surgery after induction vs. definitive therapy and paranchym preserving vascular techniques
DESCRIPTION
Surgery after induction vs. definitive therapy and paranchym preserving vascular techniques. Alper Toker, MD İstanbul University , İ stanbul Medical School Department of ThoracicSurgery. Neoadjuvant treatment. Invasion to vital organs To have Easier resectability , - PowerPoint PPT PresentationTRANSCRIPT

12th April, 2012 Antalya
Surgery after induction vs. definitive therapy and paranchym preserving vascular
techniques
Alper Toker, MDİstanbul University, İstanbul Medical School
Department of ThoracicSurgery
12th April, 2012 Antalya
Neoadjuvant treatment
Invasion to vital organs • To have Easier resectability,• To achieve negative margins• To prevent seeding• To prevent radioresistance due to possible hypoxemiaof the tissue
• Rectum, • Lareynx,• Osephagus,• Prostate,• Soft tissue sarcomas• Pancreas.
.
12th April, 2012 Antalya
Preoperative therapy
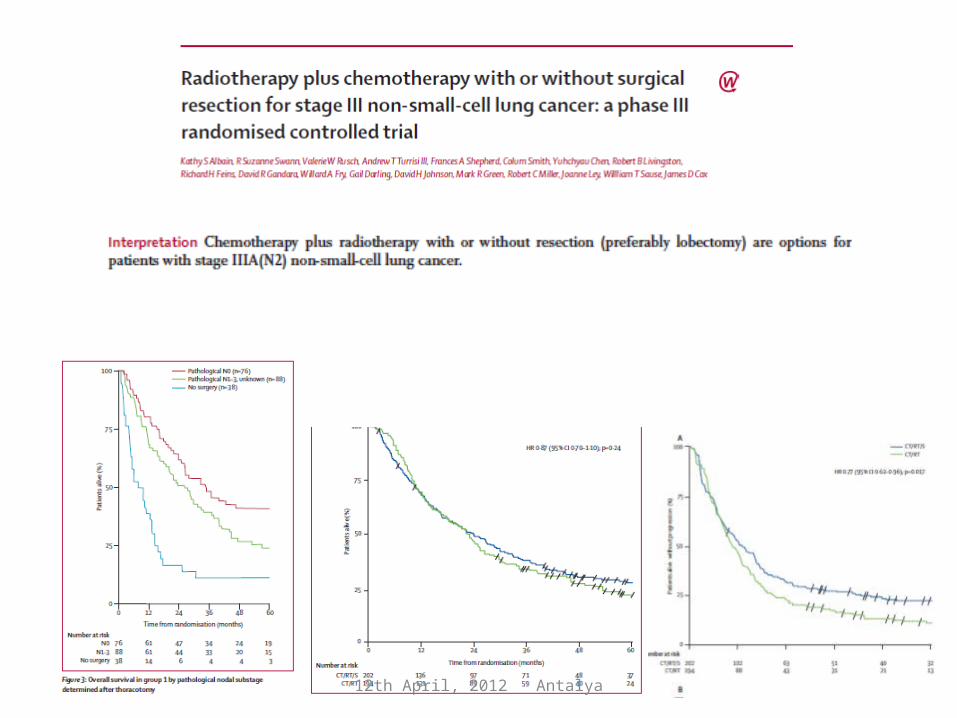
• Induction CT + surgery • Induction CT + RT (45Gy) + surgery
• Vs.
• Definitive CxRT (60Gy) + surgery
Definitive RT: Advantages Definitive RT: disadvantages

12th April, 2012 Antalya
3 D treatments – Calculating the area

12th April, 2012 Antalya
Decreasing the radiotherapy doseof healthy tissues
12th April, 2012 Antalya
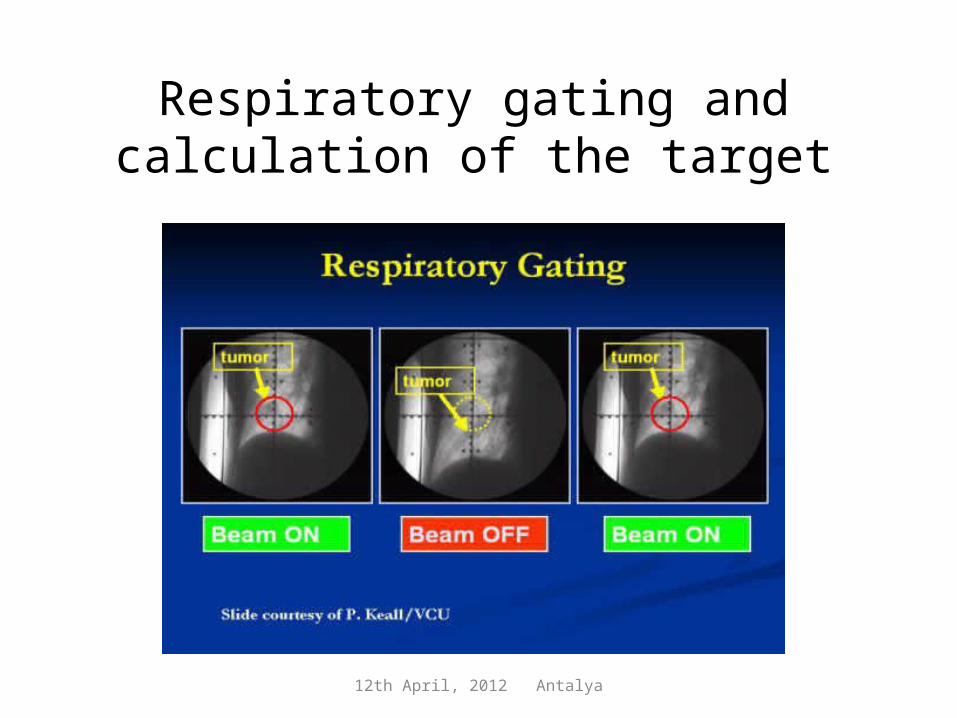
Respiratory gating and calculation of the target
12th April, 2012 Antalya
12th April, 2012 Antalya
12th April, 2012 Antalya
12 Nisan, 2012 Toraks Kongresi Antalya
12 Nisan, 2012 Toraks Kongresi Antalya

