professor dipak kalra digital health assembly 2015
TRANSCRIPT

Electronic Health Records for Clinical Research
GLOBAL SHARING FOR GLOBAL
HEALTH:
TRUSTWORTHY REUSE OF HEALTH
DATA
Digital Health Assembly, Cardiff
Dipak Kalra President of EuroRec
Professor of Health Informatics, UCL

Responding to a convergence of needs
2
Need to remove the bottlenecks to accessing and combining
health data from diverse sources across Europe
Clinical Research needs
Optimise clinical research processes
•achieve faster and more accurate
patient identification
• identify sites that have access to the
most suitable patients
• reduce protocol amendments
Enhance access to Real World Data
•study the use of new medicines in real
populations
•conduct comparative effectiveness
studies
•monitor long term safety
•gather evidence for adaptive licensing
Healthcare needs
Improve quality and safety of care
•enhance care co-ordination
• increase adherence to clinical
evidence
• reduce medical errors and treatment
delays
Support patients in self-care and health
maintenance
Improve efficiency of care
•optimise care pathways to improve
outcomes
•collate evidence for public health
strategy and decision-making

Interoperability Data security, privacy &
ethics
Scalability and
sustainability
Common challenges to the use of health data for person
centred care, and the re-use of health data for clinical research
3
Confidence in data

Electronic Health Records for Clinical Research

Electronic Health Records for Clinical Research
A unique initiative
EHR4CR – Electronic Health Records for Clinical
Research
Re-use of EHR data for optimising Clinical trials
Mandated by IMI
One of the largest European public/private
partnership projects in this area
4-year project (2011-2015)
Extended into 2016 for making the transition to a sustainable
platform.
Budget of € >16m
5
For more information:
http://www.ehr4cr.eu/

Electronic Health Records for Clinical Research
Brings together key stakeholders
6
35 participants
including
pharmaceutical
industry, academia ,
hospitals, small and
medium-sized
enterprises, patient
associations and
public authorities
11 hospital
sites
Advisory
boards and
other experts

Identifying and recruiting suitable patients and trial sites are principal causes of trial delays
Delayed trials waste costly resources and slow access to new drugs
Patient recruitment a major cause of trial delays
7
50% of today’s clinical trials fail to achieve the target recruitment rate4
Almost
half of all trial
delays caused by patient recruitment problems2
1. State of the Clinical Trials Industry: A Sourcebook of Charts and Statistics, Center Watch, 2008. 2. Study Participant Recruitment and Retention in Clinical Trials: Emerging strategies in Europe, the US and Asia, Business Insights, June 2007. 3. Beasley, “Recruiting” 2008 4. Tufts -http://clinicalperformancepartners.com/wp-content/uploads/2012/07/Fixing-Feasibility-Final-Jan-2012.pdf
Each day a drug is delayed from market, sponsors lose up to
$8m3
The percentage of studies that complete enrolment on time:
18% in Europe,
7% in the US1

