the “acontractile” bladder - comtecgroup “acontractile” bladder - fact or fiction? jacob...
TRANSCRIPT
THE “ACONTRACTILE” BLADDER -
FACT OR FICTION?
Jacob Golomb
Department of Urology
Chaim Sheba Medical Center
Tel Hashomer
NEUROGENIC UNDERACTIVE DETRUSOR
Central (complete/incomplete):
• Spinal cord injury- trauma, vascular, disc disease, spinal stenosis
• Spinal cord disease- myelitis, tumor, MS, spina bifida
• Conus medullaris injury (cauda equina syndrome)
NEUROGENIC UNDERACTIVE DETRUSOR (cont.)
Peripheral- pelvic plexus injury:
• Trauma
• Infection (herpes zoster, Guillain-Barre’ syndrome)
• Pelvic tumor extending to nerves
• Major pelvic ablative surgery (Miles operation, low anterior resection
of rectum, radical hysterectomy)
Diabetic cystopathy:
Decreased bladder sensation Increased capacity
Impaired contractility
• Permanent catheter drainage
• Intermittent catheterization
• Sphincterotomy
Treatment of all entities aims at adequate bladder emptying and
low-pressure storage
TREATMENT OPTIONS FOR NEUROGENIC UNDERACTIVE DETRUSOR
NON-NEUROGENIC UNDERACTIVE DETRUSOR
• DOIC (Detrusor Overactivity with Impaired Contractility)
• Psychogenic urinary retention
• Long-standing bladder outlet obstruction
• Aging
• Idiopathic conditions
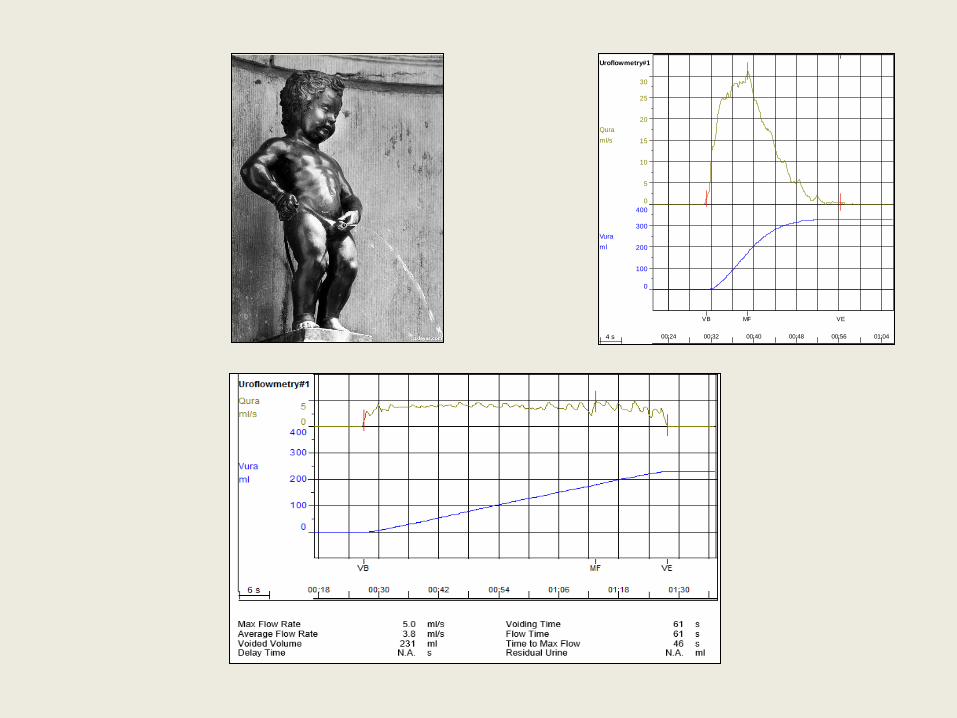
“ICS Standard Urodynamic Test: Uroflowmetry and PVR plus
transurethral cystometry and pressure-flow study, all performed in the patient’s
preferred or most usual position; usually comfortably seated and or standing
if physically possible.
The patient(s) may be then reported as having had an ICS standard
urodynamic test (ICS-SUT)’.”.
Peter F.W.M Rosier et al: International Continence Society Standard Good Urodynamic Practices and
Terms 2015. Urodynamics, Uroflowmetry, Cystometry and Pressure-Flow Study.
www.ics.org/Documents/DocumentsDownload.aspx?DocumentID=3077.
