sorafenib and mfolfox6 for metastatic colorectal cancer 1
TRANSCRIPT
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
1
Sorafenib in Combination with Oxaliplatin, Leucovorin, and Fluorouracil (modified
FOLFOX6) as First-line Treatment of Metastatic Colorectal Cancer: The RESPECT Trial
Josep Tabernero,1 Rocio Garcia-Carbonero,2 James Cassidy,3 Alberto Sobrero,4 Eric Van
Cutsem,5 Claus-Henning Köhne,6 Sabine Tejpar,5 Oleg Gladkov,7 Irina Davidenko,8 Ramon
Salazar,9 Liubov Vladimirova,10 Sergey Cheporov,11 Olga Burdaeva,12 Fernando Rivera,13 Leslie
Samuel,14 Irina Bulavina,15 Vanessa Potter,16 Yu-Lin Chang,17 Nathalie A. Lokker,17 and Peter J.
O'Dwyer18
Authors’ Affiliations
1Vall d’Hebron University Hospital and Vall d’Hebron Institute of Oncology (VHIO), Universitat
Autònoma de Barcelona, Barcelona, Spain; 2Hospital Universitario Virgen del Rocio – Instituto
de Biomedicina de Sevilla [IBIS (Universidad de Sevilla, CSIC, HUVR)], Sevilla, Spain; 3Beatson
Laboratories, Glasgow UK*; 4Oncologia Medica, Genova, Italy; 5University Hospitals Leuven
and KU Leuven, Belgium; 6University Oldenburg, Oldenburg, Germany; 7Chelyabinsk Regional
Clinical Oncology Center, Chelyabinsk, Russia;8Clinical Oncology Center #1, Krasnodar,
Russia; 9Instituto Catalán de Oncología, Barcelona, Spain; 10Rostov Research Institute of
Oncology, Russia; 11Regional Clinical Oncology Hospital, Yaroslavl, Yaroslavl, Russia;
12Arkhangelsk Regional Clinical Oncology Center, Arkhangelsk, Russia; 13Hospital Marques de
Valdecilla, Santander, Spain; 14Aberdeen Royal Infirmary, Aberdeen, UK; 15Sverdlovsk Regional
Oncology Center, Ekaterinburg, Russia; 16Nottingham University Hospital NHS Trust,
Nottingham, UK; 17Onyx Pharmaceuticals, South San Francisco, CA, USA; 18Abramson Cancer
Center, Philadelphia, PA, USA.
*Dr. James Cassidy is currently with Roche Pharmaceuticals, Nutley, NJ, USA
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
2
Running title: Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
Keywords: metastatic colorectal cancer, sorafenib, oxaliplatin, leucovorin, and fluorouracil
Financial Support
Sponsored by Bayer Healthcare LLC and Onyx Pharmaceuticals, Inc.
Corresponding author
Josep Tabernero, MD, PhD
Medical Oncology Department
Vall d'Hebron University Hospital and Vall d'Hebron Institute of Oncology (VHIO)
Universitat Autònoma de Barcelona
P. Vall d'Hebron 119-129
08035 Barcelona, Spain
Tel +34 93 489 4301
Fax +34 93 274 6059
Email: [email protected]
Disclosures
OB, FR, TS, and EVC have received research funding from Onyx Pharmaceuticals and Bayer.
NL and YLC are employees of Onyx Pharmaceuticals and own stock.
RGC, AS, BI, and TS have consultancy or advisory relationship with Bayer.
AS has received honoraria from Bayer.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
3
Trial Registry ID: ClinicalTrial.gov NCT00865709
Word count (excluding references): 3188
Tables: 4
Figures: 2
References: 50
Supplementary material: Supplementary Appendix, Tables A1, A2, and A3
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107

Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
4
Statement of Translational Relevance
Fluorouracil-based treatment regimens have provided incremental improvements in outcomes
for patients with metastatic colorectal cancer (mCRC). Adding targeted therapies to these
regimens may provide additional benefit. Monoclonal antibodies that target signaling pathways
associated with cellular differentiation, proliferation, and survival have been developed in
mCRC, with epidermal growth factor and vascular endothelial growth factor being key targets.
Targeting a broader spectrum of molecules involved in CRC cell proliferation and death, such as
receptor and intracellular tyrosine kinases, may confer anti-cancer activity with less risk of tumor
resistance. Sorafenib is an oral multikinase inhibitor that targets both intracellular kinases and
cell surface receptor kinases. A randomized, double-blind, placebo-controlled phase II trial was
carried out to assess the combination of sorafenib with modified FOLFOX6 (leucovorin,
oxaliplatin, and fluorouracil) as a first-line therapy in patients with mCRC.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
5
Abstract
Purpose: This randomized, double-blind, placebo-controlled, phase IIb study evaluated adding
sorafenib to first-line modified FOLFOX6 (mFOLFOX6) for metastatic colorectal cancer
(mCRC).
Patients and Methods: Patients were randomized to sorafenib (400 mg BID) or placebo,
combined with mFOLFOX6 (oxaliplatin 85 mg/m2; levo-leucovorin 200 mg/m2; fluorouracil 400
mg/m2 bolus and 2400 mg/m2 continuous infusion) every 14 days. Primary endpoint was
progression-free survival (PFS). Target sample was 120 events in 180 patients for >85% power
(2-sided α=0.20) to detect a hazard ratio (HR)=0.65.
Results: Of 198 patients randomized, median PFS for sorafenib plus mFOLFOX6 was 9.1
versus 8.7 months for placebo plus mFOLFOX6 (HR=0.88, 95% CI 0.64−1.23; P=.46). There
was no difference between treatment arms for overall survival (OS). Subgroup analyses of PFS
and OS showed no difference between treatment arms by KRAS or BRAF status (mutant and
wild-type). The most common Grade 3/4 adverse events in the sorafenib and placebo arms
were neutropenia (48% v 22%), peripheral neuropathy (16% v 21%), and Grade 3 hand-foot
skin reaction (20% v 0%). Treatment discontinuation due to adverse events was 9% and 6%,
respectively. Generally, dose intensity (duration and cumulative doses) was lower in the
sorafenib arm than in the placebo arm.
Conclusion: This study did not detect a PFS benefit with the addition of sorafenib to first-line
mFOLFOX6 for mCRC. KRAS and BRAF status did not appear to impact treatment outcomes
but the subgroups were small. These results do not support further development of sorafenib in
combination with mFOLFOX6 in molecularly-unselected patients with mCRC.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107

Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
6
Introduction
Several fluorouracil-based chemotherapy regimens have been successfully developed for
patients with metastatic colorectal cancer (mCRC). Incremental improvements in response
rates, progression-free survival (PFS), and overall survival (OS) have been observed with
fluorouracil in combination with leucovorin and oxaliplatin (FOLFOX), leucovorin and irinotecan
(FOLFIRI), and leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI). Nonetheless, survival
remains limited with a 5-year rate of less than 8% (1). Strategies to further improve outcomes
have focused on adding targeted therapies to established regimens.
Advances in our understanding of the molecular basis of cancer proliferation, angiogenesis, and
metastasis enabled the development of therapies that target signaling pathways associated with
cellular differentiation, proliferation, and survival. Among these, epidermal growth factor (EGF)
and vascular endothelial growth factor (VEGF) are key targets (1). The addition of monoclonal
antibodies (mAbs) that target tyrosine kinase (TK) activity (ligands or receptors) to mCRC
chemotherapy regimens improved clinical outcomes with acceptable toxicity. These include
bevacizumab (inhibits VEGF) (2-5), and the EGF receptor (EGFR) inhibitors cetuximab and
panitumumab (6-9). Nonetheless, response can be absent if the target is not a disease driver,
and resistance can be present at the start of treatment or can emerge when tumor or stromal
cells switch to alternative pathways. The constitutive KRAS and BRAF mutations confer
resistance to cetuximab and panitumumab, and KRAS is now a valid biomarker for cetuximab
and panitumumab (10). Approximately 40% of patients with CRC have a KRAS mutation,
meaning a significant proportion will not be eligible for EGFR inhibitors (10).
Targeting a broader spectrum of molecules involved in CRC cell proliferation and death, such as
receptor and intracellular TKs, may confer anti-cancer activity with less risk of resistance (11).
Sorafenib is an oral multikinase inhibitor that targets intracellular kinases (CRAF, BRAF, mutant
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
7
BRAF), as well as cell surface receptor kinases, including platelet-derived growth factor receptor
(PDGFR), VEGFR-1–3, stem cell factor receptor (KIT), and Feline McDonough Sarcoma (FMS)-
related tyrosine kinase 3 (FLT3) (12, 13). Clinical efficacy and tolerability of sorafenib have been
shown in renal cell carcinoma (14) and hepatocellular carcinoma (15, 16). Preclinical evidence
indicates the primary target of sorafenib in renal cell carcinoma is angiogenesis via VEGFR,
whereas in hepatocellular carcinoma, cell proliferation and survival are targeted via the
RAF/MEK/ERK pathway, and angiogenesis via VEGFR and PDGFR (12, 17, 18).
