who drug informationapps.who.int/medicinedocs/documents/s23256en/s23256en.pdf · who drug...
TRANSCRIPT

151
WHO Drug Information Vol. 31, No. 2, 2017
Contents
Medicines regulation153 Regulating medicine manufacturers:
is an on-site inspection the only option?
158 Placebo and drug kits in clinical trial design
Quality monitoring162 Survey of the quality of selected
antiretroviral medicines circulating in five African countries
Safety news166 Safety warnings
Dulaglutide;Darbepoetin alfa ;Caspofungin ;Pneumococcal vaccine ;Pembrolizumab ;Vemurafenib ;Denosumab;Gadolinium contrast agents
168 RestrictionsCodeine, tramadol
168 To be removed from the marketOxymorphone injection
169 New guidelinesVancomycin ;Opioids
170 Known risksEluxadoline ;Canagliflozin ;Certain hepatitis C medicines ;Bosutinib Severe skin reactions ;Ponatinib; Idelalisib ;Hypnotics and anxiolytics ;Anaesthetics and sedatives in young children; Iodinated contrast media
172 Unchanged recommendationsSelexipag ; Factor VIII-containing medicines ;Mefloquine ;Docetaxel
173 Reviews startedDirect-acting antivirals;Daclizumab; Fingolimod ;Valproate
174 Non-compliance with good practicesMicro Therapeutic Research Labs ;Mylan Laboratories;Qinhuangdao Zizhu; FDA warning letters; TGA reminder on good data management requirements
176 Falsified product alertsMeningococcal ACWY vaccine in West Africa;Hepatitis C medicine in Germany
Regulatory news177 Pre-market assessment
Assessment of generics in China;New fast-track pathway in India ;Australian orphan drug programme;EU Priority medicines scheme;EU medical devices regulation
179 Adverse events reportingPharmacovigilance in Europe;Adverse events of illicit drugs in UK
180 SupplyGMP for compounded medicines;Reporting of shortages in Canada;Dispensing categories in Switzerland
180 Antimicrobial resistanceIndia national action plan;New investments in Canada; Tripartite alignment on requirements for antibacterials
181 Collaboration EU and African regulators meet;Report on EMA–FDA assessment pilot; Swiss–Austrian agreement;MedDRA expands global reach;EMA and academia
183 Transparency and databases Publication of clinical study reports; India builds centralized regulatory portal; Ingredients catalogue in Australia
184 Under discussion
186 ApprovedNaldemedine ; Cerliponase alfa ; Nonacog beta pegol ; Dupilumab ; Abaloparatide ; Inotuzumab ozogamicin ; Durvalumab ; Midostaurin ; Ribociclib ; Brigatinib ; Niraparib ; Ocrelizumab ; Sarilumab ; Avelumab ; Autologous chondrocyte suspension ; Edaravone ; Valbenazine ; Deutetrabenazine ; Triple combination for COPD; Cenegermin
190 BiosimilarsInsulin lispro; Rituximab; Etanercept; Infliximab
191 Extensions of indicationsMaraviroc ; Sofosbuvir, ledipasvir and sofosbuvir ; Pembrolizumab ; Regorafenib ; Tocilizumab ; Ivacaftor
192 Early accessGlecaprevir/pibrentasvir
192 EU rulingParacetamol/ibuprofen fixed-dose combination
Continued
WHO Drug Information
152
WHO Drug Information Vol. 31, No. 2, 2017
Publications and events193 Access to medical products
Fair Pricing Forum; Information guide on biosimilars;WHO to pilot prequalification of biosimilars;Updated Essential Medicines List ;MPP licence for investigational hepatitis C medicine;Regulatory reforms in Mexico; Access to Vaccines Index 2017;Reporting of clinical trial results
196 Safety evaluation and monitoringConfirmatory clinical studies lacking; Importance of monitoring new drugs
196 Medicines supply and useNew industry alliance to curb antimicrobial resistance;Antibiotics consumption in eastern Europe and central Asia;Off-label use of medicines in Europe;Combating medication errors; Toolkit to protect supply chains
198 Disease updatesPoliomyelitis ;Depression ;Neglected tropical diseases ;Malaria ;Hepatitis ;Ebola
200 Upcoming eventsIreland to host 18th ICDRA; Joint manufacturers meeting
201 WHO newsSeventieth World Health Assembly;New WHO Director-General elected;Medicines prequalification updates
Consultation documents202 The International Pharmacopoeia 202 Mebendazole tablets206 Capreomycin sulfate 210 Capreomycin for injection 214 Transition from microbiological to
physicochemical assays in monographs on capreomycin active pharmaceutical ingredients and products
220 Atenolol 224 Capillary electrophoresis235 WHO Medicines quality guidelines ▪ Good practices for desk assessment ▪ Considerations for requesting analysis of
medicines samples▪ Model certificate of analysis▪ “SRA” collaborative procedure▪ Good herbal processing practices
ATC/DDD classification236 ATC/DDD classification (temporary)238 ATC/DDD classification (final)
International Nonproprietary Names (INN)241 Proposed INN: List 117
Continued
Abbreviations and websitesCHMP Committee for Medicinal Products for Human Use (EMA)EMA European Medicines Agency (www.ema.europa.eu)EU European UnionFDA U.S. Food and Drug Administration (www.fda.gov)Health Canada Federal department responsible for health product regulation in Canada (www.hc-sc.gc.ca)IGDRP International Generic Drug Regulators Programme (https://www.igdrp.com)MHLW Ministry of Health, Labour and Welfare, JapanMHRA Medicines and Healthcare Products Regulatory Agency, United Kingdom
(www.mhra.gov.uk)Medsafe New Zealand Medicines and Medical Devices Safety Authority (www.medsafe.govt.nz)PRAC Pharmacovigilance Risk Assessment Committee (EMA)PMDA Pharmaceuticals and Medical Devices Agency, Japan (www.pmda.go.jp/english/index.htm)Swissmedic Swiss Agency for Therapeutic Products (www.swissmedic.ch)TGA Therapeutic Goods Administration, Australia (www.tga.gov.au)U.S. United States of America WHO World Health Organization (www.who.int)WHO EMP WHO Essential medicines and health products (www.who.int/medicines/en/)WHO PQT WHO Prequalification team (https://extranet.who.int/prequal/)
Note:The online version of this issue (freely available at www.who.int/medicines/publications/druginformation) has direct clickable hyperlinks to the documents and websites referenced.
153
WHO Drug Information Vol. 31, No. 2, 2017
Medicines regulationRegulating medicine manufacturers: is an
on-site inspection the only option?
The Australian approach to meeting inspection demands
On-site inspections of manufacturing and testing sites for medicines are resource-intensive for both regulators and manufacturers, especially as an increasing number of sites are located outside regulatory authorities’ territories. To maximize the impact of limited resources, it is therefore good regulatory practice to leverage available evidence from other agencies as part of a risk-based inspection planning process.
The Australian Department of Health’s Therapeutic Goods Administration (TGA) has been using a risk- and reliance-based approach in inspection planning for some time. This article describes the TGA’s pathways for granting good manufacturing practice (GMP) clearance.
BackgroundA cornerstone of effective medicine regulation is ensuring that the medicines available within a market meet appropriate quality standards. To this end, a national regulatory authority (NRA) will assess product quality data during pre-market assessment. Generally, this involves assessment of quality data provided as part of the application dossier (1) by the applicant, and an onsite inspection of the product manufacturer against compliance with the applicable Good Manufacturing Practice (GMP) standards, such as those developed by WHO and used in its Prequalification Programme (2,3) or those of the Pharmaceutical Inspection Convention/
Pharmaceuticals Inspection Cooperation Scheme (PIC/S).(4)
Where the manufacturer has been previously inspected and approved by the NRA, an onsite assessment may be avoided if the manufacturing steps are the same. If the product is approved for supply, the NRA monitors the manufacturer’s compliance with applicable GMP standards via regular inspections, either announced or unannounced.
A key objective of a GMP inspections programme is to provide the NRA with a proactive mechanism for identifying and preventing quality related medicine safety risks. Once a manufacturer is approved for supplying medicines to the market, re-inspections are usually conducted
Authors:Hongxia Jin, Nicola Carr, Harry RothenfluhManufacturing Quality Branch, Therapeutic Goods Administration, Australian Department of Health

Medicines regulation WHO Drug Information Vol. 31, No. 2, 2017
154
within a risk framework that takes into account product and process risks and manufacturer compliance history.(e.g. 5,6) The objective should be to conduct more frequent inspections of manufacturers with a higher risk profile. In contrast, where a manufacturer has demonstrated a high level of voluntary compliance with GMP standards over time, re-inspections could be conducted on a less frequent basis.
Challenges in meeting demand for GMP inspectionsMaintaining an effective GMP inspections programme can be challenging for many reasons, including the following:
Availability of appropriately trained and qualified staffGiven the technical nature of the work involved in planning, conducting and closing out GMP inspections, GMP inspectors must have appropriate academic qualifications and professional experience.
Factors that may impact on an NRA’s ability to build and maintain a team of appropriately experienced GMP inspectors include the presence of a domestic manufacturing industry, tertiary education institutions that offer suitable courses and the ability of a regulator to offer salaries that are competitive with those offered by industry.
Inspecting international manufacturers Depending on the size and diversity of the domestic pharmaceutical market, NRAs may need to regulate a large number of domestic and/or overseas pharmaceutical manufacturers. In some countries, including Australia, there are many more international manufacturers than domestic manufacturers supplying the market.
Challenges associated with inspecting international manufacturers include travel costs and logistics, visa and other entry requirements, language barriers and inspector health and security risks.
Demand for inspections outstrips capacityAs the pharmaceutical supply chain becomes more complicated, the demand for GMP inspections can exceed the capacity of an NRA to meet that demand. In particular, with the emergence of contract manufacturing, multiple manufacturing sites may be associated with a single product. This can be mitigated to some extent by relying on the supplier qualification processes of the finished dosage form manufacturer.
Nevertheless, with increasing investment by international pharmaceutical companies in emerging medicine manufacturing economies, it is likely that the demand for GMP inspections will increase over time.
Consequences of not meeting demand for GMP inspections The consequences of insufficient resources being available to meet the demand for GMP inspections include:
Delayed access to new medicines by patientsDelays in inspecting new manufacturers, or new manufacturing steps conducted by previously approved manufacturers, may delay product approvals. This may delay access of patients to new or essential medicines, which in turn may adversely impact on public health programmes.
Reduced ability of the NRA to identify and manage medicine quality risksFailure to conduct GMP inspections within risk-based re-inspection timeframes reduces
Australian approach to meeting inspection demands

155
WHO Drug Information Vol. 31, No. 2, 2017 Medicines regulation
the NRA’s ability to identify manufacturing failures that may affect the safety profile of medicines. This increases the risk that patients may be exposed to medicines that do not meet applicable specifications and quality standards. Such medicines pose a risk to consumers as they may not achieve the desired health outcomes. Further, in the case of medicines used to treat infectious diseases, substandard medicines may promote the emergence of resistant strains of the infectious agent.
Lengthy approval times may deter investments and importsDelays in approval times may be a disincentive for foreign investors to build manufacturing capacity in target countries. It may also be a disincentive for local distributors to apply for permits to import and supply medicines made by international manufacturers. This in turn may limit access to medicines that patients need.
Meeting the challenge: The Australian approachThe Australian Department of Health’s TGA is responsible for regulating the supply, import, export, manufacturing and advertising of therapeutic goods in Australia.
Under Australian law an applicant seeking pre-market approval of a medicinal product must supply evidence demonstrating that each manufacturer involved in the manufacture of the product has acceptable manufacturing and quality control procedures in place. It is also a condition of ongoing product approval that such evidence is supplied on request.
The TGA conducts GMP inspections of all Australian manufacturers of medicines. For manufacturers located outside of Australia,
the applicant must obtain a TGA GMP clearance for each site, that specifies which manufacturing steps for the required dosage forms can be undertaken.
TGA conducts 80–120 inspections of international manufacturers and about 150–200 inspections of Australian manufacturers every year. However, the Agency does not have the resources to maintain a regular inspection programme for every international manufacturer that supplies API and/or finished product to the Australian market. The TGA has developed a risk-based desktop assessment process that relies on information from recognized regulators. This process has reduced the number of overseas on-site inspections to be performed.(7)
There are two types of desk top assessments that TGA conducts to make a decision about whether to issue a TGA GMP clearance to the international manufacturer:
Mutual Recognition Agreement PathwayThe TGA accepts GMP Certificates issued by a country with which Australia has a Mutual Recognition Agreement (MRA), based on an inspection within their own borders. Evaluation under the MRA pathway includes an assessment of a current GMP Certificate to identify the manufacturing site, to ensure an equivalent GMP standard is applied, and to verify that the scope (manufacturing steps and dosage forms) is relevant to the product to be supplied in Australia.
Compliance Verification PathwayTGA may also accept evidence from the following:• An MRA regulatory authority, for
inspections performed outside their own borders; or
• the U. S. FDA, for inspections performed inside or outside its own border; or
Australian approach to meeting inspection demands

Medicines regulation WHO Drug Information Vol. 31, No. 2, 2017
156
Australian approach to meeting inspection demands
• a recognized regulatory authority of a country with which Australia does not have an MRA (e.g. PIC/S members1), for inspections performed within their own borders.
This pathway requires additional data to be supplied by the applicant (Table 1). A Compliance Verification assessment includes a detailed assessment of a recent GMP certificate and an inspection report prepared by an overseas regulatory agency recognized by the TGA, together with supporting manufacturing documentation supplied by the applicant or international manufacturer. The extent of the assessment
1 https://www.picscheme.org/en/members
process depends on the regulatory evidence required and increases with product risk and the complexity of manufacture.
The MRA and Compliance Verification assessments may result in a TGA decision to:• issue a GMP Clearance, valid for a
specified period, based on the date of the last on-site inspection performed by the recognized regulator;
• issue a GMP Clearance, valid for a specified period but with one or more conditions; or
• not issue a GMP Clearance where the evidence does not support the scope of the GMP Clearance application.
Table 1 – Evidence required for Compliance Verification Assessments
All non-sterile dosage forms & APIs
Sterile and Biotech APIs and Sterile Dosage forms
Contract Testing Laboratories and Contract Sterilizers
Current GMP Certificate Current GMP Certificate Current GMP Certificate
A list of all regulatory inspections conducted within the past 3 years, and a copy of the most recent inspection report
A list of all regulatory inspections conducted within the past 3 years, and a copy of the most recent inspection report
A list of all regulatory inspections conducted within the past 3 years, and a copy of the most recent inspection report
Details of any regulatory actions in the past 3 years
Details of any regulatory actions in the past 3 years
Details of any regulatory actions in the past 3 years
Site Master File, Quality Manual or equivalent
Site Master File, Quality Manual or equivalent
Quality Manual / Laboratory Manual or equivalent
GMP agreement between the sponsor and the manufacturer(a)
GMP agreement between the sponsor and the manufacturer(a)
GMP agreement between the sponsor and the contract test laboratory or sterilizer(b)
List of products intended for supply in Australia
List of products intended for supply in Australia
A list of tests a laboratory is authorized to perform
Copy of the procedures for release for supply of products included in the Clearance application(a)
Copy of the procedures for release for supply of products included in the Clearance application
For botanical ingredients, evidence that authenticated standard reference materials are used
Validation Master Plan
Latest Product Quality Review(a) not required unless requested(b) or principal manufacturer and laboratory/sterilizer

157
WHO Drug Information Vol. 31, No. 2, 2017 Medicines regulation
TGA currently has MRA (or equivalent arrangements) with the European Union and several other jurisdictions covering 29 countries, and recognizes evidence from an additional 17 regulatory authorities.
Where there is no suitable evidence available from a recognized regulator to support a GMP Clearance application, the TGA will perform an onsite inspection of the international manufacturing site. The TGA always reserves the right to inspect an international manufacturing site regardless of what other evidence is available, particularly if issues have been identified during the compliance verification assessment or if there are concerns about the site’s GMP compliance.
ConclusionsThe TGA’s GMP clearance system was created in the early 2000s to facilitate the efficient and effective management of the Agency’s regulatory compliance programmes and reduce the regulatory burden on industry. The widespread use of GMP clearances has significantly reduced the number of overseas TGA inspections required. The Agency is also undertaking an increasing number of joint inspections with other regulators and is contributing to the development of information-sharing mechanisms through the International Coalition of Medicines Regulatory Authorities (ICMRA2).(8) These initiatives are consistent with the principle adopted by the Australian Government that “if a system, service or product has been adopted under a trusted international standard or risk assessment, no additional requirements should be imposed for approval in Australia,
2 http://www.icmra.info
unless it can be demonstrated that there is a good reason to do so”.(9) This principle of regulatory reliance is today more relevant than ever.
References1 ICH Harmonised tripartite guideline. The
Common Technical Document for the registration of pharmaceuticals for human use: Quality – M4Q(R1). September 2002.
2 WHO Good Manufacturing Practices for Pharmaceutical Products: Main Principles. Annex 2. In: WHO Technical Report Series 986. Geneva: WHO, 2014.
3 WHO good manufacturing practices for active pharmaceutical ingredients. Annex 2. In: WHO Technical Report Series 957. Geneva: WHO, 2010.
4 PIC/S GMP Guide. PE 009-13. 1 January 2017. Available at: www.picscheme.org/en/publications?tri=gmp; accessed 19 May 2017.
5 PIC/S. A recommended model for risk-based inspection planning in the GMP environment. PI 037-1. 1 January 2012.
6 TGA. Manufacturer inspections - an overview [webpage]. Available at: www.tga.gov.au/manufacturer-inspections-overview, accessed 19 May 2017.
7 TGA. Australian Regulatory Guidelines. Good Manufacturing Practice (GMP) clearance for overseas manufacturers.
8 Trends in Australian and international regulation and regulatory cooperation. Presentation by John Skerritt at the ACRS Scientific Congress, Canberra, Australia, 10-11 August 2016. Available at: https://www.tga.gov.au/sites/default/files/presentation-trends-in-australian-and-international-regulation-and-regulatory-cooperation.pdf.
9 Australian Government. Cutting red tape. International Standards and Risk Assessments [webpage]. Available at: https://www.cuttingredtape.gov.au/resources/international-standards-and-risk-assessments, accessed 25 May 2017. å
Australian approach to meeting inspection demands

Medicines regulation WHO Drug Information Vol. 31, No. 2, 2017
158
Placebo and drug kits in clinical trial design
New and improved medicinal products are continuously needed throughout the world to prevent and treat diseases. Good quality clinical trials are key in bringing new safe and effective medicines to patients.
Some information is outlined below on specific aspects of conducting clinical studies, namely the use of placebo as a control intervention and the use of drug kits for effective blinding of trials.
IntroductionBefore novel medicinal products are introduced into widespread use, they must be assessed in clinical trials. Randomized controlled trials (RCTs) are often considered the gold standard in this regard, although other study designs can also yield valid research results. Clinical trials should be designed in such a way that the effects of the experimental intervention are compared with those of a control intervention. In a controlled trial, the subjects in the study and control group should be drawn from the same population, and should preferably be assigned to the groups by randomization to remove bias in the allocation of participants. Where feasible, clinical trials should be blinded, so that the subjects – and in double-blinded studies also the researchers – are unaware of who is receiving which intervention. This helps to avoid behaviour changes that may influence the study outcomes.(1)
Two questions are discussed below that commonly arise in developing and evaluating clinical trial designs, namely in what situations it is acceptable to use placebo in the control arm, and how to achieve effective blinding.
The use of placeboA placebo has been defined as “an inert substance or sham procedure that is provided to research participants with the aim of making it impossible for them, and usually the researchers themselves, to know who is receiving an active or inactive intervention.”(1)
Placebos typically consist of the ingredients employed in the medicinal product under study minus the active ingredient, making them inert. The inactive ingredients (excipients) employed in a pharmaceutical product must be “generally recognized as safe”1 for use in humans, otherwise a medicinal product would not be authorized for use.
In vaccine research, the term “placebo” is also applied to non-inert substances. In this context, an existing vaccine not studied in the trial is added to both the investigational and the control product in order to avoid giving an “empty” injection to the subjects in the control group. A disadvantage of this approach is that it complicates the
1 The U.S. Food, Drug, and Cosmetic Act makes provision for food additives to be shown to be “Generally Recognized As Safe” (GRAS) through scientific procedures. Similar approaches are used in other jurisdictions.
This article originates from a request for advice sent to the WHO Prequalification Team. We thank Dr Matthias Stahl for his technical input. The article outlines selected concepts as found in published literature. It should not be considered as WHO guidance on the subject.

159
WHO Drug Information Vol. 31, No. 2, 2017 Medicines regulation
evaluation of the safety and reactogenicity of the vaccine under study.(2)
As the risks associated with the placebo product are typically very low or non-existent, the use of placebos is generally uncontroversial where there is no established effective intervention for the issue being researched. Where an established effective intervention exists, on the other hand, the use of placebo often raises controversy among members of research ethics committees (RECs), regulators, and policy-makers. The CIOMS Guideline 5, Choice of control in clinical trials, advises as follows:“As a general rule, the research ethics committee must ensure that research participants in the control group of a trial of a diagnostic, therapeutic, or preventive intervention receive an established effective intervention.
Placebo may be used as a comparator without providing the established effective intervention to participants only if:• there are compelling scientific reasons for
using placebo; and • delaying or withholding the established
effective intervention will result in no more than a minor increase above minimal risk to the participant and risks are minimized, including through the use of effective mitigation procedures.”
Risks and benefits of other study interventions and procedures should be evaluated according to the criteria set out in Guideline 4 – Potential individual benefits and risks of research.”(1)
A WHO expert group has identified five situations when placebos may be acceptable in the context of vaccine trials despite the existence of an effective intervention, namely when the existing vaccine: (1) is not affordable or not accessible to the target population, (2) has not been proven effective
in the target population, (3) has been proven ineffective in the target population, (4) has an unknown or uncertain public health impact in the target population which is to be evaluated against a placebo; or (5) is not acceptable to target population (e.g. a vaccine containing porcine gelatine in populations that have religious restrictions on the consumption of pork). However, the risks and benefits of conducting a placebo-controlled design should always be weighed against those of alternative trial designs such as response-adaptive designs, observational studies, or historical comparisons.(1,2)
The use of placebo may require risk mitigation even if no established effective intervention exists. For example, in the Ebola vaccine trial conducted in Guinea the use of a placebo or an unrelated vaccine in the control group was deemed ethically unacceptable as it would leave vulnerable individuals unprotected against Ebola virus disease when a potentially effective investigational vaccine was available. Instead, vaccination of control subjects was delayed by 21 days, the minimal delay that would enable researchers to determine vaccine efficiency.(3)
The use of drug kits Specifically for researching new pharmaceuticals, clinical trials should preferably have a randomized double-blind design. Blinding can take place at several levels: it may apply to the researchers who assign subjects to groups, the subjects themselves, the health care workers who take care of patients in a study, and the researchers who record and assess the outcomes.(4)
A method of blinding clinical trials is the use of drug kits, in which the investigational or control product is packaged for distribution to investigational
Placebo and drug kits in clinical trial design

Medicines regulation WHO Drug Information Vol. 31, No. 2, 2017
160
sites. Each kit is labelled with a neutral ID, without indication of its content, enabling investigators to administer study or control drug to subjects in a blinded manner without the assistance of an unblinded pharmacist.(5) Each kit contains sufficient product for a extended period, typically two or three weeks,(6) although the quantity will vary depending on the study design.
The key component to the successful use of drug kits is the creation of a kit list, where kit IDs are randomly assigned to kit types (investigational or control). This kit list is used at the time of manufacture to label the kits, during shipping to track the kits, and during the study to assign kits to patients.(6)
Many trials involve multiple clinical sites. To avoid the need for an unblinded pharmacist at each site, use is often made of a randomization centre to randomize study subjects and manage the supply of drug kits i.e., track drug kit inventory at each site, ship kits to sites, and assign kits to patients. In this way, information on whether a kit contains test or control product does not accompany the kit but is available from the randomization centre.(6)
The coding used in creating the kit list and the distribution patterns and resupply methods employed are key factors in blinding a clinical trial. A good design should achieve a balance between kit efficiency and successful blinding. This can be illustrated by two simple scenarios. In a trial where each kit handed out to a subject triggers a replacement by a single kit of the same type, no kits are wasted but the researcher can deduce that the patients dosed with these two kits belong to the same study arm. In the opposite scenario the randomization centre would send two replacement kits (one active and one control) for each kit handed out to a patient, and would inactivate one of the two when
a kit is assigned to the next patient. This is successful blinding at the expense of wasting one kit per subject.(5)
An analogous approach to the “waste-one-kit” method could be used to blind a trial where the control subjects receive a delayed intervention, by scheduling additional visits in both groups. In the Ebola vaccine trial conducted in Guinea this was not possible due to operational challenges; instead, to reduce the risk of bias arising from behaviour changes that might follow vaccination, participants were informed that it is not known if the vaccine works, and that they must still take steps to avoid infection.(3)
In practice, the design of algorithms for coding and supplying blinded drug kits will take into account a range of factors specific to each study, such as any additional trial arms, kit inventory size, enrolment rate at the sites, and times between subject enrolments in relation to shipment time for replacement kits. Operational characteristics of different types of kit lists(6) and supply methods(5) have been discussed in published literature. A criterion has also been proposed for evaluating the strength of blinding in a clinical trial, even if the researcher has been unblinded to the contents of one or more kits. This is of interest because it is not uncommon for an investigator to be unblinded to a subject’s treatment assignment for safety reasons or from the subject’s adverse event or efficacy profile.(5)
ConclusionsWith today’s swift pace of product development in a globalized market, designing, assessing, and authorizing clinical trials can be challenging. Cooperation among regulators, ethics committees, and sponsors to reach consensus on key ethical
Placebo and drug kits in clinical trial design

161
WHO Drug Information Vol. 31, No. 2, 2017 Medicines regulation
and regulatory questions is essential, and has proved particularly valuable in situations of urgency and in low-resourced environments.(7)
Efficient conduct of the trials without unnecessary regulatory barriers is equally important. Excessively cumbersome regulations, for example on importation and dispensing of placebos for clinical trials, could delay access to effective and sometimes lifesaving medicines. WHO stands ready to assist countries in identifying well-balanced approaches for clinical trials, including those requiring the use of placebos.
Lastly, well-designed clinical trials must be complemented by reliable post-approval safety assessment mechanisms. Many new medicinal products are introduced early and/or exclusively into countries with limited pharmacovigilance capacities. New guidance has become available on safety surveillance of vaccines, proposing a structured process for evaluating whether significant knowledge gaps exist, whether passive safety surveillance is adequate, and if not, how active vaccine safety surveillance studies can be designed and implemented.(8)
References1 International Ethical Guidelines for Health-
Related Research Involving Humans, Fourth Edition. Geneva: Council for International Organizations of Medical Sciences; 2016.
2 WHO. Expert Consultation on the Use of Placebos in Vaccine Trials. Geneva; 2014.
3 The ring vaccination trial: a novel cluster randomised controlled trial design to evaluate vaccine efficacy and effectiveness during outbreaks, with special reference to Ebola. BMJ 2015;351:h3740.
4 Fathalla MF. A Practical Guide for Health Researchers. Cairo: WHO Regional Office for the Eastern Mediterranean; 2004.
5 Yu R, Coleman DA. Blinding Properties of Methods for Supplying Drug Kits to Investigational Sites. Contemporary Clinical Trials Communications. 2015;1:22-27.
6 Coleman DA, Yu R. The Other Randomization – Methods for Labeling Drug Kits. Contemporary Clinical Trials.2014;38(2):270-274. (Requires subscription)
7 The African Vaccine Regulatory Forum (AVAREF): A platform for collaboration in a public health emergency. WHO Drug Information 2015; 29(2):127-131.
8 CIOMS. Guide to Active Vaccine Safety Surveillance. Report of CIOMS Working Group on Vaccine Safety. Geneva: Council for International Organizations of Medical Sciences (CIOMS); 2017. Available at: www.cioms.ch/shop. å
Placebo and drug kits in clinical trial design

162
WHO Drug Information Vol. 31, No. 2, 2017
Quality monitoringSurvey of the quality of selected antiretroviral medicines
circulating in five African countries
This article presents an overview of the findings of a sample testing survey organized by WHO as part of its quality monitoring activities for medicines. The survey confirmed the positive impact of WHO prequalification in assuring the quality of antiretrovirals used in HIV treatment programmes of WHO Member States. A full report of the survey is in preparation.
IntroductionA quality survey was organized in 2015 and 2016 by the WHO Prequalification Team (WHO-PQT) in cooperation with the National Medicines Regulatory Authorities/ Ministries of Health in five countries in Sub-Saharan Africa. The objective of the survey was to assess the quality of selected antiretroviral medicines (ARVs) obtained at approved (authorized or accredited) public and private sector procurement and treatment sites.
This is the fifth survey of this nature organized by WHO-PQT. Reports of previous surveys are available on the WHO website. (1,2,3,4) The survey results are intended to assist the responsible authorities in participating countries to evaluate their markets and propose possible strategies and implementation plans to address any problems identified. In addition, the active engagement of regulatory staff is expected to help build capacity for coordinated post-market quality surveillance in WHO Member States.
MethodologyMedicines samples were collected at official public and private sector procurement and treatment centres in Burkina Faso, Democratic Republic of the Congo (DRC), Nigeria, Rwanda and Zambia. The survey targeted selected ARVs used in large volumes as reported by international procurers. The focus was on those products with the highest probability of quality problems, prioritizing paediatric formulations – for which there has been a steady increase in prequalification in the past five years – and products of which substandard or falsified versions had been reported to the WHO Global Surveillance System.(5) The following ARVs were included in the survey:• efavirenz 600mg tablets;• efavirenz/ emtricitabine/ tenofovir
disoproxil fumarate 600/200/300mg tablets;
• lamivudine 150mg tablets;• lamivudine/ nevirapine/ zidovudine
30/50/60mg dispersible tablets;
This article was contributed by Mr Rutendo Kuwana and Dr Jitka Sabartova, who jointly coordinated the quality testing survey.

163
WHO Drug Information Vol. 31, No. 2, 2017 Quality monitoring
• lamivudine/ nevirapine/ zidovudine 150/200/300mg tablets;
• lamivudine/ zidovudine 30/60mg dispersible tablets;
• lamivudine/ zidovudine 30/60mg tablets;• lamivudine/ zidovudine 150/300mg
tablets; and• nevirapine 50mg dispersible tablets.The quality of the samples was verified by testing at four WHO-prequalified laboratories according to the monographs of The International Pharmacopoeia, British Pharmacopoeia and US Pharmacopeia as applicable. Testing according to official pharmacopoeial monographs made it possible to compare products from different manufacturers. However, individual products may be registered in countries or prequalified by WHO with methods and specifications that differ from those set for this survey. The protocol therefore required that if a sample of a prequalified product was found to be out of specification when using the pharmacopoeial method, it was to be re-tested using the manufacturer’s validated method accepted by WHO-PQT. The decision on compliance was then based on the result of the method used in the re-testing.
The survey was conducted in good compliance with the pre-established protocol. As in previous surveys organized by WHO-PQT, the outcomes were discussed with representatives of regulatory authorities, who participated in the formulation of recommendations.
Results
Number of samples testedA total of 126 samples were collected and tested.
Origin of samplesThe samples collected represented medicines produced by eight different manufacturers, all of whom were based in India. The authenticity in terms of batch number, manufacturing and expiry dates, and manufacturing site was confirmed for all samples by the relevant manufacturers. Therefore it is highly unlikely that any falsified products were present among the collected samples.
The large majority of samples (98%, 123 of 126 samples) were of WHO-prequalified products.
Testing resultsOf the 126 samples tested, 125 fully complied with the specifications set for the survey. This included two samples that did not comply with pharmacopoeial specifications during initial testing, but complied when re-tested with approved manufacturer’s methods.
There was only one non-compliant finding in the survey: In one of two collected containers of a sample the tablets were stained with drying agent from a burst sachet, causing them to fail the pharmacopoeial requirements for appearance. The stained tablets were excluded from further testing.
DiscussionThe survey provided a snapshot picture of the quality of the sampled products and generated information about the availability of the target medicines in selected countries, their prequalification and registration status, and the storage conditions in procurement and treatment centres in participating countries.
Testing at WHO-prequalified laboratories according to the common protocol and specifications can be considered as reliable.
Survey of the quality of selected ARVs in five African countries

Quality monitoring WHO Drug Information Vol. 31, No. 2, 2017
164
However, when interpreting the outcomes of the survey it should be kept in mind that the results relate to a limited set of countries, a specific selection of medicines and a limited number of samples taken at official procurement and treatment centres.
The survey showed that pharmacopoeial methods are not always applicable for quality control of specific products. Although in the majority of cases they seemed to be sufficient to control products appropriately, there were two cases where – contrary to the approved manufacturers’ methods – they provided marginally failing results.
Compared with the results of the study organized by WHO-PQT in 2007,(1) the failure rate decreased from 1.8% to 0.8%, indicating a marginal improvement of the quality of ARVs found in official distribution and treatment centres. The share of prequalified products among samples increased from 53% to 98%. The survey reconfirmed the positive impact of WHO prequalification in making ARVs of consistently good quality available for procurement in countries.
In the five quality surveys organized to date by WHO-PQT across product categories, 113 of 682 non-prequalified product samples failed to comply with specifications, compared with only seven of 464 WHO-prequalified product samples. For two of the seven it could be shown that the problem was likely caused after manufacture.(2) These results demonstrate that WHO prequalification reliably assures uniform quality standards.
ARVs procured for HIV treatment programmes are mostly donor- or government-funded, and are typically subject to quality policies that require them to be WHO-prequalified or approved for use in a stringent regulatory environment. As can be expected, all the samples collected
in the survey were of imported products, none of them represented locally produced medicines.
The complexity of procurement and distribution of ARVs was illustrated by the fact that some manufacturers did not know to which markets their products were supplied in the end, and re-distribution of medicines among countries was frequent. This highlights the importance for regulators to take into account the risks associated with such complex supply channels.
In principle, the selected medicines were available at procurement and treatment centres, although there were differences in the number of generic versions that were available. For certain medicines targeted in the survey the availability was influenced by local therapeutic guidelines and practices.
Rigorous registration policies are applied in some participating countries – notably in Nigeria and Zambia – but other legally acceptable mechanisms that bypass normal registration processes are also used to ensure a continued supply of needed medicines, as was the case in Burkina Faso, DRC and Rwanda. It was not assessed to which extent the responsible national authorities verified whether the ARVs targeted in this survey were in line with the specifications and conditions accepted by WHO-PQT, for example by using the WHO collaborative registration procedure.(6) Four of the five countries included in the survey (Burkina Faso, DRC, Nigeria and Zambia) were participating in the collaborative procedure at the time of the study. However, only two products registered through this pathway were sampled in the survey, namely lamivudine 150mg tablets and lamivudine/ zidovudine 150/300mg tablets in Nigeria1.1 A list of collaboratively registered products is
available at https://extranet.who.int/prequal/content/collaborative-registration-faster-registration.
Survey of the quality of selected ARVs in five African countries

165
WHO Drug Information Vol. 31, No. 2, 2017 Quality monitoring
The survey results further indicate that storage conditions in procurement and treatment centres in participating countries were in principle under control and did not have a negative impact on medicines quality.
Conclusions and recommendationsAlthough antiretrovirals with a higher probability of substandard quality were targeted in this survey, the results indicate that ARVs available at official procurement and treatment sites are of good quality.
The method of multistate collaborative sampling, centralized testing, with common data analysis, has once more proved to be a useful approach in independent quality monitoring of prioritized medicines. The approach was commended by participating countries during the debriefing session.
It was recommended that future surveys should incorporate non-destructive in-country screening before samples are submitted to designated laboratories, and that parallel in-country testing of samples in national quality control laboratories could be conducted as an element of proficiency testing to build capacity and confidence. WHO should also make efforts to develop
data-sharing platforms or repositories of testing results for use by Member States.
References1 WHO. Survey of the quality of antiretroviral
medicines circulating in selected African countries. September 2007.
2 WHO. Survey of the quality of selected antimalarial medicines circulating in six countries of sub-Saharan Africa. January 2011.
3 WHO. Survey of the quality of anti-tuberculosis medicines circulating in selected newly independent states of the former Soviet Union. November 2011.
4 Survey of the quality of medicines identified by the United Nations Commission on Life-Saving Commodities for Women and Children. WHO: 2015.
5 WHO Global Surveillance and Monitoring System [webpage]. www.who.int/medicines/regulation/ssffc/surveillance/en/
6 WHO. Collaborative procedure between the World Health Organization (WHO) prequalification team medicines and national medicines regulatory authorities in the assessment and accelerated national registration of WHO- prequalified pharmaceutical products and vaccines. Annex 8. In: WHO Technical Report Series 996, 2016. å
Survey of the quality of selected ARVs in five African countries

