the safety and efficacy of a new patient-controlled
TRANSCRIPT
Henry Ford Hospital Medical Journal Henry Ford Hospital Medical Journal
Volume 34 Number 2 Article 9
6-1986
The Safety and Efficacy of a New Patient-Controlled Analgesia The Safety and Efficacy of a New Patient-Controlled Analgesia
Device in Hospitalized Trauma and Surgery Patients Device in Hospitalized Trauma and Surgery Patients
Terry J. Baumann
Luz Maria Gutschi
Brack A. Bivins
Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal
Part of the Life Sciences Commons, Medical Specialties Commons, and the Public Health Commons
Recommended Citation Recommended Citation Baumann, Terry J.; Gutschi, Luz Maria; and Bivins, Brack A. (1986) "The Safety and Efficacy of a New Patient-Controlled Analgesia Device in Hospitalized Trauma and Surgery Patients," Henry Ford Hospital Medical Journal : Vol. 34 : No. 2 , 105-108. Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol34/iss2/9
This Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Henry Ford Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons.

Xhe Safety and Efficacy of a New Patient-Controlled Analgesia pevice in Hospitalized TVauma and Surgery Patients
Terry J. Baumann, PharmD,* Luz Maria Gutschi, PharmD,̂ and Brack A. Bivins, MD*
The objective ofthis investigation was to evaluate a new patient-controlled analgesia (PCA) device. Eighteen trauma and surgical patients were allowed to use a self-activated, intravenous infusion device for two to seven days for postoperative pain relief. Initial PCA dosage/interval settings were adjusted to provide a 0.5 to 1 mg dosage of morphine per injection with a six-minute lockout interval. Adjustments were made to these initial settings based on the individual patient's response. Pain arul sedation scores and respiratory rates were recorded. Subjective evaluations of PCA indicated that 17 of the 18 patients (94.4%) participating in the study "preferred this [PCA] method" or would "probably choose this [PCA] method" for pain relief in the future. Patients self-administered narcotic analgesic to a maximum level of pain relief with minimum sedation. No respiratory depression was noted with use of the PCA device. Investigators judged and patients attested to PCA being safe, effective, capable of accommodating wide fluctuations of analgesic needs, and suitable for widespread use. (Henry Ford Hosp Med J 1986;34:105-8)
I
The regimen for pain relief in postsurgical, terminally i l l , or trauma patients is traditionally determined by the attending
physician who prescribes a specific dose of a narcotic agent to be administered at specific time intervals. Such a regimen may not meet the patient's need for relief between these intervals; effective refief from pain and discomfort is not necessarily coincident with time constraints or dosages administered. A large dose of narcotic administered intramuscularly and intended to last from four to six hours may at first overtreat the patient and then result insome degree of sedation. Toward the end ofthe prescribed time interval, then, the dosage is insufficient to relieve the patient's pain and discomfort before the next dose is permitted. Consequently, pain is not always optimally managed. Both over-treatment and undertreatment can occur as a result of cyclical variation of pain, interpatient variability, and the nature of the illness, trauma, or surgical procedure involved.
Concem with suboptimal management of pain in hospitalized patients has led to the development of patient-controlled analgesia (PCA) delivery systems. This study was undertaken to clinically evaluate PCA pain management techniques in hospitalized trauma and surgery patients and to test the safety and efficacy of a new PCA device.
Materials and Methods Over a four-month period 18 patients who had sustained a
traumatic injury or who were hospitalized for surgical pro-'̂ edures (about 3% of the patient population) were entered into our investigation (Table I). Entry into the study was restricted to 'he following patients: (a) those between 21 and 68 years of age; (h) patients taking no psychotropic dmgs; (c) those with no history of psychiatric or neurological disorders; (d) patients with no '̂̂ hve, serious metabolic abnormalities or marked debilitation
of chronic disease; (e) those with no history of alcohol or substance abuse; and (f) patients with no history of morphine allergy. After informed consent was obtained, patients were instmcted in the use of the PCA device (Abbott Lifecare PCA Pump, Abbott Laboratories, Abbott Park, North Chicago, IL).
The PCA device used is a versatile infusion device with an adjustable lockout interval and automatic recording of dmg administration. All patients initially received either 0.5 or 1 mg of morphine sulfate per injection (morphine sulfate and syringes [1 mg/mL], Abbott Laboratories, Abbott Park, North Chicago, IL). An inactivation period of six minutes was imposed following each dose, thereby allowing that dose to exert its peak effect before another could be given. An optimal dose per injection (DPI) was defined as that which induced acceptable analgesia without sedation. If a patient did not obtain an analgesic effect following a single bolus dose, the DPI was increased by 50%. If the patient was found to be drowsy after a single dose, the DPI was decreased by 50%.
