theacquisition of tacts, mands, intraverbals individuals ... · receiving dilantin and...
TRANSCRIPT

The Analysis of Verbal Behavior 1990,8, 83-99
The Acquisition of Tacts, Mands, and Intraverbals byIndividuals With Traumatic Brain Injury
Mark L. SundbergSundberg and Associates, Concord, CA
AND
Belinda San Juan, Marijorie Dawdy, and Marilla ArguellesConsensus Brain Injury Rehabilitation Center, Berkeley, CA
Two individuals who sustained traumatic brain injuries from motorcycle accidents weretaught several verbal responses by using tact, mand, and intraverbal training procedures. Therate of acquisition for each operant and the transfer to untrained verbal operants involving thesame response topography were measured. The results showed that tacts and intraverbalswere acquired quickest, and training on the tact produced the greatest amount of transfer tothe untrained verbal operants. Intraverbal training also resulted in transfer for both subjects,but to varying degrees. Direct mand training proved to be the least efficient way to generate amand repertoire, and when acquired showed least amount of transfer to the untrained oper-ants. These results seem to be in contrast with the findings of similar research with develop-mentally disabled individuals, and may have implications for methods of language instruc-tion for the brain injured population.
Individuals who sustain a traumaticinjury to the brain frequently experiencesevere and long-term physical and verbaldeficits. Rehabilitation after strokes, comas,vehicle accidents, and the like, often takesyears and may be only marginally success-ful. Verbal deficits, such as aphasia, tend tobe especially difficult to remediate. Hagen(1984) noted that aphasia produced by atraumatic brain injury "presents thespeech-language pathologist with a uniqueand complex diagnostic, prognostic, andtreatment challenge" (p. 245).Furthermore, professional opinion on
the most effective assessment and treat-ment strategies for those suffering fromaphasia, as well as other verbal disordersresulting from head injury, varies consider-ably (see Chapey, 1986; Darley, 1972;Doyle, Goldstein, & Bourgeois, 1987;Holland, 1984; Mowrer, 1988; Sidman,1971). There is an extensive body of experi-
The authors would like to express their apprecia-tion to Genae Hall, Joe Lancaster, Kathy Madigan,Jack Michael, and Cindy Sundberg for their com-ments on an earlier version of the manuscript. Reprintrequests should be addressed to Mark L. Sundberg,1236 Stafford Ave., Concord, CA 94521.
mental research on the topic (e.g., Chapey,1986), but most of it is derived from tradi-tional psycholinguistic theories whichemphasize cognitive or neurological causesof language (Muma, Hamre, & McNeil,1986). As a result, the focus of the clinicalassessment and intervention is often on theassumed underlying causes of the deficits.For example, in his review of the literatureon post-closed-head-injury (CHI), Hagen(1984) states that
this literature indicates that the CHI patientincurs impairments in concentration, attention,memory, nonverbal problem solving,part/whole analysis and synthesis, conceptualorganization, abstract thought, and speed ofprocessing...it would seem reasonable to assumethat post-CHI-language dysfunction is heavilyinfluenced, and in some instances created, bycognitive dysfunction. (p. 249)
The research supporting this cognitiveposition is complicated by the fact that theindependent and dependent variables inexperimentation are often not clearly iden-tified, and methodological problems resultwhich make replication nearly impossible.Sidman (1971) pointed out that "anyonewho has attempted seriously to survey the
83

84 MARK L. SUNDBERG et al.
literature on aphasia is familiar with theinevitable frustration" (p. 413). Salvatoreand Thompson (1986) expressed a similarconcern with the existing literature onglobal aphasia stating that "the specifictreatment procedures employed in theseinvestigations are lacking in operationalspecificity, making it impossible to deter-mine what variables affected patientchange and even more important for theclinician, the procedures cannot be repli-cated" (p. 410).A new direction for the assessment and
treatment of the language problems facedby the brain injured population may bederived from Skinner's (1957) analysis ofverbal behavior and aphasia. Skinnerwrites:
The pathological condition of verbal behaviorcalled aphasia often emphasizes functional dif-ferences which are hard to understand from thetraditional account. The aphasic may not be ableto name an object, though he will emit the nameimmediately in manding it; or he may be able toname the object although he cannot repeat thename after someone else or read it from a text ashe once was able to do. But it is only traditionaltheory which makes this surprising. The aphasichas lost some of the functional relationshipswhich control his verbal behavior. A response ofa given form may no longer be under the con-trol of one functional relation, although it is stillunder the control of another. (p. 190)
While the effects of aphasia may not besurprising to the behaviorist familiar withSkinner's (1957) Verbal Behavior, theresearch on the behavioral treatment ofaphasia remains sparse. One of the fewattempts to apply behavioral methods tostudy this problem can be found in a seriesof studies conducted by Sidman and hiscolleagues (Kirshner & Sidman, 1972;Leicester, Sidman, Stoddard, & Mohr, 1971;Mohr, Sidman, Stoddard, Leicester, &Rosenberger, 1973; Sidman, Stoddard,Mohr, & Leicester, 1971). Like Skinner,Sidman proposed that a brain injury mayaffect specific classes of stimulus-responserelations, but not others. For example, witha stroke patient Sidman et al., (1971) testedfour different types of stimulus-responserelations (simultaneous matching-to-sam-ple, delayed matching, oral naming, andwritten naming), across three differentmodalities (vision, audition, and touch).
The results of this study demonstrated aclear separation in the strength of the oper-ants tested. In addition, they showed "theexistence of orderly but different recoverycourses for the various stimulus-responserelations" (p. 135). Some relations, such asthe echoic and transcriptive repertoires,were clearly stronger than the others. Theauthors note that the
patient was able to repeat words when he couldnot say them in response to appropriate visualand tactile stimuli. He was able to match andwrite visual and tactile word samples that hecould not name. His naming deficits, thereforewere not simply an amalgram of receptive andexpressive elements; they were a distinctly sepa-rate category. (pp. 136-137)
The authors go on to suggest that thesefindings could have implications for thediagnosis and treatment of individuals suf-fering from aphasia. For example, if a spe-cific repertoire can be identified as beingweak, then an intervention can be designedto directly strengthen that repertoire.The current research is an extension of
Sidman's efforts to identify the effects ofbrain injury on specific verbal relations. Inaddition, the research incorporates thefindings from the growing body of litera-ture on the application of Skinner's (1957)analysis of verbal behavior (e.g., Braam &Poling, 1983; Carroll & Hesse, 1987; Hall &Sundberg, 1987; Lamarre & Holland, 1985;Lee & Pegler, 1982; Oah & Dickinson, 1989;Sigafoos, Reichle, Doss, Hall, & Pettitt,1990; Watkins, Pack-Teixteira, & Howard,1989).Both of the subjects in the present study
could easily emit echoic and textualresponses, but they had great difficultyemitting correct tact, mand, and intraver-bal responses. For example, one subjectcould echo the word binoculars, point tothem when asked to, pantomime how touse them, and read the written word. Buthe could not say binoculars when asked toname them (tact), or ask for them whenneeded (mand), or correctly talk aboutthem in conversation (intraverbal).
