that’s why it’s a 5-year program: resident acquisition of anorectal disease management...
TRANSCRIPT
Journal of Surgical Research 173, 187–192 (2012)doi:10.1016/j.jss.2011.05.048
ASSOCIATION FOR ACADEMIC SURGERY
That’s Why It’s a 5-Year Program: Resident Acquisition of Anorectal Disease
Management Competence
SethMiller, M.D.,1 Vance Sohn,M.D., MarlinWayne Causey,M.D.,MatthewMartin,M.D., TommyBrown,M.D.,and Scott Steele, M.D.
Department of General Surgery, Madigan Army Medical Center, Tacoma, Washington
Originally submitted March 20, 2011; accepted for publication May 25, 2011
Background. Although surgical residents are ex-pected to be proficient in the diagnosis and manage-ment of anorectal pathology upon graduation, thereis little data related to the timing and degree of profi-ciency acquired during training.Methods. Prospective study of new patients pre-
senting to a colorectal surgical clinic for evaluationof anorectal complaints over a 3-y period. Trainees per-formed an initial evaluation and recorded their examfindings, diagnosis, and treatment plan. A separateevaluation by a staff colorectal surgeon was per-formed, with results compared by an independentreviewer.Results. A total of 236 patient evaluations were in-
cluded. The accuracy of referral diagnosis was signifi-cantly better when originated from a surgeon thanfrom all other referral sources (91.7% versus 59.1%,P[ 0.031). The most common conditions were internalhemorrhoids (25%), anal fissures (22%), and externalhemorrhoids (19.5%). Internal hemorrhoids were mostcommonly misdiagnosed as external hemorrhoids(58%). Anal fissures were missed 38% of the time, andwere most often given the diagnosis of internal hemor-rhoids (45%). Residents also demonstrated difficulty inidentifying thrombosis in external hemorrhoids, witha 45% error rate.Medical students and residents had an overall cor-
rect primary diagnosis of 69.5%; however, there wasa significant improvement in the accuracy of diagnosisfrom medical students and interns to upper level resi-dents (62.9% versus 81.2%, P [ 0.003). Medical treat-ment plans agreed between resident and staff in 74%,the surgical management agreed in 62%, and overall
1 To whom correspondence and reprint requests should be ad-dressed at Department of General Surgery, Madigan Army MedicalCenter, 9040 Fitzsimmons Drive, Tacoma, WA 98431. E-mail: [email protected].
187
the residents had the correct diagnosis and corre-sponding treatment plan in 44%. Additional adjunctiveprocedures were proposed in 66 patients with resi-dents stating the correct adjunct in 79%. The most fre-quently missed adjuncts were endorectal ultrasound(34%) and colonoscopy (28%).Conclusion. Surgical trainees demonstrated signifi-
cant deficiencies in the ability to evaluate andmanageanorectal pathology; however, marked improvementoccurred with time in training. Common areas of mis-diagnosis and therapeutic errors were identifiedwhich could aid in curriculum development. Published
by Elsevier Inc.
Key Words: resident education; colorectal exam; ano-rectal pathology; resident proficiency.
INTRODUCTION
Graduating general surgeons are expected to be pro-ficient in the diagnosis and management of commonanorectal pathology, yet there is little data availableas to the timing and degree of proficiency acquired dur-ing medical school and resident training. The Accredi-tation Council for Graduate Medical Education hasemphasized core competencies and outcomes-based ed-ucation all within the confines of mandated structuralchanges, such as the 80-h work-week. These changeshave led to organized outcomes-based approacheswithin varying residencies that emphasize formal profi-ciency evaluations [1–3]. Additionally, new emphasishas been placed on how well prepared residents are totransition into practice, both in terms of acquiring ad-vanced technical skills as well as having a knowledgebase that prepares themto function effectively as aprac-ticing surgeon [4–7]. While the management of anorec-tal disease is a common component of most general
0022-4804/$36.00Published by Elsevier Inc.
