w10 linac based mutic final - aapm
TRANSCRIPT

ViewRay Experience
Sasa Mutic, Ph.D.Washington University School of
Medicine

“You can observe a lot, just by watching”
-Yogi Berra

Does organ motion matter?A slide often used to illustrate RT capabilities
Does organ motion matter?

Outline of Presentation
• ViewRay System• Commissioning Work• Some Early Cases• Adaptive Radiotherapy Implementation

Learning Objectives
• Describe overall design of the ViewRay System• Describe early clinical observations• Describe work for implementation of ART on the
ViewRay system

ViewRay
• 0.345T MRI• 3 Co-60 heads – (~550 cGy/min @ iso)
• 3 fully divergent MLCs (minimized penumbra)• Large imaging FOV (50 cm) and Tx volume (27cmx27cm)
• Conformal RT and\or IMRT• Integrated planning system
– Monte Carlo dose calculation– Fast optimization and calculation (9 field plan ~ 30 sec)
• Continuous MR Therapy Control

ViewRay
• Routine clinical instrument from the first use• No limitations of any kind• Easily reproducible process
– Can implement at other institutions• Staged in three steps (all with same goals as above)
– MR-IGRT (similar to CBCT-IGRT)– MRTC - MR Treatment Control (a.k.a. MR Gating)– On couch ART (Adaptive Radiation Therapy)
Implementation Strategy

First MR-IGRT TreatmentJanuary 15, 2014

• ViewRay Imaging– Split Supercon 28 cm gap, 0.345 T, 14.7 MHz 50 cm DSV, warm
bore 1.05 m– Split Gradient 28 cm gap, 5 mm former in gap, slew 200
mT/m/ms, 18 mT/m peak, 30 kW heat removal– Isocenter matched to RT Iso (2mm)– Body coil & surface coils -thin uniformly attenuating, electronics
out of the beam
• Washington University Evaluation– FDA testing and acceptance testing (manuscript in preparation)– Clinical comparison of onboard MR and CT (manuscript
submitted)– Requirements from AAPM, ACR, NEMA, & IEC

Imaging System Evaluation
Noelle, C. et. al., manuscript submittedWashington University Study
Clinical study comparing 0.35T MR and CBCT

What else can we see with MR?
Washington University Study
Radiation Damage - Edema

Imaging system evaluationClinical study comparing 0.35T MR and CBCT
Onboard CTOnboard MR

Treatment Planning System Evaluation• Dedicated TPS
– Integrated from prescription though delivery and adaptive therapy (including on couch optimization and planning)
– Supports only Monte Carlo based calculation with and without magnetic field effects
– Beam numbers in increments of 3 (3 heads)– Planning on CT or MR or fusion of both
• Washington University Evaluation– FDA related testing and acceptance testing (manuscript in
preparation) – Clinical plan comparison studies (manuscript in preparation)– AAPM & ACR

