stakeholders’ knowledge in obstetric complications...
TRANSCRIPT
Working Paper No. 18
Stakeholders’ Knowledge in Obstetric Complications and Role of Health
Providers in Accessing Emergency Obstetric care: Experiences from
Nilphamari District
Morsheda Banu Hashima-E-Nasreen
Sarawat Rashid
February 2011
Research and Evaluation Division, BRAC, 75 Mohakhali, Dhaka 1212, Bangladesh Telephone: (88-02) 9881265-72, 8824180-7 (PABX) Fax: (88-02) 8823542 E-mail: [email protected], Website: www.brac.net/research

Working Paper No. 18 Copyright © 2011 BRAC February 2011 Published by: BRAC 75 Mohakhali Dhaka 1212 Bangladesh Telephone: (88-02) 9881265-72, 8824180-7 (PABX) Fax: (88-02) 8823542 Website: www.brac.net/research Printing and Publication Altamas Pasha Cover design Md. Abdur Razzaque Design and layout Md. Akram Hossain BRAC/RED publishes research reports, scientific papers, monographs, working papers, research compendium in Bangla (Nirjash), proceedings, manuals, and other publications on subjects relating to poverty, social development and human rights, health and nutrition, education, gender, environment, and governance. Printed by BRAC Printers at Tongi, Gazipur, Bangladesh.

iiiMNCH intervention in obstetric emergencies
Acknowledgements We are grateful to BRAC for giving us the opportunity to conduct this study. BRAC is supported by countries, donor agencies and others who have the mission to work with people whose lives are dominated by extreme poverty, illiteracy, disease and other disadvantages. We are grateful to the participants for giving us time and cooperation in exploring BRAC emergency obstetric care service in rural areas of Bangladesh. The cooperation of BRAC health providers was also instrumental. The support of Dr. Imran Matin, deputy executive director, BRAC International, is also gratefully acknowledged. Dr. Syed Masud Ahmed, senior research coordinator, Research and Evaluation Division, BRAC, and Dr. Shamsun Nahar, consultant, BRAC and Dr. Fazlul Karim, research coordinator, BRAC are thankfully acknowledged for reviewing the paper. Thanks are also due to Mr. Hasan Shareef Ahmed, chief, editing and publication for editing the manuscript. The Research and Evaluation Division (RED) is supported by BRAC's core funds and funds from donor agencies, organizations and governments worldwide. Current major donors of BRAC and RED include AED ARTS (USA), Aga Khan Foundation Canada, AIDA (Spain), AusAID (Australia), Bill and Melinda Gates Foundation (USA), BRAC-USA, Campaign for Popular Education (Bangladesh), Canadian International Development Agency, Department for International Development (UK), DIMAGI (USA), EKN (The Netherlands), Emory University (USA), European Commission, Family Health International (USA), Fidelis, France, Government of Bangladesh, GTZ (Germany), Hospital for Sick Children (Canada), ICDDR,B (Bangladesh), Institute of Development Studies (UK), Inter-cooperation Bangladesh, Karolinska University (Sweden), Land O Lakes (USA), Manusher Jonno Foundation (Bangladesh), Micronutrient Initiative (Canada), NORAD (Norway), OXFAM NOVIB (The Netherlands), Oxford University (UK), Plan International Bangladesh, Rockefeller Foundation (USA), Rotary International (Bangladesh), Save the Children (UK), Save the Children (USA), Scojo Foundation Incorporation (USA), Stanford University (USA), Swiss Development Cooperation (Switzerland), The Global Fund (USA), The Population Council (USA), UNICEF, University of Leeds (UK), World Bank and World Food Programme.
iv RED Working Paper No. 18
Abbreviations
AMDD Averting Maternal Death and Disability ANC Antenatal Care APH Antepartum Haemorrhage BHC BRAC Health Centre DH District Hospital EmOC Emergency Obstetric Care FGD Focus Group Discussion MCWC Mother and Child Welfare Centre MNCH Maternal, Neonatal and Child Health MBBS Bachelor of Medicine and Bachelor of Surgery NHW Newborn Health worker OT Operation Theatre PO Programme Organizer PPH Postpartum Haemorrhage RpMCH Rangpur Medical College Hospital SS Shasthya Shebika SK Shasthya Kormi TBA Traditional Birth Attendant UHC Upazila Health Complex UNICEF United Nations Children’s Fund WHO World Health Organization

vMNCH intervention in obstetric emergencies
Abstract This study aimed to explore the stakeholders’ knowledge in obstetric complications, role of MNCH intervention in accessing Emergency Obstetric Care (EmOC) and factors associated with delays. A community-based qualitative study carried out during May–June 2007 among 42 obstetrically complicated women and 18 community health workers (CHW) in three upazilas of Nilphamari district. The findings reveal that a substantial proportion of women pointed out at least three obstetric complications but family members’ knowledge found inadequate, whereas the level of knowledge among CHWs found average. CHWs referred 36 women and assisted in accessing EmOC in the facility. Nineteen respondents delayed in deciding to seek care for financial constraints, informal treatment, failure to recognize the complication, absence of household head, and lack of emergency preparedness. Gender role found important in decision-making. Eleven women got delayed treatment at facility level due to lack of doctors trained in EmOC, operation facility, blood bank and poor performance of pathology and non-functional transport. The programme should give emphasis on educating pregnant women and their family members especially husbands. Capacity development of newborn health workers in assessing the severity of illness, appropriate referring, and making linkage with local transport facility to transfer patients during obstetric complications is needed.
