v°’ume 霊鷲1二 - japanese nursing association critical discourse analysis of labor imnrd...
TRANSCRIPT

V°’ume霊鷲1二
OLt7i6ial Publication Of the
I,Il[
li
l・
l
i
;l・
l
[1
1111・
i
l
I
l
:l
/
International Journal of Childbimh '
Editors-in-Chief
Denis Walsh, PhD, RM
Division ofMidwijlery
U}iiversity ofNbttingham, tlK
Kerri D. Schuiling, PhD, NP-BC, CNM, IIACNM
School ofMrsiug Nbrthern Michigan Uhiversiip; USA
1
II
i
ll・
I,l
's-','
Ellen Annandale, BSc, MA, PhD
Maria Helena Bastose
Marie Berg, Phl]), MNSc, MPH,
RN, RMSusan Bewiey MA, MD, FRCOGSheena Byrom, RM, MA
Ng Cheung, PhD, MSc, RM, RGNKYllike Christensson
Hannah Dahlan, RN, RM,
BN(Hons),MCommN, PhD, EACMAnke De Jong, DM, PhD
Raymond De Viries, PhD
Declan Devane, PhD, MSc,
PgDip(Stats), BSc, DipHE,
RGN, RM, RNTNadine Edwards
DeputyEditor
Soo Downe, BA(Hons), RM, MSc, PhDSchool ofPublic Hizalth and Clinical Sciences
Uhiversity ofCentralLancashire, Cll(
Associate Editors
Duncan Fisher
Vivette GIove4 MA, PhD, DSc
Mechthild Gross, RM, RN, MSc
Gil1 Gyte, BSc, MPhi1
Eileen Hutton, RM, RN, PhD
Ken Johnson, PhD
Holly Kennedy
Patrick Laveryl MD
Nicky Leap, DMid, MSc, RM
HeloisaLessa
Lisa Kane Low] PhD, RN, CNM,
IIACNMAns Luyi)en, RM, PGDE, PDM, PhD
MargaretMaimbolwaJayne Marshall, Phl), MA, PGCEA,
ADM, RM, RGNEtsuko Matsuoko, PhD
Chris McCourt, BA, PhD
Marianne Mead, RM, PhD
Judith Merces BSN, MS, DNS
Mary Newburn, BSc, Hons, MSc
Sally Pairman
MallavarapuPrakasamma
Andrea Robertson
Verena Schrnidt, RM, BSc
Julia Seng, PhD, CNM, FAAN
Theresa Ann Sipe, CNM, MPH,
MN, PhDNick Tlaub
Jim Thornton
Octabio Vai gens
Saras Vedam
Kim Wlttts, PhD, PGCAR MSc,
RM, RN
international journal of Childbirth is published quarterly by Springer Publishing Compans LLC, New Ybric
Business Ctffice: All business correspondence, including subscriptions, renewals, and address changes, should be addressed to Springer
Publishing CompanM LLC, 11 West 42nd Street, 15th Fl,, New Ybrk, NY 1O036. www.springerpub,com
EditorialCltfice:Manuscriptsforpublicationshouldbesubmittedelectronicall)rusingEditorialManager:www.editorialrnartagencornlijcbirth
Subscription Rates lper feari: For institutions: Print & Online, $250, For indtviduals: Print & Online, $50. 0utside the Iinited States-for
institutions: Print & Online, $325. For individuals: Print & Online, $90.
Permission is granted by the copyright owner for libraries and others registered with the Copyright Clearance Center (CCC) to photocopyen.ar,tiMie.h,e,r;;'n,,fo,r,g・g・8,O,&e,2,E・:p.y,o.f,,th,e.ar,/;.cVe.・・a,7a.}e.ngs.s,h;gl,g.b.e,fe,?t.d,ir,:.ct.iy,2ofe,C,o.p,eeggt.C.i;ff,,fl,}c.e,,C.ee:ee.?,7.,C?.ng.r,e,sgifarfixg,
Rf,.COell,,"k,SSSI,l.a,9,8,O.P.l?:Y::irthg,e,"eAalfo,di.St,/'.b."ti,figl,i%dbV2rt,ifill'lg,ggdPl.OgSl,ti.・O,",ftls.urbp,fi:・xsk`6e,al:}l}fl,{;lelr,c.o.llectiveworks・orforresale・
postmaster: send address changes to intern61ional journtil ofChildbirthlSpringer Publishing Cornpanl; LLC,
11 West 42nd Street, New Ybrk, N'Y 1O036,
Copyright @ 201 1 Springer Publishing Compairy; LLC, New Ybrk. ISSN2156-5287
/ ,,..,k,L--,Sinbet ''''

rl・ /tt
'1]li'' i"
'
' ew.ili・l・・il・ silil, ii ・ ・l・ 'tt't't l'i'' "'tm' .s
1,, {,,
ee
'i
,.'S,l
fit
lat
'
{i'i'i
I',//・iliil,1・i!1 ..ew" '/;t '
International Journal of Childbirth
Vblume 1, Numbcr 1, 2011
,
hkr
i/1
1
i/
EDITORIALInternational Journal of Childbirth
Denis Wblsh, Klerri Schitiling and Soo Dorvne
2
ARTICLESCompetence and Competency: Core Concepts for International Midwifery Practice
Judith T Fullerton, AtfGhe'rissi, Peter G, Johnson, and fo7ce B. Thonipson
Becoming a Mother: Wbmen's Journe〉,s From Expectation to Experience in Three European Countries
Ans G, Luyben, Sue R. Kinn, and Vinterie E M, Fleming
General Practitioner Involvement in Remote and Rural Maternity Care:
[Ibo Big a Challenge?
lan Caldoiil Vbnora J-lundteJc Edwin van 7bijlingen, Jbhn Reid; Alice Kige4
lanet lltcken Jilly J}'elan`L Fiona Harris. Jane Fbrmen and Helen Bi;yers
Expanding Postpartttm IIcmorrhage Prevention to the Community in
Resource-Poor Contexts: Critical Considerations and Next Steps
S),dnay A. Spaizgiei; Alissa I〈bski, Deborah Armbrusten and Clynthia Stanton
Struggling to Get Into the 1'oel Room? A Critical Discourse Analysis of Labor IMnrd
Midwives' Experiences of Water Birth
Kitn Rttssell
4
13
27
39
52
COMMENTARYThe Necessity and Challenge of International )vlidwifery Science
Raymond G, De V}'ies, Marianne Nieuwenhuijze, Rcijbei van Crinipen,
and the members of the Mid,vijlery Science Wbrkgro up
61
'
)・l
:h.
x
)ixeeNal.44,,.Z.:
23, 4,
sS〉 asEgexs06wh%

/
1
/
l
:
1/
/
!
/
lt
!
!'
:r,,,!um ,:r. wa
..
ww
IiL/rEiiS・t;iiwwl
International Journal of Childbirth
The launch of a new childbirth journal is a cause for cel-
abration. It provides an opportunity for researchers, service
users, dnicians, and materniLy service staLreholders to get
their messages out quickLy and more efectively at a time
when maternity provision worldwicLe is changing rapidl}L
In this editorial, wc flag up what we believe are the more
significant influenccs and challeTiges that face us all over the
coming decade; but thirst-why a tiew childbirth journal?
There are currcntly too few childbirth journals that
could be truly described as multidisciplinar}L i clusive of
the developing world perspective, and holistic in scope
regarding all aspects of childbirth. rvIost journals target a
particular audiellce, demographic or professional group,
and this results in `'silo'] thinking with limited cross fertil-
ization ofideas, dissemination ofbest practice, or research,
For example, midwives mav read obstetric journals and
obstetricians may rarely read midwi fery journals. Sociolo-
gists do not often publish in midwifery or obstetric titles,
and service users only occasionally submit to professional
journals. Therefore, an ongoing dialogue in the literature
is ahsent, and when conLrovcrsy docs "breakoue' in major
journals, the debatc is frcqucntly polarized; look no fur-
ther than the heated exchangcs of home birth research,
recently (de Jonge et aL, 2009; Wiix ct al., 201O).
The internationat fournal of Childbirth wM pro-
vide an opportunity for all voiccs and all perspectives to
be heard, The jour'nal's niissien is to:
. Disseminate original research, theoretical insights,
and accounts ofpracticc-based innovations and
organization ofcare
. Provide a fbrum for exploration, debate, and critique
in childbirth research, education, and practice
- Promote multicultural and interdisciplinary perspec-
tives in the examination ofchildbirth experience and
knowledge. Actively promote research, education, and practice
activity in neglccted arcas such as normal birth,
measurement ofwell-being as opposed to pathology;
indigenous childbirth practices and culture, and the
public health consequcnccs of childbirth
. Disseminate original case studies ofnor[nal, although
unusual births, with a significant reflective component
This journal is needed more than ever no"4 because
maternity carc continues to undergo radical change across
theworldinrcsponsctoseveralimperativesandinfiuences.
The high levels ofmaternal and perinatal mortality in thc
developingworldarcunacceptable,particularlywhensolu-
tions exist that would rcduce the rate substantiallM How-
eve4 even within Lhese known shared solutions, there is
tension over whether to address the causes (trade injustice,
povert〉s and the unequai distribution of resources) or treatthe symptoms through technolog}l drugs, and provision of
skillecl attendarits, Which ofthese should take priorit〉s andis a twinned approach realistic and achievable?
This debate reflects another worldwide tension
around how matcrnity services should evolve-should a
social or biomedical model take the lead? In many parts
of the world, the biomedical model dominates and, wherc
it does, esca]ating intervention rates are observed. The
caesarcan epidemic is but one example, Howevec in other
parts of the world, home birth and midwifery led carc
characterizes large sections ofprovision, with a generally
encouraging safeLy and ethcacy record (Hatem, Sandall,
Devane, Soltani, & Gates, 2008). Can the two approaches
coexist with mutual understanding and respect?
There continues to be a debate concerning child-
bearing womenis autonomy choice, and agency, which are
played out within the biomedical and social model, with
voices articulating access to universal elective epidural
proyision and birth centrelhome binh options within these
respective modcls. This debate reverses in sub-Saharan
Mica where homc birth with traditional binh attendants
is blamed for high perinatal mortalit)l and where hospital
provision of epidui'aJ services is patclry at best. In recent
months, anothcr layer of complexity is revealed in initia-
tives, to address obstetric violence in Vlenezuela, where Ieg-
islation has been enacted to make nonconsensual obstetric
procedures illegal (D'Gregorio, 2010), and in the United
States, where inhumane treatment of laboring women is
once again a ncws item (Goeg 201O).
""tl', C:"t-"
-. -i, di5'?xi"・
et -,t-"t-t
iN71ERNATiONAL JOURNAL OF CHtLDBtRTH Vblwme 1, lssue 1, 201 1@ 2011 Springer Publlsh[ng Company, LLC v(Lnv,springerpub,comDOiltO,t89112156-5287.IA.2
L

ee
Editorial 3
1
1
,
The discourse around risk is having a major impact
in many western maternity care systems, and results in
defensivc practice and institutional se] flprotection, Elabo-
rate policies and mechanisms, in an efibrt to shift blame to
women or individLiaL practitioners and away from system
fal1ures, are eviden[e of a system that is in need of change
(MacKenzie Bryers & van 1'eljLingen, 2010). Sociologists
have warncd health services of the dangers of this dis-
course driving change, but litigious, adversarial models of
compensation dominate, currently (Carter, 2010).
Accompanying the aforcmentioncd tensions and
making them werse is the economic argument that is
raging over the affordabilibr and eguity of provision of
carewithinandbctweencountries,Mostnationalmodels
of maternity care have a mixed ecenomy of public and
private provision. Perverse incentives can operate in pri-
vate models that reward intervention and overtreatment.
For example, a recent study has demonstrated the high
financial cost of routine intervention in normal child-
birth in the U.S. system (Conrad, Mackie, & Mehrotra,
2010). Rising use of pharmacology and technology fbr
childbirth in pub]icly funded s〉'stems suggests that soci-cty is willing to expcnd resources in this area, evcn when
the public purse is under intense prcssure. This raises
interesting sociological and organizational questions
that can best be explored by cross-discipiinary investiga-
tion. Givcn this milieu, a journal that publishes papers
acress thc spectrum ofthese challenges and opportuni-
ties is welcome. "le are honored to bc supported by the
International Confederation of Midwives, which has
glebal reach with mere than 80 mernbcr societics,
As editors, we want to encourage the submission
ofpapers related to childbirth from all over thc world
and from many ditl'crent stakcholders.
REFERENCES
Carter, S. (2010). Beyond control: Body and selfin women's
chi]dbearing narratives. Sociology of Health th Illness,
32(7),993-1009.
Conrad, R, Mackie, T,, & Mehrotra, A. (2010). Estimating
the costs of medicalizat'ion. Social Science c}・ Medicine,
70(12),1943-194Z
de Jonge, A,, van der Goes, B., Ravelli, A., Amelink-Vbr-
burg, M., Mol, B., Nijhuis, J,, ... Buitendijk, S. (2009).
Petinatal mortality and morbidity in a nationwide
cohort of 529,688 Iow-risk planned home and hospital
births, BJOG: An Internatiotial Journal of Obstetrics th
(lynaecolQgy, 116(9), lt77-1184. doi:10.1111/j.1471-
05282009.0217S,x
D'Gregorio, R, (201e), Obstetric violence: A new tegal term
introducedinVenezucla[SpecialEditorial].I}tternational
lottrnal of Clynecology and Obstetrics, ll l, 2e l -202.
Goer, II. (2010), Cruelty in maternity warcls: Fifty years later,
k)urnal oj'Ilerinatal Education, I9(3), 33-42.
Hatem,M.,Sandall,J,,Devane,D,,Soltani,H,,&Gates,S,(2008).
Midwife-led versus other models of care Sbr childbear-
ing women. Cochranc Database of Systematic Reviews,
lssue 4. Art No.: Cl)O04667. doi:10,le02/14651858.
CDO04667,pub2
MacKenzieBryers,H.,&vanTleijlingen,E(2010).Ilisk,theor"
social and medical models: A critical analysis of the
concept c)f risk in maternity care, Midivij'erp,, 26(5),
488-496.
Wax, J. R., Lucas, E L., Lamont, M., 1'inette, M. G., Cartin,
A., & Blackstone, J. (2010), Maternal and newborn
outcomes in plannecl home birth vs planned hospital
births: A meta-analysis. American Journal ofObstetrics
c}" (lynaecotogy, 203(3), e1-e8.
Denis Walsh, Co-Editor-in-Chief
KerriSchuiling,Co-Editer-in-Chief
Soo Downe, Deputy Editor
1

t)i
l
l
/
l・l,, ,
}tt・]I,'il'iii,i{,ga
iGii@{.gllwwsw.l,ttilk,11iiiill・ilme,・・;・,,i,,.,Illime
":i[i[1
Competence and Competency: Core Conceptsfor International Midwifery Practice
fttdith T thdlerton, AifGhtirissL Peter G. Jbhnson, andfoyce B. [IIP!ompson
'
・li
The global health community has imptemented several initiatives over thc past in the intercst of accel-
erating country-by-countrv progrcss toward the MMennium Deyelopment Geal ef improving maternal
health. Ski11ed attendance at every birth has been recognized as an essential componcnt ofapproaches
for reducing maternal and perinataL morbidity and mortality
Midwives have been acknowlcdged as a preferred cadre of skilled birth attcndant. The lnterna-
tional Confederation ofMidvvives (rCM) speaks for the global community of ftdly qualificd (profes-
sional) midwives, The ICM document entitled Essential Cotnpetenciesfor Basic iXc[idvvijbry Practice is a
core policy statement that defincs the domains and scope of practice for those individuals who meet the
international definition ofmidwife. This article explores the meaning of competencc and competency
as core concepts for the midwifery profession. An understanding of the meaning of these terms can
help midwives speaking individua]ly at the clinical practi[e level and midwifery associations speaking
at the policy level to articulate more clearly the distinction of fu11y qualified midwives within the skMed
birth attendant and sexual and reproductive health workfbrce, Competence and competcncy are funda-
mental to the domains of midwifery education, legislation, and regulation, and to Lhe deployment and
retentionofprofessionalmidwives.
KEYWORDS: professional midwifery; competence; essential competencies; sl(illed attendance
1
INTRODUCTION
The inauguration of the Safe Motherhood Initiative
in the mid-1980s focused the attention of the global
health communibr on the reproductive・and human
rights of women, infants, and families, The Millennium
Development Goals (MDGs) were an ambitious agenda
for improvement in global hea]th concerns that were
adopted by 192 United Nations (UN) member states and
many internationat organizations in 2000 (UN, 2000).
MDGs 4 (reduce child mortality) and 5 (improve rnater-
nal health) emerged as an cxpression of the concerns of
world citizens and governmcnts about the tragedy of
maternal, newborn, and infant death.
A clear consensus has emerged among thoseresponsible fbr tracking movcment toward estab-
lished MDG targets, and that is, that providing skilled
attendance at every birth is an essential component
s"-1/tS"ltJ
i, d2tCSNi・S.
:t -,'s-','-'
of approachcs for reducing maternal and perinata]
morbidity and mortalit}1 and promoting reproductive
health. The availability ofa health provider with specific
midwifery ski11s and competencies, particularly the
lifesaving functions of basic emergency obstetric and
neonatal care (i.e., the skiiled attendant), working within
a supportiye and enabling environment (i.e,, ski11ed
attendance), is acknowledged to be a key componcnt
of any safe motherhood strategy (Bullough et al., 2005;
Carlough & McCall, 2005; Hoimeyr et al., 2009; Lec
etal.,2009).Incrcasingtheproportionofbirthsattended
by ski1led personncl is one ofthe targets established fbr
tracking progress toward achievement of MDG 5.
The globai health community has implementcdseyeral initiatives 6ver the past decade to bring skilled
attendants to the community in the interest of acceler-
ating country-by-country progress toward improving
maternal health (MDG 5) and the target ofreducing the
INTERNATtONAL JOURNAL OF CHiLDBiRra Vblume 1, issue 1, 201 1@ 2011 Springer Publishlng Cornpany, LLC wLnv,springerpub.comDO[110,189112156-5287.1.1.4
t
'(
I

r. ;/tt
xli'
t"/
Il
1
ge
Cvmpetence and Competency/ Core Concepts for [nternationnl Midwlfery Pract]ce Fulferton etal. 5
maternal mortality ratio by 75% by 2015, Many of these
effbrts, particularly in lower resource countries, have
included the education of new cadres of personnel who
are preparcd with a very narrow and limited dotnain of
practicc, tbcused primarily on the knowledge and ski11s
surrounding childbirth and the irnmediate neonatal and
postpartum period. The title of "comrnunity midwife" is
commonly assigned to these birth providers. [,awn et al.
(201O) report that there is some limited, but Iesser qual-
ibr evidence that these providers are effective in reduc-
ing perinatal and neonatal mortality.
The International Confederation of Midwives
(IC)vl) speaks fbr the global community of fully qualified
(professional)midwives,apreferredcadreofskilledbirth
attendants. The role ofthe ICM is to define the concept of
professional midwifery and to work collaborativety with
other global organizations at country levels to promote
and to strengthen thc voice of professional midwifery in
policy and practice arenas. The ICM has promulgated an
international definition ofthe midwife since 1972, with
endorsement by the World Health Organization (WHO)
and the International l`ederation of Obstetricians and
Gynecologists. The most recent revision was in 2005
(ICM, 2005). The ICM has set forth additionaL policy
and practice statements in the ensuing decades that can
assist ICM member associattons to translate the core
beliefs set forth in these documents into regulatory and
worldi]rce policy at Lheir country level.
The ICM document entitled Essential Competen-
cies for Basic Midivijbry Practice (a.k.a. Essential Com-
petencies) (Fullerton, Scverino, Brogan, & Thompson,
2003; ICM, 2002) is (}ne of these core policy state-
ments. The Essential Competencies document defines
the domains and scope of midwifery practicc. The ICM
expects that the Essential Competencies document wil1
be adopted or expanded at the country level to promote
the development of professional midwifery within the
country. 'Uhe ICM published the first set of Essential
Competencies in 2002. A second version, updated to
reflect the emerging state of evidence-based practice
(Fullerton & Thompson, 2005), was approved by the
ICM Board in December, 2010,
The purpose of this article is to review the context
within which the concepts of competence and compe-
tency emerged, to explore the meaning of competency
as a core concept for the midwifery profession, and to
place this gcneral discussion within the specific context
ofprofessional midwifery practice. An understanding of
the meaning of competency can hclp midwives sp eaking
individualLy at the clinical practice level and midwifery
associations speaking at the policy level to articulate
more clearly the distinction of fu11y qualified midwives
within the ski11ed birth attendant and sexual and repro-
ductive health workforce. Competency is fundamental
to the domains of midwifery education, legislation, and
regulation, and to the deployment and retention of all
providers of repro ductive health services,
THE EMERGENCE OF THE CONCEPTS OFCOMPETENCE AND COMPETENCY
De Ketclc (2000) asscrts that the concepts ofcompetence
and competency emerged in thc late 20th century when
economic globalizati'on stirnulated increased competi-
tiveness in the international marketplace. He describes a
growing censciousness among employers that there was
a perceivable association betsveen higher levels of edu-
catlonal attainment of the workforce and the ability to
adapt or conform to job perfbrmance requiremcnts. De
Ketele therefbre described the concept of competency
as one ofseveral successive milestones and an advanced
step on the pathwa}r ef knowledge acquisition.
Employers, motivated by the requiremcnts of
competitiveness and profitabilitM and in search of the
most efficient ways to mobilize a werkfbrce, began to
create their own training units. The aim was to enable
newly hired employccs to learn the job-related tasks, to
perform them with a quality close to "zero defect;' and
further, to be able to identify solutions to problems that
arose during the perforrnance of their job functions. Ib
that end, it was neccssary to craft a precise dclineation
of the activities (tasks) that were associated with any
specific job title, and to identify the associated knowl-
edge and skills (the competencies) that would have to be
acquired to enable satisfactory task performance.
Z/aining units wcre attuned to the need for an inter-
vention that began from the bottom up, The employment
sector worked cooperatively with the education sector
to develop a vocational training system that offered
the opportunity fbr learners to prepare themselves for
emplo〉rment through acquisition ofsmaller units ofskillsets that were both progressive and cumulative. Prereg-
uisite kiiowledge and skills were defined for entry into a
learning unit, The competencies that were to be mastered
as evidence of successfu1 complction of the unit and the
means by which succcssfu1 mastery of the ski11 would be
measured were simi]arly defined.
These initiatives modeled in the vocational and
occupational employment arenas were noted by those
invoLved in professional education (ihcluding health pro-
fessions). Professional task competencies werc identified.

11
i
as
-
6 Competence and Competency: Core Concepts for lnternationai Midwifery Practice Fullerton et al.
Crosscutting arid general competencies (e.g., communi-
cationanddecision-makingski11s)thatwouldberequired
across all domains ofprofessional performance were also
acknowledged. The field of professional competency
assessment began to evolve.
viewed as an integrative concept because it considers,
at the same time, the relevant intellectual content, the
activities to be conducted at a specified level of perfor-
mance, and the situations in which those activities are to
be performed (Roegiers & De Ketele, 2000).
THE CORE CONSTRUCTS OF COMPETENCEAND COMPETENCY
An understanding of the meaning of competency first
requires that a distinction be made between the terms
cormpetence and competency. Both terms are multilay-
ered and distinct. Howeve4 simply stated, mairy theo-
rists define competence in relationship to behavioral
tasks, and competency in relationship to the personal
characteristics that underpin the performa,nce of those
tasks (Wbodruffe, 1993).
The literature presents three common approaches
to the description and measurement of competence,
although none of them is precisely distinct from the
other, and none actually crafts a clear distinction
between competence and competency The debate is
summarized by McMuilan et aL (2003) as follows. The
hehavioral lpecformance) approach defines competence
through a description of actions that can be demon-
strated or observed and assessed. In this approach,
successfu1 performance is only possible when the neces-
sary and underlying knowledge and understanding are
present The generic a2proach defines competence as
broad clusters of abilities, such as knowledge or capacity
for critical thinking, that act together to promote expert
performance. This approach ignores the context, assum-
ing that these abilities will serve as well in various cir-
cumstances. The holistic approach combines the general
underlyingattributesofthepractitionerwiththecontext
in which they are applied, and allows the incorporation
of ethics and values as elements in competent perfor-
mance. The Dreyfus model of sldl1 acquisition (Dreyfus
& Dreyfus, 1980), articulated by Benner (1984) in the
context of nursing practice, actually incorporates ele-
ments of each of these three approaches in her descrip-
tion ofcompetence, portraying them as a developmental
sequence in the progression from novice to expert.
CompetencM in its turn, has been variously
described as a multidimensional construct that irrvolves
a complex interaction of cognitive activities related to
the gathering of information, the processing of that
information for translation into action, described as
know-acting (Lasnie4 2000; Le BoterC 2000), orproblem
solvitzg; and followed by enactment. Competency is
COMPETENCE IN THE ACADEMIC ANDCLINICAL CONTEXT OF MtDWIFERYEDUC,orION AND PRACTICE
The qualitative research methodology ofconcept analy-
sis has been used to explore the concept of competence
as it relates to nursing and midwifery education and
clinical practice (AxleM 2008; Chiarella, Thoms, Lau, &
Mclnnes, 2008; Cowan, Norman, & Coopamah, 2007;
Scott-Tillex 2008; Valloze, 2009), These reports con-
firm, at minirnum, a consensus that there is no single,
universally accepted definition of competence. In fact,
the concept itself continues to evolve in pace with
advances in science and technology which challenge
us to keep pace with emerging knowledge and new
evidence-based clinical practices.
Therefbre, various definitions haye been devel-
oped fbr use in a relevant application. The ICM has cho-
sen the holistic definitional approach and has defined
competence in the context of midwifery education and
practice as the combination qfknowlecige, psychomoton
communication, and decision-makiug skills that enable
an individual to pettbrm a specijlc task to a dE}flned level
ofprqflciency (ICM, personal communication, 2010).
MIDWIFERY COMPETENCY
Moving forward in the delineation of these constructs,
an important next step is consideration of the situational
context of professional practice within which compe-
tence is demonstrated (the integrative understanding of
the concept). The definition of midwijler:y competency
emerges as a comhination of knowlecige, projlessional
behavion and specij}c skills that are demonstrated at a
dElflned level ofprqficiency in the context qf midwijlerly
education and practice. Definitions of the fundamental
components of these definitions of competence and
midwifery competency are presented in Figure 1.
Tlie 2002 version of the ICM's Essential Competencies
document delmeates one crosscutting and five practice-
specfic demains ofmidwifery competenc)c The document
detals the knowledge, skills, and behaviors that comprise
the essence of each domain. (A seventh competency
"'t''tt''t"fo"t/i't' '' ttt t ..t.

Competence and Competcncyt Core C/oncepts for ]nternatlonnb Midwifery Practice Eui/erton et aL 7
1
J
Abil"y: The quality of bein gable to perform; a nat"ral or acquircd skill or tn]ent
Attitvde: A person's views (values and beliefs) about a thing, proccss, or anoTher person that often lead to positlve Dr negative reaction.
Behavlor: A person's way of relating or responding to the actions of others or to an environmentaj stimulus.
Compctcnce; The cornbinatjon of knowlcdge, psychomotoq camtnunication, and decision-makins ski[ls that enable an individua]
to perform a spec]fic task to a def]ned leve] of proficienc},.
Compctcncy (midwlfery): A combination of knowledge, professional behnvioq and specific ski]ls that are demonstrated nt a
defined level of proficiency im the context of midwifery education and practice,
Knowledge: A fund of 1nformation that enables an individual to have confident understanding of a subject with the ability to use it
foraspecificpurpose.
t
I
Skill: Abi[ity [earnnd through education and training or acquirad by experience to perform specific actions or tasks to a specified
]evel of measurab[e performancu,
fask: A specific component of a larger body of work.
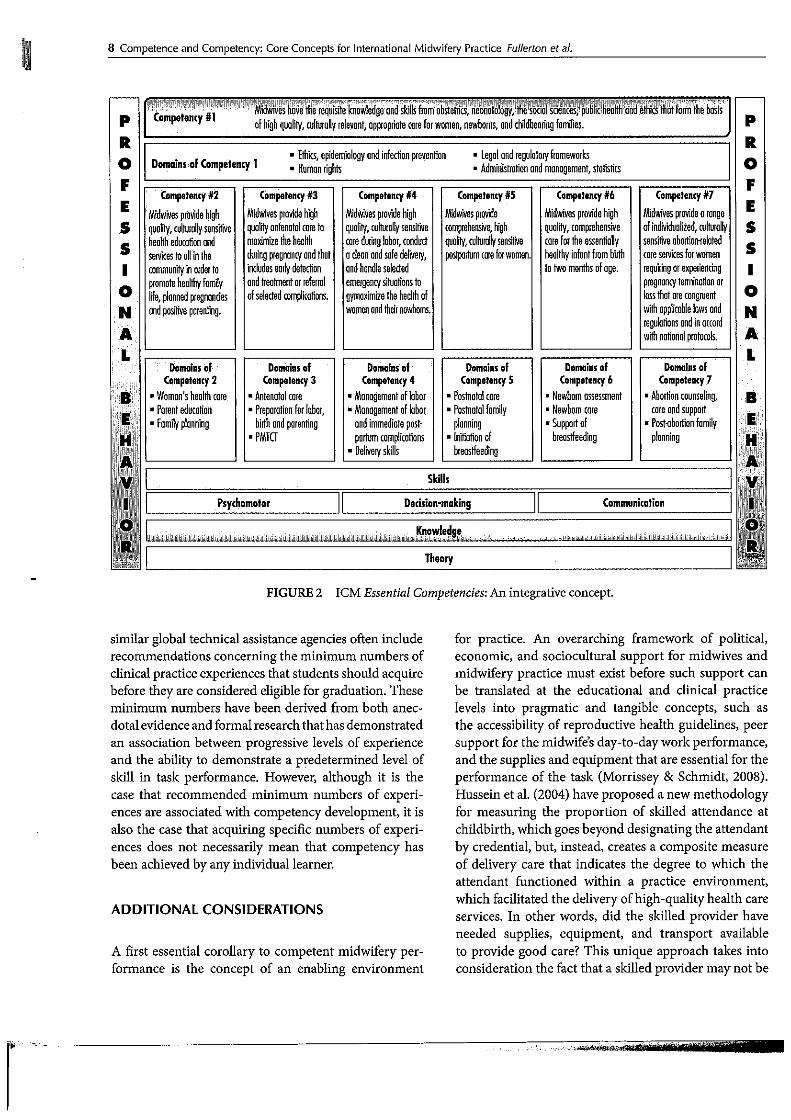
FIGURE 1 ICM clefinitions,
/
domain related to abortion-related care services was added
to the Essentinl Conrpetencies approved by the ICM Board in
Decembc4 2010). Figure 2 presents a pictorial dcpiction of
the ICM's integrative definition. Theory from the biological
and soctal sciences underpins the acquisition of ktiowledge,
which then enables acquisition of ski11s in the psychomotor
and affectise domains. Thc crosscuttjng content of com-
petency clomain 1 overarches the scope ofclmical practice
(competency domains 2 through 6). Professional behavior
infuses throughout and is essential to the essencc of mid-
Lviferycompetency
Midwifery cducation programs use the kiiowledge
and expected prot'essional behavior statements cited in
the ICM document as an external reference criterion.
Similarl" the ICM Essential Competencies document sets
forth thc various clinical skills that would be expected of
a graduate at the time of entry into practice as a profes-
sional midwife. The depth and breadth of the content of
an education program's curriculum of midwifery studies
can be compared to the expected content as delineated
in the ICM doc"ment (a curriculum development and
review method also known as "curriculum mapping").
The specific clinical skiIIs and the associated
knowledge staternents are designated as basic or addi-
tional, A basic dcsignation indicates that the knowledge
or ski11 should be considered to be common to all mid-
wives, Any item of 1〈nowledge or ski11 designated to beadditional can bc included within a curriculum because
of relevance te a country's burden of disease, or it can
be considered to be optional for midwives who wish or
need to acquire it. For example, midwifery cducation
programs located in high-resource countries may con-
sider thc ski11s of colposcop〉r or ultrasonography to be
clinical preventive services that all graduates should be
prepared to offer. Similarl" education programs located
in low-resource settings may find that including certain
ski11s within the basic program of studies (e.g,, manual
vacuum evacuation foIlowing miscarriage) could be
lifesaving for thc women served by program graduates.
Other midwives may wish to acquire certain skills fbr the
sake of increasing women"s access to particular services.
Many midwives have acquired thesc additional
skiIls through continued education and/or in-service
programs, As midwives gain experience and develop
proficiency across the core competencies that are the
core elements of entry-levcl professional practice, they
are ready to take on new expandecl practice roles.
COMPETENCY-BASED EDUCATION
Knowlcdge, skills, and associated professional attitudes and
behaviors for the professional practice of mid"tifery arc
taught and modeled within a competency-based midwifery
education prograin. A competency-based curriculum of
studies forges links betrveen curriculum content and the
expectedoutconiesofaprogramofstudy(Farrand,McMul-
lan, Jowett, & Htimphreys, 2006). The defining attributes of
a competency-based curriculum are the teaching ofknowl-
edge and ski11s in all domains for the practice role, instruc-
tion that focuscs on spccific outcomes er competencies,
alowanceforincreasinglevelsofcompetencxaccountal)ilit〉rof the learne4 practice-based learning, self-assessment, aricl
indiyidualized learning experiences (Scott-Truex 2008).
Guidance documents developed fbr midwifery
education programs b〉r the ICM and the WHO and
as
8 Competence and Competency: Core Concepts for lnternational Midwifery Practice Fullerton et aL
tampetencv #1es"e'E'tol'stienleS;・'puli1ie
hildbeoringfom[ies.
eo[fi'.:'MdiKff¥trci''i"ifi'i':''tt'//i sr/''
Domains of Cornpetenry 1. Ethies, epidemiolegv and infedion prevenfion
- Human [ights
- Legol ond regulatory ftameworks
" Administretien oRd monagement, statisias
CompetennyS2
MiGwivesprevidehigh
qualitv,culturu1lysensMve
heolthetiucottonaed
servicestea1[[nthe
communilyinorderto
premotehealthvfomily
1ffe,plennedpragnondes
andposifueparenting,
Competen{v S3
Midwivesprovidehigh
qualilyantenotoIcoreto
maximiietheheo1th
dvringpregnannyandthot
includesear[ydetedion
endtreotmentoTraferral
ofselected[omplicatiDns.
Competenny#4
Midwhtesprovidehigh
quoliv",avlaurullysensime
caredu[igglabor,conduct
acleonQpdsafedelivery,
ondhondleselected
ernengencysituotiensto
gvmaximiiethehealthef
womeilandthetrnewboms,
Competenny#S
mawhespnvmle
comp[ehensive,high
qvainMeshn1lysemstwe
postpomimco[eforwomen.
CompetennyS6
Midwivesprovidehigh
qualily,comptehensive
carefoTtheessentiallv
healthvinfentfiombirth
to two months Df oge.
Cempstenny#1
MidwivesprovideGrange
ofinrfividuoETed,ou1turolly
senstweabodioorelated
[oreservicesforwomeR
reqummgerexpeEle"[mg
ptegnoncyterminedonor
lessthotare[ongruent
withapp[icob[elawsand
tegulgtionsandiRa[cord
withn"tionalprotocels.
Domainsof
Competencv 2
- Womom's health cere.
-Porenteducotion
" Farnilv plonning
Domairsof
Compatency3
-Antenatal[ere
. PreparatiDn for Iaber,
binhandparenfing
-PnvG
bahains'of'
Competenny 4
tMenagemeRtoflebDT
tMoRogementoflabor
DndiimmediGteposti
ptmbmcompli[ations
" De[ivery skills
bomainsof
CompetenryS
-Poshetalcare
-PostnGtolfomilv
plomning
- [nitiatien ef
bteasffeeding
Domainsef
Competen{y6
- Newborn fissessment
- Newbom care
.Supportof
breostfeeding
bemainsof
Compete"cv7
- Abonion [ounseling,
[areandsupport
t Pesttbonien fomilv
plannin9
Psychomotor Detision-rnaking CommunTcation
-FIGURE 2 ICM Essential Competencies: An integrative concept.
similar global technical assistance agencies often include
recommendations concerning the minimum numbers of
clinical practice experiences that students should acquire
before they are considered eligible fbr graduation. These
minimum numbers have been derived from both anec-
dotalevidenceandformalresearchthathasdemonstrated
an association between progressive Ieyels of experience
and the abdity to demonstrate a p;edetermined level of
skill in task performance. Howeve4 although it is the
case that recommended minimum numbers of experi-
ences are associated with competency development, it is
also the case that acquiring specific numbers of experi-
ences does not necessarily mean that competency has
been achieved by any indMdual learner.
ADDITIONAL CONSIDERATIONS
A first essential corollary to competent midwifery per-
formance is the concept of an enabling environment
fbr practice. An overarching framework of political,
econemic, and sociocultural support for midwives and
midwifery practice must exist before such support can
be translated at the educational and clinical practice
Ievels into pragmatic and tangible concepts, such as
the accessibility of reproductive health guidelines, peer
support for the midwife's day-to-day work performance,
and the supplies and equipment that are essential for the
performance of the task (Morrissey & Schmidt, 2008).
Hussein et al, (2004) have proposed a new methodology
for measuring the proportion of skilled attendance at
childbirth, which goes beyond designating the attendant
by credential, but, instead, creates a composite measure
of delivery care that indicates the degree to which the
attendarit functioned witliin a practice environment,
which facilitated the deliyery of high-quality health care
services. In other words, did the ski11ed provider have
needed supplies, equipment, and transport available
to provide good care? This unique approach takes into
consideration the fact that a ski11ed provider may not be

