pre-eclampsia – possible to predict? - diva-portal.org563136/fulltext01.pdf · acta universitatis...
TRANSCRIPT

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2012
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 835
Pre-eclampsia – Possible
A Biochemical and Epidemiological Study
MARIE BOLIN
ISSN 1651-6206ISBN 978-91-554-8523-8urn:nbn:se:uu:diva-183394
to Predict?
of Pre-eclampsia
Dissertation presented at Uppsala University to be publicly examined in Rosénsalen,Akademiska sjukhuset ingång 95, Uppsala, Friday, December 14, 2012 at 09:00 for the degreeof Doctor of Philosophy (Faculty of Medicine). The examination will be conducted in Swedish.
AbstractBolin, M. 2012. Pre-eclampsia – Possible to Predict?: A Biochemical and EpidemiologicalStudy of Pre-eclampsia. Acta Universitatis Upsaliensis. Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty of Medicine 835. 66 pp. Uppsala.ISBN 978-91-554-8523-8.
Pre-eclampsia is a major cause of maternal and perinatal morbidity and mortality worldwide.A predictor of pre-eclampsia would enable intervention, close surveillance and timely delivery,and thereby reduce the negative consequences of the disorder.
The overall aim of this thesis was to study potential predictors of pre-eclampsia bybiochemical and epidemiological methods.
Angiopoietin-1 (Ang-1) and Angiopoietin-2 (Ang-2) are regulators of angiogenesis, whichis important for placental development. In a prospective and longitudinal study of a low-riskpopulation the Ang-1/Ang-2 ratio was evaluated. The Ang-1/Ang-2 ratio increased duringpregnancy in all women but at gestational week 25 and 28 the ratios were significantly lowerin women who later developed pre-eclampsia. The relevance of Histidine-rich glycoprotein(HRG), a protein with angiogenic properties, was furthermore evaluated. HRG levels decreasedin all women, with significantly lower levels at gestational week 10, 25 and 28 in womenwho later developed pre-eclampsia. Thus both Ang-1/Ang-2 ratio and HRG may predict pre-eclampsia.
To evaluate the predictive value of HRG in combination with uterine artery Doppler earlyin pregnancy a study was performed in a high-risk population. The results revealed that thecombination was better able to predict preterm pre-eclampsia than each marker individually,with a sensitivity of 91% at a specificity of 62%.
A possible association between hyperemesis gravidarum and pre-eclampsia, as well as otherplacental dysfunctional disorders, was investigated. Hyperemesis gravidarum may be caused byhigh levels of human chorionic gonadotrophin (hCG) and increased levels of hCG in the secondtrimester is associated with later development of pre-eclampsia. A cohort of all pregnancies inthe Swedish medical birth register between 1997 and 2009 was studied. After adjustment forconfounding factors an association between hyperemesis gravidarum in the second trimesterand preterm pre-eclampsia, placental abruption and infants born small for gestational age wasdemonstrated.
In conclusion, the ratio of Ang-1/Ang-2 as well as HRG in plasma may be potential predictorsof pre-eclampsia. Combination with uterine artery Doppler further increases the predictivevalue of HRG for preterm pre-eclampsia. Hyperemesis gravidarum in the second trimester maybe considered as a clinical risk predictor of pre-eclampsia and other placental dysfunctionaldisorders.
Keywords: pre-eclampsia, angiopoietin, histidine-rich glycoprotein, hyperemesis gravidarum
Marie Bolin, Uppsala University, Department of Women's and Children's Health, Akademiskasjukhuset, SE-751 85 Uppsala, Sweden.
© Marie Bolin 2012
ISSN 1651-6206ISBN 978-91-554-8523-8urn:nbn:se:uu:diva-183394 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-183394)

To my beloved family


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Bolin M, Wiberg-Itzel E, Wikström AK, Goop M, Larsson A, Olovsson M, Åkerud H. Angiopoietin-1/Angiopoietin-2 ratio for prediction of preeclampsia. American Journal of Hypertension. 2009;22(8):891-5
II Bolin M, Åkerud P, Hansson A, Åkerud H. Histidine-rich glycoprotein as an early biomarker of preeclampsia. American Journal of Hypertension. 2011;24(4):496-501
III Bolin M, Wikström AK, Wiberg-Itzel E, Olsson AK,
Ringvall M, Sundström-Poromaa I, Axelsson O, Thiliganathan B, Åkerud H. Prediction of preeclampsia by combining serum Histidine-rich glycoprotein and uterine artery Doppler. American Journal of Hypertension. 2012. Aug 16. doi: 10.1038/ajh.2012.112.[Epub ahead of print].
IV Bolin M, Åkerud H, Cnattingius S, Stephansson O, Wikström AK. Hyperemesis gravidarum and risks of placental dysfunction disorders: a population based cohort study. Submitted to British Journal of Obstetrics and Gynaecology.
Reprints were made with permission from the respective publishers.


Contents
Introduction ................................................................................................... 11 Background .............................................................................................. 11 History ...................................................................................................... 11 Definition ................................................................................................. 12 Epidemiology ........................................................................................... 13 Pathophysiology ....................................................................................... 13 Early-onset and late-onset pre-eclampsia ................................................. 16 Risk factors ............................................................................................... 16
Hyperemesis gravidarum, a possible clinical risk predictor ................ 17 Prevention and prediction of pre-eclampsia ............................................. 18
Biochemical predictors ........................................................................ 19 Angiopoietins ....................................................................................... 20 Histidine-rich glycoprotein .................................................................. 21 Accuracy of the biochemical predictors .............................................. 22 Biophysical markers ............................................................................ 23 Combined methods for prediction of pre-eclampsia ............................ 25 Gene expression ................................................................................... 26 Prophylactic treatment ......................................................................... 27
Aims .............................................................................................................. 29
Material and Methods ................................................................................... 30 Paper I and II ............................................................................................ 30
Study population .................................................................................. 30 Methods ............................................................................................... 30
Paper III .................................................................................................... 31 Study population .................................................................................. 31 Methods ............................................................................................... 32
Paper IV ................................................................................................... 32 Study population and exposure ............................................................ 32 Outcomes ............................................................................................. 33 Covariates ............................................................................................ 34
Results ........................................................................................................... 36 Paper I ...................................................................................................... 36 Paper II ..................................................................................................... 37 Paper III .................................................................................................... 39 Paper IV ................................................................................................... 41

Discussion ..................................................................................................... 44 Methodological considerations................................................................. 44 Angiopoietins ........................................................................................... 45 Histidine-rich glycoprotein....................................................................... 46 Pre-eclampsia and hyperemesis................................................................ 47 Prediction of pre-eclampsia, at present and in the future ......................... 49
Conclusions ................................................................................................... 52
Sammanfattning på svenska .......................................................................... 53
Acknowledgement ........................................................................................ 55
References ..................................................................................................... 58

Abbreviations
AFP Alfa fetoprotein Ang Angiopoietin AOR Adjusted odds ratio AUC Area under the curve BMI Body mass index CI Confidence interval ELISA Enzyme-linked immunosorbent assay GWAS Genome-wide association studies HbF Foetal haemoglobin hCG Human chorionic gonadotropin HRG Histidine-rich glycoprotein H-hCG Hyperglycosylated hCG ICD International classification of diseases MAP Mean arterial pressure MBR Medical birth register MoM Multiples of the median OR Odds ratio PAPP-A Pregnancy-associated protein A PI Pulsatility index PlGF Placental growth factor PP13 Placental protein 13 RI Resistance index ROC Receiver-operator characteristic sFlt-1 Soluble fms-like tyrosine kinase-1 SGA Small for gestational age SNP Single nucleotide polymorphism STMP Syncytiotrophoblast microparticles Tie Tyrosine kinase endothelial receptor VEGF Vascular endothelial growth factor


11
Introduction
Background Pre-eclampsia, a pregnancy-specific disorder, is one of the major causes of maternal and perinatal morbidity and mortality worldwide. Studies of the differences between normal pregnancies and those complicated by pre-eclampsia may give important information, useful for finding a possible predictor of pre-eclampsia. Identification of such a predictor would make intervention and close surveillance a possibility and, hopefully, reduce the negative consequences of the disorder.
History In the pre-Hippocratic Coan Prognosis XXXI there is a description of pre-eclampsia and its severe consequence eclampsia: “In pregnancy, drowsiness and headache accompanied by heaviness and convulsions are generally bad“.1 Later the presence of a circulating agent, a toxin of foetal or placental origin, was supposed to be the cause of eclampsia and the disease has been called “toxaemia of pregnancy”.2 It was not until the middle of the 19th cen-tury that the connection between eclampsia and proteinuria was made, and then, at the end of the same century, an association with hypertension was observed.1
We have had relatively well-functioning maternal health care in Sweden since the start of the 20th century, when blood pressure controls as well as screening for proteinuria were introduced.3 In 1948 less than 40% of the pregnant women in Sweden attended maternal health care clinics, but ten years later the attendance rate had increased to 82%.3 In Sweden, eclampsia was the prime cause of maternal mortality during the 1940s, accounting for 34% of the maternal deaths.4 During the 1950s maternal mortality due to eclampsia decreased significantly, which was achieved by improvements to antenatal and obstetrical care.4
Modern obstetric care has reduced the incidence of eclampsia in high-income countries. In Scandinavia the incidence of eclampsia is 0,05%.5 In low-income countries the incidence varies but a figure from WHO is 2,8%.6
Pre-eclampsia and eclampsia are still among the most important causes of maternal mortality, both in high- and low-income countries.6,7

12
Definition There has been a lack of consistency in the definition of pre-eclampsia8 and to be able to compare different studies and results a definition of hyper-tension and pre-eclampsia is required. The International Society for the Study of Hypertension in Pregnancy (ISSHP) has suggested the following definitions for study purposes but has also considered a proposal for clinical diagnostic criteria.9
Classification of hypertension in pregnancy • Pre-eclampsia - eclampsia • Gestational hypertension • Chronic hypertension (essential or secondary) • Pre-eclampsia superimposed on chronic hypertension
Research definition of pre-eclampsia • New onset of hypertension with a systolic blood pressure ≥140 and/or a
diastolic blood pressure ≥90 mm Hg after gestational week 20 AND
• Proteinuria ≥300 mg/24 hour or a spot urine protein/creatinine ratio ≥30 mg/mmol.
The blood pressure should return to normal postpartum.
Clinical definition of pre-eclampsia • New onset of hypertension with a systolic blood pressure ≥140 mm Hg
and/or a diastolic blood pressure ≥90 mm Hg AND de novo appearance of one or more of the following:
• Proteinuria ≥300 mg/24 hour or a spot urine protein/creatinine ratio ≥30 mg/mmol
• Renal insufficiency (creatinine ≥0,09 mmol/L or oliguria) • Liver disease (increased levels of liver transaminases and/or severe right
upper quadrant or epigastrical pain) • Neurological symptoms: convulsions (eclampsia), hyperreflexia with
clonus, severe headache with hyperreflexia, persistent visual distur-bances (scotoma)
• Haematological disturbances: thrombocytopenia, disseminated intravas-cular coagulation, haemolysis
• Foetal growth restriction The blood pressure should return to normal postpartum within 3 months.
Subtypes of pre-eclampsia There is still an inconsistency among the definitions of different subtypes of pre-eclampsia. Various classifications are used in the definition of mild, moderate and severe10 as well as early- and late-onset pre-eclampsia where

13
the dividing line varies from gestational week 32 to 37.11,12 Another classifi-cation of pre-eclampsia is preterm and term disorder, indicating pre-eclampsia with a preterm (before gestational week 37) or term delivery (at gestational week 37 or later).13
Epidemiology Pre-eclampsia complicates about 2-8% of all pregnancies and the syndrome results in more than 63,000 maternal deaths every year worldwide.6,14 The maternal mortality rate is highest in low- and middle income countries but pre-eclampsia is also a potentially life threatening condition in high income countries.7 Known complications related to pre-eclampsia are eclampsia, abruptio placentae with disseminated intravascular coagulopathy, cerebral haemorrhage, pulmonary oedema, hepatic failure, HELLP (Hemolysis Elevated Liver enzymes Low Platelet count) syndrome and acute renal failure.14,15
Pre-eclampsia increases perinatal mortality five-fold, with most deaths caused by iatrogenic prematurity.16 Preterm birth in itself is responsible for the majority of neonatal deaths and nearly one half of all cases of congenital neurologic disability.17 In the US pre-eclampsia is responsible for 15% of premature births.16 Another risk for the infants is intrauterine growth restric-tion. A study from Norway reveals that women with pre-eclampsia have a four times higher risk of having an infant small for gestational age (SGA) compared to normal pregnancies. If the disorder occurs in early pregnancy 53% of the infants are SGA.18 Furthermore, to be born SGA increases the risk of hypertension, diabetes and coronary heart disease as adults.19
Later in life, women who have had pre-eclampsia have an increased risk of early cardiac, cerebrovascular and peripheral arterial diseases and cardio-vascular mortality.20 Severe and recurrent hypertensive disorders during pregnancy have a stronger association with ischemic heart disease later in life compared with mild and non-recurrent disease.21
Pathophysiology The pathophysiology of pre-eclampsia is not precisely known but a two-step model that is widely accepted has been described.22 The physiological change during a normal pregnancy involves spiral artery remodelling. Trophoblasts invade and replace the arteries’ endothelial cells and induce arterial smooth muscle cell apoptosis, resulting in large nonvasoactive vessels.23 The first step in the model has been proposed to be abnormalities of either differentiation of morula to blastocyst or the differentiation of trophoblast to cytotrophoblast or syncytiotropho-blast,24 which may cause
14
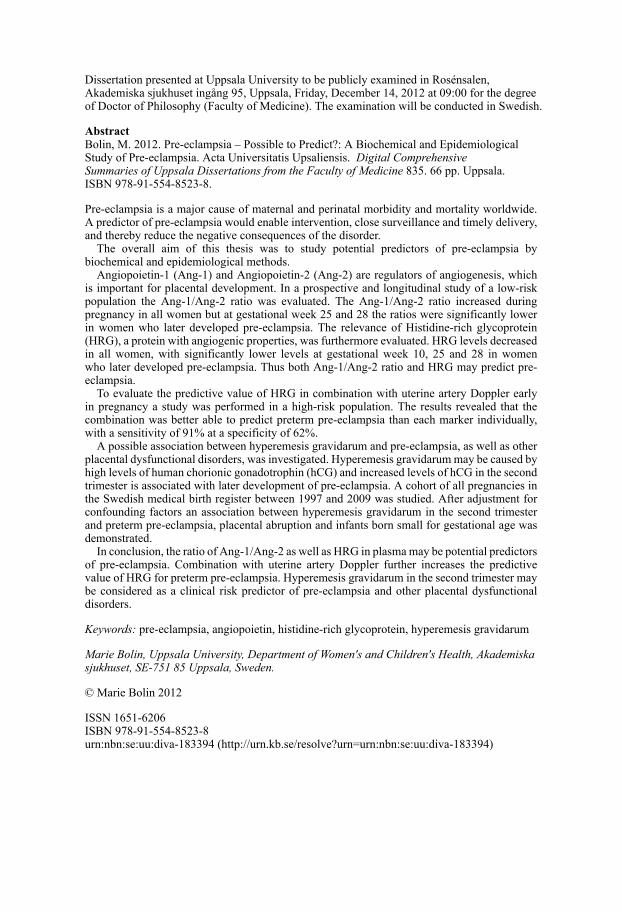
inappropriate invasion of trophoblasts into the spiral arteries, as illustrated in figure 1. The result is an inadequate placentation, followed by intermittent perfusion of the intervillous space and fluctuating levels of oxygen. Due to hypoxic-reoxygenation injuries, oxidative stress arises with widespread pla-cental lipid and protein oxidative modifications, mitochondrial and endo-plasmic reticulum stress and tissue apoptosis and necrosis. This may affect the formation of the syncytiotrophoblast as well as its turnover via its down-stream regulation of syncytin and Placental Growth Factor (PlGF). The hemodynamic changes in placenta increase the volume and alter the profile of the shed debris, for instance the syncytiotrophoblast microparticles (STMP), from the placenta to the maternal vasculature.25
Figure 1. Pathophysiological changes in pre-eclampsia. From Lam, C. et al. Hyper-tension 2005;46:1077-1085. Reprinted with permission from AHA Journals.
15
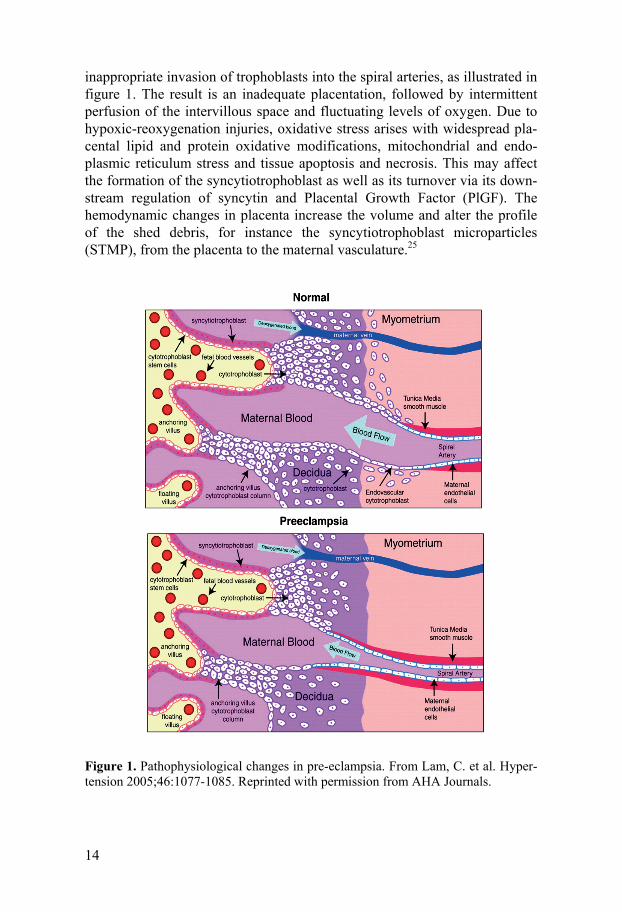
The second step in the model is characterized by a general systemic inflam-matory response of which endothelial dysfunction is a prominent part (figure 2).26 Oxidative stress is induced, which further stimulates the inflammatory process, forming the foundation for a positive feed-back system.27 A number of circulating factors that contribute to maternal endothelial dysfunction, increased vascular permeability and oxidative stress are identified; such factors are STMP, cytokines, apoptotic factors and anti-angiogenic factors.27 An activation of the coagulation cascade with formation of occlusive microthrombi is also a result of the endothelial dysfunction.16 The ability of the maternal system to handle the deficits in placentation and subsequent challenge to the maternal cardiovascular system partly depend on the immune system, as systemic inflammatory stress plays a key role in endo-thelial cell activation.25,27 Women with a pre-gestational endothelial dysfunction, such as pre-existing hypertension, obesity and dyslipidemi, have an increased risk of pre-eclampsia.
Figure 2. The two-step model of the pathophysiology of pre-eclampsia.
TrophoblastInadequate invasion
PlacentationIschemia-reperfusion
Oxidative stress
Components from the intervillous spacereleased into the
maternal circulation
Inadequate maternalresponse or removal
Endothelialdysfunction
Maternal factors
Increased placentalmass
Stage I
Stage II
Complementand clottingactivation
ProteinuriaHypertension