Sedation and respiratory rates were evaluated by nursing personnel each hour during the first 12 hours and then every two hours for the remainder of the study period. Pain was ranked both one hour after PCA startup and daily by the patient in response to the question, "Which of the following describes how you feel/have felt since yesterday?" Possible answers included 1) comfortable, 2) in mild discomfort, 3) in pain, 4) in bad pain, and 5) in very bad pain. Nurses evaluated sedation by using the
Submitted for publication: May 1, 1986. Accepted for publication: June 19. 1986. *Department of Pharmacy Services. Henry Ford Hospital. tDepartment of Pharmacy Services. St Boniface Hospital. Winnipeg, Manitoba. tDivision of Trauma Surgery. Nutritional Support Service, Henry Ford Hospital. Address correspondence to Dr Baumann. Department of Pharmacy Services, Henry Ford
Hospital, 2799 W Grand Blvd, Detroit, Ml 48202.
ii;, Ford Hosp Med J—Vol 34, No 2, 1986 PCA Device—Baumann et al 105
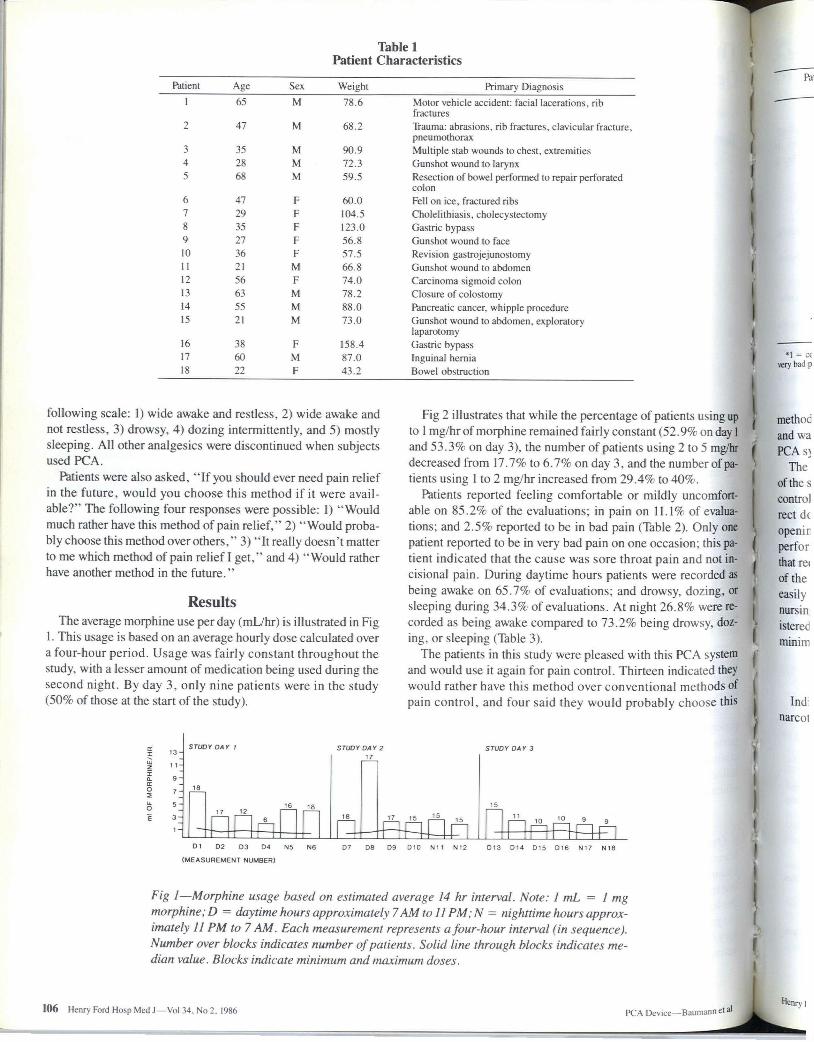
Table 1 Patient Characteristics
Patient Age Sex Weight Primary Diagnosis 1 65 M 78.6 Motor vehicle accident: facial lacerations, rib
fractures 2 47 M 68.2 Trauma: abrasions, rib fractures, clavicular fracture,
pneumothorax 3 35 M 90.9 Multiple stab wounds to chest, extremities 4 2S M 72.3 Gunshot wound to larynx 5 M 59.5 Resection of bowel performed to repair perforated
colon 6 47 F 60.0 Fell on ice, fractured ribs 7 24 F 104.5 Cholelithiasis, cholecystectomy
s 3--S F 123.0 Gastric bypass 9 27 I- 56.8 Gunshot wound to face 10 36 f 57.5 Revision gastrojejunostomy 11 21 M 66.8 Gunshot wound to abdomen 12 56 F 74.0 Carcinoma sigmoid colon 13 63 M 78.2 Closure of colostomy 14 55 M 88.0 Pancreatic cancer, Whipple procedure 15 21 M 73.0 Gunshot wound to abdomen, exploratory
laparotomy 16 3N I- 158.4 Gastric bypass !̂ 60 M 87.0 Inguinal hernia 18 22 F 43.2 Bowel obstruction
following scale: I) wide awake and restiess, 2) wide awake and not restiess, 3) drowsy, 4) dozing intermittentiy, and 5) mostly sleeping. All other analgesics were discontinued when subjects used PCA.