i'
1
1
:
b
Campeten[e and Competen[y/ Core Conc'epts fer lnternntional /Viidwifery Practice Fuitc'rtoneta/, 9
able to save lives ifshe or he does not have thc reseurces
available to allow thc deliver}r ofclinically proficient care
services-both are necded. Kayongo, Rubardt, Butera,
Mboninyibuika, and Madili (2006) demonstrated that
placing a t'ocus on maintaining functional health facili-
ties aided the providcrs in those facilities to increase the
proportion of emergency obstetrical and neonatal care
services that they were able to otfer.
Additional cero]laries to competent midwifery per-
formance are the allied concepts ofcor!fidence or capability.
The midwife may have demonstrated the ability to per-
form a task to a certain expected tevcl ofteclmical accuracy
at a given time, but m ay not yet have attained any degree of
internal assurance that she or he could do so ifca"ed on to
perform that ski11, and particularly so in emergcncy situa-
tions, or when other skilled assistance is not inimediately
available (Farrand et al., 2006; Gardne4 Hase, Gardner,
Dunn, & Carrye4 2008). Additionatts technical compe-
tency attained for any sLcM and the correlated confidence
related to task perfbrmarice are rarely sustained at the same
level, even from day-to-day (Scotland & Bullough, 2004),
because the conditions, circumstances, and uncommon
situations that affect peak performance change.
Finallyinanyclinicalsituation,competenccmaydif
fer from performance. Competence itselfis onlyofvalue as
a prerequisite for performance in a rcal clinical situation. It
may well be about recognizing one's own limits, which, in
turn, is related to the concept ofprofessional behaviors that
are grounded in the ethics of professional practice, The
competent midivifery practitioner would nlake decisions
considering the human and reproducti e rights of women
and fami1ies, and not bascd on personal attitudes or values
(ICM, 2003; Vanaki & Memarian, 2009).
DISCUSSION
Adelineationofthecompetenciesthatshouldbeexpected
of the fu]ly qualified midwife at entry into practice of the
profession is fundamental to understanding the role
of the professional midivife. It also has ver}r pragmatic
applicattons in academic settings and in the workplace.
Professional inidwifery education programs are
always faccd with the challenge (and sornetimes pres-
sure) of enrolling sufficient numbers of students to
meet country workfbrce needs, This challenge is coun-
terbalanced by the very real resource limitations that
most programs encountcL Such 1imitations may include
faculty!student ratio, classroom, library and skills lab
resources, and access to clinical practice experiences.
In some countries, these challenges include educational
policies that focus on shorter term workfbrce solutions
that include the training ofmore narrowly qualified birth
providers (e.g., the community midwife) who compete
for access to clinical experiences and teaching rcsources.
A commitment to competency-based education should
play some role in helping policy makers andeducational
adrninistrators makc educational policy decisions in the
context ef the rights of students to acquire the knowl-
edge, professional behaviors, and skills relevant to the
professional role, and in the context of the rights of the
clients to expect skiIIed care from their previders.
Simultaneously, it is usefu1 for employers and
employees to have a clear understanding of the scope
of work that can be expected of the midwife in the
workplace, so that midwifery skills can be fully and
appropriatcly used, and that the scope of practice is
neither cxploited nor constrained (Homer et al,, 2007),
The job description for a midwife should bc based on
linkage between thc competency-based education that
the midwife has completed, the reproductive health
guidelines that are in place in the countr" and the mid-
wife's pcrsonal assessment of her or his confidence and
competence to practice that role. For example, midwives
in Brazil were able to advocate fbr a more appropriate
utilization of midwifery practitioners by documenting
the `Cdisconnect'] between their competency-based edu-
cation and the role to which they were assigned in the
public health care system (Narchi, 2009). Doctors, mid-
wives, and other health professionals working in a pub-
lic referral hospital in Palestine identified the fact that
the widely held perception that midwives were at the
lowest level of the health professional hierarchy made
it very difflcult for them to be effective advocates for
improvements in the guality of care offered to women
and infants, including the resources required for quality
service (Hassan-Bitar & Narrainen, 2009).
The ICM encourages countries to adapt the core set
of basic competencies to refiect the particular needs and
circumstances of the country: ,For example, midwives in
Africa collaborated to expand the competencies to reflect
trie role of midwivcs in combating rnalaria and HIVI
AIDS in that region (WI{O, 2006). In a second example,
a Delphi survey of stakeholders in 1[Unisia, including
midwives, health providers, health progratn managers,
women, educators, professional organizations, and deci-
sion makers, explored the centributions that midwives
could makc to meeting health carc needs in that country:
Findings were operationalized through delineation of
core cornpetencies for midwifery practice, thus establish-
ing midwives as a contributing member of the rcproduc-
tive health workfbrce (Gh6rissi. 2008). The (CM also

1O Competence and Competency/ Coro Clemcepts for lnternat[onal Midwifery Practice Fuller[on ot al.
-
urges countries to use thc Essential Competencies as com-
plernentary to the competency delineation documents
produced by and fbr other cadres who also provide sexual
and reproductive health care services (BarrM Allegrante,
Lamarre, Auld, & [faub, 2009; WHO, 201 1),
The cultural andpoliticaL appropriateness ofeach of
the core competencies should aiso be considered (ButleB
Frase4 & Murplry; 2008). tl'he TCM has taken great care to
craft the statement ofcore competcncies with sensitivity
for language and culture. Nevcrthclcss, it is the case that
some of the tasks that have bcen dcfincd as basic knowl-
edge or skill are not yet authorized for midwifery practice
by regulatory policy in certain countries.
In many countries, midwives are also educated and
credentialed as nurses. These combi[ied prograrns may
require a Lenger period of study to acquire competencies
for both professions (e.g., midwifery studies fbllowing
completion of nursing studies), and ma}r, therefore, be
more expensive for stuclents and fbr educational institu-
tions, There is an acknowledgcd advantage to dual prepa-
ration,Individualshavepersonalchoiceinsornecountries
te practice either or both of thosc roles, thus generating
opportunities for job mobility and autonomy in career
choices. ln other countries, graduates must complete
an obligatery period of public service. Human resource
departments have the optien of assigning these dual-
credentialed nurse-inidwives to any setting, based on
the priority workfbrcc needs of the heaLth facility: These
dual-credentialed practitioners are also more broadly
prepared for practice in health faci]ities where only a few
health workers are assigned, for examplc, in rural health
clinics or health posts (Francis, 2009; Hundley et al,, 2007;
Ireland et al,, 2007). On the other hand, tliere is the risk
of de-skilling when practitioners practice one role to the
exclusion of the other. Unless human resource personnel
and supervisors recognize their added value, the advan-
tage ef unique midwifery skills can be lost (Scotland &
Bullough, 2004), SimilarlM it is sometimes the case that
individuals are preparcd as midwives but never actually
work as midwives. This could be viewed as a waste of
precious educational resources.
CONCLUSIONS AND [MPLNCATIONSFOR GLOBAL PRACTICE
A clear understanding of thc concepts of competence
and competency serves an important purpose for indi-
vidual midwives and for the education and practice
communities where they serve. These concepts under-
pin the global cal1 to action to strengthen midwifery te
save lives and promote the health of women and new-
borns (ICM et a]. 201O).
The ICM Essential Competencies prevides the
individual midwife with an external reference criterion
fortheknowledge,professionalbehaviors,andskiIIsthat
define professional midwifery practice, against which
she or he can assess the individual level of need fbr con-
tinued learning. Midwives can also use the concept of
competency as a means to analyze new practices as they
are asked to consider adding them to their practice. For
exarnple, a midwife being asked te assume responsibility
for vacuum extraction can use competency as a logical
framework for exploring whether she or he has suth-
cient access to thc evidence-based information, skiiled
experts, anatomic models, clinical equipment, supplies,
and paticnt experiences needed to obtain the knowl-
edge, communication, clinical decision, and psychomo-
tor skills associated with developing and maintaining
competence in this new area.
Competencies provide educational administrators
with a tneans of ensuring that curriculum and educa-
tional resources are directed toward achieving learning
outcomes that arc consistent with safe, beginning-level
midwifery practice. Thc ICM recently develeped global
standards and guidelincs for midwifery education that
can serve as a framework for strengthening the initial
preparation of fully qualified midwives based on the
ICM Essential Competencies.
Competencies can be used by national regulators,
midwiferycouncils,andrcgionalhealthdistrictandlocal
facility managers responsible for maintaining the guality
of care, A reproductive health care system that relies on
midwives (or any other cadre of birth attendant) who
are Iess than competent to provide care at entry into
practice and over the professional practice ltfetime is
dangerous te women, their families, and cemmunities,
Specifically, midwifery cempetencies can be used to
prioritize delivery of continuing education and ski11s
assessment that arc most needed to ensure that efTective
services arc dclivcrcd by the midwifery workibrce. A
focus can be placed on clinical services that require tlie
most complex set ofslci]Ls, that do not reguire frequent
performance, and that have high potential for morbid-
ity; if not performed competentlM
The conccpts ot' competence, competencM and
competency-based education have received a great deal
ofattention in recent years. Widespread understanding
and application of these essential constructs can lead
to transformative educationaL clinicaL and regulator〉rimprovements in nations struggling to build a quality
midwifery workforcc aimed at meeting relevant MDGs.
g, ,/, .,.".t."sv4.',le.wh '
'

Competence and C/ompetency: Core C/oncepts for lnternational Midwifery Practice Futlefton et al. 11
!
/
'
1
:
/
REFERENCES
AxleB l. (2008). Competency: A concept analysis. Nursing
Forum, 43(4), 214-222,
Barry M. M., Allegrante, J. R, Lamarre, M. C., Auld, M. E., &
Taub, A. (2009). Thc Galway Consensus Conference:
Tnternational collaboration on the development ofcore
competencies for health protnotion and health educa-
tion. Global Health Promotion, l6(2), 5-・1I.
Benner, l', (1984), Frotn novice to expert: Excellence and
power in clinical nursing practice. Menlo Park, CA:
Addison-Wesley
Bullough, C., Meda, N., Makowiecka, K., Ronsmans, C.,
Achadi, E. L., & Hussein, J. (2005). Current strategies
for the reduction of maternal mortality. British fournal
flf'Obstetrics and (lynaecolqgy, 112(9), L 180-1 188,
Butler, M. M,, I;raser, D, M., & MurphB R, J. (2008), What are
the essential competencies required ofa midwLfe at thc
peint of rcgistration? Midwijbry, 24(3), 260-269.
Carlough, M., & McCall, M, (2005). Skilled birth attendance:
What does it mean and how can it be measured? A
c]inical skills assessment of maternal and child health
workers in Nepal, lnternational fournal of (lynaecology
and Obstetrics, 89(2), 20e-208.
Chiarella, M,, Thoms, D., I.au, C., & Mclnnes, E, (2008), An
overview of the competency movement in nursing and
midwifer}L Collegiatt, 15(2), 45-53.
Cowan, D. T,, Norman, I,, & Coopamah, V P, (2007). Com-
petence jn nursing practice: A controversial concept-a
focused review of the Iiterature, Accident and Emer-
gency Nursing, 15(1), 20-26,
De Ketele, J. M. (200e). Approche socio-historique des compe-
tences dans 1'enseignement rSoclo-historic approach of
competencies in education]. In C. Bosman, E M. Gerard,
& X, Roegiers (Eds.), Quell avenir pour les cotnpetencese
Coliection Ptidagogies en de'veloppement (pp. 83-92), Bru-
sells, Belgium; Edition De Bocck Univcrsite.
I)reyfus. S., & Dreyfus, H. (1980). A five-stage modcL of thc
inental activities involved in directed skill acquisition.
Uliiversity (if CalijimJia Berkelay Press. Retrieved from
h(tp:Uwrvw.storrningmedia,ust15t1554fA155480.htm!
Farrand, R, McMullan, M., Jowett, R,, & Humphreys, A.
(2006). Imprementing competency recomrnendations
into pre-registration nursing curri[ula: Effects upon
leve]s of confidence in clinica) ski11s. Nurse EducatiotJ
R)tlay, 26(2), 97-103.
I:rancis, K. (2009). Rural nursing and midwifery workfbrce:
Sustaining and growing our future workfbrcc. Austra-
tian fournal Rttrat Hca{th, 1 7(5), 287,
Fullerton, J,, Sevcrino, R., Brogan, K., & Thompson, J. (2003).
Thc International (]onfederation of Midwives' study
of essential competencics of midwifery practice. Mid-
ivijlery, l9(3), 174-190.
Fulterton, J. rC, & Thompson, J. B. (2e05), Examining the
evidence for the International Confederation of Mid-
wives' essential competcncies for midwifery practice,
Midwipry, 21(1), 2-13.
Gardner, A,, Hase, S., Gardner, G,, Dunn, S. V, & Carr〉,er, J. (2008). From competcnce to capability: A study of
nurse practitioners in clinical practice. fournal ofClini-
cal Nursing, 17(2), 250-258,
Gh6rissi, A. (2008). Pour une meilleure integration des sayoirs
dans la formation aux professions de sante [How to
better integrate all knowledges in health profession
education programmes 1 . Ecole Supgrieure des Sciences et
fechniqttes de la Sante' (pp, 12-89), TUnisia: Uniyersite
Tunis-El Manar.
Hassan-Bitar S., & Narrainen S. (2e09). "Shedding light" on
thechallengesfacedbyPalestinianmaternalhealth-care
providers.Midrvijlery.doi:1O.IO161j.midve2009.05.007
Hofmeyr, G. J., Haws, R, A,, Bergstr6m, S,, Lee, A. C., Okong,
R, Darmstadt, G. L., ,..Lawn, J. E. (2009). Obstetric
care in low-rcseurce setLings: What, who, and how to
overcome challenges to scale up? tnternational journal
of (lynaecolog), and Obstetrics, 107(Supp). 1), S21-S45.
Homer, C. S., Passant, L,, Kildea, S., Pincombe, ],, 'rhorogood,
C,, Lcap, N., & Brodie, P. rvl, (2007), The development
of national competency standards for the midwife in
Australia,Midwij2iry,23(4),350-360,
HundleM V A., TUckeq J. S., van Tbijlingen, E., Kigeil A,,
Ireland, J. C., Harris, E, . . . Bryers, H. (2007), Midwives'
competence: Is it affected b}r ;vorking in a rural loca-
tion? Rural Rentote Health, 7(3), 764 (e-pub).
Hussein, I,, Bell, I., Nazzar, A,, Abbe¥ M., Adjei, S., & Graham,
1・V, (2004). The ski11ecl attendance index: Proposal for a
new measure ef skilled attendance at de]iverpt Repro-
ductive Health iVIatters, 12(24), 1 60-170.
Intcrnational Confederation of Midwives. (2002). Essential
competencies for basic midvvijVry practice. The Hague,
Netherlands, Rctrieved from http/tl;vi"v.international
midwives.orgll'ortals/51DocumentationfEssential%20
Compsenglish-2e02-JF-2e07%20FINAL,pdf
Intcrnational Confedcration of Midwivcs. C2003). Cvde ofelhics.
Retrievcd from http:/lwwwinternationalmidwives.org/
Docurnentation/Coredocumentsltabid13221Default,aspx
International Confederation of Midwives. (2005). Definition
ofthernidwijle,RetrievcdfromhttpVtswuv.international
midwives,orgfPortalst5/DocumentationflCM9!n20
Definition%20of%20thc%20Midwife%202005.pdf
International Confeclaration of Midwives. (n,d,). Clobal Stan-
dards for Midrvijlery Education. Retrieyed from http:/t
www.internationalmidwives.org

'f
ee
12 Competence and Competency: Core Concepts for lnternational Midwifery Practice fullerton et aL
InternationalConfederationofMidwives,UnitedNationsPopu-
lation Fund, Johns Hopkins Prograrn for international
Education in Gynecology and Obstetrics, Wbrld Health
Organization,GlobalHealthWbtkForceAlliance,Uhited
Nations Children Fund, ,,. Wbrld Bank, (2010). A
global call to action: Stretrgthen midwijlery to save lives
and promote health of women and newborns. Retrieved
from http:I/wwwLwho,intlworkforcealliance/medial
events120101midwifery=jointstatement.pdf
Ireland, J,, Bryers, H., van Tlelj1ingen, E,, HundleF XC, Farmeg
J., Harris, E,...Caldow; J. (2007). Competencies and
ski11s for remote and rural maternity care: A review
of the Iiterature. journal ofAdvanced NLirsitrg3 58(2),
105-115.
Kayongo, M,, Rubardt, M., Butera, J., Mboninyibuika, A., &
Madili, M. (2006). Making EmOC a reality-CARE's
experiences in areas of high maternal mortality in
Africa.bzternationalJburnaloj'(lynaecologyandObstet-
rics, 92(3), 308-319.
Lasnie4 E (2000). Re'ussir la formation par compe'tences [Suc-
ceeding competency-based trainingl (pp. 22, 31, 42, 63,
73, 159-174, 324, 480-485). Quebec, Canada: Guerin
EditeurItee.
Lawn, J,, KinneM M., Lee, A. C., Chopra, M., DonnaF E,
Paul, V:, . . . Darmstadt, G. L. (2010). Reducing intra-
partum-related deaths and disability: Can the health
system deliver? international journal oj' (lynaecoleg],
and Obstetries, 107, S123-142.
Le Boterg G. (2000). De quel concept de competences les
entreprises et les administrations ont-elles besoin?
[Which concept of competences do rnanufactures and
administration need?]. In C. Bosman, E M, Gerard,
& X. Roegiers (Eds.), wriich concept of competences do
mannjincturers and administration need? (pp. 15-19).
Brussels, Belgium: Edition De Boeck Universite,
Lee, A. C,, Lawn, J. E., Cousens, S,, Kuma4 V:, Osrin, D.,
Bhutta, Z. A,. , , Darmstadt, G, L, (2009). Linking fami-
lies and facilities for care at birth: What works to avert
intrapartum-related deaths? biternational journal qf
(lynaecolctgy, and Obstetrics, 107(SuppL 1), S65-S88.
McMullan, M., Endacott, R., Gral; M. A., Jaspe4 M,, Mille4 C.
M,,Scholes,J,,&Webb,C.(20e3).Portfoliosandassess-
ment of competency: A review of the literature. Jburnal
ofAdvanced NLtrsing, 41(3), 283-294.
MorrisseF C. S., & Schmidt, M. L, (2008). Fixing the system, not
the women: An innovative approach to faculty advance-
ment. Jburnal of Wbmen's Health, 1 7(8), 1399-1408.
Narchi, N. Z, (2009). Exercise of essential competencies for
midwifery care by nurses in Stto Paulo, Brazil, Mid-
wijlery.doi:10.106/j,midwL2009.04,O07
Roegiers, X., & De Ketele, J, M. (2000), Une pedagogie dc
1'integration,Competencesetintegrationdesacquisdan:
l'enseigement [An integrative pedagogyL Competencie:
and integration ofachievements in teaching], Collectiot
Ptidcrgogies en dtiqppement (pp. 46, SO, 55-62, 65-66
74, 81-82, 126, 130-133, 157-173), Brusells, Belgium
Edition De Boech Uhiversite.
Scotland, G. S., & Bullough, C. H, (2004), What do doctor:
think their caseload should be to maintain their ski11:
for delivery care? international journal of Clynaecologr
and Obstetrics, 87(3), 301-307.
Scott-TilleB D. D, (2008). Competency in nursing: A concep
analysis. Jburnal of Continuing Education in Ntirsing
39(2),58-64.
United Nations, (2000). Millennium development goals
Retrievedfromhttp://ww.un.orglmillenniumgoals
Vhlloze, J. (2009), Competence: A concept analysis. Iliachiny
and Learning in Nursing, 4(4), 115-118.
Vltnaki, Z., & Memarian, R. (2009). Professional ethics
Beyond the clinical competencp fournal ofPrzlt2issiona
Mrsingt 25(5), 285-291.
Wbodruffe, C, (1993). What is meant by a competencyi
Leadership and Organizational Develqpment journal
14, 29-36,
Wbrld Health Organization. (2006), Consensus on essen
tial competencies oj' skilled attendant in the ijicat
region, Report of regional consultation, Brazzaville
27th February-lst March 2006. Retrieved from wwy
.mps-report.con$ensus-essential-competencies-fina
Mlorld Health Organization. (2011). Sexual and reproductiv4
health core competencies in pritnat:y care. Retrievec
from: www.who,intfreproductivehealth/publications,
sexual healthlenl
Correspondence regarding this article should be directed t(
Judith 1[: Fullerton, 7717 Canyon Point Lane, San Diego, CP
92126.E-mail:j.fu11erton@hotmaiLcom,
Iudith [[: Fullerton, Independent Consultant, San Diego, CA.
AtfGherissi, Assistant Professo; Education Science, High
School for Sciences and Health Tlechniques, TUnis-El Manar
University:
Peter G. Johnson, Jhpiego-An affiliate of Johns Hopkins
University; Global Learning Directo4 Baltimore, MD.
Joyce B. Thompson, Western Michigan Uhiversity (Emerita),
Uhiversity ofPennsylvania (Emerita), Delton, MI,
..lt"/' ",,AU"L..,as.mb

/
'
'
Becoming a Mother: Womerfs Journeys
From Expectation to Experience in
Three European Countries
Ans G. Layben, Sue R. Kinn, and 1lalerie E. M FIeming
J
I
I
OBJECTIVH: Tb investigate important aspects of provision of routine antenatal care frem women's
points ofview in thc Netherrands, Scotlalld, and Switzerlanc! tind to construct a conceptual model of
care during pregnancy, informed by women,
DESIGN: Grounded theory using semistructured interyiews to explore women's views, 'l'he interviews
were undertaken in Dutch, English, and German.
FINDINGS: ln the main study, one single cross-national model emerged, which had implications
for women beyond the antenatal pcriod. [tMothering the mother" emerged as a core categorM 'rhere
were two subcategories: "creating a bond" and `tbecoming a mother:' The subcategory of "becoming
a mother," which incorporated the stagcs of "expecting," "familiarizing," and "embarking on moth-
crhQod;' is rel)orted in this artide. Women defined becoming a mether as the aim ofprovision of
maternity care in wliich they described their journeys from creating expectations in early pregnancy to
completing the expcrience approximately a year after childbirth, Mistnatches between expectation and
experience at the end of these journeys indicated cross-national differenccs in the proyision of mater-
nity care, particularly regarding the woman-care provider relationships.
CONC[.USION: The findings from this study suggest that an essential aim of thc maternity services
was to support women in the process of becoming a mother, in the context of their own social svorld.
Supportive conditions include wornan-care provider 1)artnerships, involvetnentof women's individual
social worlds in care provision, and continuity of the ca re proyiding process, These conditions should
be taken into account, whilc designing effective rnodels of maternity care,
KEYWORDS: prenatal carc; effectiveness; women's views; Europe; grounded theory; becoming a mother
1
t
tNTRODUCTION
Over the last few decades, how best to approach thc pro-
vision of efflective content of routine antenatal care pro-
grams has been a topic of discussion in Western European
maternity care literature (HaLl, Macintyre, & Porter, 1985J
Heringa, I998; W6rld Health Organization [WHO], 1987).
The United Kingdom's (UK) program ofantcnatal care, in
its present format, was introduced in 1929, with the prin-
cipal aim of reducing higlt rates of maternaL and infant
mortality Other European countries followcd the British
example, initiating very similar programs (Brezinka, 1997;
Heringa, 1998). AIthough, originallM the emphasis was en
educating mothers to take care of themselves and their
babies, a shift toward preventative medicine, and the pro-
fessional supervision of expectant mothers was observed
shordy after Wbrld Whr [. The reduction in matemal and
perinatal mortality and morbidity during the course ofthe
20th century was viewed as evidence ofvaluc ofthese pro-
grams, without taking into consideration other social fac-
tors, which may have affected these figures (Oakleyl l982).
In the early 1970s, howeve4 consumcrs and health
providcrs in the UK bcgan to call for a systematic
evaluation of the effectiveness of maternity care services
tN7EnAVLIIOAL4L JOURAL4L OF CHILDEIR7'H Llotume 1, tssue 1, 2011 @ 2011 Sprlnger Publishing Company, LLC www,spri"gerpub.com DOIIIO,I891X2I56-5287.1.1.13
sttT/ cstt-ev.
i. (g2"¢xl"i
bt k,dr/ttt
L
E

14 Becoming a Mother: Women's Journeys From Expectation to Experience in Three European Countries Luyben et at,
'
(Cochrane, 1999; Garcia, 1982). Concurrent})g advancing
European integration led to concerted interdisciplinary
concern about the effectiveness of antenatal care. As a
result, antenatal care programs and their content were
subjected to extensive research and evaluation during the
1980s and 1990s, both within Europe and within interna-
tionally (Enldn & Chalmers, 1982; Heringa, 1998; VruaB
Carroli, Khan-Neelofug Piaggio, & Gulmezoglu, 2001).
These studies found that the effectiveness of many proce-
dures used in antenatal care was yet to be proved, and that
a reduction in the number and content of the antenatal
care visits was possible without affecting maternal and
perinatal outcomes (Vmuar et al., 2001). Some of these
evaluations, particularly in the UK, involved women's
experiences and satisfaction. The principal complaints
reported by women were the lack of agreement between
the organizational aspects of antenatal care and their
personal needs, the information they were receiving, a
lack of continuity of care, and the impersonal treatment
received at antenatal care clinics (Garcia, I982; Jacoby &
Cartwright, 1990; Reid & Garcia, 1989).
Researchers, therefore, are currently divided about
the value of antenatal care programs in Wlestern Europe.
Although some studies found that antenatal care led to
better pregnancy outcomes (Richardus et al,, 1997; Vruar
et aL, 2001), others could not find a causal relationship
between the content of a program and its effects (Fink,
Yano, & Goya, 1992), or stated that increased medical con-
tent negatively affected women's health (Heringa, 1998). It
was even suggested that the ritualistic significance of the
antenatal care visits was more important than tlie actual
content (Enldn & Chalmers, 1982; Heringa, 1998). Both
Graham and Oakley (1981) and Field (1990) highlighted
the existence of difflerent perspectives on the aims of
aritenatal care, which would influence the approach to the
evaluation of effectiveness. These researchers remained
among the few to criticize the prevai1ing approach to the
evaluation of effectiveness, and to define the aims of ante-
natal care from women's perspectives,
This study aimed to investigate important aspects
ef provision of antenatal care from women's points of
view in three European countries (the Netherlands.,
Scotland, and Switzerland) with different health care sys-
tems. The objective was to construct a conceptual model
of care during pregnancy informed by women.
METHODOLOGY AND METHODS
GroundedtheorsaccordingtoStraussandCorbin(1998),
was chosen to attain the objectives of this studF because
it offers an inductive appreach through generating theory
from data grounded in every(lay reality: This constructiv-
ist methodology aims to explore analytically the magni-
tude of the research area in which significant themes and
patterns are discovered. During subsequent stages of the
study; it allows for increased focus on these themes whiIe
developing a conceptual framework that underpins theo-
rizing (Strauss & Corbin, 1998). In this way; the chosen
approach took into account the many factors that could
influence provision of antenatal care in the three coun-
tries involved.
From a grounded theory perspective, the research
field had to be addressed as one unit, even though
it involved women in three countries with three dif
ferent languages. Any variable had to earn its place
in the theory based on its relevance. This mearit that
language, for instance, cannot be defined in advance
as a mediating or differentiating factor in the theory
(Glaseg 1978). Howeve4 language has been seen as the
consequence of the creation ofjoint meanings of sym-
bols created through interaction with the social context
and, thus, from this perspective, minimal translation
should take place (Blumeg 1998; Strauss & Corbin
1998). Therefore, based on theoretical sampling in this
studx two or more interviews carried out in the same
language were treated as a unit of meaning ("language
unit"; Glaser & Strauss, 1967; Strauss, 1999). Consis-
tency of meaning was achieved by the construction of
similar concepts among women in each language. After
constant cornparative analysis within each 1anguage
unit, further comparison was used to integrate concepts
from each unit to the whole. This way comparison of
concepts took place at a higher abstractien level (Brislin,
Lonne4 & Thorndike, 1973; Gales, 2010). Through
using language units, theoretical sampling was left intact
within and across countries.
Rigor was ensured in this study by the fact that
one multilingual researcher managed the collected
data in all three languages, The researcher's reflexiv-
ity is an integral element of grounded theory both
to the process of data collection and analysis, and is
guided by memo writing (Strauss & Cerbin, 1998).
Therefbre, the supervisors of the study (VEME SRK)
checked the analysis of the data. [[b further safeguard
and promote reflexivitM the results of this analysis and
the established audit trail of memos, field notes, and
other relevant information were discussed with these
supervisors, as well as two maternity care professionals
in each countrM on a regular basis. Resulting concepts
were validated by checking them with wornen within
and across languages.
..t,・,'./it,.h,'/,.t'・..u',.,,t/',le...'-M',.-.tuLde'

Becomlng n Mother: Women's journeys From Expectation to Experience in Three Eufopean Countries t"yben et aL 15
1
t
1
4
:
Ijl
:
1'
!
/
SETTING
NVbmen were recruited to the study from three European
countrics: Scotland, Switzertand, and the Nethcrlands.
The localities involved wcre west of Scotland, the
German-speaking part of Switzerland, and the eastern
and wcstern part of the Nctherlands.
SAMPLE
Theparticipantswerehealthywomenatdifferentstagesof
uncompLicated pregnancies. 'J'hey were initially followed
up to 6 months after giving birth. Based on theoretical
samplinb,, this was then extended to a year after giving
birth (see Thble l). Routine antenatal care was defined as
attending the normal contcnt and frcquency of visits, as
set by thc health system of the country involved.
NVdrnen were recruited using convenience and the-
oretical sampling approaches. The first round of inter-
vlews was conducted using a convenience sample and
includcd five women from Scotland, five women from
Switzerland, and seven women from the Netherlands.
As the theory emerged, it became clear that more
data from specific contexts or women were required.
Theoretical sampling was, therefore, used to reflect on
the diflltrent kinds of care providen as well as to dem-
onstrate the evolving process during pregnancx child-
birth, and postpartum and sLLbsequcnt pregnancies (see
1[hble I). This rneant, for example, that three women in
each country were interviewed a year after having their
first child to reflect on the course and completion of the
childbirth and postnatal process, whereas others were
interviewed in theirsecond or third pregnancy to reflect
on the development of this process in subsequent preg-
nancies.Theoreticalsamplingconcerningdifferentkinds
of care providers involved a Swiss wo]nan attending care
with a female care gynecologist, and in Scotland, two
women with an independent midwife. In addition, in
each sarnple of cach countrM one ef the wemen from a
previous sample was again interviewcd up to a period of
5 years after giving birth to verify and discuss the results
ofthe anatysis.
did not require additional ethical approval in the
Netherlands and Switzerland.
Based on the criteria for sampling, recruitment took
place in Scotland by both supervisors of the study and the
care providers, and in Switzerland and the Netherlands,
by the researcher herselfand the care providers.
'['lte women were provided with an infbrma-
tion sheet about the study) and were asked to centact
the researcher if they were interested, No woman
approached refused to participate, and none later with-
drew their consent.
All womcn gave written conscnt to the researcher
befbre the intcrviews took place. The researcher trans-
Iated all information and consent t'orms into the thrcc
languages used; English, German, and Dutch. These
translations were then checked b〉, persons living ineach of the countries involved. A Iist was created with
culturally appropriate first names, and each participant
was assigned one of these names for reporting purp oses,
to aid anorrymity
DATA COLLECTION
The data werc collected through one-on-Dne audio-
tapcd interviews in English, Dutch, or German, as
appropriate, by the researche4 at a convenient place for
the women. Thc interviews were semistructured, using
an interview guideline as a reference, Interviews lasted
froni 2l to 126 minutes. No woman refused tape recoi'd-
ing of the intervie w:
The leading interview question was `CIf 〉rou coulddetcrminethecontentofcareduringpregnancyyoursclL
base(l on your needs and expectations, what would bc
important to you?'] Following this question, the women
werc cncouragcd to tell thcir stories, during which some
topics, such as access to care, werc introduced by thc
interviewer, In the interviews of the women samplcd
theoreticallF new topics from thc emerging categorics
guided the discussion, FieLd notes were made to guide
data collection. Most women were interviewed once,
threc women were intervLewed twlce, and two wornen
were interviewed thrice (see [fablc 1).
ACCESS AND ETHICAL CONSIDERATIONSDATA ANAI:YSIS
Ethical approval was gained from thc Ethics Committee
of Glasgow Caledonian University and the Lanarkshire
Ethics ef Research Committee, Access to the participants
Five procedures contributed to data analysis: transcribins,,
coding,writingmemos,classifyingandcategorizinginone
Ianguage and, finall)g the cross-language comparison and
integration, The interviews were transcribed verbatim,