JOURNAL OF SURGICAL RESEARCH: VOL. 173, NO. 2, APRIL 2012188
surgeons’ practice, there is often little emphasis on theeducation of anorectal pathology, with U.S. surgicaltrainees performing an average of only 30 anorectalcases throughout a 5-year residency [8]. In many cases,this small operative experience encompasses themajor-ity of exposure to anorectal pathology, as outpatientclinical experience is also severely limited [9]. Defi-ciencies must then be made up by lecture andtextbook-based learning, neither of which may suffi-ciently expose the trainee to the complex nature of ano-rectal disease, which is often encountered in practice.With additional limitations in place by the current envi-ronment of residency training, it becomes extremely im-portant to build a core curriculum around both commonareas of pathology and dedicated instruction on gaps inknowledge. The aim of this study, therefore, was to eval-uate the competence of medical students and surgicalresidents in the diagnosis, treatment, andmanagementof anorectal pathology. In addition, our goal was to as-sess for improvement with increasing levels of trainingexperience, and to help identify common deficiencies inknowledge to help guide curriculum development.
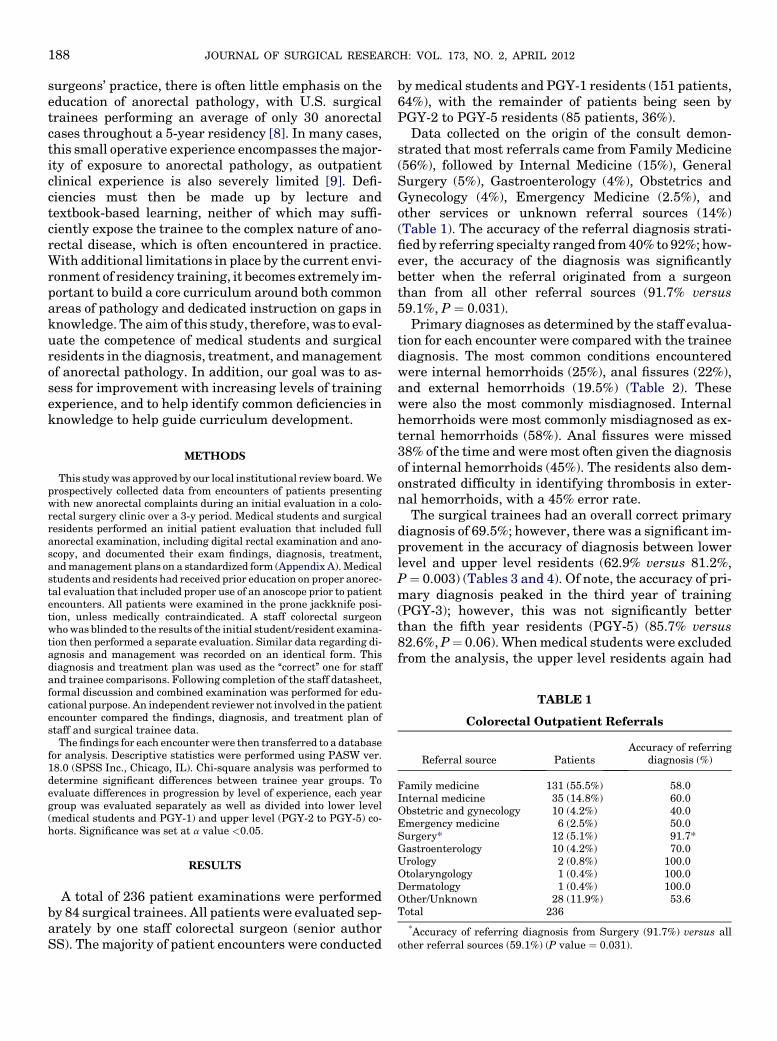
TABLE 1
Colorectal Outpatient Referrals
Referral source PatientsAccuracy of referring
diagnosis (%)
Family medicine 131 (55.5%) 58.0Internal medicine 35 (14.8%) 60.0Obstetric and gynecology 10 (4.2%) 40.0Emergency medicine 6 (2.5%) 50.0Surgery* 12 (5.1%) 91.7*
METHODS
This studywas approved by our local institutional review board.Weprospectively collected data from encounters of patients presentingwith new anorectal complaints during an initial evaluation in a colo-rectal surgery clinic over a 3-y period. Medical students and surgicalresidents performed an initial patient evaluation that included fullanorectal examination, including digital rectal examination and ano-scopy, and documented their exam findings, diagnosis, treatment,andmanagement plans on a standardized form (Appendix A).Medicalstudents and residents had received prior education on proper anorec-tal evaluation that included proper use of an anoscope prior to patientencounters. All patients were examined in the prone jackknife posi-tion, unless medically contraindicated. A staff colorectal surgeonwhowas blinded to the results of the initial student/resident examina-tion then performed a separate evaluation. Similar data regarding di-agnosis and management was recorded on an identical form. Thisdiagnosis and treatment plan was used as the ‘‘correct’’ one for staffand trainee comparisons. Following completion of the staff datasheet,formal discussion and combined examination was performed for edu-cational purpose. An independent reviewer not involved in the patientencounter compared the findings, diagnosis, and treatment plan ofstaff and surgical trainee data.
