registered managers network 20 th march 2014
TRANSCRIPT

Registered Managers Network20th March 2014



Registration RegulationsRegistration Regulations
Proposed ChangesProposed Changes


The Francis ReportFundamental Standards below which care should never fall
Care Quality Commission
Alan Rosenbach – SCA Conference“A New Start” – November Network Meeting
Draft Regulations to replace Essential Standards
Duty of Candour and Fit and Proper Persons Test. This consultation does not cover the proposed new Duty of Candour or the Fit and Proper Persons requirement for Directors of providers registered with CQC. We will consult separately on each of these proposals, although the intention is to introduce these measures alongside the Fundamental Standards as part of the same set of regulations.
“The current outcomes are over-bureaucratic and fail to separate clearly what is absolutely essential from that which is merely desirable.” Francis Enquiry
Fundamental Standards More Precise – Outcomes to Achieve or AvoidClearly Stated
“..for those cases that CQC considers serious enough to warrant prosecution, it will not need to issue a warning notice before bringing a prosecution. ……….that stronger enforcement action should be available where necessary.”
This supports CQC's new emerging approach to inspection and enforcement which is based less around checking compliance with detailed regulations, and is instead focuses on five questions about care: • Is it safe? • Is it effective? • Is it responsive? • Is it caring? • Is it well-led?
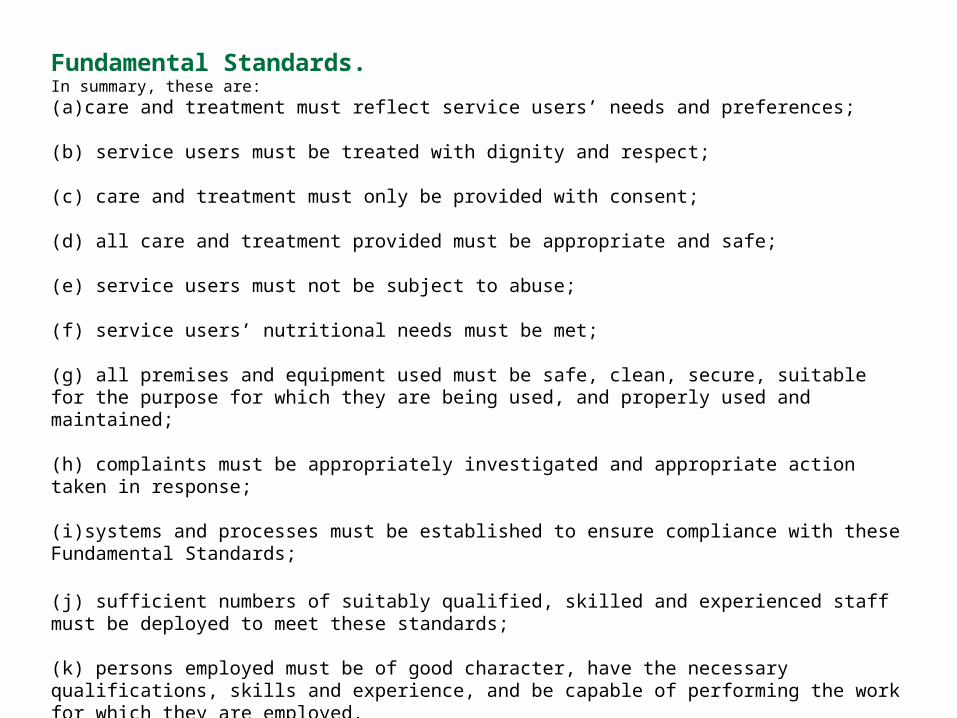
Fundamental Standards.In summary, these are: (a)care and treatment must reflect service users’ needs and preferences;
(b) service users must be treated with dignity and respect;
(c) care and treatment must only be provided with consent;
(d) all care and treatment provided must be appropriate and safe; (e) service users must not be subject to abuse;
(f) service users’ nutritional needs must be met;
(g) all premises and equipment used must be safe, clean, secure, suitable for the purpose for which they are being used, and properly used and maintained;
(h) complaints must be appropriately investigated and appropriate action taken in response;
(i)systems and processes must be established to ensure compliance with these Fundamental Standards;
(j) sufficient numbers of suitably qualified, skilled and experienced staff must be deployed to meet these standards;
(k) persons employed must be of good character, have the necessary qualifications, skills and experience, and be capable of performing the work for which they are employed.
Clearer offences - removing the need for a notice for prosecution for some offences Our draft requirements include clear outcomes that providers must meet (for example, “service users must not be subject to abuse”). If a provider is not meeting that outcome, they are committing an offence. In all cases it is important that providers can be held to account for the quality of care that they have provided, including by the courts where this is appropriate. Our intention is that where a breach of a requirement has an outcome which could directly result in a person or group of people being harmed, CQC has the power to bring a prosecution straight away, but where a breach has not or would not directly result in harm, CQC would use its other enforcement powers.