Most of the previous research on proce-dures for teaching weak or missing verbaloperants has been done with developmen-tally disabled individuals or young chil-

TRAUMATIC BRAIN INJURY AND VERBAL BEHAVIOR 85
dren (e.g., Braam & Poling, 1983; Carroll &Hesse, 1987; Hall & Sundberg, 1987). Thecurrent study attempts to replicate some ofthese procedures, while examining theissue of separate verbal functions as sug-gested by Skinner (1957). In addition, thestudy attempts to determine the effects ofteaching one verbal operant on the devel-opment of others involving the sameresponse topography. Specifically, theresearch addresses the following questions.(1) Which verbal operant will be acquiredfirst? (2) Will a response established undermand conditions occur under tact andintraverbal conditions without direct train-ing? (3) Will a response established undertact conditions occur under mand orintraverbal conditions without direct train-ing? And finally (4), will a response estab-lished under intraverbal conditions occurunder mand or tact conditions withoutdirect training?
METHOD
Subjects and Setting
Two males who sustained traumaticbrain injuries from motorcycle accidentsserved as subjects. These individuals werechosen as subjects because of their severeverbal deficits. Subject 1 was 40 years oldand was involved in an accident 19 yearsprior to the start of the study. As a result ofthe accident he sustained a severe headinjury and was briefly comatose. He wastreated with decompression of a predomi-nantly left sided subdural hematoma, anda small portion of his left temporal brainwas resected. He also had a treacheostomy.Currently, he has right spastic hemiparesis,and grand mal seizures for which he isreceiving dilantin and phenobarbital. Averbal assessment (Sundberg, 1983) con-ducted at the beginning of the studyshowed that the subject had strong recep-tive, echoic and textual repertoires, andweak mand, tact, and intraverbal reper-toires.
Subject 2 was 33 years old and wasinvolved in an accident 10 years prior tothe start of the study. As a result of theaccident he sustained a severe closed head
injury with brain contusions and cervicalspine fractures. He was comatose for aboutone month, and received dilantin forseizures for about three years after the acci-dent. Currently he has a right hemiparesisof the arm and leg. A verbal assessment(Sundberg, 1983) conducted at the begin-ning of the study showed the subject hadstrong receptive, echoic, and textual reper-toires, and weak to moderate mand, tact,and intraverbal repertoires.Both subjects attended a non-profit trau-
matic brain injury rehabilitation programin Berkeley 3-5 days a week. The study wasconducted at the program in a 3 m x 5 mroom. The experimenter and the subjectsboth sat along a counter where the materi-als and data sheets were kept. The subjectssat in a chair approximately 1 meter awayfrom the experimenter, and were workedwith individually. On days that reliabilitywas taken the reliability observer sat alongthe wall opposite to the counter.
Materials
The materials used in the experimentconsisted of 18 common objects. Theobjects were divided into six sets (using aprocedure described later), with three setsfor each subject. For Subject 1, set 1 con-sisted of a funnel, electrical tape, and a rowof staples. Set 2 consisted of a plastic bag, abottle brush, and a three pronged adapter.And set 3 consisted of an extension cord, atire gauge, and a nut cracker. For Subject 2,set 1 consisted of a box of dental floss,binoculars, and a crow bar. Set 2 consistedof a staple remover, wire cutters, and apaper clip. And set 3 consisted of a nightlight, a lint brush, and a paint stirrer. Theseitems were chosen because they werefamiliar to the subjects (correct receptiveand functional use behaviors), but theyfailed to emit the correct tact, mand, andintraverbal responses during the baselinecondition. Several other materials wereused to contrive establishing operations(Michael, 1988) during mand testing andtraining. For example, bicycle tires wereused to help create an establishing opera-tion for the mand tire gauge, and wire was

86 MARK L. SUNDBERG et al.
used to help create an establishing opera-tion for the mand wire cutters.
Response Definitions and Independent andDependent Variables
A response was recorded as correct if thesubject's first response corresponded withthe item being tested. Often, responsessuch as Ahh, Let's see, that's a..., or Oh yeahthat's a... preceded the targeted response.These were scored as correct as long as thekey word was emitted. If the subject said adifferent word first, or part of a differentword, the response was scored as incorrect.If the subject reversed the order of a pair ofwords such as calling a paper clip a clippaper the response was scored as incorrect.The independent variables consisted of
the specific training procedures (describedlater) used for each of the targeted verbaloperants. Basically, the proceduresinvolved the use of contrived establishingoperations, prompting, fading, and differ-ential reinforcement. In general, there werenine dependent variables: the acquisitionof tacts, mands, and intraverbals for sets 1,2, and 3. Specifically, the dependent vari-ables consisted of the percentage of correctresponses during the training and probeconditions, and the number of training tri-als required to meet the session termina-tion criterion (described later).There were two types of reinforced
probes used in the study. One type was afirst-trial probe in which the first trial of atraining session constituted a probe. Theother type was a one-trial generalizationprobe on the operants not targeted forintervention. These generalization probeswere conducted on all the untrained oper-ants prior to the training segment of a ses-sion. For example, during mand trainingprobes were first conducted under tact andintraverbal conditions for each word (thesewere interspersed with probes from othersets). Then the first trial of the mand ses-sion constituted the mand probe. The gen-eralization probes were conducted onapproximately 33% of the sessions. Theseprobes were always conducted by the firstauthor. The training probes and sessionswere mainly conducted by the first and
second authors. Correct responses werereinforced with social praise (e.g., Right!),and the delivery of the manded item undermand conditions. Incorrect responses werefollowed by what was believed to be a neu-tral Ok.
Reliability
Reliability was assessed by having a sec-ond observer simultaneously but indepen-dently score the subjects' responses.Reliability measures were taken onapproximately 20% of the sessions, includ-ing baseline and intervention, and used theformula (agreements/agreements + dis-agreements x 100). In baseline the meanreliability was 100%, and during interven-tion the mean reliability was 99%.