/
-
t'-'
16 Becoming a Mother: Wome-'s Journcrys From Expectation to Experlence in Three European Couturies t.uyben et aL
TABLEI CharacteristicsoftheSamples
COUNTRYXNAME PIBIM CAREPROVIDER
NL- Er]n
NL- Mar[anne
NL- Hannah
NL- Mirei[Ie
NL- Saskia
NL- Ariane '
NL- Joelle
NL- Kerstin
NL- Laura
NL- Maren
NL- Eiena
NL- Nicole
SL- Heather
SL- Megan
SL- Nera
SL- Susan
SL- Jan
SL- Lynn
SL-Vanessa SL- Emily
SL- Deborah
' SL- Hol]y
CH- ibola
CH-Yvonne
CH- Li[ian
CH-Ve;enaCH- Barbara
CH-Sarah
CH- Rosemary
CH- Catharina
CH- Lea
111fO
21110
312/1
1/OfO
2/Oll
2/1/O
212/O
511/4
3/210
11110
2/2tO
1fOfO
211fO
110fO
31210
2/210
2/210
5/3f2
4/2f2
1/OfO
211/O
3/31e
2/1/1
/St3fO
2/O/1
2/2!O
31210
212/2
lfOtO
111fO
4/212
Midwife
Midwife
Midwife
Midwife
Midwife
Midwifc
Midwife
Midwife,
Ref birth
Midwifo
/V[dwife,
Refb[rth
GynMidwife
Shared care
Shared care
Shared care
Shared care
Sharedcare
Midwile
Midwife
Shared cnre
Shared care
Shnredcare
GynGyn {mldwife)
Clynlmidwife
Gyntmidwlfe
Midwlfe/birth
center
GynGyn
GynGyn
CH- Sonja 2fl /O Gyn
Nbtes, Countrv: NL = the Nelhcr];mds; Sl.
Midwife = independent rnidwife; Gyn =
interviews: this number is referred to as (1),{
NUMBEROF T]MEDURINGINTERVIEWS PREGNANCY
2
1
3
1
1
1
1
1
1
1
1
1
1
1
1
1
3
1
1
1
1
1
1
2
1
1
1
1
1
1
2
(2} 30 weeks
1 6 weeks
26 weeks
11 weeks
34 weeks
33 weeks
29 weeks
29 weeks
30 weeks
24 weeks
32 weeks
33 weeks
8 weeks
30 weeks
36weeks
22 weeks
TIMEDURINGPOSTPARTUM
(1 ) 2 months
(1)6weeks(2) 16 months
(3) S years
2 weeks
8 weeks
1 year
5 months
S months
{1 ) 2 weeks
{2) 9 months
(3) 5 yenrs
5 months
6 months
8 weeks
5 inonths
(1 } 5 months
{2) 16 months
2 weeks
6 weeks
1 year
(1 ) 8 weeks
(2)3.5 years
REASONS FORTH[ORET)CALSAMPMNG
D[fferencesfirst-second
pregnancy
Verify/discusscategories
Verify/discusstheory
Medical care provision
lterative process in
subsequentpregnancies
Progress ot process
Process and medlca[ care
Variation in [ontrolAet go
Verify/discusscategories
Verifyfdiscusstheory
Different ca re provider
Different ca re provider
Process in first pregnancy
Process until1 year
Iterative process in subse-
'quentpregnancles
Verifyfdiscusscategories
Fema]e care provicler
Process ]n ti rst pregnan-
cy/ Gyn only
Process in first pregnancy
lterative process in subse-
quentpregnanclesVerifyfdiscusscategories
Process unti[1 year
" Scottand; CH = Switzerland; PIBtM = nvmber of prcBnancics, t}irths and rniscarriages; Care proyider:
gyneculog{st (in Switzerland: private practice}; Refbirth = referraL to the hospital during birth; Number of
?.).{3)undertimepregnancytpestpartuni.
/
/
... ,".' /O・,'w-.Mh.Edein-・Ntitt'・-

Becoming a Mother: VVomen's Journeys FFom Expectatl on tv Expericnce 'in Three European Countfies L"yben et ai. 17
1
L1
!
gi1
:
and identifying data werc removed. The researcher
herself performed the analysis in each of the languages
concerned. Analysis in each of the language units was
checkcd by the supervisors of the study.
Coding technigues, according to Strauss and
Cerbin (1998), were used, which involved open, axial,
and selective coding, }Vithin each of the language units,
the transcripts of the interviews were coded in a line-
by-line, and somctimes word-by-word, fashion. Codes
were collapsed into concepts and were given a name
in the original Ianguage, fitting the meaning given by
the women in the intervicws. SubsequentlF the con-
cepts that emergcd from the three separate language
units were compared between uiiits, translatcd, and
integrated in an overall cross-natlonal unit; resulting
in concepts at a higher abstraction level (Brtslin et al.,
1973). As a consequence, these concepts could be closely
examined again in a deconstructive way for similarities
and differences in each of the langua.aes, The results
from this examination provided criteria for following
theoreticalsampling.
During axial coding, categories were linked to each
other, renamed, and then, collapsed or subsurned into
larger categories through further comparison. Sclective
coding completcd the construction of the grounded the-
ory through the integration and refincment ofthe theory
at which point, theoretical saturation was achieved. The
final results efthis analysis were verified in an interview
ivith one woman in each of the countries,
RESUUI"S
Thetotalsamplecomprised39interviewswith32women.
TNvclve women were interviewed in the Nethcrlands, 1O
in Scotland, and 10 in Switzerland (see Table 1),
The participating women werc either expecting or
had given birth to their first, second, or third child. 'Ien
women had experienced previous miscarriages. lnterviews
took place in different stages ofpregnancy or up to 5 ycars
after giving birth to their chiIdren. The wemen received
care in difurent models of care by different care providers.
One single cross-national model for women in
three European countries emerged (Luyben, 2008),
which contained three main categories of "mother-
ing the mothcr;' [Ccreating a bond;' and "becoming
a mothez" This model, with its categories and their
relationships, is presented in Figure 1, This highlights a
process of carc that went beyond pregnancy to include
both childbirth and postpartum. On selective analysis,
"mothering the mother" appeared to be the core cat-
egory containing the content that women needed from
l
l
/
/
:
1f 'Iil ,geee
uewa
/"ms
Faniiliarizing
SharmgresponsTbtTity
Maintaimngautonomy Gaintngconfidencct
Methcringthemothcc
ettxeqt,;・i '
xesi" ai ・ ・ s Sptptee ''
$ss
1,.
li・)
eeW,ia
"'t
k }..,
.ta,/ /t'/'3yr
FIGURE 1 The model of content ofcare during pregnanc" childbirth, and
postnatal period that emerged from the study. "Bccoming a mother" describes
the maternal dcvclopmentprocess from the beginning of pregnancy until
approximately ] year after b{rth (J = dccrease, T = increase). The mediating
factor of"Creating a bend" (with care providers) effectively connects content
of caie (core category; "Ntothering the inother") with this process.
'11

gg
18 Becoming a Mother: Womcri's Journeys From Expectation to Experience in Three EuroE)can Countries Luyben et al.
,lithww[it i,,
,I,'Ill
ameesfiptrg,,,・
Developing awareness
Comparing
Balancing
Adapting
FIGURE2 Theprocessofbecomin
ii iifi[11iii,
tt
itlt///il it lt/t
t! !tijtl ll lt tl tlt
'' 'i;FII[ii
g a mother with its stag
e#l・l,///n
l.llli ig
'/t/i
i・llligllllli・li`
cs and properties,
maternit}r care. This core catesory subsumed the others,
whereas "becoming a mother;' described the maternal
development process and "creating a bond;' reflected
relationships with carc providers and the social envi-
ronment that women crcatcd to be able to receive the
content of care they needed to undergo "becoming a
mothen" effectiveLy.
This article describes the precess of "becoming a
rnotherr' It involved three stages of "expecting;' "familiar-
izing;' and "embarking on motherhood" (see Figure 2).
BECOMING A MOTHER
expectations of pregnancy3 childbirth, and their future
with a new famjly. The women thernselves were the first
to suspect a pregnancy because of missing a period or
perceiving bodily changes, and confirmed this by per-
fo rmm
g a pregnancy test at home.
I had donc that test; well I am pregnant and hip,
hip, hooray, Ykts, of course, you keep your mouth
shut the first3 months that I'd learn[ed] abit
about that, that you shouldn't sa}r too much the
first 3 inonths.
(Mariannelthe Netherlands)
The data suggested that for thc women in this study, sup-
port in the process of "becoming a rnother" should be
the aim of provision of maternity care, They described
becoming mothers as personal developmental journeys
from creating expectations in early pregnancy until
completing the expericnce durjng the postnatal period,
approximately a ycar after childbirth. These journeys
were iterative processes, which were repeated in subse-
quentpregnancics.1;romtheseprocesses,womengained
confidence and autonomy to take up family responsibil-
ity (see Figure l). "Becoming a mother" involved three
stages and started with the stage of "expectingr'
Expecting
The stage of expecting Iasted f'rom early pregnancy until
childbirth in which women diagnosed their pregnancM
became increasingly aware of themselves and their
pregnant situation, and, conscquently, created several
A few women consulted a known health careprovider to get an objective confirmation, Feeling sure
about being pragnant was an important condition for
inducing a process of increased awareness about their
new situatiDn to precede the process of becoming a
mother. NVDmcn in their first pregnancy described how
they opened up to things related to pregnancF which
was perceived as a new and exciting area.
Bccause it was, everything was new to me, it
was as if someone saying to me you're pregnant,
as if sorneone gave to me this big Christmas
prcsent, it was wonderfu1, and I wanted to know
all about it
(Heather/Scotland)
Becoming awa re was a requirement fbr Iearning and
personal development, and the creation of expectations.
F-'''-s'imts' 'e lj.

El
i・
1
1ii
i
1
L
/
1
/t
Becoming a /Viether: Women's )ourneys From Expectation to Experience in Three Eur()pean Countrles Luybef] etal. 19
It was also a condition for actively taking rcsponsibility:
This state of [nind was characterized by increased "think-
ing activities" in which different types ofknowledge, such
as knowledge about daily and family life, cxperiences of
pregnancy and childbirth, and views and beliefs, were
reflected on and comparcd. While prcparing for the
future, this dynamic proccss involved three stages of
interaction with the self ancl with the world: the present,
being pregnant, and having a new famil}c Lilian, in Swit-
zerland, characterized hcr current scenario, thus,
/....
tt t.
We]1, concerning the partnership, it is not
necessarily the simplest composition. And
I think, in regard to culture, my partncr has a
totally different background in regard to having
ahandicapped child. That is a different scenario '
that one is creating then. That Ihave the feeling
that, somehow, I mightbe standing quite alone
there. And, I could uot imagine it that way,
(LilianlSwitzerland)
Creatitrgapictureinvolvcdtheconstructionoffuture
scenarios('[expectations")atdifferentperiodsofpregnanc〉rand childbirth and having a family IXbrnen with previous
experiences used these for crcati g their pictures,
I actualry found this birth even rnore diMcult
than my first child, Whereas, I think, with the
aniount ofpressure and contractions Hiave had
right through my prcgnnncyl I was expecting an
easier birth but, in fact, it was even more diMcult /
(SusanfScotland)
XNlamen with no previous or with different experi-
ences (c.g., a twin pregnancy) created "foreign pictures"
with information from other women in their social envi-
ronment, brochures or books, and care providers; Iike
Mireille in the Netherlands who was told by her general
practitioner to visit a midwife and call a day care center,
Ijust wanted to know more about all the things
I had to do, And not just, that he talked about
going to the midwife, but also right away; 1ike,
take care that you call a children's daycare
centler]. And I suddenly thought iikc, gosh,
I just know that I am pregnant, do I already
have to cal1 aday care cent[erJ now?"
(pt{ireille/theNetherlands)
Because this search for information also created
anxieties, some women, Iike Sonja in Switzerland, chose
not to know too much,
All is, from A to Z, everything is really in there.
But, it can also drive you crazy: If one reads,
everything, The negative. You should not eat
this and that, And then this happens, and that,
and so en.
(SonjatSwitzerland)
These pictures were then used as a reference and
as something to hold on to during pregnancp as Erin, in
the Netherlands, stated,
Thus, you are creating a scenario, Because you
hear from people, like it has to go like that and
that. Normally And that, you like to have it Iike
that yourselq of course.
Finallyi you can hold on to that Bccause
you think, well, end of the pregnancy, you have
to give birth, a birth will be something Iike this.
And that is a picture. And then the rest will fo1-
lowl and that will be approximately like this.
And that is another picturc. Thus, therc you are
living towards that (picture). That is your, your
point to, to hold on to.
(Erin/theNetherlands)
These expcctations coiltained subjects that were
important to women; for example, mode of birth, atti-
tude of care previder, beins, at home with the bab}r,
and their environment Women in Scotland mentioned
a large number of subjects, whereas Swiss women
described enly fewL These cross-national differences
scemed to be related to the amount of information that
women had available or received from care providers,
Expectation pictures provlded women with confi-
dence,describedasafeelingofaninnersecurit}r(Luyben
& Fleming, 2005). A complete picture ofa particular set
of expectations brought women's thinking processes
about that issue to a halt and gave them peace of mind,
Most women, however, fbund gaps in the picture (such
as missing pieces in a jigsaw puzzle), which led to pei:-
ceiviug uncertainiies and continuation of the thinking
process. This was terrned "worrying" in which different
scenaries were considered, but the right `Efit" could not
be found. As women felt responsible, they aimed for a

-
r'
20 Becominga Mod]er: Women's Jeurnevs From Expectatlon to Experience '[nThree European Countries Luyberr et al.
reduction of risk and closing the picture with the best
scenario. Vanessa, in Scotland, considcred a home birth,
but also considered the risks to her own 1ife.
/tt ttttttt
I didn'L want to be in a situation where I was
going to put my own life at risk, 'cause that
would be worse fbr Robin, than, than a bit of
jealousy about this new baby,
(VanessalScotland)
As to counteract this sense ofuncertaint" al women
were needing experience that they usually found in a bond
with an experienced maternity care provicler (see Figure 1),
"Expecting;' however, was an iterative process of creating
expectations, which started all over again, ifnew informa-
tion arose. Women, therefore, searchcd this new experi-
ence through a continuity of the bond with their chosen
care provider (scc Figure 1). Thus, thcy aimed to complete
the pictures and restore their feelings of confidence and
autonomy (Luyben & Fleming, 2005), during familiarizing
themselves with the experience ofbecoming a mother,
Familiarizing
Familiarizing meant that women were getting acquainted
with the expericnce ofbeing pregnant, giving birth, and
having a family of one's own aftcr childbirth. Some
Dutch womcn talked about "feeling the reatityr' During
the time, women socialized to motherhood, the expecta-
tion pictures changed into experience pictures, and they
felt "at homc" with this exp erience, FamiliaritM thus, pro-
vided a fecling of confidence, which was refiected in the
SwissandDutchexpressionsof"beingfamiliar:'Expecta-
tions were cognitively built, whereas actual experienciug
involved all the senses, Although Nicole, in the Nether-
lands, was wel]-informed about being pregnant through
reading books and the additional information from her
midwife, her real experience was quite different,
Of coursc, you read sometimes that somebody
has an, an awfu1 pregnancs yes, though you read l'
that not that often. In booklets, is of'ten 1ike, how
great a pregnancy is. Also, if they, if' the tnidwife
is Iike, "o, those nice butterfies in your bellyr'
But well, at 3 o'clock at night, J do not think 1ike,
let's havc a nice play, Yles, that is just annoying,
Because that wakes me up. And T knew that all,
But now that you are really expcriencing that.
(Nicole/thcNetherlands)
Through their experiences, women were develop-
ing arvareness by creating new knowledge, which raised
questions and changed thc way they thought. This led
to the construction of ncw experience pictures, which
they were comparing with the existing expectatien pic-
turc, Joelle, in the Netherlands, compared the experl-
ence ofher secend child with what she knew from the
first one,
X"le11, for examplc, he moved an awfu1 lot {n iny
bellv I thought well, is that, is that normal? The
first one had been quite quiet, and this one, he
just halg kicked iny ribs apart,
(Joelle/theNetherlands)
Women tried to make a new experience fit their
existing picture through balancing both pictures of
cxpectation and experience to maintain equilibrium and
achicve a state of rest. 1'ime to discuss, as well as infbrma-
tion and reassurance from care providers, were factors
nceded to fil1 in missing knowlcdge, Paola, in Switzerland,
had professional friends who she could always ask.
I was luckyL Because I had my own relation-
ship$, I did not feel that unsure. That means
I had unsure, always had Ltnsure moments.
And those unsure moments, Ijust directly
compensated. That meansJ I called someone.
Someone, that I knew really well, a docter.
And there I got my additional informatioii, or
what I lacked. Or I kiiew a midwife.
(PaolalSwitzerland)
New information and experience led to the cxpec-
tation picture belng reconstructed, rejected, or neither,
which led to worrying by the women, XMhile Megan, in
Scotland, chose not to worry about information from her
care provider who thought she was `"small" and expected
her to have complications during childbirth, Marcn's, in
thc Nctherlands, worries increased after giving birth.
Well, my nature is, 1 don't }vorry about that.
I know in other countries, females are much
smaller than I am, and they stil1 have had the
babies. And 1OO years ago, people were much
shorter than they arc now. So, well I don't worry
(Megan/Scotland)
,.b'.;--'・Wttts・・

Lilltl
/
:!
1
i
'
l11
;
:lt
'
1
/
/
/
:Il
l
l
E//
:
/
L
:
'
p
Becom]ng a Mother: Women's journeys From Expectation to Experience in Three European Countries Luyben etal, 21
And then suddeniB you have that worrB like oh
god, now you also have such a child. What do
1 do with it? Yes, you have to look after it the
whole time, Is she laying down well, yes, you are
quite nervous, And Iike now, it alljust goes welL
Aftcr a few months, then it al1 is familiar and,
yes, I found it quite scarM
(MarenltheNetherlands)
Balancing, resulting in a ncw developed picture
ef experience, and subsequently adapting, was a nec-
essary activity to achieve personal growth, which
gradually took placc. In this studF womcn having
their first child wcre most affected by this change,
whereas women having a subsequent child experi-
enced more stability Marianne, in the Netherlands
(second pregnancy), and Lea, in Switzerland (after
having her second child), reflected on their personal
changes in becoming a mother.
And if you go for the first, first time, for your
first baby, you are just a ]ay person in that
area. The further pregnancy proceeds, the
more, the more you comc to know, actually.
And now you are, well I won't say an expert,
but you just know an awful lot, maybe eyen a
bit toe much,
(MariannettheNetherlands)
Ybu have to develop a new familiarit}r in your-
sclC because it is a process, you do not know
yourself an)rmore. Ybu have to learn to kt)ow
yourself again. Define new. Yes, you have to
rcally open your eyes,
(LeafSwitzcrland)
During familiarizing, thc bond with more expe-
rienced people, particularly carc providcrs, assisted
women to complete their picturcs of experience to
gain confidence, while maintaining their autonorny
and sharing responsibilit〉T (see Figure 1). The pro-cess of familiarizing was repeated, if new experi-
ences happened. Women, howevcn hardly had time
to adapt their pictures during childbirth and the early
pestnatal period, Therefbre, reflcction and reconstruc-
tion had to take place during the stage ofembarking
on motherhood.
Embarking on Motherhoocl
1[he aim of women's journeys was t[emhatking on moth-
ethood" in which they reflected on their experience,
reconstructed and c]osed their pictures, so that they could
begin the enterprise ofbeing a mother, "bmen, therefore,
had to leave the journcy of "becoming a mother" behind
them physicallB psychologicalIF and emotionally This
stage started some time after chj]dbinh, when women had
a new Iife routine, and ended only after conipleting their
picture approximately a year after birth, but sometimes
longen For Lynn, in Scotland, this process involved three
pregnancies and was related to mccting her expectations.
/ttt
I've come, I've come fuII circ]e. I've got to thc
point where I thought I would be embarking on
motherhood, I suppose my expectations have now
been met. And, it's happened the way I envisaged.
BtLt, it's taken Tne quite a long tirne, a few )rears, to
get to that point It has been a big journeB but I'm
there. I won't. I don't think kvill have any more,
(l;ynntScotland)
While Scottish and Dutch women chose the word
"embarking;' Lea, in Switzerland, preferred a journey as
a metaphor,
Wbll,Ithink that is also, that is, those (bccoming
and being a mother) are two different pair[s] of
shoes. And, I believe, the bigger journey is after-
wards. If the child is there and, then, you are a
mother. Now for me, that with that ship, I would
take a country road. 1・Vhatever; train, bic)rcle, car.
(LeaiSwitzcrland)
In having a routine, women experienced a new
normality in their ever}rday situation, They felt secure
in being with and caring for the babM and experienced
an increascd stability in their Iife. After having her third
babB Holly; in Scotland, had more dithculties finding
this routine than with her first one.
lBut I start to get into my routine and everything
noLsr, T think, because I had, yoti know, I had, my
oldest son to get to nursery. And, I had a, al1 ofa
sudden, I had a new babM a toddler, and a 4-year-
oLd, having to get 1iim up, readyL And I would saty;
J, I felt it more this time, that way Than I did, I
mean, the first, your first prcgnancy
(HollyfScotland)

22 Becoming a Mother: Women's Journeys :'rom Expectation to Experience in Th[ee Eurepean Countries l.uyben et aL
The time needed to find a new routine difft]red
individually and rclated to women's own well-being and
the behavior of the baby Once a routine was achicvcd,
there was a resulting sense of peace and harmony
Women had time to reflect, which they did not have
during childbirth and the early postnatal period. During
this time, they could reconstruct their picture and fiLl in
gaps in their awarcness.
Yl)s, when did I start to do that? I think, that
after, yes, really after a rnonth, that all went well
a bit again, I think, a month of three, four, that
I thought 1ike, gosh, yes, how did it aU go actu-
ally? And does it al1 fit with, Iike what you had
in your heacl a bit, and, also cverything after
that, reall" like, that you are going to work, and
how you expericnce that, and if it is a bit like,
how you have thought it would be.
CErinltheNetherlands)
Some women relied on their shared awareness with
the care providers with whom they had a bond to debrief
them and help them fi11 in the missing pieces to complete
their osvn awareness. Thus, the experience could be under-
stood and integrated, 1ike what Maren had aimed to do,
I harte missed that. It all went very fast, they
(health nurses) came to check me, everything
was fine, Goodbye, gone, I had needed more
from that. Just, some time to taLk with you, how
the birth has taken place. Ybu have so rnany
questions coming up at once, and you can not
deal with that in the first coupLc of days, I could
could not process that,
(rv{arenl the Netherlands)
After reconstruction, women wcre matching their
actual experience with the expectation, and judging it
While reconciling, women came to t/
aspects of their experience, which had not
expectations. This meant that they ha(1
some aspects of their expectations that w
to them, and deal with the loss ef som(
was a balancing activity as described b'
Scotland.
[ think as well you have to balance yc
your perception of how it is going to
the reality of how it did go and kind
to an understanding between the twe
I know that it causes women after thc
lot of kind of psychological problemE
nevcr had a natural birth and there iE
intervention, you know.
(Hcathe
SeveralwomenexperiencedamisrT:expectations and experiences. In thc c
this was often due to antenatal inforrr
they had themselves or from family, fri
providers and had been used to creatc
pictures in "expecting." A few women r
negattve feelings regarding the experi(
complaining, either orally or in writin!
women wrote a letter of complaint, ai
tish woman had considered this. Al
related to the attitude of care provic
however, women altered their expectati
realitv Therefore, although some aspe/
"missed," they generally expressed sati/
the experience.
Consequentls closing the picture al]
to leave the experience behind, so that t
fbr new experiences of being a mothcr
was reused as a reference for creating nc
expectations in a subsequent pregnancy I
Netherlands, closed her picture after tall
midwife.
Andthen comcs the postnatal period. That wil1
be somethh]g like that. And if the picture indeed,
does not match, then you feel, I think, very disap-
pointed, And, if that picture matches, then you
are very happy And my picture matched coinci-
dentdly; But I had ever}rthing really perfect. I havc ・
had a good birth and a good postnatal period. ,
(ErintNetherlands)'
But I could still ask that knd of qucs
then. And that was very impertant to
get the picture complete, Tb get the q
answered, So thatI could leave it bch
it did notmove about in my mind, Ii]
have done that, or if I had done this,
(Kerstinlthe N/

:1
Li
4
1t
1
11
i
/
/
1
/
/
ii1
'
1
L
,
1
1
l・
'
11
e
Bctc/oming a MaTher: Wemen's lvurneys From Expectation to Experience in1hree European Countr]es tuyben et al, 23
Several women in the current study, however,
could not completely close a previous experience, like
Deborah, in Scotland, who reflected on her first experi-
ence duri ng her second pregnancM
Maybe for a ctosure, what [ should have done
was, make an attempt to write a letter of' com-
p!aint about what I felt was wrong with my
care. But I am not very good at getting around,
sort of these kind of things. So,Ijust, so I
probably have taken it with me. Some part ofit '
is closed, and over with, But some part is stru
there, you know.
(DeborahlScotland)
This issue ofnonclosure was not explored further
in the current study/ Through cLosing, women feIt con-
fident to take up family responsibility on their own, and
physically and mentally moved on inte the new experi-
ence of being a mother,
DISCUSSNON
The cnrrent study resulted in the emergence ofone single
cross-nationalconceptualmodelof"becomingamother"
for all women in threc European countries as an aim ef
provision ofmaternity care, From the wemen's perspec-
tive, this highlighted the importance of the development
of women's pictures ot' family responsibility and offered
new perspectives on existing maternity care 1(nowledgc
and pra[tice, The study showed that the grounded theory
approach provides a rigorous frameworl〈 for cross-national research.
Limitations that were encountered wcre mainly
caused by organizational and ]inguistic factors. Becausc
oflimitations in time and financial resourccs, the num-
ber of woinen per language unit had to bc planned in
advance, and not all interviews could be analyzed before
the next interview to()k place in each of the countries,
[lb adhere to the principles of grounded thcorM field
notes werc used to assist data collection. Thc inclusion
ofthree different languages, en the other hand, required
a very detailed analysis within each unit and the use of
concepts at a higher abstraction lcvel for cross-national
comparison, The intensity of this process influenced
the number of women and thc amount of time needed
to achicve the objcctives and, thus, saturation of the
categories. Using concepts at a higher abstraction level
increased the credibility of qualitative cross-national
interpretation, as meanings were validated in each of
the language units befbre being integrated. At the same
time, thcoretical sampling was riche4 as the meanings of
these similarities and differences for the women could
be explored in more depth and verified in thc interviews
in each of the countries involved.
The model of"becoming a mother" jn the current
study described a continuous process of women's per-
sonal development from expectation toward the expe-
rience of their own farnily responsibilityl which lasted
from thc beginning of pregnancy to about a year after
birth and was repcated in subsequent pregnancies.
This process consistcd of thrcc stages of changes in
women's scenarios (or "pictures") in which they changed
physically and emotionallM as did their vicws on their
existing world. This process showed paralleLs with a
socialization or acculturation process (Gudjons, 2003).
Previous studies had addressed only fragmented parts
ofthis process, such as the expectation before and expe-
rience after childbirth (A}rers & Pickering 2005; Green,
Coupland, & Kitzinger, 1990, 1998), becoming a mother
in the iast trimester of pregnancy and the postnatal
period (Martell, 2001; Mercer, 1995; Rogan, Schmied,
Barclayl Everitt, & Wyllie, 1997), or several tasks since
becoming a mother (Merce4 2004; Nelson, 2003; Rubin,
1984). The continuous proccss, as described in this
studM involved a time frorn early pregnancy to a year
er more after childbirth, included women's social world,
and connected expectation to experience. 'Vhis also led
to a different perspective on the meanings of some of
the findings from these previous studies. For instance,
Barcla" Everitt, Rogan, Schnied, and Wyllie (1997)
interpreted "loss" in the early postnatal period in a
negative waF but th is was a normal phenomenon during
reconcitiation within the context of women's transfor-
mative processes in the current study The continuous
social character of these processes highlighted the need
for continuity of the care providing process and involve-
ment of women's social environment in the design and
provisionofcare.
The transfbrrnation of pictures of expectations
into pictures of women's own expcriences of becoming a
mother resembled a biographica], experiential Iearning
precess (Piaget, 1975; Strauss, 2005). Women first expe-
rienced the transition, which generated questions. The}r,
then, sought personal information that assisted them in
developing arid closing their pictures, while sharing this
withtheircareproviders,Closurebroughtpeaceofmind,
even if it was only temporarM until the next disruptive
eventorinformation.]iffectiveprovisionofinformation.
therefbrc, had to be cxperience- and time-related, Thesc

'
24 [lec/oTTiinB n Mother: Women's Iourneys From Expectatlon to Exporicnce in Three European Countrics Luyben et aL
findings arc consistent with the effects ofprovision ot'
information reported in other studies. Several studies
showed the limited effects of antenatal education and
information in preparing womcn fbr being a mother
and emphasized the need for increased information
in the postnatal period (Ho & Holroyd, 2002; Nolan,
1997; Razurel, Bruchon-Schweitze4 Dupanloup, Irion,
& ]tpiney in press), whereas Lcvy (1999) described how
womcn acccpted and rejected information to preserve
the balance in their own world. The results of the cur-
rent study suggest the need for an increase in postnata!
education, but even more for individualized, timely care
packages that rnatch womenis own unique experience
and requirements, and that arc focused on "becoming
mother" and not just on well-being, from a purely
clinical perspective. In this waF a close match between
expectation and experience could bc achieved,
A few researchers have highlighted the irnpor-
tance of women's reconstruction of their pictures in
the postnatal period in which fi11ing in the "missing
pieces" during the postnatal period facilitated women to
reconstruct their childbirth experience (Affbnso, 1977;
Mercer, 1995). Although the importance of closing the
expcricnce to continue liying in a new situation has
been cmphasized (Affbnso, 1977), these findings had
not been related to a continuous process of opening,
sharing, and closing awareness that already startecl in
the beginning of pregnancy as described in the current
studv When maternity care providers assisted women
in completing their pictures, cLosure provided them
each time with confidence, and, thus, an inner securityl
to go a step toward family responsibilityL
wriereas security is well-rccognized as meaning to
reduce anxieties (Melender & Lauri, 2002), most studies
emphasized external sources, and little has been described
about inner sources of security (1";ndress, 2002; Melender
& Lauri, 2002; Petermann, 1996). Erikson (1966), how-
evcr, mentioned trust and rcliance on oneself as a source
ofinncrsecurityduringpsychosocialdevelopment,which
is consistent with the findings in the current studv
Because of the closed pictures cluring the course of the
process ("expectations"), women gained confidence and
were able to express this particu]ar preference and make
decisions in an autonomous way (Luyben & Fleming,
2005). If women stayed uncertain because of conflicting
information, risks, or complications, howeve" they were
likely to rely on their care providcrs and the choices theY
madc. Because this issue was not explored further within
the framework of the current studM further research is
ld. , ,. , ,1 .." .. .../,
Final closure ef the picture of becom
took place at the end of the process, whe[
ence could be left bchind to embark on
of rnotherhood. Although women had c]
minds during the process, they had a fixed
view about their experience after its closu
of the experience involved comparing th
with the expectation. As a result, women
expectations to match rcality and reconcilc/
Thus, they were usually satisfied with th
(e,g,, healthy mothcr, healthy baby) but also
aspects in relationship to their expectations
mode of birth), which has been noticed in
(Bramadat & Driedge4 l993; Porter & Ma`
Proctog1998).'1'hesefindingsindicatethat
care during pregnancy and childbirth, firs
ask for women's satisfaction, but for what
and, second, they should take place only
of the picture. ConcurrentlB "becominJ
provides a basis for development of indicat
ation of this proccss by describing aims, p
outcomes from women's points of view
CONCLUSION
In this article, the subcategory of"becomi
arising from an invcstigation of importa
provision of routine antenatal care from w・
of view in thrcc European countries v
maternity care systems, is described. One s
tual cross-national model for women in tk
emerged, which rcpresented women's jou
family responsibility from creating expect[
pregnancy to cornpleting the experience E
one year after birth. 'I'his rnodel resemb!・
ential learning proccss in which women I
emotionally changed, as did their views on
world. The bond with a maternity care pro
women to reccive the content of care th
complete this process and, thus, create E
between expectation and experience,
Provision of maternit〉F care shouinclude principles of experiential learni
women's process of becoming a motherown social world is a central aim. Support
include sharing care-providing relationshi
of this care during women's processes, an(
of women's indlvidual social worlds. ThE
AL-..11 LA -lm- :--n Apfitt-""- wT-;ln Anp:m