12 Nisan, 2012 Toraks Kongresi Antalya

12 Nisan, 2012 Toraks Kongresi Antalya
12th April, 2012 Antalya
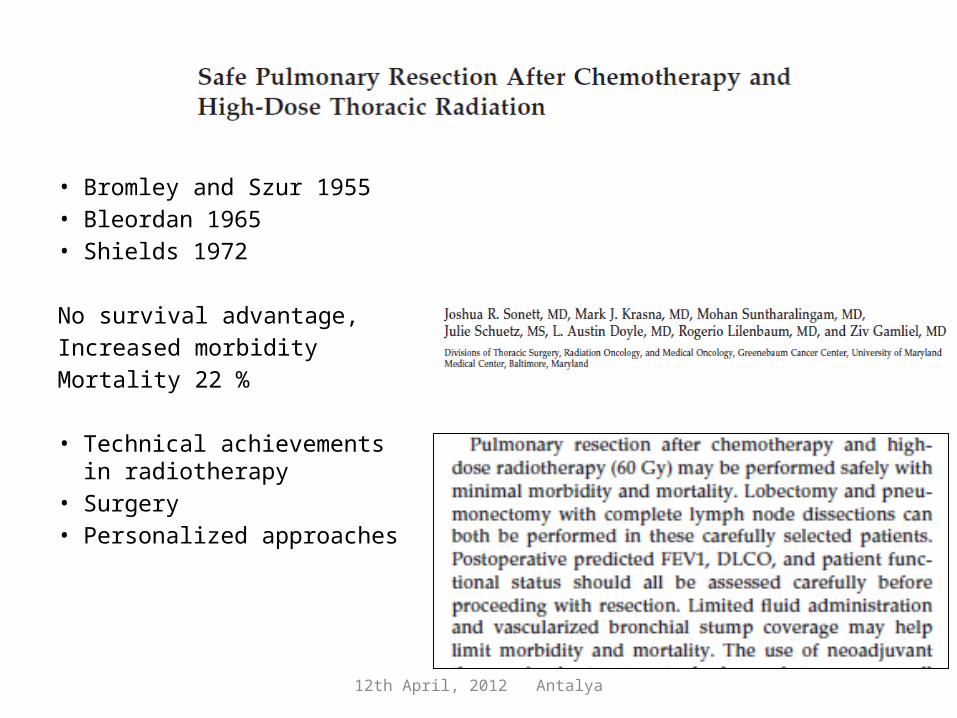
• Bromley and Szur 1955• Bleordan 1965• Shields 1972
No survival advantage, Increased morbidity Mortality 22 %
• Technical achievements in radiotherapy
• Surgery • Personalized approaches
12th April, 2012 Antalya
12th April, 2012 Antalya
12th April, 2012 Antalya
12th April, 2012 Antalya
12th April, 2012 Antalya
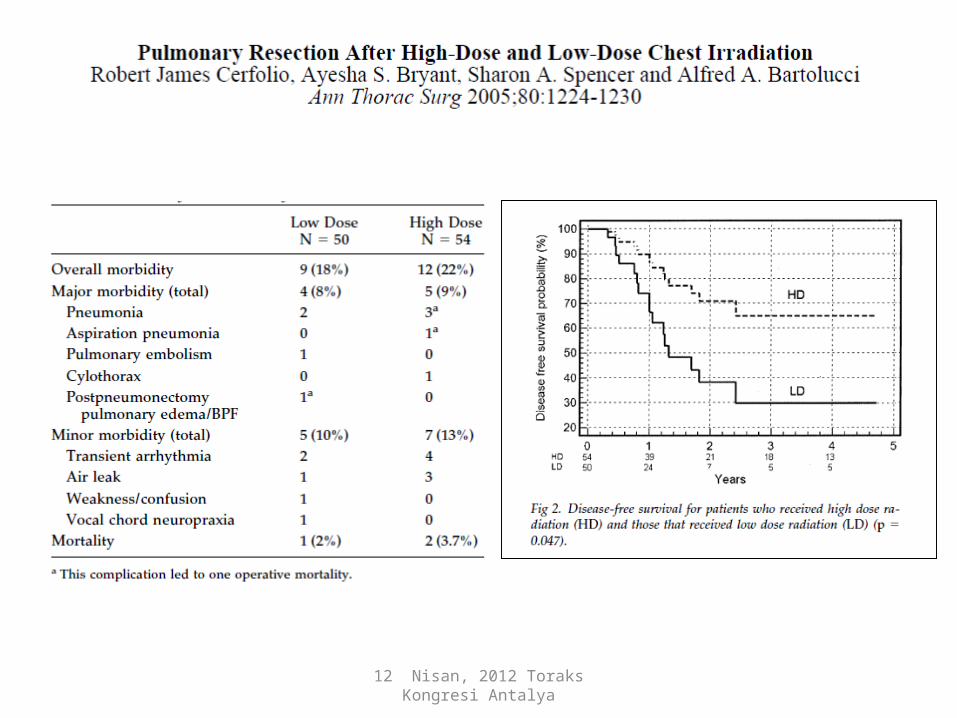
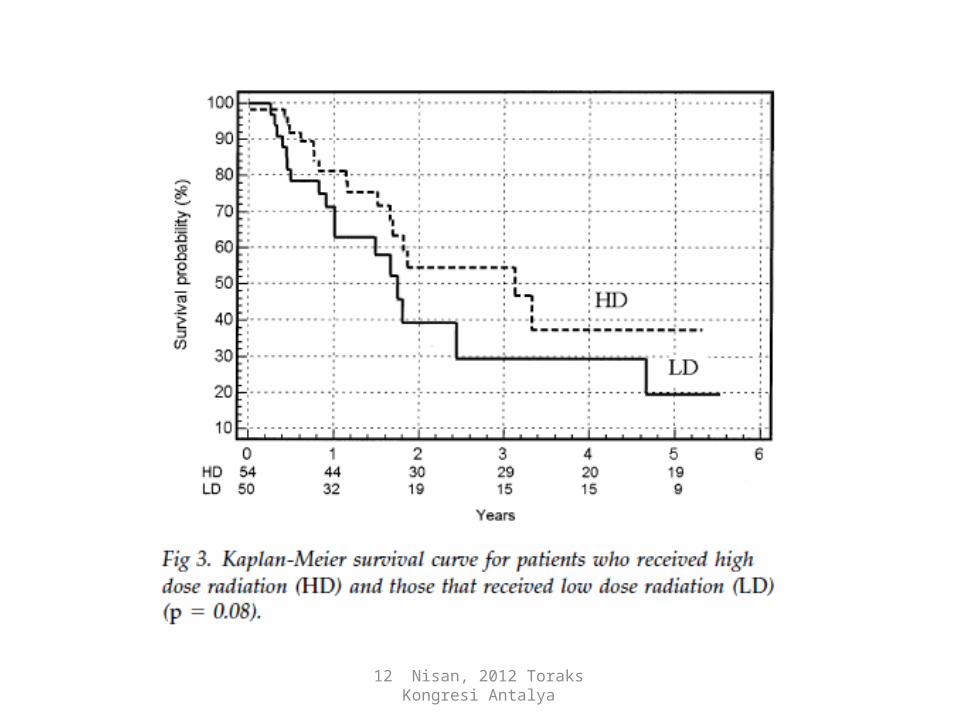
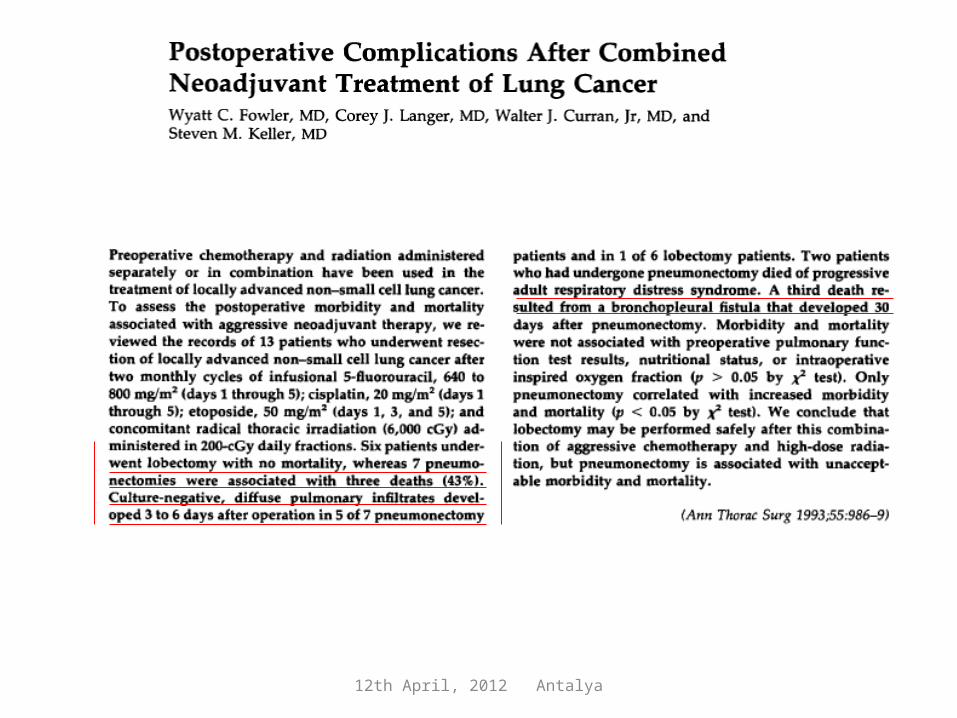
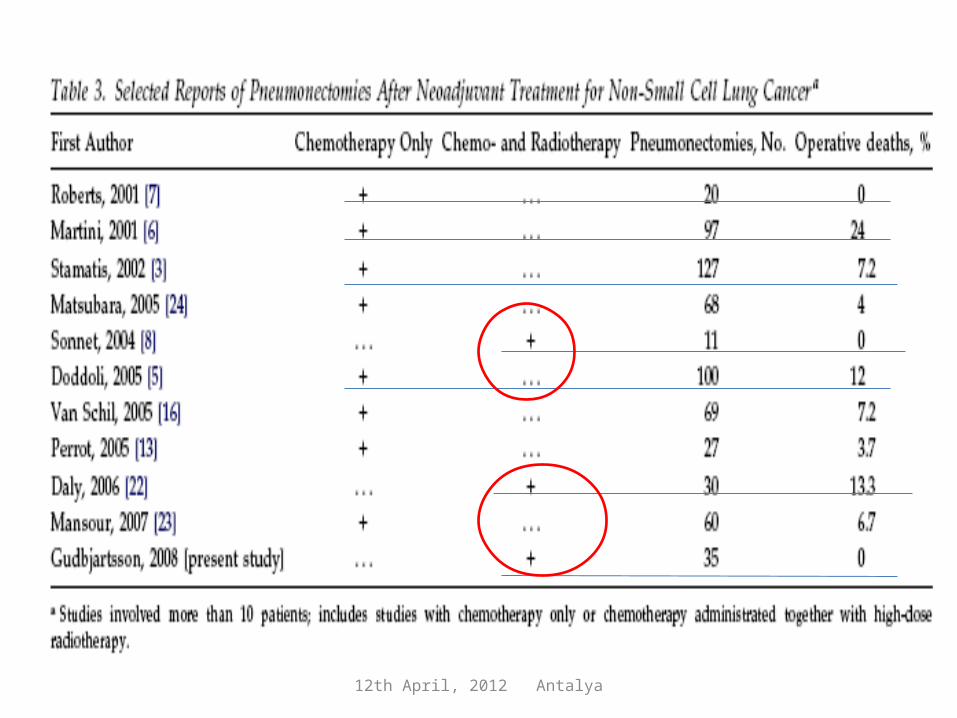
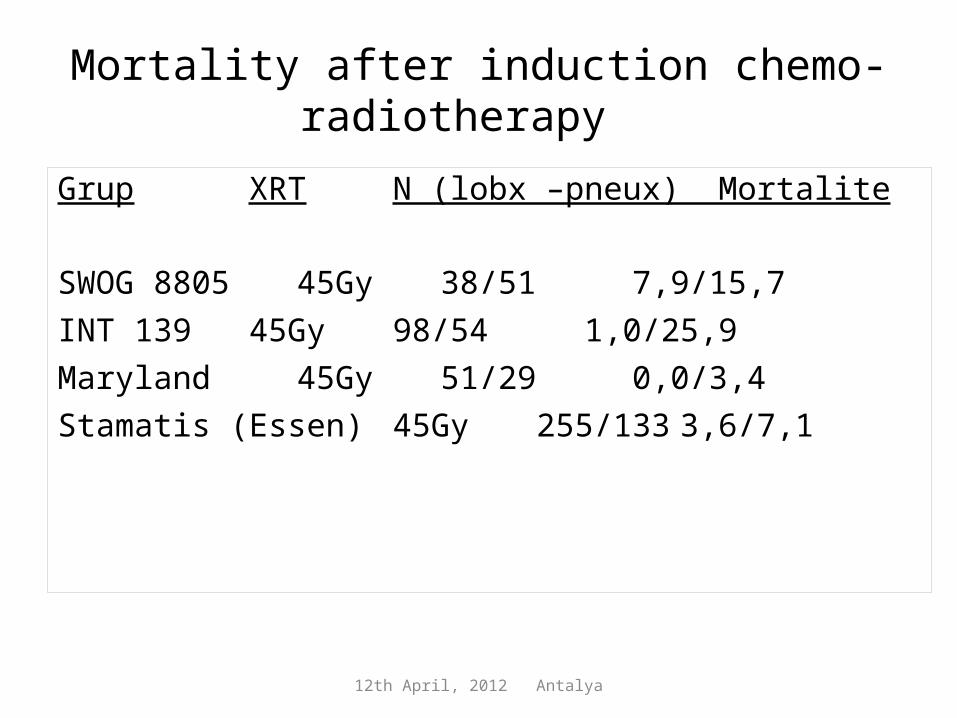
Mortality after induction chemo-radiotherapy
Grup XRT N (lobx –pneux) Mortalite
SWOG 8805 45Gy 38/51 7,9/15,7INT 139 45Gy 98/54 1,0/25,9Maryland 45Gy 51/29 0,0/3,4Stamatis (Essen) 45Gy 255/133 3,6/7,1

