“sonographic fetal findings with borderline significance and down syndrome” micaela della torre,...
TRANSCRIPT
“Sonographic fetal findings with borderline significance and
Down Syndrome”
Micaela Della Torre, MD MSMaternal Fetal Medicine
Tuesday, April 18, 2023
Objectives Learn how to recognize the
most common sonographic signs associated with trisomy 21 in the second trimester to improve recognition of affected fetuses
Learn sensitivity, specificity and likelihood ratios of the different signs
Learn how to better use genetic ultrasound in the contest of maternal screening test
Tuesday, April 18, 2023

Tuesday, April 18, 2023
I declare that I do not have a financial interest or other relationship with any manufacturers of any commercial products that may be discussed during this presentation

Outlines
Screening for Down syndrome and risk assessment
NT NB, tricuspide regurgitation, abnormal ductus venosus cystic hygroma
Pyelectasis Hyper-echoic bowel Ventriculomegaly Single umbilical artery Long bones Others
Tuesday, April 18, 2023

“Observations on an ethnic classification of idiots” by Langdon Down in 1866
…The hair is not black, as in the real Mongol, but of a brownish color, straight and scanty. The face is flat and broad, and destitute of prominence. The cheeks are roundish, and extended laterally. The eyes are obliquely placed, and the internal canthi more than normally distant from one another. The palpebral fissure is very narrow. The forehead is wrinkled transversely from the constant assistance which the levatores palpebrarum derive from the occipito-frontalis muscle in opening of the eyes. The lips are large and thick with transverse fissures. The tongue is long, thick, and is much roughened. The nose is small. The skin has a slight dirty yellowish tinge, and is deficient in elasticity, giving the appearance of being too large for the body.’ …
Tuesday, April 18, 2023

Tuesday, April 18, 2023

Last three decades major improvement in pregnancy screening for open neural tube defect (ONTD) and aneuploidy
Now screening primarily for adjusted risk of chromosomal abnormalityT18 and T21
Better detection rate of ONTD by ultrasound alone
Tuesday, April 18, 2023
Chromosomal defects: frequency and occurrence
Natural frequency for chromosomal abnormalities at birth is estimated to be 6:1000Most common is trisomy 21 (overall 1:700)
The risk of Down syndrome varies drastically w maternal age
USA women 35-49 of age
4.7% of live births in 1974 12.6% of live births in 1997
Tuesday, April 18, 2023

Down syndrome
Three separate mechanisms
Non disjunction (95%) 95% of non disjunction is maternal in origin
Translocation Mosaicism
Tuesday, April 18, 2023

Maternal and paternal age riskRelationship between age
and increased risk was first noticed by Penrose in 1933
Prevalence also increases w paternal ageFathers more than 39 of age
have 3 times higher risk than in father less than 35 of age
True even if adjusted for maternal age
Lansac et al 1997Jalbert 1995
Tuesday, April 18, 2023

1970s maternal age alonePredictive value of maternal screening alone is
poorlower than 25%1 affected fetus over 125 invasive proceduresEven worst now that the proportion of pregnant
women over 35 is increasingScreening protocols allow detection of
trisomy21 among younger women and better assessment of the risk in older women
Tuesday, April 18, 2023
1980s – more tools were introduced to better assess the risk of Down syndromematernal ageconcentration of various fetoplacental products in
the maternal circulation (maternal biochemistry)a-fetoprotein, estriol, human chorionic gonadotropin
(hCG) (total and free-b)
method of screening is more effective than maternal age alone
Tuesday, April 18, 2023

1990sMaternal ageFetal nuchal translucency thickness at 11–14 weeks
of gestationPPV 75% w FP rate 5%
Even more recently Maternal age Fetal nuchal translucencyMaternal serum biochemistry
free b-hCGPAPP-Aabout 90%
PPV 90% w FP rate 5% Now different options are available
Tuesday, April 18, 2023

Down syndrome detection
First trimesterlevels of PAPP-A and free -hCG NT Detection rate of 85% with 5% false positive
rate (FPR)Second trimester quad screen
levels of AFP, hCG, estriol, and inhibin ADetection rate of 81% with 5% FPR
Step-wise sequentialDetection rate of 95% with 5% FPR
Tuesday, April 18, 2023
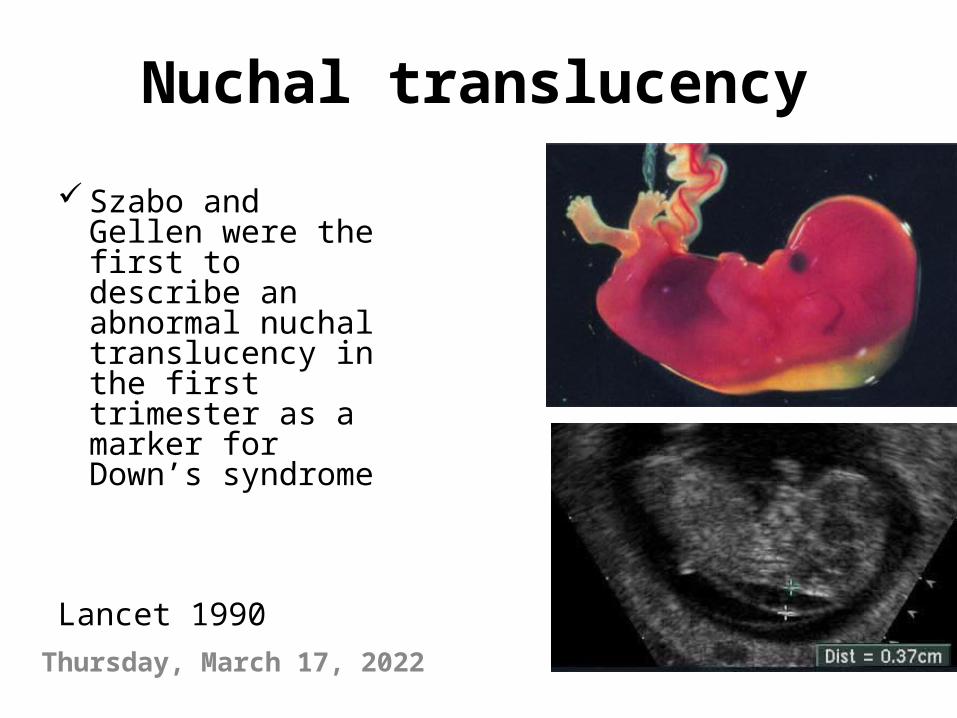
Nuchal translucency
Szabo and Gellen were the first to describe an abnormal nuchal translucency in the first trimester as a marker for Down’s syndrome
Lancet 1990
Tuesday, April 18, 2023