viiMNCH intervention in obstetric emergencies
Executive summary Introduction
The rural maternal, neonatal and child health (MNCH) project was launched in late 2005 in Nilphamari district to provide health services to the poor and disadvantaged women and children. This study aimed to explore the stakeholders’ knowledge on obstetric complications, role of MNCH intervention in accessing emergency obstetric care (EmOC) and factors associated with delays. Methods
A community-based study was during May-June 2007 among obstetrically complicated women in three upazilas of Nilphamari district using qualitative methods. Forty-two referred cases for obstetric complications were identified from MNCH office registers for in-depth interviews. One focus group discussion (FGD) was conducted with family members and informal discussion with 18 community health providers. Analysis was completed thematically. Key findings
Our study reveals that a substantial proportion of women pointed out at least three pregnancy warning signs but family members’ knowledge on complication of pregnancy, childbirth, and postpartum period found inadequate. Level of knowledge regarding maternal complications among community health workers (CHW) found average. This study shows that the use of communication technology, such as cell phones, helps in communicating referral linkages. Indeed, CHWs of BRAC found to improve referral system using the cell phone and women used it for informing CHWs about the complications. At community and facility CHWs played important role in facilitating the access of EmOC; around 36 women were referred by them and were assisted in accessing EmOC in the facility. This study reveals that 19 respondents delayed in deciding to seek care due to multiple reasons like – financial constraints, tried at home with traditional and informal treatment, absence of household head, and lack of emergency preparedness. This study shows few of the respondents made delay in complication recognition. Gender and family members’ role in decision-making considered having a significant influence on delay during the course of illness and husbands was the prime decision-maker.

viii RED Working Paper No. 18
Distance and lack of free government transport are other key factors. Most of the government hospitals both at upazila and district levels had no functional ambulances. In our study, 11 women got delayed treatment at facility level due to lack of operation facility, blood bank and EmOC trained doctors, poor performance of pathology and non-functional transport. These put women in threat of death during obstetric emergency. Conclusion and recommendations
Although the knowledge on warning signs of obstetric complications is raising among women but there is still space to give more emphasis on educating pregnant women and their family members especially husband. Indeed family members are very important in providing support during emergency. By upgrading existing basic EmOC facilities many obstetric complications can be resolved and doctors should get EmOC training. Community people felt that BRAC should provide facility for comprehensive EmOC service for rural people. Health facilities are widely scattered in rural setting, programme should make linkage with local transport facility to transfer women during obstetric complications. Proper monitoring of health providers’ activities is needed. Emphasis should be given on capacity development of NHWs regarding obstetric complications, assessment of the seriousness of illness and appropriate referring to higher facility.
1MNCH intervention in obstetric emergencies
Introduction
Each year over 500,000 women die from pregnancy and childbirth-related causes, 95% being in Asia and Africa (WHO 2005a, WHO 2005b). World Health Organization (WHO) estimated that 15% of the pregnancies develop life threatening complications such as haemorrhage, eclampsia, sepsis, unsafe abortion and obstructed labour (Nasreen et al. 2006, Islam et al. 2005, Ali et al. 2005) which are unpredictable and require special care (Ali et al. 2005, Islam et al. 2005). The majority of maternal deaths can be prevented by recognition of obstetric complications, and instigation of appropriate emergency referral procedures including efficient and well-equipped transport facilities, and by promoting timely and adequate care (Parkhurst and Rahman 2007, Murray and Pearson 2006, Josiah et al. 1998). A joint collaboration between the government of Bangladesh, UNICEF and the Averting Maternal Death and Disability (AMDD) Programme started strengthening 59 district hospitals, 120 upazila health complexes (UHC) in 1993 to provide 24-hour comprehensive emergency obstetric care (EmOC) services (Islam et al. 2005). Universally, EmOC has broadly been categorized into two groups – basic and comprehensive – based on the performance of certain signal functions (Table 1) (Paxton et al. 2006, Nasreen et al. 2007, UNICEF 1997). But at community level, barriers in seeking EmOC services in maternal complications are delay in making decision to seek care, delay in arrival at a health facility, and delay in receiving adequate treatment (Killewo et al. 2006) Table 1. EmOC functions at facility level
Basic EmOC Comprehensive EmOC Parenteral antibiotics Parenteral oxitocic drugs Parenteral anticonvulsants Manual removal of placenta Removal of retained product of placenta Assisted vaginal delivery
All basic EmOC &
Cesarean section Blood transfusion
Source: Nasreen HE et al. 2007, UNICEF 1997 Maternal, neonatal and child health project
Through its essential healthcare programme, BRAC has been delivering basic package of health services since 1991 and in 1995 it opened BRAC health centres (BHC) to offer curative care. Few upgraded BHCs providing comprehensive EmOC and minor surgical intervention since 2001 (BRAC 2007). Bringing health services to poor and disadvantaged women and children rural maternal, neonatal and child health (MNCH) project was launched in late 2005 in Nilphamari district.

