think kidneys education event 7th october master slide deck final 071014
TRANSCRIPT

Are you educating people about Acute Kidney Injury? Working together to share experiences and develop education resources for the future Education workshop| Version 0.1 7th October 2014 10.00-16.00 Prepared by the Think Kidney team 07.10.2014

PROGRAMME 10.00 Welcome and housekeeping 10.10 Setting the scene
• The AKI National Programme • Why is education important to AKI?
10.25 AKI Education – maximising learning 11.00 What type of educational resources are available at the moment 12.10 Question Time Panel 12.30 Soapbox – an opportunity for delegates to present their resources 13.00 Lunch 13.45 Group Work in your clinical perspective 14.55 Feedback from Group Work 15.10 Using social media to reach a wide range of stakeholders 15.40 Closing remarks and next steps 16.00 Close

Setting the scene 10.10 – 10.25
The AKI National Programme and why education is important to AKI?
Mike Jones Acute Physician Royal College of Physicians

National Acute Kidney Injury
(AKI) Programme
• It is estimated that 1 in 5 emergency admissions into hospital are associated with AKI (Wang et al, 2012)
• Up to 100,000 deaths in secondary care are
associated with AKI and 1/4 to 1/3 have the potential to be prevented (National Confidential Enquiry into Patient Outcome and Death (NCEPOD) Adding Insult to Injury 2009)
• Not a specialty specific issue - the majority of cases arise and/or are managed in the community or across all specialities within secondary care (Selby et al, 2012).
• Estimated additional cost to NHS of £500 million (NHS Kidney Care)
Acute Kidney Injury

Acute Kidney Injury

Acute Kidney Injury

”One in five emergency admissions to hospital will have
AKI”
"AKI is 100 times more deadly than MRSA infection”
”Around 20 per cent of AKI cases are preventable”
”costs of AKI to the NHS are £434-620m pa”

‘reducing avoidable death, long-term disability and
chronic ill health…’
•VTE prevention: estimate 25,000 deaths pa
Data derived from: Hospital Episode Statistics Annual Report 2010,
DoH VTE Prevention Programme 2010 and Selby et al 2012

Incidence of AKI is increasing
Hsu CY et al. Kidney International (2007) 72, 208
* Per 100,000 person years
Hsu RK et al. JASN 2013;24:37-42
* Per million person years
AKI not requiring dialysis Dialysis-requiring AKI
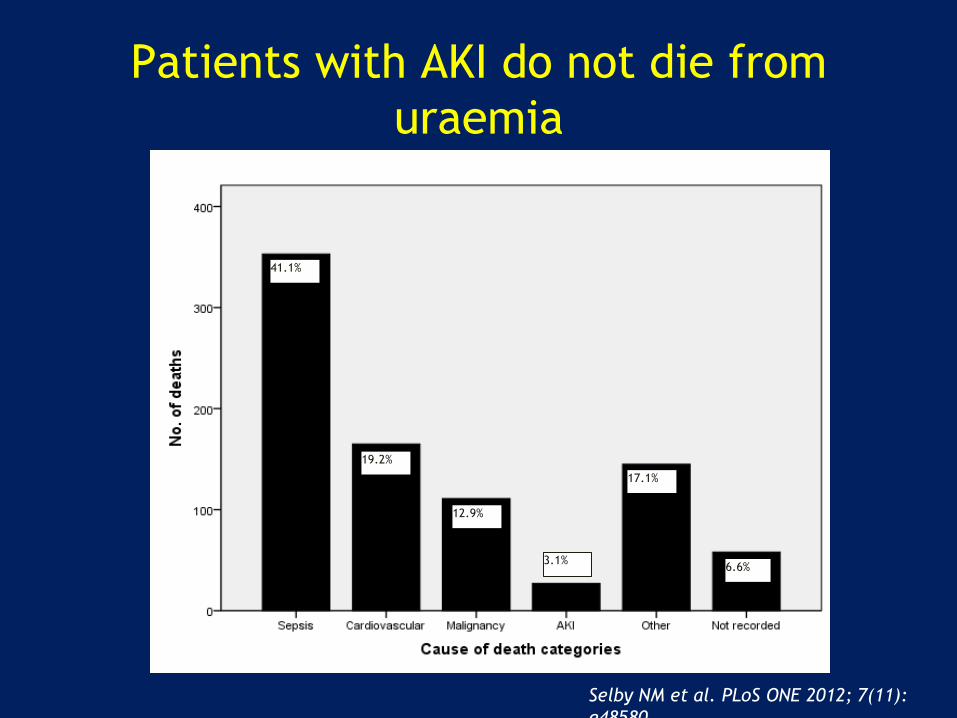
Patients with AKI do not die from
uraemia
41.1%
19.2%
12.9%
17.1%
6.6% 3.1%
Selby NM et al. PLoS ONE 2012; 7(11):
e48580

