wellcome news 71
DESCRIPTION
Wellcome News' tells the stories of the Wellcome Trust's work. This issue features Peter Rothwell, a Trust Senior Investigator working on how aspirin can prevent cancer and stroke, an illustrated guide to aspirin, and the story of scientists working on mitochondrial inherited diseases - and a family whose baby daughter has one. Also inside: the winners of the Wellcome Image Awards, a journey from secondary-school science teacher to Cambridge professor, and the latest Trust funding and research news.TRANSCRIPT

PB | Wellcome NEWS Summer 2012 | 1
Wellcome NEWSIssue 71, summer 2012
TAKING A CLOSER LOOKAnnouncing the winners of the Wellcome Image Awards 2012.
2 | Wellcome NEWS Summer 2012 | 3
Marius Kwint and Richard Wingate
The Mind as Matter
Featuring rare and astonishing images of real brains, including historical artefacts and contemporary photography, Brains follows the long quest to manipulate and decipher this most exceptional of human organs.
Accompanied by illuminating commentary from neuroscientist Richard Wingate and art historian Marius Kwint, Brains is a fascinating exploration of how humans have imagined, interacted and tried to come to terms with this infi nitely mysterious organ.
160pp | ISBN: 9781781250402
The book ties in with Brains, a recent major exhibition at Wellcome Collection in London.
“ A book for anyone with an interest in this mythic organ”
Dr Barry Gibb, author of The Rough Guide to the Brain
Scan the QR code to see more sample pages from the book.

2 | Wellcome NEWS Summer 2012 | 3
In brief
Message from the Director
Funding news
Research news
In depth
How I Got Into… protein research: Prof. Jane Clarke
Best of the blog: Get that grant
The simple truth: Prof. Peter Rothwell
In the hot seat: Dr Mayada Elsabbagh
Out of the shadows: Freeing families from mitochondrial disease
Analysing the Nazi mind: Prof. Daniel Pick investigates
Opinion
Research careers need to be flexible
Appliance of science: Turning heart failure into poetry
Picture features
Close-up: Wellcome Image Awards
Nuts and Bolts: Aspirin
From the Archive: Everard Digby’s De Arte Natandi
4
6
8
10
12
14
23
26
30
13
34
20
24
32
CONTENTS
INSIDE THIS ISSuE
14Stroke prevention in Oxford
Marius Kwint and Richard Wingate
The Mind as Matter
Featuring rare and astonishing images of real brains, including historical artefacts and contemporary photography, Brains follows the long quest to manipulate and decipher this most exceptional of human organs.
Accompanied by illuminating commentary from neuroscientist Richard Wingate and art historian Marius Kwint, Brains is a fascinating exploration of how humans have imagined, interacted and tried to come to terms with this infi nitely mysterious organ.
160pp | ISBN: 9781781250402
The book ties in with Brains, a recent major exhibition at Wellcome Collection in London.
“ A book for anyone with an interest in this mythic organ”
Dr Barry Gibb, author of The Rough Guide to the Brain
Scan the QR code to see more sample pages from the book.
4 | Wellcome NEWS Summer 2012 | 5
Cover: Scanning electron micrograph of caffeine crystals, a Wellcome Image Award winner. For more, see page 20. Annie Cavanagh and David McCarthy
4 | Wellcome NEWS
This document was printed on material made from 25 per cent post-consumerwaste & 25 per cent pre-consumer waste.
50%
MESSAGE fROM ThE DIRECTOR SIR MARK WALPORT
The best way to find something out is to ask a question. That is as true for scientists as for anyone else, and one of the most fundamental skills in science is asking the right question. A good research question defines what new knowledge is being sought, and although research can be deeply complex at the cutting edge of today’s science, there is much to be said for having a simple question at the heart of it.
For Peter Rothwell, Professor of Clinical Neurology at the university of Oxford, the right questions have sometimes seemed almost trivial in their simplicity, but his research has had enormous impact. Important as it certainly is to understand the genetic and molecular basis of stroke, Peter also saw more immediate issues in his clinic that others might not have considered: for example, why were some people who had had a minor stroke missing their follow-up appointments? The answer – that they had suffered major strokes in the meantime (see page 14) – helped to change the way we treat these patients in the NHS.
Stroke still kills more than 50 000 people each year in the uK and leaves thousands more severely disabled. Stroke research has struggled at times to attract the attention and level of funding given to cancer and heart disease, but that has begun to change in recent years. Today, there is a cadre of dedicated scientists – including Peter, now a Wellcome Trust Senior Investigator – studying the epidemiology of stroke, the mechanisms by which it occurs and what we can do to treat people who have strokes or to prevent them having one at all.
This May was the uK’s first Action on Stroke Month. On the Wellcome Trust blog, we published a series of articles, films and infographics looking at all aspects of research into stroke, from statistics and risk factors to treatment and rehabilitation. It shows the breadth of stroke research being supported by the Trust and other funders.
Stroke is a major burden on health services around the world; it is also a rich area for research that will continue to draw on and extend our understanding of the brain, the heart and blood vessels, ageing, inflammation, genetics, cognition, and more besides. There is much to be discovered; we just have to ask the right questions.
Telling the stories of the Wellcome Trust’s work
Editor Chrissie GilesAssistant Editor Tom FreemanWriters Chrissie Giles, Lydia HarrissDesign Marianne Dear Professor Jane Clarke illustration cumi ltdPhotography David SayerPublisher Mark Henderson
Ideas, comments, suggestions? Get in touch:Wellcome NewsWellcome TrustGibbs Building 215 Euston RoadLondon NW1 2BEE [email protected]/wellcomenews
To subscribe:T +44 (0)20 7611 8651E [email protected]/subscribe
All images, unless otherwise stated, are from the Wellcome Library. You can get copies through Wellcome Images (images.wellcome.ac.uk).
Wellcome TrustWe are a global charitable foundation dedicated to achieving extraordinary improvements in human and animal health. We support the brightest minds in biomedical research and the medical humanities. Our breadth of support includes public engagement, education and the application of research to improve health. We are independent of both political and commercial interests. www.wellcome.ac.uk
This is an open access publication and, with the exception of images and illustrations, the content may, unless otherwise stated, be reproduced free of charge in any format or medium, subject to the following constraints: content must be reproduced accurately; content must not be used in a misleading context; the Wellcome Trust must be attributed as the original author and the title of the document specified in the attribution. The views and opinions expressed by writers within Wellcome News do not necessarily reflect those of the Wellcome Trust or Editor. No responsibility is assumed by the publisher for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions or ideas contained in the material herein. ISSN 1356-9112. First published by the Wellcome Trust, 2012. Wellcome News is © the Wellcome Trust and is licensed under Creative Commons Attribution 2.0 UK. The Wellcome Trust is a charity registered in England and Wales, no. 210183. Its sole trustee is The Wellcome Trust Limited, a company registered in England and Wales, no. 2711000 (whose registered office is at 215 Euston Road, London NW1 2BE, UK).PU-5423/17K/06-2012/MD
Wellcome NEWS