12th April, 2012 Antalya
12th April, 2012 Antalya
12th April, 2012 Antalya
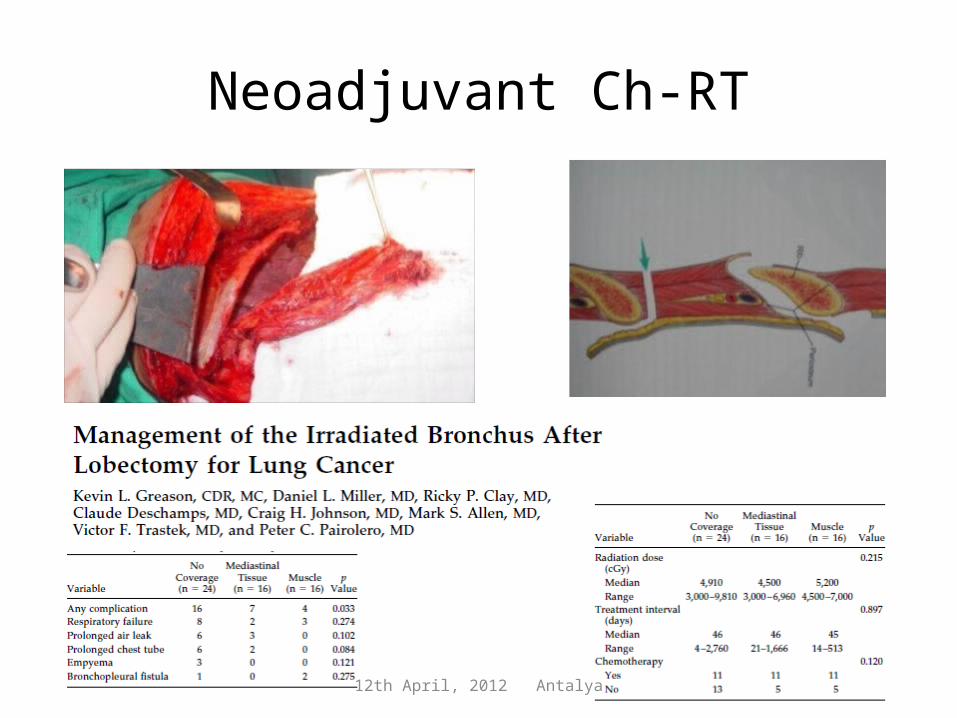
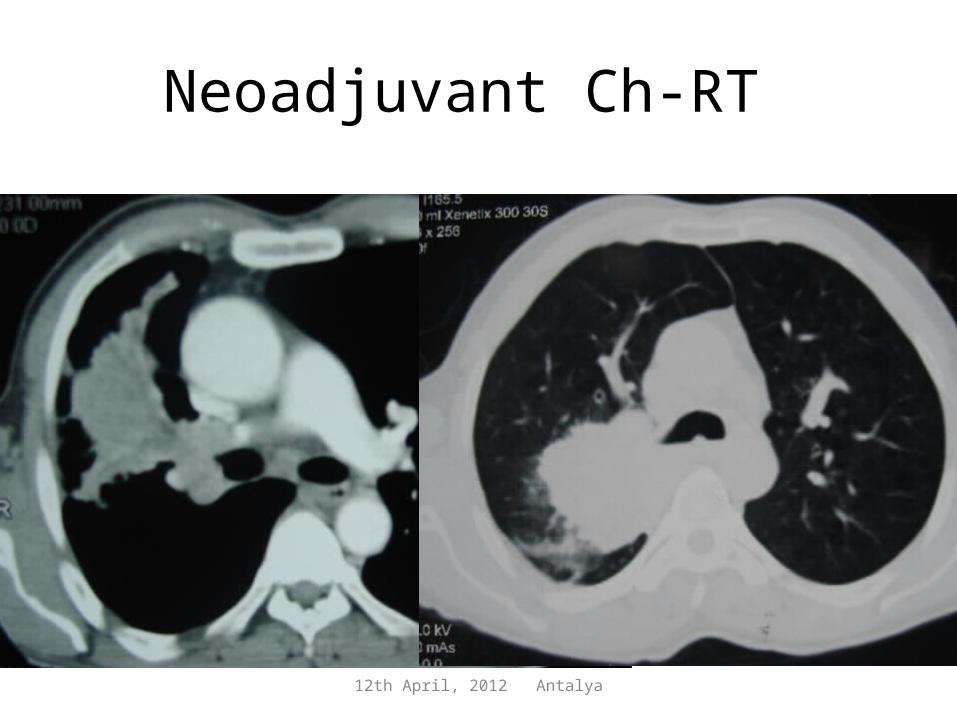
Neoadjuvant Ch-RT
12th April, 2012 Antalya
Adj dose RT -CT

12th April, 2012 Antalya

12th April, 2012 Antalya
CT and RT

12th April, 2012 Antalya
12th April, 2012 Antalya

12th April, 2012 Antalya
12th April, 2012 Antalya
Neoadjuvant Ch-RT

12th April, 2012 Antalya
12th April, 2012 Antalya
12th April, 2012 Antalya

12th April, 2012 Antalya
Not after RT
12th April, 2012 Antalya

12th April, 2012 Antalya
12th April, 2012 Antalya

12th April, 2012 Antalya
N2-T4 primary lung cancerInduction chemotherapy and chemoradiotherapy
(45 Gy / 60 Gy) and lung resection
• Morbidity• Mortality• Survival
Istanbul Medical School Lung Oncology Group

12th April, 2012 Antalya
Patients and methods
December 2002 – December 2011 154 patients
– Age– Gender– Cytology (Epidermoid / Non epidermoid)– Induction treatment (CT / CT-RT45 / CT-RT60)– Pulmonary function Tests ( >%80, %80-60, <%60)– CO diffusion test ( >%80, %80-60, <%60)– Resection type– Mortality– Morbidity– Survival
– Prospectively recorded data
12th April, 2012 Antalya
Patients and methods
Treatment modalities– CT: 89 patients– CT-RT 45: 46 patients– CT-RT 60: 19 patients
Patients operated within the past 24 months were excluded (119/154 patients)
12th April, 2012 Antalya
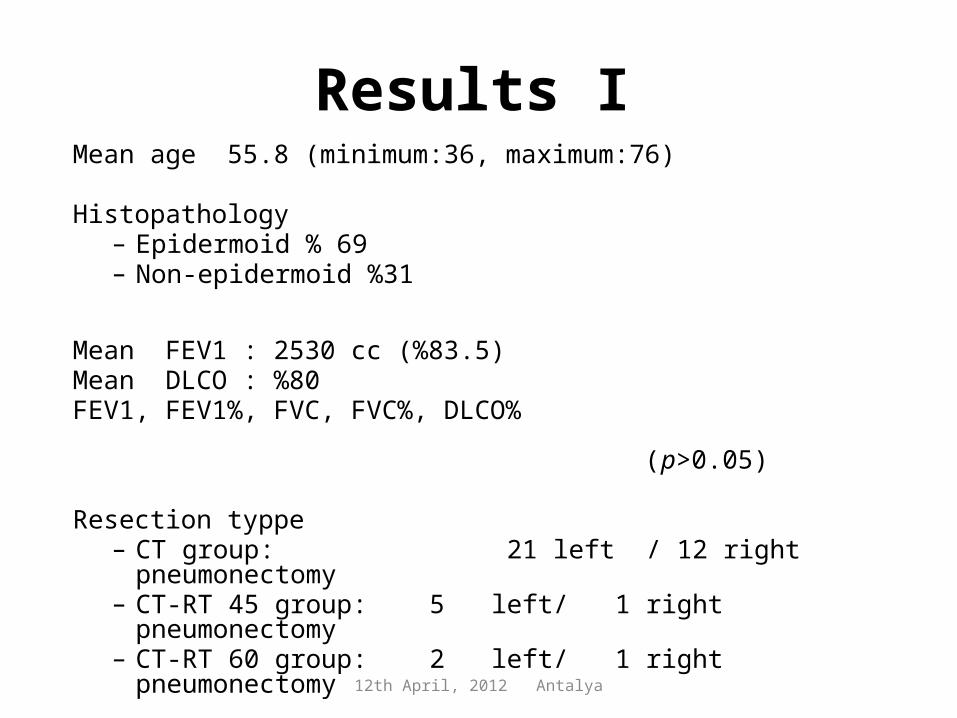
Results IMean age 55.8 (minimum:36, maximum:76)
Histopathology– Epidermoid % 69– Non-epidermoid %31
Mean FEV1 : 2530 cc (%83.5)Mean DLCO : %80FEV1, FEV1%, FVC, FVC%, DLCO% (p>0.05)
Resection typpe– CT group: 21 left / 12 right pneumonectomy – CT-RT 45 group: 5 left/ 1 right pneumonectomy – CT-RT 60 group: 2 left/ 1 right pneumonectomy
12th April, 2012 Antalya
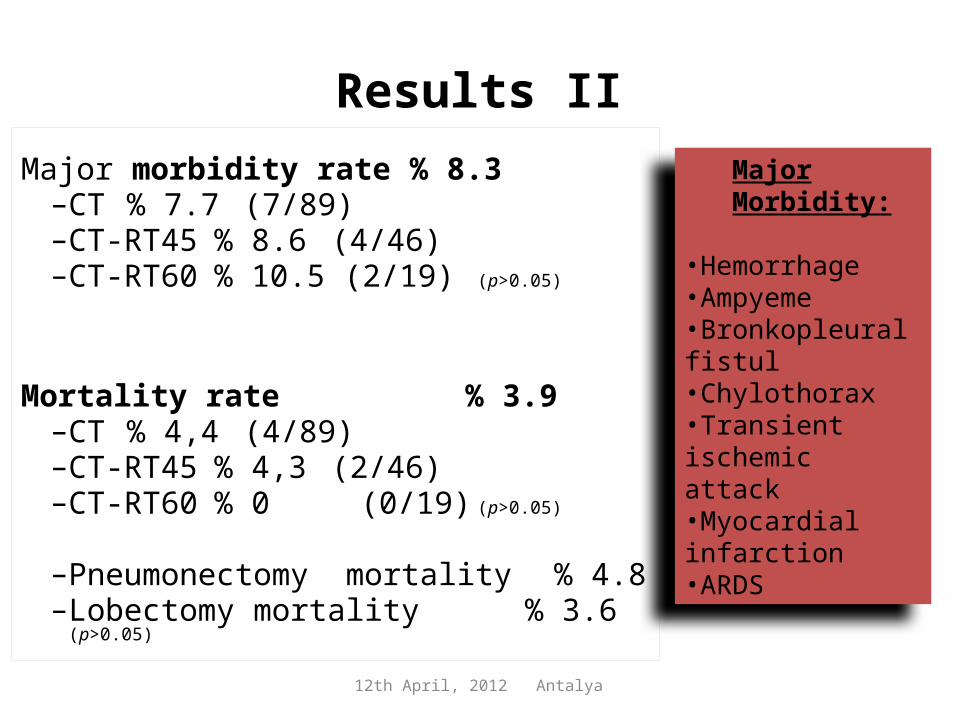
Results IIMajor morbidity rate % 8.3
– CT % 7.7 (7/89)– CT-RT45 % 8.6 (4/46)– CT-RT60 % 10.5 (2/19) (p>0.05)
Mortality rate % 3.9– CT % 4,4 (4/89)– CT-RT45 % 4,3 (2/46)– CT-RT60 % 0 (0/19) (p>0.05)
– Pneumonectomy mortality % 4.8– Lobectomy mortality % 3.6 (p>0.05)
Major Morbidity:
•Hemorrhage•Ampyeme•Bronkopleural fistul•Chylothorax•Transient ischemic attack•Myocardial infarction•ARDS

12th April, 2012 Antalya
Results III
Median followup: 31 monnths– (Minimum 24 mts – maximum 108 mts)
Median survival :27 mts– Induction CT (n:76) 24 mts– Induction CT-RT (n:43) 33 mts
(Kaplan Meier, p: 0.595)
– A correct survival analyze is impossible due to non-homogenous operative periods of groups.
12th April, 2012 Antalya
DiscussionSurgery after induction treatment for N2 or T4 disease
– Type of induction treatment (CT & CT-RT 45 & CT-RT 60)
– PFT - DLCO – Histopathology– Type of resection (Lobectomy &
pneumonectomy) were not different statistically in terms of major morbidity and mortality.