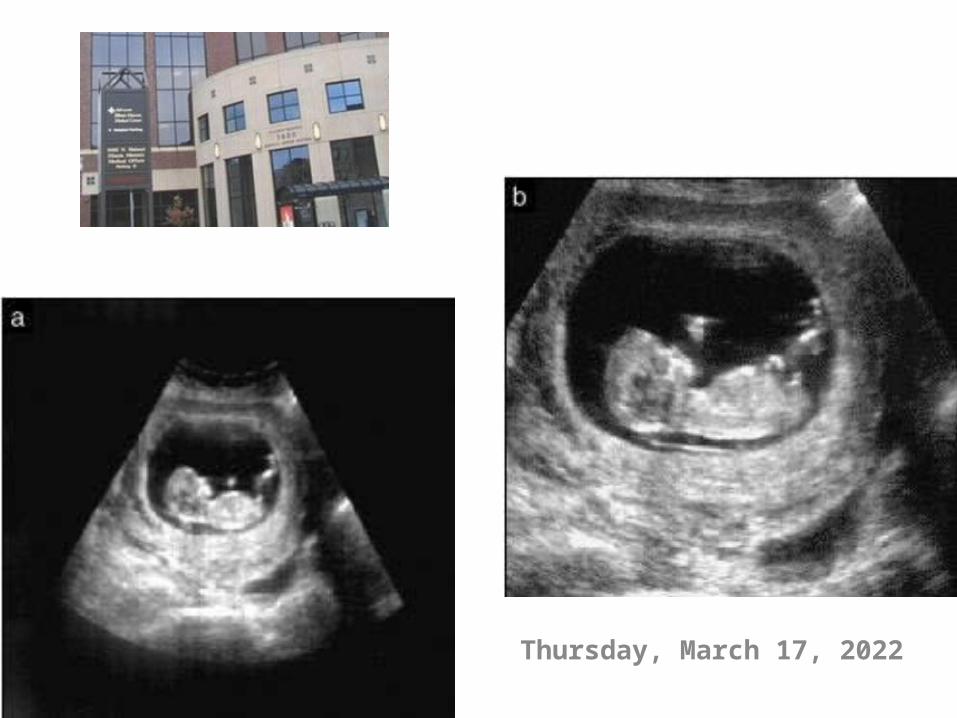
Technique
CRL 39 to 84mm Sagittal view - magnification
should be such that the fetus occupies at least three-quarters of the image
Careful distinguish between fetal skin and amnion
NT should be measured with the fetus in the neutral position –
Hyperextension increase up to 0.6mm
Flexion decrease up to 0.4mm If umbilical cord is around the
neck the NT measurements can be falsely increased
Tuesday, April 18, 2023
Tuesday, April 18, 2023

Tuesday, April 18, 2023
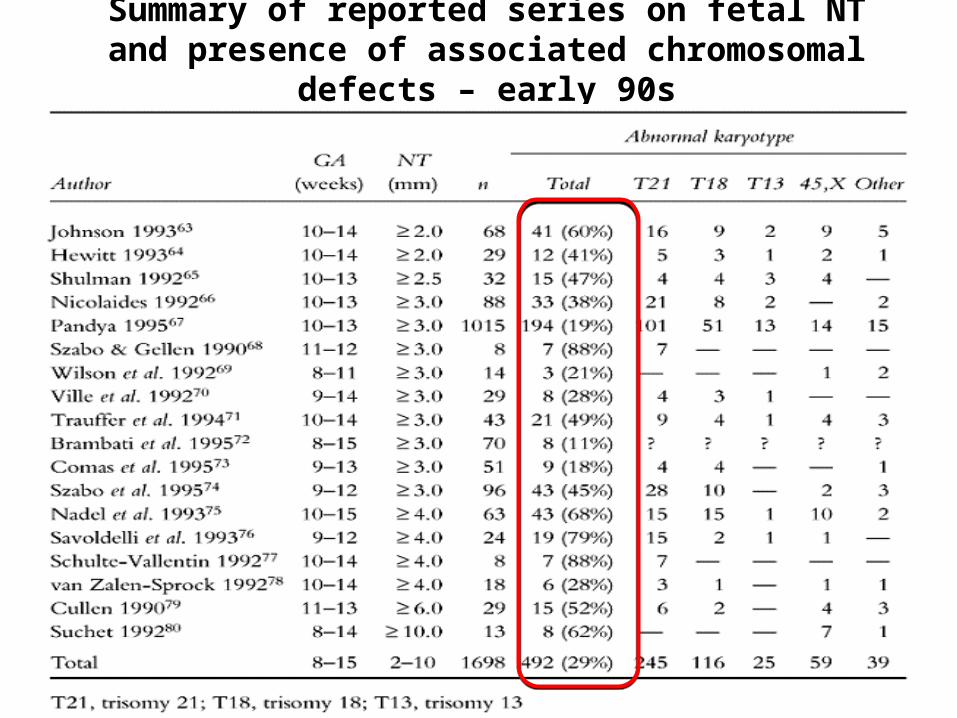
Summary of reported series on fetal NT and presence of associated chromosomal defects – early 90s