Annexe 1
General 3. A registered person must, in so far as they are applicable to each regulated activity, comply with regulations 4 to 14 in carrying on the regulated activities in respect of which they are registered.
SECTION 2 Fundamental standards
Person-centred care 4.—(1) The care and treatment of service users must reflect their needs and preferences.Dignity and respect 5.—(1) Service users must be treated with dignity and respect. Need for consent 6.—(1) Care and treatment must only be provided with, and in accordance with, the consent of the relevant person. Safe and appropriate care and treatment 7.—(1) All care and treatment provided to service users must be appropriate and safe. Safeguarding service users from abuse 8.—(1) Service users must not be subject to abuse.
Meeting nutritional needs 9.—(1) The nutritional needs of service users must be met. Cleanliness, safety and suitability of premises and equipment 10.—(1) All premises and equipment used by the registered provider must, in accordance with generally accepted professional standards, practices and principles, be— (a) safe, clean and secure, (b) suitable for the purpose for which they are being used, and (c) properly used and maintained. Receiving and acting on complaints 11.—(1) Any complaint received must be appropriately investigated and appropriate action must be taken in response to the complaint. Good governance 12.—(1) Systems or processes must be established and operated effectively to ensure compliance with the requirements in this Part. Staffing 13.—(1) The registered person must deploy sufficient numbers of suitably qualified, skilled and experienced persons in order to meet the requirements of this Part.

Fit and proper persons employed 14.—(1) Persons employed by the registered person must— (a) be of good character, (b) have the qualifications, skills and experience which are necessary for the work to be performed, and (c) be physically and mentally capable, after reasonable adjustments are made, of properly performing tasks which are intrinsic to the work for which they are employed.

Safeguarding service users from abuse 8.—(1) Service users must not be subject to abuse. (2) Appropriate steps must be taken— (i) to prevent abuse before it occurs, and (ii) to respond to any allegation of abuse.
(3) For the purposes of this regulation, “abuse”, in relation to a service user, includes— (a) sexual abuse, (b) physical or psychological ill-treatment, (c) theft, misuse or misappropriation of money or property, or (d) neglect and acts of omission which cause harm to a service user or place the service user at risk of harm.

To respond to this consultation, you can:
Answer the questions online, at http://consultations.dh.gov.uk/standards/fundamental-standards
Email your responses to [email protected]
Post your responses to: Fundamental Standards Consultation c/o John Culkin Room 2E11 Quarry House Quarry Hill Leeds, West Yorkshire LS2 7UE

Key findings
The Committee’s key finding is that the Act is not widely implemented. To address this the Committee recommends that responsibility for implementing the Act be given to an independent body.
The Committee’s second key finding is that the Deprivation of Liberty Safeguards are not fit for purpose. The Committee recommends that they be replaced with new provisions.
Lord Hardie, Chairman of the Committee said:
“The Committee believes that the Act is good and it needs to be implemented. What we want to see is a change in attitudes and practice which reflects the empowering ethos of the Act. To achieve this we recommend that overall responsibility for the Act be given to an independent body whose task will be to oversee, monitor and drive forward implementation.”
“We were very concerned by what we heard about the safeguards. The evidence suggests that tens of thousands of people are being deprived of their liberty without the protection of the law, and without the protection that Parliament intended. Worse still, in some cases the safeguards are being wilfully used to oppress individuals and to force decisions upon them. The Government needs to go back to the drawing board to draft replacement provisions that are easy to understand and implement, and in keeping with the style and ethos of the Mental Capacity Act.”