16
Early-onset and late-onset pre-eclampsia The heterogeneity of pre-eclampsia has drawn attention to the different characteristics of early- and late-onset pre-eclampsia with a suggested dividing line at 34+0 weeks.28 However the dividing line between early- and late- onset pre-eclampsia varies between different studies, from gestational week 28 to gestational week 37, which is a problem for interpreting the results.11,12 In a study from Norway early-onset pre-eclampsia, defined as delivery before 37 gestational weeks, comprises about 7% of all cases.12 Early-onset preeclampsia tends to be more severe for the mother and the foetus than late-onset pre-eclampsia.12,29 A stronger association with in-adequate and incomplete spiral artery remodelling has been proposed for early- compared with late-onset pre-eclampsia, which might be visualized by alterations in uterine Doppler artery profiles.30 These findings support the theory that early-onset pre-eclampsia more often has a placental origin, while late-onset pre-eclampsia is more related to maternal constitution that is susceptible to, or suffers from, microvasculature disease.31
There is morphological as well as molecular evidence that supports the theory that early- and late-onset pre-eclampsia is different with regard to pathophysiology. In a study from Egbor et al, placentas from women with early-onset pre-eclampsia were compared with late-onset examples and volume and total surface area of the terminal villi was significantly reduced in early-onset placentas compared to late-onset.32 Another study of placenta demonstrated a difference on molecular basis, since placentas from early-onset pre-eclampsia had a different oxygen sensing than placentas from late-onset pre-eclamspia and controls.33
Risk factors The known risk factors for pre-eclampsia are of multivariate origin. Not all studies have reported the same risks34 but one way to categorize the different risk factors is as in table 1.35
One of the strongest risk factors is a previous pregnancy with pre-eclampsia. The recurrence rate for pre-eclampsia varies widely between studies, but a rate up to 65% is described.36 The risk is related to gestational age at onset, the severity of pre-eclampsia, if the foetus was growth restricted or not and whether there are any underlying medical conditions with vascular or renal implications.37
Factors that reduce the risk of pre-eclampsia are a previous normal preg-nancy and smoking. However, the damaging effects of smoking on general health and perinatal outcomes outweigh the positive effect of lowered incidence of pre-eclampsia.37

17
Table 1. A categorization of risk factors for pre-eclampsia35
Risk factors
Maternal-specific risk factors: History of previous pre-eclampsia Maternal age, long interval between pregnancies Family history
Partner-related risk factors: Nulliparity/primipaternity Limited sperm exposure, donor insemination
Presence of specific underlying disorders: Chronic hypertension and renal disease Obesity, insulin resistance, low maternal birth weight Gestational diabetes, type-1 diabetes mellitus Activated protein C resistance (factor V Leiden), protein S deficiency Antiphospholipid antibodies
Pregnancy-associated risk factors Multiple pregnancy Foetus with chromosomal anomalies (trisomy 13) Hydatidiform moles
Hyperemesis gravidarum, a possible clinical risk predictor Hyperemesis gravidarum, a severe form of nausea and vomiting, is a preg-nancy complication which occurs in 0.5-3% of pregnancies.38,39 It is the most common cause of hospitalization in the first half of the pregnancy and the second cause of hospitalization for pregnancy overall.40 The aetiology of hyperemesis gravidarum is not fully understood but human chorionic gonadotropin (hCG) is often stated as the most likely cause since the highest incidense of hyperemesis gravidarum coincide with the peak level of hCG at gestational week 10-12 and conditions associated with higher levels of hCG, such as twins and molar pregnancies.41 These conditions are also predispos-ing for pre-eclampsia.35
As early as in an embryo with 8 cells, hCG-subunits are transcribed and are therefore suggested as possible key regulators of the implantation.42 Several variants of hCG are characterized. Hyperglycosylated hCG (H-hCG), secreted by syncytiotrophoblast, is a variant of hCG that stimu-lates trophoblast invasion and is the major form of hCG during the first weeks of pregnancy.43,44 HCG, secreteted by trophoblasts, has many

18
important functions during pregnancy including promotion of progesterone production, implantation and decidualization, angiogenesis, cytotrophoblast differentiation and immune cell regulation.44
Since hCG is of importance both for the invasion of trophoblasts and angiogenesis, which, in pregnancies complicated by pre-eclampsia and other disorders due to placental dysfunctional, are known to be insufficient, several studies have investigated the potential of hCG to predict these disorders.45-47
Low first trimester βhCG, which is a hyperglycosylated variant of the β-subunit of hCG, and increased second trimester hCG are associated with adverse obstetrical outcome.45-50
Elevated hCG levels in the second trimester could be due to a reduced production of (H-hCG) early in pregnancy, which results in an insufficient trophoblast migration into the spiral arteries, with a subsequent placental hypoxia that stimulates secretion of the pro-angiogenic hCG as a compensa-tory mechanism.51
As hCG levels may be both a cause and an effect of placentation, time of onset of hyperemesis gravidarum may be a clinical marker of risks of pre-eclampsia and other abnormal placentation disorders. In very early preg-nancy, high hCG levels may favour normal pregnancy development, while later in pregnancy, abnormal placentation may cause high hCG levels and thereby hyperemesis gravidarum.
A meta-analysis has reported an increased risk of SGA in women with hyperemesis gravidarum but pre-eclampsia was not evaluated.52 One previous study has described a weak association between pre-eclampsia and hyeremesis gravidarum but the number of women included was limited and preterm was not separated from term pre-eclampsia.53
Prevention and prediction of pre-eclampsia To prevent pre-eclampsia would be a very important contribution for maternal health. Prevention may be categorized into primary, secondary or tertiary, where primary prevention means avoiding occurrence of a disease, secondary prevention is interception of the process of the disease before clinical signs are observed and tertiary prevention means prevention of complications, which is more or less synonymous with treatment.35 Today, the only guaranteed primary prevention of pre-eclampsia is avoidance of pregnancy, although, there are identified risk factors, where intervention could allow primary prevention, such as maternal age, interval between pregnancies and maternal weight. Secondary prevention demands knowledge of the pathophysiological mechanism. Furthermore, the availability of techniques for early detection and intervention in the pathophysiological process are necessary. Tertiary prevention of pre-eclampsia is a proper

19
antenatal care which provides screening for hypertension and proteinuria, making intervention, such as timely delivery possible. With an organised antenatal care, such as is found in most high in-come countries, the maternal mortality and serious morbidity have decreased since the 1950s.35
The major value of secondary prevention would be to identify women at high risk of pre-eclampsia and make a medical intervention so that the disorder never occurs or is postponed. The ultimate predictor of pre-eclampsia should presumably identify women with an increased risk of the disorder as early as in the first trimester. The test should also be simple, rapid, non-invasive, inexpensive and the technology widely available. Fur-thermore it should be valid, reliable and reproducible with a high positive and a low negative likelihood ratio.54
Biochemical predictors
The biochemical predictors of pre-eclampsia studied so far reflect our knowledge of the pathophysiology of pre-eclampsia. Several potential predictors describe the foetal and placental endocrine functions and the maternal endothelial dysfunction, some of them will be presented below:55
Molecules from the trophoblasts Placental protein 13 (PP 13), expressed by the syncytiotrophoblasts, has been shown to be at a lower level in the first trimester in women who later develop early-onset pre-eclampsia compared to normal pregnancies.56 An inappropriate formation of trophoblasts may also produce a reduced amount of placenta derived proteins such as pregnancy-associated protein A (PAPP-A) in women later developing pre-eclampsia.57
The failure of trophoblast invasion may contribute to the alteration of the surface layer of the syncytiotrophoblasts and result in leakage of alfa fetoprotein (AFP) into the maternal circulation resulting in an increased level of these proteins in women with pre-eclampsia.58
Inhibin A and Activin A belong to the transforming growth factor β superfamily and are both elevated before the onset of pre-eclampsia. In women who develop early-onset pre-eclampsia the levels increased at an earlier gestational week than for women with late-onset pre-eclampsia.59
Foetal cells cross the placenta during pregnancy. In pregnancies where pre-eclampsia develops the amount of foetal cells and cell-free foetal DNA and RNA have been demonstrated to be higher than in normal pregnancies. This may be explained by placental necrosis and apoptosis and an impaired DNA elimination.60,61

20
Inflammatory markers Women who later develop pre-eclampsia have, compared to healthy preg-nancies, higher levels of C-reactive protein, a marker of cellular or immune activation, and Pentraxin 3, an inflammatory molecule expressed in response to inflammatory stimuli by a variety of cells including endothelial cells.62,63 Soluble tumour necrosis factor receptor 2 is another factor that reflects intra-vascular inflammation and has been shown to be increased in pre-eclampsia.64
Angiogenic and anti-angiogenic factors Pre-eclampsia is characterized by an imbalance between different factors that regulate vasculogenesis and angiogenesis. Vasculogenesis occurs mainly during foetal development when the formation of the vasculature derived from endothelial progenitor cells, angioblasts, form a primitive vascular network. Angiogenesis, development of new blood vessels from pre-existing ones, occurs during embryo implantation and placentation.65 In pre-eclampsia there is an imbalance in the angiogenic state where anti-angiogenesis dominates. A disturbed balance of these factors are proposed as one cause of the deterioration of the endothelial cell dysfunction and increased vascular permeability seen in pre-eclampsia.25
A variety of pro-angiogenic factors such as Vascular Endothelial Growth Factor (VEGF) and PlGF and anti-angiogenic factors i.e. soluble fms-like tyrosine kinase-1(sFlt-1) and Endoglin have been studied as potential markers of pre-eclampsia.66,67
In pregnancies subsequently developing pre-eclampsia, especially early-onset, lower levels of PlGF and higher levels of sFlt-1 and Endoglin have been demonstrated weeks before diagnosis. A combination of these factors has been shown to potentially improve the predictive value.67
To achieve higher predictive power not only combination of markers are of interest, also new potential predictors are of importance.
Angiopoietins Angiopoietins have been shown to be of importance during implantation and placentation.68,69 They are, together with the Ephrins and VEGF, important regulators of both vasculogenesis and angiogenesis.70 Angiopoietin-1 (Ang-1) regulates vascular maturation by recruiting and stabilizing attach-ment of pericytes.71-73 Angiopoietin-2 (Ang-2) is a natural inhibitor of Ang-1 and loosens the attachment of pericytes and stimulates angiogenesis in the presence of VEGF.71 Ang-1 and Ang-2 are expressed in syncytiotrophoblasts and endothelial cells in the placenta.68 The angiopoietins act via vascular tyrosine kinase receptors called Tie-1 and Tie-2, which are expressed pre-dominantly in endothelial cells.74 Factors related to the angiogenic balance,

21
such as the angiopoietins, could potentially be used as predictive biomarkers of pre-eclampsia.
By evaluating immunohistochemical staining on placenta performed in our laboratory at the Department of Women´s and Children´s Health in Uppsala, Ang-1 and Ang-2 were found to be present in endothelial cells as well as in the trophoblasts (figure 3). No staining was found in the stroma. Their corresponding receptors Tie-1 and Tie-2 were furthermore found at the same localisations in placental tissue (unpublished data). There was also a difference in staining intensity between Ang-1 and Ang-2, where Ang-1 was visualised with a higher intensity in the syncytiotrophoblasts compared to Ang-2. The intensity was on the other hand higher for Ang-2 in endothelial cells. No difference according to staining intensity was found related to Tie-1 or Tie-2.
Figure 3. Ang-1 (A), Ang-2 (B), Tie-1 (C) and Tie-2 (D) in normal placenta.
Histidine-rich glycoprotein In normal pregnancy, the vascular endothelial cell surface is thrombo-resistant and protects against clot formation. In pre-eclampsia however, endothelial cell dysfunction alters local anticoagulant properties, which in turn results in generally enhanced clot formation.26,75 The increased coagula-bility in the vasculature includes disturbances of the coagulation, as well as the fibrinolytic system.76 Enhanced activation of platelets and increased activity of factor VIII have been detected in pre-eclampsia.77-79
A B
C D
endothelial cells trophoblasts
endothelial cellstrophoblasts
endothelial cellsendothelial cells
trophoblaststrophoblasts

