salpingostomy in the treatment of hydrosalpinx: a ... · introduction...
TRANSCRIPT

REVIEW Infertility
Salpingostomy in the treatmentof hydrosalpinx: a systematic reviewand meta-analysisJ. Chu1, H.M. Harb1, I.D. Gallos1, R. Dhillon1, F.M. Al-Rshoud2,L. Robinson1, and A. Coomarasamy1,*1Academic Department, School of Clinical and Experimental Medicine, University of Birmingham, 3rd Floor, Birmingham Women’s HospitalFoundation Trust, Metchley Park Road, Edgbaston, Birmingham B15 2TG, UK 2Medical School, Hashemite University, Az Zarqa, Jordan
*Correspondence address. Academic Department, School of Clinical and Experimental Medicine, University of Birmingham, 3rd Floor,Birmingham Women’s Hospital Foundation Trust, Metchley Park Road, Edgbaston, Birmingham, B15 2TG, UK. Tel: +44-121-623-6835;Fax: +44-121-626-6619; E-mail: [email protected]
Submitted on December 22, 2014; resubmitted on May 18, 2015; accepted on May 20, 2015
study question: What is the chance of natural conception when salpingostomy is used to treat hydrosalpinx?.
summaryanswer: The natural clinical pregnancy rate following salpingostomy is 27%, in the hands of experienced surgeons who publishtheir results.
what is known already: Tubal surgery is not commonly offered for women withhydrosalpinges since the advent of assisted conceptiontreatment. This is the first systematic review to investigate natural conception rates following salpingostomy in the treatment of hydrosalpinx.
study design, size, duration: A systematic review and meta-analysis of 22 observational studies encompasses 2810 patientsundergoing salpingostomy and attempting natural conception.
participants/materials, setting, methods: Literature searches were conducted to retrieve observational studies whichreported salpingostomy for hydrosalpinx. Databases searched included MEDLINE, EMBASE, Cochrane Central Register of Controlled Trialsand CINAHL, with no language restriction. Only studies that focused on salpingostomy (rather than other tubal conserving surgeries) for the treat-ment of hydrosalpinx were included. A total of 22 studies matched the inclusion criteria.
main results and the role of chance: The pooled natural clinical pregnancy rate from the 22 observational studies (including2810 patients) was 27% (95% confidence interval (CI): 25–29%) after salpingostomy was performed for hydrosalpinx. The cumulative clinicalpregnancy rates were 8.7% (95% CI: 6.6–11.5%) at 6 months, 13.3% (95% CI: 10.6–16.7%) at 9 months, 20.0% (95% CI: 17.5–22.8%) at 12months, 21.2% (95% CI: 18.6–24.1%) at 18 months and 25.5% (95% CI: 22.2–29.4%) at 24 months after salpingostomy. The pooled livebirth rate (10 studies, 1469 patients) was 25% (95% CI: 22–28%) after salpingostomy was performed for hydrosalpinx. The pooled ectopic preg-nancy rate (19 studies, 2662 patients) was 10% (95% CI: 9–11%). The pooled miscarriage rate (seven studies, 924 patients) was 7% (95% CI:6–9%). The included studies scored well on the Newcastle Ottawa quality assessment scale.
limitations, reasons for caution: Strict inclusion criteria were used in the conduct of the systematic review. However, thestudies included are clinically heterogeneous in many aspects including patient characteristics, surgical technique and duration of follow-upafter salpingostomy.
wider implications of the findings: The findings of this systematic review suggest that salpingostomy is an alternative treatmentstrategy to tubal clipping or salpingectomy in patients presenting to fertility services with hydrosalpinx. Further prospective, large and high qualitystudies are needed to identify the subpopulation that would most benefit from tube conserving surgery.
study funding/competing interest(s): No external funding was either sought or obtained for this study. The authors have nocompeting interests to declare.
trial registration number: N/A.
Key words: hydrosalpinx / salpingostomy / clinical pregnancy / tubal surgery / tubal disease
& The Author 2015. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved.For Permissions, please email: [email protected]
Human Reproduction, Vol.0, No.0 pp. 1–14, 2015
doi:10.1093/humrep/dev135
Hum. Reprod. Advance Access published June 16, 2015 by guest on June 17, 2015
http://humrep.oxfordjournals.org/
Dow
nloaded from

IntroductionApproximately 25% of all female fertility is caused by tubal factors (Sharifand Coomarasamy 2012). The majority of tubal infertility is caused byascending infection from sexually transmitted diseases leading to pelvic in-flammatory disease (PID) (Bahamondes et al., 1984). If untreated, severePID can lead to chronic inflammation of the distal Fallopian tubes, whichcan lead to blockage and fluid accumulation known as a hydrosalpinx.
There is substantial evidence that proceeding with in vitro fertilization(IVF)/intra-cytoplasmic sprem injection (ICSI) treatment with an un-treated hydrosalpinx approximately halves the chances of clinical preg-nancy (Andersen et al., 1994; Kassabji et al., 1994; Strandell et al.,1994, 1999; Vandromme et al., 1995; Akman et al., 1996; Flemmingand Hull, 1996; Katz et al., 1996; Blazer et al., 1997; Wainer et al.,1997; Freeman et al., 1998; Murray et al., 1998; Van Voorhis et al.,1998; Zeyneloglu et al., 1998; Camus et al., 1999). The exact cause forthis has not been fully confirmed but it has been suggested that thismay be due to the embryotoxic effect (Kassabji et al., 1994; Savarisand Giudice, 2007) or the mechanical washout effect of the fluid (Stran-dell et al., 1994).
Before IVF/ICSI treatment became commonplace it was the remitof reproductive surgeons to correct tubal pathology (including hydrosal-pinx) to enable women to increase their chances of natural conception(Winston and Margara, 1991; Winston, 1992; Vandromme et al.,1995; Chanelles et al., 2011). These techniques included peritubal adhe-siolysis, fimbrioplasty and in the most severe tubal disease, salpingos-tomy. However, since the increased use of IVF/ICSI treatment,salpingostomy is now rarely performed with the preference towardssterilizing surgery, such as salpingectomy and tubal occlusion, toensure that hydrosalpingeal fluid is kept separate from the endometrialcavity where the embryo is placed. There is evidence that using thesesterilizing techniques doubles the chances of IVF/ICSI success (Strandellet al., 1994; Akman et al., 1996; Johnson et al., 2010) in women withhydrosalpinges and this has now become common clinical practice.