Electronic Health Records for Clinical Research
1. A self-sustaining economic model
2. A roadmap for pan-European adoption
A SET OF TOOLS AND SERVICES
Project deliverables
8
BUSINESS MODEL
A set of tools and services
Validated through pilots
Different therapeutic areas (e.g. oncology, neuroscience, diabetes, CVS…)
Several countries (under different legal frameworks)
1. Protocol Feasibility
2. Patient Identification and Recruitment
3. Clinical Trial Data Exchange
TECHNICAL PLATFORM
Requirements informed by stakeholders
95% in favour of reuse of EHR data
(internal & external stakeholders)
Identified issues that need to be addressed
Priority services: protocol feasibility,
patient identification and recruitment,
exchanging data with EHRs for clinical trial
data collection, adverse event reporting
Interviews with stakeholders helped inform
software requirements (Protocol Feasibility
Service and Patient Identification and
Recruitment Service)
9
203 respondents from
23 EU countries
Pharma, academia, CROs,
Patient advocacy groups, Health
agencies, IT providers
EU survey
95% rated compliance with
ethical, legal and privacy
requirements as the
highest, or equal highest
driving force for success
of EHR4CR1
1. Kalra D, Schmidt A, Potts HWW, Dupont D, Sundgren M, De Moor G, on behalf of the EHR4CR Research
consortium. Case Report from the EHR4CR Project: A European Survey on Electronic Health Records Systems
for Clinical Research. iHealth Connections 2011; 1(2): 108-113.
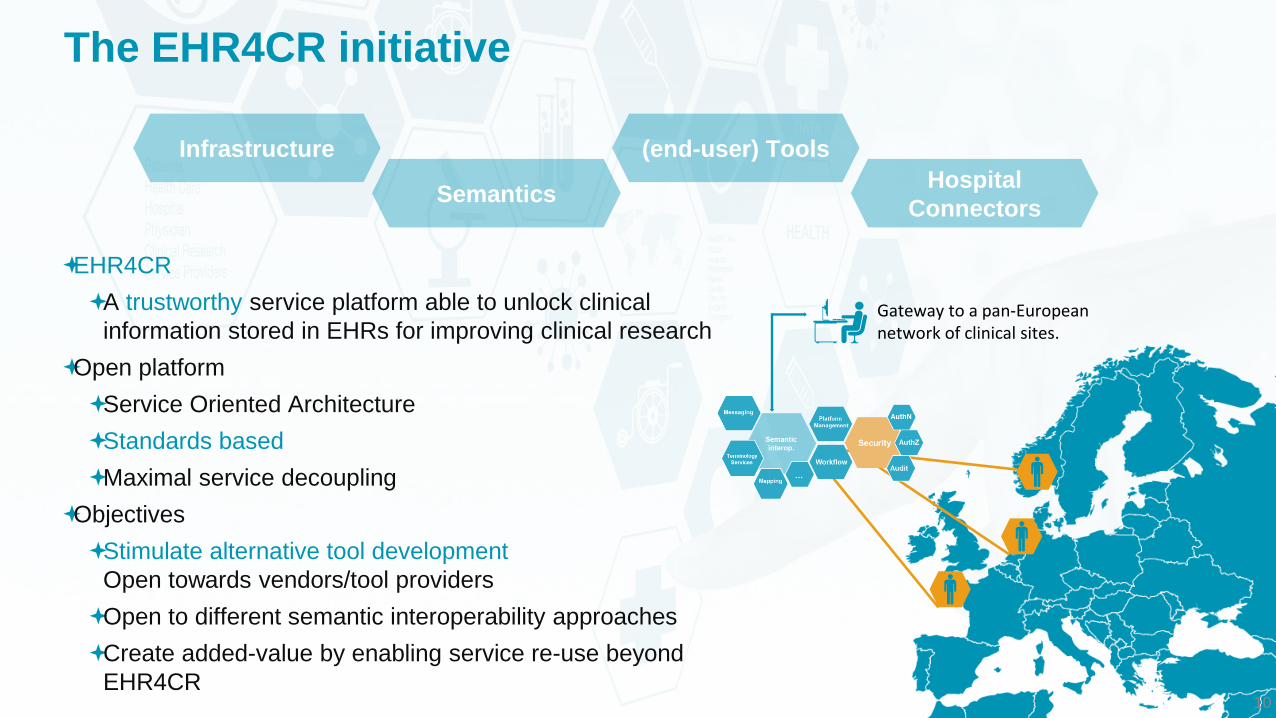
Gateway to a pan-European network of clinical sites.
The EHR4CR initiative
10
EHR4CR
A trustworthy service platform able to unlock clinical
information stored in EHRs for improving clinical research
Open platform
Service Oriented Architecture
Standards based
Maximal service decoupling
Objectives
Stimulate alternative tool development
Open towards vendors/tool providers
Open to different semantic interoperability approaches
Create added-value by enabling service re-use beyond
EHR4CR
Infrastructure
Semantics
(end-user) Tools
Hospital
Connectors