:
Ei]
lL
/
:
,
÷
1
11
11
1
11
i
:
g/
:1
/
/
!
ti
11
!
s
i
11
'
'
i
1
llecoming a MoL[ior: Womcn's Journeys Frotn Expectation to Experience in Three Eurepean Countries Luyben et al. 25
REFERENCES
Affbnso, D, D. (1977). `iMissing pieces": A study ofpostpartum
feelings. Birth and the 1・'amily fournal, 4(4), 159-164.
Ayers, S., & l'ickering, A, D, (2005), }Vt)men's expectations and
experience of birth. Rsycholqgy and Hbalth, 20( 1 ), 79-92.
Barclay, L., Everitt, I.., Rogan, F,, Schmied, V., & }V}rllie, A.
(i997). Becoming a mother-an analysis of womcn's
expericnce of early motherhood. journal of fldvanced
Nttrsing, 25(4), 719-728,
Blume- H. "998). Symbotic interactionistn: Perspective
and triethod (Renewed). Berkelev; CA: University of
CaliforniaPress.
Bramadat, I, J., &Driedger, M. (1993), Satisfaction with child-
birth: Theory and development. Birth, 20(1), 22-29.
Brezinka, C, C1997). Schwangerschcijl in Osterreich, iUfediLHin,
l(bstenrechnung und SoziaLgesetagebutrg in der Schwan-
gerenvorsorge, Gebttrt ttnd Karenzzeit [Pregnancy
in Austria. rvtedictne. costs and social legislation in
prenatal care, birth and postnatal period]. Konstanz,
Germany: Hartung-Gorre Verlag,
Brislin, R, MC, Lonne4 W J.. & 1'horndike, R. M. (1973).
Cross-cultural research methods. Compc;rative studies in
behavioralscieJtce. New Ybrk, NY: John Wilcy & Sons.
Cochrane, A. (1999). EZtfbctiveness and efliciency, Random
reflectionsonhealthservices(Reprint).London,England:
Royal Society of Medicine Press.
Endress, lvl. (2002). Vlertrauen E"ust]. Bielefeld, Germany:
TranscriptVertag.
Enkin, tvl., & Chalmers, I. (19g2). I!fflectiveness antl satiEfhc-
tion in antenatal care. London, England: Heinemann
rvledicalBooks.
Erikson, E. H. (1 966). Jdentitht undLebansayklus [IdenLity and life
cycle], Frtmkfurt am Main, Germany: Suhrkamp Verlag.
Field, ll A, (1990). Efll,ctiveness and eMcacy ofantenatal care.
Mid,v ijLiry, 6, 215-223.
Fink, A., Yano, E, M., & Goya, D. (1992), Prenatal programs:
What the literature reveals, Obstetrics and Gynecology,
80(5), 867-872.
Gales, L, M. (2010). Linguistic sensltivity in cross-cultural
organisational research: positivist, post-positivist, and
groundcd theory approaches. Langttage and bitercttl-
tural Communication, 3(2), pp, 131-140.
Garcia, J. (1982). Women's views on antenatal care. In M.
Enkin & I, Chalmers( Eds,), Iltibctiveness and satiofbc-
tion in antenatal care (pp. 81-91). I.ondon, ISngland:
Heinemann Mcdical Books,
Glascr, B, G. (197S). 71heoretical sensitivity: Advances in
tPte methodelogy of greiinded theory. Mill Vlalley CA:
SociologyPress.
Glaser, B. G., & Strauss, A, L. (1967), The discover〉, qfgrounded theot)t: Sttntagies for qualitative tesearch. Chicago, II.:
Aldine Publishi"g.
Graham, H., & OakleF A. (1981). Competing ideologies of
reproduction: Medical and maternal pcrspectives on
prcgnancr In H. Roberts H. (Eds.), Ltlotnen, health and
mproduction(pp.69-74).London,England:Routhledge
& Kegan Paul,
Green, J. M., Coupland, V A,, & Kitzingc4 I. M (1990). Expec-
tations, experiences, and ps〉tchological outcomes of childbirth: A prospectjve study of 825 women. Birth,
17(1), 15-24,
Green, J. M., Coupland, V: A,, & Kitzinge4 J. V (1998). Great
expectations: A prospective stucty of women's expecta-
tions and experiences (if childbirth. Cheshire, United
Kingdom: Books for Midwives Press.
Gudjons, H. (2003). Padagogisches Grtindwissen [Pedagogical
basis knowledge] (8th cd.), Bad Heilbrunn, Germany:
Vi]rlag Julius Klinkhardt,
Hall, M., Macintyre, S., & Porte4 M. (1985). Antenatat care
assessed: A case stucly of an innovation in Aberdeen.
Aberdeen, United aungdom: Abcrdeen University Press.
Heringa, M, (I998), Computer-ondersteunde screening in de
prenatale zorg [Computer-aided screening in antenatal
care] (Doctoral thesis). Univcrsity of Groningen.
Grontngen; Dijkliuizen Xlan Zanten bv.
Ho, I., & Holroyd, E. (2e02), C]hinese women's perceptions of
the effectiveness of antenatal education in the prepara-
tion for the motherhood. journal qfAdvanced Ntirsitrg,
3S(1), 74-85,
Jacoby, A., & Cartwright, A. (1990). I:inding out about the
vlcws and experiences ofmaternity-service uscrs, In J,
Garcia, J. Kilpatrick, & M. Richards (Eds.), Ilie politics
of materrtity care services for childbearing women in
20th centurLy Britain (pp. 239-2S5), Oxfbrd, United
Kingdom: Oxfbrd University Press,
I.ev}r, V. (1999). Maintaining equilibrium: A grounded theory
study of the process involved when women make
inforrned choices during pregnanc}L MidtvijZiry, 15(2),
I09-119.
Luyben, A, G, (2008). Mothering the mother: A stttcly of
qLfective content of routine care during pregnancy Jfom
ivomen's points oj' view in three European countries
(Unpublished doctoral thesis), Glasgow, UK: Glasgow
(]aledonian University:
I.uyben, A, G., & Fleming, Y E, M. (2005), Women's needs
from antenatal care in three European countries.
Mid,vdery,21(3),212-223,,
Martell, I- K, (2001), Hcading tovvard the new normal: A con-
tcmporary postpartum cxperience. fournal ofObstetric,
(lynecologic, and Neonatal Nblrsing, 30(5}, 496-506.
26 Becoming a Mother: Women's Journeys From Expectation to Experience in Three European Countries Luyben et aL
Melende4 H. L., & Lauri, S. (2002). Experiences of security
associated with pregnancy and childbirth: A study
of pregnant women. Jnternational journal of Nursing
Practice, 8(6), 289-296.
Merce4 R. Z (1995). Becoming a mother. New Ybrk, NX
SpringerPublishing,
Merce4 R. 1: (2004). Becoming a mother versus maternal
role attainment. fournal of Nursing Scholarship, 36(3),
226-232.
Nelson,A,M.(2003).1[tansitiontomotherhood.journalqfObstet-
riq (lynecolqgi'q and jVbonainl Mrsingl 32, 465-477.
Nolan, M. (1997). Antenatal education-where next? journal
ofAdvanced NLtrsing, 25, 1198-1204,
OakleB A. (I982), The origins and development of antenatal
care. In M, Enkin & I. Chalmers (Eds.), Ilt7lactiveness
and satiEfaction in antenatal care (pp. 1-21). London,
England: Heinemann Medical Books.
Petermann, E (1996). Rsycholqgie des lilertrauens [Psychology
of trust]. G6ttingen, Germany: Hogrefe Verlag,
Piaget, J. (1975), Das Erwachen der intellgenz beim Kinde
[The awakening of intelligence in the child]. Stuttgart,
Germany: Ernst Klett Verlag.
Porter M,, & Maclntyre S, (1984). What is, must be best: A
research note on conservative or deferential responses
to antenatal care provision. Social Science Medicine,
19(11), 1197-1200.
Procto4 S, (1998), What determines quality in maternity care?
Comparingtheperceptionsofchildbearingwomenand
midwives. Birth, 25(2), 85-93.
Razurel, C,, Bruchon-Schweitze4 M,, Dupanloup, A., Irion,
O., & Epiney M. (in press). Stressfu1 events, social
support, and coping strategies of primiparous women
during the postpartum period: A qualitative studv
Midwijiiry,doi:10.10161j,midw;2009,06.005
Reid, M., & Garcia, J. (1989), Wbmen's views of care during
pregnancy and childbirth. In I. Chalmers, M. Enkin,
& M, J, N, C, Keirse (Eds,), llt7lective care in pragnancy
and childbirth (pp. 131-142). Oxford, United Kingdom:
Oxfbrd University Press.
Richardus, J. H., Graafuians, IM C, van der
M,,Amelink-Verburg,M.R,Verloove-i
Mackenbach, J. R (1997). An European
investigatingthevalidityofperinatalm
come indicator for the quality of anten
care. Jburnal oj'Perinatal Mbdicine, 25, ,
Rogan,E,Schmied,XC,Barclay;L,Everitt,L,,&
Becoming a mother: Developing a ne'
motherhood, journal ofAdvanced Nitrs,
Rubin, R, (1984). Mbternal identity and the
ence. New Ybrk, Nth Springer Publishfi
Strauss, A. L. (1999). Qualitative analysis jZ
Reprint. Cambridgq England: Carnbride
Strauss, A. L. (2005). Mirrors and masks: 11h
tity, New Brunswick, NJ! 1[hransaction.
Strauss, A. L., & Corbin, J. (1998), Basics qfqt
nchniques and procedures for devE
theor), (2nd ed.). Thousand Oaks, CA/
VillaB J., Carroli, G., Khan-Neelofug D.,
Gulmezoglu, M. (2001). Patterns of
care for low-risk pregnancv 11he Cot
Oxford: UPdate Software, Ltd.
Wbrld Health Organization. (1987). Hbving ,
Reportonastucly,PublicHealthinEurop
Denmatk: WHO Regional Othce for Ei
Correspondence regarding this article sh,
to Ans G. Luyben, RM, PhD, Department
Uriiversity of Applied Sciences, Murtenstra
Bern, Switzerland. E-mail: [email protected]
Ans G, Luyben, RM, PhD, head of Research
ment MidwiferF Department ofHealth, Ber
of Applied Sciences, Bern, Switzerland.
Sue R. Kinn, BSc, MSc, PhD, team leader an
manage; Department for International Dev・
United Kingdom.
Valerie E, M, Fleming, RM, MA, PhD, Inter.
Consultant for Nursing and Midwifery GIas

Il
L
r
LF
1
I
!1
,
General Practitioner Involvement in Remote and
Rural Maternity Care: Too Big a Challenge?
fan CaldoMl Slanora Hundlq)4 Edwin van [llaijlingen, Jbhn ReicL
AZice Kige4 fanet 71icke4 lilly Irelana Fiona Elarris, Jane Flarme4 and
Helen Btlyers
/
r
1
/
lt
i/
it
1
i
:
BACKGROUND: In the United Kingdoin, general practitioner (Gl') involvement in maternity care has
declined significantly over the past decade. This is particularly so in remote and rural areas where mid-
wives haye stepped up and taken over units to ensure that women in these areas continue to have a ser-
vice. A recent report by the King's Fund argues for a greater role for the GP in maternity care provision;
howcver, this raises questions about whether GPs have the sl〈ills and training to provjde such care.
AIM: 'fo explore the views of GPs on the skills and training required to deliver safe and appropriate
local intrapartum seryices in reniote and rural settings.
rvlETHODS: ]vlixed-method stud)r consisting of qualitative interviews wlth a purposive samp]e of GPs
in six remQte and rurat sites. Tb triangulate the intcrview findings and identify features that might have
been missed in the interviews, a questionnaire was developcd using initial key themes identified.
FINDINGS: Maternity care accounted fbr lcss than 1O% of most reniote and rural GPs' workload, yet
interviewees reported that their i'ole required them to be competent in a wide range of procedures. This
was seen as a major barrier to recruitment and retcntion in rural areas. Although selfreported competence
and confidence was high, several GPs felt cle-skilled and feIt that they were fighting a losing battle to main-
tain skills. GPs regarded iso}ation, need for comprehensive expertise, limited resources, and transportation
diraculties as factors afflecting the decline in their contribution to remote and rural matcrnity carc.
CONCLUSION: Although rural GPs and midwives might traditiona]ly have been in competition, pro-
viding a woman-centered service in remote areas may be easiet to achieve throLigh collaborative workins.
Howcver, if GPs are to play a grcater role, then they will need to be prepared to make a strategic com-
rnitment to the maintcnance of remote and rural maternity care. This wM require innovative methods
of training, special consideration ofeducational needs, and incentives for pracLitioners to settle in rural
areas, but it rnay already be too latc for GPs to have a substantial input into maternity [are.
KEYwaRDS: general practitioncrs; mulLidisciplinary education; midwifery; maternit)r care; remote
and rural setting
:
INTRODUCTION
Although midwives in the United Kingdom attend
morc than half of all births and provide most of the
maternity care (Health Commission, 2008), particu-
larly where xvomen have uncomplicated pregnancies
(National Health Service [NHS] Qualiry Improvement
Scotland, 2007), the role that gencral practitioners (GPs)
play has recently been put back in the spotlight with the
publication of a ncw report by thc King's Fund (S[nith,
Shakespeare, & Dixon, 2010), The report argues for a
greater role for GPs in maternity care, one which might
see them sharing wemen's care with midwives, and
concludcs that changes to medical training are needed
JNTIInNATVObtAL JOURNAL OF CHtLDB"ATi-i Vbiume 1, issue 1. 201 O @ 2011 Springer Publi$hing Company, LLC www.springerpub.com DO[:10,1891i2156-5287.1.1,27
"totp' Ctbtt--.
・,l (:ifN[:,
ef -/a:L-"

28 Genera[ Practitioner [nvolvement in Remote and Rura[ Maternity Care: Tbo Big a Chal[enge? Caldbw et al.
to ensure that GPs are "adequately skilled to look after
women safely" (Smith et al., 2010, p. 19). In this article,
we explore GPs' skills and training, and ask the question,
"Is GP involvement in remote and rural maternity care
too big a challenge?"
BACKGROUND
Smith and Jeweil (1999) have reminded us that "com-
plete obstetric care" was very much the role of the GP at
the beginning of the 20th centurs with more than 85%
of women in the Uhited Kingdom birthing under GP
care. The push to move maternity care, and birth in par-
ticular, into facilities was a major factor for declining GP
irrvolvement. ,By 1995, only 18% of GPs surveyed pro-
vided intrapartum care, although 28% wanted to do so
(DeVties, Salvesen, Wiegers, & Williams, 2001). A more
recent study found that only 7% of GPs had attended a
birth within the year (Hewison, 2001). Involvement in
routine antenatal and postnatal care continued to be
much higher at more than 90% (General Medical Ser-
vices Committee, 1992), although in more recent years,
this too has declined (Smith et al., 2010).
In contrast, in remote and rural Scotland, GPs con-
tinued to maintain an intrapartum role for much longer.
Maternity care was often provided in GP units within
district hospitals, although these units also came under
threat in the late 1980s and early 1990s (Murphy-Black,
1992). Early in 1990, there were 65 small GP-led mater-
nity units in England (Smith & Jewell 1991, p. 14) and 28
such units in Scotland with its large rural area but much
smaller population than England (Scottish Oence Home
and Health Department, 1993, pp. 59-61). In Scotland,
the number of all maternity units (i.e., from the largest
academic hospitals to the smallest cottage hospital) fe11
from 52 units in 1995 to 38 in 2008, a drop of 26.9%,
whereas the overail number of births in Scotland over
the same period dropped by only 6,2%, from 60,261 to
56,537 (Information Services Division, 2010).
Changes in service provision and policy at the begin-
ning of this century led to a decline in births in remote
and rural settings (Department of Health, 2003; Scottish
Executive Health Department [SEHD], 2002; Scottish
OMce Department of Health, 1998). Maternity service
prevision was affected by the centralization of obstetric
and anesthetic services in tertiary units (Department of
Health, 2003; Mungall, 2005; SEHD, 2002). This central-
ization, combined witli a decreasing inyolvement of GPs
in intrapartum care (Smith, 1997), meant that many rural
maternity units closed altogether or became midwife-led.
Although the Royal College of General Practitio-
ners (RCGP) and the British Medical Association (BMA)
have both stressed the importance ofpersonal, continu-
ing, and comprehensive care provided by a primary
care maternity team, the BMA has reported a general
withdrawal of GPs from intrapartum care (BMA, 2007;
RCGP Maternity Care Group, 1995). With GP involve-
ment in intrapartum care under threat from falling
birth rates and the centralization of maternity care, the
2003 contract for general medical services removed GP
payments for maternity care, further reducing the likeli-
hood of GP input (The NHS Confederation, 2003).
At the sarne time, the Expert Group on Acute Mater-
nity Services (EGAMS) in Scotland developed a list ofcore
ski11s and competencies that were considered essential for
professionals to have C`to provide effective and safe care
for low-risk women and to manage obstetric emergencies
within remote and non-specialist units" (SEHD, 2002,
p. 22). These are listed in Box 1. The SEHD commissioned
us to conduct a scoping exercise of remote and rural
health professionals involved in maternity care in Scotland
to explore staffviews on the skills and training required to
deliver safe and appropriate local intrapartum services in
rernote and rural settings (Kiger et al., 2003; TUcker et al.,
2005). Within that studF interviews were carried out with
a Iarge number of health professionals, including GPs.
This article situates the GP interviews within the context
of the larger body of data and specifically explores koy
issues raised by GPs workng in those settings,
METHODS
This mixed-methods study comprised a qualitative and
a quantitative stage incorporating GP participation as
follows:
1. Interviewstage
A purposive sample of 10 GPs was identified through
midwife managers at 10 study sites selected following
a telephone census of the 32 rural and remote deliyery
units in Scotland. Each GP was sent an appointment
letter and informadon about the preject. Interviews
toekplaceatanappropriatelocationandlastedfrom15
to 60 minutes, the majority taking 30 to 45 minutes.
An interview schedule, informed by literature
review and experience within the project team and
an advisory group, was designed and reviewed for
content validity (see Box 2). Piloting was under-
taken (van Tleijlingen & HundleM 2005) and minor
amendments were made in response to feedback
,...,.,・1・11,wh・"・-・tw・・・ -

1'
:
1 General Practitioncr lnve[vement in Remote and Rural Meternity C[ire: foo Big a Chal [enge? Caldbw et aL 29
e
[
t
L
1
'
r
t
41
/
l
1
11
!
1
BOX1 CoreSkillsorCompetenciesIdentifiedby
Expcrt Group on Acute Maternity Services as Necessary
for Staff Providing Intrapartum Care (Skills included in
the guestionnaire are shown in bold italic)
. Management ofnormaf defivery---supporting normal
[abor ancl ch"dbirth
. Clinicaifucigment and decision-making skills
. Maternai histor,v taking
. Cbunselingandcommunicationskits
. Riskassesstnentnndmanagementskills
. Intravenous aV7 cannulation
. Managing IV fiuld replacement
. Management ofantepartum hemorrhage
. Managementofcordprolapse
. Manngementofshoulderclystocia
. Management ofhreeeh deliverr
. Management ofpostpartum hemorrhage
. Adult resuscitation
. Basic obstetric life sapport
. Neonatal resuscitation-assess, resuscitate, and stabilize
the neonnte prior to ongoing management
. Repair ofperineal trnun]a
. ilain management
. Initial and discharge examination of the newborn-
inspection and detailed examination of the baby
. Prcscn'ption ofch'ugs-such as analgesie in ]abo- drugs
used [n resL]scitation, and those invo]ved in normal
childbirth such as Konakion and anti-D.
Additional competencies required fer remote units-should
be achieved by at least one team member:
. Uttrasonicscanning
.. . Ungertaking.a ventg.use lift-gut de.liyerr
2005), Thcse infbrmed the design ofthe questionnaire.
Second, a full manual analysis ofthe transcribed inter-
view data was carried out, Each transcript was read
and analyzcd by at least two of the authors.
2, Questionnaire stage
Questionnaires wcre sent to the 10 GPs who had been
selected for interview and an additional 8 GPs from
matched rural and remote units. Units were matched
based on the unit size and modcl of service (ranging
from horne delivery to fUll consultant-led maternity
unitwitlineonatalfacMties).Furthermorc,selectionwas
aimed to ensure geographic spread from al1 regions in
ScotLand and to include island and mainland scttings.
Tb triangulate the interview findings and iden-
tify features that might have been missed in the
interviews, a qucstionnaire was developed using
initial key themes identified, Demographic questions
werc included. Most questions were closed and pre-
coded. Likert-type rating scales were used to gauge
agreement with opinions and attitudes elicited in
the interviews. Rcspondents could make additional
comments. The questionnaire was accompanied by
an explanatory cover Iettcr and reply-paid envelope.
Questionnaires contained idcntifying numbers to
allow reminders to be sent after 3 weeks.
Quantitative data were collated and analyzed
using the Statistical Package for the Social Sciences
(SPSS) for Windows, Descriptive statistics were pro-
duced fbr all variables.
1
'
i
The semistructured interview method gave scope to
develop discussion on the main rescarch questions
(van [[leljIingen & Ireland, 20e3). Interviews, carricd
out by two expcrienced qualitative rcsearchcrs, werc
tape-recorded with consent and transcribed verbatirn.
Field netcs were recordcd to provide further contex-
tnal data on each of the 10 case study sites,
The analysis of the interviews was iterative; first,
emerging themes were identificd as the interviews pro-
gressed (Forrest I〈eenan, van 1"eljlingen, & Pitchforth,
BOX2 Interyiew[[bpics
. Currentcase size flnd mix
. I'erceived and required skills and competencies
. Perceived [ack of skills
. Access to tra[ning
. Existing peer review and supervision structures
. Barriers to training
. Muitidiscip[inary education
. I]rcferences fortraining methods
. aood practlce ]n updating and mainta[ning ski]rs
Ethical Approval
Advice was sought from all relevant research ethics
committees, but ethical approval was not requircd at thc
time because no patient data were used and the commit-
tees, thcrefbre, classed the study as audit
RESUUI'S
Response
Ofthe 1O GPs approached for interview; 2 were unavail-
able, thus 8 GP interviews (8096) were conducted at six
sites. Six GPs had been in post for more than a decade
and the other two fbr 5 years and 18 months respectively,
Most had related qualifications in obstetrics and gynecol-
ogri All had worked in obstetrics fbr at least 6 months and
were cxperienced GPs. The number of deliveries in each
area varied from eccasiona! to 150 per ycar. Maternity
care provision included midwife-lcd units and primary
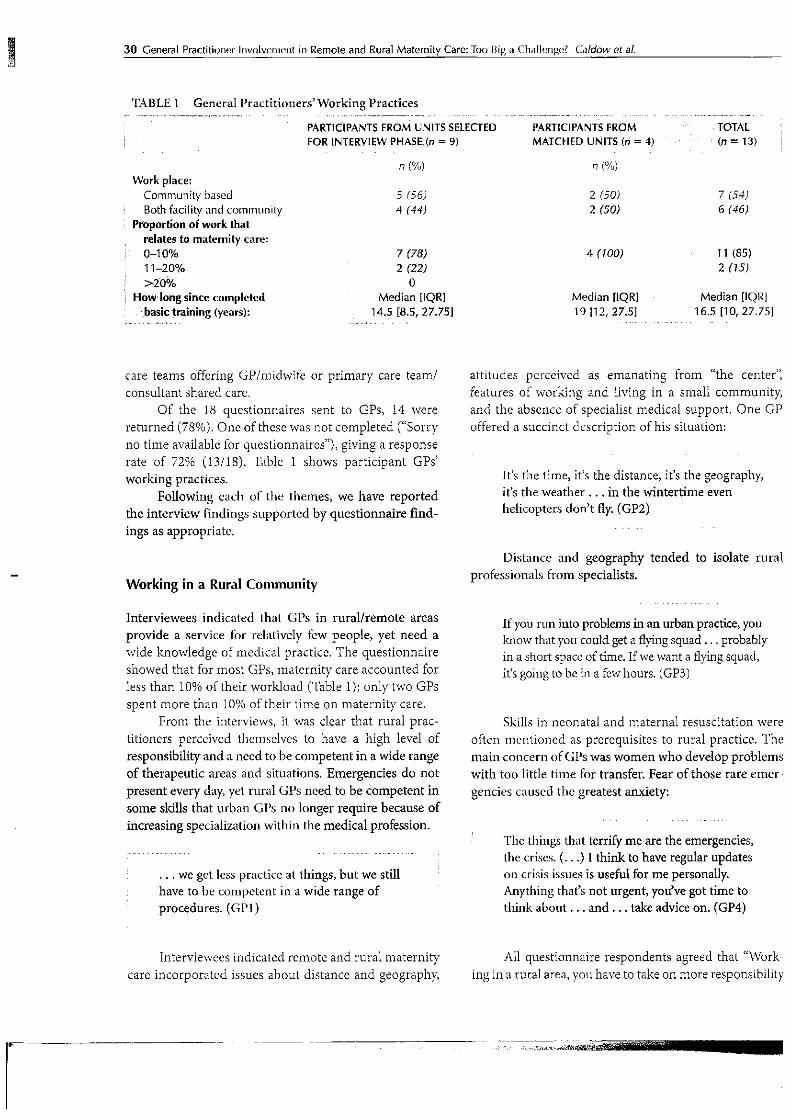
ee
30 Generel Practitioner ]"vo[vcmcnt in Remole and Rural Matern[ty Care: foo Big a Chnllengel C/iildow et al.
TABLEI GeneralPractitioners'SVbrkngPractices
l/
Workplace: Community based Both fac[[ity and community
Proport;on of work that
relates to maternlty care;
O-1O% ll-20%
〉20%i HoW Iongsince completed
. .'.ig.as. ig.tra;ning (ycars):
PAR=CIPANTSFROMUNITSSELEorEDFOR LNTERYIEW PHASE(n = 9)
n(%)
5 r56) 4 (44)
7 r78) 2 C22) o Median [iQR] . ..14;E. [8.S, 27.7s]
PART:CIPANTSFROMMATCHED UNITS (ri = 4)
n (%)
2 (50)
2 (50)
4 (100)
Median {IQRI
19 {1 2, 27151
TOIAL
(n ±' 13)
7 (54)
6 (46)
11 (85)
2 "5J
Median [IQR]
16.5 [10, 27.75]
/
1!
-
care teams offbring GPImLdwife or primary care team!
consultant shared care,
Of the 18 questionnaires sent to GPs, 14 were
re turned (78%). One of thesc was not completed ("Sorry
no time available for questionnaires"), giving a response
rate of 72% (13118). Table 1 shows participant GPs'
workingpractices.
Following each of the themes, we have reported
the interview findings supported by guestionnaire find-
ings as appropriate.
Working in a Rural Community
attitudes perceived
features of working
and the absencc ofs
offered a succinct dcscription of his situation:
as emanating from "the center];
and living in a small communit"
pecialist medical support, One GP
It"s the time, it's the distance, it's the geographv,
it's the weather . . . in the wintertime even
heliceptcrs don't flr (GP2)
Distance andprofessionals fi'om s
geography
pecialists.
tended to isolate rural
Interviewees indicated that GPs in rural/remote areas
provide a service for relativcly fow people, yet need a
wide knowledge of medical practice, The questionnaire
showed that for most GPs, matcrnity care accounted fbr
less than 1096 of their workload (Table 1); only two GPs
spent more than 1OO/6 of their time on maternibr care,
From the interviews, it was clear that rural prac-
titioners perceived themselves to have a high level of
responsibility and a nced to be competent in a wide range
of therapeutic areas and situations, Emergencies do not
present every day, yet rural GPs need to be competent in
some skills that urban Gl's no longer require because of
increasing specialization within the medical profession.
. . , we get less practice at things, but we still
have to be competent in a wide range of
procedures. (GPI)
/
If you rLm into problems in an urban practice, you
know that you co uld geta flying squad ,,,probably
in a short spacc of time. If we want a flying squad,
it's going to be in a few hours, (GP3)
Skills in neonatal and maternal resuscitation were
often mentioned as prerequisites to rural practicc. The
main concern ofGPs was wemen who develop problems
with too little time for transfer. Fear of those rare emer-
gencles caused the greatest anxiety,
The things that terrify me are the emergencies,
the crises. (...) I think to have regular updates
en crisis issues is usefuI for rne personallp
Anything that's not urgent, you've got time to
think about...and...take advice on. (GP4)
Interviewees indicated reniote and rural maternity
care incorporated issues about distance and geography,
AII questionnaire respondents agreed that "1eclork-
ing in a rural area, you have to take on more responsibility
r '-,,,,' .' . -,,.・/,' .t:';",,'v'.
'.,M

!
'
Gemeral Practitioner lnvolvement in Rerriote and Rural Maternity Care: foo Big a Chn[lenge? Caldovv et aL 31
li/
/
i
'
l:
/
:
)
:
[[ABLE2 ThcChalJengesofWbrkinginaRuralArea(n=13)ge,,, "',//,・・i.".g. i,,. 1'"l,tli, II' ,, '1;・:"' i,;ri" ,,lr'""",/l・ "li.lg・"',ll"'1'//tw/rk//1/1,'1"' S'11gi.'',illJ''''R.oalk1・"1-G.,l,,.li"''ii,l・l'/i,'//i・X,,'d'tiVl・ll/'
tt ' ' ttt tt ttt tt /tt t tt tt t t/ t l When working inarural area, you have to take on more - -- - 61.5 38.S l responsibility than in nn urban area.
Dealing with obstetric emergencies is a big ski11s issue
in this area,
Dea]ing with neonatal emergencies is a big skiiis issue
in this area.
With few deliveries, you quick[y become de-ski[lecl
when working [n a rural area.
"lt's [ike riding a bike"-nce you have delivered babies,
, youdon'tforgethow. When working in this area, you have to have the confi clence
to make difficult clecisions and stick with them.
- 8 nv- 61.5 31
- 38.5 23 3S,5 -
t
1
j
1
1
1
1
1
1
i1
!
1
h
4
than in an urban area" (Thble 2). The majority agreed that
deaLing with emergencies, whether obstetric or neonatal,
was a big issue fbr their areas, All a!so agreed that "Wbrk-
ing in this area, you have to have the confidence to make
diMcult decisions and stick with tliemr'
SKILLS
Associated with the rare emergencies was the occasional
need to perform instrumental delivcries, Most of the GPs
interviewed were cither not involved in intrapartuin care or
did not use forceps. The need to remain ski11ed in all phases
of maternity care, virttially to the point of specialization,
was scen to be unigue to remote/rural settings, whereas in
urban units, maternity staffmcmbers only had to maintain
their skills in their specialt}T area of practice, Sevcral GPs
felt de-skiIled, believing midwives to be more sldlled at
neonatal resuscitation than they were, for examplc:
I have had to do basic resuscitation on infants
but nothing more than a skilled midwife could
have done...I could not see myseif finding the
time to practice neonatal resuscitation more than
once a year, whereas the midwives established
their own programme with resuscitation training
every 3 months. So there was a recognition that 1
it was going to be impossible to match those
standards...(GP5)
disagreementaboutwhctherthesmarlnumberofdeliver-
ies attended by GPs was a factor in maintaining skills.
"lell, I suppose the reason why we gave up obstet-
rics was that we felt we were fighting a losing battle
to retain ski1ls and that was to do with the numbers
invoked. . . . attending relatively few deliverics,
almost all normal, so having to c]o a forceps
delivcrB probably did one a year maybe. (GP5)
Reasons for not wanting to keep maternity skills
up-to-date included GPs having to make decisions
about attcnding specialist courses based on available
time and the many relcvant specialties,
...in theory there is so much thatIshould be
doing from an educational point of view that I
wouldn't have time to see patients... yeu have
to try...each year,,, to identify what you
think are your core educational needs. (GP6)
'fable 3 shows GPs' self-rated competence and
confidence regarding the competencies identified by
EGAMS (SEHD, 2002). With the exception of ultra-
sound scanning and breech deliver" selfreported cem-
petence and confidencc svere surprisingly high.
/
1]
/
:'
ln rural general practice, maternity and neonatal
care is a small part of GI's' remit, and some feIt this insufl
ficient to maintain their obstetric skil!s, There was some
Recruitment
Interviewees associated with GP-led maternity units
indicated growing recruitment problems caused by
:
/
1
N.t

