philosophies of predoctoral care
TRANSCRIPT

1 | P a g e
PHILOSOPHIES OF PREDOCTORAL CARE
Contents PHILOSOPHY ON HEALTH PROMOTION, DISEASE PREVENTION, CARIOLOGY AND OPERATIVE DENTISTRY . 1
PHILOSOPHY ON DENTAL MATERIALS, BIOMATERIALS, and DEVICES .................................................................. 19
TREATMENT PLAN PHILOSOPHY ........................................................................................................................... 21
PHILOSOPHY ON PREDOCTORAL FIXED and REMOVABLE TREATMENT PROCEDURES ........................................ 23
PHILOSPOHY ON DENTAL IMPLANTS ................................................................................................................. 25
PHILOSOPHY ON SINGLE TOOTH IMPLANT........................................................................................................ 33
PHILOSOPHY ON IMMEDIATE COMPLETE DENTURE ............................................................................................ 42
PHILOSOPHY ON ORAL APPLIANCE MANAGEMENT OF OBSTRUCTIVE SLEEP APNEA .......................................... 46
PHILOSOPHY ON MANAGEMENT OF THE PERIODONTIUM IN HEALTH AND DISEASE ......................................... 40
PHILOSOPHY OF ENDODONTIC CARE .................................................................................................................... 50
PHILOSOPHY OF PREDOCTORAL ORAL SURGERY CLINIC ...................................................................................... 53
PHILOSOPHY ON URGENT CARE ............................................................................................................................ 57
PHILOSOPHY ON DENTAL STUDENT TREATMENT OF PEDIATRIC PATIENTS ......................................................... 63
PHILOSOPHY of ORTHODONTIC TREATMENT ....................................................................................................... 73
GUIDELINES FOR CROWN PREPARATION AND CEMENTATION ............................................................................ 76
GUIDELINE FOR ALL CERAMIC CEMENTATION ...................................................................................................... 77
CLINICAL DECISION TOOLS: ANTIBIOTICS .............................................................................................................. 80
CLINICAL DECISION TOOLS: ANTIBIOTICS .............................................................................................................. 81
Dated: 4/15/2021

2 | P a g e
PHILOSOPHY ON HEALTH PROMOTION, DISEASE PREVENTION, CARIOLOGY AND OPERATIVE DENTISTRY
DEPARTMENT OF RESTORATIVE DENTISTRY
1. Risk assessment, evaluation of disease activity, and treating disease (caries) in UIC clinics.
All patients must be evaluated to determine risk for disease, including caries, periodontal disease, and oral cancer. It is important to shift the focus from repairing teeth to enhancing health.
Results of patient risk assessments must be documented in the electronic patient record using the following codes:
D0601—Caries Risk Assessment & Documentation, finding of low risk D0602—Caries Risk Assessment & Documentation, finding of moderate risk D0603—Caries Risk Assessment & Documentation, finding of high risk
The caries action plan (in Axium) must be approved and presented to the patient in attempt to improve home compliance. The dental record must confirm that these measures have been implemented. There must be periodic re-assessments to document the effects of the proposed interventions.
Treatment plans must include proposals to alter modifiable risk factors, reduce or eliminate potential pathological factors and add or enhance preventive or protective factors.
All clinicians must include the full array of caries treatment options in patient care. This includes topical use of fluoride and chlorhexidine pastes, varnishes and rinses. Products such as MI paste (GC America) that contain supplemental calcium and phosphate and various Xylitol chewing gums or mints may be prescribed for medium- high risk patients.
D9630.1-Prevident 5000 Booster Plus D9630.2-PerioGuard D9630.3-Prevident 5000 Dry Mouth D9630.4-MI Paste D9630.5 -Extreme Risk Bundle (PerioGuard, Prevident 5000 Dry Mouth, MI Paste)
2. Caries Diagnosis: Diagnosis of dental caries includes: review of the patient medical history, risk assessment and carious lesion detection.
• Detection of carious lesions: Detection relies on an assessment of clinical and radiographic findings supported by faculty experience and judgment.
• Detection methods: Visual/Tactile: teeth must be dried and plaque must be removed with the explorer
or by prophylaxis to visualize possible lesions at their earliest stage of development. Magnification is helpful during the visual examination.
Radiographs: Each patient must have current radiographs that are obtained or updated after the clinical examination. Radiographic sensitivity and specificity varies according to the location and the lesion progression.

3 | P a g e
• Advanced technology such as laser fluorescence or fiber optic trans-illumination may be used, if available, with an awareness of the demonstrated limitations in specificity. False positives are common (detection of lesions that are not actually present).

4 | P a g e
Attempting to use a sharp explorer to determine if it will “stick” in a pit or fissure must be discouraged, as it may cause iatrogenic damage to the enamel surface and progression of caries. The use of a sharp explorer to detect primary occlusal caries adds little information in the caries diagnosis process.
An explorer “catch” or staining of a pit or fissure cannot be interpreted alone as a reliable indication that active disease is present. A stained or discolored pit or fissure without visible cavitation should not be classified as carious unless there are other signs of disease present.
Charting carious lesions
An examination using the 2015 ADA Caries Classification System (CCS) is conducted on clean air-dried teeth, using good lighting, and a rounded explorer or ball-end probe. Radiographs should also be available during the examination process. The ADA CCS includes both non-cavitated and cavitated lesions. When charting carious lesions in Axium:
• In low risk patients, lesions without enamel breakdown should be charted as “non-
cavitated” and may receive treatment to promote remineralization. • An assessment of the disease activity, (active, inactive, arrested) must be made for all lesions.

5 | P a g e
Diagnostic criteria and guidelines for treatment decision
Diagnostic criteria Suggested intervention Cavitation / active caries ADA Advanced caries (D3
lesion) ADA Moderate caries
(D2 lesion)
Operative intervention/ 38% SDF solution
No cavitation / inactive ADA Initial caries (E1, E2, D1 lesion)
No restorative intervention (see flowchart.) Continue periodic evaluations and preventive therapy
No cavitation / active ADA Initial caries (E1, E2, D1 lesion)
No restorative intervention. (see flowchart.) Prescribe antimicrobials, attempt remineralization – based on determination of caries risk. For “high risk patients”, early surgical intervention might be indicated.
3. Caries management / treatment of disease
• The cause of the disease (etiology) must be evaluated and treated. Repairing defects
caused by disease without implementing measures to treat the disease is NOT an acceptable practice.
• Proper patient care and material selection is based on the individual risk assessment. • Emphasis must be placed on altering the caries balance between protective and
pathological factors to favor health and to prevent future disease.
Non-restorative management of non-cavitated and cavitated carious lesions of permanent teeth (Adapted from JADA, October 2018 recommendations guidelines).

6 | P a g e
*:Application every 3-6 months ** Biannual application. Informed consent must be provided to the patient regarding side effects (blackened
surfaces) ++ Resin infiltration as a non-invasive treatment option for non cavitated lesions may be added as an accepted
procedure once significant evidence exists to support it at our UG clinics. Evidence is under ongoing review.
Non cavitated Cavitated Non cavitated
5% NaF
Varnish*
38% SDF
solution**
Facial/ Lingual
Interproximal
5% NaF varnish*
Resin
38% SDF
solution**
Cavitated Cavitated Non cavitated
Occlusal
Coronal Caries
38% SDF
solution**
Sealants/5%
Na F Varnish*

12 | P a g e
5% NaF Varnish* 38% SDF solution
Root Caries
Noncavitated/ Cavitated
1.1 % NaF 5000 PPM fluoride***
*** At home application once a day.
Lesions should be monitored periodically for hardness, texture and color throughout the course of treatment.
OPERATIVE DENTISTRY –
General Considerations:
The goal to preserve healthy tooth structure influences the selection of material for restorative interventions. There is not a restorative material that is a reliable substitute for healthy enamel or dentin. A primary goal for restorative dentistry is to minimize removal of healthy/sound tissue.
Management of Anterior Teeth: The materials of choice for anterior direct restorations are resin composite and resin-modified glass ionomers. The latter is primarily indicated for cervical and root surface lesions
Management of Posterior Teeth: The restorative management of teeth affected by carious lesions is based on location and extent of disease progression. For primary and secondary carious lesions limited to occlusal surfaces, resin composite is the first choice for restorative material.
For Interproximal primary and secondary lesions, resin composite and amalgam are suitable material choices. Material selection should be based on: the tooth location (premolar, molar), extent of the lesion, ability to control contamination and moisture, patient risk and predicted patient compliance.
General Guidelines:
• Occlusion must always be evaluated prior to beginning restorative treatment. Marking the occlusal contacts with articulating film prior to beginning a preparation allows evaluation of existing

13 | P a g e
centric stops and anticipation of potential occlusal problems. Occlusion may also be evaluated using the patient’s articulated diagnostic casts, when casts have been fabricated.
• Use rubber dam isolation for operative dentistry procedures. Rubber dam isolation must be used unless the supervising instructor determines that it is not indicated. It is well documented that current bonding systems cannot produce clinically acceptable results when isolation is lacking. Rubber dam isolation techniques are still a critical part of most licensure examinations and students need to master proper techniques. Rubber dam isolation helps prevent contamination of the operating area and is an essential aid for protection of the practitioner as well as the patient. In restoration of posterior teeth, isolate at least one tooth posterior to the tooth to be restored and extend the rubber dam to the midline or to the opposite canine. For anterior restorations, isolate the entire anterior portion from first bicuspid to first bicuspid. When conditions permit, other than for gingival retraction for cervical lesions, do not place a retainer on the tooth to be restored. Single tooth isolation is not often used for restorative dental procedures.
• Conserve tooth structure. Keep preparations as narrow as the caries progression or defect will allow. Do not extend preparations into occlusal grooves unless the grooves are carious. If extension through non-carious grooves is indicated, use a conservative approach, making the extension as narrow as possible using burs such as #1/2 or #1/4 round, #329 MWV burs and #1169.
• Seal the dentin beneath restorations.
4. Clinical Guidelines for placement of tooth-colored direct
restorations Pit & Fissure Sealants (Procedure code is 01351.)
• There are good indications for sealant use in adult patients. • The use of sealants as minimally invasive treatment for active, non-cavitated carious lesions is
supported by strong evidence and is, therefore, a reasonable approach when patient caries risk is low.
• Sealant use depends on detection of dental defects (pits or fissures) and determination of patient’s risk
• Rubber dam isolation is strongly recommended • Following proper etching, use of a system containing an adhesive and a primer is
thought to be advantageous prior to sealant application.
Preventive Resin Restorations (Procedure code is 02385.)
Minimally invasive restorative procedures should be employed when tooth preparation is indicated, as opposed to attempting remineralization.
• Rubber dam isolation is critical. • Preparations are made by conservatively extending through the enamel, with a 1/4 or 1/2
round bur, to access the carious lesion. Carious dentin is removed without consideration for the retention and resistance form that would be necessary for placement of amalgam restorations.
• Preparations do not need to resemble preparations that would be made for amalgam restorations. Preparations require adequate access for removal of diseased tooth structure while focusing on preservation of healthy tooth structure.
• The enamel margins are not beveled.

14 | P a g e
• After removal of carious tooth structure, the remaining affected pits and fissures are etched, rinsed and dried, and the tooth is then restored with a combination of resin composite and flowable composite or resin sealant material.
Resin composite restoration procedures
• Clean the teeth to be restored and those adjacent using a slurry of pumice. Flour of pumice (Preppies, Whip-Mix) mixed with water should be used rather than commercial prophy pastes.
• Select an appropriate shade prior to rubber dam isolation
• Use rubber dam isolation. Any saliva contamination will result in a significantly compromised prognosis for an adhesive restoration. Do not desiccate the prepared tooth. Dentin bonding is enhanced when current generation bonding agents are applied to “moist dentin”. Dentin can be re-moistened with water or a cavity cleaning agent such as 2% chlorhexidine gluconate.
• Minimally invasive preparations are advocated. For restorations with all margins in enamel, internal retentive features are less critical. Non-carious dentin must be conserved when possible. For restorations which extend onto root surfaces, the bond to enamel and dentin should be augmented by mechanical retentive features. Preparations for resin composite involve conservation of tooth structure and removal of decay, they do not need to resemble amalgam preparations.
• Most restorations require incremental build-up of material to minimize the adverse affects from polymerization shrinkage. Shallow cervical lesions may be restored by placing resin-composite material in a single increment.
Direct Posterior resin composite restorations
Treatment Guidelines 1. The primary indications for use of resin composite for direct posterior
restorations are to achieve a more esthetic result and to conserve healthy tooth structure
2. The tooth to be restored MUST be isolated by placement of a rubber dam 3. The faciolingual width of the cavity preparation should be restricted to no greater
than two thirds of the intercuspal dimension. 4. Gingival cavosurface margins MUST be located on intact enamel 5. Cuspal replacement with resin composite is NOT appropriate 6. Centric occlusal stops should be on enamel 7. The patient should not exhibit excessive wear from clenching or bruxing. 8. Resin materials must never be used for patients who report allergy to the material 9. Resin composite should not be used to restore portions of teeth that will incorporate
occlusal rests for removable partial dentures
• Limit the extent of the preparation to eliminate diseased tooth structure, barely break interproximal contact when indicated. Generally cavosurface bevels are not placed on the occlusal enamel margins. Other cavosurface margins may be beveled slightly past 90 degrees if they are on enamel. Do not bevel gingival margins if they end on dentin or cementum.

15 | P a g e
• A ring system such as the Garrison ComposiTight and sectional matrix can be used to achieve a proper proximal contact more easily. An alternative to the sectional matrix system is the use of universal “dead soft” matrix bands in the Tofflemire retainer. Mylar strips are not acceptable as the matrix for posterior resin composite restorations.
5. Contemporary enamel/dentin bonding system and clinical recommendations for Pre-doctoralclinics
• To obtain clinically acceptable bonded restorations, the clinician must consider thelimitations of the material, provide a contamination-free environment for its use and manipulate the material appropriately.
• The dentin must remain moist, though not excessively moist, while the primers are applied. Formation of a hybrid layer, resin-impregnated collagen layer, is vital for effective dentin bonding.
• The technique for removal of the smear layer, conditioning and priming of dentin varies, depending on the bonding concept designed for each specific material.
Sequence for total etch technique using ScotchBond Universal Adhesive System (3M ESPE).
1. Apply phosphoric acid etchant for 15-20 seconds
2. Rinse thoroughly for 20 seconds
3. Remove excess moisture while keeping the surface wet
4. Apply 1-2 consecutive coats of the adhesive and rub it in for 20 seconds
5. Remove excess solvent by drying the surface gently for at least 5 seconds
6. Light-cure for 20 seconds
7. Place resin composite restorative material incrementally
The Department of Restorative Dentistry advocates a total-etch technique using a phosphoric acid gel etchant when using this system, even though it is marketed as and may be used as a self-etching system.
6. Clinical Guidelines for placement of Silver Amalgam Restorations
• Use rubber dam isolation. When interproximal lesions are to be restored, place wooden wedges immediately after application of the rubber dam. This helps to retract the rubber dam and the underlying gingiva. Pre- contoured wedges are recommended.
• Use minimally invasive restorative procedures when possible. Extension to non-carious fissures for anticipated prevention of caries is not indicated. “Slot preparations” may be used when there is no occlusal involvement – but generally when this is appropriate, the restorative material of choice would be resin composite rather than amalgam. Internal line angles must generally be slightly rounded. Discolored dentin near the pulp that cannot be removed with a sharp spoon excavator should be retained. Any discolored dentin located at the dentin-enamel junction should be removed. An enamel hatchet or a gingival margin trimmer may be used to remove unsupported enamel rods at the gingival cavosurface margin of a Class II preparation. The UIC COD recommended bur for conservative amalgam preparations is the Brasseler #329 MWV.

