summer 2014 › portals › 5 › files › journal › summer...all your patient payment needs in...
TRANSCRIPT

Summer 2014
The Dangers of Agreeing To An Independent Review Organization Requirement In Hospital Services Agreements
Public Private Speaking Tips
How the Revenue Cycle Professional Can Develop the Mindset of a Champion
Will Your Next Four Quarters Equal A Dollar?
2014 AAHAM ANI Speakers & Schedule

All your patient paymentneeds in one place.
Introducing Salucro Healthcare Solutions, a trusted partner of
With Salucro’s payment processing solution, you will:
• Increase patient payments by more than 9%.1
• Save up to 20%1 using a simple flat-blended rate with no hidden charges.
• Reach more patients with Online Bill Pay.
• Tap into 140 million+ active PayPal consumers with billions in spending power.
Plus, you can receive funds while giving your patients more time to pay with Bill Me Later®, a PayPal service.2
See what you’ll save. Visit salucro.com/save or call 866-430-7333 to request your free Cost Benefit Analysis.
1 Payment volume increase and rate savings are derived from Salucro Healthcare Solutions. Claims are unaffiliated with industry partners.2 Bill Me Later®, a PayPal service, is subject to patient credit approval, as determined by the lender, Comenity Capital Bank.
© 2014 Salucro Healthcare Solutions, LLC. All rights reserved. Salucro and the Salucro logo are registered trademarks of Salucro Healthcare Solutions, LLC.PayPal and the PayPal logo are registered trademarks of PayPal, Inc. Designated trademarks and brands are the property of their respective owners.
Salucro Healthcare Solutions is making healthcare more profitable by helping providers simplify transactions and accept patient payments at every encounter.
Online Payments Patient Financing In-Person Payments
Your Healthcare System
Summer 2014 1
8 The Dangers of Agreeing To An Independent Review Organization Requirement In Hospital Services Agreements By Richard Lovich, Esquire
12 Public Private Speaking Tips By Sheryl Roush
14 How the Revenue Cycle Professional Can Develop the Mindset of a Champion: Proven Techniques to Skyrocket Your Performance, Especially During Challenging Times By Jack Singer, Ph.D
16 Will Your Next Four Quarters Equal A Dollar? By Rob Borchett and Don Borchett, BA and Tim Borchett, MBA, PMP
19 2014 AAHAM ANI Speakers & Schedule
32 Meet a Committee Chair: Doris Dickey, CRCE-I, CRCS Certification Chair
2 Letter from the Executive Director
4 Letter from the National President
6 Washington Wire By Paul A. Miller, PLC
34 From the Desk of the Certification Director By Maria LeDoux, CAE
36 CRCP Certification Corner By Brenda Chambers, CRCE-I,P
36 CRCS Certification Corner By Doris Dickey, CRCE-I
37 CRCE Certification Corner By Erin Selin, CRCE-I, CCT
38 From the Desk of the Membership Director By Moayad Zahralddin
44 Did You Know? By Moayad Zahralddin
45 National Calendar/The JHAM network
Inside front cover Salucro Healthcare Solutions www.salucro.com
12
19
8
16
table of contents
features
advertiser index
departments
AAHAM National Office Staff11240 Waples Mill Road, Suite 200, Fairfax, VA 22030
Executive Director Sharon R. Galler, CMP 703.281.4043, ext. 204 [email protected]
Membership Director Moayad Zahralddin 703.281.4043, ext. 202 [email protected]
Certification Director Maria LeDoux, CAE 703.281.4043, ext. 201 [email protected]
Finance Manager Christelle Isambo 703.281.4043, ext. 216 [email protected]
Certification Amanda Leibert Manager 703.281.4043, ext. 211 [email protected]
Manager of Danielle Burns Meetings & Events 703.281.4043, ext. 209 [email protected]
Art Direction Christopher R. Izzo & Graphic Design CRI Design 401.821.1849 [email protected]
AAHAM National Executive Officers President Victoria DiTomaso, CRCE-I System Director, CBO Lee Memorial Health System P O Box 150107 Cape Coral, FL 33915 239.242.6011 | 239.242.6005 [email protected]
Chair of the Board Christine Stottlemyer, CRCE-I Director Patient Accounting Memorial Hospital 325 S. Relmont Street York, PA 17403 717.849.5431 | 717.815.2474 [email protected]
First Vice President John Currier, CRCE-I Executive Director Revenue Cycle Management Gibson Area Hospital & Health Services 1120 N Melvin Street Gibson City, IL 60936 217.784.2613 | 217.784.5853 [email protected]
Second Vice President Lori Sickelbaugh, CRCE-I Director, Facilty Patient Access Wake Forest Baptist Medical Center Medical Center Boulevard Winston Salem, NC 27157 336.716.4053 | 336.713.4198 [email protected]
Treasurer Amy Mitchell, CRCE-I PFS, Business Services Director University of Utah Hospital 127 South 500 East #400 Salt Lake City, UT 84120 801.587.6486 | 801.587.6675 [email protected]
Secretary Linda Patry, CRCE-I Director, Patient Financial Services Mary Washington Healthcare 2300 Fall Hill Avenue Fredericksburg, VA 22401 540.741.1591 | 866.774.9287 [email protected]
Legal Counsel Richard Lovich, Esquire Stephenson, Acquisto, & Colman 303 North Glenoaks Blvd. #700 Burbank, CA 91502 818.559.4477 | 818.559.5484 [email protected]
letter from the executive director
Sharon R. Galler
2 The Journal of Healthcare Administrative Management
Welcome to our special pre-ANI issue, can you believe we are less than two months away? We are all busy planning and putting on the finishing touches to our
ANI, “Sail into Revenue Cycle Success,” October 15-17 in scenic San Diego, California, at the centrally located Manchester Grand Hyatt. We know funds are limited and have made the ANI as economical as possible. We include most of your meals and have a jam packed list of speakers and sessions. Earn your CEUs all at one place and all at one time. You will also meet exhibitors that offer you solutions to your at work challenges. We offer many fun networking opportunities to help you build integral relationships and give you the edge in today’s competitive economy and job force. This year the “nautical” theme will be everywhere and will add to the fun and excitement. Wear your favorite hat, deck shoes and seafaring attire to the banquet and get into the San Diego spirit!
We hope you find this issue of the Journal informative and timely. Our new legal counsel, Richard Lovich’s cover article about IRO’s is very thought provoking as well as the article by the Borchert family. ANI keynote speakers Sheryl Roush and Jack Singer both wrote interesting articles, be sure to attend their sessions at the ANI.
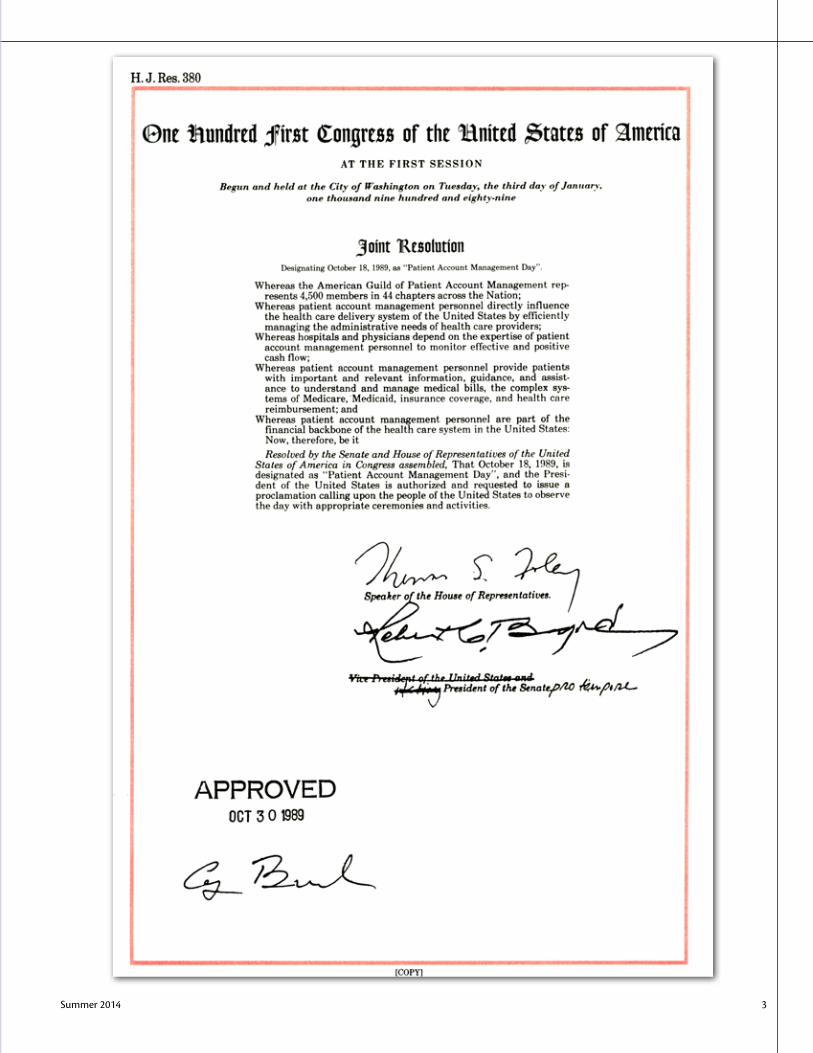
We frequently get asked why we hold Patient Account Management (PAM) Day when we do. Although other organizations celebrate it and may claim “ownership”, it was an AAHAM (then AGPAM) movement and actually proclaimed by Congress in 1989 to fall on October 18th of every year. We decided many years ago to celebrate it the entire week the 18th falls in. This year PAM Week is October 18-25, our theme is “Our Team Spirit is Key.” We will have many new gift items and new ideas to help you celebrate and recognize your department and staff.
Be sure to check out my blog on our website for some ANI tips, networking ideas and other news. A big AAHAM thank you to our advertisers, exhibitors and sponsors, we couldn’t do it without you!
Warm regards, Sharon
Summer 2014 3

letter from the national president
Deadlines & Submission GuidelinesThe Journal welcomes submissions from AAHAM
members. Submission deadlines are as follows: Journal Issue Submission Deadline Fall 2014 September 26, 2014
Send submissions to:Executive Director, AAHAM
11240 Waples Mill Road, Suite 200Fairfax, VA [email protected]
n Please send a copy of your submission on a CD or flash drive, or e-mail it to: [email protected].
n Leave a one-inch margin on the top, bottom, and sides.
n Use upper- and lower-case letters as you would in typing any correspondence.
n Indent the first line of each paragraph five spaces.
n Include a cover page with the following information: Author’s name, (degrees, certifications) Place of employment Position Address Phone/Fax number AAHAM Chapter Affiliation (if any)
n Any article submitted for reprint in the Journal must be accompanied by written permission to reproduce from the original source.
n Do not use abbreviations or italics.
n All photos become the property of AAHAM, unless you specifically request that they be returned. Each picture should be accompanied by a listing of all individuals in the picture (left to right). Black and white pictures reproduce better than color.
n All articles are subject to editing by AAHAM. AAHAM reserves the right to hold articles for future Journal issues when space is limited.
n Articles referring to or endorsing specific products or services will not be considered.
The Journal is published quarterly by the American Association of Healthcare Administrative Management, 11240 Waples Mill Road, Ste. 200, Fairfax, VA 22030. Opinions expressed in this publication represent the viewpoint of each author, and do not necessarily reflect the policy of AAHAM. Advertisements do not necessarily imply sponsorship by AAHAM. Subscriptions are included with AAHAM membership. Reprints are available from the National Office in portable document format (PDF) for a $75 fee per article. Prepayment is required.
© Copyright 2014 by the American Association ofHealthcare Administrative Management.
www.aaham.org
Victoria DiTomaso, CRCE-I
4 The Journal of Healthcare Administrative Management
“Summertime and the livin’ is easy…” Is it really already the middle of the summer? Not sure about the easy living part, nothing about healthcare feels easy right now, no
matter what the season!We have certainly been busy this summer with AAHAM business. The fight to modern-
ize the TCPA act has continued on with a lot of activity, meetings, and phone calls. Our man in Washington, Paul Miller, has continued to pound the pavement for us in D.C., and the message is getting out there. I am so hopeful that all of AAHAM’s visits at Legislative Day and after will pay off with a sorely needed update to this antiquated act. We can certainly take great pride in our involvement in this cause. Our organization makes a difference!
Summertime also means another round of certification exams. I know that several local chapters have done a phenomenal job in offering coaching sessions, and that is very evident in the ever increasing numbers of members holding these prestigious designations. Just a reminder that the webinar study sessions for the Certified Revenue Cycle Executive (CRCE) exam starts in July and the new Certified Revenue Cycle Professional (CRCP) study sessions begin in September. This is a great way to prepare for the exam, brush up on your skills and earn CEUs at the same time.
Have you noticed the amazing increase in our presence on social media? AAHAM has always tried to be forward-thinking, and everything we do is to bring value to our members. In our continuing quest to stay relevant, and bring breaking updates and information to you in real time, we have made a firm commitment to this program.
Social media is very important to organizations like ours because it helps to expand awareness of our name, mission and goals. We strive to use social media to provide engaging industry news, educational posts, photographs and fun facts, and it is also great to promote events such as Legislative Day, the ANI and the fabulous webinars our education committee has been so diligently providing every month.
AAHAM is out there on LinkedIn, Face Book, Twitter, You Tube, Blogs and Pinterest. A great foundation for our presence on social media has been established, and many more opportunities exist. If you are not already a “friend” or following AAHAM on these media outlets, hop on board today! Make sure you look for TBT on Thursdays. It is been so much fun seeing the photos of many members from past events. Our reach gets bigger every month, and helps to continually bring others into our organization so they too can share all we have to offer.
Now that we are in the midst of summer, it will be ANI time before we know it. Make your plans now to join us in beautiful San Diego October 15-17th. I have gotten a sneak peek at the education, and it is exactly what you are looking for. The venue and weather on the west coast is amazing, and I can’t wait to see all of you there!
Enjoy the rest of your summer. Remember to give back to others; you will gain so much more than you give. “When we give cheerfully and accept gratefully, everyone is blessed.” Maya Angelou
Sincerely,Victoria Di Tomaso, CRCE-INational President

Note: A CEU is defined as a sixty (60) minute period of education
* Be Sure to Attach Supporting Documentation
Mail Completed Recertification Form and backup documentation to:
AAHAM National OfficeProfessional CEUs
11240 Waples Mill Rd #200Fairfax, VA 22030
Signature _____________________________________________________________________ Date _____________________________
Certification Designation:
First Name: Last Name: National Members ID#:
Address:
City: State: Zip:
Work Phone: Home Phone: Email:
No. of X Weight = CEUs Description:
Hours/Units Earned Date Earned:
No. of X Weight = CEUs Descritpion:
Hours/Units Earned Date Earned:
No. of X Weight = CEUs Descritpion:
Hours/Units Earned Date Earned:
No. of X Weight = CEUs Descritpion:
Hours/Units Earned Date Earned:
AAHAM Professional Recertification FormContinuing Education Units (CEUs)
CRCE-I/CRCE-P
Weight Activity Qualifying for Continuing Education Units (CEUs)1.0 unit Each hour proctoring a professional certification exam
1.0 unit Each hour proctoring a technical certification exam
1.0 unit Each professional exam section completed and graded by deadline
1.0 unit Each hour in attendance at an educational program or class relating to the healthcare field
1.0 unit Each hour coaching an organized technical certification review session
1.0 unit Question, answer and reference material submitted and accepted into the professional exam bank
2.0 units Each hour in attendance at an AAHAM sponsored educational program
2.0 units Authored an article published in an AAHAM Chapter publication
2.0 units Attendance at a National President’s meeting
2.0 units Director or Chapter Committee Chairperson
2.0 units Each hour coaching an organized professional certification review session
3.0 units Attendance at an AAHAM audio conference
3.0 units Authored an article published in a National AAHAM publication
3.0 units Given presentation related to AAHAM, patient accounting or healthcare administrative management (AAHAM related credit given if made at an AAHAM sponsored event or if presenter is representing AAHAM)
3.0 units Chapter Officer
4.0 units National Committee Chairperson
6.0 units Officer of National AAHAM
8.0 units Attendance at AAHAM Legislative Day
6 The Journal of Healthcare Administrative Management
One has to ask what is happening in Washington this year. I’m not talking
about their legislative agenda. We all know it has moved at a snail’s pace, but what is happening with the primary elections in various states?
Let’s start with the circus in Virginia where we had an unknown college professor from Randolph-Macon College shock the political world by knocking off the second ranking Republican in the House of Rep-resentatives. Just two days before the pri-mary, all the so-called experts had Rep. Eric Cantor cruising to a primary victory by ten points or more. This should have had peo-ple nervous considering two months earlier Rep. Cantor was up by thirty points over the unknown Dave Bratt.
You can’t point to one specific reason why Cantor lost, but you can blame it on a combination of three critical factors. First, Cantor, although he spent $5 million on this primary (to Bratt’s $122,000), he didn’t seem to take it too seriously or be too con-cerned. The joke after the election was that Cantor spent more on a steak dinner fun-draiser than Bratt did on his entire cam-paign (which is actually true). According to the Federal Election Commission, Rep. Cantor spent over $168,000 on steak din-ners as part of fundraising efforts to Bratt’s $122,000 spent on his entire campaign. In another move of pure arrogance, Rep. Can-tor skipped one of the most important Vir-ginia political events. Every April, Virginia hosts their annual shad planking event, which for politico’s, is a must attend event if you’re running for office. This year Rep. Cantor decided to skip this event and in-stead was traveling around the country rais-ing money for other candidates. This left Bratt as the only candidate in this race at this event talking with constituents about
their concerns. This event also gave Bratt free rein to hammer Cantor on being out of touch with Virginia and more concerned with national politics, which was evident by him not being at this event and instead spending time with voters in other districts outside of Virginia.
Some were concerned by Cantor’s dis-missive attitude towards Bratt and the pri-mary. People started to see the poll numbers shift to the point where some heavyweights offered to lend a hand to Cantor, which he declined. The U.S. Chamber of Commerce was so concerned that they volunteered to come in and help the Congressman, but were told it wasn’t necessary. This has every-one shaking their heads. Had the Chamber come in, you might have seen a very differ-ent outcome.
On primary day, you had the good Congressman sipping coffee in downtown D.C. at a fundraiser instead of home in the district shaking hands with voters outside the polls. This was seen by voters as the norm for their Congressman. He was never back in the district, even though it’s only an hour outside of Washington. He never met with constituents and was routinely criticized for spending his time with donors outside the district or spending time in other districts raising money for other candidates. There was a real sentiment among voters this year that Rep. Cantor was simply out of touch with the needs of his constituents. For most politicians this would have been enough for them to lose, but when you are the second most powerful Republican in the House, can spend unlimited money on your cam-paign, and still strong arm Republicans to get behind you, you have to point to other factors that helped turn voters against you.
The second issue you can point to as to why Rep. Cantor lost is immigration.
Rep. Cantor is seen by Democrats as hold-ing up any real attempts to pass meaningful immigration reform. You have comments from the Congressman himself that paint a picture of possibly waffling on this issue. Then add in the timing of the thousands of kids storming the border wanting to enter the United States, and now if you are Can-tor, you have a real problem just days before the election. Cantor’s opponent, a self-pro-claimed Tea Party candidate (keep in mind the Tea Party spent a paltry $1,200 to help Bratt win) made immigration a major is-sue in the last stages of the campaign. He painted Cantor as someone who waffles on the issue of immigration and who supports amnesty. If you are a Republican, this is a no-no.
The third issue, if the first two weren’t bad enough for a candidate to deal with, was the crossover vote by some Democrats. In Virginia, there is an open primary, meaning anyone can vote in a party’s primary as long as they are a registered voter. Democrats in Virginia and nationally have made Rep. Eric Cantor public enemy number one. Cantor was seen as an obstructionist by Democrats. They knew however that unseating him would be difficult without Democrats cross-ing over and voting in a Republican pri-mary. That is exactly what Democrats did. Hard to say in how big of numbers, but it was enough to push this race from close to a blowout in Bratt’s favor.
This race wasn’t one that went down to the wire. This race was called early in the evening and had everyone on both sides scrambling to figure out what it meant. It sent an obscure candidate into the national spotlight. Bratt didn’t just win and knock off a political giant; he flat out gave him a good “ol fashioned whoopin” as they like to
Paul A. Miller, PLC, Lobbyist
washington wire
Continued on page 7
Washington’s Wild Primary Season: What Does It Mean?