22
The coagulation system involves a number of different proteins, with the enzymatic cleavage of fibrinogen to fibrin as the important end point. During normal pregnancy, the plasma level of fibrinogen increases, but in women with pre-eclampsia the fibrinogen level is even higher.79-81 Fibrinogen is known to interact with Histidine-rich glycoprotein (HRG), a multi-domain protein involved in haemostasis as well as in the angiogenic pathway that has both angiogenic and anti-angiogenic properties.82,83
The anti-angiogenic effect of HRG has been suggested to be mediated by signal transduction targeting focal adhesions and thereby interrupting VEGF-induced endothelial cell motility.84 The pro-angiogenic effect could be expressed by modulation of the anti-angiogenic activity of thrombo-spondin.82
Apart from the known changes in the angiogenic/anti-angiogenic pathway and the coagulation/fibrinolysis system related to pre-eclampsia, the activated vascular endothelium is also known to trigger a generalized intra-vascular inflammatory reaction.85 HRG has been demonstrated to act as a negative acute phase reactant, since plasma levels are reduced as a response to tissue injury.86,87
HRG is present at high levels in plasma; it is synthesized by parenchymal liver cells and transported as a free protein as well as being stored in α-granules of platelets and released after thrombin stimulation.88 HRG has been found in embryos and it has been suggested that the embryo produces HRG, which may be of importance for placentation.89
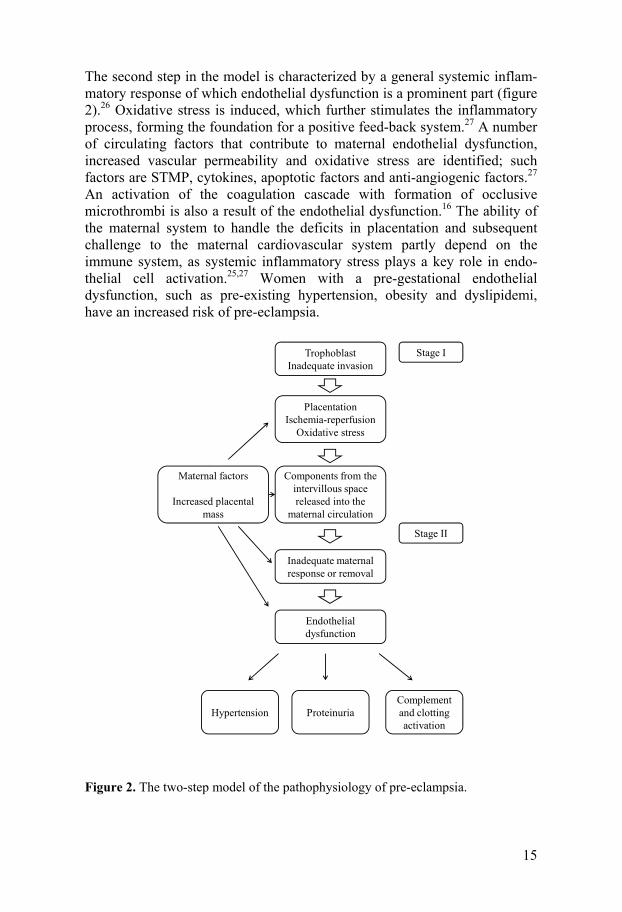
Accuracy of the biochemical predictors Despite several years of research in the field, a single test accurate enough to provide a screening tool for pre-eclampsia has not yet been found.54,90 A review91 of different biochemical markers for pre-eclampsia before the 25th week of gestation in cohort and case control studies revealed no test with a sensitivity and specificity over 90%. A summary of some of the biomarkers’ accuracy is presented in table 2.
When focusing on prediction of pre-eclampsia in the first trimester, a recent evaluation of biomarkers90 reveals that low levels of PP13, PlGF and PAPP-A and elevated levels of Inhibin A are significantly associated with the development of pre-eclampsia later in pregnancy. The sensitivity ranged from 22% to 83% at a specificity of 90%.
To improve the predictive value, a combination of biomarkers may achieve improved accuracy. An example is foetal haemoglobin (HbF)/Haemoglobin ratio and α1-microglobulin, that has demonstrated 90% sensitivity and 77% specificity for prediction of pre-eclampsia in early preg-nancy.92
23
Table 2. Biochemical predictors and their accuracy to predict pre-eclampsia91
Predictor Specificity % Sensitivity %
AFP 96 9
Fibronectin, total 94 65
Foetal DNA 88 50
hCG 89 24
Inhibin-A 95 30
Activin-A 89 61
PAPP-A 94 10
Kallikreinuria 98 83
Biophysical markers Normal placentation requires a trophoblastic invasion of the maternal decidua, myometrium and blood vessels. The spiral arteries thereby lose their musculoelastic coat, which allows blood to flow with low resistance into the intervillous space. This process starts in the first trimester and is more or less completed at the end of the second trimester.93 Abnormal placentation, as seen in pre-eclampsia, is associated with in-adequate uteroplacental blood flow. Doppler ultrasonography might be used to assess the velocity of uterine blood flow and thereby indirectly evaluate the trophoblastic invasion of the spiral arteries.94 Histopathological findings of decreased endovascular trophoblast invasion have been demonstrated to be associated with high-resistance uterine artery Doppler indices.95
Several different Doppler indices are used to evaluate the blood flow and the most commonly used are:
• Pulsatility Index (PI): peak systolic flow minus end diastolic flow divided by mean flow
• Resistance index (RI): peak systolic flow minus end diastolic flow divided by peak systolic flow
• Notching: presence of early diastolic notching indicating de-creased early diastolic flow compared to later diastolic flow in the uterine artery (figure 4)

24
Low end-diastolic velocities and an early diastolic notch characterize the waveforms of uterine artery blood flow in non-pregnant and early pregnant women. Abnormal flow velocity ratios and a persistent diastolic notch after gestational week 24 have been associated with inadequate trophoblast inva-sion.96
Figure 4. Uterine artery Doppler without and with a notch. The notch is indicated by an arrow. Reprinted with permission from Eva Bergman, MD, PhD, Department of Women’s and Children’s health, Uppsala University.
A systematic review of the ability of uterine artery Doppler ultrasonography to predict pre-eclampsia revealed that pre-eclampsia is best predicted by an increased pulsatility index (PI) with diastolic notching in the second trimester.96 In table 3 and 4 a summary based on this review is presented.

25
Table 3. The best uterine artery Doppler indices and their accuracy in the first tri-mester96
Population Pre-eclampsia
Doppler indices
Sensitivity (%)
Specificity (%)
Positive likelihood ratio
Negative likelihood ratio
Low risk Overall
PI 95 5.4 0.78 25
Severe
PI 40 90 4.0 0.67
High risk Overall
Notching 91 46 1.7 0.20
Severe Notching 91 46 1.7 0.20
Table 4. The best uterine artery Doppler indices and their accuracy in the second trimester96
Population Pre-eclampsia
Doppler indices
Sensitivity (%)
Specificity (%)
Positive likelihood ratio
Negative likelihood ratio
Low risk Overall
PI and Notching
23 99 7.5 0.59
Severe
PI 78 95 15.6 0.23
High risk Overall
Notching 96 20.2 0.17 83
Severe RI 80 78 3.7 0.26
Combined methods for prediction of pre-eclampsia Since pre-eclampsia is characterized by a complex pathophysiology with heterogeneous clinical and laboratory findings, it may not be realistic to search for a single marker to predict the disorder. A combination of two or more independent markers, each representing separate pathophysiological processes, should theoretically improve the possibility for predicting pre-eclampsia with a high degree of accuracy.
A systematic review by Giguere et al97 showed that a combination of bio-chemical and ultrasonographic markers might improve the prediction of pre-eclampsia. In low risk populations several combinations, including PP13, PAPP-A, a disintegrin and metalloproteinase (ADAM), activin A or inhibin A measured in the first or early second trimester, combined with uterine artery Doppler investigation, showed a sensitivity of 60-80% and a

26
specificity of >80%. A combination of PP13 and uterine artery Doppler showed a sensitivity of 90% and a specificity of 90 % for severe pre-eclampsia in a high risk population.
Another review by Kuc et al,90 where first trimester predictors were evaluated, concluded furthermore that the combination of biomarkers and uterine artery Doppler ultrasound predicted pre-eclampsia better than a single predictor. The sensitivities varied between 38% and 100% at a specificity of 90%.
Taking into account maternal characteristics such as previous pregnancy with pre-eclampsia, maternal age, diabetes mellitus, hypertension and obesity, prediction of pre-eclampsia might be improved in the first trimes-ter.98 Women developing pre-eclampsia later have higher systolic blood pressure and mean arterial pressure (MAP) before the onset of clinical dis-ease.99 In a review, MAP has been demonstrated to be a better predictor of pre-eclampsia than systolic and diastolic blood pressure.100 The combination of maternal characteristics in the first trimester, including mean arterial pressure, uterine artery pulsatility index and the biochemical markers PAPP-A and PlGF in the first trimester has revealed predictive values with 95% specificity and 93% sensitivity for early-onset and 36 % for late-onset pre-eclampsia.101 Another large study combine maternal character-istics, including mean arterial pressure, uterine artery pulsatility index and the biochemical markers PAPP-A, PlGF, PP13, sEndoglin, Inhibin-A, Activin-A, Pentraxin 3 and P-Selectin. The result at 95% specificity was, for early-onset 91% sensitivity, intermediate onset 79% sensitivity and late-onset pre-eclampsia 61% sensitivity.102
Gene expression Prevalence of pre-eclampsia – eclampsia in certain families indicates a genetic contribution to the disorder.103 Whether the susceptibility for pre-eclampsia depends on a single gene or multiple ones has been debated.104
The technique of whole genome microarrays opens up new possibilities in the search for gene(s) contributing to the development of pre-eclampsia. Through genome-wide association studies (GWAS) it is possible to find single nucleotide polymorphism (SNP) that is associated with a disease and indicates a region of the human genome which influences the risk of the specific disorder. Studies of populations with different ancestors have demonstrated a common maternal pre-eclampsia locus on chromosome 2, although at different positions.105-107
To evaluate which genes in the genome are expressed, studies of RNA transcriptions are performed. A comparison of maternal blood from women developing early onset severe pre-eclampsia with blood from women with healthy pregnancies, has demonstrated 72 genes either up- or down-regulated in women with pre-eclampsia.108 The differential gene expression

27
of placentas with inadequate placentation, according to existing notch with Doppler ultrasonography, indicates that the progression of pre-eclampsia may be driven by induction of pro-inflammatory genes, in contrast to those pregnancies that did not develop pre-eclampsia.109
To predict pre-eclampsia, genetic studies could focus on SNPs associated with well known risk factors, such as vascular disease, to find a possible SNP that could predict pre-eclampsia110 but, at present, no specific SNP has yet been identified for this role.
Another approach is to further investigate the protein products of the genes of interest. Up-regulated HbF genes and accumulation of HbF protein in placentas from women that developed pre-eclampsia have been demon-strated.111 These findings support the case for further studies of HbF as a possible predictor of pre-eclampsia.
Prophylactic treatment The pathophysiology of pre-eclampsia is not sufficiently well characterized to provide a specific prophylactic treatment. However, several studies have investigated the potential effect of antiplatelet agents, i.e. low dose aspirin <75 mg.112,113 Antiplatelet drugs have anti- inflammatory properties and affect the imbalance of prostacyklin and tromboxane seen in pre-eclampsia.114 A Cochrane review described that aspirin was associated with an overall 17% reduction in the risk of pre-eclampsia, with a number needed to treat of 72. The risk reduction in a high risk population was higher, with a number needed to treat of 19.115 Another review113 revealed a major reduc-tion of preterm pre-eclampsia when treatment with low dose aspirin was initiated before or at 16 weeks of gestation. Treatment with low dose aspirin seems, furthermore to be safe, with few known side effects on the mother and child.112,116
Another possible prophylactic treatment for pre-eclampsia is calcium supplementation. In a Cochrane review it was concluded that a daily intake of at least 1g calcium reduced the risk of pre-eclampsia by about 50%.117 The effect was most obvious in women with a predicted high risk according to known risk factors and also in women with a low dietary calcium intake. Although the incidence of pre-eclampsia was reduced, there was no clear reduction in severe pre-eclampsia, eclampsia or admission to intensive care.
Supplementation of calcium seems to reduce blood pressure and may also affect the uteroplacental blood flow by lowering the resistance index in uterine and umbilical arteries.118 Supplementation of calcium is relatively cheap and the substance is already available on the market. It is likely to be safe for both the woman and the foetus, though more studies are required.117
In placentas from women with pre-eclampsia, thrombotic lesions have been observed.119 To prevent the vascular pathology, the possible prophylactic role of anti-thrombotic agents, such as low molecular weight

28
heparin, have been studied. Promising results, with a reduction of pre-eclampsia and eclampsia, have been described but the number of studies and participants included were small.120 To date, prophylactic treatment is not recommended but further research is required.
In conclusion, medical intervention, with aspirin as well as calcium, seems to be possible, indicating that a screening test would be of importance.

29
Aims
• to analyse whether there is a difference in the ratio between Ang-1 and Ang-2 throughout pregnancy between women who develop pre-eclampsia and those who do not and, furthermore, to determine if the ratio between Ang-1 and Ang-2 can be used as a predictor of pre-eclampsia in a low risk population
• to analyse whether there is a difference in circulating levels of
HRG throughout pregnancy between women who develop pre-eclampsia and those who do not and, furthermore, to determine if HRG can be used as a predictor of pre-eclampsia in a low risk population
• to determine if the combination of HRG and uterine artery
Doppler ultrasonography in early pregnancy can be used as a predictor of pre-eclampsia
• to investigate if there is an association between hyperemesis
gravidarum in the first or second trimester and pre-eclampsia as well as other placental dysfunction disorders

30
Material and Methods
Paper I and II Study population A cohort of healthy pregnant women (n = 469) was enrolled in gestational week 8–12 at five participating prenatal centres in the county of Värmland, Sweden, during autumn 2004–spring 2007. Only women with singleton pregnancies were recruited. Women with a concurrent diagnosis such as chronic hypertension, episodes of high blood pressure before pregnancy, persistently elevated blood pressure before the 20th week of gestation, upper urinary tract infection, pre-existing renal disease, diabetes mellitus, and drug abuse were not included.
Plasma samples were collected in lithium/heparin containing tubes at gestational weeks 10, 25, 28, 33 and 37.
Pre-eclampsia was defined as new-onset hypertension (≥140/90 mm Hg) observed on at least two separate measurements ≥6 h apart, combined with proteinuria (≥2 on a dipstick or in a 24h urine sample showing ≥300 mg/24 h). Clinical and laboratory routine parameters were registered.
The studies were approved by the regional Ethics Committee of the Medical Faculty of Uppsala University, and informed consent was obtained from each patient included in the study.
Methods
Measurement of Ang-1, Ang-2 and HRG in plasma Plasma samples were analysed for levels of Ang-1 and Ang-2 by enzyme-linked immunosorbent assay (ELISA) using commercially available kits.
HRG was analysed by an ELISA set up in the laboratory of the Department of Women’s and Children’s Health, Uppsala University.
31
Statistics All statistical analysis was performed by the SPSS 15.0 for Windows soft-ware package (SPPS, Chicago, IL). Among the background variables a chi-square test was used for proportions. For comparisons of median values a Mann–Whitney U test was used for independent samples and for mean values students t-test was used.
The Kaplan-Meier method was used to illustrate time to onset of pre-eclampsia in gestational week 25 by using a cut-off value of the ratio.
All significance tests were two-tailed. P-values ≤0.05 were considered as statistically significant. Receiver–operator characteristic (ROC) curves were constructed to test arbitrarily chosen Ang-1/Ang-2 and HRG cut-off values for predicting pre-eclampsia.
Paper III Study population The patients were recruited between 2002 and 2005 as part of an ongoing prospective study of Doppler ultrasound and serum markers for pre-eclampsia in women attending a routine antenatal care visit at St. George’s Hospital Obstetric Unit, London. Multiparas with a high risk profile, such as essential hypertension, previous pregnancy with pre-eclampsia or intra-uterine growth restriction and all primiparas were included. Pregnancy out-comes were obtained from the delivery suite database or from general practitioners.
The study was designed as a case-control study and involved 175 women who were randomly selected from the cohort: 86 women with an un-complicated pregnancy (controls) and 89 women who developed pre-eclampsia (cases).
Maternal blood was collected in non-heparinized tubes. The blood sam-ples were on average collected at gestational week 14.
Patient characteristics including demographics, smoking status, and obstetric and medical history were obtained from women at the first hospital visit and entered into a foetal medicine unit database.
Pre-eclampsia was defined as two recordings of blood pressure of 140/90 mmHg or greater at least 4 hours apart and proteinuria of 300 mg or more within 24 hours, or two readings of at least 2 on dipstick analysis of urine if a 24-hour collection was not available, and developed after 20 weeks of gestation.
32
Women with pre-eclampsia who were delivered in gestational week 37 or later were defined as term pre-eclampsia and women who were delivered before 37 weeks of gestational age were defined as preterm pre-eclampsia.
Approval was obtained for the study from the local Research Ethics Committee at Wandsworth, UK, and all women gave written, informed consent prior to inclusion.
Methods
Doppler ultrasound As part of routine antenatal scans, uterine artery PI was abdominally measured in the first or second trimester of those women who gave their permission. The ultrasound examination was, on average, performed at gestational week 14+6 and in 159 of the 175 women Doppler indices were registered.
The uterine artery PI was expressed as multiples of the median (MoM) to correct for changes in the normal values with gestational age.
Measurement of HRG in serum HRG was analysed by an ELISA set up in the laboratory of the Department of Women’s and Children’s Health, Uppsala University.
Statistics All statistical analyses were performed by SPSS 18.0 for Windows software pack (SPSS, Chicago, IL, USA). Comparisons between different continuous variables were made with Student’s t-test and a Chi-square-test was used for proportions. Non-normally distributed variables were compared by Mann-Whitney U test. A receiver-operator characteristic (ROC) curve was constructed to determine the best cut-off values of HRG and PI for prediction of pre-eclampsia. Two tailed p-values<0.05 were considered as statistically significant.
Paper IV Study population and exposure From the Swedish Medical Birth Register (MBR) a cohort was created of singleton births, born at a gestational age of 22 weeks or more, where the pregnancy was estimated to have started January 1st 1997 or later and resulted in a birth December 31st 2009 or earlier. The MBR includes prospectively collected information, including demographic data,