166
WHO Drug Information Vol. 31, No. 2, 2017
Safety news
Safety warnings
Dulaglutide:Anaphylaxis and angioedemaJ a p a n – The PMDA has informed health professionals that cases of anaphylaxis have been reported in patients treated with dulaglutide (Trulicity®) outside Japan. Angioedema-related symptoms have been frequently observed in the cases associated with anaphylaxis, and independent cases of angioedema have also been reported. The product information in Japan will be updated to reflect the risk of these adverse events.
► PMDA Summary of investigation results and MHLW Revision of precautions, 30 May 2017.
Darbepoetin alfa: Severe skin reactionsC a n a d a – Health Canada has informed health professionals about international reports of severe blistering, mucosal ulceration, and exfoliation cutaneous reactions, including life-threatening Stevens-Johnson syndrome and toxic epidermal necrolysis in patients treated with darbepoetin alfa in the post-marketing setting. No cases have been reported in Canada. Darbopoetin alfa is indicated for the treatment of anaemia associated with chronic kidney disease or anaemia in cancer patients receiving chemotherapy.
► Health Canada Advisory, 5 May 2017.
Caspofungin: Severe skin reactionsJ a p a n – The MHLW and PMDA have jointly recommended updates to the product information for the antifungal medicine caspofungin acetate to warn about the risk of toxic epidermal necrolysis and Stevens-Johnson syndrome. This follows reports of cases of these serious skin reactions in patients treated with caspofungin acetate both in Japan and elsewhere. Similar updates have been made to the product information in the U.S. and Europe.
► PMDA Summary of investigation results and MHLW Revision of precautions, 20 April 2017.
Pneumococcal vaccine: Injection site necrosisJ a p a n – The PMDA/MHLW have recommended to update the product information for pneumococcal vaccine (Pneumovax®) to advise health professionals that the cellulitis-like reactions that can occur primarily on the injection site may result in necrosis or ulcer. This follows reports of injection site necrosis or ulcer reported in patients immunized with pneumococcal vaccine in Japan.
► PMDA Summary of investigation results and MHLW Revision of precautions, 30 May 2017.
Pembrolizumab: Severe skin reactionsC a n a d a – Health Canada has informed health professionals that cases of Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), some with fatal outcomes,

167
WHO Drug Information Vol. 31, No. 2, 2017 Safety news
have been reported in patients treated with the cancer medicine pembrolizumab (Keytruda®). Patients should be counselled about this risk and early symptoms. In case of a severe skin reaction pembrolizumab should be suspended and patients referred for immediate specialized evaluation and treatment. Pembrolizumab should be permanently discontinued if SJS or TEN is confirmed. The product information is being updated to include these recommendations.
► Health Canada Advisory, 20 March 2017.
MyocarditisJ a p a n – Following reported cases of myocarditis in patients treated with pembrolizumab, the MHLW and PMDA have recommended updates to the product information to reflect the risk of this adverse event.
► PMDA Summary of investigation results and MHLW Revision of precautions, 20 April 2017.
Vemurafenib: Fibrosis in hands and feetN e w Z e a l a n d – The marketing authorization holder, in consultation with Medsafe, has informed health professionals of the increased risk of Dupuytren’s contracture and plantar fascial fibromatosis in patients treated for melanoma with vemurafenib (Zelboraf®). These conditions are characterized by thickening or appearance of visible cords in the hands and feet. The product information has been updated to recommend temporary or permanent discontinuation of vemurafenib in case of these adverse events, and to provide guidance on dosage modification.
► Medsafe Safety information, posted 27 March 2017.
Denosumab:Fractures after discontinuationJ a p a n – The MHLW and PMDA have informed health professionals that multiple vertebral fractures, which may be associated with a temporary increase in bone resorption, may occur in patients with osteoporosis after discontinuation of denosumab, and that transitioning to an alternative antiresorptive agent should be considered when denosumab is stopped.
A higher incidence of multiple new vertebral fractures was seen in patients that had discontinued denosumab compared with placebo in follow-up clinical studies. The time to onset was not inconsistent with that of a temporary increase in bone resorption observed after stopping denosumab in pre-approval clinical studies. The product information for denosumab is being updated to reflect this information.
► PMDA Summary of investigation results and MHLW Revision of precautions, 20 April 2017.
Gadolinium contrast agents: Accumulation in the brainE u r o p e a n U n i o n – The EMA’s Pharmacovigilance and Risk Assessment Committee (PRAC) has concluded its review of gadolinium agents used to enhance magnetic resonance imaging (MRI) body scans. The PRAC has recommended suspension of marketing authorizations for four linear gadolinium contrast agents, i.e. intravenous injections of gadobenic acid, gadodiamide, gadopentetic acid and gadoversetamide. Instead, macrocyclic agents should be used at the lowest dose that enhances images sufficiently to make diagnoses, and only when unenhanced body scans are not suitable.
The review found convincing evidence of gadolinium accumulation in the brain.
Safety news WHO Drug Information Vol. 31, No. 2, 2017
168
Although this has not been linked to any symptoms or diseases the PRAC took a precautionary approach, noting that data on the long-term effects of gadolinium in the brain are limited.
Two linear agents will remain available: gadoxetic acid used at a low dose for liver scans, which meets an important diagnostic need, and a formulation of gadopentetic acid injected directly into joints, which has a very low gadolinium concentration. Both agents should be used at the lowest dose that enhances images sufficiently to make diagnoses and only if unenhanced scans are not suitable.(1)
At the request of some marketing authorization holders of gadolinium-containing contrast agents a re-examination will be conducted and is expected to conclude in July 2017.(2)
U n i t e d S t a t e s o f A m e r i c a – The FDA has announced that to date it has not identified any harmful effects with brain retention of gadolinium-based contrast agents for MRIs, and that its review will continue. The Agency plans to hold a public meeting in the future to discuss this issue.(3)
► (1) EMA Press release, 10 March 2017.(2) EMA News, 5 May 2017.(3) FDA Drug Safety Communication, 22 May 2017.
Restrictions
Codeine, tramadol: Further restrictionsU n i t e d S t a t e s o f A m e r i c a – The FDA has further restricted the use of codeine- and tramadol-containing medicines in children due to the serious risk of slowed or difficult breathing which can be potentially fatal. Codeine is contraindicated to treat pain or cough in children under 12 years of age, and
tramadol is contraindicated to treat pain in these children. Neither medicine should be used in adolescents aged 12–18 years who are obese or have conditions such as obstructive sleep apnoea or severe lung disease.
Single-ingredient codeine-containing products and all tramadol-containing products are FDA-approved only for use in adults. The FDA has also recommended against the use of codeine and tramadol medicines in breastfeeding mothers due to the risk of adverse reactions, including serious, potentially fatal breathing problems.
► FDA Drug safety communication, 20 April 2017.FDA Statement, 20 April 2017.
A u s t r a l i a – The TGA has informed health professionals that following a December 2016 decision, all medicines containing codeine will be rescheduled as prescription medicines with effect from 1 February 2018, and may then no longer be advertised to the public.
► TGA. Changes to advertising for medicines containing codeine. 8 May 2017.
To be removed from the market
Oxymorphone injection: Abuse, dangerous consequencesU n i t e d S t a t e s o f A m e r i c a – The FDA has requested the removal of oxymorphone hydrochloride injection (Opana ER®) from the market. A review of all available post-marketing data had shown a significant shift in the route of abuse from nasal to injection, following the product’s reformulation as an injection. The injection abuse of the product has been associated with a serious outbreak of HIV and hepatitis C, as well as cases of thrombotic microangiopathy, a serious blood disorder.

169
WHO Drug Information Vol. 31, No. 2, 2017 Safety news
This is the first time that a currently marketed opioid pain medication is removed from sale in the U.S. due to the public health consequences of abuse. The product had been reformulated 2012 to reduce the potential for abuse; however, the reformulation has had unintended consequences. As a part of the its response to the opioid epidemic in the United States, the FDA will continue to examine the risk-benefit profile of all approved opioid analgesic products and will take further actions as appropriate.
► FDA News release, 8 June 2017.
New prescribing guidelines
Vancomycin: Fighting antimicrobial resistanceE u r o p e a n U n i o n – The European Medicines Agency (EMA) has recommended changes to the prescribing information for vancomycin to ensure its appropriate use in the context of the fight against antimicrobial resistance. Vancomycin remains an important therapeutic option for the treatment of serious infections. The updated recommendations are as follows.• Vancomycin infusion can continue to
be used for the treatment of serious infections caused by certain bacteria including methicillin-resistant Staphylococcus aureus (MRSA) and to prevent bacterial endocarditis in patients undergoing surgery. The starting dose should be calculated according to the age and weight of the patient. Any dose adjustments should be based on serum concentrations to achieve the target therapeutic concentrations.
• Oral vancomycin should be used only to treat Clostridium difficile infections. The maximum dose should not exceed 2 g
per day. In patients with inflammatory intestinal disorders, vancomycin serum concentration should be closely monitored. Children under 12 should be given age-appropriate formulations. Oral vancomycin should no longer be used to treat staphylococcal enterocolitis or for gastro-intestinal decontamination in immunocompromised patients.
• Vancomycin formulations authorized for intraperitoneal use can continue to be used to treat infections in patients undergoing a peritoneal dialysis. ► EMA Press release, 19 May 2017.
Opioids:Updated prescribing guidance in CanadaC a n a d a – The Government of Canada has announced the publication of an updated guideline on opioid prescribing to mitigate the impact of the current opioid crisis. The guideline recommends that patients with chronic non-cancer pain should first try non-opioid options to manage pain before considering a trial of opioid therapy. Patients starting opioid therapy should be given less than 90 morphine equivalents daily (MED) and the maximum prescribed dose should be restricted to less than 50 mg MED. Patients already on high doses of prescribed opioids (90 mg MED or more) should be encouraged to taper the doses gradually in collaboration with their prescribers, with multidisciplinary support offered to those who experience challenges.
Health Canada and the Canadian Institutes of Health Research provided funding for the updating of the guideline and associated training tools for prescribers, as part of efforts to address problematic prescription drug use.
► Government of Canada. News release, 8 May 2017.

Safety news WHO Drug Information Vol. 31, No. 2, 2017
170
Known risks
Eluxadoline: Risk of pancreatitis in certain patientsU n i t e d S t a t e s o f A m e r i c a – The FDA has warned that eluxadoline (Viberzi®), used for the treatment of irritable bowel syndrome with diarrhoea, should not be given to patients who do not have a gallbladder. An FDA review found that these patients have an increased risk of developing serious pancreatitis that could result in hospitalization or death. Pancreatitis may be caused by spasm of the sphincter of Oddi in the small intestine.(1)
In the EU, a similar warning was included in the product information for eluxadoline (Truberzi®) in 2016 at the time of approval.
► FDA Drug Safety Communication, 15 March 2017.
Canagliflozin: Lower limb amputationsU n i t e d S t a t e s o f A m e r i c a – The FDA has confirmed the increased risk of leg and foot amputations with the diabetes medicine canagliflozin, and has required new warnings, including the most prominent “Boxed Warning” to be added to the product information for canagliflozin to describe this risk. This follows an FDA warning published in May 2016 on the basis of interim clinical trial results.(1)
Earlier in 2017 the EMA had confirmed this risk for canagliflozin and had required updates to the product information. A warning about this potential risk was also added to the product information of dapagliflozin and empagliflozin.(2)
► (1) FDA Drug Safety communication, 16 May 2017.(2) EMA. Human medicines. Article 20 referral: SGLT2 inhibitors (previously canagliflozin). 10 February 2017.
Certain hepatitis C medicines: Interaction with ethinyloestradiolA u s t r a l i a – The TGA has advised health professionals that, while in the product information for the hepatitis C medicines Viekira PAK® (paritaprevir/ritonavir/ombitasvir tablets and dasabuvir tablets) and Viekira PAK-RBV® (paritaprevir/ritonavir/ombitasvir tablets, dasabuvir tablets and ribavirin tablets) the use of ethinyloestradiol-containing medicines is listed as a contraindiction, not all ethinyloestradiol-containing medicines currently provide similar information.
In clinical trials for the hepatitis C medicines, elevations of liver enzymes to more than five times the upper limit of normal occurred in approximately 1% of participants, and occurred more frequently in women taking contraceptives containing ethinyloestradiol. Contraceptives containing ethinyloestradiol must be discontinued prior to starting treatment and alternative contraceptive agents used. Ethinylestradiol-containing medicines can be restarted approximately two weeks following completion of treatment with Viekira PAK® or Viekira PAK-RBV®.
► Medicines Safety Update. Volume 8, Number 2, April-May 2017.
Bosutinib: Severe skin reactions J a p a n – A warning about the risk of toxic epidermal necrolysis, Stevens-Johnson syndrome and erythema multiforme has been added to the product information of bosutinib, used to treat certain forms of leukaemia. This follows reported cases of these severe skin reactions in patients treated with bosutinib in Japan.
This risk is also reflected in the product information for bosutinib approved in the EU.
► PMDA Summary of investigation results and MHLW Revision of precautions, 30 March 2017.

171
WHO Drug Information Vol. 31, No. 2, 2017 Safety news
Ponatinib:Update on dose adjustmentU n i t e d K i n g d o m – The MHRA has provided health professionals with an update on dose modifications to mitigate the risk of blood vessel blockages with ponatinib (Iclusig®). For patients with chronic-phase chronic myeloid leukaemia who have achieved a major cytogenetic response while on treatment, the dose can be reduced to 15 mg/day based on an individual patient assessment. If the dose is reduced, close monitoring of response is recommended.
This advice is supported by additional long-term follow-up data that have become available since this risk was first communicated in 2014.
► MHRA Drug Safety Update volume 10, issue 9, April 2017: 2.
Idelalisib: Risk of serious infections C a n a d a – Health Canada has updated the product information for the cancer medicine idelalisib (Zydelig®) to warn about the increased risk of serious and potentially fatal infections, and to recommend antibiotic prophylaxis against Pneumocystis jirovecii pneumonia and monitoring of patients for cytomegalovirus infection. Idelalisib is not authorized in Canada for use in first-line chronic lymphocytic leukaemia and early-line indolent non-Hodgkin lymphoma outside of a clinical trial.
In 2016 a number of clinical trials involving idelalisib had been stopped due to serious side effects, and several regulatory authorities initiated safety reviews and published safety communications. In the EU, product information was updated in July 2016 with recommendations to mitigate this risk.
► Health Canada. Summary Safety Review. 3 March 2017.
Hypnotics and anxiolytics: Risk of dependence even with recommended useJ a p a n – The PMDA has completed its review of dependence-related adverse events reported with the use of hypnotics and anxiolytics. The review had been requested by the Ministry of Health, Labour and Welfare (MHLW) in view of the high reported use of hypnotics and anxiolytics in Japan. The PMDA recommended updates to the product information for these medicines to emphasize the risk of dependence regardless of patients’ predispositions to drug abuse and to warn against prolonged use even for approved indications and at recommended doses.
To discourage inappropriate prescribing, a demerit point system had been introduced in Japan as part of the 2012 and 2014 revisions to health insurance regulations. Furthermore, given that risk of abuse was confirmed for zopiclone and etizolam, the MHLW had issued an announcement in September 2016, newly specifying these drugs as psychotropics and recommending a maximum treatment duration of 30 days.
► PMDA. Report on investigation results, 28 February 2017.
Anaesthetics and sedatives in young children:Harm to developing brainU n i t e d S t a t e s o f A m e r i c a – The FDA has approved previously announced changes to the product information of general anaesthetic and sedation medicines, warning against their lengthy or repeated use in children under 3 years of age and in pregnant women during the third trimester. Data from studies in young animals suggest that exposure to these medicines for more

Safety news WHO Drug Information Vol. 31, No. 2, 2017
172
than 3 hours can cause widespread loss of nerve cells in the developing brain.
► FDA Drug safety communication, 27 April 2017.
Iodinated contrast media: Hypothyroidism, affecting growth and developmentC a n a d a – A Health Canada assessment has revealed a possible association between exposure to iodinated contrast media (ICM) and development of hypothyroidism in adults and children, particularly in infants. Hypothyroidism in infants may be harmful for growth and development, including mental development. The Agency encourages healthcare professionals to evaluate and monitor thyroid function in infants exposed to ICM, and if abnormal, continue to monitor until it has normalized. Prescribing information for these products will be harmonized to include this information.
In 2015 the FDA had requested manufacturers to include information related to rare cases of hypothyroidism reported in infants following the use of ICM products.
► Health Canada Advisory, 24 April 2017.
Unchanged recommendations
Selexipag: No increased risk of mortalityE u r o p e a n U n i o n – The European Medicines Agency (EMA) has completed its review of selexipag (Uptravi®) which was initiated following five patient deaths in France. The data reviewed did not suggest that selexipag is associated with a higher risk of mortality than other medicines used to treat pulmonary arterial hypertension. EMA has confirmed that selexipag can continue to
be used by both new and existing patients according to the current prescribing information.
► EMA News, 7 April 2017.
Factor VIII-containing medicines: No differences in inhibitor developmentE u r o p e a n U n i o n – The EMA has completed its review of factor VIII medicines to evaluate the risk of inhibitors developing in patients with haemophilia A who have not previously been treated with these medicines. The review was triggered by the outcomes of a study which found this risk to be greater with recombinant factor VIII medicines than with plasma-derived ones. The review did not find any clear and consistent evidence of a difference in inhibitor development between the two classes of factor VIII medicines.(1)
A marketing authorization holder has requested a re-examination, which will start upon receipt of the grounds for the request.(2)
► (1) EMA News, 5 May 2017.(2) EMA News, 9 June 2017.
Mefloquine: Clarifications on adverse events C a n a d a – A Health Canada safety review launched at the end of 2016 has not found conclusive evidence that mefloquine can cause long-lasting and permanent neurological and psychiatric adverse events. Mefloquine remains a first-line option a first-line option to protect Canadians from malaria when travelling to areas with a high infection risk. The product information for mefloquine will be updated with a checklist of contraindications for prescribers, as well as clearer information for patients on the risk of damage to the vestibular system in
173
WHO Drug Information Vol. 31, No. 2, 2017 Safety news
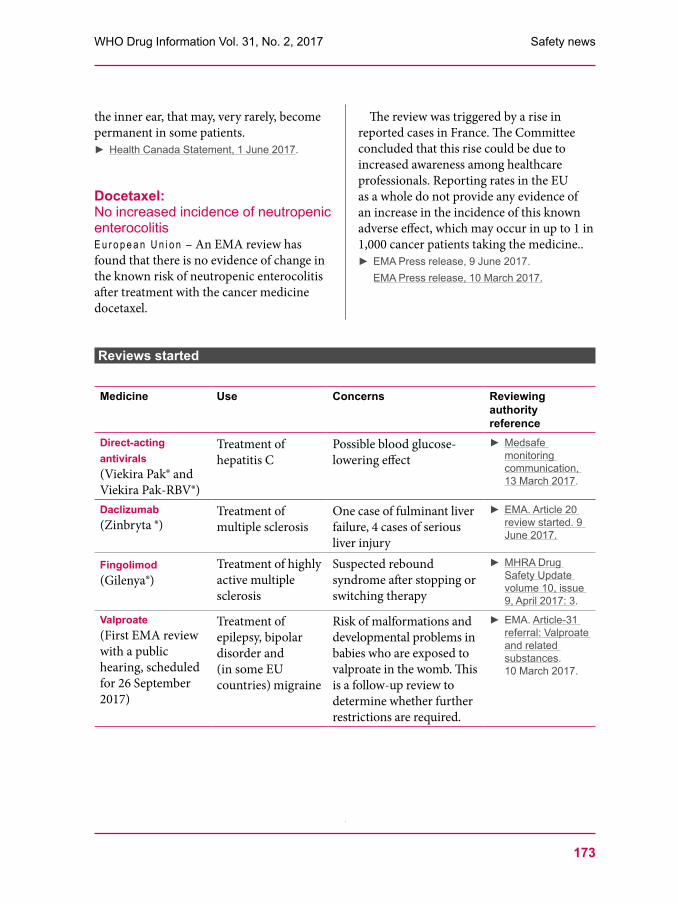
Reviews started
Medicine Use Concerns Reviewing authority reference
Direct-acting antivirals(Viekira Pak® and Viekira Pak-RBV®)
Treatment of hepatitis C
Possible blood glucose-lowering effect
► Medsafe monitoring communication, 13 March 2017.
Daclizumab(Zinbryta ®)
Treatment of multiple sclerosis
One case of fulminant liver failure, 4 cases of serious liver injury
► EMA. Article 20 review started. 9 June 2017.
Fingolimod (Gilenya®)
Treatment of highly active multiple sclerosis
Suspected rebound syndrome after stopping or switching therapy
► MHRA Drug Safety Update volume 10, issue 9, April 2017: 3.
Valproate(First EMA review with a public hearing, scheduled for 26 September 2017)
Treatment of epilepsy, bipolar disorder and (in some EU countries) migraine
Risk of malformations and developmental problems in babies who are exposed to valproate in the womb. This is a follow-up review to determine whether further restrictions are required.
► EMA. Article-31 referral: Valproate and related substances. 10 March 2017.
the inner ear, that may, very rarely, become permanent in some patients.
► Health Canada Statement, 1 June 2017.
Docetaxel: No increased incidence of neutropenic enterocolitisE u r o p e a n U n i o n – An EMA review has found that there is no evidence of change in the known risk of neutropenic enterocolitis after treatment with the cancer medicine docetaxel.
The review was triggered by a rise in reported cases in France. The Committee concluded that this rise could be due to increased awareness among healthcare professionals. Reporting rates in the EU as a whole do not provide any evidence of an increase in the incidence of this known adverse effect, which may occur in up to 1 in 1,000 cancer patients taking the medicine..
► EMA Press release, 9 June 2017.EMA Press release, 10 March 2017.
Safety news WHO Drug Information Vol. 31, No. 2, 2017
174
Non-compliance with good practices
Micro Therapeutic Research Labs: EMA suspends products due to unreliable bioequivalence dataE u r o p e a n U n i o n – The EMA has recommended suspending a number nationally approved medicines for which bioequivalence studies were conducted by Micro Therapeutic Research Labs in India. For critically important medicines the national authorities can postpone the suspension in the interest of patients. The Agency also recommended that medicines under evaluation and studied at these sites should not be authorized until bioequivalence is demonstrated using alternative data. For some of the products affected, alternative bioequivalence data were subsequently provided and the suspensions were lifted.
Inspections conducted at the two sites in February 2016 had identified concerns regarding misrepresentation of study data and deficiencies in documentation and data handling. This triggered an EMA review, which concluded that data from studies conducted at the two sites between June 2012 and June 2016 are unreliable. The issue affects more than 300 approvals and applications.
► EMA Press release, 24 March 2017.
Mylan LaboratoriesU n i t e d S t a t e s o f A m e r i c a – The FDA has warned the India-based company Mylan over issues with quality management and data integrity at its manufacturing site at F4 & F12 Malegaon MIDC, Sinnar, Nashik observed during an FDA inspection in September 2016.(1) According to the Global Fund’s Price and Quality Reporting (PQR) database, almost half of all
grant-funded antiretrovirals supplied in 2016 were produced by Mylan.(2) WHO has prequalified 21 finished pharmaceutical products manufactured at the Nashik site. Of these, 10 are also manufactured at other Mylan sites which are not affected by the current warning letter. The Prequalification Team had inspected the Nashik site in 2015 and found it compliant after implementation of corrective and preventive action. WHO has recommended increased vigilance and post-shipment testing. The manufacturer has been asked to provide an impact assessment on prequalified products. Thereafter another WHO inspection will be conducted.(3) In an update, WHO-PQT summarized the findings from the impact assessment and concluded that there were no concerns regarding the quality of the WHO- prequalified products manufactured at the Nashik site.(4)
► (1) FDA Warning letter 320-17-32, 3 April 2017.(2) PQR Transaction summary. Available from www.theglobalfund.org/en/sourcing-management/price-quality-reporting/, accessed 12 April 2017.(3) WHO Prequalification team. Position paper, 4 May 2017.(4) WHO Prequalification team. Position paper, 30 May 2017.
Qinhuangdao ZizhuG e n e v a – The WHO Prequalification Team (PQT) has responded to an FDA import alert issued in March 2017 for products containing APIs from Qinhuangdao Zizhu Pharmaceutical Co Ltd following inspection findings of non-compliance with GMP, including a breach of data integrity in the quality control laboratory. WHO-PQT had inspected the site in 2015 and found it compliant with GMP after completion of corrective action. WHO-PQT is planning to re-inspect the site. Meanwhile it has advised

175
WHO Drug Information Vol. 31, No. 2, 2017 Safety news
finished products manufacturers to take additional measures to ascertain the quality of APIs from Qinhuangdao Zizhu, and is working with them to identify alternative API sources.
► WHO Prequalification team. Press release, 7 April 2017.
FDA warning lettersU n i t e d S t a t e s o f A m e r i c a – A series of warning letters were issued to pharmaceutical companies by the FDA’s Center for Drug Evaluation and Research in March, April and May 2017.(1)
An FDA inspection of the India-based active pharmaceutical ingredient (API) manufacturer Badrivishal Chemicals & Pharmaceuticals revealed that original records, water testing reports and sample notebooks had been discarded in trash bags, which later disappeared. Impurity testing chromatograms showed repeated unexplained discrepancies in run times, aborted runs and reprocessing of data.
The China-based API manufacturer Lumis Global Pharmaceuticals Co. Ltd. had generated certificates of analysis (COA) by copying and pasting analytical results from the API manufacturers onto its own letterhead. The India-based manufacturer USV Pvt Ltd was warned over repeated violations at multiple sites related to data integrity, validation of aseptic and sterilization processes and other issues. Divi’s Laboratories Ltd in Visakhapatnam, India was warned over their failure to prevent unauthorized access to data as well as manipulation and omission of data. Warnings were also issued to Opto-Pharm Pte Ltd in Singapore, Indoco Remedies Limited in India, Teva’s API manufacturing site in Hangzhou, China, Sal Pharma and Vikshara Trading & Investments Ltd in India, and
Changzhou Jintan Qianyao Pharmaceutical Raw Materials in China.
These reports highlight once more the need for stringent regulation and enforcement of adherence to regulatory requirements.
► FDA warning letters are available at: www.fda.gov/ICECI/EnforcementActions/WarningLetters/
TGA reminder on good data management requirementsA u s t r a l i a – The TGA has published a statement regarding its expectations regarding data management and integrity. The Agency is reminding applicants that it views data management and integrity issues very seriously, as reflected in its definition of a “critical” deficiency in GMP, which states: “A deficiency in a practice or process that has produced, or may result in, a significant risk of producing a product that is harmful to the user. Also occurs when it is observed that the manufacturer has engaged in fraud, misrepresentation or falsification of products or data.”
The statement goes on to outline the ALCOA+ principles1 – the basis of good data management and integrity practices – as described in the draft guidelines of the Pharmaceutical Inspection Co-operation Scheme (PIC/s). The TGA intends to use these guidelines as reference in its regulatory inspections and dossier review.
► TGA Statement, 6 April 2017.PIC/S. Draft PIC/S guidance. Good practices for data management and integrity in regulated GMP/GDP environments. PI 041-1 (Draft 2). 10 August 2016. Available at: https://picscheme.org/en/news?itemid=33
1 ALCOA+: Attributable, Legible, Contemporaneous, Original, Accurate; + complete, consistent, enduring, available.

Safety news WHO Drug Information Vol. 31, No. 2, 2017
176
Falsified product alerts
Meningococcal ACWY vaccine in West AfricaThe following is reproduced text from the WHO Medical Product Alert No. 1/2017 relating to the circulation of a confirmed falsified meningococcal ACWY vaccine discovered in Niger.
Product details This product is used to immunize against Meningococcal disease serogroups A, C, W, and Y.
Meningococcal meningitis vaccine is listed as a WHO Essential Medicine. On 31 May 2017, the manufacturer “Bio-Manguinhos/Fiocruz” informed WHO that a falsified
version of the following product was available in Niger.Product name: Polysaccharide Meningo coccal ACWY VaccineBatch number: 089UMH002 ZExpiry date: 092017Date of manufacture: 092014
The label on the product claims that it is manufactured by Bio-Manguinhos/Fiocruz and is presented in vials of 10 doses each. The falsified product had not yet been subject to laboratory analysis at the time of publishing the Medical Product Alert.
The manufacturer Bio-Manguinhos/Fiocruz has stated that:– They do not manufacture Polysaccharide Meningococcal ACWY Vaccine.– Based on examination of the photographs they can confirm that this packaging is falsified.
No adverse events following immunisation attributed to this falsified vaccine are known to have been reported at this stage. On the basis of the above information, any Meningococcal ACWY Vaccine claiming to be manufactured by “Bio-Manguinhos/Fiocruz”, should be considered falsified and reported.
Advice to health care professionals, patients and national authorities is provided in the WHO medical product alert. Authorities are asked to immediately notify WHO if these falsified products are discovered in their country by contacting [email protected]
► WHO Medical Product Alert No. 1/2017, 2 June 2017 (includes photographs).
Hepatitis C medicine in GermanyThe German regulatory authority has informed health professionals and the public that the following falsified product has been discovered in a pharmacy in the state of North Rhine-Westfalia.
Product: Harvoni® 90 mg / 400 mg tabletsBatch number: 16SFC021D (this lot number exists for the genuine
product on the German market)Expiry date: 06/2018Colour: The tablets are white instead of orange.
The content of the falsified tablets is not yet known; laboratory analysis is ongoing. The manufacturer of the genuine product, Gilead, has organized a recall of the lot with the above-mentioned number from the German market.
► Bundesinstitut für Arzneimittel und Medizinprodukte (BfArM). Press release 9/17, 6 June 2017 (in German).

177
WHO Drug Information Vol. 31, No. 2, 2017 Regulatory news
Regulatory news
Pre-market assessment
Assessment of generics in China:Demonstrating interchangeabilityIn 2016 the State Council of the Government of China launched a policy requiring that all oral solid preparations of generic medicines on the National Essential Drugs List (2012) approved before 1st October 2007 should be evaluated by the end of 2018, with a possibility to extend the deadline until the end of 2021 in case of special circumstances, for example if clinical trials are required.(1) More details about this policy are found in a recently published commentary, the abstract of which is reproduced below.(2)
Generic drugs should be interchangeable with originators in terms of quality and efficacy. With relative lower prices, generic drugs are playing an important role in controlling health expenditures and ensuring access. However, the widespread understanding of “cheap price equals low quality” has a negative impact on the acceptance of generic drugs. In China, medical doctors doubt the efficacy and quality of generic drugs manufactured domestically. To address these concerns, the Chinese State Council released a policy in 2016 to ensure the interchangeability by re-evaluating the quality and efficacy of generic drugs. It intends to make up a missed lesson in the regulation to be in line with internationally accepted practices. Generic drugs firms, depending on the availability of appropriate comparators, should conduct either comparative bioequivalence studies or full scale clinical trials. The re-evaluation will be implemented in a stepwise approach with
the essential medicines covered in the first step. The policy could achieve several benefits by increasing confidence on the Chinese produced generic drugs, upgrading regulatory standards, streamlining the Chinese generic drug industry and creating a healthy competition market. Nevertheless, enormous challenges remain in enlarging the capacity to review applications, selecting appropriate comparators, ensuring the capacity of domestic clinical research sites, and achieving the acceptance of re-evaluated generic drugs.
► (1) State Council of the People’s Republic of China. Policies. Release, 5 March 2016. (2) Huang B, Barber SL, Xu M, Cheng S. Make up a missed lesson - New policy to ensure the interchangeability of generic drugs in China. Pharmacol Res Perspect 2017:5(3). Published online 3 May 2017, doi: 10.1002/prp2.318.
New fast-track pathway in India: WHO-recommended combinationsI n d i a – The Drugs Controller General of India has issued a notice outlining a fast-track regulatory approval pathway for combination products recommended in WHO guidelines and which are used to treat HIV infection and subtypes of hepatitis B and C relevant to the Indian population. The fast-track provisions apply regardless of whether the specific combination product has been previously approved elsewhere.
The new pathway includes provisions for waiving clinical trial requirements and for early submission of abbreviated data with a commitment that complete data will be submitted prior to approval. The rationale is that combinations recommended in WHO treatment guidelines are considered to have

Regulatory news WHO Drug Information Vol. 31, No. 2, 2017
178
a positive risk-benefit balance, and that they are falling under the category of “extreme urgency” as defined in national regulations.
► CDSCO Notice, 20 March 2017.
Australian orphan drug programme:Reforms and transition arrangementsA u s t r a l i a – The TGA has announced updates to its orphan drug programme to align it with the practices of other regulatory authorities and to target the most important unmet needs. The changes take into account feedback received in two public consultations. The threshold and eligibility criteria will be adjusted so that more conditions may qualify as orphan diseases, and the validity period of orphan drug designation will be limited to 6 months, with a possibility of extension to 12 months with written justification. The changes are effective from 1 July 2017.(1) Transition arrangements are in place for existing designations made at a time when their status would not lapse.(2)
► (1) TGA. Submissions received and TGA response: Orphan drug program. 18 April 2017.(2) TGA. Reform of the Orphan Drug Program - Transition arrangements.
EU Priority medicines scheme:One year onE u r o p e a n U n i o n – The EMA has met with stakeholders to look back on one year’s experience with its PRIME (PRIority MEdicines) scheme. Of 96 requests processed, 20 were approved including 8 for orphan medicines. Among the requests that were not granted, approximately 70% lacked sufficiently robust data, about 40% had an insufficient justification of therapeutic advantage, and about 20% were at an advanced stage of development process was
already so that the use of the scheme would not have been effective.
The PRIME scheme was launched in March 2016 to provide early support to developers of medicines targeting unmet treatment needs. It assists applicants in optimizing development plans, collecting robust data and submitting high quality applications enabling timely authorization of needed products.
► EMA News, 19 May 2017.
EU medical devices regulation:Strengthened rulesE u r o p e a n U n i o n – The European Parliament has adopted two new regulations on medical and in vitro diagnostic medical devices. The new rules will impose tighter controls on high-risk devices such as implants, on clinical trials and on the independent notified bodies that can approve the marketing of medical devices. The new rules will also cover certain previously unregulated aesthetic products. A new system for risk classification in line with international guidelines will apply to in vitro diagnostic medical devices (IVDs). The rules will also improve the traceability of medical devices in the supply chain by using a unique identification number reflected in the new European database of medical devices (EUDAMED). Manufacturers will be obliged to collect data about their performance and EU countries will coordinate more closely in the field of market surveillance.
Medical devices such as diagnostics, companion tests and delivery devices are playing an increasingly important role in guiding and supporting the use of medicines. The new rules address the need for revision of the existing regulatory framework and for stronger market surveillance in the area of medical devices.

179
WHO Drug Information Vol. 31, No. 2, 2017 Regulatory news
The rules were adopted by the European Parliament in April 2017, for publication in the Official Journal in May. They will become effective after a transitional period of three years from publication for medical devices and five years from publication for in vitro diagnostics.
► European Commission. Press release, 5 April 2017.
Adverse events reporting
Pharmacovigilance in Europe:Updates and system upgradeE u r o p e a n U n i o n – The following revised guidance has been published on the Agency’s Good Pharmacovigilance Practice (GVP) website: Module II – Pharmacovigilance system master file (Rev 2), which completes the transition to the 2010 EU pharmacovigilance legislation including the ‘“Article 57” database for medicinal products, and a major revision of Module V – Risk management systems along with consequent revisions of Module XVI – Risk minimisation measures. The GVP introductory cover note has been updated accordingly.(1)
In addition, the EMA’s experience with its coordinated “single assessments” of manufacturers’ periodic safety update reports (PSUR) is reflected in two new documents: an explanatory note on the GVP Module VII addressing issues that have been raised by companies, and a question-and-answer document that guides assessors throughout the evaluation process. In the single assessment process the EMA’s Pharmacovigilance Risk Assessment Committee (PRAC) reviews all PSURs for medicines containing the same active
substance(s) together. Each review is led by an assessor from one nominated national authority. The recommendations are legally binding in all EU Member States. Before the introduction of this process in 2015, marketing authorization holders submitted their PSURs for nationally authorized medicines separately to each national authority.(2)
In May 2017 a new and improved version of EudraVigilance successfully passed an independent audit leading to a positive recommendation by the PRAC. EudraVigilance is the European information system of suspected adverse reactions to medicines. The enhanced system will be launched in November 2017.(3)
► (1) EMA. Good pharmacovigilance practices [website].(2) EMA News, 6 April 2017.(3) EMA News, 22 May 2017.
Adverse events of illicit drugs in UK:New reporting schemeE u r o p e a n U n i o n – The MHRA has launched a pilot scheme for reporting adverse events observed in people using illicit drugs, particularly new psychoactive substances. The scheme’s reporting form is intended to be used by health professionals working in services such as emergency departments, general practice, drug treatment services, sexual health services and mental health services.
The pilot scheme was created following a marked increase in hospital admissions for poisoning by psychostimulants with abuse potential. The data from the pilot are intended to support provision of clinical guidance to professionals.
► MHRA Drug Safety Update volume 10 issue 8, March 2017: 2.