12th April, 2012 Antalya
Conclusion
Lung resection after induction treatment;Acceptable morbidity ve mortality rate.CT- RT 60 Gy did not have a negatife effect on mortality and morbidity.Median survival seems to be longer in CT-RT patients, however,difference is statistically insignificant when compared to CT only. Pneumonectomy decision needs to be judged carefully.
Patient selection !
12th April, 2012 Antalya
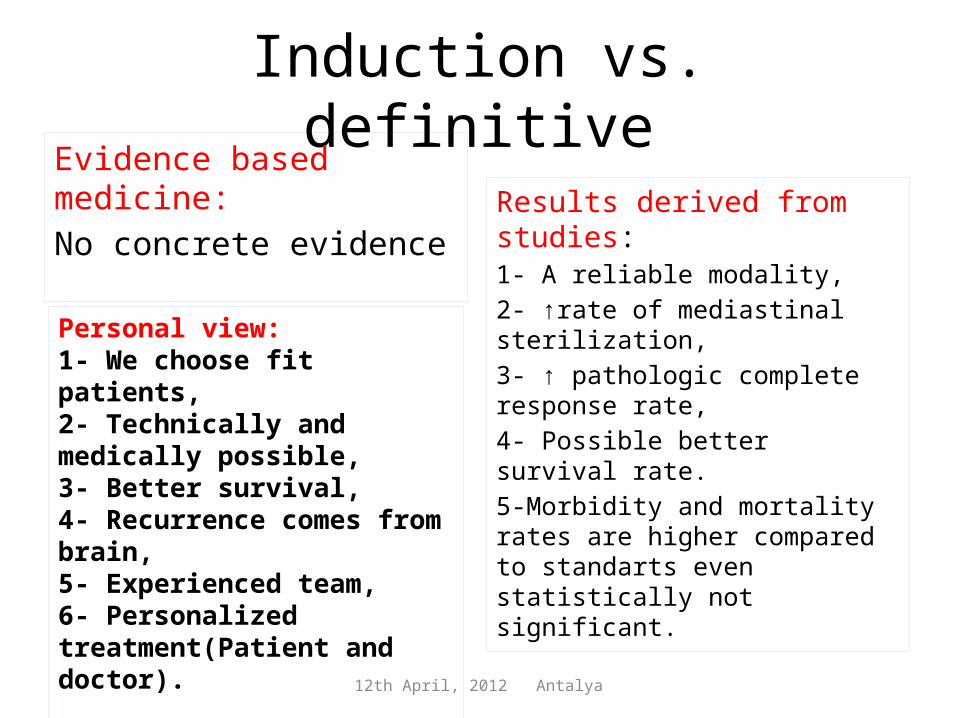
Induction vs. definitiveEvidence based medicine:No concrete evidence
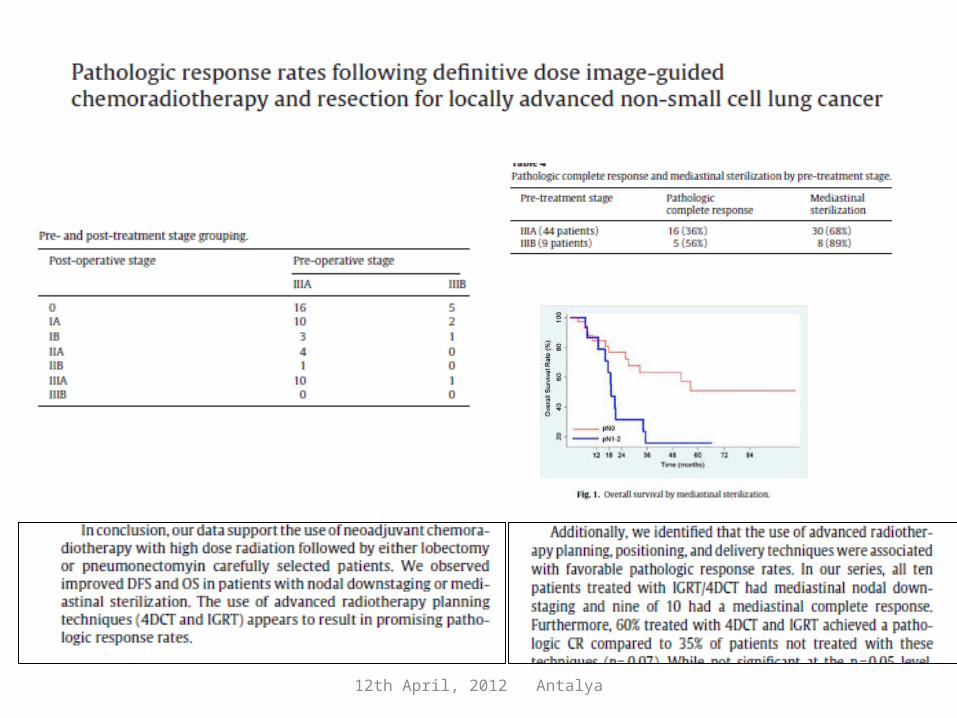
Results derived from studies:1- A reliable modality,2- ↑rate of mediastinal sterilization,3- ↑ pathologic complete response rate,4- Possible better survival rate. 5-Morbidity and mortality rates are higher compared to standarts even statistically not significant.
Personal view:1- We choose fit patients,2- Technically and medically possible, 3- Better survival,4- Recurrence comes from brain,5- Experienced team,6- Personalized treatment(Patient and doctor).

12th April, 2012 Antalya
3 rekonstrüksiyon 4 anastomoz Toker A, GKDC Dergisi 2009

12th April, 2012 Antalya
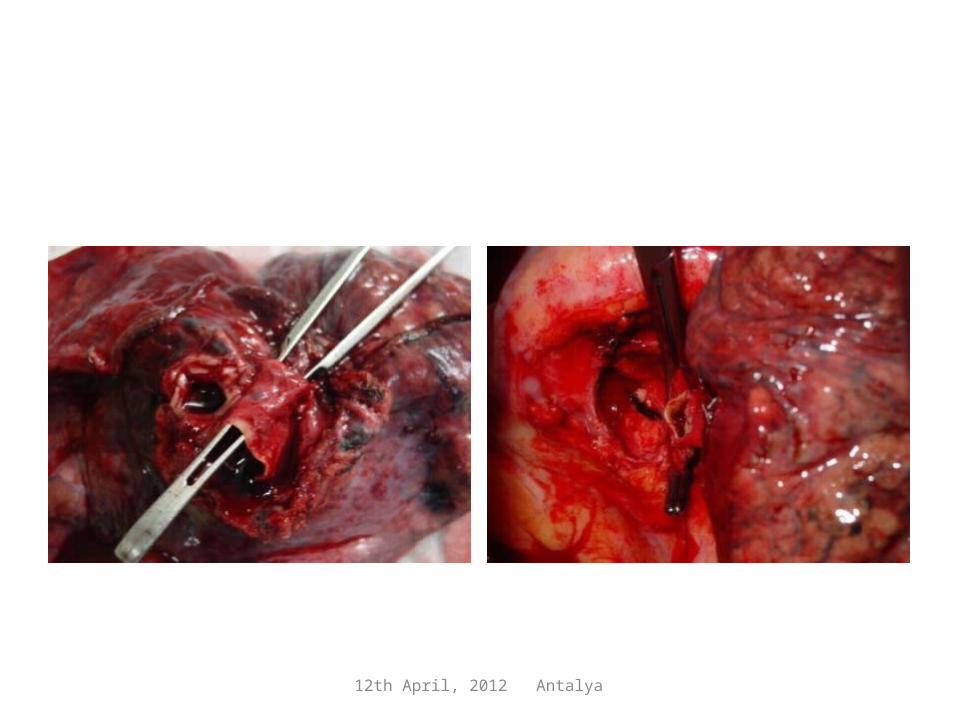
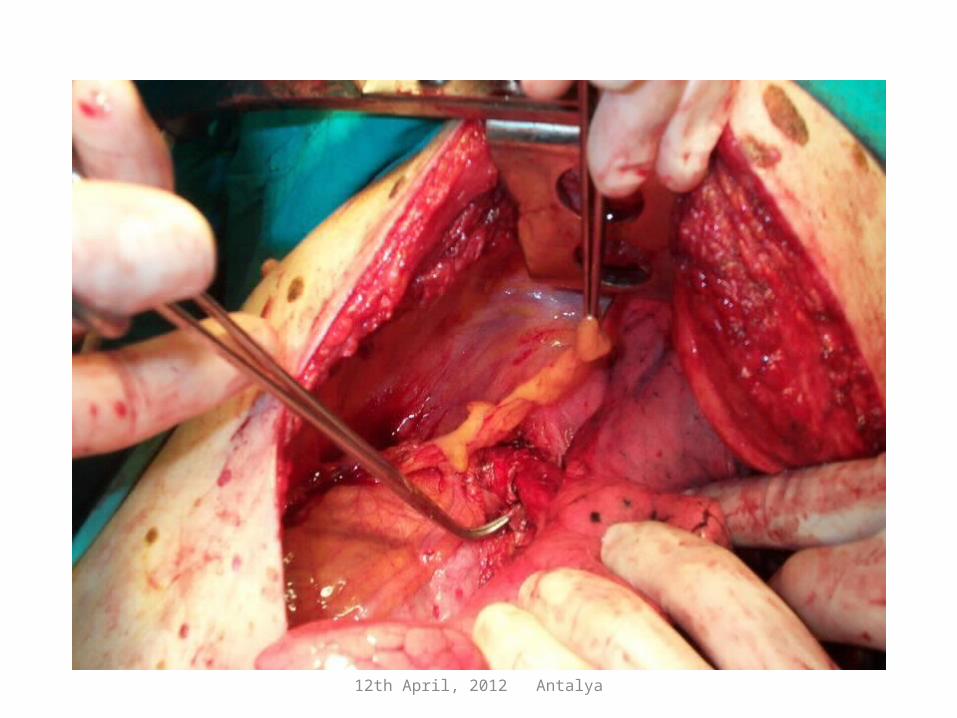
Bronchovascular sleeve resections
12th April, 2012 Antalya
12th April, 2012 Antalya