Qura
ml/s
0
5
10
15
20
25
30
Vura
ml
0
100
200
300
400
Uroflowmetry#1
4 s 00:24 00:32 00:40 00:48 00:56 01:04
VB MF VE
Qura
ml/s0
5
Vura
ml
0
100
200
300
400
Uroflowmetry#1
20 s 01:20 02:00 02:40 03:20 04:00
VB MF VE
Qura
ml/s0
5
Vura
ml
0
100
200
300
400
Uroflowmetry#1
15 s 00:00 00:30 01:00 01:30 02:00 02:30 03:00
ST
VB
MF VE
Qura
ml/s0
5
Vura
ml
0
100
200
300
400
Uroflowmetry#1
8 s 00:56 01:12 01:28 01:44 02:00 02:16
VB MF VE
Qura
ml/s
0
5
10
15
Vura
ml
0
100
200
300
400
Uroflowmetry#1
4 s 00:44 00:52 01:00 01:08 01:16 01:24 01:32
VB MF VE
Qura
ml/s
0
5
10
15
20
Vura
ml
0
100
200
300
400
Uroflowmetry#1
4 s 00:28 00:36 00:44 00:52 01:00 01:08 01:16
VB MF VE
Vura
ml0
500
Pdet
cmH2O
0
100
200
300
Pves
cmH2O
0
100
200
300
Pabd
cmH2O
0
100
200
300
Qura
ml/s
0
50
100
150