Bi-directional relationship of AKI and CKD
Ishani A et al. JASN 2009; 20: 223–228
233,803 hospitalised patients aged over
67
AKI increased risk of ESKD by 13 fold
Baseline renal
function
Rate ratio for
hospital admission
with AKI*
eGFR >60 1.0
eGFR 45-59.9 2.3
eGFR 30-44.9 5.6
eGFR 15-29.9 13
*non-proteinuric group shown; similar pattern seen across all
levels of proteinuria
James MT et al. Lancet 2010; 376: 2096-2103
1million patients with baseline assessments
of serum creatinine and proteinuria
CKD and proteinuria increase risk of AKI

NCEPOD report published in 2009
Poor assessment of risk factors for AKI and acute illness
Delays in recognising AKI
Most patients with AKI are not cared for by nephrologists
Post admission AKI avoidable in 21%
‘Good’ care in <50% cases

Key findings
Only 50% of AKI care considered good
Poor assessment of risk factors
Unacceptable delay in recognition of
post-admission in AKI in 43%
22 patients died with a primary
diagnosis of post-admission AKI which
was predictable and avoidable
Complications missed (13%),
avoidable (17%) or badly managed
(22%)

Conclusion
Systematic failings in AKI
Failures in:
Recognition and management of AKI
Recognition and management of
complications
Referral and support
Failures in recognition of the acutely ill

Primary Aim
The primary aim of the National Programme is to ensure avoidable harm related to AKI is prevented in all care settings.

The purpose of the National Programme is to deliver and implement a structure and tools within three years that will lead to a fall in the number of preventable episodes of AKI, and with that a reduction in deaths associated with AKI. It will lead work on the development of clinical tools, information and levers and prioritise patient empowerment. It will utilise commissioning pathways and other clinical networks. It will also establish local and national data collection and audit leading to further safety improvement and target research towards areas that require elucidation.
Programme Purpose

The primary aim of the National Programme is to ensure avoidable harm related to AKI is prevented in all care settings. It will aim to do this by: • Ensuring that a variety of tools and interventions are developed and
implemented to support the prevention, early detection, treatment and enhanced recovery of patients with AKI.
• Ensuring that patients who develop AKI are appropriately managed to reduce further deterioration, long term disability and death.
• Ensuring that appropriate education and training programmes are developed for all health professionals based on best available evidence.
• Ensuring that commissioners, health care professionals and managers are aware of the importance and risks of AKI and appropriate local strategies to reduce the burden of AKI are developed.
Programme Objectives

• Developing a national registry and audit for AKI leading to an improvement strategy on a national and local basis to reduce unwarranted variation in care.
• Involving patients and the public in understanding the risk of AKI and preventative measures through education and appropriate access to personal information.
• Supporting the development of a commissioning structure to allow local service configuration to provide quality care to individuals with AKI.
• Identifying the research agenda for AKI (including basic science, clinical care and service delivery).
Programme Objectives continued

We
ll G
rou
p
Acute Kidney Injury Patient Pathway
AKI National Programme
At
Ris
k G
rou
p
Dia
gno
sis
Tre
atm
en
t
Re
cove
ry
At
Ris
k +
Eve
nt

Education Workstream
Formalised Education Publicity Campaign
Core Education Workstream Group
Michael Jones Michael Wise Cat Shaw Nicky Wood Michelle Timoney Chris Laing Sue Shaw Kathryn Griffith Claire Scott Karen Thomas Winnie Wade Martin Christian Pauline Pinkos

AKI Education – maximising learning
10.25 – 11.00
Winnie Wade
Director of Education
Royal College of Physicians

Winnie Wade and David Parry
Royal College of Physicians
AKI Education - maximising learning
October 2014

Objectives
• Identify factors that affect learning
• Recognise the significance of different learning styles
• Identify different modes of learning
• Consider the challenges in designing educational programmes
• Propose solutions to maximise learning

What comes first – the subject or the learner?