4 | Wellcome NEWS Summer 2012 | 5
Fun and games at Wellcome CollectionAs competitors from around the globe prepare to give their best performances at this summer’s Olympic Games, Well-come Collection examines the lengths that humans go to in order to improve their abilities. From elite athletes to comic-book heroes, the Superhuman ex-hibition (19 July–16 October) asks what human enhancement is and where it might lead. An accompanying family ac-tivity trail is available from 18 August.
On 26 July, ‘Sporting Minds’ takes a look at that other essential sporting ele-ment: the spectator. The speakers, who include a sports presenter, radio sound
engineer and a brain researcher, will consider what effect a crowd can have on athletes and how a TV or radio spec-tator’s experience can be enhanced.
Light relief from the competitive spirit comes in the form of ‘Treats on Laughter’, an evening of discussion and performance on the nature of laughter (19 July). See www.wellcomecollection.org for more.
Brainy books aboundIn a flurry of literary activity, a number of Wellcome Trust grantholders and staff have published books of a brainy nature in recent months. Dr Tali Sharot, Wellcome Trust Career Redevelopment Fellow at university College London, has written The Optimism Bias (Constable and Robin-son). In it, she uses her work in neuroim-
aging to explore why the human brain is biased towards generating hope.
In The Geek Manifesto: Why science matters (Bantam Press), Mark Henderson, the Trust’s Head of Communications, ar-gues how and why we need to entrench scientific thinking more deeply into public life, and calls on geeks to unite and take action. Dr Barry Gibb, Science Multimedia Producer at the Trust, has published the second edition of The Rough Guide to the Brain (Penguin). Fully updated to reflect
advances made since the 2007 first edi-tion, this also includes a new chapter on ‘The technological brain’.
Finally, although the exhibition is now closed, you can still enjoy the wonder of Brains: The mind as matter in the book of the same name. It includes 100 images and essays from art historian Marius Kwint and neuroscientist Richard Wingate. Find out more at www.wellcomecollection.org.
Thalidomide papers available2012 marks 50 years since thalidomide was withdrawn for use in the uK. Now, the Wellcome Library has catalogued the ar-chive of the Thalidomide Society, which in-cludes documents on its creation, fundrais-ing schemes and publications. Also catalogued are the papers of Prof. Richard Smithells, a paediatrician who co-discov-ered the harmful effects the drug had on unborn children. This collection includes a copy of Alphabet Zoop, a children’s book he wrote for the NSPCC, as well as different texts on thalidomide he collected during his life. The records are available for use by researchers. To find out more, search the Archives and Manuscripts catalogue (library.wellcome.ac.uk/node49.html) with references SA/TSY (the Society’s ar-chive) and PP/SML (the Smithells papers).
Writing prizeJust under 600 aspiring science writers have entered the 2012 Wellcome Trust Science Writing Prize in association with the Guardian and the Observer. Their efforts will be pored over by a six-strong judging panel that includes comedian Robin Ince and presenter Liz Bonnin alongside Guardian journalists and senior Wellcome Trust staff.
The two winners of the competition – now in its second year – will be announced at a ceremony at Wellcome Collection in September 2012. www.wellcome.ac.uk/swp
Above: A woman affected by thalidomide with her mother, daughter and dog. Larry Dunstan/Wellcome Images
Above: Charles Atlas bodybuilding poster, 1939. Wellcome Library
6 | Wellcome NEWS Summer 2012 | 7
fUNDING NEWS
New investment business announcedThe Wellcome Trust has announced the creation of a new investment busi-ness that will invest in emerging busi-nesses and technologies in the health-care and life sciences sectors.
The business has initial capital of £200 million drawn from the Trust’s endowment and is in the final stages of closing the necessary agreements for operation. it will allow the Trust to identify, invest in, and retain owner-ship positions in promising healthcare
companies, while remaining commit-ted to its other private equity holdings in partnerships with venture investors.
Sir Mark Walport, Director of the Wellcome Trust, said: “This important investment opportunity will help the Trust to fulfil its vision of achieving ex-traordinary improvements in health, by generating returns that can be used to fund the work of outstanding research-ers in the biomedical sciences and the medical humanities.”
Involvement will also enable busi-nesses to turn exciting advances in the life sciences into diagnostics and therapies that contribute to improved patient care.
Global health researchThe Wellcome Trust has launched a new £3.5 million five-year fund to support Centres for Global Health Research. This call expands the remit of the Trust’s existing Centres for Research in Clinical Tropical Medicine and provides opportunities for other institutions to take part. The new funding will support public health and tropical medicine researchers, including clinicians and non-clinicians from the UK and researchers from low- and middle-income countries. wellc.me/LdxPCS
Mood disorders centreAt the University of Exeter, a new £3.6 million building dedicated to researching ways to treat mood disorders has been launched by Sir Mark Walport. The Sir Henry Wellcome Building for Mood Disorders Research provides state-of-the-art facilities to carry out experimental and applied clinical research into mood disorders, including bipolar depression and major depression. www.exeter.ac.uk/mooddisorders
Changing FuturesGene therapy holds huge potential for treating people with cystic fibrosis. The Changing Futures project brought young people with the disease together with a team of artists, scientists and educationalists to explore the history and current state of gene therapy. The project gave the 13-to-18-year-olds a chance to express their experiences of life with cystic fibrosis, as well as their thoughts on gene therapy. The project was developed by Nowgen, supported by a Wellcome Trust People Award. www.changing-futures.co.uk
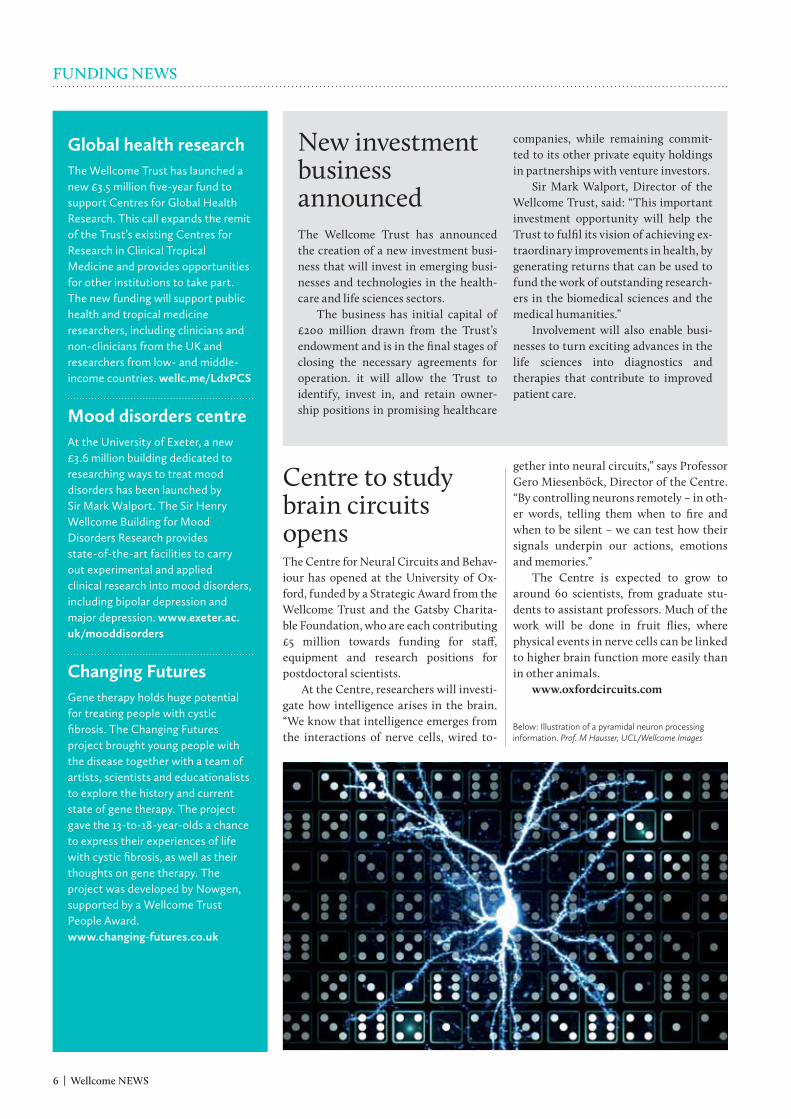
Centre to study brain circuits opensThe Centre for Neural Circuits and Behav-iour has opened at the university of Ox-ford, funded by a Strategic Award from the Wellcome Trust and the Gatsby Charita-ble Foundation, who are each contributing £5 million towards funding for staff, equipment and research positions for postdoctoral scientists.
At the Centre, researchers will investi-gate how intelligence arises in the brain. “We know that intelligence emerges from the interactions of nerve cells, wired to-
gether into neural circuits,” says Professor Gero Miesenböck, Director of the Centre. “By controlling neurons remotely – in oth-er words, telling them when to fire and when to be silent – we can test how their signals underpin our actions, emotions and memories.”
The Centre is expected to grow to around 60 scientists, from graduate stu-dents to assistant professors. Much of the work will be done in fruit flies, where physical events in nerve cells can be linked to higher brain function more easily than in other animals.
www.oxfordcircuits.com
Below: Illustration of a pyramidal neuron processing information. Prof. M Hausser, UCL/Wellcome Images
6 | Wellcome NEWS Summer 2012 | 7
A feast of festival fundingWellcome Trust People and Arts Awards are funding a wealth of thought-provoking events over the summer. If you’re planning to be at the Green Man Festival in Wales in August, then make sure you go to ‘Einstein’s Garden’ – workshops, installations and per-formances that blend science and nature with entertainment, art, craft and design (see below).
The Trust is also supporting a series of events at the Edin-burgh International Book Festival (11–22 August) and several shows at the Fringe. These include two highly personal accounts of living with serious medical conditions, which will tour later in the year. Richard Tyrone Jones’s show is all about life after being diagnosed with a serious heart condition (for more, see page 34), and in ‘Mess’, Caroline Horton weaves a darkly comic theatrical performance out her experience of anorexia nervosa.
Also on a food-related topic, the Dark Side of Eating exhibition explores the darker side of food, comparing medieval ideas with modern scientific research. This runs until the end of September 2012, and is part of the ‘You Are What You Ate’ project, part-fund-ed by the Wellcome Trust.
New call for Health Innovation Challenge Fund Changes to the Health Innovation Challenge Fund will now make it easier for organisations and groups to submit research proposals. The Fund, which is supported equally by the Depart-ment of Health and the Wellcome Trust, facilitates translational health research to create innovative healthcare products, tech-nologies and interventions for use in the NHS and beyond.
The scheme has changed from issuing a series of themed calls and is instead inviting proposals across a set of research topics, valid for all of the rounds of funding in 2012 and in 2013. The five areas of interest are: the clinical applications of genetics; early de-tection and diagnosis of chronic diseases; minimising the impact of trauma and serious injury; informing clinical management through software-based analysis of complex datasets; and repur-posing of medicines and medical devices.
Proposed projects must have already demonstrated proof of principle, supported by experimental data, and must anticipate completion of first testing in humans within the duration of the project. The next preliminary application deadline is 3 September 2012. www.wellcome.ac.uk/HICF
Below: A ‘Science at Play’ attraction at last year’s ‘Einstein’s Garden’. Kendi Muchungi
Portfolio Review
Malaria 1990–2009Our third portfolio review is now published – focusing on human malaria research over the 20 years from 1990 to 2009.
This new report presents an analysis of the key landmarks in the development of human malaria research over the last two decades, and attempts to identify the role of the Wellcome Trust within this.
Available to download: www.wellcome.ac.uk/malariareview/wn
Mos
quit
o in
flig
ht. H
ugh
Stur
rock
/Wel
lcom
e Im
ages

8 | Wellcome NEWS Summer 2012 | 9
RESEARCh NEWS
Mutations key to differences in cancer drug responseScientists have found new information about why not all patients with the same type of cancer respond to the same drugs. Teams from the Massachusetts General Hospital Cancer Center and the Cancer Genome Project at the Wellcome Trust Sanger Institute are collaborating in a five-year programme to catalogue how cancer cells respond to different drugs depending on the precise genetic mutations they have.
The researchers took over 600 cell lines – populations of cells derived from real human cancers – and tested the effec-tiveness of 130 drugs against them. Their results showed that the power of most cancer drugs is influenced by the nature of
the mutations in the cells being treated.“Our work is helping to move cancer
therapeutics away from the conventional tissue-based treatment to a more molecu-lar-based treatment,” said Prof. Daniel Haber, a senior author, from the Massa-chusetts General Hospital Cancer Center. “The next steps are to evaluate some of the key findings using tumour samples and test new candidate therapeutic strategies in clinical trials so we can hopefully im-prove the way we treat cancer patients.”
Garnett et al. Systematic identification of genomic markers of drug sensitivity in cancer cells. Nature 2012;483:570–5.
Researchers use virtual reality to measure brain activityResearchers have developed a new technique that allows them to measure the individual activity of more nerve cells across larger brain areas.
until now, scientists have been re-stricted to measuring individual cell activity across brain areas of typically fewer than a few hundred neurons (in, for example, moving rats). Dr Misha Ahrens, a Sir Henry Wellcome Postdoc-toral Fellow based at Harvard universi-ty and the university of Cambridge, worked with colleagues to develop a technique that allows neuroscientists to study as many as 2000 neurons si-multaneously, anywhere in the brain of a transparent zebrafish.
They created a virtual environment in which they could monitor the ze-brafish’s neural responses when adapt-ing its behaviour. They then manipu-lated the virtual environment to simulate the fish suddenly becoming more ‘muscular’. This served as a sim-plified version of what happens when the brain needs to adapt the way it drives behaviour (e.g. when water tem-
perature changes the efficacy of the muscles).
“Our behaviour is determined by thousands, possibly millions, of nerve cells working in harmony,” says Dr Ah-rens. “The zebrafish performs complex behaviours, with a brain of about 100 000 neurons, almost all of which are accessible to optical recording of neural activity. Our new technique will help us examine how large networks mediate behaviour, while telling us what each individual cell is doing.”
Ahrens MB et al. Brain-wide neuronal dynamics during motor adaptation in zebrafish. Nature 2012 [epub ahead of print].
Pete
r Wat
son
and
John
Sch
wab
e
Spotting the differencesUniversity of Oxford researchers led an international collaboration to identify how protein domains called bromodomains recognise epigenetic changes (heritable characteristics) to histones, the proteins that organise DNA. Using biophysical techniques, the team found that over half the known human bromodomains recognise combinations of epigenetic marks simultaneously, rather than individual changes, as previously thought. This work may lead to the devleopment of new specific inhibitors targeting diseases influenced by the recognition of histone modification. Filippakopoulos P et al. Cell 2012;149(1):213–31.
Diabetes drugSupported by a £2.3 million Wellcome Trust Translation Award, researchers at King’s College London have begun a project to develop the drug MultiPepT1De. MultiPepT1De is designed to counter the immune system response that attacks the beta cells in the pancreas that make insulin, as happens in type 1 diabetes. If successful, this could prevent the disease from developing.
Podo gene linksResearchers have found three gene variants linked to the neglected tropical disease podoconioisis (or ‘podo’), which causes foot swelling and ultimately elephantiasis, and is thought to affect 4 million people worldwide. The genetic variants all fall within a region of the genome known as the HLA class II, which is important in controlling immune responses. Combined, these variants increase the risk of developing podoconiosis by a factor of two to three.Ayele FT et al. The HLA class II locus confers susceptibility to podoconiosis. NEJM 2012 [epub ahead of print].
Above: Zebrafish. Wellcome Images
8 | Wellcome NEWS Summer 2012 | 9
Above: The 13-lined ground squirrel’s genome was one of the 38 searched for virus DNA. Marit & Toomas Hinnosaar on Flickr
Ancient viruses are ‘superspreaders’More than 90 per cent of every mammal’s genome has no known function. This ‘dark matter’ includes DNA from ancient viruses that infected our ancestors as long ago as the age of the dinosaurs. Now, an international team including researchers from the university of Oxford has shown that these viruses are ‘superspreaders’, taking over substantial amounts of their host’s genome.
The team searched the genomes of 38 mammals, including mouse, bat, squirrel, human, elephant and dolphin, and collect-ed and compared genetic material from all viruses present.
One particular group of viruses had lost the ability to infect new cells. While the genetic material is still able to amplify itself, the whole life cycle of the virus is
passed within a single cell. This change, the researchers found, was followed by a dramatic proliferation of the virus’s genet-ic material within the host genomes. They found this to be a universal phenomenon across these viruses.
Oxford’s Dr Robert Belshaw, who led the study, says: “We suspect that these vi-ruses are forced to make a choice: either to keep their ‘viral’ essence and spread be-tween animals and species, or to commit
to one genome and then spread massively within it. This is the story of the epidemic within every animal’s genome, a story which has been going on for 100 million years and which continues today.”
Magiorkinis G et al. Env-less endogenous retroviruses are genomic superspreaders. Proc Natl Acad Sci USA 2012 [epub ahead of print].
Mouse model sheds light on delirium A new mouse model of delirium developed by researchers at Trinity College Dublin has united two theories about its causes.
Delirium is a profound state of mental confusion that can include hallucinations and severe mood swings. It can occur in situations such as after surgery or infec-tion. This has led to the ‘neuroinflamma-tory hypothesis’: systemic inflammation induces inflammation in the brain, which disturbs brain function. But under the ‘cholinergic hypothesis’, delirium results from the decreased action of acetylcholine, a chemical transmitter in the nervous system. Causes could include the loss of brain cells that normally make the chemical, or medi-cation that disrupts its release or action.
using a mouse model, researchers showed that systemic inflammation dis-turbs short-term memory (a key symptom of delirium), but only in mice that had al-ready lost cholinergic cells. “Our work shows that both inflammation and prior damage to the cholinergic cells can com-bine to produce the delirium-like state,” says Dr Colm Cunningham, who led the research. Importantly, neither inflamma-tion nor cholinergic cell loss individually was sufficient to cause this disturbance. Field R et al. Prior pathology in the basal forebrain cholinergic system predisposes to inflammation-induced working memory deficits: reconciling inflammatory and cholinergic hypotheses of delirium. J Neurosci 2012 [epub ahead of print].
Focus on strokeMay was the Stroke Association’s first Action on Stroke month. As part of this, the Welcome Trust blog ran a se-ries of articles, infographics, patient stories, videos and more about the con-dition, which affects 150 000 people per year in the uK and many more
around the world. Through the ‘Focus on stroke’ series, you can find out more about the current state of stroke in the uK, how it can be prevented, and the latest research into ways to treat and rehabilitate people who have had a stroke. Read, share and comment at wellcometrust.wordpress.com/tag/focus-on-stroke/