Procedure
For each subject, the nine items wererandomly divided into three groups andassigned to one of three training sets (threewords per set). The three sets were (1) tacttraining, (2) mand training, and (3)intraverbal training (Table 1). The ran-domization procedure consisted of listingthe items on nine separate index cards andshuffling them. The second author pickeda card out of the upside down stack whilethe first author, looking away, started adigital stopwatch with a 1/100 of a secondreading. When the second author said Stopthe watch was stopped, and if the 1/100 ofa second was between 1 and 3 the word
Table 1The three-word sets and assigned training conditionsfor Subjects 1 and 2.
Subject 1 Subject 2Tact Training (Set 1)
funnel dental flosstape binoculars
staples crow bar
Mand Training (Set 2)plastic bag staple removerbottle brush wire cutters
adapter paper clip
Intraverbal Training (Set 3)extension cord night light
tire gauge lint brushnut cracker paint stirrer

TRAUMATIC BRAIN INJURY AND VERBAL BEHAVIOR 87
was assigned to the tact set, if it wasbetween 4 and 6 it went to the mand set,and if it was between 7 and 9 it went to theintraverbal set. A zero resulted in repeat-ing the procedure. For each subject all nineobjects were individually assigned to atraining condition using this procedure.Once a set was filled with three items theprocedure was repeated until there was anumber for an open set.
In the training conditions interventionoccurred for the targeted verbal operants,while the other two operants were probed.All the probes of the untrained operantswere conducted first, followed by the spe-cific training conditions (Table 2). A typicalsession followed the order indicated by thenumbers in the boxes of Table 2. This orderof conditions remained constant across ses-sions, but the order of the individualwords within a set was changed each ses-sion. Subject 1 received training prior toSubject 2.
Table 2The training and probe conditions for each set of threewords. The number in boxes indicates the order of theconditions.
Probe Probe Training
SetI1 Mand Intraverbal Tact
Trainin Probe Probe Training
Seat2 Tact Intraverbal MandTraining Probe Probe TrainingTraining(1) (4) (7)
nSet3 Tact MandI ntraverbalaTraining Probe Probe TrainingTraining(3), (6), (9),
Baseline and object selection. For both sub-jects a pool of familiar objects was gath-ered. The subjects were tested on their abil-ity to emit tact, mand, and intraverbalresponses appropriate for each item.During the tact condition the experimenterwould hold up an item and ask What is this?All responses were followed by a neutral Okfrom the experimenter and recorded. Duringthe mand condition subjects were first askedto (nonverbally) complete a chain of behav-
iors, then an establishing operation wascontrived using a procedure similar to theone used by Hall and Sundberg (1987). Forexample, after the subject had demon-strated the successful use of an adapter, theexperimenter would give the subject athree pronged plug and a two prongedsocket, but withhold the adapter. Theexperimenter would then ask him to con-nect them, thus creating a conditionedestablishing operation by momentarilyaltering the value of an adapter (Michael1982, 1988). All responses were followedby a neutral Ok by the experimenter andrecorded. Intraverbal performance wasassessed by presenting a verbal questionsuch as What do you use to connect a threepronged plug to a two pronged socket? Again,all responses were followed by a neutralOk from the experimenter and recorded.During the mand and intraverbal condi-tions stimulus objects were kept out ofsight by either placing them in an opaquebag, or putting them under the counter.Each operant was tested twice for each
item across two sessions, except undermand conditions where it was only testedonce (due to a procedural error). If the sub-ject was correct on any single trial for anyoperant during baseline the item was notused. The baseline procedure was contin-ued until 9 items met the zero-correct crite-rion (twice for the tact and intraverbal andonce for the mand). For Subject 1 a pool of12 items was needed, and for Subject 2,who had stronger verbal behavior, a poolof 35 items was needed to meet the zero-correct criterion. Subject 2 received oneadditional tact and intraverbal baselinesession on the specific words used bySubject 1.Once the 9 items were obtained for both
subjects they were tested under echoic andtextual conditions to assess the strength ofthose repertoires. During the echoic assess-ment the experimenter would present thesubject with the verbal stimulus Say -All responses were followed by a neutralOk and recorded. During the textualassessment the subject was presented withthe word printed on a flash card, or on apiece of paper, and asked What word is this?

88 MARK L. SUNDBERG et al.
All responses were followed by a neutralOk and recorded.
Intervention: Phase I. Each subject's ninewords were divided into three sets usingthe procedure previously described.During Phase I either tact, mand, orintraverbal training was given on each ofthe three sets. For Subject 1 interventionbegan with tact training only. Intraverbaltraining was added after the sixth session,and mand training was added after thetwelfth session. For Subject 2, who hadstronger verbal behavior and easily han-dled the large number of trials, all threeconditions began simultaneously.
Tact training. Each session began with atact probe for each word. Correctresponses were reinforced with praise, andincorrect responses initiated the start of thetraining procedure. The procedure used fortact training was essentially the same pro-cedure used by Sundberg (1980, 1987) withdevelopmentally disabled individuals.Stimulus control was transferred fromechoic control to tact control by use ofprompting, fading, and differential rein-forcement. The experimenter would holdup an object and say What is this? If noresponse, or an incorrect response occurredwithin approximately 5 seconds an echoic
prompt was given. Following a correctechoic response, the experimenter re-pre-sented the original verbal prompt What isthis? Correct responses were followed bysocial praise, and the next object was pre-sented. Incorrect responses were followedby a mild No, and the repetition of thetransfer procedure (the correction loop).Echoic prompts were gradually faded fromthe full word to the initial sound of theword. The tact training session endedwhen the subject correctly tacted all threeobjects in a row (starting with the first itemon the list) without the echoic prompt, orwhen five transfer trials (tact-echoic-tact)on each word had been given, whichevercame first. (Initially the session terminatedafter 10 trials, but Subject 1 began to showsigns of fatigue, so beginning with thesixth session, and the addition of intraver-bal training, the criterion was reduced to 5trials. Subject 2 started with only 5 trials oneach word.)Mand training. Each session began with a
mand probe for each word (see Table 3).Correct responses were reinforced withpraise and the presentation of the missingobject. Upon receipt of the missing objectthe subject would complete the chain.Incorrect responses initiated the start of the
Table 3The contrived establishing operations and the targeted response for the mands used with Subjects 1 and 2.