“Tell me and I forget”
“Show me and I remember”
“Involve me and I learn”

Quiz

Activity
In pairs, answer the quiz questions on the handout. Form a group with 4 people seated near you. Reach a consensus on your answers.

Answers to quiz
1. ii
2. iii
3. i
4. ii
5. All of them
6. i

Activity
Maximising learning about AKI – what are the challenges?

What are the Challenges?
Time
Number of
learners

Change in role
Teacher as ‘expert’
Teacher as ‘facilitator’

Change in role
Teacher as Expert Teacher as Facilitator Teaching objectives Learning objectives
Telling Listening
Discourage participation Encourage participation
Ask fewer questions Ask a lot of questions
No feedback Constructive feedback

Some people prefer to take in information through:
DOING PICTURES WORDS
CONCRETE ABSTRACT
Learning styles

Learning Styles
• Activists
• Reflectors
• Theorists
• Pragmatists (Honey and Mumford, 1986)

Adult Learning
• Effective learning environment
• Involve learners – learner-teacher collaboration
• Learners diagnose own needs
• Learners formulate their learning objectives
• Develop learner’s skills of critical reflection
The Educational Cycle
• Assessing the individual’s needs
• Setting educational objectives
• Choosing and using a variety of methods of teaching and learning
• Assessing that learning has occurred

online Face-to-face
Blended
learning
Flexible provision/Flexible delivery
Learning Resources Learning Resources
Learning Resources
On-the-job
learning
Learning Resources

Strengths of learning about AKI on-the-job
• Rich in context and clinical content
• Often 1:1, so more tailored teaching
• Opportunities for active learning, feedback and role modelling
• Good place to learn clinical skills and clinical reasoning
• Context of learning matches context for future practice

Maximising Learning
• Recognise individual learning needs
• Encourage autonomy in learning
• Create a safe, supportive learning environment
• Encourage self-reflection
• Provide a variety of modes of learning
Train the teachers

Questions?
What type of educational resources are available at the moment 11.00 – 12.10 AKI: a national learning programme for pharmacy- Sue Shaw, Advanced Renal Services Pharmacist, Royal Derby Hospitals NHS Foundation Trust Engaging health care professionals using electronic learning resources – Gang Xu, Senior Nephrology Trainee, East Midlands Deanery Apps for Education, - Ben Bray, Quality Improvement Fellow, King's College London NICE AKI online learning for nurses and healthcare support workers – Elaine Whitby, Associate Director – Education and Support, NICE How Can We Translate Improved Education on AKI into Better Care For Patients? – Andy Lewington, Consultant Renal Physician/Honorary Clinical Associate Professor, Director of Undergraduate Medical Education Leeds Teaching Hospitals Trust

What type of educational resources are available at the moment
11.00 – 12.10
AKI: a national learning programme for pharmacy
Sue Shaw
Advanced Renal Services Pharmacist
Royal Derby Hospitals NHS Foundation Trust

Dr Sue Shaw
Advanced Renal Services Pharmacist,
Royal Derby Hospital
Adrian Coleman, Caroline Ashley, Claire Morlidge, Emily Horwill, Rania Betmouni, Renal Pharmacists.
Nick Selby,
Consultant Nephrologist.



CPPE learning@lunch

1. Clinical Pharmacist (Pre-reading materials)

2. Case discussions (Medicines optimisation in AKI, Contrast-induced nephropathy, ‘Sick Day Rules’)

Case Three:
• Pankaj Gupta is a 76-year-old male with stage 3 CKD and hypertension. He has presented to A&E after being unwell with diarrhoea and vomiting for more than 24 hours.
• DHx: Bendroflumethiazide 2.5mg OM
Ramipril 10mg ON
Simvastatin 40mg ON
Trimethoprim 200mg BD (UTI)

• Good uptake of the programme including at national pharmacy events
• Linked to national Medicines Optimisation Toolkit produced by the UK Renal Pharmacy Group
• Supports the Royal Pharmaceutical Society work for community pharmacists regarding ‘Sick Day’ rules and local CQuin pathfinder project

What type of educational resources are available at the moment
11.00 – 12.10
Engaging health care professionals using electronic learning resources
Gang Xu, Senior Nephrology Trainee, East Midlands Deanery

+ Engaging health
care professional
using electronic
learning
resources…
Improving Outcomes in Acute Kidney Injury
(AKI)through education.
G Xu, R Westacott, R Baines, N Selby, S Carr.