Summer 2014 7
say. Bratt won by eleven points and did so in an impressive manner considering he only had himself and two other paid staff as his campaign team. What makes this even more impressive is that Bratt was outspent 22-1 by Cantor. His win puts Bratt in a category of creating one of the biggest political upsets in history.
This is not the only anomaly of this primary season.
If you have been following the pri-maries across the country, you have to be glued to your seat with what’s happening in Mississippi. In June, Mississippi held its Republican primary pitting an incumbent Senator at the young age of 76 against an even younger Tea Party challenger. To win the primary you needed 50% of the vote to move onto the November general election. On Election Day neither candidate got the 50% of the vote needed, which forced a run-off election three weeks later. Heading into the run-off a lot of pundits had written Cochran off and we’re ready to anoint Mc-Daniel as the Republican nominee and next U.S. Senator from Mississippi. You had still others who saw the momentum heading in McDaniel’s direction and thought Republi-can donors would pull out, thus giving Mc-Daniel the edge and the win. Oh were they so wrong about the donors and the strategy.
Two reasons why the voters of Missis-sippi are going to send the 36-year veteran back to Washington. The first is while most politicians are criticized for doing nothing, Cochran scored high with voters on tak-ing care of Mississippi and bringing money home to the state. This matters in Mississip-pi and Cochran was rewarded in part for it.
The biggest reason for Cochran’s win is the Democratic crossover votes he received. Had Cochran not decided to try and appeal to Democrats, he would have lost this race and chance to return to the Senate. Cochran spent the run-off wooing Democrats and pointing to his record in the state versus what his opponent would do in Washing-ton. It is a strategy that is being criticized by both sides. Democratic leaders are furious that some in their party would openly help
Sen. Cochran win re-election. Republicans for their part are equally outraged by the Senators strategy, claiming this went against the principles of the party and what it stands for. Granted this strategy was a gamble by Cochran, but one clearly the McDaniel camp dismissed and it cost them.
What makes Mississippi so interest-ing is that by helping Sen. Cochran win his primary, Democrats all but guaranteed Cochran would be re-elected to the U.S. Senate. By voting for Cochran, Democrats made a statement that they would prefer Cochran as their Senator than their own nominee. Granted, had McDaniel won the primary the general election would have been his to lose, but it would have made it a race Democrats could have competed for and possibly stole. Instead, Democrats helped re-elect the senior Senator from Mis-sissippi from the opposing party.
The other interesting thing about this race, that I could see playing a role in other states and districts with open primaries, is the idea of candidates broadening their ap-peal. In recent times, especially with the advent of the Tea Party, we have seen can-didates in the Republican Party pushed farther right than they truly are. In the Co-chran case, he moved more to the middle versus a strong Tea Party challenger and it paid off. This won’t work in all districts or states, but it is something you will see can-didates on both sides of the aisle consider in future races. This could also be a strategy for “establishment” candidates to use to help neutralize their Tea Party opponent in a pri-
mary. Again, this is a unique case and set of circumstances that can’t be easily repeated, but it is a strategy that more candidates may consider and map out in the future.
There are a lot of lessons to learn from both the Virginia and Mississippi races, but the most important one to remember, is this is politics and anything can happen and you need run like you’re ten points be-hind your opponent and never let up. Rep. Cantor learned that the hard way. What do these two races mean on a national scale? For me, they mean two things. The first is, although Virginia will elect a so-called Tea Party member to the House of Representa-tives, you can point to more states where these candidates were beaten by “establish-ment” supported candidates. This means the Bratt victory in a heavily Republican district means little to the overall make-up of the House. In 2010, the Tea Party came roar-ing onto the stage with a big win in special election in New York. From there the move-ment really took off. In 2012, the Tea Party candidates defeated “establishment” candi-dates in primaries, but lost badly in the gen-eral election, leaving Republicans with two straight elections cycles of not being able to recapture the Senate. In 2014, Republicans are presented with a last opportunity to gain control of the U.S. Senate. Starting in 2016, Republicans will have to defend more seats than Democrats, making it harder to regain the majority when you have to focus on more of your own seats and fewer Demo-cratic seats in play.
washington wirecontinued from page 6
Continued on page 11

8 The Journal of Healthcare Administrative Management
By Richard Lovich, EsquirePartner, Managing Litigation Attorney
Stephenson, Acquisto & ColmanAAHAM Legal Counsel
Independent Review Organizations (IROs) have recently gained favor in the
payer community. Proposed contract lan-guage requiring their use has been creeping into Hospital Services Agreements (HSA) for over a year. It is essential the provider community be aware of the danger involved in agreeing to their use.
As clinical denials become more fo-cused and widespread, many health insur-ance plans are taking aggressive measures to stack the deck against the provider. One of the most prominent of these tactics is the inclusion of a requirement that the provider submit all appeals for clinical denials to In-dependent Review Organizations, (IROs). The provisions have a significant negative impact on the provider’s chances of success in challenging medical necessity denials.
The obvious purpose behind the IRO language is to limit provider recoveries on clinical denials. The use of an IRO tips the scale against the provider by taking the de-termination of medical necessity cases away from the arbitrator or judge and requiring they be submitted to an IRO essentially con-trolled by the plan. There is little if anything “independent” about these organizations. In addition to the lack of independence, there are other, very significant problems with agreeing to IRO provisions.
1. Waiver of arbitration or trial One of the most dangerous aspects of
the IRO provisions is the absence of the abil-ity to arbitrate or file a lawsuit to determine the validity of the clinical denial. If the plan denies a claim based upon medical necessity, level of care, or that the treatment was inves-tigative or experimental, the provisions usu-ally require the provider to request the claim be submitted exclusively to the IRO, whose decision is binding. No arbitration or trial in front of a neutral officer is allowed.
2. Separate appeal deadlinesThere are typically separate time dead-
lines for submission of clinical claims than for other claims, and failure to appeal prop-erly can deprive the provider of any further ability to pursue the claim. Most HSAs in-clude an arbitration clause. Most contracts previously required all disputes be resolved through timely submission to arbitration af-ter the appeals process is exhausted. Thus all claims were treated the same for purposes of timing. Now, under the new IRO language, claims denied or underpaid based upon med-ical necessity have an additional, and in fact conflicting time deadline. Most importantly, if the deadline is not met, the plan’s denial can be considered final and the facility has no further recourse. The fact the failure to timely appeal pursuant to the terms of an IRO provision may be fatal; means providers must pay close attention to the IRO time-lines, especially if they differ from the HSA’s standard appeal timeline. For example, the contract may require all clinical claims be ap-
pealed through the standard appeal process outlined therein. While contracts may differ on the time period, there is usually a provi-sion that indicates within 180 days from the plan’s medical necessity determination, the provider must request an IRO review, on a special form, and mailed to a special address. The Operations Manual however may say such submissions must be done within 365 days of the claim determination. To be com-pletely safe and not allow this to be an issue, a provider should gauge its time period by the IRO time requirement.
3. Control of the list of IROs Typical language has been requiring the
available IRO’s are only those chosen by the plan. The provider can choose from a list, but the list is supplied, created, and main-tained exclusively by the plan. The plan’s operations manual, which is commonly in-corporated into the contract, allows the plan to supply a list with as few as two IROs from which to choose. Because the plans are at-tempting to include the IRO requirement in all if their HSAs, all of the claims sub-mitted to the IROs will have that plan as a respondent, while, the claimant provider will change. Thus from an economic stand-point, the IRO has a significant incentive to side in favor of the plan in order stay on the eligible panel.
4. No guarantee of a qualified reviewer
The provider’s ability to choose is not only limited to one of the plan’s IRO’s, but are
Independent
Continued on page 10
Independent Review Organization
The Dangers of Agreeing to an
ReviewOrganizationRequirement in Hospital Services Agreements

Summer 2014 9
Independent Review Organization

10 The Journal of Healthcare Administrative Management
also limited in the type of reviewer that will make the decision. The IRO assigns the spe-cific physician to review the claim. Under the template language the only requirement for this reviewer is that it be a person who pos-sesses a medical license in the United States. Thus, there is no guarantee that a specialist will review a treating specialist’s treatment.
5. No guarantee appropriate supporting documents will be reviewed
If the issue on appeal is whether the claim is experimental or investigational, the issue should be decided by, at minimum, a review of the appropriate peer reviewed ar-ticles and literature, as well as other appropri-ate sources of information. The contractual IRO language may not allow for this type of review. Typically the language indicates the review of a claim will be limited to only those medical records that were submitted to the plan when the decision was made to deny the claim. Unless all of the aforementioned litera-ture is submitted as part of the medical record at the claim submission stage, it will not be considered. In contrast, the typical arbitration or trial of a medical necessity case involves the records being reviewed by medical experts. If there are missing records, the expert identi-fies them and instructs the provider to send them and they are used in support of the pro-vider’s position. Thus, along with the medical records there is a thorough delineation of the latest medical literature supporting the treat-ment provided. Absent this supporting docu-mentation it is at best a gamble whether the IRO reviewer will research the point or even have the requisite level of expertise to under-stand the treatment.
6. You may have no input at all if the pa-tient seeks review first
There is another problem with this limitation on information. The contract may indicate that if the patient has previ-ously requested an IRO review of a medical necessity decision, the facility is bound by that decision. Thus, the provider is at the mercy of whatever the patient submitted in support of the medical necessity of the
treatment because the records cannot be augmented at that point.
7. IROs are not qualified to adjudicate the legal aspect of the issue
Medical necessity is both a clinical and a legal determination as is determining whether certain treatment falls within a con-tractually defined level of care. Specifically, the interpretation of the contract language is a matter of law. However, under the typical IRO provision, there is no guarantee the re-viewer will even see the contract. And if they do, are they qualified to interpret it?
8. Provider’s advantage in advocating the superiority of the treating physician’s decisions is eliminated
The IRO provisions virtually elimi-nate all advocacy. The provider does not have the opportunity to cross examine the plan’s medical reviewer who originally made the determination to deny the claim. This is extremely important because by case law (in California and many other states), the treating physician’s opinion should be given great weight in determining whether the treatment provided was medically neces-sary. This makes infinite sense because the treating physician is in the best position to make the determination as to what treat-ment is necessary, given the information known at the time. The treating physician directly examines the patient, interacts with the patient, and makes decisions at the time the treatment is being provided. This is in contrast to the plan’s medical reviewer who is basing the denial solely on a review of the medical records; no examination or interac-tion with the patient, and many months, if not years after the treatment is provided; all
with the benefit of hindsight. An effective argument at arbitrations
and trial is “Monday morning quarterback-ing” is virtually irrelevant to the determina-tion of medical necessity. The inquiry is not retrospective; it is not whether the treatment was necessary once you know the outcome of the treatment. The inquiry is “given the information known at the time, does the treatment provided fit within the contrac-tual definition of medical necessity?” The IRO process robs the provider of this key advantage.
9. The IRO process makes pursuit of smaller claims economically unfeasible
The IRO contract language usually does not delineate the costs involved, nor does it limit the amount that can be charged by the IRO. In addition, IRO provisions can be a winner takes all proposition. In some IRO provisions if the IRO decides the plan was correct in denying the claim, the provider is solely responsible for paying the IRO’s fee. With the stacked deck created by the IRO provision, this will be a common result. Fur-ther, the plan pays only if the IRO reverses the denial completely. If there is a split in the decision, such as where several days are de-nied and a few are overturned, the fee is split.
Thus if you have a claim that is rela-tively small, is it worth the gamble that not only will you not recover on the claim, but will have to pay out the fee for the IRO?
The bottom line is to be aware and vigi-lant of the proposed IRO language and to limit it as much as possible if it cannot be eliminated entirely.
Mr. Lovich can be reached at [email protected]
continued from page 8
Summer 2014 11
The Tea Party isn’t dead like some will have you believe. The Tea Party is deeply wounded, just not dead. Next year will be their true test of whether they can survive or will simply fade out over time, similar to Ross Perot’s third party efforts of the 90’s. If the Tea Party is able to capture the Speaker-ship or control the agenda in 2015, then I’d say they will get off the ropes and become a stronger force to be reckoned with leading up to the 2016 congressional and Presidential elections. If Speaker Boehner comes back in 2015 with a heavy fist and controls the agen-da and his caucus with the help of outside allies like the business community, I’d say the Tea Party may be become even weaker and find themselves struggling to be heard. This is why politics is so fun, anything can happen!
In the Senate the dynamics are a little different. Republicans need to pick-up six seats to regain the majority. This year that is very possible. First, the President is hovering around 40% in approval ratings. You have a President who is losing support from his own party, which is not good heading into an election. The President should be an as-
set, but as of today, there are more Demo-crats asking the President to stay out of their states than you do asking him to come and campaign for them back home. You also have the Senate controlled by the Democrats today and an agenda at a standstill. Some of the issues critical to Democratic voters, like gun control and immigration reform, will not move this year in large part due to the elections. Those Democrats up for re-elec-tion in states like Louisiana, Arkansas, and North Carolina cannot vote for these issues and expect to be re-elected. This being the case, Republicans keep hammering away at a party doing nothing to help create jobs and working families, which has translated. They continue to hammer on the President and issues like the IRS scandal, Benghazi, recess appointments, and problems in the Middle East, all issues falling on the President, but also being hung around the neck of every Democrat running for re-election this year.
Oh yeah, don’t forget about the Afford-able Care Act (ACA). This is an issue you don’t see Republicans continuing to force votes on, they finally woke up and got smart and saw this did nothing to help their cause, but they do continue to hammer home the
continued challenges and so-called failures the program is experiencing. This is going to continue to be a drag on Senate Democrats up for re-election, especially if you were one of those Democrats who voted for the bill.
For me, the biggest obstacle for Demo-crats keeping control of the Senate or even having a glimmer of hope at regaining con-trol of the House, is the Republicans. For the first time in quite a while it looks like Re-publicans have a winning strategy that may actually work. They are nominating more electable candidates, which should have the Democrats very concerned. Republicans appear to have thrown out the playbook of 2012 when nominating far right candidates in states and districts wasn’t going to win them crossover votes they needed to win general elections, may help win primaries, but hurt them with general election voters. In some of those cases, they nominated can-didates their own party could not, and did not support. This year it appears the goal is electability and Republicans, at least today, seem to be winning on that strategy.
A lot can happen between now and November so stay-tuned and expect an ugly and nasty roller coaster ride!
continued from page 7
CRCE–I Certified Revenue Cycle Executive – Institutional
CRCE–P Certified Revenue Cycle Executive – Professional
Certification opens the door to the possibility of career advancement. Earning an AAHAM certification demonstrates that you have mastered the common body of knowledge for your profession. Sitting for these exams requires commitment and dedication. The CRCE–I,P Exam Study Manual will help assist you in preparing for the CRCE–I,P Exams.
Written by AAHAM, for AAHAM’s own certifica-tion programs ensures that this manual is thegateway to studying for and passing these professional exams. Included in the manual are chapter review questions and study tips. Log on to www.aaham.org for more information and to order your Exam Study Manual today!
12 The Journal of Healthcare Administrative Management
SpeakingTips
By Sheryl RoushPresident/CEO,
Sparkle Presentations, Inc.
Whether addressing your staff or Board of Directors, conferring with col-
leagues or vendors, advising a patient or their loved ones, how you communicate and convey that message makes all the difference in its effectiveness. There are four types of “presentations” and depending on the objective and de-sired outcomes of your message, you may use one, or more of these: to inform, edu-cate, persuade, and/or inspire. Regardless of which type you use, there are three main factors in the listener’s ears and mind de-termining the success of the message:1. Content (words, research, facts, statistics,
case studies, stories, testimonials, docu-mentation, quotations, references, etc.)
2. Delivery (style, tone, vocal variety, pace, pitch, volume, body language, facial ex-pression, etc.)
3. Congruency (authenticity and genuine-ness). Do the content and delivery match the messenger? Although the first two fac-tors are important, this third factor is vi-tal! Your listener subconsciously observes and determines the real message (meta-message) of what is being communicated. Do the emotions, movements and overall tone appropriately align with the mes-sage? Is the speaker believable?
Practice your presentation in front of a mirror, ensuring that what you look like (facial expressions, eye movement, body lan-
guage) is what you want to look like, sound like, be like. Would you believe you?
If you are not comfortable with public speaking, consider checking out the Toast-masters Club. They offer a safe place to prac-tice with a supportive audience where you receive keen feedback. Practice impromptu and prepared presentations, listening, think-ing and speaking skills to enhance your lead-ership and advocacy.
25 Public Speaking Tips for the Non-Professional Speaker
1. Believe the audience sincerely wants you to succeed and learn from you
2. Affirm you have a message they need to hear and offers value
3. The more time you devote to advance preparation, the less anxious you will be
4. Mind map your concepts initially (not starting with a lined memo pad!)
5. Draft a simple outline indicating po-tential flow, content and transitions
6. Incorporate the multiple communica-tion modalities of listeners
7. Sit quietly and see yourself presenting this program, hear your words
8. Write out your entire presentation word-for-word
9. Craft a solid “grabber” opening state-ment and a purposeful closing
10. Read it out loud as if you were giving it live
11. Edit it more, to be in your “voice.” Speak it so it sounds like you,
12. Condense your major points as bullet point reminders on one index card
13. Practice using the handwritten index
card to enhance visual memory14. Rehearse your delivery, being as natural
as possible, standing in front of a mir-ror
15. Observe your timing, pacing and flow. Be genuine and confident.
16. If using slides, practice run-throughs several times, and have a back-up plan
17. Visualize yourself presenting this pro-gram successfully. See it, hear it, feel it.
18. Be congruent with your body language, movement, voice and facial expressions
19. Add audience interaction, activities and more conversation into your timing
20. Video record yourself, a head-to-toe view; watch it closely, with the sound off!
21. Visualize the improvements. Video re-cord and watch it again.
22. Further prepare by rehearsing at the lo-cation
23. Create short, memorable, positive affir-mations to say to yourself
24. Arrive early at the location, get equip-ment set-up and get settled-in
25. Meet people, ask them what they came to learn, and deliver it!
What to do before you speak:• Plan your wardrobe and all pieces that go
with it• To combat stress, eat raw green vegetables• For dry throat, eat Asian Pears and Water-
melon• Get a good night’s sleep the night before• For stress, use Bach Flower’s Rescue Rem-
edy• Gargle with warm water
Continued on page 13
Public and Private
Summer 2014 13
• Drink plenty of water, lukewarm or hot• Brush your teeth• Apply light chapstick or Vaseline to lips/
teeth• Get up, move around, and stretch• Use the restroom. Wash with warm water.• Be quiet for a minute before you’re on• Thump your chest like Tarzan for energy
What to avoid before speaking:• Apologizing• Sitting still• Ice and cold beverages• Throat drops with menthol• Alcohol, diuretics and decongestants• Eating anything with nuts, seeds or ber-
ries• Cheeses, creamy sauces, sour cream,
cream cheese• Negative people and depressing conversa-
tions• Caring what people think about you...• People asking if you are nervous?
Hear Sheryl Roush at the Thursday keynote session at the ANI. For more information, visit www.SherylRoush.com
continued from page 12