The disadvantage of sterilizing surgery is that the patient with bilateraldisease is then reliant on IVF/ICSI treatment for all future attempts atachieving pregnancy. An alternative management strategy, which con-serves a patient’s Fallopian tubes, would be to perform salpingostomyfollowed by a trial of natural conception. If pregnancy is not achieved,women can then be offered IVF treatment with or without sterilizingsurgery. The aim of our review was to investigate the chances ofnatural pregnancy after salpingostomy is performed for hydrosalpinx.
Methods
Literature searchThe population of interest consisted of women who underwent salpingos-tomy for hydrosalpinx. The primary outcome was natural clinical pregnancy.Secondary outcomes included live birth rates, ectopic pregnancy and miscar-riage rates.
The following electronic databases were searched: MEDLINE, EMBASE,Cochrane Central Registerof Controlled Trials and CINAHL (from inceptionto March 2015). A search strategy was developed based on the following keywords and/or medical subject heading (MeSH) terms: tubal surgery, salpin-gectomy, salpingostomy, in vitro fertilization, intracytoplasmic sperm injec-tion, assisted reproductive techniques, hydrosalpinx, Fallopian tube diseaseand pregnancy. The reference lists of all primary and review articles were
examined to identify relevant articles not captured by the electronicsearches. No language restrictions were applied in any of the searches orstudy selection.
Study selectionCriteria for inclusion in the study were established prior to the literaturesearch. Study selection was carried out by four independent reviewers(J.C., H.M.H., F.M.A. and R.D.). First, the titles and abstracts of the electronicsearches were scrutinized by the independent reviewers. Each title and ab-stract were included or excluded independently according to the predefinedinclusion criteria; any disagreements regarding inclusion were resolved by afurther reviewer (I.D.G.). The full manuscripts of the titles and abstractsthat were considered to be relevant for inclusion were obtained. In casesof duplicate publication, the most recent and complete versions wereselected. Studies that did not explicitly report results from salpingostomyfor hydrosalpinx were excluded. In particular, we excluded studies thatwere ambiguous with their description of surgical treatment and did notreport specifically on salpingostomy.
Data were extracted from full manuscripts by two independent reviewers(J.C. and H.M.H.).
Validity assessmentTwo reviewers (J.C. and H.M.H.) completed the quality assessment. TheNewcastle-Ottawa Quality Assessment Scales for Observational studieswere implemented for quality assessment. The quality checklist awardsone star as maximum for all items except comparability where a maximumof two stars can be awarded. We used an arbitrary score based on the as-sumption of equal weight of all items included in the Newcastle-OttawaScale. This was used to give a quantitative appraisal of overall quality of theindividual studies. The score ranged from 0 to 9, with a score of either 0 or1 for each item. From each study, outcome data were extracted by tworeviewers (J.C. and H.M.H.).
Statistical analysisClinical pregnancy, ectopic pregnancy, live birth and miscarriage rates wereextracted from each study. The log of the ratio and its corresponding stand-ard error for each study was computed. Meta-analysis using inverse-varianceweighting was performed to calculate the random-effects summary esti-mates. The square root of this number is the estimated SD of the underlyingeffects across studies. Because we had relative measures of effect, the confi-dence intervals (CI) were centred on the natural logarithm of the pooled es-timate and the limits exponentiated to obtain an interval on the ratio scale.Forest plots were created for each outcome, showing individual study pro-portions with CIs and the overall DerSimonian–Laird pooled estimate.Heterogeneity of the treatment effects was assessed graphically withforest plots and statistically analysed using the x2-test. Statistical analyseswere performed using Stata 12.0 (StataCorp, College Station, TX, USA).
Lastly, we performed a stratified analysis splitting studies from 1972 to1999 and from 2000 to 2014 to explore the temporal effects on clinical preg-nancy rates.
ResultsThe PRISMA flow diagram (Liberati et al., 2009; Moher et al., 2009) of thereview process is presented in Fig. 1. The search strategy yielded 14 396citations of which 14 231 publications were excluded because it was clearfrom the title or abstract that they did not fulfil the selection criteria. Fullmanuscripts of 165 articles were obtained. A total of 143 of these pub-lications were excluded because 63 were review articles, opinion letters,case reports or questionnaires; two were duplicate articles; 17 articles
2 Chu et al.
by guest on June 17, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from

did not specify the nature of the tubal disease and 46 performed tubalsurgeries other than salpingostomy, e.g. salpingectomy, essure or trans-vaginal drainage of hydrosalpinx; six reported outcomes that were not ofinterest, e.g. ovarian response after tubal surgery or endometrialreceptivity; two articles reported salpingostomy in the IVF populationand seven articles reported data that could not be extracted. There-fore, the total number of observational studies included in the reviewwas 22.
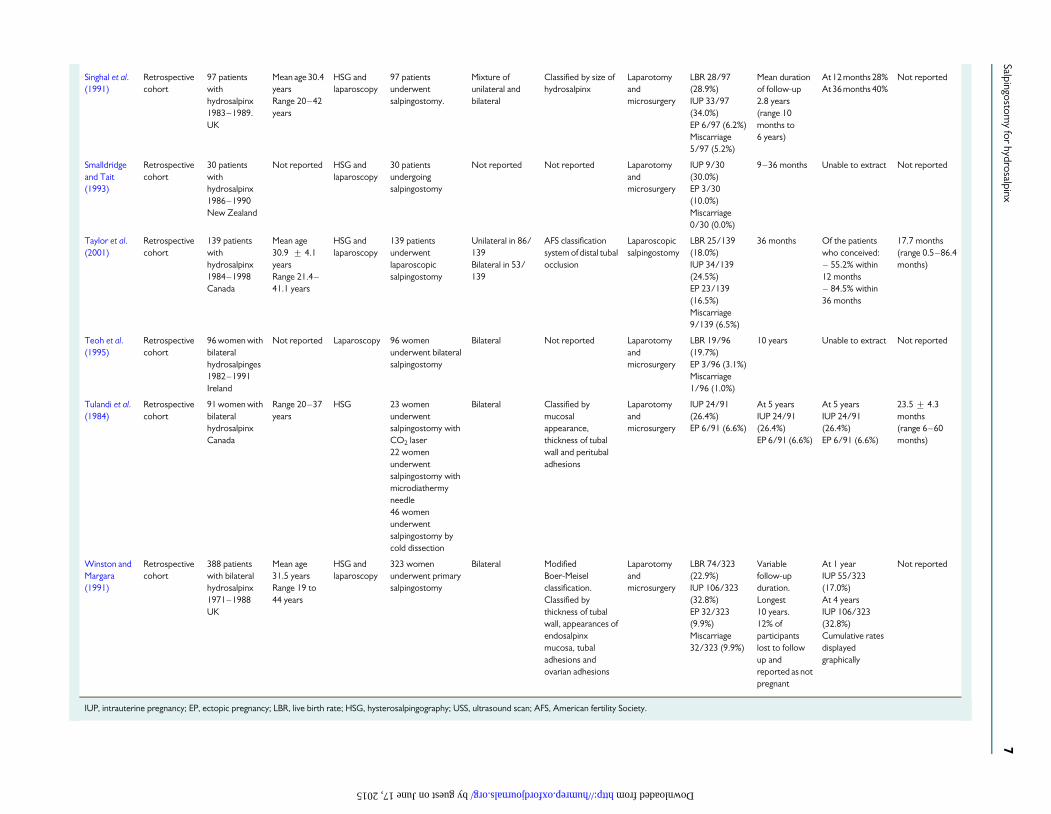
Study characteristicsThe characteristics of the 22 studies are presented in Table I. Publicationdates of the studies varied between 1972 and 2014. Sample sizes variedfrom 10 women to 467 women. Of the 22 included studies, 13 reportedthe ages of their sample populations. Twelve of the studies had a meanage ranged from 27.5 to 32.6 years. One study had a higher mean ageof 35.5 years. Five studies diagnosed hydrosalpinx using hysterosalpingo-gram, four diagnosed hydrosalpinx using laparoscopy with 13 studiesusing a combination of the two diagnostic modalities. Thirteen of the22 studies reported results after laparotomy and microsurgery, sixreported results after laparoscopic salpingostomy and three reported
results from mixed surgical techniques. Fourteen of the includedstudies classified the severity of tubal disease. Two studies reportedresults after unilateral salpingostomy, five studies reported results afterbilateral salpingostomy, while the remaining 15 studies reported onresults from a mixture of unilateral and bilateral disease. After surgerythe length of follow-up of women undergoing salpingostomy variedbetween 12 and 71 months.