+
NECEPOD report showing bad data for kidney patients.

+

+

+

+ eLearning….

+

+
http://www.uhl-library.nhs.uk/aki/index.html

+
http://www.uhl-library.nhs.uk/aki/index.html

+
http://www.uhl-library.nhs.uk/aki/index.html

+
http://www.uhl-library.nhs.uk/aki/index.html

+
http://www.uhl-library.nhs.uk/aki/index.html

+ Lectures / Small group session:
Integrated into established “protected” teaching sessions (Program
expanded)
Grand round / department meetings.

+ Measure the changes:
Using TurningPoint software collected data on knowledge
and confidence of clinicians when treating patients with AKI.
Before and after the educational package was developed and
deployed.

+ What did we find ( n = 319)…

+ Did any one learn anything???

+ Did any one learn anything???

+ MCQ test on AKI knowledge.

+ Still much to be done….
Low number of doctors used the e-learning tool
However higher than expected uptake from other health care
professionals.
Post intervention number of patients with AKI having
documented urine-dip:

+ Summary:
Better education needed still…
Electronic resources is a potentially powerful tool
Engagement remains the key
Traditional teaching still has a firm place.

+ Thank you for your time…..

What type of educational resources are available at the moment
11.00 – 12.10
Apps for Education
Ben Bray
Quality Improvement Fellow
King's College London

RCPE AKI App
Outline of project & features
Learning points

Outline
• Funded by NHS Kidney Care
• Produced & owned by RCP Edinburgh
• Content written by clinicians
• Clinical content approved by Renal Association, RCP Edinburgh & Society of Acute Medicine
• Free for users
• Launched June 2013
• Technical update Sep 2014








7078 unique users

Global reach
0 10 20 30 40 50 60
Europe
Asia
North America
South America
Middle East
Central America
Africa
Oceania
% active users

0 10 20 30 40 50
iPhone
iPad
Android Phone
Android Tablet
% active users
vs

Learning points
− Expensive & time consuming
− Relationship with developers v important
− Needs commitment to update and maintain
+ Wide reach
+ Democratic & accessible
+ Usage analytics

Download
• Search “AKI app” for RCPE app on iTunes store or Google Play store
• Search “London AKI app” for London AKI app on iTunes store
More info:
[email protected] [Bryony Jackson]

What type of educational resources are available at the moment
11.00 – 12.10
NICE AKI online learning for nurses and healthcare support workers
Elaine Whitby
Associate Director – Education and Support
NICE

NICE AKI online learning for nurses and healthcare support workers Elaine Whitby Oct 2014

Page No. | Date
NICE guidance & e-learning
• August 2013 NICE guideline published: Acute kidney
injury: prevention, detection and management of acute
kidney injury up to the point of renal replacement therapy
• Search for existing e-learning: programmes or modules
for doctors or pharmacists, nil specific to nursing
• Recognition - nurses & healthcare support workers
crucial to identifying risk and early detection
• NICE commissioned e-learning resource
• Published March 2014

Page No. | Date
Aim & objectives
Audience • Nurses and healthcare support workers Aim • The aim of this learning programme is to support nurses and healthcare support workers in all
settings in preventing and identifying AKI. Learning outcomes for nurses: • Define AKI • Recognise and assess patients at risk of AKI • Recognise and assess signs and symptoms of AKI • Escalate patients with AKI risk factors, signs or symptoms to medical staff or advanced nurse
practitioner (ANP) • Support the multidisciplinary team in the management of a patient with AKI in primary or
secondary care • Support patients and carers throughout the course of their illness and afterwards Learning outcomes for healthcare support workers: • Contribute to the assessment of patients at risk of AKI • Report results to the nurse or doctor responsible for the patient’s care • Escalate any result that shows positive for blood or protein • Calculate and record an early warning system (EWS) tracker and urine output (U/O). • Record and escalate an abnormal EWS tracker or abnormal U/O

Page No. | Date
5 Sections:
• What is AKI and who is at risk?
• How do we recognise and prevent AKI?
• How do we manage AKI?
• How do we support patients and carers?
• Clinical case study
Nurses - all sections
HSWs - section 2
Structure





