uscap hep syphilis 2015
TRANSCRIPT
Dhanpat JainYale University School of Medicine, New
Haven, CT
Clinical history
59‐year‐old African American man CLL Pain in the right hand for 2‐3 weeks Persistent fever with chills and night sweats for 6 months Weight loss of 50‐Lbs
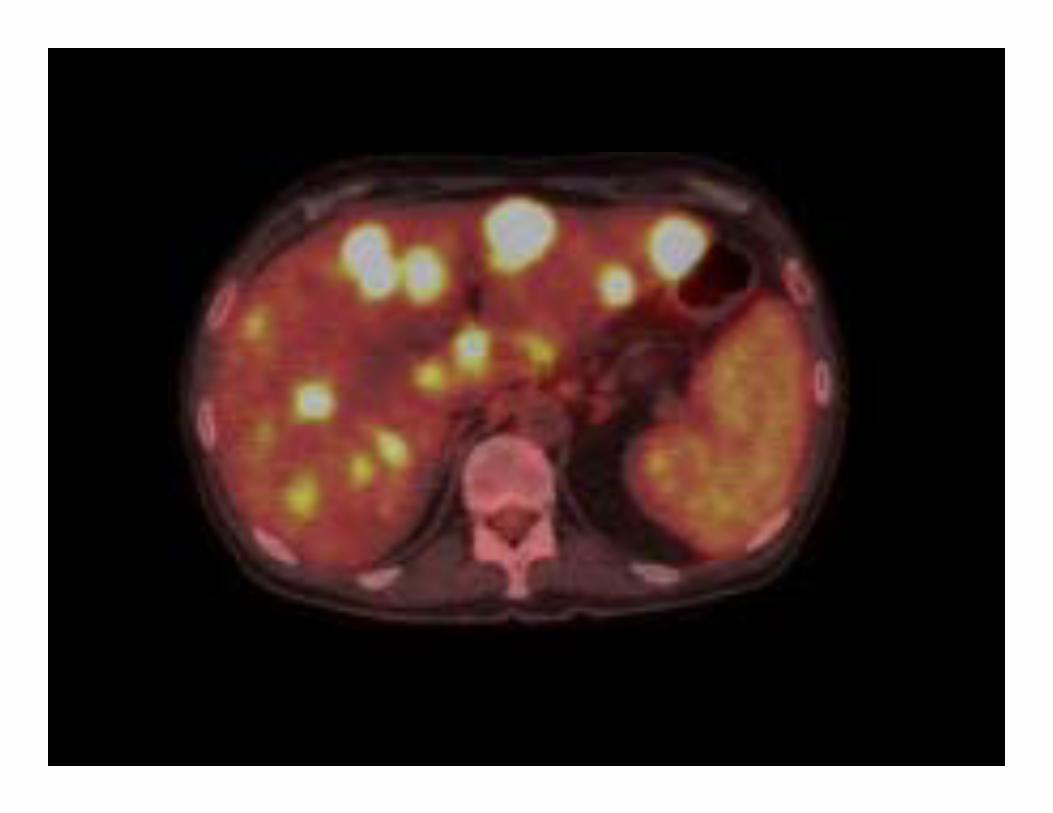
CT scan/MRI showed numerous mass lesions in the liver (seen better on PET scan
Labs show AST‐20u/L, ALT ‐20u/L, Alk phos112 u/L




Differential diagnosis
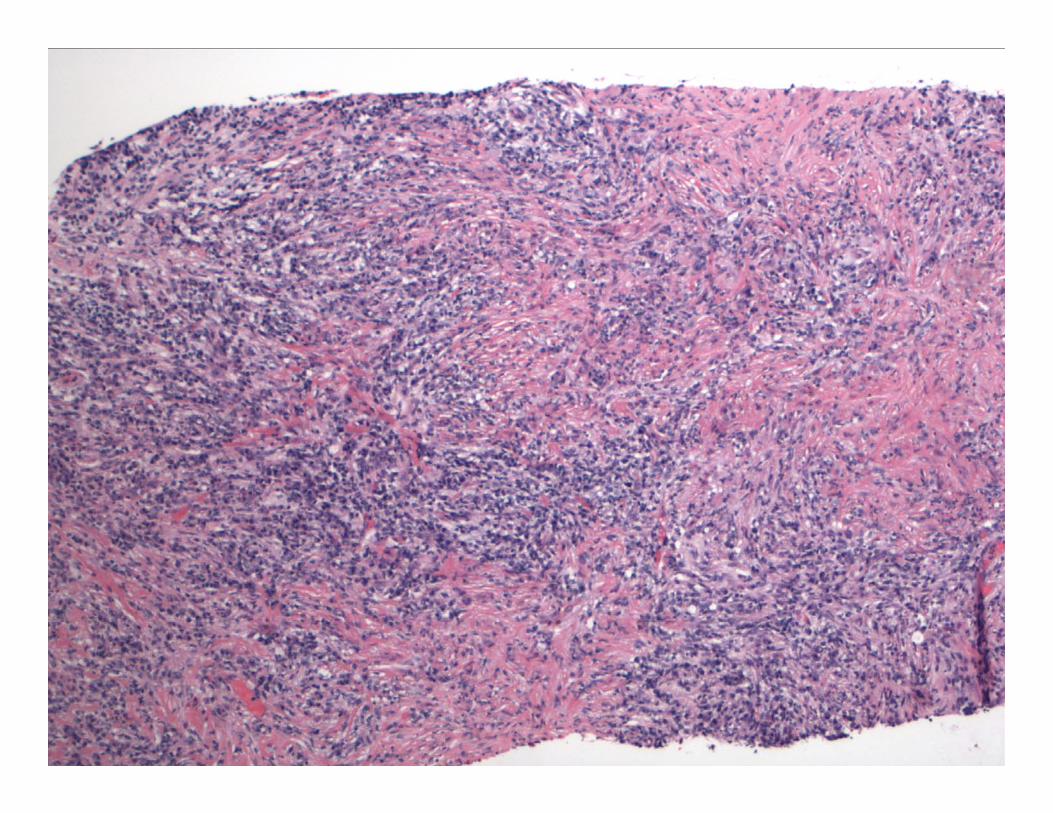
Spindle cell neoplasm with inflammatory cells Leiomyosarcoma GIST Inflammatory myofibroblastic tumor Angiomyolipoma
Spindle cell carcinoma Primary (HCC, CC, or mixed tumor) Metastatic