Late 1990,s - detection rate
Tuesday, April 18, 2023

More recent detection rates
Year N NT ct-off FPR DR for T21
Schuchter 2001 9342 2.5 2.1 58
Wayda 2001 6841 2.5 4.1 100
Panburana 2001 2067 2.5 2.9 100
Zoppi 2001 10111 95th percentile 5.1 81.3
Gasiorek-wiens 2001 21959 95th percentile 8.0 82.9
Comas 2002 7345 95th percentile 4.9 100
Chasen 2003 2246 95th percentile 3.4 75
Brizot 2001 2492 95th percentile 6.4 70
Audibert 2001 4130 3.0 1.7 58.3
Rozemberg 2002 6234 3.0 2.8 61.9
Total 72769 4.1 81.5

CounselingBoth first trimester and sequential screening
have been established as reliable risk assessment toolsEspecially if NT is less than 95th percentile
Invasive testing should be offered to all cases of increased NT (3 to 3.5 mm)
If karyotype is normal, fetal echocardiogram should be obtainedFISH for 22q11.2 deletion
If karyotype is normal, normal outcome is expected in more than 85% of cases
Tuesday, April 18, 2023

Year N NT Cardiac defectsHyett 1997 1389 2.5-3.4mm
≥3.5mm6/1102 .54%9/287 3.14%
Ghi 2001 1319 2.5-3.4mm≥3.5mm
18/722 2.5%42/597 7%
Lopes 2003 275 2.5-3.4mm≥3.5mm
2/159 1.26%11/51 21.5%
Galindo 2003 353 2.5-3.9mm≥ 4mm
7/131 5.34%25/222 11.26%
McAuliffe 2004 177 2.5-3.4mm≥3.5mm
5/122 4.1%8/55 14.5%
Total 3448 38/2236 1.7%95/1212 7.84%Tuesday, April 18, 2023
Prevalence of major cardiac defects in normal chromosome fetuses w increased NT – Hyett et al 1996