Page No. | Date
The story so far
• 1st NICE online learning specifically for nurses
• Evaluation: 669 people enrolled
Qualitative feedback:
• ‘I found the tool extremely useful’
• ‘Great learning resource’
• ‘It was helpful to be able to judge my level of understanding
as I worked through the units’.
• ‘The presentation is interactive and memorable ….flowed
well making it easy to work through’
Problems:
• Monitoring completion
• Obtaining certificates

Page No. | Date
Next steps
Addressing technical issues
Increasing feedback
Widening access: discussions with e-learning for healthcare (e-LfH) to
host the module
Tool access: http://www.nice.org.uk/guidance/cg169/resources

What type of educational resources are available at the moment
11.00 – 12.10
How Can We Translate Improved Education on AKI into Better Care For Patients?
Andy Lewington, Consultant Renal Physician / Honorary Clinical Associate Professor, Director of Undergraduate Medical Education Leeds Teaching Hospitals Trust

Acute Kidney Injury: What Taught
Programmes Are Available?
Dr AJP Lewington
Consultant Renal Physician/Honorary Associate Professor
Director of Undergraduate Medical Education
Leeds Teaching Hospitals

Declaration of Interest
• AbbVie – Advisory Board for Melanocortin
therapy for AKI, Honoraria for Lectures
• AM Pharma – Advisory Board and Co Chief
Investigator for Alkaline Phosphatase therapy for
AKI
• Alere – Honoraria for chairing meeting
• Bioporto – Advisory Board for NGAL
• Fresenius – Honoraria for lecture at ICS
• Baxter – Honoraria for lecturing on IV Fluids

Leeds Teaching Hospitals/University of Leeds

Levers
• NCEPOD
– Adding Insult to Injury 2009
• NICE
– AKI CG 169 2013
– AKI Quality Standard 2014
– IV Fluids CG 174 2013
• NHS England
– AKI warning March 2015


Guidelines need an
implementation strategy

Patient Education?

Undergraduate Medicine
• Identify where renal medicine is taught in
the curriculum and what is covered
– University of Leeds
• 1st Yr – Body Systems
– 10 lectures/3 seminars
• 2nd, 3rd and 5th Yr clinical placements
• RRAPID simulation course
– scenarios with patients developing sepsis, hypovolaemia
and AKI
• Assessment – written and OSCEs

Recognising And Responding To Acute
Patient Illness And Deterioration
ALT Conference 2014, Warwick
S. Bickerdike, L. Smith, A. Dean,
I. Kozieradzka-Ogunmakin, A. Lewington

The RRAPID curriculum spiral

Video demonstrations
Photographs
Medical charts


iPhone app

New version
NEWS calculator
AKI Risk Calculator
Facilitate transition from student to Foundation Year
iPhone app

The RRAPID eBook and iPhone app
Available in the App Store FREE
or
eBook at rrapid.leeds.ac.uk/ebook
Website rrapid.leeds.ac.uk

Postgraduate Medicine

Primary Care
• Renal Medicine?
• Building a case
• secondary care placements in Renal
Medicine - Leeds
• Target Teaching Days
– Make it relevant
– Link CKD and AKI
– with a GP
– cases

Challenge Make AKI the remit of ALL GP’s and General medicine teams
• The greater the number of risk factors an individual patient has for AKI the greater the likelihood of AKI being present on admission.
• About 50% of acute medical patients are taking nephrotoxic medication prior to admission

Secondary Care
• Local postgraduate programmes
– FY, CMT, StRs, Grand Rounds
– Departmental
• National programmes
– CCrISP – Care of the Critically Ill Surgical
Patients – Royal College of Surgeons
– IMPACT

Conferences - UK
• Royal Society of Medicine
– AKI Frontiers – 26 Sept 2014
• Royal College of Physicians - London
– 28 Oct 2014 – AKI Update
• Renal Association/EDTA - London
– 28/31 May 2015
• British Renal Society
• Royal Free/UCL
– AKI Academy – 18/19 Oct 2014

Conferences - UK
• Yorkshire & Humber AKI Patient Care
Initiative (AKIPCI) – Wakefield
– 17 October 2014
• STOP AKI Study Day – Leeds
– 6 November 2014
• Leeds 2nd Critical Care Nephrology
Conference
– 19 May 2015

Conferences - International
• CRRT – San Diego
– 17-20 Feb 2015
• International Society of Nephrology –
Cape Town
– 13-16 March 2015
• Need an AKI conference calender on AKI
website