Differential diagnosis
Infectious etiology Bacterial abscess Fungal Syphilis
IgG4 associated liver disease Inflammatory pseudotumor
Inflammtory MyofibroblasticTumor: Plasma cell granuloma, inflammatory
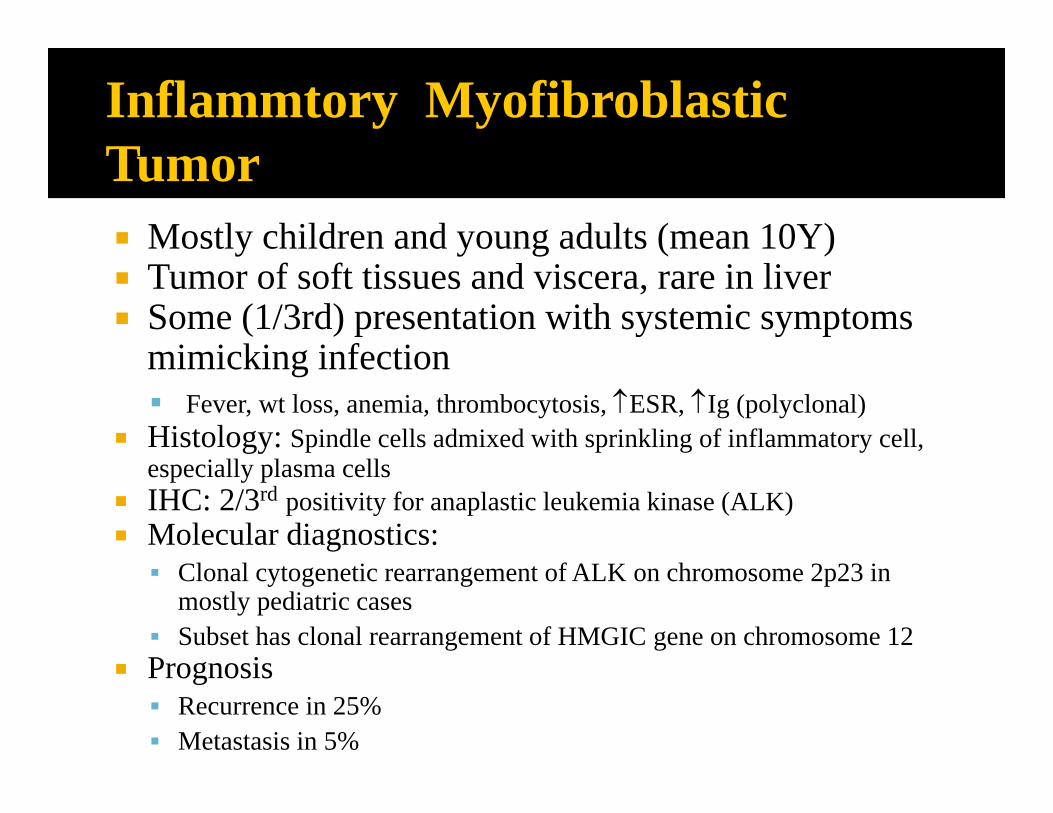
Mostly children and young adults (mean 10Y) Tumor of soft tissues and viscera, rare in liver Some (1/3rd) presentation with systemic symptoms
mimicking infection Fever, wt loss, anemia, thrombocytosis, ESR, Ig (polyclonal)
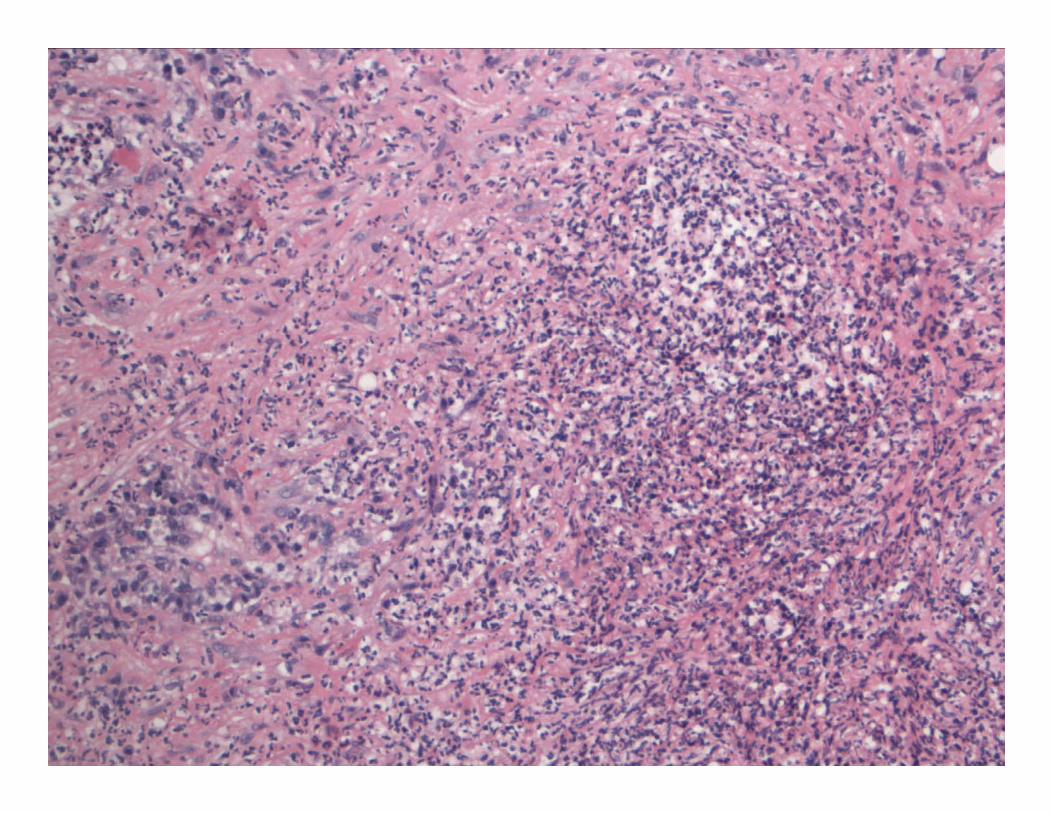
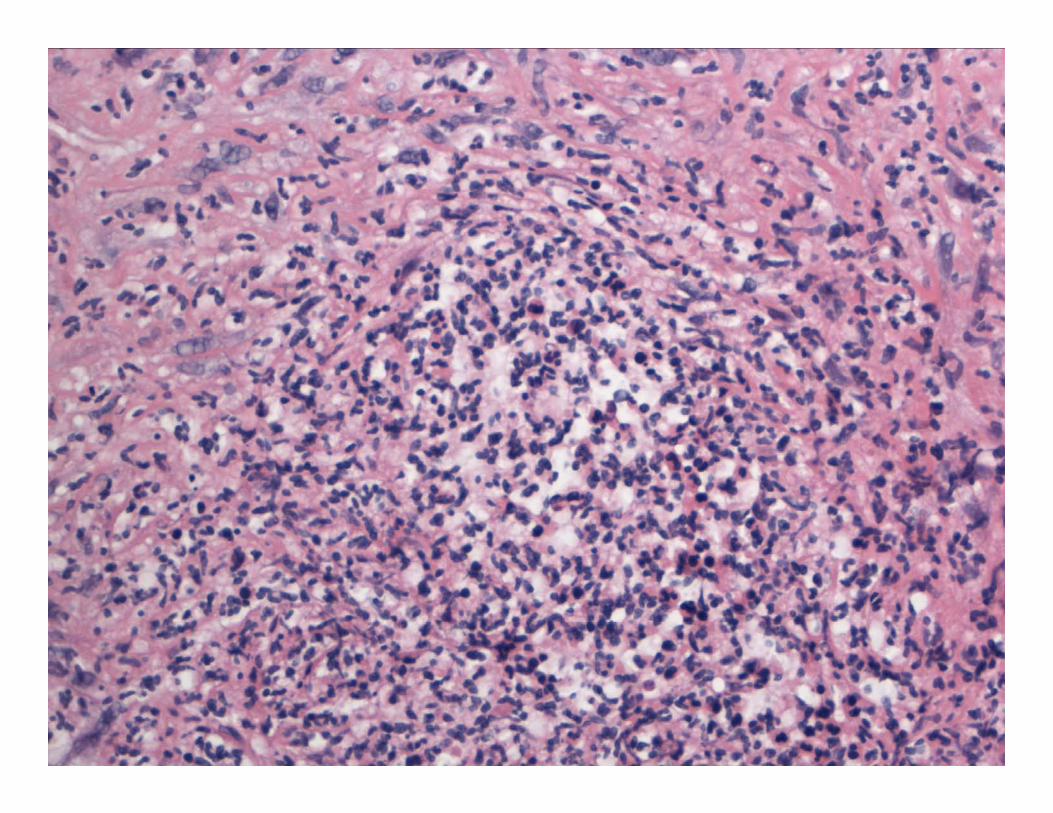
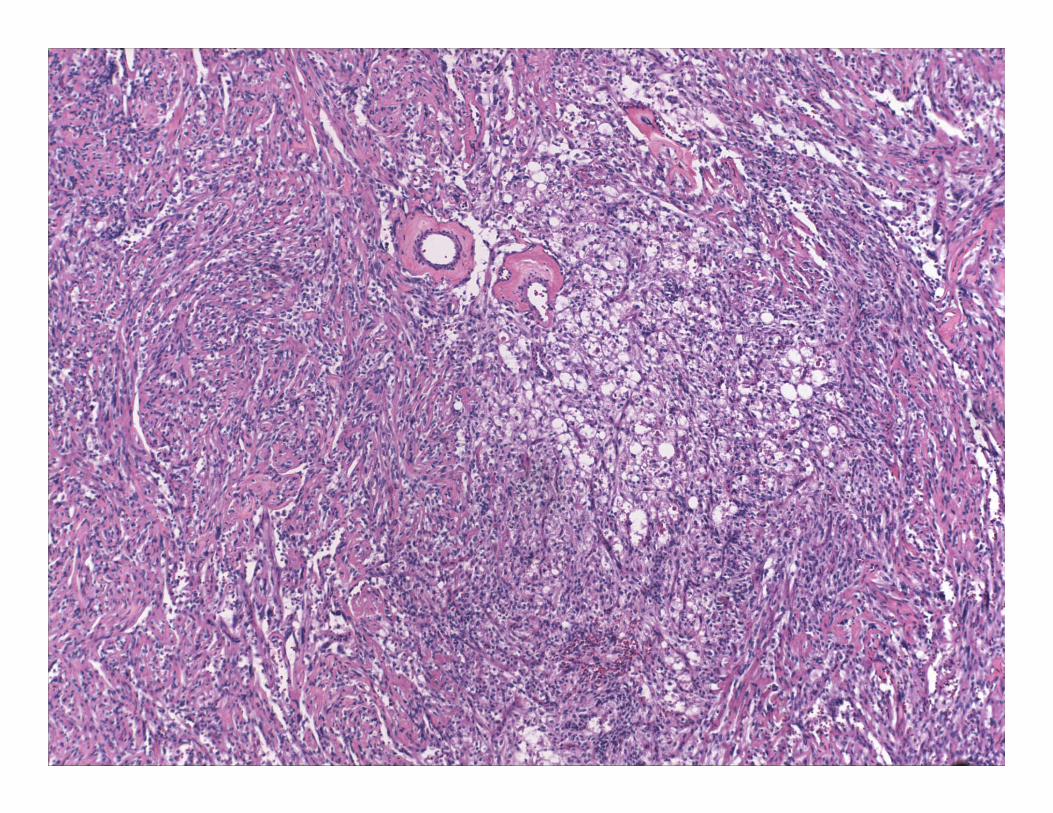
Histology: Spindle cells admixed with sprinkling of inflammatory cell, especially plasma cells