Regulatory news WHO Drug Information Vol. 31, No. 2, 2017
180
Supply
GMP for compounded medicinesAustralia – The TGA has published new guidance text to assist companies and pharmacists in the interpretation of the PIC/S good manufacturing practice (GMP) requirements for compounded medicinal products. The text provides point-by-point annotations to the main chapters of the PIC/S GMP guide as well as its annexes on manufacturing sterile products and on computerized systems.
Compounding is the preparation of a medicine under the supervision of a pharmacist to meet the specific needs of a patient when no suitable authorized dosage form is available. The guidance provides valuable detail on how to implement good practices in compounding to ensure patient safety.
► TGA. Compounded medicines and good manufacturing practice (GMP). 17 May 2017.
Reporting of shortages in Canada:Now mandatory via new websiteC a n a d a – Pharmaceutical companies are now required by law to report medicines shortages and discontinuances on a new, independent website1. The following must be reported: an anticipated drug shortage; a discontinuation of a drug six months in advance; and any previously unreported shortage within five days of learning about it.
The new website replaces the industry-run website2 where manufacturers have been voluntarily reporting medicines shortages and discontinuances since 2012. The new system offers enhanced notification features and a mobile application. It also provides updated information for health care
1 www.DrugShortagesCanada.ca2 www.drugshortages.ca
providers and patients, including tools and guidance to help manage shortages.
► Health Canada News release, 14 March 2017.
Dispensing categories in Switzerland:Revision to encourage self-medicationS w i t z e r l a n d – Changes have been made in Swiss regulations to encourage self-medication without jeopardizing patient safety. Dispensing category C (in-pharmacy sales only) will be abolished. Drugstores will be able to dispense all medicinal products that do not require a prescription (category D), and certain products currently in that category will be reassigned to category E (sale in all shops). Swissmedic is re-evaluating the products concerned, with a focus on the risks of abuse and possible interactions. The Agency is also re-defining the lists of products that can be dispensed by various types of professional therapists. The project is expected to be concluded by 2019.
► Swissmedic Announcement, 10 April 2017.
Antimicrobial resistance
India national action planI n d i a – The Union Minister of Health and Family Welfare of India has announced the finalization of India’s comprehensive and multi-sectoral National Action Plan to combat antimicrobial resistance (AMR). The announcement was made at the Inter-Ministerial Consultation on AMR containment, where representatives of various Ministries under the Government of India signed a declaration, pledging to strategize collectively to prevent and contain AMR.
► Press Information Bureau of India, 19 April 2017.Delhi Declaration on Antimicrobial Resistance – an interministerial consensus. 19 April 2017.
181
WHO Drug Information Vol. 31, No. 2, 2017 Regulatory news
New investments in CanadaC a n a d a – Health Canada has announced new rules for veterinary drugs to combat antimicrobial resistance. The new rules impose stricter quality requirements for active pharmaceutical ingredients and restrict the personal importation of certain products. They also require manufacturers, importers and compounders to report annual sales of medically important antimicrobials, and they simplify the importation of low-risk veterinary health products, including those that may be used as alternatives to antimicrobials.(1)
Furthermore, the Government of Canada has announced funding of 1.39 million Canadian Dollars (approximately 1 million USD) from the Canadian Institutes of Health Research to support five research teams whose work will advance innovations in point-of-care diagnostics, with the goal of implementing the best diagnostic tools in health care settings and appropriate use of antibiotics.
► (1) Health Canada News release, 17 May 2017.(2) Public Health Agency of Canada. News release, 24 May 2017.
Tripartite alignment on requirements for antibacterialsE u r o p e a n U n i o n , J a p a n , U n i t e d S t a t e s o f A m e r i c a – The EMA, the PMDA and the FDA have agreed to align their data requirements for certain aspects of the clinical development of new antibiotics. The Agencies will update their respective guidance documents, and will provide advice to individual medicine developers.
The agreement was reached at the second tripartite meeting to discuss regulatory approaches for the evaluation of antibacterial agents, held in Vienna on
26–27 April 2017. A first tripartite meeting on the subject had taken place in September 2016; a third is planned for October 2017. The alignment aims to stimulate the development of new treatments to fight antimicrobial resistance and protect global public health.
► EMA News, 12 June 2017.EMA. Second tripartite meeting held between EMA, PMDA and FDA to discuss regulatory approaches for the evaluation of antibacterial agents (webpage).
Collaboration
EU and African regulators meetM a l t a – A workshop jointly organized by the EMA and the Maltese Presidency of the EU on 2–3 March 2017 has brought together scientific experts from EMA’s Committee for Medicinal Products for Human Use (CHMP) and regulators from across Africa. The participants discussed how to promote reliance on the scientific output of the CHMP, in particular the Agency’s “Article 58” procedure for global health products intended for use outside the EU. This procedure aims to increase access to high quality, safe and effective medicines by patients in low- and middle-income countries.
This was the first time that CHMP experts met with non-EU regulators in such a forum. The workshop was organized with support from the Bill & Melinda Gates Foundation and WHO. It is in line with the World Health Assembly Resolution WHA67.20, which calls for regulatory systems strengthening.(1)
L o n d o n – On 18–19 May 2017 a delegation from the East African Community (EAC) visited the EMA to gather information and experience to support the potential

Regulatory news WHO Drug Information Vol. 31, No. 2, 2017
182
creation of a networking medicines agency for the EAC. The EAC has six partner States: Burundi, Kenya, Rwanda, South Sudan, Tanzania and Uganda. Participants discussed the structure and operations of EMA that could serve as a model for regional collaboration in the regulatory assessment of medicines.(2)
► (1) EMA News, 10 March 2017.(2) EMA News, 23 May 2017.
Report on EMA–FDA assessment pilotE u r o p e a n U n i o n – The EMA and the US FDA have released the report on their joint pilot programme for the parallel assessment of applications containing Quality by Design (QbD) elements as reflected in ICH Q8, Q9 and Q10 guidelines. The pilot demonstrated a solid alignment between the two Agencies on the implementation of QbD-related concepts, and has opened up a platform for continuous dialogue.
Launched in 2011 and subsequently extended, the pilot programme concluded in April 2016. Two applications for marketing authorization, three variation applications and nine scientific advice applications were evaluated under this programme. The pilot led to the adoption of three sets of Question-and-Answer documents that also addressed comments from the Pharmaceuticals and Medical Devices Agency (PMDA) of Japan, which participated as an observer.
► Report from the EMA-FDA QbD pilot program. 19 April 2017.
Swiss–Austrian agreementV i e n n a – A memorandum of understanding (MoU) has been signed by the Swiss Agency for Therapeutic Products (Swissmedic) and the Austrian Agency for Health and Food
Safety (AGES). The MoU provides a formal basis for intensifying collaboration and for working together on bilateral initiatives. Swissmedic now has cooperation agreements with the medicines regulatory authorities in all German-speaking countries.
► Swissmedic Press release, 14 March 2017.AGES Press release, 15 March 2017 (German).
MedDRA expands global reachM o n t r e a l , C a n a d a – Over 5 000 organizations in 103 countries now subscribe to MedDRA, the Medical Dictionary for Regulatory Activities. This reflects the successful adoption of MedDRA as a worldwide standard in the protection of public health.
MedDRA was developed by ICH in the 1990s to facilitate sharing of regulatory information internationally. The update was presented at the MedDRA Management Board meeting, held in Montreal, Canada on 27–28 May 2017. The Board noted the successful collaboration between the MedDRA Maintenance and Support Services Organization (MSSO) and the WHO Collaborating Centre for International Drug Monitoring (the Uppsala Monitoring Centre) in expanding the MedDRA user base, and acknowledged the significant work of the CIOMS SMQ Implementation Working Group in developing Standardised MedDRA Queries (SMQs).
► ICH. Press release, 12 June 2017.
EMA and academiaE u r o p e a n U n i o n – The EMA has developed a framework and action plan to formalize and further develop its interactions with the academic community. The aim is to increase academia’s engagement in the

183
WHO Drug Information Vol. 31, No. 2, 2017 Regulatory news
European regulatory system in order to foster technological advances and to ensure that the best scientific expertise is available on time to support regulatory processes and decision-making.
A new webpage has also been published with information on EMA’s activities that are most relevant to academia.
► EMA Press release, 3 April 2017.EMA. Academia [webpage].
Transparency and databases
Publication of clinical study reports:Release of EMA documents haltedL u x e m b o u r g – The EU Court of Justice of the European Union has dismissed two appeals by the EMA against interim orders of the General Court, thus upholding the suspension of the release of clinical study reports on two medicines.
This follows court cases brought against EMA in December 2015 by the two pharmaceutical companies manufacturing the respective products. Both companies argue that the release of the documents would infringe their right to protect commercially confidential information contained in their marketing authorization applications. The two cases are still ongoing.Meanwhile the EMA will respect the interim orders and will not release the documents concerned. The Agency will continue to process requests for access to other documents made under the terms of the EU’s Transparency Regulation.
The EMA’s policy on access to documents, which entered into force in 2010, is the EU’s central instrument to achieve transparency in regulatory decision-making. In October 2016, EMA launched its policy on the
proactive publication of clinical study reports that support applications for marketing authorization for medicines.
► EMA News, 14 March 2017.
India builds centralized regulatory portalI n d i a – The Drug Controller of India has requested pharmaceutical manufacturers to register their sites on the online “SUGAM” portal. Companies are required to register only once and can then enter information on all their facilities, even if they are located in different States.
The portal was launched in November 2015 and is intended for filing, tracking and processing of applications for various types of services rendered by the Central Drugs Standard Control Organization (CDSCO) of India. The latest phase includes modules for manufacturing facilities, approved pharmaceutical products as well as retail and wholesale licences.
► CDSCO. Notice, 3 April 2017.
Ingredients catalogue in Australia A u s t r a l i a – The TGA has published an online catalogue of ingredients approved for use in listed medicines. The catalogue provides a single, searchable online source of information on excipients and associated requirements, increasing transparency for industry and consumers and reducing complexities for business. The catalogue is can be accessed through the Ingredient Table search facility on the TGA’s Business Services website.
► TGA News, 4 April 2017.TGA Business Services website. https://www.ebs.tga.gov.au/.

Regulatory news WHO Drug Information Vol. 31, No. 2, 2017
184
Under discussion
E u r o p e a n U n i o n – The EMA has published draft guidance on the type and format of data on antimicrobial use by animal species. The guidance is intended for EU member states that might provide such data to EMA from their national data collection systems on a voluntary basis.
► EMA Consultation, 24 March 2017.Closing date: 24 September 2017.
Health Canada is proposing regulations that would make a warning sticker and patient information handout mandatory with all prescription opioids at the time of sale. Final publication of the regulations would mark the first time the Canadian government requires a warning sticker and patient handout with a dispensed medicine.
► Health Canada News release, 16 June 2017.Closing date: 31 August 2017.
The EMA has released a draft guideline outlining the practical arrangements for notification of serious breaches of clinical trials authorized in the EU. It aims to provide advice on what should be classified as a serious breach and what should be reported.
► EMA Consultation, 23 May 2017.Closing date: 22 August 2017.
E u r o p e a n U n i o n – The EMA has released a draft concept paper in view of updating its 2006 guidance on the role of pharmacokinetics in developing medicines for children. The proposed revision reflects scientific advances and the experience gained over the last decade.
► EMA Consultation, 4 May 2017.Closing date: 31 July 2017.
E u r o p e a n U n i o n – The EMA has proposed a concept paper to clarify the regulatory expectations for data to support the approval of novel medicines to treat influenza. Several new antiviral agents are being developed for this indication.
► EMA Consultation, 4 May 2017.Closing date: 31 July 2017.
C a n a d a – The Government of Canada has launched a consultation on proposed amendments to the Patented Medicines Regulations. The amendments are intended to provide new regulatory tools and information to protect Canadian consumers from high prescription drug prices.
► Health Canada News release, 16 May 2017.Closed 28 June 2017.
U n i t e d S t a t e s o f A m e r i c a – The FDA has solicited input on its proposal for the future of patient engagement so that the perspectives of patient communities can be better captured. For this purpose the Agency is considering to establish a new Office of Patient Affairs.
► FDA Notice in the Federal Register, 14 March 2017.Closed 12 June 2017.
L o n d o n , U K – The EMA has released a concept paper on the need for revision of its guidance on the quality of water for pharmaceutical use. The guideline was originally adopted in 2002.
► EMA Consultation, 6 March 2017.Closed 6 June 2017.
U n i t e d S t a t e s o f A m e r i c a – The FDA has extended the period for comments on its draft guidance on the data and information

185
WHO Drug Information Vol. 31, No. 2, 2017 Regulatory news
Under discussion
expected for a biological product to meet the standard for interchangeability.
► FDA Docket ID: FDA-2017-D-0154. Docket folder summary.Extended until 19 May 2017.
A u s t r a l i a – The TGA has released a consultation document on proposed options for the future regulation of so-called “low risk” products, such as antiperspirants, over-the-counter (OTC) products, disinfectants, sunscreens, class I medical devices, vitamins and minerals, and homoeopathic products.
► TGA Consultation, 31 March 2017.Closed 12 May 2017.
The TGA has also informed the public about a new notifications process to be introduced for “very low risk” variations of registered medicines.
► Notifications process: requests to vary registered medicines where quality, safety and efficacy are not affected. Version 1.0, June 2017 (pending legislative amendments). 8 June 2017.
C a n a d a – Health Canada has proposed to permit emergency imports of bulk quantities of foreign-authorized medications, i.e. medications that have been authorized in the U.S., the EU or Switzerland, but not yet in Canada. The permits would be valid for one year, renewable. The most immediate need is expected to be for medicines to treat opioid use disorder.
► Health Canada News release, 21 April 2017.Comment period: 15 days.
A u s t r a l i a – The TGA has invited comments from interested parties on its proposed provisional approval registration process and post-market requirements for provisionally registered medicines. This follows a recommendation from the Review of Medicines and Medical Devices regulation to
implement expedited pathways in Australia. A consultation paper on the proposed eligibility criteria and designation process for the two proposed expedited pathways (priority review and provisional approval) was published by the TGA in October 2016.
TGA Consultation, 20 March 2017. Closed 1 May 2017.
A u s t r a l i a – The TGA has sought comments on its proposed changes that will strengthen safety monitoring for medicines available in Australia. The changes will apply to medicines only and will be implemented progressively from late 2017 onward.
TGA Consultation, 20 March 2017.Closed 1 May 2017.
I n d i a – The Ministry of Health and Family Welfare has launched a public consultation on the development of an electronic platform for tracking the supply of medicines in India. All manufacturers, wholesalers and distributors will be required to register on this portal and enter batch numbers, quantities supplied and expiry dates of all medicines supplied, sold or returned to the manufacturers. This tracking system is intended to complement the bar coding, which has been introduced for export purposes.
► Ministry of Health and Family Welfare. Public Notice X.11035/1010/2016-DRS, 16 March, 2017.
C a n a d a – The Government of Canada has proposed amendments to the Protecting Canadians from Unsafe Drugs Act (Vanessa’s Law). Under the amended regulations, Health Canada would be able to require companies to conduct new tests and studies. Companies would also have to notify Health Canada of any drug safety-related actions required by a regulator in another jurisdiction.
► Health Canada Statement, 21 April 2017.
Regulatory news WHO Drug Information Vol. 31, No. 2, 2017
186
Approved
Naldemedine for constipation caused by opioidsProduct name: Symproic®Dosage form: TabletClass: Opioid antagonistApproval: FDAUse: Treatment of opioid-induced constipation in
adults with chronic non-cancer pain.Benefits: Increase in number of spontaneous
bowel movements, compared to placebo. ► FDA. Drug trials snapshot. Symproic.
Cerliponase alfa for a rare neurodegenerative disorder in childrenProduct name: Brineura®Dosage form: Solution for intracerebroventricular
infusionClass: Enzyme replacement therapy; ATC code:
A16ABApproval: EMA (marketing authorization under
exceptional circumstances, accelerated assessment; orphan designation) FDA (priority review, breakthrough therapy; orphan drug designation)
Use: Treatment of neuronal ceroid lipofuscinosis type 2 (CLN2) disease in children.
Benefits: Ability to slow the progression of motor and language decline.
Note: This is the first EMA- and FDA-approved medicine for CLN2 disease, also known as tripeptidyl peptidase 1 (TPP1) deficiency, a very rare neurodegenerative genetic disorder that usually leads to the death of the child between the ages of eight and twelve years.
► EMA Press release, 21 April 2017.FDA News release, 27 April 2017.
Nonacog beta pegol for haemophilia BProduct name: Refixia®Dosage form: Powder and solvent for solution for
injection
Class: Recombinant coagulation factor IX; ATC code: B02BD
Approval: EMA (orphan designation)Use: Treatment and prophylaxis of bleeding in
patients 12 years and above with haemophilia. Benefits: Ability to prevent and treat bleeding in
patients with haemophilia B. ► EMA CHMP opinion, 23 March 2017.
Dupilumab for atopic dermatitisProduct name: Dupixent®Dosage form: Subcutaneous injectionClass: Antibody binding to the interleukin-4
receptor alpha subunit (IL-4Ra) protein; ATC code (temporary): D11AH05
Approval: FDA (priority review, breakthrough therapy)
Use: Treatment of adults with moderate to severe eczema (atopic dermatitis) not controlled adequately by topical therapies. Can be used with or without topical corticosteroids.
Benefits: Greater efficacy than placebo to clear skin and reduce itch.
► FDA News release, 28 March 2017.
Abaloparatide for osteoporosisProduct name: Tymlos®Dosage form: Injection for subcutaneous useClass: Human parathyroid hormone related
peptide analogApproval: FDAUse: Treatment of postmenopausal women with
osteoporosis at high risk of fractures.Benefits: Ability to reduce the risk of vertebral
and nonvertebral fractures.Safety information: A dose-dependent increase
in the incidence of osteosarcoma was found in animal studies. This medicine is not recommended in patients at increased risk for osteosarcoma. Cumulative use with other parathyroid hormone analogs for more than

187
WHO Drug Information Vol. 31, No. 2, 2017 Regulatory news
Approved
two years during a patient’s lifetime is not recommended.
► FDA Prescribing information, revised 04/2017. Available from: Drugs@FDA: FDA Approved Drug Products.
Inotuzumab ozogamicin for acute lymphoblastic leukaemiaProduct name: Besponsa®Dosage form: Powder for concentrate for solution
for infusionClass: Specific humanised immunoglobulin
class G subtype 4 (IgG4) antibody; ATC code: L01XC26
Approval: EMA (orphan designation)Use: Treatment of adults with relapsed or
refractory CD22-positive B cell precursor acute lymphoblastic leukaemia.
Benefits: Ability to increase the proportion of patients who have complete remission and molecular remission and to delay the progression of disease.
► EMA/CHMP Opinion, 21 April 2017.
Durvalumab for bladder cancerProduct name: Imfinzi®Dosage form: Injection for intravenous useClass: Programmed death-ligand
1 (PD-L1) blocking antibody; ATC code (temporary): L01XC28
Approval: FDA (accelerated approval, priority review, breakthrough therapy)
Use: Treatment of patients with locally advanced or metastatic urothelial carcinoma not responding, or no longer responding, to platinum-containing chemotherapy.
Benefits: Ability to shrink tumours in approx. 17% of patients treated.
► FDA web post, 1 May 2017.
Midostaurin for acute myeloid leukaemiaProduct name: Rydapt®Dosage form: CapsulesClass: Kinase inhibitor; ATC code: L01XE39
Approval: FDA, fast track designation (for the AML indication), priority review (for the mastocytosis indication), breakthrough therapy
Uses: – Treatment of newly diagnosed, FLT3
mutation-positive acute myeloid leukaemia (AML), in combination with standard cytarabine and daunorubicin induction and cytarabine consolidation.
– Treatment of aggressive systemic mastocytosis, systemic mastocytosis with associated haematological neoplasm, or mast cell leukaemia.
Benefits: In AML: longer survival and longer progression-free survival period than with chemotherapy alone (a specific median survival rate could not be reliably estimated).
► FDA News release, 28 April 2017.
Ribociclib for breast cancerProduct name: Kisqali®Dosage form: TabletsClass: Cyclin-dependent kinase 4/6 inhibitor;
ATC code (temporary): L01XE42Approval: FDA (breakthrough therapy, priority
review)Use: In combination with an aromatase inhibitor
as initial endocrine-based therapy, treatment of postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced or metastatic breast cancer.
Benefits: Improvement in investigator-assessed progression-free survival. Overall survival data are immature.
Safety information: Ribociclib can cause QT interval prolongation, hepatobiliary toxicity, neutropenia, and harm to an unborn child.
► FDA. Approved drugs. Ribociclib (Kisqali). 13 March 2017.
Brigatinib for certain lung cancersProduct name: Alunbrig®Dosage form: Tablets

Regulatory news WHO Drug Information Vol. 31, No. 2, 2017
188
Approved
Class: Tyrosine kinase inhibitor; ATC code (temporary): L01XE43
Approval: FDA (accelerated approval)Use: Treatment of patients with anaplastic
lymphoma kinase (ALK)-positive metastatic non-small cell lung cancer who have progressed on or are intolerant to crizotinib.
Benefits: Ability to shrink tumours in approximately half of the patients enrolled in the clinical study.
► FDA Prescribing information, April 2017. Available from: Drugs@FDA: FDA Approved Drug Products
Niraparib for certain recurrent cancersProduct name: Zejula®Dosage form: CapsulesClass: Poly ADP-ribose polymerase (PARP)
inhibitor; ATC code (temporary): L01XX54Approval: FDA (fast-track, priority review,
breakthrough therapy; orphan drug designation)
Use: Maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube or primary peritoneal cancer, whose tumours have completely or partially shrunk in response to platinum-based chemotherapy.
Benefits: Longer progression-free survival than with placebo.
► FDA News release, 27 March 2017.
Ocrelizumab for multiple sclerosisProduct name: Ocrevus®Dosage form: Intravenous infusionClass: Selective immunosuppressant; ATC code:
L04AA36Approval: FDA (breakthrough therapy, fast-track
designation, priority review)Use: Treatment of adults with relapsing forms
of multiple sclerosis and primary progressive multiple sclerosis.
Benefits: Longer time to the worsening of disability, compared to placebo.
Safety information: Ocrelizumab should not be given to patients with active hepatitis B virus infection.
Notes: This is the first FDA-approved treatment of primary progressive multiple sclerosis. Ocrelizumab is also under review by EMA (1) and Health Canada. (2)
► FDA News release, 29 March 2017.(1) EMA. Applications for new human medicines under evaluation by the Committee for Medicinal Products for Human Use. March 2017.(2) Health Canada. Drug and health product submissions under review (SUR).
Sarilumab for rheumatoid arthritisProduct name: Kevzara®Dosage form: Solution for subcutaneous injectionClass: interleukin inhibitor, specific human
monoclonal antibody (IgG1 subtype); ATC code: L04AC14
Approval: EMAUse: Treatment of moderately to severely active
rheumatoid arthritis in adult patients who have responded inadequately to, or who are intolerant to one or more disease-modifying anti rheumatic drugs (DMARDs).
Benefits: Ability to reduce the signs and symptoms of rheumatoid arthritis and to improve physical function.
► EMA/CHMP Opinion, 21 April 2017.
Avelumab for rare skin cancerProduct name: Bavencio®Dosage form: InjectionClass: Programmed death ligand-1 (PD-L1)
blocking antibodyApproval: FDA (accelerated approval, priority
review, breakthrough therapy; orphan designation)
Use: Treatment of adults and children 12 years and older with metastatic Merkel cell carcinoma.
Benefits: Ability to shrink tumours in approx. 33% of patients treated.
Note: This is the first FDA-approved treatment option for metastatic Merkel cell carcinoma.
► FDA News release, 23 March 2017.

189
WHO Drug Information Vol. 31, No. 2, 2017 Regulatory news
Approved
Autologous chondrocyte suspension to repair cartilage defects in the kneeProduct name: Spherox®Dosage form: Implant suspensionClass: Autologous chondrocytes;
ATC code: M09AX02Approval: EMAUse: Repair of certain cartilage defects of the
knee.Benefits: Ability to repair symptomatic cartilage
defects in the knee with defect sizes up to 10 cm2.
Notes: This is an advanced therapy medicinal product in the form of a suspension containing 10–70 three-dimensional spheroids/cm², each composed of a cartilage matrix with the patient’s own chondrocytes, isolated from healthy cartilage and cultured in vitro. The CHMP positive opinion was based on an assessment by the Committee for Advanced Therapies.
► EMA Press release, 19 May 2017.
Edaravone for amyotrophic lateral sclerosisProduct name: Radicava®Dosage form: Intravenous infusionClass: Free radical scavengerApproval: FDA (orphan drug designation)Use: Treatment of patients with amyotrophic
lateral sclerosis (ALS), also known as Lou Gehrig’s disease.
Benefits: Ability to slow the decline of daily functioning.
Notes: This is the second FDA-approved medicine for ALS, after riluzole, which gained FDA approval in 1995. Edaravone was previously approved in Japan.
► FDA News release, 5 May 2017.
Valbenazine for tardive dyskinesiaProduct name: Ingrezza®Dosage form: CapsulesClass: Vesicular monoamine transporter 2
(VMAT2) inhibitor
Approval: FDA (fast track, priority review, breakthrough therapy)
Use: Treatment of adult patients with tardive dyskinesia, a neurological disorder characterized by repetitive involuntary movements seen in some patients treated with certain medications.
Benefits: Ability to reduce the severity of involuntary movements, compared with placebo.
► FDA News release, 11 April 2017.
Deutetrabenazine for choreaProduct name: Austedo®Dosage form: TabletsClass: Vesicular monoamine transporter 2
(VMAT2) inhibitorApproval: FDAUse: Treatment of chorea associated with
Huntington’s disease.Benefits: Ability to reduce chorea in Huntington’s
disease patients.Safety information: This medicine increases the
risk of depression and suicidal thoughts. It is contraindicated in patients who are suicidal, and in patients with untreated or inadequately treated depression.
► FDA. Drug trials snapshots: Austedo.
Triple combination for COPDProduct name: Trimbow®Dosage form: Solution delivered by pressurized
metered dose inhaler Class: Triple combination of an inhaled
glucocorticoid (beclometasone dipropionate), a long-acting beta-2 receptor agonist (formoterol fumarate dihydrate) and a long-acting muscarinic antagonist (glycopyrronium bromide). ATC code: R03AL09
Approval: EMAUse: Maintenance treatment of moderate to
severe chronic obstructive pulmonary disease (COPD).
Benefits: The product can relieve and prevent symptoms such as shortness of breath,

Regulatory news WHO Drug Information Vol. 31, No. 2, 2017
190
Approved
wheezing and cough and reduce exacerbations of COPD symptoms.
► EMA/CHMP Opinion, 18 May 2017.
Cenegermin for a rare eye disease Product name: Oxervate®Dosage form: Eye drops solutionClass: Recombinant form of human nerve growth
factorApproval: EMA (accelerated assessment; orphan
designation)Use: Treatment of moderate or severe
neurotrophic keratitis in adultsBenefits: Cenegermin can stimulate corneal
healing and restore eye surface integrity in patients with neurotrophic keratitis suffering from persistent epithelial defects or corneal ulcers.
Notes: Neurotrophic keratitis is a rare eye disease that can lead to loss of sight. It is caused by damage to the trigeminal nerve, resulting in reduced sensation in the cornea and reduced production of substances that play a role in repairing damage and ensuring survival of cornea cells.(1)
Patients in the United Kingdom will get early access to the product under the MHRA’s early access to medicine (EAMS) scheme.(2)
► (1) EMA Press release, 19 May 2017.(2) MHRA. Decision, 7 June 2017.
Biosimilars
Insulin lisproProduct name: Insulin lispro Sanofi®Reference product: Humalog®Approval: EMAUse: Treatment of diabetes mellitus.
► EMA/CHMP Opinion, 18 May 2017.
Rituximab
Product name: Rixathon®Reference product: Mabthera®Approval: EMA
Use: treatment of non-Hodgkin’s lymphoma, chronic lymphocytic leukaemia, rheumatoid arthritis, granulomatosis with polyangiitis and microscopic polyangiitis.
► EMA/CHMP Opinion, 21 April 2017.
Product name: Riximyo®Reference product: Mabthera®Approval: EMAUse: Treatment of non-Hodgkin’s lymphoma,
rheumatoid arthritis, granulomatosis with polyangiitis, and microscopic polyangiitis.
► EMA/CHMP Opinion, 21 April 2017.
Product name: Blitzima®Reference product: Mabthera®Approval: EMAUse: Treatment of non-Hodgkin’s lymphoma,
chronic lymphocytic leukaemia, granulomatosis with polyangiitis and microscopic polyangiitis.
► EMA/CHMP Opinion, 18 May 2017.
Product name: Tuxella ®Reference product: Mabthera®Approval: EMAUse: Treatment of non-Hodgkin’s lymphoma,
chronic lymphocytic leukaemia, granulomatosis with polyangiitis and microscopic polyangiitis
► EMA/CHMP opinion, 18 May 2017.
Product name: Ritemvia ®Reference product: Mabthera®Approval: EMAUse: the treatment of non-Hodgkin’s lymphoma,
granulomatosis with polyangiitis and microscopic polyangiitis.
► EMA/CHMP opinion, 18 May 2017.
EtanerceptProduct name: Erelzi®Reference product: Enbrel®Approval: EMAUse: Treatment of rheumatoid arthritis, juvenile
idiopathic arthritis, psoriatic arthritis, axial

191
WHO Drug Information Vol. 31, No. 2, 2017 Regulatory news
Approved
spondyloarthritis, plaque psoriasis and paediatric plaque psoriasis.
► EMA/CHMP Opinion, 21 April 2017.
InfliximabProduct name: Renflexis® (infliximab-abda)Reference product: Remicade®Approval: FDAUse: Treatment of Crohn’s Disease, paediatric
Crohn’s disease, ulcerative colitis, rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis and plaque psoriasis.
► Drugs@FDA: FDA Approved Drug Products. Biologic License Application (BLA): 761054.
Extensions of indications
Maraviroc for use in children Product name: Celsentri®Approval: EMANewly approved use: Treatment of adolescents
and children of 2 years of age and older and weighing at least 10 kg with certain types of HIV-1 infection.
► EMA/CHMP Summary of opinion, 21 April 2017.
Sofosbuvir, ledipasvir and sofosbuvir for use in children and adolescentsProduct name:
Sofosbuvir: Sovaldi® Ledipasvir/sofosbuvir: Harvoni®
Approval: FDANewly approved use: Treatment of certain types
of hepatitis C virus infection in children 12 years of age and older or weighing at least 35 kg.
► FDA News release, 7 April 2017.
Pembrolizumab for tumours with a certain biomarkerProduct name: Keytruda®Approval: FDA (accelerated approval, priority
review)
Newly approved use: Treatment of adults and children with unresectable or metastatic tumours having a biomarker referred to as microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR), including: – solid tumours that have progressed following prior treatment and who have no satisfactory alternative treatment options and –colorectal cancer that has progressed following treatment with certain chemotherapy drugs.
Note: This is the first FDA approval based on a tumour’s biomarker without regard to the tumour’s original location.
► FDA News release, 23 May 2017.
Regorafenib for liver cancerProduct name: Stivarga®Approval: FDA (priority review; orphan drug
designation)Newly approved use: Treatment of patients with
hepatocellular carcinoma who have been previously treated with sorafenib.
Note: This is the first FDA-approved treatment for liver cancer in almost a decade.
► FDA News release, 27 April 2017.
Tocilizumab for giant cell arteritisProduct name: Actemra®Approval: FDA (breakthrough therapy, priority
review)Newly approved use: Treatment of giant cell
arteritis, a form of vasculitis impeding adequate blood flow in the inflamed arteries.
Note: Tocilizumab was previously FDA-approved for certain types of arthritis. The newly approved indication provides the first FDA-approved therapy specific to this type of vasculitis.
► FDA News release, 22 May 2017.
Ivacaftor to treat additional mutations of cystic fibrosis Product name: Kalydeco®Approval: FDA

Regulatory news WHO Drug Information Vol. 31, No. 2, 2017
192
Extensions of indications
Newly approved use: Treatment of additional gene mutations in patients with cystic fibrosis.
Note: The approval triples the number of rare gene mutations that the drug can treat, from 10 to 33. The agency based its decision on the results of laboratory testing, in conjunction with evidence from earlier human clinical trials. This pathway was used because many cystic fibrosis mutations have such small patient populations that clinical trial studies are not feasible.
► FDA News release, 17 May 2017.
Early access
Glecaprevir/pibrentasvir for chronic hepatitis C infection Dosage form: Film-coated tabletsClass: Fixed-dose combination of two direct-
acting antiviralsApproval: MHRA Early Access to Medicines
Scheme (EAMS)Use: Treatment of chronic hepatitis C virus
(HCV) infection in adults. In the context of the EAMS, use of glecaprevir/pibrentasvir is restricted to certain patient groups.
Benefits: High cure rates of hepatitis C infection across HCV genotypes in patients with or without cirrhosis.
► MHRA EAMS. Decision, 10 May 2017.
EU ruling
Paracetamol/ibuprofen fixed-dose combinationThe EMA’s Committee for Medicinal Products for Human Use (CHMP) has concluded that marketing authorization can be granted for the analgesic fixed-dose combination paracetamol/ibuprofen 500mg/150mg film-coated tablets in relevant EU member states.
The matter had been referred to the CHMP because no agreement could be reached during joint assessment of the application under the EMA’s “Decentralized procedure”. The CHMP
concluded that this combination is more effective than the individual components, while its safety profile is similar. Using the combination may avoid having to use stronger painkillers such as opioids, which have risks of abuse and misuse. Post-marketing data show that similar combinations have not led to significant long-term use (which is not authorized for this product) or increased safety concerns.
► EMA. Questions and answers on Paracetamol/ibuprofen 500mg/150mg film-coated tablets and associated names (tablets containing 500 mg paracetamol and 150 mg ibuprofen). 19 May 2017. å

193
WHO Drug Information Vol. 31, No. 2, 2017
Publications and events
Access to medical products
Fair Pricing ForumA m s t e r d a m – The first Fair Pricing Forum was held in Amsterdam, the Netherlands, on 11 May 2017. The main objective of this Forum was to discuss options for a fairer pricing system that is sustainable for both health systems and innovation. The event was an initiative of WHO and was organized in collaboration with the Dutch Ministry of Health, Welfare and Sport. About 200 stakeholders from countries around the world came together to explore options to remedy essential medicines shortages that may be due to low profit margins, expand networks for exchange of experience, and identify research gaps specific to the current innovation and pricing system.
Background information about the challenges of the current system of setting prices for medicines is found in the report of the WHO Advisory Group meeting held in November 2016 in preparation for the event.
► WHO Essential medicines and health products. Fair pricing of medicines [webpage].Fair Pricing Forum. Informal Advisory Group Meeting report. Geneva: WHO, March 2017.
Information guide on biosimilarsB r u s s e l s – The EMA and the European Commission (EC) have published a new information guide for healthcare professionals, providing reference information on the science and regulation underpinning the use of biosimilars.(1) It complements earlier EC publications on
biosimilars, including a guide for patients and a consensus information paper.
The guide was launched at the stakeholder conference on biosimilar medicines held in Brussels on 5 May 2017. The event was attended by representatives of patients, healthcare professionals, regulatory authorities, payers and the pharmaceutical industry. An updated report on the impact of biosimilar competition in Europe was also released at the conference.(2)
► EMA Press release, 5 May 2017.European Commission. Third stakeholder conference on biosimilar medicines [webpage].
WHO to pilot prequalification of biosimilarsG e n e v a – WHO has announced that it will launch a pilot project for prequalification of two biosimilar cancer medicines, rituximab and trastuzumab, in 2017. An invitation for expression of interest and submission of applications by manufacturers will be published in September. The WHO prequalification list is used by a wide range of national and international entities and thus promotes competitive pricing.
The decision to launch the pilot follows a two-day meeting between WHO, national regulators, pharmaceutical industry groups, patient and civil society groups, payers and policymakers. WHO also plans to explore options for prequalifying insulin.
To support the biosimilars prequalification pilot, WHO will review its 2009 Guidelines on the evaluation of similar biotherapeutic products. Furthermore the Organization will advocate for greater awareness of the benefits
Publications and events WHO Drug Information Vol. 31, No. 2, 2017
194
and risks of biosimilars and will support the development of sustainable price-setting strategies for all biotherapeutics.
► WHO News release, 4 May 2017.
Updated Essential Medicines List G e n e v a – WHO has published the 2017 update of its Essential Medicines Lists (EML) for adults and children. The list includes new advice on the use of antibiotics and 55 additional medicines, bringing the total to 433 medicines deemed essential for addressing the most important public health needs. The updates were recommended by the WHO Expert Committee on the Selection and Use of Essential Medicines at its 21st meeting, held on 27–31 March 2017.
For the first time, antibiotics used to treat 21 of the most common general infections have been grouped into three categories: “Access” (available at all times for a wide range of infections), “Watch” (first- or second-line treatments for a small number of infections) and “Reserve” (last-resort options for use in the most severe circumstances). The advice supports WHO’s Global action plan on antimicrobial resistance.
Furthermore, the following medicines: were added to the EML:• 10 antibiotics for adults and 12 for children• dasatinib and nilotinib for oral treatment
of chronic myeloid leukaemia that has become resistant to standard treatment;
• sofosbuvir + velpatasvir as the first combination therapy to treat all six types of hepatitis C;
• dolutegravir for HIV infection; • HIV pre-exposure prophylaxis (PrEP)
with tenofovir alone, or in combination with emtricitabine or lamivudine;
• delamanid for children and adolescents, and clofazimine for children and adults with multidrug-resistant tuberculosis;
• child-friendly fixed-dose combination formulations of first-line anti-tuberculosis medicines,
• two artemisinin-based combination therapies (pyronaridine+artesunate and dihydroartemisinine+piperaquine) and a rectal artesunate formulation for young children, for the treatment of malaria: and and
• fentanyl skin patches and methadone for pain relief in cancer patients.(1)
The Expert Committee further recommended to develop an Essential Diagnostics List (2).
► (1) WHO News release, 6 June 2017.WHO Model List of Essential Medicines. 20th List (March 2017).WHO Model List of Essential Medicines for Children. 6th List (March 2017).(2) WHO-EMP News, 15 June 2017.
MPP licence for investigational hepatitis C medicineA m s t e r d a m – The Medicines Patent Pool (MPP) and the Egyptian company Pharco Pharmaceuticals have signed a licence for the investigational medicine ravidasvir, a direct-acting antiviral (DAA) with the potential of working across all six major hepatitis C genotypes.
The new MPP licence expands the geographic scope of an earlier licence signed by the Drugs for Neglected Diseases initiative (DNDi) and Presidio, the original developer of ravidasvir. Combined, the MPP and DNDi agreements would benefit an area which is home to 85% of people living with hepatitis C in low- and middle-income countries.
► MPP Press release, 21 April 2017.

