tele-medicine in or and icu – optimizing patient outcomes · tele-medicine in or and icu –...
TRANSCRIPT

Tele-Medicine in OR and ICU –Optimizing Patient Outcomes
Prof. Lisa Weavind MBBCh FCCMDepartment of Anesthesiology
Division of Critical CareVanderbilt University
Disclosure
Grant funding from Medtronic to evaluate the clinical feasibility and necessity for respiratory surveillance monitoring in general care floor patients.

Goal and Objectives
• The use of Telemedicine in the OR and ICU environment
• Objectives:– Discuss Tele-‐monitoring in the OR and ICU– Review evidence of the effect of Tele-‐ICU on outcomes
– Understand the practical aspects of implementing Tele-‐ICU

Technology can improve…..
• Situational Awareness–Make information available without searching– Provider receives information at point-‐of-‐care– Integration of information from multiple modalities
• Decision support and best practice guidelines for timely and effective care
• Communication with reduction in errors

TeleOR Support

What is Telemedicine?
• Information technology combined with audio-‐visual communication to provide medical care from a remote location

Is Telemedicine New?• Einthoven (1906) ECG transmission over phone lines
• 1950 – Psychiatric consultation (Nebraska Psychiatric Institute and a state mental hospital.)
• 1960 –– Massachusetts General Hospital and ER at airports -‐TV microwave link
– NASA and Lockheed used audiovisual technologies to create STARPAHC (Space Technology Applied to Rural Papago Advanced Health Care) – Papago Indian reservation in Arizona and Astronauts

Situational Awareness
• Perception of environmental elements
• Comprehension of their meaning
• Predict future state based on those elements and their meaning
1. Wright MC. Objective measures of situation awareness in a simulated medical environment. Quality and Safety in Health Care. 2004;13(suppl_1):i65-‐i71.

Monitoring technology in the OR
Security Screen

Case Board -‐ Detailed

History and Physical

Notification RangeAdjustment

Multiview

Augmented Vigilance

Patient View

Tele-‐ Rapid Response Team
Tele-‐ICU
Promises
• Improved patient outcomes• Improved ICU throughput• Improved economic outcomes $81.7 B– In 2005, critical care medicine costs represented 13.4% of hospital costs, 4.1% of national health expenditures, and 0.66% of the gross domestic product.1
• Leverage of scarce resources• Intensivist support for rural/underserved areas• Improved evidenced based care in ICU
1 Halpern N.,Critical Care Medicine: January 2010 - Volume 38 - Issue 1 - pp 65-71

Human Error in the ICU
• 178 patient activities/day in ICU• 1.7 errors per patient/day• 29% deemed severe or potentially detrimental (2 per day)
• Error spikes with increased activity/reactivity/initiation or change of shift
• Communication between physicians and nurses
Donchin Y, et al:A look into the nature and causes of human errors in the intensive care unit. Crit Care Med 1995;; 23:294-300

Why do we need Tele-‐ICU?
• Intensivist Presence in the ICU–Reduced mortality (15-‐60% decrease)–Reduced complications –Reduced length of stay–Greater throughput –Reduced costs
JAMA 252:2023. 1984.
Chest 96:127. 1989.
JAMA 260:3446. 1988.
JAMA 276:322. 1996.
AJRCCM 157:1468. 1998.
AnnSurg 229:163. 1999.
MayoClinProc 72:391. 1997.
CCM 27:270. 1999.
JAMA 281:1310. 1999.