32 General Practitioner invoivement in Remote and Rura] dVtaternity Cafe/ foo Big a Chal]enge? datdowetal.
rllABLE3 Self:ReportedCompetenceandConfidenceforExpertGrouponAcuteMatemityServices'Identifie
}ig"・ ,, -#gi-''gg 1!agge 'ag-er"''ge 5//.・eSee,.ikiiS.T"ast,.R,,: 7ee"llec'Se?INxD-:fi'liS."M,M.,",",ag・
lt
intravenous(IV}cannulation 12 92 12 Managing lV fluid replacetnent l3 IOO 13 Management of antepartum hemorrhage 11 85 11 U[trasonic scanningn 3 25 3 Management of noTmal delivery 9 75 9 Management of cord pro[apse 11 S5 6 Management of shoulder dystocia 7 58 6 Managementofbreechdelivery 4 31 2 Undertakingaventouse[ift-outdeliveryb 7 54 7 Management of postpartum hemorrhage 11 85 9 Basic obstetric [ife support 12 92 11 Neonatal resuscitation 12 S12 9 Repalr of perineal trauma 10 77 7 Initial and discharge examination of the 12 92 11 newborn P[gficri?tion ofg.rugs. . . .. 13. .. . 10e .. '[3 ...
"In the question on cenfidence, four respendefi Ls stated that this was not appli[ub[e te their role.
hln the questio]i on confiden[e, one respondellt stated that this was not applicnble te his role.
rural practitioners being required to maintain such a
wide range of skills, This is exacerbated by the fact that
basic medical training no longer provides dectors with
sucacient obstetric skills.
Doctors coming through now don't have the
obstetric skills, and even as medical students,
they don't attend or do the number.of deliveries ]
as doctors graduat{ng 20 to 30 years ago would
have. (GPI)
..E
This was confirmcd in the surveB with 11 of the
13 GPs (85%) agreeing, "There is difficulty recruiting
suitab!y qualified staff to work in this locality:' The other
2 GPs responded, `tlo not know;" In some areas, there is
a fragile structure, and ifjust one doctor were to leave,
maternity care would not be sustainable.
"" i
,,. the structure that they've got in place...
is working ok at the moment, but , . . it would
oniy take a couple of doctors to leave and not
be replaced, and the whole system would come
tumbling down. (GP6)
l
T.1 1 !.. .... .r --" AA.. .d..A" n:-n" -..Un" d
area) movcd to another region, thisE
of GP involvement because the GP "
two GPs who supported the midwivc
Lntrapartum care.
TVvelve of the 13 survey responder
that ")glaternity care in this area is dif
because it depends on a few skilled pe`
GP respondcd, [ao not knove"
In contrast, one GJ' suggested,
even going right back to medical s(
think that there should be some fo
ing package for people who want t
rural practice ,
Training
(GP2)
GPs who are keen to preserve thcir mi
ment usually maintained ski11s throue
becoming a trainer. All agreed that tr2
de-skilling and was the best way to sus
even when low numbers of births mea
tice. Frequency of training was viewE
A favoured method was hands-ongain further experience in obstetric p]
r"t"olliT ImooA mafprnitv cprp nrnv;tlpt

t
L
a
l
(]enera[ Prnciitloner involvernent in Rernote and Rural Maternity Care: lbo Big a Cha[lenge? Catdow etaL 33
a short placement in a
suggestcd:
'
large urban hospital. One GP
. . . one problem perhaps is that a lot of medical
schools are centered around teaching hospi-
tals, and theyire not always the best places for
hands-on experience. I think, probabls more
use of the smaller hospitals wo u]d be usei'ut.
(GP4)
More than two th]rds ofthe survey respondents
had undertakcn same form of continuing medical
education (CME) related to maternity care within
the previous year (Tlable 4). Most of these events
were concerned with updating emergency skills.
TWo barriers to CME-"lack of time" and [` getting
staff cover"-were rated as important by all GPs." Distance to training" was an impertant barrier for
nearJy aU GPs.
MuEtidiscipLinary
Many GPstraining as b
Education
regarded multidisciplinary education or
eneficial:
It's (multidisciplinary training) much better
because that is how we work. If we have an
emergency in the matetnity unit, everybody is
working together. (GPI)
However, some felt training and education should
be tarb.eted at specific professienal groups:
I think one of the prablems with multidisci-
plinary training is often that it's diencult to
pitch the cducation at the right level for Lhe
whole audience, (GP5)
The differing views on "It's difficult to have joint
courses (multidlsciplinary) that suLt the needs of all
professions involvcd in matcrnity carc" were echoed in
the survey: Seven (54%) disagreed with this statement
whereas six (46%) agreed. However, all GP respon-
dents agreed that "Multidisciplinary training is usefu1
because it makes you more aware of the role of other
professionsr'
Videoconferencing
If videoconferencing was available, it was not generally
used or recognized as being very useful, although one
GP thought it had potential for training and diagnostic
support.
/
/
1
I need to be conyinced.I think our big lack in
that context is nctworking and making per-
sonal contact, which I don't think you can do
by videoconferencing. (...) It has a value in
talking to people or showing things, or perhaps
taLking through a procedure. The real value of
[T (information technology) is in the transfer
of images, ultrasoulld imagcs or faices of CTGs
(cardiotocograpliy) or, particularIB ultrasound
images in maternity that would be a huge ben-
efit. (GP7)
Most GPs had acccss to videoconferencing facili-
ties (n = ll, 85%). Only 8 (73%) of the 11 GPs with
access to these facilitics knew how to use them, 1'he
facilities tended to bc used on avcrage twice a month
[IQR: O.9, 7], usually for clinical purpose (n = 8, 73%) or
meetings (n = 8, 7396). Less than half the respondents
(n = 5, 45%) reported videoconfercncing being used for
education or training,
DISCUSSION
This study found that maternity care accounts fbr lcss
than 10% of most remote and rural GPs' workload,
yet requires fully skilled, experienced practitioners to
recognize and address complications. Thc fact that the
necd for care around birth is unpredictable, and often
demanding in terms of time and skiIIs required, has
resulted in fewer GPs being invo]ved in intrapartum
care than a few decades ago. A rccent comment by the
RCGPs' chairman suggesting that "many GPs are kecn
to see a return to this worre' raises questions about how
GPs will attain and maintain these skiIls (Ficld, 201O).
Smith et al. (2010) highlight the vital information
that GPs have regarding the medical historics of women
and their famiIics. Our findings confirm that knowlcdge
of the individual woman and what constitutes normality
were regarded as valuable attributes by GPs, facilitat-
ing the ability to react quickly in emergency situations.
Although selfreported competen[e arid confidence for
specific skills was surprisingly high among respondents,
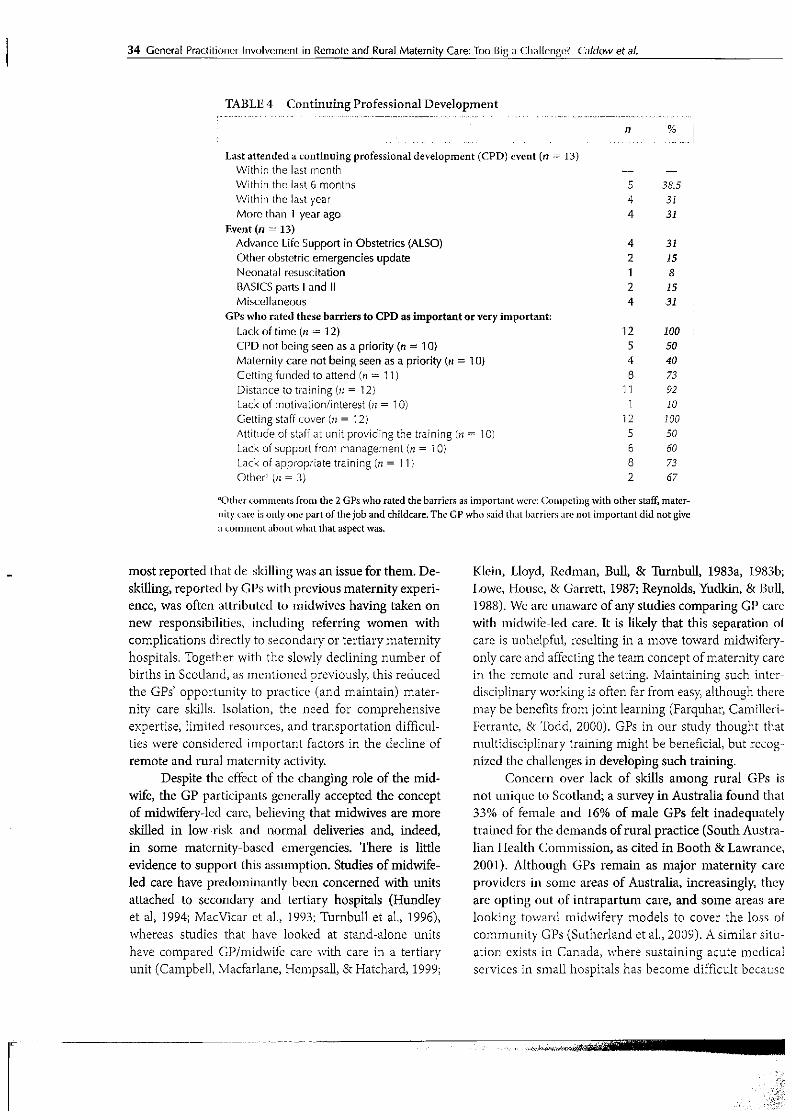
34 General Practitioner lnvolvement in Remote and Rura] Maternity Care: lbo Big n {/hnl[cngot C/iildow et aL
IIABLE4 ContinuingProfessiona
t....-.---・---
1Development
Last attended a continuing professienai deyelopment (CPD) cvent (n =-:- 13)
Within the last month
VVIthin the iast 6 months
Within the last year
Moro than 1 year ago
Event (n =" 13)
Advance Life Support in Obstetrics (ALSO)
Other obstetric emergencies update
Neonntalresuscitation
BASICS parts1and 11
Misce]laneous
GPs who rated tliese barriers to CPD as impertant or very important:
Lack of time (n ='L 12)
C['D not being seen as a priority (n = 1 O)
Maternity care not being seen as a priority Cn = 1O}
Cetting funded to attend (n t= 1 D
Distance to training (n = 12}
Lack of motivationlinterest {n = 1 O)
Getting staff [over (n = 12)
Attitude of staff at unit providing the tra[ning Cn == 1O)
Lack of support from management (n == 1O)
Lack of appropriate train[ng (n = 1 1)
Other" Cn = 3}
n
5
4
4
4
2
1
2
4
12
5
4
8
11
1
12
5
6
8
2
%1....1
38.5
31
31
31
J5
8
15
31
IOO
50
40
73
92
IO
100
50
60
73
67
']Othe]'cemmentsfromthe2GPswhoratedthebarriersasimportantwcre:(]omF)eliJigwithotherstaEmater-
nityc4ireisonlyonepartofthejobandchildcare,TheGPwhosaidthatbarricrsarenotimportantdidnotgive
ncon]nientaboutwhntthataspectwas,
-most reported that de-ski]ling was an issue for them. De-
skilling, reported by GPs with previous maternity experi-
ence, was often attributed to midwives having takon on
new responsibilities, including referring women with
complications directly to secondary or tertiarymaternity
hospitals, Tbgether with the slowly declining number of
births in Scotland, as mentioned previouslM this reduced
the GPs' opportunity to practice (and maintain) mater-
nity care skills. Isolation, the need for comprehensive
expertise, limited resources, and transportation difficul-
ties were considered important factors in the decline of
remote and rural matcrnity activityL
Despite thc cffect of the changing role of the mid-
wife, the GP participants genera]ly accepted the concept
of midwifery-lcd carc, believing that midwives are more
skiIled in low-risk and normal deliveries and, indeed,
in some matcrnity-bascd emergencies. There is liule
evidence to support this assumption. Studies of midwife-
led care hffve predominantly been concerned with units
attached to secondary and tertiary hospitals (Hundley
et aL 1994; MacVicar ct aL, 1993; TUrnbul1 et al,, 1996),
whereas studics that have looked at stand-alone units
have compared GPImidwife care ivith care in a tertiary
unit (Campbe]1, Macfarlane, Hempsall, & Hatchard, 1999;
Klein, Lloyd, Redman, Bull, & 1[Urnbull, 1983a, 1983b;
I.owe, Housc, & Garrett, 1987; Reynolds, Ytidkin, & Bull,
l988). Wb are unaware of any studies comparing GP care
with midwif'e-led care. It is likely that thls separation ol
carc is unhelpfu1, resulting in a move toward niidwifery-
only care and affbcting the team concept ofmaternity care
in thc remote and rural setting, )vlaintaining such intcr-
disciplinary working is often far from easy although there
may be bcnefits from joint learning (Farquha4 Camilleri-
Ferrantc, & 'lbdd, 2000), GPs in our study thought that
multidisciplinary training might be beneficial, but rccog-
nizcd thc challenges in developing such training.
Concern over lack of ski11s among rural GPs is
not unique to Scot]and; a survey in Australia found that
33% of female and 16% of male GPs felt inadequately
trained for the dcmands of rural practice (South Austra-
lian IIealth Commission, as cited in Booth & Lawrance,
2001). Although GPs remain as major maternity care
providers in some areas of Australia, increasingtF thcy
are opting out of intrapartum care, and some areas are
looking toward midwifery models to cover the loss of
community GPs (Sutherland et al,, 2009), A sirnilar sjtu-
ation exists in Canada, where sustaining acute medical
services in small hospitals has become difficult becausc
r -- -- ------ --
t/t

'
'
Gcnernl Practitioner lnvo[vement in Remote and Rura1 Matcrnity Care: lbo Big a Cha[lenge? Calclow et aL 35
ofuniversalmedicalworkfbrceregulationscompounded
with the challenges ofstaff recruitment and retention in
remote and rural areas (Benoit, Carrol, & Millar, 2002),
One respondent in our survey felt that specialist
training fbr rural practice would be beneficiaL This
is interesting as the cvidence points to this as a sig-
nificant factor in the recruitment and retention of
rural GPs (Australian Medical Workl/orce Advisory
Committee, 2005; Laven & Wilkinson, 2003; Mungall,
2004), and arguc that specialist medical training may
be instrumental in reestablishing obstetric services
in rural areas (Caudle et al., 1995). Other studies
indicate the importance of carly exposure of medical
students to rural practicc (Rolfe, Pearson, O'Connell, &
Dickinson, 2005; Wang, 2002), and that training wholly
in consultant units may make them (practitioners)
fearfu1 ofcommunity-based obstetrics (Bafrd, Jewell, &
LAvlalker, 1995).
GPs in our study thought education is thebest way
of combating de-skilling and suggested that this was
best achieved through short training periods working
in maternity hospitals to update technique and practice
skills. Two thirds of respondents reported they had
undertaken some form of maternity care CME within
the last year. HoweveB most faced barriers in attending
such events (time, staff coveg and distance). Lack of
access to CME has been identified as a potential cause of
de-ski11ing, with 219t} ofAustralian GPs reporting dith-
culty accessing CME for obstetrics (Booth & Lawrance,
2001). It has also been found to be a reason for GPs
deciding not to rernain in rural areas (Brookman, 2004;
Gardiner, Sexton, Durbridge, & Garrard, 2005),
Telemedicjne is increasingly being used in mater-
nity care (Ireland ct al., 2007), and Cronin, Cheang,
Hlynka, Adair, and Roberts (2001) in Canada fbund
that videoconferencing enhanced neonatal resuscitation
education in areas where experienced instructors are in
short supply It might, therefore, have been expected that
these technological advanccs would have been seen as a
means ofovercoming some training dithculties, but our
study findings did not indicate this. An Australian study
howeve4 suggests face-to-face contact, which remains
the preferred method of learning (Booth & Lawrance,
2001). It is possiblc that this rclates to the importance
GPs attach to networking and social contact. Some
respondents mentioned the isolation associated with
rural practice and the responsibility of working alone.
Isolation and having fewer colleagues ivith whom to
discuss professional issues have been identified as fac-
tors in GPs' decisions to Ieavc rural practice (Gardiner
et aL, 2005),
Strengths and Limitations of the Study
The strength of the study was the mixed methodology
whereby the qucstionnaire results triangulated the inter-
views. This validated the interview findings and showed
general agreement with the matched sample, One of
the limitations was the small numbers. Although it is
ackiiowledgcd that this was a smal1 sample of GPs, it was
representativc of different rural areas within Scotland.
The reportcd study is part ofa larger study (Kiger et
al., 2003; IIUcker et al., 2005), where 72 interviews were
conductcd with various remote and rural maternity care
providcrs, and the data were enhanced by being situated
within the themes gcnerated by the wider study How-
even caution must be exercised in generalizing from the
study findings given the small number ofGPs involved.
Furthermore, the interviews were conducted in 2003,
and therefbrc, the data can be viewed as slightly dated.
Although GPs views may have changed over time, the
fact that matcrnity care has rnoved away from GPs'
spherc of practice is only likely to have increased the
challengcs that GPs face, Despite these limitations, we
believe that our research findings wM inform the debate
about GP involvement in maternity care, particularly in
remotc and rural arcas.
Implications for Clinical Practice
Reinstating thc GP's rote in maternity care provision is
1ikely to prove difficult without a significant commit-
ment by GPs to retraining and skil1 maintenance, Our
findings shDwed that the perceived numbers of practi-
cal episodes required for competence varied widel)c
The frcqucncy of relevant clinical events in hospital
units might not permit sufficient experience during
attachments, and other health professionals in train-
ing might have priority A further problem is that there
exists insufficient evidence to suggest such training will
be effective. Although life-support training has been
recommended as a means of maintaining competence
with regard to obstctric emergencies (National Instit"te
for Clinical Exccllence, SEHD, & Department of Health,
Social Services and Public Safetyi 2001), a systematic
review found liLtle evidence of whether such courses
improve actual practice, although practitioner confi-
dence can be increased (Black & Brocklehurst, 2003).
Some form ot' tailored return-to-practice course may
be va]uablc, particularly for GPs who intend to provide
maternity care in remote and rural areas, However,
other considerations include barriers to GPs gaining
tl ttt t tt t tttttt

FM"
36 Generil1 Practitloner [nvo]vement ln Remote ilnd Rura[ Maternity Care: foo Big a Challenge? Caidow et ni,
practical cxperience in a hospital environmcnt, because
contracts of employment assuring Crown Indemnity
are not available in maternibr hospitals and because
backfilling in the primary care unit is difficult, Clearly,
the issuc ofhow to go about retraining GPs will require
carefu1 consideration, and the support of other health
professionals, particularly midwives, will be vital.
The withdrawal of GPs from maternity service
provision also has implications fbr the U.K. government's
plans to make GPs central to the commissioning ofhealth
services. Atthough the government proposes that the lead
role in commissioning maternity services wiI1 be taken by
the NHS Commissioning Board (Deparbnent of Health,
2010, p. 13), GP commissioning ivi11 have implications fbr
the wider framework of hea!th care provision in which
the matcrnity services operate. It is essential, therefore,
that GPs work in close partnership with inidwives to
ensure that services remain women-centcrcd.
CONCLUSION
Fewer rural births and problems with recruitment/
retention of professionals have made it more difficult
to staff rural maternity units. "ihere such units have
remained open, midwives have steppcd up and taken
over units to ensure that women in these arcas continue
to havc a service. Although rural GPs and midwives
might traditionally have been in competition in the area
of matcrnity care, providing a woman-centered service
in remote areas may bc easier to achicvc through col-
laborati ve working. Howeve4 if GPs are to have a greater
role, then they will need to be prepared to make a strate-
gic commitment to the maintenance of remote and rural
maternity care. This will require innovative methods of
training, special considcration of educational needs, and
incentives for practitioners to settle in rural areas, but
it may already be teo late for GPs to have a substantial
mput ]nto matermty care,
REFERENCES
Austra]ian }vtedical "iorl〈force Advisory Committee, (2005). I)octors in yocatlonal training: Rural ba[kground and
rural practice intentions. Australian Journal of Rtiral
Health, 13, 14-20.
Baird, A. (l., Jewell, D., & Walke4 J. J, (1996). Management ol'
labour in an isolatcd rural maternity hospital, British
iVfedical fournal, 312, 223-226.
Benoit, C,, Carrol, D., & Millany A. (2002). But is it good for
non-urban woman's health? Regionalizing maternity
care services in British Columbia. Canadian Revieiv of
Sociology andAnthropology, 39(4), 373-395.
Black, R. S., & Brocklehurst, R (2003). A systematic review of
training in acute obstetric emergencies, British journal
qfObstetrics and (lynaecology, l10, 837-84l.
Booth, B., & Lawrance, R, (2001), Quality assurance and con-
tinuing education needs of rural and rernete general
practitionetsi How are they changing? Australian ]bur-
nal ofRural Health, 9, 265-274.
British Medical Association. (2007). Nintional enhanced
service-intrapartum care. Retrieved September 17,
201O,fronuv}vstbma,org.uklemplo)Tnentandcontractsl
independenLcontractorslenhanced"scryiceslNES
mtrapartunl"sp
Brookman, D. (2004). Rural medical manpower planning: A
plea for rationalit)c Australian journat of Rural Hbalth,
l2(4), 172.
Campbell, R., Macfarlane, A., Hempsall, V, & Hatchard, K,
(1999). Evaluation of midwife-led care provided at the
Royal Bournemouth LIospitaL Midwijler),, 15, l83-193.
Caudle, M. R., CIapp, M., Stod〈ton, D., & Neutens, L (1995). Advan[edobstetricaltrainingforfamilyphysicians:The
futurc for rural obstetric care. fournal ofFamily Practice,
4j,123-125.
Cronin, C., Cheang, S., Hlynka, D,, Adai4 E., & Roberts,
S. (2001). Videoconferencing can be used to assess
neonatal resuscitation skMs. Medicat Education, 35,
1013-1023.
Department o"Iealth. (2003). The raport of the maternity and
neonatal vvorig?)rce grotgJ to the Department of Health
Children3 Tasigbrce, London, United Kingdom: Depart-
mentofHealth.
Department of Health. (2010). Liberating the NHS: Commis-
sioningforpatients, London, United Kingdom: Depart-
ment of Health.
DeVties, R., Salvesen, H, B,, Wiegcrs, T A,, & Williams, A. S.
(20e1). What (and why) do women want? In R. DeVlries,
C, Benvit, E, van Teij]ingen, & S, NVrede (Eds,), Birth
by design (pp, 243-266). London, United Kingdom:
Rout}cdge.
Farquha4 M., Camilleri-Ferrante, C,, & lbdd, C. (2000),
General practitioners' views ofworking with team mid-
wiferv British Journal oj' General Practice, 50, 211-213.
Field, S, (2010), King's .fttnd inquiry into maternity care-
RCC;P response, Retrieved September 17, 2010, from
http:/lwwimrcgp.org.uk/newslnews-20101kings-fund-
mqutrvaspx
Forrest Keenan, K,, van [[le ijlingen, E,, & Pitch forth, E. (2005),
The analysis of qualitative research data in family
-----
'#ee

General E]ractitloner lnvolvement in Remote and Rural Maternity Care/ Tbo Big a Cha]lenge? Catdo'vv etaf. 37
planningandreproductiyehealthcare,JournalofFarnily
Planning and Rep roductive Heatth Ca re, 31(1), 40-43,
Gardiner, M., Sexton, R., Durbridge. M., & Garrard, K. (2005).
'1'hc role of psychological well-being in retaining ruraL
generalpractjtioners.AustralianJournalofRuralHealth,
l3(3), 149-155.
Genera1MedicalServiccsCommittee.(1992),GetieratMedicalSer-
vices Cbmmittee mport London, United Kingdom: BMA,
Health Commission. (2008). TbTvards better births: A revievv (if
nraternityservicesinEngland.I.ondon,UnttedKingdom:
Commission for Healthcarc Audit and Inspcction.
Hewison. J. (2001). Dia'crent models ofmaternity care: An evalu-
ationoftherolesofprimar〉rhealthcareworkers[SLllnrriary number 574]. 7ke Research i:inditlgs Registen Retrieved
September IZ 2010, from ww"itdh.goyukfenlAboutusl
RescarchanddevclepmentlALoZfMotherandchildhealthl
DH-4016310?PageOperation=email
Hundley; V A., Cruickshank, F. M., Lang, G. D., Glazener.
C. M,, Milne, J. M., lhrner, M., ... Donaldson, C.
( 1994). Midwife managed dclivery unit: A randomised
controlled comparison with consultant ]ed care. British
iVedical Journal, 309, 1400-140iL
Informatien Services L)ivision. (2elO), rsD ivoinen th chil-
drenk health itijbrmation prQgramme, births th babies,
live births by mode of deliverT and induced. Retrieved
September 17, 2010, from http:/Azz-v,isdscotland,org/
isdl1807.html
Ireland, J., Bryers, H., van TbijIingen, E., Hundte" NC, Farmer,
J., Harris, E,...Caldoig J. (2007), Competencies and
skills for remote and rural maternit〉' care] A review of the literature. journal qf Advanced Nursiirg, 58(2),
105-115.
Kiger, A., TUcker, J., Bryers, H., C]aldoig J,, Farmer, J,, Harris,
F., , , , yan [rbijlingen, E, (2003), Stistaitiabte niaternity
service provision in remote and rural areas ofScotland:
lhe scoping of core multidisciplinary skills and explora-
tion of best practice in the development and mainte-
nance of skilis [Report NHS Education fbr Scotland],
Abcrdeen, United Kingdom: University ofAberdeen.
Klein, M., Lloyd, I., Rcdman, C., Bull, M,, & 1'urnbull, A. C.
(1983a), A comparison of ]ow-risk pregnant women
booked for delivery in two systems ofcare: Shared-care
(consultant) and integrated general practice unit I.
Obstetrical procedures ancl neonatal outcome. British
Jburnal ofObstetrics and (lynaecology, 90, 118-122.
Klein, M., Lloyd, I,, Rcd[nan, C,, Bull, M,, & [[Lirnbul1, A, C.
(1983b). A comparison of low-risk pregnant women
boeked for dclivery in twe systems of care: Shared-
care (consultant) amd integrated genera1 practice unit.
II. I.abour and delivery management and neenatal out-
come. British jot.trnat of Obstetrios and Clyttaecotqgy, 90,
123-128,
Laven, G., & Wilkinson, D. (2003). Rural doctors and rural
backgrounds: How strong is the evidencc? A systematic
reviewL Austtmlian fournal ofRural Health, 1 J, 277-284.
Lowe, S. W!, House, W, & Garrctt, 'll (1987). Comparison of
outcome of Iow-risk Iabour in an isolated beneral prac-
tice maternity unit and a specialist maternity hespitaL
Jottrnal of the Royal Collage ofGeneral Pnictitioners, 37,
484-487,
MacVicar, J,, Dobbie, G., Owen-Johnstone, L,, Jagger, C,, Hop-
kins, lvl., & Kcnnedy, J. (1993). Simulated home delivery
in hospital: A randomised controlled trial. Jlritish Jbur-
nal ofObstetrics and (lynaecology, 100, 316-323,
Munga]1, I. J, (2004). Ruralgeneratpractice [RCGP Informa-
tion Sheet No 231. London, United Kingdom: RCGP
2004. Retrieved September 17, 2010,
Mungall, I. J, (20e5). Trend towards centralisation of hospi-
tal services, and its effect on access to care for rura]
and remote communities in the U,K, [serial Qnlinel.
Rural Remote Htialth, 5, 390. Retrieved September 17,
20IO, frorn wwwLrrh.org.au/articleslshowarticlenew
.asp?ArticlelD '-' 390
Murphy-BIack, T, (1992). Svstems ofmaternity care in use in
Scotland. Midwijbry, 8, 113-124,
The National Health Service Conl'ederation. (2003). Investing
in general practice-The nevv general medical services
contract. London, United Kingdom: BMA.
NationalHealthServiceQualityImprovementScottand.(2007).
IVbtional overvierv ofmaternity services-Janttary 2007.
Edinburgh, Scotland: Author. Retrieved September 17,
2010, from http:11wrviv.nhshealthquality.urglnhsqisl
fileslMATSERV-NOVJAN07.pdf
National Institute for Crinical Excellcnce, SceLtish Executivc
Health Department, & Dcpartment of Health, Social
Services and 1]ublic Safety: Northern ]reland. (2001).
Why methers die 1997-1999: lhe conjidential enquir),
into maternal deaths in the Uitited Kitzgdom. London,
United Kingdom: RCOG Press.
Reynolds, J. L., Yinclkin, P L., & Bull, M. J. (1988). General practi-
tioner obstetrics: Does risk prediction work? fi)urnal ofthe
1(qyal Cbllage ofGetteral Practitioners, 38, 307-31O.
Rolfe, I, E., Pearson, S. A,, O'Connell, D, L,, & Di[kinson, J. A.
(1995). Finding solutions to the rural doctor shortage:
The roles of selection versus undergraduate medical
education at Ncwcastle, Australian and New Zealand
Journal ofMedicine, 25, S12-517.
Royal College of Gencral Practitioners Maternity Care Group.
(1995), 11he role (ifgeneralpractice in maternity care.
I.ondon, Unitcd Kingdom: Author.
Scottish Executive I'Iealth Department, (2002). Expert Group
on Acute Maternity Services rofirrence report. Edinburgh,
United Kingdom: Authon
g/'.
38 General Practitioner tnvolvement in Remote and Rura[ Maternity Care: R]o Big n (lha]lenge? datdowetaL
Scottish Office Department of Health, (1998), Acttte services
revieiv report. Edinburgh, United Kingdom: The Sta-
tionary Office.
Scottish Othce IIome and Hcalth Department, (1993), Provi-
sion of maternity services in Scotland: A poliay reviei"
Edinburgh, United Kingdom: HMSO,
Smith, A., Shakcspcare, )., & Dixon, A. (201O). 71ie role of GRs
in nJaternity care-ivhat does thefLiture hold? London,
United Kingdom: King's Fund.
Smith, L. E (1997). 1'rcdictors ofthe provision ofintrapartum
care by generat practitioners: five year cohort studv
British journal of (;eneral Practice, 4Z 627-630.
Srnith, L. E, & Jcwcll, 1). (1991). ']'he contribution of general
practitioners to hospital intrapartum care in maternity
units in Englancl and Whles in 1988. British Medical
journat, 302, 13-16,
Smith, L, F,, & Jewell, D. (1999), General practitioners'
contributions--what's really going on? In G, Marsh &
lvl. Renfrcw (Eds.), Opt]rd generalpractice series: Coni-
mttnity-based maternit7 care. Oxford, United Kingdom:
OxfordUniversityPress.
Sutherland, G,, Ydlland, I,, N'Vicbc, J,, Kelly, J,, rvlarLowe, R, &
Brown, S. (2009). Role of general practitioners in pri-
mary matcrnity care in Seuth Australia and Victoria.
Australian and New Zealand fournal oj' Obstetrics and
(lynaecolqEv,,49,637-641.
:[Ucke4 J., Hundle" M, Kigeg A., Bryers, H., Caldow; J., Farme4
J,, , , , van '1'eijlingen, E. (2005). Sustainable maternity ser-
vices in remote and rural ScotLand? A qualitative survey
of staff views on requircd slciLls, competencies and train-
ing. Quatity a,td Scipty in Health Care, 14, 34-40.
:[Urnbul1, D,, Holmes, A., Shields, N., Cheyne, H., Twaddte, S,,
Gilrnour, "C H.,..,T.unan, C, B, (1996), Randomised,
controlled trial of efficacy of midwife-managed care.
Lancet, 348, 213-218.
van Tleijlingen E., & IIundle- V. (20e5). Pilot studies in fam-
ily planning and reproductivc health care, Journal of
Family Pianning aitd I(eproductive Hlealth Care, 31(3),
219-221.
van [feijlingen, E., & Ircland, J. (2003), Research interviews in
midwiferyt 1(oyal CoUege ofMidvvives, 6(6), 260-263.
Wt!ng, I,. (2D02). A comparison ofmetropolitan and rural med-
ical schools in China: NVhich schools provide rural physi-
cians? Austratian Journal ofRural Health, 1O, 94-98,
Acknoivle4gments. This study was funded by NHS Education
for Scotland (NES; Grant number CP123). We acknowledge
the advicc, support, and assistance of the NES steering group
and the professional advisory group of experts.
Wb would like to thank the secretaries of the Centre of
Academic Primary Care and Dugald Baird Centre forRescarch in Wt)meiis Health, Aberdeen UniversitF for tran-
scribing the int¢rviews. We would also like to thank all headsofScottish maternity units and the general practitioners who
participatcd in thc interviews. We appreciate their valuab[e
time and insight, without which this study would not have
beenpossiblc.
Correspondence regarding this article should be directed to
Vanora Hundley, Nursing, Midwifer〉' and Allied Health Profes-sions Research Unit, University of Stirling, Stirling, FK9 4I,A,
Scotland,UnitedKingdom,E-maiI:vanora,hundley@stir,ae.uk
Jan Caldow, E3Sc, RGN, MSc, fbrmerly University ofAberctcen.
Vlinora HundleM BN. RGN, RM, MSc, PhD, George Mason
Universit" USA and the University ofStirling, UK.
Edwin van 'l'eijlingen, MA, MEd, PhD, Bournemouth
University, UK, and the University of Aberdeen, UK,
John I〈eid, MBChB. MSc (Econ), FRCGR DRCOG,University of Aberdcen, UK.
A]ice Kige; RN, MA, MSc, PhD, University of Aberdeen,
UK, and Visoka SoLa za Zdravstveno Nego Jesenice, Slovenia.
Janet Tucker, BSc, PhD, University ofAberdeen, UK,
Ji]ly Ireland, IUvi, BA, MSc, Dip Psych Poole NHS Foundation
Trust, Poole, and Bournernouth University, UK,
Fiona Harris, MA, PhD, Uniyersity ofStirling, UK.
Jane E:ar;ner, l'hD, La Trobe Rural Health School, Bendigo,
Australia.
Helcn Bryers, RM, BA, MM, PhD, NHS Highland, UK and
thcUniversityofAberdeen,UK.
.-,..,1・L,,.,/・,a-../,,silt-mu--s',whinitGva
,.,:・s 'me
',,.l g .
..1,,1.1..,/,va tlje・・nm

Expandmg Postpartum Hemorrhage Preventionto the Community in Resource-Poor Contexts:
Critical Considerations and Next Steps
Sydnay A. Spangle4 Alissa Kbski, Dehorah Armbruste4 and
(lynthia Stanton
Increasing the proportion of pregnant women with medically skilled care at childbirth is widely
regarded as the bcst strategy fot reducing maternal mortality and morbidity in resource-poor contexts.
For many countries, however, local conditions nccessitate continuing discussion concerning the role
of targeted, community-based interventions in effbrts to tackle this problem, Onc such intervention
gaining momentum is community-based use ofuLcrotonic drugs to prevent postpartum hemorrhage
(PPH). But how this intervention fits within the lm'ger maternal health agenda sti]I needs addrcssing, as
do questions regarding whether, where, and how to proceed. This artic]e presents a usable framework
fbr coii text-based decision making around PPH prevention, evaluating why and under what circum-
stances it might make sense to implement uterotonic drugs at the community levcl. Using Demographic
and Health Survcys (DHS) data alQng with current evldence, we identify four critical considerations
for policymakers to take inte account: (a) where births are happening, (b) ;vhich women are deliver-
ing in what settings, (c) capacity ofhcalth care systems, and {d) criteria for selecting specific uterotonic
drugs. Incorporating these considerations, we propose a checklist to aid policymal〈ers in deterininingwhat strateg}r realistically suits the neecls of their particular country contexts, Although a large and
rigorous body of evidence sul)ports PPH prevention methods, research gaps remain. Even wiLh suf-
ficient evidence, howeve4 a gLobal consensus may not be reached becausc of the ongoing debates over
community- versLis faci!ity-based interventiens, Despite thesc issues, it is still poss{ble to arrive at policy
decisions on communi".-based use of uterotonic drugs by taking a carefut, context-based approach.
In many settings, implementation of this intervention can be pursued in conjunction with improve-
ments to facility-based care. As a complement to skilled attendance, expanding PPH preyention to the
community can be part efa national push to target the reduction of PPH as an a[hievable goal.
KEYWORDS: maternal health policy; postpartuni hemorrhage; community-based interventions;
uterotonic drugs; maternal mortality
INTRODUCTtON
Death and disabilibr from pregnancy-related complica-
tions remain a significant challenge in resource-poor
contexts. Estimates of maternal mortality worldwide
rangc from 536,OOO in 2005 (Wbrld Health Organiza-
tion LWHOI, 2007a) to 342,900 in 2008 (Hogan et al.,
2010), but agree that the great majority of maternal
deaths occur in sub-Saharan Africa and South Asia.
The global health community recognizes this issue as a
priority problcm; reducing the maternaL mortality ratio
by three-fourths is one of eight UN Mdiennium Devel-
opmcnt Goals (MDGs) to be reached by the year 2015,
Rcgardless ef which estimate is used, progress toward
this goal has been unacceptably slew Between 1990
and 2005, maternal mortality in most devetoping coun-
tries has decreased at rates well below the 5.5% annual
decline needed to achieve MDG-5.
INIERAL4nOAtAL JOURALtlL OF CHILDBIRffI blolume 1, tssue 1, 2011 @ 2011 Springer Publishimg Company, LLC www.springerpub.com DOIilO,189V2156-5287.i].39
-sr.l c;t-.-
';, dS "xli・s
7J -,,d-/t-t
"de,,t
. ..t l/.