16 | P a g e
• The recommended dentin sealer beneath amalgam restorations is GLUMA
• Burnishing amalgam is merely lightly rubbing and smoothing the surface, forceful burnishing, such as is done for gold, must be avoided, since this merely draws mercury to the surface and weakens the restoration. Newly placed amalgam restorations should not be burnished to produce a shiny appearance.
Repair of Resin Composite and Amalgam Restorations Indication: Secondary caries, fractures and wear of existing restorations lead to the need to make decisions regarding repair or replacement. Replacement of restorations sacrifices sound tooth structure, reduces the likelihood of continued pulp vitality and increases the complexity and the risk of failure of dental restorations. Repair increases the longevity of restorations and has high patient acceptance. Repair of restoration is indicated for localized secondary caries and fracture; while replacement is best considered when generalized or severe defects are present. Technical Considerations:
• Repair of marginal defects involves careful opening and cleaning to assess undermining disease and to smooth surfaces.
• The restorative protocol includes surface etching, use of a bonding system and restoring with a flowable composite (small marginal repair) or bulk resin composite (major repair).
• Repair of amalgam restorations requires placement of retentive grooves or coves and condensing freshly triturated amalgam.
7. Clinical Guidelines for Pulpal Protection
• A cavity sealer, such as Gluma, should be placed under an amalgam restoration. • A cavity liner is indicated for tooth preparations when the remaining dentin thickness is
insufficient to prevent pulpal irritation from the presence of bacteria or bacterial byproducts.
• An indirect pulp cap may be completed using calcium hydroxide or MTA only in asymptomatic teeth in the area closest to the pulp.
• Although success rates exceeding 90% are reported for direct pulp caps for vital pulps following small mechanical exposures, success drops dramatically when pulp capping of carious exposures is attempted.
• In deep carious lesions with no symptoms or signs of reversible pulpitis, selective removal of affected dentin (partial caries excavation) is recommended. Manual and rotary instrumentation such as spoon excavators and low speed handpieces with large round burs are recommended for the removal of the outer layer of softened carious dentin. The final restoration should be placed during the same appointment.
• Indirect or direct pulp capping is discouraged when an indirect restoration is planned. • Bases are only indicated for indirect restorations to block undercuts or to achieve ideal
thickness for the planned restoration.

17 | P a g e
Steps for pulp protection beneath amalgam restorations:
Ideal preparations • Complete cavity preparation under rubber dam isolation • Apply one coat of Gluma using a gentle rubbing motion • Wait for 30 sec. Rinse then gently air dry • Place the amalgam restoration
Deeper preparations (close to pulp)
• Complete cavity preparation under rubber dam isolation • In an area of dentin transparency, apply a thin layer of calcium hydroxide or MTA. • Cover the Ca(OH)2 with a thin layer of Fuji lining LC / Vitrebond. Light cure for 20 seconds. • Apply one coat of Gluma using a gentle rubbing motion on the entire cavity preparation • Wait for 30 sec. Rinse then gently air dry • Place the amalgam restoration
Steps for pulp protection beneath resin composite restorations: Ideal preparations
• Complete cavity preparation under rubber dam isolation • Follow the total etch technique and sequence for bonding with 3M Scotchbond Universal • Place resin composite restoration
Deeper preparation (close to pulp)
• Complete cavity preparation under rubber dam isolation • In an area of dentin translucency, apply a thin layer of Ca(OH)2
• Cover the Ca(OH)2 with a thin layer Fuji lining LC / Vitrebond. Light cure for 20 sec. • Follow the total etch technique and sequence for bonding with 3M Scotchbond Universal • Place the resin composite restoration.
If Gluma is used as a desensitizer under adhesive restorations, apply the Gluma after removal of the smear layer and prior to application of bonding agent.
Steps for pulp protection beneath indirect restorations: • A base of RMGI (Fuji lining LC) is indicated to block preparation undercuts and ‘base back toideal” • In the case of a deep preparation or pulpal proximity, the protocol for deep
preparation under amalgam should be followed.
RESTORATION OF CERVICAL LESIONS:
A determination of lesion etiology is necessary to properly design a cavity preparation for a cervical defect. The etiology might be carious involvement, abrasion, or abfraction (stress induced cervical lesions).
For carious defects the decay is excavated and enamel margins are beveled to improve marginal seal and esthetic finishing of the restoration. Abrasion is generally restored without cavity preparation and relies on proper cleaning and conditioning of the tooth surface to enhance potential bonding. Areas of sclerotic dentin should be lightly abraded with a fine diamond bur. Abfractions require addition of mechanical retention within the preparation (a gingival groove at the axiogingival line angle and

18 | P a g e
occlusoaxial or incisoaxial grooves or retentive coves) for more predictable retention of resin composite restorations.
Materials with greater flexibility such as microfilled resins (UIC: Renamel Microfill) are the best choice for restoration of lesions where tooth flexure is considered to be a part of the etiology (abfraction). Opaquers can be used to reduce the translucency of restorations that are placed on exposed root surfaces
For patients with high caries risk an open sandwich technique can be used. A glass ionomer or resin-modified glass ionomer material is used as the first increment with the fluoride releasing material extending to the cavosurface margins. A resin composite is veneered on the surface for enhanced finishing and translucency.
Technique suggestions to minimize post-operative sensitivity with placement of all direct posterior resin composite restorations:
• Use GLUMA to seal dentinal tubules • Use a resin modified glass ionomer liner such as Vitrebond Plus or Fuji II Lining LC on pulpal or
axial walls of deeper preparations • Use an incremental build-up to reduce stress from polymerization shrinkage
UIC College of Dentistry required textbooks: Operative Dentistry and Cariology
Sturdevant CM, Roberson TM, Heymann HO, & Sturdevant JR. The Art and Science of Operative Dentistry. 7th Edition. Mosby.
Rosensteil SF, Land MF, and Fujimoto J. Contemporary Fixed Prosthodontics. 5th Edition. Mosby.
Craig RG and Powers JM Restorative Dental Materials 14th
Edition. Mosby.
Slayton et al, ADA Evidence based clinical practice guidelines on nonrestoartive treatments or carious lesions. October 2018

19 | P a g e
PHILOSOPHY ON DENTAL MATERIALS, BIOMATERIALS, and DEVICES
Department of Restorative Dentistry The selection of preventive and restorative dental materials, biomaterials and devices supports the
current departmental preventive and restorative philosophies outlined in other sections of the
philosophy document. Dental materials, biomaterials and instruments used in the UIC pre-doctoral DMD/DMDAS programs
are selected by considering the best available evidence related to long-term working performance of
various materials when used properly after training, comparing cost of acceptable materials available
from the various manufacturers, considering handling characteristics and infection controls needs
within a learning environment (i.e. unit dose packaging) to provide materials that can be manipulated
successfully by beginning practitioners. The Dental Materials Advisory Committee reports to the Restorative Department Chair and Dean for
Clinic Affairs periodically as the list of approved dental materials and instruments is reviewed and
updated. The committee is composed of 8-12 members, including representative of all aspects of
preventive and restorative dentistry, including course directors, managing partners, and faculty. Only
those dental materials and devices that have been approved by the Dental Materials Advisory
Committee may be used in dental clinics and in pre-patient care instructional sessions. A list that incorporates all approved restorative materials accepted for use in pre-patient care
instruction and in clinics can be found in the intranet: https://dentistry.uic.edu/dental-equipment-
materials. A hard copy can be provided upon request in the department or clinical affairs office.
A list of approved devices (instruments and burs) accepted for use in pre-patient care instruction and
in clinics can be found in the intranet: https://dentistry.uic.edu/dental-equipment-materials. A hard
copy can be provided upon request in the department or clinical affairs office.

20 | P a g e
There should NOT be substitutions with generic alternatives unless approved by the advisory
committee/administration.
Dental materials from outside sources that have not been approved and included in the dental
materials lists may not be used in UIC pre-doctoral DMD/DMDAS programs.
A mechanism is in place for consideration of additional materials or instruments that are not
currently available, utilizing a request form found in the intranet:
https://dentistry.uic.edu/dental- equipment-material. A hard copy is also available in the clinics.
In addition, issues that develop in practice related to the currently accepted materials can also
be reported to the advisory committee using the same form. The form allows a mechanism for
feedback to the clinical or pre- patient care faculty regarding their concerns and suggestions in
some specific circumstances.
21 | P a g e
TREATMENT PLAN PHILOSOPHY UIC COD follows an evidence-based, comprehensive care model. Multiple comprehensive treatment plans should be offered to accommodate multiple patient modifiers. All treatment is phased and re-evaluations after each phase are performed. Upon completion of a comprehensive care, a Phase III re-evaluation is performed and the patient is placed on an appropriate recall schedule. For comprehensive care patients, regardless of the extent of the treatment, there must be a treatment plan in the electronic health record, which includes the planned treatment procedures, associated fees, and sequence of care. College policy requires that the individual providing oral health services discuss with the patient the possible benefits, outcomes, risk, and side-effects of the proposed treatment and any alternative treatment. The patient must have an opportunity to review and have questions answered regarding the proposed treatment. Written informed consent (signed treatment plan) is required for treatment rendered in the context of urgent care, comprehensive, and limited care. Steps to be completed prior to Treatment planning:
1) All patients must have a complete EPR including: medical history form, dental history form, risk factors, odontogram, etc.
2) Students should have a restorative and periodontal COE completed prior to developing a treatment plan.
3) When phase III restorative procedures are indicated, diagnostic cast must be articulated on a semi-adjustable articulator using a facebow and appropriate interocclusal record.
4) Diagnostic casts for potential RPD should be articulated, surveyed, and a preliminary design drawn.
5) Diagnostic wax-up needs to be completed when applicable. 6) All appropriate consultations must be completed prior to finalizing the treatment plan, including
implant, digital, endodontic, and oral surgery consultations. 7) When pre-prosthetic surgery is indicated, a preprosthetic surgery form must be completed and
approved by the restorative and surgical faculty. 8) Students should be able to formulate a problem list, findings, and diagnoses
and present it to the faculty. 9) Current ADA caries classifications should be used. 10) All patients must be evaluated to determine risk for disease, including caries, periodontal
disease, and oral cancer. Treatment planning
1) All treatment plans must include a caries action plan based on the patient risk, with
proposals to alter modifiable risk factors, reduce or eliminate potential pathological factors and add or enhance preventive or protective factors.
2) Treatment plans should ideally include an “Optimal” and an “Alternative” option.
3) Treatment Plans should be developed following appropriate phasing and sequencing

22 | P a g e
(Stefanac et al). a. Phase 1 – Disease Control b. Phase 2 – Surgical/Orthoodontic/Endodontics c. Phase 3 - Restorative d. Phase 4 – Maintenance e. At the end of each phase, a phase I, II, or III re-evaluation is completed. f. All patients with scaling and root planing require a periodontal re- evaluation
(D0170) 6-8 weeks after completion of periodontal care.
4) Treatment plans should be discussed and approved by a restorative faculty (COE) in the GP clinic prior to scheduling patient for treatment plan presentation.
5) Patients must be recalled at their proper recall interval based on risk and prognosis. All
dentate patients will be recalled at a minimum of a 6 month interval. For edentulous patients, a minimum of a 1 year recall is recommended.
6) All care must be provided in a timely fashion to avoid any adverse outcomes.

23 | P a g e
PHILOSOPHY ON PREDOCTORAL FIXED and REMOVABLE TREATMENT PROCEDURES
DEPARTMENT OF RESTORATIVE DENTISTRY
Due to time constraints in the curriculum, the need to focus on teaching fundamental restorative principles, as well as the basic level of student understanding and their ability at this stage of clinical training, it is necessary to limit complicated and extensive restorative treatment at the predoctoral level. Students must also be able to recognize the level of their diagnostic and treatment capabilities, and the indications for patient referral. The Prosthodontic Diagnostic Index (PDI) assessment must be completed for all partially and completely edentulous patients. The following guidelines must be adhered to at the predoctoral level:
1. Only materials identified by the Department of Restorative Dentistry (Dental Materials
Committee) and dispensed by the College of Dentistry may be used in the preclinical courses and clinics. Students or faculty must not use personal supplies and materials for patient care.
The following treatment procedures may not be initiated at the predoctoral level:
2. Posterior Resin Composite restorations must not be used unless adequate isolation can be obtained by placement of a rubber dam. In addition, Posterior Resin Composite restorations must not be used for: a. Restorations that are greater than two-thirds of the intercuspal dimension. b. Cuspal replacement. c. Centric occlusal stops. d. Restoration of occlusal rest areas for a removable partial denture.
3. Treatment involving any change in the patients presenting occlusal vertical dimension. The
only exception are patients with at least one completely edentulous arch.
4. Overlay removable partial dentures for the purpose of altering the occlusal vertical dimension.
5. Fixed prosthodontic rehabilitation involving bilateral posterior reconstruction where the
stability of posterior occlusion may be interrupted. At least one posterior occlusal vertical stop must be maintained as part of any fixed care.
6. All PDI type IV and many PDI type III partially and completely edentulous patients.
7. Fixed partial denture treatment involving more than 4 connected units.
8. Anterior esthetic rehabilitation involving more than 4 adjacent units. This can be
increased to 6units with Managing Partner and prosthodontic consultant approval.
9. No more than a total of 6 units of Fixed Prosthodontic care can be treatment planned for a patient, including all single and FPD units. Exceptions to this may be considered up to a maximum of 8 units. However, the prosthodontic consultant and Managing Partner must

24 | P a g e
review and approve the exception (8 units of fixed prosthodontic care) in Axium. 10. A cantilevered FPD may be indicated for replacing a maxillary or mandibular lateral
incisor. They may also be considered for a maxillary or mandibular premolar when opposed by a removable prosthesis. When a premolar cantilever FPD is utilized it must include double abutments. Lateral incisor cantilevers can use canines as single abutment.
All patients that a cantilever FPD is being considered for must have an implant consultation prior to completion of the treatment plan and the initiation of any care involving the area under consideration.
11. Semi-precision or precision attachments for fixed or removable prostheses. This does
not preclude implant or root supported attachments such as Locators and Ball attachments used with full overdentures.
There are no exceptions to the above guidelines, unless approved in writing by one of the Managing Partners in Axium. These treatment limitations should not interfere with student learning through discussions of diagnosis and treatment planning options that may include the above. If the patient needs any of the above therapies during the treatment planning process, s/he should be referred to the prosthodontic specialty program or to the faculty dental practice for evaluation.
Other items to consider:
1. Resin Bonded FPD guidelines: There must be adequate enamel and sound tooth structure for preparation and etching. The occlusal clearance and preparation must allow adequate interocclusal space. Single tooth replacement only. Patients with Class III and/or reverse articulation (crossbites) must not be treated with resin bonded FPD’s. Resin bonded bridges have a much higher success rate and longevity when they are only bonded with one wing.
2. Valplast or Cu-Sil type of RPD as a treatment alternative must be reviewed and
approved with the Managing Partner and a patient consent form must be signed.
3. No unilateral Removable Partial Dentures of any type.