Preclinical studies also demonstrated the activity of sorafenib against colon cancer cells, but
also indicated differential targeting of cell proliferation and/or angiogenesis by tumor model (12,
19-21). Early clinical studies demonstrated the feasibility of combining sorafenib with
chemotherapies used in mCRC, such as irinotecan, oxaliplatin, and 5- fluorouracil/leucovorin,
with encouraging activity in solid tumors including mCRC (22-24). In a phase I study of 37
patients with advanced solid tumors, 7/9 patients with CRC treated with oxaliplatin (130 mg/m2
on Day 1 of a 3-week cycle) and the standard sorafenib dose (400 mg twice daily [BID]
continuously) achieved stable disease for at least 6 weeks (23).
Here we present results from a phase IIb, double-blind, placebo-controlled, randomized trial that
assessed the addition of sorafenib to first-line modified FOLFOX6 (mFOLFOX6) in patients with
mCRC. The standard sorafenib regimen (400 mg BID continuously) was used based on the
collective results from the phase I combination studies (22-24) as well as its proven benefit in
other difficult-to-treat adenocarcinomas (14-16). Modified FOLFOX6 was chosen because it was
the most commonly used FOLFOX regimen across the various centers and countries of this
international study. The objective was to determine whether efficacy and tolerability results
would support a phase III confirmatory trial.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
8
Patients and Methods
Patients
Eligible patients were ≥18 years old, with histologically confirmed, measurable metastatic
adenocarcinoma of the colon or rectum (stage IV) (25), and an Eastern Cooperative Oncology
Group (ECOG) performance status 0–1. Prior radiotherapy was allowed, but at least 1
measurable, non-irradiated, metastatic lesion was required, as was a tumor tissue sample for
analysis of KRAS and BRAF mutations. Patients who had received prior chemotherapy for
metastatic disease were not eligible, nor were patients with brain metastases, active cardiac
disease, or serious bone marrow, liver, or renal dysfunction. Patients who had received adjuvant
treatment for CRC, including a FOLFOX regimen, were eligible provided that they had
completed treatment at least 12 months before randomization. The protocol was approved by
the independent ethics committees/institutional review boards of all participating sites or
countries. The trial was conducted according to Good Clinical Practice Guidelines and in
accordance with the Declaration of Helsinki. All patients provided written informed consent. The
study is registered at ClinicalTrials.gov (NCT00865709).
Study Design
This was a phase IIb, randomized, double-blind trial conducted at centers in Belgium, Romania,
Russia, Spain, the United Kingdom, and the United States. Patients were stratified by radiologic
evidence of liver involvement and number of metastatic sites (<3 or ≥3) and randomly assigned
(1:1) to mFOLFOX6 plus sorafenib or matching placebo.
Treatment
The mFOLFOX6 regimen was administered every 14 days and consisted of oxaliplatin, levo-
leucovorin (or leucovorin if levo-leucovorin not available), and fluorouracil. On Day 1 of each 14-
day cycle, patients received oxaliplatin 85 mg/m2, levo-leucovorin 200 mg/m2, then a fluorouracil
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
9
400 mg/m2 bolus followed by a 2400 mg/m2 continuous infusion (46–48 hours). All patients
received prophylactic anti-emetic treatment with intravenous dexamethasone and a 5-
hydroxytryptamine-3 antagonist 30 minutes prior to each infusion. Sorafenib and the matching
placebo were initiated on Day 1 at 400 mg BID. Dose reductions of sorafenib/placebo were
required for hand-foot skin reaction (HFSR, Grades 2/3), hypertension (symptomatic Grade 2
and Grades 3/4), proteinuria (>2g/24 hours), hematologic toxicities (Grades 3/4), or other Grade
3/4 toxicities associated with sorafenib/placebo.
In the case of dose modification or discontinuation of 1 study drug (oxaliplatin, fluorouracil/levo-
leucovorin, or sorafenib or placebo), administration of the other study drugs could be continued
at the protocol-specified doses. Any patient who continued treatment with at least 1 study drug
was considered on study.
Study Endpoints
The primary endpoint was PFS. Secondary endpoints included OS, time to progression (TTP),
overall response rate (ORR), duration of response (DOR), safety, and tolerability. Tumor
response was investigator assessed and evaluated radiologically at baseline and every 8 weeks
using Response Evaluation Criteria in Solid Tumors (RECIST) (26). Active follow-up was
extended to patients who discontinued treatment without disease progression. Adverse events
(AEs) were graded using Common Terminology Criteria for Adverse Events (version 3.0).
Serious AEs (SAEs) included events that resulted in death, were life-threatening, required or
extended hospitalization, or resulted in persistent or significant disability.
Statistical Analyses
Analysis of PFS was based on the log-rank test. Based on historical data, the expected PFS in
the control arm was 8 months (4). A sample size of 120 events would provide >85% power with
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
10
a 2-sided α= 0.20, assuming a target hazard ratio (HR) of 0.65 between sorafenib and placebo.
The target study population was 180 patients. Analysis of OS was planned after 120 deaths.
Time-to-event endpoints were analyzed by the Kaplan-Meier method in the intent-to-treat (ITT)
population. For PFS, patients without documentation of progression or death at the time of
analysis were censored at final tumor assessment or post-randomization visit; patients who
initiated non-study cancer treatment and were without disease progression were censored at
last tumor assessment prior to the start of the new treatment; patients with no post-baseline
tumor assessment were censored at Day 1; and patients who experienced progressive disease
(PD) or death 18 weeks or longer from the last tumor assessment were censored at the last
tumor assessment. A stratified log-rank test with the randomization stratification factors as
covariates was used to compare treatment arms, and the relative risk for sorafenib versus
placebo was estimated with a stratified Cox regression model.
Secondary analyses of PFS included a per-protocol analysis (patients with no major protocol
violations), and a non-stratified analysis. Planned subgroup analyses of PFS and OS were
performed using the Kaplan-Meier method and a non-stratified Cox regression for subgroups
defined by baseline factors of liver involvement (yes or no), number of metastatic sites (<3 or
≥3), region (East or West), KRAS status (wild-type or mutant), and BRAF status (wild-type or
mutant). KRAS and BRAF mutant status was determined by allelic discrimination
(Supplementary Appendix) and centrally evaluated at University Hospital Gasthuisberg,
Leuven, Belgium (S.T.). Exploratory analyses of PFS and OS were performed for subgroups
defined by NRAS and PIK3CA status (wild-type or mutant), age (<65 or ≥65 years), gender,
ECOG performance status (0 or 1), disease stage at diagnosis (I–III or IV), and months since
initial diagnosis (<2 or ≥2). ORR was compared between groups using the Cochran-Mantel-
Haenszel test, adjusting for the stratification factors. Descriptive statistics summarized safety
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
11
and tolerability variables, including study drug exposure and AE rates. Statistical analyses were
performed with SAS version 9.1 or later (SAS Institute, Cary, NC). The lead author (JT) had full
access to study data and analyses, which were available to all authors upon request.
Results
Patient recruitment occurred between March 2009 and February 2010 with 198 patients
randomized (Figure 1). Data cut-off for the primary analysis of PFS, response, safety, and
tolerability was January 31, 2011. An analysis of OS was subsequently conducted after 123
deaths with a cut-off date of December 1, 2011, and a median follow-up of 22.4 months.