195
WHO Drug Information Vol. 31, No. 2, 2017 Publications and events
Regulatory reforms in MexicoA recent publication describes the implementation and impact of a multi-faceted series of regulatory and legal reforms instituted by the Government of Mexico and the national medicines regulatory agency, COFEPRIS. The reforms aimed to facilitate the implementation of a new national access to medicines policy and to align the regulatory system with international standards. They encompassed administrative processes, clinical trials oversight, reliance on market authorization information and reports of other trusted regulators, and validation of activities by the Pan American Health Organization (PAHO) and WHO.
The paper shows that the reforms have increased the availability and affordability of safe, effective, quality medicines in the private and public sectors, and have facilitated expansion of the Mexican pharmaceutical industry. The regulatory optimization approach undertaken by Mexico could be a useful model for other countries that wish to facilitate access to needed quality medicines while encouraging local economic development.
► Arriola Peñalosa MA, Cavazos Cepeda R, Alanis Garza M, Lumpkin MM. Optimized Medical Product Regulation in Mexico: A Win-Win for Public and Economic Health. Therapeutic Innovation & Regulatory Science. Published online 5 May 2017; DOI: https://doi.org/10.1177/2168479017701503.
Access to Vaccines Index 2017A m s t e r d a m – The Access to Medicines Foundation has published its first Access to Vaccines Index, the first publically available tool that maps how vaccine companies are responding to global calls to increase access to vaccines. The Index assesses eight key vaccine suppliers, and looks at their efforts to develop, manufacture and supply
preventive vaccines for 69 high priority diseases across 107 high-need countries. The Index finds that the companies evaluated do this in a variety of ways depending on their diverse pipelines, portfolios and revenues.
The Access to Medicine Foundation published its first benchmark of industry activity in the 2008 Access to Medicine Index, which is now in its fifth iteration. The Foundation is also developing the first Antimicrobial Resistance Benchmark.
► Access to Medicine Foundation. News release, 6 March 2017.
Reporting of clinical trial resultsGeneva - Some of the world’s largest funders of medical research and international non-governmental organizations have agreed on new standards that will require all clinical trials they fund or support to be registered, and the results to be disclosed publicly. New policies will be developed and implemented within the next 12 months. Most of these trials and their results will be accessible via WHO’s International Clinical Trials Registry Platform.
Today, about half of all clinical trials go unreported, often because the results are negative. This leaves an incomplete and potentially misleading picture of the risks and benefits of vaccines, medicines and medical devices and can lead to use of suboptimal or even harmful products. The agreement means that the ethical principles laid down in the 2015 WHO position on public disclosure of results from clinical trials, which builds on the World Medical Association’s 2013 Declaration of Helsinki, will now be enforced in thousands of trials every year.
► WHO News release, 18 May 2017. WHO. International Clinical Trials Registry Platform (ICTRP) [website]. http://www.who.int/ictrp/en/

Publications and events WHO Drug Information Vol. 31, No. 2, 2017
196
Safety evaluation and monitoring
Confirmatory clinical studies lackingThe outcomes of a systematic review show that post-market studies are not always conducted to confirm the expected benefits of medicines that gained regulatory approval based on limited evidence. The review characterized the prospective controlled clinical studies for novel drugs that were first approved by the U.S. FDA between 2005 and 2015 on the basis of limited evidence. It included 117 products approved on the basis of a single pivotal trial, pivotal trials that used surrogate markers of disease as primary endpoints, or both. The review found that the quantity and quality of post-approval clinical evidence varied substantially for these products, with few controlled studies published after approval that confirmed efficacy using clinical outcomes for the original FDA-approved indication.(1)
► Pease AM, Krumholz HM, Downing NS. Postapproval studies of drugs initially approved by the FDA on the basis of limited evidence: systematic review. BMJ 2017;357:j1680.
Importance of monitoring new drugsA third of FDA-approved medicines have significant post-market safety events. In a recent study 71 of 222 novel therapeutics approved by the FDA in the period from 2001-2010 were affected by one or more significant event (withdrawal, “boxed warning” and/or safety communication). Products that gained accelerated approval were twice as likely to have postmarket safety events than other products. Safety events were also found to be more likely for biologicals, medicines to treat psychiatric conditions, and products approved near the regulatory deadline for approval.
These findings highlight the importance of continuous safety monitoring of medicinal products throughout their life cycle.
► Downing NS, Shah ND, Aminawung JA et al. Postmarket Safety Events Among Novel Therapeutics Approved by the US Food and Drug Administration Between 2001 and 2010. JAMA. 2017;317(18):1854-1863. doi:10.1001/jama.2017.5150.
Medicines supply and use
New industry alliance to curb antimicrobial resistanceB e r l i n – The International Federation of Pharmaceutical Manufacturers & Associations (IFPMA) has announced the launch of the AMR Industry Alliance, which brings together research-based companies to drive and measure industry progress to curb antimicrobial resistance (AMR). The announcement was made at the B20 Health Conference in Berlin. The Alliance will ensure that signatories collectively deliver on the commitments made in the the Industry Declaration on AMR signed at the World Economic Forum in Davos in January 2016 and the AMR Roadmap. A reporting mechanism will be developed to track progress, identify gaps and set targets for the future.
► IFPMA News release, 18 May 2017.
Antibiotics consumption in eastern Europe and central AsiaA new report released by the WHO Regional Office for Europe sheds light on antibiotic consumption in eastern European and central Asian countries. The data were gathered through the WHO Antimicrobial Medicines Consumption (AMC) Network. and include information from a number of non-EU countries.
197
WHO Drug Information Vol. 31, No. 2, 2017 Publications and events
The WHO AMC Network was established by the WHO Regional Office for Europe in 2011 to assist countries in setting up or strengthening national AMC surveillance and to contribute to region-wide AMC surveillance.
► WHO Regional Office for Europe. News, 1 May 2017.
Off-label use of medicines in EuropeA new study describes the complex field of off-label use of medicinal products in the EU, i.e. the use of the products outside the terms approved as part of the marketing authorization under which a product can be used safely and effectively.
The study was conducted by the Netherlands institute for health services research (NIVEL), the Dutch National Institute for Public Health and the Environment (RIVM) and the European Public Health Alliance (epha) for the European Commission. Applying a wide range of methods, it provides information on the prevalence and incidence of off-label use and its drivers. It investigates the balance between the benefits and risks for patients and describes the national frameworks that govern the off-label use of medicinal products in EU Member States. The study shows how authorities have addressed the issue and how patients, healthcare professionals and industry react to this.
► Weda M, Hoebert J, Vervloet M et al. Study on off-label use of medicinal products in the European Union. Utrecht, Bilthoven: NIVEL, epha, RIVM; February 2017.
Combating medication errorsG e n e v a – WHO has launched a global initiative to reduce severe, avoidable medication-associated harm by 50% over
the next five years. The Global Patient Safety Challenge on Medication Safety aims to improve the ways in which medicines are prescribed and distributed in health systems, and to increase awareness among patients about the risks associated with the improper use of medication.
Medication errors cause at least one death every day and injure approximately 1.3 million people annually in the United States of America alone. While low- and middle-income countries are estimated to have similar rates of medication-related adverse events to high-income countries, the impact is about twice as much in terms of the number of healthy life years lost. Globally, the cost associated with medication errors has been estimated at US$ 42 billion annually or almost 1% of total global health expenditure. Many countries lack good data, which will be gathered as part of the initiative.
► WHO News release, 29 March 2017.
Toolkit to protect supply chainsThe Asia Pacific Economic Cooperation (APEC) has published an interactive PDF document to protect the medical product supply chains. (1). The document contains interactive links to recommended best practices and tools that can help to prevent and detect substandard and falsified medical products before they reach the consumer, and to efficiently respond to incidents. The document is the outcome of collaboration of ten work streams under the APEC Global Supply Chain Security and Integrity Roadmap project. It includes links to relevant tools and guidance provided by the WHO Member State mechanism on substandard/spurious/falsely-labelled/falsified/counterfeit medical products

Publications and events WHO Drug Information Vol. 31, No. 2, 2017
198
and the WHO Global Surveillance and Monitoring System.
► The APEC Harmonization Centre. News, 31 March 2017. APEC. Supply chain security toolkit for medical products (PDF, 6.6 MB).
Disease updates
Poliomyelitis: Towards eradicationG e n e v a , B r a z z a v i l l e , N e w Yo r k , D a k a r – The largest-ever synchronized vaccination campaign of its kind was conducted in 13 countries across west and central Africa to tackle the threat of polio. All children under five years of age in Benin, Cameroon, Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of Congo, Guinea, Liberia, Mali, Mauritania, Niger, Nigeria and Sierra Leone – were immunized with bivalent oral polio vaccine (bOPV).
The security-compromised areas in Borno state, north-eastern Nigeria, is widely considered to be the last remaining polio reservoir. Due to its epidemic-prone nature the virus could easily spread to under-protected areas of neighbouring countries. With the strong commitment of Africa’s leaders polio could now be eradicated.(1)
In May 2017 the WHO Emergency Committee under the International Health Regulations concluded that polio remains a public health emergency of international concern, but that the world is now closer to polio eradication than ever before. The Committee’s temporary recommendations will be maintained for another 3 months, with some changes to the categories of countries subject to the recommendations.(2)
► (1) Joint UNICEF/WHO news release, 23 March 2017.(2) WHO Statement, 2 May 2017.
Depression: Leading cause of disabilityG e n e v a – WHO has released its new estimates of the prevalence of depression and other mental disorders at the global and regional level, together with data concerning the consequences of these disorders in terms of lost health. More than 300 million people were living with depression in 2015, an increase of more than 18% since 2005.
On average, only 3% of government health budgets are invested in mental health. Fewer than half of people affected globally (and fewer than 10% in many countries) receive appropriate treatment. This is mainly because of a lack of resources and trained health care providers, and because of social stigma associated with mental disorders.
Depression increases the risk of substance use disorders and diseases such as diabetes and heart disease. Conversely, people with these conditions have a higher risk of depression. According to a WHO-led study, low levels of recognition and access to care for depression and anxiety cause economic losses of a trillion US dollars every year in total to households, employers and governments.
► WHO News release, 30 March 2017.WHO. Depression and Other Common Mental Disorders. Global Health Estimates. Geneva: World Health Organization, 2017.
Neglected tropical diseases: Remarkable achievementsG e n e v a – The fourth WHO report on neglected tropical diseases shows that there is tremendous progress in some areas, but also much remaining to do. The report was released at the Global Partners’ Meeting on Neglected Tropical Diseases (NTDs) on 19 April 2017. The event marked ten years of multi-stakeholder collaboration and the

199
WHO Drug Information Vol. 31, No. 2, 2017 Publications and events
5th anniversary of the WHO NTD Roadmap and the London Declaration.
Remarkable achievements have been made in tackling lymphatic filariasis, onchocerciasis, Guinea-worm disease, African human trypanosomiasis, trachoma, visceral leishmaniasis and rabies. The report outlines four main areas that remain to be addressed. Firstly there is a need for investments to develop innovative disease prevention and management interventions. Secondly, vector control needs to be strengthened globally as it can prevent the transmission of many NTDs. A response plan for 2017–2030 was welcomed by the delegates at the Seventieth World Health Assembly. The WHO Prequalification team will play a crucial role in assessing the quality of long-lasting insecticide-treated bed nets, indoor residual spraying, space sprays and larvicides. Thirdly, public health measures must be intensified to combat zoonotic diseases, for example to ensure the availability of rabies vaccine meeting internationally accepted quality standards. Finally, safe water, sanitation and hygiene are critical in fighting NTDs, and measures to this effect will be part of the global plan.
► WHO News release, 19 April 2017.WHO. Integrating neglected tropical diseases into global health and development. 2017.
Malaria: Push for preventionG e n e v a , N a i r o b i – On World Malaria Day 2017 WHO has called for a faster scale-up of efforts to prevent malaria. Proven prevention approaches include insecticide-treated nets – which account for more than two thirds of cases prevented since 2001 – as well as indoor residual spraying with insecticides and preventive medicines for pregnant women, under-fives and infants. Across
the Sahel, WHO also recommends malaria chemoprevention during the rainy season. The uptake of some of these measures needs to be accelerated, especially in Africa, which bears 90% of the global malaria burden.(1)
B r a z z a v i l l e –The World Health Organization Regional Office for Africa (WHO/AFRO) has announced that Ghana, Kenya and Malawi will participate in a WHO-coordinated malaria vaccine pilot programme in selected areas, beginning in 2018. The vaccine under study, the RTS,S® vaccine, could be added to the current malaria control tools as a complementary preventive measure. The pilot will show whether the vaccine’s protective effect in children aged 5–17 months shown in Phase III testing can be replicated in real life. Specifically, the pilot programme will assess the feasibility of delivering the required four doses of RTS,S®, the vaccine’s potential role in reducing childhood deaths, and its safety in the context of routine use.(2)
► (1) WHO News, 24 April 2017.(2) WHO/AFRO. Press release, 24 April 2017.
Hepatitis: Need for urgent global responseG e n e v a – A new WHO report describes, for the first time, the global and regional estimates on viral hepatitis in 2015. The data set the baseline for tracking progress in implementing the new global strategy endorsed by the World Health Assembly in 2016. The report highlights the urgency of closing the gaps in access to life-saving testing and treatment.
The report focuses on hepatitis B and C, which cause 96% of overall hepatitis mortality. An estimated 325 million people worldwide are living with chronic hepatitis B

Publications and events WHO Drug Information Vol. 31, No. 2, 2017
200
or C virus infection. Mortality is increasing, with 1.34 million deaths in 2015.
For hepatitis B virus (HBV) new infections are falling thanks to increased vaccination coverage among children. HBV infection requires lifelong treatment, WHO currently recommends tenofovir for this purpose.
For hepatitis C virus (HCV) there is currently no vaccine available. Unsafe injections are considered to be the most common route of transmission. Approximately 1.75 million people were newly infected in 2015, bringing the global total of people living with HCV to 71 million. HCV infection can now be cured with the new direct-acting antiviral medicines (DAAs). Prices are falling but remain unaffordable in many countries.
► WHO News, 21 April 2017.WHO. Global Hepatitis Report, 2017.
Ebola: Response to new outbreakA new outbreak of Ebola virus disease has been reported from the Democratic Republic of the Congo (DRC). The outbreak appears to be geographically relatively limited. WHO and partners are supporting the Ministry of Health in all aspects of the response, including epidemiological investigation, surveillance, logistics and supplies, communications and community engagement.
Following the official confirmation of the outbreak, Gavi, the Vaccine Alliance has stated that it stands ready to support the Government of the DRC in bringing the epidemic under control. A 2016 agreement between Gavi and Merck, the developer of the Ebola vaccine rVSV-ZEBOV, ensures
that 300 000 vaccine doses are available for emergencies. The WHO and others will determine if and when deployment of vaccine in this outbreak is warranted.
► WHO Statement, 12 May 2017.Gavi, the Vaccine Alliance. Statement, 12 May 2017.
Upcoming events
Ireland to host 18th ICDRAD u b l i n – Ireland has been confirmed as the location for the next International Conference of Drug Regulatory Authorities (ICDRA). The Conference will take place in Dublin on 3–7 September 2018. This biennial WHO-organized event provides regulatory authorities with a unique forum to meet and discuss ways to strengthen global collaboration in the area of medicines’ regulation in order to improve the quality, safety and efficacy of medicines globally.
► HPRA News, 19 April 2018.WHO. International Conference of Drug Regulatory Authorities (ICDRA) [webpage].www.who.int/medicines/icdra/en/
Joint manufacturers meeting The 2017 joint UNICEF–UNFPA–WHO manufacturers meeting will take place in Copenhagen, Denmark, on 18–21 September 2017. The joint manufacturers meeting provides information for suppliers of medical products for use by UN agencies and other international organizations. WHO Prequalification website. Events.https://extranet.who.int/prequal/

201
WHO Drug Information Vol. 31, No. 2, 2017 Publications and events
WHO news
Seventieth World Health AssemblyG e n e v a – The Seventieth World Health Assembly was held in Geneva on 22–31 May 2017. Delegates made decisions on a wide range of health-related issues, including WHO’s response to health emergencies, the International Health Regulations and Pandemic Influenza Preparedness. Important decisions were also taken relating to polio, antimicrobial resistance, access to medicines and vaccines, the health of refugees and migrants, improving vector control, adolescent health and chemicals management, as well as on noncommunicable diseases (NCD), including dementia, cancer – including access to affordable treatment – and preparations for the 2018 UN General Assembly High-Level Meeting on NCDs.
The Assembly approved the programme budget for the biennial period 2018–19, which includes a 3% increase in assessed member contributions. In past years, voluntary contributions – which are often tied to specific activities – have overtaken assessed contributions, providing the majority of WHO’s income.
► WHO Media centre. Seventieth World Health Assembly. Available at: www.who.int/mediacentre/events/2017/wha70
New WHO Director-General electedG e n e v a – The Member States of WHO have elected Dr Tedros Adhanom Ghebreyesus as the Organization’s new Director-General. Prior to his election he served as Minister of Foreign Affairs of Ethiopia from 2012–2016 and as Minister of Health from 2005–2012. Dr Tedros has also served as chair of the Board of the Global Fund to Fight AIDS, Tuberculosis and Malaria; as chair of the
Roll Back Malaria (RBM) Partnership Board; and as co-chair of the Board of the Partnership for Maternal, Newborn and Child Health.
Dr Tedros Adhanom Ghebreyesus will succeed Dr Margaret Chan, who has been WHO’s Director-General since 1 January 2007. He will begin his five-year term on 1 July 2017.
► WHO News release, 23 May 2017.
Medicines prequalification updates1. The WHO Prequalification Team:
medicines (PQTm) has prequalified the following “firsts”: •First sofosbuvir active pharmaceutical
ingredient (API) – providing a quality source for generic manufacturers who wish to produce hepatitis C medicines.
•First ethionamid dispersible tablet, a child-friendly formulation to treat tuberculosis.(1)
2. The following revised invitations for evaluation of products (“EOIs”) have been published:•14th EOI for APIs; •4th EOI for anti-hepatitis products; •15th EOI for antimalarials; and•15th EOI for HIV-related products.(2)
3. PQT-m has clarified its expectations regarding bioequivalence (BE) studies. On a trial basis, PQTm will consider prior scientific justification from applicants for the use of the reference-scaled approach for AUC acceptance criteria in BE studies for highly variable APIs.(3)
► (1) WHO Prequalification of medicines. News. https://extranet.who.int/prequal/news(2) WHO Prequalification of medicines. FPPs & APIs Eligible for Prequalification (“EOIs”).(3) WHO/PQT: medicines. Guidance document, 9 June 2017. å

202
WHO Drug Information Vol. 31, No. 2, 2017
Consultation documentsTo receive draft monographs by email please contact Mrs Wendy Bonny ([email protected]), stating that you wish to be added to the electronic mailing list.
The International Pharmacopoeia
Mebendazole tablets(Mebendazoli compressi)
This is a draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/16.685, March 2017).
The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Category. Anthelmintic.
Storage. Mebendazole tablets should be kept in a tightly closed container.
Additional information. Strengths in the current WHO Model List of Essential Medicines (EML): 100 mg, 500 mg. Strengths in the current WHO EML for children: 100 mg, 500 mg.
RequirementsComply with the monograph for Tablets.
Definition. Mebendazole tablets contain not less than 90.0% and not more than 110.0% of the amount of mebendazole (C16H13N3O3) stated on the label.
Manufacture. The formulation, manufacturing process and product packaging of mebendazole tablets are designed and controlled so as to minimize the conversion of the polymorphic form of mebendazole from C to A. They ensure that, at any stage of the life cycle of the product, when tested by a suitable method such as infrared spectrometry (see Identity test A) or X-ray powder diffractometry, the mebendazole in the tablets is predominantly in the form of polymorph C.
203
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
Identity tests • Either tests A and B or tests A and C may be applied.A. To a quantity of the powdered tablets containing 0.05 g of Mebendazole add 20 mL of water
R, shake, filter and wash the residue with three quantities, each of 10 mL of water R. Dry the residue overnight under vacuum at room temperature and carry out the examination with the residue as described under 1.7 Spectrophotometry in the infrared region. The two infrared absorption bands at about 3405 cm-1 and 1720 cm-1 are concordant with those in the spectrum obtained from mebendazole RS (containing mebendazole polymorph C).
B. Carry out the test as described under 1.14.1 Thin-layer chromatography using silica gel R6 as the coating substance and a mixture of 85 volumes of dichloromethane R, 5 volumes of methanol R, 5 volumes of acetone R and 5 volumes of anhydrous formic acid R as the mobile phase. Apply separately to the plate 5 μL of each of the following solutions. For solution (A) add 2 mL of formic acid R to a quantity of the powdered tablets containing 20 mg of mebendazole and sonicate for about 5 minutes. Add 18 mL of acetone R, mix, filter and use the filtrate. For solution (B) dissolve 10 mg of mebendazole RS in 1 mL of formic acid R and shake. Add 9 mL of acetone R and mix. After removing the plate from the chromatographic chamber allow it to dry in air and examine the chromatogram in ultraviolet light (254 nm).
The principal spot obtained with solution (A) corresponds in position, appearance and intensity with that obtained with solution (B).
D. Carry out the test as described under 1.14.4 High-performance liquid chromatography using the conditions under “Assay”. The retention time of the principal peak in the chromatogram obtained with solution (1) corresponds to the retention time of the peak due to mebendazole obtained with solution (2).
Related substancesCarry out the test as described under 1.14.4 High-performance liquid chromatography using a stainless steel column (10 cm × 4.6 mm) packed with base-deactivated particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl groups (3 μm).1
Use the following conditions for gradient elution:
mobile phase A: 7.5 g/L solution of ammonium acetate R; mobile phase B: Acetonitrile R.
Time (min)
Mobile phase A (% v/v)
Mobile phase B (% v/v)
Comments
0–15 80 to 70 20 to 30 Linear gradient15–20 70 to 10 30 to 90 Linear gradient20–25 10 90 Isocratic25–26 10 to 80 90 to 20 Return to initial composition26–36 80 20 Isocratic re-equilibration
Operate with a flow rate of 1.2 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 250 nm. Maintain the column temperature at 40°C.1 A HYPERSIL BDS C18 column has been found suitable.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
204
Prepare as a solvent a mixture of 60 volumes of methanol R and 40 volumes of water R.
For solution (1) transfer a quantity of the powdered tablets, containing about 100 mg of mebendazole, accurately weighed, to a 100 mL volumetric flask. Add 30 mL of anhydrous formic acid R and sonicate for about 20 minutes. Dilute to volume with solvent mixture, mix and filter. For solution (2) dilute 1.0 mL of solution (1) to 100.0 mL with the solvent mixture. Dilute 5.0 mL of this solution to 20.0 mL with the solvent mixture. For solution (3) transfer 10 mg mebendazole RS to a 10 mL volumetric flask, add 5 mL of methanol R and 1 mL of sodium hydroxide (~40 g/L) TS solution, heat in a water bath at 60°C for 1 hour, cool to room temperature and adjust the solution to pH 7 with hydrochloric acid (~36.5 g/L) TS. Dilute with methanol R to volume and mix.
Inject 10 µL of solution (3). Use the chromatogram to identify the peak due to impurity A. The impurity is eluted at the relative retention of 0.4 with reference to mebendazole (retention time about 12 minutes).
The test is not valid unless in the chromatogram obtained with solution (3) the resolution between mebendazole and impurity A is at least 10.
Inject alternately 10 µL each of solution (1) and (2).
In the chromatogram obtained with solution (1):
• the area of any peak corresponding to impurity A is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (0.25%).
Dissolution For 100 mg tablets. Carry out the test as described under 5.5 Dissolution test for solid oral dosage forms using 900 mL of hydrochloric acid (~3.65 g/L) TS as the dissolution medium and rotating the paddle at 75 revolutions per minute. At 120 minutes withdraw a sample of 10 mL of the dissolution medium through an in-line filter. Allow the filtered sample to cool to room temperature. Dilute 5.0 mL of the filtrate to 50.0 mL with the dissolution medium.
Determine the content of mebendazole (C16H13N3O3) in the medium by 1.14.4 High-performance liquid chromatography using the conditions described under “Assay” and a suitable solution of mebendazole RS as a reference solution.
For each of the six tablets tested calculate the total amount of mebendazole (C16H13N3O3) in the medium using the declared content of C16H13N3O3 in mebendazole RS. The amount in solution for each tablet is not less than 60% (Q) of the amount declared on the label.
For 500 mg tablets. Carry out the test as described under 5.5 Dissolution test for solid oral dosage forms using 900 mL of a 1.0% solution of sodium dodecyl sulfate R in hydrochloric acid (~0.365 g/L) TS as the dissolution medium and rotating the paddle at 75 revolutions per minute. At 60 minutes withdraw a sample of 10 mL of the dissolution medium through an in-line filter. Allow the filtered sample to cool to room temperature. Dilute 1.0 mL of the filtrate to 50.0 mL with the dissolution medium.

205
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
Determine the content of mebendazole (C16H13N3O3) in the medium by 1.14.4 High-performance liquid chromatography using the conditions described under “Assay” and a suitable solution of mebendazole RS as a reference solution.
For each of the six tablets tested calculate the total amount of mebendazole (C16H13N3O3) in the medium using the declared content of C16H13N3O3 in mebendazole RS. The amount in solution for each tablet is not less than 70% (Q) of the amount declared on the label.
Assay Carry out the test as described under 1.14.4 High-performance liquid chromatography using a stainless steel column (10 cm × 4.6 mm) packed with octadecylsilyl base-deactivated silica gel for chromatography R (3 µm).2
As the mobile phase use a solution prepared as follows: dissolve 7.5 g of ammonium acetate R in 1000 mL of water R, mix and filter. Mix 750 mL of this solution with 250 mL of acetonitrile R.
Prepare as a solvent a mixture of 60 volumes of methanol R and 40 volumes of water R.
Prepare the following solutions. For solution (1) weigh and powder 20 tablets. Transfer a quantity of the powdered tablets, containing about 100 mg of mebendazole, accurately weighed, to a 100 mL volumetric flask. Add 30 mL of anhydrous formic acid and sonicate for about 20 minutes. Dilute to volume with solvent mixture, mix and filter. Dilute 5.0 mL of the filtrate to 100.0 mL with the solvent mixture. For solution (2) transfer 25.0 mg of mebendazole RS to a 25 mL volumetric flask, add 10 mL of the anhydrous formic acid R and sonicate to dissolve. Dilute to volume with the solvent mixture. Dilute 5.0 mL of this solution to 100.0 mL with the solvent mixture.
Operate with a flow rate of 1.2 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 250 nm.
Inject alternately 10 µL each of solutions (1) and (2).
Measure the areas of the peaks corresponding to mebendazole obtained in the chromatograms from solution (1) and (2) and calculate the percentage content of mebendazole (C16H13N3O3) in the tablets using the declared content of C16H13N3O3 in mebendazole RS.
Reagents to be establishedHydrochloric acid (~0.365 g/L) TS
Hydrochloric acid (~250 g/L) TS, dilute with water to contain 0.365 g of HCl in 1000 mL.
***
2 A HYPERSIL BDS C18 column has been found suitable.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
206
Proposed revision of the monograph on
Capreomycin sulfate (Capreomycini sulfas)
This is a draft revision of a monograph for The International Pharmacopoeia (Working document QAS/16.689, May 2017). It is proposed to revise the monograph as follows:• add a new reference substance – Capreomycin sulfate for identification RS –
suitable for identity tests A and B (identification by IR and TLC);• add a note of the Secretariat with respect to ongoing discussions about the
transition from microbiological to physicochemical assays for antibiotics; • update the style of the monograph.The working document with line numbers for commenting is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. In the online document changes from the current monograph are indicated in the text by insert or delete.
[Note from the Secretariat. The user of the monograph should note that the monograph describes a chromatographic assay to determine if the concentrations of capreomycin IA, IB, IIA and IIB of a sample under investigation complies with the definition (see section definition). Other pharmacopoeias have the activity of the substance determined for assay by means of microbiological methods. A correlation between the concentration of IA, IB, IIA and IIB and the activity of the substance, determined with microbiological methods, has not been established yet.]
β-Lysyl =
Component R1 R2Capreomycin IA OH β-Lysyl
Capreomycin IB H β-Lysyl
Capreomycin IIA OH H
Capreomycin IIB H H
Capreomycin (base) IA IB IIA IIBMolecular formula C25H44N14O8 C25H44N14O7 C19H32N12O7 C19H32N12O6
Relative molecular mass 668.7 652.7 540.5 524.5CAS Reg. no. 37280-35-6 33490-33-4 62639-89-8 62639-90-1Theoretical value of n in neutral sulfate salt 2 2 1.5 1.5

207
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
Chemical namesCapreomycin IA: sulfate salt of ([(Z){(3S,9S,12S,15S)-15-amino-3-[(4R)-2-amino-1,4,5,6-tetrahydropyrimidin-4-yl]-9-({[(3S)-3,6-diaminohexanoyl]amino}methyl)-12-(hydroxymethyl)-2,5,8,11-14-pentaoxo-1,4,7,10,13-pentaazacyclohexadecan-6-ylidene}methyl]urea.Capreomycin IB: sulfate salt of [(Z){(3S,9S,12S,15S)-15-amino-3-[(4R)-2-amino-1,4,5,6-tetrahydropyrimidin-4-yl]-9-({[(3S)-3,6-diaminohexanoyl]amino}methyl)-12-methyl-2,5,8,11-14-pentaoxo-1,4,7,10,13-pentaazacyclohexadecan-6-ylidene}methyl]urea.Capreomycin IIA: sulfate salt of [(Z){(3S,9S,12S,15S)-15-amino-9-(aminomethyl)-3-[(4R)-2-amino-1,4,5,6-tetrahydropyrimidin-4-yl]-12-(hydroxymethyl)-2,5,8,11-14-pentaoxo-1,4,7,10,13-pentaazacyclohexadecan-6-ylidene}methyl]urea.Capreomycin IIB: sulfate salt of [(Z){(3S,9S,12S,15S)-15-amino-9-(aminomethyl)-3-[(4R)-2-amino-1,4,5,6-tetrahydropyrimidin-4-yl]-12-methyl-2,5,8,11-14-pentaoxo-1,4,7,10,13-pentaazacyclohexadecan-6-ylidene}methyl]urea.
CAS Reg. no. 1405-37-4 (for capreomycin sulfate).Description. A white or almost white powder.Solubility. Very soluble in water, practically insoluble in ethanol (~750 g/L) TS and in ether.Category. Antituberculosis drug.Storage. Capreomycin sulfate should be kept in a tightly closed container or, if sterile, in a hermetically closed container.Labelling. The label states, where applicable:(1) that the substance is free from bacterial endotoxins;(2) that the substance is sterile.
RequirementsDefinition. Capreomycin sulfate is a mixture of the sulfates of antimicrobial polypeptides produced by the growth of Streptomyces capreolus. It contains not less than 70.0% of capreomycin, calculated with reference to the dried substance and taking into account the sum of capreomycin IA, IB, IIA and IIB. The content of capreomycin IA and IB is not less than 90.0% of the sum of capreomycin IA, IB, IIA and IIB.
Identity testsEither tests A and E or tests B, C, D and E may be applied.
A. Carry out the examination as described under 1.7 Spectrophotometry in the infrared region. The infrared absorption spectrum is concordant with the spectrum obtained from capreomycin sulfate for identification RS or with the reference spectrum of capreomycin sulfate.
B. Carry out the test as described under 1.14.1 Thin-layer chromatography using silica gel R5 as the coating substance and a mixture of 30 volumes of phenol R, 10 volumes of water R and 1 volume of ammonia (~260 g/L) TS as the mobile phase. Apply separately to the plate 4 μL of each of the following two solutions in water R. For solution (A) use 10 mg of the test substance per mL and for solution (B) use 10 mg of capreomycin sulfate for identification
Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
208
RS per mL. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air. Spray with triketohydrindene/methanol TS and heat the plate for 3 minutes at 120°C. Examine the chromatogram in daylight.The spots obtained with solution A correspond in position, appearance and intensity with those obtained with solution B.
C. The absorption spectrum (1.6) of a 20 µg/mL solution of the test substance in hydrochloric acid (0.1 mol/L) VS, when observed between 230 nm and 350 nm, exhibits a maximum at about 268 nm.
D. The absorption spectrum (1.6) of a 20 µg/mL solution of the test substance in sodium hydroxide (0.1 mol/L) VS, when observed between 230 nm and 350 nm, exhibits a maximum at about 287 nm.
E. A 20 mg/mL solution of the test substance yields reaction A described under 2.1 General identification tests as characteristic of sulfates.
pH value (1.3). pH of a 30 mg/mL solution of the test substance in carbon-dioxide-free water R, 4.5–7.5.
Loss on drying. Dry for 4 hours at 100°C under reduced pressure (not exceeding 0.6 kPa or about 5 mm of mercury); it loses not more than 100 mg/g.
Heavy metals. Use 1.0 g of the test substance for the preparation of the test solution as described under 2.2.3 Limit test for heavy metals, Procedure 3; determine the heavy metals content according to Method A; not more than 30 μg/g.
Sulfated ash (2.3). Not more than 10.0 mg/g.
Bacterial endotoxins. If intended for use in the manufacture of a parenteral dosage form, carry out the test as described under 3.4 Test for bacterial endotoxins; contains not more than 0.5 IU of endotoxin per mg of capreomycin sulfate.
Sterility. If intended for use in the manufacture of either a parenteral or other sterile dosage form without a further appropriate sterilization procedure, complies with 3.2 Test for sterility.
Related substances. Carry out the test as described under 1.14.4 High performance liquid chromatography using the conditions given under “Assay”.
Prepare the following solutions using Mobile phase A as diluent. For solution (1) use 2.0 mg of the test substance per ml. For solution (2) dilute a suitable volume of solution (1) to obtain a concentration of 10 µg of capreomycin sulfate per mL.
Operate with a flow rate of 1.0 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 268 nm.
Inject 20 μL of solution (1). The test is not valid unless the resolution between the two major peaks corresponding to capreomycin IA (with a relative retention of about 0.89) and capreomycin IB (retention time about 38 minutes) is at least 2.0 and the resolution between the peaks corresponding to capreomycin IIA and capreomycin IIB (with a relative retention of 0.53 and 0.63, respectively) is at least 3.5.
Inject separately 20 μL each of solutions (1) and (2).
209
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
In the chromatogram obtained with solution (1) the area of any peak, other than the four major peaks corresponding to capreomycin IA, IB, IIA and IIB, is not greater than 4 times the sum of the areas of the four major peaks obtained with solution (2) (2.0%). The area of not more than one such peak is greater than twice the sum of the areas of the four major peaks obtained with solution (2) (1.0%). The sum of the areas of all peaks, other than the four major peaks, is not greater than 14 times the sum of the areas of the four major peaks obtained with solution (2) (7.0%). Disregard any peak with an area less than 0.1 times the sum of the areas of the four major peaks in the chromatogram obtained with solution (2) (0.05%).
Assay. Carry out the test as described under 1.14.4 High performance liquid chromatography using a stainless steel column (25 cm x 4.6 mm) packed with base deactivated particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl groups (5 μm).
The mobile phases for the gradient elution consist of a mixture of mobile phase A and mobile phase B, using the following conditions:
mobile phase A: 5 volumes of acetonitrile R and 95 volumes of phosphate buffer pH 2.3;mobile phase B: 15 volumes of acetonitrile R and 85 volumes of phosphate buffer pH 2.3.
Prepare the phosphate buffer pH 2.3 by dissolving 54.4 g of potassium dihydrogen phosphate R in 1500 mL of water R, adjust the pH to 2.3 by adding phosphoric acid (~105 g/L) TS, add 9.4 g of sodium hexanesulfonate R and dilute to 2000 mL with water R.
Time(min)
Mobile phase A(% v/v)
Mobile phase B(% v/v)
Comments
0–25 55–52 45–48 Linear gradient25–40 52 48 Isocratic40–60 30 70 Isocratic60–70 55 45 Isocratic re-equilibration
Prepare the following solutions using mobile phase A as diluent. For solution (1) use 2.0 mg of the test substance per mL. For solution (2) use 2.0 mg of capreomycin sulfate RS per mL.
Operate with a flow rate of 1.0 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 268 nm.
Inject 20 μL of solution (1). The assay is not valid unless the resolution between the two major peaks corresponding to capreomycin IA (with a relative retention of 0.89) and capreomycin IB (retention time about 38 minutes) is at least 2.0 and the resolution between the peaks corresponding to capreomycin IIA and capreomycin IIB (with a relative retention of 0.53 and 0.63, respectively) is at least 3.5.
Inject separately 20 μL each of solutions (1) and (2).
Measure the areas of the peak responses for capreomycin IA, IB, IIA and IIB obtained in the chromatograms from solutions (1) and (2) and, using the sum of the areas, calculate the percentage content of capreomycin using the declared content in capreomycin sulfate RS.
***

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
210
Proposed revision of the monograph on
Capreomycin for injection (Capreomycini ad injectionem)
This is a draft revision of a monograph for The International Pharmacopoeia (Working document QAS/16.690, May 2017). It is proposed to revise the monograph as follows:• add a new reference substance - Capreomycin sulfate for identification RS -
suitable for identity test A and B (identification by IR and TLC);• add a note of the Secretariat with respect to ongoing discussions about the
transition from microbiological to physicochemical assays for antibiotics; • determine the percentage content of capreomycin per sealed container;• update the style of the monograph.The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. In the online document changes from the current monograph are indicated in the text by insert or delete.
[Note from the Secretariat. The user of the monograph should note that the monograph describes a chromatographic assay to determine if the concentrations of capreomycin IA, IB, IIA and IIB of a sample under investigation complies with the definition (see section definition). Other pharmacopoeias have the activity of the substance determined for assay by means of microbiological methods. A correlation between the concentration of IA, IB, IIA and IIB and the activity of the substance, determined with microbiological methods, has not been established yet.]
Description. A white or almost white powder.
Category. Antituberculosis drug.
Storage. Capreomycin for injection should be stored in a well-closed container.
Labelling. The designation on the container of capreomycin for injection should state that the active ingredient is in the sulfate form and the quantity should be indicated in terms of the equivalent amount of capreomycin.
Additional information. Strength in the current WHO Model List of Essential Medicines (EML): 1 g. Strength in the current EML for children: 1 g.
The injection is reconstituted by dilution of Capreomycin powder for injections in Water for injections.The reconstituted injection should be used immediately after preparation.