25 | P a g e
PHILOSPOHY ON DENTAL IMPLANTS
Department of Restorative Dentistry
Assessment, Consultation, Diagnosis and Treatment Planning Completed Patient Record
Before considering implant therapy for a patient, the entire Axium Electronic Health Record (EHR) must be completed. This includes (but is not limited to) the medical history, odontogram, periodontal charting, treatment planning module and radiographic records.
Diagnostic Assessment
A diagnostic assessment must be completed for all patients considering implant-supported prostheses. The assessment checklists in Axium must be completed prior to obtaining a Restorative consultation. Acceptable diagnostic wax-up for STI and clinically acceptable complete dentures must be present. Acceptable patients must meet all of the diagnostic criteria.
Health History
1) The health history must be updated and reviewed.
2) ASA Classification - Patients must be within ASA Class I, II, or III.
3) There should be no significant pre-existing medical condition(s) that will exclude patients from consideration for clinical implant care.
4) Psychosocial considerations – There should be no significant psychosocial issue(s) that
would contraindicate care. Radiographic and Clinical Assessment
Radiographic Evaluation
The following recommendations for radiographic evaluation are based on the American College of Prosthodontics position paper, Diagnostic Imaging in the Treatment Planning, Surgical, and Prosthodontic Aspects of Implant Dentistry.
1) Conventional panoramic and/or intraoral periapical imaging is recommended for initial
diagnostic evaluation. CBCT is not recommended for routine initial examination.

26 | P a g e
2) If the clinical examination and conventional radiography have failed to adequately demonstrate relevant anatomical boundaries or important anatomical structures, cross sectional imaging is advised. Cross-sectional imaging (CBCT is preferable over CT due to its significantly lower radiation dose) is recommended for preoperative implant assessment.
3) The rationale for CBCT imaging must be justified based on clinical evaluation.
4) CBCT imaging should be used for the esthetic zone, pre- and post-bone grafting or sinus
augmentation 5) The region of interest (ROI) should be imaged using a minimal field of view (FOV)
6) CBCT is recommended for the evaluation of any suspected postoperative complications Note:
All CBCT scans should include a professional CBCT review and report per Axium form following COD CBCT workflow.
Clinical Evaluation: 1) Indications – Inclusion and exclusion criteria on the checklist must be followed.
Exceptions will be made pending the approval of the Predoctoral Implant Director. 2) Adequate ridge width (both mesial-distal, buccal lingual) must be present clinically 3-4
mm below the crest of the ridge. No significant buccal or lingual concavities may be present.
3) Adequate restorative (interocclusal) space must be present to allow esthetically pleasing and
mechanically sound restoration delivery. No loss of occlusal vertical dimension may be present. 4) Lip Line – No anterior restorations may be considered for patients with high lip lines
displaying the gingival tissues prominently. 5) Occlusion – Patient must present a manageable occlusal scheme displays an even/regular
occlusal plane, and a stable maximum intercuspation. Any supra-eruption of the opposing dentition into the edentulous site must be corrected as part of any treatment plan involving implant supported care.
6) Soft Tissue – Adequate attached tissues must be present. If inadequate tissue is present but can
be corrected, an additional fee will be charged for any corrective soft tissue procedure. 7) Surgical Intervention - Surgical revision of the implant site may be indicated other than the
planned implant placement (e.g., hard tissue augmentation, soft tissue revisions, insufficient interarch space, etc). If the surgical revision is minor and can be accomplished on the same day as the implant surgery, the patient is acceptable for treatment at the Predoctoral level. However, if major surgical intervention is required, (e.g., block grafts, major sinus lifts, etc.) the patient will not be considered for implant placement in the Predoctoral program. The final

27 | P a g e
decision of patient acceptability will be made by the Predoctoral Implant Director. 8) Immediate Placement – Immediate implant placement may be considered in cases where the
prosthodontic and surgical consultants feel it is the best treatment option. These patients must have ideal bone levels, with minimal bone or tissue grafting requirements. There will be no immediate loading of dental implants in the Predoctoral Implant Program. No sign of pathology may be present.
9) Implant Placement – Implants will be placed at the buccal-lingual center of a line drawn
through the centers of the adjacent teeth. In all cases – the implant fixtures will be placed so the resting platform is level with the existing crest of bone, and at least 2mm apical to adjacent CEJ for STIs.
10) Immediate Loading-There will be no immediate loading at the predoctoral level. If a
patient is a candidate for this approach, they must be referred to post-graduate prosthodontics for completion of treatment.
Treatment Planning The treatment plan is developed by the student and approved by the primary restorative instructor in the group practice clinic. The student must present the signed checklist to the restorative instructor before the final implant portion of the treatment plan is approved. The treatment plan must be signed by the patient before initiating of any implant-related procedures.
Surgical Assignment and scheduling
Surgical phase will follow after the completion of phase I and II comprehensive treatment. The approved patient will be assigned to the designated surgical provider according to the UIC COD Restorative Department protocol by the Predoctoral Implant Director.
Once the implant surgery is scheduled, the student must obtain the selected implants and associated parts from the designated staff in predoctoral implant clinic at least TWO WEEKS prior to the surgery. If this protocol is not followed, implants and associated parts may not be available for the appointment.
An appointment for the implant surgery is scheduled with the patient and the surgical resident. THE STUDENT MUST ATTEND THE IMPLANT SURGERY WITHOUT EXCEPTION.
Surgical Guide
A Radiographic/Surgical Guide must be fabricated in the Predoctoral Implant Clinic by completing a diagnostic wax-up and duplicating it with clear acrylic resin. The guide will generally cover at least 6 teeth, 3 teeth on either side if possible. A surgical guide must be used during the surgical

28 | P a g e
placement.
Surgical Protocols Patient Approval and Informed Consent must be obtained prior to surgical therapy. All potential complications must be explained to the patient in detail. Implant Type and Location
Implants will be endosseous root form implants. The implants used can be any of the following: 1) Dentsply EV 3.6mm, 4.2mm or 5.0mm in diameter, and at least 8 mm in length or 2) Straumann SLA Active 3.3mm (NC), 4.1mm (RC) or 4.8mm (RC) in diameter and at least 8 mm in length.
Medication
1) Antibiotic therapy is indicated for implant placement procedures. Patients will be pre-
medicated 1-hour before the surgery using established AHA guidelines. Post insertion antibiotics will be utilized when appropriate based on patient’s medical history etc.
2) Pain Medication - Patients may be provided an appropriate medication for pain
management as needed. 3) Anti-inflammatory Medication - Non-steroidal anti-inflammatory (Motrin) will be
prescribed for short term use up to 7 days post-operatively, unless the patient is non- tolerant of such medication.
4) Plaque Control/Oral Hygiene- Peridex rinses or an equivalent will be prescribed for a
period of one week post surgery to aid in plaque control. Peridex should not be used for the initial 2 days after surgery.
Implant Surgery
Immediate placement is to be considered at the time of the initial implant consultation when a tooth is still present at the future implant site. In cases that the site is potentially candidate for an immediate placement, a diagnostic CBCT must be taken PRIOR to surgical consult. Extra attention should be given to any presence of infection and its extent, need for extensive grafting in cases of type 2 or 3 sockets, esthetic demands etc. If site deemed appropriate for potential immediate placement, ALL PHASE 2 TREATMENT SHOULD HAVE BEEN COMPLETED PRIOR TO IMPLANT PLACEMENT. If immediate implant is placed, no interim prosthesis should be connected (immediate provisionalization) or interim removable prosthesis should be used at the site.

29 | P a g e
1) A one or two-stage protocol will be used for the implants placed.
o For the one-stage protocol, after implant placement and1) if primary stability achieved is adequate, 2) no grafting at the time pf placement was done and 3) there is no need for any type of removable interim prosthesis (Essix, interim RPD) - to avoid any occlusal loading at the site- an appropriate healing abutment will be connected to the implant. After 3 months of healing, the implant level impression will be taken.
o For the two-stage protocol, placement of the implant fixture and primary wound closure will be followed by a healing period of at least 3 months. A second stage surgery is then used to uncover and gain access to the implant fixture.
The day of the implant placement:
1. Vital signs will be taken including blood pressure and pulse 2. Local anesthesia as indicated 3. A midcrestal incision should be made dividing the remaining keratinized tissue. The length of
the incision should facilitate flap reflection that will allow adequate visualization of anatomic structures and possible undercuts.
4. Once exposed, the bone should measure a minimum of 6 mm Facio-lingually at the coronal aspect. Apically, the F-L bone thickness should allow for at least 1mm of bone on either side of the implant.
5. The placement of the implant will be facilitated and verified by scoring the crestal bone with a round bur. The surgical guide will be used to verify this location.
6. Utilizing the surgical guide - A pilot hole will be drilled per the existing drill sequence. The appropriate drill sequence will then be followed as indicated by the implant system used.
7. The implant fixture will be placed using the manufacturer protocol. Care must be taken to avoid any contact with the implant surface. In general, the top of the implant fixture will be placed at the level of the osseous crest.
8. An appropriate cover screw or healing abutment will be placed followed by wound closure with sutures.
9. Any pre-existing removable prostheses must be lightly relieved adjacent to the surgical site, in cases of stage two surgeries. In case of stage one, no removable prosthesis should be used over the site.
10. A periapical and/or panoral radiograph will be taken immediately post-operatively. 11. The patient will be provided oral and written post-operative instructions, and the
indicated prescriptions, if needed. 12. The surgical guide should be cleaned, disinfected and appropriately maintained so
that it can be used to assist in the second stage surgery. Post-Operative Follow-up
1. Post-operative evaluation and suture removal 7-10 days post-surgery 2. Recalls as needed thereafter until second stage surgery 3. Periapical radiographs should be taken at 3 months post-surgery prior to uncovery

30 | P a g e
Second-Stage Surgery (when indicated)
Second-stage surgery will proceed 3 or more months after the initial implant placement surgery. The location of the implants will be determined via clinical examination and use of the disinfected radiographic/surgical guide. Local soft tissue anesthesia will be obtained. A small incision over the implants and within the keratinized tissue will expose the top of the implant. Use of tissue punch should be avoided. The cover screws will be removed.
A healing abutment of the appropriate length and width will be placed to optimize esthetic contours. The healing abutment will be hand tightened in each of the implant fixtures. It should extend at least 2mm above the soft tissue. Sutures will be placed if needed. The soft tissue will be allowed to heal a minimum of 2 weeks prior to implant level impression. The patient will be provided oral and written post-operative instructions.
Prosthetic Protocol-Post Surgical
All restorative patient care will occur within the Predoctoral Implant Clinic. The diagnostic assessment and treatment plan must be reviewed with an instructor prior to any restorative appointments.
Maintenance Care
Single Tooth Implant-Supported Fixed Prostheses
Patients with Single Tooth Implant supported restoration require regular maintenance. Maintenance/ recall visits should be scheduled at 1 month, 3 months, six months, then annually. Patients will be responsible to cover the expenses associated with maintenance including but not limited to replacement of implant, its supported restorations, adjustments, and repairs. Patients will be responsible for fees associated with any maintenance radiographsThe following should be evaluated at each recall appointment:
1. Implant/ Crown stability 2. Occlusion 3. Marginal Integrity 4. Restoration integrity 5. Soft tissue color, contour, consistency, texture 6. Clinical probing depth 7. Bleeding on probing 8. Presence/ absence of suppuration 9. Location of soft tissue margin 10. Presence/ absence of keratinized tissue 11. Adjacent teeth 12. Periapical radiograph (annually)

31 | P a g e
*If patient presents a possible diagnosis of peri-implant mucositis or peri-implantitis at a recall appointment, a referral will be made to the designated implant surgical disciplines placed the implants.
Mandibular Implant-Supported Complete Denture
Patients with implant-supported overdentures with attachments require regular maintenance within the Predoctoral Implant Clinic. Patients will be responsible to cover the expenses associated with maintenance including but not limited to replacement of attachments, adjustments, repairs and relining. Patients will be responsible for the fees associated with any maintenance radiographs
Recall and assessment will be as follows:
- One week • Any adjustments to the reline area • Patient comfort and satisfaction • Tissue health adjacent to the abutment areas • Attachment integrity • Occlusion
- One month- same as above - Three months- same as above - Six months- same as above
- Annually- Same as above, in addition to • Implant stability • Soft tissue color, contour, consistency, texture • Bleeding on probing • Presence/ absence of suppuration • Location of soft tissue margin • Presence/ absence of keratinized tissue • Periapical radiograph (annually)
*If patient presents a possible diagnosis of peri-implant mucositis or peri-implantitis at a recall appointment, a referral will be made to the designated implant surgical disciplines placed the implant.
UIC College of Dentistry Required Reading Materials for Implant Care
1. Carl Misch. Contemporary Implant Dentistry. Mosby; 3rd edition (November 26, 2007)

32 | P a g e
2. Blackboard Website: PIP 101 Predoctoral Implant Clinic-contains all policies,
procedures and protocols for the Predoctoral Implant Clinic.