Number of recommendations applicable to the organisation 0Number of recommendations met 0Percentage of recommendations met
NICE recommendationGuideline reference
Who should take action?
Is the recommendation relevant to the organisation? Current activity/evidence
Developing and reviewing policies for safe and effective use of medicinesCommissioners and providers (organisations that directly provide health or social care services) should review their policies, processes and local governance arrangements, making sure that it is clear who is accountable and responsible for using medicines safely and effectively in care homes. 1.1.1 CommissionersCare home providers should have a care home medicines policy, which they review to make sure it is up to date, and is based on current legislation and the best available evidence. The policy should include written processes for:● sharing information about a resident's medicines, including when they transfer between care settings● ensuring that records are accurate and up to date● identifying, reporting and reviewing medicines-related problems● keeping residents safe (safeguarding)● accurately listing a resident's medicines (medicines reconciliation)● reviewing medicines (medication review)● ordering medicines● receiving, storing and disposing of medicines ● helping residents to look after and take their medicines themselves (self-administration)● care home staff administering medicines to residents, including staff training and competence requirements● care home staff giving medicines to residents without their knowledge (covert administration)● care home staff giving non-prescription and over-the-counter products to residents (homely remedies), if appropriate. 1.1.2 Care home providers
Supporting residents to make informed decisions and recording these decisionsHealth and social care practitioners (care home staff, social workers, case managers,GPs, pharmacists and community nurses) should ensure that care home residents have the same opportunities to be involved in decisions about their treatment and care as people who do not live in care homes, and that residents get the support they need to help them to take a full part in making decisions. 1.2.1
Health and social care practitioners (care home staff, social workers, case managers, GPs, pharmacists and community nurses)
The health professional prescribing a medicine or care home staff should record a resident's informed consent in the resident's care record. Consent does not need to be recorded each time the medicine is given but a record of the administration should be made on the medicines administration record. 1.2.2
Care home staff (registered nurses and social care practitioners working in care homes)Recommendations for health and social care practitioners also apply to care home staff / Health
Care home staff (registered nurses and social care practitioners working in care homes) should record the circumstances and reasons why a resident refuses a medicine (if the resident will give a reason) in the resident's care record and medicines administration record, unless there is already an agreed plan of what to do when that resident refuses their medicines. If the resident agrees, care home staff should tell the health professional who prescribed the medicine about any ongoing refusal and inform the supplying pharmacy, to prevent further supply to the care home. 1.2.3
Care home staff (registered nurses and social care practitioners working in care homes)Recommendations for health and social care practitioners also apply to care home staff
Health and social care practitioners should identify and record anything that may hinder a resident giving informed consent. Things to look out for include mental health problems, lack of (mental) capacity to make decisions, health problems (suchas problems with vision and hearing), difficulties with reading, speaking or understanding English and cultural differences. These should be taken into account when seeking informed consent and should be regularly reviewed. 1.2.4
Health and social care practitioners (care home staff, social workers, case managers, GPs, pharmacists and community nurses)
Baseline assessment tool for NICE guideline on Managing medicines in care homes




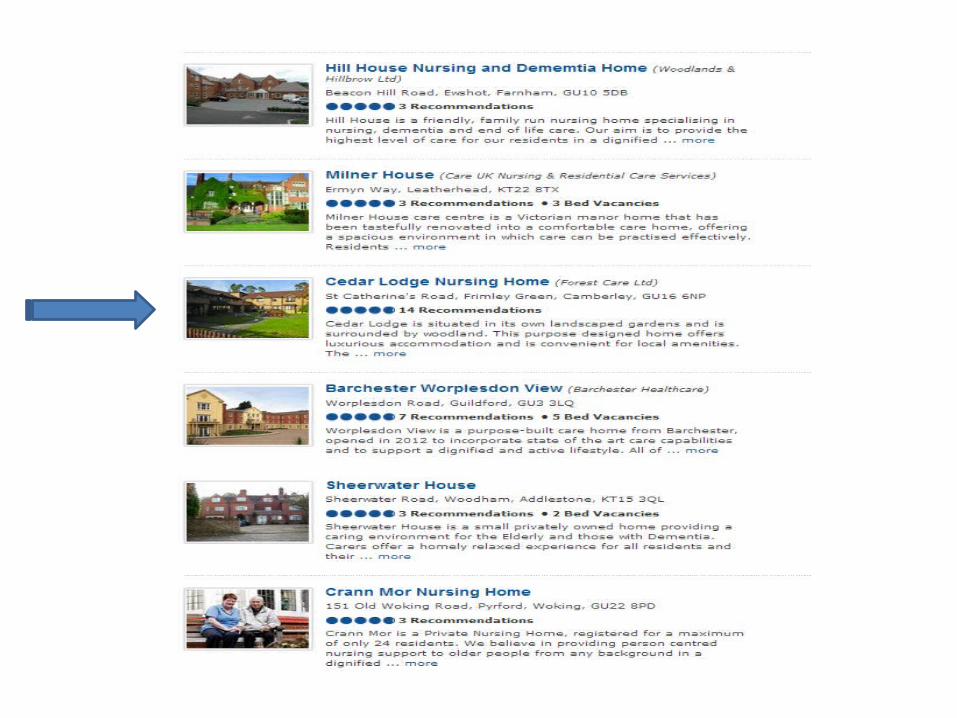
Rapid increase in sites offering information on perceived quality of care services
Main types:
•Assessment and Approval
•Consumer Feedback – Trip Advisor style
•Listing Sites also increasing – links to CQC are most common quality checkn.b. Some established listing sites starting to introduce ratings facility
Why does it matter?
Web search is becoming the most common tool for finding goods/services
Reputation/Competition/Marketing