Other markers…
Further improvements in screening performance may be achievable in the futureNasal BoneTricuspid regurgitation by pulsed wave Doppler Abnormal blood flow through the ductus venosus
ADAM 12 – placental glycoprotein
Tuesday, April 18, 2023
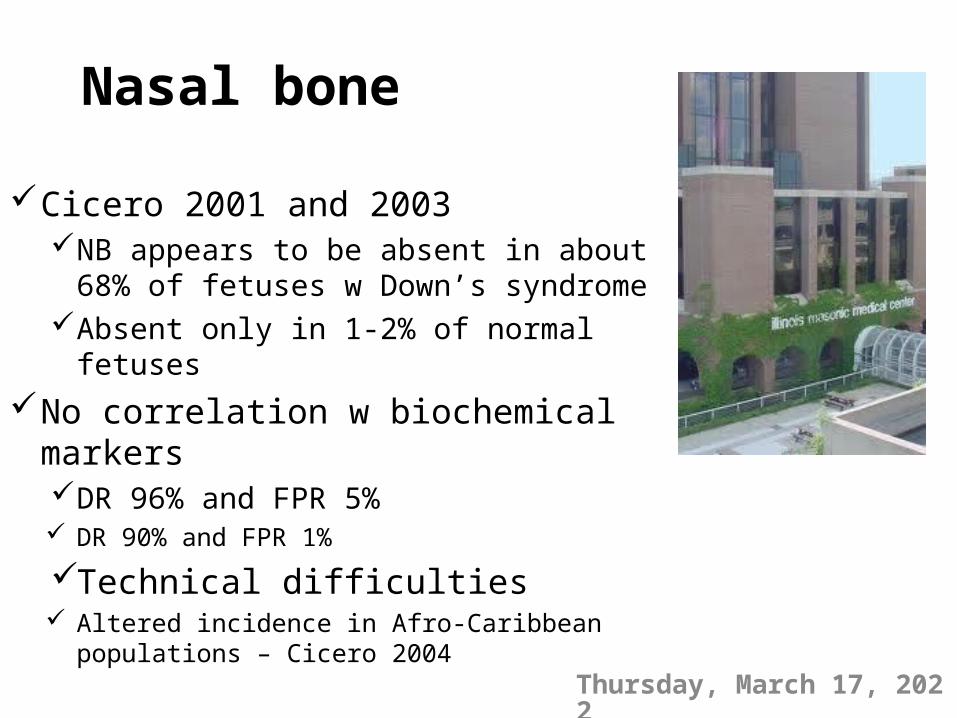
Nasal bone
Cicero 2001 and 2003NB appears to be absent in about 68% of
fetuses w Down’s syndrome Absent only in 1-2% of normal fetuses
No correlation w biochemical markersDR 96% and FPR 5% DR 90% and FPR 1%
Technical difficulties Altered incidence in Afro-Caribbean populations
– Cicero 2004Tuesday, April 18, 2023
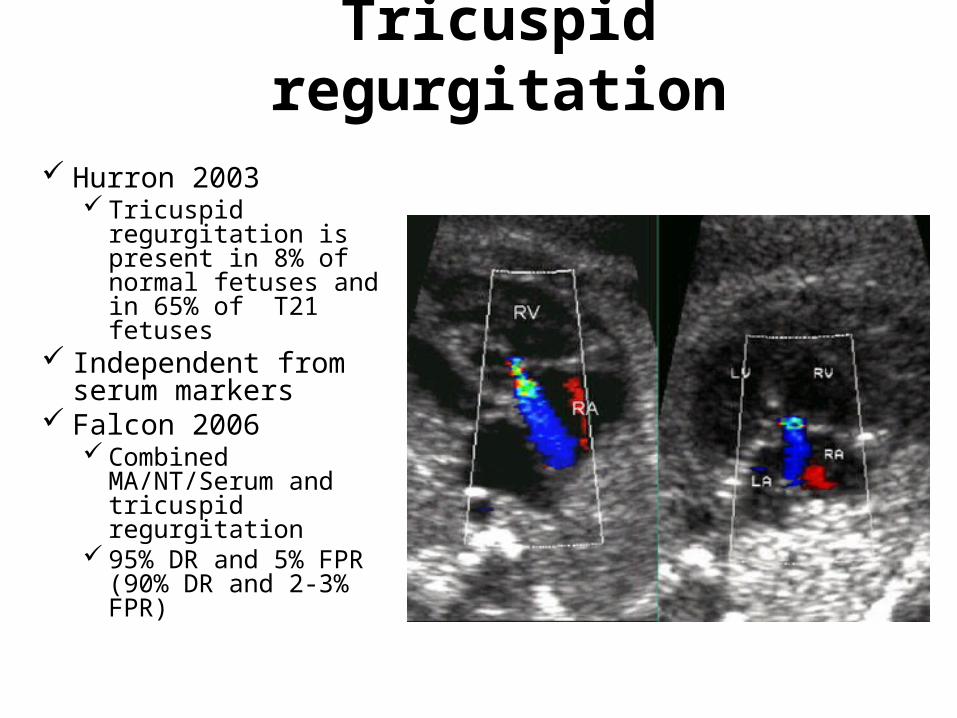
Tricuspid regurgitation
Hurron 2003 Tricuspid regurgitation
is present in 8% of normal fetuses and in 65% of T21 fetuses
Independent from serum markers
Falcon 2006 Combined
MA/NT/Serum and tricuspid regurgitation
95% DR and 5% FPR (90% DR and 2-3% FPR)
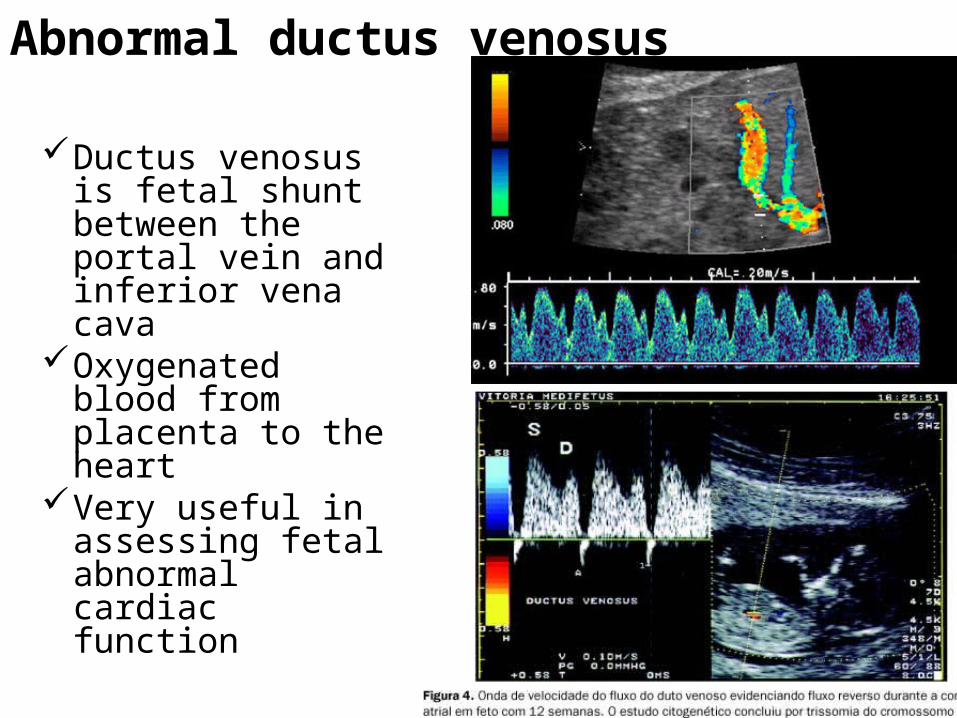
Abnormal ductus venosus
Ductus venosus is fetal shunt between the portal vein and inferior vena cava
Oxygenated blood from placenta to the heart
Very useful in assessing fetal abnormal cardiac function
Abnormal ductus venosus flowMattias et al 1998Perform ductus venosus Doppler in fetuses
with increased NTAbnormal ductus in 57 of 63 (90.5%)
chromosomally abnormal fetusesAbnormal ductus in 13 of 423 (3.1%)
chromosomally normal fetuses7 of 13 with absent or reversed flow had major cardiac
defect demonstrated 14–16 weeks
Tuesday, April 18, 2023

