the shoulder unit 16. upper extremity injuries upper extremities are vulnerable to a variety of...
TRANSCRIPT

The ShoulderUnit 16

Upper Extremity Injuries
Upper extremities are vulnerable to a variety of injuries depending on the sport, including:– Sprains– Strains– Dislocations– Fractures

Upper Extremity Injuries
Upper extremities are vulnerable to a variety of injuries depending on the sport, including:– Separations to the thoracic cage, shoulder,
arm, and hand– Repetitive motion injuries such as arthritis,
bursitis, tendonitis

Shoulder Complex Physiology
Bones Muscles Tendons Ligaments Articulations

Bones
Humerus Scapula Clavicle
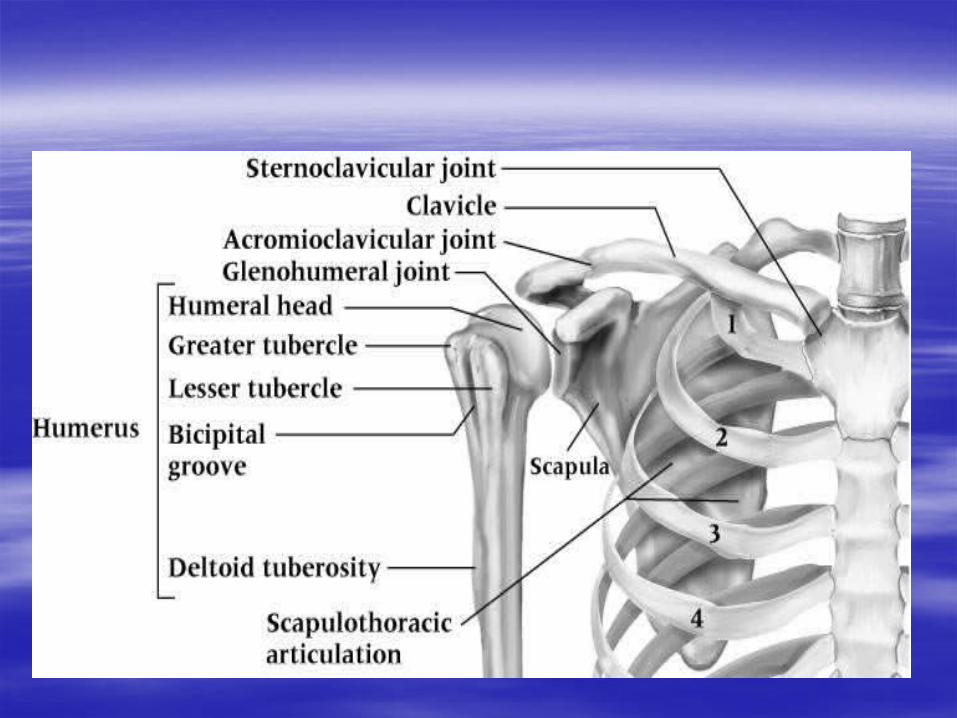



THE JOINTS
Sternoclavicular joint (SC joint)– Sternoclavicular ligament
Coracoclavicular joint– Coracoclavicular ligament
Acromioclavicular joint (AC joint)– Acromioclavicular ligament
Coracoacromial joint– Coracoacromial ligament
Glenohumeral joint– Glenohumeral ligaments
Scapulothoracic articulation




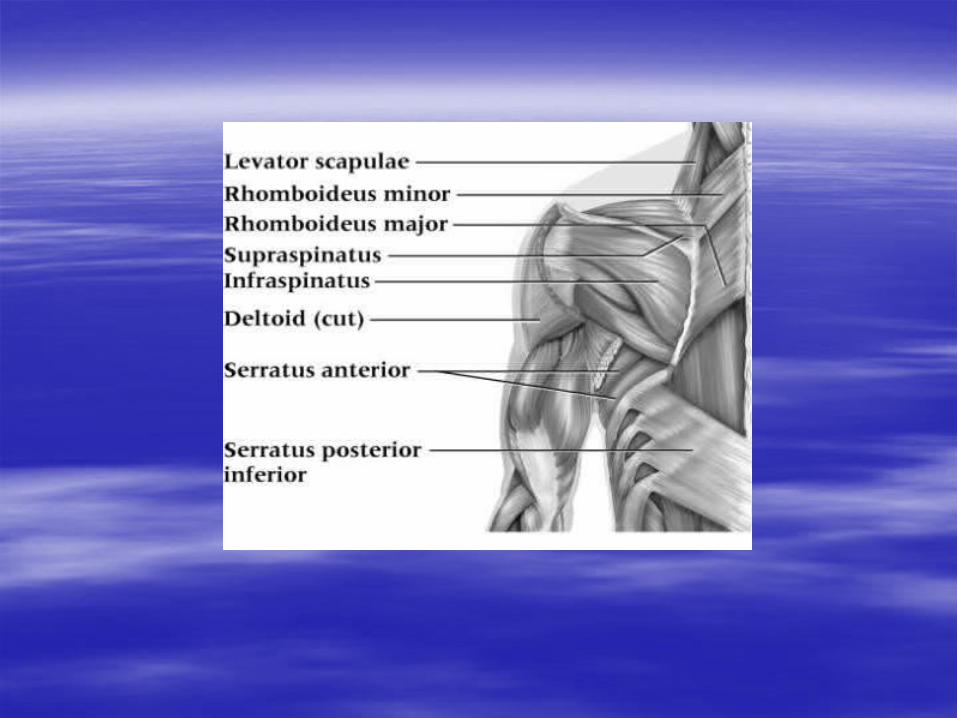
Muscles in motion
FLEXION
Anterior deltoid– Primary mover
Biceps brachii– Secondary mover