10 | Wellcome NEWS Summer 2012 | 11

10 | Wellcome NEWS Summer 2012 | 11
always wanted to teach, it was a family tradition. My great-grandmother, grandmother and mother were all teachers.
I took a degree in biochemistry in York,
then did a PGCE and taught science for six years in comprehensives in Leicestershire and Tottenham. I believe in state education, my children went to comprehensive schools, and I feel really strongly that those schools need fantastic teachers and good scientists. After my children were born, I continued teaching part-time. I loved it. It was fulfilling and fun and I was good at it.
Then my husband got transferred to Atlanta, so we moved there as a family. I didn’t have the right qualifications to teach there, so I did a part-time Master’s degree in applied biology at Georgia Tech. That had a research component, which I loved, and a fantastic course on protein structure – so I decided to do some research on proteins.
When we came back to the uK, I tried to get a PhD place in Cambridge, where we live. I went to the biochemistry department and talked to a number of people there, who essentially brushed me off. They more or less told me I’d been out of science so long, was too old to start a science career at 40, and had two children to look after. So I went to see Alan Fersht,
who was a world leader in protein science, and he said, “I’ll give you a studentship, start in October.”
I think it’s a great job to combine with being a mum. When I was a teacher I couldn’t take time off to see my children doing an assembly or work at home if they were ill. As a researcher your working hours are your own. I got childcare in the early morning to get the kids to school. That allowed me to start work very early and be home by 5pm to have tea with them, help with their homework, take them to their clubs and so on. I could go into work at the weekends if I needed to.
We lose too many young women in science. About half our students are women, but there are only four permanent female group leaders here, out of a staff of 60. And I’m the only one with children. It’s a shocking message to give the young women here.
Of course you have to be efficient and you might not always be able to have a tea break with everybody else. But it can be done, and it can be done with fun. I loved it and never looked back. Doing a job well is about the quality of your output, not the number of hours you put in.
Straight after my studentship, I got an MRC Training Fellowship and I stayed in Alan’s group for another three years, learning nuclear magnetic resonance spectroscopy. Then I got
a Wellcome Trust Research Career Development Award and I’ve been with the Trust ever since. I’m now on my third Senior Research Fellowship – my fourth fellowship from the Trust.
I’m Assistant Head of Department at Cambridge at the moment. I have a small group of great people and we work very closely together, so coming to work’s a joy. I’m still teaching, but in a different way, nurturing their careers and encouraging clever young scientists to knock ideas around.
Science is one of the most cooperative, supportive, creative jobs anybody could have. Every time you discover something, it opens up more questions and possibilities. As I once said to the Trust at an interview when I was asked what I’d be doing in five years, “If I could tell you, then you shouldn’t give me the money.”
• For more on the Trust’s flexible research career support, see page 13.
CAREERS
PROFESSOR JANE CLARKE
HOW I GOT INTO... PROTEIN RESEARCHFrom the blackboard to the bench: the university of Cambridge’s Professor of Molecular Biophysics, Jane Clarke, started her career as a science teacher in a comprehensive school in the uK. She later moved with her family to Atlanta, where she took a Master’s degree that kick-started her new career in research. She talks to Penny Bailey.

12 | Wellcome NEWS
A longer version of this article is on the Wellcome Trust blog (wellc.me/KQKOzD). There, you can share it with colleagues, and let us know your thoughts by commenting. For more blog posts, see wellcometrust.wordpress.com.
BEST OF THE BLOG
GET THAT GRANT
ONLINE hIGhLIGhTS
Launched in 2011, Wellcome Trust Investigator Awards work towards our strategic goal of supporting the brightest researchers with the best ideas. So how do you get one? Professor Danny Altmann, Head of Pathogens, Immunology and Population Health, tells you how.
Blog
Investigator Awards are different from conventional grants, so your mindset needs to be different from that for usual applications. Think about the current state of your field and the narrative of your research so far. Then, try to think of the big, transformative questions that you could take on to really move the field forward. Be bold and creative.
Once you’ve checked that you’re eligible (see www.wellcome.ac.uk/investigators), use the initial CV check on our eGrants system to see if your research question is suitable.
At this stage, we’ll be looking for evidence of a successful ongoing contribution to your field. This is likely to be reflected in a combination of publications, grant income and other markers of esteem. Next, you will be invited to submit your full application for the scheme.
With a different scheme comes a different application form. Do all you can to tell the Expert Review Group that will be reading it about your past contributions: choose your most significant publications, key breakthroughs, impact through mentorship and past funding history.
The next part is the research plan. Here you’ll need to strike a fine balance: your proposal will be read by both specialists and non-specialists in your research area, and must be equally accessible. It must offer a high-level, exciting view of your big research vision, while also offering sufficient substance that a referee would be able to understand what you aim to do, how you plan to do it and analyse it, and whether it’s likely to work.
The panel has been briefed to reject proposals that are merely incremental, worthy or solid and to seek out the ideas that are transformative, bold and exciting.
As with any application, if success depends on access to particular technology, collaborations or resources, be sure to spell out that you have these in place. Ensure that the questions you’re asking are realistic with respect to the length of time and costs you’ve requested. It’s worth noting that the scheme allows for joint applications from two investigators (see Bill Cookson and Miriam Moffatt’s story in Wellcome News 70).
The proposal will be sent out to members of the appropriate review group, two or three of whom will be asked to present it to the rest of the panel. Their task is to debate the strengths and weaknesses of each application. They are not briefed to accept proposals up to any particular budget or quota cut-off. Scoring allows
them to rank proposals into those recommended to go to the next stage, those that might do so, and those that should not be taken any further. Any ‘possibles’ are re-evaluated at a joint meeting of all the review groups and the best of these progress to the next phase: interview by a Selection Panel.
At interview, the Selection Panel is composed of outstanding international scientists who are used to taking a ‘generalist’ view of scientific strategy. No matter how much of an old hand you are at presenting your work, we recommend that you get senior colleagues to grill you at mock interview.
You may be addressing a room of people who, though massively experienced in biomedical science, may not have a detailed insight into your field. They will need to be won over. But remember, they will be armed with a detailed critique from the expert reviewers. They may seek to probe you on precisely how the work will be done and analysed. You will be allowed to bring three PowerPoint slides to help you explain your vision – choose these wisely.
If successful, we’ll call you to tell you the good news and start negotiating the details of your funding package.
Any questions? Contact us or pop in for a chat. Email [email protected] or call our Grants Management Service Desk on 020 7611 2020.
Wel
lcom
e Im
ages

Summer 2012 | 13
Professor Dame Kay Davies is a Governor and Sir Mark Walport is Director of the Wellcome Trust.Find out more at our new flexible research careers web page: wellc.me/JzXMBm
PROFESSOR DAME KAY DAVIES AND SIR MARK WALPORT
“Research careers need to be flexible – for all”OPINION
hat proportion of board members of FTSE 100 companies are women? Not half, not even a quarter – just 15 per cent. According to a 2011 report by Lord Davies it would, at the current
rate of change, take over 70 years to achieve equality on these boards.
This disparity is not unique to business. The further you move along the scientific career pathway, the fewer women you see. Recent analysis of a group of Wellcome Trust-funded PhD students showed that while 93 per cent of the men were still working in academia three years after completing their PhDs, the percentage of women was only 48. Representation at the senior levels is even lower. Only 30 per cent of lecturers and a mere 12 per cent of professors in the uK are female.
understanding the reasons behind these stark statistics is not straightforward. It can also be difficult for anyone who has taken a substantial career break to return to research. Various organisations are working to address these issues and, here at the Trust, we’re trying too. For example, we’ve created Research Career Re-entry Fellowships, which provide an opportunity for researchers who have been away from the bench for over two years to rejoin the workforce, as well as the chance to work flexibly on our grants. While we strive to develop ways to ensure that we offer
fair and flexible grant funding, the patterns of behaviour and the choices women make don’t appear to be changing significantly. Clearly, we can and must do more.
So we are making it easier to find details of our relevant funding schemes and other information that promotes flexible research careers for women and men, by gathering this material together on a new web page. We are changing our grant application forms so that they prompt people to tell us about past career breaks and part-time working, and to request flexible working if they wish. We will also be asking universities where we fund how they support flexibility and equality in the workforce.
We are looking at how our flexible funding approaches are making a difference. We keep track of the demographics of our applicants and awardees and we will use our Career Tracker, a longitudinal study of Trust awardholders’ careers over time, to inform what we do in the future.
We believe passionately that breakthroughs in research emerge when the most talented researchers are given the resources and freedom they need to pursue their goals. Success in this demands diversity – of people, ideas and approaches. So we will continue to provide flexibility in the range of scientific career opportunities that we offer.

14 | Wellcome NEWS
Peter Rothwell at the John Radcliffe Hospital, Oxford.

Spring 2012 | 15
STROKE PREVENTION
PROFESSOR PETER ROTHWELL
From tracing missing patients to raiding dusty basements, Peter Rothwell has been finding new approaches to preventing stroke and cancer in some surprising places. He tells Lydia Harriss how the search for answers doesn’t have to be complicated.
THE SIMPLE TRuTH
have written lots of rants in various journals over the years,” says Peter
Rothwell, Professor of Clinical Neurology and
Director of the Stroke Prevention Research unit at the university of Oxford, with a hint of amusement. It’s hard to imagine the softly spoken Peter, sitting in his office with its tranquil views over leafy Oxfordshire, raging against the medical establishment. “You just wouldn’t believe how much ridiculously simple clinical research hasn’t been done that should have been addressed 50 years ago.”
Peter’s own knack for asking what he describes as “simple clinical questions” has led to an impressive array of discoveries that have challenged established medical understanding and helped transform clinical practice. His primary focus over the past 20 years has been to understand what causes stroke and what can prevent it, particularly in patients who have already had a minor stroke or transient ischaemic attack (TIA).
Stroke is estimated to be responsible for around 10 per cent of deaths
worldwide and is caused either by blockage of a blood vessel supplying blood to the brain or by bleeding inside the brain. “From the patient’s point of view, it causes a sudden-onset loss of some neurological function. It might be a sudden weakness down one side of the body or loss of speech or vision,” Peter explains.
In the uK, 150 000 people are estimated to have a stroke each year. According to Peter, roughly a third of these have major strokes that are “relatively disabling and require hospital admission”. The other two-thirds have less severe and more transient symptoms, caused by strokes that fall into two categories: TIAs that last for under 24 hours and minor strokes that last from 24 hours up to several days.
Working at the John Radcliffe Hospital in Oxford in the late 1990s, Peter was treating patients who had experienced transient stroke-like symptoms and had been referred by their GPs for further investigation. unsurprisingly, there were always some patients who did not turn up for their appointments. Had they forgotten?
Did they have more urgent things to do? No. When Peter and his colleagues conducted an audit to answer the seemingly trivial question – what happened to the missing patients? – they found that nearly every one had been admitted to hospital having had a major stroke.
Warning signs“until then, minor strokes and TIAs were thought to be relatively benign,” Peter says. Previous research had shown that following a ‘warning’ TIA or minor stroke, “the risk of a major stroke was only about 1–2 per cent at one month and 2–4 per cent at one year”. However, patients were only studied when they came to hospital for their appointments, which, Peter says, were often two to three weeks or sometimes months after the initial minor stroke or TIA. Consequently, clinicians and researchers had missed the short-term risk of major stroke during the first few days following a warning event.
Peter started a collaboration with local GPs. “We wanted to define the natural history [progression] of minor