Nuchal
Translucency
Chromosomal
Defects
Fetal Death
Major Fetal
Abnormalities
Alive and
Well
<95th % 0.2% 1.3% 1.6% 97%
95th-99th % 3.7% 1.3% 2.5% 93%
3.5-4.5mm 21.1% 2.7% 10.0% 70%
4.5-5.4mm 33.3% 3.4% 18.5% 50%
5.5-6.4mm 50.5% 10.1% 24.2% 30%
>6.5mm 64.5% 19.0% 46.2% 15%Nicolaides, K.H.(2005). The 11-13+6 weeks scan. pp 72.
What is this?
Intracardiac echogenic focusMicro-calcification within the papillary muscle of
the heart0.5 to 20% - mostly in left ventricle, but it can be
right or bilateralCaucasians 3.5 to 10.5%AA 5.5 to 5.9%Asians 10 to 30%
Isolated in low risk population – no increased riskLikelihood ratio 1.8 – rarely a low risk patient becomes an high
risk patientHigh risk population or associated with other findings –
addition counseling is warranted
Tuesday, April 18, 2023

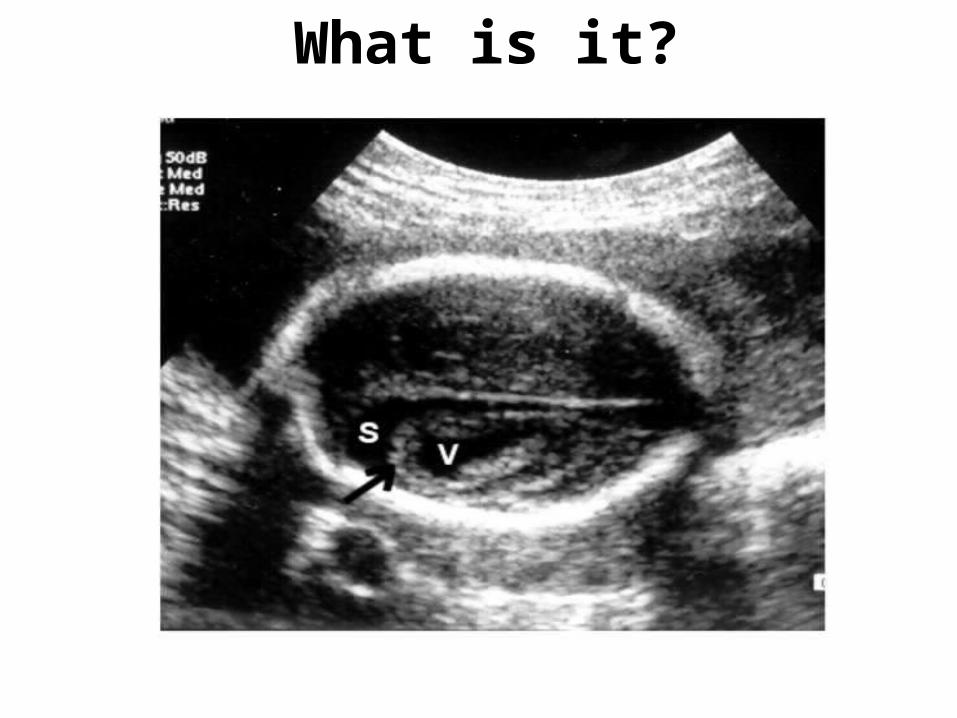
What is it?
Tuesday, April 18, 2023

Tuesday, April 18, 2023
Single Umbilical Artery0.5-2% of all prenatal ultrasound
caucasian 3 times higher than AAvery rare in Japanese descent3 to 4 fold increase in twins
Targeted imaging to rule out concurrent anomalies (15-45% associated anomalies)If other anomalies not seen in utero, 7-10%
chance of findings at birthAssociated anomalies-high risk aneuploidy (20-25% to
45% if CNS anomalies)Isolated SUA in AGA fetus- risk aneuploidy age related
- Parilla et al 1995Some literature suggest slight increase, approximately
1%
2 vessels cord IUGR in as high as 28% of
cases of isolated single umbilical artery
Placental anomalies found in 16 to 78% of cases
Most common small placenta and abnormal cord insertion
Perinatal mortality increased after adjustment for associated anomalies
Tuesday, April 18, 2023

What is it?