Protocol feasibility demonstration
11

Electronic Health Records for Clinical Research
Subject Identification & Recruitment
12
(Re-)define study Invite sites of interest Start study Track progress
Identify & Recruit Report Update Accept
Electronic Health Records for Clinical Research
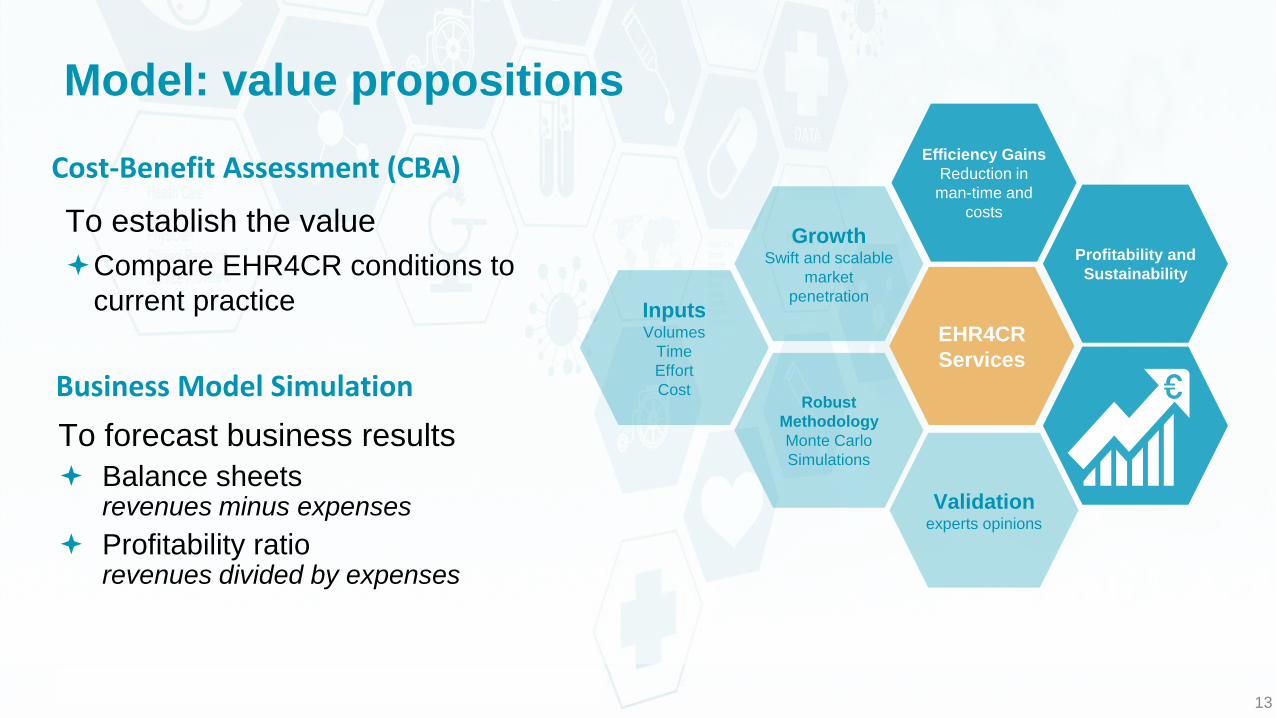
Model: value propositions
To establish the value
Compare EHR4CR conditions to
current practice
13
Cost-Benefit Assessment (CBA)
Inputs Volumes
Time
Effort
Cost
EHR4CR
Services
Efficiency Gains
Reduction in
man-time and
costs
Robust
Methodology
Monte Carlo
Simulations
Growth Swift and scalable
market
penetration
To forecast business results
Balance sheets revenues minus expenses
Profitability ratio revenues divided by expenses
Business Model Simulation
Profitability and
Sustainability
Validation experts opinions

Electronic Health Records for Clinical Research
Where we are now…
EHR4CR - IMI
research project
14
Operational pan-
European platform
Project pilot hospitals
11 major hospitals in 5 countries.
Germany (2), France (2), UK (5),
Switzerland (1), Poland (1)
12 studies, de-identified data
from >500k patients over 11
sites
Scaling up the
solutions!
Technology
Operations
Governance
Sustainability
Operational pan-European platform
Permanent network of clinical sites
giving access to millions of patients in close
to real time
Trial design and recruitment supported by
real-world evidence on a European scale

Electronic Health Records for Clinical Research
ENSURING TRUST
WHEN RE-USING
EHRS FOR
RESEARCH