211
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
RequirementsThe powder for injection and the reconstituted injection comply with the monograph for Parenteral preparations.Definition. Capreomycin for injection is a sterile powder containing Capreomycin sulfate. It contains not less than 90.0% and not more than 115.0% of the amount of capreomycin stated on the label, taking into account the sum of capreomycin IA, IB, IIA and IIB.
Identity testsEither tests A and E or tests B, C, D and E may be applied.
A. Carry out the examination as described under 1.7 Spectrophotometry in the infrared region. The infrared absorption spectrum is concordant with the spectrum obtained from capreomycin sulfate for identification RS or with the reference spectrum of capreomycin sulfate.
B. Carry out the test as described under 1.14.1 Thin-layer chromatography using silica gel R5 as the coating substance and a mixture of 30 volumes of phenol R, 10 volumes of water R and 1 volume of ammonia (~260 g/L) TS as the mobile phase. Apply separately to the plate 4 μL of each of the following two solutions in water R. For solution (A) dissolve a quantity of the powder to obtain a solution containing 10 mg of the powder for injection per mL. For solution (B) use 10 mg of capreomycin sulfate for identification RS per mL. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air. Spray with triketohydrindene/methanol TS and heat the plate for 3 minutes at 120°C. Examine the chromatogram in daylight.The spots obtained with solution A correspond in position, appearance and intensity with those obtained with solution B.
C. Dissolve a quantity of the powder for injection in hydrochloric acid (0.1 mol/L) VS to obtain a solution containing the equivalent of 20 µg of capreomycin per mL. The absorption spectrum (1.6) of this solution, when observed between 230 nm and 350 nm, exhibits a maximum at about 268 nm.
D. Dissolve a quantity of the powder for injection in sodium hydroxide (0.1 mol/L) VS to obtain a solution containing the equivalent of 20 µg of capreomycin per mL. The absorption spectrum (1.6) of this solution, when observed between 230 nm and 350 nm, exhibits a maximum at about 287 nm.
E. A solution of the powder for injection containing the equivalent of 20 mg of capreomycin per mL yields reaction A described under 2.1 General identification tests as characteristic of sulfates.
Clarity of solution. A freshly prepared solution of the powder for injection containing the equivalent of 1 g of capreomycin in 10 mL of carbon-dioxide-free water R is clear.
pH value (1.13). pH of a solution of the powder for injection containing the equivalent of 0.3 g of capreomycin in 10 mL of carbon-dioxide-free water R, 4.5–7.5.
Bacterial endotoxins. Carry out the test as described under 3.4 Test for bacterial endotoxins; contains not more than 0.35 IU of endotoxin per mg of capreomycin.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
212
Related substances. Carry out the test as described under 1.14.4 High-performance liquid chromatography using the conditions given under “Assay”.
Prepare the following solutions using Mobile phase A as diluent. For solution (1) dissolve a quantity of the powder for injection to obtain a solution containing the equivalent of 2.0 mg of capreomycin per mL. For solution (2) dilute a suitable volume of solution (1) to obtain a concentration of 10 µg of capreomycin per mL.
Operate with a flow rate of 1.0 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 268 nm.
Inject 20 μL of solution (1). The test is not valid unless the resolution between the two major peaks corresponding to capreomycin IA (with a relative retention of about 0.89) and capreomycin IB (retention time about 38 minutes) is at least 2.0 and the resolution between the peaks corresponding to capreomycin IIA and capreomycin IIB (with a relative retention of 0.53 and 0.63, respectively) is at least 3.5.
Inject separately 20 μL each of solutions (1) and (2).
In the chromatogram obtained with solution (1) the area of any peak, other than the four major peaks corresponding to capreomycin IA, IB, IIA and IIB, is not greater than 4 times the sum of the areas of the four major peaks obtained with solution (2) (2.0%). The area of not more than one such peak is greater than twice the sum of the areas of the four major peaks obtained with solution (2) (1.0%). The sum of the areas of all peaks, other than the four major peaks, is not greater than 14 times the sum of the areas of the four major peaks obtained with solution (2) (7.0%). Disregard any peak with an area less than 0.1 times the sum of the areas of the four major peaks in the chromatogram obtained with solution (2) (0.05%).
Assay. Carry out the test as described under 1.14.4 High-performance liquid chromatography using a stainless steel column (25 cm x 4.6 mm) packed with base-deactivated particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl groups (5 μm).
The mobile phases for the gradient elution consist of a mixture of mobile phase A and mobile phase B using the following conditions:
mobile phase A: 5 volumes of acetonitrile R and 95 volumes of phosphate buffer pH 2.3;mobile phase B: 15 volumes of acetonitrile R and 85 volumes of phosphate buffer pH 2.3.
Prepare the phosphate buffer pH 2.3 by dissolving 54.4 g of potassium dihydrogen phosphate R in 1500 mL of water R, adjust the pH to 2.3 by adding phosphoric acid (~105 g/L) TS, add 9.4 g of sodium hexanesulfonate R and dilute to 2000 mL with water R.
Time(min)
Mobile phase A(% v/v)
Mobile phase B(% v/v)
Comments
0–25 55–52 45–48 Linear gradient25–40 52 48 Isocratic40–60 30 70 Isocratic60–70 55 45 Isocratic re-equilibration

213
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
Weigh and mix the contents of 5 containers. Prepare the following solutions using mobile phase A as diluent. For solution (1) dissolve a quantity of the mixed contents, containing the equivalent of about 100 mg of capreomycin, accurately weighed, and dilute to 50.0 mL. For solution (2) use a solution containing 2.75 mg of capreomycin sulfate RS per mL.
Operate with a flow rate of 1.0 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 268 nm.
Inject 20 μL of solution (1). The assay is not valid unless the resolution between the two major peaks corresponding to capreomycin IA (with a relative retention of 0.89) and capreomycin IB (retention time about 38 minutes) is at least 2.0. and the resolution between the peaks corresponding to capreomycin IIA and capreomycin IIB (with a relative retention of 0.53 and 0.63, respectively) is at least 3.5.
Inject separately 20 μL each of solutions (1) and (2).
Measure the areas of the peak responses for capreomycin IA, IB, IIA and IIB obtained in the chromatograms from solutions (1) and (2) and, using the sum of the areas, calculate the percentage content of capreomycin per sealed container using the declared content in capreomycin sulfate RS.
***
Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
214
Concept paper for comment
Transition from microbiological to physicochemical assays in monographs on capreomycin active pharmaceutical
ingredients and products
This is a concept paper (Working document QAS/16.695, April 2017) proposed by the Secretariat of The International Pharmacopoeia.
The strength of antibiotics can be determined using microbiological or physicochemical assays. While traditionally microbiological methods were predominantly used in quality control of antibiotics, physicochemical methods are nowadays preferred for various reasons. The transition from microbiological to physicochemical assays has been largely completed for single-component antibiotics. For multicomponent antibiotics, however, the use of physicochemical methods remains challenging.
Following discussions and decisions at meetings of the WHO Expert Committees on Specifications for Pharmaceutical Preparations and on Biological Standardization, the Secretariat of The International Pharmacopoeia is seeking information and international collaboration in order to establish a chromatographic assay as an alternative to microbiological assays for the essential medicine capreomycin powder for injection and the corresponding active pharmaceutical ingredient (API) capreomycin sulfate. In addition, this initiative aims at harmonizing quality control requirements for these products. It may also provide new insights which can facilitate transitions of other antibiotics.
The Secretariat of The International Pharmacopoeia invites stakeholders, in particular regulatory authorities, pharmacopoeias and manufacturers of capreomycin sulfate, capreomycin powders for injection and other medicines containing multicomponent antibiotics, to comment on the proposals made in this document. Subsequent steps, in particular the performance of a bridging study to link the mass with the activity of capreomycin, will be decided inter alia based on the discussions of the comments received.
The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects.
Scope of the documentThis document proposes steps to finish the transition of the tuberculostatic aminoglycoside capreomycin that has been started with the publication of chromatographic assay methods in the monographs on Capreomycin sulfate and Capreomycin powder for injection of The International Pharmacopeia. In the course of the transition, factors that may pose a risk to the safety of patients shall be identified and controlled, in particular by means of two surveys: a landscape analysis of capreomycin APIs and products on the global market and a comparison
215
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
of national capreomycin reference substances. Besides, this proposal aims at the international harmonization of quality control requirements for capreomycin.
Background informationAntibiotics produced by fermentation often consist of complex mixtures of structurally related components with different activities. Microbiological methods were historically used to quantify the total activity of these mixtures. As evidence of their structure and composition increased, transitions from microbiological to physicochemical assays, in particular chromatographic methods, were possible and envisaged as they are often more discriminative and easier or faster to perform. Microbiological assays, on the other hand, measure the total (in vitro) activity of antibiotics against a reference microorganism, integrating all moieties that contribute to this effect.
While the transition from microbiological to physicochemical assays has been largely completed for single-component antibiotics, it remains challenging for substances containing several components.
Discussions at meetings of WHO Expert CommitteesPoints to consider when switching from biological to physicochemical assays were discussed at the meetings of the Expert Committee on Specifications for Pharmaceutical Preparations (ECSPP) and the Expert Committee on Biological Standardization (ECBS) in 2007. In 2009, the ECSPP recommended that microbiological assays shall be replaced by, in particular, chromatographic methods, where possible and appropriate. Following this decision, chromatographic assays were elaborated and published as part of the monographs on Capreomycin sulfate and Capreomycin for injection in The International Pharmacopoeia.
Following the publication of these monographs, the comparability of analytical results gained with the new chromatographic assay method and with so far used microbiological assays was discussed. At the meetings of the ECSPP and ECBS in 2016 it was agreed that the Secretariat of The International Pharmacopoeia should contact manufacturers to obtain further information about the prevailing composition of capreomycin active pharmaceutical ingredient (API), methods used to determine the content of capreomycin powders for injection and information regarding a correlation between the mass and the microbiological activity of the antibiotic.
Capreomycin for injection in the WHO Model List of Essential MedicinesIn the WHO Model List of Essential Medicines (EML) (19th Edition) the strength of capreomycin powder for injection is given as “1 g (as sulfate) in vial”. Considering that in the past pharmacopoeias described microbiological methods for the assay of capreomyin products, the information regarding the strength given in the EML should be interpreted as “capreomycin sulfate equivalent to the activity of 1 g capreomycin in vial”. This interpretation would correspond to the way the comparator product, Capastat®, is labelled, namely “Each vial contains the equivalent of 1 g capreomycin activity”.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
216
The monographs on Capreomycin sulfate and Capreomycin for injection in The International PharmacopoeiaCapreomycin is a mixture of four structurally related compounds, Capreomycin IA, IB, IIA and IIB with different specific activities. In the monograph on Capreomycin sulfate the active substance is defined on a mass basis: “Capreomycin sulfate is a mixture of the sulfates of antimicrobial polypeptides produced by the growth of Streptomyces capreolus. It contains not less than 70.0% of capreomycin, calculated with reference to the dried substance and taking into account the sum of capreomycin IA, IB, IIA and IIB. The contents of capreomycin IA and IB is not less than 90.0% of the sum of capreomycin IA, IB, IIA and IIB”.
The Chinese Pharmacopoeia (CP), the Indian Pharmacopoeia (IP) and the United States Pharmacopeia (USP) have similar requirements regarding the composition of Capreomycin sulfate. However, in these pharmacopoeias the capreomycin content of APIs and finished products is determined using microbiological methods.
In 1969, the specific activities of the isolated four main components were determined. The results of these investigations showed that there is a significant difference between the activities of components IA versus IB and I versus II. As the applied techniques to separate and purify substances have become more specific and efficient in past decades, WHO was advised to re-establish the data should succeeding decisions be based on them.
While the monograph on Capreomycin currently limits the capreomycin II contents to maximum 10%, the ratio between capreomycin IA and IB is not defined at present. Further information and guidance is sought regarding the relevance of such an additional limit with a view to ensure that products even with extreme differences in the IA and IB concentrations consistently comply or not comply with the different compendial assays.
Capreomycin sulfate reference substancesSubsequent to the publication of the capreomycin monographs, a reference substance, capreomycin sulfate ICRS Batch 1, was established for use according to the prescribed compendial tests. Following a comprehensive analytical characterization of the candidate material, a defined capreomycin base concentration per vial, expressed in mass units, was assigned to the standard to render it suitable, i.e. for assay by high performance liquid chromatography (HPLC).
The ECSPP released capreomycin sulfate ICRS Batch 1 at its meeting in 2016 with the following note in the leaflet: “The International Chemical Reference Substance for capreomycin sulfate ICRS is intended to be used as described in The International Pharmacopoeia for assay by HPLC according to the monographs for capreomycin sulfate and capreomycin for injection. The substance is suitable to serve as a reference for the quantitative determination of the content of capreomycins IA, IB, IIA and IIB from the declared content in capreomycin sulfate RS. A correlation between the concentration of IA, IB, IIA and IIB and the activity of the substance, determined with microbiological methods, has not been established.”
217
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
A Capreomycin WHO International Standard for Antibiotics (ISA) to define the activity of capreomycin in microbiological assays was established in 19681 and discontinued in 2000 following an enquiry to determine whether there was a continued necessity for the standard.2 The reference substance served as a primary reference standard for pharmacopoeias to calibrate their national, secondary reference standards, subsequently used in routine laboratory tests and assays.
Landscape analysis of capreomycin APIs and products on the global marketThe aim of this survey is to provide an overview on the composition of capreomycin APIs and products on the market. Together with information on the activity and toxicity of the different components, the results of the chromatographic analysis will help to evaluate the comparability of capreomycin products. Based on the results of this survey, additional limits regarding the chemical composition of capreomycin, in particular a limit to specify the ratio IA to IB, shall be discussed and implemented if need be.
To initiate the survey, WHO shall invite manufactures to share the following information and samples:
Manufacturers of capreomycin or capreomycin sulfate:1. A sample of capreomycin or capreomycin sulfate (about 10 g), representative for the
authorized manufacturing process, together with the certificate of analysis and the material safety data sheet.
2. A compilation of the specifications of the product together with a description of the methods used to determine them. For the methods to determine the content/strength and composition of the product the reference substance(s) used, the name(s) of the authorizing organization(s) and the declared strength(s) or assigned content(s) shall be indicated. In case chromatographic methods are used sample chromatograms shall also be submitted.
3. The outcome of investigations to correlate the total microbiological activity of capreomycin/capreomycin sulfate (or the activity of the components) with the mass concentration of the components (including information about the design of the performed study, a description of the methods used and details of the results obtained) (if available).
4. Information about the toxicity of capreomycin with respect to its composition (if available).
Manufacturers of capreomycin powder for injection:1. A sample of each authorized capreomycin powder for injection (10 vials each of 1 g for
each product belonging to the same batch, together with the corresponding certificate(s) of analysis) and a copy of the packaging indicating the labelled strength of the products.
2. A compilation of the specifications of the product together with a description of the methods used to determine them. For the methods to determine the content/strength and composition of the product the reference substance(s) used, the name(s) of the authorizing
1 WHO Technical Report Series, No. 384.2 WHO Technical Report Series, No. 924.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
218
organization(s) and the declared strength(s) or assigned content(s) shall be indicated. In case chromatographic methods are used sample chromatograms shall also be submitted.
3. The outcome of investigations to correlate the total microbiological activity of capreomycin/capreomycin sulfate (or the activity of the components) with the mass concentration of the components (including information about the design of the performed study, a description of the methods used and details of the results obtained) (if available).
4. Information about the toxicity of capreomycin with respect to its composition (if available).
Comparison of national capreomycin reference substances Not only assay methods based on different principles, also the lack of an international primary reference substance defining the activity of capreomycin may have affected the comparability of capreomycin dose regimes over time. To obtain relevant evidence, WHO shall organize laboratory investigations to determine:
1. the antimicrobiological activity of a common sample, capreomycin sulfate International Chemical Reference Substances (ICRS)3, according to the current provisions in the CP, IP and USP; and
2. the percentage mass concentrations of capreomycin IA, IB, IIA and IIB of the national reference substances prescribed by CP, IP and USP and analysed using the HPLC method described in the monograph on Capreomycin sulfate of The International Pharmacopoeia.
Based on the results of this survey, WHO shall evaluate jointly with i.a. the concerned pharmacopoeias the need to re-establish capreomycin ISA. The results will also help to further elucidate how the composition of capreomycin determines its activity.
Bridging study to link the mass with the activity of capreomycinConsidering the results of the landscape analysis of capreomycin APIs and products and on the comparison of national capreomycin reference substances, pharmacopoeias (in particular the CP, IP, USP and The International Pharmacopoeia) may decide to finish the transition from microbiological to a physicochemical assay for the capreomycin content by performing a bridging study to link the mass with the activity of the substance. Such a linkage would allow manufacturers to retain the current labelling of their products (i.e. the strength labelled in activity) and to seek regulatory approval to use a chromatographic method for the testing of their products.
A USP guidance document4 provides points to consider for the development of chromatographic or other physicochemical methods to replace microbiological assays. As a
3 Capreomycin sulfate ICRS is proposed as a common test sample because the chemical composition of the substance was thoroughly investigated during its establishment as a reference substances for physico-chemical tests according to The International Pharmacopoeia. The available analytical data, together with the results of the antimicrobiological determination may help to understand and to establish the correlation between the composition of capreomycin and its activity. Capreomycin ICRS is also needed as a reference substances for the determination under (2).
4 USP 39, chapter 1223, Validation of alternative methods to antibiotic microbial assays.
219
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
pivotal step, the process would involve the separation and purification of each antimicrobial moiety, process impurity and degradation product of the antibiotic and a subsequent determination of their individual, relative microbial activity.
To determine these relative microbial activities an international (primary) reference substance, capreomycin ISA, which defines the activity of capreomycin sulfate, would have to be re-established.
The alternative chromatographic method should be composition- and stability-indicating and would have to consider the specific absorptivity of the different components (in case the absorptivities differ significantly). The already published HPLC method in The International Pharmacopoeia is proposed to be used for this purpose.
International harmonization of pharmacopoeial requirements for capreomycinThe joint bridging study and its results shall also foster harmonization of pharmacopoeial requirements for capreomycin API and products. With the knowledge of the correlation between the composition and activity of capreomycin other pharmacopoeias, in particular CP, IP and USP, may consider to also switch to the alternative chromatographic method published in The International Pharmacopoeia.
In addition, the gained insights may facilitate future transitions from microbiological to physicochemical assays in monographs of other multicomponent antiobiotics.
***

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
220
Proposed revision of the monograph on
Atenolol (Atenololum)
This is a draft revision of a monograph for The International Pharmacopoeia (Working document QAS/17.700, May 2017). It is proposed to revise the monograph based on information found in the European Pharmacopoeia and in the scientific literature.
The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. In the online document changes from the current monograph are indicated in the text by insert or delete.
C14H22N2O3
Relative molecular mass. 266.3
Chemical name. 2-[p-[2-Hydroxy-3-(isopropylamino)propoxy]phenyl]acetamide (racemate); CAS Reg. No. 29122-68-7.
Description. A white or almost white powder.
Solubility. Sparingly soluble in water; soluble in ethanol (~750 g/L) TS; slightly soluble in dichloromethane R.
Category. Cardiovascular agent; β-adrenoreceptor blocking agent.
Storage. Atenolol should be kept in a tightly closed container.
RequirementsAtenolol contains not less than 99.0% and not more than 101.0% of C14H22N2O3, calculated with reference to the dried substance.
Identity tests•EithertestAortestsBandCmaybeapplied.
A. Carry out the examination as described under 1.7 Spectrophotometry in the infrared region. The infrared absorption spectrum is concordant with the spectrum obtained from atenolol RS or with the reference spectrum of atenolol.
221
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
B. The absorption spectrum of a 0.10 mg/mL solution in methanol R, when observed between 230 nm and 350 nm, exhibits 2 maxima at about 275 nm and 282 nm. The ratio of the absorbance at 275 nm to that at 282 nm is between 1.15 and 1.20.
C. Carry out the test as described under 1.14.1 Thin-layer chromatography using silica gel R4 as the coating substance and a mixture of 99 volumes of methanol R and 1 volume of ammonia (~260 g/L) TS as the mobile phase. Apply separately to the plate 10 μL of each of 2 solutions in methanol R containing (A) 10 mg of the test substance per mL and (B) 10 mg of atenolol RS per mL. After removing the plate from the chromatographic chamber allow it to dry in air and examine the chromatogram in ultraviolet light (254 nm).
The principal spot obtained with solution (A) corresponds in position, appearance and intensity with that obtained with solution (B).
Solution S. Dissolve 0.10 g of the test substance in carbon-dioxide-free water R and dilute to 10.0 mL with the same solvent.
Optical rotation (1.4). Use solution S; α = +0.10 to –0.10.
Clarity and colour of solution. Solution (S) is clear and not more intensely coloured than degree 6 of the range of reference solutions of the most appropriate colour, when compared as described under 1.11.2 Degree of coloration of liquids, Method II. [Note from the Secretariat. Chapter 1.11 Colour of liquids is currently under revision. Reference is already made to a new test procedure to be added under section 1.11.2 Degree of coloration of liquids.]
Chlorides. Dissolve 0.25 g in a mixture of 2 mL of nitric acid (~130 g/L) TS and 20 mL of water and proceed as described under 2.2.1 Limit test for chlorides; the chloride content is not more than 1.0 mg/g.
Sulfated ash (2.3). Not more than 1.0 mg/g, determined using 1.0 g.
Loss on drying. Dry 1.0 g of the test substance to constant mass at 105°C; it loses not more than 5.0 mg/g.
Related substances. Carry out the test as described under 1.14.4 High-performance liquid chromatography using a stainless steel column (12.5 cm × 4.0 mm) packed with particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl groups (5 μm). Prepare the following solution to be used as the mobile phase: dissolve 1.0 g of sodium octanesulfonate R and 0.4 g of tetrabutylammonium hydrogen sulfate R in 1000 mL of a mixture of 80 volumes of a 3.4 mg/mL solution of potassium dihydrogen phosphate R, the pH of the solution adjusted to 3.0 with phosphoric acid (~1440 g/L), 18 volumes of methanol R and 2 volumes of tetrahydrofuran R.Prepare the following solutions in mobile phase. For solution (1) dissolve 50 mg of the test substance in 20 mL and dilute to 25.0 mL. For solution (2) dilute 1.0 mL of solution (1) to 100.0 mL. Dilute 1.0 mL of this solution to 10.0 mL. For solution (3) dissolve 2 mg of atenolol for system suitability RS (containing atenolol and the impurities B, F, G, I and J) in 1.0 mL of the mobile phase. Operate with a flow rate of 0.6 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of about 226 nm.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
222
Inject 10 μL of solution (3). Record the chromatograms for about 5 times the retention time of atenolol (retention time about 8 minutes). Use the chromatogram obtained with solution (3) and the chromatogram supplied with atenolol for system suitability RS to identify the peaks due to atenolol and the impurities B, F, G, I and J.
The test is not valid unless the resolution between the peaks due to the impurities J and I is at least 1.4.
Inject alternately 10 μL each of solutions (1) and (2).
In the chromatogram obtained with solution (1):• the area of any peak corresponding to impurity B is not greater than 2 times the area of the
peak due to atenolol in the chromatogram obtained with solution (2) (0.2%);• the area of any peak corresponding to either impurity F, G, I or J is not greater than 1.5 times
the area of the peak due to atenolol in the chromatogram obtained with solution (2) (0.15%);• the area of any other impurity peak is not greater than the area of the peak due to atenolol in
the chromatogram obtained with solution (2) (0.10%);• the sum of the areas of all impurity peaks is not greater than 5 times the area of the peak due
to atenolol in the chromatogram obtained with solution (2) (0.5%). Disregard any peak with an area less than 0.5 times the area of the peak due to atenolol in the chromatogram obtained with solution (2) (0.05%).
Assay. Dissolve about 0.200 g, accurately weighed, in 80 mL of glacial acetic acid R1 and titrate with perchloric acid (0.1 mol/L) VS as described under 2.6 Non-aqueous titration, Method A, determining the end-point potentiometrically.
Each mL of perchloric acid (0.1 mol/L) VS is equivalent to 26.63 mg of C14H22N2O3.
Impurities
A. 2-(4-hydroxyphenyl)acetamide
B. 2-[4-[(2RS)-2,3-dihydroxypropoxy]phenyl]acetamide
D. 2-[4-[(2RS)-3-chloro-2-hydroxypropoxy]phenyl]acetamide
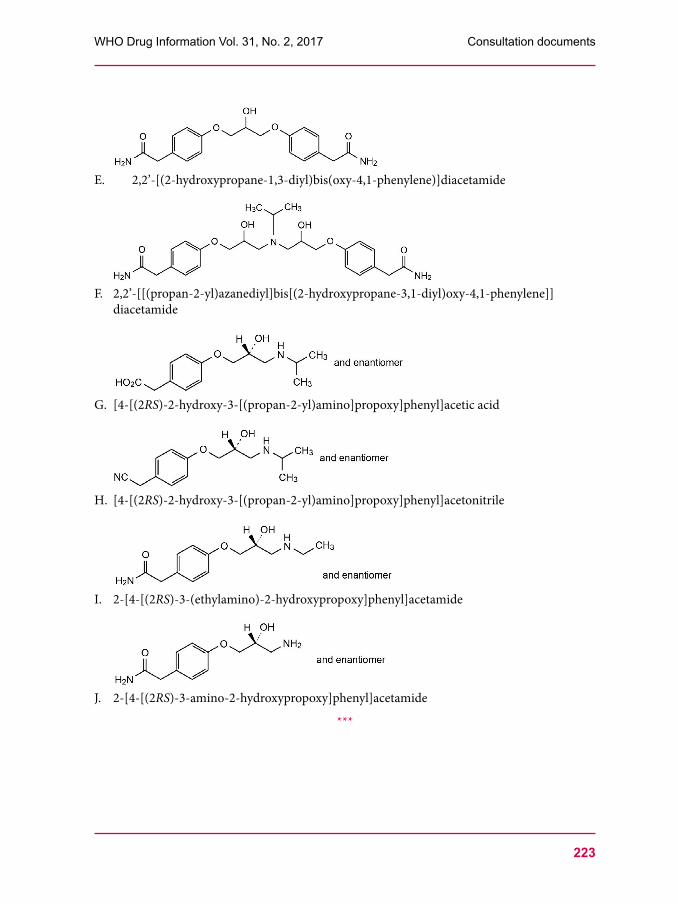
223
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
E. 2,2’-[(2-hydroxypropane-1,3-diyl)bis(oxy-4,1-phenylene)]diacetamide
F. 2,2’-[[(propan-2-yl)azanediyl]bis[(2-hydroxypropane-3,1-diyl)oxy-4,1-phenylene]]diacetamide
G. [4-[(2RS)-2-hydroxy-3-[(propan-2-yl)amino]propoxy]phenyl]acetic acid
H. [4-[(2RS)-2-hydroxy-3-[(propan-2-yl)amino]propoxy]phenyl]acetonitrile
I. 2-[4-[(2RS)-3-(ethylamino)-2-hydroxypropoxy]phenyl]acetamide
J. 2-[4-[(2RS)-3-amino-2-hydroxypropoxy]phenyl]acetamide
***

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
224
1.15.1
Capillary electrophoresis
This is a draft proposed text for The International Pharmacopoeia (Working document QAS/16.698, May 2017). This text is based on the internationally harmonized texts developed by the Pharmacopoeial Discussion Group (PDG). It has been developed in line with the style and requirements used in The International Pharmacopoeia. The permission to reproduce the text will be requested when the text is adopted by the WHO Expert Committee on Specifications for Pharmaceutical Preparations.
The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects.
This text is based on the internationally harmonized texts developed by the Pharmacopoeial Discussion Group (PDG). It has been developed in line with the style and requirements used in The International Pharmacopoeia.
General principlesCapillary electrophoresis is a physical method of analysis based on the migration, inside a capillary, of charged analytes dissolved in an electrolyte solution under the influence of a direct-current electric field.The migration velocity of the analyte under an electric field of intensity E is determined by the electrophoretic mobility of the analyte and the electroosmotic mobility of the buffer inside the capillary. The electrophoretic mobility of a solute (µep) depends on the characteristics of the solute (electrical charge, molecular size and shape) and the characteristics of the buffer in which the migration takes place (type and ionic strength of the electrolyte, pH, viscosity and additives). The electrophoretic velocity (νep) of a solute, assuming a spherical shape, is as follows:
in which q is the effective charge of the solute; η is the viscosity of the electrolyte solution; r is the Stoke’s radius of the solute; V is the applied voltage; and L is the total length of the capillary.When an electric field is applied through the capillary filled with buffer, a flow of solvent, called electroosmotic flow, is generated inside the capillary. Its velocity depends on the electroosmotic mobility (µeo), which in turn depends on the charge density on the capillary internal wall and the buffer characteristics. The electroosmotic velocity (νeo) is given by the equation:
in which ε is the dielectric constant of the buffer; ζ is the zeta potential of the capillary surface; and the other terms are as defined above.

225
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
The velocity of the solute (ν) is given by the equation:ν = vep+ νeo
The electrophoretic mobility of the analyte and the electroosmotic mobility may act in the same direction or in opposite directions, depending on the charge of the solute. In normal capillary electrophoresis, anions will migrate in the opposite direction to the electroosmotic flow and their velocities will be smaller than the electroosmotic velocity. Cations will migrate in the same direction as the electroosmotic flow and their velocities will be greater than the electroosmotic velocity. Under conditions in which there is a fast electroosmotic velocity with respect to the electrophoretic velocity of the solutes, both cations and anions can be separated in the same run. The time (t) taken by the solute to migrate the distance (l) from the injection end of the capillary to the detection point (capillary effective length) is as follows:
in which the other terms are as defined above.
In general, uncoated fused-silica capillaries above pH 3 have negative charge due to ionized silanol groups in the inner wall. Consequently, the electroosmotic flow is from anode to cathode. The electroosmotic flow must remain constant from run to run to obtain good reproducibility in the migration velocity of the solutes. For some applications, it might be necessary to reduce or suppress the electroosmotic flow by modifying the inner wall of the capillary or by changing the concentration, composition and/or the pH of the buffer solution.After the introduction of the sample into the capillary each analyte ion of the sample migrates within the background electrolyte as an independent zone according to its electrophoretic mobility. Zone dispersion, that is the spreading of each solute band, results from different phenomena. Under ideal conditions, the sole contribution to the solute-zone broadening is molecular diffusion of the solute along the capillary (longitudinal diffusion). In this ideal case, the efficiency of the zone, expressed as the number of theoretical plates (N), is given by:
in which D is the molecular diffusion coefficient of the solute in the buffer.In practice, other phenomena, such as heat dissipation, sample adsorption onto the capillary wall, mismatched conductivity between sample and buffer, length of the injection plug, detector cell size and unlevelled buffer reservoirs, can also significantly contribute to band dispersion. Separation between two bands (expressed by the resolution RS) can be obtained by modification of the electrophoretic mobility of the analytes, by the electroosmotic mobility induced in the capillary and by increasing the efficiency for the band of each analyte as follows:
in which µepa and µepb are the electrophoretic mobilities of the two analytes to be separated; is the average electrophoretic mobility of the two analytes calculated as:

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
226
ApparatusAn apparatus for capillary electrophoresis is composed of a high voltage controllable direct current power supply; two buffer reservoirs held at the same level and containing specified anodic and cathodic solutions; two electrode assemblies (cathode and anode) immersed in the buffer reservoirs and connected to the power supply; a separation capillary usually made of fused-silica, sometimes with an optical viewing window aligned with the detector, depending on the detector type, with the ends of the capillary placed in the buffer reservoirs and the capillary being filled with a solution specified in a given monograph; a suitable injection system; a detector capable of monitoring the amount of substance of interest passing through a segment of the separation capillary at a given time, generally based on absorption spectrophotometry (ultraviolet (UV) and visible), fluorimetry, conductimetric, amperometric, or mass spectrometric detection, depending on the specific applications, or even indirect detection to detect non-UV-absorbing and nonfluorescent compounds; a thermostatic system capable of maintaining a constant temperature inside the capillary, recommended to obtain good separation reproducibility; a recorder; and a suitable integrator or a computer.The definition of the injection process and its automation are critical for precise quantitative analysis. Modes of injection include gravity, pressure or vacuum, or electrokinetic injection. The amount of each sample component introduced electrokinetically depends on its electrophoretic mobility, leading to possible discrimination using this injection mode.It is expected that the capillary, the buffer solutions, the preconditioning method, the sample solution, and the migration conditions will be specified in the individual monograph. The electrolytic solution employed is filtered to remove particles and degassed to avoid bubble formation that could interfere with the detection system or interrupt the electrical contact in the capillary during the separation run. To achieve reproducible migration time of the solutes, it would be necessary to develop, for each analytical method, a rigorous rinsing routine.
Capillary zone electrophoresisPrincipleIn capillary zone electrophoresis, analytes are separated in a capillary containing only buffer without any anticonvective medium. In this technique, separation takes place because the different components of the sample migrate as discrete bands with different velocities. The velocity of each band depends on the electrophoretic mobility of the solute and the electroosmotic flow on the capillary (see “General principles”). Coated capillaries can be used to increase the separation capacity of those substances adsorbing on fused-silica surfaces.This mode of capillary electrophoresis is appropriate for the analysis of small (molecular weight < 2000) and large (2000 < MW < 100,000) molecules. Due to the high efficiency achieved in capillary zone electrophoresis, separation of molecules having only minute differences in their charge-to-mass ratio can be effected. This separation mode also allows the separation of chiral compounds by addition of chiral selectors to the separation buffer.