2 RED Working Paper No. 18
The project focused on competency development of community health workers (CHWs) for offering health services, the empower community, timely refer to quality health facilities, and develop linkages with government, local government, community members and NGOs. Shasthya shebikas (SS), the front line female health volunteers, identifies all suspected pregnancies through regular house hold visits which the shasthya kormis (SK) confirm, provide monthly antenatal check-up which includes measurement of blood pressure; checking of foetal position, anaemia, jaundice and oedema; and provides messages on diet, rest, pregnancy danger signs, etc. and women receive delivery kits, iron-folic acid tablets from SS. During the third trimester, the programme organizers (PO) visit and discuss about birth plan and birth preparedness. The BRAC-trained newborn health worker (NHW) assists with delivery and offers newborn care whereas, SS offers Misoprostol tablets to prevent postpartum haemorrhage. In case of complications, Figure 1 shows SS, NHW or family members contact the referral PO who arranges referral for women to appropriate facility. One referral PO is employed at upazila level and two referral POs are employed at tertiary level facility to facilitate women with obstetric complications in getting treatment (BRAC 2007). Figure 1. Referral system of MNCH project
This study investigated how MNCH intervention and referral network performs in managing maternal complications in rural areas of Nilphamari district. This study aimed to explore the stakeholders’ knowledge on obstetric complications, role of MNCH intervention in accessing EmOC and factors associated with delays.
CHWs involved in referral Levels of referral facility
Medical college hospital
Obstetric complications
PO
SS SK NHW
Tertiary facility
Secondary facility
Primary facility
District hospital
From community
Upazila health complex
3MNCH intervention in obstetric emergencies
Materials and methods
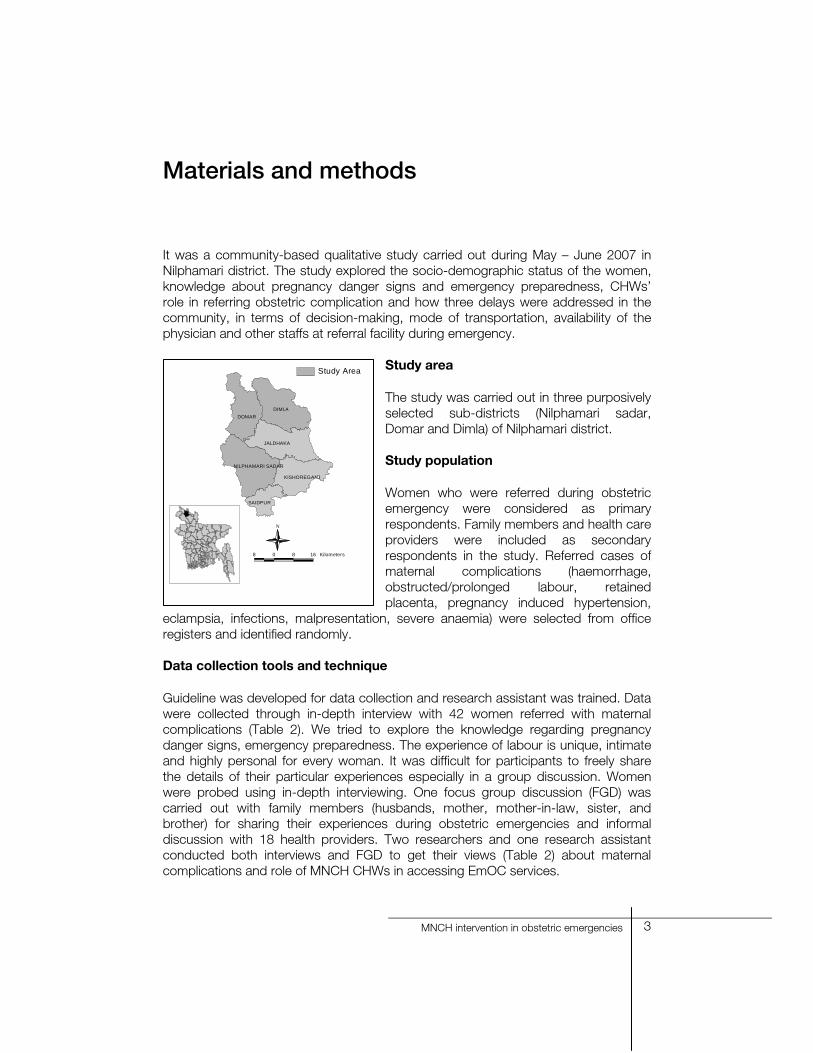
It was a community-based qualitative study carried out during May – June 2007 in Nilphamari district. The study explored the socio-demographic status of the women, knowledge about pregnancy danger signs and emergency preparedness, CHWs’ role in referring obstetric complication and how three delays were addressed in the community, in terms of decision-making, mode of transportation, availability of the physician and other staffs at referral facility during emergency.