12th April, 2012 Antalya
12th April, 2012 Antalya
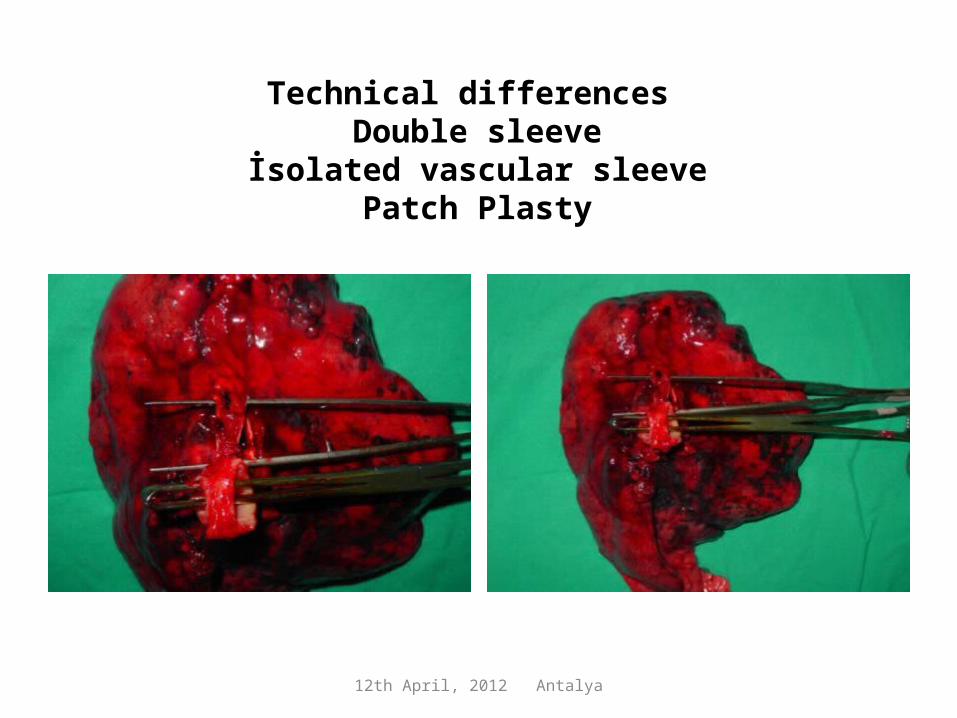
Technical differences Double sleeve
İsolated vascular sleevePatch Plasty

12th April, 2012 Antalya
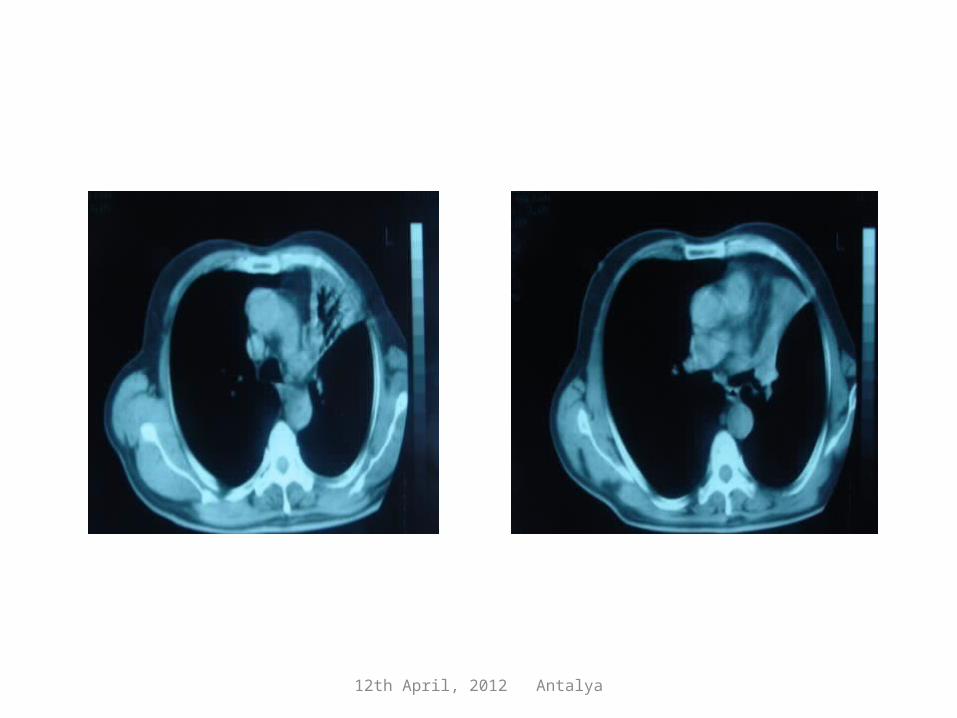
Lung tumor after Neoadjuvant CT

12th April, 2012 Antalya
12th April, 2012 Antalya
anastomoz
12th April, 2012 Antalya
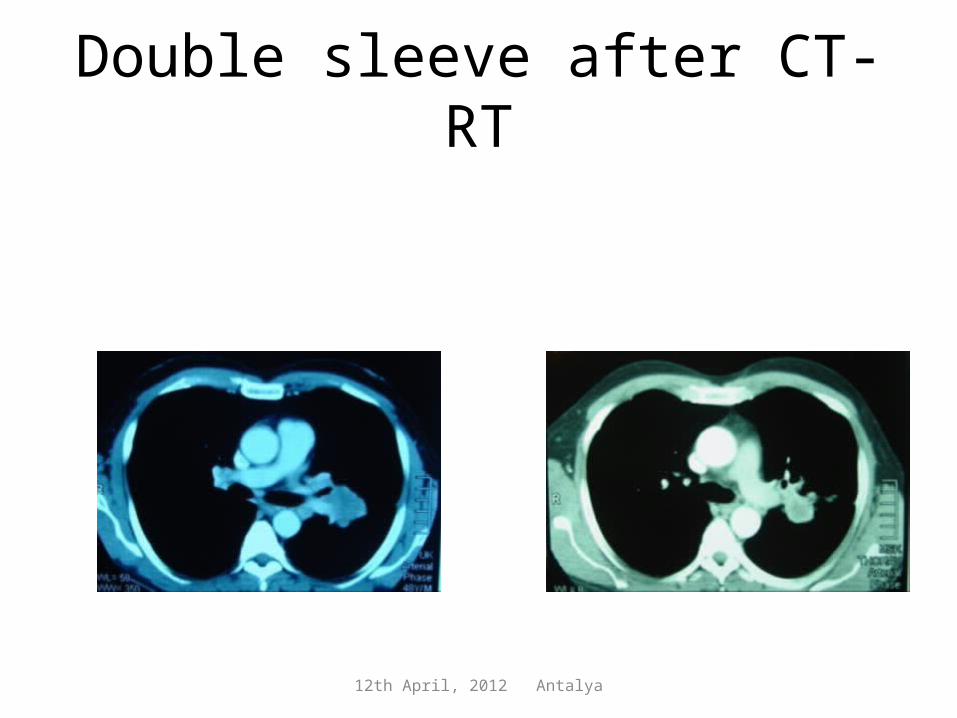
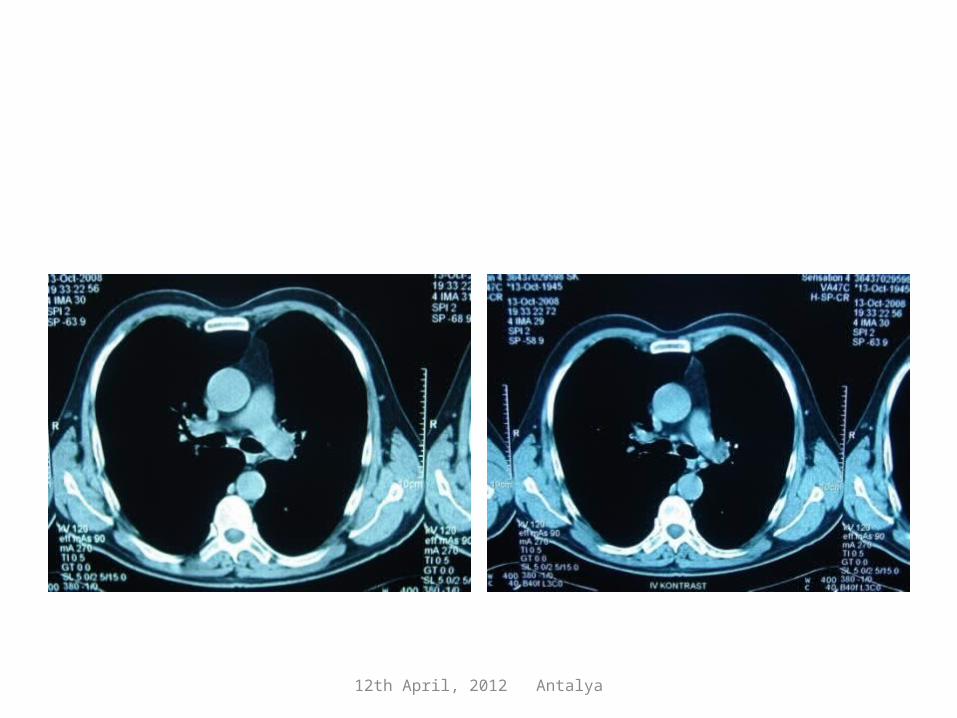
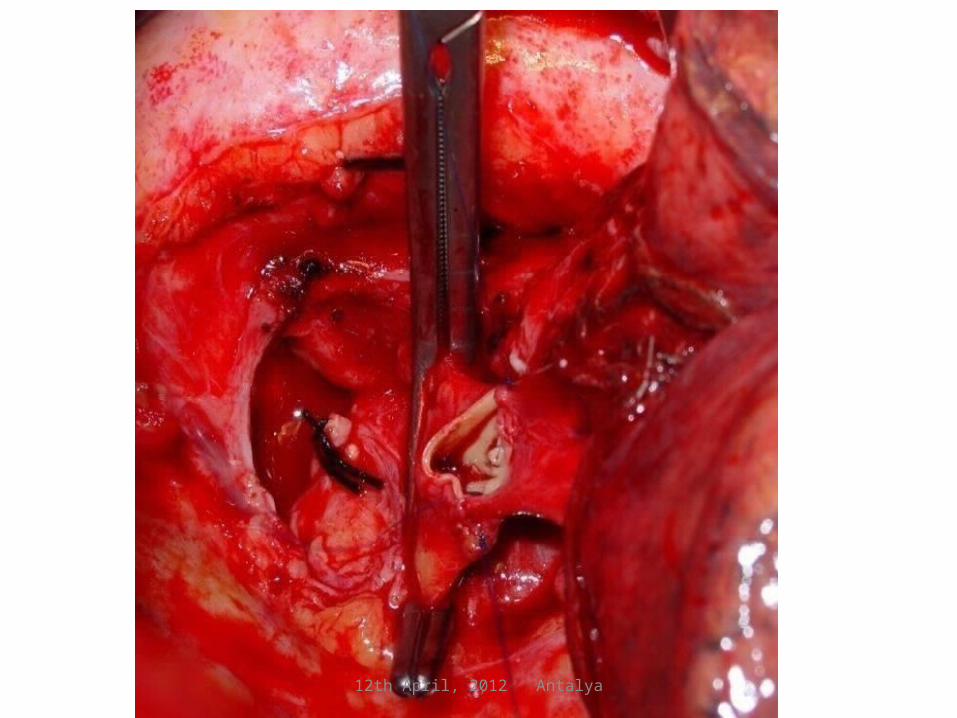
Double sleeve after CT-RT
12th April, 2012 Antalya