Patients were also asked, " I f you should ever need pain relief in the future, would you choose this method if it were available?" The following four responses were possible: 1) "Would much rather have this method of pain relief," 2) "Would probably choose this method over others," 3) "It really doesn't matter to me which method of pain relief I get," and 4) "Would rather have another method in the future."
Results The average morphine use perday (mL/hr) is illustrated in Fig
I . This usage is based on an average hourly dose calculated over a four-hour period. Usage was fairly constant throughout the study, with a lesser amount of medication being used during the second night. By day 3, only nine patients were in the study (50% of those at the start ofthe study).
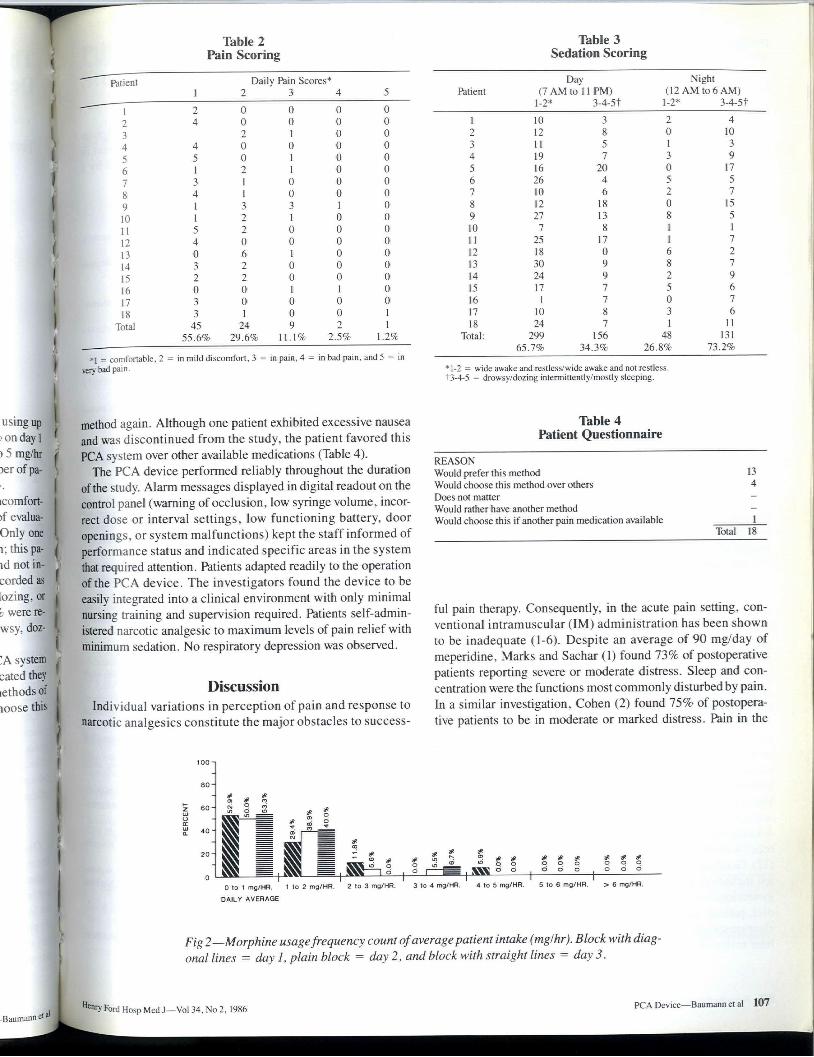
Fig 2 illustrates that while the percentage of patients using up to 1 mg/hrof morphine remained fairly constant (52.9% on day I and 53.3% on day 3), the number of patients using 2 to 5 mg/hr decreased from 17.7% to 6.7% on day 3, and the numberof patients using 1 to 2 mg/hr increased from 29.4% to 40%.