Study area
The study was carried out in three purposively selected sub-districts (Nilphamari sadar, Domar and Dimla) of Nilphamari district. Study population
Women who were referred during obstetric emergency were considered as primary respondents. Family members and health care providers were included as secondary respondents in the study. Referred cases of maternal complications (haemorrhage, obstructed/prolonged labour, retained placenta, pregnancy induced hypertension,
eclampsia, infections, malpresentation, severe anaemia) were selected from office registers and identified randomly. Data collection tools and technique
Guideline was developed for data collection and research assistant was trained. Data were collected through in-depth interview with 42 women referred with maternal complications (Table 2). We tried to explore the knowledge regarding pregnancy danger signs, emergency preparedness. The experience of labour is unique, intimate and highly personal for every woman. It was difficult for participants to freely share the details of their particular experiences especially in a group discussion. Women were probed using in-depth interviewing. One focus group discussion (FGD) was carried out with family members (husbands, mother, mother-in-law, sister, and brother) for sharing their experiences during obstetric emergencies and informal discussion with 18 health providers. Two researchers and one research assistant conducted both interviews and FGD to get their views (Table 2) about maternal complications and role of MNCH CHWs in accessing EmOC services.
DIMLADOMAR
JALDHAKA
NILPHAMARI SADAR
KISHOREGANJ
SAIDPUR
Study Area
8 0 8 16 Kilometers
N

4 RED Working Paper No. 18
Table 2. Data collection methods and respondents
Type of respondents
Area Methods No. of
respondents Women referred for obstetric complication
Community In-depth interview
42
Health providers (SS, SK, NHW, PO)
Community Informal discussion
18
Family members Community FGD 8 Data analysis
We attempted to identify common responses of the women, and to elaborate the qualitative features from their narratives. Bangla versions of narratives were translated into English by researchers and meticulously verified. The documented descriptions were reviewed and coded to identify the sub-categories, categories and themes.
5MNCH intervention in obstetric emergencies
Results
Socio demographic characteristics
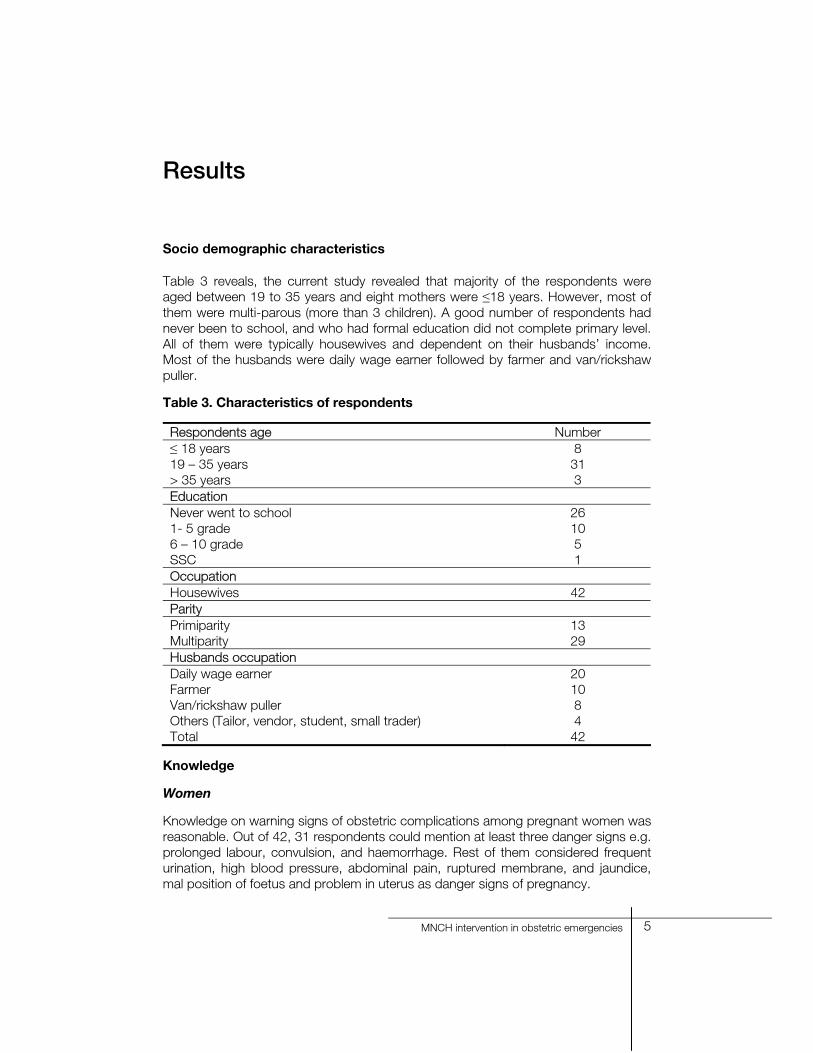
Table 3 reveals, the current study revealed that majority of the respondents were aged between 19 to 35 years and eight mothers were ≤18 years. However, most of them were multi-parous (more than 3 children). A good number of respondents had never been to school, and who had formal education did not complete primary level. All of them were typically housewives and dependent on their husbands’ income. Most of the husbands were daily wage earner followed by farmer and van/rickshaw puller.