12th April, 2012 Antalya
Positive bronchial margins
12th April, 2012 Antalya
12th April, 2012 Antalya
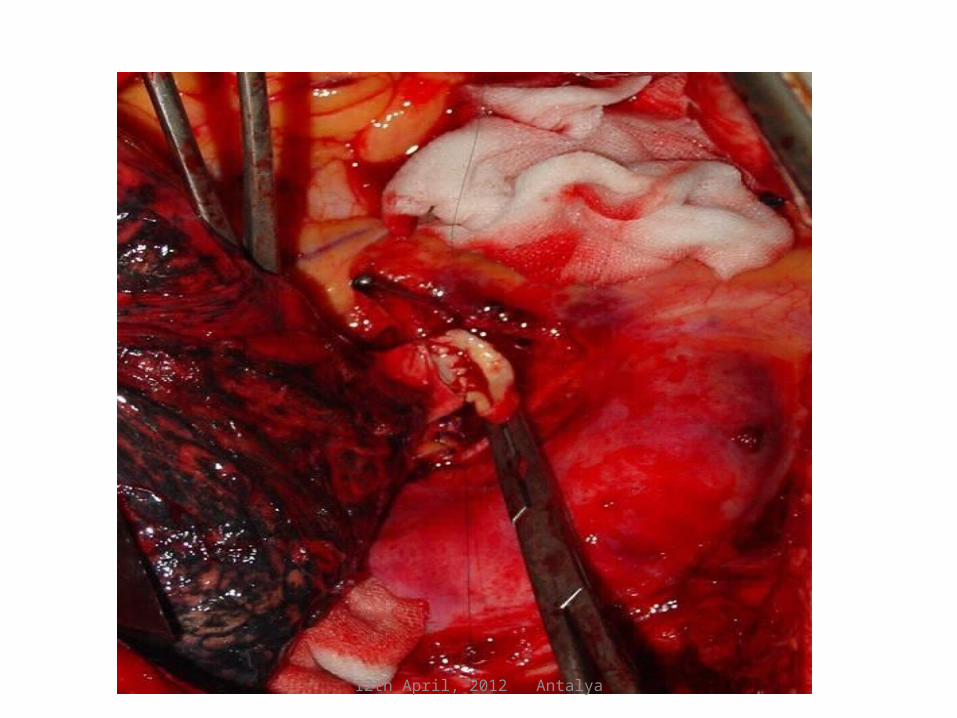
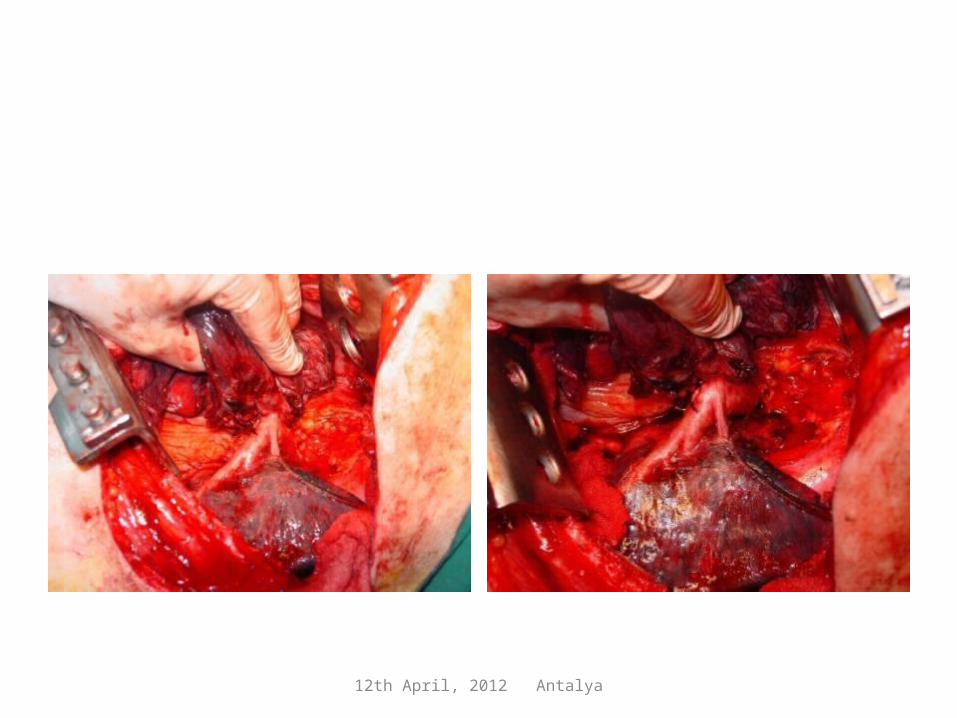
Isolated patch plasty
• Technically easier Available materials (pericardium, vascular grefts, veins, etc)
• Lesser rate of complication.• No need to anticoagulate.
• Surgical margins, always trouble
• Posterior part sutures• Placing the patch may
need vascular technique experience.

12th April, 2012 Antalya
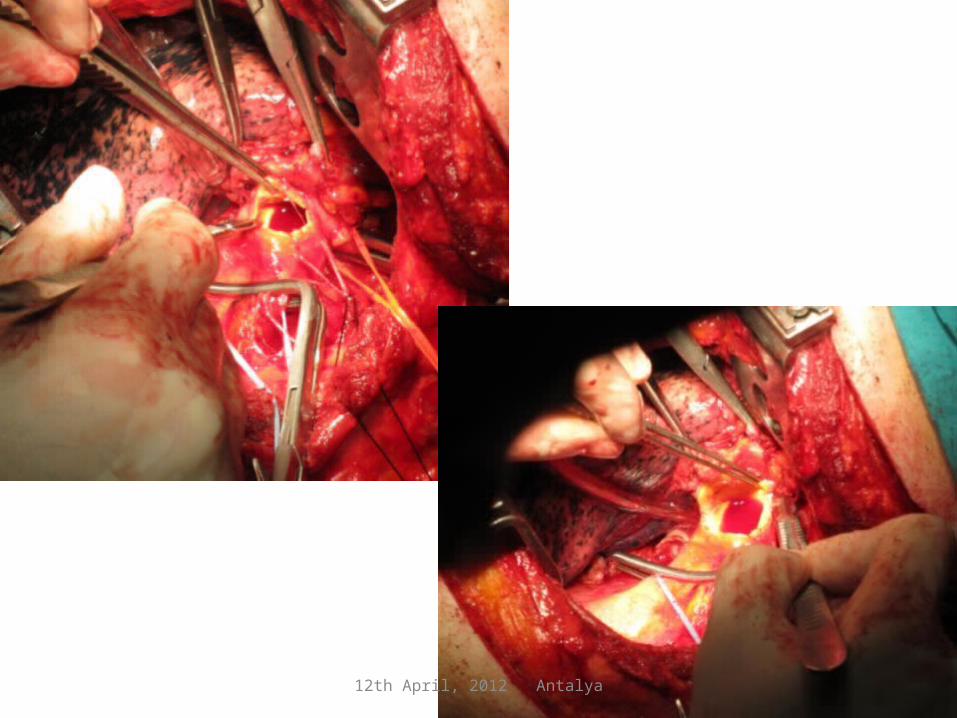
Technics

12th April, 2012 Antalya
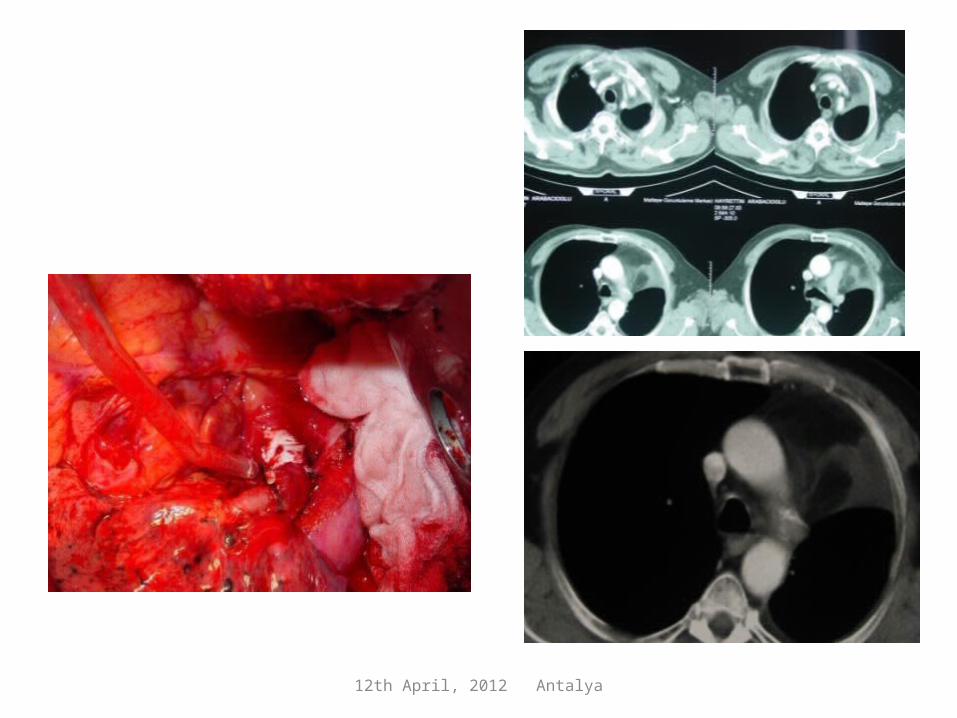
Isolated Patch Plasty

12th April, 2012 Antalya
Sol santral lezyon
12th April, 2012 Antalya
12th April, 2012 Antalya

12th April, 2012 Antalya
87 year-old patient with left hilar mass
12th April, 2012 Antalya
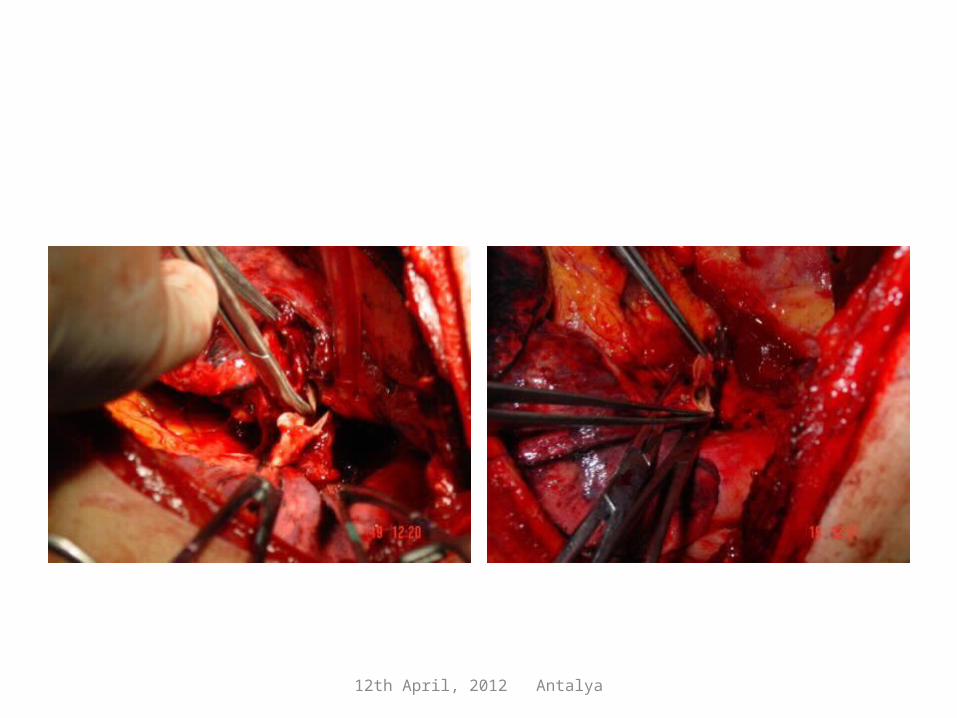
Bronchial sleeve and patch plasty
Bronchus first,Approximate and control the pulmonary artery when the lung is inflated,Select the proper reconstructive material,Air leak control,A viable tissue between the sutures of bronchus and pulmonary artery.