16 | Wellcome NEWS Summer 2012 | 17
stroke and TIA properly, by studying patients from the onset of the event,” he says. With a Senior Clinical Fellowship from the Medical Research Council, he established the Stroke Prevention Research unit at the John Radcliffe Hospital in 2000 and the Oxford Vascular Study (OXVASC) in 2002. OXVASC has given Peter and his team access to almost all patients with minor strokes, TIAs and other acute vascular events within a population of 100 000.
Even Peter was surprised by what they found. “We worked out that the risk of [recurrent] stroke in the first week after a ‘warning’ event was about 10 per cent,” he says.1 As this was significantly higher than previously thought, he felt it called for a dramatic change in the way that the medical establishment and patients viewed TIA and minor stroke: “We wrote dozens of papers, boring our colleagues senseless, trying to rebrand this condition as an emergency.”
Although OXVASC had made the case for treating minor stroke and TIA as emergencies, changes to medical guidelines and healthcare systems required more evidence. “We knew that antiplatelet drugs and blood-pressure-lowering drugs [common
treatments for stroke] reduced the long-term risk of stroke, but there was no evidence that starting them immediately made much difference compared to starting them a week or two later,” Peter explains.
Reducing the waitHis solution was to use OXVASC to study the effect of reducing the time that patients waited for treatment. OXVASC had already been seeing patients urgently in a daily clinic for two-and-a-half years, but had only been advising GPs on what treatments to prescribe. Peter and his colleagues made two simple changes. First of all, instead of using appointments, the clinic operated a ‘walk-in’ service that allowed patients to be assessed more quickly. Secondly, treatments were started in the clinic rather than after a return visit to the GP (see box on page
18). He and his team compared the risk of recurrent stroke in patients seen before the changes and patients seen after.
The results were striking. “We found that there was an 80 per cent reduction in the risk of early recurrent stroke,” he says.2 Such a marked improvement was difficult to dispute, and Peter’s tenacity was finally rewarded when medical guidelines in the uK and internationally were changed to recognise minor stroke and TIA as urgent conditions requiring immediate treatment. Almost all hospital trusts in England now offer specialist clinics for the rapid assessment and treatment of these conditions.
“Stroke is one of the most common diseases in the developed world, yet we didn’t even understand its natural history. I think that the public – and even non-clinical research colleagues –
You just wouldn’t believe how much ridiculously simple clinical research hasn’t been done that should have been addressed 50 years ago.”

Left: Peter Rothwell’s colleague Linda Bull demonstrating a blood-pressure test. Above right: Contrast-enhanced magnetic resonance angiograms showing the main arteries from the heart to the brain in a patient with a recent minor stroke. Below right: A patient’s home blood-pressure measurements, sent to the Research Unit via Bluetooth.
16 | Wellcome NEWS Summer 2012 | 17
would be surprised about how much simple clinical research is yet to be done.” It’s an issue that Peter says extends beyond stroke. “For example, blood pressure is probably the most important single modifiable risk factor for disabling disease in the world, possibly apart from smoking. It causes dementia, heart attacks, stroke, all sorts of things, and yet we really don’t understand it very well.”
Rising pressure“The clinical guidelines advised that doctors should measure the ‘usual blood pressure’,” a theoretical baseline, by taking blood pressure measurements many times over weeks and calculating an average. However, a patient’s blood pressure often varies so much from one day to the next that, Peter says, the average level is not particularly informative. “Consequently, many GPs often found it difficult to apply the guidelines. They tended to believe the lower values, thinking that these probably represented the underlying ‘usual’ blood pressure, and ignored the peaks.”
Determined to explore this variation, Peter himself wore a blood pressure monitor 24 hours
a day for six months. It made a whirring noise every 15 minutes as the cuff around his arm inflated to make a measurement. “It annoyed my wife intensely,” he laughs, but “it did reassure me that this variability business was real. until then, many people regarded variability of blood pressure as meaningless background noise.”
It also revealed how strongly his own blood pressure depended on the activities he was doing. “Certain colleagues put my blood pressure up, other colleagues lowered it.” In a single day at the 2008 World Stroke Conference, his blood pressure soared when he chaired a difficult meeting, dropped again afterwards, then cycled through a series of peaks and troughs as he gave a series of lectures.
By analysing existing data from several large studies of patients previously treated for TIA or high blood pressure, the Oxford team has highlighted flaws in the ‘usual blood pressure’ hypothesis3 and shown that measurements of variability of blood pressure over time (such as the standard deviation) are more strongly related to a patient’s risk of stroke than their average blood pressure level.4
They have also found that some
drugs being used to reduce average blood pressure, such as beta-blockers, increase blood pressure variability5 and actually increase the risk of stroke. Others, such as calcium-channel-blockers and diuretics, reduce variability and are particularly effective at preventing stroke. Peter says, “It’s another example of simple clinical research that could have been done a long time ago.”
Peter’s talent for seeing new potential in old data has opened up another avenue for his research. Driven by an interest in aspirin that stems from the Oxford TIA and minor stroke clinics’ prescribing it to some 2000 patients every year, he has begun to look more closely at how it influences diseases other than stroke and heart attack. “Aspirin affects the main pathway that’s responsible for inflammation and other fundamental processes in disease,” he says. “It’s inconceivable that it would only affect the risk of vascular events [such as heart attacks and strokes].”
He has spent months in dusty basements trawling through boxes of yellowing papers, hunting down data from old clinical trials involving aspirin. using cancer registrations and other

Right: Peter Rothwell and colleague Dr Alastair Webb checking patient files.
18 | Wellcome NEWS Summer 2012 | 19
Treating minor strokesPatients who have had minor strokes or transient ischaemic attacks can attend walk-in clinics at the Stroke Prevention Research Unit, University of Oxford. The process is:• All initial investigations conducted on
the same day – typically including magnetic resonance brain and arterial imaging and ultrasound imaging to measure blood flow, electrocardiography to detect heartbeat irregularities, and blood pressure monitoring.
• Treatment started immediately and patient sent home.
• Patient usually wears a heart rate monitor for five days to detect transient irregularities in heart rate and rhythm.
• Patient manually takes three sets of blood pressure measurements every day for at least a month. Results are automatically transmitted to the SPRU.
• Clinicians monitor blood pressure readings daily and modify treatment accordingly.
documents to track patients’ health after these trials finished, he has found that a daily dose of aspirin substantially reduced the risk of patients’ developing colorectal, oesophageal and other cancers for several years after the trials ended.6
These findings have exciting implications for preventing cancer, which Peter and his team are continuing to explore. One of his most recent studies7 indicates that aspirin can also prevent metastasis, the spread of cancer to other parts of the body. “I hope that will end up being a big new avenue for improving cancer survival rates,” he says.
Research conducted in the 1960s showed that aspirin reduced cancer metastasis in mice,8 but wasn’t investigated further at the time. “It’s a good illustration of how there is sometimes a lack of joined-up thinking from the basic lab work to the clinical work. People don’t always ask: ‘How could we answer that question with existing data?’” Although Peter’s tone is matter-of-fact, it’s clear that he finds it frustrating.
Making more of the data and treatments already available is a theme that continues to run throughout Peter’s research. With support from a Wellcome Trust Senior Investigator Award, he’s developing techniques to predict the longer-term risk of recurrent stroke more accurately and looking at whether blood pressure variability plays a causal role in the development of other diseases, such as dementia. Aspirin also remains an important part of his work and he’s continuing to explore the risks and benefits associated with it.
“Obviously we need to do basic laboratory-based research to develop new diagnostic tests and treatments…but we also need to put more effort into trying to do better with the tools that we already have,” Peter says. His own work is a compelling example of what this can achieve. If his “rants” don’t persuade his colleagues, perhaps his results will.
• Read more about the history and uses of aspirin on page 24.
1 Coull AJ et al. Population based study of early risk of stroke after transient ischaemic attack or minor stroke: implications for public education and organisation of services. BMJ 2004;328:326–30.
2 Rothwell PM et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet 2007;370:1432–42.
3 Rothwell PM. Limitations of the usual blood-pressure hypothesis and importance of variability, instability, and episodic hypertension. Lancet 2010;375:938–48.
4 Rothwell PM et al. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet 2010;375:895–905.
5 Webb AJ et al. Effects of antihypertensive-drug class on interindividual variation in blood pressure and risk of stroke: a systematic review and meta-analysis. Lancet 2010;375:906–15.
6 Rothwell PM et al. Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet 2011;377:31–41.
7 Rothwell PM et al. Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers during randomised controlled trials. Lancet 2012;379:1591–601.
8 Gasic GJ et al. Antimetastatic effects associated with platelet reduction. Proc Natl Acad Sci USA 1968;61:46–52.

