tackling health care corruption and governance woes in developing countries maureen lewis advisor,...
TRANSCRIPT

Tackling Health Care Corruption and Governance Woes in
Developing Countries
Maureen Lewis
Advisor, HD Vice Presidency
Nonresident Fellow, CGD

Outline of Presentation
Define corruption and poor governance for the health sector
Demonstrate the relative importance of poor governance to health outcomes
Measure corruption and poor governance in health care delivery
What to do about it?

Institutions matter
Health systems are the institutions and will carry the burden In reaching the MDGs In making “cost effective” meaningful In absorbing more funding
Poor governance and corruption undermine the effectiveness of donor and country efforts to achieve better health status

Governance and corruption
Not typically addressed in health Spending often occurs even when there are
indications of poor governance KKM components of importance:
Government effectiveness Control of corruption Voice and accountability
Corruption: “use of public office for private gain”

Percent Perceiving Corruption in the Health Sector
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Sri Lanka (2002)
Khazakhstan (2001)
Peru (2001)
Bangladesh (2002)
Kyrgyz (2001)
Bosnia (2000)
Bulgaria (2002)
Senegal (2001)
Romania (2000)
Croatia (2002)
Macedonia (2002)
Slovakia (2000)
Albania (2002)
Bolivia (2001)
Madagascar (2001)
Serbia (2002)
Morroco (2001)
Moldova (2000)
Tajikistan (2001)

Control of Corruption
4060
8010
012
0
-2 -1 0 1 2Government effectiveness (KKM 2005)
4060
8010
012
0
-2 -1 0 1 2Control of corruption (KKM 2005)
R² = 0.293
R² = 0.222
4060
8010
0
-2 -1 0 1Voice and accountability (KKM 2005)
R² = 0.085
Gov’t Effectiveness Voice & Accountability
Relationship Between Corruption Indices and Immunization

Regression results on the determinants of measles immunization coverage
KKM government effectiveness indicator positive, robust and significant
Ethno-linguistic fractionalization consistently negative and significant
Average primary school completion of women important to better coverage
GDP per capita irrelevant

Separating governance from corruption Some are obvious:
“selling” official positions kickbacks, outright theft
Others are less clear Sometimes it is simply mismanagement,
inefficiency, inertia, etc. Incentives are often wrong Tracking performance tends to be a low
priority and hard to do in health

Drugs and Supplies
Drugs often go missing Costa Rica 32 of users are aware of theft Uganda drug leakage in 10 rural clinics
averaged 73% China about 30% of drugs are expired or
counterfeit Ethiopia and Nigeria recorded missing
equipment: in Ethiopia only 21 percent of hospitals have autoclaves
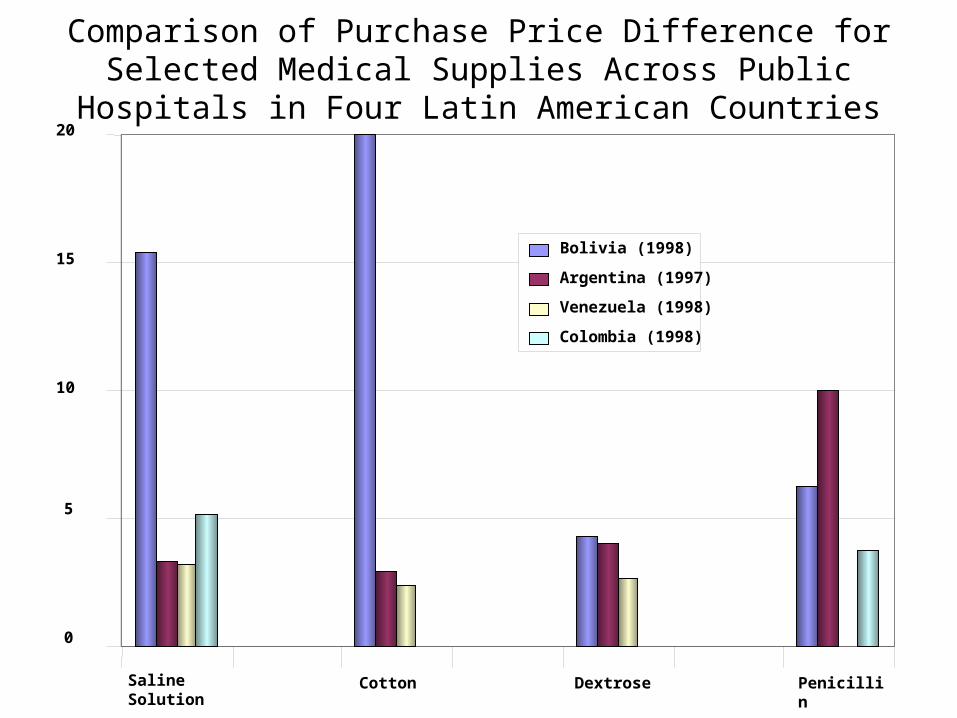
0
5
10
15
20
Saline Solution
Cotton Dextrose Penicillin
Bolivia (1998)
Argentina (1997)
Venezuela (1998)
Colombia (1998)
Comparison of Purchase Price Difference for Selected Medical Supplies Across Public Hospitals in Four Latin
American Countries