Press release DH 25th April
•comments from the public on their experience of care and services, including links to existing comment sites•from next month the ability for the public to give services star ratings•Ofsted-style ratings for care services as they are developed
David Behan:“As this online resource develops, care homes and other registered care and support serviceswill expand their profiles to include performance against specific standards to allow peopleto compare different providers. This will include falls, bed sores, medication management,staff stability, training of staff as well as missed and timely visits for home care.”

The Department of Health has been engaging with a number of third party websites tobring their social care reviews into NHS Choices. The following organisations have helpedmake comments from their site available to NHS Choices, with more set to follow:
Good Care GuideCompare Care HomeReally CareYourcarehome.co.ukSocial Care Institute for ExcellenceSearch Care
These sites have a direct feed to CQC

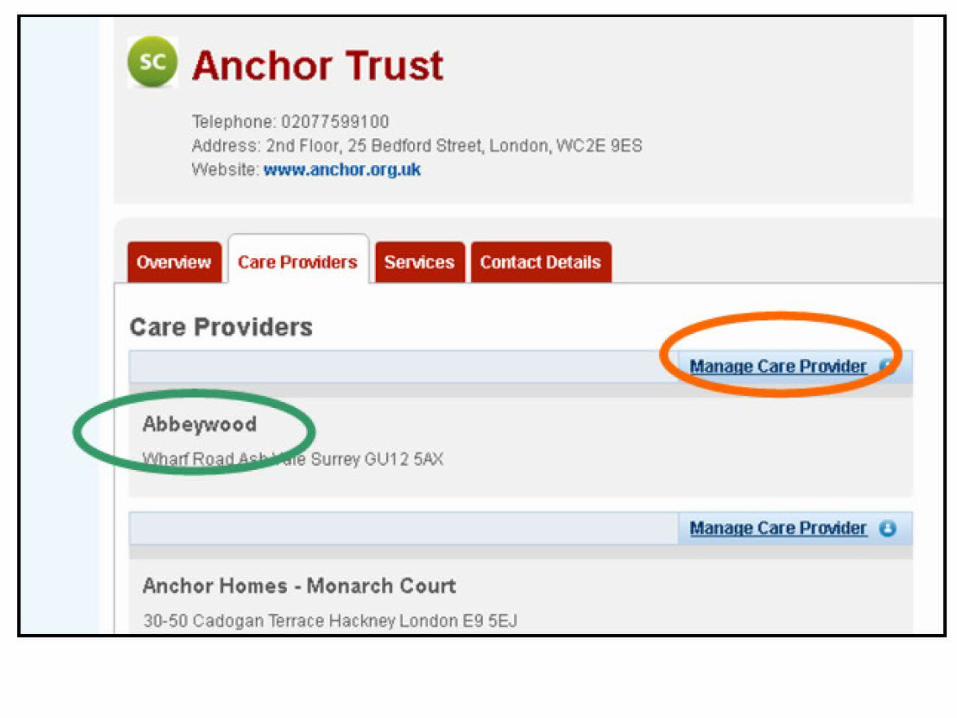
All Providers Have A Profile Already On Here
You Can Manage It or Leave It To Chance



Obtaining your editing rightsTo obtain editing rights for your profile, please [email protected], providing your full name, email address, jobtitle, contact number and postcode for each care organisation profile you would liketo manage.If your care service is part of a larger organisation or operates from severalsites, please contact your head office in the first instance before requestingediting access.