12th April, 2012 Antalya
Bronchial sleeve and patch plasty
12th April, 2012 Antalya
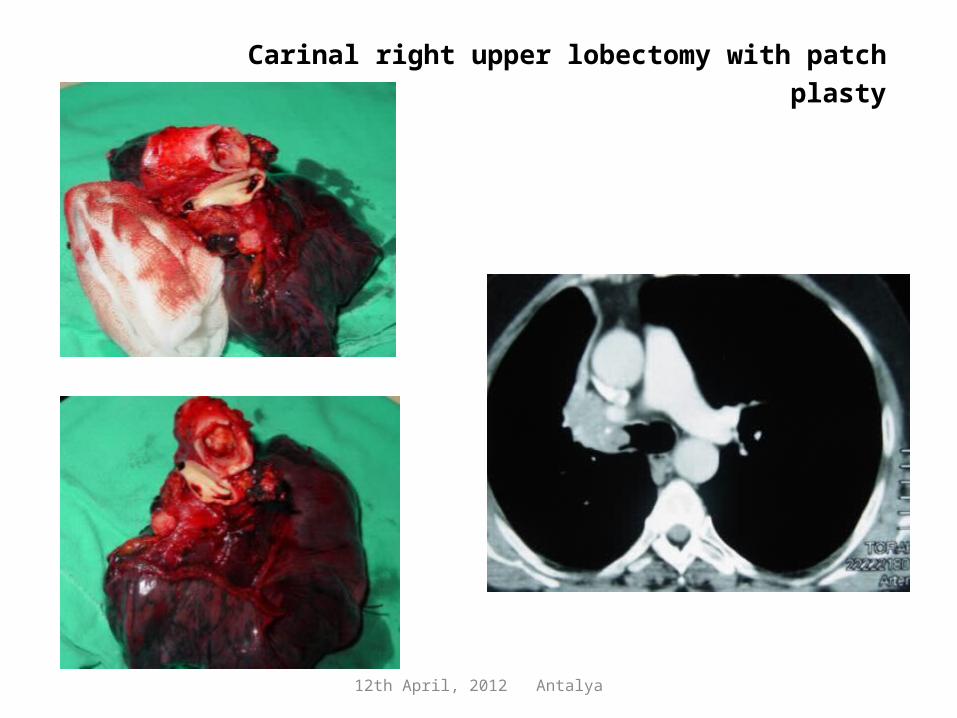
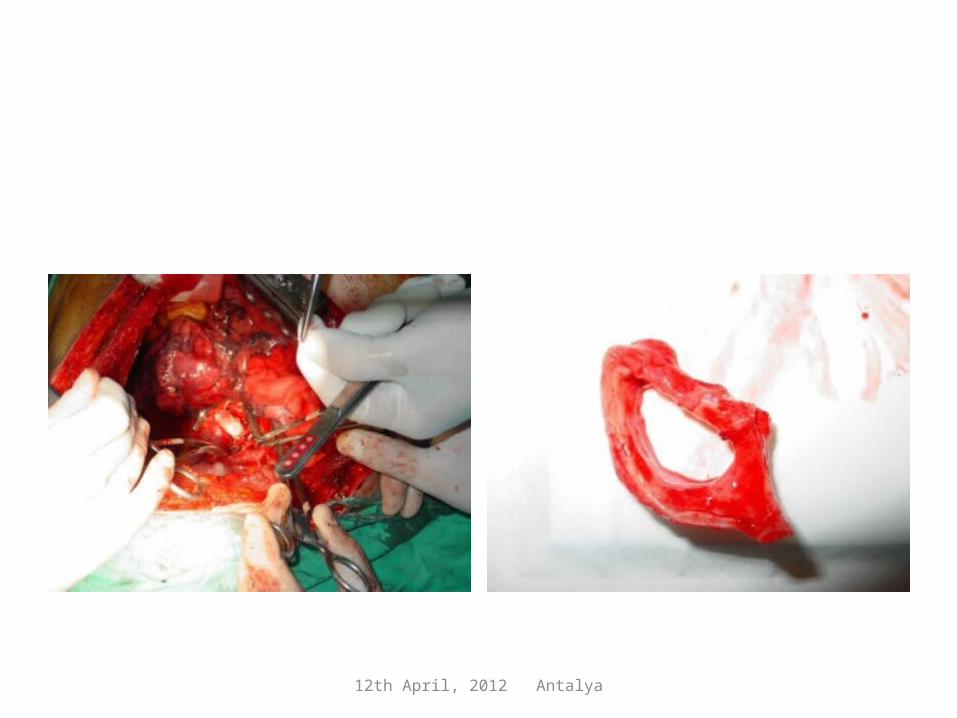
Carinal right upper lobectomy with patch plasty
12th April, 2012 Antalya
12th April, 2012 Antalya
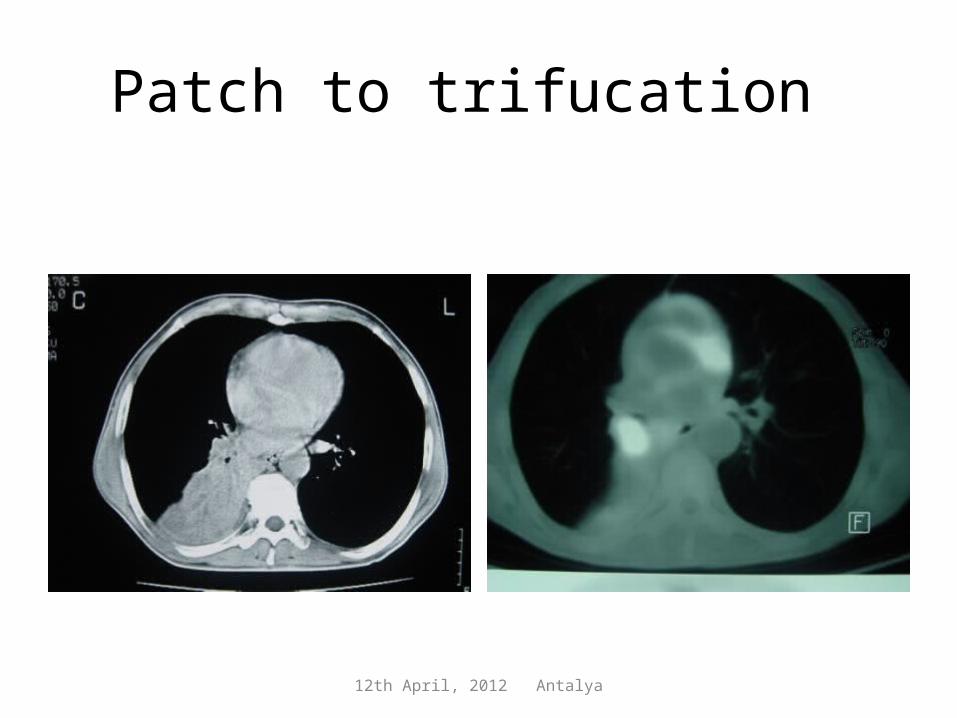
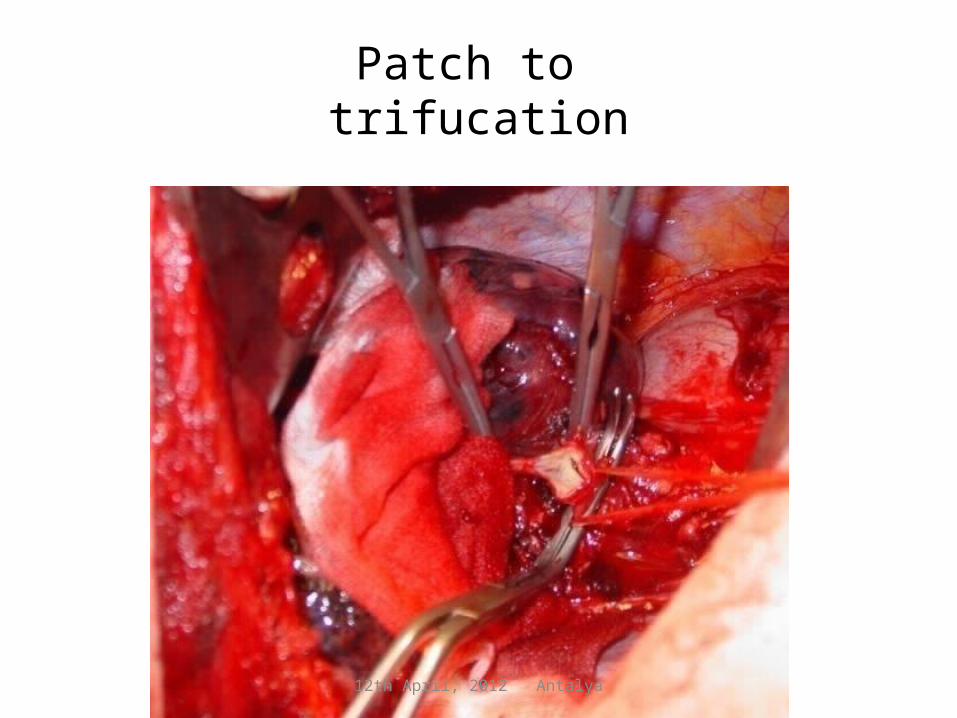
Patch to trifucation
12th April, 2012 Antalya
Patch to trifucation