Intensivists are a Scarce Resource

Leveraging scarce resources
Virtual ICU workflow
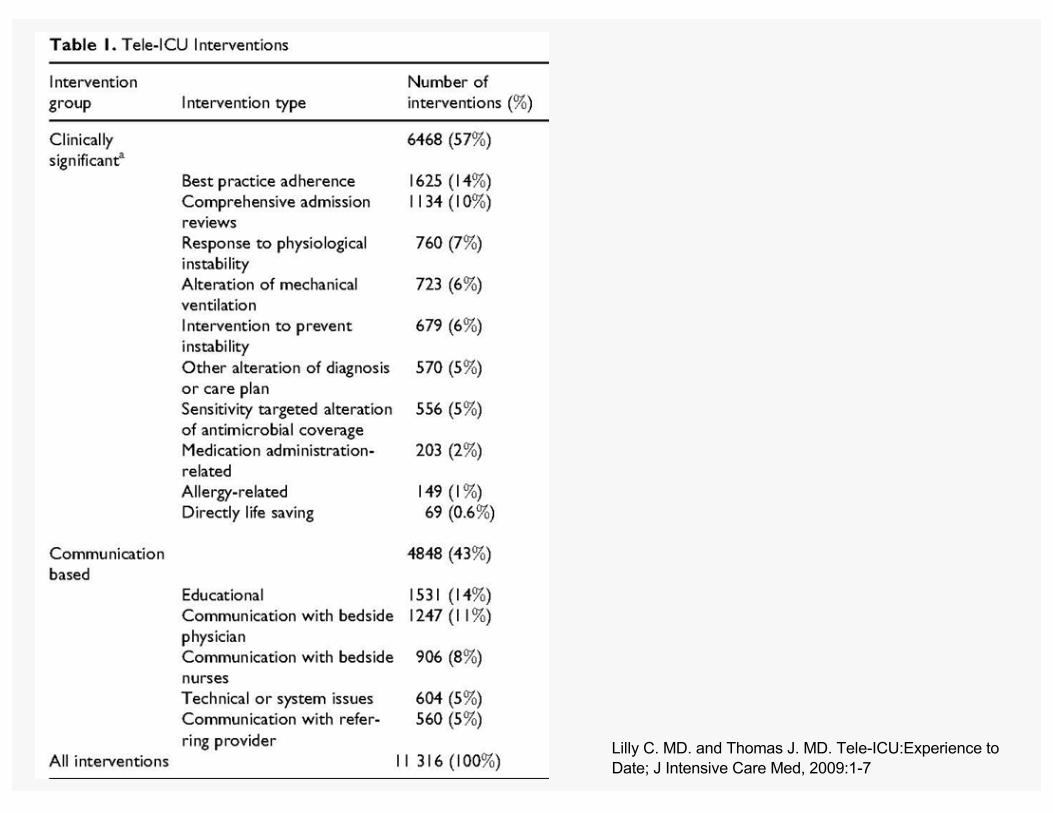
Lilly C. MD. and Thomas J. MD. Tele-ICU:Experience to Date;; J Intensive Care Med, 2009:1-7

TeleICU Impact on Rural Healthcare System
• Rural Healthcare– 40% of US hospitals in rural area– 25% of population 10% of physicians– Sub-‐specialist Care
• Urban 134.1/100,000• Rural 40.1/100,000
• Study Hospitals– 1,000,000 pts over >1,550 sq. miles– 1 tertiary care hospital (506 beds)– 3 Regional Hospitals (10,6,10 ICU beds)– 2 Community Hospitals (< 100 total beds)– 9 Critical Access Hospital (<25 beds)
Zawada ET Post Grad Med 2009: 121;; 160-170
Tele-‐ICU Impact on Rural Healthcare System
• 37.5% reduction in number of patients requiring transfer
• Decreased ICU mortality• Decreased ICU LOS (3.79 days -‐2.08 days)• Decreased Hospital LOS (10.08 days – 7.81 days)
• $ 10 mil cost savings from transfer costs, ICU and hospital costs driven by LOS
Zawada ET Post Grad Med 2009: 121;; 160-170

Let’s put the fun into dysfunction
Why isn’t everybody doing this?

Barriers to deployment of Tele-‐ICU• Culture
– Vision, leadership and willingness/need to change • Technology
– Integrated EMR, radiology, labs, CPOE and pharmacy• Reimbursement
– None• Regulation
– State – must have license to practice medicine in the state that the hospital is being monitored.
– Hospital – credentialing • Malpractice• Financial

Goals of the Demonstration Project:• Does the application of this technology
• save lives?• Shorten ICU length of stay?• Shorten hospital length of stay?• Improve practice guideline
adherence?• Improve ICU throughput?

Tele-‐ICU Outcomes

In Massachusetts -‐ Tele-‐ICU could save 350 additional lives, hospitals would make money and payers would
save $122 million

Lilly JAMA 2011;; online first May 16, 2011


Successful Tele-‐Medicine Initiative
• Patient focused quality improvement outcomes
• Detailed needs assessment • Asses barriers to change• Prioritize specific goals• Integrate all care partners• Transparency with data collection and reporting

Questions?