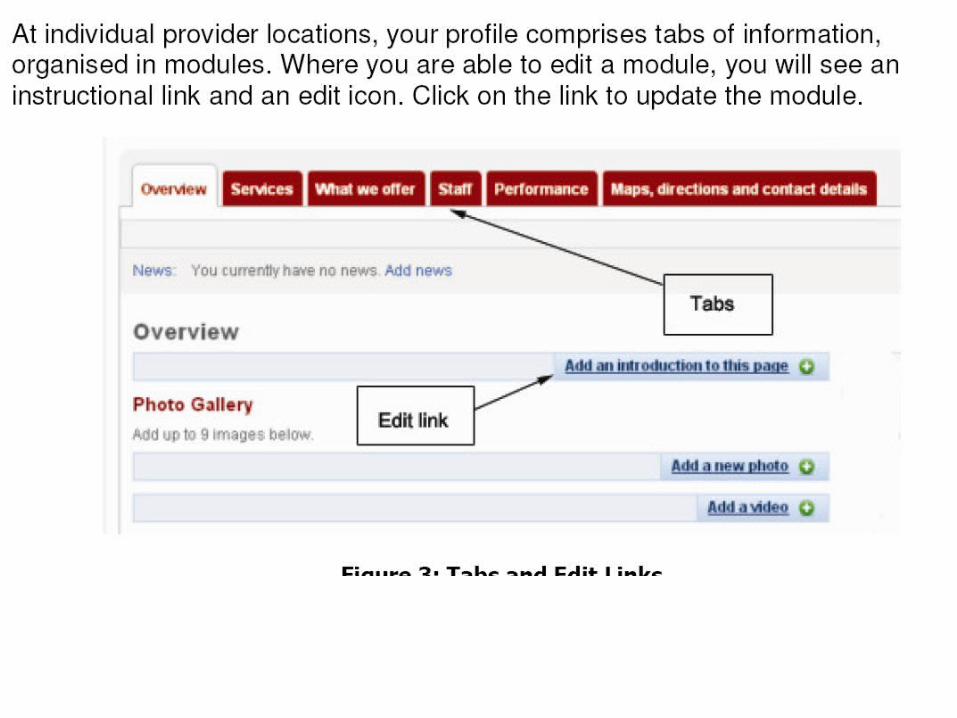
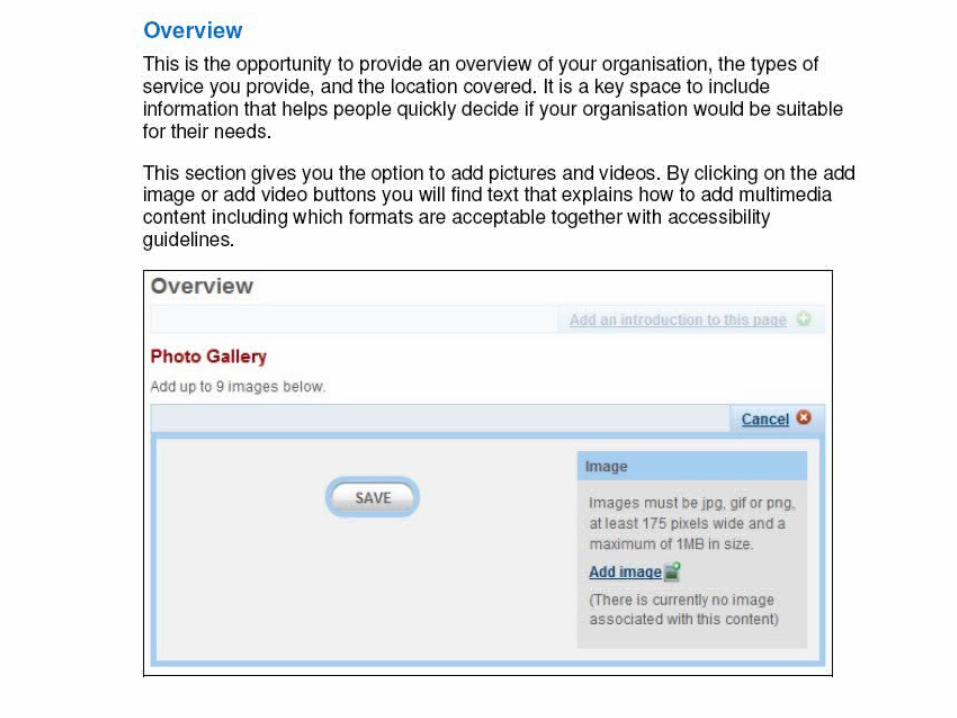
Overview
Services
What we Offer
Staff
Performance
Maps, directions, and contact details