Subject 1 Subject 2
Contrived establishing operation Response Contrived establishing operation Response
1. The subject was given a three pronged plug and a 1. The subject was given a card with a staple intwo pronged socket and asked to connect them. Adapter it and asked to remove it. Staple remover
2. The subject was given a deep bottle and asked to 2. The subject was given a piece of wire andclean the bottom. Bottle brush asked to cut it. Wire cutters
3. The subject was given a cracker and asked put it 3. The subject was given a few pieces of paper andin something to keep it fresh. Plastic bag asked to connect them. Paper dip
4. The subject was given a Calistoga bottle with a 4. The subject was asked to clean between his teeth. Flosssmall opening and a bottle of water and asked 5. The subject was asked to read a poster on theto pour the water in the small bottle. Funnel opposite side of a room visible through a
5. The subject was given a hose with a hole in it window. Binocularsand asked to fix it. Tape 6. The subject was asked to separate two boards
6. The subject was given an empty stapler and nailed together. Crow barasked to connect some papers together. Staples 7. The lights were turned off and the subject
7. The subject was asked to plug in an appliance was asked what he needed to turn on if he werewhich was too far from the outlet. Extension cord sleeping. Night light
8. The subject was presented with a tire and asked 8. The subject was shown a pair of pants withto check it. Tire gauge lint on them and asked to clean them. Lint brush
9. The subject was given a hard nut and 9. The subject was given a can of paint andasked to open it. Nut cracker asked to mix it up. Paint stirrer

TRAUMATIC BRAIN INJURY AND VERBAL BEHAVIOR 89
training procedure. The mand trainingprocedure was essentially the same proce-dure used by Hall and Sundberg (1987)with developmentally disabled individu-als. Conditioned establishing operationswere contrived by removing an item froma stimulus array and asking the subject tocomplete a response chain (often the exper-imenter would add the prompt What do youneed?). Completion of the chain was impos-sible without the missing item. Correctresponses were followed by praise and thepresentation of the missing object.Incorrect responses were followed by amild No, and the correction procedure con-sisting of an echoic prompt, reinforcement(praise) for correct echoic behavior, and there-presentation of the initial verbal requestto complete the chain. The missing itemwas only presented when the responseoccurred without the echoic prompt.Echoic prompts were gradually faded fromthe full word to the initial sound of theword. Mand training ended when the sub-ject correctly manded for all three objectsin a row (starting with the first item on thelist) without the echoic prompt, or fivetransfer trials (mand-echoic-mand) on eachword, whichever came first.
Intraverbal training. Each session beganwith an intraverbal probe for each word(see Table 4). Correct responses were rein-
forced with praise, and incorrect responsesinitiated the start of the training procedure.The intraverbal training procedure wasessentially the same procedure used byBraam and Poling (1983) with develop-mentally disabled individuals, exceptechoic rather than tact prompts were used.Stimulus control was transferred fromechoic control to intraverbal control by theuse of prompting, fading, and differentialreinforcement. Attempts were made toavoid the same verbal stimuli that weregiven during the mand probes on thesewords, although that was not always pos-sible (see Table 4). The experimenterwould present the subject with a verbalstimulus (e.g., What do you use to fix a hole ina radiator hose?), and reinforce correctresponses. If no response, or an incorrectresponse, occurred within approximately 5seconds an echoic prompt was given.Following a correct echoic response, theexperimenter re-presented the original ver-bal stimulus. Correct responses were fol-lowed by social praise, and the next objectwas presented. Incorrect responses werefollowed by a mild No, and the repetitionof the transfer procedure. Echoic promptswere gradually faded from the full word tothe initial sound of the word. Intraverbaltraining ended when the subject correctlyresponded to all three questions in a row
Table 4The verbal stimulus and the targeted response for the intraverbals used with Subjects 1 and 2.
Subject 1 Subject 2
Verbal stimulus Response Verbal stimulus Response1. "What do you need to use to plug a three 1. "What do you use to pul a staple out of
pronged plug into a two pronged socket?" Adapter something?" Staple remover2. "What do you use to dean the bottom of 2. "If you're setting up your stereo and you need to
a deep jar?" Bottle brush cut the speaker wire what do you use?" Wire cutters3. "What do you put food in to keep it fresh?" Plastic bag 3. "What can you use to connect a few4. "What do you use to pour oil into your car so papers together?" Paper clip
you won't spill any?" Funnel 4. "What do you use to clean between your teeth?" Floss5. "What do you use to fix a hole in your 5. "What do you use to see something that is far
radiator hose?" Tape away?" Binoculars6. "If a stapler is empty, what do you need 6. 'What do you use to pry apart two boards
to put in it?" Staples nailed together?" Crow bar7. "If an electrical cord won't reach a plug what 7. "If you're going to bed and you want a little
do you need to get?" Extension cord light in your room what do you turn on?" Night light8. "If you have a tire that is low, what do you use 8. '"hat do you use to dean the bits of dirt off
to check the air pressure?" Tire gauge your clothes?" Lint brush9. "If you have a hard nut that you can't open what 9. "If you want to paint a house, what do you use
do you need to use?" Nut cracker to mix up the paint?" Paint stirrer
90 MARK L. SUNDBERG et al.
(starting from the first item on the list)without the echoic prompt, or five transfertrials on each word, whichever came first.
Intervention: Phase II Following the suc-cessful acquisition of the tacts for both sub-jects, the tact training condition (set 1) wasdiscontinued. Also, following acquisitionintraverbal training (set 3) was discontin-ued for Subject 2. The remaining condi-tions, mand training for both subjects andintraverbal training for Subject 1, werechanged to tact training. Specific mand andintraverbal training was discontinued, butmand and intraverbal probes were stillconducted. In Phases II all aspects of thetraining procedure described above for tacttraining were implemented for all theremaining words (set 2 for both subjects,and set 3 for Subject 1).
RESULTS
Baseline and Object Selection
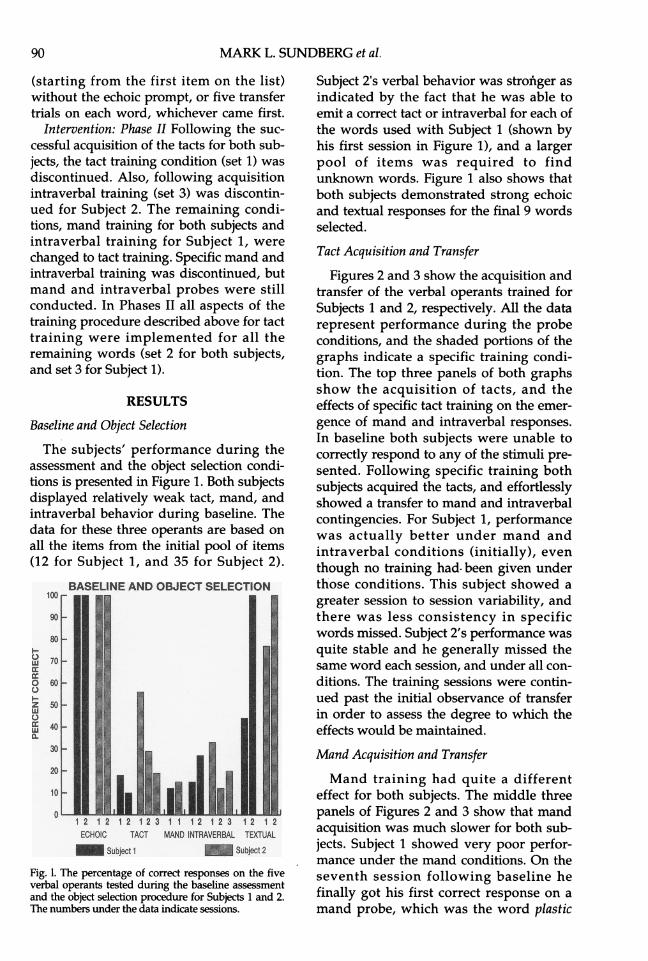
The subjects' performance during theassessment and the object selection condi-tions is presented in Figure 1. Both subjectsdisplayed relatively weak tact, mand, andintraverbal behavior during baseline. Thedata for these three operants are based onall the items from the initial pool of items(12 for Subject 1, and 35 for Subject 2).