18 | Wellcome NEWS Summer 2012 | 19
20 | Wellcome NEWS Summer 2012 | 21
CLOSE-UP
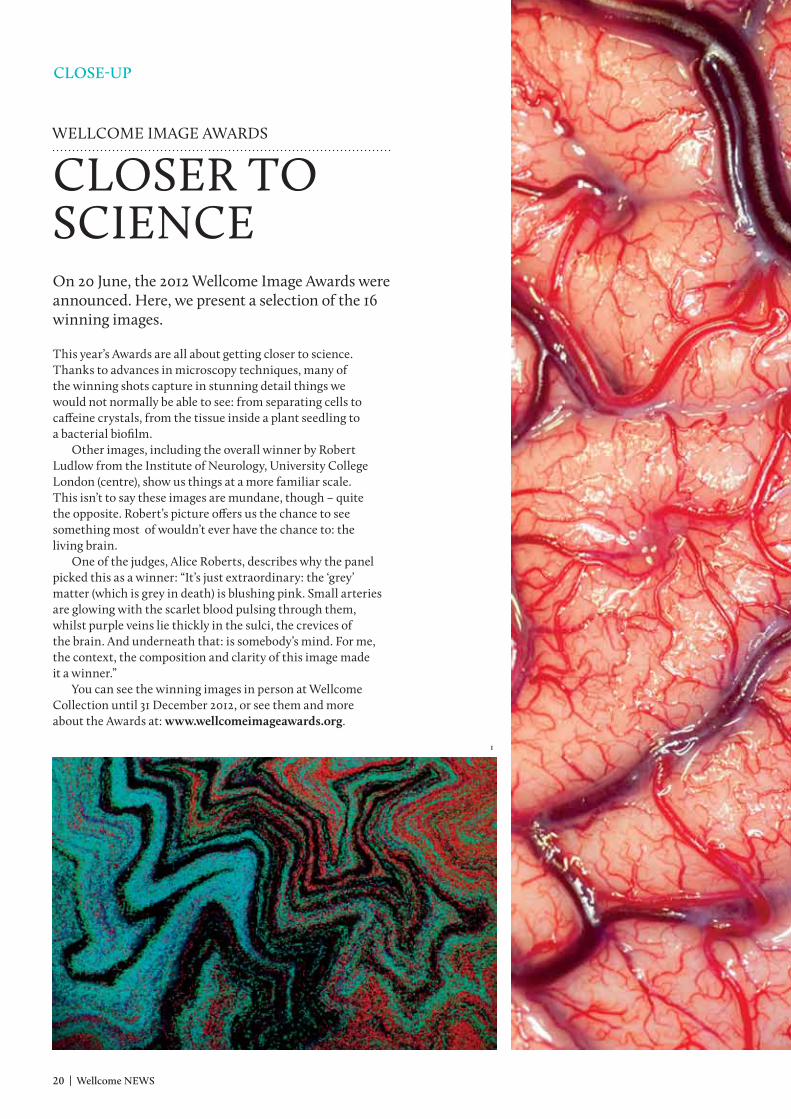
This year’s Awards are all about getting closer to science. Thanks to advances in microscopy techniques, many of the winning shots capture in stunning detail things we would not normally be able to see: from separating cells to caffeine crystals, from the tissue inside a plant seedling to a bacterial biofilm.
Other images, including the overall winner by Robert Ludlow from the Institute of Neurology, university College London (centre), show us things at a more familiar scale. This isn’t to say these images are mundane, though – quite the opposite. Robert’s picture offers us the chance to see something most of wouldn’t ever have the chance to: the living brain.
One of the judges, Alice Roberts, describes why the panel picked this as a winner: “It’s just extraordinary: the ‘grey’ matter (which is grey in death) is blushing pink. Small arteries are glowing with the scarlet blood pulsing through them, whilst purple veins lie thickly in the sulci, the crevices of the brain. And underneath that: is somebody’s mind. For me, the context, the composition and clarity of this image made it a winner.”
You can see the winning images in person at Wellcome Collection until 31 December 2012, or see them and more about the Awards at: www.wellcomeimageawards.org.
1
WELLCOME IMAGE AWARDS
CLOSER TO SCIENCEOn 20 June, the 2012 Wellcome Image Awards were announced. Here, we present a selection of the 16 winning images.
20 | Wellcome NEWS Summer 2012 | 21
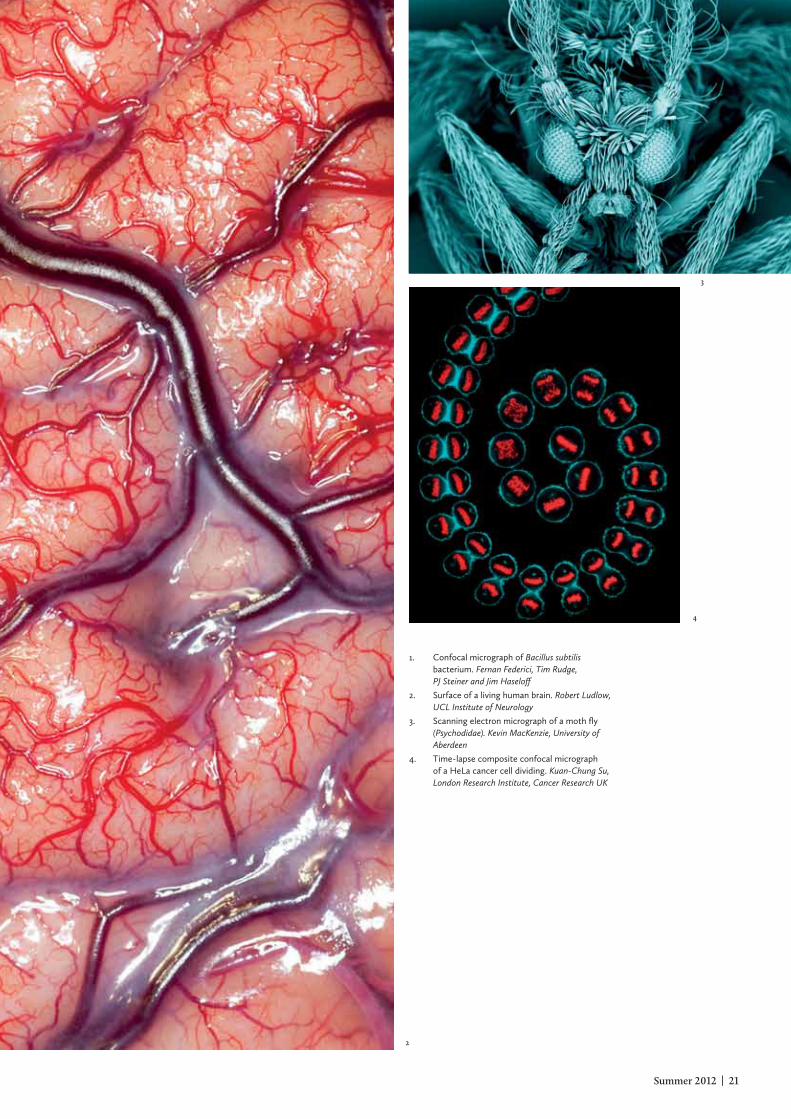
1. Confocal micrograph of Bacillus subtilis bacterium. Fernan Federici, Tim Rudge, PJ Steiner and Jim Haseloff
2. Surface of a living human brain. Robert Ludlow, UCL Institute of Neurology
3. Scanning electron micrograph of a moth fly (Psychodidae). Kevin MacKenzie, University of Aberdeen
4. Time-lapse composite confocal micrograph of a HeLa cancer cell dividing. Kuan-Chung Su, London Research Institute, Cancer Research UK
2
4
3

Global health trials: third call for outline proposals
£12 million is now available to fund late-stage efficacy and effectiveness trials of interventions that will address major causes of mortality and morbidity in low- and middle-income countries.
Interventions of all kinds are eligible, including behavioural interventions, complex interventions, disease management, drugs, vaccines, hygiene and diagnostic strategies. Social science research is also encouraged where relevant.
Proposals are now invited from academic groups based either in the low- and middle-income countries where the studies will take place or in the uK. The submission deadline for outline applications is 11 September 2012.
For more information, visit www.mrc.ac.uk/jointghtrials or email [email protected]
Maximising impact, improving health A
nurs
e in
Eth
iopi
a. S
asha
And
rew
s/W
ellc
ome
Imag
es

AuTISM RESEARCH TRAINING PROGRAM
DR MAYADA ELSABBAGH
IN ThE hOT SEAT
How did this work come about?This paper was the scientific, peer-reviewed version of a report for the World Health Organization. The project aimed to assemble evidence from around the globe on a number of questions around autism. We were asked to look at prevalence using a systematic review methodology. Why is prevalence important?In research we tend to focus on a very narrow subset of the human population, by virtue of where we’re actually conducting the research. So, most studies up until the time we did this review came from small subsets in high-income countries. Prevalence gives you an insight into the true burden of autism in different countries and so is critical for policy makers to make informed decisions.
How did you do this work?We went to our wider research networks and invited people from different countries to contribute to the systematic review. We asked them to take their standard, mainstream search-engine approach but also asked them to use search engines that we may not have used before – those in different languages or that might highlight literature that has not made it to the forefront of autism research. For example, if you look at the main search engines in the West, you may think there are no estimates of prevalence in China; that’s just not the case.
What about places with few studies?In areas where there was very little capacity for research we tried to get the perspective from people on the ground, ensuring any studies that had been done were accounted for. We appraised all studies to ensure they met a few standards. Those that didn’t were still mentioned in the paper, because we wanted to be as comprehensive as
possible and bring these changes to the consciousness of the wider research community. We couldn’t find any prevalence studies on Africa – the entire continent – in mainstream literature, something confirmed by a team working in South Africa. We did get a lot of helpful information from the researchers describing the situation, though, who affirmed findings from the 1970s that defining features of autism in African children were comparable to observations made in the uK. We managed to address some of the mythology – that autism is a Western concept, for example.
Did anything surprise you?This work presented some interesting investigative exercises! We ended up being able to say this is where data exists, and here is where it doesn’t, so if you’d like to make big claims, you better have evidence. Looking at the prevalence estimates that exist, we found very little evidence that there is a difference between prevalence in different geographical regions.
On a personal note, because I’m a brain scientist and not an epidemiologist, this was a really great learning exercise for me. Projects like these force scientists to contextualise what we do in a broader framework of how to resolve the challenges that confront communities in which we live as well as those across the world.
Our engagement with those communities may support evidence-based policies and, at the same time, provide important and relevant feedback to the research community about where the most pressing needs are, and some inspirational ideas to think differently around the research agenda. It’s this reciprocal process that I’m really interested in.
Elsabbagh M et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res 2012 [epub ahead of print].
Interested in the ‘common ground’ bringing together researchers and the communities in which their findings can have an impact, Dr Mayada Elsabbagh from McGill university, Canada, coordinated researchers across the world to understand more about what we know – and don’t know – about the prevalence of autism.
Autis
m R
esea
rch
Trai
ning
Pro
gram
Summer 2012 | 23

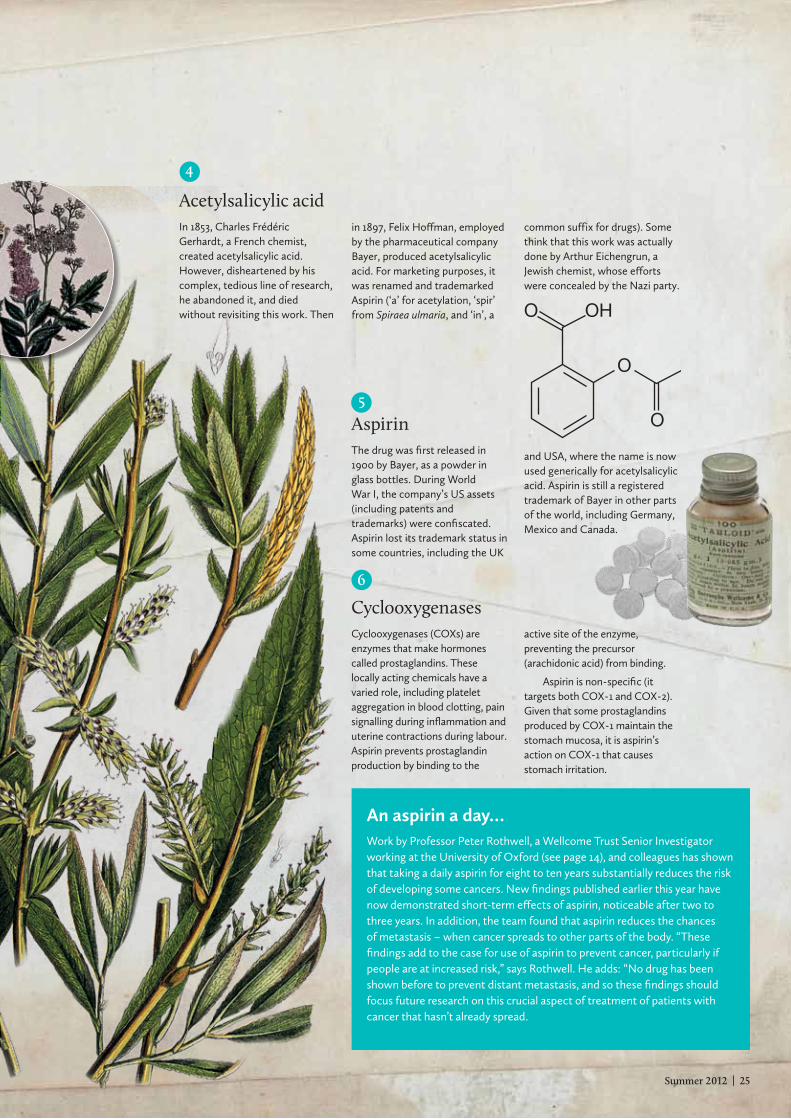
Cheap and widely available, aspirin has been lauded as perhaps the world’s most commonly used drug. Find out more about its history and use today in this quick guide by Chrissie Giles.
NUTS AND BOLTS
DRuGS
ASPIRIN
1
WillowMembers of the genus Salix, willows are trees and shrubs whose bark and leaves contain salicin (see above). The pain-relieving capacity of willow bark was recognised in ancient Greece, and has been used ever since to relieve pain, fever and inflammation.
2
SalicinThis bitter-tasting chemical is found in willow leaves and bark. In the body it is broken down to salicylic acid, which is similar to the active ingredient in aspirin. Oxfordshire vicar Edward Stone spent five years testing the ability of the dried bark of the white willow (Salix alba) to cure fevers. He wrote to the Royal Society with his findings in 1763.
3
MeadowsweetThis herb (Filipendula ulmaria, formerly Spiraea ulmaria; see right) was traditionally used in bridal bouquets and as a strewing herb, to spread over floors. Its medical potential was revealed in the 1830s, when a pharmacist from Berne, Johann Pagenstecher, distilled meadowsweet flowers
to produce salicylaldehyde, which he sent to chemist Karl Lowig. Lowig oxidised this chemical to produce what he named spirsäure, which was in fact salicylic acid. Unwanted side-effects of this drug included mouth irritation, stomach bleeding and tinnitus.
24 | Wellcome NEWS
According to the Aspirin Foundation (which is supported by the pharmaceutical industry), some 35 000 tonnes of aspirin are made and consumed each year, equivalent to 100 billion tablets. Hundreds of other medications include aspirin in their ingredients.
Chemicals similar to aspirin occur naturally in plants such as willow, the bark of which has been used to reduce fever and pain for thousands of years. By studying these chemicals, researchers eventually created acetylsalicylic acid – the active ingredient in aspirin. More palatable and with fewer side-effects than its naturally occurring relatives, acetylsalicylic acid caught on quickly after its launch in 1899. In 2003 the World Health Organization included the chemical in its list of essential medicines.
Like other salicylates, aspirin reduces fever, inflammation and pain (acting, respectively, as antipyretic, anti-inflammatory and analgesic). Through its effects in platelets on the enzyme cyclooxygenase 1, aspirin can reduce the chance of heart attack and stroke. It also shows promise in protecting against cancer (see box, far right). John Vane, Sune Bergström and Bengt Samuelsson won a Nobel Prize in 1982 for their research into prostaglandins and aspirin.
There is still plenty of research into aspirin happening today. For example, scientists are working to find the dosage that will give maximal efficacy with minimal side-effects. Others are exploring whether some patients really are ‘resistant’ to the drug’s effects on platelets.
One thing we know is that not all animals can tolerate aspirin. The enzyme that breaks down the drug in the liver has evolved into a non-functioning form in some creatures, meaning that even small doses could be fatal for cats, as well as brown hyenas and northern elephant seals.
• Find out more at: www.rcsb.org/pdb/101/motm.do?momID=17 and uchomp.bsd.uchicago.edu/ppt/23aspirin.ppt
All images from Wellcome Images
HO
OH
OH
OH
OH
O
O
5
AspirinThe drug was first released in 1900 by Bayer, as a powder in glass bottles. During World War I, the company’s US assets (including patents and trademarks) were confiscated. Aspirin lost its trademark status in some countries, including the UK
and USA, where the name is now used generically for acetylsalicylic acid. Aspirin is still a registered trademark of Bayer in other parts of the world, including Germany, Mexico and Canada.
6
CyclooxygenasesCyclooxygenases (COXs) are enzymes that make hormones called prostaglandins. These locally acting chemicals have a varied role, including platelet aggregation in blood clotting, pain signalling during inflammation and uterine contractions during labour. Aspirin prevents prostaglandin production by binding to the
Summer 2012 | 25
An aspirin a day…Work by Professor Peter Rothwell, a Wellcome Trust Senior Investigator working at the University of Oxford (see page 14), and colleagues has shown that taking a daily aspirin for eight to ten years substantially reduces the risk of developing some cancers. New findings published earlier this year have now demonstrated short-term effects of aspirin, noticeable after two to three years. In addition, the team found that aspirin reduces the chances of metastasis – when cancer spreads to other parts of the body. “These findings add to the case for use of aspirin to prevent cancer, particularly if people are at increased risk,” says Rothwell. He adds: “No drug has been shown before to prevent distant metastasis, and so these findings should focus future research on this crucial aspect of treatment of patients with cancer that hasn’t already spread.
4
Acetylsalicylic acidIn 1853, Charles Frédéric Gerhardt, a French chemist, created acetylsalicylic acid. However, disheartened by his complex, tedious line of research, he abandoned it, and died without revisiting this work. Then
in 1897, Felix Hoffman, employed by the pharmaceutical company Bayer, produced acetylsalicylic acid. For marketing purposes, it was renamed and trademarked Aspirin (‘a’ for acetylation, ‘spir’ from Spiraea ulmaria, and ‘in’, a
common suffix for drugs). Some think that this work was actually done by Arthur Eichengrun, a Jewish chemist, whose efforts were concealed by the Nazi party.
OHO
O
O
active site of the enzyme, preventing the precursor (arachidonic acid) from binding.
Aspirin is non-specific (it targets both COX-1 and COX-2). Given that some prostaglandins produced by COX-1 maintain the stomach mucosa, it is aspirin’s action on COX-1 that causes stomach irritation.