Table 3. Characteristics of respondents
Respondents age Number ≤ 18 years 8 19 – 35 years 31 > 35 years 3 Education Never went to school 26 1- 5 grade 10 6 – 10 grade 5 SSC 1 Occupation Housewives 42 Parity Primiparity 13 Multiparity 29 Husbands occupation Daily wage earner 20 Farmer 10 Van/rickshaw puller 8 Others (Tailor, vendor, student, small trader) 4 Total 42
Knowledge
Women
Knowledge on warning signs of obstetric complications among pregnant women was reasonable. Out of 42, 31 respondents could mention at least three danger signs e.g. prolonged labour, convulsion, and haemorrhage. Rest of them considered frequent urination, high blood pressure, abdominal pain, ruptured membrane, and jaundice, mal position of foetus and problem in uterus as danger signs of pregnancy.
6 RED Working Paper No. 18
Findings reveal that the women who went school were more conscious about themselves and they followed the advices.
Rina (20) was a school graduate and said, “I experienced pain in abdomen and headache at five months of my pregnancy…informed BRAC apa…she said that I had high blood pressure and should visit a medical doctor…later I visited a local MBBS doctor and my father took me to Rangpur Medical College Hospital for better treatment. I took adequate rest, food and avoided heavy work as recommended. Soon after I felt labour pain at term, went hospital and the baby was born normally.”
Family members
More than half of the husbands could mention at least one of the danger signs which needs medical intervention. “I knew few as BRAC apa visited my wife and hanged a poster with those pictures” – said a husband. Other husbands and family members were not very clear about danger signs. “Health workers visited my daughter-in-law but they did not talk with me. I do not know what I should do during complications and how long it can be waited at home” – a mother in law said. Brother of a deceased mother said, – “Elder members of family were making different decisions…Some said we can wait more than 12 hours…we should go hospital after 2 to 3 days, my sister died in postpartum bleeding with retained placenta because of our lack of knowledge, we knew those things after her death.” Community health providers
SKs considered short stature (below 145 cm) pregnant women, aged below 18 or above 35 years, high blood pressure, haemorrhage, severe headache, fever, oedema of hand and foot, convulsion, previous history of still birth or caesarean section, multi parity (4th or more pregnancy), diseased as danger signs of pregnancy. They also stated that at intra-partum period pregnant women might suffer labour pain more than 12 hours, any foetal part or cord comes before head, haemorrhage, and ruptured membrane and after delivery retained placenta and haemorrhage considered as obstetric complications. Shasthya shebikas and trained NHWs could mention at least three and referral PO could say less than four pregnancy danger signs. Role of MNCH health providers in accessing EmOC services
BRAC established referral linkages with upazila health complex (UHC) at primary level followed by district hospital (DC) in secondary level and all unmanageable maternal complications were referred to tertiary health facility. Thirty-six maternal complications were identified by SKs, SSs and NHWs at community. They communicated with PO using cell phone and referred women to UHCs and DHs. A SS stated, “Most of the times we arrange transport to send the patient to hospitals”. Twenty-six respondents were assisted by CHWs in arranging transport in

7MNCH intervention in obstetric emergencies
accessing EmOC. A husband in Nilphamari said, “I tried to manage a rickshaw van when my wife started bleeding after delivery. Van pullers refused to take such a woman who had gave birth currently, and said, after delivery women become unholy and her touch will be dangerous for his van. After a long hour when I failed to arrange the local, MNCH PO brought a transport for her.” However, six women were referred by family members and PO identified them at hospitals and referred them to tertiary facilities for better management. At facility PO played important role in facilitating treatment; helped getting admitted, communicated with clinicians and arranged blood. Moreover, renting transport with payment for sending women to distant facility and bought medicine for very poor patients were their responsibilities. Gitali said, “when I experienced bleeding in pregnancy my husband informed the PO just after he recognized the symptoms. The PO managed everything for receiving treatment from a medical college hospital otherwise it was not possible to save my life.” Five respondents were reported that referral POs managed blood from some volunteer blood donors and from blood bank during emergencies. Findings showed that 37 women were saved, 11 of them were managed at tertiary level, eight at DH hospital, and six at UHC, five at different clinics and MCWC and one at updated Shushasthya. Complications were commonly prolonged or obstructed labour followed by haemorrhage, pre-eclampsia or eclampsia, infection, and retained placenta. Life threatening complications like eclampsia, haemorrhage or cardiac disease aggravated by pregnancy ended up with four maternal deaths. Factors affected in accessing EmOC services
Delay at household level
