ostomy Continence Nurs. 1994;21(6):251–256.
12. Martins L, Ayello EA, Claessens I, Steen Hansen A, Hentze Poulsen L, Sibbald RG, et al. The ostomy skin tool: tracking peristomal skin changes. Br J Nurs. 2010;19(15):932–934.
13. Bosio G, Pisani F, Lucibello L, Fonti A, Scrocca A, Morandell C, et al. A proposal for classifying peristomal skin disorders: results of a multicenter observational study. Os-tomy Wound Manage. 2007;53(9):38–43.
14. Jemec GB, Martins L, Claessens I, Ayello EA, Hansen AS, Poulsen LH, et al. Assessing peristomal skin changes in ostomy patients: validation of the Ostomy Skin Tool. Br J Dermatol. 2011;164(2):330–335.
15. Iizaka S, Sugama J, Nakagami G, Kaitani T, Naito A, Koyanagi H, et al. Concurrent validation and reliability of digital image analysis of granulation tissue color for clinical pressure ulcers. Wound Repair Regen. 2011;19(4):455–463.
16. Yamamoto T, Takiwaki H, Arase S, Ohshima H. Derivation and clinical application of special imaging by means of digital cameras and Image J freeware for quantification of erythema and pigmentation. Skin Res Technol. 2008;14(1):26–34.
17. Setaro M, Sparavigna A. Quantification of erythema using digital camera and computer-based colour image analysis: a multicentre study. Skin Res Technol. 2002;8(2):84–88.
18. Romanelli M. Objective measurement of venous ulcer debridement and granulation with skin colour reflectance analyzer. WOUNDS. 1997;9(4):122–126.
19. Terry M, Halstead LS, O’Hare P, Gaskill C, Ho PS, Obecny J, et al. Feasibility study of home care wound management using telemedicine. Adv Skin Wound Care. 2009;22(8):358–364.
20. Konya C, Mizokami Y, Kamide R. Tokunaga K, Sanada H, Nakagami G. Reliability and accuracy of the Japanese version of the DET score. J Jpn WOCM. 2010;14(3):272–278. (article in Japanese)
21. Landis JR, Koch GG. The measure of observer agreement for categorical data. Bio-metrics. 1977;33(1):159–174
22. Clarys P, Alewaeters K, Lambrecht R, Barel O. Skin color measurements: comparison between three instruments: skin color measurements: comparison between three in-struments: the Chromameter, the DermaSpectrometer, and the Mexameter. Skin Res Technol. 2000;6(4):230–238.
23. Van Poucke S, Haeghen YV, Vissers K, Meert T, Jorens P. Automatic colorimetric cali-bration of human wounds. BMC Med Imaging. 2010;10:7.
24. Nybaek H, Lophagen S, Karlsmark T, Bang Knudsen D, Jemec GB. Stratum corneum integrity as a predictor for peristomal skin problems in ostomates. Br J Dermatol. 2010;162(2):357–361.
25. Charousaei F, Dabirian A, Mojab F. Using chamomile solution or a 1% topical hydro-cortisone ointment in the management of peristomal skin lesions in colostomy pa-tients: results of a controlled clinical study. Ostomy Wound Manage. 2011;57(5):28–36.
DO NOT D
UPLICATE