The results of the Newcastle-Ottawa Quality Assessment are pre-sented in Table II. All studies scored well on the Newcastle-OttawaQuality Assessment Scale, achieving scores between six and eight.
Clinical pregnancyAll 22 studies reported on clinical pregnancy rate as an outcome (Fig. 2).These studies showed a pooled clinical pregnancy rate of 27% (95% CI:25–29%). There was a substantial level of heterogeneity in these studiesindicated by an I2 value of 53.9%, P ¼ 0.001.
Clinical pregnancy rates by publication dateThe studies were grouped according to their publication date (Fig. 3).Studies published before 2000 had a pooled clinical pregnancy rate of
Figure 1 Study selection for review on salpingostomy treatment for hydrosalpinx and natural conception.
Salpingostomy for hydrosalpinx 3
by guest on June 17, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from

..........................................................................................................................................................................................................................................................
Table I Study characteristics of included studies.
Author(year)
Studydesign
Studypopulation
Age ofstudypopulation
Method ofdiagnosis
Salpingostomygroup
Unilateralor bilateraldisease
Classification ofhydrosalpinx
Surgicaltechnique
Outcomes(pregnancyrate)
Duration offollow-up
Cumulativepregnancydata
Mean time toconception
Audebert(1980)
Retrospectivecohort
172 patientswithhydrosalpinx1976–1979France
Range20–40 years
Laparoscopy 96 salpingostomy toampulla, isthmic,type 1 and type 2
Mixture By stage ofhydrosalpinx
Laparotomyandmicrosurgery
IUP 29/96(30.2%)
24 months 1–3 month1/96 (1.0%)4–6 months7/96 (7.3%)7–9 months14/96 (14.6%)10–12 months22/96 (22.9%)12–23 months27/96 (28.1%)At 24 months29/96 (30.2%)
Not reported
Audebertet al. (2014)
Retrospectivecohort
434 patientswith distal tubalocclusion1988–2000France
Range21–42 years
HSG andlaparoscopy
434 patientsunderwent evertingneosalpingostomy
Mixture Classified accordingto mucosalappearancesand adhesions
Laparoscopy IUP 125/434(28.8%)LBR 106/434(24.4%)EP 43/434(9.9%)
60 months At 3 months IUP14/432 (3.2%)At 6 months IUP40/432 (9.3%)At 9 months IUP58/432 (13.4%)At 12 months IUP70/432 (3.2%)At 18 months IUP85/432 (19.7%)At 24 months IUP101/432 (23.4%)At 36 months IUP116/432 (26.9%)
Not reported
Bayrak et al.(2006)
Retrospectivecohort
40 patientshydrosalpinges1999–2002USA
Mean age35.5 + 5.5yearsRange21–42 years
HSG 40 patientsunderwent cuffsalpingostomyAuthors noted highage of studypopulation
Bilateral 30/40(75.0%)Unilateral 10/40(25.0%)
By size of thehydrosalpinx,presence of rugaeand adhesions
Laparoscopy32/40(80.0%)Laparotomy8/40 (20.0%)
IUP 2/40(5.0%)EP 1/40 (2.5%)
22 months At 4 months IUP1/40 (2.5%)At 7 months IUP2/40 (5.0%)At 22 months IUP2/40 (5.0%)
Not reported
Beyth andBercovici(1982)
Retrospectivecohort
31 patientswithhydrosalpinx1976–1979Israel
Range20–43 years
HSG andlaparoscopy
31 patientsunderwentsalpingostomy
Mixture By size ofhydrosalpinx
Laparotomyandmicrosurgery
IUP 5/31(16.1%)
42 months Not reported Not reported
Boer-Meiselet al. (1986)
Retrospectivecohort
108 patientswithhydrosalpinxtubal infertility1974–1981TheNetherlands
Mean age 27.5yearsRange20–40 years
HSG andlaparoscopy
108 patentsunderwent terminalsalpingostomy
MixtureBilateral 74/108(68.5%)Unilateral 34/108(31.5%)
Classified by size ofhydrosalpinx,thickness of tubalwall and condition ofendosalpinx
Laparotomy IUP 50/108(46.3%)term pregnancy24/108 (22.2%)EP 19/108(17.6%)miscarriage7/108 (6.5%)
Unable toextract data
Not reported Not reported(only mediantime of 10.5cycles reported)
4C
huetal.