Information governance framework and products
16

EHR4CR governance design principles
Analyse de-identified health records at participating hospital sites
Platform only connected to dedicated repository approved by each
hospital for EHR4CR use
For protocol feasibility and patient identification/recruitment, only
patient counts (totals and sub-totals) are returned from each
hospital to the central EHR4CR Platform, never patient level data
Platform never stores or communicates data about single data subjects
Data about individuals, who might be invited into a study, remain
internal to the hospital and abide by its local governance rules
Only treating physicians can re-identify candidate patients
EHR data is only shared - within the hospital - with a clinical
research team if the patient has given that specific consent
17

Ensuring robust governance
Only approved users are formally registered and given secure log in credentials
Users have no means of requesting or obtaining patient level data through the services
Even patient numbers are suppressed if the numbers are very low
State of the art information security measures are used throughout
Audit logs are captured at key communications points:
Pharma sites, within the Platform and at hospitals
A Code of Practice and Standard Operating Rules will govern the actions of all parties using the EHR4CR services
18

Electronic Health Records for Clinical Research
Slides courtesy of
Brendan Delaney Professor of General Practice, KCL

Translational Research and Patient Safety in Europe
www.transformproject.eu
• €7.5M EU Framework 7 Project
• March 2010-May 2015*
• Funded under the Patient Safety Work program of FP7
– To support decision making
– To support clinical trials
– As part of a ‘Rapid Learning Healthcare System’
*requested extension to Nov ‘15

Translational Research and Patient Safety in Europe
Aims of TRANSFoRm
• To develop methods, models, services, validated architectures and demonstrations to support the learning health system, via three use cases:
– Epidemiological research using primary care records, including genotype-phenotype studies and other record linkages across multiple sites
– Research workflow embedded in the EHR with PROMS
– Decision support for diagnosis linked to an EHR

Translational Research and Patient Safety in Europe
An Learning Health System that is
trusted and valued
• Building confidence and trust in the data inputs.
– PROVENANCE model
– Model for collecting meta-data for data quality
– PROMs via mobile and web
• Building confidence and trust in the process
– Analysis of EU data protection policies using a graphical approach and a ‘zone model’ (Kuchinke et al Int J Med Inf 214)
– Approach to privacy based on existing processes of data owners and processors based on the zone model

Translational Research and Patient Safety in Europe
Non-care zone
Care zone
Subzone 2
Research zone
Data controller
Res
earc
h q
ues
tio
n
Secondary DB
privacy
filter
Subzone 1
Care DB
GP
filter
privacy
New linked DB
privacy
filter
researcher
Data controller
database
Res
earc
h q
ues
tio
n
filter
privacy Privacy filter
L Linker
L
L

EMIF IMI Project

EMIF consortium
25
56 partners
14 European countries
represented
56 MM € worth of resources
(in-kind / in-cash)
“3 projects in one”
5 year project
(2013 – 2017)
To be the trusted European hub for health care data intelligence
enabling new insights into diseases and treatments

Focus of EMIF Secondary use of health data to improve life sciences research
26
The value of healthcare data for secondary uses in
clinical research and development - Gary K. Mallow,
Merck, HIMSS 2012

Project Vision: “Think Big”
27
To enable and conduct novel research into human health
by utilising human health data at an unprecedented scale
• Access to information on ~ 50 million patients
• AD research on 10-times more subjects than ADNI
• Metabolics research on > 20,000 obese & T2DM subjects
• Linkage of clinical and omics data
• Build a network of data sources and relevant research
• Development of a secure (privacy, legal) modular platform

EMIF – platform for modular extension
28

Available data source – EMIF-Platform
29

EMIF systems view
30

EMIF proposed service levels
31

EMIF Catalogue main headings
32
1. Database Administrative Information
2. Database Characteristics
3. Database Population
4. Data Held
5. Ability to Gather Supplementary Data
6. Ethical Issues
7. De-identification, Linkage
8. Data Set Description, Metadata
9. Examples of Events and Outcomes
10.Documents and Publications
11.Comments
12.EMIF Database Fingerprint Provenance