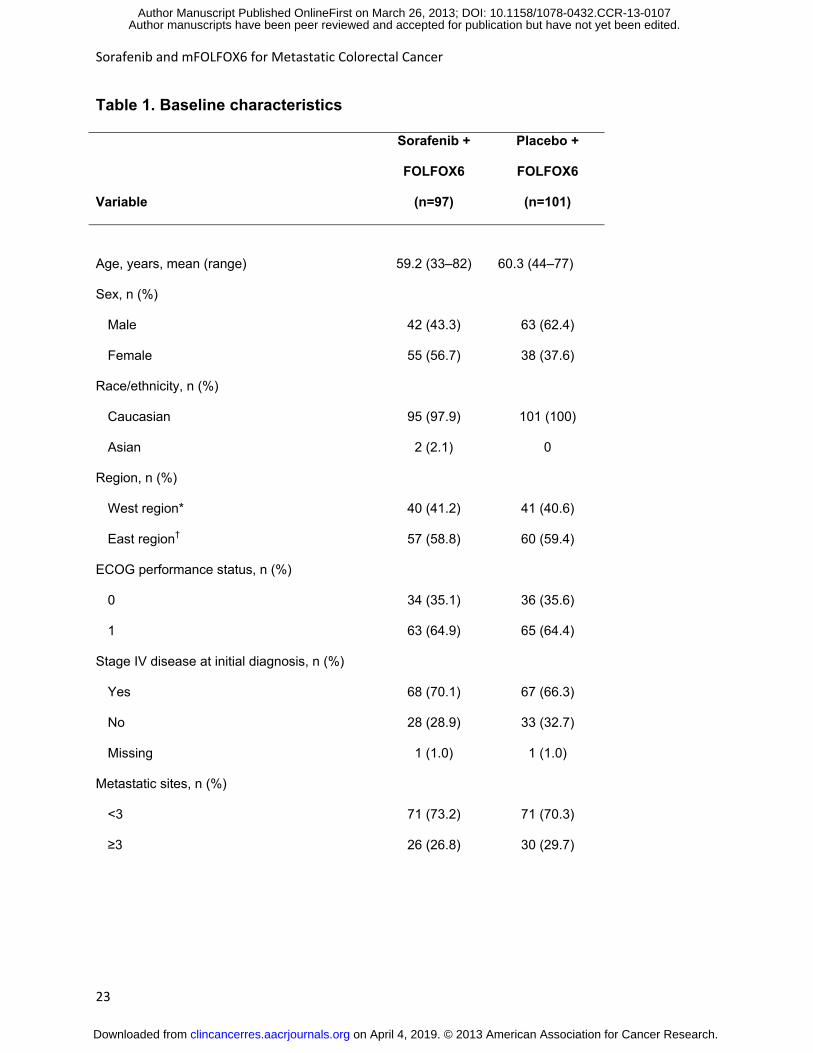
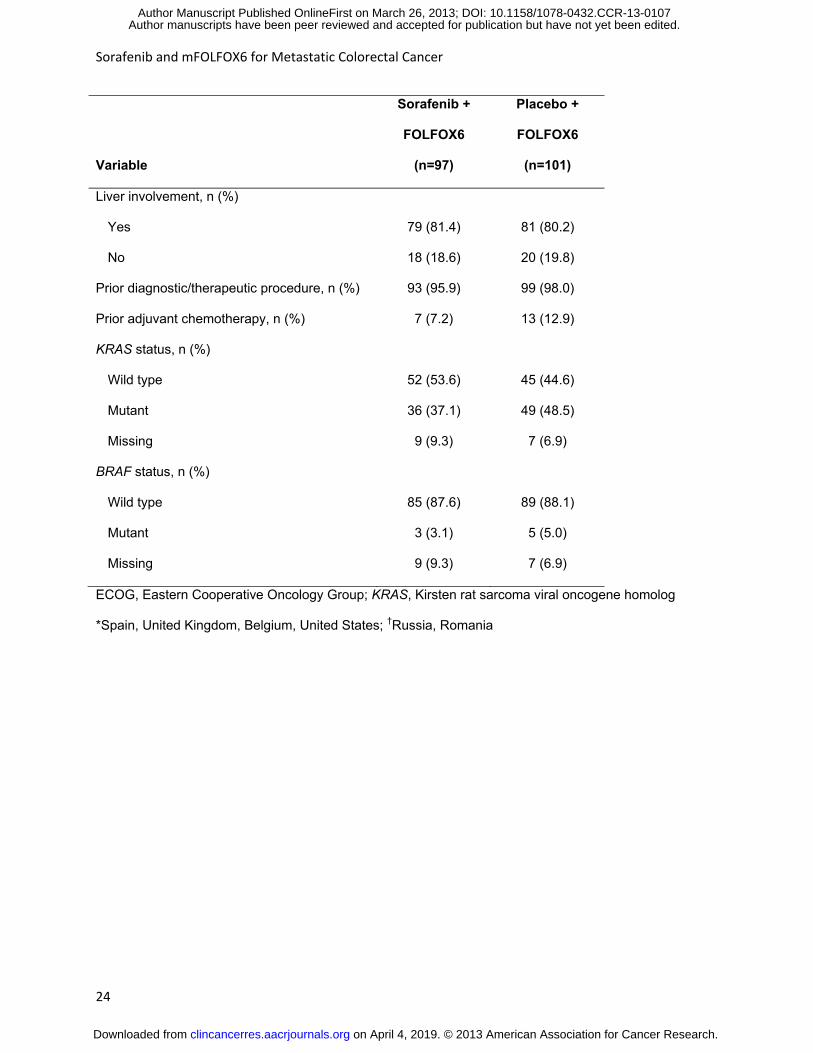
Baseline characteristics were generally balanced between treatment arms (Table 1). Most
patients had an ECOG performance status of 1 (64.6%), stage IV disease as initial diagnosis
(68.2%), <3 metastatic sites (71.7%), and liver involvement (80.8%). Of note, the sorafenib arm
had fewer males compared with the placebo arm (43.3% v 62.4%), less exposure to adjuvant
chemotherapy (7.2% v 12.9%), and lower rates of KRAS mutations (37.1% v 48.5%). BRAF
mutations were infrequent in both arms (3.1% v 5.0%).
Efficacy Outcomes
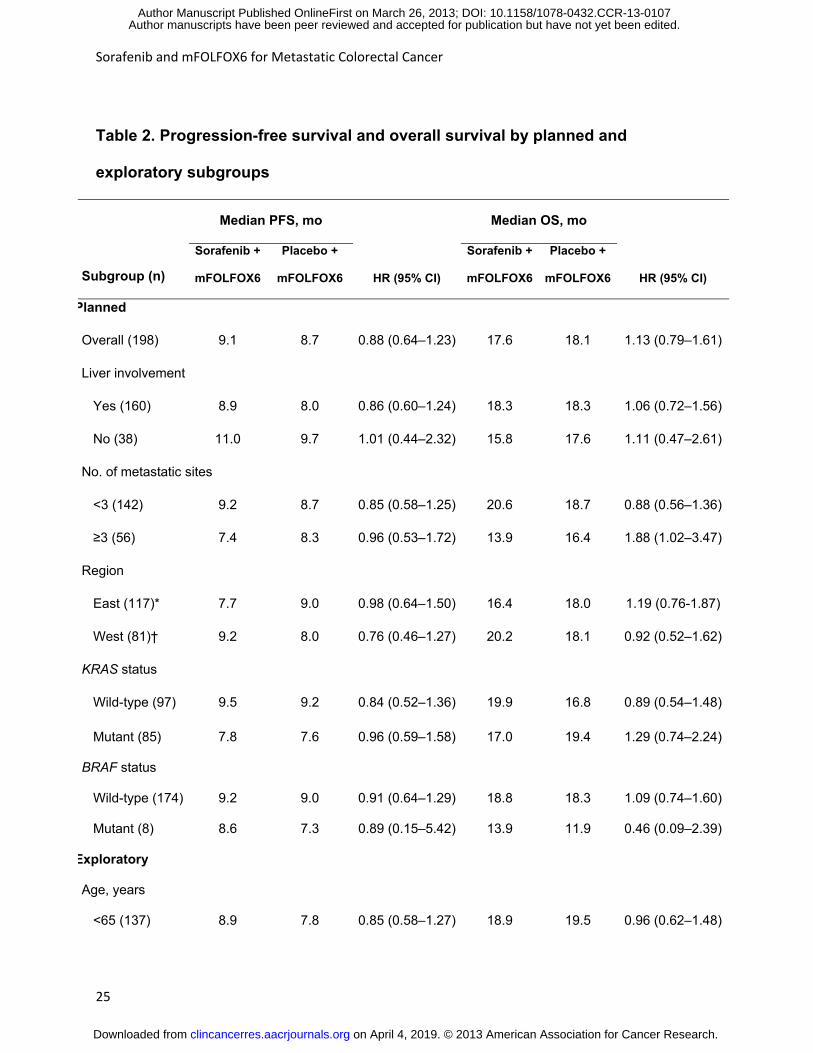
Median PFS was 9.1 months for the sorafenib arm and 8.7 months for the placebo arm
(HR=0.88; 95% confidence interval [CI] 0.64–1.23; P=.46) (Figure 2). Similar results were
observed in the prespecified subgroup analyses (Table 2). In patients with wild-type KRAS, the
median PFS was 9.5 versus 9.2 months, respectively (HR=0.84; 95% CI 0.52–1.36), with
corresponding medians of 7.8 versus 7.6 months, respectively, in the mutant KRAS subgroup
(HR=0.96; 95% CI 0.59–1.58). In patients with wild-type BRAF, the median PFS was 9.2 versus
9.0 months, respectively (HR=0.91; 95% CI 0.64–1.29), and the median PFS for mutant BRAF
was 8.6 versus 7.3 months, respectively (HR=0.89; 95% CI 0.15–5.42).