by guest on June 17, 2015 http://humrep.oxfordjournals.org/ Downloaded from

Bontis andDinas (2000)
Retrospectivecohort
258 patientswithhydrosalpinxGreece
Not reported Notreported
258 patientsunderwent surgeryfor salpingostomy
Not reported Classified by degreeof severity Stages I–IV
39/258(15.1%)patientslaparoscopy219/258(84.9%)patientslaparotomyandmicrosurgery
IUP 44/258(17.1%)EP 23/258(8.9%)
36 months At 36 monthsIUP 44/258(17.1%)
Not reported
Chanelleset al. (2011)
Retrospectivecohort toassess amanagementprotocol
81 patientswithhydrosalpinxmanaged with atubal surgeryprotocol2003–2007France
Mean age 32.6years +4.7years
HSG or USSandlaparoscopy
10 patientsunderwentunilateralsalpingostomy
Unilateral Classified bymucosal and tubalstages I– IV
Not reported IUP 3/10 (30%) 12 months At 12 monthsIUP 3/10 (30%)
2 months
Chong(1991)
Retrospectivecohort
34 patientswith bilateralhydrosalpinx1982–1988USA
Mean age 30.2 HSG 19 patientsunderwent cufftechniquesalpingostomy15 patientsunderwent Bruhattechniquesalpingostomy
Bilateral Not reported Laparotomyandmicrosurgery
IUP 9/34(26.5%)EP 2/34 (5.9%)
Not reported No reported Not reported
Cohen et al.(1972)
Retrospectivecohort
706 patientsundergoingtubal surgeryFrance
Not reported Notreported
188 patientsunderwentunilateralsalpingostomy:70 terminalsalpingostomy68 medio-ampullarsalpingostomy.279 patientsunderwent bilateralsalpingostomy:104 terminalsalpingostomy,122medio-ampullarsalpingostomy.
MixtureBilateral 188/467(40.3%)Unilateral279/467 (59.7%)
Not reported Laparotomy IUP 89/467(19.1%)EP 46/467(9.9%)
18 months At 18 monthsIUP 89/467(19.1%)
Not reported
Dubuissonet al. (1994)
Retrospectivecohort
81 infertilewomen withhydrosalpinx1986–1991France
Mean age30.1 + 4.7yearsRange 20–39years
HSG 81 womenunderwentunilateral orbilateralsalpingostomy
MixtureBilateral 39/81(48.1%)Unilateral42/81 (51.9%)
Classified byseverity of disease.Stages I-IV
Laparoscopicsalpingostomy
IUP 26/81(32.1%)EP 4/81 (4.9%)
24 months IUP cumulativeAt 12 months26.4%At 18 months28.7%At 24 months29.8%
Not reported
Continued
Salpingostomy
forhydrosalpinx
5
by guest on June 17, 2015 http://humrep.oxfordjournals.org/ Downloaded from

..........................................................................................................................................................................................................................................................
Table I Continued
Author(year)
Studydesign
Studypopulation
Age ofstudypopulation
Method ofdiagnosis
Salpingostomygroup
Unilateralor bilateraldisease
Classification ofhydrosalpinx
Surgicaltechnique
Outcomes(pregnancyrate)
Duration offollow-up
Cumulativepregnancydata
Mean time toconception
Dubuissonet al. (1995)
Retrospectivecohort
123 infertilewomen withhydrosalpinx1986–1993
Mean age28.5 + 4.9yearsRange 19–39years
HSG 123 underwentlaparoscopicsalpingostomy
Not reported Classified byseverity of disease.Stages I-IV
Laparoscopicsalpingostomy
IUP 34/123(30.4%)EP 9/123 (8%)
Over 24months
IUP cumulative23.5% at12 months26.0% at15 months27.7% at18 months28.6% at24 months
Not reported
Jansen(1980)
Retrospectivecohort
107 patientswithhydrosalpinx1966–1975Australia
All patients,40
Notreported
91 patientsunderwent bilateralsalpingostomy16 patientsunderwentunilateralsalpingostomy
MixtureBilateral 91/107(85.0%)Unilateral16/107 (15.0%)
Not reported Laparotomy IUP 24/107(22.4%)
Unable toextract
Unable to extract Unilateralsalpingostomy104 weeksBilateralsalpingostomy 61weeks
Kosasa andHale (1988)
Retrospectivecohort
93 patientswithhydrosalpinx1981–1986Hawaii
Mean age31 yearsRange 21–39years
Laparoscopy 93 patientsunderwentmicrosurgicalevertingsalpingostomy
MixtureUnilateral 27/93(29.0%)Bilateral 66/93(71.0%)
Not reported Laparotomyandmicrosurgery
Termpregnancy34/93 (36%)EP 13/93 (14%)Miscarriage3/93 (3%)
Not reported Not reported Not reported
Mage andBruhat(1983)
Retrospectivecohort
68 patientswithhydrosalpinx1977–1981France
Range 20–38years
HSG andlaparoscopy
30 patientsunderwentsalpingostomy byelectrosurgery38 patientsunderwentsalpingostomy byCO2 laser
Mixture Not reported Laparotomyandmicrosurgery
Termpregnancy14/68 (20.6%)EP 6/68 (8.8%)Miscarriage3/68 (4.4%)
Not reported Not reported Not reported
McCombTaylor(2001)
Retrospectivecohort
23 patientswith unilateralhydrosalpinxand a patentcontralateralfallopian tube1988–1997Canada
Mean age 31.9yearsRange 25–39years
Laparoscopy 23 Unilateralsalpingostomyunderwentlaparoscopicsalpingostomy18 salpingostomiessutured, 5 notsutured
Unilateral Not reported Laparoscopy IUP rate 10/23(43.5%)EP rate 1/23(4%)
6 years At 72 months 10/23 (43.5%)
13.4 months
Milingoset al. (2000)
Retrospectivecohort
61 patientswithhydrosalpinx1990–1997Greece
Mean age31 + 3.9yearsRange 23–38years
HSG andlaparoscopy
61 patientsunderwentlaparoscopicbilateralsalpingostomy
Bilateral Classified using theAFS scoring systemof distal tubalocclusion
laparoscopy IUP rate14/61 (23.0%)EP rate2/61 (3.3%)
2 years Unable to extract Not reported
6C
huetal.
by guest on June 17, 2015 http://humrep.oxfordjournals.org/ Downloaded from
Singhal et al.(1991)
Retrospectivecohort
97 patientswithhydrosalpinx1983–1989.UK
Mean age 30.4yearsRange 20–42years
HSG andlaparoscopy
97 patientsunderwentsalpingostomy.