EMGave
uV
0
10000
20000
30000
Filling & Voiding Cystometry#1
7 s 11:29 11:43 11:57 12:11 12:25 12:39 12:53
CC PI10
VB
PI11 PI12 MF
PI13
PI14
MP
PI15
PI16
VEPI17
Unobstructed
Equivocal
Obstructed
Qura [ml/s]
Pdet [cmH2O]
2 4 6 8 10 12 14 16 18 20 22 24 26
20
40
60
80
100
120
140
160
180
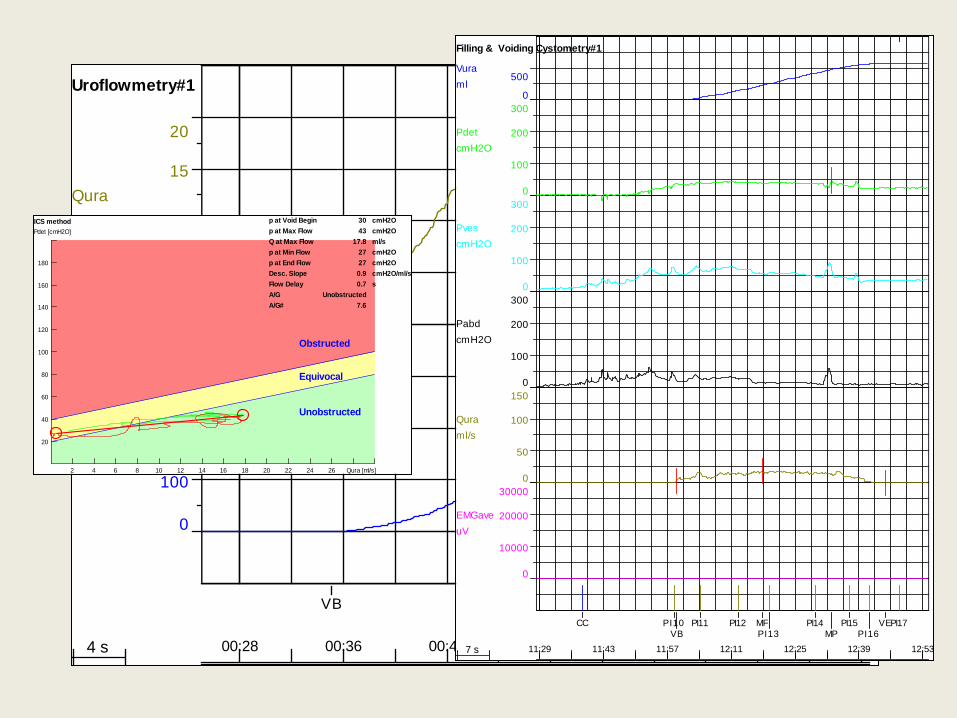
ICS method p at Void Begin cmH2O30
p at Max Flow cmH2O43
Q at Max Flow ml/s17.8
p at Min Flow cmH2O27
p at End Flow cmH2O27
Desc. Slope cmH2O/ml/s0.9
Flow Delay s0.7
A/G Unobstructed
A/G# 7.6
Qura
ml/s
0
5
10
Vura
ml
0
100
200
300
400
Uroflowmetry#1
6 s 01:24 01:36 01:48 02:00 02:12 02:24
VB MF VE
Vura
ml0
500
Pdet
cmH2O
0
100
200
300
Pves
cmH2O
0
100
200
300
Pabd
cmH2O
0
100
200
300
Qura
ml/s
0
50
100
150
EMGave
uV
0
100
200
300
Filling & Voiding Cystometry#1