IHC: 2/3rd positivity for anaplastic leukemia kinase (ALK) Molecular diagnostics: Clonal cytogenetic rearrangement of ALK on chromosome 2p23 in
mostly pediatric cases Subset has clonal rearrangement of HMGIC gene on chromosome 12
Prognosis Recurrence in 25% Metastasis in 5%



HMB45
Differential diagnosis
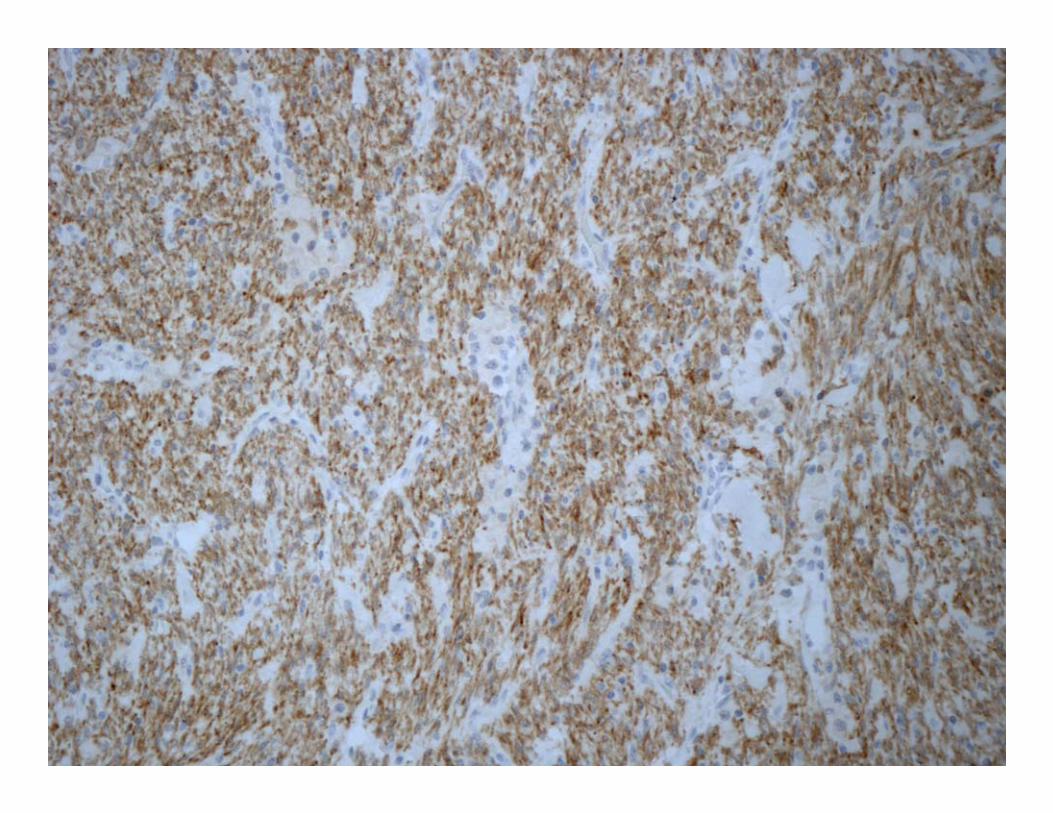
Spindle cell neoplasm with inflammatory cells SMA, desmin, ALK, DOG1, CD34, CD31, S100, HMB45, MelanA, Vimentin, CD68, Pan cytokeratin, EMA,
Not a good fit for most sarcomas and Spindle cell carcinoma
Infectious etiology Grocott, AFB, Warthin‐Starry, B&B, Fever and chills (6 months) but no localizing signs or no symptoms of infection