Leakage Rates for Health Care, Selected Countries
COUNTRYYEAR LEAKAGE
RATETYPE OF
EXPENDITURE
Ghana 2000 80% Non-salary budget
Peru 2001 71 “Glass of Milk” Program
Tanzania 1999 40 Non-salary budget
Uganda 2000 70 Drugs and supplies
Source: Lindelow, Kushnarova, and Kaiser, 2005
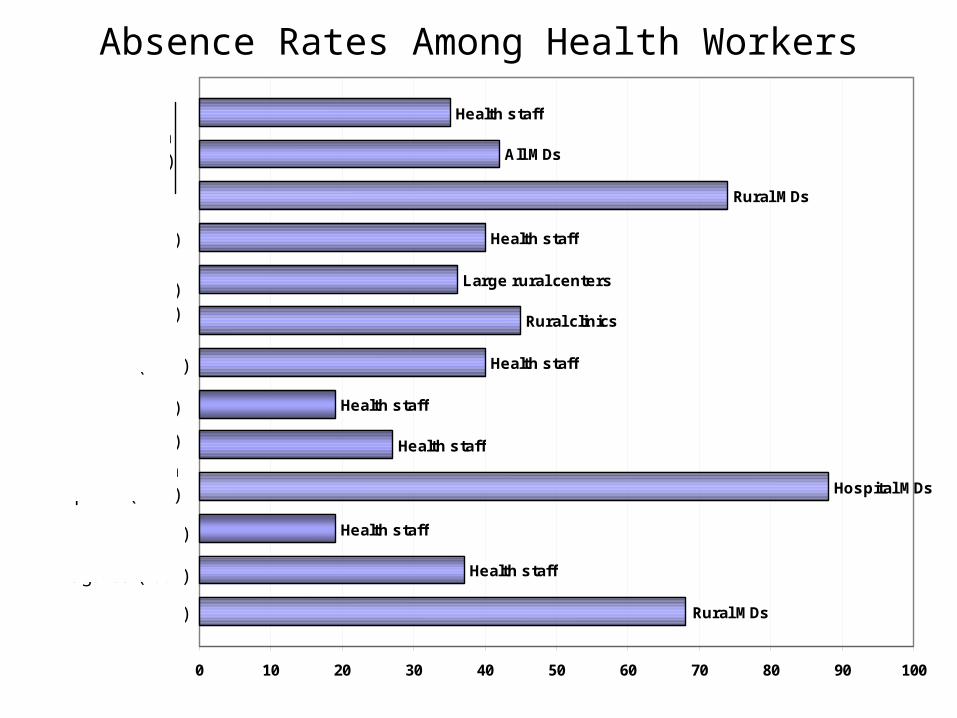
Absence Rates Among Health Workers
Health staff
Health staff
Hospital MDs
Health staff
Health staff
Health staff
Rural clinics
Large rural centers
Health staff
Rural MDs
All MDs
Health staff
Rural MDs
0 10 20 30 40 50 60 70 80 90 100
India (Udaipur) (2004)
Bangladesh(2004)
Mozambique (2003)
Indonesia (2004)
PNG (2000)
Dominican Republic (1989)
Honduras (2001)
India (2003)
Uganda (2004)
Uganda (1997)

Proportion Making Informal Payments Among Users
0 10 20 30 40 50 60 70 80 90 100
Ghana (2000)
Vietnam (1992)Thailand (2000)
Indonesia (2001)Cambodia (2000)
Peru (2001)Paraguay (1999)Colombia (2001)
Bolivia (2002)
Sri Lanka (2001)Pakistan (2002)
Nepal (2002)India (2002)
Bangladesh (2002)
Slovakia (2000)Russia (2002)
Romania (2000)Moldova (2002)
Macedonia (2002)Latvia (1998)
Kyrgyz Republic (2001)Kosovo (2000)
Hungary (2002)Czech Republic (2002)
Croatia (2002)Bulgaria (2001)
Bosnia (2002)Armenia (2001)
Albania (2001)

Informal Payments as % of Half-monthly Income
0 50 100 150 200 250
Thailand (1999)
Tajikistan (1999)
Sri Lanka (2001)
Russia (2002)
Peru (2001)
Pakistan (2002)
Krygyz (2001)
Kazakhstan (2002)**
India (2002)
Ghana (2000)
Cambodia (1999)
Bulgaria (2001)
Bolivia (2001)
Bangladesh (2002)
Armenia (2001)
Albania (2002)*
Albania (2002)
Inpatient
Outpatient

Are patients satisfied?
Corruption is common: Out of 23 countries health ranked in the top 4
most corrupt sectors in 10 countries Evidence from Pakistan, Indonesia, El
Salvador and Turkey show similar views: Low quality of public health care Limited hours and long waits Lack of non-labor inputs

What to do? Improve government effectiveness:
Mixed evidence on the impact of higher salaries, sometimes more corruption
Better incentives for health workers: employment security recruitment and promotion criteria; and capable management more important
Raise accountability (hire & fire staff locally) Improved oversight; sometimes inspectors
improve performance

Improve government effectiveness (cont.) Increase audit by central government and
autonomy of local government to ensure following of financial procedures
Address who pays: raise formal fees and ban informal payments
Contract out services with pay-for-performance
Citizen “report cards” Local oversight can be helpful

Control corruption
National anti-corruption strategy Data base of staff to bolster administration Improve records and oversight of info In Colombia and Argentina cost of supplies
declined with the use of price lists and transparent purchasing
More information to citizens about public health care expectations and performance
Make government accountable to communities/national government/oversight board

Voice: mixed results
Voting and NGO presence have minimal if any effect on corruption in Bolivia, but corruption is lower where local organizing groups are active
In Uganda and Philippines voter turnout and corruption levels are unrelated
Suggests that public service delivery does not affect voting patterns or candidate selection
Voting may be too blunt an instrument

Conclusions
Returns to health investment may be very low with corruption and low effectiveness
Institutions matter: health systems cannot be divorced from efforts to improve governance
Institutional factors need to be strengthened along with spending to improve performance
Need more evidence Health can’t be sidelined in overall corruption
agenda of donors or countries