Patients reported feeling comfortable or mildly uncomfortable on 85.2% of the evaluations; in pain on 11.1% of evaluations; and 2.5% reported to be in bad pain (Table 2). Only one patient reported to be in very bad pain on one occasion; this patient indicated that the cause was sore throat pain and not incisional pain. During daytime hours patients were recorded as being awake on 65.7% of evaluations; and drowsy, dozing, or sleeping during 34.3% of evaluations. At night 26.8% were recorded as being awake compared to 73.2% being drowsy, dozing, or sleeping (Table 3).
The patients in this study were pleased with this PCA systera and would use it again for pain control. Thirteen indicated they would rather have this method over conventional methods of pain control, and four said they would probably choose this
I
7
5 -
STUDY DAY I
16 18
SrUDl ' DAY 2 17
STUDY DAY 3
El Dl D2 D3 04 N5 N6
(MEASUREMENT NUMBER)
07 D8 D9 DIO N i l N12 D13 D14 D15 D16 N17 N18
Fig 1—Morphine usage based on estimated average 14 hr interval. Note: 1 mL = 1 mg morphine; D = daytime hours approximately 7 AM to 11 PM; N = nighttime hours approximately II PM to 7 AM. Each measurement represents a four-hour interval (in sequence). Number over blocks indicates number of patients. Solid Une through blocks indicates median value. Blocks indicate minimum and maximum doses.
106 Henry Ford Hosp Med J—Vol 34. No 2. 1986 PCA Device—Baumann etal
Patient
Table 2 Pain Scoring
Daily Pain Scores* 1 2 3 4 5
1 2 0 0 0 0 ; 4 0 0 0 0 3 2 1 0 0 4 4 0 (1 0 0
.•̂ 5 0 1 0 0
6 1 2 1 0 0
7 3 1 (1 0 0 S 4 1 0 0 0 9 1 3 3 1 0 10 1 2 1 0 0 11 5 2 0 0 0 12 4 0 0 0 0 13 0 6 1 0 0 14 3 2 0 0 0 \S 2 2 0 0 0 16 0 0 1 1 0 17 3 0 0 0 0 18 3 I 0 0 1
Total 45 24 9 2 1 55.6% 29.6% 11.1% 2.5% 1.2%
*1 = comfortable, 2 ^ in mild discomfort, 3 ^ in pain, 4 ^ in bad pain, and 5 = in very bad pain.
Table 3 Sedation Scoring
Day Night Patient (7 AM to 11 PM) (12 AM to 6 AM)
1-2* 3-4-5t 1-2* 3-4-51
1 10 3 2 4 2 12 8 0 10 3 11 5 1 3 4 19 7 3 9 5 16 20 0 17 6 26 4 5 5 7 10 6 2 7
12 IS 0 15 9 27 13 s 5 10 7 S 1 1 1 1 2.̂ 17 1 7 12 IS 0 6 2 13 30 9 s 7 14 24 9 2 9 15 17 7 ."̂ 6 16 1 7 0 7 17 10 8 3 6 18 24 7 I 11
Total: 299 156 48 131 65.7% 34.3% 26.8% 73.2%
*l-2 = wide awake and restless/wide awake and not restless. t3-4-5 = drowsy/dozing intermittently/mosdy sleeping.
method again. Although one patient exhibited excessive nausea and was discontinued from the study, the patient favored this PCA system over other available medications (Table 4).
The PCA device performed reliably throughout the duration ofthe study. Alarm messages displayed in digital readout on the control panel (waming of occlusion, low syringe volume, incorrect dose or interval settings, low functioning battery, door openings, or system malfunctions) kept the staff informed of performance status and indicated specific areas in the system that required attention. Patients adapted readily to the operation ofthe PCA device. The investigators found the device to be easily integrated into a clinical environment with only minimal nursing training and supervision required. Patients self-administered narcotic analgesic to maximum levels of pain relief with minimum sedation. No respiratory depression was observed.