The findings for each encounterwere then transferred to a databasefor analysis. Descriptive statistics were performed using PASW ver.18.0 (SPSS Inc., Chicago, IL). Chi-square analysis was performed todetermine significant differences between trainee year groups. Toevaluate differences in progression by level of experience, each yeargroup was evaluated separately as well as divided into lower level(medical students and PGY-1) and upper level (PGY-2 to PGY-5) co-horts. Significance was set at a value <0.05.
Gastroenterology 10 (4.2%) 70.0Urology 2 (0.8%) 100.0Otolaryngology 1 (0.4%) 100.0Dermatology 1 (0.4%) 100.0Other/Unknown 28 (11.9%) 53.6Total 236
*Accuracy of referring diagnosis from Surgery (91.7%) versus allother referral sources (59.1%) (P value ¼ 0.031).
RESULTS
A total of 236 patient examinations were performedby 84 surgical trainees. All patientswere evaluated sep-arately by one staff colorectal surgeon (senior authorSS). The majority of patient encounters were conducted
bymedical students and PGY-1 residents (151 patients,64%), with the remainder of patients being seen byPGY-2 to PGY-5 residents (85 patients, 36%).
Data collected on the origin of the consult demon-strated that most referrals came from Family Medicine(56%), followed by Internal Medicine (15%), GeneralSurgery (5%), Gastroenterology (4%), Obstetrics andGynecology (4%), Emergency Medicine (2.5%), andother services or unknown referral sources (14%)(Table 1). The accuracy of the referral diagnosis strati-fiedby referring specialty ranged from40% to 92%; how-ever, the accuracy of the diagnosis was significantlybetter when the referral originated from a surgeonthan from all other referral sources (91.7% versus59.1%, P ¼ 0.031).
Primary diagnoses as determined by the staff evalua-tion for each encounter were compared with the traineediagnosis. The most common conditions encounteredwere internal hemorrhoids (25%), anal fissures (22%),and external hemorrhoids (19.5%) (Table 2). Thesewere also the most commonly misdiagnosed. Internalhemorrhoids were most commonly misdiagnosed as ex-ternal hemorrhoids (58%). Anal fissures were missed38% of the time andweremost often given the diagnosisof internal hemorrhoids (45%). The residents also dem-onstrated difficulty in identifying thrombosis in exter-nal hemorrhoids, with a 45% error rate.