Mixture ofunilateral andbilateral
Classified by size ofhydrosalpinx
Laparotomyandmicrosurgery
LBR 28/97(28.9%)IUP 33/97(34.0%)EP 6/97 (6.2%)Miscarriage5/97 (5.2%)
Mean durationof follow-up2.8 years(range 10months to6 years)
At 12 months 28%At 36 months 40%
Not reported
Smalldridgeand Tait(1993)
Retrospectivecohort
30 patientswithhydrosalpinx1986–1990New Zealand
Not reported HSG andlaparoscopy
30 patientsundergoingsalpingostomy
Not reported Not reported Laparotomyandmicrosurgery
IUP 9/30(30.0%)EP 3/30(10.0%)Miscarriage0/30 (0.0%)
9–36 months Unable to extract Not reported
Taylor et al.(2001)
Retrospectivecohort
139 patientswithhydrosalpinx1984–1998Canada
Mean age30.9 + 4.1yearsRange 21.4–41.1 years
HSG andlaparoscopy
139 patientsunderwentlaparoscopicsalpingostomy
Unilateral in 86/139Bilateral in 53/139
AFS classificationsystem of distal tubalocclusion
Laparoscopicsalpingostomy
LBR 25/139(18.0%)IUP 34/139(24.5%)EP 23/139(16.5%)Miscarriage9/139 (6.5%)
36 months Of the patientswho conceived:– 55.2% within12 months– 84.5% within36 months
17.7 months(range 0.5–86.4months)
Teoh et al.(1995)
Retrospectivecohort
96 women withbilateralhydrosalpinges1982–1991Ireland
Not reported Laparoscopy 96 womenunderwent bilateralsalpingostomy
Bilateral Not reported Laparotomyandmicrosurgery
LBR 19/96(19.7%)EP 3/96 (3.1%)Miscarriage1/96 (1.0%)
10 years Unable to extract Not reported
Tulandi et al.(1984)
Retrospectivecohort
91 women withbilateralhydrosalpinxCanada
Range 20–37years
HSG 23 womenunderwentsalpingostomy withCO2 laser22 womenunderwentsalpingostomy withmicrodiathermyneedle46 womenunderwentsalpingostomy bycold dissection
Bilateral Classified bymucosalappearance,thickness of tubalwall and peritubaladhesions
Laparotomyandmicrosurgery
IUP 24/91(26.4%)EP 6/91 (6.6%)
At 5 yearsIUP 24/91(26.4%)EP 6/91 (6.6%)
At 5 yearsIUP 24/91(26.4%)EP 6/91 (6.6%)
23.5 + 4.3months(range 6–60months)
Winston andMargara(1991)
Retrospectivecohort
388 patientswith bilateralhydrosalpinx1971–1988UK
Mean age31.5 yearsRange 19 to44 years
HSG andlaparoscopy
323 womenunderwent primarysalpingostomy
Bilateral ModifiedBoer-Meiselclassification.Classified bythickness of tubalwall, appearances ofendosalpinxmucosa, tubaladhesions andovarian adhesions
Laparotomyandmicrosurgery
LBR 74/323(22.9%)IUP 106/323(32.8%)EP 32/323(9.9%)Miscarriage32/323 (9.9%)
Variablefollow-upduration.Longest10 years.12% ofparticipantslost to followup andreported as notpregnant
At 1 yearIUP 55/323(17.0%)At 4 yearsIUP 106/323(32.8%)Cumulative ratesdisplayedgraphically
Not reported
IUP, intrauterine pregnancy; EP, ectopic pregnancy; LBR, live birth rate; HSG, hysterosalpingography; USS, ultrasound scan; AFS, American fertility Society.
Salpingostomy
forhydrosalpinx
7
by guest on June 17, 2015 http://humrep.oxfordjournals.org/ Downloaded from

..........................................................................................................................................................................................................................................................
Table II Appraisal of methodological quality (Newcastle-Ottawa Scale) of included studies.
Study Case-cohortrepresentative
Ascertainmentof exposure
Outcomenegative at start
Comparability bydesign or analysis
Outcomeassessment
Durationof follow-up
Adequacyof follow-up
Score
Audebert (1980) * * * * * * * 7
Audebert et al. (2014) * * * * * * * 7
Bayrak et al. (2006) * * * * * * * 7
Beyth and Bercovici (1982) * * * * * x * 6
Boer-Meisel et al. (1986) * * * * * x * 6
Bontis and Dinas (2000) * * * * * x * 6
Chanelles et al. (2011) * * * x * * * 6
Chong (1991) * * * * * x * 6
Cohen et al. (1972) * * * x * * * 6
Dubuisson et al. (1995) * * * ** * * * 8
Dubuisson et al. (1994) * * * ** * * * 8
Jansen et al. (1980) * * * x * * * 6
Kosasa and Hale (1988) * * * * * x * 6
Mage and Bruhat (1983) * * * * * x * 6
McComb Taylor (2001) * * * * * * * 7
Milingos et al. (2000) * * * * * * * 7
Singhal et al. (1991) * * * * * * * 7
Smalldridge and Tait (1993) * * * * * * * 7
Taylor et al. (2001) * * * * * * * 7
Teoh et al. (1995) * * * * * x * 6
Tulandi et al. (1984) * * * * * * * 7
Winston and Margara (1991) * * * * * * * 7
* indicates that a feature is present. X indicates that a feature is absent. However for comparability by design or analysis this checklist awards the maximum of two stars (**), one (*) or none if the feature is completely absent (x).
8C
huetal.
by guest on June 17, 2015 http://humrep.oxfordjournals.org/ Downloaded from

28% (95% CI: 25–30%) and studies published after 2000 had a pooledclinical pregnancy rate of 25% (95% CI: 22–29%).
Cumulative clinical pregnancy ratesCumulative clinical pregnancy rates over the follow-up period are dis-played graphically in Fig. 4. The cumulative clinical pregnancy rateswere 8.7% (95% CI: 6.6–11.5%) at 6 months, 13.3% (95% CI: 10.6–16.7%) at 9 months, 20.0% (95% CI: 17.5–22.8%) at 12 months,21.2% (95% CI: 18.6–24.1%) at 18 months and 25.5% (95% CI: 22.2–29.4%) at 24 months. There is a plateau of cumulative clinical pregnancyrate after 24 months.
Clinical pregnancy rates in women with bilateral hydrosalpingesWe analysed the studies that performed salpingostomy in women withbilateral hydrosalpinges, as the baseline pregnancy rates (without anysurgical treatment) would have been expected to be extremely low inthis subpopulation. The pooled clinical pregnancy rate from the fivestudies of women with bilateral hydrosalpinges was 29.0% (95% CI:25–34%, Fig. 5). There was statistical heterogeneity between thesefive studies as indicated by an I2 value of 17.8%, P ¼ 0.301.
Live birthTen studies reported the outcome of live birth (Fig. 6). These studiesshowed a pooled live birth rate of 25% (95% CI: 22–28%). Thesestudies showed a moderate level of heterogeneity indicated by an I2
value of 28.8%, P ¼ 0.180.
Ectopic pregnancyNineteen studies reported on the outcome of ectopic pregnancy (Fig. 7).These studies showed a pooled ectopic pregnancy rate of 10% (95% CI:9–11%). These 19 studies showed a moderate level of heterogeneityindicated by an I2 value of 41.8%, P ¼ 0.029.