IgG4: Not done! Inflammatory pseudo‐tumor (“plasma cell granuloma”)
? Sampling error
Biopsy was repeated 2 more times Same findings and diagnosis About to be called Inflammatory Pseudo‐tumor for the 3rd time

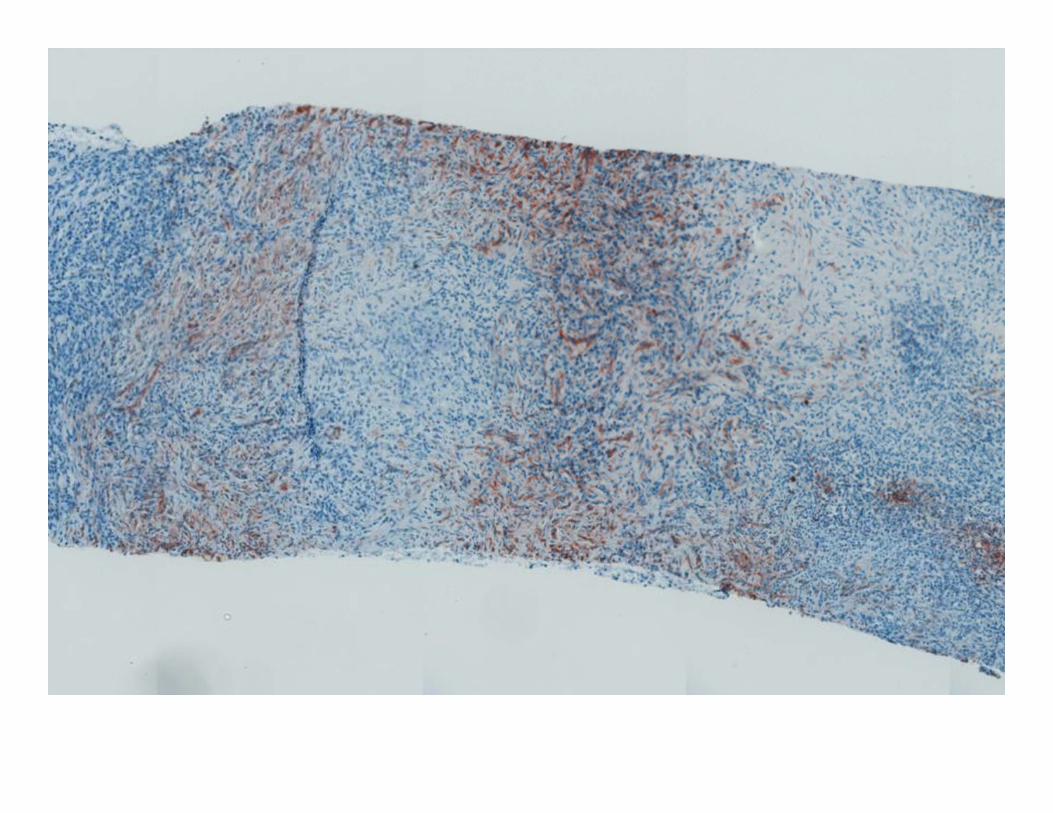
RPR test for Syphilis was positive Treponema IHC: Strongly positive on all 3 biopsies
Repeat Warthin‐Starry stains: Negative


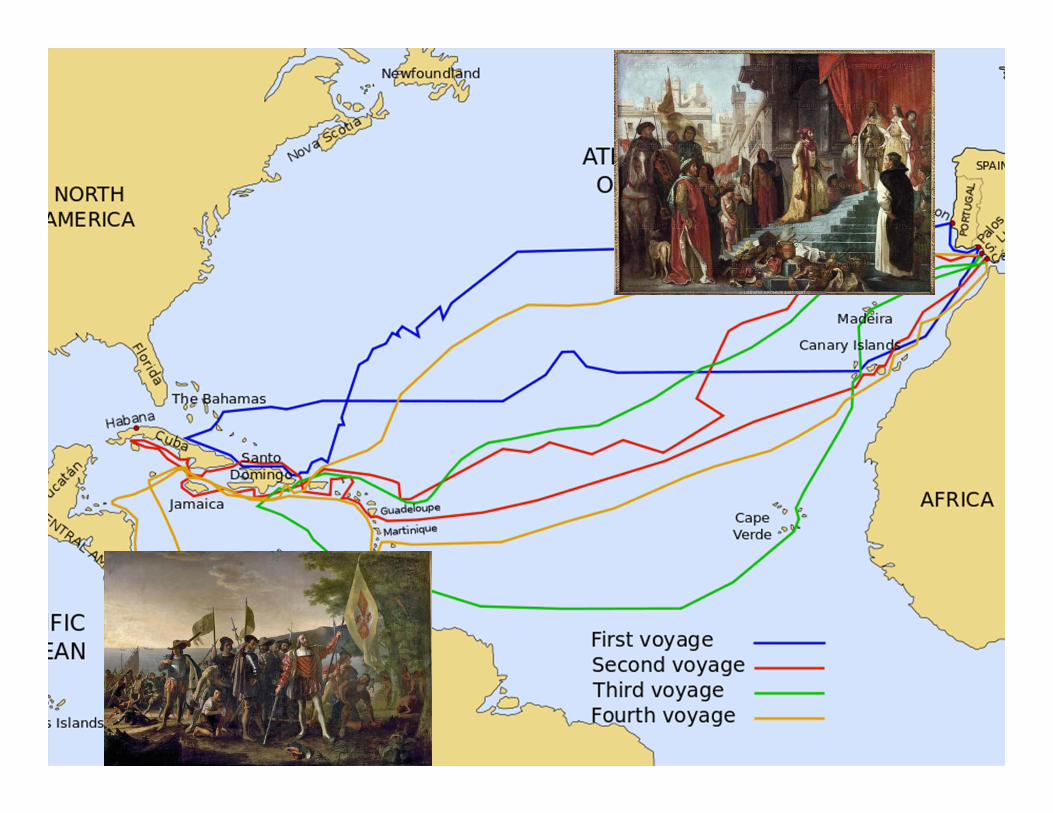
“In reality, it appears that venereal syphilis was theby-product of two different populations meeting andexchanging a pathogen. It was an adaptive event,the natural selection of a disease, independent ofmorality or blame.”Carol Clark. Anthropologist, Emory University, Dec 2011