Discussion Individual variations in perception of pain and response to
narcotic analgesics constitute the major obstacles to success-
Table 4 Patient Questionnaire
REASON Would prefer this method Would choose this method over others Does not matter Would rather have another method Would choose this if another pain medication available
13 4
i Total 18
ful pain therapy. Consequently, in the acute pain setting, conventional intramuscular (IM) administration has been shown to be inadequate (1-6). Despite an average of 90 mg/day of meperidine, Marks and Sachar (1) found 73% of postoperative patients reporting severe or moderate distress. Sleep and concentration were the functions most commonly disturbed by pain. In a similar investigation, Cohen (2) found 75% of postoperative patients to be in moderate or marked distress. Pain in the
0 to 1 mg/HR.
DAJLY AVERAGE
= o 6 ^ " o o q q q q q o
= ^SSrn g I § r - ^ I MS ° ° ^ ° o o ^ o o ° 1 to 2 mg/HR. 2 to 3 mg/HR. 3 to 4 mg/HR. 4 to 5 mg/HR. 5 to 6 mg/HR. > 6 mg/HB.
Fig 2 —Morphine usa ge frequency count of average patient intake (mg/hr). B lock with diagonal lines = day 1, plain block = day2. and block with straight lines = day3.
•̂ n̂ry Ford Hosp Med J—Vol 34, No 2,1986 PCA Device—Baumann et al 107
postoperative setting is common, and its incidence is high despite the availability of potent narcotic analgesics (3- 5,7).
Many factors can contribute to the inadequacy of postoperative analgesia. Conventional IM dosing is largely unsupervised by physicians who merely prescribe narcotics on an "as needed" basis. The initiative for requesting analgesia then falls on the patient or nurse. The results are often long delays between need for analgesia and narcotic administration (6). The time required from patient recognition of analgesic need and relief of pain from an intramuscular narcotic has been estimated to be over 30 minutes (7). IM administration can also result in unpredictable and variable absorption from patient to patient. Austin et al (8) showed a fivefold interpatient range and a twofold intra-patient range in semm concentrations of meperidine given every four hours. Morphine administration has often been associated with sedation. Its incidence has been reported to be as high as 46% (9) and is considered to be dose-dependent (10). Moreover, sedation is exacerbated by the common practice of concomitant administration of antiemetics and anxiolytics (11,12). Semm levels fall quickly due to the rapid metabolism of morphine (13), and pain subsequentiy reemerges. In effect, a repetitive cycle of both pain and sedation is observed as peak and trough serum drug concentrations are achieved (8). Sedation was minimal with PCA in this series of patients.
PCA is a method by which the problems inherent with conventional IM dosing may be overcome. PCA employs an infusion pump integrated with a timing device which allows patients to self-administer small doses of narcotics intravenously. By activating a switch similar to a nursing call button, patients consistently titrate their analgesia so as to maintain a balance between adequate analgesia and undesirable sedation (6). Patients thus self-administer their medication effectively, with serum morphine concentrations remaining within a narrow range (14). The efficacy and safety of PCA has been demonstrated by Keeri-Szanto and Heaman (15), Bennett et al (16), Scott (17), and Nayman (18). Fear of addiction and tolerance has not been realized as dosing rates uniformly decline in most PCA patients (19). Comparison of PCA to conventional IM administration in 24 gastric bypass patients demonstrated use of larger amounts of analgesic by the IM patients. Moreover, 92% of the PCA group felt they received adequate analgesia while only 58% of the IM group responded in this manner (20). An investigation involving upper abdominal surgery demonstrated that PCA patients' pulmonary function tests returned to baseline faster than the IM group (21). Respiratory rates determined every two hours showed no respiratory depression in 50 laparotomy patients using PCA; of 1,333 measurements only 1.2% were less than 16 breaths/min (22). In this series, 94.4% of the patients were highly satisfied with the PCA device, and respiratory depression was not seen.
Using pain and sedation scores, investigators have found pain relief with PCA to be preferred over conventional IM dosing (22). Good control of pain was seen in various populations studied including gastric bypass surgery (20), laparotomy (22), gynecologic surgery (17), and terminally ill patients (23). Moreover, patients prefer to tolerate some pain so as to maintain a clear sensorium (24). In summary, the results of this study and a brief review ofthe literature support the safety and effectiveness
of PCA as a means of providing pain relief to trauma and surgical patients. Future studies need to address the cost-effectiveness of this new dosing technique.