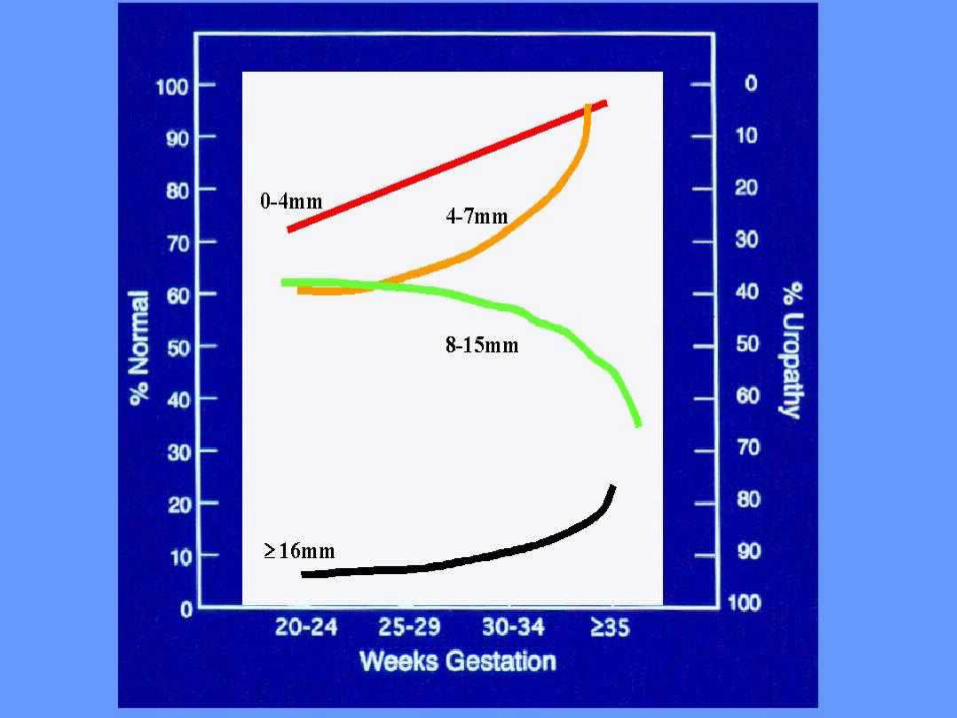
Mild pelviectasisDistention of fetal renal pelvis by urine
Most often bilateral, when unilateral right more common than left
Up 16% associated with other anomalies< 4 mm, < 33 weeks< 7 mm, > 33 weeks> 10 mm is always pathologicCommon finding – 2-3% in normal fetuses
More common in male than female 2:1Trisomy 21 – likelihood 1.6 Risk of Uropathy UPJ obstruction, VUR, primary nonrefluxing megaureter,
UVJ obstruction, ectopic ureter, PUV, magacystic megaureter, physiologic dilatation, multicystic dysplastic kidneys, ARPKD, extrophy, prune belly syndrome

Counseling
Increased risk of Down syndrome If not screening test available, risk is about 1%If screening test is available, risk is increased
slightly compared adjusted maternal riskAmniocentesisRepeat ultrasound after 32 weeks
Tuesday, April 18, 2023

Counseling
30-50% of fetuses with isolated pyelectasis will have normal postnatal course
Vast majority of affected fetuses do not require surgical intervention (99%)
Consider neonatology and pediatric urology evaluation at time of birth(tertiary center??, evaluation can be delayed to
day 2-3 of life)
Tuesday, April 18, 2023

What is it?
Tuesday, April 18, 2023
Echogenic bowelNon specific findingBowel should have echogenicity similar to bone
structuresGain setting down until other soft tissue cannot be
seen – only echogenic bowel and bonesNyberg classification
Grade 1 moderate diffuse echogenicityGrade 2 focal echogenicity (more likely to be associated
with problems)Grade 3 very echogenic , as bone
Tuesday, April 18, 2023

Most cases of isolated finding do have normal outcomes
Simon-Bouy 2003Prospective study of 682 cases447 normal outcome (65.5%)
Tuesday, April 18, 2023
Can be associated with GI anomaliesbowel atresia, anorectal
malformations, volvulus, obstruction (2-10%)
CF (2-4%)Viral infection (3-4%) – CMV,
Toxoplasmosis, Parvo B19Down syndrome
Tuesday, April 18, 2023
Aneuploidy riskBansiak et al 2001
Cumulative 9.5% aneuploidy (63/663)Isolated 3% (13/439) and DS was the most
commonSimon Bouy et al 2003
Cumulative 4.3% (29/682)Shipp et al 2002
Increase 5.5 times the a priori risk for DSNyberg et al 2001
Likelihood ratio for DS 6.7 if isolated hyperechoic bowel