By Jack Singer, Ph.Dprofessional speaker, trainer and
licensed Clinical/Sport Psychologist
Why is it that some Revenue Cycle Professionals with the most talent
are often not the most successful? What gets in their way? How can those who possess less natural administrative and leadership talent over-achieve and reach much more success than their more talented or experi-enced colleagues? Are there specific mental skills that can lead anyone toward cham-pionship levels of job performance? What separates the mindset of a champion from that of the also-rans?
As a Professional Clinical/Sport Psy-chologist for more than thirty years, I have worked with Olympic, Professional and World Champion athletes in every sport imaginable and I can tell you what separates the good performer from the world class performer is the mental mindset, not the athletic talent. With medical administrative professionals, it is much the same. The men-tal/emotional mindset of the professional is the difference between good performance and consisitently stellar performance.
The good news is this mindset is a learned series of mental skills, that anyone is capable of developing and practicing, de-spite the challenges of government regula-tions, decreasing reimbursements, staffing shortages, budget constraints, ICD10, 501r and confusion surrounding ACA! You see, my training and experience leads me to conclude that everyone is gifted. They may “open their gifts” at different stages in their lives, or, sadly, they may remain unopened. But everyone can learn how to open and use
their gifts for greatness by developing the mindset of a champion.
Below is one of the powerful compo-nents of the mindset of a champion that you will learn at my keynote at the ANI in San Diego. Put these ideas into action today and watch your performance skyrocket and your stress levels decrease.
Engage the “linguistic nutrition” of championship performance
Your self-talk is the foundation of your belief system and your belief system deter-mines your attitudes about your success (or lack of it) in your career. Your internal think-ing patterns either set you up for success or failure. So often, people unconsciously use self-limiting thoughts which prevent them from being successful. It’s a form of unin-tended self-sabotage. Some examples of such self-talk phrases are: “because I don’t know all of the nuances of the ACA, I will look confused and unsure of myself when I train my staff,” or “patients are going to be very upset when we tell them they need to make up front payments.” Maintaining these kinds of thoughts will erode your pro-fesssionalism and will become self-fulfilling prophecies. It’s like always eating junk food once you convince yourself that a healthy eating lifestyle is just too difficult to main-tain. Self-defeating thoughts will always set you up for failure.
Your thoughts determine your beliefs, your beliefs develop your attitudes, and your attitudes determine your behaviors and actions. Therefore, negative, pessimistic thoughts will ultimately lead to procrastina-tion, avoiding some of your responsibilities and less than stellar leadership behaviors in front of your staff.
Action Plan: Keep a written journal of negative thoughts that enter your mind regarding your daily challenges at work and notice the patterns. Then, use rational thinking to counterpunch each negative thought with a healthy, positive thought. For example, change “because I don’t know all of the nuances of the ACA, I will look confused and unsure of myself when I train my staff” to “I will train my staff to master what we do know about the nuances of the ACA, and we will build into our operating procedures exceptions and modifications that can be made once there is more defini-tive information. Perfection is not the goal, here. I am a sharp, creative person and I will make sure that my staff is well trained and flexible.”
The key here is to believe that you will succeed, despite all of the challenges, obsta-cles and setbacks that are inevitable in the Revenue Cycle career. Continue to believe you will succeed, even in the face of resis-tance, rejection and perhaps hostility. How you explain to yourself and react to setbacks in your career is a crucial determinant of how successful you will ultimately be. Just as with the elite athlete, training yourself to look at setbacks as temporary challenges and minimizing those setbacks with the knowl-edge that you can find a solution and over-come them, predicts ultimate success.
This concept and action plan is a sample of what you will learn in my keynote at the ANI in San Diego. Your road to remarkable performance begins with my keynote pre-sentation! Hear Jack Singer at the Wednes-day keynote session at the ANI. For more information, visit www.funspeaker.com or email him at [email protected] n
14 The Journal of Healthcare Administrative Management
How the Revenue Cycle Professional Can Develop the Mindset of a Champion: Proven Techniques to Skyrocket Your Performance, Especially During Challenging Times
How the Revenue Cycle Professional Can Develop the Mindset of a Champion:
Proven Techniques to Skyrocket Your Performance, Especially During Challenging Times

How the Revenue Cycle Professional Can Develop the Mindset of a Champion: Proven Techniques to Skyrocket Your Performance, Especially During Challenging Times
❏ Enclosed is my check. Please make payable to AAHAM.
❏ Please charge my credit card: ❍ AMEX ❍ MasterCard ❍ VISA
Card Number: ________________________________________________________
Name on Card: ___________________________________ Exp. Date: ___________
Signature: ___________________________________________________________
SHIPPING INFORMATION
Name: ______________________________________________________________
Address: ______________________________________________________________
City: __________________________________ State: ________ Zip: ___________
CONTACT INFORMATION
Name: __________________________________ Phone: ___________________
Email Address: _______________________________________________________
❏ Yes, I want all 4!
❍ 4 Part Series on CD ROM: $350.00 Member rate
❍ 4 Part Series on CD ROM: $450.00 Non- member rate
❏ No, I only want the following sections: $125 per section on CD ROM - Member rate $225 per section on CD ROM - Non-member rate Individual Sections: Please check which section(s) you want:
❍ Part 1 Access
❍ Part 2 Billing
❍ Part 3 Credit & Collections
❍ Part 4 Accounts Receivable Management
Email, fax or mail this registration form along with your payment to:AAHAM CRCE-I/CRCE-P Study Session CD ROMs,11240 Waples Mill Road Suite 200, Fairfax VA 22030
Fax: 703.359.7562 • Email: [email protected] • Questions? Please call 703.281.4043 x202
Company: ___________________________________________________________
Professional CertificationWebinar Series
Available Now On CD ROM
AAHAM and top CRCE-I & CRCE-P present afour part Webinar Study program
for the AAHAM Professional Exams:
Access • Billing • Credit & Collections • Accounts Receivable Management
The entire 4 part recorded CD ROM series costs $350.00.Individual parts can be purchased separately for $125.00 each.

16 The Journal of Healthcare Administrative Management
By Rob BorchertMBA, FHFMA, CRCE-I
Best Practice Associates, LLCDon Borchert, BA
Consulting Manager, Altarum InstituteTim Borchert, MBA, PMP
Deputy Director, Altarum Institute
It is now the summer of 2014 and people are relaxing and preparing for a wonder-
ful vacation either away from the house or around the house, just as long as it is away from work! For those of us on the busi-ness side of the healthcare industry, this is not only a time of vacation but a time of planning. When the summer vacation sea-son ends, we will have four quarters before major changes happen. Four quarters that, if not planned correctly, may not equal a dollar in reimbursement. We would like to give you some suggested steps to help reduce stress, maintain productivity and keep cash flow stable, if not better. First, in order to prepare for an active, positive and success-ful October 1, 2015, one must document a plan. This plan will include required steps, recommended steps, and potential nega-tive effects if not done, plus achievable goals for each quarter. Some suggestions for each quarter are described below.
First Quarter: (October thru December)
For the successful outcome of the next four quarters, responsibility and account-ability are the two key factors. You should already have an ICD-10 Implementation (Steering) Committee and now is the time
to make it a truly action-oriented team. Your committee should consist of key staff mem-bers from information technology (IT), health information management (HIM), patient financial services (PFS), finance, clinical providers (physicians and nurses), patient access (registration), revenue integri-ty, ancillary departments, and others as you see fit. This committee should finalize the list of areas that may need additional help in meeting the goals and objectives of the facil-ity/system/practice. Here are some targeted areas for consideration:• Managed care contracts (either re-written
or amended)• Access stations to address the new man-
aged care environment with pre-authori-zation criteria, medical necessity criteria, admission criteria, and ACA delegates
• Admission reports and ancillary volume reports by medical specialty (physician)
• Outpatient surgery reports by medical specialty
• Clinic visits (physician visits) by medical specialty
• Discharged-not-final-billed (DNFB) re-port (weekly with as much specificity as possible)
• Inpatient chart backlog (over 5 days since discharge) by physician/medical specialty
• Weekly query count by physician/medical specialty
• Physician liaison position for education, clinical documentation improvement, etc.
• Outpatient chart backlog (over 3 days since discharge) by ancillary department
• Outpatient surgery chart backlog (over 3 days since discharge)
• Transcription backlog by physician
• Initial claim edit report by type, by rea-son, by physician, by payer
• Review of the HIPPA 275 claim report (daily/weekly)
• Accounts receivable report greater than 90 days by payer (monthly)
• Top ten denials by payer (by type and dol-lar value, by physician) [weekly]
• Report of appeals by payer (in process, wins and losses) [weekly/monthly]
These sixteen (16) reports, plus any others that you want to use, are the basic groundwork for this committee to re-com-mit themselves toward a successful and non-eventful conversion to the new ICD-10 environment. The chair of this committee should assign the responsibility to moni-tor these reports and be held accountable if they show signs of a negative position. The person responsible will certainly be work-ing with other members of this committee as well as other staff members to assure the accurate presentation of the report each re-porting period. For instance, along with the weekly query count and the backlog reports must involve some activity with the clinical documentation improvement (CDI) group.
During this first quarter, the discussion of these groundwork reports should gener-ate questions, value, interaction, recom-mendations, etc. for the purpose of under-standing and enhancement of each process wherever possible. For instance, managed care contracts…• Check the language of each contract re-
garding any suggested amendment per-taining to the limitation of reimburse-
EqualA Dollar?
Continued on page 17
Will Your Next Four Quarters
Spring 2014 17
ment during the “adjustment period” of ICD-10 such as “budget neutrality” or “reimbursement same as”
• All diagnostic-related group (DRG) reim-bursement needs to be tested and re-test-ed to examine any DRG weight changes with the new coding system. This can di-rectly affect reimbursement.
• Evergreen contracts need to be reviewed
for updating of language, base rates, an-nual increases, coverage areas, etc.
• With the delayed implementation, until at least October 2015, you have time to deal with the critical managed care con-tract companies and be assertive with them in obtaining the best reimburse-ment terms now. Payers also have an in-terest in remaining budget-neutral with this transition.
During this first quarter, the ground-
work needs to be set in order for the re-maining three quarters to produce positive outcomes in each of the critical areas of the revenue cycle.
Second Quarter: (January through March)
It is now after the holidays and time to revisit your goals. If the goals have not been
Continued on page 18
continued from page 16

18 The Journal of Healthcare Administrative Management
continued from page 17
prioritized during the first quarter, this is the time to do it. This is the key to success. At each committee meeting, the member held accountable for their revenue cycle process area needs to be making true progress re-ports. During the second quarter, some of the outcome goals are:• Identifying the managed care contracts
that need revision regarding reimburse-ment
• Identifying the managed care companies that require electronic claims acceptance testing (what about Medicaid? For exam-ple Maine had not started testing prior to the delay and has not communicated their new plan)
• Identifying the physicians who will need further assistance with clinical documen-tation, medical necessity requirements
• Identifying medical specialties that will need further assistance with clinical docu-mentation requirements and coding ex-pertise
• Process flow improvements for outpatient services, surgery data collection, EHR uti-lization, concurrent review, coding proto-cols, etc.
• DNFB reduction• Top ten denials by payer• Top ten appeals (by payer?), both winners
and losers• Physician champions, ancillary champi-
ons, and coding champions
Each member of the committee should have measurable goal(s), outcomes and the steps to reach that goal(s) by the end of the first quarter. Second quarter begins the activities to reach the goal(s). The commu-nication among the committee members should be interactive between meetings to avoid surprises and to build and maintain the cross-sectional revenue cycle depen-dence.
Deliverables during the Second Quarter:
• New/revised managed care contracts un-derway
• End-to-end testing with government pay-ers
• End-to-end testing with top three major payers
• Scheduling of end-to-end testing with other payers for third quarter
• Physician specialties (and physicians) identified for additional education re-garding CDI
• Process flow improvements validated and initial areas selected to begin implementa-tion
• Additional resource (if needed) identified and contracted for the two weeks prior to October 1, 2015 for any coding backlog
• Current processes reviewed and validated for each payer denial
• Internal champions identified begin par-ticipation in all ICD-10 projects as appro-priate
Third Quarter: (April through June)This is a very important quarter as it is
just before the summer and the traditional distractions that come with that season. During this quarter, the meetings of the ICD-10 committee should be on a weekly basis with direct reports from the members. The priority goals should be presented first and all accomplishments recognized, pub-lished in the communication channel and sent to senior administration and the Board. As we know from the first two quarters (at least from this article), there are priority ele-ments that need to be concluded during this quarter. Some of items (but not limited to) from the first two quarters that need goal completion are:• Managed care contracts• End-to-end testing with all payers• Process flow implementations throughout
the organization• All documents, by-laws, encounter forms,
policies, procedures, etc. should be ready for October 1, 2015
• Pointed focus on the education and train-ing of all supportive staff in the data col-lection processes, i.e. ancillary depart-ments, surgical staff, CDI finalization, concurrent review finalization, etc.
• All backlogs need final focus and clean-up; outstanding payer denials; DNFB in both inpatient and outpatient; cash post-ing; over 90 day clean-up; etc.
• All champions (physician, ancillary, cod-ing) must give a report on their standing and where they see further focus needed
The meetings in June should directly re-port on the status of each goal. Some should be complete while others may continue on. The purpose of the status reporting is to identify where to put more effort to reach the desired goal/outcome before the end of the fourth quarter. This is a critical time to document the status and re-prioritize the in-ternal effort based on requirements need to complete a goal.
Fourth Quarter: (July through September)
This is it! Summer may be the hottest time of the year but the heat will most cer-tainly will be on if all of the projects are not complete and all of the goals met. This is the timeline to make sure any backlog support-ive help is in place and ready to go based on a phone call. It is the period to make sure that the physicians are accepting the documen-tation changes and also the time to identify if some physicians may need a support staff person after September 30th to make sure that all the documentation is collected at each patient encounter to ensure quality.
This quarter is the ‘hot’ quarter since it is that last timeline to be pro-active in your actions and make success the cornerstone of all activity. This quarter is also the reporting time to senior management and administra-tion of the successful activities that the en-tire ICD-10 committee has achieved. This last quarter should be categorized by the ‘green checkmark’ indicating the successful completion for each of the goals set forth a year ago.
With four successful quarters, October 1, 2015 equals one full dollar in reimburse-ment!
Rob Borchert can be reached at 315.345.5208 and [email protected] Borchert can be reached at 207.807.1922 and [email protected] Borchert can be reached at 703.328.3953 and [email protected]
Summer 2014 19
2014 AAHAM ANI
October 15-17, 2014Manchester Grand Hyatt
San Diego, California