33 | P a g e
PHILOSOPHY ON SINGLE TOOTH IMPLANT
Department of Restorative Dentistry
Implant Supported (STI) and Overdentures
Prosthetic Protocol-Post Surgical All restorative patient care will occur within the Predoctoral Implant Clinic. The diagnostic assessment and treatment plan must be reviewed with an instructor prior to any restorative appointments.
Implant supported prosthesis
Indications: A single or two contiguous missing teeth in the maxilla or mandible. This may involve any tooth except maxillary central incisors and any second or third molars. Tooth #’s 23-26 and second molars may only be treated with the approval of the Predoctoral Implant Director. If a 3-unit implant supported FDP is indicated, the approval of the Predoctoral Implant Director must be obtained. Opposing implant restorations are acceptable.
• Single Tooth Replacement (STR) - The Mesial-Distal edentulous ridge width must be
at least 7 mm between roots as examined clinically and by periapical radiograph. 7mm may be acceptable for maxillary lateral incisors and mandibular incisors, however increased ridge width may be required for other teeth.
• Two Teeth Replacement (TTR) - The Mesial-Distal edentulous ridge width must be
at least 14 mm between roots as examined clinically and by periapical radiograph.
• Implant supported FDP (ISFDP) - The mesial-distal edentulous ridge must be at
least 21 mm between roots as examined clinically and radiographically. Only can be applied to replace Canine and posterior teeth (no second and third molar), 3 units (2 implants and 1 pontic): P-X-M or C-X-P. Only one ISFPD per patient will be accepted. ISFDP restoration can be screw or cement-temp- bond (PFM) retained. An ideal occlusal plane is expected.
Provisional restorations: A provisional restoration will be fabricated for all anterior restorations using an implant level impression technique. The provisional restoration will be fabricated in the Implant clinic under the supervision of the faculty. A customized impression coping will be fabricated for final impression using implant level technique. A healing abutment may be used for posterior restorations.
Single tooth implant (STI) restorations

34 | P a g e
Appointment #1 • Tissue will be evaluated for color, contour, thickness, consistency and overall
health. • Healing abutment will be removed. Final impression method (open or
closed tray method) will be determined by the specific situation. In general, the impression of choice will be a closed tray implant level impression.
• All necessary records will be obtained from the patient in the following sequence:
Shade (Must be taken before the final impression) Opposing impression or cast Occlusal registration in Maximum Intercuspation Position with
teeth in contact and per fixed philosophy. Impression of provisional restoration or duplicate of diagnostic
wax-up
Laboratory Steps • Student must obtain implant replica from the dental assistant • Student will pour up the soft tissue working cast and mount the casts on a semi-
adjustable articulator • Student will complete lab form in Axium to request a custom abutment
Appointment #2
• Custom abutment will be tried-in intra-orally. A vertical bitewing will be taken to verify the seating of the abutment.
• Student must assess adequate fit, occlusal clearance, and margin position of the custom abutment.
Laboratory Steps
• Student will complete lab form in Axium to request a restoration. The material of choice for the restoration will be based on the clinical situation guided by the supervised faculty.
Appointment #3
• Custom abutment and final restoration will be tried-in intra-orally. The restoration will be seated and adjusted in the following sequence (per fixed philosophy):
Interproximal contacts Margins verified/crown disclosed and adjusted if
necessary Occlusal adjustment Any additional contours needing adjustment
• Custom abutment will be torqued according to the manufacturer’s recommendation. A bitewing will be taken to verify the seating of the restoration on the abutment. The appropriate restoration luting agent will be used according to the department’s philosophy.
• A bitewing will be taken to verify no excess cement on restoration with cement-

35 | P a g e
retained restoration.

36 | P a g e
Implant supported FDP (ISFDP)-Cement retained
Appointment #1 • Tissue will be evaluated for color, contour, thickness, consistency and overall
health. • Both healing abutment will be removed. Final impression method: open tray
method and Floss with GC resin pattern • All necessary records will be obtained from the patient in the
following sequence: Shade (Must be taken before the final impression) Opposing impression or cast Occlusal registration in Maximum Intercuspation Position with
teeth in contact and per fixed philosophy. Impression of provisional restoration or duplicate of diagnostic
wax-up Laboratory Steps
• Student must obtain both implant replicas from the dental assistant • Student will pour up the soft tissue working cast and mount the casts on a semi-
adjustable articulator • Student will complete lab form in Axium to request custom abutments
Appointment #2
• Custom abutments will be tried-in intra-orally. A vertical bitewing will be taken to verify the seating of the abutment.
• Student must assess adequate fit, occlusal clearance, and margin position of the custom abutments.
• Student will take another bite registration with GC resin pattern with abutments. A final mounting with GC pattern resin on custom abutments will be verified.
Laboratory Steps
• Student will complete lab form in Axium to request a restoration. The material of choice for the restoration will be based on the clinical situation guided by the supervised faculty.
Appointment #3
• Custom abutment and final restoration will be tried-in intra-orally. The restoration will be seated and adjusted in the following sequence (per fixed philosophy):
Interproximal contacts Margins verified/crown disclosed and adjusted if necessary Occlusal adjustment Adjust the gingival portion of the pontic with fit checker. The
pontic should not give too much pressure on the gingiva. Any additional contours needing adjustment
• Torque the custom abutments according to manufacturer’s recommendation.

37 | P a g e
• A bitewing will be taken to verify the seating of the restoration on the abutment.

38 | P a g e
• Fill the access hole with Teflon tapes • Cement the ISFDP with temp-bond
Implant supported FDP (ISFDP)-Screw-retained
Appointment #1 • Tissue will be evaluated for color, contour, thickness, consistency and overall
health. • Both healing abutments will be removed. Final impression method: open tray
method and Floss with GC resin pattern • All necessary records will be obtained from the patient in the
following sequence: Shade (Must be taken before the final impression) Opposing impression or cast Occlusal registration in Maximum Intercuspation Position with
teeth in contact and per fixed philosophy. Impression of provisional restoration or duplicate of diagnostic
wax-up Laboratory Steps
• Student must obtain both implant replicas and UCLA abutments from the dental assistant
• Student will pour up the soft tissue working cast and mount the casts on a semi- adjustable articulator
• Student will complete lab form in Axium to request a custom abutment Appointment #2
• Abutment metal framework will be tried-in intra-orally. A vertical bitewing will be taken to verify the seating of the abutment.
• Student must assess adequate fit, occlusal clearance, margin position and rocking of the metal framework. If needed, metal framework needs to be sectioned in the junction on one of the pontic and abutment (extra orally). Place back both pieces intra orally and reconnect both pieces together with GC resident intraorally.
• Take another bite registration with GC resin pattern. A final mounting with GC pattern resin on custom abutments will be verified.
Laboratory Steps
• Student will complete lab form in Axium to request a restoration. The material of choice for the restoration will be based on the clinical situation guided by the supervised faculty
Appointment #3
• Final restoration will be tried-in intra-orally. The restoration will be seated and adjusted in the following sequence (per fixed philosophy):
Interproximal contacts Margins verified/crown disclosed and adjusted if necessary

39 | P a g e
Occlusal adjustment

40 | P a g e
Adjust the gingival portion of the pontic with fit checker. The pontic should not give too much pressure on the gingiva
Any additional contours needing adjustment • A vertical bitewing will be taken to verify the seating of the restoration on the
abutment. • Torque the IS-FPD according to manufacturer’s recommendation. • Fill the access hole with Teflon tapes • Fill the access hole with composite
Implant supported overdenture (IOD)
Denture Relief/Relines
• Relief of the mandibular denture in the area of the healing abutments will be needed to allow complete seating and normal occlusion of the denture prostheses. This should be scheduled in the Predoctoral Implant Clinic on the same day the healing abutments are delivered.
• A soft or hard reline of the denture adjacent to the surgical site may be required
depending on the extent of the implant surgery/alveolar ridge reduction. If needed, an initial soft reline must be completed no more than three weeks after the initial implant placement. The patient must be scheduled in the Predoctoral Implant Clinic for this procedure. The implant faculty will determine if a soft reline is needed at this stage, and if a hard reline will be needed prior to the final attachment completion.
Final Prosthetic Abutment Placement
• The healing abutment will be removed and a Locator abutment of appropriate length placed, extending 2mm above the soft tissue.
• The abutments will then be torqued according to the manufacturer’s recommendation.
• A localized, direct acrylic reline technique will then be used to pick-up the Locator abutment in the mandibular denture. All excess material will be trimmed and the denture polished.
• Post abutment insertion instructions will be given to the patient.
Maintenance Care The maintenance/recall care should follow the proposed protocol according to the Dental Implants

41 | P a g e
philosopy. UIC College of Dentistry Required Reading Materials for Implant Care
1. Carl Misch. Contemporary Implant Dentistry. Mosby; 3rd edition (November 26, 2007)
Blackboard Website: PIP 101 Predoctoral Implant Clinic-contains all policies, procedures and protocols for the Predoctoral Implant Clinic

42 | P a g e
PHILOSOPHY ON IMMEDIATE COMPLETE DENTURE
DEPARTMENT OF RESTORATIVE DENTISTRY Definitions
CID - conventional immediate denture (extraction of the posterior teeth; after healing, an immediate denture is fabricated which is relined as needed and used as a definitive prosthesis); IID - interim immediate dentures (using Classic teeth by Trubyte). After healing is complete, a new denture is fabricated as a definitive prosthesis; IOD - immediate overdentures (see tooth-supported overdenture philosophy)
1. Advantages of immediate complete dentures
a. Patient appearance is maintained b. Muscle support and VDO is maintained c. Less post-operative pain d. Duplication of the existing teeth (if their position is acceptable) e. Less adaptation problems f. Can be relined with tissue conditioners
2. Disadvantages of immediate complete dentures
a. Modified final impression methods b. Errors in centric relation record c. Errors in the arrangement of the anterior teeth (esthetics) d. May require more appointments and be more expensive e. Post-operative discomfort for the first several days f. Denture reline or fabrication of the new denture is indicated in most cases
3. Contraindication for immediate complete dentures
a. Patients with poor health or who are considered to have high surgical risks b. Patients who are uncooperative or who are unable physically or mentally to cope with
immediate dentures. For these patients, extractions in a controlled setting, followed by six months of tissue healing and conventional dentures procedures is preferred.
c. Patients with very mobile teeth that may be extracted during impression taking.
4. Explanations to the patients regarding limitations and expectations
a. Patient must be advised of the potential difficulty in transitioning from a dentate situation to a completely edentulous one.

43 | P a g e
b. Probable use of tissue conditioner and/or adhesives to improve retention and stability of
the immediate denture may be required c. Discomfort during wearing of the dentures d. Temporary difficulty in eating and speaking with the dentures, frequent lack of stability e. Unpredictable esthetics of the dentures, especially lip support f. Increased salivation, new chewing sounds, possible gagging while wearing the dentures g. At the time of delivery, the dentures may not fit when preparing to be inserted. Patient
may have to be sent home without the dentures h. Patient must NOT take out the immediate dentures for the first 24 to 48 hour i. Immediate dentures may require that a definitive new set of dentures will need to be
made j. Fees for tissue conditioning, relines, adjustments or a new set of dentures are the
patient's responsibility
5. Implant care for mandibular overdentures
a. During the initial appointment, all immediate denture patients must be advised about the benefits of having two implants placed in the mandibular arch after the fabrication of their maxillary and mandibular dentures. All potential mandibular immediate denture patients must have an implant screening appointment in the pre-doctoral implant clinic – room 311 (Mon, Wed, Thurs, Fri) prior to any treatment planning or treatment. Scheduling is done using AxiUm or by contacting the Predoctoral Implant Clinic Director.
b. The importance of considering two implants for the mandibular arch must again be reviewed with the patient following completion of the immediate denture therapy by the student and clinical faculty. Patient should be encouraged to proceed with the implant therapy. Patients previously approved for the implant therapy during the diagnostic phase and desiring implant-supported care should be referred to proceed with the detailed evaluation, assessment and care, following the established Predoctoral Implant Protocols (posted on the Blackboard Site).
c. Immediate implant placement (placement of the implant at the time of tooth extraction) for implant supported mandibular overdentures is not performed in the Pre-doctoral Implant Clinic unless determined necessary and approved by the Pre-doctoral Implant Clinic Director.
6. Sequence of the clinical procedures – All clinical procedures must be supervised by the
same clinical instructor.
a. Basic diagnostic procedures i. review of the patient’s chief complaint
ii. review of the medical and dental histories iii. intraoral examination with complete radiographic evaluation iv. oral cancer screening examination v. full periodontal evaluation and/or periodontal consult with charting of probing
depths of the remaining teeth

44 | P a g e
vi. endodontic evaluation if immediate overdentures are considered vii. oral surgery consultation regarding multiple extractions, tori removal and
alveoloplasty (if indicated) viii. preliminary impressions, diagnostic casts and their mounting
ix. evaluation of the existing prostheses if presentTreatment plan presentation and final decision is made with regard to which type of immediate denture option would best work for the patient
b. Treatment plan presentation and final decision is made with regard to which type of immediate denture option would best work for the patient
c. Oral surgery i. extractions of the posterior teeth except one posterior stop on each side,
followed by four weeks of healing (CID/IOD) d. New preliminary impressions and diagnostic casts (CID/IID/IOD) of the existing oral
condition e. Fabrication of the custom trays
i. TRIAD custom impression trays are prepared for the selective pressure final impression technique. A wax spacer must cover all of the tissue undercuts, edentulous secondary bearing and relief areas (one sheet of baseplate wax), and the remaining anterior teeth (two sheets of baseplate wax).
ii. Wax spacer must extend 2mm short of the outline of the custom tray. The custom tray is extended 2mm short of the depth of the vestibule or to the border between attached and unattached mucosa, to the vibrating line (maxillary tray) and must cover all of the supporting oral tissues (including retromolar pads).
f. Border molding
i. is performed sequentially by quadrants, using green stick compound (Kerr, working temp. 123 degrees) with the wax spacer ”in place.” Border molding can be achieved actively (by physiologic movements of the patient's limiting oral structures) and/or by manual manipulation of the patient's limiting oral structures. If necessary, the thickness of the border-molded labial denture border is adjusted to approximately 2-3mm.
g. Final impressions (full arch single tray) i. are made using PVS impression material (light body) after the wax spacer is
removed. A relief hole in the maxillary custom tray is made with a No. 8 round bur in the area of the palatal ruggae along the palatal suture.
h. Pouring of the final master casts (CID/IID) i. completed master casts should meet all the criteria described for complete
dentures. i. Posterior wax rims are fabricated, face-bow transfer obtained, vertical dimension of
occlusion and registration of centric relation determined (CID/IID), and master casts mounted by following all of the criteria described for complete dentures.
j. Correct incisal edge and midline must be marked. k. Set up of posterior teeth, clinical try-in (CID/IID)
i. Both the instructor and patient’s approval of the trial denture try-in are necessary prior to sending the completely festooned final set-up to the laboratory for processing. The “Denture Acceptance Form” must be signed.