33
reproductive history and complications during pregnancy, delivery and the neonatal period among more than 98% of all births in Sweden. Complica-tions during pregnancy and delivery are classified according to the Inter-national Classification of Diseases (ICD), as noted by the responsible doctor at discharge from hospital after delivery. Individual record linkage between the MBR and other registers is possible through each individual’s unique personal registration number.
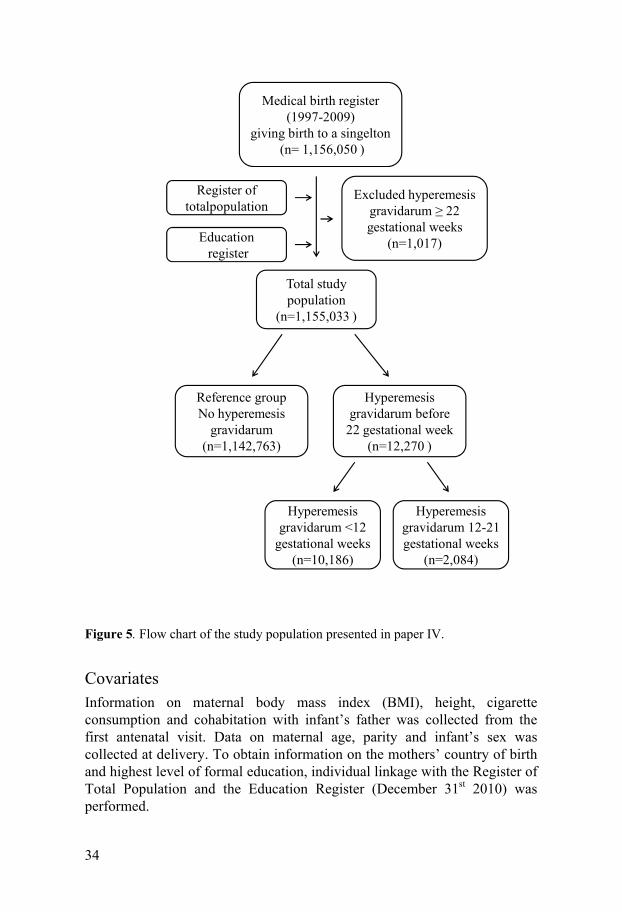
1,156,050 pregnancies were included. The exposure variable was admis-sion to hospital because of hyperemesis gravidarum. Information on expo-sure was collected through linkage to the nation-wide Patient Register, which includes information on dates of hospital admissions and discharges and diagnoses, which are classified according to ICD codes.
13,287 pregnancies with at least one admission for hyperemesis gravidarum were identified. Pregnancies with a first admission to hospital for the exposure at 22 gestational weeks or later (n=1,017) were excluded.
Pregnancies with hyperemesis gravidarum were stratified into first trimes-ter hyperemesis gravidarum, defined as first admission to hospital before 12 completed gestational weeks (n=10,186), and second trimester hyperemesis gravidarum with a first admission between 12 and 21 completed gestational weeks (n=2,084).
The final study population included 1,155,033 pregnancies, of whom 12,270 (1.1%) were exposed to hyperemesis gravidarum before 22 gesta-tional weeks (figure 5).
Outcomes The outcomes were pre-eclampsia, placental abruption, stillbirth and SGA. Pre-eclampsia was categorized into preterm (birth before 37 gestational weeks) and term (birth at 37 gestational weeks or later). We had no informa-tion on gestational age at onset of pre-eclampsia in the MBR. Gestational age was assessed by ultrasound scans or, if no early second trimester ultra-sound scan was available, the last menstrual period was used to calculate gestational age at delivery.
Pre-eclampsia was defined as a blood pressure more than or equal to 140/90 mm Hg combined with proteinuria (> 0.3 g/24 hours) occurring after 20 weeks of gestation.
Placental abruption was defined as premature separation of the placenta and identified by ICD codes. Stillbirth was defined as a foetal death occur-ring at 28 weeks of gestation or later. SGA was defined as a birth weight of 2 standard deviations or more below the mean birth weight for gestational age according to the sex-specific Swedish foetal growth curve. When analyzing risk of SGA, we excluded stillbirths and births with missing or misclassified information on birth weight and/or gestational age (n=5,036), leaving 1,146,142 births in the study population.
34
Figure 5. Flow chart of the study population presented in paper IV.
Covariates
Information on maternal body mass index (BMI), height, cigarette consumption and cohabitation with infant’s father was collected from the first antenatal visit. Data on maternal age, parity and infant’s sex was collected at delivery. To obtain information on the mothers’ country of birth and highest level of formal education, individual linkage with the Register of Total Population and the Education Register (December 31st 2010) was performed.
Medical birth register (1997-2009)
giving birth to a singelton(n= 1,156,050 )
Excluded hyperemesisgravidarum ≥ 22 gestational weeks
(n=1,017)
Total studypopulation
(n=1,155,033 )
Educationregister
Register of totalpopulation
Hyperemesisgravidarum before
22 gestational week (n=12,270 )
Reference groupNo hyperemesis
gravidarum(n=1,142,763)
Hyperemesisgravidarum 12-21 gestational weeks
(n=2,084)
Hyperemesisgravidarum <12
gestational weeks(n=10,186)

35
Information on presence of maternal hyperthyreosis was collected at the discharge from the delivery hospital. Further, information on pre-gestational diabetes and chronic hypertension was collected from the first antenatal visit and at discharge from delivery hospital.
Statistical analysis Risks of pre-eclampsia, placental abruption, stillbirth and SGA were calculated for women admitted to hospital because of hyperemesis gravidarum, using women without admission for hyperemesis gravidarum as reference. Odds Ratios (OR) with 95% confidence intervals (CI) were calculated using the generalized estimation equation (PROC GENMOD) method, since observations are not independent in women who delivered more than once during the study period. Adjustments were made for maternal factors associated with risks of the exposure and outcomes, including maternal age, parity, BMI, height, smoking, cohabitation with infant’s father, infant’s sex, mother’s country of birth, education, presence of hyperthyreosis, pre-gestational diabetes and chronic hypertension. Adjustments were also made for year of infant birth, categorized into 1997-2001, 2002-2005 and 2006-2009.
All statistical analyses were performed with Statistical Analysis Software version 9.1 (SAS Institute, Inc., Cary, NC).

36
Results
Paper I Nineteen women who developed pre-eclampsia and 43 women with a normal pregnancy were randomly selected from the study population. There were no significant differences between the groups according to maternal age, parity and body mass index.
Plasma levels of Ang-1 and Ang-2 The levels of Ang-1 and Ang-2 varied during pregnancy. The median Ang-1/Ang-2 ratio increased in all women as shown in figure 6. The ratios were significantly lower at gestational week 25 and 28 in women who later developed pre-eclampsia than in normal pregnant women (1.48 compared to 2.19 and 2.12 compared to 3.54, p<0.05 and p<0.05). After gestational week 28 the Ang-1/Ang-2 ratio was still lower in women who developed pre-eclampsia compared to women with normal pregnancy, but the difference was not statistically significant.
Figure 6. Median values of the Ang-1/Ang-2 ratio in women with normal pregnan-cies (filled circles) and in women developing pre-eclampsia (unfilled circles) at different gestational weeks.
Gestational week
An
g-1/
An
g-2
10 25 28 33 370
2
4
6

37
Cut-off value for prediction of pre-eclampsia ROC curves regarding the prediction of pre-eclampsia at arbitrarily chosen Ang-1/Ang-2 cut-off values were constructed for gestational week 25 and week 28, as illustrated in figure 7. A cut-off value of 1.41 for the Ang-1/Ang-2 ratio at gestational week 25 showed a sensitivity of 47% and a specificity of 87% to predict pre-eclampsia later in pregnancy. A cut-off value of 1.84 in gestational week 28 for the Ang-1/Ang-2 ratio resulted in a sensitivity of 50% and a specificity of 80%.
Figure 7. ROC curve illustrating the Ang-1/Ang-2 ratio (a) in gestational week 25 and (b) in gestational week 28. Area under the curve (AUC) is 0.71 and 0.72 respec-tively.
Paper II From the cohort, 20 women who developed pre-eclampsia and 44 women randomly selected from the group of normal pregnancies delivered at term were included. There were no significant differences between the groups according to maternal age, parity and body mass index.

38
Plasma levels of HRG during pregnancy The results indicated that the mean HRG levels decreased as the pregnancy proceeded in all women, irrespective of whether they developed pre-eclampsia or not (figure 8). However, in the group of women who developed pre-eclampsia the levels of HRG were significantly lower in gestational week 10, 25 and 28 compared to women with a normal healthy pregnancy (40.1 µg/mL vs 55.9 µg/mL p<0.05, 30.1 µg/mL vs 42.8 µg/mL p<0.05 and 25.6 µg/mL vs 33.8 µg/mL p<0.05).
Figure 8. Mean levels of HRG in women with normal pregnancies (filled circles) and in women developing pre-eclampsia (unfilled circles) at different gestational weeks.
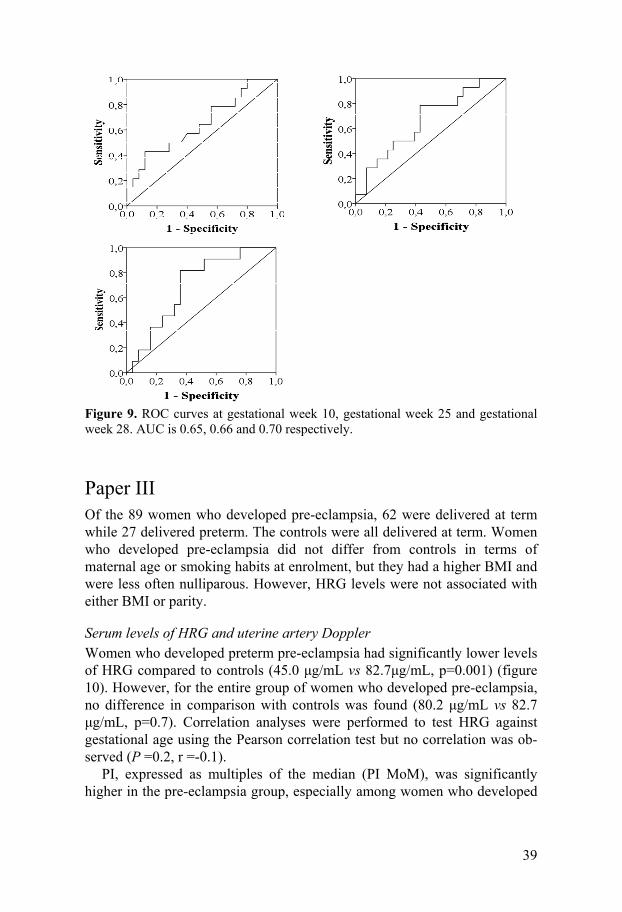
Cut-off values for prediction of pre-eclampsia ROC curves regarding the prediction of pre-eclampsia at arbitrarily chosen HRG cut-off values were constructed, as demonstrated in figure 9. A cut-off value of 49.1 µg/mL for HRG at gestational week 10 showed a sensitivity of 79% and a specificity of 44% to predict pre-eclampsia later in pregnancy, with an accuracy of 79%. For gestational week 25 a cut-off value of 32.7 µg/mL showed a sensitivity of 79% and a specificity of 57%. At gestational week 28 a cut-off value of 27.5 µg/mL gave a sensitivity of 82% and a speci-ficity of 64%.
Gestational week
HR
G (μ g
/ml)
10 25 28 33 370
20
40
60
39
Figure 9. ROC curves at gestational week 10, gestational week 25 and gestational week 28. AUC is 0.65, 0.66 and 0.70 respectively.
Paper III Of the 89 women who developed pre-eclampsia, 62 were delivered at term while 27 delivered preterm. The controls were all delivered at term. Women who developed pre-eclampsia did not differ from controls in terms of maternal age or smoking habits at enrolment, but they had a higher BMI and were less often nulliparous. However, HRG levels were not associated with either BMI or parity.
Serum levels of HRG and uterine artery Doppler Women who developed preterm pre-eclampsia had significantly lower levels of HRG compared to controls (45.0 μg/mL vs 82.7μg/mL, p=0.001) (figure 10). However, for the entire group of women who developed pre-eclampsia, no difference in comparison with controls was found (80.2 μg/mL vs 82.7 μg/mL, p=0.7). Correlation analyses were performed to test HRG against gestational age using the Pearson correlation test but no correlation was ob-served (P =0.2, r =-0.1).
PI, expressed as multiples of the median (PI MoM), was significantly higher in the pre-eclampsia group, especially among women who developed