20 The Journal of Healthcare Administrative Management
Jack SingerJack Singer, PhD, is a practicing Clinical/
Sport psychologist and a Professional Speaker, who has spoken for and consulted with hun-dreds of medical centers, private practices, and healthcare associations across the U.S. and Canada.
Dr. Jack has been a practicing Sport Psy-chologist for more than thirty years and takes the same skills he has taught to hundreds of elite athletes to develop the mindset of cham-
pions and will teach them to our AAHAM attendees.Dr. Singer is a frequent guest on MSNBC, FOX SPORTS NET, and oth-
er radio talk shows about his unique stress mastery techniques. Jack is also the author of four books, including “Dynamic Health,” along with Dr. Ber-nie Siegel and has published more than 170 professional articles, in medical, healthcare and business periodicals.
Because Dr. Jack knows that fun and entertainment are the pivotal ways to rivet attendee attention and retention, he always has his audiences roar-ing with laughter, while they absorb his proven prescriptions for shattering their self-limiting beliefs and unleashing their true potential. Dr. Jack’s never-ending passion is to show AAHAM the precise secrets for adding life to their years and years to their lives, both on and off their jobs.
So, buckle your seatbelts and get ready for an exciting ride as Dr. Jack Singer shows you “How to Develop the Mindset of a Champion.” For more information, please visit www.askdrjack.com
Sheryl Roush Sheryl Roush is a native San Diegan with
thirty-five years of helping people to get to the heart of communicating, rekindling the spirit and bringing positive change. She is the CEO of Sparkle Presentations, Inc. She has been awarded numerous speak-ing awards for enhancing global commu-nication and leadership from Toastmasters
International, National Speakers Association Greater Los Angeles Area Chapter and the San Diego Chapter. Twice crowned as “Ms. Heart of San Diego” for contributions to battered and homeless women and children in her community, Sheryl authored the Heart Book Series of inspirational books filled with original short stories, poems and quotations. She was also crowned “Queen of Hope” by The Crowns for Cure (breast cancer research).
Her books include: Solid Gold Newsletter Design; Sparkle-Tudes!®; Heart of a Woman; and Heart of a Woman in Business, Heart of a Mother and Heart of a Military Woman.
Some of her clients include: 7-Up, Abbott Labs, Alliance of the Ameri-can Dental Association (AADA), American Academy of Family Physicians (AAFP), Arizona Health Care Association (AZHCA), Arthur Ashe Wellness Center at UCLA, Association of Family Medicine Administrators (AFMA), Association of Records Management (ARMA), Healthcare Financial Man-agement Association (HFMA), International Association of Administrative Professionals (IAPP), Kaiser Permanente Physician Recruiters, National As-sociation of Professional Geriatric Care Managers, Oklahoma Department of Mental Health and Substance Abuse Services, Project Management Institute (PMI), Red Rock Behavioral Health Services, San Diego Zoo, Scripps Health Foundation, Sharp Healthcare, Social Security Administration, Southwest Airlines, The Chopra Center, UCSD Healthcare & Medical Center, U.S. Cen-sus Bureau, Victor Valley Medical Group.
For more information, please visit SparklePresentations.com
Alexandra Jaffe Alexandra Jaffe is a staff reporter at The Hill
newspaper. She covers House, Senate and the presi-dential campaigns for The Hill newspaper in Washing-ton, D.C. Born and raised in Chicago, she moved to Washington to pursue her love of politics and journal-ism. Her work has appeared in Roll Call, the Houston Chronicle, The Atlantic, National Journal and other publications. She is a frequent Fox News commen-tator and has appeared on the Bill Press Show, Sirius XM’s Press Pool, and various local Fox affiliates.
Featured Speakers

Summer 2014 21
DeVerl Austin Mr. Austin is a Senior Consultant with FranklinCovey Co., Speed of Trust Practice He has worked successfully in national and in-ternational markets. He was Director of the Stephen R. Covey and Associates Masters of Executive Excellence program that featured re-nowned speakers and was a top-ranked sales ex-ecutive and sales team leader for many years and also performed as a senior consultant coaching and training numerous executives representing Fortune 500 companies. Through his experi-ences, he knows first-hand what it takes for busi-nesses to transform themselves to achieve excel-lent results.
Dave Amann, MBA, CPAMr. Amann is Assistant Director for Banking Services at the Johns Hopkins Health System Treasury Management Services group. His du-ties include the administration of several bank-ing platforms, maintenance of the relationship with a credit card merchant bank, supervision of staff engaged in processing and recording transactions, and liaison with General Account-ing and IT. The most satisfying part of his posi-tion is the ability to influence the architecture of payment flows and accompanying reporting for a variety of different JHHS companies. He has been an employee of the Johns Hopkins Health System for almost twenty years rising from the position of staff accountant. Earlier career expe-rience includes public accounting and financial services sales. He earned his MBA from Loyola University in Maryland.
Virginia Berney, CRCE-I, P Ms. Berney has been Program Head for Medical and Coding and an Instructor at Anthem College in Minnesota. Her career has also included run-ning both operations and the billing office for an urgent care facility and was employed by Allina Clinics as Coding Educator Analyst at their Min-neapolis location. Virginia has been a member of AAHAM since 1989 and has held the position of Gopher chapter board member, Vice President, Certification Chair, and Editor for the Gopher Tracks. She has served as National Recertifica-tion Chair.
Christian Borchert Mr. Borchert is Patient Accounts Director at
Oneida Healthcare Center. He has over fifteen years of experience collaborating with and pro-viding consulting services to healthcare clients primarily in New York State. He has experience performing revenue cycle consulting services to hospitals, nursing homes and physician groups as well as selling revenue cycle technology. While addressing the day-to-day operations of the back-end of the revenue cycle for hospitals, clin-ics and nursing homes, he is also co-chairing the hospital’s ICD-10 implementation initiative and supports other committees with hospital admin-istration. He participates in several healthcare fo-rums and is an active participant in the Mid York chapter of AAHAM and the Central New York Chapter of HFMA.
Don BorchertDon is a Manager with PwC and has over fifteen years of healthcare experience in the Revenue Cycle. He has performed operational assess-ments for many large health systems as well as cash recovery programs. Don has been part of a team involving the full business process redesign of the Revenue Cycle flow for a multi-hospital health system. He has managed hospital staff during many different projects and has worked with computer vendors with the enhancement of system processes and procedures. He has also been interim senior management for large health systems.
Lorrie Borchert, MA, CRCE-I, CRCS, CPC Ms. Borchert is President of Best Practice Training Institute. She has over twenty years of experience in various revenue cycle roles. As an ICD-10 certi-fied coder and biller, she has played a valuable role in such areas as managing billing operations and interim management for healthcare facilities and physician practices. As a reimbursement analyst and coding auditor, she has been involved with both commercial audits and Veterans Adminis-tration third party contract reviews and rate veri-fications for the National Payer Relations Office. Lorrie is the Subject Matter Expert for the Depart-ment of Defense Uniform Business Office and conducts regular education and training sessions on revenue cycle issues for the Military Health Service. She has also assisted numerous healthcare institutions and physician practices with their ed-ucational and training components. She is a recog-nized speaker for many healthcare organizations.
Rob Borchert, MBA, CRCE-I, FHFMA Mr. Borchert is President of Best Practice As-sociates. He has thirty-five years of revenue cycle experience in the healthcare industry. He has performed full operational assessments, in-formation system evaluations, implementation of information systems and many other value-added projects. He has assisted clients negotiate third party payer contracts and has also imple-mented the operational activities to optimize the contract requirements. Rob is currently the Subject Matter Expert to the Department of Defense Uniform Business Office for revenue cycle enhancements within the three Armed Services. He is also Subject Matter Expert for the Veterans Administration Program Manage-ment Office regarding third party payor contract language and rate verification based on required legislation. Rob is a recognized speaker and has published numerous articles in the AAHAM na-tional journal and other healthcare publications.
Tim Borchert, MBA, PMP, CRCS-I Mr. Borchert is Deputy Director and Practice Leader for Altarum Institute, a non-profit gov-ernment contractor. He leads this practice in-volving the Uniform Business Office (UBO) for the Department of Defense as well as the Central Patient Accounting Centers (CPACs) for the Veterans Administration. He has assisted and led billing projects involving policy and pro-cedures for the Armed Services (Army, Navy, and Air Force). He has provided input into the collections practices for the UBO to improve their cash flow. For the Veterans Administration, he has led numerous projects involving collec-tions forecasting, A/R recovery projects, and the development of policies and procedures for their CPACs nationally. Tim has assisted with the implementation of kiosks in various Medical Centers and has also been part of the team for managed care contracting.
Rudy Braccili Jr., MBA, CRCE-IMr. Braccili is Executive Director, Revenue Cycle Services Boca Raton Regional Hospital where he is responsible for the Patient Access, Patient Financial Services, Revenue Integrity and Health Information Management opera-tions of this 400 bed acute care regional hospital. Prior, Rudy was the leader of Tenet Healthcare’s National Medicare & Medicaid Centers serving
General Session Speakers

22 The Journal of Healthcare Administrative Management
Tenet’s hospital facilities. Rudy led the success-ful business office centralization implementation at the North Broward Hospital District in Fort Lauderdale, Florida, where he served in various leadership roles. Rudy is a past President of AA-HAM’s South Florida chapter and has won sev-eral AAHAM & HFMA awards. He earned his MBA in Health Administration from the Uni-versity of Miami, and his undergraduate degree from Villanova University.
Lana Cabral, RN, BSN, MSM, CMACMs. Cabral is Senior Director, Case Manage-ment Clinical Revenue Cycle Services Division at Conifer Health Solutions. She brings more than twenty-five years of leadership experience in healthcare administration and consulting. An accomplished healthcare leader, her exper-tise includes utilization and case management, clinical transformation, program and outcomes management. Ms. Cabral has redesigned and implemented utilization and case management programs to support the efficient achievement of fiscal, clinical and quality goals. Her large-scale health system and payer initiatives include managing clinical projects, information sys-tem build outs and operations, and data-driven performance improvement activities. Ms. Ca-bral earned a bachelor’s degree in nursing from Thomas Jefferson University and a master’s de-gree in healthcare administration from Wilm-ington University. She is Case Management Ad-ministrator Certified (CMAC) by The Center for Case Management, Inc. and has been a fre-quent speaker at local, state, and national profes-sional and educational organizations.
Roberta Collins, CRCS-P, CRCP-P, CPC, CHCAMs. Collins is CEO of Advantage Billing Concepts and has over thirty years in the healthcare field. Roberta is a past AAHAM National Government Relations and past President of the AAHAM Go-pher chapter as well as holding other positions in the organization. She is an instructor in the Cod-ing Program at Hibbing Community College.
Doug C DewberryMr. Dewberry is Director of Business Develop-ment of Trubridge. Prior to joining Trubridge, Doug was a past CEO of a 218 bed facility in Al-abama. He also served as the CFO at that same
facility prior to being named the CEO. Previ-ously, he served as Business Office Director at two other facilities.
Doris Dickey, CRCE-IMs. Dickey is PFS Manager at Rochelle Com-munity Hospital. Her responsibilities include patient access, billing, collections, charge master and managed care contracting. She is also the Communications Team Leader at the hospital, leading the organization in following the stan-dards of behavior and developing excellent com-munication skills. She has worked in healthcare for over thirty-five years and has been an active member of the AA-HAM Illinois chapter for over thirty years and currently serves as National CRCS Chair and Chair of the Illinois chapter. Doris is a lifetime member of the AAHAM Illinois chapter and has been the recipient of the Charles Garvin Award locally and the Bill Spare Award nationally.
Tamora Ellis, CRCE-PTamora is Vice President of Client Relations at Advantage Billing Concepts and has over twen-ty-five years in the healthcare field. She currently serves as the chair of the AAHAM Gopher chap-ter as well as holding other positions in the local organization. She is Co-Chair of the Minnesota AUC Claims DD Tag group helping make deci-sions that affect us in our day to day workforce.
Joe GaldiJoe is Informatics Director at Thomas Jefferson Hospital. He is responsible for the support of all systems related to Patient Access, HIM, CDIS, and Business Services. Previously, he was a Rev-enue Cycle System Consultant in the Philadel-phia and New York metropolitan markets.
Steven M. GrossMr. Gross is CEO, Richmond Shared Services Center at Parallon Business Solutions. Previ-ously, he served as the Division Business Office Director for HCA’s Central Atlantic Division. Steven holds a BS degree from Virginia Com-monwealth University.
Katie Harwood, CHAMMs. Harwood is Manager of Patient Financial Services at the University of Utah healthcare. Katie’s current experience is in Financial Coun-seling and Authorization. She is the Treasurer
of the AAHAM Mountain West chapter and is CHAM certified through the National Associa-tion of Healthcare Access Management.
Steven F. Honeywell, MBA, CRCE-I, PSteven Honeywell is Senior Director of Patient Accounting for Professional Fee Billing at the University of Pennsylvania Health System (Penn Medicine). He has over twenty-eight years expe-rience in the physician billing arena, the major-ity of which has been in an executive level posi-tion at Penn Medicine responsible for running the Centralized Physician Billing Office that services over 1,500 physicians. Steven is on the Board of Directors for AAHAM’s Philadelphia chapter and is an active member of the Advisory Group for the Faculty Practice Solutions Center, PNC Healthcare Advisory Board and a leader of the Academic Practice Plan Associate Direc-tors organization. He is a nationally recognized speaker for these organizations. He obtained his undergraduate degree from Rutgers University and his MBA from LaSalle University.
Byron C. Johnson, MAOL, CHC, RHIA, CIRCC Mr. Johnson is a Director with Kohler Health-care Consulting and has over sixteen years of ex-perience in healthcare. He has led a wide range of projects involving healthcare regulatory compli-ance, revenue cycle, revenue integrity, litigation support, chargemaster, coding, billing, auditing, program integrity contractors, and the develop-ment and application of customized data analyt-ic and mining services for integrated healthcare systems, hospitals, physician practices, and other entities on the local, regional and national levels.
Previously, Mr. Johnson served as a Manager with Huron Healthcare as a cross-functional member of their Regulatory Risk & Compli-ance and the Non-Labor Operations Health-care Turn-Around Practices. He has served as an independent owner/operator of Kettner Moore Inc. consulting practice where he pro-vided critical support for hospital, physician, and healthcare clientele focused on compliance and reimbursement operations functions that successfully bridged clinical departments and revenue cycle initiatives.
Mr. Johnson holds a Master’s Degree in Organi-zational Leadership and a Graduate Certificate
General Session Speakers