45 | P a g e
l. Complete Root Canal Therapy for any overdenture abutments (IOD) m. Processing of the dentures (CID/IID) n. Prepare overdenture abutments as indicated (IOD), extract remaining teeth, osteoplasty
with use of the prepared surgical template (as predetermined with the mounted casts), delivery of the dentures (CID/IID/IOD).
o. Home care instructions are given to the patients at the time of denture delivery. p. Post-operative care at 24h, 48h and one week, using tissue conditioning if necessary. q. Laboratory reline or new complete dentures are made 6 months to one year after the
initial delivery. Text reference: Zarb GA, Hobkirk JA, Eckert SE, Jacob RF: Prosthodontic Treatment For Edentulous Patients Complete Dentures and Implant-Supported Prostheses 13th Ed., CV Mosby Co., St. Louis, 2013 Prepared by: Dr. Ales Obrez* Dr. Foteini Touloumi Dr. Jiyeon Kim Dr. Rand Harlow Updated 2020

46 | P a g e
PHILOSOPHY ON ORAL APPLIANCE MANAGEMENT OF OBSTRUCTIVE SLEEP APNEA
DEPARTMENT OF RESTORATIVE DENTISTRY
Oral appliance (OA) management is a reversible and cost-effective management of snoring and/or obstructive sleep apnea (OSA), indicated in adult patients diagnosed with primary snoring, mild to moderate OSA and in patients with severe OSA who are intolerant of or refuse management with the Continuous Positive Air Pressure (CPAP) device. For some patients, combination management with other types of treatments such as weight loss, surgery and CPAP may be indicated. This decision must be coordinated by the attending sleep physician. Oral Appliance Therapy has several advantages over other forms of OSA and sleep-disordered breathing (SDB) management:
a) Oral appliances are comfortable and easy to wear; b) Oral appliances are small, making them easy to carry when traveling; c) Management with oral appliances is usually reversible and non-invasive.
Before managing either snoring and/or OSA with any OA, a complete assessment by a sleep disorder specialist is important and necessary. After concluded that management with an OA is indicated, a sleep disorder physician provides the dentist, who has skill and experience in OA management, with a written referral, a copy of the diagnostic report and a prescription for AO. Because of the obvious life-threatening implications of several sleep disorders, OA management must commence only after a complete medical assessment is performed.
Oral appliances are effective in varying degrees and work by advancing the mandible and the tongue, thus increasing the airway space. The appliances should be used during sleep and must be comfortable for the patient. Finally, OAs can only be used in cooperative patients who are motivated to wear the appliance during sleep on a regular basis.
The dentist’s role in OA management involves the selection, design, fitting and follow-up of the patient using a custom designed oral appliance during sleep. Currently, there are several different oral appliances available. They can be classified by their mode of action or their design into:
1) Tongue retaining appliances that function by holding the tongue in the anterior position by means of a suction bulb. Keeping the tongue in an anterior position prevents it from collapsing during sleep and obstructing the airway.
2) Mandibular repositioning appliances reposition and maintain lower jaw (mandible) in a protruded position during sleep. This opens the airway by indirectly pulling the tongue forward. The appliance also holds the lower jaw and other structures in a stable closed position to prevent opening of the mouth.
Oral appliance fabricated using thermoplastic acrylic material allows the patient to warm the appliance in hot water before its insertion. The appliance subsequently cools and hardens intraorally, providing considerably more retention than traditionally fabricated cold-cure acrylic appliance. The combination of the appliance adjustability allowing minor lateral and vertical jaw movements,
38 | P a g e
increased retention and improved titration protocols have significantly increased the effectiveness of OA. Oral appliances for management of snoring and mild to moderate OSA have proven to be effective in improving sleep architecture and reducing sleep arousals. In most patients OAs decrease sleepiness and objectively measured snoring, and improve quality of life and behavioral function.
CLINICAL PROTOCOL FOR ORAL APPLIANCE THERAPY
The following sequence is recommended for management of snoring and/or mild to moderate OSA by OAs.
1. Medical assessment is completed by the attending physician or a sleep specialist. An
overnight polysomnogram with a detailed evaluation of the diagnostic criteria for OSA must be completed by a physician or sleep specialist before management with an OA is initiated. Written referral, prescription and a diagnostic report are forwarded to a dentist or a dental specialist.
2. Initial dental clinical examination, performed by a dentist or a dental specialist, includes
evaluating patient’s medical and dental histories, performing an intra-oral assessment of the soft tissue structures, teeth and their restorations, their periodontal status, and dental occlusion. In addition, the dentist’s initial assessment also includes evaluation of the dental radiographs, such as panoramic, and of the diagnostic casts.
During a clinical evaluation, the dentist should evaluate if the patients have sufficient number of teeth (at least eight maxillary and mandibular teeth) and no limitation of the protrusive mandibular movement (>5 mm) and/or of the mandibular opening (>25 mm). Patients who have edentulous maxillary arches and adequate number of teeth in the lower arch may experience favorable response to a mandibular repositioning appliance. Complete maxillary and mandibular edentulous status may preclude the use of a mandibular repositioning appliance, however some of these patients may experience good management response with a tongue retaining appliance. Partial dentures that replace four or fewer teeth do not preclude OA use. History of chronic temporomandibular disorder (TMD) may preclude the use of an OA in some patients. Severe occlusal wear (>20% of the clinical crown) may indicate severe bruxism and complicate OA therapy if the grinding persists.
After the clinical decision is made regarding the appropriateness of the appliance for the OSA patient, the type of the OA is selected, patient’s bite registration at the predetermined vertical dimension of occlusion and the therapeutic anterior mandibular position is registered. The laboratory prescription for the OA should include the information regarding the type and the material of the appliance.
3. During OA delivery the dentist should evaluate the appliance for its perfect fit, retention and
stability, and adjust it for the patient’s comfort. The patient is given OA hygiene instructions.
4. The follow-up appointments of the patient with an adjustable OA consist of the titration period. This period consists of incrementally advancing the mandibular part of the appliance.

39 | P a g e
Some patients stop snoring and waking up while feeling more rested shortly after the appliance is inserted. In some cases, no further advancement of the mandible is required. Others may require 2 to 6 months of slow and gradual mandibular forward repositioning before a clinically significant treatment effect is observed. When the patient and/or partner reports a cessation of snoring and resolution of the symptoms, further advancement of the mandible may not be required and the appliance is considered titrated
5. Only after the OA is fully adjusted and titrated, is the patient referred back to the sleep physician
for the re-assessment and for a repeat of the overnight sleep study. The objective assessment of OA efficacy at this time is recommended, due to the evidence that suggests that OAs may have a placebo effect on OSA symptoms and signs. If the polysomnogram study results indicate, further OA titration is initiated or possible appliance modification is performed. In selected cases redesign and its remake is recommended.
6. If the OA demonstrates to be effective and the patient is comfortable, the dentist should
schedule patient’s recall appointments every 6 months for the first 2 years. At each appointment, status of the patient’s dental status and dental occlusion/articulation is evaluated for any clinically significant change. Patients must be advised of the probability that minor occlusal changes are possible. In addition, subjective effectiveness, fit of the appliance and its comfort are monitored.
7. Regular follow-up appointments must be scheduled at least once a year to monitor OA wear,
its efficacy and its possible adverse effects. OAs generally last approximately 2 to 3 years. If the appliance is showing extensive wear, such as cracks, discoloration or lost retention, a new OA is recommended. The dentist may continue titrating the appliance further if symptoms recur. If maximum mandibular advancement is reached and symptoms still persist, the patient must be referred back to the sleep specialist for further evaluation.
8. Most side effects caused by OAs are usually mild and transient. They most frequently include
dry mouth, excessive salivation, mouth or teeth discomfort, muscle tenderness and jaw stiffness. Significant and persistent TMD signs and symptoms are rare. The most common dental changes that have been observed after regular use of the OA were a decreased anterior dental horizontal overlap, while the vertical dental overlap changes diminish with time. Although some occlusal changes might be undesirable in certain patients, the effective treatment of a life-threatening disease such as OSA supersedes the maintenance of a baseline dental occlusion/articulation.
Text Reference: Ramar K, Dort LC, Katz SG, Lettieri CJ, Harrod CG, Thomas SM, Chervin RD: Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral
Appliance Therapy: An Update for 2015. J Clin Sleep Med. 2015 Jul 15;11(7):773-827.
Prepared by: Dr. Ales Obrez* Dr. Mickey Spector Dr. Farhad Fayz

40 | P a g e
PHILOSOPHY ON MANAGEMENT OF THE PERIODONTIUM IN HEALTH AND DISEASE
DEPARTMENT OF PERIODONTICS, UIC COLLEGE OF DENTISTRY
Section I. Examination of Gingival and Periodontal Tissues
A. Comprehensive Oral Evaluation
1. Clinical and Radiographic Examination: All patients must be clinically evaluated to determine risk of gingival and periodontal diseases with an emphasis on disease prevention. Documentation must be entered into the electronic patient record and include records of:
a. Probing depths (PD) b. Gingival margin relative to the cemento-enamel junction (CEJ - FGM) c. Clinical attachment loss (CAL) d. Bleeding upon probing (BOP) e. Furcation involvement f. Mobility g. Plaque/calculus (PL/CALC) h. Deficiencies in width of keratinized tissue (MG)
This documentation must accompany radiographic images no greater than 2-3 years old and including full mouth survey (FMX) and vertical bitewings (vBW). Supplemental imaging can include panoramic and/or cone beam computed tomography surveys (CBCT) when indicated.
Section II. Diagnosis of Periodontal and Gingival Health and Disease
A. Diagnosis
A diagnosis is formulated after collection and evaluation of clinical and radiographic information using the Classification of Periodontal and Peri-Implant Diseases and Conditions guidelines derived from the American Academy of Periodontology1,2 (Figure 1).

41 | P a g e
Figure 1. Summary of periodontal disease and conditions

42 | P a g e
1. Periodontal and Gingival Health
In general, clinically healthy gingiva is associated with a localized inflammatory infiltrate and host response consistent with homeostasis that is observed in intact or a reduced periodontium. At the site level, clinically healthy gingiva can be classified as follows:
a. Clinical gingival health on an intact periodontium
Clinical gingival health on an intact periodontium is characterized by the absence of bleeding on probing, erythema and edema, patient symptoms, and attachment and bone loss. Physiological bone levels range from 1.0 to 3.0 mm apical to the CEJ.
b. Clinical gingival health on a reduced periodontium
Clinical gingival health on a reduced periodontium is characterized by an absence of bleeding on probing, erythema, edema and patient symptoms in the presence of reduced clinical attachment and bone levels. These conditions are noted in the following patients:
i. Stable periodontitis patients – These patients have successful completed
periodontal therapy (surgical or non-surgical) and are on a periodontal maintenance program. It should be recognized that successfully treated and stable periodontitis patients remain at increased risk of recurrent progression of periodontitis and must be followed closely.
ii. Non-periodontitis patients – These patients were not previously diagnosed with periodontitis but may have attachment loss manifested as gingival recession or may have had periodontal surgery such as crown lengthening surgery in the past. There is no current evidence for increased risk of periodontitis in these patients.
B. Gingival Diseases
Gingivitis is a non-specific inflammatory condition that is a consequence of sustained plaque biofilm accumulation at, and apical to, the gingival margin. Gingivitis is considered a major risk factor and a necessary prerequisite for periodontitis. The management of gingivitis is thus a primary prevention strategy for periodontitis. There are broadly two categories of gingival disease:
1. Dental plaque biofilm-induced gingivitis – Defined as an inflammatory lesion resulting from
interactions between the dental plaque biofilm and the host's immune-inflammatory response, which remains contained within the gingiva and does not extend to the periodontal attachment (cementum, periodontal ligament and alveolar bone) or the mucogingival junction and is reversible by reducing levels of dental plaque at and apical to the gingival margin. Clinical manifestations can be influenced by systemic (smoking, hyperglycemia, medications, hormones, etc.) or local (biofilm retentive restorative margins, xerostomia) risk factors. Dental plaque-induced gingivitis can be classified as:
a. Gingivitis on an intact periodontium. b. Gingivitis on a reduced periodontium in a non-periodontitis patient.

43 | P a g e
c. Gingival inflammation on a reduced periodontium in a successfully treated periodontitis patient (recurrent periodontitis cannot be ruled out in this case).

44 | P a g e
2. Non–dental plaque-induced gingival diseases – Encompass a variety of conditions not caused by plaque biofilm and usually do not resolve following plaque removal. Such lesions may be manifestations of a systemic condition (desquamative gingivitis such as lichen planus, pemphigus vulgaris, allergic reaction, etc.) or may be localized to the oral cavity (gingival abscess, foreign body reaction, etc.). Although these lesions are not caused by the dental plaque biofilm, the severity of the clinical manifestations often depends on plaque accumulation and subsequent gingival inflammation and may require management in conjunction with other health care providers.3-5
3. Clinical management of gingival diseases – Management of gingival diseases are aimed at restoring gingiva health by removing and controlling the etiology and modifying factors associated with gingival inflammation.
a. Diagnosis – Diagnosis is made after collection and evaluation of clinical and
radiographic information described in Section I.A.1. A patient diagnosed with gingivitis will present with signs of erythema, edema, BOP, and probing depths ≤ 4 mm. Symptoms may or may not be present. Inflammation will be confined to gingival tissues and not extend into the periodontium (bone, PDL, cementum) as confirmed by lack of radiographic bone loss and clinical attachment loss.
b. Therapeutic objectives – Clinical management of gingival diseases is aimed at eliminating factors triggering gingival inflammation and include calculating the O’Leary plaque index, oral hygiene instructions, patient motivation, modification of risk factors (smoking cessation, glycemic control when necessary, non-surgical periodontal therapy including mechanical dental plaque removal, and replacement of defective restorations, etc.). When indicated, antimicronial therapy (local, systemic) may be used as adjunctive therapeutic agents.6
c. Expected outcomes – Stability is characterized by successful treatment through control of local and systemic risk factors, probing depths ≤ 3 mm, minimal (< 10% of sites BOP, absence of erythema, edema, and patient symptoms in the presence of reduced clinical attachment and bone levels.7, 8
d. Maintaining gingival health – The treated and stable periodontitis patient with current gingival health remains at increased risk of recurrent periodontitis and accordingly must be closely monitored. Regularly scheduled periodontal maintenance is necessary and updated clinical findings must be entered into the patient’s electronic health record at each visit (periodontal chart and periodontal electronic record {perio EPR}).8 Treatment of non–dental plaque-induced gingival diseases may require physician consultation to help alleviate/control factors resulting in gingival inflammation.3
4. Documentation – Documentation of periodontal health and disease as described in Section I.A1 must be entered into the electronic health record. Updated clinical and radiographic findings must be entered into the patient’s electronic health record at each visit. The intent of this documentation is to aid both patient and clinician in initial assessment of periodontal and gingival health and disease, monitor gingival/periodontal health, monitor disease progression or recurrence, adjust/modify periodontal maintenance regimens as necessary, and make appropriate referrals as indicated.
D0150 Comprehensive Oral Evaluation – new or established