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107

Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
12
Median OS was 17.6 months in the sorafenib arm and 18.1 months in the placebo arm
(HR=1.13; 95% CI 0.79–1.61; P=.51). In patients with wild-type KRAS, median OS was 19.9
versus 16.8 months, respectively (HR=0.89; 95% CI 0.54–1.48), and 17.0 versus 19.4 months,
respectively, in patients with mutant KRAS (HR=1.29; 95% CI 0.74–2.24). In patients with wild-
type BRAF, median OS was 18.8 versus 18.3 months, respectively (HR=1.09; 95% CI 0.74–
1.60), and 13.9 versus 11.9 months, respectively, in patients with mutant BRAF (HR=0.46; 95%
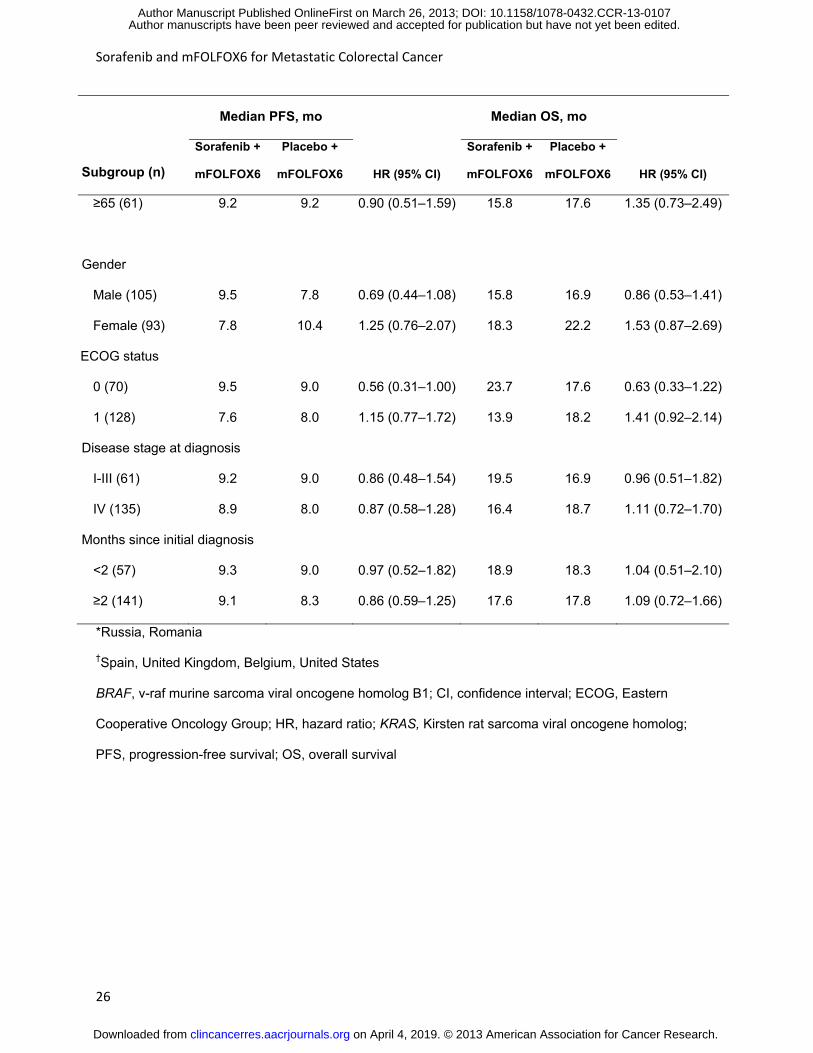
CI 0.09–2.39). Exploratory subgroup analyses showed slightly different outcomes between
treatment arms by gender and ECOG status (Table 2). There were no differences in survival
outcomes between treatment arms in the PIK3CA or in the NRAS subgroups (Supplementary
Appendix, Tables A1 and A2).
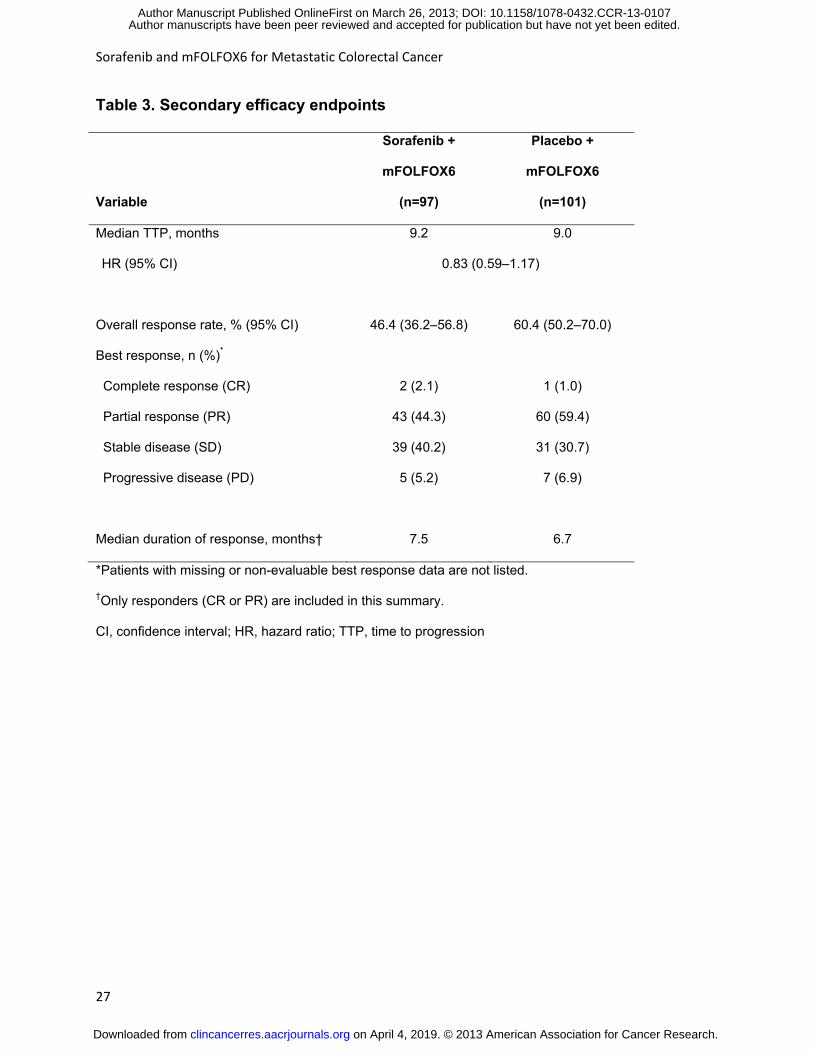
Median TTP was 9.2 months in the sorafenib arm and 9.0 months in the placebo arm (HR=0.83;
95% CI 0.59–1.17), and the ORR was 46.4% and 60.4%, respectively (Table 3). Partial
response was lower in the sorafenib arm compared with mFOLFOX6 alone (44.3% v 59.4%),
but the rate of stable disease was higher (40.2% v 30.7%). Complete response was achieved by
2 patients in the sorafenib arm and 1 patient in the placebo arm.
Safety and Tolerability
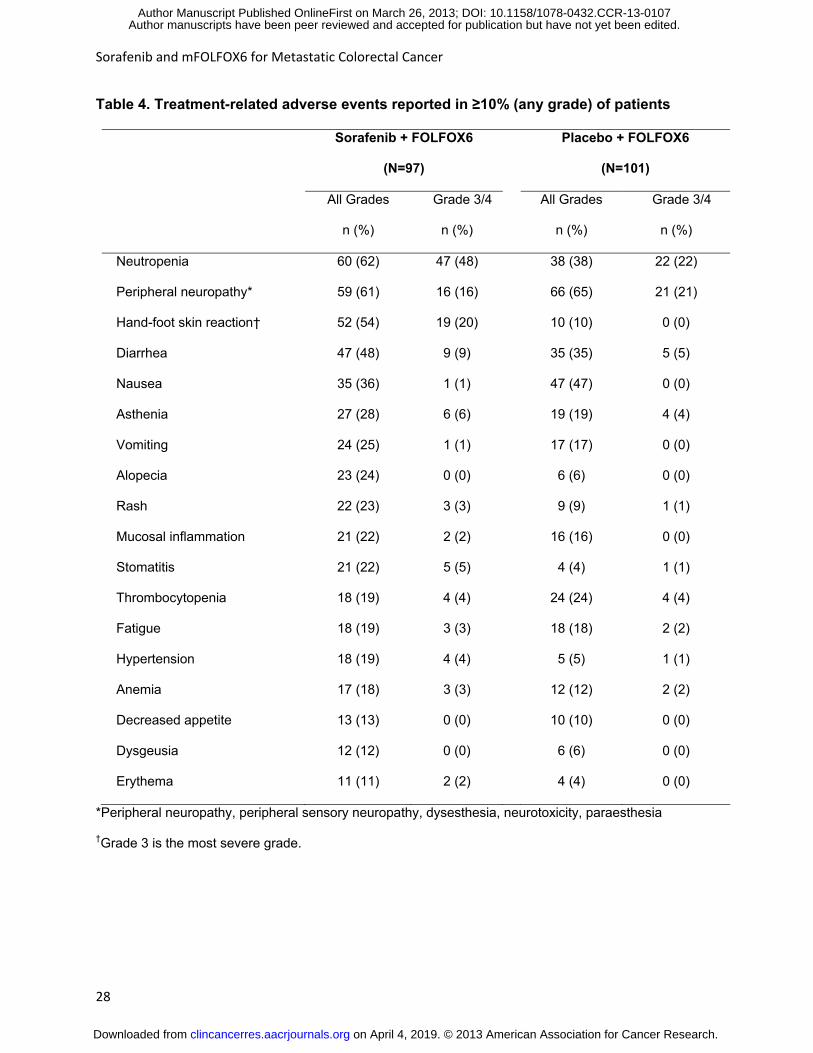
Treatment-related AEs occurring in ≥10% of patients are shown in Table 4. The most common
AEs (any grade) in the sorafenib and placebo arms included neutropenia (62% v 38%),
peripheral neuropathy (61% v 65%), diarrhea (48% v 35%), nausea (36% v 47%), HFSR (54% v
10%), and asthenia (28% v 19%). Other AEs (any grade) of interest were stomatitis (22% v 4%),
rash (23% v 9%), and hypertension (19% v 5%). The most common Grade 3/4 AEs in the
sorafenib and placebo arms were neutropenia (48% v 22%), peripheral neuropathy (16% v
21%), and HFSR (20% v 0%). Treatment-related SAEs occurred in 21 (22%) patients in the
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
13
sorafenib arm and 16 (16%) patients in the placebo arm. There were 2 treatment-related deaths
in the sorafenib arm (1 pancytopenia and 1 renal failure) and 1 in the placebo arm
(cardiovascular insufficiency).