40
preterm pre-eclampsia compared with controls (1.1 vs 1.0, p<0.05 and 1.6 vs 1.0, p<0.001) (figure 10).
Figure 10. Boxplots showing the median serum levels of HRG (µg/ml) and PI MoM for controls and preterm pre-eclampsia. The top and the bottom of the boxes repre-sent the third and the first quartiles. The horizontal line within the box represents the median value. The bars on the side of the box represent the highest and the lowest value. Extreme values are withdrawn but included in the statistical analysis.
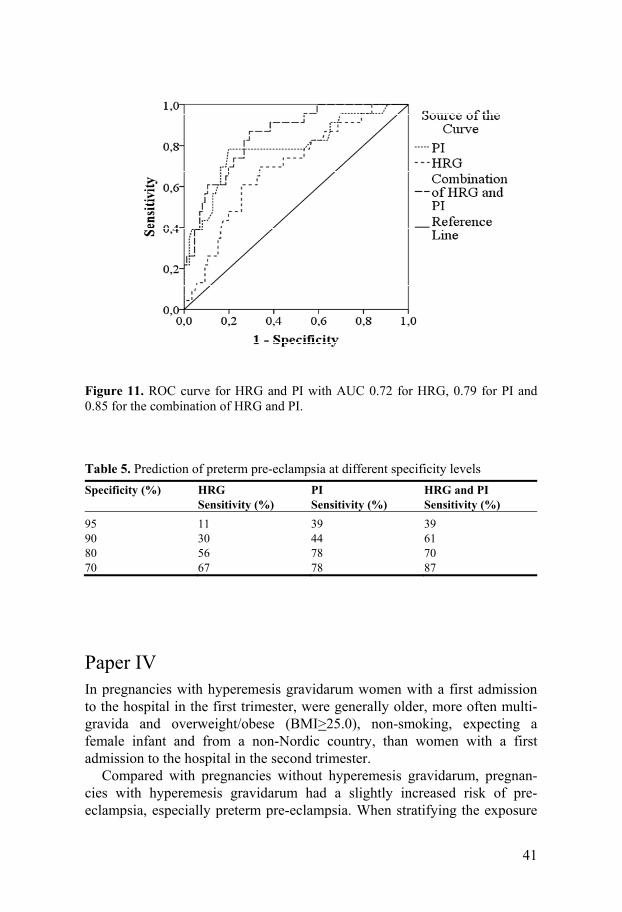
Cut-off value for prediction of pre-eclampsia ROC curves for HRG, PI MoM and a combination of HRG and PI MoM were constructed (figure 11). Sensitivities at different specificity levels for prediction of preterm pre-eclampsia were obtained. The AUC was 0.72 (95% CI, 0.61-0.83; p=0.001) for HRG, 0.79 (95% CI, 0.67-0.90; p<0.001) for PI MoM and 0.85 (95% CI 0.77-0.93; p<0.001) for the combination of HRG and PI MoM.
For prediction of preterm pre-eclampsia a suggested optimal cut-off value for HRG<67.8 μg/mL had a sensitivity of 74% and a specificity of 66%, whereas a cut-off value for PI MoM>1.3 had a sensitivity of 78% and a specificity of 81%. The highest values for prediction were found using the combination of HRG and PI MoM with a sensitivity of 91% and a specificity of 62%. As an alternative to the optimal cut-off value the predictive value of the combination of HRG and PI MoM could be presented as a detection rate of 39% and 61%, at a false positive rate of 5% and 10% respectively (table 5).
41
Figure 11. ROC curve for HRG and PI with AUC 0.72 for HRG, 0.79 for PI and 0.85 for the combination of HRG and PI.
Table 5. Prediction of preterm pre-eclampsia at different specificity levels
Specificity (%)
HRG Sensitivity (%)
PI Sensitivity (%)
HRG and PI Sensitivity (%)
95 11 39 3990 30 44 6180 56 78 7070 67 78 87
Paper IV In pregnancies with hyperemesis gravidarum women with a first admission to the hospital in the first trimester, were generally older, more often multi-gravida and overweight/obese (BMI>25.0), non-smoking, expecting a female infant and from a non-Nordic country, than women with a first admission to the hospital in the second trimester.
Compared with pregnancies without hyperemesis gravidarum, pregnan-cies with hyperemesis gravidarum had a slightly increased risk of pre-eclampsia, especially preterm pre-eclampsia. When stratifying the exposure

42
into first and second trimester hyperemesis gravidarum, the strongest association between hyperemesis gravidarum and pre-eclampsia was observed between second trimester hyperemesis gravidarum and preterm pre-eclampsia, where a more than two-fold increased risk was seen (table 6).
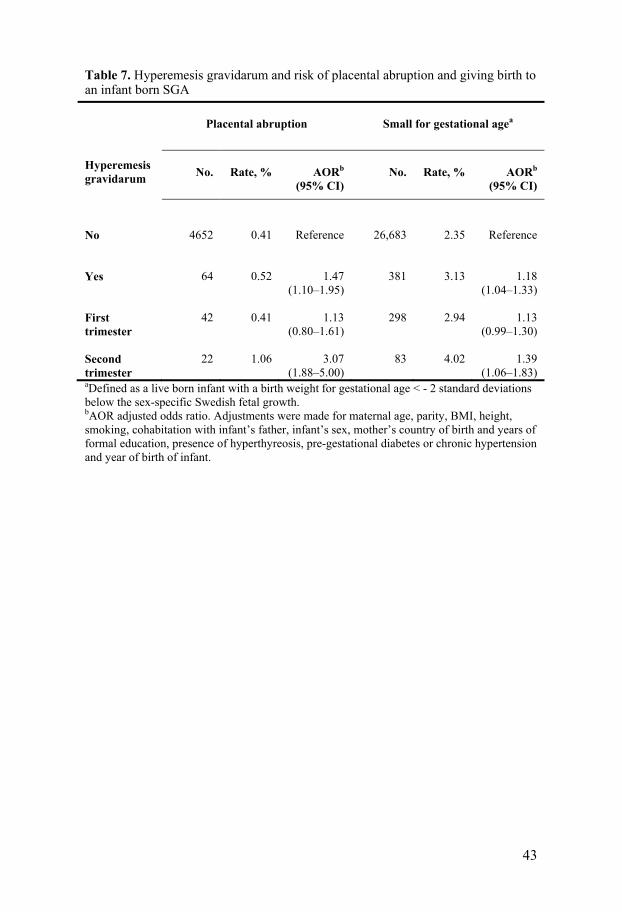
Compared with pregnancies without hyperemesis gravidarum, pregnan-cies with hyperemesis gravidarum were associated with an almost 50 % increased risk of placental abruption and a slightly increased risk of an SGA birth. When stratifying the exposure into first and second trimester hyperemesis gravidarum, the strongest risks were again observed for second trimester hyperemesis gravidarum, which was associated with a more than three-fold increased risk of placental abruption and a 39% increased risk of SGA. First trimester hyperemesis gravidarum was not significantly associated with placental abruption and SGA (table7). No association be-tween hyperemesis gravidarum and stillbirth was found.
Table 6. Hyperemesis gravidarum and risk of preterm and term pre-eclampsia
Hyperemesis gravidarum
Preterm (<37 weeks)
Pre-eclampsia
Term (≥37 weeks)
Pre-eclampsia
No.
Rate, %
AORa
(95% CI)
No.
Rate, %
AORa
(95% CI)
No
7,322
0.6
Reference
24,525
2.1
Reference
Yes
101
0.8
1.36
(1.09–1.70)
273
2.2
1.13
(0.98–1.30) First trimester
72
0.7
1.19
(0.91–1.55)
222
2.2
1.16
(0.99–1.35) Second trimester
29
1.4
2.09
(1.38–3.16)
51
2.4
1.01
(0.73–1.40) aAOR adjusted odds ratio. Adjustments were made for maternal age, parity, BMI, height, smoking, cohabitation with infant’s father, infant’s sex, mother’s country of birth and years of formal education, presence of hyperthyreosis, pre-gestational diabetes or chronic hypertension and year of birth of infant.
43
Table 7. Hyperemesis gravidarum and risk of placental abruption and giving birth to an infant born SGA Hyperemesis gravidarum
Placental abruption
Small for gestational agea
No.
Rate, %
AORb
(95% CI)
No.
Rate, %
AORb
(95% CI)
No
4652
0.41
Reference
26,683
2.35
Reference
Yes
64
0.52
1.47
(1.10–1.95)
381
3.13
1.18
(1.04–1.33) First trimester
42
0.41
1.13
(0.80–1.61)
298
2.94
1.13
(0.99–1.30) Second trimester
22
1.06
3.07
(1.88–5.00)
83
4.02
1.39
(1.06–1.83) aDefined as a live born infant with a birth weight for gestational age < - 2 standard deviations below the sex-specific Swedish fetal growth. bAOR adjusted odds ratio. Adjustments were made for maternal age, parity, BMI, height, smoking, cohabitation with infant’s father, infant’s sex, mother’s country of birth and years of formal education, presence of hyperthyreosis, pre-gestational diabetes or chronic hypertension and year of birth of infant.

44
Discussion
Methodological considerations Pre-eclampsia is one of the major causes of maternal and perinatal morbidity and mortality worldwide. A predictor of pre-eclampsia would make intervention, close surveillance, early diagnosis and timely delivery possible and thereby reduce the negative consequences of the disorder.91
When new biomarkers of pre-eclampsia are investigated, where differ-ences throughout pregnancy are likely to occur, a longitudinal approach to the collection of samples is preferable. In our studies presented in papers I and II, women from a low-risk population were prospectively included at enrolment to maternal care and blood samples were collected in gestational weeks 10, 25, 28, 33 and 37, according to general procedures for antenatal care in Sweden. This longitudinal approach is a major strength of our studies since it allowed us to follow the women through the pregnancy and, further-more, allowed us to investigate whether there were specific differences in women who developed pre-eclampsia compared to healthy controls. We could, in addition, identify at which gestational week the differences between the groups seemed to happen, which was how we evaluated whether the marker was a potential predictor of pre-eclampsia or not. In our total study population 469 women were included. Of these, 22 were diagnosed with pre-eclampsia and 44, out of 302 women with healthy pregnancies delivered at term, were randomly selected as controls. The study population selected is rather unique, since, compared with other studies where bio-markers of pre-eclamspia have been investigated, cohorts with a cross-sectional approach dominate. With a cross-sectional cohort, it is not possible to detect changes throughout pregnancy, although the number of patients in these studies can be larger than in longitudinal studies. One limitation with our studies is that the number of women included was relatively small and larger prospective studies are needed to determine whether our findings related to the Ang-1/Ang-2 ratio, as well as levels of HRG, can be used as clinically relevant predictors. In follow-up studies it might be relevant to study analyses related to early- and late- onset pre-eclampsia, as well as levels of the potential predictors in a gestational week between week 10 and 25.
Major strengths of the study presented in paper IV are the large sample size and the nationwide population-based design, where data was collected

45
prospectively which precludes recall biases. The large sample size made it possible to stratify hyperemesis gravidarum by trimester of hospitalization, and to study rare adverse outcomes, such as preterm pre-eclampsia and placental abruption. We were also able to control for a substantial number of possible confounders even if we cannot exclude that our findings may partly be due to unmeasured confounding.
One weakness of our study presented in paper IV is the lack of informa-tion on debut of symptoms of hyperemesis gravidarum. Information on maternal diet, weight loss or insufficient weight gain during pregnancy was not available. Weight loss/low weight gain during pregnancy has been shown to be a risk factor for delivery of an SGA infant, but has a negative association with pre-eclampsia risk why we doubt that the results regarding pre-eclampsia are influenced by the weight loss. There are no national guide-lines for hospitalization of women with hyperemesis gravidarum and the threshold for admission to hospital could vary between different regions, hospitals and doctors. However the proportions of women hospitalized due to hyperemesis was about the same throughout the study years which indicate that the handling of these patients was rather constant and not influenced by changes in the health care system.
Angiopoietins Angiopoietins are important in both vasculogenesis and angiogenesis and are involved in both implantation and placental development.68-70 Since pre-eclampsia seems to be a disorder characterized by an imbalance in the angiogenic – anti-angiogenic state67 the relation between Ang1 and Ang 2 is of interest. According to our study presented in paper I, there is a significant difference at gestational week 25 and 28 in the Ang-1/Ang-2 ratio in normal pregnancies and pregnancies later developing pre-eclampsia.
Our theory that the levels of the angiopoietins differ in normal pregnan-cies compared to pregnancies that develop pre-eclampsia is supported by research in the placental field. VEGF has been shown to be of importance in vasculogenesis, angiogenesis and the development of placenta.121 A number of publications have focused on the importance of the angiopoietins which act together with VEGF.68,69 Increased levels of both VEGF and Ang-1 mRNA have been demonstrated in the placenta during normal pregnancy, but the level of Ang-2 mRNA was decreased.122 It has also been reported that the angiopoietins and their receptors are crucial in the development of the early placenta.68 Furthermore, in consistent with the theory of inadequate placentation leading to subclinical placental hypoxia, a reduction of pO2 has been shown to up-regulate Ang-2 and VEGF mRNA, but not the expression of Ang-1 or the Tie-2 receptor.69,123,124

46
In a study with a cross-sectional design, where women were included at onset of clinical signs of pre-eclampsia, levels of Ang-2 in serum were analysed and a significant difference in women with pre-eclampsia compared to normal pregnancy was demonstrated.125 These results are not comparable to ours since their blood samples were collected at the onset of clinical signs of pre-eclampsia while ours are collected prospectively and longitudinally before the onset of clinical symptoms.
In another study where levels of angiopoietins at gestational week 12-15 and 16-20 were evaluated, women with subsequent pre-eclampsia compared with controls had a higher level of Ang-2 in gestational week 16-20, while the Ang-1 levels did not differ.126 When subgroup analyses were made, the increased level of Ang-2 was only found in women with a later, severe pre-eclampsia and women with a subsequent intrauterine growth-restricted foetus. These results support our findings of a lower Ang-1/Ang-2 ratio in women who later develop pre-eclampsia.
Our results indicate that the angiopoietins might be involved in the development of pre-eclampsia and support the theory of an angiogenic imbalance. In the current field of research where biomarkers of pre-eclampsia are investigated, early prediction of pre-eclampsia is the main focus. It would be interesting to perform further studies that describe the Ang-1/Ang-2 ratio between gestational weeks 10 and 25 to find when the difference becomes significant between women who develop pre-eclampsia and healthy controls.
Histidine-rich glycoprotein In addition to the angiogenic imbalance, demonstrated by the angiopoietins above, an excessive inflammatory response and hypercoagulability have been documented in pregnancies complicated by pre-eclampsia.26,85 HRG is a protein that interacts with all these processes,127 a fact that stimulates inter-est for further investigation into its role in the development of pre-eclampsia, as well as its potential as a predictor of pre-eclampsia. Our results in paper II revealed that plasma levels of HRG decrease during pregnancy in general, with significantly lower levels in gestational weeks 10, 25 and 28 in women who later develop pre-eclampsia, compared to women with a normal preg-nancy.
HRG has previously been measured, although with another method of analysis, in normal pregnancies where blood samples from different women at gestational weeks 27 to 42 were analysed.128 In that study, levels of HRG decreased during the third trimester, which is consistent with our findings. In addition, a study of women in the third trimester described lower HRG levels for women who had developed pre-eclampsia compared to normal

47
pregnancy, but without a significant difference.129 We did not have a signifi-cant difference in HRG levels between normal pregnancies and pregnancies later complicated by pre-eclampsia at neither gestational week 33 nor 37. However, our study has increased understanding of HRG levels, since we followed women with both normal pregnancies and those later complicated by pre-eclampsia through the whole pregnancy.
We know that HRG is expressed in embryos89 and is present in placenta80 but its exact function remains to be elucidated. Our results in paper II revealed a possibility that HRG could be a predictor as early as in gestational week 10.
The suitability of HRG for predicting pre-eclampsia might be improved when combined with uterine artery Doppler measurements or in combination with other markers. In cooperation with St George’s University we were able to perform the study presented in paper III, where we demonstrated that separate measurements of HRG and PI may predict preterm pre-eclampsia, but by combining HRG and PI the accuracy increased. These results are in line with studies proposing a combination of biochemical and biophysical markers for a successful prediction of pre-eclampsia in early pregnancy.90
Early-onset pre-eclampsia has been proposed to have a stronger associa-tion with inadequate and incomplete trophoblast invasion and spiral artery remodelling than late-onset pre-eclampsia.30,31 In a previous study an association between placental HRG and early-onset pre-eclampsia has been demonstrated80, whereas in this study we present an association between HRG serum level and preterm, but not term, pre-eclampsia.
Both uterine artery Doppler and HRG concentration may reflect the impaired trophoblast invasion per se but since HRG is a negative acute phase reactant, the lower levels could also be a reflection of the inflammatory response described in pre-eclampsia. A combination of tests reflecting the same pathogenic phase in pre-eclampsia may improve the accuracy, but a combination of tests that mirror different aspects of the disorder could achieve an even higher predictive power. Further studies are needed to confirm our results and the use of additional markers might further improve the predictive values.
Pre-eclampsia and hyperemesis Hyperemesis gravidarum is, according to our results in Paper IV, associated with increased risks of pre-eclampsia, placental abruption, and SGA birth. These risks were especially associated with hospitalization due to hyperemesis gravidarum in the second trimester. As pre-eclampsia, placental abruption and SGA birth are associated with abnormal placentation,130,131

48
our findings indicate an association between abnormal placentation and hyperemesis gravidarum manifested in the second trimester.
The finding of an increased risk of pre-eclampsia for women with hyperemesis gravidarum is in agreement with one former study.53 Our study has increased understanding about the association between the disorders, since we separated preterm from term pre-eclampsia. The discovery of a stronger association between hyperemesis gravidarum and preterm rather than term pre-eclampsia suggests that hyperemesis gravidarum is associated with abnormal placentation. In addition, after stratifying hyperemesis gravidarum by hospitalization in the first or the second trimester, we could clearly show that it is hyperemesis gravidarum in the second trimester that is associated with preterm pre-eclampsia risk and accordingly with abnormal placentation.
Earlier studies report an association between high levels of total hCG in the second trimester and risk of pre-eclampsia and SGA birth.45 Our findings are in agreement with these studies, since hyperemesis gravidarum is associ-ated with high levels of hCG.41 The high levels of hCG in the second trimester could be a compensatory mechanism to an insufficient early trophoblast migration and invasion of the spiral arteries51, which could be due to a low level of H-hCG, the variant of hCG that stimulates invasion in very early pregnancy.43 Thus, abnormal placentation may cause high levels of hCG in the second trimester, which then causes hyperemesis gravidarum with a late onset.
There are also other possible explanations to our findings. Hyperemesis gravidarum is a classical example of an interaction of biological and psycho-social factors.132 There are associations with both high thyroxin and estradiol levels.133 HCG is structurally similar to thyroid-stimulating hormone and an increased production of thyroxin is associated with hyperemesis gravidarum. Women with second trimester hyperemesis might have a prolonged or delayed stimulation of thyroxin, compared to women with first trimester hyperemesis. This might affect placentation, since former studies have shown an association between hyperthyreosis and placental dysfunction disorders.134 Pre-eclampsia is mostly associated with low estradiol levels, and we therefore doubt that estradiol is a link between these disorders.135
An epidemiological study cannot explain why hyperemesis gravidarum with a late onset could be associated with placental dysfunction disorders but hyperemesis gravidarum in the second trimester may be a clinical risk predictor to consider when predicting the risk of pre-eclampsia and other disorders associated with abnormal placentation.