227
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
OptimizationOptimization of the separation is a complex process where several separation parameters can play a major role. The main factors to be considered in the development of the separations are instrumental and electrolytic solution parameters.
Instrumental parametersVoltage. A Joule heating plot is useful in optimizing the applied voltage and column temperature. The separation time is inversely proportional to applied voltage. However, an increase in the voltage used can cause excessive heat production, giving rise to temperature and, as a result, viscosity gradients in the buffer inside the capillary, which causes band broadening and decreases resolution.Polarity. Electrode polarity can be normal (anode at the inlet and cathode at the outlet) and the electroosmotic flow will move toward the cathode. If the electrode polarity is reversed the electroosmotic flow is away from the outlet and only charged analytes with electroosmotic mobilities greater than the electroosmotic flow will pass to the outlet.Temperature. The main effect of temperature is observed on buffer viscosity and electrical conductivity, thus affecting migration velocity. In some cases, an increase in capillary temperature can cause a conformational change of some proteins, modifying their migration time and the efficiency of the separation.Capillary. The length and internal diameter of the capillary affects the analysis time, the efficiency of separations and the load capacity. Increasing both effective length and total length can decrease the electric fields, at a constant voltage, which increases migration time. For a given buffer and electric field, heat dissipation (thus, sample band broadening) depends on the internal diameter of the capillary. The latter also affects the detection limit, depending on the sample volume injected into the capillary and the detection system used.The adsorption of sample components on the capillary wall limits efficiency; therefore, methods to avoid these interactions should be considered in the development of a separation method. In the specific case of proteins, several strategies have been devised to avoid adsorption on the capillary wall. Some of these strategies (use of extreme pH and adsorption of positively charged buffer additives) only require modification of the buffer composition to prevent protein adsorption. Other strategies include the coating of the internal wall of the capillary with a polymer covalently bonded to the silica that prevents interaction between the proteins and the negatively charged silica surface. For this purpose, ready-to-use capillaries with coatings consisting of neutral-hydrophilic, cationic and anionic polymers are commercially available.
Electrolytic solution parametersBuffer type and concentrations. Suitable buffers for capillary electrophoresis have an appropriate buffer capacity in the pH range of choice and low mobility to minimize current generation.To minimize band distortion, it is important to match buffer-ion mobility to solute mobility whenever possible. The type of sample solvent used is important to achieve on-column sample focusing, which increases separation efficiency and improves detection. Also, an increase in buffer concentration at a given pH decreases electroosmotic flow and solute velocity.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
228
Buffer pH. The pH of the buffer can affect separation by modifying the charge of the analyte or additives and by changing the electroosmotic flow. For protein and peptide separation, a change in the pH of the buffer from above the isoelectric point (pI) to below the pI changes the net charge of the solute from negative to positive. An increase in the buffer pH generally increases the electroosmotic flow.Organic solvents. Organic modifiers, such as methanol, acetonitrile and others may be added to the aqueous buffer to increase the solubility of the solute or other additives and/or to affect the ionization degree of the sample components. The addition of these organic modifiers to the buffer generally causes a decrease in the electroosmotic flow.Additives for chiral separations. To separate optical isomers, a chiral selector is added to the separation buffer. The most commonly used chiral selectors are cyclodextrins, although in some cases crown ethers, certain polysaccharides or even proteins can be used. Because chiral recognition is governed by the different interactions between the chiral selector and each of the enantiomers the resolution achieved for the chiral compounds depends largely on the type of chiral selector used. While developing a given separation it may be useful to test cyclodextrins having a different cavity size (α-, β-, or γ-cyclodextrin) or modified cyclodextrins with neutral (methyl, ethyl, hydroxyalkyl, etc.) or ionizable (aminomethyl, carboxymethyl, sulfobutylether, etc.) moities. When using modified cyclodextrins, batch-to-batch variations in the degree of substitution of the cyclodextrins must be taken into account because it will influence the selectivity. The resolution of chiral separations is also controlled by the concentration of the chiral selector, the composition and pH of the buffer and the separation temperature. Organic additives, such as methanol or urea, can also affect the resolution of separation.
Capillary gel electrophoresisIn capillary gel electrophoresis, separation takes place inside a capillary filled with a gel that acts as a molecular sieve. Molecules with similar charge-to-mass ratios are separated according to molecular size because smaller molecules move more freely through the network of the gel and therefore migrate faster than larger molecules. Different biological macromolecules (for example, proteins and DNA fragments), which often have similar charge-to-mass ratios, can thus be separated according to their molecular mass by capillary gel electrophoresis.Characteristics of gelsTwo types of gels are used in capillary electrophoresis: permanently coated gels and dynamically coated gels. Permanently coated gels are prepared inside the capillary by polymerization of monomers. One example of such a gel is a cross-linked polyacrylamide. This type of gel is usually bonded to the fused-silica wall and cannot be removed without destroying the capillary. For protein analysis under reducing conditions the separation buffer usually contains sodium dodecyl sulfate and the sample is denatured by heating in a mixture of sodium dodecyl sulfate and 2-mercaptoethanol or dithiothreitol before injection. When non-reducing conditions are used (for example, analysis of an intact antibody), 2-mercaptoethanol and dithiothreitol are not used. Optimization of separation in a cross-linked gel is obtained by modifying the separation buffer (see “Capillary zone electrophoresis”) and by controlling the gel porosity during the gel preparation. For cross-linked polyacrylamide gels the porosity can

229
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
be modified by changing the concentration of acrylamide and/or the ratio of the cross-linker. As a rule, a decrease in the porosity of the gel leads to a decrease in the mobility of the solutes. Due to the rigidity of this type of gel, only electrokinetic injection can be used.Dynamically coated gels are hydrophilic polymers (i.e. linear polyacrylamide, cellulose derivatives, dextran, etc.) which can be dissolved in aqueous separation buffers, giving rise to a separation medium that also acts as a molecular sieve. These polymeric separation media are easier to prepare than cross-linked polymers. They can be prepared in a vial and filled by pressure in a wall-coated capillary with no electroosmotic flow. Replacing the gel before every injection generally improves the separation reproducibility. The porosity of the dynamically coated gels can be increased by using polymers of higher molecular mass (at a given polymer concentration) or by decreasing the polymer concentration (for a given polymer molecular mass). A decrease in gel porosity leads to a decrease in the mobility of the solute for the same buffer. Both hydrodynamic and electrokinetic injection techniques can be used because the dissolution of these polymers in the buffer gives low viscosity solutions.
Capillary isoelectric focusingPrincipleIn isoelectric focusing the molecules migrate under the influence of the electric field, so long as they are charged, in a pH gradient generated by ampholytes having pI values in a wide range (polyaminocarboxylic acids), dissolved in the separation buffer.The three basic steps in capillary isoelectric focusing are loading, focusing and mobilization.Loading step. Two methods may be employed.Loading in one step: The sample is mixed with ampholytes and introduced into the capillary by pressure or vacuum.Sequential loading: A leading buffer, then the ampholytes, then the sample mixed with ampholytes, again ampholytes alone, and finally the terminating buffer are introduced into the capillary. The volume of the sample must be small enough so as not to modify the pH gradient.Focusing step. When the voltage is applied, ampholytes migrate toward the cathode or the anode according to their net charge, creating the pH gradient from anode (lower pH) to cathode (higher pH). During this step the components to be separated migrate until they reach a pH corresponding to their isoelectric point, and the current drops to very low values.Mobilization step. If mobilization is required for detection, use one of the following three methods.Method 1: Mobilization is accomplished during the focusing step, under the influence of
the electroosmotic flow when this flow is small enough to allow the focusing of the components.
Method 2: Mobilization is accomplished by application of positive pressure after the focusing step.
Method 3: Mobilization is achieved after the focusing step by adding salts to the cathode reservoir or the anode reservoir, depending on the direction chosen for mobilization, in order to alter the pH in the capillary when the voltage is applied.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
230
As the pH is changed the proteins and ampholytes are mobilized in the direction of the reservoir, which contains added salts and pass the detector.
The separation achieved is expressed as ΔpI and depends on the pH gradient (dpH/dx), the number of ampholytes having different pI values, the molecular diffusion coefficient (D), the intensity of the electric field (E) and the variation of the electrophoretic mobility of the analyte with the pH (−dµ/dpH):
OptimizationThe major parameters that need to be considered in the development of separations are the following:Voltage. The use of high fields from 300 V/cm to 1000 V/cm during the focusing step.Capillary. The electroosmotic flow must be reduced or suppressed depending on the mobilization strategy selected (see above). Coated capillaries tend to reduce the electroosmotic flow.Solutions. The anode buffer reservoir is filled with a solution of a lower pH than the pI of the most acidic ampholyte, and the cathode reservoir is filled with a solution with a higher pH than the pI of the most basic ampholyte. Phosphoric acid for the anode and sodium hydroxide for the cathode are frequently used.Addition of a polymer, like methylcellulose, in the ampholyte solution tends to suppress convective forces (if any) and electroosmotic flow by increasing the viscosity. Commercial ampholytes covering many pH ranges are available and may also be mixed to obtain an expanded pH range. Broad pH ranges are used to estimate the pI, whereas narrower ranges are employed to improve accuracy. Calibration can be made by correlating migration time with the pI of a series of standard protein markers. During the focusing step, precipitation of proteins at their pI can be prevented, if necessary, using buffer additives such as glycerol, surfactants, urea, or zwitterionic buffers. However, depending on the concentration, urea can denature proteins.
Micellar electrokinetic chromatographyPrincipleSeparation takes place in an electrolytic solution that contains a surfactant at a concentration above the critical micellar concentration (CMC). The solute molecules are distributed between the aqueous buffer and the pseudostationary phase composed by the micelles according to the solute’s partition coefficient. The technique can be considered as a hybrid of electrophoresis and chromatography. It is a technique that can be used for the separation of both neutral and charged solutes maintaining the efficiency, speed and instrumental suitability of capillary electrophoresis. One of the most widely used surfactants in micellar electrokinetic chrom atography (MEKC) is the anionic surfactant, sodium dodecyl sulfate, although other surfactants, such as cationic surfactant cetyl trimethyl ammonium salts, have also been used.

231
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
The separation mechanism is as follows. At neutral and alkaline pH, a strong electroosmotic flow is generated and moves the separation buffer ions in the direction of the cathode. If sodium dodecyl sulfate is used as surfactant the electrophoretic migration of the anionic micelle is in the opposite direction, towards the anode. As a result, the overall micelle migration velocity is slowed compared to the bulk flow of the electrolytic solution. In the case of neutral solutes, because the analyte can partition between the micelle and the aqueous buffer and has no electrophoretic mobility, the analyte migration velocity will depend only on the partition coefficient between the micelle and the aqueous buffer. In the electropherogram the peaks corresponding to each uncharged solute are always between that of the electroosmotic flow marker and that of the micelle; and the time elapsed between these two peaks is called the separation window. For electrically charged solutes the migration velocity depends on both the partition coefficient of the solute between the micelle and the aqueous buffer and on the electrophoretic mobility of the solute in the absence of micelles.
Since the mechanism in MEKC of neutral and weakly ionized solutes is essentially chromatographic, migration of the solute and resolution can be rationalized in terms of the retention factor of the solute (k΄), also referred to as mass distribution ratio (Dm), which is the ratio between the number of moles of solute in the micelle to those in the mobile phase. For a neutral compound, k΄ is given as follows:
in which tr is the migration time of the solute; t0 is the analysis time of the unretained solute obtained by injecting an electroosmotic flow marker that does not enter the micelle (e.g. methanol); tmc is the micelle migration time measured by injecting a micelle marker, such as Sudan III, which migrates continuously associated in the micelle; K is the partition coefficient of the solute; VS is the volume of the micellar phase; and VM is the volume of the mobile phase.
The resolution between two closely-migrating solutes (RS) is as follows:
in which N is the number of theoretical plates for one of the solutes; α is the selectivity; and ka΄ and kb΄ are retention factors for both solutes, respectively (kb΄ > ka΄).
Similar, but not identical, equations give k΄ and RS values for electrically charged solutes.
OptimizationThe main parameters to be considered in the development of separations by MEKC are instrumental and electrolytic solution parameters.Instrumental parametersVoltage. Separation time is inversely proportional to applied voltage. However, an increase in voltage can cause excessive heat production that gives rise to temperature gradients and viscosity gradients of the buffer in the cross section of the capillary. This effect can be significant with high conductivity buffers, such as those containing micelles. Poor heat dissipation causes band broadening and decreases resolution.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
232
Temperature. Variations in capillary temperature affect the partition coefficient of the solute between the buffer and the micelles, the critical micellar concentration and the viscosity of the buffer. These parameters contribute to the migration time of the solutes. The use of a good cooling system improves the reproducibility of the migration time for the solutes.
Capillary. As in capillary zone electrophoresis, length and internal diameter of the capillary contribute to analysis time and efficiency of separations. Increasing both effective length and total length can decrease the electrical fields, working at constant voltage, and will increase migration time and improve the separation efficiency. The internal diameter controls heat dissipation, for a given buffer and electrical field, and consequently broadening of the sample band.
Electrolytic solution parametersSurfactant type and concentration. The type of surfactant, as the stationary phase in chromatography, affects the resolution because it modifies separation selectively. The log k΄ of a neutral compound increases linearly with the concentration of surfactant in the mobile phase. When k΄ approaches the value of
resolution in MEKC reaches a maximum. Modifying the concentration of surfactant in the mobile phase changes the resolution.
Buffer pH. pH does not modify the partition coefficient of non-ionized solutes, but it can modify the electroosmotic flow in uncoated capillaries. A decrease in the buffer pH decreases the electroosmotic flow and, therefore, increases the resolution of the neutral solutes in MEKC, resulting in a longer analysis time.
Organic solvents. To improve MEKC separation of hydrophobic compounds, organic modifiers (methanol, propanol, acetonitrile, etc.) can be added to the electrolytic solution. The addition of these modifiers generally decreases migration time and selectivity of the separation. The addition of organic modifiers affects critical micellar concentration; thus, a given surfactant concentration can be used only with a certain percentage of organic modifier before the micellization is inhibited or adversely affected, resulting in the absence of micelles and, therefore, the absence of the partition. The dissociation of micelles in the presence of a high content of organic solvent does not always mean that the separation will no longer be possible, because in some cases, the hydrophobic interaction between the ionic surfactant monomer and the neutral solutes forms solvophobic complexes that can be separated electrophoretically.
Additives for chiral separations. For the separation of enantiomers using MEKC a chiral selector is included in the micellar system, either covalently bound to the surfactant or added to the micellar separation electrolyte. Micelles that have a moiety with chiral discrimination properties include salts, N-dodecanoyl-l-amino acids, bile salts, etc. Chiral resolution can also be achieved using chiral discriminators, such as cyclodextrins, added to the electrolytic solutions that contain micellized achiral surfactants.

233
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
Other additives. Selectivity can be modified by adding chemicals to the buffer. Addition of several types of cyclodextrins to the buffer is also used to reduce the interaction of hydrophobic solutes with the micelle, increasing the selectivity for this type of compound. The addition of substances able to modify solute-micelle interactions by adsorption on the latter has been used to improve the selectivity of the separations in MEKC. These additives may consist of a second surfactant (ionic or nonionic), which gives rise to mixed micelles or metallic cations that dissolve in the micelle and form coordination complexes with the solutes.
QuantificationPeak areas must be divided by the corresponding migration time to give the corrected area in order to compensate for the shift in migration time from run to run, thus reducing the variation of the response. Dividing the peak areas by migration time will also compensate for the different responses of sample constituents with different migration times. Where an internal standard is used, check that no peak of the substance to be examined is masked by that of the internal standard.
CalculationsFrom the values obtained, calculate the content of a component or components being determined. When indicated, the percentage of one (or more) components of the sample to be examined is calculated by determining the corrected area(s) of the peak(s) as a percentage of the total of the corrected areas of all the peaks, excluding those due to solvents or any added reagents (normalization procedure). The use of an automatic integration system (integrator or data acquisition and processing system) is recommended.
System suitability In order to check the behaviour of the capillary electrophoresis system, system suitability parameters are used. The choice of these parameters depends on the mode of capillary electrophoresis used. The parameters include the following: retention factor k΄ (used only for micellar electrokinetic chromatography), apparent number of theoretical plates (N), the symmetry factor (AS), and the resolution (RS). In previous sections the theoretical expressions for N and RS have been described but more practical equations that allow for the determination of these suitability parameters using the electropherograms are given below.
Apparent number of theoretical platesThe apparent number of N may be calculated from the formula:N = 5.54 (tR/wh)
2
in which tR is the migration time or distance along the baseline between the point of injection and the perpendicular dropped from the maximum of the peak corresponding to the component; and wh is the peak width at half-height.

Consultation documents WHO Drug Information Vol. 31, No. 2, 2017
234
ResolutionThe RS between peaks of similar heights of two components may be calculated from the formula:RS = 1.18 (tR2 − tR1)/(wh1 + wh2)tR2 > tR1
in which tR1 and tR2 are the migration times or distances along the baseline between the point of injection and the perpendiculars dropped from the maxima of two adjacent peaks; and wh1 and wh2 are the peak widths at half-height.
When appropriate the RS may also be calculated by measuring the height of the valley (Hv) between two partly resolved peaks in a standard preparation, the height of the smaller peak (Hp), and calculating the peak-to-valley ratio:p/v = Hp/Hv.
Symmetry factorThe symmetry factor of AS may be calculated using the formula:As = w0.05/2din which w0.05 is the width of the peak at one-twentieth of the peak height; and d is the distance between the perpendicular dropped from the peak maximum and the leading edge of the peak at one-twentieth of the peak height.
Other suitability parameters include tests for area repeatability (standard deviation of areas or of area/migration time) and tests for migration time repeatability (standard deviation of migration time). Migration time repeatability provides a test for the suitability of the capillary washing procedures. An alternative practice to avoid the lack of repeatability of the migration time is to use a migration time relative to an internal standard.
Signal-to-noise ratioA test for the verification of the signal-to-noise ratio for a standard preparation or the determination of the limit of quantification may also be useful for the determination of related substances. The detection limit and quantification limit correspond to a signal-to-noise ratio of 3 and 10, respectively. The signal-to-noise ratio (S/N) is calculated as follows:S/N = 2H/hin which H is the height of the peak corresponding to the component concerned in the electropherogram obtained with the specified reference solution, measured from the maximum of the peak to the extrapolated baseline of the signal observed over a distance equal to twenty times the width at half-height; and h is the range of the background in an electropherogram obtained after injection of a blank, observed over a distance equal to twenty times the width at the half-height of the peak in the electropherogram obtained with the prescribed reference solution and, if possible, situated equally around the place where this peak would be found.
***
235
WHO Drug Information Vol. 31, No. 2, 2017 Consultation documents
WHO Medicines quality guidelines
The following medicines quality-related guidelines have been posted for public comment on the WHO website. The respective working documents with line numbers are available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects.
▪ Good practices for desk assessment Guidance on good practices for desk assessment for compliance with good manufacturing practices, good laboratory practices and good clinical practices for marketing authorization of medical productsWorking document QAS/17.713 (May 2017)
Inspection of manufacturing, testing, clinical trial and distribution sites poses an increasing burden on regulatory authorities. It is therefore good practice to rely on inspection information from other trusted authorities as part of risk-based inspection planning, so that there is no on-site inspection without well-founded cause. This text aims to provide general guidance on performing desk assessments in lieu of onsite inspections.
▪ Considerations for requesting analysis of medicines samplesWorking document QAS/16.688/Rev.1 (May 2017)
▪ Model certificate of analysisWorking document QAS/16.687/Rev.1 (May 2017)
These two documents are revisions of 2002 guidance texts. The proposed updates take into account new trends and international developments.
▪ “SRA” collaborative procedureCollaborative procedure in the assessment and accelerated national registration of pharmaceutical products approved by stringent regulatory authorities Working document QAS/17.704 (March 2017)
This text proposes scheme for national medicines regulatory authorities and pharmaceutical companies (manufacturers) to facilitate registrations of medicines approved by stringent regulatory authorities.
▪ Good herbal processing practicesRevised Draft: WHO guidelines on good herbal processing practices (GHPP) for herbal medicinesWHO/SDS/TCM (March 2017)
This text proposes technical guidance on processing of herbs to produce herbal materials, of herbal materials to produce herbal preparations, and of herbal materials or herbal preparations to produce herbal dosage forms. å

236
WHO Drug Information Vol. 31, No. 2, 2017
ATC/DDD classificationThe Anatomical Therapeutic Chemical (ATC) classification system and the Defined Daily Dose (DDD) as a measuring unit are tools for exchanging and comparing data on drug use at international, national or local levels. The ATC/DDD system has become the gold standard for international drug utilization research. It is maintained by the WHO Collaborating Centre for Drug Statistics Methodology in Oslo, Norway. Visit www.whocc.no/ for more information.
ATC/DDD classification (temporary)
The following ATC codes and DDDs were agreed at the meeting of the WHO International Working Group for Drug Statistics Methodology in March 2017.Comments or objections to the decisions from the meeting should be forwarded to the WHO Collaborating Centre for Drug Statistics Methodology before 1 September 2017. If no objections are received before this date, the new ATC codes and DDDs will be considered final and included in the January 2018 version of the ATC/DDD Index.
New ATC 5th level codesATC level name/INN ATC codeandexanet alfa V03AB38atorvastatin and perindopril C10BX15cenegermin S01XA24colecalciferol, combinations A11CC55cytisine N07BA04dolutegravir and rilpivirine J05AR21durvalumab L01XC28emicizumab B02BX06emtricitabine, tenofovir alafenamide and bictegravir J05AR20emtricitabine, tenofovir alafenamide, darunavir and cobicistat J05AR22erenumab N02CX07ermekumab L01XC29evogliptin A10BH07fimasartan and diuretics C09DA10formoterol, glycopyrronium bromide and beclometasone R03AL09guselkumab L04AC16ivacaftor and tezacaftor R07AX31lifitegrast S01XA25metformin and evogliptin A10BD22nusinersen M09AX07
Continued

237
WHO Drug Information Vol. 31, No. 2, 2017 ACT/DDD classification
Temporary
New ATC 5th level codes (continued)ATC level name/INN ATC codeoxycodone and naltrexone N02AA56plecanatide A06AX07polmacoxib M01AH07ropeginterferon alfa-2b L03AB15sirukumab L04AC15sofosbuvir, velpatasvir and voxilaprevir J05AP56tavaborole D01AE24vestronidase alfa A16AB18vilanterol, umeclidinium bromide and fluticasone furoate R03AL08
Change of ATC level namesPrevious New ATC codeeptacog alfa coagulation factor VIIa B02BD08
New DDDsATC level name/INN DDD unit Adm.R* ATC codebrexpiprazole 3 mg O N05AX16cyclizine 0.1 g P R06AE03etelcalcetide 2.1 mg P H05BX04evogliptin 5 mg O A10BH07ixekizumab 2.9 mg P L04AC13levomethadone 15 mg O N07BC05methotrexate 2.5 mg P L04AX03obeticholic acid 10 mg O A05AA04plecanatide 3 mg O A06AX07reslizumab 7.5 mg1) P R03DX08tenofovir alafenamide 25 mg O J05AF13
* Administration Route: O = oral; P = parenteral.1) DDD remains temporary for another period.
Changes of DDDsATC level name/INN Previous DDD New DDD ATC code
DDD Unit Adm.R.* DDD Unit Adm.R.*glycopyrronium bromide 3 mg P 0.3 mg P A03AB02
* Administration Route: O = oral; P = parenteral.
WHO Collaborating CentreOslo, May 2017

ACT/DDD classification WHO Drug Information Vol. 31, No. 2, 2017
238
ATC/DDD classification (final)
The following ATC codes, DDDs and alterations were agreed at the meeting of the WHO International Working Group for Drug Statistics Methodology in October 2016. These are considered as final and will be included in the January 2018 version of the ATC/DDD Index.
New ATC 5th level codesATC level name/INN ATC codebenralizumab R03DX10binimetinib L01XE41brigatinib L01XE43cerliponase alfa A16AB17dupilumab D11AH05eteplirsen M09AX06etirinotecan pegol L01XX56hydromorphone and naloxone N02AA53idursulfase beta A16AB16insulin glargine and lixisenatide A10AE54Lavandulae aetheroleum N05BX05lutetium (177Lu) oxodotreotide V10XX04mepyramine theophyllinacetate R03DA12migalastat A16AX14netarsudil S01EX05niraparib L01XX54obiltoxaximab J06BB22olaratumab L01XC27opicapone N04BX04ozenoxacin D06AX14padeliporfin L01XD07pegteograstim L03AA17plitidepsin L01XX57ramipril, amlodipine and hydrochlorothiazide C09BX03rebamipide A02BX14ribociclib L01XE42romosozumab M05BX06rosuvastatin, amlodipine and perindopril C10BX14rosuvastatin, perindopril and indapamide C10BX13rucaparib L01XX55semaglutide A10BJ06sodium zirconium cyclosilicate V03AE10sofosbuvir and velpatasvir J05AX691)
suvorexant N05CM19Continued

239
WHO Drug Information Vol. 31, No. 2, 2017 ACT/DDD classification
Final
New ATC 5th level codes (continued)ATC level name/INN ATC codetetracaine, combinations N01BA53velmanase alfa A16AB15zoster, purified antigen J07BK03
1) The ATC code will be altered to J05AP55 in connection with the implementation of the new ATC 4th level J05AP Antivirals for treatment of HCV infections in 2018.
New ATC level codes (other than 5th levels) ATC level name/INN ATC codeAntivirals for treatment of HCV infections J05AP
Change of ATC codesATC level name/INN Previous ATC New ATCargipressin H01BA06 H01BA011)
asunaprevir J05AE15 J05AP06benzydamine A01AD022) R02AX03boceprevir J05AE12 J05AP03ceftriaxone, combinations J01DD543) J01DD63daclatasvir J05AX14 J05AP07dasabuvir J05AX16 J05AP09dasabuvir, ombitasvir, paritaprevir and ritonavir J05AX66 J05AP52elbasvir and grazoprevir J05AX68 J05AP54faldaprevir J05AE13 J05AP04ombitasvir, paritaprevir and ritonavir J05AX67 J05AP53ribavirin J05AB04 J05AP01simeprevir J05AE14 J05AP05sofosbuvir J05AX15 J05AP08sofosbuvir and ledipasvir J05AX65 J05AP51telaprevir J05AE11 J05AP02
1) ATC level name altered to vasopressin (argipressin).2) Split of code. Alteration of ATC code applies only for benzydamine lozenges.3) Split of code. Combinations of ceftriaxone and other substances remain in J01DD54 while combinations
of ceftriaxone and beta-lactamase inhibitors are moved to J01DD63.
Change of ATC level names
Previous New ATC codeamoxicillin and enzyme inhibitor amoxicillin and beta-lactamase inhibitor J01CR02ampicillin and enzyme inhibitor ampicillin and beta-lactamase inhibitor J01CR01Bile acid preparations Bile acids and derivatives A05AAcefoperazone, combinations cefoperazone and beta-lactamase inhibitor J01DD62
cefotaxime, combinations cefotaxime and beta-lactamase inhibitor J01DD51Continued
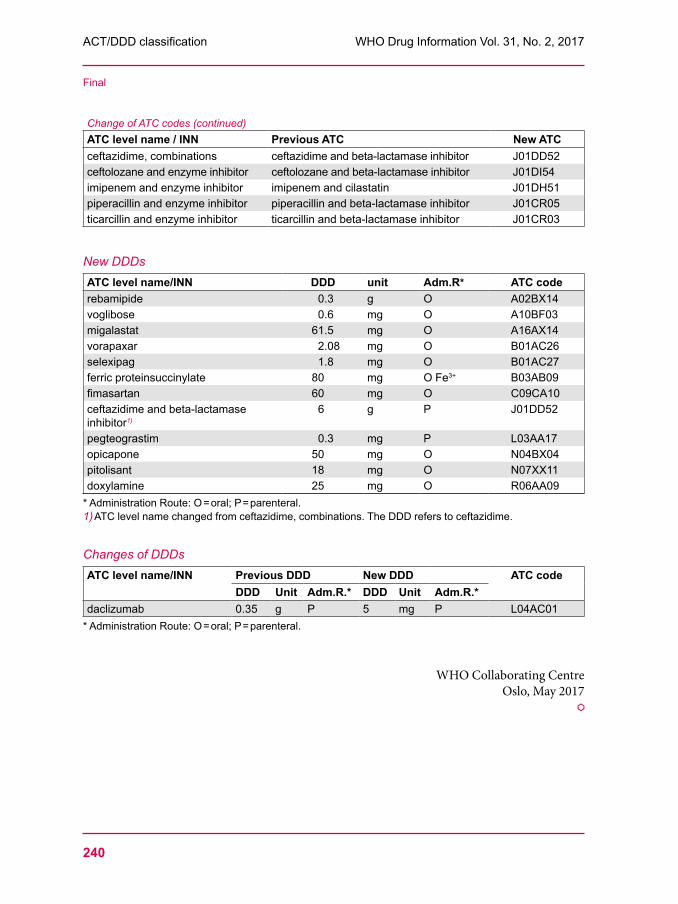
ACT/DDD classification WHO Drug Information Vol. 31, No. 2, 2017
240
Final
Change of ATC codes (continued)ATC level name / INN Previous ATC New ATCceftazidime, combinations ceftazidime and beta-lactamase inhibitor J01DD52ceftolozane and enzyme inhibitor ceftolozane and beta-lactamase inhibitor J01DI54imipenem and enzyme inhibitor imipenem and cilastatin J01DH51piperacillin and enzyme inhibitor piperacillin and beta-lactamase inhibitor J01CR05ticarcillin and enzyme inhibitor ticarcillin and beta-lactamase inhibitor J01CR03
New DDDsATC level name/INN DDD unit Adm.R* ATC coderebamipide 0.3 g O A02BX14voglibose 0.6 mg O A10BF03migalastat 61.5 mg O A16AX14vorapaxar 2.08 mg O B01AC26selexipag 1.8 mg O B01AC27ferric proteinsuccinylate 80 mg O Fe3+ B03AB09fimasartan 60 mg O C09CA10ceftazidime and beta-lactamase inhibitor1)
6 g P J01DD52
pegteograstim 0.3 mg P L03AA17opicapone 50 mg O N04BX04pitolisant 18 mg O N07XX11doxylamine 25 mg O R06AA09
* Administration Route: O = oral; P = parenteral.1) ATC level name changed from ceftazidime, combinations. The DDD refers to ceftazidime.
Changes of DDDsATC level name/INN Previous DDD New DDD ATC code
DDD Unit Adm.R.* DDD Unit Adm.R.*daclizumab 0.35 g P 5 mg P L04AC01
* Administration Route: O = oral; P = parenteral.
WHO Collaborating CentreOslo, May 2017
å
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
241
International Nonproprietary Names for Pharmaceutical Substances (INN)
Notice is hereby given that, in accordance with article 3 of the Procedure for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances, the names given in the list on the following pages are under consideration by the World Health Organization as Proposed International Nonproprietary Names. The inclusion of a name in the lists of Proposed International Nonproprietary Names does not imply any recommendation of the use of the substance in medicine or pharmacy.
Lists of Proposed (1–113) and Recommended (1–74) International Nonproprietary Names can be found in Cumulative List No. 16, 2015 (available in CD-ROM only). The statements indicating action and use are based largely on information supplied by the manufacturer. This information is merely meant to provide an indication of the potential use of new substances at the time they are accorded Proposed International Nonproprietary Names. WHO is not in a position either to uphold these statements or to comment on the efficacy of the action claimed. Because of their provisional nature, these descriptors will neither be revised nor included in the Cumulative Lists of INNs.
Dénominations communes internationales des Substances pharmaceutiques (DCI) Il est notifié que, conformément aux dispositions de l'article 3 de la Procédure à suivre en vue du choix de Dénominations communes internationales recommandées pour les Substances pharmaceutiques les dénominations ci-dessous sont mises à l'étude par l'Organisation mondiale de la Santé en tant que dénominations communes internationales proposées. L'inclusion d'une dénomination dans les listes de DCI proposées n'implique aucune recommandation en vue de l'utilisation de la substance correspondante en médecine ou en pharmacie.
On trouvera d'autres listes de Dénominations communes internationales proposées (1–113) et recommandées (1–74) dans la Liste récapitulative No. 16, 2015 (disponible sur CD-ROM seulement). Les mentions indiquant les propriétés et les indications des substances sont fondées sur les renseignements communiqués par le fabricant. Elles ne visent qu'à donner une idée de l'utilisation potentielle des nouvelles substances au moment où elles sont l'objet de propositions de DCI. L'OMS n'est pas en mesure de confirmer ces déclarations ni de faire de commentaires sur l'efficacité du mode d'action ainsi décrit. En raison de leur caractère provisoire, ces informations ne figureront pas dans les listes récapitulatives de DCI.
Denominaciones Comunes Internacionales para las Sustancias Farmacéuticas (DCI) De conformidad con lo que dispone el párrafo 3 del "Procedimiento de Selección de Denominaciones Comunes Internacionales Recomendadas para las Sustancias Farmacéuticas", se comunica por el presente anuncio que las denominaciones detalladas en las páginas siguientes están sometidas a estudio por la Organización Mundial de La Salud como Denominaciones Comunes Internacionales Propuestas. La inclusión de una denominación en las listas de las DCI Propuestas no supone recomendación alguna en favor del empleo de la sustancia respectiva en medicina o en farmacia.
Las listas de Denominaciones Comunes Internacionales Propuestas (1–113) y Recomendadas (1–74) se encuentran reunidas en Cumulative List No. 16, 2015 (disponible sólo en CD-ROM). Las indicaciones sobre acción y uso que aparecen se basan principalmente en la información facilitada por los fabricantes. Esta información tiene por objeto dar una idea únicamente de las posibilidades de aplicación de las nuevas sustancias a las que se asigna una DCI Propuesta. La OMS no está facultada para respaldar esas indicaciones ni para formular comentarios sobre la eficacia de la acción que se atribuye al producto. Debido a su carácter provisional, esos datos descriptivos no deben incluirse en las listas recapitulativas de DCI.