More frequent dose interruptions and reductions were observed for sorafenib than placebo
(Supplementary Appendix Table A3). The average daily dose of sorafenib was lower than
placebo (mean, 553.1 v 728.1 mg), which corresponded to a greater frequency of dose
reductions (66.0% v 27.7%) and a shorter mean duration of treatment (30.5 v 33.7 weeks).
Similar trends were observed for components of mFOLFOX6, although the magnitude of the
difference between treatment arms was less pronounced. Overall, 9.4% of patients discontinued
treatment due to AEs in the sorafenib arm compared with 5.9% in the placebo arm.
Discussion
In this randomized phase IIb trial, the addition of sorafenib 400 mg BID to mFOLFOX6
compared with placebo did not demonstrate an improvement in PFS to support a phase III trial.
Generally, there was no differential outcome across subgroups, including KRAS and BRAF
subgroups. There was also no improvement in TTP or ORR. There were no unexpected
toxicities associated with the addition of sorafenib, but there were increases in some Grade 3/4
AE rates, most notably neutropenia and HFSR, which led to increased rates of dose
modifications and treatment discontinuations for reasons other than disease progression.
Overall, the average daily dose of sorafenib was lower than placebo, and exposure to each of
the mFOLFOX6 components was also lower in the sorafenib arm.
While these results allow us to exclude a strong therapeutic benefit with sorafenib plus
mFOLFOX6, a number of factors may have influenced the results and should be considered.
First, the sample size would have been too small to adequately assess a modest therapeutic
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107

Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
14
benefit. Given the inter- and intra-patient heterogeneity in primary and metastatic CRC tumor
types (27, 28), a more modest benefit would not be unexpected for a targeted therapy. Second,
use of sorafenib in mCRC may be better suited for regimens that are less active than
mFOLFOX6 but more tolerable and where an increase in activity would be more easily
detected. Third, the 400 mg BID dose of sorafenib may not have provided sufficient target
inhibition, which may have been accentuated by the decrease in dose intensity of both sorafenib
and mFOLFOX6 over the course of treatment.
Thus far, results of studies with targeted therapies in combination with mCRC chemotherapy
have been mixed, ranging from significant improvements in PFS or OS to decreases in PFS or
OS, depending on the chemotherapy regimen and patient population (2-5, 9, 29-31). A number
of phase III studies have shown that adding bevacizumab to fluorouracil-based regimens
improves PFS with or without a corresponding improvement in OS (2-4, 29), but the magnitude
of the benefits have been inconsistent (5). This may be related to the fluorouracil backbone
combined with bevacizumab and/or the line of therapy (2-4). Variability in results has also been
observed across cetuximab (6, 9, 31) and panitumumab studies (7, 8). It has been hypothesized
that inconsistencies in outcomes with mAbs could also be related to their high specificity, which
may make them susceptible to resistance through redundant signaling pathways (11). Attempts
to broaden activity by combining different mAbs have not proven fruitful in mCRC (32-34).
Results with small-molecule multikinase inhibitors with a broader spectrum of inhibitory targets
than mAbs (35) have also been mixed, although limited data are available in addition to the
results reported here (36-40). In 2 phase III trials in mCRC, adding vatalanib (targets VEGFR1-
3, PDGFRβ, and KIT) to first- or second-line FOLFOX4 did not improve PFS or OS (36, 37), and
a phase III study of sunitinib (targets VEGFR1-3, PDGFRα/β, KIT, FLT3, CSF1R, RET) with
FOLFIRI failed to demonstrate an improvement in the primary endpoint of PFS (41). Cediranib
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
15
(targets VEGFR1-3, PDGFRβ, and KIT), has been evaluated with FOLFOX in mCRC in 3
different phase II/III trials (42-44), with only 1 study demonstrating a statistically significant but
clinically modest improvement in median PFS (+0.4 months) (45). Nevertheless, other
multikinase inhibitors may have potential in mCRC. In a phase III trial, regorafenib (targets
VEGFR1-3, Tie-2, PDGFR, FGFR, KIT, RET, and BRAF) provided a survival benefit when
added to best supportive care in patients with refractory mCRC (46, 47). It is notable that
regorafenib was active in the refractory setting as monotherapy, whereas mCRC studies with
other targeted agents lacked single-agent activity or were paired with chemotherapy in the first-
or second-line setting.
Several factors may explain the variability in results with targeted therapies in mCRC. It is
becoming evident that the genetic profiles of tumors are predictive of treatment response to
targeted therapies. In our study, by adding sorafenib to a standard first-line chemotherapy for
mCRC, several pathways shown to be critical in mCRC were targeted, like angiogenesis via
extracellular TK receptors VEGFR1-3 and PDGFR, as well as downstream protein effectors of
TK receptors (e.g., EGFR) including CRAF, BRAF, and mutant BRAF (12, 13, 20, 21). As RAF
is targeted by sorafenib and is downstream of RAS, we hypothesized that mCRC patients could
potentially derive benefit by the addition of sorafenib independent of KRAS and BRAF gene
mutation status. However, this is a highly redundant pathway with complex feedback loops,
which makes it unlikely for RAF inhibition alone to be sufficient for antitumoral activity (48).
In the current study, the tumor sample was taken from either the primary or metastatic site, and
it does not appear that KRAS or BRAF status had a significant impact on outcomes in patients
receiving sorafenib. However, the size of the study population and subgroups limits the
interpretation of these data. Sorafenib may be more active with other chemotherapy regimens
and/or in more specific patient populations. Although a pharmacokinetic interaction between
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
16
sorafenib and oxaliplatin was not detected in a phase I trial of solid tumors (23), some preclinical
evidence suggests that sorafenib may reduce cellular uptake of platinum compounds (49). The
addition of sorafenib to other mCRC regimens, such as irinotecan alone (50) or FOLFIRI
(NCT00839111), are being explored. In addition, studies in various mCRC models showed
differential response to sorafenib (12, 20, 21). Sorafenib demonstrated inhibition of tumor
growth and angiogenesis in HT-29 colon cells (BRAF V600E mutation), inhibition of tumor
growth in HCT-116 cells (activating KRAS mutation), but notably less activity in DLD-1
(activating KRAS mutation) and Colo-205 (BRAF V600E mutation) cells. Further assessment of
sorafenib and other targeted therapies across mCRC models may help us to better understand
and predict treatment response of primary and metastatic tumors in CRC patients.
In conclusion, the dose and schedule of sorafenib with first-line mFOLFOX6 in this study did not
demonstrate a PFS benefit in patients with mCRC to support a phase III trial of similar design.
KRAS and BRAF status did not appear to impact response to sorafenib, but patient numbers
were small. Further assessment of tumor samples for biomarkers are ongoing and includes
gene expression profiling. Although the results of this study do not support further development
of sorafenib with this combination in an unselected patient population, they may help to guide
the design of future clinical trials in mCRC with targeted therapies focusing on molecularly-
characterized populations.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
17
Acknowledgments
This study was supported by Bayer Healthcare Pharmaceuticals and Onyx Pharmaceuticals.
The authors would like to thank Melanie Watson, PhD and Michael Raffin (Fishawack
Communications) for providing writing and editorial assistance which was funded by Bayer
HealthCare Pharmaceuticals and Onyx Pharmaceuticals. EVC and ST are senior investigators
of the Fund for Scientific Research Flanders and are supported by the Belgian Foundation
against Cancer.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107

Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
18
References
1. Gravalos C, Cassinello J, Fernandez-Ranada I, Holgado E. Role of tyrosine kinase
inhibitors in the treatment of advanced colorectal cancer. Clin Colorectal Cancer 2007;6:691-9.
2. Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, et al.
Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N
Engl J Med 2004;350:2335-42.
3. Giantonio BJ, Catalano PJ, Meropol NJ, O'Dwyer PJ, Mitchell EP, Alberts SR, et al.
Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for
previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology
Group Study E3200. J Clin Oncol 2007;25:1539-44.
4. Saltz LB, Clarke S, Diaz-Rubio E, Scheithauer W, Figer A, Wong R, et al. Bevacizumab
in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal
cancer: a randomized phase III study. J Clin Oncol 2008;26:2013-9.
5. Loupakis F, Bria E, Vaccaro V, Cuppone F, Milella M, Carlini P, et al. Magnitude of
benefit of the addition of bevacizumab to first-line chemotherapy for metastatic colorectal
cancer: meta-analysis of randomized clinical trials. J Exp Clin Cancer Res 2010;29:58.
6. Van Cutsem E, Kohne CH, Hitre E, Zaluski J, Chang Chien CR, Makhson A, et al.
Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med
2009;360:1408-17.