Acknowledgements The authors would like to acknowledge the nursing and phar
macy staff of Henry Ford Hospital for all of their support in helping to complete this study. This work was supported by Grant from Abbott Laboratories.
References 1. Marks RM. Sachar EJ. Undertreatment of medical inpatients with narcotic
analgesics. Ann Intern Med 1973;78:173-81. 2. Cohen FL. Postsurgical pain relief: Patients' status and nurses' medication
choices. Pain 1982;9:265-74. 3. Angell M. The quality of mercy. N Engl J Med 1982;306:98-9. 4. Wadell D, Brody RV. Inadequate treatment of pain in hospitalized patients.
NEnglJMed 1982:307:55. 5. Utting JE, Smith JM. Postoperative analgesia. Anaesthesia
1979;34:320-32. 6. Graves DA, Foster TS, Batenhorst RL, Bennett RL. Baumann TJ. Patient-
controlled analgesia. Ann Intern Med 1983;99:360-6. 7. Vache E. Inadequate treatment of pain in hospitalized patients. N Engl J
Med I982;307:55. 8. Austin KL, Stapleton JV. Mather LE. Relationship between blood
meperidine concentrations and analgesic response: A preliminary report. Anesthesiology 1980;53:460-6.
9. Kaiko RR Wallenstein SL, Rogers AG, Grabinsky PY, Haude KW. Analgesic and mood effects of heroin and morphine in cancer patients with postoperative pain. NEnglJMed 1981;304:1501-5.
10. Forest WH, Brown CR, Defalque R, et al. Dextroamphetamine with morphine for the treatment of postoperative pain. N Engl J Med 1977;296:712-5.
11. Hupert C, Yacoub M, Turgeon LR. Effect of hydroxyzine on morphine analgesia for the treatment of postoperative pain. Anesth Analg 1980;59:690-6.
12. McGee JL, Alexander MR. Phenothiazine analgesia—fact or fantasy? Am J Hosp Pharm 1979;36:633-40.
13. Berkowitz BA. The relationship of pharmacokinetics to pharmacological activity: Morphine, methadone and naloxone. Clin Pharmacokinet 1976;1:219-30.
14. Dahlstrom B, Tamsen A, Paalzow L, Hartvig P. Patient-controlled analgesic therapy. Part IV: Pharmacokinetics and analgesic plasma concentration of morphine. Clin Pharmacokinet 1982;7:266-79.
15. Keeri-Szanto M, Heaman S. Postoperative demand analgesia. Surg Gynecol Obstet 1972;134:647-51.
16. Bennett RL, Batenhorst RL. Bivins BA. et al. Patient-controlled analgesia: A new concept of postoperative pain relief. Ann Surg 1982;195:700-5.
17. Scott JS. Obstetric analgesia: A consideration of labor pain and a patient-controlled technique for its relief with meperidine. Am J Obstet Gynecol 1970;106:959-78.
18. NaymanJ. Measurement and control of postoperative pain. Ann Roy Coll Surg Engl 1979;61:419-26.
19. Medical news: Results are better when patients control their own analgesia. JAMA 1982;247:945-7.
20. Bennett RL. Batenhorst RL, Graves DA, et al. Variations in postoperative analgesic requirements in morbidly obese following gastric bypass surgery. Pharmacotherapy 1982;2:50-3.
21. Bennett RL, Batenhorst RL, Foster TS, Griffen WO, Wright BD. Postoperative pulmonary function with patient-controlled analgesia. Anaesth Analg I982;6I:17I.
22. Bennett RL, Batenhorst RL, Graves DA, et al. Morphine titration in postoperative laparotomy patients using patient-controlled analgesia. Curr Ther Res 1982;32:45-52.
23. Keeri-Szanto M. Demand analgesia for the relief of pain problems in terminal illness. Anesth Rev 1976;2:19-21.
24. Keeri-Szanto M. Drugs or drums: What relieves postoperative pain? Pai" 1979;6:217-30.
.1
1
u;: travenc be con pears t' well-ci tients 1 demor of 721
The inject have I consi Anim the s)
Ex clinic the p chan the s num atter evali anin cove
1 seie left exp cul
108 Henry Ford Hosp Med J—Vol 34, No 2, 1986 PCA Device—Baumann et a