MiscarriagePooling of results from the seven studies that reported on miscarriage asan outcome (Fig. 8) showed a miscarriage rate of 7% (95% CI: 6–9%).There was moderate heterogeneity between these studies with an I2
value of 42.1%, P ¼ 0.110.
DiscussionThis systematic review including 22 studies suggested that in women whoundergo salpingostomy for hydrosalpinx, the chances of achieving aspontaneous pregnancy is 27%. Moreover, the live birth rate for thesewomen is 25%. However, salpingostomy for hydrosalpinx carries a10% risk of ectopic pregnancy.
Our analysis was strengthened by several factors. We implemented anextensive search strategy and a valid data synthesis method. In addition,no language restrictions were applied. The Newcastle-Ottawa QualityAssessment Scale was used to assess the quality of the includedstudies. The assessment of all studies scored well on this scale, suggestinglow risk of bias.
Figure 2 Natural pregnancy rates after salpingostomy treatment for hydrosalpinx.
Salpingostomy for hydrosalpinx 9
by guest on June 17, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from

There is a high degree of clinical heterogeneity of the included studies.Some degree of clinical heterogeneity is to be expected between thestudies included in our analysis due to the evolution of the surgical tech-niques and varying approaches to the diagnosis and management of
hydrosalpinges. However, we do not feel that this is necessarily a disad-vantage as heterogeneity can increase the generalisability of the findings.
Our studies varied widely with regard to the publication dates, withthe oldest study being published in 1972 and the most recent study pub-lished in 2014. Techniques used to perform salpingostomy have changedsignificantly throughout time due to advancements in technology andequipment available (Bontis and Theodoridis, 2006). Older studieshave reported cases where the majority of surgery was performed bylaparotomy; newer studies have reported upon cases mainly operatedlaparoscopically. Although one might expect that the pregnancy rateswould be higher in the more recent studies (those published after2000, which predominately reported laparoscopic salpingostomy asopposed to laparotomy and microsurgical techniques), our resultssuggest that the reverse is true. One possible reason for this is in case se-lection. Before assisted reproductive treatments were widely available,tubal surgeons may have selected patients with milder tubal disease,with whom they would expect more favourable outcomes. Further-more, before 2000 tubal surgery was more popular as a treatment strat-egy for infertile women with hydrosalpinx. This may have meant thattubal surgeons had greater expertise and would have been expectedto achieve higher success rates. Another contributing factor is that lap-aroscopic surgery can take longer to gain competence in and thereforeit may take several decades to see the change in practice reflected inthe pregnancy rates. In theory, laparoscopic surgery should be superiordue to a decreased risk of adhesion formation.
Figure 4 Cumulative natural pregnancy rates after salpingostomytreatment for hydrosalpinx.
Figure 3 Natural pregnancy rates after salpingostomy treatment for hydrosalpinx by date of publication.
10 Chu et al.
by guest on June 17, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from

Apart from differences in the expertise of the surgeon, there were dif-fering surgical techniques reported in performing salpingostomy, withsome using cold dissection and others using electrosurgery. Some sur-geons performed their salpingostomies with an everted edge while
others left the edges uneverted. Differing pregnancy outcome may beexpected from differing surgical techniques.
The age of patient populations undergoing salpingostomy did not varysignificantly between the majority of studies. In 12 studies where the
Figure 6 Live birth rates after salpingostomy treatment for hydrosalpinx.
Figure 5 Natural pregnancy rates after bilateral salpingostomy treatment for bilateral hydrosalpinges.
Salpingostomy for hydrosalpinx 11
by guest on June 17, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from
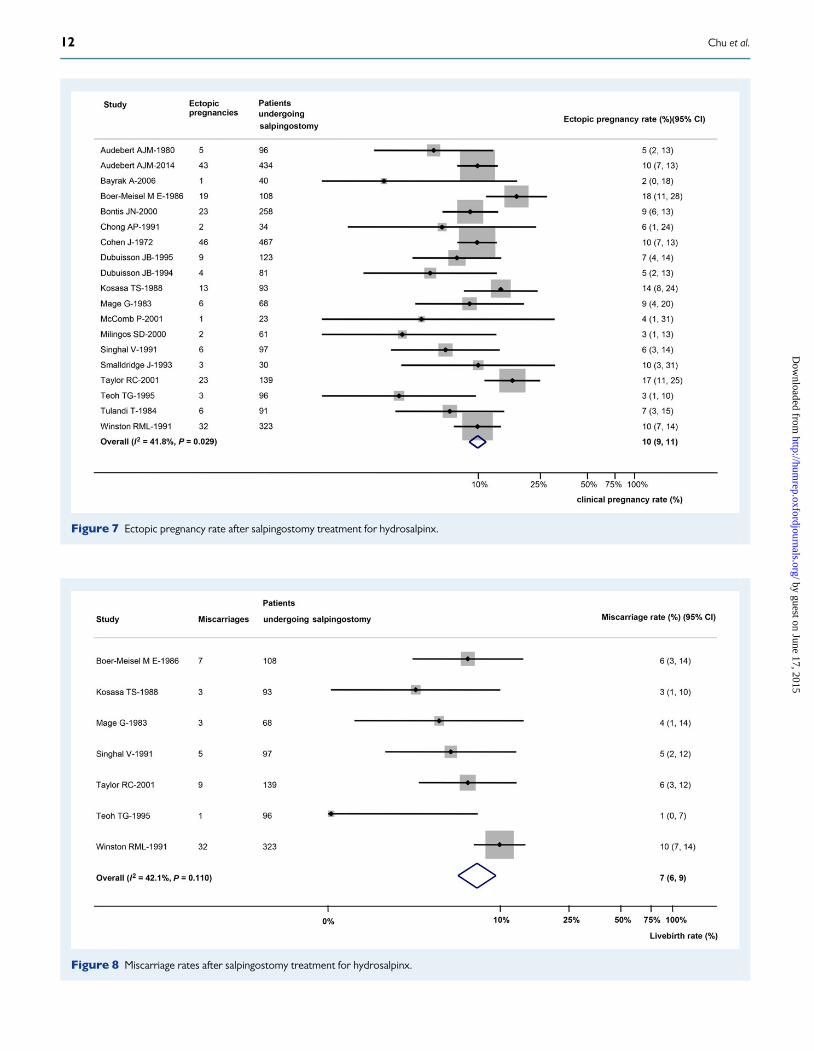
Figure 7 Ectopic pregnancy rate after salpingostomy treatment for hydrosalpinx.
Figure 8 Miscarriage rates after salpingostomy treatment for hydrosalpinx.