26 | Wellcome NEWS
ight weeks after Bella Williams was born, her mother, Jessica, knew that something
was terribly wrong. “At six weeks old, she was still
not fitting into newborn clothes,” says the 32-year-old primary-school teacher, who’d been told that her first child was simply a fussy feeder. On later advice, Jessica gave up breastfeeding and put Bella on formula milk, but to no avail.
“She was quite floppy and I could feel her spine. She didn’t really have a bottom. I was also worried about her eyesight, because she’d try to make eye contact and her eyes would go in different directions.” Her GP ordered further investigations; an MRI scan revealed lesions on the brainstem, dating back to early pregnancy.
Then came a barrage of terms that Jessica and her soldier husband, Karl, had never heard before – metabolic disorder, mitochondrial inherited disease (MID) and suspected Leigh syndrome – and the sit-down talk that every parent with a sick child fears the most. To have serious symptoms at such a young age, they were told, probably signalled a severe form of MID, which means her cells are not making enough energy to function properly. The prognosis for Bella, now four months old, would be uncertain but she would
be unlikely to survive to school age. The Williams family must now live with the chronic uncertainty that is the hallmark of MID, and the painful knowledge that there is probably very little that medical science can do for Bella.
Energy crisis“I explain to my patients and families that if you have a severe defect in your batteries, it is incompatible with life,” explains Doug Turnbull, Professor of Neurology at Newcastle university’s Institute for Ageing and Health. He and his colleagues – Professors Robert Lightowlers, Patrick Chinnery, Robert Taylor, Mary Herbert and Zofia Chrzanowska-Lightowlers – have been awarded a total of £5.8 million (£4.4m from the Wellcome Trust and £1.4m from the university) to establish the Wellcome Trust Centre for Mitochondrial Research.
As well as advancing fundamental understanding of how mitochondria power our bodies – and how they go wrong – the Centre also has a profoundly important social goal in mind: to perfect radical advances in IVF techniques that could free some families like Bella’s from the shadow of MID for ever. What this means is that the Newcastle team don’t only have to overcome the technical challenges of perfecting these techniques. They also
have to make a very different social and ethical argument, to win the support of ministers and MPs for the change in the law that would allow them to start treating patients.
There are hundreds of MIDs, with their origins in malfunctioning mitochondria. Technically, mitochondria are organelles (small, independent subcellular entities) that exist inside our cells and convert carbohydrates and fat into chemical energy, called ATP (adenosine triphosphate). ATP is the fuel of life – without it, cells can’t function properly – and any mis-step in its chemical supply chain can disrupt normal cell functioning. Every cell of your body (apart from red blood cells) contains mitochondria.
Each mitochondrion carries multiple copies of mitochondrial DNA (mtDNA). This DNA is quite distinct from the DNA in the cell nucleus, to which mothers and fathers contribute equally. Instead, mtDNA is a genetic heirloom handed down exclusively from mothers to their children, through the generations. The mitochondria that power your cells contain mtDNA that you inherited from your mother, which she inherited from her mother, and so on.
26 | Wellcome NEWS
INhERITED CONDITIONS
AVOIDING TRANSFER OF MITOCHONDRIAL DISEASES
OuT OF THESHADOWSMitochondrial inherited diseases can devastate families, but there is hope that new techniques could prevent them passing from mother to child. Anjana Ahuja speaks to the researchers at the forefront of this research, and a family living with the reality of such a condition, to find out more.
Summer 2012 | 27
In a person with MID, something goes wrong in the biochemical kitchen. If only a few mitochondria in the crowd are out of action, then the cell might still be able to produce enough ATP to function. But if most mitochondria in the cell are compromised, then ATP production isn’t possible.
Scientists believe that if the proportion of malfunctioning mitochondria in a cell exceeds a threshold – say around 60 per cent – then the cell is plunged into an energy crisis. This is why disease sometimes takes a while to emerge: the division and replication of mitochondria during a person’s development allows a critical mass of faulty mitochondria to accumulate and eventually shut down cell metabolism.
Many symptoms, few optionsIn the clinic, every patient has a different distribution of uncompliant mitochondria, and so symptoms can be as bewilderingly diverse as muscle weakness, diabetes, neurological disorders and blindness – and their severity spans the whole spectrum of disease. Muscle weakness that worsens over time is one of the best-known features of MID; the Muscular Dystrophy Campaign has worked very closely with the Newcastle team.
“Some people have no symptoms,
while some patients die within the first 48 hours of life,” says Doug Turnbull, who, with colleagues in Newcastle, also runs one of three clinics offering nationwide diagnosis and treatment for patients with MID in the uK (the others are in London and Oxford).Interestingly, an estimated one in 200 people carries a pathogenic mtDNA mutation, but the incidence of diagnosed disease is much lower, at one in 10 000 (perhaps because many people with milder impairments never seek medical help).
When it comes to treatment, though, clinicians are frustratingly short of options. “There aren’t really good treatments out there,” Turnbull admits, although transplantation can be an option when disease is confined to a specific organ, such as the heart or kidneys. “There are a few things we can do to help – so if the heart is involved, we can use drugs to reduce the load of the heart. We can sometimes increase the amount of mitochondria through exercise. But we can’t correct the genetic defect and there’s no tablet yet that makes the mitochondria work better.”
Looking for a revolutionGiven the limited menu of treatment options, Turnbull believes that one way to make headway is to stop transmission in the first place. Pre-
implantation genetic diagnosis has been used to help a few families to minimise the risk of having affected children. It involves a couple undergoing IVF treatment to produce multiple embryos, which can then be tested for the mtDNA mutation. The idea is to rank the embryos according to their mtDNA mutation level and choose one with a low mutation level. But it doesn’t work for everyone.
“Some couples produce embryos that have high levels of mtDNA mutation,” Turnbull points out. “If all your embryos have mutation rates of 50 per cent or more, what do you do? One of my patients lost seven children with the same defect, six within the first 48 hours of life and a seventh child at 21. In those circumstances we have to find a new way of helping those families.”
This is why researchers are looking at the possibility of mitochondrial transplants. One such technique is pronuclear transfer (PNT). If successful, this could be as revolutionary for MID as IVF was for infertility. PNT is a reproductive technique that has the potential to prevent the transmission of mutated mtDNA, not just to the resulting child but potentially to all future descendants. Since faulty mtDNA is transmitted through the egg (mtDNA resides in the cytoplasm, the jelly-like substance surrounding the
Clockwise from left: Mitochondria (in red) in a liver cell (University of Edinburgh/Wellcome Images), Profs Patrick Chinnery, Mary Herbert (Newcastle University), Doug Turnbull (Medical Research Council/Noel Murphy) and Susan Golombok.