Summer 2014 23
in Servant Leadership, a Graduate Certificate in Healthcare Compliance and Bachelor’s Degree in Health Information Management.
Chris Johnson, FHFMAMr. Johnson is Vice President of Revenue Cycle Management-Regional Facilities at Carolinas Healthcare System where he is responsible for oversight of the revenue cycle operations of re-gional healthcare facilities affiliated with the Healthcare System. Chris has over twenty-five years of experience in revenue cycle operations in sole community providers, an academic medical center and an integrated healthcare delivery sys-tem. Chris received his Bachelor’s degree in from Montreat College. Chris is a Fellow in the HFMA and an active member of the North Carolina chapter, where he has served in numerous leader-ship positions including Chapter President.
Jeffrey JohnsonMr. Johnson is Chief Sales and Marketing Of-ficer of Hawes Financial Group. He is a nation-ally acclaimed motivational trainer, speaker and facilitator and a veteran in the credit and collec-tions industry. Previously, Jeff was the Manager of Client Relations for Columbia Ultimate Busi-ness Systems and Director of the International Division of the FranklinCovey Leadership Cen-ter where he worked with Fortune 500 compa-nies to better improve their internal processes through pinpoint training. Jeff earned his degree in Business Management with a minor in Human Resources from Brigham Young University. He is a certified 7-Habits Trainer and has numerous professional memberships and currently serves as Secretary of the Oregon chapter of HFMA.
Joshua A. Johnson, CRCS-I, PJosh is the Director of Patient Financial Services at Gibson Area Hospital and Health Services in Gibson City, Illinois. His duties include man-aging the Patient Access Department and the Central Business Office. Josh specializes in Cus-tomer Service with emphasis on Patient Access, Pre-Registration, Insurance Benefits and Point of Service Collections processes. Josh is very ac-tive in AAHAM and is currently serving as Sec-ond Vice-President of the Illinois chapter
Lisa Killam, CPC Ms. Killam is the Patient Access/Revenue In-tegrity Manager at St Joseph Hospital in Bangor,
Maine and has over fifteen years of experience in various areas of the revenue cycle. She has been instrumental in developing a successful Patient Access Department over the past year and is cur-rently in the process of installing various products to automate functions that her team does on a daily basis. She also oversees the hospital charge master and acts as a liaison between the revenue cycle departments.
Kenny Koerner, MBA, CRCE-IKenny is the Director of Patient Accounts at CGH Medical Center in Sterling, Illinois. His du-ties include managing the Scheduling, Registra-tion, Billing and Managed Care Contracting for CGH Medical Center, CGH Home Infusion and CGH Homecare. Kenny has his undergraduate degree from Olivet Nazarene University and his MBA from St. Ambrose University. Kenny cur-rently serves as President of the AAHAM Illinois chapter and is active in the HFMA McMahon-lllini chapter.
Suzanne Lestina, FHFMA, CPCMs. Lestina is Vice President of Revenue Cycle Innovation at Avadyne Health. She executes strategies that lead the industry in next-genera-tion revenue cycle concepts. She helps custom-ers implement change to transform the revenue cycles and achieve positive outcomes. Suzanne has extensive revenue cycle experience, includ-ing revenue cycle consulting and hospital rev-enue cycle leadership roles in the Chicago area.Prior to joining Avadyne Health, Suzanne was HFMA’s director of revenue cycle MAP where she served as the technical expert and con-sultant for HFMA’s MAP product lines and
served in an advisory capacity regarding the technical aspects of revenue cycle performance improvement.
Mark MathiaMr. Mathia is the CEO & Executive Coach for Trident Coaching Systems & Tiburon Health-care Solutions Group. He is a certified coach, speaker and trainer and more than twenty years of leadership experience, has led business lead-ers to high levels of success, performance, and fulfillment. Mark’s passion for making a differ-ence in teams and leaders around the country is evident. In addition to coaching his own team-mates as the CEO of Tiburon Financial, Mark’s current role includes one-on-one executive coaching, executive retreats, speaking engage-ments and delivering personalized experiences for business leaders and teams with a focus on helping people to improve their performance in business and life. Mark has his undergraduate degree from Dana College and his MBA from Bellevue University.
Kevin McLaren, MPA, MSW, CMPE, CCS-P, CPCMr. is Associate Director of Revenue Cycle En-hancement at the University of California, San Francisco Faculty Medical Group. His respon-sibilities include leading initiatives to optimize revenue cycle performance, ICD-10 implemen-tation and integration of recently acquired and affiliated hospital and physician practices. He has worked in both the public and private sec-tors of the healthcare industry for over twenty years. Kevin is a UCSF subject matter expert in charge capture and clinical documentation
General Session Speakers
24 The Journal of Healthcare Administrative Management
Katherine H. Murphy, BA, CHAMMs. Murphy is Vice President of Revenue Cycle Consulting at Passport/Experian. She has over twenty years of experience in hospital revenue cycle management specializing in Access pro-cesses, redesign and implementation. As Access Director in a multi-facility Midwest health sys-tem, Katherine chaired the Registration Coun-cil and the Metropolitan Chicago Healthcare Access Committee. Katherine received her BA from Northern Illinois University and graduate Certificate from Benedictine University. She is an active member in NAHAM and HFMA.
John Ninos, MS, MT (ASCP), CCS Mr. Ninos is a Senior Manager with Kohler Healthcare Consulting. He has over thirty-five years of experience in the healthcare field, both on the provider and the payer side. He has led a wide range of projects involving chargemaster review, health care billing, coding, regulations, policy, fraud and abuse, and audits. He has been responsible for performing charge-master reviews, and coding and billing audits for both individual hospitals and corporate health-care entities and has worked with clients on a local and national level to provide support for billing and compliance issues, coding and bill-ing reviews. Mr. Ninos has worked in all facets of the Revenue Cycle, with specific emphasis in Charge Description Master (CDM), Process Improvements, Rates and Reimbursement and compliance.
Darren Parncutt, BSBAMr. Parncutt is a Senior Systems Analyst at Thomas Jefferson Hospitals. He is responsible for the support of systems related to Patient Access and Business Services. Previously, was a Systems Analyst. Darren earned his BSBA de-gree from Shippensburg University.
Sandra R Pawelk, CRCE-I, PMs. Pawelk is a Medical Billing and Coding AAS Degree and Diploma Program Head at Anthem College. She teaches courses in Healthcare Deliv-ery and Insurance Management, Reimbursement and Legal Issues, Professional Coding Practice, Medical Records and Documentation, Medical Office Procedures, Health Information Technol-ogy and Medical Billing and Coding. Previously, she was Director of Business Services, respon-sible for the activities of the patient financial ser-
vice department including billing, insurance, and follow up of patient accounts, compliance with third party payer regulations and audits, cash collections, customer service activities, vendor management, employee productivity and ongo-ing improvements to key revenue cycle indica-tors. She is an active member of the AAHAM Gopher chapter and serves as their certification chair and board member. Chad Powers, EsquireMr. Powers is Vice President and General Coun-sel at Medical Reimbursements of America. He manages the Legal Department and Compli-ance at MRA. In addition to his corporate legal responsibilities, Mr. Powers advises on opera-tional issues including managed care, ERISA, Medicare/Medicaid, MSP Compliance, work-ers’ compensation, third-party recoveries as well as HIPAA/HITECH compliance. Given the complexity of changes in healthcare, Mr. Pow-ers provides educational and training events to professional associations in the industry and to hospital employees nationwide. Mr. Powers is a licensed attorney and member of the Tennessee Bar Association.
Kimberley ScottMs. Scott is the Government Supervisor and Claims Resolution & Improvement Team Su-pervisor at Intermountain Healthcare. She is responsible for overseeing the day to day func-tions of billing, collections and audit’s for Medi-care as well as overseeing the Claims Resolution & Improvement Team to ensure corrected bill-ing and collections are done on accounts that were audited by compliance for overage or un-der charges on accounts. She is the Secretary and an active member of the AAHAM Moun-tain West chapter.
Franklin SmithMr. Smith is Director of Patient Financial Ser-vices at Calvert Memorial Hospital. His ex-tensive revenue cycle experience began on the payer side working the Blue Cross of Virginia. Previously, he was a healthcare consultant sev-eral large healthcare consulting firms. During his time as a consultant, he gained valuable experi-ence solving complex issues for institutions and physicians groups to help improve operations and performance.
Carolyn SwansonMs. Swanson is a Revenue Cycle Consultant with C. Swanson Consulting. She assists hos-pitals increase cash and improve processes throughout the revenue cycle. Previously, she was responsible for delivering superior custom-er service to and serving as point of contact for client hospitals throughout the United States and a Senior Director of Revenue Cycle services and a Patient Financial Services Director and held several Central Business Office director po-sitions. Carolyn is an active member of the Tex-as Bluebonnet chapter of AAHAM and serves as their education chair. She holds a Bachelor of Business Administration degree from Montreat College in North Carolina.
Michele Szymborski, CPHQ Ms. Szymborski is a Corporate Manager, Case Management Services at Conifer Health Solu-tions. She brings more than twenty-five years of healthcare leadership experience in the areas of case management, healthcare quality, patient safety, regulatory management, and health in-formation management. In her health system corporate leadership roles, Ms. Szymborski was responsible for managing transformation activi-ties for comprehensive care management and quality programs; incorporating workflow and process redesign, change management strate-gies, benefits realization, and technology en-ablement.
Julie VanPelt, CHFP, CPC, CRCE-I, CRCS-I, PMs. VanPelt is the Vice President of Operations at Avadyne Health Systems. She is responsible for the operations of revenue cycle manage-ment focusing on insurance follow up and self pay receivables in two locations working with over fifty acute care and critical access facilities in several states. She serves on the AAHAM Il-linois chapter Board of Directors and chairs the executive certification committee.
Judy I. Veazie, CRCE, CCTJudy is a Consultant/Project Manager/Interim Revenue Cycle at Childrens’ Oakland/ Univer-sity of California at San Francisco. She has over thirty years of experience in healthcare and has consulted extensively on the Revenue Cycle in-cluding HIM, accounts receivable, admitting, and charge master management. She has been
General Session Speakers

Summer 2014 25
the Editor for Aspen Press for over ten years, editing The Biller and writing a monthly column in The Healthcare Collector. She is a frequent speaker and has extensive teaching experience as an instructor for Edmonds Community College and Lower Columbia College with a concentra-tion in Medical Office Practice and HIM cur-riculum for Distance Education. She is an active member and serves on the AAHAM Evergreen chapter Board of Directors. She graduated from Marylhurst University in Portland Oregon with a BS in Business and Management.
Susan Walberg, JD, MPA, CHC Susan is a Vice President/National Director of Compliance at Kohler Healthcare Consulting. She has over twenty-five years of experience in the healthcare field, both on the provider and the payer side. Her experience includes medi-cal underwriting, contract and benefit analysis, and Part B audits and investigations. She has been a Regulatory Attorney and Privacy Officer for a large multi-state health system, responsible for the interpretation, analysis, and application/implementation of both state and federal laws including HIPAA and the Deficit Reduction Act, as well as policy development and imple-mentation. Susan analyzed contracts to ensure compliance with Stark and Anti-Kickback re-quirements, and provided education to corpo-rate and staff at the various entities on those top-ics as well as others. Susan was responsible for leading internal reviews and investigations, and directing overpayment situations. She collabo-rated closely with the business office, Informa-tion Security, Human Resources, Internal Audit, and other departments in order to ensure all im-pacted departments were fully aware in chang-ing laws, policies, and enforcement activity. She was also involved in responding to privacy and security breaches, and helped develop the re-sponse process and related policies.
Susan has also worked as the Corporate Com-pliance Officer in two health systems, and man-aged the staff and facility compliance activities in those organizations. She had oversight of the physician documentation and coding team, and was responsible for assisting those activities. She has both led and collaborated on attorney-client privileged audits and investigations, and has worked with a variety of regulators to response to their reviews. Recently, Susan worked with a sub-contractor under CMS, providing support
for fraud and abuse audits and policy analysis on Medicare Parts C and D.
Harriett Wall, MBAMs. Wall is a Senior Project Manager and Busi-ness Analyst at the Center for Healthcare Trans-parency, Network for Regional Healthcare Im-provement (NRHI). Ms. Wall is a versatile senior executive with over twenty years of achievement in growing healthcare consulting practices and delivering successful engagements. Harriett has held executive leadership positions in complex project management and consulting operations. Harriett brings expertise in clinical documenta-tion improvement, denials’ management, com-pliance, revenue cycle, and physician education. She is a proven facilitator of multi-disciplinary and executive teams; encouraging expression of diverse perspectives while fostering alignment of common goals. A few years ago, when health, work, and relationship factors collided, Harriett began her personal journey to better understand and manage stress. Harriett shares her experi-ences as well as well-researched information in a desire to help others manage stress. Harriett was awarded her BS in Physical Therapy from Northeastern University and her MBA from Harvard Business School. Harriett is a member of the HCCA and HFMA. She is an author and speaker on a range of industry topics.
Shauna Wardrop, CRCE-IShauna War/drop is the Director of Client Re-lations for Cardon Outreach. She is responsible for building successful business relationships with hospital administrative and management teams, in order to ensure clients are receiving the services committed to them and that com-munication lines are flowing smoothly. Previ-ously, she was employed by a large hospital organization where she started on the ground floor and worked up to be a Director in the Central Billing Office. She has a proven ability as a leader, innovator, organizer and trainer in Customer Service, Management and Compli-ance programs. Shauna attended Weber State University and is the President and an active member of the AAHAM Mountain West chap-ter and has served for many years in a variety of roles. She was the first recipient of the Bill Spare Award, awarded by National AAHAM. Shauna is also active in the HFMA and NAHAM orga-nizations and currently participates on several
boards and committees for the local chapters of these groups in various states.
Jimmy Watson Mr. Watson is Director of Patient Financial Services and Patient Experience at Providence Health & Services/Little Company of Mary Medical Center. He has more than twenty years of healthcare experience to include the clinical and non-clinical setting, having held positions in hospitals, home health and healthcare solution settings. Jimmy’s experience includes oversight of pbx/communications, scheduling, insurance verification, financial counseling, admissions, bed placement/patient throughput; pre-admit nursing, assistance with case management, pa-tient financial services and the patient experience for the hospital.
Ralph Wuebker, MBA, MDDr. Wuebker serves as Chief Medical Officer of Executive Health Resources. He provides clini-cal leadership and works closely with hospital leaders to ensure strong utilization review and compliance programs. Dr. Wuebker also over-sees EHR’s Audit, Compliance and Education physician speaking team, which is focused on providing onsite education for clinicians and hospital management. He works to help hospi-tals identify potential compliance vulnerabili-ties through ongoing internal audits. An expert in CMS regulations, medical necessity compli-ance, utilization review, denials management, and program integrity efforts, Dr. Wuebker is also an industry speaker and thought leader and editorial advisor to the media. He has been pub-lished in many prominent industry trade publi-cations and is an active participant and respect-ed source for industry discussion boards, blogs, and other social media. Dr. Wuebker has served as a hospitalist and instructor of medicine at Washington University School of Medicine and St. Louis Children’s Hospital. In addition to his work at EHR, he continues his clinical practice. Previously, he worked as Medical Director for the Midwest Region of Great-West Healthcare doing medical necessity case reviews. Dr. Wueb-ker earned his medical degree and a bachelor’s degree in biology from the University of Mis-souri-Kansas City School of Medicine and Mas-ter of Business Administration degree from the Washington University in St. Louis, Missouri.
General Session Speakers

26 The Journal of Healthcare Administrative Management
Professional Certification – Get your CEUs!Industry professionals on average, enjoy higher salaries and wages than non-
certified individuals. Remember, continuing education units (CEUs) are necessary to maintain your AAHAM certifications. Earn two (2) CEUs per each educational hour attended.
The AAHAM ANI offers the solutions you need to succeed, no matter what your challenge or experience level. With the ANI’s five distinct learning tracks and over 30 sessions, the ANI offers unparalleled education and training to meet every individual’s needs.
Tuesday, October 14th
6:00pm – 8:00pm
Registration
Wednesday, October 15th
7:30am – 5:30pm
Registration
9:00am – 11:00am
Certification Coaching Session “CRCE & CRCS Coaching Treasure Hunt”Roberta Collins, CRCS, CPC, CHCA, CEO, Advantage Billing ConceptsTamora Ellis, CRCE-P, Vice President Client Relations, Advantage Billing ConceptsSandra R Pawelk, CRCE-I, P, MBC Program Head/Extern Coordinator, Anthem CollegeVirginia Berney, CRCE-I, P Whether you are preparing to take the certifica-tion exams or just want to brush up on your skills, this session will take you through the certification topics and questions that tend to upset the waters. The instructors will calm the certification seas and assure attendees have smooth sailing when they are ready to take that voyage. Learn the material and knowledge needed to navigate comfortably at the helm.
12:00pm – 1:30pm
CRCE Certification Luncheon and Certification Awards PresentationAll CRCE certified members are invited to join us as we recognize our newly certified CRCE mem-bers and bestow special achievement awards. This luncheon is open to CRCEs only.
1:45pm – 4:15pm
Opening Keynote Session & Awards CeremonyKeynote Speaker: Jack Singer, PhD“Developing and Maintaining the Mindset of a Champion”Access to care, government regulations, rising costs, decreasing reimbursements, 501r & ACA challenges, staffing issues, all are facts of life these days for Healthcare Revenue Cycle professionals. The key ingredients for you to have consistent suc-cess in your career are to maintain an optimistic mindset and build psychological resilience to all of these challenges.
In this cutting edge keynote presentation, Dr. Jack will teach you the exact same skills he teaches elite, champion athletes to use in order to perform their best, despite their challenges and setbacks. You will learn how to recognize the self-talk that will lead you to either stress or success, how to identify and eliminate the self-limiting beliefs that cause your stress and how to employ a simple mental toughness routine to build resilience and remain optimistic, despite any challenges you face. 5:00pm- 6:00pm
First Timer & New Member Reception All new members and first-time ANI attendees are invited to join the AAHAM Board of Directors at a special networking reception in your honor.
6:00pm- 7:00pm
Welcome Reception in the Exhibit Hall Join your friends, colleagues and ANI exhibitors at the opening event of the ANI. Enjoy delicious appetizers as you tour our exhibit booths and learn about the latest products and services avail-able to our industry.
Thursday, October 16th, 2014
7:30am – 4:30pm
Registration
8:00am – 9:00am
Continental Breakfast in the Exhibit HallSponsored by Financial Credit Services/Med-max Financial Solutions
Start your day off right with delicious pastries and coffee while you visit with our exhibitors.
9:15am – 10:45am
KEYNOTE SESSIONSheryl Roush“How to Keep a Sparkling Attitude Everyday, How to Keep Your Sanity through Tides of Change” You’re doing more, with less. Taking on extra work and no spare time, conversations become short, tones get sharp, deadlines are tight, merg-ers, changes, oh my! How do you keep your sanity through it all? This lively, interactive program of-fers a little fresh ocean air, with tools to boost your attitude, simple stress management tips, and valu-able communication techniques to help set sails through the ebb and flow of challenging situations and dealing with difficult people.
Schedule of Events (tentative)

Summer 2014 27
11:00am – 12:30pm
CONCURRENT SESSIONS
MANAGEMENT/REVENUE CYCLE TRACK
“Operationalizing New Transparency Expectations and Requirements: The New Normal“Katherine H. Murphy, CHAM, Vice President Revenue Cycle Consulting , PassportLisa Killam, Patient Access/Revenue Integrity Manager, St. Joseph HospitalThis session will discuss communicating the complex process of pricing transparency re-quiring an understanding of physician, clinical, hospital and financial information as well as regulatory requirements. It’s not for the timid, yet certainly attainable. Transparency extends to the uninsured and insured whether sched-uled, shoppers, walk-in or Emergent. The trick is to provide a standard process to patients 24-7. Explore the new normal that will prevail as the industry moves forward with Afford-able Care and how to accomplish the call for change that comes along with it. Best practices in transparency are attainable and rewarding!
COMPLIANCE/SPECIALTY TRACK
“The Hidden Dangers of Billing Liability” Chad Powers, Vice President, Medical Reimbursements of America This session will provide an overview of the com-plexity of managing accident claims including best practices in billing, patient advocacy, and compliance for every patient and every payment source across the U.S. With the speaker’s legal and HIPAA expertise, the content presents insights to avoid legal issues while optimizing the reimburse-ments available to hospitals for accident claims. Much detail is provided regarding the challenges hospitals face in managing this unique financial class along with real-life examples of legal viola-tions and damages incurred in recent years.
ACCESS/QUALITY MANAGEMENT TRACK
“How to Make Self Pay Collections Work for Your Hospital”Franklin Smith, Jr., CRCE, Director, Patient Financial Services, Calvert Memorial HospitalDoug C. Dewberry, Director of Business
Development, TrubridgeThis session will focus on specific tools for a hospital to use to improve its collection of self-pay accounts. Franklin Smith will speak from the position of a hospital Patient Accounts Director that deals every day with struggles of the self-pay collection process. The presenta-tion will look at each of the following areas of the self-pay collection process: Preadmissions, Registration, Upfront Collections, Advance Beneficiary Notice, Charity Care policies, Bad debt Write-off, and Outside Collections, Doug Dewberry will give insight to this pro-cess from the view of a CEO and CFO.
LEADERSHIP/PROFESSIONAL DEVELOPMENT
“The Speed of Trust” DeVerl Austin, Senior Consultant, FranklinCovey Co. The Speed of Trust challenges our age-old as-sumption that trust is merely a soft, social virtue and instead demonstrates that trust is a hard-edged, economic driver, a learnable and measurable skill that makes organizations more profitable, people more promotable, and relationships more energizing. You’ll discover the powerful principles from the book, The Speed of Trust™ and learn about the 4 Cores of Credibility™ the 13 Behaviors of High Trust™ leaders, as well as measuring Trust Taxes™ and Trust Dividends™ within your team or organi-zation. Mr. Austin emphasizes that nothing is as fast as the speed of trust and that the abil-ity to establish, grow, extend, and restore trust with all stakeholders is the critical leadership competency of the new global economy.
SPECIALTY TRACK
“CRCS Certification: Creating A Program for Success” Julie VanPelt, CHFP, CPC, CRCE-I, Vice-President of Operations, Avadyne HealthKenny Koerner, MBA, CRCE, Director of Patient Accounts, CGH Medical CenterJosh Johnson, CRCS-I, P, Director of Patient Financial Services, Gibson Area Hospital & Health Services. This fast paced, interactive program will as-sist the PFS Manager looking to pursue CRCS certification whether on an individual basis or for their employees. A global review of success-ful coaching and programs will be followed by detailed study tips with particular emphasis
on the updates provides in the National AA-HAM CRCS Ex am Study Manual .
12:30pm - 2:00pmBuffet Luncheon in the Exhibit Hall Sponsored by HGS EBOS
Enjoy a delicious buffet luncheon while you visit and learn from our exhibitors.
2:00pm - 3:00pm
CONCURRENT SESSIONS
MANAGEMENT/REVENUE CYCLE TRACK
“Preparing for Health Reform-Improving Business Processes to Effectively Collect in a Consumer World”Suzanne Lestina, FHFMA, Vice President Revenue Cycle Innovation, Avadyne HealthThis session will discuss the impact of health reform on the revenue cycle and examine the organizational imperatives to help prepare for new regulations. As the traditional world of employment and benefits transforms into a new reality, the healthcare industry is facing significant changes. Insurance companies are
Tentative Schedule Continued