EXTENSION
Posterior deltoid– Prim. Mover
Triceps brachii– Sec. Mover

ABDUCTION
Supraspinatus – 1st 5-10 degrees
Middle deltoid– Last 90 degrees
Trapezius– Assists in movement above 90 degrees

ADDUCTION Latissimus dorsi Pectoralis major

HORIZONTAL FLEXION Pectoralis major Anterior deltoid

HORIZONTAL EXTENSION Posterior deltoid Infraspinatus Teres minor/major Rhomboids Trapezius
– Stabilizer

CIRCUMDUCTION Basically all muscles of the shoulder

INTERNAL ROTATION Subscapularis Pectoralis major
– Little help
EXTERNAL ROTATION Infraspinatus Teres minor/major

Scapular Elevation Scapular Depression Scapular protraction Scapular retraction ****find muscles that perform these motions

Assessing Shoulder Injuries
H O P S

History– What is the cause of pain?– Mechanism of injury? – Previous history?– Location, duration and intensity of pain?– Creptitus, numbness, distortion in temperature– Weakness or fatigue?– What provides relief?
Observation– Elevation or depression of shoulder tips– Position and shape of clavicle– Acromion process– Biceps and deltoid symmetry– Postural assessment (kyphosis, lordosis,
shoulders)– Position of head and arms– Scapular elevation and symmetry– Scapular protraction or winging– Muscle symmetry – Scapulohumeral rhythm

Palpation– Bony structure palpation should occur bilaterally
and simultaneously if possible– Palpate soft tissue structures for point
tenderness, swelling, spasms, lumps, guarding or trigger points
– Be sure to palpate anteriorly and posteriorly

Special Tests– ROM test for external rotation of the shoulder– ROM test for internal rotation of the shoulder– Specific ROM tests for the shoulder
including abduction, adduction, flexion, extension,
horizontal adduction, horizontal abduction

Manual muscle tests for the shoulder – External rotation strength tests– Internal rotation strength test for the shoulder– Extension strength test for the shoulder – Flexion strength test for the shoulder– Abduction and adduction strength tests for the shoulder– Empty can test

• Apprehension test (Crank test)
Apprehension test used for anterior glenohumeral instability – This motion
should not be forced

• Test for Shoulder Impingement– Neer’s test and Hawkins-Kennedy test for
impingement used to assess impingement of soft tissue structures
– Positive test is indicated by pain and grimace

Test for Supraspinatus Weakness
Empty Can Test– 90 degrees of
shoulder flexion, internal rotation and 30 degrees of horizontal abduction
– Downward pressure is applied
– Weakness and pain are assessed bilaterally
Types of Shoulder Injuries
Fractures Clavicle, humerus, scapula Cause: fall on outstretched arm, direct
blow S/S: pain, deformity, decreased ROM,
swelling Perform percussion test, compression
test
Treatment– Sling/splint– PRICE– Physcian/EMS– Follow orders
Prevention: – Instruct how to fall– Proper equipment