7. Douillard JY, Siena S, Cassidy J, Tabernero J, Burkes R, Barugel M, et al. Randomized,
phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4)
versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic
colorectal cancer: the PRIME study. J Clin Oncol 2010;28:4697-705.
8. Peeters M, Price TJ, Cervantes A, Sobrero AF, Ducreux M, Hotko Y, et al. Randomized
phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI)
compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal
cancer. J Clin Oncol 2010;28:4706-13.
9. Bokemeyer C, Bondarenko I, Makhson A, Hartmann JT, Aparicio J, de Braud F, et al.
Fluorouracil, leucovorin, and oxaliplatin with and without cetuximab in the first-line treatment of
metastatic colorectal cancer. J Clin Oncol 2009;27:663-71.
10. Pritchard CC, Grady WM. Colorectal cancer molecular biology moves into clinical
practice. Gut 2011;60:116-29.
11. Petrelli A, Giordano S. From single- to multi-target drugs in cancer therapy: when
aspecificity becomes an advantage. Curr Med Chem 2008;15:422-32.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
19
12. Wilhelm SM, Adnane L, Newell P, Villanueva A, Llovet JM, Lynch M. Preclinical
overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF
receptor tyrosine kinase signaling. Mol Cancer Ther 2008;7:3129-40.
13. Strumberg D. Preclinical and clinical development of the oral multikinase inhibitor
sorafenib in cancer treatment. Drugs Today (Barc) 2005;41:773-84.
14. Escudier B, Eisen T, Stadler WM, Szczylik C, Oudard S, Staehler M, et al. Sorafenib for
treatment of renal cell carcinoma: Final efficacy and safety results of the phase III treatment
approaches in renal cancer global evaluation trial. J Clin Oncol 2009;27:3312-8.
15. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in
advanced hepatocellular carcinoma. N Engl J Med 2008;359:378-90.
16. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacy and safety of
sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase
III randomised, double-blind, placebo-controlled trial. Lancet Oncol 2009;10:25-34.
17. Liu L, Cao Y, Chen C, Zhang X, McNabola A, Wilkie D, et al. Sorafenib blocks the
RAF/MEK/ERK pathway, inhibits tumor angiogenesis, and induces tumor cell apoptosis in
hepatocellular carcinoma model PLC/PRF/5. Cancer Res 2006;66:11851-8.
18. Chang YS, Adnane J, Trail PA, Levy J, Henderson A, Xue D, et al. Sorafenib (BAY 43-
9006) inhibits tumor growth and vascularization and induces tumor apoptosis and hypoxia in
RCC xenograft models. Cancer Chemother Pharmacol 2007;59:561-74.
19. Walker T, Mitchell C, Park MA, Yacoub A, Graf M, Rahmani M, et al. Sorafenib and
vorinostat kill colon cancer cells by CD95-dependent and -independent mechanisms. Mol
Pharmacol 2009;76:342-55.
20. Wilhelm SM, Carter C, Tang L, Wilkie D, McNabola A, Rong H, et al. BAY 43-9006
exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and
receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res
2004;64:7099-109.
21. Wilhelm S, Chien DS. BAY 43-9006: preclinical data. Curr Pharm Des 2002;8:2255-7.
22. Mross K, Steinbild S, Baas F, Gmehling D, Radtke M, Voliotis D, et al. Results from an in
vitro and a clinical/pharmacological phase I study with the combination irinotecan and sorafenib.
Eur J Cancer 2007;43:55-63.
23. Kupsch P, Henning BF, Passarge K, Richly H, Wiesemann K, Hilger RA, et al. Results of
a phase I trial of sorafenib (BAY 43-9006) in combination with oxaliplatin in patients with
refractory solid tumors, including colorectal cancer. Clin Colorectal Cancer 2005;5:188-96.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
20
24. Figer A, Moscovici M, Bulconic S, Radu P, Atsmon J, Shmuely E, et al. Phase I trial of
BAY 43-9006 in combination with 5-fluorouracil (5-FU) and leucovorin (LCV) in patients with
advanced refractory solid tumors. Ann Oncol 2004;15:iii87. Abstract 327.
25. Edge S, Byrd D, Compton C, Fritz A, Greene F, Trotti A, editors. AJCC Cancer Staging
Manual. 7th ed. New York, NY: Springer; 2010.
26. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al.
New guidelines to evaluate the response to treatment in solid tumors. European Organization
for Research and Treatment of Cancer, National Cancer Institute of the United States, National
Cancer Institute of Canada. J Natl Cancer Inst 2000;92:205-16.
27. Li Z, Jin K, Lan H, Teng L. Heterogeneity in primary colorectal cancer and its
corresponding metastases: a potential reason of EGFR-targeted therapy failure? Hepato-
gastroenterology 2011;58:411-6.
28. Baldus SE, Schaefer KL, Engers R, Hartleb D, Stoecklein NH, Gabbert HE. Prevalence
and heterogeneity of KRAS, BRAF, and PIK3CA mutations in primary colorectal
adenocarcinomas and their corresponding metastases. Clin Cancer Res 2010;16:790-9.
29. Hurwitz HI, Fehrenbacher L, Hainsworth JD, Heim W, Berlin J, Holmgren E, et al.
Bevacizumab in combination with fluorouracil and leucovorin: an active regimen for first-line
metastatic colorectal cancer. J Clin Oncol 2005;23:3502-8.
30. Stathopoulos GP, Batziou C, Trafalis D, Koutantos J, Batzios S, Stathopoulos J, et al.
Treatment of colorectal cancer with and without bevacizumab: a phase III study. Oncology
2010;78:376-81.
31. Van Cutsem E, Kohne CH, Lang I, Folprecht G, Nowacki MP, Cascinu S, et al.
Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic
colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF
mutation status. J Clin Oncol 2011;29:2011-9.
32. Saltz L, Badarinath S, Dakhil S, Bienvenu B, Harker WG, Birchfield G, et al. Phase III
Trial of Cetuximab, Bevacizumab, and 5-Fluorouracil/Leucovorin vs. FOLFOX-Bevacizumab in
Colorectal Cancer. Clin Colorectal Cancer 2011.
33. Hecht JR, Mitchell E, Chidiac T, Scroggin C, Hagenstad C, Spigel D, et al. A randomized
phase IIIB trial of chemotherapy, bevacizumab, and panitumumab compared with chemotherapy
and bevacizumab alone for metastatic colorectal cancer. J Clin Oncol 2009;27:672-80.
34. Tol J, Koopman M, Cats A, Rodenburg CJ, Creemers GJ, Schrama JG, et al.
Chemotherapy, bevacizumab, and cetuximab in metastatic colorectal cancer. N Engl J Med
2009;360:563-72.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107

Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
21
35. Broekman F, Giovannetti E, Peters GJ. Tyrosine kinase inhibitors: Multi-targeted or
single-targeted? World J Clin Oncol 2011;2:80-93.
36. Hecht JR, Trarbach T, Hainsworth JD, Major P, Jager E, Wolff RA, et al. Randomized,
placebo-controlled, phase III study of first-line oxaliplatin-based chemotherapy plus PTK787/ZK
222584, an oral vascular endothelial growth factor receptor inhibitor, in patients with metastatic
colorectal adenocarcinoma. J Clin Oncol 2011;29:1997-2003.
37. Van Cutsem E, Bajetta E, Valle J, Kohne CH, Hecht JR, Moore M, et al. Randomized,
placebo-controlled, phase III study of oxaliplatin, fluorouracil, and leucovorin with or without
PTK787/ZK 222584 in patients with previously treated metastatic colorectal adenocarcinoma. J
Clin Oncol 2011;29:2004-10.
38. Chen E, Jonker D, Gauthier I, MacLean M, Wells J, Powers J, et al. Phase I study of
cediranib in combination with oxaliplatin and infusional 5-Fluorouracil in patients with advanced
colorectal cancer. Clin Cancer Res 2009;15:1481-6.
39. Stewart MW. Aflibercept (VEGF-TRAP): The Next Anti-VEGF Drug. Inflamm Allergy
Drug Targets 2011;10:497-508.
40. Carrato A, Swieboda-Sadlej A, Staszewska-Skurczynska M, Lim R, Roman L, Shparyk
Y, et al. Final results from a randomized, double-blind, phase III study of sunitinib plus FOLFIRI
vs. placebo plus FOLFIRI in first-line treatment of patients (pts) with metastatic colorectal cancer
(mCRC). Ann Oncol 2010;21:vi19. Abstract O-0026.
41. Mross K, Buchert M, Fasol U, Jaehde U, Kanefendt F, Strumberg D, et al. A preliminary
report of a Phase II study of folinic acid, 5-fluorouracil, irinotecan (FOLFIRI) plus sunitinib with
toxicity, efficacy, pharmacokinetics, biomarker, imaging data in patients with colorectal cancer
with liver metastases as 1st line treatment. Int J Clin Pharmacol Ther 2011;49:96-8.
42. Cunningham D, Wong RP, D'haens G, Douillard J, Robertson J, Saunders O, et al. A
phase II, double-blind, randomized multicenter study of cediranib with FOLFOX versus
bevacizumab with FOLFOX in patients with previously treated metastatic colorectal cancer
(mCRC): Final PFS results. ASCO Meeting Abstracts 2008;26:4028.