9 s 09:54 10:12 10:30 10:48 11:06 11:24 11:42
CC VB MP MF VE
Unobstructed
Equivocal
Obstructed
Qura [ml/s]
Pdet [cmH2O]
2 4 6 8 10 12 14 16 18 20 22 24 26
20
40
60
80
100
120
140
160
180
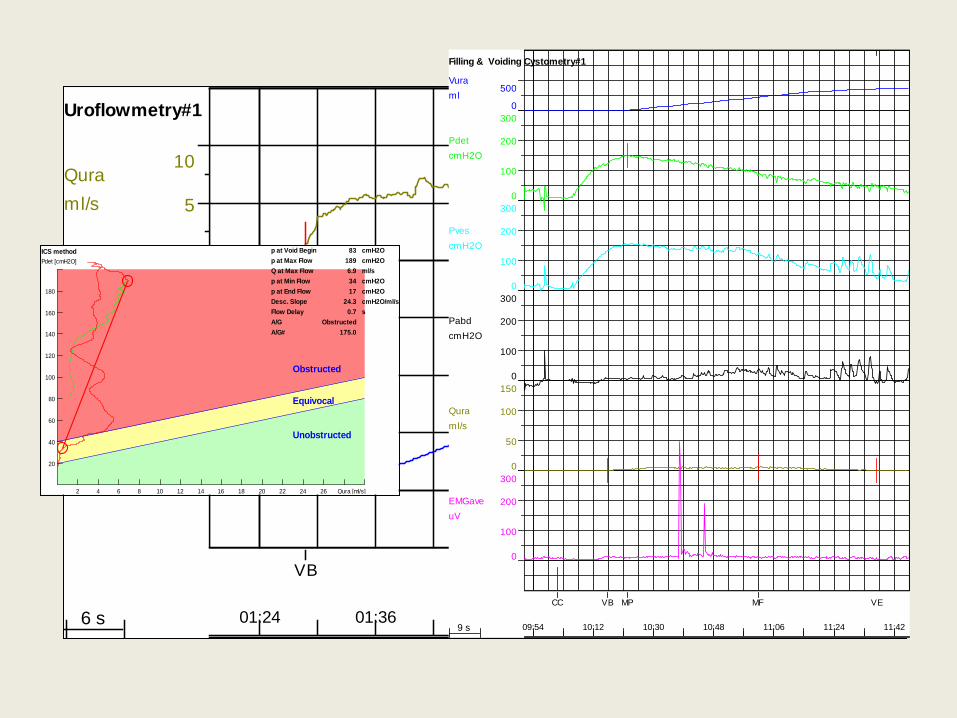
ICS method p at Void Begin cmH2O83
p at Max Flow cmH2O189
Q at Max Flow ml/s6.9
p at Min Flow cmH2O34
p at End Flow cmH2O17
Desc. Slope cmH2O/ml/s24.3
Flow Delay s0.7
A/G Obstructed
A/G# 175.0
Qura
ml/s0
5
Vura
ml
0
100
200
300
400
Uroflowmetry#1
20 s 01:20 02:00 02:40 03:20 04:00
VB MF VE
Vura
ml0
500
Pdet
cmH2O
0
100
200
300
Pves
cmH2O
0
100
200
300
Pabd
cmH2O
0
100
200
300
Qura
ml/s
0
50
100
150
EMGave
uV
0
20
40
60
Filling & Voiding Cystometry#1
15 s 09:52 10:22 10:52 11:22 11:52
CC
PI16
PI17
PI18
PI19
VB
PI20
PI21
MF
PI22