The surgical trainees had an overall correct primarydiagnosis of 69.5%; however, there was a significant im-provement in the accuracy of diagnosis between lowerlevel and upper level residents (62.9% versus 81.2%,P¼ 0.003) (Tables 3 and 4). Of note, the accuracy of pri-mary diagnosis peaked in the third year of training(PGY-3); however, this was not significantly betterthan the fifth year residents (PGY-5) (85.7% versus82.6%,P¼ 0.06).Whenmedical students were excludedfrom the analysis, the upper level residents again had

TABLE 2
Frequency of Diagnoses
Diagnoses Patients
Normal exam 6 2.5%Internal hemorrhoids 58 24.6%External hemorrhoids
(nonthrombosed)46 19.5%
External hemorrhoids (thrombosed) 13 5.5%Anal bleeding 1 0.4%Fissure 52 22.0%Fistula 8 3.4%Pilonidal 4 1.7%Pruritis 8 3.4%Cancer/mass 8 3.4%Benigns mass/skin tag 17 7.2%Abscess 2 0.8%Incontinence 1 0.4%Condyloma 5 2.1%Stricture 1 0.4%Rectocele/enterocele 2 0.8%Rectal prolapse 4 1.7%Total 236
TABLE 4
Accuracy of Primary Diagnosis
Lower level Upper level Total P value
Primary diagnosis correctYesNumber of patients 95 69 164 0.003% 62.9 81.2 69.5
NoNumber of patients 56 16 72% 37.1 18.8 30.5
TABLE 5
Surgical Management
(A)
Surgical intervention Patients
Hemorrhoidectomy 43 (18.2%)Excision 32 (13.6%)LIS 4 (1.7%)I & D 6 (2.5%)
MILLER ET AL.: RESIDENT ACQUISITION OF ANORECTAL DISEASE MANAGEMENT COMPETENCE 189
a statistically significant improvement in accuracy ofdiagnosis (64.5% versus 81.2%, P ¼ 0.015).
Overall, themedical treatment plans, (including fiberregimen, Sitz baths, topical treatments, botulinumtoxin injections, or need for surgery or biopsy) agreedbetween trainee and staff in 74%, with no statistical dif-ference between lower and upper level residents (70.2%versus 80.0%, P ¼ 0.10). With medical students ex-cluded, the values remained similar (74.7% versus80.0%, P ¼ 0.49).
The locations of anorectal lesions identified on examwere documented using a standardized diagram.When the residents correctly diagnosed an internalhemorrhoid, the documented location of the hemor-rhoid matched the staff’s documented location in 70%.Of the missed locations, over half were documented onthe exact opposite site indicating confusion betweenleft and right, or anterior and posterior. When the diag-nosis was anal fissure, the residents accurately docu-mented the location in 81% of patients. However, theremaining 19% of patients had midline fissures thatwere incorrectly documented as lateral in location.
TABLE 3
Summary of Resident Performance
Lower levelresidents
Upper levelresidents P value
Correct primary diagnosis 62.9% 81.2% 0.003Correct medical treatment 70.2% 80.0% 0.101Correct surgical treatment 56.3% 71.8% 0.019Correct use of adjuncts 76.2% 84.7% 0.256
Surgical intervention was required in 52% of thepatient encounters. These interventions includedhemorrhoidectomy (35.2%), excision of skin tag ormass (26.2%), hemorrhoid banding (14.8%), exam un-der anesthesia with or without seton placement(9.0%), incision and drainage (4.9%), biopsy (4.1%),lateral internal sphincterotomy (3.3%), and fistulot-omy (2.5%). Overall, trainees documented the correctsurgical plan in 61.9%, with upper level residents be-ing significantly more likely to document a correctsurgical plan (56.3% versus 71.8%, P ¼ 0.019)(Table 5). These findings persisted after exclusion ofmedical students (56.1% versus 71.8%, P ¼ 0.035).
Adjunctive procedures were ordered in 66 patients(29%). These adjuncts included colonoscopy (65.2%),endorectal ultrasound (13.6%), defecography (6.1%),flexible sigmoidoscopy (4.5%), CT scan (3%), anal ma-nometry (3%), biopsy (3%), and esophagoduodenoscopy(1.5%). The trainees documented a correct adjunctiveprocedure in 79% of these patient encounters, and
Fistulotomy 3 (1.3%)EUA 6 Seton 11 (4.7%)Banding 18 (7.6%)Biopsy 5 (2.1%)None/Other 114 (48.3%)Total 236 (100%)
(B)
Lower level Upper level P value
Correct surgical plan 85 (56.3%) 61 (71.8%) 0.019Incorrect surgical plan 66 (43.7%) 24 (28.2%)

TABLE 6
Adjuncts
(A)
Adjunct
Colonoscopy 43 (65.2%)Flexible sigmoidoscopy 3 (4.5%)ERUS 9 (13.6%)Defecography 4 (6.1%)CT scan 2 (3.0%)Anal manometry 2 (3.0%)EGD 1 (1.5%)Biopsy 2 (3.0%)Total 66 (100%)
(B)
Lower level Upper level P value
Correct adjunct 115 (76.2%) 72 (84.7%) 0.256Incorrect adjunct 35 (23.2%) 13 (15.3%)
JOURNAL OF SURGICAL RESEARCH: VOL. 173, NO. 2, APRIL 2012190
there was no significant difference between upper andlower level residents in documenting appropriate ad-junctive procedures (76.2% versus 84.7%, P ¼ 0.256;with exclusion of medical students 78.5% versus84.7%, P ¼ 0.352). The most frequently missed ad-juncts were endorectal ultrasound (34%) and colono-scopy (28%) (Table 6).