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
242
Proposed International Nonproprietary Names: List 117 Comments on, or formal objections to, the proposed names may be forwarded by any person to the INN Programme of the World Health Organization within four months of the date of their publication in WHO Drug Information, i.e., for List 117 Proposed INN not later than 6 November 2017. Publication date: 7 July 2017
Dénominations communes internationales proposées: Liste 117 Des observations ou des objections formelles à l'égard des dénominations proposées peuvent être adressées par toute personne au Programme des Dénominations communes internationales de l'Organisation mondiale de la Santé dans un délai de quatre mois à compter de la date de leur publication dans WHO Drug Information, c'est à dire pour la Liste 117 de DCI Proposées le 6 novembre 2017 au plus tard. Date de publication: 7 juillet 2017
Denominaciones Comunes Internacionales Propuestas: Lista 117 Cualquier persona puede dirigir observaciones u objeciones respecto de las denominaciones propuestas, al Programa de Denominaciones Comunes Internacionales de la Organización Mundial de la Salud, en un plazo de cuatro meses, contados desde la fecha de su publicación en WHO Drug Information, es decir, para la Lista 117 de DCI Propuestas el 6 de Noviembre de 2017 a más tardar. Fecha de publicación: 7 de Julio de 2017
Proposed INN (Latin, English, French, Spanish) DCI Proposée DCI Propuesta
Chemical name or description: Action and use: Molecular formula Chemical Abstracts Service (CAS) registry number: Graphic formula Nom chimique ou description: Propriétés et indications: Formule brute Numéro dans le registre du CAS: Formule développée Nombre químico o descripción: Acción y uso: Fórmula molecular Número de registro del CAS: Fórmula desarrollada
adafosbuvirum adafosbuvir propan-2-yl N-[(P5'S)-4'-fluoro-2'-C-methyl-P-O-phenyl-
5'-uridylyl]-L-alaninate antiviral
adafosbuvir N-[(P5'S)-4'-fluoro-2'-C-méthyl-P-O-phényl-5'-uridylyl]- L-alaninate de propan-2-yle antiviral
adafosbuvir N-[(P5'S)-4'-fluoro-2'-C-metil-P-O-fenil-5'-uridilil]-L-alaninato de propan-2-ilo antiviral
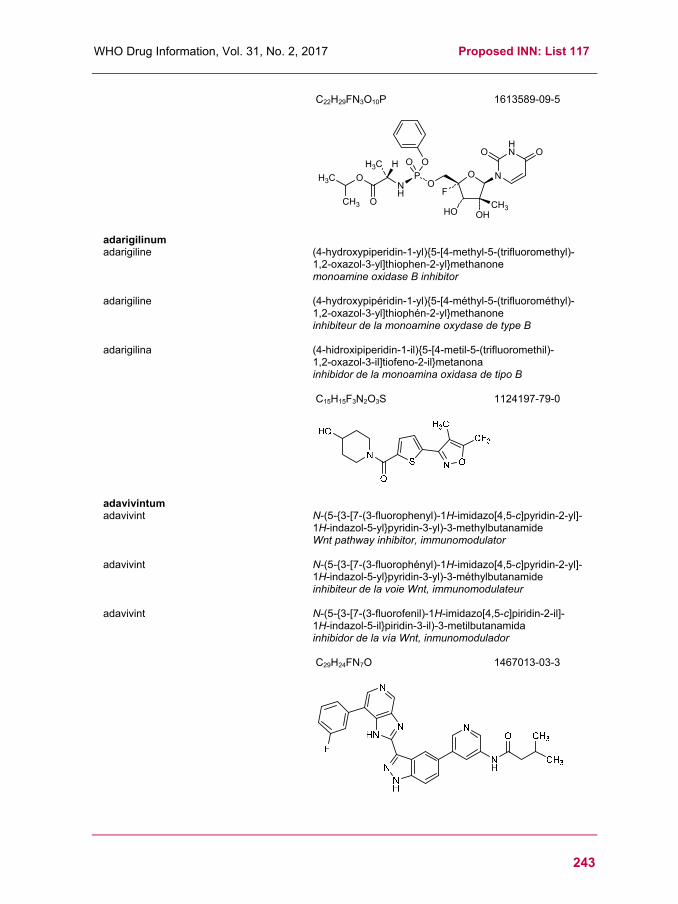
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
243
C22H29FN3O10P
1613589-09-5
adarigilinum adarigiline (4-hydroxypiperidin-1-yl){5-[4-methyl-5-(trifluoromethyl)-
1,2-oxazol-3-yl]thiophen-2-yl}methanone monoamine oxidase B inhibitor
adarigiline (4-hydroxypipéridin-1-yl){5-[4-méthyl-5-(trifluorométhyl)-1,2-oxazol-3-yl]thiophén-2-yl}methanone inhibiteur de la monoamine oxydase de type B
adarigilina (4-hidroxipiperidin-1-il){5-[4-metil-5-(trifluoromethil)- 1,2-oxazol-3-il]tiofeno-2-il}metanona inhibidor de la monoamina oxidasa de tipo B
C15H15F3N2O3S
1124197-79-0
adavivintum adavivint N-(5-{3-[7-(3-fluorophenyl)-1H-imidazo[4,5-c]pyridin-2-yl]-
1H-indazol-5-yl}pyridin-3-yl)-3-methylbutanamide Wnt pathway inhibitor, immunomodulator
adavivint N-(5-{3-[7-(3-fluorophényl)-1H-imidazo[4,5-c]pyridin-2-yl]-1H-indazol-5-yl}pyridin-3-yl)-3-méthylbutanamide inhibiteur de la voie Wnt, immunomodulateur
adavivint N-(5-{3-[7-(3-fluorofenil)-1H-imidazo[4,5-c]piridin-2-il]- 1H-indazol-5-il}piridin-3-il)-3-metilbutanamida inhibidor de la vía Wnt, inmunomodulador
C29H24FN7O
1467013-03-3
O N
HN
OP
NH
OH3C
O OOO
HO OHCH3
OCH3
HH3C
F
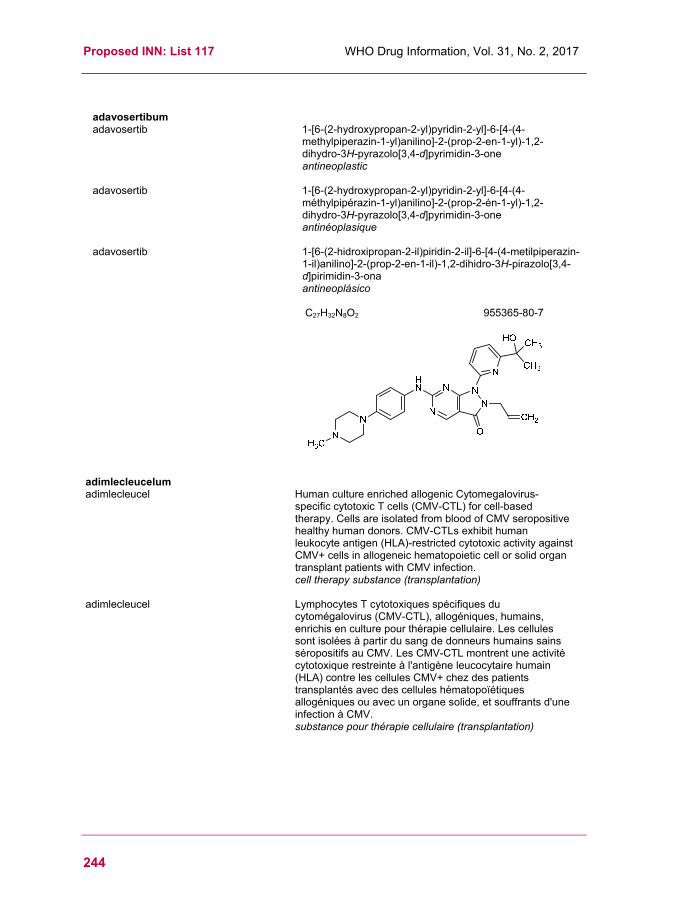
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
244
adavosertibum adavosertib 1-[6-(2-hydroxypropan-2-yl)pyridin-2-yl]-6-[4-(4-
methylpiperazin-1-yl)anilino]-2-(prop-2-en-1-yl)-1,2-dihydro-3H-pyrazolo[3,4-d]pyrimidin-3-one antineoplastic
adavosertib 1-[6-(2-hydroxypropan-2-yl)pyridin-2-yl]-6-[4-(4-méthylpipérazin-1-yl)anilino]-2-(prop-2-én-1-yl)-1,2-dihydro-3H-pyrazolo[3,4-d]pyrimidin-3-one antinéoplasique
adavosertib 1-[6-(2-hidroxipropan-2-il)piridin-2-il]-6-[4-(4-metilpiperazin-1-il)anilino]-2-(prop-2-en-1-il)-1,2-dihidro-3H-pirazolo[3,4-d]pirimidin-3-ona antineoplásico
C27H32N8O2
955365-80-7
adimlecleucelum adimlecleucel Human culture enriched allogenic Cytomegalovirus-
specific cytotoxic T cells (CMV-CTL) for cell-based therapy. Cells are isolated from blood of CMV seropositive healthy human donors. CMV-CTLs exhibit human leukocyte antigen (HLA)-restricted cytotoxic activity against CMV+ cells in allogeneic hematopoietic cell or solid organ transplant patients with CMV infection. cell therapy substance (transplantation)
adimlecleucel Lymphocytes T cytotoxiques spécifiques du cytomégalovirus (CMV-CTL), allogéniques, humains, enrichis en culture pour thérapie cellulaire. Les cellules sont isolées à partir du sang de donneurs humains sains séropositifs au CMV. Les CMV-CTL montrent une activité cytotoxique restreinte à l'antigène leucocytaire humain (HLA) contre les cellules CMV+ chez des patients transplantés avec des cellules hématopoïétiques allogéniques ou avec un organe solide, et souffrants d'une infection à CMV. substance pour thérapie cellulaire (transplantation)
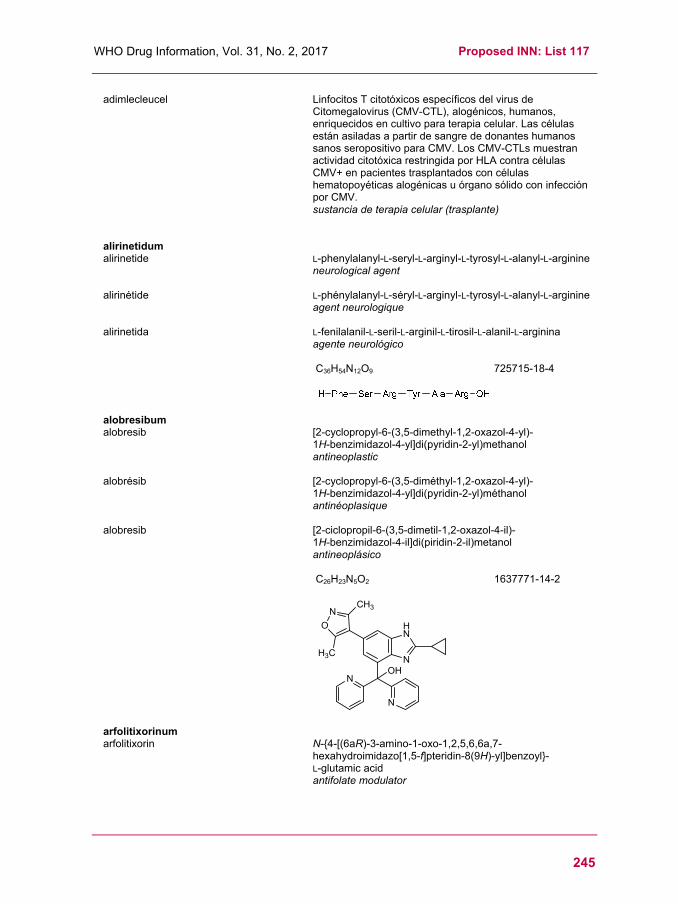
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
245
adimlecleucel Linfocitos T citotóxicos específicos del virus de Citomegalovirus (CMV-CTL), alogénicos, humanos, enriquecidos en cultivo para terapia celular. Las células están asiladas a partir de sangre de donantes humanos sanos seropositivo para CMV. Los CMV-CTLs muestran actividad citotóxica restringida por HLA contra células CMV+ en pacientes trasplantados con células hematopoyéticas alogénicas u órgano sólido con infección por CMV. sustancia de terapia celular (trasplante)
alirinetidum alirinetide L-phenylalanyl-L-seryl-L-arginyl-L-tyrosyl-L-alanyl-L-arginine
neurological agent
alirinétide L-phénylalanyl-L-séryl-L-arginyl-L-tyrosyl-L-alanyl-L-arginine agent neurologique
alirinetida L-fenilalanil-L-seril-L-arginil-L-tirosil-L-alanil-L-arginina agente neurológico
C36H54N12O9
725715-18-4
alobresibum alobresib [2-cyclopropyl-6-(3,5-dimethyl-1,2-oxazol-4-yl)-
1H-benzimidazol-4-yl]di(pyridin-2-yl)methanol antineoplastic
alobrésib [2-cyclopropyl-6-(3,5-diméthyl-1,2-oxazol-4-yl)- 1H-benzimidazol-4-yl]di(pyridin-2-yl)méthanol antinéoplasique
alobresib [2-ciclopropil-6-(3,5-dimetil-1,2-oxazol-4-il)- 1H-benzimidazol-4-il]di(piridin-2-il)metanol antineoplásico
C26H23N5O2
1637771-14-2
arfolitixorinum arfolitixorin N-{4-[(6aR)-3-amino-1-oxo-1,2,5,6,6a,7-
hexahydroimidazo[1,5-f]pteridin-8(9H)-yl]benzoyl}- L-glutamic acid antifolate modulator
N
HN
N
O
CH3
H3C
N
N
OH

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
246
arfolitixorine acide N-{4-[(6aR)-3-amino-1-oxo-1,2,5,6,6a,7-
hexahydroimidazo[1,5-f]ptéridin-8(9H)-yl]benzoyl}- L-glutamique modulateur antifolate
arfolitixorina ácido N-{4-[(6aR)-3-amino-1-oxo-1,2,5,6,6a,7-hexahidroimidazo[1,5-f]pteridin-8(9H)-il]benzoil}- L-glutámico modulador antifolato
C20H23N7O6
31690-111-6
asivatrepum asivatrep (2E)-N-{(1R)-1-[3,5-difluoro-
4-(methanesulfonamido)phenyl]ethyl}-3-[2-propyl- 6-(trifluoromethyl)pyridin-3-yl]prop-2-enamide transient receptor potential vanilloid 1 (TRPV1) antagonist
asivatrep (2E)-N-{(1R)-1-[3,5-difluoro- 4-(méthanesulfonamido)phényl]éthyl}-3-[2-propyl- 6-(trifluorométhyl)pyridin-3-yl]prop-2-énamide antagoniste des récepteurs membranaires vanilloïdes sous-type 1
asivatrep (2E)-N-{(1R)-1-[3,5-difluoro- 4-(metanosulfonamido)fenil]etil}-3-[2-propil- 6-(trifluorometil)piridin-3-il]prop-2-enamida Antagonista de los receptores membranarios vaniloides subtipo 1
C21H22F5N3O3S
1005168-10-4
atabecestatum atabecestat N-{3-[(4S)-2-amino-4-methyl-4H-1,3-thiazin-4-yl]-
4-fluorophenyl}-5-cyanopyridine-2-carboxamide beta-secretase inhibitor

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
247
atabécestat N-{3-[(4S)-2-amino-4-méthyl-4H-1,3-thiazin-4-yl]- 4-fluorophényl}-5-cyanopyridine-2-carboxamide inhibiteur de la secrétase bêta
atabecestat N-{3-[(4S)-2-amino-4-metil-4H-1,3-tiazin-4-il]-4-fluorofenil}-5-cianopiridina-2-carboxamida inhibidor de la secretasa beta
C18H14FN5OS
1200493-78-2
atidortoxumabum # atidortoxumab immunoglobulin G1-kappa, anti-[Staphylococcus aureus
alpha toxin (AT, alpha-hemolysin, alpha-HL, hly, hla) and bi-component leukocidins (HlgAB, HlgCB, LukED, and LukSF (Panton-Valentine leukocidin, PVL)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-448) [Homo sapiens VH (IGHV4-38-2*01 (92.90%) -(IGHD) -IGHJ6*03) [9.7.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), hinge (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K2>del (448)) (120-448)], (222-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (95.80%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (228-228'':231-231'')-bisdisulfide immunomodulator
atidortoxumab immunoglobuline G1-kappa, anti-[Staphylococcus aureus toxine alpha (AT, hémolysine alpha, HL-alpha, hly, hla) et leucocidines à deux composants (HlgAB, HlgCB, LukED, LukSF (leucocidine de Panton-Valentine, PVL)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-448) [Homo sapiens VH (IGHV4-38-2*01 (92.90%) -(IGHD) -IGHJ6*03) [9.7.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), charnière (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K2>del (448)) (120-448)], (222-214')-disulfure avec la chaîne légère (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (95.80%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (228-228'':231-231'')-bisdisulfure immunomodulateur
atidortoxumab inmunoglobulina G1-kappa, anti-[Staphylococcus aureus toxina alfa (AT, hemolisina alfa, HL-alfa, hly, hla) y leucocidinas con dos componentes (HlgAB, HlgCB, LukED, LukSF (Panton-Valentine leukocidina, PVL)], Homo sapiens anticuerpo monoclonal;

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
248
cadena pesada gamma1 (1-448) [Homo sapiens VH
(IGHV4-38-2*01 (92.90%) -(IGHD) -IGHJ6*03) [9.7.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), bisagra (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K2>del (448)) (120-448)], (222-214')-disulfuro con la cadena ligera (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (95.80%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (228-228'':231-231'')-bisdisulfuro inmunomodulador
1939108-95-8
avadomidum avadomide rac-(3R)-3-(5-amino-2-methyl-4-oxoquinazolin-
3(4H)-yl)piperidine-2,6-dione antineoplastic
avadomide rac-(3R)-3-(5-amino-2-méthyl-4-oxoquinazolin- 3(4H)-yl)pipéridine-2,6-dione antinéoplasique
avadomida rac-(3R)-3-(5-amino-2-metil-4-oxoquinazolin- 3(4H)-il)piperidina-2,6-diona antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
249
C14H14N4O3
1015474-32-4
avalglucosidasum alfa # avalglucosidase alfa mutated human acid α-glucosidase produced in Chinese
hamster ovary (CHO) cells, glycoform alfa, conjugated to a synthetic branched hexasaccharide containing two terminal mannose-6-phosphate (M6P), via aminooxy linkers; [His143>Arg,Arg167>His,Val724>Ile]prepro-lysosomal α-glucosidase (EC=3.2.1.20) (human) (57-952)-peptide, expressed in CHO cells, glycoform alfa, with 5~9 sialyl end groups of glycan residues being oxidized and chemically modified to 5-acetamido-3,5,7-trideoxy-7-[(E)-(2-oxo-2-{2-[4-({O-(6-O-phosphono-α-D-mannopyranosyl)-(1→2)-O-α-D-mannopyranosyl-(1→6)-O-α-D-mannopyranosyl-(1→6)-O-[O-(6-O-phosphono-α-D-mannopyranosyl)-(1→2)-O-α-D-mannopyranosyl-(1→3)]-β-D-mannopyranosyl}oxy)butanoyl]hydrazinyl}ethoxy)imino]-β-L-arabino-2-heptulo-2,6-pyranosylonic acid groups enzyme replacement therapy
avalglucosidase alfa α-glucosidase acide humaine modifiée, produite dans des cellules ovariennes de hamster chinois (CHO), glycoforme alfa, liée à un hexasaccharide de synthèse dont les résidus terminaux sont deux mannose-6-phosphates via un groupe aminoxy; [His143>Arg,Arg167>His,Val724>Ile]prépro-α-glucosidase lysosomale (EC=3.2.1.20) (humaine) (57-952)-peptide, exprimé dans des cellules CHO, glycoforme alfa: 5~9 résidus sialyl terminaux sont oxidés et chimiquement modifiés en acide 5-acétamido-3,5,7-tridésoxy-7-[(E)-(2-oxo-2-{2-[4-({O-(6-O-phosphono-α-D-mannopyranosyl)-(1→2)-O-α-D-mannopyranosyl-(1→6)-O-α-D-mannopyranosyl-(1→6)-O-[O-(6-O-phosphono-α-D-mannopyranosyl)-(1→2)-O-α-D-mannopyranosyl-(1→3)]-β-D-mannopyranosyl}oxy)butanoyl]hydrazinyl}éthoxy)imino]-β-L-arabino-2-heptulo-2,6-pyranosylonique traitement enzymatique substitutif
avalglucosidasa alfa α-glucosidasa ácida humana modificada, producida en las células ováricas de hamster chino (CHO), glicoforma alfa, conjugada con un glicano hexasacarídico sintético que contiene dos manosa-6-fosfatos (M6Ps) terminales, vía un grupo aminoxi;

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
250
[His143>Arg,Arg167>His,Val724>Ile]prepro-α-glucosidasa lisosomal (EC=3.2.1.20) (humana) (57-952)-péptido, expresada en las células CHO, glicoforma alfa: con los 5~9 restos sialil terminales están oxidados y químicamente modificados en ácido 5-acetamido-3,5,7-tridesoxi-7-[(E)-(2-oxo-2-{2-[4-({O-(6-O-fosfono-α-D-manopiranosil)-(1→2)-O-α-D-manopiranosil-(1→6)-O-α-D-manopiranosil-(1→6)-O-[O-(6-O-fosfono-α-D-manopiranosil)-(1→2)-O-α-D-manopiranosil-(1→3)]-β-D-manopiranosil}oxi)butanoil]hidrazinil}etoxi)imino]-β-L-arabino-2-heptulo-2,6-piranosilónico tratamiento enzimático de sustitución
1802558-87-7
avapritinibum avapritinib (1S)-1-(4-fluorophenyl)-1-(2-{4-[6-(1-methyl-1H-pyrazol-
4-yl)pyrrolo[2,1-f][1,2,4]triazin-4-yl]piperazin-1-yl}pyrimidin-5-yl)ethan-1-amine tyrosine kinase inhibitor, antineoplastic
avapritinib (1S)-1-(4-fluorophényl)-1-(2-{4-[6-(1-méthyl-1H-pyrazol- 4-yl)pyrrolo[2,1-f][1,2,4]triazin-4-yl]pipérazin-1-yl}pyrimidin-5-yl)éthan-1-amine inhibiteur de la tyrosine kinase, antinéoplasique
avapritinib (1S)-1-(4-fluorofenil)-1-(2-{4-[6-(1-metil-1H-pirazol- 4-il)pirrolo[2,1-f][1,2,4]triazin-4-il]piperazin-1-il}pirimidin- 5-il)etan-1-amina inhibidor de la tirosina kinasa, antineoplásico
Sequence / Séquence / SecuenciaQQGASRPGPR DAQAHPGRPR AVPTQCDVPP NSRFDCAPDK AITQEQCEAR 50GCCYIPAKQG LQGAQMGQPW CFFPPSYPSY KLENLSSSEM GYTATLTRTT 100PTFFPKDILT LRLDVMMETE NRLHFTIKDP ANRRYEVPLE TPRVHSRAPS 150PLYSVEFSEE PFGVIVHRQL DGRVLLNTTV APLFFADQFL QLSTSLPSQY 200ITGLAEHLSP LMLSTSWTRI TLWNRDLAPT PGANLYGSHP FYLALEDGGS 250AHGVFLLNSN AMDVVLQPSP ALSWRSTGGI LDVYIFLGPE PKSVVQQYLD 300VVGYPFMPPY WGLGFHLCRW GYSSTAITRQ VVENMTRAHF PLDVQWNDLD 350YMDSRRDFTF NKDGFRDFPA MVQELHQGGR RYMMIVDPAI SSSGPAGSYR 400PYDEGLRRGV FITNETGQPL IGKVWPGSTA FPDFTNPTAL AWWEDMVAEF 450HDQVPFDGMW IDMNEPSNFI RGSEDGCPNN ELENPPYVPG VVGGTLQAAT 500ICASSHQFLS THYNLHNLYG LTEAIASHRA LVKARGTRPF VISRSTFAGH 550GRYAGHWTGD VWSSWEQLAS SVPEILQFNL LGVPLVGADV CGFLGNTSEE 600LCVRWTQLGA FYPFMRNHNS LLSLPQEPYS FSEPAQQAMR KALTLRYALL 650PHLYTLFHQA HVAGETVARP LFLEFPKDSS TWTVDHQLLW GEALLITPVL 700QAGKAEVTGY FPLGTWYDLQ TVPIEALGSL PPPPAAPREP AIHSEGQWVT 750LPAPLDTINV HLRAGYIIPL QGPGLTTTES RQQPMALAVA LTKGGEARGE 800LFWDDGESLE VLERGAYTQV IFLARNNTIV NELVRVTSEG AGLQLQKVTV 850LGVATAPQQV LSNGVPVSNF TYSPDTKVLD ICVSLLMGEQ FLVSWC 896
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro26-53 36-52 47-71 477-502 591-602 882-896
Glycosylation sites (N) / Sites de glycosylation (N) / Posiciones de glicosilación (N)Asn-84 Asn-177 Asn-334 Asn-414 Asn-596 Asn-826 Asn-869
Methionine S-oxide / S-Oxyde de méthionine / S-Óxido de metionina (~50 %)Met-66 Met-90 Met-116 Met-117
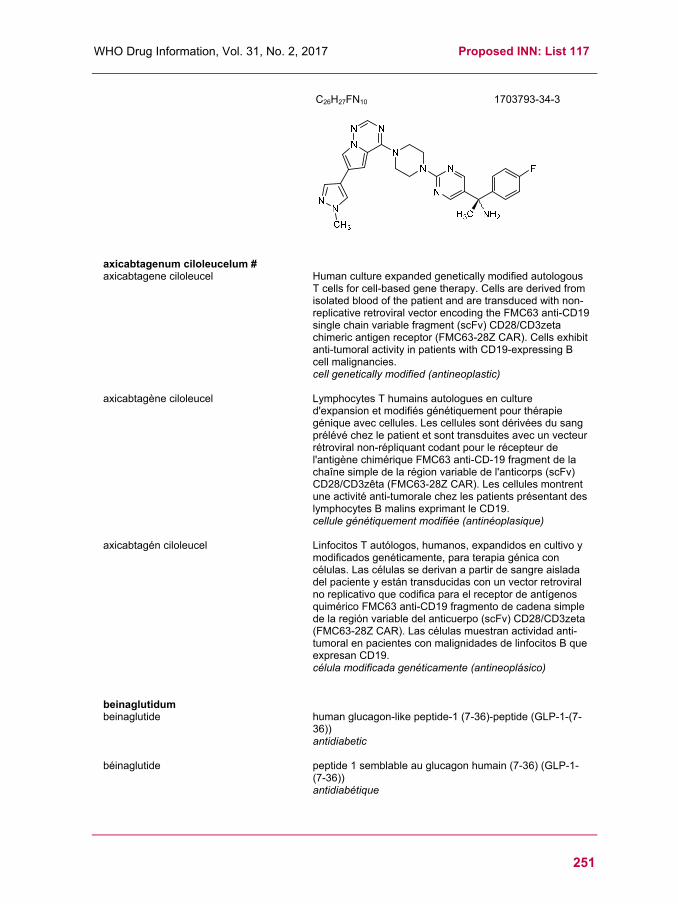
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
251
C26H27FN10
1703793-34-3
axicabtagenum ciloleucelum # axicabtagene ciloleucel Human culture expanded genetically modified autologous
T cells for cell-based gene therapy. Cells are derived from isolated blood of the patient and are transduced with non-replicative retroviral vector encoding the FMC63 anti-CD19 single chain variable fragment (scFv) CD28/CD3zeta chimeric antigen receptor (FMC63-28Z CAR). Cells exhibit anti-tumoral activity in patients with CD19-expressing B cell malignancies. cell genetically modified (antineoplastic)
axicabtagène ciloleucel Lymphocytes T humains autologues en culture d'expansion et modifiés génétiquement pour thérapie génique avec cellules. Les cellules sont dérivées du sang prélévé chez le patient et sont transduites avec un vecteur rétroviral non-répliquant codant pour le récepteur de l'antigène chimérique FMC63 anti-CD-19 fragment de la chaîne simple de la région variable de l'anticorps (scFv) CD28/CD3zêta (FMC63-28Z CAR). Les cellules montrent une activité anti-tumorale chez les patients présentant des lymphocytes B malins exprimant le CD19. cellule génétiquement modifiée (antinéoplasique)
axicabtagén ciloleucel Linfocitos T autólogos, humanos, expandidos en cultivo y modificados genéticamente, para terapia génica con células. Las células se derivan a partir de sangre aislada del paciente y están transducidas con un vector retroviral no replicativo que codifica para el receptor de antígenos quimérico FMC63 anti-CD19 fragmento de cadena simple de la región variable del anticuerpo (scFv) CD28/CD3zeta (FMC63-28Z CAR). Las células muestran actividad anti-tumoral en pacientes con malignidades de linfocitos B que expresan CD19. célula modificada genéticamente (antineoplásico)
beinaglutidum beinaglutide human glucagon-like peptide-1 (7-36)-peptide (GLP-1-(7-
36)) antidiabetic
béinaglutide peptide 1 semblable au glucagon humain (7-36) (GLP-1-(7-36)) antidiabétique

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
252
beinaglutida péptido tipo 1 similar al glucagón humano (7-36) (GLP-1-
(7-36)) hipoglucemiante
C149H225N39O46 123475-27-4
bemarituzumabum # bemarituzumab immunoglobulin G1-kappa, anti-[Homo sapiens FGFR2
(fibroblast growth factor receptor 2, keratinocyte growth factor receptor, KGFR, bacteria-expressed kinase, BEK, craniofacial dysostosis I, CFDI, Jackson-Weiss syndrome, JWS, CD332) isoform b (FGFR2b)], humanized monoclonal antibody; gamma1 heavy chain (1-444) [humanized VH (Homo sapiens IGHV1-46*01 (80.60%) -(IGHD) -IGHJ4*01) [8.8.7] (1-114) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (211) (115-212), hinge (213-227), CH2 (228-337), CH3 E12 (353), M14 (355) (338-442), CHS (443-444)) (115-444)], (217-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-33*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (223-223'':226-226'')-bisdisulfide immunomodulator, antineoplastic
bémarituzumab immunoglobuline G1-kappa, anti-[Homo sapiens FGFR2 (récepteur 2 du facteur de croissance des fibroblastes, récepteur du facteur de croissance des kératinocytes, KGFR, kinase exprimée dans des bactéries, BEK, dysostose craniofaciale I, CFDI, syndrome de Jackson-Weiss, JWS, CD332) isoforme b (FGFR2b)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-444) [VH humanisé (Homo sapiens IGHV1-46*01 (80.60%) -(IGHD) -IGHJ4*01) [8.8.7] (1-114) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (211) (115-212), charnière (213-227), CH2 (228-337), CH3 E12 (353), M14 (355) (338-442), CHS (443-444)) (115-444)], (217-214')-disulfure avec la chaîne légère (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-33*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (223-223'':226-226'')-bisdisulfure immunomodulateur, antinéoplasique
bemarituzumab inmunoglobulina G1-kappa, anti-[Homo sapiens FGFR2 (receptor 2 del factor de crecimiento de fibroblastos, receptor del factor de crecimiento de keratinocitos, KGFR, kinasa expresada en bacterias, BEK, disostosa craneofacial I, CFDI, síndrome de Jackson-Weiss, JWS, CD332) isoforma b (FGFR2b)], anticuerpo monoclonal humanizado;

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
253
cadena pesada gamma1 (1-444) [VH humanizado (Homo
sapiens IGHV1-46*01 (80.60%) -(IGHD) -IGHJ4*01) [8.8.7] (1-114) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (211) (115-212), bisagra (213-227), CH2 (228-337), CH3 E12 (353), M14 (355) (338-442), CHS (443-444)) (115-444)], (217-214')-disulfuro con la cadena ligera (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1-33*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (223-223'':226-226'')-bisdisulfuro inmunomodulador, antineoplásico
1952272-74-0
bemcentinibum bemcentinib 1-(6,7-dihydro-5H-benzo[6,7]cyclohepta[1,2-c]pyridazin-
3-yl)-N3-[(7S)-7-(pyrrolidin-1-yl)-6,7,8,9-tetrahydro- 5H-benzo[7]annulen-2-yl]-1H-1,2,4-triazole-3,5-diamine tyrosine kinase inhibitor, antineoplastic
bemcentinib 1-(6,7-dihydro-5H-benzo[6,7]cyclohepta[1,2-c]pyridazin- 3-yl)-N3-[(7S)-7-(pyrrolidin-1-yl)-6,7,8,9-tétrahydro- 5H-benzo[7]annulén-2-yl]-1H-1,2,4-triazole-3,5-diamine inhibiteur de la tyrosine kinase, antinéoplasique
bemcentinib 1-(6,7-dihidro-5H-benzo[6,7]ciclohepta[1,2-c]piridazin-3-il)-N3-[(7S)-7-(pirrolidin-1-il)-6,7,8,9-tetrahidro- 5H-benzo[7]anulen-2-il]-1H-1,2,4-triazol-3,5-diamina inhibidor de la tirosina kinasa, antineoplásico

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
254
C30H34N8
1037624-75-1
berdazimerum natricum berdazimer sodium polysodium poly[{[3-(methylamino)propyl]silasesquioxane}-
co-{[3-(1-methyl-2-nitroso-2-oxidohydrazin-1-yl)propyl]silasesquioxane}-co-silicate (1:3:6 x)], partially hydrolysed (Si : OH ~ 10 : 5) antimicrobial
berdazimère sodique poly[{[3-(méthylamino)propyl]silasesquioxane}-co-{[3-(1-méthyl-2-nitroso-2-oxidohydrazin-1-yl)propyl]silasesquioxane}-co-silicate (1:3:6 x)] polysodique, partiellement hydrolysé (Si : OH ~ 10 : 5) antimicrobien
berdazímero de sodio poli[{[3-(metilamino)propil]silasesquioxano}-co-{[3-(1-metil-2-nitroso-2-oxidohidrazin-1-il)propil]silasesquioxano}-co-silicato (1:3:6 x)] polisódico, parcialmente hidrolizado (Si : OH ~ 10 : 5) antimicrobiano
[(C4 H9 N3 Na O3.5 Si)3 (C4 H10 N O1.5 Si) (Si O2)6 (H O0.5)5]0.1n
1846565-00-1
NH
NN
N
N N
HN
NH2
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
255
berlimatoxumabum # berlimatoxumab immunoglobulin G1-kappa, anti-[Staphylococcus aureus
LukGH (LukAB) bi-component leukocidin], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-448) [Homo sapiens VH (IGHV4-39*01 (94.90%) -(IGHD) -IGHJ6*04) [10.7.11] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), hinge (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K2>del (448)) (120-448)], (222-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (94.70%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (228-228'':231-231'')-bisdisulfide immunomodulator
berlimatoxumab immunoglobuline G1-kappa, anti-[Staphylococcus aureus LukGH (Luk AB) leucocidine à deux composants], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-448) [Homo sapiens VH (IGHV4-39*01 (94.90%) -(IGHD) -IGHJ6*04) [10.7.11] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (CH1 (120-217), charnière (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K2>del (448)) (120-448)], (222-214')-disulfure avec la chaîne légère (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (94.70%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (228-228'':231-231'')-bisdisulfure immunomodulateur
berlimatoxumab inmunoglobulina G1-kappa, anti-[Staphylococcus aureus LukGH (Luk AB) leucocidina con dos componentes], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-448) [Homo sapiens VH (IGHV4-39*01 (94.90%) -(IGHD) -IGHJ6*04) [10.7.11] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (CH1 (120-217), bisagra(218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K2>del (448)) (120-448)], (222-214')-disulfuro con la cadena ligera (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (94.70%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (228-228'':231-231'')-bisdisulfuro inmunomodulador