BASELINE AND OBJECT SELECTION100
so-LU 70-
ONo00
ECHCC40C MAD-TAERA ETA
I0-
20
10-
-1 2 1 2 12 123 1 1 12 12312 1 2ECHOIC TACT MAND INTRAVERBAL TEXTUAL
Subjec 1 S_SUW 2
Fig. 1. The percentage of correct responses on the fiveverbal operants tested during the baseline assessmentand the object selection procedure for Subjects 1 and 2.The numbers under the data indicate sessions.
Subject 2's verbal behavior was stroinger asindicated by the fact that he was able toemit a correct tact or intraverbal for each ofthe words used with Subject 1 (shown byhis first session in Figure 1), and a largerpool of items was required to findunknown words. Figure 1 also shows thatboth subjects demonstrated strong echoicand textual responses for the final 9 wordsselected.
Tact Acquisition and Transfer
Figures 2 and 3 show the acquisition andtransfer of the verbal operants trained forSubjects 1 and 2, respectively. All the datarepresent performance during the probeconditions, and the shaded portions of thegraphs indicate a specific training condi-tion. The top three panels of both graphsshow the acquisition of tacts, and theeffects of specific tact training on the emer-gence of mand and intraverbal responses.In baseline both subjects were unable tocorrectly respond to any of the stimuli pre-sented. Following specific training bothsubjects acquired the tacts, and effortlesslyshowed a transfer to mand and intraverbalcontingencies. For Subject 1, performancewas actually better under mand andintraverbal conditions (initially), eventhough no training had. been given underthose conditions. This subject showed agreater session to session variability, andthere was less consistency in specificwords missed. Subject 2's performance wasquite stable and he generally missed thesame word each session, and under all con-ditions. The training sessions were contin-ued past the initial observance of transferin order to assess the degree to which theeffects would be maintained.
Mand Acquisition and Transfer
Mand training had quite a differenteffect for both subjects. The middle threepanels of Figures 2 and 3 show that mandacquisition was much slower for both sub-jects. Subject 1 showed very poor perfor-mance under the mand conditions. On theseventh session following baseline hefinally got his first correct response on amand probe, which was the word plastic

TRAUMATIC BRAIN INJURY AND VERBAL BEHAVIOR 91
UAE SPECIRCTACT TRAININGUNE105.
TACT PROSEa 4 SUBJECTI
Z O
BAEIN MANDCMNWRINN PROBE1B _INTVERBAL PROBE
A. J
10
....o15 63 51 4l 5 70
MEI ~SMCIFICIVMMDTRI INGBAENE
100m
ej ] ~~~~~~...- . . M~~~~LANDPROBE
w -.
IC)
....INTRAVE LPROBE
* - ,---.--.---I---.--.--L. .....-l-.. .. .. .. .. .. ..---.-1.----.. '-....5 10 15 20 25 ) 36 40 45 51 55 5)06 70
BASEUNE SPECIFIC IV TRAINING BASMEJN
100N
IMAERC PROSE
5 0 5 3 TACT45 TRA60N65 7
Fig. 2. Percentage of correct responses on tact, mand, and intraverbal probes across the three-word sets for Subject 1.Shaded panels indicate specific training conditions. &

92 MARK L. SUNDBERG et al.
SPECIFI TACT TRAININ1U-T
A PB E CT 2
,..........................
5 10 15 a
MAND PROBE
ccINmsVmF .P.o_
1 15 ...................S
~~MAlt - AN POB
Cd'BS£LiK:n.77"GIL . '0*LIN.
Si#
.LEi..... .
5 10 15 .
Fig. 3. Percentage of correct responses on tact, mand, and intraverbal probes across the three-word sets for Subject 2.Shaded panels indicate specific training conditions.

TRAUMATIC BRAIN INJURY AND VERBAL BEHAVIOR 93
bag (initially the word was sandwich bag,but the subject manded for it as plastic bagand it was accepted as correct). Once hestarted getting that mand correct, he beganto show some transfer to the other verbaloperants, although only with plastic bag.On the 15th session he got a second wordcorrect (bottle brush) on both the mandand intraverbal probes. The transfer to theuntrained operants did occur, but wasmuch less than the transfer that occurredwith tact training. Transfer from mand tointraverbal was slightly better than transferfrom mand to tact, possibly due to theintraverbal variables present in the mandconditions.
Subject 2 also demonstrated his worstperformance under the mand conditions.Even when he began to get the mand cor-rect there was no immediate transfer to theother operants. When transfer did occur itwas always with the words that he wasgetting right under the mand conditions.The only word that showed a consistenttransfer to tact and intraverbal conditionswas wire cutters. This is interesting becausethis subject had been a telephone repairman previous to his accident. However, itstill took ten training sessions under mandconditions before a consistent transfer totact conditions occurred.
Intraverbal Acquisition and Transfer
The bottom three panels of Figures 2 and3 show that both subjects performed rela-tively well under intraverbal conditions.Subject l's performance on the probesoscillated between 33% and 67% correct,and some transfer of control to theuntrained operants occurred, but it was notconsistent. For this subject the pattern wassimilar to that of mand training, but sub-stantially different from tact trainingwhere transfer was fast and consistent.Subject 2 acquired the intraverbalresponses quickly, and showed transfer tothe other operants in a pattern similar to,but slightly better than, tact training.Performance on the probes, as a measure
of long-term retention, showed that bothsubjects demonstrated the strongest long-term retention under tact and intraverbal
conditions, and the weakest under mandconditions. Subject 1 performed slightlybetter under tact conditions than underintraverbal conditions, while Subject 2showed the exact opposite, performing bet-ter under intraverbal conditions thanunder tact conditions.
