power and privilege of patient and family centered care jim conway, ms adjunct faculty, hsph senior...
Post on 19-Dec-2015
216 views
TRANSCRIPT
Power and Privilege of Patient and Family Centered Care
Jim Conway, MSAdjunct Faculty, HSPH
Senior Fellow, [email protected]
1

Objectives
• Explore the power and privilege of providing patient and family centered care
• Examine the leadership behaviors necessary for patient and family centered care and to sustain patient experience change
2
OutlinePatient and Family Centered Care
• Why me talking about this?• Why are all of us talking about this?• What is it?• Up, down, and all around• Great examples, great work• Making it the way WE do the work• Resources
3

“I don’t care who you are. I’m going to stay with my child.”
Pediatric Mother, 1976
4

5
DANA-FARBER ADMITS DRUG OVERDOSE CAUSED DEATH OF GLOBE COLUMNIST, DAMAGE TO SECOND WOMANWhen 39-year-old Betsy A. Lehman died suddenly last Dec. 3 at Boston's Dana-Farber Cancer Institute, near the end of a grueling three-month treatment for breast cancer, it seemed a tragic reminder of the risks and limits of high-stakes cancer care. In fact, it was something very different. The death of Lehman, a Boston Globe health columnist, was due to a horrendous mistake: a massive overdose of a powerful anticancer drug that ravaged her heart, causing it to fail suddenly….
3/23/19955

The Time Is Now
If health and/or healthcare is on the
table, then the consumer (public,
patient, family member) must be at
the table, every table. NOW!
Lucian Leape Institute, 2008 6
http://content.hcpro.com/pdf/content/257750.pdf

Health Reform Priorities
1. Care coordination for chronic disease2. Overuse3. Palliative end-of-life care4. Patient and family engagement5. Population health6. Safety
7
http://www.nationalprioritiespartnership.org/Priorities.aspx
8

IOM: Patient and Family Centered Care
• Care based on continuous healing relationships • Customized according to patient needs and
values• Patient is the source of control• Knowledge is shared and information flows freely • Transparency is necessary• Needs are anticipated
9
IOM Crossing the Quality Chasm 2001

Four Key Concepts of PFCC
• Dignity and respect: Providers listen and honor patient and family perspectives and choices.
• Information sharing : Providers share complete and unbiased information in ways that are affirming and useful.
• Participation: In care and decision-making• Collaboration: In policy and program development,
implementation and evaluation, as well as the delivery of care
10
American Hospital Association and the Institute for Family-Centered Care. (2004). Strategies for leadership—Patient and family-centered care toolkit. Washington, DC.

It is also what clinicians want…
…it is why they went into health care.…it just isn’t designed into health care.
11
Question 1What are some examples of patient and
family centered care (personal and public engagement) already going on in your exam room, clinic, unit, or system?
Huddle for a few minutes with those around you?
12