EMIF profiling tools: examples
33

Detailed analysis - e.g. using TranSMART
34

EMIF: transient “Private Research Environments”
35
EMIF-Platform
Data
Aggregators
Users will only have access to
data they need for an
approved study
Enables each data source to
release only the data set needed
for a study
Only focused ethical approvals are
needed
Constrained set of data sharing
stipulations to comply with
Contains the number of users,
uses, time window of access
Tractable disclosure control
Contained accountability for EMIF User
• Permitted through data
sharing agreements
• Covered by ethical approvals
• Governed by disclosure and
usage policies
• Held by TTP
• Protected by PET
• Fully audited
• Limited availability
Data Sources

EMIF Ethical Code of Practice - in development
36
Developed in order to help ensure:
that the EMIF Platform and Services are used in ways that
comply with legislation and policies on data protection
that EMIF is visibly upholding best practices in the protection of
personal privacy
that EMIF is promoting best practices in the conduct of clinical
research using health data for the public good

EMIF Ethical Code of Practice - main principles
37
Defines the concept of bona fide research, and bona
fide research organisations
Formalises the provisions of data sharing agreements
Stipulates transparency by data sources
of the nature, quality and currency of their data, identifier and
linkage mechanisms
of the arrangements for data sharing, including permitted uses,
approvals process, access fees, publication policy, governance
arrangements
Stipulates the conduct of data users
adhering to permitted uses, maintaining records of users and
use, protecting patient privacy, acknowledging data sources

EMIF Ethical Code of Practice - main principles
38
The CoP also covers:
Collection and use of data subject consent
Ethical approvals
Data and privacy protection
Information security measures
Re-identification and informing research subjects
Collection and use of human biological samples
Establishes oversight by, and escalation to, an Ethical and Governance
Team

39
Need to remove the bottlenecks to accessing and combining
health data from diverse sources across Europe
• Distributed queries
• Only patient counts leave a hospital
• Specific use for protocol feasibility and
patient recruitment
• Platform never stores or communicates
data about single data subjects
• Only treating physicians can re-identify
candidate patients
• Standard operating rules
• Robust identify management,
information security and audit
• Provenance metadata captured throughout
the architecture
• Strong separation between zones for
clinical use and research use
• Pseudo-identification and linkage managed
by a trusted “middle” zone
• Transient data pools per specific
research question and team
• Ethical code of practice
• Limited to bona fide research
• Requirement for data sharing
agreements
• Transparency of data sources
• Pre-agreed purposes of use
• Stipulated conduct of all parties to
protect privacy, ensure equity and
appropriate acknowledgement
There is a need for harmonised best practices & sustainability

Electronic Health Records for Clinical Research

The European Institute for Innovation through Health
Data
41
Specifications and standards
Value
assessment
research
programs
Accreditation
and
Certification
Oversight,
governance,
auditing
Guardian of
shared
Intellectual
Property
Best
practices in
standards
development
and adoption
Critical to the sustainability of a clinical research e-infrastructure
Provides a trusted environment for a research platforms ecosystem to develop
Not-for-profit, formally registered company providing services to registered members (e.g. data providers, data users, service providers)
Funded by license fee, subscriptions, certification, membership (cover cost of operations and providing services to registered members)
Incomes reinvested to improve services & fund public interest research