28 The Journal of Healthcare Administrative Management
covering less of the total hospital bill, with patient out-of-pocket expenses increasing. The complex issues of health reform are forc-ing healthcare systems to reduce costs while improving workflows and the patient experi-ence. Learn how to improve self-pay processes, including developing comprehensive up front patient communications and how with sound strategic planning; healthcare financial manag-ers can improve financial outcomes while cre-ating a positive patient experience.
COMPLIANCE/SPECIALTY TRACK
“Only an Ostrich Should Stick its Head in the Sand! A Practical Discussion on Marrying Compliance and Revenue Cycle Activities with Data Analytics” Byron C. Johnson, MAOL, CHC, RHIA, CIRCC, Director, Kohler Healthcare ConsultingJohn Ninos, MS, CS, MT (ASCP) Senior Manager, Kohler HealthcareThis session is designed to awaken and motivate revenue cycle professionals to proactively moni-tor billing and payment data on an ongoing con-tinual basis. This monitoring is accomplished through a “deep dive” into billing and payment transaction files in collaboration with the com-pliance officer program. The session will edu-cate the professional on how the government and its agencies contractors are utilizing your electronic transaction data to identify and then investigate your organization on an ongoing ba-sis (we can no longer pretend or hide from dan-ger; like an ostrich sticking its head in the sand). Learn about these electronic data sets, discuss how to obtain them, and how to utilize them in a monitoring and detection fashion. The session will cover examples of identified errors, the ap-propriate investigation process necessitated by the detection, and possible outcomes.
ACCESS/QUALITY MANAGEMENT TRACK
“Bookends of the Patient Experience: Little Company of Mary’s Improvement Strategies from Admission to Discharge” Jimmy Watson, Director, Patient Financial Services and Patient Experience, Providence Health & Services/Little Company of Mary Medical CenterIn this presentation, Little Company of Mary
Medical Center will share its strategies to im-prove the patient experience across the continu-um of care, from pre-service, to time of service to post-service activities. The session will share rev-enue cycle tools and processes used to stream-line patient access, coordinate patient care and conduct patient follow-up post discharge, all while monitoring patient interactions to ensure clear and accurate communication from the first point of contact to the last. Attendees will walk away with proven methods to impact patient ex-perience at their organizations.
LEADERSHIP/PROFESSIONAL DEVELOPMENT TRACK
“Managing Stress: Your Action Plan” Harriett Wall, Ms. Wall is a Senior Project Manager/Business Analyst, Center for Healthcare Transparency, Network for Regional Healthcare Improvement (NRHI)
This interactive session will provide a tool for attendees to assess stress in their lives utiliz-ing the Holmes and Rahe scale. There will be an opportunity to share scores and experiences. The session includes introduction to and practice of techniques to reduce stress and includes a brief, guided meditation. Attendees are given the op-portunity to develop a personal action plan to help to manage stress as part of the session.
SPECIALTY TRACK
“ICD10 In Practice, What Are We Going To Do?” Round Table DiscussionLisa Hennigan, CRCE-I, Senior Manager, Revenue Cycle, Western Psychiatric Institute and Clinic of UPMC Presbyterian ShadysideKenny Koerner, MBA, CRCE, Director of Patient Accounts, CGH Medical CenterBarbara Winwood, CRCE-I, Access Director, UPMC ShadysideJose Guevarez, Senior Vice President of Business Development, BCA Financial Services, Inc.Patt Lowe, Director Self-Pay & Charity, Texas Health ResourceThis round table will focus on the practical implementation of ICD10 from the front line provider’s perspective. Hosted by AAHAM members from the Education Committee, this session is designed to be an interactive discussion among all attendees on the issues that ICD10 poses for Patient Access, Central-
ized Scheduling, Authorization management, Specialized Billings, Contracting and Finance. The objective is to engage providers and iden-tify the areas that are the most problematic and discuss possible solutions.
3:15pm – 4:15pm
CONCURRENT SESSIONS
MANAGEMENT/REVENUE CYCLE TRACK
“Operationalizing & Optimizing a revenue Cycle Shared Services Model”Steven M. Gross, CEO, Richmond Shared Services Center The healthcare industry is rapidly adopting shared service models to improve efficiencies and effectiveness. Explore key considerations for migrating from a stand-alone revenue cycle environment to a shared services model. Hear about lessons learned from over twelve years of experience designing, managing and optimizing the industry’s leading shared services platform.
COMPLIANCE TRACK
“Optimizing Return on Hospital Medicare Bad Debt While Passing the Auditor’s Review”Rudy Braccili, Jr., MBA, CRCE, Executive Director, Revenue Cycle ServicesThe session will provide tips and best practice recommendations on how hospitals can en-sure maximum return on Medicare bad debts in a compliant manner such that submitted Medicare bad debt logs will pass the scrutiny of an auditor. A real life case study of a hospital which dramatically increased return on Medi-care bad debts through process improvement over a three year period. The session will pro-vide useful detailed information for hospital receivables managers to consider as they pre-pare annual Medicare bad debt logs
ACCESS/QUALITY MANAGEMENT TRACK
“Creative Data-driven Strategies to Improve Hospital Outcomes: A Case Manager’s Guide”Lana Cabral, RN, BSN, MSM, CMAC, Senior Director, Case Management/Hospital Case Management/Clinical Authorization Services.Michele Szymborski, CPHQ, Corporate Manager, Case Management Services, Conifer Health Solutions.
Tentative Schedule Continued

Summer 2014 29
This session will provide practical advice on how to best manage data to support the optimi-zation of hospital case management programs, and demonstrate the most effective tools to achieve desirable organizational clinical and financial outcomes. Case managers must develop the necessary data management skills in order to leverage in-formation in their decision-making processes, performance monitoring and the evaluation of outcomes. The enterprise-wide intelligence that case management information systems can deliver through their design, operations and reporting is of critical importance to any hospital-based case manager.
LEADERSHIP/PROFESSIONAL DEVELOPMENT TRACK
“Communication in a Sound Bit Generation”Judy Veazie, CRCE, CCT, Consultant, Project Manager, Interim Revenue Cycle Manger, Children’s Oakland/UCSFThis workshop provides insight into the root causes of some of our communications chal-lenges. Technology has transformed our work-place and our ability to communicate effectively has not kept up with the pace of this change. This session will explore written communica-tion and meetings/conference calls and will ex-amine participant’s communication styles and changes to the way they now do business.
SPECIALTY TRACK
“Windows Tips & Tricks”Joseph Galdi, CRCE-I, Informatics Director, Thomas Jefferson University Hospitals, Inc. Darren Parncutt, CRCE-I, Senior System Analyst, Thomas Jefferson University Hospitals, Inc. Learn Windows tips & tricks available in the Windows software environment. Attendees will be provided with a list of helpful Windows shortcut keys. Learn how to automate the re-trieval, reformatting, and delivery of reports using functions that readily available. Find out about various Excel functions that can help be more effective when using spreadsheets.
6:00 pm – 7:00 pm
President’s ReceptionAll attendees are invited to join AAHAM Presi-dent, Victoria Di Tomaso, CRCE-I, for a network-ing reception before the banquet festivities begin.
7:00 pm – 11:00pm
Annual Awards BanquetWine Sponsored by EOS CCA
Friday, October 17th, 2014
8:45am - 12:00pm
Registration
8:00am - 9:00am
Continental Breakfast in the Exhibit HallStart your day off right with delicious pastries and coffee while you visit with our exhibitors.
9:15am – 10:15am
CONCURRENT SESSIONS
MANAGEMENT/REVENUE CYCLE TRACK
“Managing Bad Debt Unmanageable Times”Chris Johnson, FHFMA, Vice President Revenue Cycle Management, Carolinas Healthcare System. Carolyn Swanson, Revenue Cycle Consultant, C. Swanson Consulting This session focuses on the flow from patient access through patient accounting and the need to use key tools in managing trends and outcomes of your bad debt. There are lots of takeaways with easy tools to use and ideas for each facility’s departments to assist in the re-duction of a hospitals bad debt results.
COMPLIANCE TRACK
“Fraud and Abuse; Current Trends and Enforcement Activities”Susan Walberg , JD, MPA, CHC, Vice President, National Director of Compliance, Kohler Healthcare Consulting , Inc.This session will review current healthcare fraud and abuse cases and enforcement trends, including areas that are planned areas for en-forcement by the Office of the Inspector Gener-al and current areas of enforcement focus. This session will provide an overview of the broad areas now under scrutiny and will also provide recommendations for key areas where health-
care providers should focus their resources to mitigate audit and enforcement risks.
ACCESS/QUALITY MANAGEMENT TRACK
“Registration Quality and Payment Estimator Tools: Lessons Learned”Kimberly Scott, Government Supervisor and Claims Resolution & Improvement Team Supervisor, Intermountain Healthcare The presentation will encompass the Revenue Cycle, Patient Access, Billing and Collections, and Revenue Cycle Management. It will step the attendees through what information is required at time of registration, information required for billing, and the insurance collection process.
LEADERSHIP/PROFESSIONAL DEVELOPMENT TRACK
“Be Incredible”Jeffery Johnson, Chief Sales & Marketing Officer, Hawes Financial GroupThis session will introduce you to the principles to help you change from ordinary into incred-ible. Within every human being are the makings of “incredible”. However, daily responsibilities tend to stop us from making that incredible hap-pen. The truth is that most people want to be incredible, but are often left wondering how to get started. Too many people focus on abstract ideas and advice, but do not come across spe-cific principles that allow them to start being incredible. Learn the steps to incredible!
SPECIALTY TRACK
“Managing Through the Maze of Current Changes; The Impact From the ACA and ICD-10 On the Revenue Cycle” (Part 1)Lorrie Borchert, MA, CRCE, CPAT, CPC President, Best Practice Training InstituteRob Borchert, MBA, CRCE-I, FHFMA, President, Best Practice AssociatesChristian Borchert, Patient Accounts Director, Oneida HealthcareDon Borchert, MBA, Manager, PwCTim Borchert, MBA, PMP, Deputy Director and Practice Leader, Altarum InstituteThis family team of experts consisting of fa-cilities directors, managers, and consultants will present the impact of the Affordable Care Act (ACA) from the focused view of: Clinical documentation for ICD10; Case mix changes;
Tentative Schedule Continued