Syphilis: Incidence and demographics
With HIV emergence: STD declined With control of HIV: STD increasing CDC: 56, 471 cases reported in MSM (75%) Younger individual (20‐29Y) Higher incidence in African Americans, Hispanics and other ethnic minorities Often asst. with HIV and high risk sexual behaviors

Natural history and clinical features Primary Syphilis: Ulcer at the site of inoculation Chancre
Secondary Syphilis: dissemination weeks to months after exposure Maculopapular rash on palms and soles Lymphadenopathy Systemic symptoms
Tertiary Syphilis Gummatous syphilis Cardiovascular and/or neurosyphilis
Syphilis: Lab diagnosis Serologic diagnosis: Non‐treponemal tests (RPR, VDRL, TRUST)▪ Cheaper, rapid, easily available and easy to perform▪ Titers useful for response to treatment
Treponemal tests (FTA‐ABS, MHA‐TP, TP‐PA)▪ Specific▪ Remain reactive even after treatment
Demonstration of organisms in tissues▪ Smears: Dark field illumination/ DFA‐TP▪ IHC: Monoclonal/polyclonal antibody ▪ Silver Stain: Warthin‐starry, Steiner, Dieterle▪ PCR based assays
Secondary syphilis: a histologic and immunohistochemicalevaluationMai P. Hoang, WhitneyA.High and Kyle H. Molberg. J Cutaneous pathology; 2004.
Skin biopsies 17 patients (19 biopsies) IHC (monoclonal Treponema antibody): 71% sensitivity
Silver Stain: 41% sensitivity


Hepatic Syphilis
Occurs during secondary or tertiary stage 6‐10% of untreated patients (30‐40% in HIV patients)
Transmission reported with infected transplanted solid organs
Disproportionate Alk Phos elevations Liver Bx: Often not required Non‐specific chronic hepatitis Plasma cell rich/Neutrophil rich/ histiocyte rich Peliosis

Treatment
Parenteral injection of Benzathine penicillin G is the treatment of choice
Modified treatment required for Patients allergic to penicillin Secondary/tertiary syphilis Immunosuppressed individuals

The great mimic
Any other questions??