Poor obstetrical outcomesRochon and Eddleman 2004
14-18% of pregnancies complicated by echogenic bowel also experience growth restriction and IUGR
Increased risk of IUFD and neonatal deathSimon-Bouy 2003
2% unexplained IUFDAmniocentesis, CF screening, TORCHSerial ultrasoundANT
Tuesday, April 18, 2023
What is it?
VentriculomegalyWidth of the atria of the lateral ventricles >10mm
Mild 10-12Severe >15
1-2/1000Trisomy 13,18,21; triploidy, umbalanced
translocations (4%)Normal variantCongenital infection – toxoplasmosis, CMV, syphylisAbsence corpus callosumHydrocephalus – aqueductal stenosis, ONTD, Dandy
WalkerTuesday, April 18, 2023
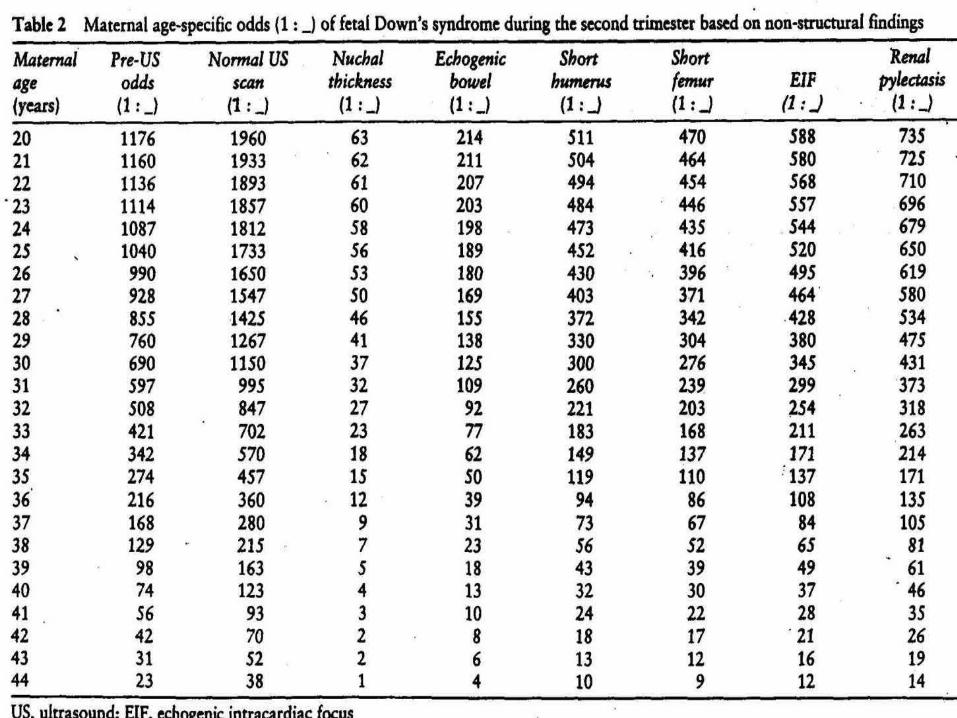
Age-adjusted ultrasound risk assessment for trisomy 21
AAURA is a priori risk (MA) X LR resulting from presence or absence of specific US findings for each patientLilelihood ratio = sensitivity / false-positive rate
as an isolated findingCase-control study
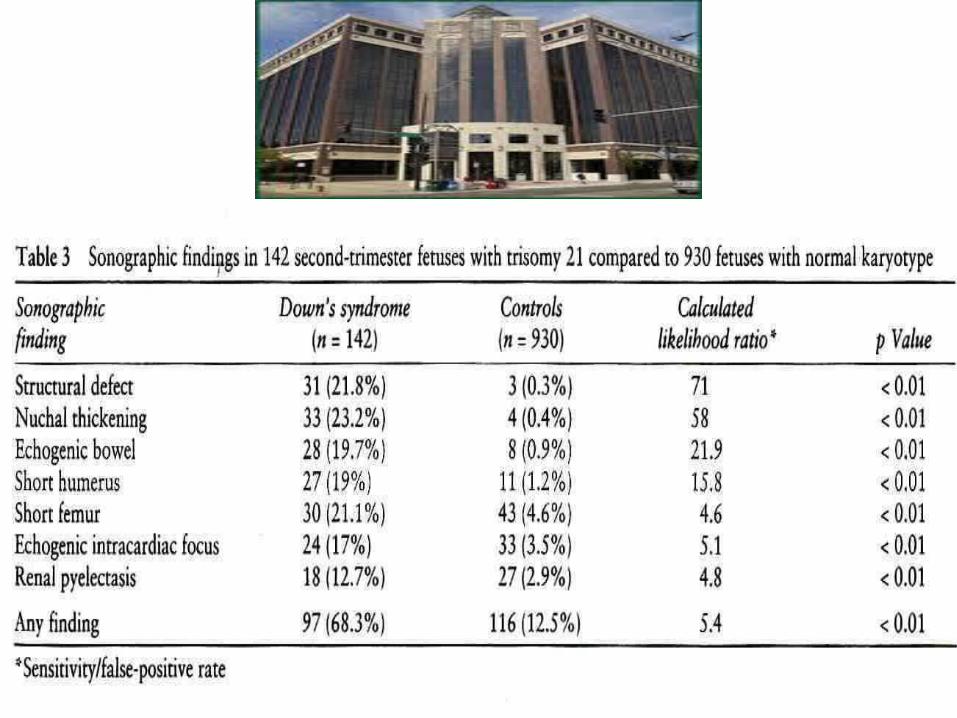
142 fetuses with trisomy 21 and 930 fetuses with normal karyotypeAll patients underwent 2nd trimester US at single
institution through standardized US protocol w/o knowledge karyotype
Nyberg 1998