We found 19 respondents delayed in deciding to seek care due to multiple reasons like – financial constraints, tried at home with traditional and informal treatment, absence of household head, failed to recognize the seriousness of the illness and lack of emergency preparedness. Most common was financial problem. Generally they were poor and had no savings. Mahmuda’s mother expressed, “Hospital treatment is so expensive for us.” Thirty years old Mahmuda’s husband took her to UHC when she developed eclampsia. Doctor started medication and referred her to Rangpur medical college hospital (RpMCH) at night. The family delayed for 16 hours in managing money and ultimately she died at RpMCH within few hours after admission. A trained TBA said, “Rural people did not try to understand the severity of the complications, always requested for home management in traditional way to avoid going hospital as it is expensive.” Failed to recognize the severity of illness
Findings reveal the gaps in recognizing fatal condition. Family members as well as healthcare providers usually made delay as they could not assess the disease severity. Fatal complications like eclampsia, postpartum haemorrhage (PPH), retained placenta with haemorrhage, hepatitis in pregnancy and pre-existing cardiac disease
8 RED Working Paper No. 18
were delayed concern by them. When they realized the condition it was too late to save them. Two maternal deaths occurred at RpMCH, one at DH and another one died on the way to third referral facility. Merina (26) died during her third delivery due to retained placenta with PPH…the trained traditional birth attendant (TBA) tried for placenta delivery for two hours, she applied several strategies, fastened her lower abdomen with a cloth and cord tied with Merina’s thigh. However, she failed to stop bleeding and placental delivery. When she advised Merina’s family members to transfer her to a hospital then it was too late. “TBA did not tell us that it was a life threatening condition and we should transfer Merina immediately to hospital” – said Merina’s brother. Role of decision-maker in the family Husbands played important role in making decision to seek care. “My husband did not pay much attention when bleeding started at night during nine months of my pregnancy. He advised me to lie down as bleeding was more in standing position. He decided to seek care in the next morning. After changing three facilities I delivered an asphyxiated baby by caesarean section in the evening in a private clinic at Nilphamari after transfusing blood. It cost us Tk. 13,000 which was managed by loan,” said a patient of gestational hypertension with antepartum haemorrhage (APH). Women did not have right to decide where they should go and everything was depended on their husbands’ opinion during emergency. Resistance came from their in-law’s family members also. Strong believe and preference of traditional treatment Preference of traditional treatment was one of the major causes of delay in seeking medical care. They preferred TBA for normal delivery and traditional healer, ayurvedic and homeopathy for pregnancy with hepatitis, postpartum infection, and APH. Even in deadly condition like eclampsia a relative said, “We thought it was Dos doshi (evil spirit), so we used to expel that spirit by Kabiraj whole night when Naju developed convulsion during seventh month of her pregnancy.” Her husband got the news, took her at district hospital then to tertiary level of health facility but failed to save her life. Lack of emergency preparedness Despite having knowledge of emergency preparedness we found a single pre-arranged blood donor, seven respondents had cash, and none had pre-arranged transport. Most of the respondents (35) had no savings for the emergency. In response to our question about savings majority used to say, “We knew it but it was not possible to separate money from daily expenses….even earning food for two times is difficult for us.” Hardly Tk. 1,000 to 1,500 was saved by each of the seven women for delivery purpose. Geographical situation and lack of transport Six women delayed in accessing the transport and in reaching selected facilities during obstetric complications. Apart from of urban and rural setting, geographical

9MNCH intervention in obstetric emergencies
distance of any range may cause barriers in seeking medical care. Situation becomes more complicated during obstetric emergency. Distance and mode of transport is always interrelated with each others. The findings show that the respondents’ houses were situated at various distances like 3 to 18 kilometres from UHC and 18 to 75 km from tertiary facility. Most hospitals have no ambulance to transfer the patient to a tertiary facility. The government has provided ambulances to government hospital like UHC, DH, but patient could never utilized the facility as most of the time it remained out of service. Similarly, private clinic and BRAC health centre also have no distant transport facility. Patients’ attendants had to rent expensive private transport to transfer the patient during her life threatening obstetric complication. Indeed, delay had been made in taking decision for the expense or arranging money for renting distant transport. Thus patients died on the way, they were too ill to be helped when they arrived at tertiary facility.