49
Prediction of pre-eclampsia, at present and in the future Prediction of pre-eclampsia, which would make possible early detection and give the opportunity to intervene by correcting the pathophysiological changes, demands increased knowledge about the process that leads to the development of pre-eclampsia. Through studies of potential predictors we have learned more about the pathophysiology of pre-eclampsia.
A reliable predictive test would help us to individualize the level of surveillance during pregnancy. It is, though, important to remember that there are a number of, mainly low-income, countries around the world, where the majority of the maternal and perinatal complications related to pre-eclampsia appear, that would benefit from just a better and well-functioning maternal care. However, an easy and sensitive predictive test would help to save lives, even in poorer countries, since this could help the midwife to recommend the woman to come for more frequent controls and maybe also to be delivered at a hospital. In high-income countries a predictor of pre-eclampsia could be used to prevent or postpone the disorder by prophylactic treatment.
To be able to intervene with defects in implantation and placentation that might lead to increased risk of pre-eclampsia, the ultimate predictor should be able to identify women with an increased risk as early as in the first trimester. Since pre-eclampsia is a very heterogenous disorder, a predictive test should be constructed by using different markers of importance that reflect different aspects of the pathogenesis. Potential components of such a combination could be anamnestic risk factors, angiogenic, inflammatory and other biochemical factors, uterine artery Doppler and MAP. We postulate that the biochemical markers HRG and the Ang-1/Ang-2 ratio that we have studied would be interesting to study in a combined model for prediction of the disease. Hyperemesis gravidarum in the second trimester as a clinical risk predictor could also be considered, as demonstrated in our epidemio-logical study.
It has been discussed which category of patients a test should be capable of identifying and, since women with early-onset pre-eclampsia often have worse symptoms and a more severe disease, it might be postulated that this category would be of interest to focus on. This would make it possible to offer prophylactic treatment and increased surveillance, which presumably should be more cost effective with a reduced maternal and foetal morbidity and mortality as a consequence. Potentially, it should be possible to construct a predictive test for pre-eclampsia of a placental origin by includ-ing biochemical factors that reflect different steps of inadequate implantation and/or placentation in combination with uterine artery Doppler. Pre-eclampsia with a maternal origin could possibly be identified with a relatively high sensitivity and specificity by a combination of known risk factors and MAP.

50
The combination of biophysical methods and several other factors makes the tests more expensive and several of the tests use technologies that are not widely available. In low-income countries there is a need for more studies of potential predictors that use simple and inexpensive technology, as well as non-invasive screening methods such as dipstick tests of urine. Some studies have investigated the potential to use urinary analyses for prediction of pre-eclampsia136-138 although the results have varied.
The theory that hyperemesis gravidarum in the second trimester is induced by high levels of hCG, which is increased as a compensatory mechanism to low H-hCG early in pregnancy, has aroused interest in H-hCG as another potential predictor of pre-eclampsia. In contrast to hCG produced by syncytial trophoblast, extravillous trophoblast secretes H-hCG that has been demonstrated to stimulate invasion.43 H-hCG levels, in serum and in urine, seem to be a reliable test to diagnose pregnancies after in vitro fertili-sation treatment as early as six days after embryo transfer, and, in addition, to separate whether a pregnancy is a clinical pregnancy or a biochemical pregnancy.139 As a predictor of pre-eclampsia, lower levels of H-hCG in the urine have been demonstrated in the second trimester for women who later developed pre-eclampsia compared with normal pregnancies.136 Since H-hCG is of importance from the very beginning of the implantation and is the most common form of hCG during the first weeks afterward, it is an interesting potential predictor. An advantage is the possibility for detecting H-hCG in urine in very early pregnancy. Further studies of the ability for H-hCG to predict pre-eclampsia early in pregnancy would be of interest.
In the search for new potential predictors of pre-eclampsia, GWAS offers, new possibilities to screen the human genome and further evaluate different gene expressions. The result of genetic studies could either be a specific SNP as a predictor of pre-eclampsia or a protein or molecule that the different gene expressions are coding for.
For screening tests in general a premium is placed on a low rate of false positive results but for pre-eclampsia a false negative result could pose a high risk and therefore a somewhat lower specificity than usual should be accepted.91 Suggested cut-off values out of the ROC curves in study II and III were chosen to prioritize a high sensitivity, even if relatively low specificity may cause increased concern and anxiety for the women.
With a low specificity, several women who would never have developed pre-eclampsia would be offered prophylactic treatments and increased surveillance. This fact increases the need for the treatment to be safe and without any side-effects. The level of surveillance also has to be acceptable for the women. The possibilities of prophylactic treatment are limited, since no specific treatment is provided, but for a high risk group antiplatelet drugs, i.e. low dose aspirin, seems to have a relative good effect in preventing or postponing the disorder, at least if the treatment is started early in pregnancy.113 It is also important to evaluate other different possible

51
prophylactic treatments, where a substance such as heparin might be of interest. Intervention as early and as specific as possible in the development of pre-eclampsia is recommended. The ultimate would be to start treatment before the trophoblast invasion of the myometrium happens. It might also, in the future, be possible to start a potential prophylactic treatment even before the pregnancy begins, based on genetic testing and counselling. The possibility of over-expressing angiogenic factors in viral vectors for injection in the myometrial wall to optimize the angiogenic status has also been discussed but there are no such studies on-going on humans yet.
At present there are several predictive tests that do reach rather high sensitivity and specificity. The next step is to evaluate whether these tests, in combination with prophylactic treatment and/or increased surveillance, reduce the incidence or postpone diagnosis and improve the maternal and neonatal outcome. To perform these studies a multicenter approach with randomized controlled trials has to be made to achieve a decent number of patients at risk of pre-eclampsia.
The title of this thesis is “Pre-eclampsia – possible to predict?” The answer is “Yes, pre-eclampsia might be possible to predict”. To investigate whether there are any clinical benefits related to prediction, further studies are needed.

52
Conclusions
Ang-1/Ang-2 ratio increases during pregnancy in all women, but the ratios are significantly lower at gestational weeks 25 and 28 in women who later develop pre-eclampsia compared with normal pregnancies.
Ang-1/Ang-2 ratio is a possible predictor for later onset of pre-eclampsia in a low-risk population. The level of HRG decreases during pregnancy in all women, but the levels are significantly lower at gestational weeks 10, 25, and 28 in women who later develop pre-eclampsia compared with normal pregnancies. HRG may be a possible predictor for later onset of pre-eclampsia in the first trimester in a low-risk population. The combination of HRG and uterine artery Doppler in early pregnancy is a better predictor of preterm pre-eclampsia than each marker individually and may be a possible predictor for later onset of preterm pre-eclampsia. An association between hyperemesis gravidarum in the second trimester and preterm pre-eclampsia, as well as other placental dysfunction disorders, is demonstrated.

53
Sammanfattning på svenska
Preeklampsi, som är en graviditetsspecifik multiorgan sjukdom, utgör en av de vanligaste orsakerna till maternell och perinatal morbiditet och mortalitet världen över. I Sverige drabbas omkring 3% av alla gravida men i många andra länder är förekomsten högre. Orsaken till preeklampsi är inte full-ständigt klarlagd men, framför allt vid tidigt debuterande sjukdom, kan en möjlig förklaring vara en defekt infästning av moderkakan vilket i sin tur orsakar en ökning av substanser som är skadliga för moderns blodkärl. Vid preeklampsi har förändrade nivåer i blodet, av bland annat blodkärls-nybildande faktorer och inflammatoriska markörer, konstaterats flera veckor innan sjukdomsdebut vilket kan användas för att prediktera vilka kvinnor som har en ökad risk att utveckla preeklampsi. Möjligheten att kunna förhindra, eller att modifiera utvecklingen av preeklampsi, ökar ju tidigare som skillnaden mellan en normal graviditet, och en som senare utvecklar sjukdomen, upptäcks.
Blodkärlsnybildning regleras bland annat av Angiopoietin-1 och Angiopoietin-2 och påverkas även av Histidin rikt glykoprotein (HRG) som också är involverad i inflammatoriska processer. Ett annat ämne som påverkar infästningen av moderkakan och blodkärlsnybildningen är Humant chorion gonadotropin (hCG). Tidigare studier har visat att höga nivåer av hCG i andra trimestern är kopplat till utvecklingen av preeklampsi. Höga nivåer av hCG anses även kunna orsaka graviditetsillamående.
Målet med detta avhandlingsarbete har varit att uppnå ökad förståelse för bakomliggande orsaker till preeklampsi, att hitta ett tillförlitligt sätt att prediktera preeklampsi med enbart biokemiska markörer eller i kombination med en biofysisk markör såsom dopplerundersökning av arteria uterina samt att undersöka om det finns en korrelation mellan svårt graviditetsillamående och inadekvat infästning av moderkakan.
Till det första delarbetet inkluderades tidigare helt friska kvinnor i samband med inskrivning på mödravården. Blodprover samlades därefter in i graviditetsvecka 10, 25, 28, 33 och 37. Blodproverna från 19 kvinnor som utvecklade preeklampsi och 43 kvinnor med normala graviditeter analyserades med avseende på nivån av Angiopoietin-1 (Ang-1) och Angiopoietin-2 (Ang-2), med hjälp av kommersiellt tillgängliga enzyme-linked immunosorbent assay (ELISA) kit. Analysen visade att kvoten Ang-1/Ang-2 steg under graviditeten för alla kvinnor men i graviditetsvecka 25 och 28 var den kvoten signifikant lägre för kvinnor som senare utvecklade

54
preeklampsi. Kvoten Ang-1/Ang-2 är således en möjlig prediktor för preeklampsi.
I samma population som beskrivits ovan analyserades dessutom nivåerna av Histidin rikt glykoprotein (HRG) med hjälp av ELISA utvecklat på Institutionen för kvinnors och barns hälsa i Uppsala. Resultatet visade att HRG sjönk under graviditeten för alla kvinnor men nivåerna var signifikant lägre i graviditetsvecka 10, 25 och 28 för kvinnor som senare utvecklade preeklampsi. HRG är alltså en möjlig tidig prediktor för preeklampsi.
För att utvärdera om HRG i kombination med Dopplerundersökning av arteria uterina skulle förbättra den prediktiva förmågan genomfördes en studie i samarbete med St George’s hospital i London. Blodprovstagning och Dopplerundersökning genomfördes i genomsnitt i graviditetsvecka 14. 175 kvinnor med ökad risk för att utveckla preeklampsi bestående av först-föderskor, kvinnor med essentiell hypertoni, tidigare preeklampsi eller med barn födda små för gestationsåldern (SGA) deltog. 89 kvinnor utvecklade preeklampsi, 27 förlöstes före graviditetsvecka 37 och 62 i fullgången tid. 86 kvinnor hade en normal graviditet. Resultatet visade att kombinationen av HRG och Dopplerundersökning av arteria uterina var bättre på att förutsäga vilka kvinnor som skulle drabbas av preeklampsi före graviditetsvecka 37 än varje markör för sig, med en sensitivitet på 91% och en specificitet på 62%.
Ett eventuellt samband mellan inläggningskrävande svårt graviditets-illamående och preeklampsi, samt andra sjukdomar orsakade av defekt infästning av moderkakan, undersöktes i en kohort bestående av alla singelgraviditeter i Medicinska födelse registret mellan åren 1997 och 2009 (n=1,156,050). En länkning till patientregistrerades genomfördes. Riskerna för preeklampsi, moderkaksavlossning, dödföddhet och SGA jämfördes med graviditeter utan inläggningskrävande graviditetsillamående som referens samt justerades för moderns ålder, paritet, BMI, längd, rökning, samman-boende med barnafadern, barnets kön, moderns födelseland, utbildningsnivå, hypertyreos, diabetes mellitus, kronisk hypertoni och år då barnet föddes. Analysen visade att kvinnor med ett första vårdtillfälle på grund av graviditetsillamående i andra trimestern har en mer än fördubblad risk för prematur preeklampsi, tre gånger ökad risk för moderkaksavlossning och en 39%-ig riskökning för SGA. Resultatet talar före ett samband mellan svårt graviditetsillamående i andra trimestern och ett senare insjuknande i sjukdomar associerade med inadekvat infästning av moderkakan.
Sammanfattningsvis har våra studier visat att kvoten mellan Ang-1/Ang-2 samt nivåerna av cirkulerande HRG i plasma avviker hos kvinnor som senare utvecklar preeklampsi. Denna skillnad innebär en möjlighet att prediktera vilka kvinnor som kommer att drabbas av preeklampsi. HRG i kombination med Dopplerundersökning av arteria uterina förbättrar den prediktiva förmågan av tidigt debuterande preeklampsi. Hyperemesis i andra trimestern är en klinisk prediktor att beakta gällande preeklampsi och andra tillstånd orsakade av inadekvat infästning av moderkakan.

55
Acknowledgement
This thesis was conducted at the Department of Women’s and Children’s Health, Uppsala University.
I would like to thank the women who participated in this study and all those who supported, assisted and encouraged me during this process. I especially wish to express my gratitude to:
Helena Åkerud, Associate Professor at the Department of Women’s and Children’s Health, Uppsala University, and my main supervisor, for sharing your great knowledge and enthusiasm about science with me. Your intelli-gence and how you manage a large family, research, clinical work and training is impressive. Besides, you are a generous and wise person who has opened your home for me during my stays in Uppsala and offered interesting discussions about all things important in life.
Anna-Karin Wikström, Associate Professor at the Department of Women’s and Children’s Health, Uppsala University and my co-supervisor, for being so supportive and understanding. You have introduced me into epidemiology with great competence and patience. Your warmth and openness has ren-dered me many laughs.
Inger Sundström Poromaa, Professor at the Department of Women’s and Children’s Health, Uppsala University and my co-supervisor, for your intelligent remarks and interesting discussions and for, together with Alkistis Skalkidou, arranging an intensive week of research in Crete which offered both hard work and a hard walk.
Basky Thilaganathan, Professor at the Division of Clinical Development Sciences, Department of Obstetrics and Gynecology, St George’s University of London, for your generosity with material, competence and encourage-ment.
Ove Axelsson, Professor Emeritus of the Department of Women’s and Children’s Health, Uppsala University, for valuable support and fruitful discussions.