12 Chu et al.
by guest on June 17, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from

mean age was reported, the mean age ranged from 27.5 to 32.6 years.The pooled clinical pregnancy rate of these 12 studies was 31%. Onestudy published by Bayrak et al. (2006) had a higher mean age (35.5years) and had the lowest clinical pregnancy rate (5%). This maysuggest that salpingostomy and waiting for natural pregnancy are not asuitable management strategy in older women with hydrosalpinx.However, this was a small study of only 40 patients and thereforestrong conclusions cannot be drawn.
Some women in the study population had unilateral disease whilstothers had bilateral disease. It may be expected that women with unilat-eral disease have a more favourable outcome. Despite this, clinical preg-nancy rates for women with bilateral hydrosalpinges treated withsalpingostomy were still favourable (29% in 605 patients). Thesestudies reporting bilateral salpingostomy showed minimal statistical het-erogeneity with a low I2 value, however this must be interpreted withcareas therewere only fivestudies,which reduces the powerof statisticalheterogeneity tests. The size of hydrosalpinx also differed within study aswell as between studies, with milder hydrosalpinx treatment potentiallyleading to better fertility outcomes.
The duration of follow-up of women in the included studies variedwidely. Those studies with a shorter duration of follow-up may nothave reported on women who naturally conceived beyond this timeand may have therefore under-reported their clinical natural conceptionrates.
The interval between salpingostomy and pregnancy is a clinically im-portant factor to consider when counselling women with hydrosalpinx.Women choosing to have tubal conserving surgery in the form of salipin-gostomy would want to know the duration of time that they shouldattempt natural conception before considering further treatment. Ourdata suggest that there is a plateau of cumulative clinical pregnancy rateat �24 months.
A Cochrane review published by Johnson et al. (2010) concluded thatsurgical treatment (salpingectomy or tubal occlusion) should be consid-ered for all infertile women with hydrosalpinges prior to IVF treatment.The review did not identify any randomized trials to investigate the effect-iveness of salpingostomy versus salpingectomy or tubal occlusion priorto IVF treatment. To date there have still been no studies to investigatethis. The Cochrane review recommended that further research wasrequired to assess the value of tubal restorative surgery as an alternative(or as a preliminary treatment) to IVF. Our systematic review addsfurther weight to this recommendation from the Cochrane review, asour results demonstrate that reasonable clinical pregnancy rates canbe achieved with salpingostomy in carefully selected patients.
Salpingostomy may be an important alternative option in selectedpopulations. Women may wish to have the option to have salpingostomyto continue to attempt natural conception before having more definitivesterilizing surgery in the form of salpingectomy, which would lead to a re-liance on assisted reproductive treatments with no further opportunitiesto try to conceive naturally. In older women or in women with moresevere hydrosalpinges it may be more advisable to proceed directly tosalpingectomy and IVF treatment as time and the chances of natural con-ception are more limited.
SummaryIn the assisted reproduction setting, since the increasing availability ofIVF treatment there has been a general trend for the removal or
disconnection of fallopian tubes in women who have hydrosalpinx(Gomel and Taylor, 1992). It is likely that the ability of reproductive spe-cialists to restore normal tubal anatomy has been reduced due to an overreliance on tubal removal or disconnection followed by IVF treatment.Importantly, women with hydrosalpinx may not be given the full rangeof treatment choices in the clinical setting and are then left with noother option than to pursue and fund IVF treatment.
The findings of this systematic review have re-introduced the possibilityofconsidering tubal restorative surgery foracarefully selectedgroupof womenwith hydrosalpinx. Further research is required to identify the women whowould benefit from tube conserving surgeryas opposed to the current man-agement of tube removal. It may also be beneficial to investigate the besttechnique to perform salpingostomy in these selected patients.
AcknowledgementsWe thank Mr Derrick Yates for his assistance in developing the searchstrategy. We also thank Professor JL Pouly for providing additionaldata from one of the included studies.
Authors’ RolesJ.C., H.M.H. and A.C. were responsible for defining the research ques-tion. J.C. designed the strategy for the literature search. J.C., H.M.H.,F.M.A. and R.D. participated in study selection. J.C. and H.M.H. per-formed the quality assessment of included studies. Data extractionwas carried out by J.C. and H.M.H. Data analysis was performed byI.D.G. J.C., H.M.H. and A.C. were the major contributors in manuscriptwriting.
FundingNo external funding was either sought or obtained for this study.
Conflict of interestNone declared.
ReferencesAkman MA, Garcia JE, Damewood MD, Watts LD, Katz E. Hydrosalpinx
affect the implantation of previously cryopreserved embryos. HumReprod 1996;11:1013–1014.
Andersen AN, Yue Z, Meng FJ, Petersen K. Low implantation rate afterin-vitro fertilisation in patients with hydrosalpinges diagnosed byultrasonography. Hum Reprod 1994;9:1935–1938.
Audebert AJM. Tubal surgery for infertility: report on 172 distalsalpingoplasties [French]. Gynecologie 1980;31:485–489.
Audebert AJM, Pouly LP, Bonifacie B, Yazbeck C. Laparoscopic surgery fordistal tubal occlusions: lessons learned from a historical series of 434cases. Fertil Steril 2014;102:1203–1208.
Bahamondes L, Bueno JGR, Hardy E, Vera S, Pimental E, Ramos M.Identification of main risk factors for tubal infertility. Fertil Steril 1984;61:478–482.
Bayrak A, Harp D, Saadat P, Eliran M, Paulson RJ. Recurrence ofhydrosalpinges after cuff neosalpingostomy in a poor prognosispopulation. J Assist Reprod Genet 2006;23:285–288.
Beyth Y, Bercovici B. Evaluation of microsurgical approach to reconstructivesurgery in 80 infertile patients. J Obstet Gynaecol 1982;2:237–243.
Salpingostomy for hydrosalpinx 13
by guest on June 17, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from

Blazer AS, Hogan JW, Seifer DB, Frishman GN, Wheeler CA, Haning RV.The impact of hydrosalpinx on successful pregnancy in tubal factorinfertility treated by in vitro fertilisation. Fertil Steril 1997;67:517–520.
Boer-Meisel ME, te Velde ER, Habbema JD, Kardaun JW. Predicting thepregnancy outcome in patients treated for hydrosalpinx: a prospectivestudy. Fertil Steril 1986;45:23–29.
Bontis JN, Dinas KD. Management of hydrosalpinx: reconstructive surgery orIVF? Ann N Y Acad Sci 2000;900:260–271.
Bontis JN, Theodoridis TD. Laparoscopic management of hydrosalpinx. AnnN Y Acad Sci 2006;1092:199–210.
Camus E, Poncelet C, Goffinet F, Wainer B, Merlet F, Nisand I, Philippe HJ.Pregnancy rates after in-vitro fertilization in cases of tubal infertility withand without hydrosalpinx: a meta-analysis of published comparativestudies. Hum Reprod 1999;14:1243–1249.