Phase II
The results of Phase II are presented inthe right-hand columns of Figures 3 and 4.Since both subjects did not effectivelyacquire the mands during specific mandtraining, and Subject 1 did not effectivelyacquire the intraverbals during specificintraverbal training, it was speculated thatspecific tact training would result in atransfer pattern similar to that observedduring Phase I. As a result, the mand andintraverbal conditions were simultane-ously changed to tact training for Subject 1(Figure 2), and the mand condition waschanged to tact training for Subject 2(Figure 3). Training on the tacts from set 1was discontinued for both subjects. ForSubject 1 tact training on the words thathad been previously in the intraverbal con-dition had an immediate and robust effecton performance during the mand probes,thus replicating the effects observed inPhase I. Tacts were acquired in a patternsimilar to Phase I, and tact trainingresulted in four consecutive sessions of100% correct performance under the mandprobe conditions. In addition, the tacttraining improved this subject's intraverbalperformance, stabilizing it at 67% (healways missed the same word, tire gauge).The change from mand training to tact
training did not, however, have the sameeffects as the tact training in Phase I, or asthe change from intraverbal to tact forSubject 1. In fact, tact training on thesewords was very slow and did not substan-tially improve the mand performance foreither subject. Subject 1 did eventuallyshow some improvement on the intraver-bal, however, Subject 2 performed unchar-acteristically poor on the intraverbal. Theearly history of failure in the mand condi-tion of Phase I clearly affected the later

MARK L. SUNDBERG et al.
INTERVENTION
TACT TRAINING
MAND TRAINING
INTRAVERBAL TRAINING -Suj*ec 1
Su. Subject 2
94
BASE
100 LINE
90
80I-0 70LU
c 600Q50
<,>40
g1.30
20
10
100
90
80
LU
m 6000501-z
940
80
a.
20
10
100
90
80I-070-Lu
m4600050I-z40
Wu30-a.20-
10
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37SESSIONS
Fig. 4. The percentage of correct within-session responses during tact, mand, and intraverbal training for Subjects 1 and 2.

TRAUMATIC BRAIN INJURY AND VERBAL BEHAVIOR 95
10 INTERVENTION
O' 60* so TACT TRAINING
t~~~ ~~ eF F I:
70
Z OD
t
E9 I^~~~~~AN'RAINING
I-P
70
z
0
1.2 3 -4 5 B 7 8. 8 10 111213 14 1516 17 18 19 2 21 22 2a 24 3 X 2 X 2X 30 31 32 33 34 33X
I-~~ ~ ~ ~ ~ ~ ~ N
Fig. 5. The number of trials to criterion during tact, mand, and intraverbal training for Subjects 1 and 2.
acquisition of other verbal operants involv-ing the same response topography.
Within-Session Measures
Figure 4 shows the percent correct dur-ing training on each condition. These dataindicate that within-session performance,or short-term retention, was weakest undermand conditions for both subjects. Subject1 had extreme difficulty with this condi-tion, however, he did show a slow butsteady acquisition rate. Only twice (during
the last two sessions) did he score above60% correct. Subject 2 also had difficultywith the mand condition, but he was ableto obtain 100% correct on three sessions.Both subjects' within-session perfor-
mance was best on tact and intraverbaltraining. In terms of individual results,Subject 1 initially performed better duringintraverbal training, but as training pro-gressed he performed better during tacttraining reaching 100% correct on six ses-sions, while never reaching 100% correct

96 MARK L. SUNDBERG et al.
on intraverbal training. Subject 2 clearlyperformed better during intraverbal train-ing reaching 100% correct on ten sessions,while reaching 100% correct only fourtimes during tact training.The results of the second within-session
measure, trials-to-criterion, are presentedin Figure 5. A trial was defined as a singlestimulus-response-consequence relation,and a perfect score for a session was threetrials (one for each word in a set, and allcorrect responses). These data show thatthere was a clear decrease in the number oftraining trials required to meet criterion forboth subjects, for all conditions. This, alongwith the probe data, demonstrates that thespecific training procedures employedwere effective in generating the missingverbal operants. The data also show thatmand training was the most difficult forboth subjects. Subject 1 received an aver-age of 30.2 mand trials per session (636training trials over 21 sessions), comparedto an average of 13 training trials per ses-sion for the tacts (456 training trials over 35sessions), and an average of 12.5 trials persession for the intraverbals (326 trainingtrials over 26 sessions). Subject 2 receivedan average of 15.7 mand trials per session(251 training trials over 16 sessions), com-pared to an average of 9.9 trials per sessionfor the tacts (158 training trials over 16 ses-sions), and an average of 7.3 training trialsper session for the intraverbals (117 train-ing trials over 16 sessions).These data indicate that both subjects
demonstrated the strongest short-termretention under tact and intraverbal condi-tions, and the weakest under mand condi-tions. Subject 1 initially performed betterduring intraverbal training, but later intraining performed better during tact train-ing. Subject 2 performed clearly better dur-ing intraverbal training. These data areconsistent with the long-term retentiondata, with the exception of Subject l's ini-tial performance during intraverbal train-ing. In addition, a comparison of the sub-jects' acquisition rate on the long-termversus short-term trials shows there was asimilar learning pattern. The within-ses-sion measures of trials-to-criterion and per-
cent correct during Phase II tact trainingfollowing intraverbal training were verysimilar to the results obtained on the tactcondition in Phase I. However, the resultsof the trials-to-criterion and percent correctmeasures taken during Phase II tact train-ing, following Phase I mand training, werevery similar to those of Phase I mand train-ing.
DISCUSSION
The results of this study suggest that tactand intraverbal training may be the mostefficient way to generate mands for someindividuals who have sustained a trau-matic brain injury. Direct mand trainingproved to be the least efficient method toproduce manding. These results wereunexpected given previous research withthe developmentally disabled that hadshown mands were acquired faster thantacts (Sundberg, Milani, & Partington,1977), and that direct mand training wasnecessary to establish reliable manding(Hall & Sundberg, 1987).