Summary
• Need to develop Educational strategy
– covers undergraduate and postgraduate training
• curriculum
• organic
– multiprofessional/interprofessional
– interesting
• link in with sepsis, fluids etc
• link with national programmes
– assessed
– sustainable

Thank You

Question Time Panel 12.10 – 12.30
Panel Members
Sue Shaw, Advanced Renal Services Pharmacist, Royal Derby Hospitals NHS Foundation Trust
Gang Xu, Senior Nephrology Trainee, East Midlands Deanery
Ben Bray, Quality Improvement Fellow, King's College London
Elaine Whitby, Associate Director – Education and Support, NICE
Andy Lewington, Consultant Renal Physician/Honorary Clinical Associate Professor, Director of Undergraduate Medical Education Leeds Teaching Hospitals Trust

Soap Box Session
12.10 – 12.30 An opportunity for delegates to present their resources in a rapid fire session where each presenter will be allowed 2 minutes to present their resource Kathryn Griffith General Practitioner Royal College of General Practitioners

Reverse Brainstorming How to Damage Marjory’s Kidneys
Kathryn E Griffith
Clinical Champion for Kidney Care
Royal College of General Practitioners

Causes of AKI Exposures Susceptibilities
Sepsis Dehydration or volume depletion
Critical illness Advanced age
Circulatory shock Female gender
Burns Black race
Trauma CKD
Cardiac surgery especially
bypass
Chronic heart, lung or liver
disease
Major surgery Diabetes mellitus
Nephrotoxic drugs Cancer
Radiocontrast agents Anaemia
Poisonous plants and animals

Marjory Aged 88 Group1
• Marjory lives alone and enjoys life
• What can she do to damage her kidneys?

How to Damage Marjory’s Kidneys
Group 1: Age 88 what can she do?
Group 2: BP 170/90 what can you do?
Group 3: Dysuria and frequency what can you do?
Group 4: AMI What can the Cardiologist do?
Group 5: Heart Failure ramipril and eplerenone what can you do?
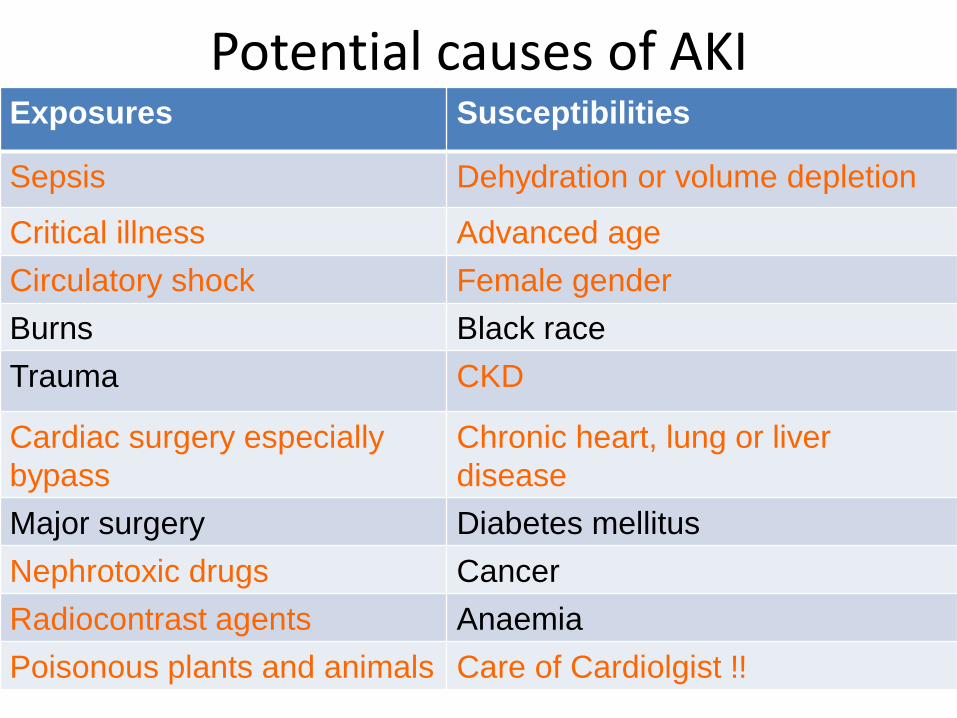
Potential causes of AKI Exposures Susceptibilities
Sepsis Dehydration or volume depletion
Critical illness Advanced age
Circulatory shock Female gender
Burns Black race
Trauma CKD
Cardiac surgery especially
bypass
Chronic heart, lung or liver
disease
Major surgery Diabetes mellitus
Nephrotoxic drugs Cancer
Radiocontrast agents Anaemia
Poisonous plants and animals Care of Cardiolgist !!