Chanelles O, Ducarme G, Sifer C, Hugues J-N, Touboul C, Poncelet C.Hydrosalpinx and infertility: what about conservative surgicalmanagement? Eur J Obstet Gynecol Reprod Biol 2011;159:122–126.
Chong AP. Pregnancy outcome in neosalpingostomy by the cuff vs Bruhattechnique using the carbon dioxide laser. J Gynecol Surg 1991;7:207–210.
Cohen J, Feinerman D, Palmer R, Rumeau RC. Results of a retrospectivestudy on the outcome of tubal repair surgery in sterility. Acta Eur Fertil1972;3:321–327.
Dubuisson JB, Chapron C, Morice P, Aubriot FX, Foulot H, Bouquet de JJ.Laparoscopic salpingostomy: Fertility the tubal mucosal appearance.Hum Reprod 1994;9:334–339.
Dubuisson JB, Morice P, Chapron C, Aubriot FX, Foulot H, Bouquet de JJ.Laparoscopic salpingostomy: Fertility results [French]. Contracept FertilSex 1995;23:109–114.
Flemming H, Hull MGR. Impaired implantation after in vitro fertilisationtreatment associated with hydrosalpinx. Br J Obstet Gynecol 1996;103:268.
Freeman MR, Whitworth M, Hill GA. Permanent impairment of embryodevelopment by hydrosalpinges. 1998.
Gomel V, Taylor PJ. In vitro fertilization versus reconstructive tubal surgery. JAssist Reprod Genet 1992;9:306–309.
Jansen RPS. Surgery-pregnancy time intervals after salpingolysis, unilateralsalpingostomy, and bilateral salpingostomy. Fertil Steril 1980;34:222–225.
Johnson NP, van Voorst S, Sowter MC, Strandell A, Mol BW. CochraneDatabase CD002125. 2010.
Kassabji M, Sims JA, Butler L, Muasher SJ. Reduced pregnancy outcome inpatients with unilateral or bilateral hydrosalpinx after in vitro fertilisation.Eur J Obstet Gynecol Reprod Biol 1994;54:129–132.
Katz E, Akman MA, Damewood MD, Garcia JE. Deleterious effect of thepresence of hydrosalpinx on implantation and pregnancy rates with invitro fertilisation. Fertil Steril 1996;66:122–125.
Kosasa TS, Hale RW. Treatment of hydrosalpinx using a single incisioneversion procedure. Int J Fertil 1988;33:319–323.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP,Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement forreporting systematic reviews and meta-analyses of studies that evaluatehealthcare interventions: explanationand elaboration. BMJ 2009;339:b2700.
MageG, Bruhat MA. Pregnancy following salpingostomy: comparisonbetweenCO2 laser and electrosurgery procedures. Fertil Steril 1983;40:472–475.
McComb PF, Taylor RC. Pregnancy outcome after unilateral salpingostomywith a contralateral patent oviduct. Fertil Steril 2001;76:1278–1279.
Milingos SD, Kallipolitis GK, Loutradis DC, Liapi AG, Hassan EA,Mavrommatis CG, Miaris SG, Michalas SP. Laparoscopic treatment ofhydrosalpinx: factors affecting pregnancy rate. J Am Assoc GynecolLaparosc 2000;7:355–361.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferredreporting items for systematic reviews and meta-analyses: the PRISMAstatement. BMJ 2009;339:b2535.
Murray DL, Sagostin AW, Widra EA, Levy MJ. The adverse effect ofhydrosalpinges on in vitro fertilisation pregnancy rates and the benefit ofsurgical correction. Fertil Steril 1998;69:41–45.
Savaris RF, Giudice LC. The influence of hydrosalpinx on markers ofendometrial receptivity. Semin Reprod Med 2007;25:476–482.
Sharif K, Coomarasamy A. Assisted Reproduction Techniques: Challenges andManagement Options. UK: Wiley-Blackwell Press, 2012.
Singhal V, Li TC, Cooke ID. An analysis of factors influencing the outcome of232 consecutive tubal microsurgery cases. Br J Obstet Gynaecol 1991;98:628–636.
Smalldridge J, Tait J. The results of tubal surgery in the treatment of infertility inWellington 1986–90. N Z Med J 1993;106:124–126.
Strandell A, Waldenstrøm U, Nilsson L, Hamberger L. Hydrosalpinx reducesin-vitro fertilization/embryo transfer pregnancy rates. Hum Reprod, 1994;9:861–863.
Strandell A, Lindhard A, Wldenstrom U, Thorburn J, Janson PO,Hamberger L. Hydrosalpinx and IVF outcome: a prospective, randomizedmulticentre trial in Scandinavia on salpingectomy prior to IVF. Hum Reprod1999;14:2762–2769.
Taylor RC, Berkowitz J, McComb PF. Role of laparoscopic salpingostomy inthe treatment of hydrosalpinx. Fertil Steril 2001;75:594–600.
Teoh TG, Kondaveeti U, Darling MR. The management of female infertility bytubal microsurgical reconstruction: a ten year review. Ir J Med Sci 1995;164:212–214.
Tulandi T, Farag R, McInnes RA, Gelfand MM, Wright CV, Vilos GA.Reconstructive surgery of hydrosalpinx with and without the carbondioxide laser. Fertil Steril 1984;42:839–842.
Vandromme J, Chasse E, Lejeune B, Van Rysselberge M, Delvigne A, Leroy F.Hydrosalpinges in in-vitro fertilization: an unfavourable prognostic feature.Hum Reprod 1995;10:576–579.
Van Voorhis BJ, Sparks AET, Syrop CH, Stovall DW. Ultrasound-guidedaspiration of hydrosalpinges is associated with improved pregnancy andimplantation rates after in-vitro fertilization cycles. Hum Reprod 1998;13:736–739.
Wainer R, Camus E, Camier B, Martin C, Vasseur C, Merlet F. Doeshydrosalpinx reduce the pregnancy rate after in vitro fertilisation? FertilSteril 1997;68:1022–1026.
Winston RM. Tubal surgery or in vitro fertilization (IVF)? J Assist Reprod Genet1992;9:309–311.
Winston RM, Margara RA. Microsurgical salpingostomy is not an obsoleteprocedure. Br J Obstet Gynaecol 1991;98:637–642.
Zeyneloglu HB, Arici A, Olive DL. Adverse effects of hydrosalpinx onpregnancy rates after in-vitro fertilization-embryo transfer. Fertil Steril1998;70:492–499.
14 Chu et al.
by guest on June 17, 2015http://hum
rep.oxfordjournals.org/D
ownloaded from