Age-adjusted ultrasound riskassessment for trisomy 21
Tuesday, April 18, 2023
AAURA detection rate for DS was 74% 137/930 78.6% (81/103) from women 35 61.5% (24/39) from women < 35
Overall false-positive rate of 14.7% 4% (21/519) for women < 35 28.2% (116/411) for women 35 12.5% (42/337) for women 35-39 100% (74/74) for women 40
References1. Textbook of fetal abnormalities 2nd Edition – Peter Twining 20072. Diagnostic Imaging Obstetrics First Edition – Woodward 20053. Diagnostic Imaging of Fetal Anomalies – Nyberg 20034. Diploma in fetal medicine & ISUOG educational series Chapter 1-www.centrus.com5. Spencer “Aneuploidy in first trimester screening” America Journal of Medicine
Genetics Part C: Seminars in medical genetics; Vol 145C, Issue1, 18-32- 20076. Hyett “Does nuchal translucency have a role in fetal cardiac screening?’ Prenat Diagn
2004; 24:11307. Falcon et al “Screening for trisomy 21 by fetal tricuspid regurgitation,
nuchal…”Ultrasound Obstet Gynecol 2006: 27(2); 1518. Mavrides et al “Screening for aneuploidy in the first trimester by assessment of
blood flow in the ductus venosus” BJOG 2002, vol 109, 10159. Borrell et al “Ductus venosus assessment at the time of nuchal translucency
measurement in the detection of fetal aneuploidy” Prenat Diagn 2003; 23(11):92110. Muta et al ‘Application of ductus venosus Doppler Velocimetry for the detection of
fetal aneuploidy in the first trimester of pregnancy’ Fetal Diagn Ther 2002, 17: 308
Tuesday, April 18, 2023
11. Zoppi et al “First trimester dusctus venosus velocimetry in relation to nuchal translucency thickness and fetal karyotype” Fetal Diagn Ther 2002; 17(1):52
12. Favre et al “The role of fetal nuchal translucency and ductus venosus Doppler at 11-14 wks of gestation in the detection of major congenital heart defects” Ultrasound Obstet Gynecol 2003; 21(3): 239
13. Borell et al “First trimester screening for Down sdr with ductus venosus Doppler studies in addition to nuchal translucency and serum markers” Prenat Diagn 2005; 25(10): 901
14. Devine et al “Nuchal translucency and its relationship to congenital heart disease” Semin Perinatol 2000, 24(5): 343
15. Neuman et al “ First trimester screening for congenital heart disease” Minerva Cardioangiol 2006; 54(3): 337
16. Guis F, Y Ville et all “Ultrasound evaluation of the length of the nasal bones throughout gestation” Ultrasound Obstet Gynecol. 5 (1995); 304-307
17. Cicero S, Curcio P et all “Absence of nasal bone in fetuses with trisomy 21 at 11-14 weeks of gestation: an observational study” Lancet; vol 358; November 17, 2001
18. Sonek JD and Nicholaides KH “Prenatal ultrasonographic diagnosis of nasal bone abnormalities in three fetuses with Down Syndrome” Am J Obstet Gynecol 2002; 186: 139-41
19. Otano L et al “ Association between first trimester absence of fetal nasal bone on ultrasound and down syndrome” Prenat Diagn 2002; 22:930
20. Gomez et al “ US measurement of nasal bone in a low risk population at 19-22 gestational weeks” -Ultrasound Obstet Gynecol 2004; 23: 152
21. Viora et al “Fetal nasal bone and trisomy 21 in the second trimester” Prenat Diagn 2005: 25; 511
Tuesday, April 18, 2023

22. Odibo et al “Association between fetal nasal bone hypoplasia and aneuploidy” Obstet Gynecol 2004; 104: 1229
23. Cicero et al “Maternal serum biochemistry at 11-13 wks in relation to the presentcee or absence of the fetal nasal bone on ultrasonography in chromosomally abnormal fetuses: an updated analysis of integrated ultrasound and biochemical screening” Prenat Diagn 2005: 25; 977
24. Ville “What is the role of fetal nasal bone examination in the assessment of risk for trisomy 21 in clinical practice? AJOB 2006; 195:1
25. Cicero et al “Nasal bone in first trimester screening for trisomy 21” AJOB 2006: 195:109
26. Sonek et al “Nasal bone assessment in prenatal screening for trisomy 21” AJOB 2006 195; 1219
27. Weingertner et al “Interest of fetal nasal bone measurement at first trimester Trisomy 21 screening” Fetal Diagn Ther 2006; 21:433
28. Zoppi et al “Absence of fetal nasal bone and aneuploidies at first trimester nuchal translucency screening in unselected pregnancies” Prenat Diagn 2003; 23: 496-500
29. Cicero et al “ Absence of nasal bone in fetuses with trisomy 21 at 11-14 wks of gestation: an observational study” Lancet 200: 358, 2001
30. Snijders et al – ‘ Assessment of risks” Ultrasound markers for fetal chromosomal defects – Parthenon Publishing: Carnforth 1996; 63-120
31. Nicolaides “Screening for chromosomal defects” Ultrasound Obstet Gynecol 2003; 21: 313
32. Cicero et al “ Likelihood ratio for trisomy 21 in fetuses with absent nasal bone at the 11-14 wks scan” Ultrasound Obstet Gynecol 2004; 23: 218
33. Malone et al ‘First trimester nasal bone evaluation for anuploidy in the general polulation” Obstet Gynecol vol 104; No6; December 2004
Tuesday, April 18, 2023

Thank You and questions???
Tuesday, April 18, 2023