Merina’s husband took her to UHC by van… medical officer compelled to refer her to tertiary facility… health complex ambulance service was not available…BRAC referral PO rented a micro-bus and sent her… her home was 3 km away from UHC and Rangpur is 75 km away…whatever the transport was, Merina died on the way of Rangpur. (A case of retained placenta with PPH)
Delay at facility level
The current study revealed that there was no obstetrician, ill equipped labour room and non functional operation theater in UHC and at DH manpower was insufficient there. Findings depicted that 11 referred women with obstetric complications got delayed management at facility level due to lack of hospital logistics. Comprehensive EmOC services were not provided after 2.00 p.m. as obstetrician remained unavailable in DH. A mother said, “Nurse delivered a baby who did not cry and when bleeding started she referred me to tertiary facility as there was no doctor.” “District hospital was the worst place she ever visited and hopes Allah will not wish to go there again.” Marufa said, “In DH nurse gave a visit one hour after my admission though my mother-in-law called them three to four times.” BRAC Shushasthya had on call obstetrician for providing comprehensive EmOC services after the office hour and private clinic was found unaffordable for poor. At primary and secondary level there was no blood bank, pathologies were poorly functioned and duty nurse performed normal deliveries. Delay was made in managing blood, and referral POs used to collect blood from some volunteer college students. Patient’s attendants have had a conception on donating blood; they thought close relative can donate blood whenever they need irrespective of blood group and this was the main cause of delay occurred in starting treatment.

10 RED Working Paper No. 18
Discussions
Women’s knowledge regarding obstetric complication during pregnancy and child birth is diverse. Majority of women reported at least one specific maternal complication in Bangladesh maternal health services and maternal mortality survey 2001 and significant minority could name three or more (NIPORT, ORC Macro, John Hopkins University, ICDDR,B 2003, Koenig et al. 2007). The first step in improving national maternity healthcare is to identify women’s knowledge level on warning signs and try to improve it. Our study reveals that a substantial proportion of women pointed out at least three pregnancy warning signs but family members’ knowledge on complication of pregnancy, childbirth, and postpartum period found inadequate. Similar findings were reported in Nigeria (Odimengwu et al. 2005). Level of knowledge regarding maternal complications among community health workers found average but there is still room for improvement by regular training, similar findings were discussed in another study in Bangladesh (Nasreen et al. 2006). Experiences in Uganda, Malawi, Kenya, Sierra Leone and Ghana showed that the use of communication technology, such as cell phones, helps in communicating referral linkages and increase the number of referrals (Islam et al. 2005, Krasovec 2004). Indeed, CHWs of BRAC also found to improve referral system using the cell phone and women used it for informing CHWs about the complications. At community and facility CHWs played important role in facilitating the access of EmOC; around 36 women were referred by them and were helped in accessing EmOC in the facility. Findings from a study stated that community health provider’s assistance in accessing EmOC significantly reduces delays in taking decision and reaching facility (Banu et al. 2010). Studies in India and Nepal examined that project intervention and safe motherhood programme effort on EmOC services declined the case fatality rate in obstetric emergencies (De Costa et al. 2009, Rana et al. 2009). This study reveals that respondents made delay in deciding to seek care mainly due to financial constraints followed by multiple reasons like – tried at home with traditional and informal treatment, absence of household head, and lack of emergency preparedness. Other studies in Gambia, Bangladesh reported similar findings (NIPORT, ORC Macro, John Hopkins University, ICDDR,B 2003, Cham et al. 2005, Killewo et al. 2006, Gill et al. 2004). In Bangladesh maternal health services and maternal mortality survey 2001, majority of women delayed in decision making to seek care due to late recognition of complication (NIPORT, ORC Macro, John Hopkins University, ICDDR,B 2003). This study shows few of the respondents made delay in complication recognition. It indicates that majority community health providers had the ability to judge the severity of obstetric complications while they were informed. Intervention should emphasize on educating the community people on obstetric danger signs and emergency preparedness so that they can transfer women promptly to appropriate facilities.
11MNCH intervention in obstetric emergencies
Gender and family members’ role in decision-making considered having a significant influence on delay during the course of illness (APHRC 2006, Afsana et al. 2000). Other studies show that in most of the cases husband was the prime decision-maker (Odimegwu et al. 2005, Banu et al. 2010). The present study reflected the same image. Distance and lack of free government transport are other key factors. A study found that most hospitals in the study districts of Pakistan have no functional ambulances (Ali et al. 2005). In this study we observed similar situation in our government hospitals both at upazila and district levels. In our study, 11 women got delayed treatment at facility level due to lack of operation facility, blood bank and EmOC trained doctors, poor performance of pathology and non-functional transport. These put women in threat of death during obstetric emergency. Several studies reveal the similar findings (Ali et al. 2005, Killewo et al. 2006, Nasreen et al. 2006, Ganatra et al. 1998).

12 RED Working Paper No. 18
Conclusion and recommendations
Although the knowledge on warning signs regarding maternal complications is raising among women there is still space to give more emphasis on educating pregnant women and their family members especially husband. Indeed, family members are important in providing support during emergency. Community people felt that BRAC should provide facility for comprehensive EmOC service to rural people. Health facilities are widely scattered in rural setting. The programme should make linkage with local transport facility to transfer women during obstetric complications. By upgrading existing basic EmOC facilities many obstetric complications can be resolved and doctors should get training on EmOC. Proper monitoring of health providers’ activities is needed. Emphasis should be given on capacity development of the community health workers regarding obstetric complications, assessment of the seriousness of illness, and appropriate referring to higher facility.