However, it is possible that the currentdata may simply demonstrate some of thedifferences between these two populations.The studies with developmentally disabledindividuals involved naive subjects whoexhibited very little verbal behavior at theoutset of the studies. The subjects in thecurrent study were at one time competentspeakers, and even after the injury emittedsome successful verbal behavior. Thesesubjects could, for example, mand for avariety of other reinforcers, especiallythose controlled by unconditioned estab-lishing operations, and it was clear thattheir mand repertoires were not com-pletely absent. There is some evidence inthe mand and tact literature that suggeststhat this manding history may play a keyrole in the transfer of control from tact tomand variables.Skinner (1957) suggested that a mand
frame could facilitate this transfer. Forexample, if a person has a successful his-tory of manding with a frame such as Iwant..., then newly-acquired tacts couldemerge within the mand frame withoutdirect training. Hall and Sundberg (1987)
TRAUMATIC BRAIN INJURY AND VERBAL BEHAVIOR 97
did find that newly trained tacts led to theemergence of untrained mands following asuccessful history of mand training. Theseeffects were also demonstrated by Sigafooset al., (1990) who found that the presenceof the mand frame Want... was sufficient toobtain the transfer of control from tact tomand variables. In the current study, thistransfer effect occurred for both subjects. Inaddition, transfer occurred from tact tointraverbal for both subjects, and fromintraverbal to mand, and intraverbal to tactfor Subject 2.
It still remains unclear as to why themand was so difficult to directly teach,especially since it emerged so easily aftertact training. It could be argued that theconditioned establishing operations weresimply not strong enough to evoke thebehavior. However, all the mands in thestudy involved mild conditioned estab-lishing operations occurring in daily liv-ing, and were randomly assigned to train-ing conditions. The sizeable differencesobserved between the direct and indirecttraining conditions would seem to negatelack of controlling strength as a variable.Note also that on two occasions Subject l'sbest performance across two consecutivesessions was under the untrained mandprobe conditions.The results are also inconsistent with
Skinner's (1957) analysis of the order ofdamage in aphasia which suggests that themand would be stronger than the tact andintraverbal. Skinner (1957) states that
aphasia is a condition of lowered probability ofresponse... Damage is usually most severe inverbal behavior receiving generalized reinforce-ment. The order of damage seems to follow theorder of "difficulty" deducible from the avail-ability of a minimal repertoire. Textual andechoic behavior often survive (unless relevantsensory defects are involved) while intraverbalsand tacts appear to be most vulnerable....Verbalbehavior which has been reinforced in relationto some special condition of deprivation or aver-sive stimulation [mands]...remains relativelyaccessible. (p. 218-219)
A possible explanation for this discrep-ancy concerns the two different types ofmands identified by Michael (1988). Somemands did survive following the subjects'accidents, but they were those mainly con-trolled by unconditioned establishing oper-
ations. However, the current studyinvolved relatively mild conditioned estab-lishing operations. It seems possible thatthe controlling conditions for these typesof mands are actually more complicatedthan those for unconditioned establishingoperations. A mand controlled by a condi-tioned establishing operation involves thepresentation of stimuli which alter theeffectiveness of other stimuli as conditionedreinforcers. The targeted response may beharder to bring under the control of thisrather complicated stimulus arrangement.In addition, the stimuli presented in orderto contrive the establishing operation mayhave overshadowed the development ofcontrol by the conditioned establishingoperation. This seems quite plausible sincethe subjects already had a history of emit-ting other verbal and nonverbal responsesin the presence of these stimuli. For exam-ple, the subjects would frequently pan-tomime the action of the missing item, asin closing the hands as if cracking a nut.Another possibility may be that these
mand conditions resemble quite closelyaversive problem solving contingencieswhich these subjects unsuccessfullyencounter on a daily basis (e.g., trying toask for a needed item at a store). Both sub-jects had long histories of failure, particu-larly under difficult conditions, and asSkinner (1957) further pointed out "ver-bal...behavior which as been punished islikely to be relatively weak" (p. 219). Thispoint was supported by the subjects' poorperformance in Phase II following theunsuccessful mand condition. It was notedthat Subject 2 swore quite frequently dur-ing failed mand trials, often sayingDammit, I know this, dammit, or Oh shit,shit.... It is also possible that these condi-tions, and others like them, have becomeconditioned aversive stimuli elicitingrespondent behaviors which may competewith establishing operant stimulus control.During a trial in the baseline condition thissame subject suffered a severe panic attackwhere he hyperventilated and stiffened hisbody for several minutes.The other verbal operants may have
been acquired faster than mands because it

98 MARK L. SUNDBERG et al.
was simply easier to bring the behaviorunder stimulus control. As Skinner (1957)pointed out, in the echoic and textualrepertoires there is point-to-point corre-spondence between the stimulus and theresponse product, and they involve a mini-mal repertoire. This relatively tight form ofstimulus control may partly explain whythese repertoires remained at strength afterthe subjects' accidents. The tact relationused in the current study involved a formof stimulus control where a single stimuluscontrolled a single response, and the rela-tion tends to be quite consistent (e.g., a nutcracker is always called a nut cracker). Theintraverbal condition also involved stimuliwhich evoke specific responses in a consis-tent manner (e.g., you fix a hole in a hosewith...tape). The mand, however, as statedpreviously, may have involved stimuliwhich evoked behaviors other than the tar-geted behavior.There are some additional variables to
consider in evaluating these results. Theoperants tested were not pure verbal oper-ants. The mand condition also involved anintraverbal prompt such as What do youneed.... The tact condition also involvedintraverbal variables with the verbalprompt What is this? And finally, theintraverbal condition often containedechoic variables in the question as in nut inthe nut cracker trial. It might be noted,however, that in the later sessions of themand and tact conditions both subjects fre-quently gave the answer before the experi-menter could say the intraverbal prompt.In the intraverbal, however, there was ini-tially some concern over the unavoidableechoic variable in some questions. Thiswas especially of concern when, for Subject2, the three most echoically promptedresponses ended up (randomly) groupedtogether in the mand condition. However,that data show that the subject still consis-tently missed these in the early sessions,while correctly responding to otherintraverbals both when trained directly onthe intraverbals, and when trained indi-rectly via the tacts.
It is unclear what the effects of the trans-fer trials themselves were on the transfer
process. The mand probes may have beennecessary to get the effects, that is, theremay need to be some contact with themand conditions. It could be speculatedthat transfer would occur, but it is mostlikely that the opportunity to emit theresponses under the control of the othervariables played a role in the transfer,especially since correct responses werereinforced in the probe condition. Thisissue should be examined in futureresearch.The results support Sidman et al.'s,
(1971) findings that there is a differentrecovery course for different operants. Inaddition, the results demonstrate the valueof Skinner's analysis of verbal behavior forthe assessment and treatment of verbalproblems faced by brain injured individu-als. Once these verbal deficits are identi-fied, a more efficient verbal interventionprogram can be designed. For example,Subject 1 in the current study, could benefitfrom extensive tact training, a moderatelevel of intraverbal training, and the peri-odic arrangement of the establishing oper-ations necessary to evoke a mand. Subject 2could benefit from a similar program, butwould probably benefit from moreintraverbal training than Subject 1. Theseresults are important because, for example,much of the focus of the verbal interven-tion prior to the study for Subject 1 hadinvolved intraverbal training. In fact, it hadtaken hundreds of direct training trials toobtain some simple intraverbal relations.The current results demonstrate whyacquisition was so slow-the tact reper-toire was missing. This is importantbecause often a substantial amount of theverbal intervention provided for braininjured individuals involves intraverbal-only training. This is exemplified by manyof the standard activities in rehabilitationprograms such as group counseling, verbalmemory tasks, problem solving exercises,convergent and divergent thinking exer-cises, reading comprehension, computertasks, etc. This may, in part, explain whythis population tends to progress so slowlyafter the acute stages of rehabilitation.