28 | Wellcome NEWS Summer 2012 | 29
nucleus), the idea is to remove the nuclear genetic material from a healthy donor egg (keeping the donor mtDNA) and replace it with the nuclear genetic material from the affected couple’s embryo.
The resulting child would still derive half its genes from the mother and half from the father, but would carry the healthy mtDNA of the donor rather than the biological mother.
Turnbull’s work with Mary Herbert, from the renowned Newcastle Fertility Centre, has pioneered research in this area. They have shown, using eggs and embryos unsuitable for IVF, that it works in principle.1 A donor egg can have its nuclear genetic material removed and replaced with the nuclear genetic material from another fertilised egg, and the embryo can develop normally in the lab (before being destroyed, as required by law). The technique has not been without controversy: the revelation two years ago that scientists were studying PNT led to headlines about the ‘three-parent embryo’ with its biological mother and father, and its additional ‘mitochondrial mum’.
But the law has to change if the technique is ever going to benefit patients. In a legal proviso originally intended to prevent the unethical use of reproductive technologies – such as designer babies or human cloning – the
Human Fertilisation and Embryology Act 2008 does not allow the implantation of an embryo whose nuclear DNA or mitochondrial DNA has been altered. Last year, the Human Fertilisation and Embryology Authority (HFEA) stated that the technique deserved backing. The Department of Health has asked the HFEA to seek the public’s views on the possible use of this technique for treatment. Working with Sciencewise, the HFEA will begin the consultation later this year. Another technique for transplanting mitochondria technique also being studied by the Newcastle team and other groups is metaphase spindle transfer, which is essentially the same as PNT except that fertilisation occurs after, rather than before, transfer of the nuclear genetic material.
Ethics and genetics of parenthoodThe Nuffield Council on Bioethics ran a recent consultation about the ethical issues raised by these techniques, and its findings should be released shortly.
As well as the obvious safety considerations about minimising harm to both mother and child, this method does not just manipulate the child’s mtDNA but – if the child is a girl – could also alter the mtDNA of all her descendants. The long-term effects of altering the germline in this way are unknown, although evidence in mice indicates no ill-effects on subsequent generations. If a girl is born through PNT, then scientists may be placed in the extraordinary position of having to monitor her descendants.
The psychological welfare of children born through PNT is also a consideration. But Professor Susan Golombok, who directs the Centre for Family Research at the university of Cambridge, and who has conducted extensive research on the welfare of IVF children, does not foresee a big ethical battle ahead.
Golombok says: “Whether you believe a PNT child has three parents depends on how you define ‘parent’. We already have children whom we can
Some people have no symptoms, while some patients die within the first 48 hours of life”