Treatment Planning System Evaluation
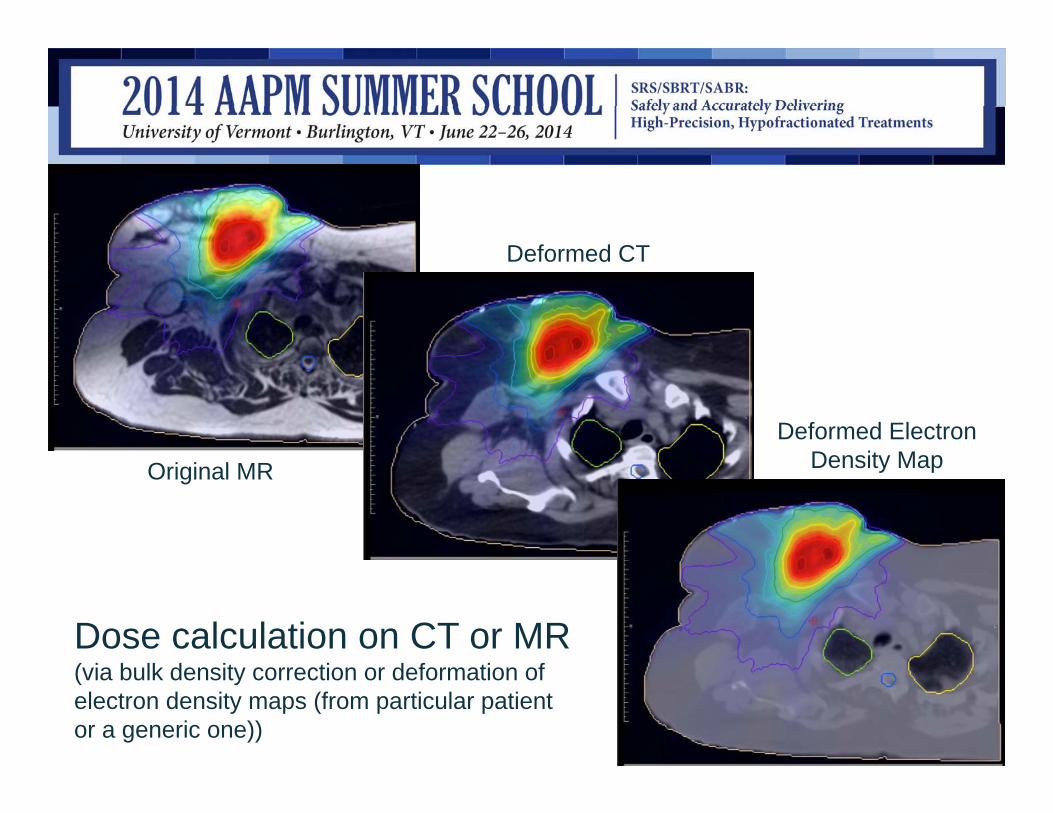
Original MR
Deformed CT
Deformed Electron Density Map
Dose calculation on CT or MR (via bulk density correction or deformation of electron density maps (from particular patient or a generic one))

ViewRay: 60Co IMRT Clinical plan: 18 MV IMRT
SKINRECTUM BLADDER
PTV
ViewRay(solid DVH)
Clinical(dashed DVH)
Treatment Planning System Evaluation

Clinical plan: 3D conformal using non-coplanar 6 MV beams. ViewRay: 60Co coplanar IMRT
PTVR. LUNG
HEART
ViewRay(solid DVH)
Clinical(dashed DVH)
Treatment Planning System Evaluation
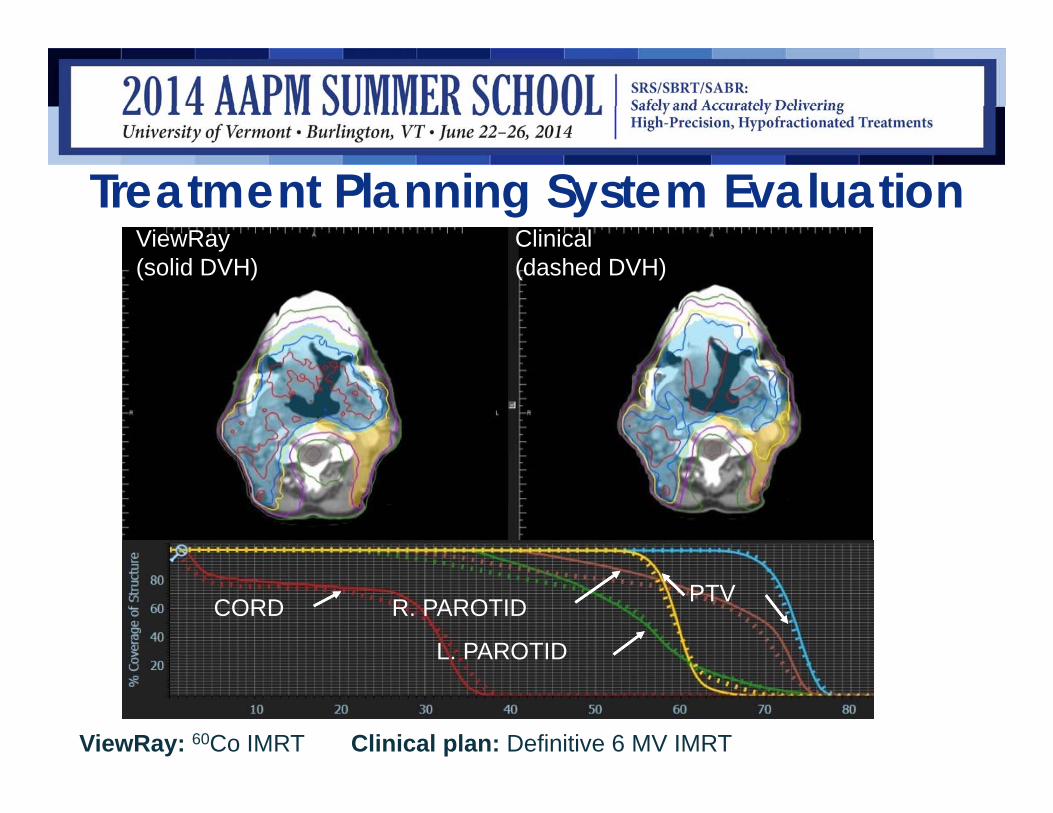
ViewRay: 60Co IMRT Clinical plan: Definitive 6 MV IMRT
ViewRay(solid DVH)
Clinical(dashed DVH)
PTVR. PAROTID
L. PAROTID
CORD
Treatment Planning System Evaluation