56
Jan Gustafsson, Professor and head of the Department of Women’s and Children’s Health, Uppsala University, for giving me the opportunity to perform my PhD-studies in Uppsala.
All coauthors for their contributions to this thesis.
Marju Dahmoun, Kenneth Challis and Kicki Rapp, present and former heads of the Department of Women’s health in Sundsvall, for providing work conditions that enabled me to start this project, encouraging me and giving me the opportunity to develop.
The Department of Research and Development in Sundsvall for financial and practical support and Erling Englund for statistical guidance.
Eva Bergman and Birgitta Segebladh, former colleagues in Sundsvall and now working in Uppsala, for initiating this thesis by introducing me to Helena Åkerud, and for being living examples of how to combine clinical work in Sundsvall with research in Uppsala.
Jesper Agrell, Sahruh Turkmen and Per Kempe, colleagues and friends, in the obstetrical section of the Department of Women’s health in Sundsvall, for close and smooth collaboration with challenging discussions as well as good laughs.
Lotta Andréen, Anna Enander, Anna Palm, Heléne Dalemo Lundin, Lena Enesund and all other colleagues and friends, at the Department of Women’s health in Sundsvall, for the combination of hard work, interesting discussions and an enjoyable atmosphere with many laughs which always has made me go to work with a light step.
Ingela Danielsson and Helena Blom, senior research fellow and PhD student at the Department of Research and Development in Sundsvall, for encouragement and for giving me other perspectives of my research.
Peter, Erik, Gustav, Axel and Astrid Åkerud for letting me be a part of your everyday life and always making me feel welcome.
Helena Nilsson, Karin Langlet, Catarina Haag, Petra Waleij, Lotte Wargentin, Nina Hagwall and Catharina Björkman, the very best friends I can imagine, for better or for worse. I do wish we could meet more often.
Hjalmar och Margret Bolin, my parents in law, for all the help and support throughout the years as well as many nice dinners.

57
Yngve och Vivi, my parents, for your endless love, support, encouragement and for always being there when needed.
Fredrik, Annika and Sara, my family bonus, for your openness, warmth, wit and generosity. Your talents, although very different, are impressive!
Göran, my beloved husband and closest friend, for sharing my life and stick with me through thick and thin.
Axel, Märta and Theodor, my children and treasures, for being just those you are which make me full of joy and pride. You are the meaning of it all and simply the best!

58
References
1. Chesley LC. History and epidemiology of preeclampsia-eclampsia. Clin Obstet Gynecol. 1984;27(4):801-20.
2. Salas SP. What causes pre-eclampsia? Baillieres Best Pract Res Clin Obstet Gynaecol. 1999;13(1):41-57.
3. Berglund. Svensk kvinnosjukvård under ett sekel. Uppsala: Almqvist och Wiksell tryckeri, 2001.
4. Hogberg U, Joelsson I. The decline in maternal mortality in Sweden, 1931-1980. Acta Obstet Gynecol Scand. 1985;64(7):583-92.
5. Andersgaard AB, Herbst A, Johansen M, Ivarsson A, Ingemarsson I, Langhoff-Roos J, et al. Eclampsia in Scandinavia: incidence, substandard care, and potentially preventable cases. Acta Obstet Gynecol Scand 2006;85(8):929-36.
6. WHO. Make every mother and child count. In: World health report. Geneva, Switzerland. 2005.
7. Khan KS, Wojdyla D, Say L, Gulmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet 2006;367(9516):1066-74.
8. Chappell L, Poulton L, Halligan A, Shennan AH. Lack of consistency in research papers over the definition of pre-eclampsia. Br J Obstet Gynaecol. 1999;106(9):983-5.
9. Brown MA, Lindheimer MD, de Swiet M, Van Assche A, Moutquin JM. The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertens Pregnancy. 2001;20(1):IX-XIV.
10. Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet. 2010;376(9741):631-44.
11. Murphy DJ, Stirrat GM. Mortality and morbidity associated with early-onset preeclampsia. Hypertens Pregnancy. 2000;19(2):221-31.
12. Rasmussen S, Irgens LM. Fetal growth and body proportion in preeclampsia. Obstet Gynecol. 2003;101(3):575-83.
13. Vatten LJ, Skjaerven R. Is pre-eclampsia more than one disease? BJOG. 2004;111(4):298-302.
14. Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol. 2009;33(3):130-7.
15. Sibai BM, Caritis S, Hauth J. What we have learned about preeclampsia. Semin Perinatol. 2003;27(3):239-46.
16. Lain KY, Roberts JM. Contemporary concepts of the pathogenesis and management of preeclampsia. Jama 2002;287(24):3183-6.
17. Goldenberg RL, Rouse DJ. Prevention of premature birth. N Engl J Med. 1998;339(5):313-20.
18. Odegard RA, Vatten LJ, Nilsen ST, Salvesen KA, Austgulen R. Preeclampsia and fetal growth. Obstet Gynecol. 2000;96(6):950-5.
19. Barker DJ. The developmental origins of well-being. Philos Trans R Soc Lond B Biol Sci 2004;359(1449):1359-66.

59
20. McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ. Cardiovascular sequelae of preeclampsia/eclampsia: a systematic review and meta-analyses. Am Heart J. 2008;156(5):918-30.
21. Wikstrom AK, Haglund B, Olovsson M, Lindeberg SN. The risk of maternal ischaemic heart disease after gestational hypertensive disease. BJOG. 2005;112(11):1486-91.
22. Roberts JM, Hubel CA. The two stage model of preeclampsia: variations on the theme. Placenta 2009;30 Suppl A:S32-7.
23. Pijnenborg R, Dixon G, Robertson WB, Brosens I. Trophoblastic invasion of human decidua from 8 to 18 weeks of pregnancy. Placenta. 1980;1(1):3-19.
24. Huppertz B. Placental origins of preeclampsia: challenging the current hypothesis. Hypertension 2008;51(4):970-5.
25. James JL, Whitley GS, Cartwright JE. Pre-eclampsia: fitting together the placental, immune and cardiovascular pieces. J Pathol 2010;221(4):363-78.
26. Roberts JM, Taylor RN, Musci TJ, Rodgers GM, Hubel CA, McLaughlin MK. Preeclampsia: an endothelial cell disorder. Am J Obstet Gynecol. 1989;161(5):1200-4.
27. Redman CW, Sargent IL. Placental stress and pre-eclampsia: a revised view. Placenta 2009;30 Suppl A:S38-42.
28. von Dadelszen P, Magee LA, Roberts JM. Subclassification of preeclampsia. Hypertens Pregnancy 2003;22(2):143-8.
29. MacKay AP, Berg CJ, Atrash HK. Pregnancy-related mortality from preeclampsia and eclampsia. Obstet Gynecol 2001;97(4):533-8.
30. Valensise H, Vasapollo B, Gagliardi G, Novelli GP. Early and late preeclampsia: two different maternal hemodynamic states in the latent phase of the disease. Hypertension. 2008;52(5):873-80.
31. Ness RB, Roberts JM. Heterogeneous causes constituting the single syndrome of preeclampsia: a hypothesis and its implications. Am J Obstet Gynecol 1996;175(5):1365-70.
32. Egbor M, Ansari T, Morris N, Green CJ, Sibbons PD. Morphometric placental villous and vascular abnormalities in early- and late-onset pre-eclampsia with and without fetal growth restriction. BJOG 2006;113(5):580-9.
33. Rolfo A, Many A, Racano A, Tal R, Tagliaferro A, Ietta F, et al. Abnormalities in oxygen sensing define early and late onset preeclampsia as distinct pathologies. PLoS 2010;5(10):e13288.
34. Pabinger I. Thrombophilia and its impact on pregnancy. Thromb Res. 2009;123 Suppl 3:S16-21.
35. Dekker G, Sibai B. Primary, secondary, and tertiary prevention of pre-eclampsia. Lancet. 2001;357(9251):209-15.
36. Sibai BM, Mercer B, Sarinoglu C. Severe preeclampsia in the second trimester: recurrence risk and long-term prognosis. Am J Obstet Gynecol. 1991;165 (5 Pt 1):1408-12.
37. Dildy GA, 3rd, Belfort MA, Smulian JC. Preeclampsia recurrence and prevention. Semin Perinatol. 2007;31(3):135-41.
38. Bailit JL. Hyperemesis gravidarium: Epidemiologic findings from a large cohort. Am J Obstet Gynecol 2005;193(3 Pt 1):811-4.
39. Vikanes A, Grjibovski AM, Vangen S, Magnus P. Variations in prevalence of hyperemesis gravidarum by country of birth: a study of 900,074 pregnancies in Norway, 1967-2005. Scand J Public Health 2008;36(2):135-42.
40. Gazmararian JA, Petersen R, Jamieson DJ, Schild L, Adams MM, Deshpande AD, et al. Hospitalizations during pregnancy among managed care enrollees. Obstet Gynecol 2002;100(1):94-100.

60
41. Verberg MF, Gillott DJ, Al-Fardan N, Grudzinskas JG. Hyperemesis gravidarum, a literature review. Hum Reprod Update 2005;11(5):527-39.
42. Licht P, Fluhr H, Neuwinger J, Wallwiener D, Wildt L. Is human chorionic gonadotropin directly involved in the regulation of human implantation? Mol Cell Endocrinol 2007;269(1-2):85-92.
43. Handschuh K, Guibourdenche J, Tsatsaris V, Guesnon M, Laurendeau I, Evain-Brion D, et al. Human chorionic gonadotropin produced by the invasive trophoblast but not the villous trophoblast promotes cell invasion and is down-regulated by peroxisome proliferator-activated receptor-gamma. Endocrinology 2007;148(10):5011-9.
44. Cole LA. Biological functions of hCG and hCG-related molecules. Reprod Biol Endocrinol 2010;8:102.
45. Lepage N, Chitayat D, Kingdom J, Huang T. Association between second-trimester isolated high maternal serum maternal serum human chorionic gonadotropin levels and obstetric complications in singleton and twin pregnancies. Am J Obstet Gynecol 2003;188(5):1354-9.
46. Huang T, Hoffman B, Meschino W, Kingdom J, Okun N. Prediction of adverse pregnancy outcomes by combinations of first and second trimester biochemistry markers used in the routine prenatal screening of Down syndrome. Prenat Diagn 2010;30(5):471-7.
47. Ree PH, Hahn WB, Chang SW, Jung SH, Kang JH, Cha DH, et al. Early detection of preeclampsia using inhibin a and other second-trimester serum markers. Fetal Diagn Ther 2011;29(4):280-6.
48. Ong CY, Liao AW, Spencer K, Munim S, Nicolaides KH. First trimester maternal serum free beta human chorionic gonadotrophin and pregnancy associated plasma protein A as predictors of pregnancy complications. BJOG 2000;107(10):1265-70.
49. Ranta JK, Raatikainen K, Romppanen J, Pulkki K, Heinonen S. Decreased PAPP-A is associated with preeclampsia, premature delivery and small for gestational age infants but not with placental abruption. Eur J Obstet Gynecol Reprod Biol 2011;157(1):48-52.
50. Karagiannis G, Akolekar R, Sarquis R, Wright D, Nicolaides KH. Prediction of small-for-gestation neonates from biophysical and biochemical markers at 11-13 weeks. Fetal Diagn Ther 2011;29(2):148-54.
51. Chen JZ, Sheehan PM, Brennecke SP, Keogh RJ. Vessel remodelling, pregnancy hormones and extravillous trophoblast function. Mol Cell Endocrinol 2012;349(2):138-44.
52. Veenendaal MV, van Abeelen AF, Painter RC, van der Post JA, Roseboom TJ. Consequences of hyperemesis gravidarum for offspring: a systematic review and meta-analysis. BJOG 2011;118(11):1302-13.
53. Zhang J, Cai WW. Severe vomiting during pregnancy: antenatal correlates and fetal outcomes. Epidemiology. 1991;2(6):454-7.
54. Conde-Agudelo A, Villar J, Lindheimer M. World Health Organization systematic review of screening tests for preeclampsia. Obstet Gynecol 2004;104(6):1367-91.
55. Cetin I, Huppertz B, Burton G, Cuckle H, Gonen R, Lapaire O, et al. Pregenesys pre-eclampsia markers consensus meeting: What do we require from markers, risk assessment and model systems to tailor preventive strategies? Placenta. 2011;32 Suppl:S4-16.
56. Romero R, Kusanovic JP, Than NG, Erez O, Gotsch F, Espinoza J, et al. First-trimester maternal serum PP13 in the risk assessment for preeclampsia. Am J Obstet Gynecol. 2008;199(2):122 e1-22 e11.

61
57. Smith GC, Stenhouse EJ, Crossley JA, Aitken DA, Cameron AD, Connor JM. Early pregnancy levels of pregnancy-associated plasma protein a and the risk of intrauterine growth restriction, premature birth, preeclampsia, and stillbirth. J Clin Endocrinol Metab. 2002;87(4):1762-7.
58. Audibert F, Benchimol Y, Benattar C, Champagne C, Frydman R. Prediction of preeclampsia or intrauterine growth restriction by second trimester serum screening and uterine Doppler velocimetry. Fetal Diagn Ther. 2005;20(1): 48-53.
59. Muttukrishna S, North RA, Morris J, Schellenberg JC, Taylor RS, Asselin J, et al. Serum inhibin A and activin A are elevated prior to the onset of pre-eclampsia. Hum Reprod 2000;15(7):1640-5.
60. Holzgreve W, Li JJ, Steinborn A, Kulz T, Sohn C, Hodel M, et al. Elevation in erythroblast count in maternal blood before the onset of preeclampsia. Am J Obstet Gynecol. 2001;184(2):165-8.
61. Levine RJ, Qian C, Leshane ES, Yu KF, England LJ, Schisterman EF, et al. Two-stage elevation of cell-free fetal DNA in maternal sera before onset of preeclampsia. Am J Obstet Gynecol. 2004;190(3):707-13.
62. Thilaganathan B, Wormald B, Zanardini C, Sheldon J, Ralph E, Papageorghiou AT. Early-pregnancy multiple serum markers and second-trimester uterine artery Doppler in predicting preeclampsia. Obstet Gynecol 2010;115(6):1233-8.
63. Cetin I, Cozzi V, Papageorghiou AT, Maina V, Montanelli A, Garlanda C, et al. First trimester PTX3 levels in women who subsequently develop preeclampsia and fetal growth restriction. Acta Obstet Gynecol Scand. 2009;88(7):846-9.
64. Sibai B, Romero R, Klebanoff MA, Rice MM, Caritis S, Lindheimer MD, et al. Maternal plasma concentrations of the soluble tumor necrosis factor receptor 2 are increased prior to the diagnosis of preeclampsia. Am J Obstet Gynecol. 2009;200(6):630 e1-8.
65. Zygmunt M, Herr F, Munstedt K, Lang U, Liang OD. Angiogenesis and vasculogenesis in pregnancy. Eur J Obstet Gynecol Reprod Biol. 2003;110 Suppl 1:S10-8.
66. Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, et al. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004;350(7):672-83.
67. De Vivo A, Baviera G, Giordano D, Todarello G, Corrado F, D'Anna R. Endoglin, PlGF and sFlt-1 as markers for predicting pre-eclampsia. Acta Obstet Gynecol Scand. 2008;87(8):837-42.
68. Seval Y, Sati L, Celik-Ozenci C, Taskin O, Demir R. The distribution of angiopoietin-1, angiopoietin-2 and their receptors tie-1 and tie-2 in the very early human placenta. Placenta. 2008;29(9):809-15.
69. Zhang EG, Smith SK, Baker PN, Charnock-Jones DS. The regulation and localization of angiopoietin-1, -2, and their receptor Tie2 in normal and pathologic human placentae. Mol Med. 2001;7(9):624-35.
70. Kuijper S, Turner CJ, Adams RH. Regulation of angiogenesis by Eph-ephrin interactions. Trends Cardiovasc Med. 2007;17(5):145-51.
71. Maisonpierre PC, Suri C, Jones PF, Bartunkova S, Wiegand SJ, Radziejewski C, et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science. 1997;277(5322):55-60.
72. Suri C, McClain J, Thurston G, McDonald DM, Zhou H, Oldmixon EH, et al. Increased vascularization in mice overexpressing angiopoietin-1. Science. 1998;282(5388):468-71.