DISCUSSION
Anorectal pathology is a common component of mostgeneral surgery practices, yet there is little emphasisplaced on the training of residents in anorectal disease.While other subspecialties, such as cardiothoracic andneurosurgery, which are rarely a common componentof a general surgical practice, have entire sections de-voted to them in general surgical textbooks, anorectaldisease does not often have its own section and withinsurgical texts anorectal pathology is usually repre-sented in only a single chapter. Furthermore, clinicalexperience and overall operative experience are lackingcompared with other surgical pathology such as breast,hernia, hepatobiliary, gastrointestinal, and vascularoperations [10]. With such little emphasis placed onanorectal pathology, it is not surprising that overall de-ficiencies in diagnosis, evaluation, and managementwere noted in our study.
The most common errors occurred in the diagnosis ofhemorrhoids and fissures—two of the most commonanorectal complaints. Lower level residents had diffi-culty in distinguishing between internal and externalhemorrhoids as well as determining whether or notan external hemorrhoid was thrombosed. As this has
a significant impact on therapeutic options, it is impor-tant to identify these weaknesses at all levels for bothproper care and lifelong learning. The residents failedto document the presence of an anal fissure 38% of thetime. More importantly, they frequently documentedfissures to be in a lateral, off-midline position demon-strating a knowledge deficit as to the significance ofa lateral fissure in suggesting the possibility of otherdisease processes, such as Crohn’s. The above defi-ciencies identified in this study could be easily remediedwith brief lectures on anorectal anatomy and pathologyand picture representation or patient examples of vari-ous common anorectal pathologies. However, as theseconditions are common, these deficienciesmay be easilyoverlooked in residency programs that place so littleemphasis on anorectal pathology and lead to improperpatient care.
Some may argue that the limited exposure duringresident training is inadequate for the proper diagnosisand management of anorectal pathology. Furthermore,perhaps these conditions should be managed exclu-sively by colorectal surgeons [8]. Supporters of this ar-gue that colorectal surgeons may be better equippedto manage anorectal disease following dedicated train-ing during fellowship where substantially more anorec-tal procedures are performed in 1 y of fellowship thanthe average trainee performs in 5 y of residency [11].However, given the prevalence of anorectal disease, rel-egating this realm to colorectal surgeons is impracticalin most settings and even unnecessary, given our find-ing of general surgeons’ accurate referral diagnosis in92% of cases. Yet considering the deficiencies noted bythe trainees, certainly there remainsmuch room for im-proving resident curriculum in regards to anorectal pa-thology. Indeed, in the era of the 80-h work wk, thequestion of experience and proficiency affects all facetsof general surgery, not just anorectal pathology.
While the deficiencies noted in the lower level resi-dents seemed to improve over experience in residency,the exposure to anorectal pathology decreased in thelater years of training with only 36% of the patients inthis study being seen by upper level residents. Whilenot statistically significant, the peak diagnostic accu-racy in the third year of training offers some evidencethat some competencies may be lost over time with de-creased exposure to anorectal pathology in the lateryears of training. It would stand to reason that defi-ciencies noted in the upper level resident evaluationcould be improved with dedicated colorectal surgeryoutpatient clinic experience during the final year priorto graduation.