Delivery Evaluation
• Conventional:– IGRT machine with three heads and all related geometric and
dosimetric concerns (TG142, TG51, etc.)• Novel:
– On couch dose prediction, re-optimization and calculation– MR Controlled Treatment MRTC (real-time accounting for
target position and shape)– Two headed mode (if there is a problem with one head)
• Phantom and simulated delivery with patient data studies• QA tolls and methods, immobilization, workflow, practicality, etc.
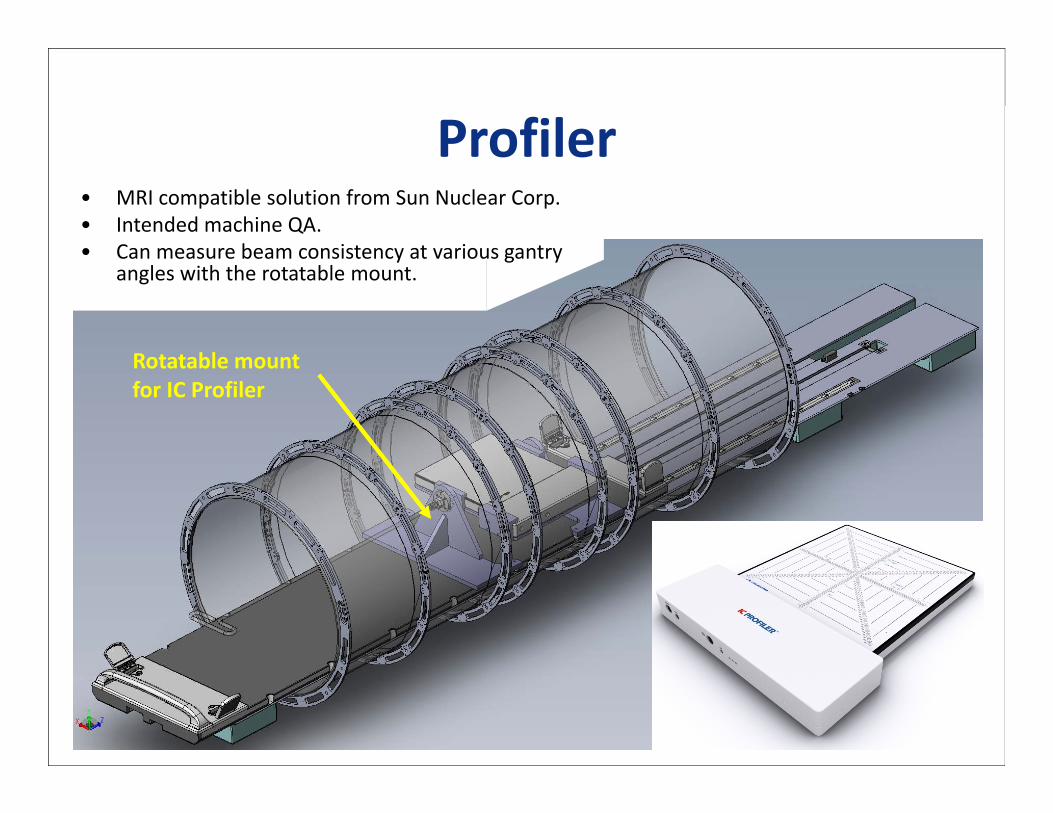
Profiler• MRI compatible solution from Sun Nuclear Corp. • Intended machine QA.• Can measure beam consistency at various gantry
angles with the rotatable mount.
Rotatable mount for IC Profiler