62
73. Lobov IB, Brooks PC, Lang RA. Angiopoietin-2 displays VEGF-dependent modulation of capillary structure and endothelial cell survival in vivo. Proc Natl Acad Sci U S A. 2002;99(17):11205-10.
74. Yuan HT, Venkatesha S, Chan B, Deutsch U, Mammoto T, Sukhatme VP, et al. Activation of the orphan endothelial receptor Tie1 modifies Tie2-mediated intracellular signaling and cell survival. FASEB J. 2007;21(12):3171-83.
75. Shamshirsaz AA, Paidas M, Krikun G. Preeclampsia, hypoxia, thrombosis, and inflammation. J Pregnancy 2012;2012:374047.
76. Cerneca F, Ricci G, Simeone R, Malisano M, Alberico S, Guaschino S. Coagulation and fibrinolysis changes in normal pregnancy. Increased levels of procoagulants and reduced levels of inhibitors during pregnancy induce a hypercoagulable state, combined with a reactive fibrinolysis. Eur J Obstet Gynecol Reprod Biol 1997;73(1):31-6.
77. Konijnenberg A, Stokkers EW, van der Post JA, Schaap MC, Boer K, Bleker OP, et al. Extensive platelet activation in preeclampsia compared with normal pregnancy: enhanced expression of cell adhesion molecules. Am J Obstet Gynecol. 1997;176(2):461-9.
78. Holthe MR, Staff AC, Berge LN, Lyberg T. Different levels of platelet activation in preeclamptic, normotensive pregnant, and nonpregnant women. Am J Obstet Gynecol. 2004;190(4):1128-34.
79. Williams VK, Griffiths AB, Carbone S, Hague WM. Fibrinogen concentration and factor VIII activity in women with preeclampsia. Hypertens Pregnancy. 2007;26(4):415-21.
80. Karehed K, Wikstrom AK, Olsson AK, Larsson A, Olovsson M, Akerud H. Fibrinogen and histidine-rich glycoprotein in early-onset preeclampsia. Acta 2010;89(1):131-9.
81. Manten GT, Sikkema JM, Franx A, Hameeteman TM, Visser GH, de Groot PG, et al. Increased high molecular weight fibrinogen in pre-eclampsia. Thromb Res. 2003;111(3):143-7.
82. Simantov R, Febbraio M, Crombie R, Asch AS, Nachman RL, Silverstein RL. Histidine-rich glycoprotein inhibits the antiangiogenic effect of thrombospondin-1. J Clin Invest 2001;107(1):45-52.
83. Olsson AK, Larsson H, Dixelius J, Johansson I, Lee C, Oellig C, et al. A fragment of histidine-rich glycoprotein is a potent inhibitor of tumor vascularization. Cancer Res. 2004;64(2):599-605.
84. Lee C, Dixelius J, Thulin A, Kawamura H, Claesson-Welsh L, Olsson AK. Signal transduction in endothelial cells by the angiogenesis inhibitor histidine-rich glycoprotein targets focal adhesions. Exp Cell Res. 2006;312(13):2547-56.
85. Redman CW, Sargent IL. Pre-eclampsia, the placenta and the maternal systemic inflammatory response--a review. Placenta. 2003;24 Suppl A:S21-7.
86. Jespersen J, Gram J, Bach E. A sequential study of plasma histidine-rich glycoprotein and plasminogen in patients with acute myocardial infarction and deep vein thrombosis. Thromb Haemost. 1984;51(1):99-102.
87. Saigo K, Yoshida A, Ryo R, Yamaguchi N, Leung LL. Histidine-rich glycoprotein as a negative acute phase reactant. Am J Hematol. 1990;34(2):149-50.
88. Blank M, Shoenfeld Y. Histidine-rich glycoprotein modulation of immune/autoimmune, vascular, and coagulation systems. Clin Rev Allergy Immunol. 2008;34(3):307-12.
89. Nordqvist S, Karehed K, Hambiliki F, Wanggren K, Stavreus-Evers A, Akerud H. The presence of histidine-rich glycoprotein in the female reproductive tract and in embryos. Reprod Sci 2010;17(10):941-7.

63
90. Kuc S, Wortelboer EJ, van Rijn BB, Franx A, Visser GH, Schielen PC. Evaluation of 7 serum biomarkers and uterine artery Doppler ultrasound for first-trimester prediction of preeclampsia: a systematic review. Obstet Gynecol Surv 2011;66(4):225-39.
91. Cnossen JS, ter Riet G, Mol BW, van der Post JA, Leeflang MM, Meads CA, et al. Are tests for predicting pre-eclampsia good enough to make screening viable? A review of reviews and critical appraisal. Acta Obstet Gynecol Scand. 2009;88(7):758-65.
92. Anderson UD, Olsson MG, Rutardottir S, Centlow M, Kristensen KH, Isberg PE, et al. Fetal hemoglobin and alpha(1)-microglobulin as first- and early second-trimester predictive biomarkers for preeclampsia. Am J Obstet Gynecol 2011;2011:23.
93. Robertson WB, Brosens I, Dixon G. Maternal uterine vascular lesions in the hypertensive complications of pregnancy. Perspect Nephrol Hypertens 1976;5:115-27.
94. Harrington KF, Campbell S, Bewley S, Bower S. Doppler velocimetry studies of the uterine artery in the early prediction of pre-eclampsia and intra-uterine growth retardation. Eur J Obstet Gynecol Reprod Biol 1991;42 Suppl:S14-20.
95. Prefumo F, Sebire NJ, Thilaganathan B. Decreased endovascular trophoblast invasion in first trimester pregnancies with high-resistance uterine artery Doppler indices. Hum Reprod. 2004;19(1):206-9.
96. Cnossen JS, Morris RK, ter Riet G, Mol BW, van der Post JA, Coomarasamy A, et al. Use of uterine artery Doppler ultrasonography to predict pre-eclampsia and intrauterine growth restriction: a systematic review and bivariable meta-analysis. CMAJ. 2008;178(6):701-11.
97. Giguere Y, Charland M, Bujold E, Bernard N, Grenier S, Rousseau F, et al. Combining biochemical and ultrasonographic markers in predicting preeclampsia: a systematic review. Clin Chem 2009;56(3):361-75.
98. Pedrosa AC, Matias A. Screening for pre-eclampsia: a systematic review of tests combining uterine artery Doppler with other markers. J Perinat Med 2011;39(6):619-35.
99. Leslie K, Thilaganathan B, Papageorghiou A. Early prediction and prevention of pre-eclampsia. Best Pract Res Clin Obstet Gynaecol 2011;25(3):343-54.
100. Cnossen JS, Vollebregt KC, de Vrieze N, ter Riet G, Mol BW, Franx A, et al. Accuracy of mean arterial pressure and blood pressure measurements in predicting pre-eclampsia: systematic review and meta-analysis. BMJ 2008;336(7653):1117-20.
101. Poon LC, Kametas NA, Maiz N, Akolekar R, Nicolaides KH. First-trimester prediction of hypertensive disorders in pregnancy. Hypertension. 2009;53(5):812-8.
102. Akolekar R, Syngelaki A, Sarquis R, Zvanca M, Nicolaides KH. Prediction of early, intermediate and late pre-eclampsia from maternal factors, biophysical and biochemical markers at 11-13 weeks. Prenat Diagn 2011;31(1):66-74.
103. Chesley LC, Annitto JE, Cosgrove RA. The familial factor in toxemia of pregnancy. Obstet Gynecol 1968;32(3):303-11.
104. Roberts JM, Cooper DW. Pathogenesis and genetics of pre-eclampsia. Lancet 2001;357(9249):53-6.
105. Arngrimsson R, Siguroardottir S, Frigge ML, Bjarnadottir RI, Jonsson T, Stefansson H, et al. A genome-wide scan reveals a maternal susceptibility locus for pre-eclampsia on chromosome 2p13. Hum Mol Genet 1999;8(9):1799-805.

64
106. Laivuori H, Lahermo P, Ollikainen V, Widen E, Haiva-Mallinen L, Sundstrom H, et al. Susceptibility loci for preeclampsia on chromosomes 2p25 and 9p13 in Finnish families. Am J Hum Genet 2003;72(1):168-77.
107. Moses EK, Lade JA, Guo G, Wilton AN, Grehan M, Freed K, et al. A genome scan in families from Australia and New Zealand confirms the presence of a maternal susceptibility locus for pre-eclampsia, on chromosome 2. Am J Hum Genet 2000;67(6):1581-5.
108. Sun CJ, Zhang L, Zhang WY. Gene expression profiling of maternal blood in early onset severe preeclampsia: identification of novel biomarkers. J Perinat Med 2009;37(6):609-16.
109. Centlow M, Wingren C, Borrebaeck C, Brownstein MJ, Hansson SR. Differential gene expression analysis of placentas with increased vascular resistance and pre-eclampsia using whole-genome microarrays. J Pregnancy 2011;2011:472354.
110. Lykke JA, Bare LA, Olsen J, Lagier R, Tong C, Arellano A, et al. Vascular associated gene variants in patients with preeclampsia: results from the Danish National Birth Cohort. Acta Obstet Gynecol Scand 2012;91(9):1053-60.
111. Centlow M, Carninci P, Nemeth K, Mezey E, Brownstein M, Hansson SR. Placental expression profiling in preeclampsia: local overproduction of hemoglobin may drive pathological changes. Fertil Steril 2008;90(5):1834-43.
112. Askie LM, Duley L, Henderson-Smart DJ, Stewart LA. Antiplatelet agents for prevention of pre-eclampsia: a meta-analysis of individual patient data. Lancet. 2007;369(9575):1791-8.
113. Roberge S, Villa P, Nicolaides K, Giguere Y, Vainio M, Bakthi A, et al. Early administration of low-dose aspirin for the prevention of preterm and term preeclampsia: a systematic review and meta-analysis. Fetal Diagn Ther 2012;31(3):141-6.
114. Bussolino F, Benedetto C, Massobrio M, Camussi G. Maternal vascular prostacyclin activity in pre-eclampsia. Lancet. 1980;2(8196):702.
115. Duley L, Henderson-Smart DJ, Meher S, King JF. Antiplatelet agents for preventing pre-eclampsia and its complications. Cochrane Database Syst Rev. 2007(2):CD004659.
116. James AH, Brancazio LR, Price T. Aspirin and reproductive outcomes. Obstet Gynecol Surv. 2008;63(1):49-57.
117. Hofmeyr GJ, Lawrie TA, Atallah AN, Duley L. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane 2011(8):CD001059.
118. Carroli G, Merialdi M, Wojdyla D, Abalos E, Campodonico L, Yao SE, et al. Effects of calcium supplementation on uteroplacental and fetoplacental blood flow in low-calcium-intake mothers: a randomized controlled trial. Am J Obstet Gynecol 2009;202(1):45 e1-9.
119. Moldenhauer JS, Stanek J, Warshak C, Khoury J, Sibai B. The frequency and severity of placental findings in women with preeclampsia are gestational age dependent. Am J Obstet Gynecol. 2003;189(4):1173-7.
120. Dodd JM, McLeod A, Windrim RC, Kingdom J. Antithrombotic therapy for improving maternal or infant health outcomes in women considered at risk of placental dysfunction. Cochrane 2010(6):CD006780.
121. Shibuya M. Vascular endothelial growth factor-dependent and -independent regulation of angiogenesis. BMB Rep. 2008;41(4):278-86.
65
122. Geva E, Ginzinger DG, Zaloudek CJ, Moore DH, Byrne A, Jaffe RB. Human placental vascular development: vasculogenic and angiogenic (branching and nonbranching) transformation is regulated by vascular endothelial growth factor-A, angiopoietin-1, and angiopoietin-2. J Clin Endocrinol Metab. 2002;87(9):4213-24.
123. Oh H, Takagi H, Suzuma K, Otani A, Matsumura M, Honda Y. Hypoxia and vascular endothelial growth factor selectively up-regulate angiopoietin-2 in bovine microvascular endothelial cells. J Biol Chem. 1999;274(22):15732-9.
124. Mandriota SJ, Pepper MS. Regulation of angiopoietin-2 mRNA levels in bovine microvascular endothelial cells by cytokines and hypoxia. Circ Res. 1998;83(8):852-9.
125. Hirokoshi K, Maeshima Y, Kobayashi K, Matsuura E, Sugiyama H, Yamasaki Y, et al. Increase of serum angiopoietin-2 during pregnancy is suppressed in women with preeclampsia. Am J Hypertens. 2005;18(9 Pt 1):1181-8.
126. Leinonen E, Wathen KA, Alfthan H, Ylikorkala O, Andersson S, Stenman UH, et al. Maternal serum angiopoietin-1 and -2 and tie-2 in early pregnancy ending in preeclampsia or intrauterine growth retardation. J Clin Endocrinol Metab 2010;95(1):126-33.
127. Poon IK, Patel KK, Davis DS, Parish CR, Hulett MD. Histidine-rich glycoprotein: the Swiss Army knife of mammalian plasma. Blood 2011;117(7):2093-101.
128. Haukkamaa M, Morgan WT, Koskelo P. Serum histidine-rich glycoprotein during pregnancy and hormone treatment. Scand J Clin Lab Invest. 1983;43(7):591-5.
129. Halbmayer WM, Hopmeier P, Feichtinger C, Rubi K, Fischer M. Histidine-rich glycoprotein (HRG) in uncomplicated pregnancy and mild and moderate preeclampsia. Thromb Haemost. 1992;67(5):585-6.
130. Kaufmann P, Black S, Huppertz B. Endovascular trophoblast invasion: implications for the pathogenesis of intrauterine growth retardation and preeclampsia. Biol Reprod 2003;69(1):1-7.
131. Dommisse J, Tiltman AJ. Placental bed biopsies in placental abruption. Br J Obstet Gynaecol 1992;99(8):651-4.
132. Lub-Moss MM, Eurelings-Bontekoe EH. Clinical experience with patients suffering from hyperemesis gravidarum (severe nausea and vomiting during pregnancy): thoughts about subtyping of patients, treatment and counseling models. Patient Educ Couns 1997;31(1):65-75.
133. Tamay AG, Kuscu NK. Hyperemesis gravidarum: current aspect. J Obstet Gynaecol 2011;31(8):708-12.
134. Millar LK, Wing DA, Leung AS, Koonings PP, Montoro MN, Mestman JH. Low birth weight and preeclampsia in pregnancies complicated by hyperthyroidism. Obstet Gynecol 1994;84(6):946-9.
135. Shenoy V, Kanasaki K, Kalluri R. Pre-eclampsia: connecting angiogenic and metabolic pathways. Trends Endocrinol Metab 2010;21(9):529-36.
136. Bahado-Singh RO, Oz AU, Kingston JM, Shahabi S, Hsu CD, Cole L. The role of hyperglycosylated hCG in trophoblast invasion and the prediction of subsequent pre-eclampsia. Prenat Diagn 2002;22(6):478-81.
137. Lindqvist P, Grennert L, Marsal K. Epidermal growth factor in maternal urine--a predictor of intrauterine growth restriction? Early Hum Dev 1999;56 (2-3):143-50.
138. Savvidou MD, Akolekar R, Zaragoza E, Poon LC, Nicolaides KH. First trimester urinary placental growth factor and development of pre-eclampsia. BJOG 2009;116(5):643-7.

66
139. Strom CM, Bonilla-Guererro R, Zhang K, Doody KJ, Tourgeman D, Alvero R, et al. The sensitivity and specificity of hyperglycosylated hCG (hhCG) levels to reliably diagnose clinical IVF pregnancies at 6 days following embryo transfer. J Assist Reprod Genet 2012;29(7):609-14.