This study was limited by skewed distribution of res-idents participating in these patient encounters, withthe majority of patients being seen by medical studentsand first year residents. Furthermore, the exposure to

MILLER ET AL.: RESIDENT ACQUISITION OF ANORECTAL DISEASE MANAGEMENT COMPETENCE 191
anorectal disease pathology in medical school is vari-able, and refinement of medical school curriculummay be beneficial for future surgeons, as well as for pri-mary care providers who will frequently encounterthese common anorectal diseases. The relatively smallsample size of the upper level resident groups was an-other limitation, and this may have masked more sub-tle differences between year groups. Additionally,individual residents were not identified, so individualimprovement throughout training could not be demon-strated. Another limitation to this study is that the find-ings are limited to what was documented on thestandardized form. Particularly in the area of docu-menting the location of anal lesions, there was inconsis-tency in identifying the location of the lesions, whichemphasizes the importance of using proper anatomicaldescriptions as opposed to clockface descriptions. Fi-nally, while this study sought to find commonweaknessfor the purposes of curriculum improvement, this wasa single institution study and it is unclear if these find-ings are generalizable to all surgical trainees. Despitethese limitations, this was a blinded studywith an inde-pendent reviewer that led to the identification of inher-ent weakness in the core education of general surgeryresidents that can be used for curriculum development.
One strategy for improving anorectal curriculum,proposed by Hyman et al. [12] is to add a fulltime colo-rectal surgeon to the faculty of residency programs. Intheir 10-y, retrospective review, after addition of a full-time colorectal staff there was a 37% increase in anorec-tal procedures with a 442% increase in anorectal casesperformed by chief residents. Our study supports theidea of inclusion of colorectal surgery faculty intrinsi-cally as it was a project initiated by a colorectal special-ist with the very aim of identifying common deficienciesfor improved anorectal curriculum.
CONCLUSIONS
Surgical trainees demonstrated significant defi-ciencies in the ability to evaluate and manage anorec-tal pathology, but showed marked improvement withtime in residency training. The deficiencies identified
concerned common anorectal pathologies, which maybe overlooked in surgical programs, especially thosethat lack colorectal faculty. Common areas of misdiag-nosis and therapeutic errors were identified, whichcould guide curriculum development.
ACKNOWLEDGMENT
The investigators have adhered to the policies for protection of hu-man subjects as prescribed in 45 CFR 46. The views expressed arethose of the authors and do not reflect the official policy of the Depart-ment of the Army, the Department of Defense, or the U.S.Government.
REFERENCES
1. Bancroft GN, BasuCB, LeongM, et al. Outcome-based residencyeducation: Teaching and evaluating the core competencies inplastic surgery. Plast Reconstr Surg 2008;121:441e.
2. Sanfey H, Dunnington G. Verification of proficiency: A prerequi-site for clinical experience. Surg Clin North Am 2010;90:559.
3. SanfeyH, Ketchum J, Bartlett J, et al. Verification of proficiencyin basic skills for postgraduate year 1 residents. Surgery2010;148:759; discussion 766.
4. Doty B, Zuckerman R, Borgstrom D. Are general surgery resi-dency programs likely to prepare future rural surgeons?J Surg Educ 2009;66:74.
5. Hwang H. Does general surgery residency prepare surgeons forcommunity practice in British Columbia? Can J Surg 2009;52:196.
6. Javid SH, Ashley S, Breen E. A colorectal curriculum for generalsurgery residents: Are we ready for needs assessment? J SurgEduc 2007;64:324.
7. Stefanidis D, Acker CE, Swiderski D, et al. Challenges duringthe implementation of a laparoscopic skills curriculum ina busy general surgery residency program. J Surg Educ 2008;65:4.
8. Hyman NH, Hebert JC. Do general surgery residency programsadequately train surgeons to perform anorectal surgery? DisColon Rectum 1993;36:73.
9. Jones K, Lebron RA, Mangram A, et al. Practice managementeducation during surgical residency. Am J Surg 2008;196:878.discussion 881.
10. Bell RH Jr, Biester TW, Tabuenca A, et al. Operative experienceof residents in US general surgery programs: A gap betweenexpectation and experience. Ann Surg 2009;249:719.
11. Schoetz DJ Jr. Colon and rectal surgery: A true subspecialty. DisColon Rectum 1998;41:1.
12. Hyman NH. Impact of a colon and rectal surgeon on a generalsurgery residency training program. Dis Colon Rectum 1999;42:249.

JOURNAL OF SURGICAL RESEARCH: VOL. 173, NO. 2, APRIL 2012192