PI23
PI24
PI25
MP
PI26
PI27
PI28
PI29
PI30
PI31
PI32
PI33
PI34
PI35
PI36VE
PI37
Unobstructed
Equivocal
Obstructed
Qura [ml/s]
Pdet [cmH2O]
2 4 6 8 10 12 14 16 18 20 22 24 26
20
40
60
80
100
120
140
160
180
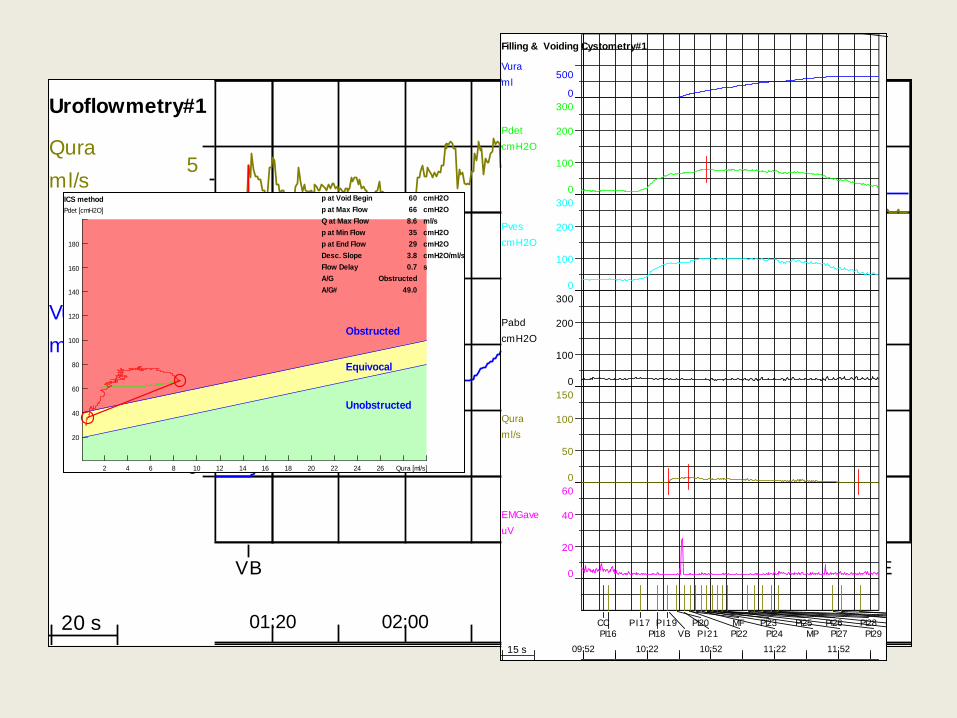
ICS method p at Void Begin cmH2O60
p at Max Flow cmH2O66
Q at Max Flow ml/s8.6
p at Min Flow cmH2O35
p at End Flow cmH2O29
Desc. Slope cmH2O/ml/s3.8
Flow Delay s0.7
A/G Obstructed
A/G# 49.0
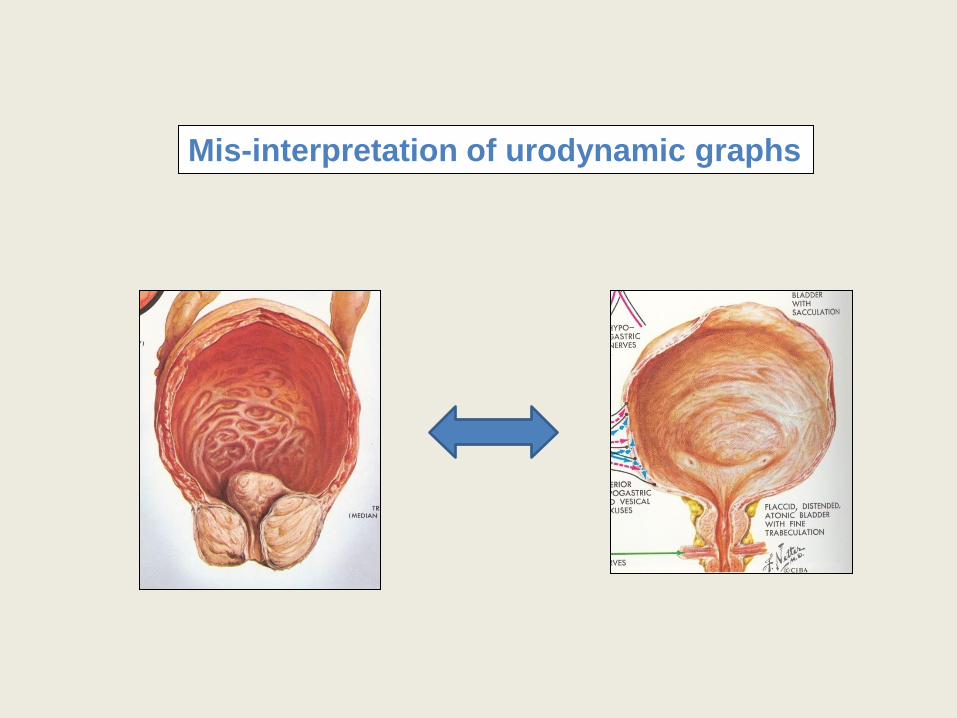
Mis-interpretation of urodynamic graphs
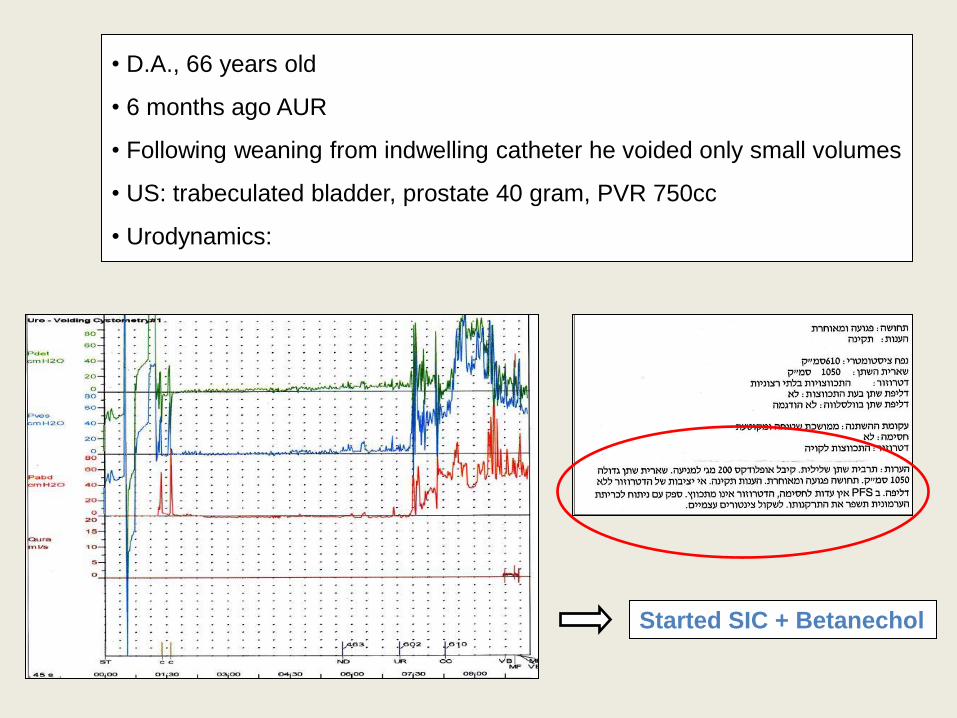
• D.A., 66 years old
• 6 months ago AUR
• Following weaning from indwelling catheter he voided only small volumes
• US: trabeculated bladder, prostate 40 gram, PVR 750cc
• Urodynamics:
Started SIC + Betanechol