'
r''
40 Expanding Postpartum Hcmorrhnge Prevention to Community Contexts SPangter et al.
Because ]ife-threatening maternal complications
tend to occur near deliverM researchers and advocates
largely agree that incrcasing the proportion ofbirths with
medicaily skilled carc is critical for alleviating this crisis
(Campbell & Graham, 2006). 'l'he }VHO, international
Confederation of Midwives (ICM), and International
Federation of Gynecology and Obstetrics (FIGO) define
a skilled birth attendant as an accredited health profes-
sional (such as a midwife, docton or nurse) trained to
proficiency in the skills nccdcd to rnanage uncomplicated
pregnancies and childbirth, as well as to identifY, manage,
and refer complications in women and newi]orns (WHO,
Department ofReproductivc Health and Research [RHR],
2004). But despitc its thcoretical appeal and inclusion of
a broad array of hcalth professionals, local conditions in
many countries limiL the extent to which this care can be
made available, Whether because ofproblems with mater-
nity care coverage, quality of services, or care-seekmg
behavio4 many women are not reaching skilIed care and
are not 1ikely to reach it in the near future, This reality
necessitates centinuing discussion regarding the role of
targeted, community-based interventions in effbrts to
promote safe motherhood, whcrc "comrnunity" refers to
low-level health facilitics (nonsurgical, nonphysician, geo-
graphically rcmotc f'rom referral-level care) as well as to
homes. Howcve4 which interventions to prornote, in what
particular contcxts, and by whom, remains a controversy
in research, policM and program arenas.
One comrnunity-bascd intervention that deserves
carefu1 consideration is prcvcntion of PPH with utero-
tonic drugs. Usc of these drugs in homes and low-level
facdities is currently gaining momentum in both research
and practice, But thc place ofthis intervention within the
global agendia for maternal-newborn health stM needs
addressing, as do questions on whethe4 where, and how to
proceed, The purpose ofthis article is to present a context-
based framework for decision making on expanding PPH
prevention to tlic community, Secondary objectives are to
summarize what is known about PPH and its prevention,
identify important gaps in the evidence base, and suggest
next steps for future research. 'rhroughout this article, we
view comniun ity-bascd PPH prcvention as a complement
to the broadcr stratcgy of ski11ed attendance-as a means
of augmenting health systems in places that are still far
from making the ideal carc available to every woman.
POSTRARTUM HEMORRHAGE PREVENTION
Obstetric hemorrhage is among the leading causes of
maternal death in the developing world, representing
34% and 319'o of maternal mortality in Africa and Asia
respectively (Klian, Mlojdyla, Sa〉r, Gulmezoglu, & VaiLook, 2006). fVthough it is difficult to determine wha
part ef obstetric hemorrhage is attributable to postpartun
complications-and even rnore clifflcult to distinguisl
these compLications from each other-it is safe to sa]
PI'H is the most common type of obstetric hemorrhage
and that uterine atony is a predominant cause of PPII
Wortdwide incidence of PPH is estimated at 10,5% of liv`
births annuall" which equates to nearly 14 million case/
per year (WHO, 2005), Survivors of PPH may face sever`
or chronic anemia, rcsulting in reduced capacity to executt
daily activities, susceptibility to infection, and poor out
corncs in fttturc prcgnancies (1[blentino & Friedman, 2007
Wblvekar & Virkud, 2e06). Given that PPH is preventabte
these figures represent nothing less than a tragedv
The most effective intervention known fbr PP}
prevention is active management of the third stage o
Jabor by a skilled attendant, shown to reduce thc risl
of PI)H by more than 6096 (Prendiville, Elbourne, 8
palcDonald, 2000). This intervention is currently define(
as administration ofa uterotonic drug within 1 minute o
newborn deliverM controlled cord traction with placenta
delivcrB and uterine massage after placental deliver]
(ICM & F]GO, 2003). Although the relative contribution:
of cord traction and uterine massage are unlmown, utero・
tonic drugs can cfll]ctively prevent PPH in the absence o
these components (Cotte4 Ness, & [[blosa, 2001; Dermai
et al., 2006). In settings where active management of th`
third stage cannot be implemented because of a lack o
skilled attendants, WHO strongly recemmends that :
uteretonic drug still be offered by a health worker traine(
in its usc fbr PPH prevention (WHO, 2007b),
Uterotonic drugs may operate through differen
mechanisms efaction, but all essentiallywork to increasc
uterine contractility and inhibit bleeding from the site o
placental separation. WHO recommends oxytocin as tlu
most effective uterotonic drug with the fewest advers4
sidc cffbcts (WHO, 2007b), Howeve4 a recent review o
this drug calls for more evidence to better assess trade
offs and benefits (Cotter et al., 2001). Although als(
effective, use of misoprostol for PPH prevention ma]
result in maternal feveB shivering, or more cases ofsevert
PPH that require therapeutic uterotonics (Giilrnczoglu
Forna, VillaB & Hoime}rr3 2007). Ergometrine and Syn
tometrine (a combined ergometrine and oxytocin drug
can cause nausea or vomiting and are contraindicated ii
the presence of heart disease or hypertension, The bal
ance of evidence does not support use of ergot alkaloid,
alone to prevcnt PPH (Cotter et al,, 2001; Liabsuetrakul
Choobun, Pecyananjarassri, & Islam, 2007),
ttt t tttt/ttly"t
.
shtcD"',"
1 '

Expandlng Pestpartum Hemotrhage Preventien to Community Contexts Spangleretal, 41
Besides effectiveness and side effects, uterotonic
drugs also differ with respect to route ofadministration,
storage requiremcnts, and costs. Oxytocin is typicaly
given via intramuscular injection or intravcnous drip,
and loses potency in temperatures higher than 30eC
(Hogerzeil, NVlalker, & de Goeje, 1993), Ergometrine is
also given parenterallM but is Iess stable than oxytocin
in high tcmperatures and is sensitive to light (Hogerzeil
& XValkcr, 1996). Administratjon routes for misoprosto]
includc oraL sublingual, buccal, or rectaL but the pre-
ferred reute remains unclear. This drug is stable with
respect to both heat and light. Whereas the acquisition
costs of uterotonics vary by context, the administra-
tion costs of misoprestol may be Iower than for drugs
requiring injection. Because misoprostol does not need
a cold chain, its storage costs are also likely to be less
than those ofother uterotonics.
CRtTICAL CONSIDERMIONS FOR EXIIANDINGPPH PREVENTION TO THE COMMUNITY LEVEL
1tt this point, we return to the question-should PPH pre-
vention methods be expanded to the community level? By
taking a context-based approach (i.e,, realizing the answer
"till not be the sanie in all placcs and at all times), we can
pethaps put fonh a more practical inquir}r: Where and
underwhatcircumstancesdoesltinakasensetoimplement
uterotonics at the communi"r level? XVhich drug should be
used in what settings? [Ib address these questions, we iden-
tify four critical considerations to take into account when
making decisions regarding PPH prevention.
Where is Childbirth Happening?
According to nationally representative survcys, the pro-
portion ofbirths attended by an accredited health profes-
sional(midwife,doctoBnurse)isabout62%indeveloping
regions. By convention, the global health community
refers to these births as taking place with a skilled atten-
dant, although data on the specific ski11s and training
of these providers are lacking. Ulsing this definitien,
births with a ski11ed attendant appear to be increasing
in ali rcgions except in sub-Saharan Afi:ica and Oceania,
where usc remains stagnant or has decreased over time
(WHO, RHR, 2008). With few exceptions, dclivery with
a health professional translates into facility-based birth.
Howeveq data on births attended by health pro fessionals
do not indicate at what kind of facility births are occur-
ring. rLb cxplore this issue, we examine DHS data from 15
geographically representative countries in sub-Saharan
Africa and South Asia (DHS, 2008a). Given the data
source, we acknowledge that some misclassification is
possiblc between public low-level facilities and govern-
ment hospitals. In addition, fa[ilities labeled "privatc"
can encompass anything from one-room dispensaries to
fully fimctional hospitals.
Figures 1 and 2 give the pcrcent distributions for
delivery place, Most notablM a good deal of childbirth
occurs at the community leveL Among the African
countries, Ethiopia has the highest proportion of home
binhs at an estimatcd S8%, whereas Nigeria is at 66% and
Ghana, '1'anzania, Uganda, and Zambia hover around the
midpoint. Adding public low-level facthties, community
births are more than 60% in evcry country except South
Aftica. Deliveries in government hospitals vary from 6%
DRC Ethiepia(2007) (2005)
FIGURE 1
Nigcria
(2ooa)
'I'anzania
(2004-05)
IJgnnda
(2006)
Percent distributions tbv place of dcl lver
Zambia(2ee7)
- Othe[ Location
- Private FacMty
D Govcrnment Hospital
1 Public [.ow-Leve] Facility
l Homc
yrsub-SaharanAfrica.
/tttt

42 Expanding Postpartum Hemorrhage Preventlon to Community Contexts SPangter et aL
FIGURE 2 Percent distributions fbr place of deliverltSouth Asia.
te 69%, but in rnost countries fall between 10% and 20%.
An even greater majority of births take place in the com-
munity among South Asian countries, with home births in
Bangladesh and Nepal reaching 83% and 81%, respectively
wrth the exception of Vietnam, deliveries in public low-
level facihties are minimal, varying from only 1% to 5%.
Tbeends in home births for the cited countries with
at least three DHS surveys over the past 20 years are
shown in Figures 3 and 4 (DHS, 2008b). The picture in
sub-Saharan Africa is varied. Ghana shows a decrease
of 15 percentage points in home births between 2003
and 2008. From the early 1990s through 2007, the
proportions ofhome births in Zambia and Uganda have
remained essentially unchanged. Nigeria and 1[hnzania
exhibit increases, jurnping eight percentage points in
Nigeria and five percentage points in [fanzania between
the early 1990s and the middle of the current decade.
In contrast, South Asian countries show steady declines
for this period, dropping from 23 percentage points in
Indonesia to 10 percentage points in Nepal. Although
these trends cannot absolutely predict where births will
occur in the future, when put into economic and politi-
cal context, they rnay give a sense of what is 1ikely to
happen in the short term.
FIGURE 3 Irends in home delivery-Sub-Saharan Africa.
Ghana
Nigeria
fanzania
Uganda
Zambia
r-v

Expanding Postpartum Ftemorrhage E'revcntion to Community Contexts Spangleret aL 43
IOO
90
80
70
60
50
40
30
20
!o
FIGURE4 'Frendsin] iome delivery-SouthAsia.
Banoladesh
lndia
lndonesia
Nepal
1'hilippines
Although place of delivery does not speak to
quality of services, it does indicate the type of care
women are accessLng in particular localities. Provided
that the data give a fair depiction, fbcusing efforts on
public low-level facilities may not greatly increase PPH
preventton in some countries, but the rnajority could
benefit from home-based intervcntion. Besides nation-
al-lcvel data, policymakers may also want to consider
delivery place at the district ievel or among even more
distinct communities within their jurisdiction.
Which Wbmen are Delivering Where?
Por a given lecalit$ it is necessary to consider vvhich
women are receiving what services by econemic and
sociodemographic characteristics. Analyses of DHS
data in up to 56 countries find enormous differences
between wealthy and poor groups in proportion of
deliveries with health professionals-a gap greater than
that of any other maternaL reproductive, or child
hcalth service examined (Gwatldn, Bhuiya, & Victora,
2004; Houweling, Ro nsmans, Campbell, & K"nst, 2007).
Country-$pecific studies also report significant positive
associations between economic status and deliveries
with health professionals or in health facilities (Anwar,
Killewo, Chowdhur" & Dasgupta, 2005; Mrisho ctal., 2007; Say & Raine, 2007; fann et al., 2007; Thind,
Mehani, Banerjee, & Hagigi, 2008; Yhnagisawa, Oum,
& Wakai, 2006).
Averaged across the 15 countries we have been
cxamining, Figures 5 and 6 give the percent distribu-
tions of delivery place by wealth quintiles. ClearlM
FIGURE5 Percentdistributions forplace ofd cliver yby wea]th quintiles-S
- Othcr
D Private FaciUty
o Govcmment Hospltal
- Public Lew-Levcl Facility
- Home
ub-Saharan Mica.
ma,lt./.

44 Expanding Postpartum Hemorrhage Prevention to Community Contexts ij)angter et al,
FIGURE6 Percentdistributions fo r placc of deliver
- Other
m Iirivate Faeilits,
m Cloveunrnent HDspital
- Pubtic Lew-Level Facility
- Home
y by wealth quinti]es-South Asia.
home delivery is inversely related to wealth. In the Afri-
can countrics, S6% ofwomen deliver at home, but these
births occur among approximatcly 75% of the poorest
group and 19% of the wealthiest, About 67% ofbirths
in the South Asian countries take place at home, but
these occur among 899'e of the poorest and 29% of the
wealthiest. In contrast, deliveries in government hospi-
tals and private facilities increasc up the wealth spec-
trum in both regions. Births at public low-level facilities
are relativcly consistent across wealth quintiles, ranging
from 15% to 20% fbr African countries and 2% to 8%
f6r South Asian countries,
Figures 7 and 8 show percent distributions of
delivery place by area of residence averaged across the
selectedcountrics,indicatingthatmosturbanbirthstake
place in govcrnment or private faci1ities, and most rural
births occur at homc. A number of studies documcnt
the cffect ofrural rcsidence on delivery care (Houweling
et al., 2007; Say & Raine, 2007; Stephenson, Baschieri,
Clcments, Hennink, & Madise, 2006; Thind et al., 2008),
Additional sociodemographic factors associated with
the use ofhealth facilities or health pro fessionals at birth
include education, age, parity3 marital status, occupa-
Lion, women's autonomB cthnicity; and religion-where
the direction and strength ofassociations are spccific to
context (Anwar et al., 2005; Bloom, Wypij`, & Das Gupta,
20el; Glei, Goldman, & Rodriguez, 2003; Mekonnen &
Mekonnen, 2003; Mpembcn{ et al., 2007; Mrisho et al,,
2007; Paul & Rumsex 2002; Stekelenburg, Kyanamina,
Mukelabai, Mlolffers, & van Roosmalen, 2004; Stephen-
son et aL, 2006; Tann et al., 2007; Thind et al., 2008;
Ylinagisawa et al., 2006).
FIGURE7 Percentdistributionsfo r place ofdelivcry by area of residence-Sub-SaharanAfrica.
eu・'

Expanding Postpartum Hemerrhage Prevention [o Community Contexts 51)angler etaL 45
90V,
80W,
70W,
60%
50%
40,%
30W,
20Y"
IOW,
oys
FIGURE8 Perccntdistributionsfo r place of delivery by area of resi
- Other
m I'rivate F:tcility
o Government Hespital
- Public Low-Levc] ];aeility
- Home
dence-SouthAsia.
Thus, cven in countries where institutional birth
appears on the rise, certain women are not receiving
this care. Better-off women receive care in higher level
faciliti'es with more highly skilled attendants, whereas
disadvantaged women deliver in the community with
attendants lacking in formal medical training. Without
explicit effbrts to reach these groups, irnplementation
ofthe strategy to increase medicaLly skilled care at birth
could be supporting inequitable outcomes (Gwatkin,
2005). HoweveB services that target excluded popula-
tions could mitigate this result-such as providing PPH
prevention in the communits whcre most marginalized
women are delivering,
Capacity ofLocal Hbalth Care Elystems to Provide
ObstetricServices
Coverage of obstetric scrvices in public and private
sectors must be assessed. If coverage is low and home
births are high, commuiiity-based PPH prevention
seems a reasonable plan. If coverage is high, the best
approach may be to improve access to this care and
ensure arrailabllity of uterotonics in facilities. Although
skilled attendance is the ideal package of services, as an
intervention it can be difficult to assess. Competencies
of skilled attendants may not match up with evidence-
based standards (Harveyct al., 2007), and guidelines t'or
whether an environment is enabling are not available.
Emergency obstetric care (EmOC) might offl]r a more
practical means of assessment becausc its monitoring
tools categorize facilities according to nine signal func-
tions, The recommended level for adequate coverage is
five EmOC facilities per 500,OOO population, at least one
ofwhich must qualify as cemprehensive EmOC (WHO,
United Nations Population Fund [UNFPA], United
Nations Children's Fund [UNICEFI, & Averting Mater-
nal Death and Disabilit}r [ArvlDD], 2009). VVle caution,
howeve4 that such assessment does not speak to quality
ofcare or to the capacity to proyide PPH prevention,
Coverage ofhcalth professionals and their skiIls in
safe delivery should also be taken into account. In 2008,
47% of women in Africa and 6S% of wornen in Asia
were attended by a health professional (WHO, 2008),
although the proportion of womcn receiving PPH pre-
vention is unknown. Making activc management ofthc
third stage of Iabor part of standardized curricula for
pre- and in-service training could increasc PPH preven-
tion coverage considerably. However, training in physi-
ological management for improving quality and safety
should not be neglected, especia!I〉F in settings that donot or cannot consistentiy employ active management.
For contexts where skilled health professionals are in
short supplB the potential for task shifting PPH prc-
vention to an existing lower skilled (fbrmally trained)
health worker cadre should be assessed-particularly
for injectable drugs but also for administering miso-
prostol, In adclition to health workers, local resources
such as women's groups, health advocacy committees,
community lcaders, and traditional birth attendants
(TBAs) should be recognized fbr their ability to assist
with sensitization as well as logistics.
Other important issucs that deserve consideration
involvc processes ofdrug registration, distribution, and
storage, Oxytocin and ergot alkaleids are registered
in most countries for PPH prevcntion and treatment,
althoughnotnecessarilyoxytocinT"inUniject,Misopros-
tol is widely rcgistercd for gastric ulcers and unspecified
obstetriclgynecological cenditions but is registered for
PPHin only 11 countries ofsub-Saharan Africa and four
L-・'il・{,/1?..4, 1・--- ..."J ,..t.-...・ /・・..-//・..-・
Ftt"
t
'
r
46 Expanding Postpnrtum 1-lemorrhage Prevention to Community Contexts Spangleret al.
countries ofSouth Asia (Vcnture Strategies Innovations,
2010). Although off-label use is common, Ministries of
Health that choose to strategically promote misoprostol
fbr PPH prevention will necd to officially register it for
this purpose, Distribution pathways from dru.a manu-
facturers to recipicnts inust also be assessed, especially
transportation and storage mechanisms for drugs that
are sensitive to heat or light-including the potential to
upgrade the supply chain in this respect.
oriteria for Selecting Specijic Uterotonic Drugs
At a minimum, criteria for the selection of uterotonic
drugs include effectiveness, safet" feasibility; cost-
effectiveness, and acccptabilitv Effectiveness essentially
refers to the ability of the intervention to decrease
PPH incidence in real world settings, As noted in the
background section, the literature supports ox〉tocin asthe most effective uterotonic drug for PPH prevention,
However, misoprostol also exhibits a credible degree
of effectiveness and is often recommended for settings
where ox}tocin is unavailable despite its side effects of
fever and shivering (Alfirevic, Blum, Walraven, Weeks,
& Winikoff; 2007; 1,angcnbach, 2006; WHO, 2007b).
Ergot alkaloids are comparablc to o)cytocin in effective-
ness, but are gencra1ly not preferable because of the risks
of nausea, vomiting, and clcvatcd blood pressure.
Safety refers to the likclihood of adverse events
such as dosage errors, ncedtc sticks, and mistimed
administration or inappropriate use of uterotonics-
the latter of which can potentially contribute to fetal
asphyxia or uterine rupturc. Three observational studies
in Tanzania, Nepal, and Afghanistan evaluate the safety
of community-based misoprostol with measures of dos-
age, timing, and side effects (Prata, Mbaruku, Gross-
man, Holston, Hsieh, 2009; Rajbhandari et al,, 2010;
Sanghvi et al., 2010); aU conclude the intervention is
safe, but none spccify a safety threshold for the param-
eters assessed. The WI IO's published statements on use
of misoprostol at the community level stress that it has
withheld recommending distribution during pregnancy
for use after delivery because its potential benefits and
harmsareunknown(WHO,RHR,201O).Severalstudiesdocument misuse of uteretonics for labor augmentation
(Flandermeye4 Stanton, & Armbrusteg 2010; Fronc-
zak, Arifeen, Moran, Caulficld, & Baqui, 2007; IyengaB
lyengar, Martines, Dashora, & Deora, 2008; Jeffery Das,
Dasgupta, & Jeffery 2007). "1'hese studies collectively
suggestthatintramuscularjnjectionofox〉tocinbybirthattendants lacking formal medical training is especially
common in South Asia. Establishing the risk of this
practice for health outcomes at the population level
needs furthcr research.
Feasibility refers to the capability of a given con-
text to properly implement uterotonics in communi-
ties, including storage, distribution, administration, and
disposal. To improve feasibility of oxytocin in terrns of
storagc, TI Pharma has initiated a program to deyelop a
heat-stablc formulation (Hawe et al., 2009). Meanwhile,
oxytocin'" in Uniject (a device designed to ensure cor-
rect dosing and minimal needle reuse) is equipped with
a timc-tcmpcrature indicator that increases its utility in
the field (PATII, 2008). Irljectable oxytocin also requires
that someone trained to administer this drug is present
at birth, and there is not a standard solution for needle
disposal in home settings, The cited studies in Nepal and
AfghanistandistributedmisoprostolforPPHprevention
through Iow-lcvcl hcalth workers or community volun-
teers; from womcn's self-reports, the former study found
that utcrotonic coverage in the study site increased
from about 12% to 2496, whereas the latter found that
nearly 70% of women offered with misoprostol, used it
(Rajbhandari et aL, 2010; Sanghvi et aL, 2010).
Although a component of feasibility, cost-effectiveness or efficiency is critical enough to deservc
its own mention. Different methods of giving oxytocin,
misoprostol, ergometrine, and Syntometrine at facility-
based births in developing countries have all been fbund
to bc cost-ethctive, but a comparative study reports
oxytocin to be the most eencient-although differences
betwecn somc methods had little practical significance
(Seligman & Liu, 2006). An anarysis of misoprostol fbr
PPH prevention at home births in India demonstrated
a 38% decrease in maternal deaths, with an incremen-
tal cost of $1,401 per life saved, compared to $IO,532
per life saved fbr comprehensive EmOC (Sutherland
& Bishai, 2009). Another model based on countries
in sub-Saharan Africa confirms the cost-effectiveness
of misoprostol at home births (Prata, Sreenivas, et al.,
201O). Still needed is a tool for cost-effectiveness evalua-
tion that can be adjusted to suit the changing conditions
ofspccific country contexts.
FinallF cven ifa particular intervention is shown
to be etTective, safe, feasible, and eMcient, the ques-
tion remains as to whcther it will be acceptable. At the
national policy level, some countries may be reluctant
to initiaLe community-based activities when facility-
based births arc bcing promoted Misoprostol may face
political barrlers over concerns about its abortifacient
propcrtics, Reccntlyl two key articles shed light on how
political priority for maternal mortalit〉T is generated(Shiffman, 2007) and how research is translated into
- ・ 7mpT:. ,'Tlll.i .ilde,'an'"・ ' 1 1il urx'-"' za' L"aww・ ;.t.I・l
/.t.;t.t
lt/il'
/./t

s
i"'
.l,
'
Expanding Postpartum Hemorrhage Prevention to Communlty Contexts Spangler etal. 47
policy in poor and transitional countries (Woelk,
Daniets, et al,, 2009), The critcrion of acceptability a!so
applies to health workers, childbcaring womcn, and
their families, At all levels, in-depth evidencc on the
acceptability of community-based uteretonics for PPH
prevention is limited, ・
NEXT STEPS
By addressing the earlier considerations, policymakcrs
can begin to identify where and under what circum-
stances PPH preyention might be expanded to the com-
munit}c Such contexts might include places with high
proportions of deliveries in homes or low-ievel facilities,
poor ceverage of obstetric services, and low ljkelihood
of a rapid shift to facility births. Even in contexts whcre
fewer women deliver at home, if these women are sys-
tematically disadvantaged, tliey should not be excluded
fi:om PPH prevention interventiop, Lastly, lecal condi-
tions must be favorable for a specific uterotonic drug;
that is, a drug considered safe, feasible, and acceptable.
As Gwatkin, Wagstaffl and Yazbeck (Gwatldn, Wagstaff]
et al., 20e5) state in the "brld Bank Report Reaching the
Poor, `CThe challenge is to find the approach that works
best in a particular setting in dealing with a particular
issuc" (p. 47).
Although a large and rigorous body of evidence
supports methods of PPH prevention, research gaps
remain, Some research priorities spec]fied by WHO
inciude determining whether oxytocin cari be safely
administered by unskilled attendants, understanding
which components of active management of the third
stage of labor are rnost effective, establishing the best
doselrouteofadministrationformisoprosLoLandexplor-
ing the role of buccal or sublingual exytocin (NVbrld
Health Organization, 2007). More information is also
needed on the safety of introducing uterotonic drugs to
communities, sustainable soluLions for feasibilit}g cost-
effectiveness of various options in particular localitics,
and the acccptability of7demand for communiLy-based
PPH prevention among policymakers, health workers,
and intended recipients of this intervention.
Another gap involves the potential implications
of community-based PPH prevention for other mater-
nal health interventions, Rajbhandari et al,'s (2010)
observational study examining the distribution of
misoprostol in Nepal rcported an increase of four per-
centage points in institutional delivery over the coursc
of the implementation period (Rajbhandari, Hodgins,
et al., 2010). Asidc from this exampie, eyidence for the
effect of community-based interventions on facility-
ba$ed care is scarce-an implication that should be
bettcr understood, evcn if it can't be well predictcd.
As uterotonics can be cmployed for multiple purposes,
the potential for misuse should also be seriously con-
sidered, If uterotonics are widely available, how often
rnight they be used unsafely for labor induction or aug-
mentation? Might an education or other kind ofinter-
vention effectively prevent such ]nisuse? Lastl)1 there
are implications for active management of the third
stage of labor and PI'H treatment If a uterotonic is
routinely being glven by someone trained to administer
it, could this person also be trained to perform uterine
massage? "rhen, where, and how should treatment be
initiated when prevention is being implementcd? Thcse
questions still need to be addressed.
More research is needed before global recommen-
dations can be issued (i.e,, implementing community-
based PPH prevention where more than SO% ofbirths
occur at home, or where more than 759'o of the poor-
est women delivcr at home). But even with surncient
evidcnce to support PPH prevention, it is possible
that a global consensus will not bc reached bccause of
the ongoing debate over commvnit〉T- versus facility-based intcrventions. In the meantime, stakeholders in
resource-poor countries continue to shape maternal
health policies. We propose Figure 9 as a checklist to aid
in assessing crltical considerations for cemmunity-based
PPII prevention. Not all countries will be able to com-
plete the checklist in fuII, but by using what data is avail-
able, this tool can assist policymakers in determining
what realistically suits their needs. In particular, it can
help answer the questions of where and among which
populations a specific intervention will likely produce
the greatest benefit. We stress that these considerations
should be applied to district or community levels as well
as to the national level because varying contexts within
a country may warrant different approaches to PPH
.PreVelltlOll.
CONCLUSION
Communit〉r-based PPH prevention can act as a com-plement or a supplement to skil]ed attendance. This
intervention is not a replacement for, a move away
from, or a reinterpretation of more comprehensive
strategies. Rather, it is a targeted action for augment-
ing health systcms that can be adapted to chang-
ing cenditions; if facility births increase in a given
poputation, it can be scaied back accordinglyL PPH
maC/,/1..'h・,i,',tt/

48 Expanding Postpartum Hemorrhage Prevention to Community Contexts SPangler et al.
PlaceofBirth
Proportienofbirthsoccurringathome
Proportionofbirthsoccurringinhealthfacilities
Publicfacilities
-Hospitals
-Healthcenters
-Healthpostsordispensaries
Privatefacilities
-Hospitals
-Healthcenters
-Healthpostsordispensaries
PlaceofBirthbySociodemographicCharacteristics
Proportionofbirthsoccurringathomebywealthquintiles
Proportionofbirthsoccurringathomebyothercharacteristicsthatmaybesalientforaparticularcontext
-Age
-Parity
-Ethnicity
-Education
-Indicatorsofwomen'sautonomy
ObstetricServicesDistribution
CoverageofEmOCfacilitiesper500,OOOpepulation
-ComprehensiveEmOCfacilities
-BasicEmOCfacilities
UterotonicDrugRegistrationforPPHPreventionandOtherUsesOxytocin
Misoprostol
Otheruterotonicdrug(specify)
SupplyChainReliabledistributionofdrugstopointsofservice
-Availabilityofuterotonicdrugsinruralareas
Coldchainforgeneraldrugdistributionandstorage
-Extensivetoremoteruralareas?
-Inclusiveofoxytocin?
HealthWorkersSki11edattendants:doctors,nurse-midwives,nurses,andotherprofessionalhealthworkerstrainedinsafedeliveryskills
-Coverageperpopulation
-CurrentlytrainedinPPHpreventionfAMTSL?
Community-levelhealthworkers:existingcadretrainedtoprovidePPHprevention(orcadrethatcouldbetrainedinthisskil1),
-Coverageperpopulation
-Legallyallowedtogiveinjections?
SpecificUterotonicDrugsforLow-LeyelFacilitiesandHomeSettings(oxytocin,misoprostol,otherdrugs)
Safeimplementation
Feasibleferservicedelivery
Cost-effective
Acceptableamongpolicymakers,healthworkers,andpopulation
Nbtes.AMTSL,activemanagementofthethirdstageoflabor;EmOC,emergencyobstetriccare;PPH,postpartumhemorrhage.
FIGURE9 Criticalconsiderationsforcommunity-basedPPHprevention.

Expanding Posti)nrturn Hemoirhage Ptovention to Community Contexts Sl)nngler et al. 49
prevention is in no way a final solution fbr PPH, but
it is capable of rcducing the incidencc ofthe problem,
and its use in communities can be implemented in
conjunction with improving access to and quality of
referral-level carc. After alt, community-level inter-
yentions and facility-focuscd services are not either-or
propositiens, NVith increasing evidence to suggest
that investing rcsources in community interventions
can reduce maternal mortality (KidneM Winter, et al.,
2e09; Pagel, Lewycka, et al., 2009), the two strategies
should be pursued alongside each other as dictated by
the needs ofa given context.
MultipleoptionsexistevensvithinPPHprcvention-
there is no one solution for all countries and individual
countries need not adopt a singular approach, Buekens and
Althabc (Buekens & Althabe, 2010) argue that although
oxytocin is the drug of choice, at this point in time, both
oxytocin and misoprostol have a place in preventing PPH.
Fundamentall〉r, the geal is to expand a medical advancethat improves maternal health and suwival to women
who are not reaching skilled care-in whatever ways this
goal can be effLtctively accomplished. Despitc a lack of
clear guidelines, we advocate fbr a carefu1, context-based
approach to determining whcre and how such expansion
might bc carried out, Commimity-based PPH prevention
can be part ofa national push to target reduction ofPPH as
an achicvable goaL Decisions with respect to this interven-
tion need not be postponed awaiting a global consensus
that may never be achieved.
REFERENCES
Alfirevic, Z., Blum, J., WtLlravcn, G,, Weeks, A., & Winikofll
B. (2007), Prevention of postpartum hemorrhage with
misoprostol, fnternationai fournal of Onecology and
Obstetrics, 99(SuppL 2), S198-S201.
Anwar, A. I,, Killewo, J,, Chowdhur" M. E. E. K,, & Dasgupta,
S. K, (200S). Bangladesh: Inequalities in utilization of
maternal hea]th care services-evidence from Matlab.
Tn D. R. Gwatkin, A. Wagstaffl & A. S. Yazbcck (Eds.),
Reaching the poor ivith health, nutrition, and popula-
tion services: VVhat works, what doesn'4 and wby (pp.
I 17-136). Wlishington, DC: The Wt)rld Bank.
Bloom, S. S,, "lypij, D,, & Das Gupta, M. (2001), Dimensions
of women]s autonomy and the influence on maternal
hcalth care utilization in a north Indian city Demagra-
phy, 38(1), 67--78.
Buekens, R. & Althabe, F. (20lO), Post-partum haemorrhagc:
Beyond thc confrontaLion between misoprostol and
oxytocin, The Lancet, 375(9710), 176-178,
Canipbell, O. M., & Graham, WL J, (2006). Strategies for reduc-
ing maternal mortality: Getting on with what works,
The Lancet, 368(9543), 1284-12Y9,
Cotter, A. M,. Ness, A., & 'Ib]osa, J. E, (2001). Prophylactic
oxytocin for the third stage oflabor, Cochrane Databasc
of Systematic Reviews. Issue 4. Art, No,: CDUOI808. doi:
10,1002Il4651858.CDeO1808
Dertnan, R. J., Kodkany; B. S., GoL,diir; S. S., Gelle; S. E.,
Nalk, NC A., Bellad, M. B,, ... Moss, N. (2006), Oral
misoprostol in preventing postpartum haemorrhagc in
resourcc-poor communities: A randomised controlled
trial. Tlhci Lance4 368(9543), 12i18-1253.
Demographic and Health Surveys, (2008a), Bangic;desh, Dem-
ocrutic Revmblic of Conga Ethiopia, Ghana, bidia, indo-
nesia, IVet)al, Nigeria, t'akistan, Pliilmpines, South Mica,
Tlanzania, tiganda, Vietnam, Zambia. Retrieved froin
http:!A"vw.measurcdhs.com/accesssurveysl
Demographic and Health Surveys. (2008b). Bangladesh,
Ghana, India, bidonesia, Nepal, Nigeria, Philippines.
Tlinzania, Uiganda, Zambia, Retrieved from http;ltwww.
measuredhs.comlaccesssurveysl
Flandermeyer, D., Stanton, C., & Armbruster, D. (2010).
Uterotonic use at heme births in low-income countries:
A literature reviewL International Jburnal oj' Clynecol(zgy
and Obstetrics, 108(3), 269-275.
Fronczak, N,, Arifeen, S. E,, rvloran, A. C,, Caulfield, L, ll., &
Bagui, A. II. (2007). Delivery ptactices of traditional
birth attendants in Dhaka slums, Bangladesh, Jburnal (lf
Ifealth, Population, and Nutrition, 25(4), 479-487,
Glei, D. A., Goldman, N., & Rodrigucz, G, (2003). Utilization
ef care during prcgnancy in rural Guatemala: Does
obstetrical need matter? Social Science 6 Medicine,
57(12),2447-2463.
GUImczoglu, A. M., Forna, E, Villar, J,, & Hofmeyr, G. J.
(2007), Prostaglandins for preventing postpartum hae-
morrhagc. Cochranc Database of Systematic Reviews.
Issue 3. Art, No.: CDOO0494. doi: 10.1002114651858.
CDOO0494,pub3
Gwatkin, D. R. C2005), How much would poor people gain
from faster progress towards the MMennium Devcl-
opment Goals for health? The Lancet, 365(9461),
813-817.
Gwatkin, D. R., Bhuiya, A., & Victora, C. G. (2004). Making
health systems more equitable. Tlhe Lancet, 364(9441),
1273-1280,
Gwatlcin, D, R., WhgstafC A., & Yazbeck, A. S. (2e05). What did
the reaching the poor studies find? In D. R. Gwatkin, A.
NVagstafC & A, S, Yazbeck (Eds.), Reaching thepoor ivith
health, nutrition, and population services: What works,
vvhat doesn'4 and rvPry (pp. 47-61), Washington, I)C:
TheWorldBank,
tt.t.i.Ll-. t.-.,.t,,.'. "・.;-vt--au.wh