43. Hoff PM, Hochhaus A, Pestalozzi BC, Tebbutt NC, Li J, Kim TW, et al. Cediranib Plus
FOLFOX/CAPOX Versus Placebo Plus FOLFOX/CAPOX in Patients With Previously Untreated
Metastatic Colorectal Cancer: A Randomized, Double-Blind, Phase III Study (HORIZON II). J
Clin Oncol 2012;30:3596-603.
44. Schmoll HJ, Cunningham D, Sobrero A, Karapetis CS, Rougier P, Koski SL, et al.
Cediranib With mFOLFOX6 Versus Bevacizumab With mFOLFOX6 As First-Line Treatment for
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
22
Patients With Advanced Colorectal Cancer: A Double-Blind, Randomized Phase III Study
(HORIZON III). J Clin Oncol 2012;30:3588-95.
45. Hoff PM, Hochhaus A, Pestalozzi BC, Tebbutt NC, Li J, Kim TW, et al. Cediranib +
FOLFOX/XELOX versus placebo + FOLFOX/XELOX in patients (pts) WITH previously
untreated metastatic colorectal cancer (mCRC): a randomized, double-blind, phase III study
(HORIZON II). Ann Oncol 2010;21:viii9. Abstract LBA 19.
46. Grothey A, Van Cutsem E, Sobrero A, Siena S, Falcone A, Ychou M, et al. Regorafenib
monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international,
multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013;381:303-12
47. Wilhelm SM, Dumas J, Adnane L, Lynch M, Carter CA, Schutz G, et al. Regorafenib
(BAY 73-4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor
tyrosine kinases with potent preclinical antitumor activity. Int J Cancer 2011;129:245-55.
48. Prahallad A, Sun C, Huang S, Di Nicolantonio F, Salazar R, Zecchin D, et al.
Unresponsiveness of colon cancer to BRAF(V600E) inhibition through feedback activation of
EGFR. Nature 2012;483:100-3.
49. Heim M, Scharifi M, Zisowsky J, Jaehde U, Voliotis D, Seeber S, et al. The Raf kinase
inhibitor BAY 43-9006 reduces cellular uptake of platinum compounds and cytotoxicity in human
colorectal carcinoma cell lines. Anticancer Drugs 2005;16:129-36.
50. Samalin E, Bouche O, Thezenas S, Francxois E, Adenis A, Bennouna J, et al. Final
results of a multicentre phase II trial assessing sorafenib in combination with irinotecan as 2nd
or later-line treatment in metastatic colorectal cancer (MCRC) patients with KRAS mutated
tumors (MT) (NEXIRI). Ann Oncol 2011;22:v10. Abstract O-0001.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
23
Table 1. Baseline characteristics
Variable
Sorafenib +
FOLFOX6
(n=97)
Placebo +
FOLFOX6
(n=101)
Age, years, mean (range)
59.2 (33–82)
60.3 (44–77)
Sex, n (%)
Male
Female
42 (43.3)
55 (56.7)
63 (62.4)
38 (37.6)
Race/ethnicity, n (%)
Caucasian
Asian
95 (97.9)
2 (2.1)
101 (100)
0
Region, n (%)
West region*
East region†
40 (41.2)
57 (58.8)
41 (40.6)
60 (59.4)
ECOG performance status, n (%)
0
1
34 (35.1)
63 (64.9)
36 (35.6)
65 (64.4)
Stage IV disease at initial diagnosis, n (%)
Yes
No
Missing
68 (70.1)
28 (28.9)
1 (1.0)
67 (66.3)
33 (32.7)
1 (1.0)
Metastatic sites, n (%)
<3
≥3
71 (73.2)
26 (26.8)
71 (70.3)
30 (29.7)
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
24
Variable
Sorafenib +
FOLFOX6
(n=97)
Placebo +
FOLFOX6
(n=101)
Liver involvement, n (%)
Yes
No
79 (81.4)
18 (18.6)
81 (80.2)
20 (19.8)
Prior diagnostic/therapeutic procedure, n (%) 93 (95.9) 99 (98.0)
Prior adjuvant chemotherapy, n (%) 7 (7.2) 13 (12.9)
KRAS status, n (%)
Wild type
Mutant
Missing
52 (53.6)
36 (37.1)
9 (9.3)
45 (44.6)
49 (48.5)
7 (6.9)
BRAF status, n (%)
Wild type
Mutant
Missing
85 (87.6)
3 (3.1)
9 (9.3)
89 (88.1)
5 (5.0)
7 (6.9)
ECOG, Eastern Cooperative Oncology Group; KRAS, Kirsten rat sarcoma viral oncogene homolog
*Spain, United Kingdom, Belgium, United States; †Russia, Romania
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
25
Table 2. Progression-free survival and overall survival by planned and
exploratory subgroups
Median PFS, mo Median OS, mo
Subgroup (n)
Sorafenib +
mFOLFOX6
Placebo +
mFOLFOX6 HR (95% CI)
Sorafenib +
mFOLFOX6
Placebo +
mFOLFOX6 HR (95% CI)
Planned
Overall (198) 9.1 8.7 0.88 (0.64–1.23) 17.6 18.1 1.13 (0.79–1.61)
Liver involvement
Yes (160) 8.9 8.0 0.86 (0.60–1.24) 18.3 18.3 1.06 (0.72–1.56)
No (38) 11.0 9.7 1.01 (0.44–2.32) 15.8 17.6 1.11 (0.47–2.61)
No. of metastatic sites
<3 (142) 9.2 8.7 0.85 (0.58–1.25) 20.6 18.7 0.88 (0.56–1.36)
≥3 (56) 7.4 8.3 0.96 (0.53–1.72) 13.9 16.4 1.88 (1.02–3.47)
Region
East (117)* 7.7 9.0 0.98 (0.64–1.50) 16.4 18.0 1.19 (0.76-1.87)
West (81)† 9.2 8.0 0.76 (0.46–1.27) 20.2 18.1 0.92 (0.52–1.62)
KRAS status
Wild-type (97) 9.5 9.2 0.84 (0.52–1.36) 19.9 16.8 0.89 (0.54–1.48)
Mutant (85) 7.8 7.6 0.96 (0.59–1.58) 17.0 19.4 1.29 (0.74–2.24)
BRAF status
Wild-type (174) 9.2 9.0 0.91 (0.64–1.29) 18.8 18.3 1.09 (0.74–1.60)
Mutant (8) 8.6 7.3 0.89 (0.15–5.42) 13.9 11.9 0.46 (0.09–2.39)
Exploratory
Age, years
<65 (137) 8.9 7.8 0.85 (0.58–1.27) 18.9 19.5 0.96 (0.62–1.48)
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
26
Median PFS, mo Median OS, mo
Subgroup (n)
Sorafenib +
mFOLFOX6
Placebo +
mFOLFOX6 HR (95% CI)
Sorafenib +
mFOLFOX6
Placebo +
mFOLFOX6 HR (95% CI)
≥65 (61) 9.2 9.2 0.90 (0.51–1.59) 15.8 17.6 1.35 (0.73–2.49)
Gender
Male (105) 9.5 7.8 0.69 (0.44–1.08) 15.8 16.9 0.86 (0.53–1.41)
Female (93) 7.8 10.4 1.25 (0.76–2.07) 18.3 22.2 1.53 (0.87–2.69)
ECOG status
0 (70) 9.5 9.0 0.56 (0.31–1.00) 23.7 17.6 0.63 (0.33–1.22)
1 (128) 7.6 8.0 1.15 (0.77–1.72) 13.9 18.2 1.41 (0.92–2.14)
Disease stage at diagnosis
I-III (61) 9.2 9.0 0.86 (0.48–1.54) 19.5 16.9 0.96 (0.51–1.82)
IV (135) 8.9 8.0 0.87 (0.58–1.28) 16.4 18.7 1.11 (0.72–1.70)
Months since initial diagnosis
<2 (57) 9.3 9.0 0.97 (0.52–1.82) 18.9 18.3 1.04 (0.51–2.10)
≥2 (141) 9.1 8.3 0.86 (0.59–1.25) 17.6 17.8 1.09 (0.72–1.66)
*Russia, Romania
†Spain, United Kingdom, Belgium, United States
BRAF, v-raf murine sarcoma viral oncogene homolog B1; CI, confidence interval; ECOG, Eastern
Cooperative Oncology Group; HR, hazard ratio; KRAS, Kirsten rat sarcoma viral oncogene homolog;
PFS, progression-free survival; OS, overall survival
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
27
Table 3. Secondary efficacy endpoints
Variable
Sorafenib +
mFOLFOX6
(n=97)
Placebo +
mFOLFOX6
(n=101)
Median TTP, months 9.2 9.0
HR (95% CI) 0.83 (0.59–1.17)
Overall response rate, % (95% CI) 46.4 (36.2–56.8) 60.4 (50.2–70.0)
Best response, n (%)*
Complete response (CR) 2 (2.1) 1 (1.0)
Partial response (PR) 43 (44.3) 60 (59.4)
Stable disease (SD) 39 (40.2) 31 (30.7)
Progressive disease (PD) 5 (5.2) 7 (6.9)
Median duration of response, months† 7.5 6.7
*Patients with missing or non-evaluable best response data are not listed.