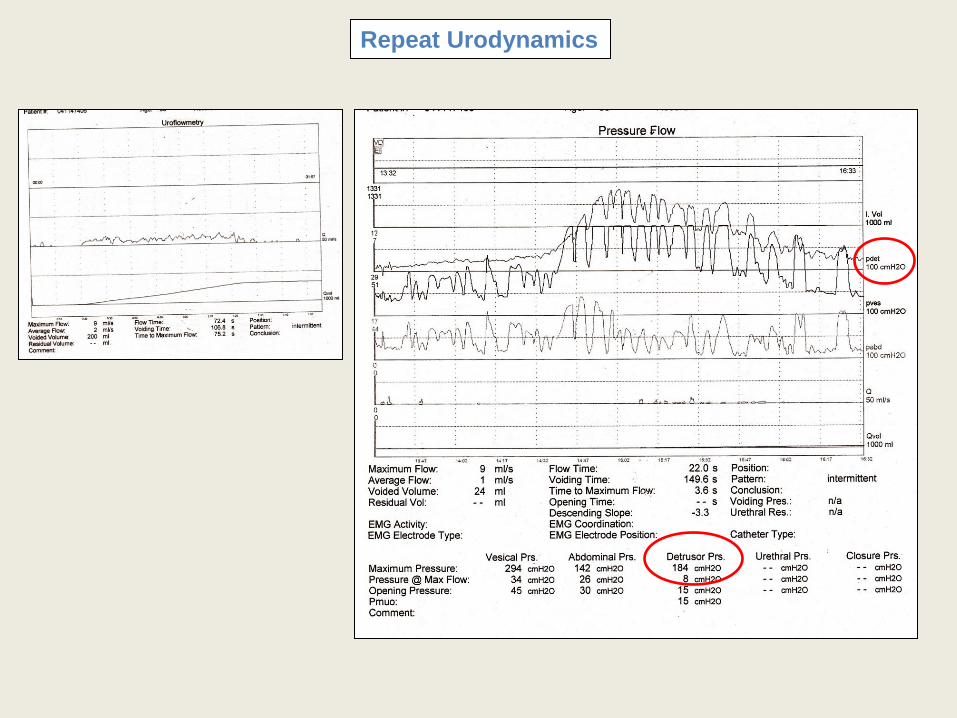
Repeat Urodynamics
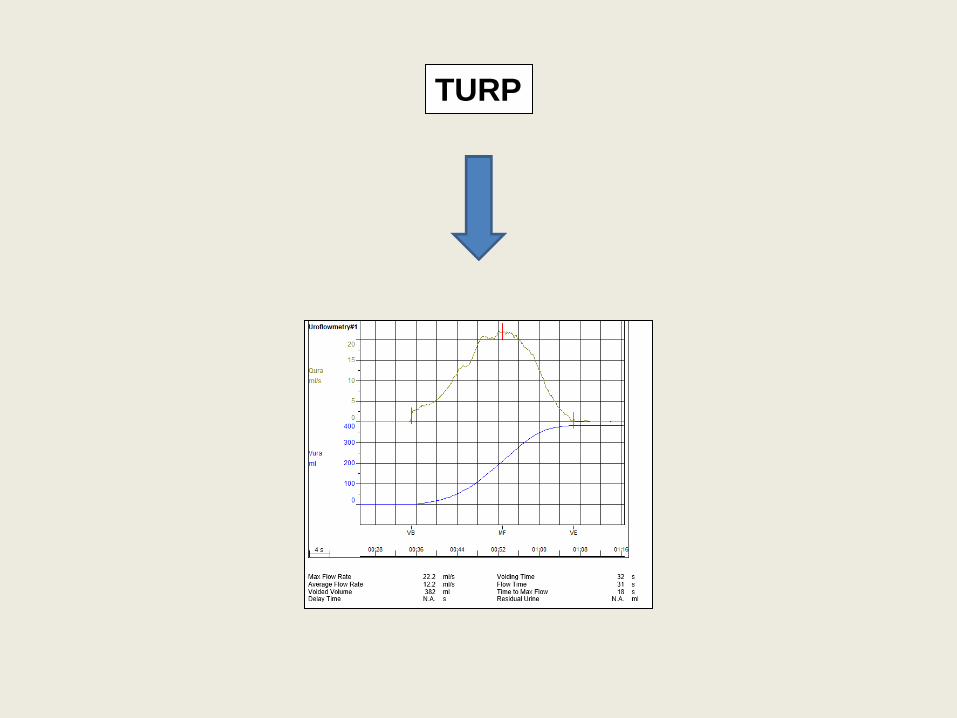
TURP
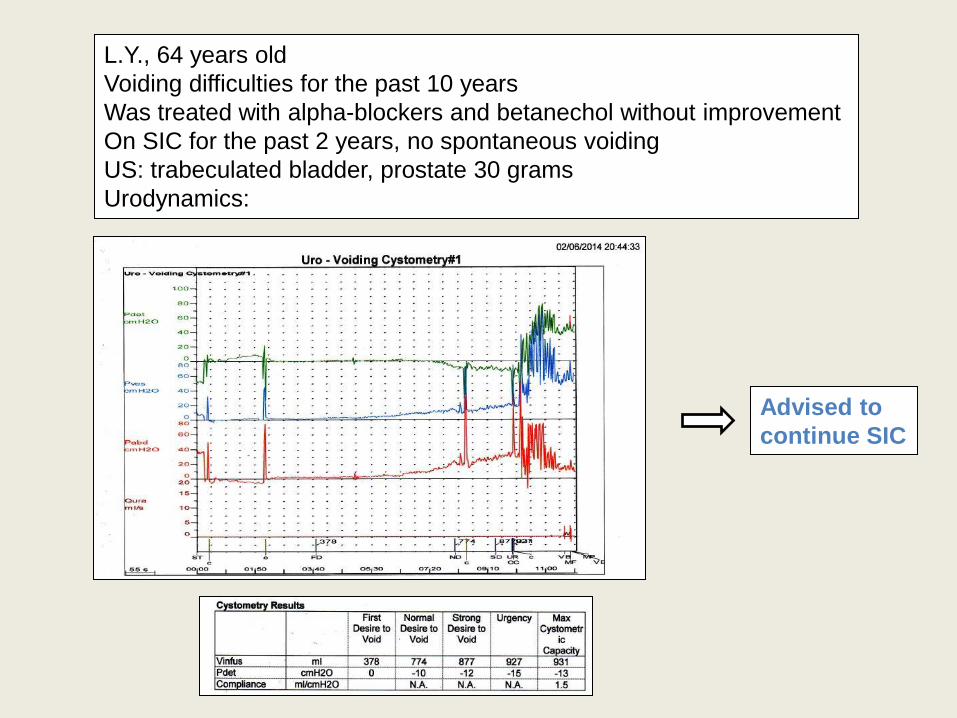
L.Y., 64 years old
Voiding difficulties for the past 10 years
Was treated with alpha-blockers and betanechol without improvement
On SIC for the past 2 years, no spontaneous voiding
US: trabeculated bladder, prostate 30 grams
Urodynamics:
Advised to
continue SIC
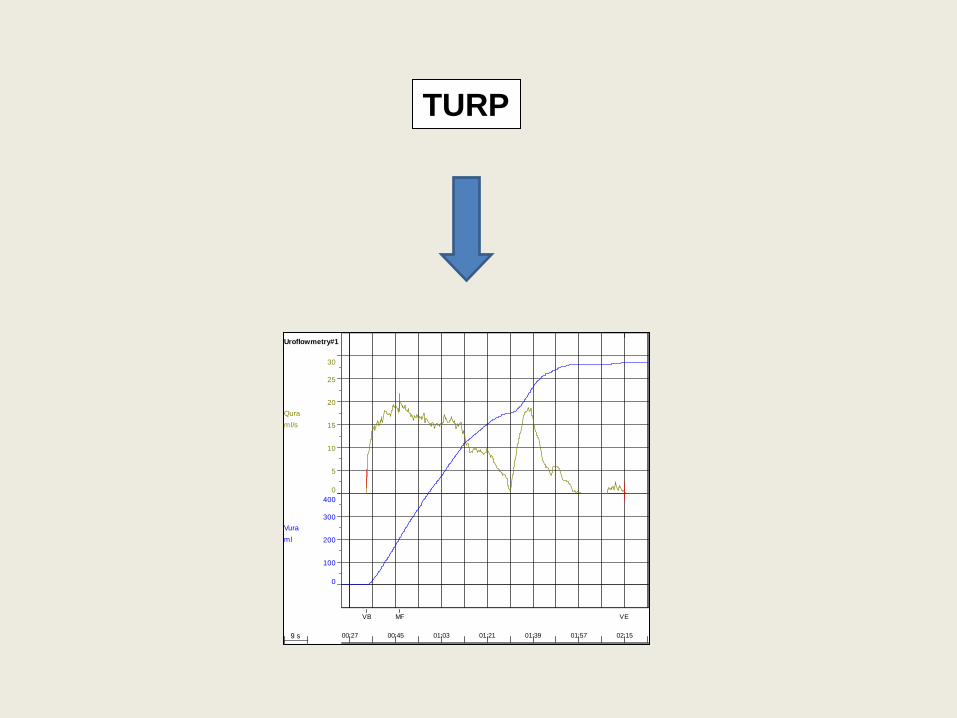
TURP
Qura
ml/s
0
5
10
15
20
25
30
Vura
ml
0
100
200
300
400
Uroflowmetry#1
9 s 00:27 00:45 01:03 01:21 01:39 01:57 02:15
VB MF VE
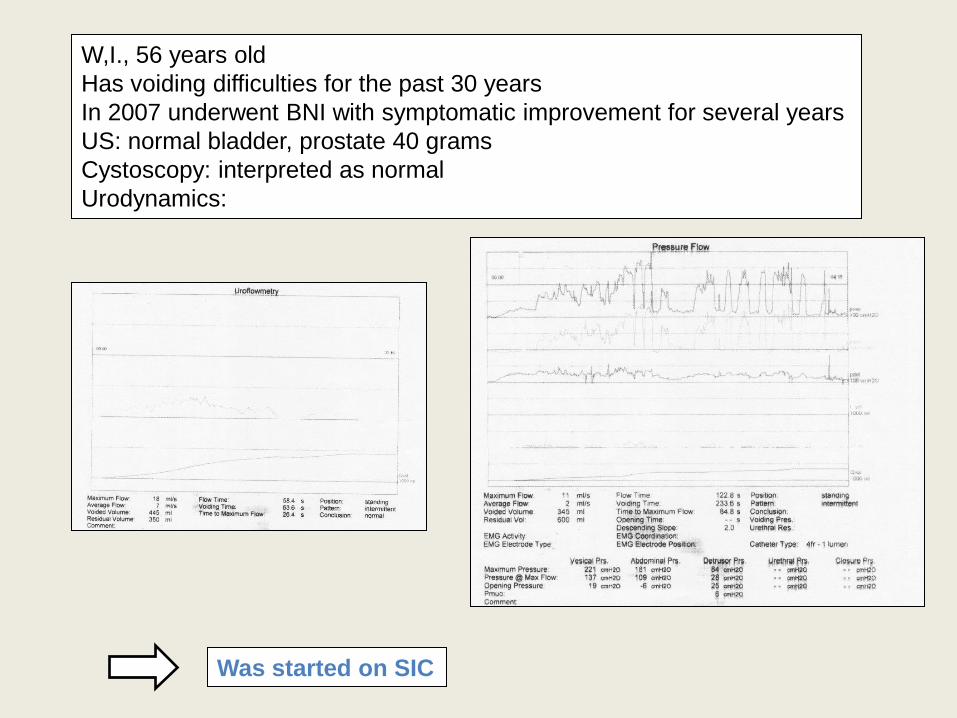
W,I., 56 years old
Has voiding difficulties for the past 30 years
In 2007 underwent BNI with symptomatic improvement for several years
US: normal bladder, prostate 40 grams