lt
50 Expanding PostFmrtum Ftemorrhage Prevention to Community Contexts SPnngler etal.
HarLres S. A., Bland6n, Y. C., McCaw-Biims, A,, Sandno, I.,
Urbina,L,,RodrfquezC,,...Djibrina,S,(2007).Areskilled
birth attendants rea]ly skillecl? A measurement method,
sorne disturbing results and a potential way fbnvard. Bttl-
letin of the Ltlorid JJtialth Organization, 85(10), 783-790,
Hawe, A., Poole, R., Rorneijn, S., Kasper, R, van der Heijden,
R., & Jiskoot, WL (2009). 'Ibwards heat-stable o)cytocin
formulations: Analysis of dcgradation kinetics and
identificationofdcgradationproducts.Pharmacolagical
Research,26(7),1679-1688.
Hogan, M, C,, Foreman, K. J., Naghavi, M., Ahn, S. YL, Wang,
M., Makela, S. M., . . . MurraM C, J. (2010). Maternal
mortality for l81 countries, 1980-2008: A systematic
analysis of progrcss towards Millennium Development
Goal 5, TV!e Lancet, 375(9726), 1609-1623,
Hoge rzeil, H. V, & Wlilker, G. J. (1996). Instability of(methyl)
ergometrine in tropica] climates: An overview, Ettro-
pean Jottrnal ofObstetrics, Ci},necology andRaprodttctive
Biology,, 69(L), 25-29.
Hogerzeil, H, V, Walker, G. J., & de Goeje, M. (1993), Stabil-
ity of itu'ectable o)q,tocics in tropical cJirnates, Geneva,
Switzerland: World Health Organization,
Houweling, T. A., Ronsmans, C., Campbell, O. M., & Kunst,
A. E. (2007). Hitge poor-rich inequalities in rnaternity
care: An international comparative study of maternity
and child care in developing countries, Bulletin oj' the
VVlorld Hbalth Organization, 85(10), 745-754.
International Confederation of Midwives, International Fed-
eration of Gynecology and Obstetrics. (2003). joint state-
ment: Mtinqgement of the third stage qf labor to prevent
postpartqm haeinorrliage. Rctrieved from http:f/www.
pphprevention.orgMlesllCM-FIGOJoint-Statement.pdf
I}rengar, S, D,, Iyengar, K., Martines, J. C., Dashora, K,, &
Deora, K. K. (2008). Childbirth practices in rural
Rajasthan, India/ Implications for neQnatal health and
survivaL Journal ofI)erinatoiog〉,, 28(Suppl, 2), S23-S30.
Jeffery, R, Das, A,, Dasgupta, J., &Jeffery, R. (2007), Unmoni-
tored intrapartum ox}stocin use in home deliveries:
Evidence froin Uttar 1]radesh, India, Reproductive
Health Matters, 15(30L 172-I78.
Khan, K, S., WOjdyla, j)., Say; 1., GOImezoglu, A. M., & Van
Look, R E (2e06). WHO analysis of causes of maternal
death: A systcmatic rcvicw/ 7Vie l,ancet, 367, 1066-1074.
KidneM E., Winte4 II. R., Khan, K. S., GUImezoglu, A. M,,
Meads, C. A., Deeks, J. J., & ",lacarthur, C. (2009). Sys-
tematic review of effect ef comfnunity-level interven-
tions to reduce maternal mortality BMC Pregnancy and
Chitdbirth, 9, 2.
Langenbach,C,(2006),Mjsoprostolinpreventingpostpartum
hemorrhage/ A mcta-analysis, Jnternational Journal of
Gynecologr, and Obstetrics, 92(1), 10-18,
Liabsuetrakul, T,, Choobun, T:, Peeyananjarassri, K., & Islam,
Q. M, (2007). Prophylactic use of ergot alkaloids in
the thircl stage of labour. Cochrane Database of Sys-
tematic Revie}vs. fssue 2, Art, No,: CDO054S6, doi:
10,1002f146S1358.CDO05456.pub2
rvlekannen, Y,, & Mekonnen, A, (2003). Factors influencing the
use of maternal healthcare services in Ethiopia. Journal of
Jicatth, Population, and Nittrition, 2J(4), 374-382.
Mpcmbcni, R. N., Killewo, J, Z., Leshabari, M. r, Massawe,
S. N., Jahn, A., Mushi, D., & Mwakipa, H, (2007), Use
pa(tcrn of maternal health services and determinants
of skil]cd care during delivery in Southern Thnzania:
Implications for achievement of MDG-5 targets. BMC
Pregnaitcy atid Childbirth, Z 29.
Mrisho, M., Schcllenberg, J, A,, Mushi, A, K, Obrist, B.,
Mshinda. H., 'ranner, M., & Schellenberg. D. (2007).
Factors affecting homedelivery in rural Tanzania, TVqi)-
ical Nfedicine and ln ternational Health, l2(7), 862-872,
Pagel, C., Lewycka, S., Colbourn, Tl, Mwansambo, C, W,
Meguid, T., (]hiudzu, G., . . , Costello, A, rvl, (2009). Esti-
rnationofpotentialelkctsofimprovedcommunity-based
drug provision, to augment health-facili"t strengthening,
on ;naLernaL mortality due to post-partum haemorrhagc
and sepsis in sub-Saharaii Africa: An equity-efflectiveness
model.IVieLartcet.374(9699),1441-1448.
Partners for Appropriate 'fechnology in Health. (2008). Intro-
d[{cing orytocin in the Uitiject device: An overvieiv Jior
decision makers. Seattle, WA: Author,
Paul, B. K., & Rumse" D. J. (2002), Utilization of health
I'acilities an(] trained birth attendants for childbirth in
rural Bangladcsh: An empirical study Social Science de
Medicine. 54(12), 1755-1765.
Prata, N., Mbaruku, G., Grossman, A. A,, Holston, M,, &
IIsieh, K. (2009). Community-based availability of
misoprostol/ Is it safe? ij'ican Jottrnal ofRaprodttctive
Health, l3(2), 1 17-128,
Prata, N,, Sreenivas, A., Greig, F., X・Xla]sh, J., & Potts, M. (20la).
Setting priorities for safe motherhood interventions in
resource-scarce settings. Health Policy, 940), 1-13,
Prendivillc, W J. P, Elbourne, D., & McDonald, S. J. (2000).
Active versus expectant management in the third stage
of labor. Cochrane Database of Systematic Reyiews.
Issue 3. ArL No.: CDOOOO07. doi: 10.10e2/14651858.
C]DOOOO07
Rajbhandari, S., Hodgins, S., Sanghvi, H., McPherson, R.,
Praclhan, Y V, Baqui, A, H,; Misoprostol Study Group.
(2010). Expanding uterotonic protection fo11owing
childbirth threugh community-based distributlon of
misoprostol: Operations research study in Nepal, Inter-
nationat Journai of Gynecology and Obstetrics, 108(3),
282-288.
''.,・'r3-/'as..i;.e"-paaniltaC'uaSliti' '
.g,tl'i""
'

Expanding Postpartum Hemorrhage Prevantion to Cornmunlty Conlexts Spangier et aL 51
SanghvL H., Ansari, N,, Prata, N. J., Gibson, H,, Ehsan, A.
T, & Smith. J. M. (2010). Prevention of postpartum
hemorrhage at home birth in Aighanistan, Internationat
Journal of Clynecology and Obstetrics, 108(3), 276-281.
Say; L., & Raine, R. (2007). A systematic review of inequali-
ties in the use of maternal health care in developing
countries: Examining the scale of the problem and the
importance of context. Bulletin oj' the Vforltl Health
Organizatiort,85(10),812-819.
Seligman, B,, & Liu, X. (2006). Economic assussment ofinterven-
tionsfor reduciirg posipartum hemorrhclge in tteveloping
countries, Bethesda, MD: Abt Associates.
Shiffinan, J, (2007). Generating political priori"r for maternal
mortality reduction in S developing countries. American
Journal ofPublic Health, 97(5), 796-803.
Stekelenburg, J., Kyanamina, S., Mukelabai, M,, Wolffers, I,,
& van Roosmalen, J. (200tl). NValting too long: Low use
of maternal health serviccs in Kalabo, Zambia. T}'opical
Medicine and rn ternativnal Health, Y(3), 390-398.
Stephenson, R., Baschieri, A., Clements, S., Hennink, M., &
Madise, N. (2006). Contcxtual inllucnces on the use of
health faci]ities for childbirth in Africa. Pttblic lfeatth
Matters, 96(1), S4-93,
Sutherland, 11, & Bishai, D. M, (2009). Cost-effectiveness
of misoprostol and prenatal iron supplemcntation as
maternal mortali"r interventions in home births in
rural lndia. international Jburnal (tf Gynecolqgy and
Obstetrics, I04(3), 189-193,
Tann, C. J., Kizza, M., Morison, L,, Mabex D., Muwanga, M.,
Grosskunh, II., & Elliott, A. M. (2007). Use of antenatal
services and dc]ivery care in Entebbc, Uganda: A commu-
nity based survey BMC Pragnancy and Childbirth, Z 23,
Thind, A., Mohani, A., Banerjee, K, Hagigi, E (2008). Where
to deliver? Analysis ofchoice ofdelivery location from a
national survey in India, BMC Pttbtic Heatth, 8, 29,
Tolentinc], K,, & FriecLnian, J. F. (2007), An update on anemia
in]essdevelopedcountries,AmericanJburnal(if11'opicat
Medicine and llygiene, 77(1), 44-51.
Venture Strategies Innovations. (2010). Global misoprostol reg-
istration by indication. Retrieved from http://backyard.
venturestrategies.org/get-file.phpl&cor=file&db=-bixbyr
treesHircij3-li9gx8&id=k〉roh30-thOls&table=treesr ita2cqrxrqls-files
walveka- V, & Virkud, A, (2006). Familial consequences. In C.
B-L〉・nch, L, G. Keith, A, B. Lalonde, & M. Karoshi (Eds.), Pk)srpartumhemorrhagu:Acomprehensivegttidetoevalu-
ation, manc{gemen4 attd surgical iittervention. Kirkma-
hec Dumfries, United Kingdom: Sapiens Pub]ishing,
Woelk,G.Daniels,K.,Cliff)J.,Lewin,S,,Seyene,E,i:ernandes,
B., . . . Lundborg, C, S. (2009). [I}:anslating rcsearch into
pc}licy: Lessons Iearned from eclampsia treatment and
malaria control in three southern.African countries.
Health Research Poticy and bystetns, Z 31.
Mlorld Health Organization, (2005), VVbrld health report
2005: Making every mother atid child coiint. Geneva,
Switzerland: Author.
;・forld Health Organization. (2007a). iUfaternal rnortality in
2005: Estimates devetoped by WflO, UNICEE UN-M,
and the VVbrld Bank. Geneva, Switzerland: Author,
INbrld Health Organization. (2007b), WHO recomrnendations
for the prevention of posrpartum hemorrhage, Geneva,
Switzerland: Author.
Wbrld}-IealthOrganization,DepartmentofReproductiveHealth
and Research, (2004). imkingpregnancy scijlir: The criticat
role of the skilled birth attendant fa joint statement by
WHO, IC]M and FIGQ). Geneva, Switzerrand; Author.
World Health Organization, Department of Reproducttye
Health and Research. (2008). Pmportion of births
attendedbyaskilledhealthworker:2008i{pdates.Gencva,
Sivitzerland: Author.
World Health Organization, Department of Reproductiyc
Health and Research. (2010). Ciariji,ing WIIO position
on misoprostol use in the community to redttce maternal
death. Gefieva, Switzerland: Author.
Wbrld Health Organization, United Nations Population Fund,
United Nations Children's I;und, Averting Maternal
Death and Disability. (2009). tL(onitoring etnergen[y
obstetric care: A handbook. Geneva, Switzcrland: Wl)rld
Health Organization,
Yanagisawa, S., Oum, S,, & "lakai, S. (2006), Determinants
ofskiIIed birth attendance in rural Cambedia. 1}'opical
Nledicine and international Health, 1l(2). 238-251,
Acknoivledgments. Support for this project was provided
by PA't'H through a grant from the Bill and Melinda Ga(es
Foundation [grant number 51592], The views expressed by
the authors do not necessarily reflect the views of RATH or
the foundation.
Correspondence regarding this article should be directed to
Sydncy A. Spangle4 PhD, CNM, Johng Hopkins School ef
Pub]ic Health, 1SOO K Street NVNe Suite 800, Washington, DC
20006.E-mail:[email protected]
Sydiiey A. Spangla; PhD, CNM, Johns Hopkns School efPublic
Heatth, NVlashington, DC
AIissa Koski, Ml'H, Johns Hopkins School ofPublic Health.
Deborah Armbruster, CNM, MPH, Pi¥rH Maternal and
Child Health and Nutrition.
Cynthia Stanton, PhD, MPH, Johns Hopkins School of
Pub]ic Health.
,,. ua{-ti-wttt

Struggling to Get Into the Pool Room
Discourse Analysis of Labor Ward Mi
Experiences of Water Birth
i
? A Critical
dwives'
Kim Russell
RESEARCH AIM: 'rhe aim oi' this article is to share the (indings from an ongoing action research
stud}, aimed at identifying inequalities in the availability of water birth on one hospital labor ward,
Efforts to encoL"'age labor ward midwives to take actio] and infiuence the delivery of normal birth care
in the maternity concerned are addressed in the larger study.
METHODS: Unit midwives who regularly werked on Iabor wards werc invited to tal〈c part in focusgroups and face-to-face interviews over an 8-month period. Critical discourse anal}rsis "'as used to
idcntify actual niidwifery practices, the social ordering of the water birLh discourse, obstacles to water
birth, dominant group intercsts, and solutions to the identified obstaclcs (Fairclough, 2001).
RESUI:I]S: The author conducted a total of tivc unstructured interviews (35-60 rninutes) with ]abor
ward matrons, a consultant midwife, labor ward managcr and clinical practice facilitator, and three
focus groups (40-60 minutes; 1 i midwives) with clinical midwives. Institutional pracLices focused on
the dc[ivery of standardized midwifery care for low-risk women and, therefore, did not promote or
encourage water birth practicc. The small number of requests and the low water birth rate were used
as evidence by soJne midwives that childbearing women no longer wanted this t)rpe of care. The key
obstacles to water birth in th{s setting werc coordinators' priorities, m{dwives' negatiye attitudes,high
wor]doads, and ]ad〈 of institutional support for this type of care.
CONCLUSIONS: 1:indings stiggest that hospital water birth practice is dependent not only on the
availability of equipment and midwifery knowledge, but also on the philosophy ef care adopted by
the organization (Stark & rvlillcr, 2009), Interycntions to improve the practice and availability of water
birth are more ]ikely to succccd if supportcd by midwifery managers, championed by coordinators, and
led by labor ward practitioners.
INTRODUCTION
'
Labor ward culture "is built on a contradiction.
[t allows individuals, in isolation, to practice
midwifery skills of care and support but can-
not acknowledge the empowering potential of
those skills for midwives" and mothers, Thus,
the voice of midwifery is muted, and midwives
"experience a professional state of leamed help-
lessness and guilt" (Kirkham, 1999, p. 738).
+"-t-/ ch..tf-".
i. dS・'"xl"T
el-h/puta-t
This statement captures some of the key political issuc
surrounding thc delivery of midwifery care in th
United Kingdom todav It implies that tnidwives' know]
edge and skiIIs are undervalued within UK midwifer
services (Downe, 2005). Use of the terms "muted" ani
"hclplessness" portray midwives as an oppressed groul
Stapleton, Kirkham, and Thomas (2002) and Kirkhan
(1999) argue that some midwives are in the unenviabl
posiLion of trying to work from a woman-centerei
perspective and empower women from a disempow
ered position. They describe a National Health Servic
tNTERAM"OAtALJOURNAL OF CHILD81RTH Vbtume 1, tssue 1, 2011@ 2011 Springer Pubtishing Company, LLC www,springerpub.comDOI:10.IB91f2156-52B7.1.1.52
.. -- /

Struggling to Get into the Pool Room? A Critical D[scourse Anaiysis of Labor N,Vard Midwives' Experien[es of VVater Blrth Russetl 53
'
(NHS) punctuated by "service" and "sacrificc" in which
midwives are denied the rights and choices they are
expected to offer to women in their care. It appears that
the NHS midwife has becorne the [`pi.agy in the middle";
caught bctween maternity policies, employers, col-
leagues, and women's diverse needs (Murphy-I.awless,
1998; O'Connell & Downe, 2009), Research has shown
that midwifery care can support the develDpment of
therapeutic and meaningfu1 relationsbips (Mander,
2001; Siddiqui, 1999), reduce the need for pharma-
cological analgesia (Eberhard, Stein, & Geissbuelheg
2005; Law & Lamb, 1999), improve vaginal birth rates
(McCourt, Page, Hewisen, & VaiL 1998; Rooks, 1997),
and decrease the length of labor and need for medical
intervention (Hodnett et aL, 2002), However, the rise
in the medica]ization of childbirth and the impact of
technology on hospital midwives' role has led many to
challenge the netion efmidwives as autonomous prac-
titioners of normal birth (Green, 2005; Hollins Martin,
& Bull, 2008; O'Connell & Downe, 2009), Normalbirth is defined as "birth without induction, without
the use of instruments, not caesarean scction, and
without gcneral, spinal, or cpidural anesthcsia before
or during delivery" (Maternity Care Working Group,
2007, p, 1). However, the boundaries between normal
and abnormal birth have become blurred, resulting in
obstetricians and midwives caring for high- and low-
risk women (ArneM 1982; Witz, 1992), and birth being
redefined as potentially pathological (Oakle〉r, 1984),In recent decades, normal birth rates in the United
Kingdom have fa11en from 60% in 1990 to 48% in 2006
(BirthChoiceUK, 2009),
The aim of this article is to share the fi ndings from
an ongoing action research study to the provision and
availability ofwater birth on ene UK laber ward. Effbrts
to encourage labor ward midwives to take action and
influence thc delivery ofnormal birth care arc addressed
in the Iargcr study
of' the Marxist phjlosopher Felix Weil (Brown & Jones,
2001). The main aim of the school was to stimulate the
development of radical dernocracies aimed at address-
ing social inequa!ity (Cohen, Manion, & rvlorrison, 2000;
Reason & Bradburx 2006), Habermas (1976) developed
the term critical theory to describe a secial philosophy;
which seeks to operate at a theorctical and practical level
(Crotty; 1998).
The rescarch inquiry fbcused on a group of dini-
cal midwives, midwifery coordinators, and managers
working in a UK hospital. 1'hc chosen unit had 3,600
births a year and was situated within a busy district gen-
cra! hospital in central England. All clinlcal midwives
rotated every 6 months betsveen the labor, postnataL
an(l antenatal wards, For this reason, all unit midwives
were invited to take part in the study (118 midwives).
METHODS
Clinical midwives were invited to take part in focus
groups, whereas labor ward coordinators (expcrienced
inidwives who were in charge of the day-to-day run-
ning of the ward area) and mangers (usually nonclinical
midwives who were responsible for monitoring and
implementing unit policies) were invited to take part
in face-to-facc intcrviews. These methods were chosen
because they support reflection and social interaction
within groups (Cohen et al., 2000), Senior midwives
and clinical midwives were interviewed separatety to
allow individuals to express opinions within a safe envi-
ronment (Krueger, 2000). Intervicws and focus groups
were conducted in a private room away from thc clini-
cal area, at the end or beginning of the working day An
interview and focus group gutde (discussion topics and
prompts for the interviewer) was used (Kruegcr, 2000)
to maintain focus and elicit participants' everyday expe-
riences of water birth practice.
L
METHODOLOGY ETHICAL CONSIDERATIONS
Action research has become a popular method for intro-
ducing change in health care practice (Hart & Bond,
1995; Hope, 1998) but has been criticized for failing
to recognize inequalities, which constrain individual
agency (Badgeg 2000; Williamson & Prosser, 2002). For
these reasons, critical theory was chosen to underpin the
research methodology: Critical theory is synonymous
with the Frankfurt School, which began in 1924 as the
German Institute forSocial Research under the direction
Bartunek and I.ouis (1996) rccomrnend that action
researchersidentifyhowpreexistingrelationshipsorinter-
ests may affect the research process (Herr & Anderson,
2005), I have been a midivifery lecturer at the local uni-
versity since thc year 2000. AJthough I was known to the
inidwives in the unit, I had not worked closely with them
as an educator or midwife becauseI was alink tutor fbr
community midwifer}r tearns. 'Ib ensure that midivives
participation was completely voluntarM I posted and

54 Struggling to Get lnto the Poo[ RoomlA Critica[ Discourse Ana[ysis of 1.nbor Ward Midwives' ExT)c-wiences of Water Birth Russell
e-mailed invitation letters along with a participants"
information sheet, consent form, reply slip, and a stamped
addressed cnvelope to all unit midwives. written consent
was sought individualy prior to interviews/focus groups,
and participants were informed that they could withdraw
this consent at any time, Anonymity was insured by
removing any identifying characteristics during tran-
scription and by storing all ofthe data on a secured, pass-
word-protected computer, Ethical approval was granted
by the rcgional NHS Ethics Committee and the Hospital
Tlrusts' Rcscarch and Development Unlt prior to com-
mencemcnt of the studv Following the interviews and
focus groups, transcripts were sent to thc participants for
validation and comment.
over an 8-month period. Despite sending individua
letters and e-mails to all midwives concerned and adver-
tising the study via unit meetings and posters, only e
small number of participants volunteered to take part
This may have been caused by the lack of intcrest in thc
research topic or difficulties accessing the fbcus groupE
during work time. However, the quality ef the data gen-
erated during the focus groups and intervicws meani
that data saturation was achieved,
ACTUAL TYPES OF MIDWIFERY PRACTICE
Medical intervention and high-risk care took priorit〉r ortheday-to-dayrunningofthelaborward,Thismeantthal
the care ofwomen in normal labor was marginalized.
DATA ANALYSIS
Critical discourse analysis (CDA) differs from other types
ofdiscoursc analysis in that it is concerned with the iden-
tification ofdiscursive practices and ideological assump-
tions hidden in written or spoken specch (Fairclough,
1989). It is important to note that in CDA, the term
discourse is used to describe the language and actions
(practicc) ofa particular social greup (Fairclough, 1989).
Data analysis oftext takes placc in two separate stages:
. Structural analysis aims to specify the social struc-
turing or order ofa particular group through the
identification ofcommon sense assumptions about
everyday activities,
. Interactionai analysis allews for a social analysis
of interaction by focusing on the identification
of cultural norms, values, and social identities
(Fairclough, 2001).
SeniorMidwde: Ybu have four inductions of labor
every day ...you have three rooms occupied purely
with inductions, high-risk women normally , . . So
you've got a heck ofa lot before you even begin airy
Iow risk . , . you have left-over inductions from the
night before who'll be on syntocinon and haye an
epidural-they need one-to-one care without a doubt
. . . so your al)thty to give care to women coming in
spontaneously is already set . . . {:Iitterview)
High workloads made it dicacult for practitieners
to provide one-to-one care for women in ]abor and
offer alternatives to standardizecl midwifery care. I'Nlatei
birth was viewed as more labor intensiye and, therefore,
more likely to intcrfere with the smooth running ofthe
labor ward.
'I'hese stages of analysis lead to actual practices,
the social Drdcring of the discourse, and obstacles to
differcnt types ofpractice being identified. The analyst
is then asked to critically reflect on these preliminary
findings in relation to dominant group interests and to
find ways past the obstacles (Fairclough. 2001).
RESUUS
The author conducted a total of five unstructured
interviews (35-60 rninutes) with labor ward matrons,
a consultant midwife, labor ward manager and clinical
practice facilitato4 together with three focus groups
(40-60 minutes; 11 midwives) with cLinical midwives
Midwijle 3; I think when you've got somebody in the
pool, you've got the luxury ofstaying in the room
with them, which you wouldn't necessarily . . , you
kno}" if they're on the monitor, you have to stay in
the room , . . if they weren]t in the pool, you'd be
doing other things as well, but generallM when you've
got somebody in the pool, you stay in ther[el,
intervievver: Is that a problem?
Midwijle 3: Staying in there? No, It's not a problem
for the midwife, but it might be for the ward.
(Focus Group)
Labor ward coordinators played a central rolc in
controlling midwifery-lcd care. All participants described
L

Struggling to Get lnto the Pool ]〈oomlA Critica] Discourse Analysis of r.abor Ward Midwives' Experiences of Water Birth Russetl 55
'
how some coordinators would "block" the use of the
pool room by saying r'no" to requests from midivives and
women, putting high-rjsk women in the pool room and,
in one extreme case, writing a `Cbogus name" on the labor
progressboard.
, Midwijle 4: The one thing that used to be very
frustrating was, because of thc situation of the pool
room, if you run out of side rooms, they would use
, the pool room as the ncxt one for an induction of
l. Iabororsomebodycomingin,APH,PPH.
interviewer: So that would block the room?
' Miclintijle 4: Yes, and that was Lised on the premise
that, well, it's nearest t]]e desk if we'rc needed, so
that used to be very, vcry, very frustrating, and then
somebody would be in the room, so if somebody had
wanted to use it, that was taken away from them , . ,
Midwijle 6: There are a few senior midwives on
here that-you know-you say water birth and they
take a deep breath and say, "NoI)'.,.I think they
(women) are often .persuaded for various reasons
l not to use the pool or a bogus person gets written
up on the pool room on the beard so you can't use
the room ,.. (Fbcus group)
time consuming than other types of practice, A rnajor
concern among participants was how they might manage
obstetric emergencies in waten
Midwijli 1O: Ybu sort of end up 1ike kneeling on the
floor, so you end up having to put a pdiow down
because your knees hurt and your sort of reaching
over-you ktiow-you've got to try and listen in to
auscultate with a water-proof sonic aid. Ies ab a little
bit awkward; you end up geuing wet ...because your
arms are in the water and you get redly wet, So, that
might put midwivcs off actually
Midwijb 8: And if thefve got a bad back-it's
that leaning over into the pool on this unit ...
(Fbcusgroup)
SeniorMidivijle: I have worked ivith pools that have
been much, much better for the woman, and much
better fbr us to use than this one.,,if there ls aprob-
Iem, 1 thiiik it would be hard to attend to an emer-
gency in the pool ...it can be very traumatic for the
woman nnd for the midwives who have been looking
after her; so, you knowl I'PH' s [postpartum hemor-
rhagcs], collapses, I've seen stillbirths, I've seen al of ,
the sorts of horrcndous things in the water: (1}tterview)
Staying in the pool room with Iaboring women
for long periods was vicwed as `Cselfisrr' by some hos-
pital midwives. Others felt that being able to stay with
laboring women for long periods was a "luxury" rather
than the norm,
Midivijle J: [rb bc fair, it is doNvn to who the midwife
is, because one of the reasons why some of them
clearl}t do not 1ike watcr births is because you have to
listen in regular1}r and you have to be in the room . . ,
which is fine, I have no quaims about it, but some
l. midwives lilce to stay in their room all night, abso-
lutely fine, but that doesn't help management of the
ward-kay? Aiid then you get the other midwife
who is quite happy to sit on desk and pop in and do
their little bit when it's necessarB se they're the ones
who don't like watcr births . . . (R)cus Group)
Participants felt that most labor ward midwives
lackedthenecessaryskjllstDt'acilitatewaterbirthbecause
of limited opportunities to witness or learn about this
type of practice, This may explain why many midwives
feltthatcaringforwomeninwaterwasdifficultandmore
THE ORDER OF THE WMER BI RTH DISCOURSE
Tb identit'y how hospital midwifery care was organized
and prioritized within the maternity unit, data analysis
fbcusedontheidentificationoftherules,whichgoverned
midwifery practice, social interactions, and midwives
social identities.
THE nRULES" OF HOSPITAL MIDWIFERY CARE
Data analysis led to the identification of socially con-
structcd "rules;' which governed the types of hospital
midwifery practicc. The "labor ward rules" not only
restrictedmidwives'waterbirthpractice,butalsoencour-
aged them to offer standardized care (see fable 1).
Sociat lnteractions
Interactions With iVbmen During Childbirth
In general, clinical midwives did not discuss the use of
water as one of the birth options and, 〉ret, believed thatall women had the right to make choices about the care
'
- . tt ,intp'./-/.,.H・ "''
tt.
''t't/"'11'
!"i}'t'/''/'

'
56 Struggling to Get [nte the Poel Room? A CriLical DisceurseAnalvsis of Labor Ward Midwives' Expcricnces of Water Birth Russetl
TABLE 1 Rules ofHospital NVater Birth Care
Must care for more than one Iabori ng woman at a time and
be active[y engaged in care.
Coordinators can overru]e requests (from women and '
midwives) to use the birthing pools.
Must put roam working and the needs of most women ffrst,
Cannot [eave laboring women a]one in a bi rthing pool, but
can [eave women receiving otheF types of care unattended,
Are allowed to "opt out" of water birth provision, but must
be ski"ed in aH other aspects of standard care.
Must be able to care for high- and [ow-risk women.
they received, 1'he small number of requests and the
low water-birth rate were used as evidence by some
midwives that childbearing womcn no longer wanted
this typc ofcare. Therefbre, women who requested water
birth wcrc more likely to be supported in their choice
than thosc who did not request this type of care.
Midwijb 1; It's likealot of things,Ithink, it (water
birth) goes in phases ,,,
Midivijii 3: You don't get many people asking for
them, I den't think . . . It (ssTater birth) only happens
if the micLwife suggests it . . . or they've had a previous'
waterbirt]i.
(iabor ward) is sometimes really busy and there's I
[a] lot of people expected to come in-quitc oftcn ,
they (coordinator) saF "No, no:' (1iocus Group)
Midwijle 2: But it's not always the staff that, the
quantity of staff; either is it, it's sometimes the staff
in charge that can, not saying you can't do it even if
you want to ,.,
Mid}i,ife 3: They (coordinator) can swing it, can't
they...
Midwijb 2: Yes, because yeu get the vibes, don't
you? And you know thc person probably woutdn't
be keen. (Fbcus Group)
Midwives'Socialldetitity
Social identities are comprised of selfvalue and trust
in one's own abilities and l〈nowledge at a personal andgroup (institutional) level (}-Iollins Martin & BuL], 2005,
2006). The characteristics associated with hospital mid-
wives' social identity are summarized as follows:
A busy, hard-working individual who runs from room
to room, actively involved in the doing, and com-
pleting tasks,
/
1
-
Midwijb l; Ybs. NOt many people come in and say; "Is
the pool free?" 1ike they used to ..,in the past they used
to ring up and saB "I"m coming in, is the pool free?" I
donit think they do that anymore , . . it's not the same,
Midwijle 4: But then it's a difft:rent gencration, per-
, haps, coming through now, (Fbcus Groirp)
Clinical Midwives Irtteractions Witli
CoordinatorsLManagers
Most of thc particip ants agreed that thc coordinators were
responsible for managing the workload. It was generally
accepted that the coordtnators had the authority to over-
ride midwives' and women's requesLs for water bitth if the
unit was busy. Midwives didn't challenge these decisions,
even ifthey didn't agree with the coordinaton because of
concerns about making their jobs more stressfu1.
Midwifb 4: If you've gotsomebody that wants to
go in the pool, sometimes you might get a little bit
of negative input from the G grade (coordinator)
because they aren't thaFyou knuw keenHlelivery
Mithvijle 1: Because if you're in a unit that has a lot
ofaugmentation and things, and a busy unit, that
〉,ou're hands on the majority of the time, to actuallysit there with your hands behind your back . . . it]s
a different situation, isn't it? A lot of the rnidwives
do, sort og think of themselves as obstetric nurscs,
rather than midwives. (liocus GrouR)
SeniorMldvvijle: But we just haven't got the time to
offer water birth to everyone-I mean, they're run-
ningaround Iike hcadlcss chickens half the timc ...
antervieioj
A team player who is loyal to the tearn leader (coordinator)
and the needs of thc institution,
'
Midii,ijb Z If the ward's busy3 they know that
if that midwife goes in that room, (pool room)
they've lost her ,.. She doesn't come out again, so
that;s taken a member of staff away, whereas if we've
got somebody on a bed with an epidural and a CTG
(fetal monitor), you can come out occasionally and
admit somebody clse. (Fbc"s Grotrp)
1・
i
1
/
'
lt
l
1
1l
'
111,