45 | P a g e
patient D1330 Oral hygiene instructions
When necessary, the following radiographic codes will be entered:

46 | P a g e
D0210 Complete series of radiographic images, or D0277 Vertical bitewings – 7 to 8 radiographic images
C. Periodontal Diseases
Periodontitis is characterized by microbially-associated, host-mediated inflammation that results in loss of periodontal attachment. This is detected as clinical attachment loss (CAL) by circumferential assessment of the erupted dentition with reference to the cemento-enamel junction (CEJ) or its surrogate (e.g. restorative margin).9 Figure 2 summarizes the various scenarios that may arise following the transition from health to gingivitis and ultimately periodontitis.
Figure 2. Overview of relationship between gingivitis and periodontitis
1. Periodontal Examination
a. Clinical and Radiographic Examination – Documentation of periodontal health and disease as described in Section I.A1 and must be entered into the electronic health record. This information should be updated at every periodontal maintenance recall appointment.
b. A patient is diagnosed with periodontitis in the context of clinical care if:
i. Interdental CAL is detectable at ≥2 non‐adjacent teeth, or
ii. Buccal or lingual/palatal CAL ≥3 mm with probing depths >3 mm is detectable at ≥2 teeth
iii. The observed CAL cannot be ascribed to non-periodontal causes such as:
Gingival recession of traumatic origin Dental caries extending in the cervical area of the tooth The presence of CAL on the distal aspect of a second molar and
associated with malposition or extraction of a third molar An endodontic lesion draining through the marginal periodontium

47 | P a g e
The presence of a vertical root fracture

48 | P a g e
c. Identification of periodontitis type
Based on pathophysiology, three clearly different forms of periodontitis have been identified. Differential diagnosis is based on history and the specific signs and symptoms of disease:
1. Periodontitis (most common form of periodontal disease) 2. Periodontitis as a direct manifestation of systemic diseases 3. Necrotizing periodontitis
i. The majority of clinical cases of periodontitis present with a range of phenotypes and complexities that require different approaches to clinical management including those with endodontic involvement10
ii. Patients with periodontitis as a direct manifestation of systemic disease include poorly controlled diabetics, immunocompromised individuals, or individuals with rare genetic disorders with a secondary manifestation of periodontitis.
iii. Presentation of patients with necrotizing periodontitis is rare and characterized by history of pain, presence of ulceration of the gingival margin and/or fibrin deposits at sites with characteristically decapitated gingival papillae, and, in some cases, exposure of the marginal alveolar bone. Symptoms are usually acute in nature and can be associated with recent emotional stress and fetid odor. The presence or absence of an uncommon systemic disease that definitively alters the host immune response is evident.
2. Staging and grading of the periodontal patient (Diagnosis)
a. Staging and grading – ln general, staging and grading of a patient suspected of having periodontal disease will follow the steps outlined in Figure 3 and is completed after collection and evaluation of clinical and radiographic information as described in Section I.A.1.

49 | P a g e
Figure 3. Three steps to staging and grading a patient9

50 | P a g e
b. Establishing Stage – The goals in staging a periodontitis patient include:
• Classify Severity and Extent of Disease – Based on currently measurable extent of destroyed and damaged tissue attributable to periodontitis.
• Assess Disease Complexity – Assess specific factors that may determine complexity of controlling current disease and managing long-term function and esthetics of the patient's dentition.
• Figure 4 summarizes staging protocol for periodontitis patients.
i. Stage I periodontitis (Mild)
• Represents the early stages of attachment loss and the transition between gingivitis and periodontitis in response to persistence of gingival inflammation and biofilm dysbiosis.
• When noted at an early age these patients may have heightened susceptibility to disease onset and should be monitored closely.
ii. Stage II periodontitis
• Stage II represents established periodontitis. • Careful evaluation of the patient's response to standard treatment principles
is essential. • The case grade plus treatment response may guide more intensive
management for specific patients.
Figure 4. Staging of the periodontitis patient9
iii. Stage III periodontitis (Severe with potential tooth loss)

51 | P a g e
• Characterized by the presence of deep periodontal lesions that extend to the middle portion of the root indicating significant damage to the attachment apparatus.

52 | P a g e
• Management is complicated by the presence of deep intrabony defects, furcation involvement, history of periodontal tooth loss/exfoliation, and presence of localized ridge defects.
• In the absence of advanced treatment, tooth loss may occur. However, in spite of the possibility of tooth loss, masticatory function is preserved, and treatment of periodontitis does not require complex rehabilitation of function.
iv. Stage IV periodontitis (Severe with potential loss of dentition)
• Characterized by the presence of deep periodontal lesions that extend to the apical portion of the root and/or history of multiple tooth loss
• Frequently complicated by tooth hypermobility due to secondary occlusal trauma and the sequelae of tooth loss: posterior bite collapse and drifting.
• Considerable damage to the periodontal support is evident and may cause significant tooth loss, and this translates to loss of masticatory function.
• The dentition is at risk of being lost.
c. Establishing Grade – The goals in staging a periodontitis patient include:
• Estimate Future Risk – Periodontitis progression and responsiveness to standard therapeutic principles
• Guide intensity of therapy and monitoring • Estimate Potential Health Impact of Periodontitis – Evaluate the impact of
systemic disease and the reverse, • Guide Systemic Monitoring and Co-Therapy with Medical Colleagues
The objective of grading is to use whatever information is available to determine the likelihood of the case progressing at a greater rate than is typical for the majority of the population or responding less predictably to standard therapy.
i. Grading Criteria
The primary criteria are noted below and in Figure 5:
• Direct evidence (clinical and radiographic history). Whenever available, direct evidence is preferred.
• Indirect evidence (age) of progression. in the absence of direct evidence, indirect estimation is made:
o Utilizes bone loss as a function of age at the most affected tooth or; o Case presentation as noted by radiographic bone loss expressed as
percentage of root length divided by the age of the subject (RBL/age).
• Clinicians should initially assume grade B disease and seek specific evidence to shift towards grade A or C, if available.
• Once grade is established based on evidence of progression, it can be modified based on the presence of risk factors such as smoking and glycemic control for diabetic patients. A risk factor, will therefore shift the grade score to a higher value independently of the primary criterion used to evaluate rate of progression.

53 | P a g e
Figure 5. Grading of the periodontitis patient9
c. Therapeutic objectives – The objectives of periodontal therapy are to alter or eliminate
the microbial etiology and contributing risk factors for periodontitis, thereby arresting the progression of disease and preserving the dentition in a state of health, comfort, and function with appropriate esthetics. 1, 11
• Stage I and II (Grade A, B): At these stages of the disease process, management of most cases typically involves standard non-surgical treatment principles involving regular personal and professional removal of plaque biofilm/hard deposits and monitoring. Successful therapy is expected to arrest disease progression.
• Stage III and IV (Grade A, B, C): Management of more advanced forms of periodontal therapy likely surgical intervention and may require stabilization/restoration of masticatory function. A referral to post-graduate periodontics clinic is indicated. In some cases, Stage II, Grade C and Stage III, Grade A patients can be treated in the pre-doctoral clinics with approval.
• Surgical therapy when indicated is aimed at regeneration of lost periodontal tissues, osseous resection, and/or pocket elimination therapy.
d. Periodontal Re-evaluation – The desired outcome of periodontal therapy in patients with periodontitis with advanced loss of periodontal support should include:8
• Significant reduction of clinical signs of gingival inflammation • Reduction of probing depths • Stabilization or gain of clinical attachment • Radiographic resolution of osseous lesions • Progress toward occlusal stability • Progress toward the reduction of clinically detectable plaque to a level
compatible with gingival health
e. Clinical setting – The table below outlines preferred clinical setting for treatment of

54 | P a g e
patients with periodontal diseases based on stage, grade, and complexity:

55 | P a g e
Stage Grade Clinic Setting
Gingivitis Gingivitis Predoctoral I A Predoctoral I B Predoctoral II A Predoctoral II B Predoctoral II C *Predoctoral, Post-graduate III A *Predoctoral, Post-graduate III B *Predoctoral, Post-graduate III C Post-graduate IV A Post-graduate IV B Post-graduate IV C Post-graduate
Table 1. Clinical setting for treatment of periodontitis patients (*preferred clinic)
D. Periodontal Maintenance
The treated and stable periodontitis patient with current gingival health remains at increased risk of recurrent periodontitis and accordingly must be closely monitored.8,12 Regularly scheduled periodontal maintenance is necessary and updated clinical findings must be entered into the patient’s electronic health record at each visit (must complete periodontal chart and update the perio EPR forms). Treatment of non–dental plaque-induced gingival diseases may require physician consultation to help alleviate/control factors resulting in gingival inflammation.3
Therapeutic objectives – Periodontal maintenance is aimed at minimizing the recurrence and progression of periodontal disease in patients who have been previously treated for periodontitis and to reduce the incidence of tooth loss by monitoring the dentition and any prosthetic replacements of the natural teeth.9
• Additional objectives include increasing the probability of locating and treating other diseases or conditions found within the oral cavity
• The desired outcome for patients on periodontal maintenance should result in maintenance of the periodontal health status attained as a result of active therapy
Required Textbooks
Newman MG, Takei H, Klokkevold PR, Carranza FA. 2019. Newman and Carranza's Clinical Periodontology, 13th Ed. Elsevier Publishing, Amsterdam, The Netherlands.

49 | P a g e
References
1. Chapple ILC, Mealey BL, Van Dyke TE, Bartold PM, Dommisch H, Eickholz P, Geisinger ML, Genco RJ, Glogauer M, Goldstein M, Griffin TJ, Holmstrup P, Johnson GK, Kapila Y, Lang NP, Meyle J, Murakami S, Plemons J, Romito GA, Shapira L, Tatakis DN, Teughels W, Trombelli L, Walter C, Wimmer G, Xenoudi P, Yoshie H. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol 2018; 89: S74-S84.
2. Caton JG, Armitage G, Berglundh T, Chapple ILC, Jepsen S, Kornman KS, Mealey BL, Papapanou PN, Sanz M, Tonetti MS. A new classification scheme for periodontal and peri-implant diseases and conditions - Introduction and key changes from the 1999 classification. J Periodontol 2018; 89: S1-S8.
3. Holmstrup P, Plemons J, Meyle J. Non–plaque-induced gingival diseases. J Periodontol 2018; 89: S28– S45. 4. Stone SJ, Heasman PA, Staines KS, McCracken GI. The impact of structured plaque control for patients
with gingival manifestations of oral lichen planus: a randomized controlled study. J Clin Periodontol 2015; 42: 356– 362.
5. The American Academy of Periodontology. Parameter on acute periodontal diseases. J Periodontol 2000; 71: 863-866.
6. The American Academy of Periodontology. Position paper: Systemic antibiotics in periodontics. J Periodontol 2004; 75: 1553-1565.
7. Trombelli L, Farina R, Silva CO, Tatakis DN. Plaque-induced gingivitis: case definition and diagnostic considerations. J Periodontol 2018; 89: S46– S73.
8. Matuliene G, Pjetursson BE, Salvi GE, Schmidlin K, Brägger U, Zwahlen M, Lang NP. Influence of residual pockets on progression of periodontitis and tooth loss: results after 11 years of maintenance. J Clin Periodontol 2008; 35: 685– 695.
9. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol 2018; 89: S149-S161.
10. Herrera D, Retamal-Valdes B, Alonso B, Feres M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J Periodontol 2018; 89 Suppl 1: S85-S102.
11. The American Academy of Periodontology. Parameter on chronic periodontitis with advanced loss of periodontal support. J Periodontol 2000; 71: 856-858.
12. The American Academy of Periodontology. Parameter on periodontal maintenance. J Periodontol 2000; 71: 849-850.

50 | P a g e
PHILOSOPHY OF ENDODONTIC CARE
Department of Endodontics
The current best available evidence is utilized to support clinical practice, in conjunction with case specific clinical judgment and consideration of patient preferences.
Cases that are beyond a practitioner’s skill level should be referred to a provider with more advanced skills or specialty training in endodontics
Diagnosis and treatment planning
I. Consider chief complaint and history, perform clinical exam, testing and appropriate imaging.
a. Intraoral radiographs should be considered the imaging modality of choice in the
evaluation of the endodontic patient. b. Well-angulated preoperative radiographic images are mandatory to facilitate safe and
efficient access. c. Although two radiographs with different angulations are often sufficient to develop a
more complete image of the tooth to be treated, cone beam computed tomography (CBCT) images may be justified and necessary to evaluate the existence of extra canals, complex morphologies, curvatures, or dental developmental anomalies.
II. Analyze data and establish correct diagnosis
III. Confirm restorability of tooth
IV. Evaluate medical status and recognize need for medical consultation and/or treatment
modifications when necessary
V. Use the AAE Case Difficulty Assessment Form (CDAF) (reference 4) and determine if referral to an endodontist is indicated
VI. Discuss treatment benefits, risks, alternatives, and prognosis with patient. Obtain informed
consent. Treatment
I. Determine need for local anesthesia. Administer effective local anesthesia when indicated.
II. Isolate tooth with rubber dam. Use of the rubber dam is the standard of care for endodontic treatment (including root canal therapy, vital pulp therapy). The use of a rubber dam during treatment is mandatory to avoid microbial contamination of the root canal system, limit aerosols, retract tissues, protect the patient from damage by chemicals, and prevent aspiration or swallowing of instruments and materials. (reference 5)

51 | P a g e
III. Perform appropriate access preparation to allow for instrumentation of all canals, while avoiding unnecessary removal of sound tooth structure. All caries should be removed.
IV. Determine proper canal working length using an electronic apex locator and radiographs as
needed.
V. Perform chemo-mechanical preparation of canal space(s) to allow for obturation. NaOCl is the preferred endodontic irrigant for disinfection of the root canal. If a predisposing risk for irrigant extrusion into the periradicular tissues is suspected, (open apices, root perforation or vertical root fracture), clinicians should proceed with caution, using diluted NaOCl or an alternative proven antimicrobial solution.
VI. Obturate all canals to the predetermined appropriate working length.
VII. Place an appropriate temporary restoration and check occlusion. Coronal bacterial leakage is a
known cause of treatment failure. Placement of a definitive coronal restoration must be considered part of the obturation process to eliminate recontamination.
VIII. Post-operative instructions. Recommend OTC analgesics and/or prescribe analgesics and
antibiotics when indicated (references 6 and 7).
Outcome evaluation and prognosis
I. Evaluate result of treatment and establish prognosis
II. Recommend appropriate post-treatment evaluation (recall) schedule
Restoration
I. Endodontically treated teeth are primarily susceptible to fracture due to loss of structure from caries, prior restorations, fractured cusps, and the access cavity. Successful final restoration of endodontically treated teeth plays a major role in the long-term prognosis and must be considered as an integral part of the endodontic treatment.
II. In teeth with minimal structural loss, intact marginal ridges, a conservative access preparation, and
no preexisting cracks, the clinician may consider a direct intracoronal bonded restoration as a valid option.
III. Evidence finds that the use of posts for crown retention has no significant influence on tooth
survival after endodontic treatment.
IV. Restoration of anterior teeth: if the only loss of tooth structure results from a conservative access preparation, a bonded composite is adequate. If the tooth is weakened by a large access preparation, proximal caries, or proximal restorations, a crown should be considered as the final restoration. A post is necessary when the remaining tooth structure (after crown preparation) will not retain the core.