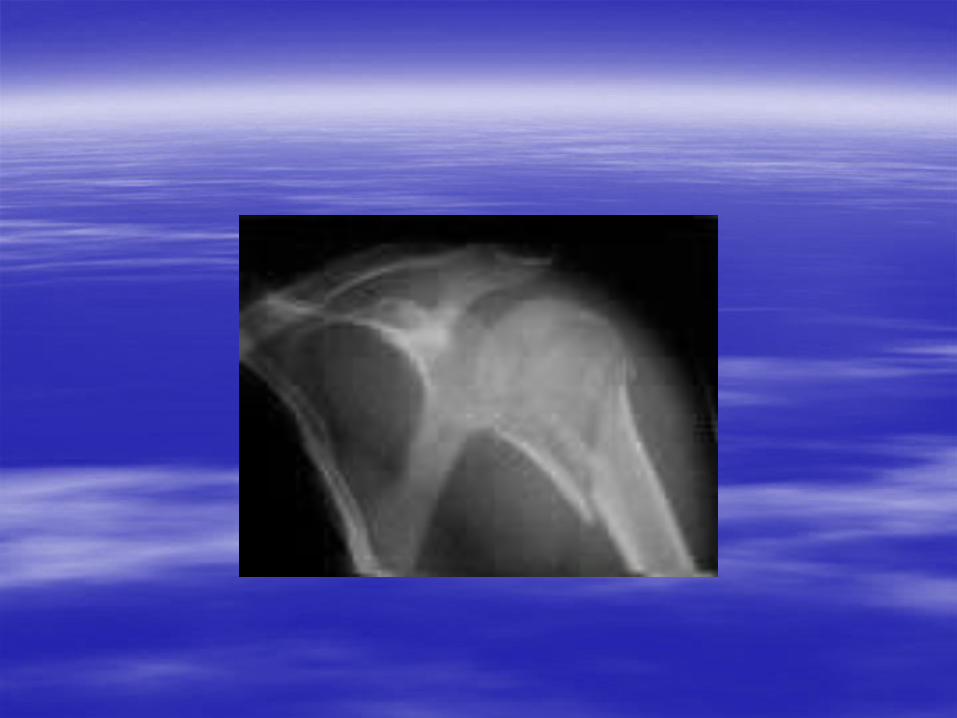
Hockey Clavicle Fracture


Dislocations and subluxations AC, SC, GH jts Cause: head of humerus forced/displaced
from glenoid S/S: pop, dead arm, pain, deformity,
swelling, loss of ROM/strength

Treatment– DO NOT relocated– PRICE– Check circulation/sensation– Physician / x-rays– Follow orders
Prevention– Strengthen jt– Proper equipment– Falling
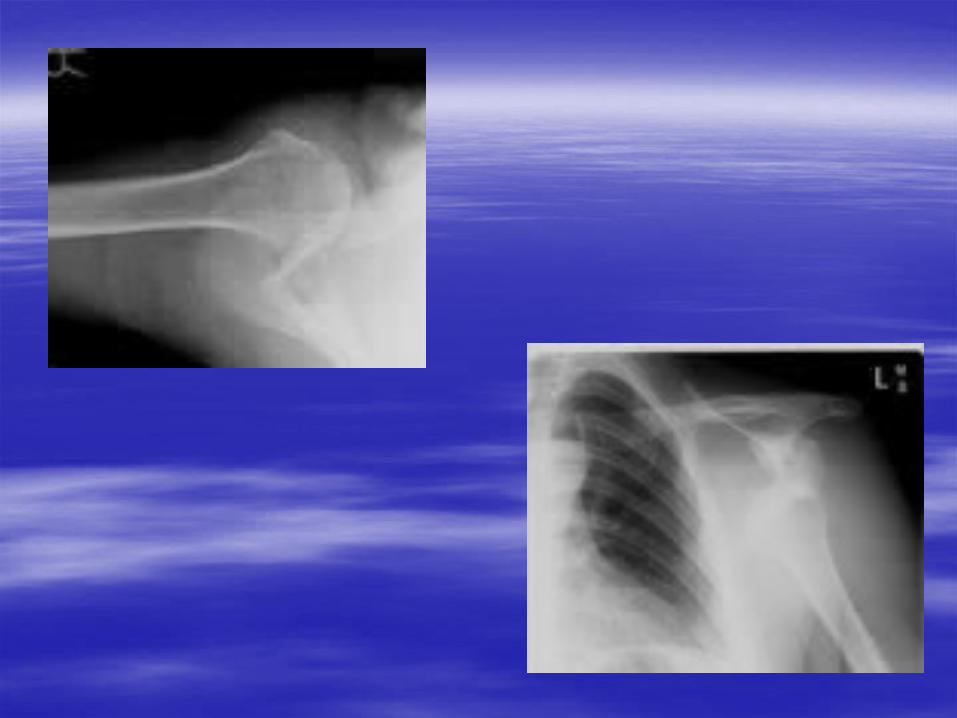

Anterior Posterior

Posterior

Shoulder dislocation-rugby Dwayne Wade http://www.youtube.com/watch?
v=09ZZbJzeKUA