CIRS Gating PhantomIntended for evaluating gating functions; tracking, beam gating, and latency

Torso coilsInserts for ion chambers
Film Chamber
MRI fluid filled
ViewRay QA Phantom

ViewRay QA PhantomMRI and CT Visibility
MRIMRI on CT

ViewRay Plan Adaptation
• ViewRay imaging system is ready to support online (or offline) ART
• Workflow– Image patient ~ 1-2 min– Deformable registration, propagation, contouring ~ 1 - 15 min– Plan generation/optimization ~ 1 min– QC, QA and approval ~ 3 min– Treatment delivery ~ normal
• Enablement of online (on-couch) ART within 15 min

No Margin vs. Margin Plans Standard Auto-contour +
adaptManual contour +
adaptMargin 5-7mm 2mm 0mmBladder V65Gy 36% 25% 12%Rectum V65Gy 16% 9% 6%Rectum V40Gy 36% 29% 24%

Results
Steps No Adaptation (min)
Auto Contouring and plan
adaptation(min)
Real-timeContour editing
and plan adaptation
(min)Imaging 1 1 1Auto-contouring 0 1 1Find Shifts 0.5 0.5 0.5Edit Contour 0 1 15Predict Dose 0 2 2Dose Evaluation 0 2 2Re-optimization 0 1 1Plan Evaluation 0 3 3Total ~2 ~12-15 ~ 25

ViewRay Plan Adaptation• QC and QA tasks*
1. Verification of contour delineations of target and organs-at-risk (OARs)
2. Plan integrity check3. Plan quality check4. Verification of dose calculation
• Normally these tasks would take hours, and measurement based QA cannot be done while patient is on the treatment table.
• Goal is to finish in 3 minutes, requiring QA\QC procedures not based on measurements
*Process-Based Quality Management for Clinical Implementation of Adaptive Radiotherapy, C. Noel, L. Santanam, P.J. Parikh, and S. Mutic, Submitted for publication Med Phys, 2014.

Plan Integrity Check (WIP)• Prescription – Rx, site and laterality• Patient setup and imaging – orientation, couch removal, VR table add-on, image
slice thickness, FOV• Target definition – CTV, PTV margin and expansion• ROI – naming, gaps, laterality, OAR overlapping, completeness, density override,
consistency between Pinnacle and VR• Isocenter and POI• Plan – # of beam, beam angles, # of segments, per segment beam-on time,
segment size, beam-eye view against PTV, total beam-on time• Dose calculation – algorithm selection, parameters, matrix size and resolution,
electron density per structure• Plan optimization – optimization parameters, normalization• Plan quality – planning objective check based on DVH and rules

Additional Fractional Check (WIP)• Purpose is to check the consistency between the re-optimized plan
and the original plan, and between treatment fractions• Consistencies of
– Prescription– Isocenter– Daily imaging parameters– Major beam parameters– Dose– DVH– ROI position and volumes– Plan quality (using planQC tool)

Monte Carlo Independent Dose Calculation for ViewRay (WIP)
Independent Monte Carlo ~ 1 min Clinical Plan

Acknowledgements
• Olga Green, PhD• Rojano Kashani, PhD• Omar Wooten, PhD• Lakshmi Santanam, PhD• Harold Li, PhD• Tianyu Zhao, PhD• Vivian Rodriguez, PhD• Deshan Yang PhD• Kari Tanderup, PhD• Greg Kamal
• Yanle Hu, PhD• James Dempsey, PhD• Iwan Kawrakow, PhD• James Victoria, CMD• Tracy Hand, CMD• Camille Noel, PhD• Parag Parikh, MD• Jeff Olsen, MD• Many others at WashU and
ViewRay

Thank you!

References1. Process-Based Quality Management for Clinical Implementation of
Adaptive Radiotherapy, C. Noel, L. Santanam, P.J. Parikh, and S. Mutic, Submitted for publication, Med Phys, 2014.
2. The ViewRay system: MR guided and controlled radiotherapy, S. Mutic and J.F. Dempsey, Accepted for publication, Seminars in Radiation Oncology, 2014.