StruggLing to Get lnto lhe PooL Room? A Critlca[ Discou[seAnaLysis of Labor Ward Midwives' Experienccs of Water Bi[th Russelt 57
11
:
it
'
1
:
/
'
, Midii,ij2i3: I thidik, when I was a student, Ijust
thought about rne and the woman; now, as a quali-
fiecl midsvife, I thinlc about my colleagues, and I
think about the safety ofother woinen on the unit,
so if there are ... if therc's only onc midwife fo[
three women, I wM spread n",self between the tlrree
women and try and keep everyone on the unit safe
that was and support my colleagucs. (}loctds Grotrp)
A caring person who wants to do the best for women in her
carc, and who believed in normal childbirth and choicc.
Midwijle IO: 1t's always qLiite disappointing for me,
because a lot of the time, when womcn ask to use the
pool, I hexTe to say"no;' ancL I think that's such a shame.
Therc's so much pressure oTi resources, and there'1l be
somebody in the room who isn't in the pool, perhaps,
Midwijb 11; Wlien I worked in DAU (Da)rAsscss-
ment Unit) 6 wccks ago, J had a lady come in, and she
said, `"I'cl lilce to have a water birth, how do I book it:t"
And [ said, "I'm terribly sorryl you can't book a water
birth, its pot-luck"...I felt awfu1 ... (R)cus Grot{tij
1[leam working was central to midwivcs' social
identitF because working as a unit was viewed as a more
productive way of getting through the work and caring
fortheneedsofmostlaboringwomen.Wordslike"busF""hardworking;' and "running" were found frequently in
the data. This suggests that hospital midwivcs' social
identities were consistent with task-orientated carc,
rather than women-centered midwifery practice.
OBSTACLES TO HOSPIIIAL WMER BIRTH
Obstacles to the proviston and availability of water
birth on the unit were identified from the network of
practices evident in the transcribed texts, The obstacles
to water birth practice were arrangcd at organizational.
individual, and consumer level to highlight the hierar-
chical nature of the barriers to this type ofpractice and
to assist in the identification ofsolutions (see Table 2).
DISCUSSION
The labor ward discourse portrayed the provision of
water birth as an alternative to mainstream rnidwifery
TABLE2 SummaryoftheObstaclestoHospital Wltter Birth Practice
ORGANIZATtONALLEVEL
Midwives' negative attitudes to wate[ birth
Fda rs around coping with emergencies in the pool
Water birth not offered as a choice!]a[k of awareness
Cannotofferone-on-onecare Lack of ski]Is and experience of water birth
/1.. ...lt.. .././ltt. . ...lt. . ... t/.//. . . .t.t. INDIVIDUAL LEVEL
Lad〈 of encouragementand support from the coordinators Unavailabi[ity of the pool room
No incentive to offer yL,ater birth as a rea] choice to women
Water birth "has gone out of fashion"-women no longer
wantthistypeofcare
f '':"' ''・ll-,・ ...1//. . ...,. 1 CONSUMER LEVEL
Women do not ask foi a water birth
Women do not want wa ter birth
practice, Participants believed in principle that the
midwives' role was concerned with promoting normal
birth and s"pporting women's birth choices, but in
reality, midwives' everyday practice focused en `C getting
through the work" as efficiently as possible (}Iunt
& Symonds, 1995). Consequentl" hospital midwives'
social identities were consistent with task-orientated
practitioners rather than autonomous midwifery prac-
tice. Fear ofwhat might go wreng when wornen labored
or gave birth in water was cornmon among participants,
They were particularly anxious about being unab]e to
help women out of the birthing pool if she collapsed
or ifa fetus is compromised. AII of which led to a
belief that wornen who used the birthing pool cou!d
not be left unattended. Irrational beliefs ernanate from
practitioners' previous experienccs of labor and birth
(Grcipp, 1992). Stark and Miller (2009) found that
practitioners who had Iimited experience of water
birth practicc were more likely to create belief systems
around the dangers of water birth. CIuett, Nikodem,
rvlcCandlish, and Burns (2009) also found institutional
settings prevented access to water on safety grounds
despite conclusive evidence to the contrary being
available, Recognizable belief systems place limits on
people's ideas and behaviors because they help define
what is right and what is wrong, what is normal and
what is not (deviant); and, by doing so, make alternative
opinions or actions to those previously defi ned absurd
(Foucault, 1977). For example, it was acceptable to ofR)r
an "ad hoc" water birth service, but epidurals had to be
available 24 hours a day
i'
hr}fufo.・
/
t
58 Struggling to Get tnto tho Pool Room? A Critical Discourse Analysis of Labor WHrd Midwives' Experiences of Water Birth Russell
The social ordering of hospital midwifery prac-
tice meant that water births were not promoted or
encouraged as a part of everyday midwife-led care,
This led to the acccpted midwifery view that water
births are an unpopLilar, unnecessary; difficult, time-
consuming, and potentially dangerous type of care,
Midwives' everyday practices were dominated by the
needs ofhigh-rislc care, and, therefore, a medical view
of birth was accepted as ccntral to hospital midwives'
role (Davis-Floyd, 1992). Most midwives were unfa-
miliar with the sl〈ills of "watching and waiting" tofacilitate physiological birth, leading some practitio-
ners to be fearfut ofundertaking Water births. Hospital
midwifery carc scrvcd the interests of the status quo
where selflprescrvation, collective decision making,
the promotlon of bed birth, pharmacological analge-
sia, and anesthesia were considered part of normal
midwifery practice, Midwives' sphere of autonomous
practice was dependent on the amount ofpower given
by the coordinators and the degree to which individu-
als fbllowed the labor ward rules,
The coordinators were viewed as authority figures,
responsible for controlling the day-to-day running of
labor ward and thc allocation of work, Green (2005)
found that coordinators ensured adherence to expected
norms, such as tbur hourly vaginal examinations, by
seeking out and challcnging midwives who didn't con-
form to expected mcdical protocols, Midwives accepted
that coordinators could prevent them using the birthing
pooL Acceptance of this Lype of behavior legitimizes
the actions ofauthority figures (Miligram, 1974), giving
them a mandate to control the actions of the less pow-
erful (Fairclough, I989). This fbrm of power is known
as hagemony (Gramsci, 1971). Hegemony is a form of
power, which opcrates through acceptance b〉r a socialgroup of a particular ideology. This type ofpower also
includesnotionsof"moralandphilosophicalleadershii'
(Bocock, 1986, p, 11), achieved through the manufac-
ture of consent by authority figures (Fairclough, 1989),
The presence of t`powerfu1 situational fbrces" (Hollins
Martin, & Bull, 200S, 2006) cnsures that behaviors,
which adversely affect thc smooth running of the ward,
were controlled (e.g., going against the coordinators'
decision to use the birthing I)ool may lead to confronta-
tion and an incrcasc in workload fbr other members of
the team). Dcviant acts like these introduce uncertainty
to the relationship between the midwife and coordinator
(Hollins Martin, & Bull, 2008), and may leave individu-
als in fear ofsocial exclusion (Kirkham, 1999),
Institutional practices, such as "blocking" the
pool and not promoting water birth with women on
admission, restricted access to the birthing poo]. Red
wood (1999) argues that institutional control of wate
birth is used by authority figures "to allow ft)r th
expression of a measure of unrest without disturbin
the prcsent unequal power relationships." Howeve r, hos
pital midwives valued choice for childbearing wome/
and belicvcd in their role as practitioners of norme
birth. It is also clear that clinical midwiyes and manag
crs recognized that the low rate of water birth on th
unit was a problem and wanted to take steps to improv
currcnt provision. Participants suggested the followin/
ways past the obstacles to water birth practice withi]
the unit:
.
.
.
Organize water birth worksheps for all midwives
with thc aim of improving midwives' knowledge,
skills, ancl confidence.
Appoint a water birth midwife coordinator to
support individual midwives, disseminate good
practice, and raise awareness of the benefits of this
typeofcare.
Improve pregnant women's knowledge of this type ot
care by previding infbrmation (DVD) at booking an`
offering antenatal water birth classes on labor ward.
CONCLUSION
Water birth enhances the physiology of childbirt}
and promotes midwifery practice in normalitM Ye
it is known to be underused in UK hospital-base(
maternity units (Royal College of Obstetricians an(
Gynaecologists [RCOG]IRoyal College of Midwive
[RCMI, 2006). The key obstacles to water birth in thi
settingwerecoordinators' priorities,midwives'ncgativ・
attitudes, high workloads, and lack of institutional sup
port for this type ofcare. This suggests that promotio]
of hospital water birth is dependent not only on avail
ability of equipment and midwifery knowledge, bu
also on thc philosophy of care adopted by the organi
zation (Stark & MilleB 2009). Cluett, Pickering, Getlic
and Saunders (2004, p. 6) agree, stating that water birtl
is a C`packagc, which includes not only the actua] watei
but also the environment in which it is offered, and thi
interactions of the women and the caregiver." There
fbre, ways of addressing the obstacles to the practic/
of water birth in the un!t are only likely to succee(
if innovatiDns are supported by midwifery managers
championed by coordinators, and led by labor wart
practttioners.

:
,r
1
r
/
ir
Strugg[ing to Get 1nt{} the Pool Room? A Crltica[ Discourse Analysis of Labor Wu[cJ Midwives' Experiences of Water Birth Russe" 59
REFERENCES
Arne〉; X・V, R, (1982). Power and the prtlfbssion of obstetrics. Chicago, IL: Univcrsity ofChicago Press.
Badger, Tl G. (2000). Action research, change, and methodolog-
ical rigour, Journal ofNursing Management, 8, 201-207,
Bartunek, J. M., & I,ouis, M. R. (1996). Insidenfoutsider team
research. Thousand Oal(s, CA: Sage.
BirthChoiceUK. (2009). Latest maternity statistics for Eng-
land and Scotland. Retrieved Junc 9, 2010, from http://
wwwLbirthchoiceuk.comfBirthChoiceUKFrame.htm?
http:/lwww.birthchoiceuk.com/NewLhtm
Bocock, R. (l986). Hagentony. Chichester, England: EIIis
Horweod.
Brown, 1[:, & Iones, L. (2001). Action research and postmod-
ernism. Congruence and critigue. Buckingham, England;
Philadelphia, I'A: Open University Press.
Cluett, E. R., Nikodem, X4 C., rvlcCandlish, R. E., & Burns,
E. E, (2009), Immersion in water in pregnancy;, Iabour
and birth. Cochrane Database of S}rstematic Reviews,
Issue 2, Art No: CDOOOIII. doi: 10.1002114651858,
CDOOOIII.pub3
Cluett, E, R., Pickering, R. M., Gctlie, K., & Saunders, N, J.
(2004). Randomised controlled trial of labouring in
water compared with standard of augmentation for
management of dystocia in tirst stage of Iaboun British
Medical journat, 328, 314.
Cohen,L,Manion,I...&Morrison,K.(2000).Researchmethodsin
educatioti (5th ed.). Lon(]oti, Englanct: Routledge Falmen
Crotty; M, (1998), lkefoundintion ofsocial rwsearch, Meaning and
perspective in the research process. r.ondon, England: Sage.
Dayis-Flo}rd, R, (1992). Birth as an American rite ofpassage.
BerkeleM CA/ University ofCalifornia Press,
Downe, S, (2005), Rebirthing midwifer〉r, Midwives (RCfVD, 8(8), 346-349.
Eberhard, J., Stein, S., & Gcissbuclhe4 XL (200S), Experiences of
pairi and analgesia with water and land births. journal qf
Itsychosotnatic Obstetries th (lynaecolqg),, 26(2), 127-133,
Fairclough, N. (1989). LangucEge and power. New Ybrk, NY:
Longman.
Fairclough, N. (2001). Thc discourse ef new labour: Inter-
textuality in criticaL discourse analaysis. In M, T:
Wetherall (Ed.), Discourse antilysis: A guidefor analysis
(pp. 229-266). 1.ondon, Englandi Sage.
Foucault, M, (1977). Discipline and punishtnent: Tlhe birth of
theprison. London, England: Allen Lane,
Gramsci, A. (1971). Sele[tionsfrom prison notebooks (Q, Hoare
& G, Nowell-Smith, Tlans,). I.ondon, England: Lawrence
and 1・Vishart.
Green, B. (20e5). Midwives coping methods fbr managing
birth uncertainties. British Jburnal ofMidivijliry, 13(5),
293-298.
Greipp, M, E. (1992). Undermedication fbr pain: An ethical
modcl. Advances in Nursing Science, l5(1), 44-53,
Haberruas, J. (1976), Legitimation crisis. London, England:
Itleincniann.
Hart, E., & Bond, M. (1995). Action research for health and
social care. A guide to practice. Bristol, PA: Open
University Press.
Her4 K., & Anderson, G. L, (2005). Tlie action research dis-
sertation. Thousand Oaks, CA: Sage,
Hodnctt, E. D., I,owe, N. K, Hannah, M. E., Wruan, A. R.,
Stevens, B. Wbstron, J. A., . . . Stremie4 R (2002). Effec-
tiveness of nurses as providers of binh labor support in
North American Hospital: A randomized controlled trial.
Journal oj'American Medical Association, 288, 1373-1381,
Hollins Martin, C]. J., & Bull R (2005), Measuring social influ-
ence ofa senior midwife on decison making in mater-
nity care. Journal of Community and Applied Social
Ps〉tchology, 15, 120-I26.
Hollins rvlartin, C. J., & Bull, R (2006), LVhat features of the
matcrnity unit promote obedient behaviour from mid-
wives. Clinical c}Cbctiveness in Nursitzg; 952, e221-e23I.
Hollins Martin, C. J., & Bull, R (2008). Obedience and confor-
mity in dinical practice. British fournal ofMidwijlery,
88, 504-509.
Hope, K. (1998). Starting out with action research. Ntirse
Researcher, 6(2), I6-26.
Hunt, S., & Symonds, A. (1995), lhe social tneaning qf n!id-
wijlery. Basingstoke, United Kingdom: MacMillan.
Kirkham, M, (1999), '!'he culture ofmidwifery in the National
IIealth Seryice in England, Journal ofAdvanced Nurs-
ing, 30 (3), 732-739.
Krueger, R. (2000), Focus groi{ps: Apracticalguide for qpplied
research (3rd ed.). London, England: Sage.
Law, Y, Y,, & Lamb, I(. Y/ (l999), A randomized controlled trial
comparing midwife-managed care and obstetrician-
managed care for women assessed to be at Iow risk in
the initial intrapartum period, journal ofObstetrics and
Clynecology I{esearch, 25, 107--112.
Mande" R. (200I). Supportive care and midwij2rry. Oxfbrd,
United Kingdom: Blackwell Science,
Maternity Care Working Ciroup. (2007). Making normal birth
a reality Concensusstatementfivm the Maternity Care
VVbrkitzg 1'arty. Retrieved September 9, 2009, from
http:ltwww.appgmaternibtotg,ukfresources.
McCourt, C., Page, L,, Hewison, J., & Xlail, A. (1998), Evalu-
ation of one-to-one midwifery: "lomen's responses to
care, Birth, 2S(2), 73-80.
ts./t..
-
ti:' 't ''
' "lii"

60 Struggling to Get [nto the Pool Room? A Critica] DiscourseAnalysis of Labor W"rd Midwives' Experiences of Water Birth Russelt
Miligram, S, (1974). Obedience to attthority, London, United
Kingdom:IhvistockPublications.
rvlurphy-Lawless, J. (1998). Readi,zg birth and death: A historLy
ofobstetric thinking, Cork, lreland: University Press,
OakleM A. (1984). The captttrechvombr A histor〉, of the tnedi- cal care qfpregnant ;vomen, Oxford, United Kingdom:
Basil Blackwell.
O'ConnelL R., & 1)owne, S. (2009). A metasynthesis of
midwives' expcricnce of hospital practice in publicly
funded scttings: Compliance, resistance, and authentic-
ity: Health, I3(6), 589-609.
Royal College of Obstctricians and Gynaecologists/Royal
College ol'Midwives. (2006). fintnersion in water during
labottr and birth. Joint statement no 1. London, United
Kingdom:Author.
Reason, R, & Bradbur〉r, H. (Eds,). (2006), Handbook ofaction research. I.ondon, England: Sage,
Redwood, R, (1999). Caring control: Methodological issues
in a disco-rse analysis of waterbirth texts. Jburnal of
Advanced rKTursing, 29(4), Y14-921,
Rooks, J. (1997), Midwijiery and childbirth in Atnerica,
Philadelphia, PA: '['emple University Press.
Siddiqui, J, (1999). The therapeutic relationship in midwifer
British Journai ofMid;vijlet:y, 7(2), 111-114.
Stapleton, H., Kirkliam, M., & Thomas, G. (2002), Qualitz・
tive study of evidence based leafiets in maternity [arc
British Medicat Jottrnal, 324(7388), 639.
Stark, rv1. A., &Miller, M, (2009). Barriers to the use ofhydrc
therapy in labon Jottrnal of Obstetric, (lynecolqgic, an
Nbonatat Ntirsing, 38, 667-67S,
Williamson, G. R., & Prosse4 S. (2002). Action researcl'
PoLitics, ethics, and participation. fournal ofAdvaitce/
Nursing, 40(5), 587-593,
Witz, A. (1992). 1'rcVlassions andpatriarcly, London, Unite,
Kingdom: Routledge.
Correspondence rcgarding this article should be directcd t,
Kim Russe]1, MA, BSc(Hons), RM, RGN, Institute of Health E
Society,TheDepartmentofAlliedHealthSciences,Universit
of Worcester, Henwick Grove, IVorcester, LVR2 6AJ, UK.
Kim Russell, MA, BSc(Hons), RM, RGN, senior lecturer
Midwifery & Wornen's Health, Institute ofHealth & Society,
The Dcpartment efAIIied Health Sciences, Universit}r of
Miorccster, UI(.
.

ee
Ii"llll・W
.ss〈
TIf・Il,l・
si/l・[
・X,[:III・,
M-tttttt
ex
i・I・",i,s,;g・i;:iiee.#,E ' if'i`su"1"'
.S/ttsth.
-gettes ,ee
The Necessity and Challenge
Midwifery Science
of International
Raymond G. De V}'ies, Marianne Nieurvenhuijze, Rcijbet van
and the members ofthe Midwijbry Science Workgroup¥
Crimpen,
/
l14
'
l'
/
/
l
What is the best way to provide care during the repro-
ductive process? What have we learncd from centuries
of experiencc and from the application of the tools of
science to thc practice Qf maternity care? Those who
consult the history and science of maternity care wil1
discover that the answers to these straightforward ques-
tions are anything but straightforward. Reading the
history ofmaternity care can be quite cenfusing. There
are histories that celebrate medical progress in reduc-
ing maternal and infant mortality (O'Dowd & Philipp,
2000), and there are histories that describc benighted
doctors unwi]]ing to wash their germ-laden hands
before attending women in birth (Nuland, 2004), There
are historles that document how professional societies
of obstetricians improved care for women (Peel, 1976),
and histories that show how those same societies limited
care to women by oppressing midwives (De Brouwere,
2007). The rcadcr ofthese histories will be awed by the
knowledge and skitl that improved care for women and
babies in distress but baffled by thc many interventions
intended to make birth "easier"-C[ prophylactic forceps;'
"trvilight sleep;' routine use of episiotomy-that were
introduced, widely used, and then discarded when
fbund unsafe and unhelpfu1 (Wertz & Wertz, 1989).
Reading the scientific literature on maternity care is
even more disorienting. Not only will the reader discever
that there are great differences in the way maternity care
is done-in ditft)rent countries and in difl'erent regions of
the same country-but also wM be puzzled by apparent
contradictions in conclusions about the safety and ethcacy
of those practices. Within the past yeaB for example, the
peer-reviewed litcrature has shown that planned home
birth is as safe as planned hospital birth (de Jonge et al.,
" Marlein Ausems, I,uc Bude, Darie Daemers, Marijke Hendrix,
Irene Korstjcns, Evelien van Lirnbeek, Hennie Wljnen, and
Bert Zeegers
20e9; Janssen et al., 2009), and that planned homc birth,
when compared to hospital birth, "is associated with a tri-
pling of the neonatal mortality rate" (Wax et al., 201O).
Of course, experienced readers of history and sci-
encc are aware that variations and contradictions in the
literature are not uncomrnon. Histories vary according to
who is doing the writing: Conquerors and the conquered
tcll very different storics about the same war, In science,
progress is made by thc process of assertion and refttta-
tion: Today's findings are tomorrow's discarded theories.
But there is something peculiar about the science
of birth, Obstetrics is the only discipline in medicine
where something happens by itself and, in most cases,
wtth no intervention, everything ends well. This allows
maternity care to become a canvas onto which mid-
wivcs, obstetricians, gencral practitioners, researchers,
and pregnant women can paint their own versions of
the "best care." Thus, in the United States, one-third of
alt births are done surgically and fewer than 1% of births
happen at home, whereas in thc Netherlands, more than
259'o of women birth their babies at home and 14% of
births are accomplished surgically (Centraal Bureau
voor de Statistiek, 2007; Menacker & Hamilton, 2010).
The late Dutch obstetrician Gerritt-Jan Kloosterman,
reacting to the strong rcsistance to his effbrts to cham-
pion midwifery and home birth, suggested that a science
ofmaternity care may be impossible.
Obstetrics is wider and broader than pure medicine.
It has to do ivith the whole oflife, the way you look at
life, makng objective discussion dicacult. Ybu are almost
unable to split the problem off into pure science; always
your outlook on life is involvcd. (De Viries, 2005, p. I80)
Kloosterman calls attention to the way our cultural
belicfs about birth and thc pcrspective we acquire as
professional caregivers and researchers create a bias that
distorts scientific studies of materni"r care. This fact
rnakes it ver〉r difficult to identify best practices forbirth,
INIEF?NATIOALAL JOURAML OF CHtLDBIR'IH Vbl"me 1, tssue 1, 20VI @ 2011 Springer Publlshing Company, LLC www.springerpub,com DOI:10.1891/2t56-5287.1.1.61
sor" ' "t"'.t
,f. (l 2"gx;,.
Ui -M-t-"
-

i
62 The Necessity and C/hnllenge ef 1nternational Midvvifery Science De 1firies et at.
How should we caregiyers and researchers respond
to the peculiari ty ofbirthcare with its conflicting histories,
contrar〉r findings, and built-in bias? -Ve could give up-itseems an objective science ofmaternity care is impossible,
so why bother? Mle could become partisans-choose a
point of view on what is the best birth and set out to prove
we are right. Or wc could build a new science of maternity
care-midwijiirly science-that capitalizes on the history of
midwifery and thc variations in maternity care to develop
a research agenda that prometes optimal care for women
and babies, care that takes into account their plrysical con-
dition and their culturaL and social situations.
WHY MIDWtFERY SCIENCEI
W}ryisrnidwiferyscicncethebestresponsetothepeculiar
problems that beset rescarch on maternity care practices?
Some researchers will arguc that a better, more expansive
obstetric sciencc should take on this task, The preference
for midwifer〉r over obstetric science lies in the differencebetsveen the tsvo approaches to materni"r care,
Histories of maternLty care-as varied as they
are-teach us two things: (1) Much progress has been
made in responding to thc complications of birth;
arid (2) interventions that alter uncotmplicated birth to
improve the process havc bccn largely unsuccessfu1,
Members of the obstetric specialty-dedicated to find-
ing ways to reduce the morbidity and mortality associ-
atedwithchildbirth-haverightlyfocusedonpathology
Midwifery begins with a fi.)cus on " physiologs" the bio-
logical and s6cial features ofundisturbed and uncompli-
cated reproduction, birth, and postpartum,
The division of labor in materni"r care should
reflect the fact that most births proceed ivithout compli-
cation, The governing science of maternity care should
focus on the factors that promote (and hinder) physiologi-
cal birth and on the early recognition of the indicators of
pathology that require specialist care, These are precisel〉rthe features of midwifery science. The goal of midwifery
science is to discover and develop basic and applied
knowledge about the dynamics of reproduction and child-
birth. Basic research-the creation and testing of tlieories
that promote greater understanding of the pbysiological
reproductive proccss-provides the basis for the develop-
ment of innovations in practicc. Applied research exam-
ines current and innovative practices, allowing quality
improvement and ensuring proper care fbr motheB child,
and fhriiilv Research in midwifery science examines:
. Factors that promete health in the short and Iong term;
. Methods for equipping the transition process to
parenthood;
. The organization of obstetric care; and
. The sociaL production ofboth scientific and Iay
knowlec{ge about maternity care, including aspects
of medicai and popular culture that encourage and
discourage physiological birth.
'1'hose who do midwifery science use theories and
methods developed in various disciplines, including mid-
wifer" public health, obstetrics, gynecolog〉l neonatolog"genetics, embryology anatornF (patho)physiology; medi-
cine, cthics, psychology sexology; sociolog}s information
sciencc, and organizational science.
Noticctwoimportantdiffiorencesbetweenmidwkry
science and obstetric science: (1) Because of its f[)cus on
physiological birth, midsvifery science is concerned with
enriching our understandmg of the process ef pregnancy
and birth experienced by the mcijoritl, ofwomen; and (2) the
interdiscipltnary approach ofmidivifery science extends tts
work beyond the bocly of the birthing woman to the birth-
ing woman herscLfl The interest of midwifery science in the
contexts In which birth occurs leads to an appreciation of
the situated naturc of knowledge about reproduction and
birth. 'lhc cxpectations of clients and their interpretations
of rcality-and noL just the signs measured by the techiiolo-
gies ofmedicine-arc taken seriously in research.
Progrcss in maternity care requires research in both
pathological and physiological birth, but the "first science"
of maternity carc should be midwifery science. Promo-
tion of thc bcst care for al1 must begin with a science that
considers the social and psychological situation of women
and famMes tmd examines how culture and societal struc-
tures infiuencc reproduction, the delivery of care and, Iast
but not least, the production and use of data on maternit〉rcare. ' I'here is an interesting historical irony here. Care at
birth was once the sole domain of midivives, But becausc
of denied access to advances in obstetric science and thc
new tcchnologies ofbimh, midwives concerned themsclves
with physiologicaL birth. Obstetricians gradualy took over
the management of pathological binh, whereas midwives
gained expertise on uncomplicated birth, expertise that
is dcsperately needed to improve care where medical
resources are scarcc, atid to lmit umecessary interventions
where mcdical resources are overused (Betrdn et al., 2007).
WHY INTERNMIONAL?
. The physiological reproductive process;
. Factors-bio]ogical, psychological, and social-that
promote the physiological process;
Our description ofmidwifery science hints at the neces-
sity ofan international midwifery science, Care practices
fbt' birth vary widel〉f around the globe. This fact offers us

The Necessity and Challcnge of [nLernalional Midwifery Science De V7ies et al. 63
1
1
/
1
a laboratory fbr studying the sources and consequences
of diversity in maternity care and provides a unique
position fbr informed critiquc Dfbirthcare. The science
of obstetrics has madc significant progress by studying
and treating the pathologies of birth without regard for
the social and cultural caTitext of the birthing woman.
This strategy has been successfuL in developing therapies
to intervene in problem births, but it does not promote
critical reflection on `Cprogress" in inaternity care (which
often means the extension oftherapies for pathology and
irrvasive preventive survcillance to healthy women).
Midwiferysciencccxplorestheconnectionsbetween
culture, birth practiccs, and oLttcomes of birth, generating
data that can reveal problems with the medical "improve-
mene' ofbinh. An intemationaL focus and respect for var-
ied approaches to attending birth creates opportunities for
maternity caregivers to learnJ}'om each other and to learn
ivith each other, Thjs ensures that mid}vifery research and
its results are accessible to othcrs arid, hence, can be used to
stimulate reflection on rnidwifery models, the organization
ofcare, and the pros and cons ofobstetric intervention,
The international orientation of midwifery science
allows a rich understanding of how physiological birth
is shaped by the many ways societics organize care for
birthing women, Efforts to promote optimal care at birth
must proceed with a clear sense of how organizational
systems and cultural ideas ar¢ implicated in birthcare.For example, the varied divisions ot' Iabor in maternity
care-including differing scopes of caregiver practice and
different ratios of midwives to gynccologists and obste-
tricians-are associated with the kind of care offered to
birthing women, And cultural notions about birth shape
the desires and choices of women in birthcare and the
content and results ofscicntific studies ofbirth (De Vlries,
Kane Lou; & Bogdan-I,ovis, 2008).
A second challengc is the organizational and cul-
tural dominance of obstetric science, Obstetric science
has gained powcr and prestige by virtue of its claim
to objective science and its embrace of technological
solutions to the problems of birth, In modern societies,
the empirical knowledge of rnidwives, often gleaned
from cxperience, is not highly valued. IIb gain respect
in contemporary societp midwifery knowledge must
be validaled by science. Effbrts to create midwifery sci-
ence, coming Iater te the disciplines of medical science,
often seem to be "obstetrics light;' a pale imitation ofthe
hard science of obstetricians, beholden to the quantita-
tive, positivist methods of medicine (Black, 1996). This
makes the reccipt of funding and public respect morc
diMcult.
'L'he incrcasing use of technology in all aspects of
our lives presents a third challenge to midwifery science.
IIlechnology surrounds us and promises to make our
lives easier-we have come to depend on computers, the
Internet `Csmart" phones, and global positioning devices.
The presence and friendliness of these technologies make
it more difficult to convince women, the public, and
fimders of research that less technological approachcs
to birth may bc prcf'crable. Furthermore, public apprc-
ciatlon of tcchnology lcads to public acceptance ofinter-
ventive, instead of watchful, medicine. It is no longer
enough for carcgivers to wait until a symptom emergcs
before rcsponding. In today's world, we expect preemp-
tive intcrvention: We want the problem to be discovered
bojbre it is a problcm. And although this approach to
health care can be harmftil-most recentl$ we learned of
thehealthdangersofearlyscreeningforbreastcancer-it
is the current model of medicine and stands as a chal-
lenge to the more watchfu1 approach of mid"dfery and
midwiferyscience.
/ THE CHALLENGE(S) OF MIDWIFERY SCIENCECONCLUSION
i1
/
'1
There is something seductivc about an obstetric sci-
ence that looks solely on the bodily mechanics of birth.
After all, a human uLerus in Marrakesh is identical to a
human uterus in Manhattan. It is much more compli-
cated to build a sciencc around the recognition that a
uterus is part of a thinking, feeling woman's body that
lives together with others in communities that shape the
experience and mcaning of reproduction and the type
and quality of care during pregnancy and birth. This is
the first among the several challenges of midwifery sci-
ence: Understanding thc man〉r birth practices aroundthe world, situating them in their cultural and orga-
nizational environment, and assessing the quality and
transferabili"r of those practices,
The problcms of maternity care in today's world-too
much unnecessary intervention in birth in many high
resource countries and too little needed intervention
in the countries of the global south-reguire a sci-
ence that does more than study pathology: Midwifery
science with its historical, social, cultural, and clinical
focus ofli]rs a way forward for the improvement of
birthing care for women in all societies. This will neces-
sarily involve morc informed midwifery practices, an
improved divisiDn of labor betsveen those who provide
maternity care (in terms of numbers and responsi-
bilities), and better cooperatien betsveen midwives and
obstetricianfgynccologists.
:
I
t/-t. .t.,,/wh
64 The Necessity and Cha[ienge of lnternational Midwifery Science De Vries et al.
REFERENCES
Betrin,A.R,Merialdi,M.,Laue4J.A.,Bing-Shun,MC,[[homas,J.,
Vah Look, R, & Whgrie4 M. (2007). Rates of caesarean sec-
tion: Analysis of global, regional, and national estimates.
IlaediatricandPerinatallipidemiolqg),,21(2),98-113.
Black, N. (1996). Why we need observational studies to evalu-
ate the effectiveness ofhealth care. British Medical Jbur-
nal, 312, 1215-1218.
Centraal Bureau voor de Statistiek, (2007). De Nlederlandse
samenleving, 2007 [Dutch society], Vborburg, The
Netherlands:Authon
De Brouwere, V (2007). The comparative study of maternal
mortakty over time: The role of the professionalisation of
childbinh.SocialHistot),ofMedicine,20(3),541-562.
de Jonge, A., van der Goes, B. Y:, Ravelli, A. C,, Ame!ink-
Verburg, M. R, Mol, B, W, Nijhuis, J, G., , . . Buitendljk,
S. E. (2009), Perinatal mortality and morbidity in a
nationwide cohort of 5,29,688 low-risk planned home
and hospital births. BJOG: An international journal of
Obstetrics th Clynaecology, 116(9), 1177-1184,
De Vties, R. G. (2005), A pleasing birth: Midwijlery and matett-
nity care in the Netherlands, Philadelphia, PA: Tlemple
UniversityPress.
DeVties,R.KaneLow;L,,&Bogdan-Lovis,E(2008).Choosing
surgical birth: Desire and the nature of bioethical advice.
In H, Lindemann, M. Vbrkerk, & M, Urban Walker (Eds.), Nbturalized bioethias (pp. 42-64), Cambridge,
United Kingdom: Cambridge University Press.
Janssen, R A., Saxell, L., Page, L. A., Klein, M, C., Liston, R. M,
& Lee, S. K, (2009). Outcomes of planned home birth
with registered midwife versus planned hospital birth
with midwife or physician. Canadian Adedical Associa-
tion Jburnal, 181(6-7), 377-383.
Menacken E, & Hamilton, B. E. (2elO). Recent trends in
cesarean delivery in the United States. NCHS Data
Brief (35), 1-8. Washington, DC: Centers for Disease
Control and Prevention (CDC), National Center for
Health Statistics (NCHS),
Nuland, S. B, (2004). Ilhe doctors' plague: Germs, childbed
foven and the strange stor), cij' igndic Semmelweis. New
Ybrk, NYI Norton,
O'Dowd, M, J,, & Philipp, E. E. (2000). 11he histor〉, ofobstetrics
and gynaecology, New Ybrk, NYI Parthenon.
Peel, J. (1976), 11he lives clf the Ilellows qf the Rayal Collqge of
Obstetricians and (lynaecologists:1929-1969. London,
United Kingdom: Heinemann Medical Books.
Wai(, J. R., Lucas, E L, Lamont, M,, Pinette, M, G., Cartin,
A,, & Blackstone, J. (2010). Maternal and newborn
outcomes in planned home birth ys. planned hospital
births: A meta-analysis, American journal of Obstetries
and (lynecology, 203(3), 243.el-e8,
Wertz, R,, & Wertz, D. (1989). lying-In: A history ofchildbirth
in America, New Haven, CT: Yhle University Press.
Correspondence regarding this article should be directed to
Raymond G, De Vicies, University ofMichigan Medical School,
CA 92126. E-mail: [email protected]
Raymond G. De Vlries, Marianne Nieuwenhuijze, and
Rafael van Crimpen, Midwifery Science Wdrkgroup,
Academie Verloskunde Maastricht, the Netherlands.
1
/
AuthorGuidelines
/
The lhternational Jburnal of Childbirth is a quarterlM peer-reviewed publication with a global fbcus on childbearing,
The journal invites the subrnrssion ofrnanuscripts that address research, practice, educatiQn, and theory as well as case
reports, personal narratives, and commentaries on all aspects of childbirth.
1
T"
iT
l
/
The fo11owing presentation style should be observed when submitting manuscripts:
/
. Clinical and Basic Science Research articles should include an Abstract, Introduction, Material and Methods,
Case History (if appltcable), Results, Discussion, Conclusion, and References.
. Review articles should provide a comprchensive synthesis of the availablc information on their chosen topic.
They must include headings and reference citations.
. Case Reports should be brief reviews ef either typical or atypical births and should include an Abstract,
Introduction, Case Report data and findings, Discussien, Conclusion, and References,
. Personal Narratives should first-hand accounts of childbirth experiences. References are not required but may be
included when needed to support data or quotatiens from published sources.
ManuscriptPreparation
The manuscripts should be prepared in accordance with the Publication Manual of the American Psycholqgical
Association, which should be consulted for matter ofstyle and fbrmatting, including text, references, and tables.
Length. Submissions are generally expected to be 15 to 25 pages in length; however, the journal considers manuscripts
that are longer or shorter.
/
Coyer Pagc. A cover page separate from the main manuscript must include the article's title and the names, academic
degrees, mailing addresses, and e-mail addresses of each of the contributing authors,
Abstract. Research articles. review articles, and case report$ should include an abstract of between 125 to 200 words
that concisely states the article's purpose, the stuc})r design, major findings, and rnain conclusion.
'
Summary. When an abstract is not appropriate for the type of article submitted, authors should include a summary of
between 12S to 200 words that provides a synopsis ef the article's thesis and conclusions,
'
Appendices, Instruments or large tables of data may be included as an appendix to the manuscript, The publication
of appendices is at the discretion of the editors.
1Letters to the Editon Letters to the editor should be concise comrnents regarding anicles published in the journal and
may include references, Letters should be under 300 word$. Those accepted fbr publication may be edited or abridged.
r'
Photographs, Drawings, and Graphs. Illustrations should be submitted as individual, high resolutiQn images in jpg,
tiff; or eps graphics Me formats (graphs created in Excel are also acceptablc). Digital images should include the figure
number in the Me name. AdditionallM a copy of each illustration should be embedded at the end of the manuscript
after the reference Iist and tables.
Submission
b Authors should submit manuscripts by e-mail to [email protected],
CopyrightAgreement
The fo11owing dated agreement signed by all authors must accompany each manuscript submitted for publication:
:
The undersigned author(s) transfers all copyright ownership of the arttcle entitled [insert the title of7our article]
to thc Springer Publishing Compan" LLC, in the event that the article is published in the International Journal of
Childbirth, This transfer of copyright includes, but is net limited to, thc worldwide rights to any and all forins of
publication now known or hereafter developed, including all forms of print and electronic media, The undersigned
author(s)warrantsandrepresentsthatthearticleisoriginal,isnotunderconsiderationbyanotherjournal,hasnotbeen
published previously, and contains no matter that is libelous, unIawfu1, or that infringes upon another copyright,
.,taAs4sde・