52 | P a g e
V. Restoration of posterior teeth: proper restoration of posterior teeth involves two phases: core placement and crown placement.
VI. A post is not indicated if three supporting walls of dentin remain or if not otherwise
necessary for core retention due to the potential for vertical root fracture.
References:
1) UIC Department of Endodontics Clinic Manual.
2) Endodontic Competency: Executive Summary. American Association of Endodontists. 2019
3) Treatment Standards: Executive Summary. American Association of Endodontists. 2019
4) AAE Case Difficulty Assessment Form (CDAF)
5) Pathways of the Pulp, 11th Ed, 2016.
6) AAE Guidance on the Use of Systemic Antibiotics in Endodontics: AAE Position Statement. Fouad AF, et al. 2017
7) Lockhardt PB, Tampi MP, Abt E, et al. Evidence-based clinical practice guideline on antibiotic use for the urgent management of pulpal- and periapical-related dental pain and intraoral swelling. J Am Dent Assoc 2019;150:906-921.

53 | P a g e
PHILOSOPHY OF PREDOCTORAL ORAL SURGERY CLINIC
DEPARTMENT OF ORAL MAXILLOFACIAL SURGERY
The UIC Pre-Doctoral Oral Surgery Clinic provides basic maxillofacial surgery care. The dentoalveolar surgical care includes exodontia, with a strong emphasis on patient evaluation and risk assessment. Other aspects include appropriate management of surgical complications and infection control.
1 . A pre-operative Patient Evaluation, including review of medical history, current medications, imaging, and review of treatment planned procedure(s) are completed. All extractions must be treatment planned and approved by Group Practice Faculty, and the treatment plan noted in the patient record. The Oral Maxillofacial Surgery Triage/Scheduling Sheet, must be signed by the OMS Faculty prior to patient scheduling.
2. Patient is evaluated at time of appointment, including vital signs, review of medical history and current medications. An evaluation of the patient’s health status will be completed and appropriate treatment modifications or request for appropriate medical consultations will be performed.* (references: a,c)
3. A clinical examination, review of treatment plan and the selection of the most appropriate radiographs are reviewed. * (reference, a)
4. A risk assessment is completed and determination of appropriateness for care or consideration of referral is made. Referral of difficult extractions beyond students’ skill level, may be made to appropriate practitioner or oral maxillofacial surgeon. Complicated surgical extractions or impacted teeth ( D7210, D7220, D7230, D7240, D7250) are examples of procedures that might be referred for management in the post-graduate oral maxillofacial surgery clinic.
5. The patient is provided detailed information relative to the care plan for the session, indicates the tooth or teeth to be extracted visually with a hand mirror, which is confirmed during a “time out”, with the student and faculty member. The "time out" serves as a double check to avoid extraction of the incorrect tooth.
6. An informed consent and documentation will be completed and maintained in the patient record. (Appendix A).
7. Appropriate and effective local anesthesia, will be provided for indicated procedure.*(reference. a,d)
8. Anxiety and fear management with the use of minimal sedation techniques including nitrous oxide and oral pre-medication may be provided. *(reference a,b,e).
9. Aseptic technique and appropriate infection controls during entire procedure will be ensured. *(reference a)
10. Appropriate surgical instruments for extractions and other oral surgical procedures will be utilized. *(reference a.)
11. Appropriate throat and soft tissue protective measures are utilized. *(reference a.)

54 | P a g e
12. Dental extraction (D7140) or selected surgical dental extraction of erupted tooth (D7210) are completed.
13. Assessment of surgical outcome and bleeding control is completed. * ( reference a). Post operative radiographs are taken when indicated if need to insure completed procedure.
14. Determination of the need for a drug prescription is made and prescription provided when appropriate, based upon difficulty and length of procedure, or presence of preexisting infection* (reference a,b)
15. Post Op instructions are provided (Appendix B)
16. Patient vital signs and physical condition, are evaluated and should be appropriate for discharge.*(reference a,c)
17. Assessment of complications and appropriate follow up treatment provided as appropriate. * (ie treatment for dry socket, or post-operative infection, or bone spicule). *(reference a)
18. Documentation completed in patient electronic health record following indicated procedure note templates in Electronic Health Record.
*References:
a. Contemporary Oral and Maxillofacial Surgery 6th or 7th Edition, Hupp, Ellis, Tucker; Elsevier Publishers.
b. Pharmacology and Therapeutics in Dentistry, Yagiela et al., 6th or more recent edition, Mosby
Publishers.
c. Dental Management of the Medically Compromised Patient, Little and Falace, 7th edition or more recent edition, Mosby Publishers. 6th edition, Mosby Publishers.
d. Handbook of Local Anesthesia, Malamed S.F, 5th edition or newer, Mosby Publishers
e. Sedation in Dentistry, Malamed S.F., 4th or 5th edition, Mosby Publishers.

55 | P a g e
Appendix A, Example of Informed Consent

56 | P a g e
Appendix B, Post-Operative Instruction Sheet.

57 | P a g e
PHILOSOPHY ON URGENT CARE
Department of Oral Medicine and Diagnostic Sciences
I) Purpose of Urgent Care Rotation
a) The Urgent Care Program expeditiously assesses, diagnoses, and provides palliative care or a referral for the Patient with urgent dental needs.
II) Assessment of the Patient’s Urgent Care needs includes:
a) Obtaining the Patient’s history b) Clinical examination c) Obtaining appropriate radiology d) Necessary consultations (both with Dental and Medical colleagues) e) Diagnosis f) Offering multiple treatment options and determining a plan consistent with the Patient’s values
III) Treatment management options for the Patient may include:
a) Restorative treatment b) Surgical treatment c) Endodontic therapy d) Periodontic therapy e) Referrals to specialty clinics and GPR programs when needed care is beyond the ability of a
student dentist f) Prescribing antimicrobial and analgesic medications g) When time does not allow for same day treatment, the student dentist will provide the Patient a
follow up appointment in the next few days
IV) Supporting documents provided to maximize Evidence Based Dental care:
a) Checklist/Guidelines for completing and Urgent Care Visit b) Antimicrobial Use for Acute Dentoalveolar Conditions Clinical Decision Support Tool c) Management of Patients with Orthopaedic Implants Undergoing Dental Procedures Online
Clinical Decision Support Tool d) Prevention of Infective Endocarditis e) Management of Acute Periodontitis Clinical Decision Support Tool

58 | P a g e

59 | P a g e

60 | P a g e
http://www.orthoguidelines.org/go/auc/default.cfm?auc_id=224995&actionxm=Terms

61 | P a g e

62 | P a g e

63 | P a g e
PHILOSOPHY ON DENTAL STUDENT TREATMENT OF PEDIATRIC PATIENTS
DEPARTMENT OF PEDIATRIC DENTISTRY
Section I. Examination, Diagnosis, and Preventative Approaches for Pediatric Dental Patients
A. Comprehensive and Periodic Oral Evaluation
1. Clinical Examinations:
Dental students are expected to complete examinations of pediatric patients according to the departmental examination protocol (attachment 1). The clinical examination will include a patient and parent interview, as well as extra-oral and intra-oral examination of the patient. Per AAPD guidelines, examinations are expected to include:
• General health/growth • Pain • Extraoral soft tissues • Temporomandibular joints • Intraoral soft tissues • Oral hygiene and periodontal health • Intraoral hard tissues • Developing occlusion • Caries risk • Behavior of child
All areas of the examination are reviewed with faculty members. Documentation of exam findings are expected to be included in the EHR including completing required forms and completing clinical notes. All aspects of examination are included under the codes D0150 (Comprehensive Oral Exam) or D0120 (Periodic Oral Exam).
2. Radiographic Examination:
Radiographic examination in pediatric patients must be individualized to the patient and situation. A radiographic plan is determined based on patient information and clinical examination. Radiographs are taken with the intent of gathering necessary diagnostic information, while minimizing radiation exposure to the lowest amount reasonably allowable. Students are expected to interpret all acquired images at the time of examination and document appropriate in the EHR.

64 | P a g e
Figure 1 AAPD Radiograph Recommendations
3. Caries Risk Assessments
As part of the examination process students are expected to complete a caries risk assessment, and provide recommendations based on this assessment. Assessments are expected to follow the AAPD guidelines and be appropriate for the age of each patients. Recommendations are made to help patients address caries risk status by improving individual factors.

65 | P a g e
Figure 2 Caries Risk Assessment for 0-5 year olds
4. Preventative Approaches
Students are expected to provide and recommend preventative approaches to appropriate manage a patients caries risk including but not limited to:
a. Prophylaxis b. Fluoride Varnish Application c. Oral Hygiene Instructions d. Diet Counselling e. Recommendation of Additional Oral Care Products f. Prescription of Oral Care Products

66 | P a g e
Figure 3 Caries Risk Assessment for 6 years and older
Section II. Diagnosis and Treatment Planning of Oral Conditions in Pediatric Patients
A. Diagnosis
The pediatric patient may present with a wide variety of oral conditions, ranging from health, to severely compromised dentitions. Students are asked to synthesize all the information gathered in the examination phase to comprehensively evaluate and determine diagnoses for the patient. This includes diagnoses for individual teeth, the oral cavity, and the patient as a whole.
1. Dental Caries – as the most common diagnosis students are expected to make an assessment of the presence and severity of caries on both primary and permanent teeth, on a tooth by tooth bases. This assessment is completed by combining visual, tactile, and

67 | P a g e
radiographic information, modulated by the patient’s caries risk and history.

68 | P a g e
2. Pulpal Status – Teeth suspected of having carious lesions present require at least a cursory assessment of pulpal health. Symptoms, clinical, and radiographic information should be used to make an assessment of pulpal health, supplemented with vitality testing when necessary.
3. Restorability – A tooth with caries should be assessed for restorability, as determined by remaining tooth and root structure.
4. Occlusion – The developing occlusion of all pediatric patients should be assessed, with the goal of recognizing pathologic occlusal issues that may require interceptive or comprehensive intervention.
5. Gingival/Periodontal Health – All patients should have the health of the periodontium assessed.
6. Other hard tissue pathology – Pathologic conditions of the dental hard tissues other than caries should be evaluated and included as diagnoses
7. Soft Tissue Pathology – Atypical conditions of the oral soft tissues, intra and extra oral, should be assessed and diagnosed
8. Dental Trauma – The dentition of all patient should be assessed for signs or symptoms of dental trauma. This assessment should include a reported history, as well as clinical or radiographic signs.
9. Implications of Systemic Disease – Any oral presentations of systemic disease should be carefully assessed and recorded
10. Temporomandibular Joint – The TMJ should be assessed for normal and asymptomatic function, including reported symptoms from the patient.
11. Child Behavior – It is vital to assess the behavioral status of the child, recorded on the Frankel scale. Behavior should be assessed and recorded at every dental visit.
B. Treatment Planning
Treatment planning for pediatric patients should incorporate all the information collection in the examination phase, and the diagnoses determined. Treatment planning for a pediatric patient requires careful assessment of the patient, their oral cavity, and the individual diagnoses, as well as an open dialogue with the child and caregiver. Treatment plans are expected to have all of the following characteristics:
1. Comprehensive – A treatment plan is expected to address all diagnoses or conditions
observed. 2. Age appropriate – Treatments should be in line with dental development and
behavioral expectations for the patient 3. Consented – All treatments must be agreed to by the legal guardian of the child, and
whenever possible the assent of the child should be obtained. The process of informed consent is critical when treatment planning for pediatric patients.
4. Documented – The treatment plan, and legal guardian consent, must be documented in the EHR.

69 | P a g e
Section III. Treatment of Pediatric Dental Patients
A. Behavior Management Every effort should be made to accommodate the pediatric patient during their treatment. Non- pharmacologic behavior management is recommended for all patient to help reduce anxiety and improve compliance with treatment. Dental students are expected to provide basic behavior management techniques, while advanced behavior guidance techniques are provided by residents and faculty members.
B. Nitrous Oxide Use
Nitrous Oxide is a valuable and useful adjunct to behavior management in pediatric patients. Nitrous Oxide administration should be administered carefully and safely, per AAPD protocols. Nitrous Oxide use must be discussed and consented to prior to use. Documentation for nitrous oxide use must include:
• Informed Consent • Indication • Dosage (Percentages and Flow Rate) • Duration • Post-operative Oxygenation
C. Local Anesthesia
Local anesthesia delivery is a key portion of providing restorative care to pediatric patients. An appropriate local anesthetic plan must be determined prior to initiating treatment. This plan must include
• Anesthetic agent selection • Location of injection • Anesthetic maximum dose • Supplemental anesthesia if needed
If local anesthesia can not be delivered safely, or adequate anesthesia cannot be obtained treatment may be aborted.
D. Restorative Treatment Restorative Treatment for pediatric patients is expected to follow evidence-based recommendations to provide the restoration with the best possible chance for success. Restoration selection must account for size and location of caries, position of the tooth in the arch form, isolation, pulpal status, and dental development. Restorative treatment in the pediatric dental patient may include:
• ITR/ART • Glass Ionomer and RMGI restorations • Composite Restorations • Amalgam Restoration • Stainless Steel Crowns • Composite Strip Crowns

70 | P a g e
E. Pulp Therapy Pulp Therapy in the pediatric dental patient may include indirect pulp caps, pulpotomies, or pulpectomies. The appropriate technique is selected based on the clinical and radiographic signs, as well as symptoms reported by the patient. Pulp therapy is only recommended when a tooth is clearly restorable. All teeth treated with pulp therapy are recommended for a full coverage restoration to maximize likelihood of success. Students are expected to be comfortable providing pulp therapy for primary teeth, and limited care for young permanent teeth.
F. Extraction Routine extractions of primary and permanent teeth may be completed for pediatric patients. Teeth that have been deemed non-restorable are indicated for extraction. Care should be taken to complete extractions in as atraumatic manner as possible. A priority is placed on maintaining the viability of the successor tooth when extracting primary teeth.
G. Space Maintenance
Space maintenance is a valuable tool to help prevent space loss in the transitional dentition. Any patient with premature loss of a primary tooth should be assessed for placement of a space maintainer. The decision to place a space maintainer should be based on the patients occlusal status, dental development, oral hygiene, and general health.
Section IV. Coordination of Specialty Care
As a comprehensive care specialty, pediatric dentistry often requires coordination and interaction with other specialty providers. In order to provide the most appropriate care to our patients, coordination with other departments is a critical feature.
A. Orthodontic All patients should be assessed for developing malocclusions during routine examinations. If a malocclusion is detected, an appropriate referral should be placed for interceptive or comprehensive