†Only responders (CR or PR) are included in this summary.
CI, confidence interval; HR, hazard ratio; TTP, time to progression
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
28
Table 4. Treatment-related adverse events reported in ≥10% (any grade) of patients
Sorafenib + FOLFOX6
(N=97)
Placebo + FOLFOX6
(N=101)
All Grades
n (%)
Grade 3/4
n (%)
All Grades
n (%)
Grade 3/4
n (%)
Neutropenia 60 (62) 47 (48) 38 (38) 22 (22)
Peripheral neuropathy* 59 (61) 16 (16) 66 (65) 21 (21)
Hand-foot skin reaction† 52 (54) 19 (20) 10 (10) 0 (0)
Diarrhea 47 (48) 9 (9) 35 (35) 5 (5)
Nausea 35 (36) 1 (1) 47 (47) 0 (0)
Asthenia 27 (28) 6 (6) 19 (19) 4 (4)
Vomiting 24 (25) 1 (1) 17 (17) 0 (0)
Alopecia 23 (24) 0 (0) 6 (6) 0 (0)
Rash 22 (23) 3 (3) 9 (9) 1 (1)
Mucosal inflammation 21 (22) 2 (2) 16 (16) 0 (0)
Stomatitis 21 (22) 5 (5) 4 (4) 1 (1)
Thrombocytopenia 18 (19) 4 (4) 24 (24) 4 (4)
Fatigue 18 (19) 3 (3) 18 (18) 2 (2)
Hypertension 18 (19) 4 (4) 5 (5) 1 (1)
Anemia 17 (18) 3 (3) 12 (12) 2 (2)
Decreased appetite 13 (13) 0 (0) 10 (10) 0 (0)
Dysgeusia 12 (12) 0 (0) 6 (6) 0 (0)
Erythema 11 (11) 2 (2) 4 (4) 0 (0)
*Peripheral neuropathy, peripheral sensory neuropathy, dysesthesia, neurotoxicity, paraesthesia
†Grade 3 is the most severe grade.
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Sorafenib and mFOLFOX6 for Metastatic Colorectal Cancer
29
Figure Legends
Figure 1. Patient disposition (January 31, 2011).
Figure 2. Survival outcomes by the Kaplan-Meier Method intent-to-treat patient
population: (A) progression-free survival (data cut-off January 31, 2011), and (B) overall
survival (data cut-off December 1, 2011).
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
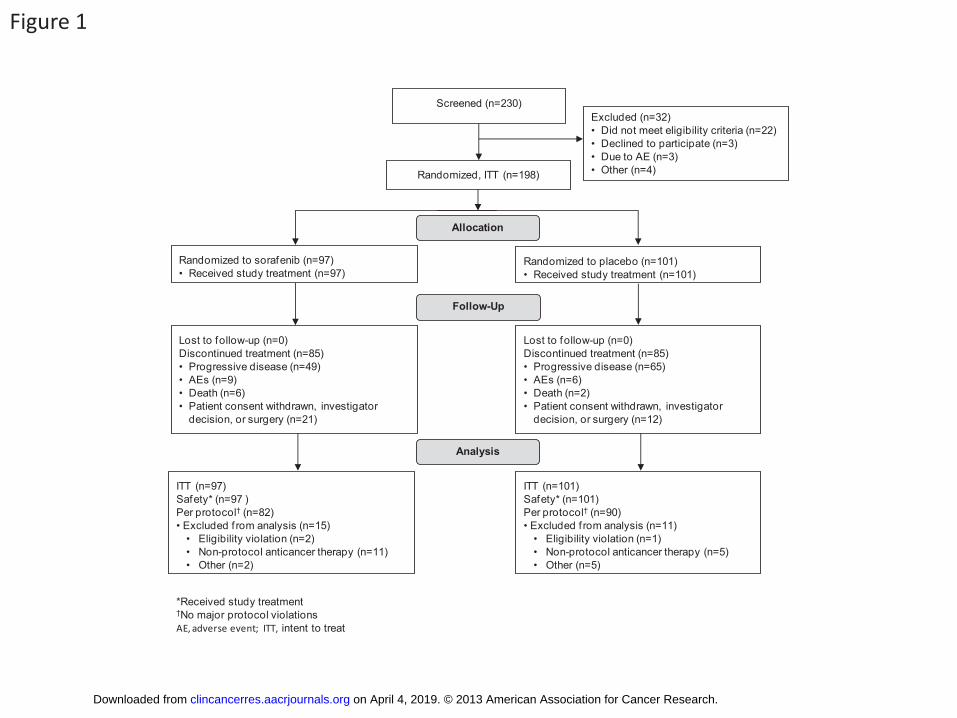
Figure 1
Analysis
ITT (n=101)
Safety* (n=101)
Per protocol† (n=90)
• Excluded f rom analysis (n=11)
• Eligibility violation (n=1)
• Non-protocol anticancer therapy (n=5)
• Other (n=5)
ITT (n=97)
Safety* (n=97 )
Per protocol† (n=82)
• Excluded f rom analysis (n=15)
• Eligibility violation (n=2)
• Non-protocol anticancer therapy (n=11)
• Other (n=2)
Lost to follow-up (n=0)
Discontinued treatment (n=85)
• Progressive disease (n=49)
• AEs (n=9)
• Death (n=6)
• Patient consent withdrawn, investigator
decision, or surgery (n=21)
Lost to follow-up (n=0)
Discontinued treatment (n=85)
• Progressive disease (n=65)
• AEs (n=6)
• Death (n=2)
• Patient consent withdrawn, investigator
decision, or surgery (n=12)
Randomized, ITT (n=198)
Follow-Up
Allocation
Randomized to placebo (n=101)
• Received study treatment (n=101)
Randomized to sorafenib (n=97)
• Received study treatment (n=97)
Screened (n=230)
Excluded (n=32)
• Did not meet eligibility criteria (n=22)
• Declined to participate (n=3)
• Due to AE (n=3)
• Other (n=4)
*Received study treatment†No major protocol violations
AE, adverse event; ITT, intent to treat
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
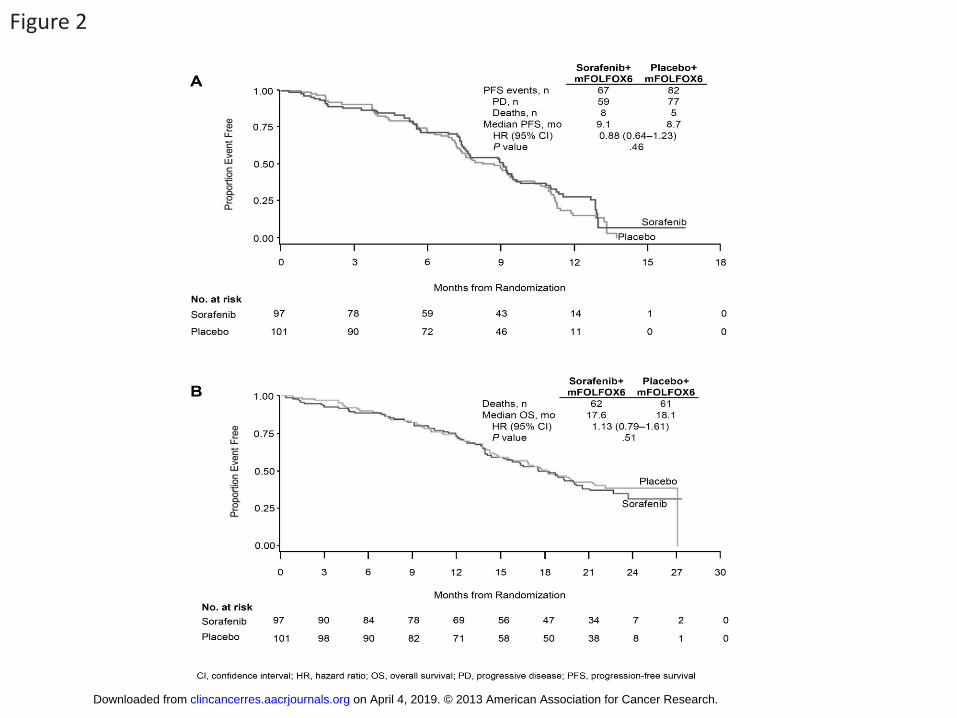
Figure 2
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107
Published OnlineFirst March 26, 2013.Clin Cancer Res Josep Tabernero, Rocio Garcia-Carbonero, James Cassidy, et al. Metastatic Colorectal Cancer: The RESPECT TrialFluorouracil (modified FOLFOX6) as First-line Treatment of Sorafenib in Combination with Oxaliplatin, Leucovorin, and
Updated version
10.1158/1078-0432.CCR-13-0107doi:
Access the most recent version of this article at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2013/03/23/1078-0432.CCR-13-0107To request permission to re-use all or part of this article, use this link
on April 4, 2019. © 2013 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on March 26, 2013; DOI: 10.1158/1078-0432.CCR-13-0107