Cystoscopy: interpreted as normal
Urodynamics:
Was started on SIC
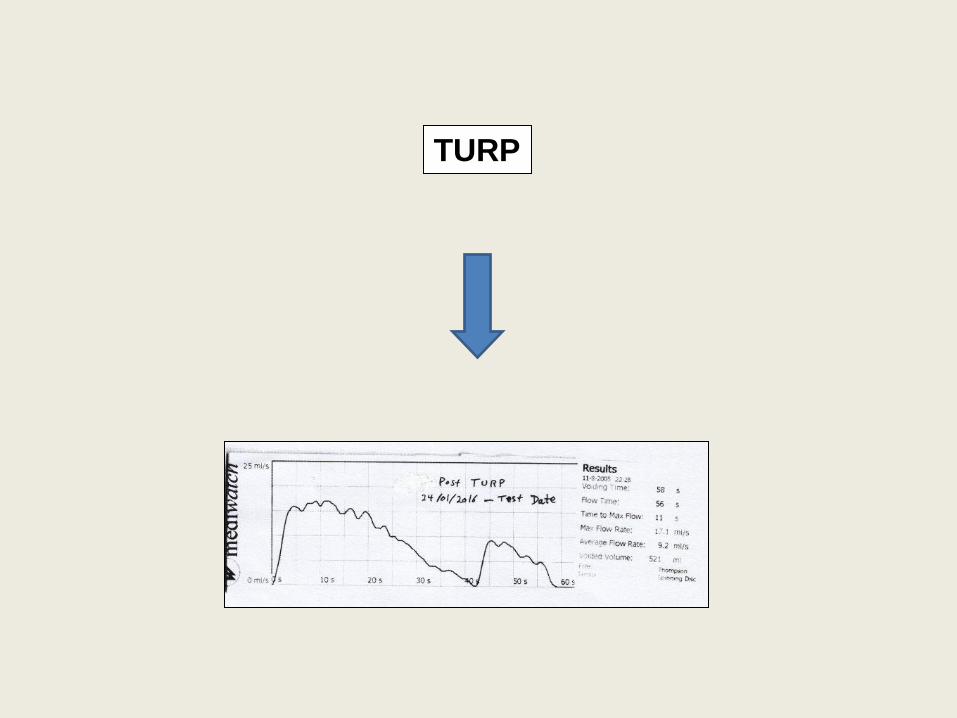
TURP
• Detrusor underactivity is defined by the International Continence Society
(ICS) as ‘‘a contraction of reduced strength and/or duration, resulting in
prolonged bladder emptying and/or failure to achieve complete bladder
emptying within a normal time span’’.
Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from
the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002;21:167–78.
• However, the ICS report falls short in specifying parameters for reduced
contraction strength, prolonged bladder emptying, or normal time span.
• Suggested working definition: “The underactive bladder is a symptom
complex, and is usually characterised by prolonged urination time with or
without a sensation of incomplete bladder emptying, usually with hesitancy,
reduced sensation on filling, and a slow stream”.
Chapple CR et al. The Underactive Bladder: A New Clinical Concept?. Eur Urol 68 (2015) 351-353.
Based on a consensus group meeting at the International Consultation on Incontinence–Research Society and ICS
annual meetings in September and October 2014.
IN SUMMARY:
• The urodynamic diagnosis of non-neurogenic detrusor
underactivity in men with LUTS needs to be based on strict criteria,
which are not defined yet.
• Permanent SIC should be applied in men with LUTS and urinary
retention with utmost prudence.
• In non-neurogenic men with urinary retention, the options of
TURP versus permanent SIC should be discussed with the patient.