The Chain of Effect inImproving Health Care Quality
Patient and Community ExperienceExperience
Aims (safe, effective, patient-centered, timely, efficient, equitable)
Micro-system ProcessProcessSimple rules/Design Concepts (knowledge-based, customized, cooperative)
Organizational Context
Facilitator ofFacilitator ofProcessesProcesses
Design Concepts (HR, IT, finance, leadership)
Facilitator ofFacilitator ofFacilitatorsFacilitators
Design Concepts (financing, regulation, accreditation, education)
Environmental Context
13Berwick D. Users Manual to the IOM Chasm Report http://content.healthaffairs.org/content/21/3/80.full.pdf
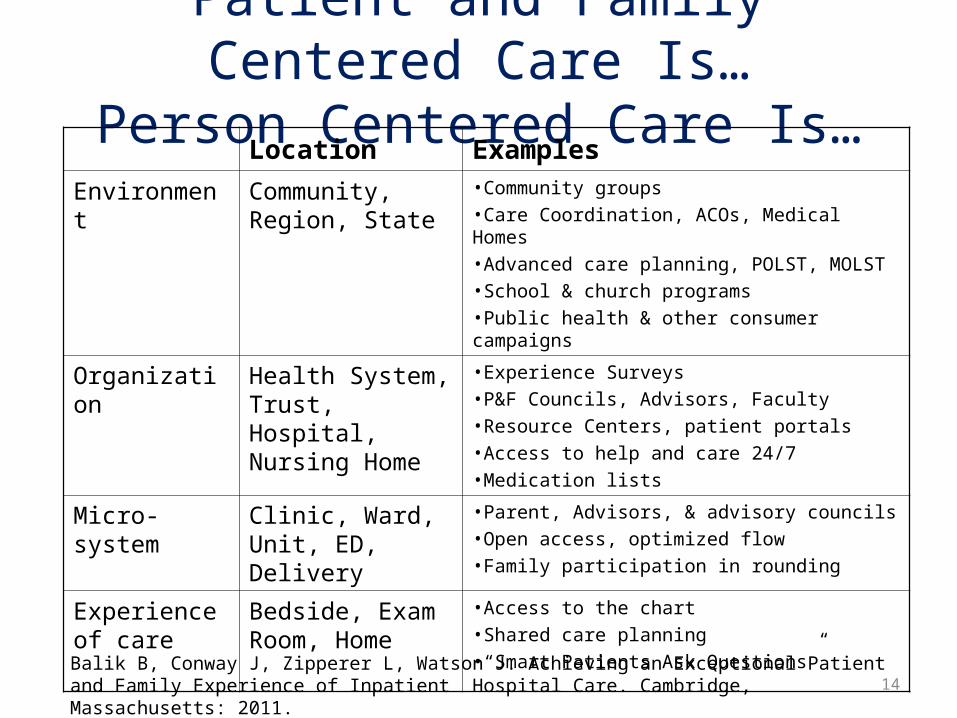
Patient and Family Centered Care Is…Person Centered Care Is…
Location Examples
Environment Community, Region, State
•Community groups•Care Coordination, ACOs, Medical Homes•Advanced care planning, POLST, MOLST•School & church programs•Public health & other consumer campaigns
Organization Health System, Trust, Hospital, Nursing Home
•Experience Surveys•P&F Councils, Advisors, Faculty•Resource Centers, patient portals•Access to help and care 24/7•Medication lists
Micro-system Clinic, Ward, Unit, ED, Delivery
•Parent, Advisors, & advisory councils•Open access, optimized flow•Family participation in rounding
Experience of care
Bedside, Exam Room, Home
•Access to the chart•Shared care planning•“Smart Patients Ask Questions”
14Balik B, Conway J, Zipperer L, Watson J. Achieving an Exceptional Patient and Family Experience of Inpatient Hospital Care. Cambridge, Massachusetts: 2011.

Patient and Family Centered Care Isn’t
Just ThreadsIt is a fabric of integrated, reinforcing strategies and partnerships•Community•Organization•Microsystem•Locus of care
15

DFCI: Overarching: Structures & Processes
• Committees:Board Quality CommitteePatient Safety CommitteeStrategic PlanningOperating
• Leadership Interviews• New Employee Orientation• Side by Side• Resource Centers• Rescue events• NPSF & IHI meetings
16

Business Case: Patient- and Family-Centered Care
“Nice but not necessary”X
17
And, the evidence keeps on coming!

Patient Experience Is Strongly Correlated With Other Key Outcomes
• Health outcomes– Patient adherence– Process of care measures– Clinical outcomes
• Business outcomes– Patient loyalty– Malpractice risk reduction– Employee satisfaction– Financial performance
Edgman-Levitan S., Shaller D. et al. The CAHPS Improvement Guide. Boston: Harvard Medical School: 2003. 18
Financial Benefits of Patient- Centered Care in Planetree
• Reduced length of stay• Lower cost per case• Decreased adverse events• Higher employee retention rates• Reduced operating costs• Decreased malpractice claims• Increased market share
Charmel P, Frampton S. Building the Business Case for Patient Centered Care. HFM. March, 2008
19

Conclusions. Most hospitalized patients participated in some aspects of their care. Participation was strongly associated with favorable judgments about hospital quality and reduced the risk of experiencing an adverse event.
20
Weingart SN, Zhu J, Chiappetta L, Stuver SO, Schneider EC, Epstein AM, David-Kasdan JA, Annas CL, Fowler FJ Jr, Weissman JS. Hospitalized patients' participation and its impact on quality of care and patient safety. Int J Qual Health Care. 2011 Feb 9. [Epub ahead of print] Center for Patient Safety, Dana-Farber Cancer Institute, Boston, MA, USA.

21
We found positive associations of FCC with improvements in efficient use of services, health status, satisfaction, access to care, communication, systems of care, family functioning, and family impact/cost. There was little available evidence, however, for some outcomes, including cost and transition.