30 The Journal of Healthcare Administrative Management
Medical necessity limitations; Insurance mas-ter file set up, etc.
Learn about ICD10 post implementation and preparation planning and testing, the impact date and lessons learned from both small and large facilities, as well as the goals of the ICD10 planning committee.
10:30 am – 11:30 am
CONCURRENT SESSIONS
MANAGEMENT/REVENUE CYCLE TRACK
“PFS Revenue Cycle Open Forum” Doris Dickey, CRCE-I, PFS Manager, Rochelle Community HospitalThis session will allow attendees from small to medium providers to network and discuss unique management issues related to providers under 150 beds. This will be an open, interac-tive session, allowing attendees to bring their current issues to the session to see how others are handling similar situations.
COMPLIANCE TRACK
“How to Best Navigate the CMS IPPS 2014 Final Rule: Recommendations from a Medical Necessity Leader”Dr. Ralph Wuebker, MBA, Chief Medical Officer, Executive Health Resources, Inc. The Centers for Medicare and Medicaid Ser-vices have proposed two separate rulings, 1455-P and 1599, which impact inpatient sta-tus determinations and systemic procedures for managing appeals. Hear insights from an industry-leading perspective in response to the August and mid-September 2013 updates, as well as the October 1 Final Rule and March 2014 update. Discussion will focus on what the new requirements mean in terms of potential course adjustment, and how they may impact patient quality of care in this time of transfor-mation for health systems and hospitals.
Learn about the the 2-Midnight Rule, Obser-vation vs. Inpatient Status, Certification and Rebilling and Physician Documentation Re-quirements.
ACCESS/QUALITY MANAGEMENT TRACK
“Surviving ACA Open Enrollment, Round 1”Katie Harwood, CHAM, Manager Patient Financial Services, University of Utah HealthcareShauna Wardrop, CRCE-I, Director of Client Relations, Cardon OutreachHear how the two presenters prepared for, and survived the 2013-2014 ACA Open Enrollment. Find out about their lessons learned, what went right, what went wrong and the impacts experi-enced in the Revenue Cycle and how to prepare for 2014 Open Enrollment, round 2. The experi-ences from this facility and others will offer ideas for managing and surviving those challenges, continuing to offer the best assistance to their patients and bringing much needed revenue to the facilities through these new programs.
LEADERSHIP/PROFESSIONAL DEVELOPMENT TRACK
“BANG!”Mark Mathia, MBA, CEO & Executive Coach, Tiburon Healthcare Solutions Group & Trident Coaching SystemThis session is a leadership driven session de-signed to encourage ethical leadership while teaching others to maximize individual and team performance. BANG! is a very interactive session that includes small group work and tai-lored workshop topics. This particular teaching is relevant to anyone who works in or around teams. The objective is to unpack the powerful idea that every leader can maximize their team’s potential by understanding the power behind personal development and its amazing ramifi-cations on team growth and development.
SPECIALTY TRACK
“Managing Through the Maze of Current Changes; The Impact From Listening to the Data Found in The Revenue Cycle” (Part 2)Lorrie Borchert, MA, CRCE, CPAT, CPC President, Best Practice Training InstituteRob Borchert, MBA, CRCE-I, FHFMA, President, Best Practice AssociatesChristian Borchert, Patient Accounts Director, Oneida HealthcareDon Borchert, MBA, Manager, PwCTim Borchert, MBA, PMP, Deputy Director and Practice Leader, Altarum Institute
This family team of experts consisting of fa-cilities directors, managers, and consultants will take apart the areas of the Revenue Cycle and focus on the impact of data found today and what data will be needed for tomorrow to manage an efficient and productive Revenue Cycle. Access management, ICD10 require-ments from scheduling on Medical manage-ment, clinical documentation requirements for ICD10 Patient Financial Services and managed care contracts
12:00pm-1:30pm
Buffet Luncheon in the Exhibit Hall Enjoy a delicious buffet luncheon while you visit and learn from our exhibitors.
1:30pm – 2:30pm
Panel Discussion, “After the ‘Big Project’ Dust Settles: Optimizing your Revenue Cycle Operations”Facilitator: Jean Hippert, Senior Vice President, Southeast Director, PNC HealthcarePANELISTS:Steven Honeywell, MBA, CRCE-I, P Senior Director of Patient Accounting, University of Pennsylvania Health SystemDave Amann, CPA, MBA, Assistant Director for Banking Services, Johns Hopkins Health SystemKevin McLaren, MPA, MSW, CMPE, CCS-P, CPC, Associate Director, Revenue Cycle Enhancement, University of California San Francisco Medical Group Academic Medical Center revenue cycle lead-ers including University Of Pennsylvania Health System (Penn Medicine) discuss experience with conversions, integrations and process improve-ments including optimizing processes for new information systems; impact of these events on revenue cycle metrics; and identifying/addressing the remaining automation gaps.
2:30pm – 3:00pm
Refreshment Break and Raffle Drawings
3:00pm – 4:00pm
Closing Keynote Session “Washington Update”Alexandra Jaffe, Staff Report, The Hill NewspaperJoin Alexandra Jaffee, the Hill Newspaper’s staff reporter for an informative session and a legisla-tive update.
Tentative Schedule Continued
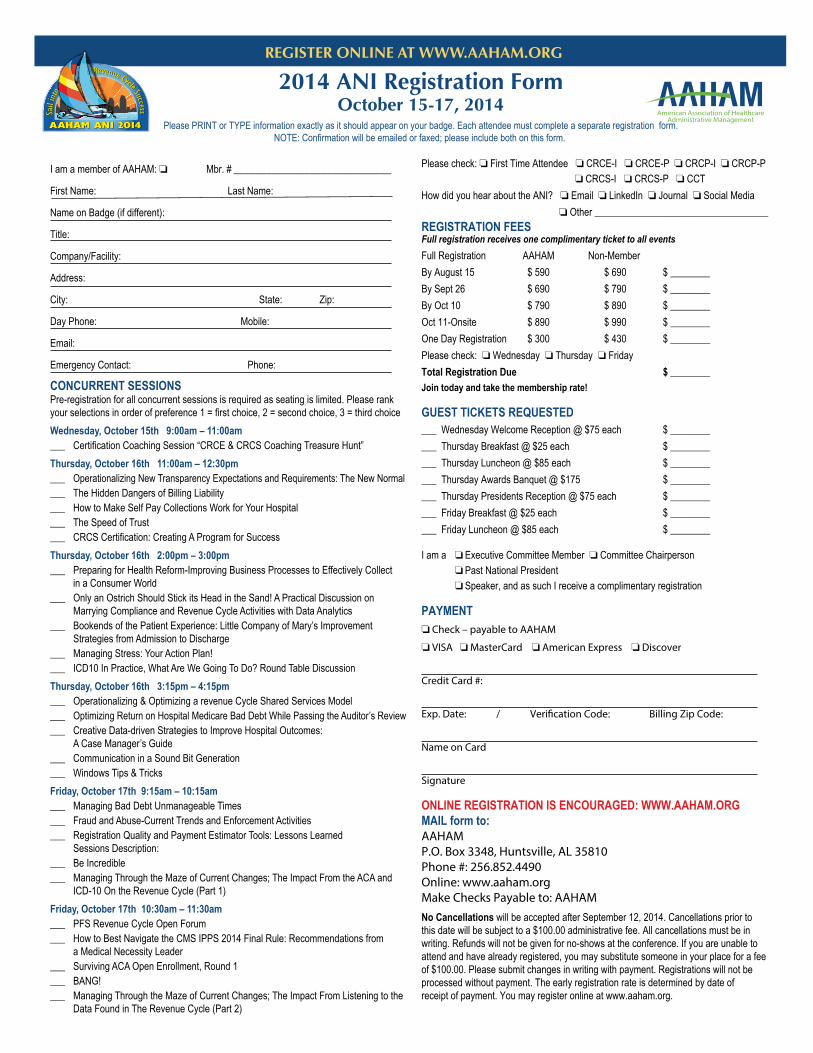
2014 ANI Registration FormOctober 15-17, 2014
Please PRINT or TYPE information exactly as it should appear on your badge. Each attendee must complete a separate registration form.NOTE: Confirmation will be emailed or faxed; please include both on this form.
I am a member of AAHAM: ❏ Mbr. #
First Name: Last Name:
Name on Badge (if different):
Title:
Company/Facility:
Address:
City: State: Zip:
Day Phone: Mobile:
Email:
Emergency Contact: Phone:
CONCURRENT SESSIONSPre-registration for all concurrent sessions is required as seating is limited. Please rankyour selections in order of preference 1 = first choice, 2 = second choice, 3 = third choiceWednesday, October 15th 9:00am – 11:00am___ Certification Coaching Session “CRCE & CRCS Coaching Treasure Hunt”Thursday, October 16th 11:00am – 12:30pm___ Operationalizing New Transparency Expectations and Requirements: The New Normal ___ The Hidden Dangers of Billing Liability___ How to Make Self Pay Collections Work for Your Hospital___ The Speed of Trust___ CRCS Certification: Creating A Program for SuccessThursday, October 16th 2:00pm – 3:00pm___ Preparing for Health Reform-Improving Business Processes to Effectively Collect in a Consumer World___ Only an Ostrich Should Stick its Head in the Sand! A Practical Discussion on Marrying Compliance and Revenue Cycle Activities with Data Analytics___ Bookends of the Patient Experience: Little Company of Mary’s Improvement Strategies from Admission to Discharge___ Managing Stress: Your Action Plan!___ ICD10 In Practice, What Are We Going To Do? Round Table DiscussionThursday, October 16th 3:15pm – 4:15pm___ Operationalizing & Optimizing a revenue Cycle Shared Services Model___ Optimizing Return on Hospital Medicare Bad Debt While Passing the Auditor’s Review___ Creative Data-driven Strategies to Improve Hospital Outcomes: A Case Manager’s Guide___ Communication in a Sound Bit Generation___ Windows Tips & TricksFriday, October 17th 9:15am – 10:15am___ Managing Bad Debt Unmanageable Times___ Fraud and Abuse-Current Trends and Enforcement Activities___ Registration Quality and Payment Estimator Tools: Lessons Learned Sessions Description:___ Be Incredible___ Managing Through the Maze of Current Changes; The Impact From the ACA and ICD-10 On the Revenue Cycle (Part 1)Friday, October 17th 10:30am – 11:30am___ PFS Revenue Cycle Open Forum___ How to Best Navigate the CMS IPPS 2014 Final Rule: Recommendations from a Medical Necessity Leader___ Surviving ACA Open Enrollment, Round 1___ BANG!___ Managing Through the Maze of Current Changes; The Impact From Listening to the Data Found in The Revenue Cycle (Part 2)
_____________________________ Please check: ❏ First Time Attendee ❏ CRCE-I ❏ CRCE-P ❏ CRCP-I ❏ CRCP-P ❏ CRCS-I ❏ CRCS-P ❏ CCT How did you hear about the ANI? ❏ Email ❏ LinkedIn ❏ Journal ❏ Social Media ❏ Other ___________________________________ REGISTRATION FEESFull registration receives one complimentary ticket to all eventsFull Registration AAHAM Non-Member By August 15 $ 590 $ 690 $ ________By Sept 26 $ 690 $ 790 $ ________By Oct 10 $ 790 $ 890 $ ________Oct 11-Onsite $ 890 $ 990 $ ________One Day Registration $ 300 $ 430 $ ________Please check: ❏ Wednesday ❏ Thursday ❏ FridayTotal Registration Due $ ________Join today and take the membership rate!
GUEST TICKETS REQUESTED___ Wednesday Welcome Reception @ $75 each $ ___________ Thursday Breakfast @ $25 each $ ___________ Thursday Luncheon @ $85 each $ ___________ Thursday Awards Banquet @ $175 $ ___________ Thursday Presidents Reception @ $75 each $ ___________ Friday Breakfast @ $25 each $ ___________ Friday Luncheon @ $85 each $ ________
I am a ❏ Executive Committee Member ❏ Committee Chairperson ❏ Past National President ❏ Speaker, and as such I receive a complimentary registration
PAYMENT❏ Check – payable to AAHAM
❏ VISA ❏ MasterCard ❏ American Express ❏ Discover
Credit Card #:
Exp. Date: / Verification Code: Billing Zip Code:
Name on Card
Signature
ONLINE REGISTRATION IS ENCOURAGED: WWW.AAHAM.ORGMAIL form to:AAHAMP.O. Box 3348, Huntsville, AL 35810Phone #: 256.852.4490Online: www.aaham.orgMake Checks Payable to: AAHAMNo Cancellations will be accepted after September 12, 2014. Cancellations prior to this date will be subject to a $100.00 administrative fee. All cancellations must be inwriting. Refunds will not be given for no-shows at the conference. If you are unable toattend and have already registered, you may substitute someone in your place for a feeof $100.00. Please submit changes in writing with payment. Registrations will not beprocessed without payment. The early registration rate is determined by date ofreceipt of payment. You may register online at www.aaham.org.
American Association of HealthcareAdministrative Management
REGISTER ONLINE AT WWW.AAHAM.ORG
32 The Journal of Healthcare Administrative Management
meet a committee chair
Q: How long have you been a national member?
A: Since I was about 10 years old, I became a member in 1987
Q: How did you get where you are today professionally?
A: I’ve worked for some really great leaders who taught me the ropes and gave me the opportunity to learn from doing and allowing me to belong to organizations such as AAHAM
Q: What made you decide to become certified?
A: My friend, Betty Burch Marschang worked in a hospital about 45 miles away. She encouraged me to get involved in AAHAM and to become certified. We did our certification study sessions together.
Q: What advice do you have for members that want to move up in their current healthcare careers?
A: Keep involved and informed in the industry. Read, read, read and know your counterparts in other facilities doing the same job. Other PFS Managers are some of my greatest resources of knowledge.
Q: What is your spouse’s name and occupation?
A: My husband Bud is retired and is a partner in a trucking company
Q: What are your children(s) names, ages and occupations?
A: Clint is 36 years old and is a heavy equipment operator. Shannon is 33 years old and works for Nestle. Between them, we have 4 beautiful grandchildren. Two boys and two girls: Allison (8), Ashley (6), Brock (3) and Luke (5).
Q: What was the last book you read? A: If it wasn’t work related, I probably read
a romance novel. But I couldn’t tell you which one. I don’t get to read for pleasure as much as I’d like to.
Q: What is your indulgence? A: I am probably going to regret admitting
this, but it’s playing Candy Crush or Pepper Panic on my cell phone
Q: What was your first job? A: I worked for a tax accountant, I was 16
years old and hand typed tax returns using Correct-Type and carbon paper. I was not very good at it!
Q: What did you have for breakfast today? A: Oatmeal and Diet Coke from
McDonalds
Q: Where did you spend your last vacation?
A: Just a few weeks ago, I had a week off work. I spent a great deal of time sitting on the back deck enjoying the weather with a few days of retail therapy thrown
in for good measure.
Q: What do you never leave home without when you travel?
A: Comfortable shoes and my cell phone
Q: I still can’t quite get the hang of....A: Line dancing and Twitter Q: What is your favorite way to celebrate
after you’ve completed a demanding project?
A: Nachos and margaritas
Q: Name something about you that most people don’t know.
A: I’ve worked for the same employer for 41 years. Remember I was 10 when I joined AAHAM.
Q: What do you know now that you wish you’d known when you were younger?
A: How much better I feel going back to work the day after getting a manicure and pedicure. Seriously, I should have known not to sweat the small stuff. I’m sure I spent too much time both professionally and personally, worrying about things that didn’t really matter.
The world would be a better place if only.... Everyone paid it forward. n
Doris Dickey, CRCE-I, CRCS Certification Chair
CRCS–I - Certified Revenue Cycle Specialist – Institutional
CRCS–P - Certified Revenue Cycle Specialist – Professional
AAHAM certifications can give you a powerful competitive advantage with employers. Certifications demonstrate that you have mastered the common body of knowledge for your profession. AAHAM Study Manuals will help assist you in preparing for AAHAM certification programs. These manuals are the gateway to studying for and passing these exams. The manuals include review questions and study tips.
Log on to www.aaham.org for more information and to order your Exam Study Manual today!

34 The Journal of Healthcare Administrative Management
from the desk of the certification director
Maria LeDoux, CAE
2014 AAHAM Certification Calendar
August 11-22, 2014Certification exam period
September 2, 2014Registration deadline for
November certification exams
November 10-21, 2014Certification exam period
December 1, 2014Registration deadline for
February 2015 exams
The August certification exam period is August 11-22, 2014. The November exam period is November 10-21, 2014. Please mark your calendars for the deadline to reg-ister for the November exam period is Sep-tember 2, 2014.
This summer, AAHAM and top CRCE coaches will hold the popular four part we-binar study program for the AAHAM Cer-tified Revenue Cycle Executive (CRCE-I, P) exams. This series is valuable whether you are planning on taking the CRCE ex-ams or just preparing for the future. You can also order the sessions on CD ROMS.
Those who take this popular series have had a higher pass rate than those who do not.
We will cover the four parts of the exam in the four part series: • Patient Access: July 18, 2014 • Billing: August 1, 2014 • Credit & Collections: August 15, 2014• Revenue Cycle Management: August 29,
2014
And…Brand new this year! AAHAM CRCP Certification Training Webinars
AAHAM and top CRCP coaches will
hold a four part webinar study program for the AAHAM Certified Revenue Cycle Pro-fessional (CRCP-I, P) exams. This new se-ries can help you whether you are planning on taking the CRCP exams or just preparing for the future. You can also order the ses-sions on CD ROMS.
We will cover the four parts of the exam in the 4 part series: • Patient Access: September 11, 2014 • Billing: September 25, 2014 • Credit & Collections: October 9, 2014• Revenue Cycle Management: October
23, 2014
Continuing Education Units (CEUs)CRCE
The new two year reporting cycle began on January 1, 2014 and will run through December 31, 2015. Make sure you submit your paperwork for the required number of CEUs to maintain your AAHAM CRCE cer-tification.
CRCE certificants are required to earn 40 CEUs over the 2 year period (20 of those must come from AAHAM sponsored events). AAHAM national membership must also be maintained in order to keep your CRCE des-ignation. You can find out how many CEUs we have recorded for you on the AAHAM website, CRCE CEU status section.
CRCP The two year reporting cycle began on
January 1, 2014 and will run through De-cember 31, 2015. Make sure you submit your paperwork for the required number of CEUs to maintain your AAHAM CRCP cer-tification. CRCP certificants are required to
earn 30 CEUs over the 2 year period (15 of those must come from AAHAM sponsored events). AAHAM national membership must also be maintained in order to keep your CRCP designation. You can find out how many CEUs we have recorded for you on the AAHAM website, CRCP CEU status section.
CRCSCRCS examinees can maintain their certi-fication with CEUs by joining as a national member of AAHAM rather than retesting every three years. They also have the option of testing every three years for those that opt not to join AAHAM at the National level. National members are required to earn 30 CEUs in the 3 year period (15 of those must come from AAHAM sponsored events) and maintain national membership in order to keep your CRCS designation. You can find out how many CEUs we have recorded for you on the AAHAM website, CRCS CEU status section.

Summer 2014 35
from the desk of the certification director
CCT Renewal using CEU’sBeginning June 1, 2014, you have the
option to retain your Certified Compliance Technician (CCT) certification by meet-ing a CEU and membership requirement. Originally, the CCT Certification required a retake every three years. The Executive Com-mittee and the Certification Committee have determined this is no longer necessary if con-tinued education and membership require-ments are met.
In order to qualify for recertification, you must:1. Be a national member in good standing
2. Submit 20 hours of continuing education units (CEUs) during a three year period (10 those credits must be AAHAM spon-sored events)
If you are dual certified; CCT and CRCE/CRCP/CRCS; The CEUs you sub-mit for those certifications may also be used toward your CCT CEUs.
If you are not currently a national mem-ber, you will need to become a national AA-HAM member by December 31, 2014, in order to maintain your CCT certification through CEUs and national membership. If your CCT certification expires in August or November 2014, then you will need to be-
come a national AAHAM member by your certification expiration date, and submit the required number of CEUs by your certifica-tion expiration date.
The recertification contact for all cer-tifications is Amanda Leibert, Certification Manager, [email protected]. You can download a CEU reporting form from the AAHAM website. Submit your CEUs by mailing the completed form to:AAHAM CEUsAmanda Leibert, Certification Manager11240 Waples Mill Rd Suite 200Fairfax, VA 22030
Congratulations to those who earned their CRCE certification in May: Maryland #13 Kate Austin, CRCE-I Lauren Kelly, CRCE-I Wendy Tricarico, CRCE-P
Virginia #27 Roderick Walker, CRCE-I
Philadelphia #29 Michele Ferguson-Davis, CRCE-P Kim Stadulis, CRCE-P
Chennai #49 Reema A., CRCE-P Vigneshwaran R., CRCE-P Swaminathan S., CRCE-P
Unassigned #99 Heather Judd, CRCE-I
Congratulations to those who earned their CRCP certification, in May:
Aksarben #01 Jenni McConville, CRCP-I
Gopher #06 Heather Elwood, CRCP-I
Joy Joens, CRCP-I MaReeNa Lor, CRCP-P Heather Rickgarn, CRCP-I Rebecca Thompson, CRCP-I Tina Uhrbom, CRCP-I Liz Villeneuve, CRCP-I Katy Vos, CRCP-P Betty Westbrook, CRCP-I
Hawkeye #07 Carrie Kuennen, CRCP-I
Illinois #09 Mary Garbe, CRCP-I
Inland Empire #10 Rosie Hartmann, CRCP-P
Keystone #11 Sue Fasnacht, CRCP-I Deborah Moyer, CRCP-I Alisha Rohrer, CRCP-I
Maryland #13 Donna Crane, CRCP-I Lori Freedman, CRCP-I Nicholas Miskelly, CRCP-I Amy Weber, CRCP-I Megan Wines, CRCP-I
Northeast PA #19 Tina Zukowski, CRCP-P
Rocky Mountain #21 Kristi Schibi, CRCP-P
Rushmore #23 Lisa Nolen, CRCP-I Amber Vanderwal, CRCP-I
Western Region #26 Elizabeth Velasquez, CRCP-I
Virginia #27 Norma Colato, CRCP-P Pamela Cornell, CRCP-I
Philadelphia #29 Darlene Holman, CRCP-P DuEwa Johnson, CRCP-I Renee Tippens, CRCP-P
Three Rivers #39 Barbara Carroll, CRCP-I Krystal Howard, CRCP-I
Music City #53 Ronald Washington, CRCP-I
Stephen Brooks, President and member of the AAHAM Music City chapter has accepted a new position as Director of Business Development with Connolly Healthcare. Way to go Stephen!
Christine Stottlemyer, CRCE-I, Chair of the Board and member of the AAHAM Keystone chapter, Stottlemyer is now Director of Patient Administrative Services at Wellspan. Congratulations Chris!
Movers & ShakersJohn Currier, CRCE-I, AAHAM 2nd Vice President, Congressman Courtney, Democrat, 2nd district, Connecticut, Steve Markesich, CRCE-I, President of the Connecticut chapter

36 The Journal of Healthcare Administrative Management
CRCS certification corner
The CRCS Committee has completed the updates to the CCT exam. We are
looking forward to moving on to the CRCS review next. We are excited about the ANI session with members Kenny Koerner, Josh Johnson and Julie VanPelt. They will be pro-viding a session on studying for the CRCS exam. They do a great job of covering all the topics. If you are unsure of what to study or where to start, try attending this ANI ses-
sion in October.I want to encourage anyone on the
fence about certification, to jump and in-vest in your career. There are so few college courses that can prepare you and improve your knowledge in the financial aspects of healthcare like AAHAM’s certification. Even if your employer is unable to financially sup-port your efforts you still need to meet this challenge. With all the mergers and acqui-
sitions happening in healthcare these days, certification will go a long ways in your per-sonal success in this business.
Just jump! You may have to test more than once to past, but so what? Who cares? The final success of passing will be worth all your effort. It probably isn’t as hard as you think it is! n
Certified Revenue Cycle Specialist
By Doris Dickey, CRCE-I
CRCP certification corner
Brenda Chambers, CRCE-I,PTechnical Certification Chair
Certified Revenue Cycle Professional
The CRCP Committee continues to meet monthly. We have so much going
on with both the CRCP and CRIP certifica-tions and that is a wonderful thing for you!
One of the most exciting things we are working on is an upcoming webinar series for those individuals interested in taking the CRCP exam. The webinar is a four part se-ries. You can sit in on all four parts or you can just sit in on one. The dates and times have been scheduled and are listed below:
September 11, 2014 – 1:00 – 2:30 EDT on Patient Access
September 25, 2014 - 1:00 – 2:30 EDT on Billing
October 9, 2014 - 1:00 – 2:30 EDT on Credit & Collections
October 23, 2014 - 1:00 – 2:30 EDT on Revenue Cycle Management
The committee is also reviewing the questions for the CRCP exam to make sure they are appropriate and comprehensive. We are constantly working to improve the exams to make them the absolute best and well respected. In addition, the CRCP manual is being reviewed to have any up-dated information added.
The CRIP (Certified Revenue Integrity Professional) certification continues to be worked on as well. Test questions are now
being developed. We are excited to have this exam and study manual completed and to offer the first exam in February of 2015. Is it hard? Oh yes it is! You must study for this exam and know the revenue cycle well. It’s all about services offered to patients and the proper way to charge. It is educational to say the least and will be a great resource for any-one to use.
As always, we try to bring our best in certification to you. Should you have any questions related to the CRCP or the new CRIP exam, please don’t hesitate to contact me. I am always here for you. n