In conclusion, the results have shown
TRAUMATIC BRAIN INJURY AND VERBAL BEHAVIOR 99
that with brain injured individuals you canteach one verbal operant, and as a result,obtain as many as two additional operantswithout, direct training. This is importantgiven the well-recognized problemsinvolving the acquisition of verbal behav-ior by individuals with brain injuries. Theresults also show that there are differencesbetween tact, mand, and intraverbal reper-toires. These differences may be seen in therate of acquisition of each operant, and inthe transfer effects observed between oper-ants, such as the robust transfer effectobserved with tact training, but not withmand training.The current data provide further support
for Skinner's (1957) assertion that there isan experimental basis to his conceptualdistinction between the verbal operants(see Oah & Dickinson, 1989, for a review).There still, however, is a need for furtherresearch on this topic. Most importantly,the current study needs to be replicatedwith other subjects, especially those whohave other types of brain injury. In addi-tion, it would be interesting to conduct thisstudy with normal children. Would theirresults look more like those of the develop-mentally disabled or the brain injured?While several questions remain to beanswered in future research, it seems clearthat Skinner's formulation of verbal behav-ior can make a substantial contribution tothe assessment and treatment of the verbaldisorders produced by traumatic braininjury.
REFERENCESBraam, S.J., & Poling A. (1983). Development of
intraverbal behavior in mentally retarded individu-als through transfer of stimulus control procedures:Classification of verbal responses. Applied Researchin Mental Retardation, 4, 279-302.
Carroll, R., & Hesse, B. E. (1987). The effects of alter-nating mand and tact training on the acquisition oftacts. The Analysis of Verbal Behavior, 5, 55-65.
Chapey, R. (1986). Language intervention strategies inadult aphasia (2nd ed.). Baltimore, MD: Williams &Wilkins.
Darley, F. (1972). The efficacy of language rehabilita-tion in aphasia. Journal of Speech and HearingDisorders, 37, 3-21.
Doyle, P. J., Goldstein, H., & Bourgeois, M. S. (1987).Experimental analysis of syntax training in Broca'saphasia: A generalization and social validationstudy. Journal of Speech and Hearing Disorders, 52,143-155.
Hagen, C. (1984). Language disorders in head trauma.In A. Holland (Ed.). Language disorders in adults (pp.245-281). San Diego: College-Hill Press.
Hall, G., & Sundberg, M. L. (1987). Teaching mandsby manipulating conditioned establishing opera-tions. The Analysis of Verbal Behavior, 5, 41-53.
Holland, A. (1984). Language disorders in adults. SanDiego: College-Hill Press.
Kirshner, H., & Sidman, M. (1972). Scanning patternsin aphasic patients during matching-to-sampletests. Neurophychologia, 10, 179-184.
Lamarre, J., & Holland, J. G. (1985). The functionalindependence of mands and tacts. Journal of theExperimental Analysis of Behavior, 43, 5-19.
Lee, V. L., & Pegler, A. M. (1982). Effects on spellingof training children to read. Journal of the Exper-imental Analysis of Behavior, 37, 311-332.
Leicester, J., Sidman, M., Stoddard, L. T., & Mohr, J.P.(1971). The nature of aphasic responses. Neuro-phychologia, 9, 141-155.
Michael, J.L. (1982). Distinguishing between discrimi-native and motivational functions of stimuli. Journalof the Experimental Analysis of Behavior, 37, 149-155.
Michael, J.L. (1984). Verbal behavior. Journal of theExperimental Analysis of Behavior, 42, 365-376.
Michael, J.L. (1988). The establishing operation andthe mand. The Analysis of Verbal Behavior, 6, 3-9.
Mowrer, D.W. (1988). Methods of modifying speech-behaviors. Prospect Heights, IL: Waveland Press.
Muma, J. R., Hamre, C. E., & McNeil, M. R. (1986).Theoretical models applicable to intervention inadult aphasia. In R. Chapey (Ed.). Language inter-vention strategies in adult aphasia (2nd ed.) (pp. 277-283). Baltimore, MD: Williams & Wilkins.
Salvatore, A. P., & Thompson, C. K. (1986).Intervention for global aphasia. In R. Chapey (Ed.)Language intervention strategies in adult aphasia (2nded.) (pp. 402-418). Baltimore, MD: Williams &Wilkins.
Sidman, M. (1971). The behavioral analysis of aphasia.Journal of Psychiatric Research, 8, 413-422.
Sidman, M., Stoddard, L. T., Mohr, J. P., & Leicester, J.(1971). Behavioral studies of aphasia: Methods ofinvestigation and analysis. Neurophychologia, 9, 119-140.
Sigafoos, J., Reichle, J., Doss, S., Hall, K., & Pettitt, L.(1990). "Spontaneous" transfer of stimulus controlfrom tact to mand contingencies. Research inDevelopmental Disabilities, 11, 165-176.
Skinner, B. F. (1957). Verbal behavior. EngelwoodCliffs, NJ: Prentice Hall.
Sundberg, M. L. (1980). Developing a verbal repertoireusing sign language and Skinner's analysis of verbalbehavior. Unpublished doctoral dissertation, WesternMichigan University.
Sundberg, M. L. (1983). Language. In J. L. Matson, &S.E. Breuning (Eds.), Assessing the mentally retarded(pp. 285-310). New York: Grune & Stratton.
Sundberg, M. L. (1987). Teaching language to thedevelopmentally disabled: A course manual. PrinceGeorge, B.C.: College of New Caledonia Press.
Sundberg, M. L., Milani, I., & Partington, J. W. (1977,Aug.). The use of sign language with hearing non-vocalmentally impaired persons. Paper presented at the85th Annual Meeting of the American Psychol-ogical Association, San Francisco.
Watkins, C. L., Pack-Teixteira, L., & Howard, J. (1989).Teaching intraverbal behavior to severely retardedchildren. The Analysis of Verbal Behavior, 7, 69-81.