71 | P a g e
orthodontic care. While patients are undergoing orthodontic therapy, pediatric dentistry should provide routine examinations, preventative services, and any necessary restorative care. Pediatric dentistry will also provide extraction services when routine extractions are required to facilitate orthodontic care.
B. Endodontics
Pediatric dentistry will carefully assess the young permanent dentition for endodontically involved teeth. Whenever possible, pediatric dentistry will perform the initial assessment of teeth, including pulpal health and restorability. In situations with a vital pulp, pediatric dentistry will attempt vital pulp therapy and monitor for success. When vital pulp therapy is unsuccessful, or not indicated, a referral to endodontics will be made. Following completion of endodontic therapy, pediatric dentistry will complete the indicated restoration for treated teeth. Pediatric dentistry will also reassess previously treated teeth and refer to endodontics for reassessment when indicated.
C. Oral Surgery Pediatric dentistry will complete routine extractions of primary and permanent teeth for cooperative patients. A referral to oral surgery will be made in the following circumstances
• Surgical extraction required • Impacted tooth indicated for extraction • Ankylosed tooth indicated for extraction • Complex pathology indicated for biopsy • Emergent dental care required (facial swelling requiring I&D) • Routine extraction requiring IV sedation or general anesthesia
D. Periodontics Pediatric Dentistry will manage routine gingival disease in children. Referrals will be made for acute gingival or periodontal conditions, or those that may require surgical intervention.
E. Oral Medicine Pediatric Dentistry will assess oral conditions, and refer those that may require long term or specialized management.
F. Graduation From Pediatric Dentistry Patients who are above 16 years of age will be considered for referral to the general undergraduate clinics to continue routine dental care.
Section V. Undergraduate and Postgraduate Care Division
A. Procedure Based Distinctions Routine pediatric dental procedures may be completed either with dental students or pediatric dentistry residents. Advanced procedures that require pediatric dental resident care may include:
• Pulpectomy • Soft tissue biopsy • Frenectomy • Young permanent tooth pulp therapy • Dental trauma requiring pulp therapy • Urgent needs requiring immediate treatment

72 | P a g e
B. Complexity Based Distinctions
In some scenarios, patient social or medical factors may become too complex for care in a dental student clinic environment. In situations where the delivery of care becomes more complex, post graduate care may be required. These situations include, but are not limited to
• Patient requires DCFS consent • Patient is ASA III or ASA II requiring multiple consultations • Patient has limited scheduling availability • Patient or family requires specific translation services
C. Behavior Based Distinctions
The primary distinguishing characteristic between dental student and pediatric dental resident care is the behavior of the patient. In general dental student care will be provided to patients with better behavior and those that are unable to be managed will be referred for pediatric dental resident care. This will vary based on the management skills of individual students, but in general
• Frankl 1 and 2 patients will be referred for pediatric dental resident care • Frankl 3 and 4 patients will remain to be treated by dental students • Patients requiring protective stabilization, oral conscious sedation, or general anesthesia
will be referred for pediatric dental resident care.

73 | P a g e
PHILOSOPHY of ORTHODONTIC TREATMENT
DEPARTMENT OF ORTHODONTICS
1. Definitions Following and adopting the American of Association of Orthodontists 2018 Guidelines (Appendix A), the basic treatment philosophy of the UIC Orthodontic Department start with DO NO HARM for the patients while providing evidence-based treatment to deliver individualized effective and efficient treatment.
2. Establishing Diagnosis, Problem List, Treatment Objectives and Treatment Plan a. Each treatment plan was established through a particular sequence which is
outlined in Appendix B (Diagnostic and Records Checklist) b. Degree of difficulty of cases was assess following American Board of
Orthodontists Discrepancy Index (DI) as outlined in Appendix C (Kusnoto) c. Diagnostic, problem list and creating of treatment objectives as well as treatment
plan will be based on the flowcharts as explained in Appendix D (Caplin/Sanchez) as well as Appendix E (Sanchez).
d. Establishment of mechanics and appliance design will be based on Appendix F – Mechanics Sequence (Kusnoto, Chwa, Sanchez, Caplin, Galang, Atsawasuwan, Belavsky, Benjamin, Yue)
3. Sequence of the clinical procedures – All clinical procedures
must be supervised by the same clinical instructor and consultants
a. Comprehensive Treatment Plan - review of the patient’s chief complaint - review of the medical and dental histories - review of any digital records in Axium, Dexis, Dolphin, OrthoCAD or any other
3rd Party software related to the establishment of the treatment plan such as ClinCheck, SureSmile, Incognito.
- Developing comprehensive treatment plan and mechanics (Appendix D, E, and F)
b. Treatment plan presentation for initial, progress is made with regard to the as treatment started and in progress. Duration of treatment depends on the severity of the problem and the amount of tooth movement desired, but with the efficient use of orthodontic appliances. Any interdisciplinary case MUST be discussed and combined/ interdisciplinary treatment plan must be discussed and approved by all faculty in each of the discipline involved.
c. Monitoring of treatment progress toward finishing
- Active caries and pulpal pathology must be eliminated. Restorations requiring detailed occlusal anatomy should not be placed until the orthodontic treatment is completed.
- Poor prognosis tooth should be removed unless the tooth will be used for gaining vertical alveolar bone height or thickness. If indicated, endodontic
74 | P a g e
treatment may be initiated. - Periodontal disease must be controlled before any orthodontic treatment
begins. Maintain good overall oral hygiene and periodontal maintenance
- For joint orthognathic surgical case please make sure to monitor decompensation procedure as well as arch coordination and interferences that might reduce the success of surgical outcome
- When indicated a remote monitoring system might be applied
d. Establish occlusion and root angulation - Establish good dental alignment and close spaces if needed. - Establish proper occlusion and stabilization phase for long-term stability - Establish good gingival harmony especially in a patient with gingival display. - Establish good implant space and root angulation for proper implant placement - Establish good intermaxillary space for proper clinical crown and/or crown/root
ratio - Establish good dental/periodontal structure for proper restorative preparation. - Establish good range of motion, protrusion, lateral excursion, opening.
e. Finishing and Detailing per ABO OGS criteria
- All cases must be evaluated in annual bases radiographically (panoramic and cephalometric radiograph) along with superimposition to evaluate the effect of treatment (mechanics) as well as growth modification (in growing patient). - At least 6-8 months towards the end of treatment when all major movements have been achieved, final finishing and detailing procedure as per ABO OGS criteria (Appendix G) as well as Appendix F (Kusnoto) need to be observed. Any necessary adjustments and repositions of brackets needs to be conducted. Any interdisciplinary cases MUST be re-visited and rediscussed for final action, such as implant placement, bone graft, periodontal issues, restoration, surgical etc.
- At the end of treatment, appropriate retention need to be delivered as well as final records (photos, radiographs, 3D intraoral scan) need to be obtained. Final presentation with superimposition need to be assessed by the supervising faculty in case-by-case bases.
f. Post-treatment phase
- Retention: An essix type of retainer is often the best choice immediately upon removing the orthodontic appliance removal. In most cases started with lower anterior crowding it is recommended to utilize lower fix bonded retainer L3-3 following orthodontic treatment. In case Hawley’s retainer with a pontic is indicated, the patient should have a definite plan for final restoration since the retainer should not be used as the patient’s final denture. Circumferential fiberotomy could be performed in severe rotated teeth. In extraction cases it is recommended to use circumferential hawley with stabilizing anterior wire. It is also recommended to check if patient need long term habit control such as tongue thrust. In this case, tongue crib can be incorporated to the hawley retainer.

75 | P a g e
Prepared by:
Dr. Phimon Atsawasuwan Dr. Budi Kusnoto Dr. Maria Therese Galang-Boquiren Dr. Jennifer Caplin Dr. Flavio Sanchez Dr. Mohammed Elnagar Dr. Kynt Chwa Dr. Isaac Yue Dr. Dale Benjamin Dr. Ben Belavsky

76 | P a g e
Guidelines for Crown Indication, Preparation and Cementation

77 | P a g e
GUIDELINE FOR ALL CERAMIC CEMENTATION
Factors Influencing the Durability of All-Ceramic
Restorations

78 | P a g e
Tooth substrates with bonding
techniques
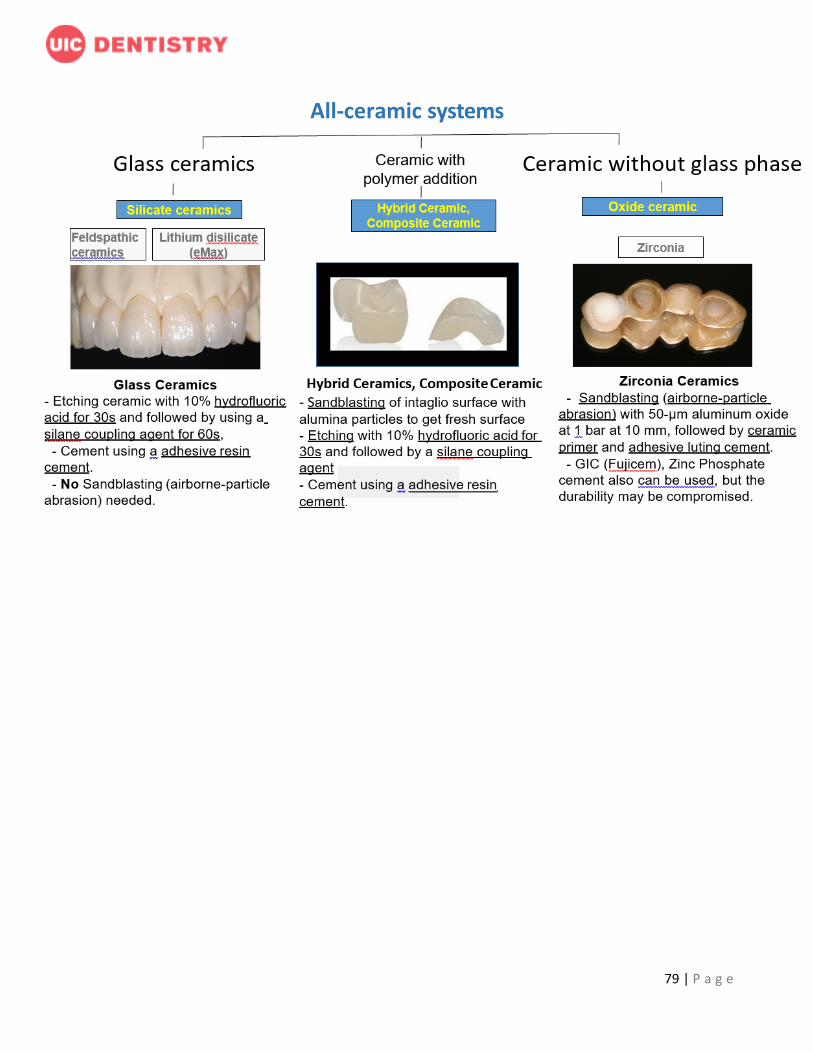
79 | P a g e
All-ceramic systems

80 | P a g e
Sandblasting Protocol and Machine Instruction
CLINICAL DECISION TOOLS: ANTIBIOTICS
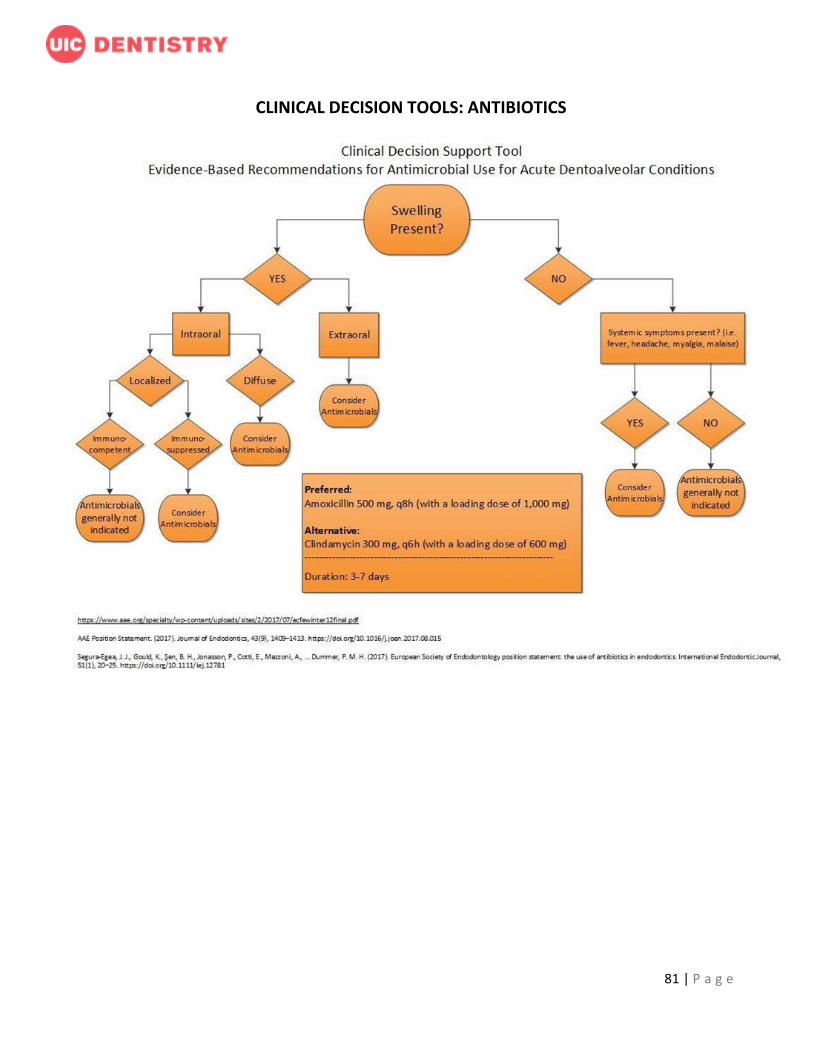
81 | P a g e
CLINICAL DECISION TOOLS: ANTIBIOTICS

82 | P a g e
http://www.orthoguidelines.org/go/auc/default.cfm?auc_id=224995&actionxm=Terms

83 | P a g e

84 | P a g e