Summer 2014 37
CRCE certification corner
I don’t know about the rest of y’all, but I’m pretty sure summer is here and I know
things are heating up!Now if you thought the weather was
hot, just wait, it’s even hotter on the AA-HAM certification front because we are roll-ing out the annual CRCE Summer Webinar series. This is a four-part series focused on getting you ready to take the Certified Rev-enue Cycle Executive (CRCE) certification exam.
Each session will focus on one section
of the exam: Patient Access, Billing, Credit & Collections, and Revenue Cycle Manage-ment. We will:• Discuss the exam format• Share study and test-taking tips• Highlight important study topics• Review formulas and calculations• Practice using sample test questions• Have fun
The webinar series is just one of the many tools available to you as you study
and prepare to sit for the exam. It is also a good way to update and refresh your skills. I want you to feel supported. I want you to feel prepared. I want you to be successful. But most of all, I want you to experience the sense of accomplishment you get when your letter comes saying you’ve passed and you join AAHAM’s elite CRCE group. You can do it and we are all here to help you be a sizzling success. n
Certification is HOT, HOT, HOT!By Erin Selin, CRCE-I,CCT
CRCS–I - Certified Revenue Cycle Specialist – Institutional
CRCS–P - Certified Revenue Cycle Specialist – Professional
AAHAM certifications can give you a powerful competitive advantage with employers. Certifications demonstrate that you have mastered the common body of knowledge for you profession. AAHAM Study Manuals will help assist you in preparing for AAHAM certification programs. These manuals are the gateway to studying for and passing these exams. The manuals include review questions and study tips.
Log on to www.aaham.org for more information and to order your Exam Study Manual today!
38 The Journal of Healthcare Administrative Management
from the desk of the membership director
Welcome New Members
Moayad ZahralddinAAHAM
Membership Director
Aksarben Chapter Sara Kloepping
Referred By: Jennifer Verbeck
Carolina Chapter Timothy Hill
Florida Sunshine Chapter Samara Chisholm
Referred By: Linda SayreShelba Dunlap Noemi Madera Brenda Williams
Gopher Chapter Debra Broitzman
Referred By: Sharese Haddy
Hawkeye Chapter Wendy St. Hilaire
Referred By: Laurie GaffneyKim Willson
Referred By: Carrie Kuennen
Illinois Chapter Cindy Collins Shauna Kramer
Referred By: Ken Koerner, CRCE-I
Jessica Martinez Greg Swedberg
Indiana Chapter Cassidy Bolen,CRCS-I
Referred By: Phyllis Stevens, CRCE-I
Pamela Fisher, CRCS-IReferred By: Phyllis Stevens, CRCE-I
Stephanie Skiles, CRCS-I
Keystone Chapter Donna Beaudoin
Referred By: Christine Stottlemyer, CRCE-IContinued on page 40
As you know, AAHAM has launched a very new and different version of the website in January. As technology is ever changing, we felt it was time our website grew up a little bit, not just aesthetically but also in content
and functionality. Our goal has always been to provide the highest level of service for our members, and we real-ized it was time to bring a high level of service to our website too.
We updated the site with user experience firmly in mind. One of the primary goals was to design the website using the latest technology so the site is compatible with today’s browsers and mobile devices. To improve on our past website we upgraded many of our current features including our social media plugins, blogs, calendar, member listserve, job line, and photo galleries. Some of our new functions include access to our local chapters via Google maps and an integration of our member’s only section with our online store.
To keep things consistent, we laid out the majority of the content of the site to be identical to the old site based of the “major” category heading, i.e. certification, membership, events, etc. For instance, if you’re looking for the Journal, the member listserve, the member directory, photo galleries from our events, the current and archived issues of the journal, archived handouts of the webinars, our member affinity programs, etc., they are all still in the member’s only section.
We plan to continue adding content and features to the site and are always interested in your feedback and ideas. We will continue to keep current with changes in technology so you can build your valuable relationships with other healthcare professionals and gain essential knowledge along the way.
I will be adding a “did you know” item specific to the website and some of our new technologically related changes to the Journal, National News, and on our social media outlets.
Thank you for letting me serve you, and I hope to see you all in San Diego for the ANI!
Did you know?Some of the menu items for members only benefits, including the list serve and jobline, are only available
when you are logged into the site.

AAHAM Certifications Offer You Solid Steps to your Professional Success:Certified Revenue Cycle Executive-I (CRCE-I)Formerly known as the Certified Patient Account Manager (CPAM) for directors and executives
Certified Revenue Cycle Executive-P (CRCE-P)Formerly known as the Certified Clinic Account Manager (CCAM) for directors and executives
NEW! Certified Revenue Cycle Professional-Institutional (CRCP-I) For mid-level managers
Certified Revenue Cycle Professional-Professional (CRCP-P) For mid-level managers
Certified Revenue Cycle Specialist-I (CRCS-I)Formerly known as the Certified Patient Account Technician (CPAT) for front-line staff
Certified Revenue Cycle Specialist-P (CRCS-P)Formerly known as the Certified Clinic Account Technician (CCAT) for front-line staff
Certified Compliance Technician (CCT) for compliance professionals
American Association of HealthcareAdministrative Management
40 The Journal of Healthcare Administrative Management
CRCE–I Certified Revenue Cycle Executive – Institutional
CRCE–P Certified Revenue Cycle Executive – Professional
Certification opens the door to the possibility of career advancement. Earning an AAHAM certification demonstrates that you have mastered the common body of knowledge for your profession. Sitting for these exams requires commitment and dedication. The CRCE–I,P Exam Study Manual will help assist you in preparing for the CRCE–I,P Exams.
Written by AAHAM, for AAHAM’s own certification programs ensures that this manual is the gateway to studying for and passing these professional exams. Included in the manual are chapter review questions and study tips. Log on to www.aaham.org for more information and to order your Exam Study Manual today!
Maryland Chapter Indiria Jeffries Sandra John
Referred By: Joyce BrooksKim Kirby, CRCS-I Dianna Lautar
Mid- York Chapter Elizabeth Testani
Mountain West Chapter Robert Carlile Chelsea Harris
Referred By: Shauna Wardrop, CRCE-IRachael Sheltra
New Jersey Chapter Manju Yadav, CRCS-I
Referred By: Claudia Gordon
Philadelphia Chapter Helena Frankowski, CRCS-I
Referred By: Holly CresswellShai Gardellis
Christina Gibbons, CRCS-IReferred By: Holly Cresswell
Antoinette Hartwell, CRCS-I Christine Shorter, CRCS-I,P
Pine Tree Chapter Cynthia Corey, CRCS-I
Rocky Mountain Chapter Aaron Knutson
Texas Bluebonnet Chapter Jonika Williams
Virginia Chapter Shannon Bartley, CRCS-I
Referred By: Chris Fisher, CRCE-IMarwa Elhassa Andrea Howell,CRCS-I
Referred By: Chris Fisher, CRCE-IPiper Neddenien
Referred By: Debra Reese
Western Region Chapter Joleen Bond-Livingston Tina Peterson Karen Schindler
Referred By: Kathi AtheyDenise Stark
Western Reserve Chapter Amy Goetz
States Without a Chapter Kathleen Puziak
continued from page 38
Coaching Kits
With the new AAHAM Coaching Kits, you are equipped toconduct interactive, thorough,and effective sessions to prepareparticipants for their CRCE–I,Por CRCS–I,P exam.
Each kit, packaged in a convenient binder, includes:• Detailed preparation instructions,
including a materials checklist• Overview of the adult learning
principles built into the kit• Scheduling suggestions so you
can customize your timetable• Tips and suggestions for
facilitating each portion of the coaching session
• CD with slides to guide participants through the session
• Materials and instructions for activities including laminated cards for learning games, quizzes, a crossword puzzle, and more
• Participant guide originals, so you can make copies and include as many exam-takers as you would like
• Extensive glossary of terms included in the exams
Each coach will need one copy of the CRCE–I,P or CRCS–I,P Exam Study Manual (sold separately).
Log on to www.aaham.org for more information and to order yourExam Study Manual today!
AAHAM Providing Excellence in the Business of Healthcare
Certification, Compliance, Leadership Development, Networking, Advocacy
AAHAM… Providing Excellence in the Business of HealthcareCertification • Compliance • Leadership Development • Networking • AdvocacyCutting Edge Training + Nationally Recognized Certification = Improved Performance
Application For National Membership
Name: ___________________________________________________ Title: ___________________________________________________
Employer/Organization Name: ________________________________________________________________________________________
Primary Address: _______________________________________ City: _______________________ State: __________ Zip: ____________
Phone: _____________________________ Fax: _____________________________ Local Chapter: _______________________________
E-mail Address: ______________________________ Website: _____________________________________________________________
Home Address: ___________________________ City: ______________ State: _____ Zip: _______ Home Phone: ____________________
How did you hear about AAHAM? o Colleague o Publication o Website o LinkedIn o Facebook
If referred by AAHAM member, please give name: _________________________________________________________________________
Membership Type: o National Member o Student Member
Payment OptionsFor Credit Card Payment: o AMEX o VISA o MASTERCARD
Card Number: __________________________________________ Exp: __________
Name as it appears on card: ___________________________ CVV2 Code: _______
Signature: ____________________________________________________________
Billing Address, If Different from Above: _____________________________________
____________________________________________________________________Please allow two weeks for processing after your application is received at the na-tional office. Dues are not tax deductible as a charitable contribution, but may be as a business expense.____________________________________________________________________Please note: Membership is on an individual, not institutional, basis and is non-trans-ferable.
For Check Payment:Please make checks payable to AAHAM and send application with your payment to:
AAHAM Membership11240 Waples Mill Road, Suite 200Fairfax, VA 22030AAHAM Tax ID# 23-1899873
Your Payment Total:
National Dues: $ __________
Local Dues: $ __________
Total Enclosed: $ __________
NATIONAL MEMBERSHIP - The fee to become a National member is $175. If you join anytime between July 1st and August 31st, the dues are $140 for the rest of the current year. If you join between September 1st and December 31st, the fee is $210 for the rest of the current year and all of the following year. STUDENT MEMBERSHIP - The student membership fee is $50. If you join between July 1st and August 31st, the pro-rated dues are $35, and if you join between September 1st and December 31st, dues are $65 (for 15 months of membership). To qualify for student membership you must currently be taking 6 credit hours per semester. Student members receive all the benefits of membership with the exception of voting, eligibility for professional certification, and cannot be a proxy for a chapter president at any national board meetings. Retired Membership – The retired membership fee is $50.00. To qualify for retired membership you must have been a National Member retired from healthcare. Retired mem-bers receive all the benefits of membership with the exception of voting.
Please Check the Appropriate Codes in Each Category Below
Years in Healthcare:o 0-5 o 6-10 o 11-20 o 21-25 o 25+
Certification:
o CRCE o CRCS o CRCP
o CHAM (NAHAM) o CHFP (HFMA)
o FHFMA (HFMA) o CHCS (ACA)
o Other (please list) ________________
Employer Type:o Vendor/Corporate Partner o Billing
o Collection Agency o Consulting
o Outsourcing o Software/IT
o Provider o Law Firm
o Other (please list) __________
Position:o CFO
o Consultant
o Director
o Executive Director
o Manager
o Partner, Principal, Owner
o Patient Acces Representative
o PFS Representative
o Supervisor/Coordinator
o Vice President
o Other (please list) ______________
Responsibility:o Accounting
o Administration/Operations
o Admitting/Access
o Audit
o Benefits
o Budget
o Business Development, Sales, Marketing
o Compliance
o Information Services/Technology
o Managed Care
o Medical Records
o Medicare/Medicaid
o PFS, Patient Billing & Collections
o Reimbursement
o Third Party Administration
o Other (please list) ______________
Name of Chapter Geographic Location Chapter Dues
Aksarben #01 Nebraska $0.00
Carolina #04 North & South Carolina $30.00
Chennai #49 Chennai, India $0.00
Connecticut #34 Connecticut $35.00
Evergreen #05 Washington State, West of the Mountains $30.00
Florida Sunshine #03 Florida $40.00
Georgia #33 Georgia $30.00
Gopher #06 Minnesota $40.00
Hawkeye #07 Iowa $0.00
Hawthorn #08 Missouri $45.00
Illinois #09 Illinois $25.00
Indiana #42 Indiana $25.00
Inland Empire #10 Washington State, East of the Mountains $25.00
Keystone #11 Central Pennsylvania $25.00
Maryland #13 Maryland $20.00
Michigan #55 Michigan $0.00
Mid-York #31 New York $40.00
Mountain West #14 Utah $30.00
Music City #53 Tennessee $25.00
New Jersey #16 New Jersey $35.00
Northeast PA #19 North East Pennsylvania $30.00
Philadelphia #29 Philadelphia, Pennsylvania $35.00
Pine Tree #22 Maine $25.00
Rocky Mountain #21 Colorado $20.00
Rushmore #23 North & South Dakota $0.00
Texas Bluebonnet #40 Texas $50.00
Three Rivers #37 Pittsburgh, Pennsylvania $30.00
Twin States #56 New Hampshire & Vermont $25.00
Virginia #27 Virginia $30.00
Western Region #26 Southern California $0.00
Western Reserve #18 Ohio $0.00
Wisconsin #44 Wisconsin $25.00
Local Chapters: AAHAM has 32 chapters throughout the US and India. Local chapters offer you more opportunities for education and networking. Please see the listing of local chapters below to help you decide which chapter you should belong to along with your National membership
44 The Journal of Healthcare Administrative Management
September 13th is Fortune Cookie Day
October 14 is National Dessert Day
November is Native American Awarness Day
did you know?By Moayad Zahralddin September 2014… Hispanic Heritage Month, International Square Dancing Month,
National Blueberry Popsicle Month, National Courtesy Month, Chicken Month, Baby Safety Month, Little League Month, Self Improvement Month2 .... National Beheading Day3 .... Labor Day5 .... Be Late for Something Day6 .... Fight Procrastination Day, Read a Book Day7 .... Grandparent’s Day8 .... International Literacy Day9 .... Teddy Bear Day10 .. Swap Ideas Day13 .. Fortune Cookie Day, National Peanut Day, Positive Thinking Day14 .. National Pet Memorial Day -second Sunday in September16 .. Mayflower Day, National Play Doh Day, Working Parents Day18 .. National Cheeseburger Day19 .. International Talk Like A Pirate Day20 .. Oktoberfest begins21 .. International Peace Day, Miniature Golf Day, National Women’s Friendship Day22 .. Business Women’s Day, Elephant Appreciation Day23 .. Dog in Politics Day28 .. Ask a Stupid Question Day, National Good Neighbor Day
October 2014… Adopt a Shelter Dog Month, Breast Cancer Awareness Month, Domestic Violence Awareness Month, National Diabetes Month, National Pizza Month, National Vegetarian Month, Sarcastic Month Weekly Celebrations… Oct 1-7 Customer Service Week, Oct 8-14 Fire Prevention Week1 .... World Vegetarian Day5 .... Do Something Nice Day, Oktoberfest in Germany ends, World Teacher’s Day6 .... Mad Hatter Day, Physician Assistant Day7 .... World Smile Day8 .... American Touch Tag Day11 .. It’s My Party Day13 .. Columbus Day14 .. Be Bald and Free Day, National Dessert Day16 .. Bosses Day17 .. Wear Something Gaudy Day19 .. Evaluate Your Life Day21 .. Babbling Day23 .. National Mole Day25 .. Make a Difference Day26 . Mother-In-Law Day30 .. Mischief Night31 .. Halloween, Increase Your Psychic Powers Day
November 2014… Child Safety Protection Month, National Adoption Awareness Month, National Epilepsy Month, Native American Heritage Month, Peanut Butter Lovers Month, Real Jewelry Month, National Sleep Comfort Month 1 .... Book Lovers Day2 .... Look for Circles Day, Deviled Egg Day3 .... Housewife’s Day, Sandwich Day6 .... Marooned without a Compass Day8 .... Cook Something Bold Day, Dunce Day11 .. Veteran’s Day13 .. Sadie Hawkins Day, World Kindness Day14 .. Operating Room Nurse Day15 .. Clean Your Refrigerator Day, America Recycles Day16 .. Have a Party With Your Bear Day17 .. World Peace Day20 .. Absurdity Day, Universal Children’s Day22 .. National Adoption Day26 .. Shopping Reminder Day29 .. Square Dance Day30 .. Stay At Home Because You Are Well Day

Summer 2014 45
national calendar
the JHAM networkMovers & Shakers
Don’t forget to give us your information for the Movers & Shakers section of The Journal. This section includes job announcements (changes or promotions), birth and death
announcements, and wedding announcements. Send your “news” to Sharon Galler at [email protected]
ChaptersPlease send us notices of your upcoming events/meetings, chapter news and
photos. We would be happy to post them for you!
Address ChangesAll address changes can be emailed to Moayad Zahralddin,
[email protected] at the National Office or you can update your information yourself on-line at www.aaham.org.
October 15-17, 2014 2014 ANI, Manchester Grand Hyatt San Diego, California
October 14-16, 2015 2015 ANI, Walt Disney World Swan and Dolphin Orlando, Florida
Follow us on
With highly informative session tracks, AAHAM’s 2014 ANI promises real-world solutions you can put into use immediately at your facility.
Mark you calendar now and put the ANI in your budget. Join us in beautiful San Diego, California and get ready to “Sail into Revenue Cycle Success.”
October 15-17, 2014October 15-17, 2014Manchester Grand Hyatt, San Diego, California
2014 AAHAM ANI2014 AAHAM ANI