13MNCH intervention in obstetric emergencies
References
Afsana K, Rashid AF (2000). Discoursing birthing care; experiences from Bangladesh. Dhaka: The University Press Limited. 128p.
Ali M, Hotta M, Kuroiwa C, Ushijima H (2005). Emergency obstetric care in Pakistan: potential for reduced maternal mortality through improved basic EmOC facilities, services, and access. Int J Gynaecol Obstet 91:105-12.
African Population and Health Research Centre (APHRC) and the World Bank (2006). Averting preventable maternal mortality: delays and barrier to the utilization of emergency obstetric care in Nairobi’s informal settlements. Nairobi, Kenya: APHRC and the World Bank.
Banu M, Nahar S, Nasreen HE (2010). Addressing the MANOSHI referral system: addressing delays in seeking emergency obstetric care in Dhaka’s slums. Dhaka: ICDDR,B. (MANOSHI Working paper No. 10)
BRAC. BRAC Annual report (2007). Dhaka: BRAC.
Cham M, Sundby J, Vangen S (2005). Maternal mortality in the rural Gambia, a qualitative study on access to emergency obstetric care. Reprod Health 2:3 doi:10.1186/1742-4755-2-3.
De Costa AD, Patil R, Kushwah SS, Diwan VK (2009). Financial incentives to influence maternal mortality in a low-income setting: making available ‘money to transport’- experiences from Amarpatan, India. Global Health Action doi:10.3402/gha.v2i0.1866.
Gill Z, Ahmed JU (2004). Averting maternal death and disability; experience from Bangladesh: implementing emergency obstetric care as a part of the reproductive health agenda. Int J Gynaecol Obstet 85:213-20.
Ganatra BR, Coyaji KJ, Rao VN (1998). Too far, too little, too late: a community-based case-control study of maternal mortality in rural west Maharashtra, India. Bull WHO 75(6):591-8.
Islam MT, Hossain MM, Islam MA, Haque YA (2005). Improvement of coverage and utilization of EmOC services in southwestern Bangladesh. Int J Gynaecol Obstet 91:298-305.
Josiah DB, Myntti C, Augustin A (1998). The “three delays” as a framework for examining maternal mortality in Haiti. Soc Sci Med 46(8):981-93.
Koenig MA, Jamil K, Streatfield PK, Saha T, Sabir AA, Arifeen SE et al. (2007). Maternal health and care-seeking behaviour in Bangladesh: findings from a national survey. Int Fam Plann Pers 33(2):75-82.

14 RED Working Paper No. 18
Killewo J, Anwar I, Bashir I, Yunus M, Chakraborty J (2006). Perceived delay in healthcare-seeking for episodes of serious illness and its implications for safe motherhood interventions in rural Bangladesh. J Health Popul Nutr 24(4):403-12.
Krasovec K (2004). Auxiliary technologies related to transport and communication for obstetric emergencies. Int J Gynaecol Obstet 85(1):14-23.
Murray SF and Pearson SC (2006). Maternity referral systems in developing countries: current knowledge and future research needs. Soc Sci Med 62(9):2205-15.
National Institute of Population Research and Training (NIPORT), ORC Macro, Johns Hopkins University and ICDDR,B (2003). Bangladesh maternal health services and maternal mortality survey 2001. Dhaka and Maryland: NIPORT, ORC Macro, Johns Hopkins University and ICDDR,B.
Nasreen HE, Imam N, Akter R, Ahmed SM (2006). Safe Motherhood Promotion Project in Narsingdi District: Baseline Survey. Dhaka: BRAC.
Nasreen HE, Ahmed SM, Begum HA, Afsana K (2007). Maternal, Neonatal and Child Health Programes in Bangladesh; review of good practices and lessons learned. Research Monograph Series No 32 July. Dhaka.
Odimegwu C, Adewuyi A, Obediyi T, Aina B, Adesina Y, Olatubara O et al. (2005). Men’s role in emergency obstetric care in Osun State of Nigeria. Afr J Reprod Health 9(3):59-71.
Paxton A, Bailey P, Lobis S, Fry D (2006). Global patterns in availability of emergency obstetric care. Int J Gynaecol Obstet 93:300-07.
Parkhurst JO and Rahman SA (2007). Non-professional health practitioners and referrals to facilities: lessons from maternal care in Bangladesh. Health Policy Plann 22:149-55.
Rana TG, Chataut BD, Shakya G, Nanda G, Pratt A, Sakai S (2009). Strengthening emergency obstetric care in Nepal: the Women’s Right to Life and Health Project (WRLHP). Int J Gynaecol Obstet 98(3):271–7.
UNICEF (1997). Guidelines for monitoring the availability and use of obstetric services. New York: United Nations Children’s Fund. 110p.
WHO (2005)a. Health and the millennium development goals. Geneva: World Health Organization.
WHO (2005)b. The world health report 2005: make every mother and child count. Geneva: World Health Organization.