Thank you for looking after me!
AKI (NH6179) module
Ferdinand Bravo ([email protected])
Renal pathway – Module leader
Sussex Kidney Unit/University of Brighton

AKI (NH6179) module • 20 credit, level 6 (degree level) post graduate
nursing module.
• Part of renal pathway course.
• Can be taken as a stand alone module or part to complete
• Acute care in professional practice (BSc-hons) or Post graduate in acute care in professional practice.

AKI (NH6179) module
Pre-requisite:
• Applicable to health care professionals in
all areas of care with at least one year’s
experience in practice.

AKI (NH6179) module
Brief description of module content:
• This module will enable the student to
develop understanding of AKI disease
process and critically explore the
preventive and therapeutic management within the sphere of practice.

AKI (NH6179) module
Teaching and Assessment:
• Blended learning
• Case presentation/PBL
• OSCE – assessment of renal functions
• 2500 word case study on AKI management with focus on prevention.

Lunch
13.00 – 13.45

Group Work in your clinical perspective 13.45 - 14.55 Instructions We have set a series of questions for each of the 5 groups to answer. The questions can be found in your group. Your name badge has the number of your group on it to indicate which group you should go to. A facilitator will be in your group to guide you through the process and to ensure you prepare a 2 minute highlight presentation to feedback to the whole group. You will find templates and pens in your groups. You have 1 hour and 10 minutes allocated for this group work.
Group Work
• Group 1 – Facilitator Mike Jones
• Group 2 – Facilitator Peter Hewins
• Group 3 – Facilitator Claire Stocks
• Group 4 – Facilitator Elaine Whitby
• Group 5 – Facilitators Annie Taylor/Richard Hull
• Group 6 – Facilitator Kathryn Griffith

Group Work Questions Groups 1-4 Group 5 Group 6
What educational resources are
missing for our profession in respect
of AKI?
What educational resources are
missing for health and care
professionals in respect of AKI?
What educational resources are missing
for our profession in respect of AKI?
What is the best medium for
education in our profession? What
resources are required?
What is the best medium for
education about AKI across the
NHS?
What is the best medium for education in
our profession? What resources are
required?
Where do you think education is
most needed? Which groups should
we target for the most impact?
Where do you think education is
most needed? Which groups should
we target for the most impact?
Where do you think education is most
needed? Which groups should we target
for the most impact?
What are the main impediments to
training for our profession?
What are the main impediments to
training for improvement agents,
managers and others (non-
clinicians) in the NHS?
What are the main impediments to
training for our profession?
How can the AKI National
Programme help the professionals
in your locality?
How can the AKI National
Programme help you and your
professional colleagues learn about
AKI?
How can the AKI National Programme
help the professionals in your locality?
What material currently exists to help
GPs explain AKI and risk to patients, how
useful is it and what else is needed?
From the patient’s perspective what
information is needed and in what
format?

Feedback from Group Work
14.55 – 15.10
• 2 minutes feedback from each group

Using social media to reach a wide range of stakeholders
15.10 – 15.40
Amy Burton
Social Media Executive
Diabetes UK

Closing remarks and next steps
15.40 – 16.00
Mike Jones Acute Physician Royal College of Physicians

How to find out more
Karen Thomas Think Kidneys Programme Manager UK Renal Registry [email protected]
Teresa Wallace Think Kidneys Programme Coordinator UK Renal Registry [email protected]
28.11.2014 Acute Kidney Injury National Programme | Introducing the Think Kidneys campaign | Karen Thomas | 145
Contact Think Kidneys
Richard Fluck National Clinical Director for Renal NHS England [email protected] Joan Russell Head of Patient Safety NHS England [email protected] Ron Cullen Director UK Renal Registry [email protected]
www.linkedin.com/company/think-kidneys
www.twitter.com/ThinkKidneys
www.facebook.com/thinkkidneys
www.youtube.com/user/thinkkidneys
www.slideshare.net/ThinkKidneys
www.thinkkidneys.nhs.uk