Press Ganey Patient–Hospital Employee Loyalty Link
22

Question 2What are immediate
opportunities you see?Discuss your ideas for a
few minutes.
23

Culture Change
Nothing About Me, Without Me
24

The Challenge is Huge
Aiken C, Keller S, Rennie M. The Performance Culture Imperative . McKinsey & Company. 2007 25

Culture Defined
“What gets rewarded around here”“The way things get done when no
one (or is it when every one) is looking”
“What has made us successful”
26

The single most important factor that distinguishes major culture
changes that succeed from those that fail is competent leadership at the top. No single effort at culture
change has been successful starting at the bottom
John P. Kotter & James L. Heskett, Corporate Culture & Performance (Free Press 1992)
27

Behavior For AllIt’s a New Day; It’s a New Partnership• Asking
– What do you think? What works and what doesn’t?– Go on the affirmative; don’t wait for patients and family
• Respectful and Active Listening– Don’t need to defend or counter ever point
• Acting– Not expected to do everything but be able to explain why.– Meet patients and families where they are
• Respecting– Don’t ask me what I think if the decision is made.– Explain the decision
• Celebrating
28

Executive LeadershipMaking It the Way We Do the Work
• Strength and clarity of the vision– How does this fit with strategy?– This isn’t an if discussion, it’s a when and how
discussion– It isn’t a gift; it’s a right!– Staff look at you and think PFCC
• Positioning people for success with training, modeling, sharing
• If it’s about care, the patient and family are part of the conversation, all conversations
• If it is important to our patients and families, it is important to us, even if it is hard
• Accountability29

GovernanceNothing More Important
• Strength and clarity of expectation• Voice of the patient, and the
patient/family– Dashboard (inpatient, outpatient,
ED)– Board committee meetings– Strategic planning meetings– Walk-rounds– Community
• Hearing it unfiltered, blunt, direct, actionable
30

Department, Division, Work Unit, Physician, Clinical, Administrative Leadership
• Reinforce organizational vision; “It’s important to me”• Monitor, coach, and reinforce• Use respectful language when describing patient / family • Daily rounds (MBWA) with patients and families
– What’s working and what’s not? What’s getting in the way?
• Patient and family are part of executive and other walk rounds• Come on down
– “We’re trying to improve this… would you be interested in helping us?” “Do you have a moment to come to my staff meeting?”
31

In Daily Outpatient Clinical PracticeCare is Designed Around the Patient
A Few Examples• Who “schleps?”
– 80% of services in close vicinity for the patient• Who waits?
– 90% of patients seen in 20 minutes of arrival• Who sees who when?
– Scheduling is a decision made together among clinicians• Who is in the room with the patient?
– Up to the patient• What questions the patient wants answered today?
– Smart patients ask questions• Whose medical record?
– The patients. It’s their illness. 32

33
http://www.ihi.org/IHI/Results/WhitePapers/AchievingExceptionalPatientFamilyExperienceHospitalCareWhitePaper.htm
34

An IHI Resource CenterLeadership Response to
a Sentinel Event: Respectful, Effective Crisis Management
http://tinyurl.com/IHIEffectiveCrisisMgmt
“In the aftermath of a serious adverse event, the patient/family, staff, and community would all say,
‘We were treated with respect.’”
35

36

A Powerful EvolutionDo it to me.Do it for me.
Do it with me.Martha HaywardPatient Advocate

“Quality improvement begins with love and vision.Love of your patients
Love of your workIf you begin with technique,
improvement won’t be achieved.”
A. Donabedian, M.D38

Comments, Questions, Answers
"Do not go where the path may lead; go instead where there is no path and
leave a trail”Ralph Waldo Emerson
39

Sample Self Assessment Tools
• Family Voices– http://www.familyvoices.org/pub/projects/fcca_UsersGuide.pdf
• Institute for Family Centered Care. Strategies for leadership. Patient and Family Centered Care. A Hospital Self Assessment Inventory.
– http://www.aha.org/aha/content/2005/pdf/assessment.pdf.
• IHI. Patient- and Family-Centered Care Organizational Self-Assessment Tool. http://www.ihi.org/IHI/Topics/PatientCenteredCare/PatientCenteredCareGeneral/EmergingContent/PFCCOrgSelfAssess.htm
• American Hospital Association-McKesson Quest for Quality Prize® Criteria http://www.aha.org/aha/content/2008/pdf/2009Q4Qcriteria.pdf.
40

Other ResourcesAssociations and Groups• Joint Commission
– http://www.jointcommission.org/NewsRoom/NewsReleases/nr_08_04_10.htm
• Picker Institute– www.pickerinstitute.org
• IHI– www.ihi.org
• WHO Patients for Patient Safety– http://www.who.int/patientsafety/
patients_for_patient/en/• Institute for Family Centered Care
– www.familycenteredcare.org• Planetree
– www.planetree.org• Partnership for Healthcare Excellence
– www.partnershipforhealthcare.org • Consumers Advancing Patient Safety
– www.patientsafety.org • New Health Partnerships
– www.newhealthpartnership.org
• What ‘Patient-Centered’ Should Mean: Confessions Of An ExtremistBerwick Health Affairs.2009; 28: w555-w565
41