12th April, 2012 Antalya
12th April, 2012 Antalya
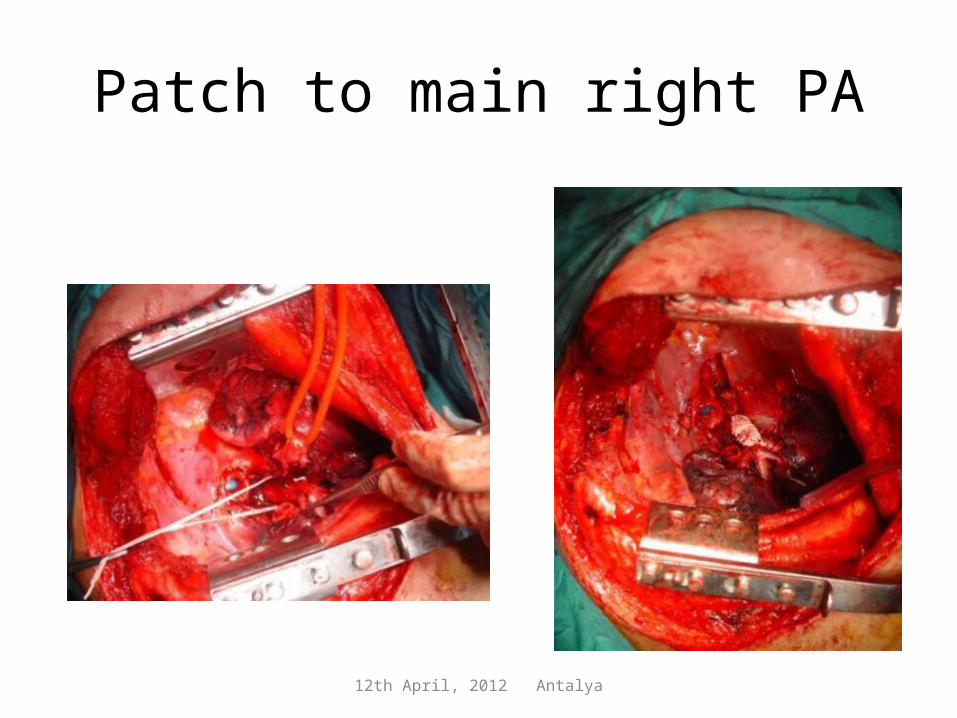
Patch to main right PA

12th April, 2012 Antalya
12th April, 2012 Antalya
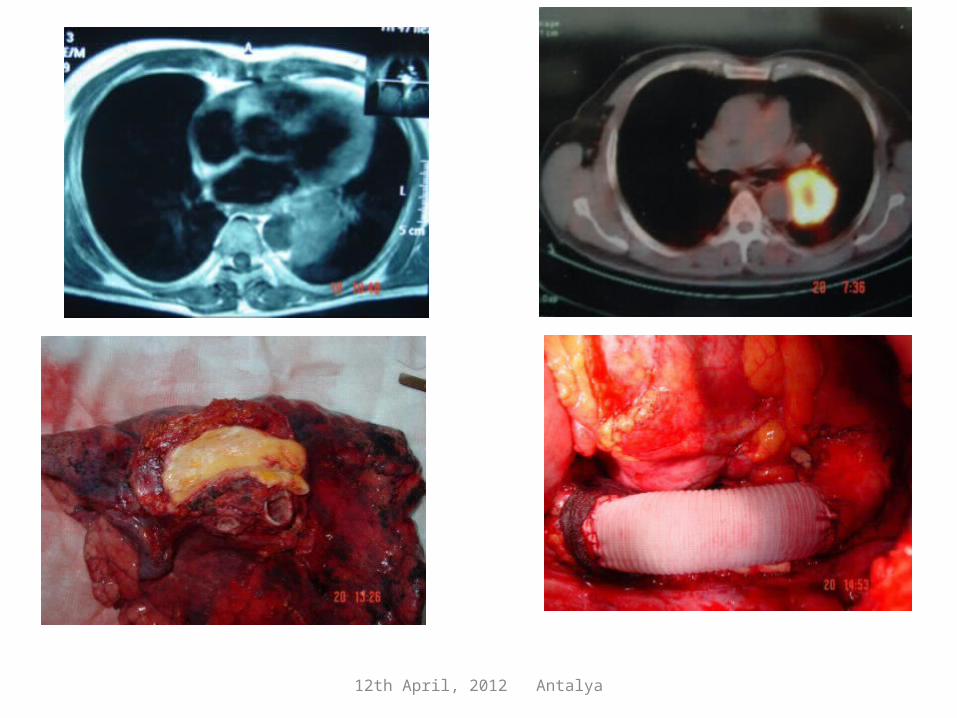
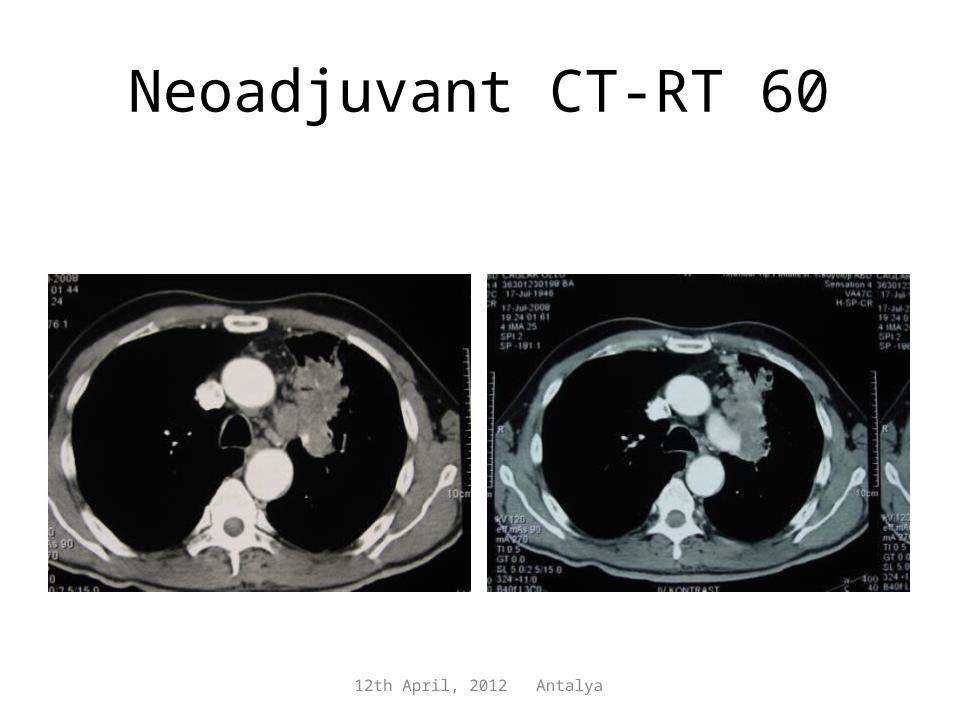
Neoadjuvant CT-RT 60

12th April, 2012 Antalya

12th April, 2012 Antalya
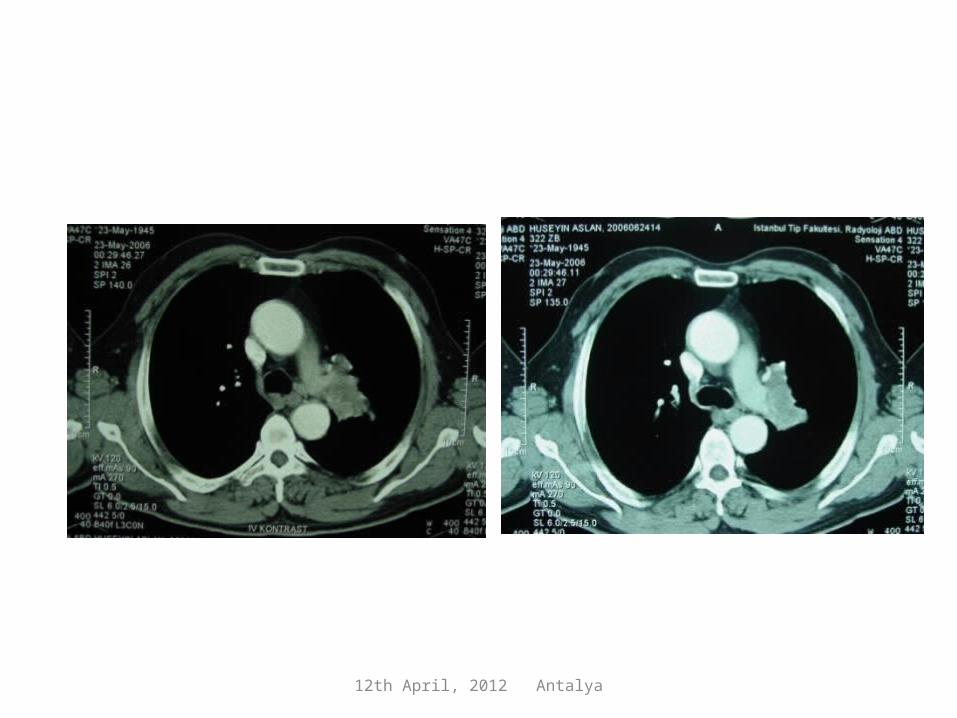
After induction treatment

12th April, 2012 Antalya

12th April, 2012 Antalya
Post operatif
12th April, 2012 Antalya

12th April, 2012 Antalya
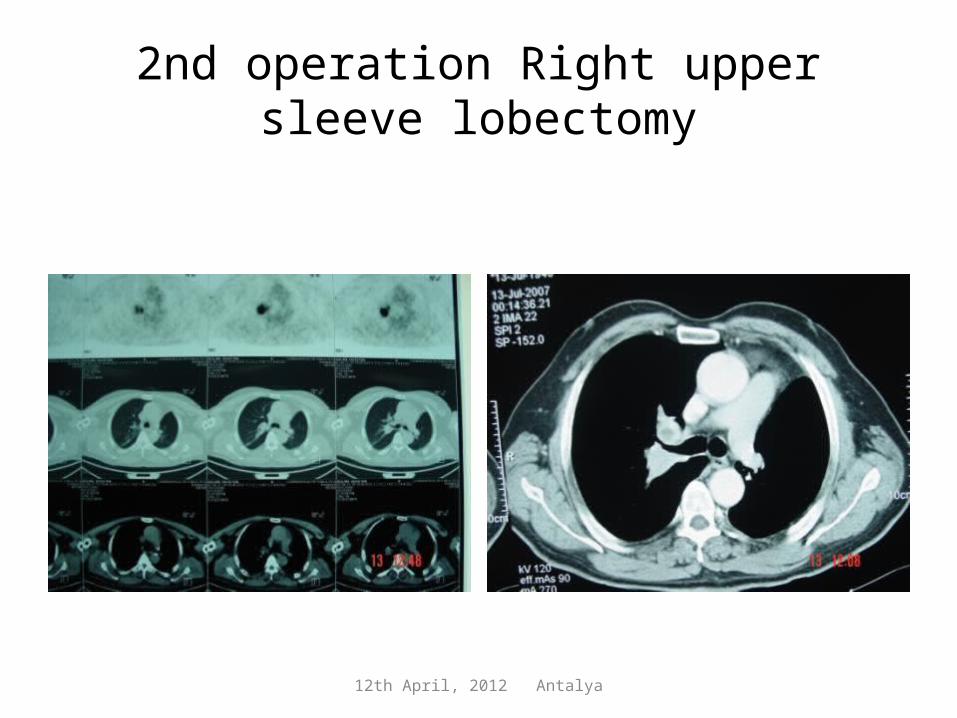
Pulmonary arterial patch brings the chance for another operation to contralateral primary lung tumor
12th April, 2012 Antalya
2nd operation Right upper sleeve lobectomy

12th April, 2012 Antalya
Tumor thrombus to main left PA
12th April, 2012 Antalya

12th April, 2012 Antalya
12th April, 2012 Antalya
12th April, 2012 Antalya
12th April, 2012 Antalya