28 | Wellcome NEWS Summer 2012 | 29
Far left: Jessica, Karl and Bella Williams. Peter Stubbs PhotographyNear left: Mitochondria (in orange) in a pancreas cell. University of Edinburgh/Wellcome Images
describe as having five parents: the egg donor, the sperm donor, the surrogate mother and the couple that brings the child up.” While many children conceived using donor sperm or a donor egg want to meet their biological parents, she says, this tends to be motivated by curiosity rather than the desire for a parent–child relationship.
“They often just want to see what the donors look like,” she adds. “But then again, some donor-conceived children show no interest at all in finding their biological parents when they grow up. For these individuals, the fact that they are donor-conceived is just not central to their identity. In fact, I suspect that PNT children really won’t regard themselves as having three parents, because the amount of mtDNA compared to nuclear DNA is so tiny” – mtDNA has 37 genes in total, compared with around 23 000 in nuclear DNA.
Turnbull and colleagues are hopeful that the public – and politicians, who will have to approve – will get behind the use of the new technique in the clinic, something they hope will be possible within the next five years: “I think if the public is informed they will feel positively towards it. We have to convey the seriousness of these diseases and why we want to prevent them in future.”
Giving Bella the best careBella, who is a little chubbier than usual because of the steroids she is taking for an infection, is lying on her play mat and has just rolled from her side onto her front. She is unlikely to ever develop the muscle strength to roll from back to front. Jessica says she would sign up for PNT tomorrow if it helped her and Karl to have healthy children. “We definitely want siblings for Bella. We don’t want this disease to define our family; if Bella has a short life, we want it to be a normal one.”
Leigh syndrome has been ruled out; the couple are awaiting the results of further genetic tests. Some light amid the gloom has been provided by the Royal Hampshire County Hospital in Winchester, which Jessica praises for its care of Bella, and by the Lily Foundation, a charity that provides information about MID, raises money for research and encourages affected families to support each other. The mothers Skype each other; some are already bereaved, while others, like Jessica, live from day to day, constantly watchful for physical changes.
“That’s what makes this disease so horrendous: you never know how it’s going to manifest itself,” says Jessica, who apologises (needlessly) for briefly losing her composure. “Bella recently went into hospital crying, and now she
doesn’t cry. The hardest thing about trying to be a strong mum for Bella is watching my four-month-old baby being so ill and yet being helpless to make her better.”
Reference
1 Craven L et al. Pronuclear transfer in human embryos to prevent transmission of mitochondrial DNA disease. Nature 2010;465:82–5.
Find out more
• The Lily Foundation: www.thelilyfoundation.org.uk
• Climb (National Information Centre for Metabolic Diseases): www.climb.org.uk
• Muscular Dystrophy Campaign: www.muscular-dystrophy.org
• Find out about the symptoms of mitochondrial disease and more about the research at the Wellcome Trust Centre for Mitochondrial Research in the full-length version of this article at www.wellcome.ac.uk/news.
30 | Wellcome NEWS Summer 2012 | 31
Whether it’s collecting scrap metal, living with rationing or the mobilisation of women into the factories, fields and airbases, the ‘War effort’ of World War II is familiar to most of us. Now, in The Pursuit of the Nazi Mind: Hitler, Hess, and the analysts, Professor Daniel Pick from Birkbeck, university of London, explores a neglected part of this effort: the Allies’ intellectual endeavours to track the Nazi state of mind during and after the War.
“The book is essentially an exploration of the way psychoanalysis, psychology and psychiatry were used in the War by the British and the Americans,” says Pick. Indeed, just as, albeit on a larger scale, scientists and mathematicians came together to work on decoding at Bletchley Park or on the atomic bomb in the Manhattan Project, Pick tells how anthropologists, political scientists, economists, historians, psychoanalysts and psychologists were united in a joint urgent mission to understand more about Nazism.
Pick provides a broad look at the role of the ‘psy’ professions but also focuses on two case studies in this book. One of these is the British Army’s attempts to understand the behaviour and mental state of the Deputy Führer, Rudolf Hess. In 1941 – apparently on a peace mission – Hess flew from Germany to Scotland, where he was captured and imprisoned, before being moved to England (spending a brief spell in the Tower of London) and Wales.
“There was some idea that you glean things from Hess that could be of interest from an intelligence point of view, but gradually his diplomatic significance decreases,” says Pick. “His
importance as another kind of case study increased, though, as he became one of a number of many German prisoners who were also being studied in psychological terms.”
Analytical approachPick’s broad approach, based around the ‘psy’ professions, reflects his own varied training. He followed an English literature degree with a PhD in history and many years of teaching, and now works in what he describes as “cultural and intellectual history”. He has also trained as a psychoanalyst at the British Psychoanalytical Society.
“It was partly a personal wish to explore the field more, to have analysis
myself, of course, and – eventually – to have direct experience of working as a clinician, but also I thought that psychoanalysis could give a different perspective that would enrich the way I understand research and the historical past.”
Does he expect any criticism of his approach? “There’s been a lot of debate amongst historians about whether psychoanalysis and psychology ought to have a place in historical methodology, whether it’s good or bad practice to draw on the insights about the unconscious minds and unconscious fantasy when thinking about the historical past.”
Work that has applied psychoanalysis to the past has often been seen (sometimes correctly) to make certain oversimplifying assumptions, such as ignoring the cultural context, Pick explains. “I think, however, a lot of very diverse work got conflated into one thing. So, I wanted to show how the use of psychoanalysis developed historically, explore the variety of what was done and ask how
A new book by Professor Daniel Pick shines a light on a neglected aspect of the Allies’ work to win the War. Chrissie Giles meets him to find out more.
MEDICAL hISTORY
PROFESSOR DANIEL PICK
ANALYSING THE NAZI MIND
Many of the things that were seen in an extreme form during the War go on being of acute concern now.”
Mat
chbo
x Vi
deo
30 | Wellcome NEWS Summer 2012 | 31
Win a copy!We have two copies of Daniel Pick’s book to give away. Just name the London street in which Freud lived in 1939 that now houses a museum bearing his name. Email your answer (one entry only per person) to [email protected] using the subject line ‘Freud competition’. Competition closes 17.00 BST, 30 July 2012, after which two entries will be randomly selected. The winner will be notified by email by 6 August 2012 and announced in a future issue of Wellcome News.
mindful the researchers in the War and its aftermath were of cultural difference, history and politics, as well as the life of the mind.”
What might we take from his book for the world today? “I think that the things the people were interested in during and after the War are not simply dead-and-buried issues. The concern with unconscious fantasies and how they are mobilised in politics remains a live issue in many ways today. Moreover, the use of ‘projection’ (for example, the denigration of out-groups into whom the unwanted aspects of humanity are put) and how an ‘us’ and ‘them’ gets created remain evident enough in a host of other contexts,” says Pick.
While some of the terminology has changed, the fundamental psychosocial and psychopolitical problems with which the Allied analysts grappled remain, he adds.
“Many of the things that were seen in an extreme form during the War go on being of acute concern now. For example, people talk about a ‘dog-whistle’ effect in politics, which appeals to people’s most base feelings. Also, there might be something in which the leaders themselves get pulled along unconsciously in megalomaniac fantasies or omnipotent delusions.”
Past and presentWhile interested in affinities between past and present, Pick is quick to emphasise that it would be wrong to imply that the moral behaviour of all modern states is equally abhorrent, or to imply that the world of Nazi concentration camps should be equated with more recent state-sanctioned atrocities. Each case needs to be understood in its historical context. “Nonetheless,” he adds, “some of the processes that might have led members of the Nazi party to comply with some of the most horrendous crimes against humanity are not things that ceased to exist in 1945.”
• The Pursuit of the Nazi Mind: Hitler, Hess, and the analysts by Daniel Pick was published by Oxford University Press in early June.
• Daniel Pick is among the speakers at the ‘Psychoanalysis in the Age of Totalitarianism’ conference at Wellcome Collection, 21–22 September 2012.
Above: Rudolf Hess as a child. Oxford University Press
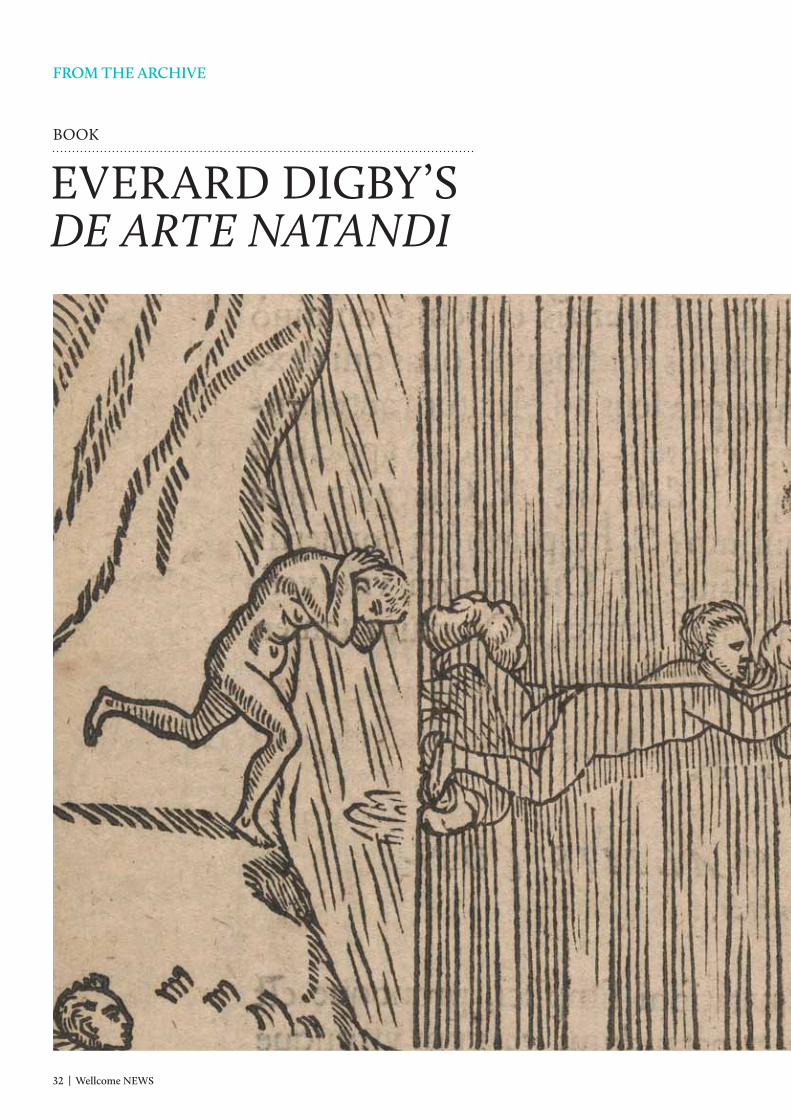
32 | Wellcome NEWS Summer 2012 | 33
BOOK
EVERARD DIGBY’S DE ARTE NATANDI
fROM ThE ARChIVE
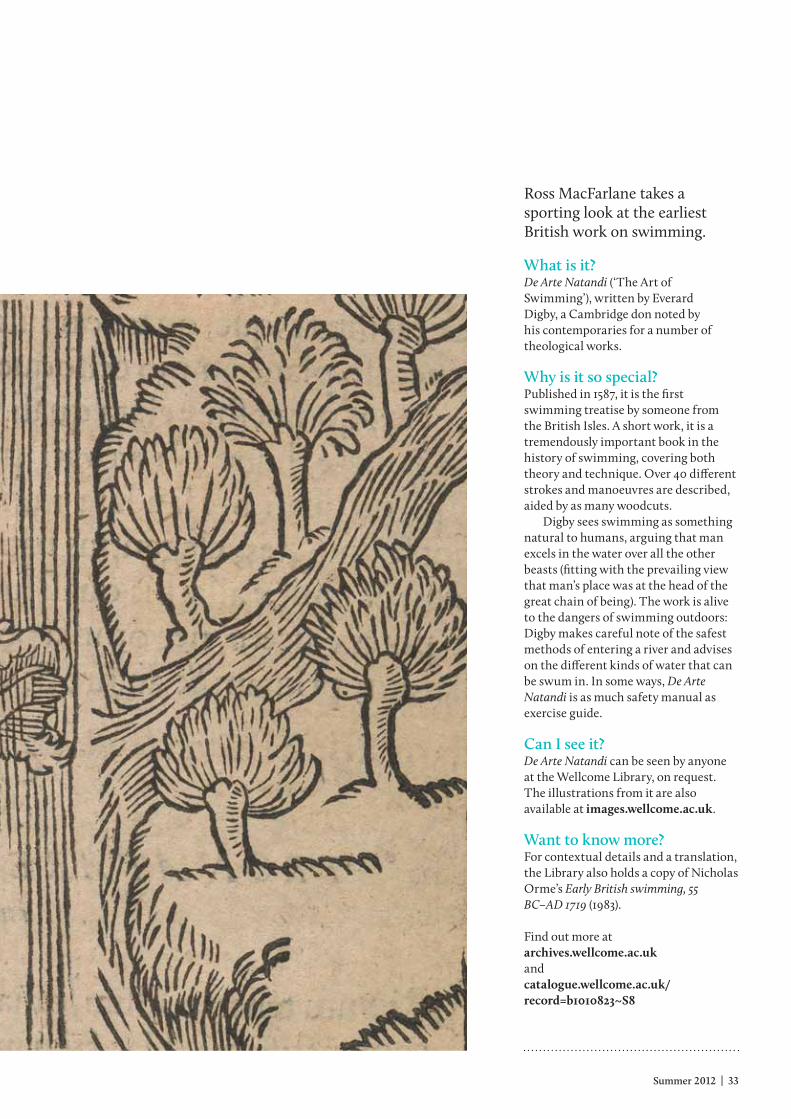
32 | Wellcome NEWS Summer 2012 | 33
Ross MacFarlane takes a sporting look at the earliest British work on swimming.
What is it?De Arte Natandi (‘The Art of Swimming’), written by Everard Digby, a Cambridge don noted by his contemporaries for a number of theological works.
Why is it so special?Published in 1587, it is the first swimming treatise by someone from the British Isles. A short work, it is a tremendously important book in the history of swimming, covering both theory and technique. Over 40 different strokes and manoeuvres are described, aided by as many woodcuts.
Digby sees swimming as something natural to humans, arguing that man excels in the water over all the other beasts (fitting with the prevailing view that man’s place was at the head of the great chain of being). The work is alive to the dangers of swimming outdoors: Digby makes careful note of the safest methods of entering a river and advises on the different kinds of water that can be swum in. In some ways, De Arte Natandi is as much safety manual as exercise guide.
Can I see it?De Arte Natandi can be seen by anyone at the Wellcome Library, on request. The illustrations from it are also available at images.wellcome.ac.uk.
Want to know more?For contextual details and a translation, the Library also holds a copy of Nicholas Orme’s Early British swimming, 55 BC–AD 1719 (1983).
Find out more atarchives.wellcome.ac.uk andcatalogue.wellcome.ac.uk/record=b1010823~S8
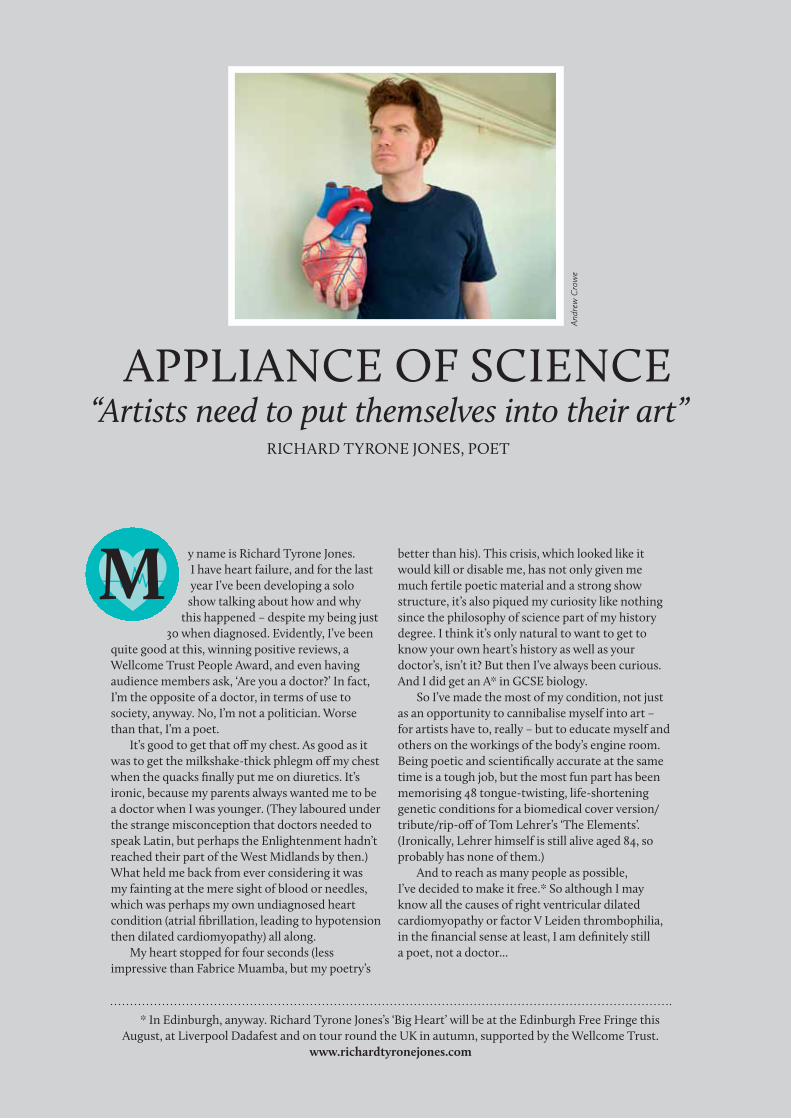
34 | Wellcome NEWS Summer 2012 | 35
y name is Richard Tyrone Jones. I have heart failure, and for the last year I’ve been developing a solo show talking about how and why
this happened – despite my being just 30 when diagnosed. Evidently, I’ve been
quite good at this, winning positive reviews, a Wellcome Trust People Award, and even having audience members ask, ‘Are you a doctor?’ In fact, I’m the opposite of a doctor, in terms of use to society, anyway. No, I’m not a politician. Worse than that, I’m a poet.
It’s good to get that off my chest. As good as it was to get the milkshake-thick phlegm off my chest when the quacks finally put me on diuretics. It’s ironic, because my parents always wanted me to be a doctor when I was younger. (They laboured under the strange misconception that doctors needed to speak Latin, but perhaps the Enlightenment hadn’t reached their part of the West Midlands by then.) What held me back from ever considering it was my fainting at the mere sight of blood or needles, which was perhaps my own undiagnosed heart condition (atrial fibrillation, leading to hypotension then dilated cardiomyopathy) all along.
My heart stopped for four seconds (less impressive than Fabrice Muamba, but my poetry’s
RICHARD TYRONE JONES, POET
“Artists need to put themselves into their art”APPLIANCE OF SCIENCE
better than his). This crisis, which looked like it would kill or disable me, has not only given me much fertile poetic material and a strong show structure, it’s also piqued my curiosity like nothing since the philosophy of science part of my history degree. I think it’s only natural to want to get to know your own heart’s history as well as your doctor’s, isn’t it? But then I’ve always been curious. And I did get an A* in GCSE biology.
So I’ve made the most of my condition, not just as an opportunity to cannibalise myself into art – for artists have to, really – but to educate myself and others on the workings of the body’s engine room. Being poetic and scientifically accurate at the same time is a tough job, but the most fun part has been memorising 48 tongue-twisting, life-shortening genetic conditions for a biomedical cover version/tribute/rip-off of Tom Lehrer’s ‘The Elements’. (Ironically, Lehrer himself is still alive aged 84, so probably has none of them.)
And to reach as many people as possible, I’ve decided to make it free.* So although I may know all the causes of right ventricular dilated cardiomyopathy or factor V Leiden thrombophilia, in the financial sense at least, I am definitely still a poet, not a doctor...
* In Edinburgh, anyway. Richard Tyrone Jones’s ‘Big Heart’ will be at the Edinburgh Free Fringe this August, at Liverpool Dadafest and on tour round the uK in autumn, supported by the Wellcome Trust.
www.richardtyronejones.com
Andr
ew C
row
e
34 | Wellcome NEWS Summer 2012 | 35
DIARYCourses, conferences and workshopsWellcome Trust Genome Campus, Hinxton, unless otherwise specified. For more, see www.wellcome.ac.uk/advancedcourses and www.wellcome.ac.uk/conferences
Genome Informatics 2012 Conference, Robinson College, Cambridge, 6–9 September
The Genomics of Common Diseases 2012 Conference, Bolger Center, Potomac, MD, uSA, 19–22 September
Infectious Disease Genomics and Global Health Conference, Churchill College, Cambridge, 1–3 October
Epigenomics of Common Diseases Conference, Johns Hopkins university, Baltimore, uSA, 12–15 October
Proteomics Bioinformatics Workshop, 5–9 November
Genetic Manipulation of ES Cells Course, 5–18 November
Rat Genomics and Models 2012 Conference, Churchill College, Cambridge, 3–6 December
Working with the Human Genome Sequence Workshop, Oxford university Clinical Research unit, Ho Chi Minh City, Vietnam, 3–6 December
Genomics and Clinical Microbiology Course, 20–25 January 2013
Complex Disease Genetics for Clinicians Workshop, 24–25 January 2013
Biomarkers for Brain Disorders: Challenges and opportunities Conference, Churchill College, Cambridge, 3–6 February 2013
Applied Bioinformatics and Public Health Microbiology Conference, Churchill College, Cambridge, 15–17 May 2013
Wellcome Collection events and exhibitions Euston Road, London. www.wellcomecollection.org Wellcome Image Awards 2012 Display, until 31 December
Superhuman Exhibition, 19 July–16 October
Medicine Man and Medicine Now Permanent exhibitions
Event listings See website for details
IN YOuR NEXT ISSuEThe latest news and features from the Wellcome Trust, with updates on funding, research and more.
Wellcome Trust Genome Campus
1–3 October 2012
This Wellcome Trust Scientific Conference focuses on the application of genomic technologies to problems of infectious disease in a global health context.
Abstract deadline: 25 July Registration deadline: 3 September
Full details at:www.wellcome.ac.uk/conferences
Infectious Disease Genomics and Global Health

www.wellcomecollection.org/superhuman | A free destination for the incurably curious
TUESDAY–SUNDAY (UNTIL 18.00), CLOSED MONDAYLATE-NIGHT THURSDAY (UNTIL 22.00)183 EUSTON ROAD, LONDON NW1 EUSTON, EUSTON SqUARE
Image: Still from CREMASTER 3: The Third Degree by Matthew Barney (2002). Courtesy Gladstone Gallery, New York and Brussels. Wellcome Collection is part of the Wellcome Trust. The Wellcome Trust is a charity registered in England and Wales, no. 210183. Its sole trustee is The Wellcome Trust Limited, a company registered in England and Wales, no. 2711000 (whose registered office is at 215 Euston Road, London NW1 2BE, UK). PU-5344.6/06-2012/MC