Governing the EHR4CR ecosystem
42
EHR4CR
SERVICE PROVIDER
APPLICATION PROVIDERS
SERVICE
USER NETWORK
PROVIDER
SERVICE
USER
OTHER DATA
AGGREGATORS
DATA PROVIDER
RESEARCH
SPONSOR
RESEARCH
SPONSOR
DATA PROVIDER
Educate and train
research and ICT
staff
ICT SOLUTION PROVIDERS
Accredit staff
and
organisations
Certify service
providers
and EHR systems
Oversee and audit
governance &
security
RESEARCH
ORGANISATIONS
APPLICATION PROVIDERS
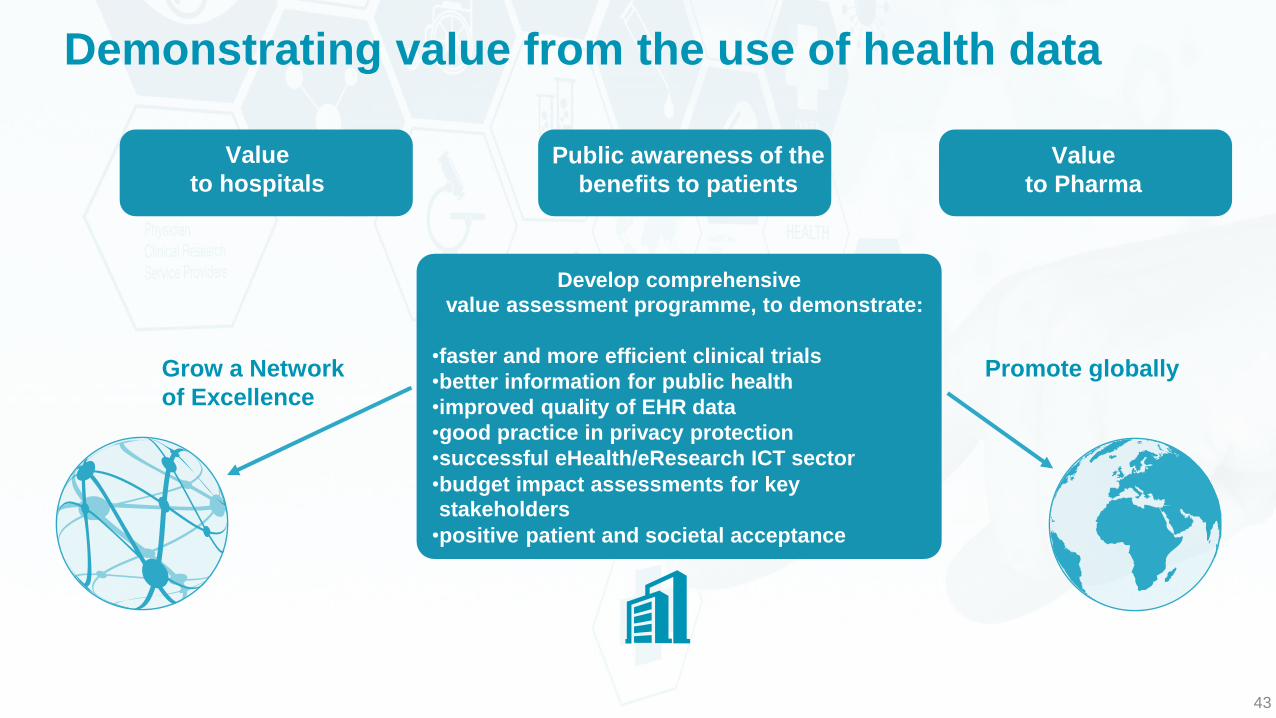
Demonstrating value from the use of health data
43
Develop comprehensive
value assessment programme, to demonstrate:
•faster and more efficient clinical trials •better information for public health •improved quality of EHR data •good practice in privacy protection •successful eHealth/eResearch ICT sector •budget impact assessments for key
stakeholders •positive patient and societal acceptance
Value
to hospitals
Public awareness of the
benefits to patients
Value
to Pharma
Grow a Network
of Excellence
Promote globally

44
Harmonised health information and
standards
Solutions for better quality health data,
and legitimate uses of health data
Intelligence derived from health data
e.g. research, clinical outcomes
Quality assessments, certification and
audit
Synergy and consensus amongst
stakeholders
Best practices in information
governance
The European Institute
for Innovation through
Health Data
Main activities

Building synergy and consensus
The Institute will act as a focal point bringing stakeholders together to share
experiences, agree common priorities and approaches, working towards
convergence and cross-fertilisation between:
45
Patient associations
Citizen, family and carer associations
Health professional associations
Clinical and informatics academia
Healthcare providers
National decision makers
Third party payers, commissioners
EHR system and applications vendors
Medical Device vendors
Pharma, Bio-tech
Regulators
Standards development organisations (SDO)
Multi-national decision makers
Social care providers
Electronic health (eHealth) competence centers

46
THANK YOU