Contusions– Cause: direct blow/bony area or muscles– S/S: pain, decreased ROM, r/o other
injuries– Treatment: ice, padding, rehab, flexibility– Prevention: proper equipment, mechanics
Myositis ossificans

Sprains– Cause: over stretch/tear ligament, capsule
What motions/events would cause this?
– S/S: pt tender, weak, swelling, instability, possible deformity, decreased ROM
– Treatment PRICE Physician, follow orders Rehab
– Prevention Proper equipment/technique Strengthening/stretching Inspect playing areas Taping/bracing

Sternoclavicular Sprain– Cause of Injury
Indirect force, blunt trauma (may cause displacement)
– Signs of Injury Grade 1 - pain and slight disability Grade 2 - pain, subluxation w/ deformity,
swelling and point tenderness and decreased ROM
Grade 3 - gross deformity (dislocation), pain, swelling, decreased ROM
– Possibly life-threatening if dislocates posteriorly
– Care PRICE, immobilization Immobilize for 3-5 weeks followed by graded
reconditioning

Acromioclavicular Sprain– Cause of Injury
Result of direct blow (from any direction), upward force from humerus, fall on outstretched arm
– Signs of Injury Grade 1 - point tenderness and pain w/ movement;
no disruption of AC joint Grade 2 - tear or rupture of AC ligament, partial
displacement of lateral end of clavicle; pain, point tenderness and decreased ROM (abduction/adduction)
Grade 3 - Rupture of AC and CC ligaments with dislocation of clavicle; gross deformity, pain, loss of function and instability

– Care Ice, stabilization, referral to physician Grades 1-3 (non-operative) will require 3-4
days (grade 1) and 2 weeks of immobilization ( grade 3) respectively
Aggressive rehab is required w/ all grades– Joint mobilizations, flexibility exercises, &
strengthening should occur immediately– Progress as athlete is able to tolerate w/out pain and
swelling– Padding and protection may be required until pain-
free ROM returns

Specific tests
– Sulcus test, apprehension test for sprain of the anterior capsule
– Acromioclavicular (AC) sprain test– Sternoclavicular (SC) sprain test

Types of Shoulder Injuries
Strains – Cause: overstretching of muscles– S/S: similar to sprains– Treatment: PRICE, physician if necessary,
follow orders, rehab– Prevention
Stretching, strengthening
– Drop arm test-specific test

What do you see?
L clavicle elevation, bruising, left shoulder higher
What do you think the injury is? Grade 2 AC sprain, left. Bull rider

Impingement – Cause: pinching of soft tissue w/overhead
activity; overuse– S/S: pain, weakness, pt tenderness
Hawkins-Kennedy test, winged scapula test– Treatment
PRICE, decrease inflam., physician Strengthen RC, scapular stabilizers
– Prevention RC strengthening, proper mechanics


– Rotator cuff tear Involves supraspinatus or rupture of other
rotator cuff tendons Primary mechanism - acute trauma (high
velocity rotation) Occurs near insertion on greater tuberosity Full thickness tears usually occur in those
athletes w/ a long history of impingement or instability (generally does not occur in athlete under age 40)
– Signs of Injury Present with pain with muscle contraction Tenderness on palpation and loss of strength
due to pain Loss of function, swelling With complete tear, impingement and empty
can test are positive

– Care RICE for modulation of pain Progressive strengthening of rotator cuff Reduce frequency and level of activity initially
with a gradual and progressive increase in intensity

Shoulder Bursitis– Etiology
Chronic inflammatory condition due to trauma or overuse - subacromial bursa
May develop from direct impact or fall on tip of shoulder
– Signs of Injury Pain w/ motion and tenderness during palpation
in subacromial space; positive impingement tests
– Management Cold packs and NSAID’s to reduce
inflammation Remove mechanisms precipitating condition Maintain full ROM to reduce chances of
contractures and adhesions from forming

Bicipital Tenosynovitis– Cause of Injury
Repetitive overhead athlete - ballistic activity that involves repeated stretching of biceps tendon causing irritation to the tendon and sheath
– Signs of Injury Tenderness over bicipital groove, swelling,
crepitus due to inflammation Pain when performing overhead activities
– Care Rest and ice to treat inflammation NSAID’s Gradual program of strengthening and
stretching

Types of Shoulder Injuries
Tendonitis– Cause: overuse to tendons
Speed’s test
– Treatment: PRICE, anti-inflammatory, rehab, etc
– Prevention: Ice post activity, conditioning, mechanics,

Synovitis and bursitis– Cause: inflammation of synovial lining/bursa
Overuse, direct trauma
– S/S: pain, crepitus, swelling, decreased mobility
– Treatment: PRICE or heat, stretching pain free ROM, mechanics, etc
– Prevention: mechanics