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
256
1939109-24-6
berzosertibum berzosertib 3-(3-{4-[(methylamino)methyl]phenyl}-1,2-oxazol-5-yl)-
5-[4-(propane-2-sulfonyl)phenyl]pyrazin-2-amine antineoplastic
berzosertib 3-(3-{4-[(méthylamino)méthyl]phényl}-1,2-oxazol-5-yl)- 5-[4-(propane-2-sulfonyl)phenyl]pyrazin-2-amine antinéoplasique
berzosertib 3-(3-{4-[(metilamino)metil]fenil}-1,2-oxazol-5-il)- 5-[4-(propano-2-sulfonil)fenil]pirazin-2-amina antineoplásico
C24H25N5O3S
1232416-25-9
brexanolonum brexanolone 3α-hydroxy-5α-pregnan-20-one
antiepileptic
Heavy chain / Chaîne lourde / Cadena pesadaELQLQESGPG LVKPSETLSL TCTVSGGSIS SGSYYWDWIR QPPGKGLEWI 50GNIYKSGSTY YNPSLKSRVT ISVDTSKNQF SLKLSSVTAA DTAVYYCARE 100RGMHYMDVWG KGTTVTVSSA STKGPSVFPL APSSKSTSGG TAALGCLVKD 150YFPEPVTVSW NSGALTSGVH TFPAVLQSSG LYSLSSVVTV PSSSLGTQTY 200ICNVNHKPSN TKVDKKVEPK SCDKTHTCPP CPAPELLGGP SVFLFPPKPK 250DTLMISRTPE VTCVVVDVSH EDPEVKFNWY VDGVEVHNAK TKPREEQYNS 300TYRVVSVLTV LHQDWLNGKE YKCKVSNKAL PAPIEKTISK AKGQPREPQV 350YTLPPSRDEL TKNQVSLTCL VKGFYPSDIA VEWESNGQPE NNYKTTPPVL 400DSDGSFFLYS KLTVDKSRWQ QGNVFSCSVM HEALHNHYTQ KSLSLSPG 448
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS LSASVGDRVT ITCRASQSIN SYLNWYQQKP GKAPKLLIYA 50ASSLQSGVPS RFSGSGSGTD FTLTISSLQP EDFATYYCQQ QFDPPFTFGG 100GTKVEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Post-translational modificationsDisulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-97 146-202 263-323 369-427
22''-97'' 146''-202'' 263''-323'' 369''-427''Intra-L (C23-C104) 23'-88' 134'-194'
23'''-88''' 134'''-194'''Inter-H-L (h 5-CL 126) 222-214' 222''-214'''Inter-H-H (h 11, h 14) 228-228'' 231-231''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:299, 299''Fucosylated complex bi-antennary CHO-type glycans / glycanes de type CHO bi-antennairescomplexes fucosylés / glicanos de tipo CHO biantenarios complejos fucosiladosG0F 42.5%, G1F 39.8%
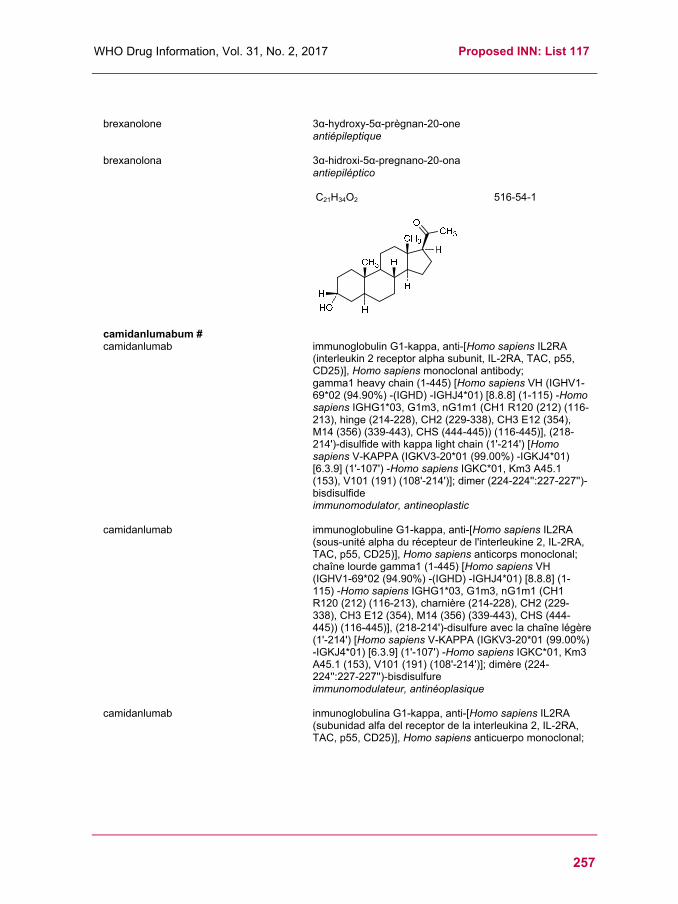
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
257
brexanolone 3α-hydroxy-5α-prègnan-20-one antiépileptique
brexanolona 3α-hidroxi-5α-pregnano-20-ona antiepiléptico
C21H34O2
516-54-1
camidanlumabum # camidanlumab immunoglobulin G1-kappa, anti-[Homo sapiens IL2RA
(interleukin 2 receptor alpha subunit, IL-2RA, TAC, p55, CD25)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-445) [Homo sapiens VH (IGHV1-69*02 (94.90%) -(IGHD) -IGHJ4*01) [8.8.8] (1-115) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (212) (116-213), hinge (214-228), CH2 (229-338), CH3 E12 (354), M14 (356) (339-443), CHS (444-445)) (116-445)], (218-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV3-20*01 (99.00%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (224-224'':227-227'')-bisdisulfide immunomodulator, antineoplastic
camidanlumab immunoglobuline G1-kappa, anti-[Homo sapiens IL2RA (sous-unité alpha du récepteur de l'interleukine 2, IL-2RA, TAC, p55, CD25)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-445) [Homo sapiens VH (IGHV1-69*02 (94.90%) -(IGHD) -IGHJ4*01) [8.8.8] (1-115) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (212) (116-213), charnière (214-228), CH2 (229-338), CH3 E12 (354), M14 (356) (339-443), CHS (444-445)) (116-445)], (218-214')-disulfure avec la chaîne légère (1'-214') [Homo sapiens V-KAPPA (IGKV3-20*01 (99.00%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (224-224'':227-227'')-bisdisulfure immunomodulateur, antinéoplasique
camidanlumab inmunoglobulina G1-kappa, anti-[Homo sapiens IL2RA (subunidad alfa del receptor de la interleukina 2, IL-2RA, TAC, p55, CD25)], Homo sapiens anticuerpo monoclonal;

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
258
cadena pesada gamma1 (1-445) [Homo sapiens VH (IGHV1-69*02 (94.90%) -(IGHD) -IGHJ4*01) [8.8.8] (1-115) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (212) (116-213), bisagra (214-228), CH2 (229-338), CH3 E12 (354), M14 (356) (339-443), CHS (444-445)) (116-445)], (218-214')-disulfuro con la cadena ligera (1'-214') [Homo sapiens V-KAPPA (IGKV3-20*01 (99.00%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (224-224'':227-227'')-bisdisulfuro inmunomodulador, antineoplásico
921618-45-3
camidanlumabum tesirinum # camidanlumab tesirine immunoglobulin G1-kappa, anti-[Homo sapiens IL2RA
(interleukin 2 receptor alpha subunit, IL-2RA, TAC, p55, CD25)], Homo sapiens monoclonal antibody conjugated to the pyrrolobenzodiazepine (PBD) dimer SCX; gamma1 heavy chain (1-445) [Homo sapiens VH (IGHV1-69*02 (94.90%) -(IGHD) -IGHJ4*01) [8.8.8] (1-115) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (212) (116-213), hinge (214-228), CH2 (229-338), CH3 E12 (354), M14 (356) (339-443), CHS (444-445)) (116-445)], (218-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV3-20*01 (99.00%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (224-224'':227-227'')-bisdisulfide; conjugated, on an average of 2 cysteines, to the pyrrolobenzodiazepine (PBD) dimer SCX, via a cleavable (valine-alanine dipeptide as cathepsine B cleavage site) maleimide type linker containing a spacer PEG (n=8) For the tesirine part, please refer to the prop.INN List 113, published in the WHO Drug Information, Vol.29, No.2, 2015.
immunomodulator, antineoplastic

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
259
camidanlumab tésirine
immunoglobuline G1-kappa, anti-[Homo sapiens IL2RA (sous-unité alpha du récepteur de l'interleukine 2, IL-2RA, TAC, p55, CD25)], Homo sapiens anticorps monoclonal conjugué au dimère de pyrrolobenzodiazépine (PDB) SCX; chaîne lourde gamma1 (1-445) [Homo sapiens VH (IGHV1-69*02 (94.90%) -(IGHD) -IGHJ4*01) [8.8.8] (1-115) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (212) (116-213), charnière (214-228), CH2 (229-338), CH3 E12 (354), M14 (356) (339-443), CHS (444-445)) (116-445)], (218-214')-disulfure avec la chaîne légère (1'-214') [Homo sapiens V-KAPPA (IGKV3-20*01 (99.00%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (224-224'':227-227'')-bisdisulfure; conjugué, sur 2 cystéines en moyenne, au dimère de pyrrolobenzodiazépine (PBD) SCX, via un linker clivable (dipeptide valine-alanine clivable par la cathepsine B) de type maléimide et comprenant un espaceur PEG (n=8) Pour la partie tésirine, veuillez vous référer à la Liste 113 des DCI prop, publiée dans le WHO Drug Information, Vol.29, No.2, 2015.
immunomodulateur, antinéoplasique
camidanlumab tesirina inmunoglobulina G1-kappa, anti-[Homo sapiens IL2RA (subunidad alfa del receptor de la interleukina 2, IL-2RA, TAC, p55, CD25)], Homo sapiens anticuerpo monoclonal conjugado con el dímero de pirrolobenzodiazepina (PDB) SCX; cadena pesada gamma1 (1-445) [Homo sapiens VH (IGHV1-69*02 (94.90%) -(IGHD) -IGHJ4*01) [8.8.8] (1-115) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (212) (116-213), bisagra (214-228), CH2 (229-338), CH3 E12 (354), M14 (356) (339-443), CHS (444-445)) (116-445)], (218-214')-disulfuro con la cadena ligera (1'-214') [Homo sapiens V-KAPPA (IGKV3-20*01 (99.00%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (224-224'':227-227'')-bisdisulfuro; conjugado, en una media de 2 cisteínas, al dímero de pirrolobenzodiazepina (PBD) SCX, mediante un espaciador escindible (dipéptido valina-alanina escindible por la catepsina B) de tipo maleimida que comprende un espaciador PEG (n=8) Para la fracción tesirina se puede referir a la Lista 113 de DCI prop., publicada en el WHO Drug Information, Vol.29, No.2, 2015. inmunomodulador, antineoplásico

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
260
1853239-04-9
canerpaturevum # canerpaturev Replication-competent, spontaneously occurring mutant of
Herpes Simplex Virus type 1 (HSV-1) with a number of deletions and insertions in the genome, resulting in the lack of functional expression of UL43, UL49.5, UL55 and UL56 antineoplastic
canerpaturev mutant spontané de Virus Herpes Simplex type 1 (HSV-1)
capable de se répliquer, avec un nombre de délétions et d'insertions dans le génome, résultant en l'absence de l'expression fonctionnelle des gènes UL43, UL49.5, UL55et UL56. antinéoplasique
canerpaturev Virus Herpes Simplex tipo 1 (HSV-1) competente de replicación, mutado espontáneamente, con un número de deleciones e inserciones en el genoma que dan como resultado la ausencia de expresión functional de los genes UL43, UL49.5, UL55 y UL56. antineoplásico
1662666-66-1

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
261
capivasertibum capivasertib 4-amino-N-[(1S)-1-(4-chlorophenyl)-3-hydroxypropyl]-1-
(1H-pyrrolo[2,3-d]pyrimidin-4-yl)piperidine-4-carboxamide antineoplastic
capivasertib 4-amino-N-[(1S)-1-(4-chlorophényl)-3-hydroxypropyl]-1-(1H-pyrrolo[2,3-d]pyrimidin-4-yl)pipéridine-4-carboxamide antinéoplasique
capivasertib 4-amino-N-[(1S)-1-(4-chlorofenil)-3-hidroxipropil]-1-(1H-pirrolo[2,3-d]pirimidin-4-il)piperidina-4-carboxamida antineoplásico
C21H25ClN6O2
1143532-39-1
cobomarsenum cobomarsen all-P-ambo-5-methyl-2'-O,4'-C-methylene-P-thiocytidylyl-
(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-5-methyl-2'-O,4'-C-methylene-P-thiocytidylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-5-methyl-2'-O,4'-C-methylene-P-thiouridylyl-(3'→5')-5-methyl-2'-O,4'-C-methylene-P-thiouridylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-O,4'-C-methylene-P-thioguanylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-O,4'-C-methylene-P-thioadenylyl-(3'→5')-5-methyl-2'-O,4'-C-methylene-P-thiouridylyl-(3'→5')-5-methyl-2'-O,4'-C-methylene-P-thiouridylyl-(3'→5')-2'-O,4'-C-methyleneadenosine antineoplastic
cobomarsen tout-P-ambo-5-méthyl-2'-O,4'-C-méthylène-P-thiocytidylyl-(3'→5')-2'-désoxy-P-thioadénylyl-(3'→5')-5-méthyl-2'-O,4'-C-méthylène-P-thiocytidylyl-(3'→5')-2'-désoxy-P-thioguanylyl-(3'→5')-2'-désoxy-P-thioadénylyl-(3'→5')-5-méthyl-2'-O,4'-C-méthylène-P-thiouridylyl-(3'→5')-5-méthyl-2'-O,4'-C-méthylène-P-thiouridylyl-(3'→5')-2'-désoxy-P-thioadénylyl-(3'→5')-2'-O,4'-C-méthylène-P-thioguanylyl-(3'→5')-2'-désoxy-P-thiocytidylyl-(3'→5')-2'-O,4'-C-méthylène-P-thioadénylyl-(3'→5')-5-méthyl-2'-O,4'-C-méthylène-P-thiouridylyl-(3'→5')-5-méthyl-2'-O,4'-C-méthylène-P-thiouridylyl-(3'→5')-2'-O,4'-C-méthylèneadénosine antinéoplasique

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
262
cobomarsén todo-P-ambo-5-metil-2'-O,4'-C-metileno-P-tiocitidilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-5-metil-2'-O,4'-C-metileno-P-tiocitidilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-5-metil-2'-O,4'-C-metileno-P-tiouridilil-(3'→5')-5-metil-2'-O,4'-C-metileno-P-tiouridilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-O,4'-C-metileno-P-tioguanilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-O,4'-C-metileno-P-tioadenilil-(3'→5')-5-metil-2'-O,4'-C-metileno-P-tiouridilil-(3'→5')-5-metil-2'-O,4'-C-metileno-P-tiouridilil-(3'→5')-2'-O,4'-C-metileneadenosina antineoplásico
C148H177N52O77P13S13
1848257-52-2
cofetuzumabum # cofetuzumab cofétuzumab
mmunoglobulin G1-kappa, anti-[Homo sapiens PTK7 (protein tyrosine kinase 7, colon carcinoma kinase 4, CCK4) extracellular domain], humanized monoclonal antibody; gamma1 heavy chain (1-448) [humanized VH (Homo sapiens IGHV1-3*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), hinge (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K>del (448)) (120-448)], (222-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV3-11*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dimer (228-228":231-231")-bisdisulfide immunomodulator, antineoplastic immunoglobuline G1-kappa, anti-[Homo sapiens PTK7 (protéine tyrosine kinase 7, kinase du cancer du côlon, CCK4) domaine extracellulaire], anticorps monoclonal humanisé;

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
263
chaîne lourde gamma1 (1-448) [VH humanisé (Homo sapiens IGHV1-3*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), charnière (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K>del (448)) (120-448)], (222-218')-disulfure avec la chaîne légère kappa (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV3-11*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dimère (228-228":231-231")-bisdisulfure immunomodulateur, antinéoplasique
cofetuzumab inmunoglobulina G1-kappa, anti-[Homo sapiens PTK7 (proteína tirosina kinasa 7, kinasa del cáncer de colon, CCK4) dominio extracelular], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-448) [VH humanizado (Homo sapiens IGHV1-3*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), bisagra (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K>del (448)) (120-448)], (222-218')-disulfuro con la cadena ligera kappa (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV3-11*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dímero (228-228":231-231")-bisdisulfuro inmunomodulador, antineoplásico
1869928-62-0

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
264
cofetuzumabum pelidotinum # cofetuzumab pelidotin immunoglobulin G1-kappa, anti-[Homo sapiens PTK7
(protein tyrosine kinase 7, colon carcinoma kinase 4, CCK4) extracellular domain], humanized monoclonal antibody, conjugated to auristatin-0101; gamma1 heavy chain (1-448) [humanized VH (Homo sapiens IGHV1-3*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), hinge (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K>del (448)) (120-448)], (222-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV3-11*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dimer (228-228":231-231")-bisdisulfide; conjugated, on an average of 4 cysteinyl, to auristatin-0101 (Aur0101), via a cleavable maleimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) type linker immunomodulator, antineoplastic
cofétuzumab pélidotine immunoglobuline G1-kappa, anti-[Homo sapiens PTK7 (protéine tyrosine kinase 7, kinase du cancer du côlon, CCK4) domaine extracellulaire], anticorps monoclonal humanisé, conjugué à l'auristatine-0101; immunoglobuline G1-kappa, anti-[Homo sapiens PTK7 (protéine tyrosine kinase 7, kinase du cancer du côlon, CCK4) domaine extracellulaire], anticorps monoclonal humanisé, conjugué à l'auristatine-0101; chaîne lourde gamma1 (1-448) [VH humanisé (Homo sapiens IGHV1-3*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), charnière (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K>del (448)) (120-448)], (222-218')-disulfure avec la chaîne légère kappa (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV3-11*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dimère (228-228":231-231")-bisdisulfure; conjugué, sur 4 cystéinyl en moyenne, à l'auristatine-0101 (Aur0101), via un linker clivable de type maléimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) immunomodulateur, antinéoplasique
cofetuzumab pelidotina inmunoglobulina G1-kappa, anti-[Homo sapiens PTK7 (proteína tirosina kinasa 7, kinasa de cáncer de colon, CCK4) dominio extracelular], anticuerpo monoclonal humanizado, conjugado con la auristatina-0101; cadena pesada gamma1 (1-448) [VH humanizado (Homo sapiens IGHV1-3*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (216) (120-217), bisagra (218-232), CH2 (233-342), CH3 D12 (358), L14 (360) (343-447), CHS K>del (448)) (120-448)], (222-218')-disulfuro con la cadena ligera kappa (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV3-11*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dímero (228-228":231-231")-bisdisulfuro;

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
265
conjugado, en una media de 3 a 4 restos cisteinil, con la
auristatina-0101 (Aur0101), mediante un conector escindible de tipo maleimidocaproil-valil-citrulinil-p-aminobenziloxicarbonil (mc-val-cit-PABC) inmunomodulador, antineoplásico
1869937-48-3
*C
4 / 8
HN
NH
N
CH3
O
H3C CH3O
HHO
NNH
CH3
HHO
H CH3
OO
CH3
H
CH3
CH3
H
H SN
H3C CH3O
O
NH
ONH
O
NH
H
H3C CH3
HN
O
NH2
NO
O
OH
H
S
NH2
CO2HH
CO2H
H
NHO
Q1
Heavy chain / Chaîne lourde / Cadena pesadaQVQLVQSGPE VKKPGASVKV SCKASGYTFT DYAVHWVRQA PGKRLEWIGV 50ISTYNDYTYN NQDFKGRVTM TRDTSASTAY MELSRLRSED TAVYYCARGN 100SYFYALDYWG QGTSVTVSSA STKGPSVFPL APSSKSTSGG TAALGCLVKD 150YFPEPVTVSW NSGALTSGVH TFPAVLQSSG LYSLSSVVTV PSSSLGTQTY 200ICNVNHKPSN TKVDKKVEPK SCDKTHTCPP CPAPELLGGP SVFLFPPKPK 250DTLMISRTPE VTCVVVDVSH EDPEVKFNWY VDGVEVHNAK TKPREEQYNS 300TYRVVSVLTV LHQDWLNGKE YKCKVSNKAL PAPIEKTISK AKGQPREPQV 350YTLPPSRDEL TKNQVSLTCL VKGFYPSDIA VEWESNGQPE NNYKTTPPVL 400DSDGSFFLYS KLTVDKSRWQ QGNVFSCSVM HEALHNHYTQ KSLSLSPG 448
Light chain / Chaîne légère / Cadena ligeraEIVLTQSPAT LSLSPGERAT LSCRASESVD SYGKSFMHWY QQKPGQAPRL 50LIYRASNLES GIPARFSGSG SGTDFTLTIS SLEPEDFAVY YCQQSNEDPW 100TFGGGTKLEI KRTVAAPSVF IFPPSDEQLK SGTASVVCLL NNFYPREAKV 150QWKVDNALQS GNSQESVTEQ DSKDSTYSLS STLTLSKADY EKHKVYACEV 200THQGLSSPVT KSFNRGEC 218
Post-translational modificationsDisulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-96 146-202 263-323 369-427
22''-96'' 146''-202'' 263''-323'' 369''-427''Intra-L (C23-C104) 23'-92' 138'-198'
23'''-92''' 138'''-198'''Inter-H-L (h 5-CL 126) * 222-218' 222''-218'''Inter-H-H (h 11, h 14) * 228-228'' 231-231''
Modified residues / résidus modifiés / restos modificados
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:299, 299''Fucosylated complex bi-antennary CHO-type glycans / glycanes de type CHO bi-antennairescomplexes fucosylés / glicanos de tipo CHO biantenarios complejos fucosilados.
crenigacestatum crenigacestat 4,4,4-trifluoro-N-[(2S)-1-{[(7S)-5-(2-hydroxyethyl)-6-oxo-
6,7-dihydro-5H-pyrido[3,2-a][3]benzoxazepin-7-yl]amino}-1-oxopropan-2-yl]butanamide gamma-secretase inhibitor, antineoplastic
crénigacestat 4,4,4-trifluoro-N-[(2S)-1-{[(7S)-5-(2-hydroxyéthyl)-6-oxo-6,7-dihydro-5H-pyrido[3,2-a][3]benzoxazépin-7-yl]amino}-1-oxopropan-2-yl]butanamide inhibiteur de la secrétase gamma, antinéoplasique
crenigacestat 4,4,4-trifluoro-N-[(2S)-1-{[(7S)-5-(2-hidroxietil)-6-oxo- 6,7-dihidro-5H-pirido[3,2-a][3]benzoxazepin-7-il]amino}- 1-oxopropan-2-il]butanamida inhibidor de la secretasa gamma, antineoplásico
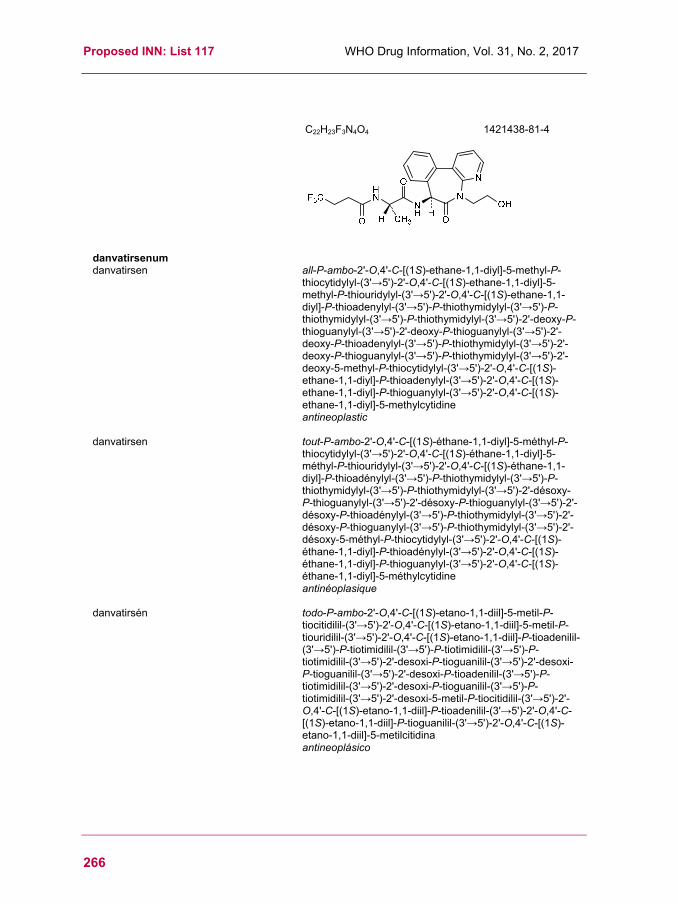
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
266
C22H23F3N4O4
1421438-81-4
danvatirsenum danvatirsen all-P-ambo-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-5-methyl-P-
thiocytidylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-5-methyl-P-thiouridylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-P-thioadenylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-5-methyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-P-thioadenylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-P-thioguanylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-5-methylcytidine antineoplastic
danvatirsen tout-P-ambo-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-5-méthyl-P-thiouridylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-P-thioadénylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-désoxy-P-thioguanylyl-(3'→5')-2'-désoxy-P-thioguanylyl-(3'→5')-2'-désoxy-P-thioadénylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-désoxy-P-thioguanylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-désoxy-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-P-thioadénylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-P-thioguanylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-5-méthylcytidine antinéoplasique
danvatirsén todo-P-ambo-2'-O,4'-C-[(1S)-etano-1,1-diil]-5-metil-P-tiocitidilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-5-metil-P-tiouridilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-P-tioadenilil-(3'→5')-P-tiotimidilil-(3'→5')-P-tiotimidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-5-metil-P-tiocitidilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-P-tioadenilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-P-tioguanilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-5-metilcitidina antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
267
C172H217N56O88P15S15
1402100-56-4
darvadstrocelum darvadstrocel Human culture expanded allogeneic adipose stromal
progenitor cells (eASC) for cell-based therapy. Cells are derived from isolated adipose tissue of healthy living donors. eASC express cell surface markers CD29, CD73, CD90 and CD105 and are capable to express factors such as vascular endothelial growth factor (VEGF), transforming growth factor-beta 1 (TGF-β1), interleukin-6 (IL-6), matrix metalloproteinase inhibitor-1 (TIMP-1), and interferon-gamma (IFN-γ) inducible indoleamine 2,3-dioxygenase (IDO). cell therapy substance (immunomodulator)
darvadstrocel Cellules progénitrices humaines allogéniques du stroma adipeux (eASC), en culture d'expansion, pour thérapie à base de cellules. Les cellules sont dérivées d'un tissu adipeux isolé à partir de donneurs vivants sains. Les eASC expriment les marqueurs de surface CD29, CD73, CD90 et
CD105 et sont capables d'exprimer les facteurs comme le facteur de croissance de l’endothélium vasculaire (VEGF), le facteur de croissance transformant beta 1 (TGF-β1), l'interleukine 6 (IL-6), l'inhibiteur tissulaire des métalloprotéases 1 (TIMP-1) et l'indoléamine 2,3-dioxygénase (IDO) induite par l'interféron gamma (IFN-γ). substance pour thérapie cellulaire (immunomodulateur)
darvadstrocel Células progenitoras del estroma adiposo alogénicas, humanas, expandidas en cultivo (eASC) para terapia celular. Las células se derivan a partir tejido adiposo aislado de donantes sanos vivos. Las eASC expresan los marcadores de superficie CD29, CD73, CD90 y CD105, y pueden expresar factores como el factor de crecimiento del endotelio vascular (VEGF), factor transformador del crecimiento beta 1 (TGF- β1), interleukina 6 (IL-6), inhibidor de metaloproteinasa de la matriz 1 (TIMP-1), e indoleamina 2,3- dioxigenasa (IDO) inducible por interferón gamma (IFN-γ) . sustancia de terapia génica (inmunomodulador)

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
268
davamotecanum pegadexamerum davamotecan pegadexamer α-acetyl-ω-{[(2RS)-2-hydroxypropyl]amino}poly[({bis[(4S)-
4-ethyl-3,14-dioxo-3,4,12,14-tetrahydro-1H-pyrano[3ʹ,4ʹ:6,7]indolizino[1,2-b]quinolin-4-yl] S,Sʹ-(6I,6IV-dideoxycyclomaltoheptaose-6I,6IV-diyl)bis(L-cysteinylglycinate)}-N2.1,N2.1'-diyl)(1-oxopropane-1,3-diyl)poly(oxyethylene)oxy(3-oxopropane-1,3-diyl)] antineoplastic
davamotécan pégadexamère α-acétyl-ω-{[(2RS)-2-hydroxypropyl]amino}poly[({bis[(4S)-4-éthyl-3,14-dioxo-3,4,12,14-tétrahydro-1H-pyrano[3ʹ,4ʹ:6,7]indolizino[1,2-b]quinolin-4-yl] S,Sʹ-(6I,6IV-didésoxycyclomaltoheptaose-6I,6IV-diyl)bis(L-cystéinylglycinate)}-N2.1,N2.1'-diyl)(1-oxopropane-1,3-diyl)poly(oxyéthylène)oxy(3-oxopropane-1,3-diyl)] antinéoplasique
davamotecán pegadexámero α-acetil-ω-{[(2RS)-2-hidroxipropil]amino}poli[({bis[(4S)-4-etil-3,14-dioxo-3,4,12,14-tetrahidro-1H-pirano[3ʹ,4ʹ:6,7]indolizino[1,2-b]quinolin-4-il] S,Sʹ-(6I,6IV-didesoxiciclomaltoheptaosa-6I,6IV-diil)bis(L-cisteinilglicinato)}-N2.1,N2.1'-diil)(1-oxopropano-1,3-diil)poli(oxietileno)oxi(3-oxopropano-1,3-diil)] antineoplásico
C2H3O-(C252H428N8O125S2)n-C3H8NO
1883668-61-8
delgocitinibum delgocitinib 3-[(3S,4R)-3-methyl-6-(7H-pyrrolo[2,3-d]pyrimidin-4-yl)-
1,6-diazaspiro[3.4]octan-1-yl]-3-oxopropanenitrile immunomodulator
delgocitinib 3-[(3S,4R)-3-méthyl-6-(7H-pyrrolo[2,3-d]pyrimidin-4-yl)- 1,6-diazaspiro[3.4]octan-1-yl]-3-oxopropanenitrile immunomodulateur
NH
O
m
HN
O
O
O
H3C
O
N
N
O
O S
HOHO
O
O
HO
HO OH
O
OH
OHO
HO
OO
OHHO
OH
O
O
OH
OH
O
O
O
HO
O
OHO
OH
OH
HO
OH
O
CH3
O
N
N
O
n
O
O
O NH
OOH
CH3
S
NHO
NH
H3C
O
O
O
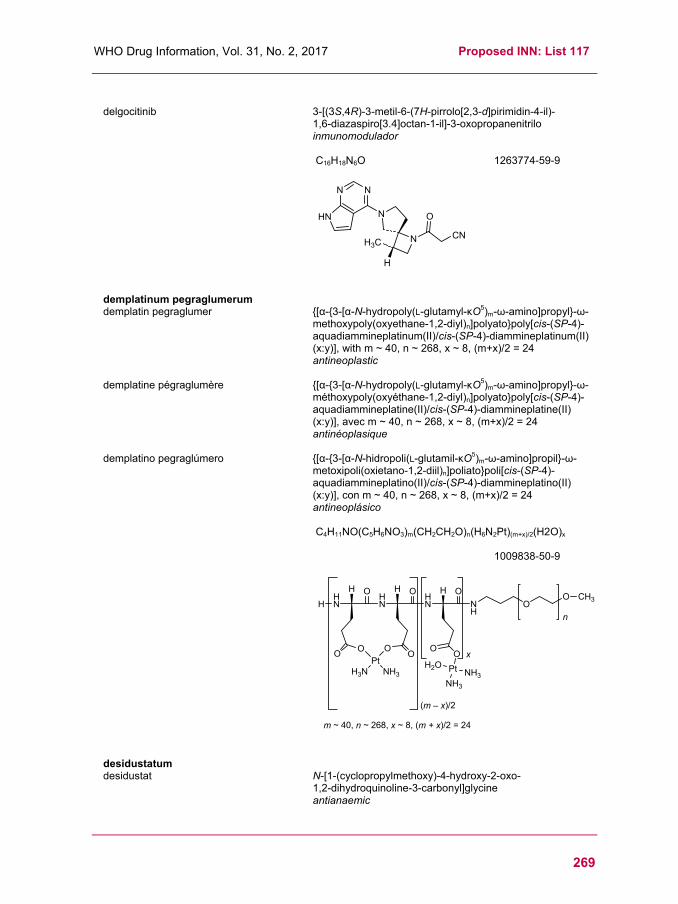
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
269
delgocitinib 3-[(3S,4R)-3-metil-6-(7H-pirrolo[2,3-d]pirimidin-4-il)-
1,6-diazaspiro[3.4]octan-1-il]-3-oxopropanenitrilo inmunomodulador
C16H18N6O
1263774-59-9
demplatinum pegraglumerum demplatin pegraglumer {[α-{3-[α-N-hydropoly(L-glutamyl-κO5)m-ω-amino]propyl}-ω-
methoxypoly(oxyethane-1,2-diyl)n]polyato}poly[cis-(SP-4)-aquadiammineplatinum(II)/cis-(SP-4)-diammineplatinum(II) (x:y)], with m ~ 40, n ~ 268, x ~ 8, (m+x)/2 = 24 antineoplastic
demplatine pégraglumère {[α-{3-[α-N-hydropoly(L-glutamyl-κO5)m-ω-amino]propyl}-ω-méthoxypoly(oxyéthane-1,2-diyl)n]polyato}poly[cis-(SP-4)-aquadiammineplatine(II)/cis-(SP-4)-diammineplatine(II) (x:y)], avec m ~ 40, n ~ 268, x ~ 8, (m+x)/2 = 24 antinéoplasique
demplatino pegraglúmero {[α-{3-[α-N-hidropoli(L-glutamil-κO5)m-ω-amino]propil}-ω-metoxipoli(oxietano-1,2-diil)n]poliato}poli[cis-(SP-4)-aquadiammineplatino(II)/cis-(SP-4)-diammineplatino(II) (x:y)], con m ~ 40, n ~ 268, x ~ 8, (m+x)/2 = 24 antineoplásico
C4H11NO(C5H6NO3)m(CH2CH2O)n(H6N2Pt)(m+x)/2(H2O)x
1009838-50-9
desidustatum desidustat N-[1-(cyclopropylmethoxy)-4-hydroxy-2-oxo-
1,2-dihydroquinoline-3-carbonyl]glycine antianaemic
N
N N
HN
N
O
CNH3C
H
HHN
OHN
H
OO
H
OO
PtNH3H3N
HN
O
NH
H O
OO
(m – x)/2
m ~ 40, n ~ 268, x ~ 8, (m + x)/2 = 24
Pt
NH3
H2ONH3
x
OO CH3
n

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
270
désidustat N-[1-(cyclopropylméthoxy)-4-hydroxy-2-oxo- 1,2-dihydroquinoléine-3-carbonyl]glycine antianémique
desidustat N-[1-(ciclopropilmetoxi)-4-hidroxi-2-oxo- 1,2-dihidroquinoleína-3-carbonil]glicina antianémico
C16H16N2O6
1616690-16-4
desmetramadolum desmetramadol rac-3-{(1R,2R)-2-[(dimethylamino)methyl]-
1-hydroxycyclohexyl}phenol central analgesic
desmétramadol rac-3-{(1R,2R)-2-[(diméthylamino)méthyl]- 1-hydroxycyclohexyl}phénol analgésique central
desmetramadol rac-3-{(1R,2R)-2-[(dimetilamino)metil]- 1-hidroxiciclohexil}fenol analgésico central
C15H23NO2
80456-81-1
efepoetinum alfa # efepoetin alfa human erythropoietin (epoetin alfa) fused to a hybrid
human immunoglobulin (Ig), consisting of the Fc fragment of the IgG4 fused to the hinge and amino-terminus of the IgD heavy chain isotype 2, produced in Chinese hamster ovary (CHO) cells, glycoform alfa; [human erythropoietin (EPO) (1-166)]-[immunoglobulin heavy chain delta (IGHD) isoform 2 constant region (133-170)-peptide (C-terminal hinge region and N-terminal CH2 domain) (167-204)]-[immunoglobulin heavy chain gamma 4 (IGHG4) constant region (121-327)-peptide (CH2 and CH3 domains) (205-411)]-fusion protein, produced in Chinese hamster ovary (CHO) cells, glycoform alfa antianaemic

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
271
éfépoétine alfa érythropoïétine humaine (époétine alfa) fusionée à une immunoglobuline (Ig) humaine hybride, consistant en un fragment Fc de l'IgG4 fusionné à la région charnière et à la chaîne lourde isotoype 2 de l'IgD sur la partie N-terminale, produite par des cellules ovariennes de hamster chinois (CHO), glycoforme alfa; [érythropoïétine humaine (EPO) (1-166)]-[région constante de la chaîne lourde delta de l'immunoglobuline (IGHD) isoforme 2 (133-170)-peptide (région charnière C-terminale et domaine CH2 N-terminal) (167-204)]-[région constante de la chaîne lourde de l'immunoglobuline gamma 4 (IGHG4) (121-327)-peptide (domaines CH2 et CH3) (205-411)]- protéine de fusion, produite par des cellules ovariennes de hamster chinois (CHO), glycoforme alfa antianémique
efepoetina alfa eritropoyetina humana (epoetina alfa) fusionada con una inmunoglobulina (Ig) humana híbrida, consistente en un fragmento Fc de la IgG4 fusionada con la región bisagra y con la cadena pesada isótopo 2 de la IgD sobre la parte N-terminal, producia por las células ováricas de hamster chino (CHO), glicoforma alfa; [eritropoyetina humana (EPO) (1-166)]-[región constante de la cadena pesada delta de la inmunoglobulina (IGHD) isoforma 2 (133-170)-péptido (región bisagra C-terminal y dominio CH2 N-terminal) (167-204)]-[región constante de la cadena pesada de la inmunoglobulina gamma 4 (IGHG4) (121-327)-péptido (dominios CH2 et CH3) (205-411)]- proteína de fusión, producida por las células ováricas de hamster chinos (CHO), glicoforma alfa antianémico
1905452-78-9

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
272
efizonerimodum alfa # efizonerimod alfa modified human immunoglobulin G4 Fc fragment fused to
tumor necrosis factor receptor-associated factor TRAF2 (human C-C domain fragment) and to the CD252 antigen (human extracellular domain fragment), hexamer, produced in Chinese hamster ovary (CHO) cells, glycoform alfa; modified human immunoglobulin G4 Fc fragment (1-229) [Homo sapiens IGHG4*01 del-CH1, [10-proline (S>P)]hinge] fusion protein with human TNF receptor-associated factor 2 (TRAF2)-(310-349)-peptide (230-269) fusion protein with des-(1-50)-human tumor necrosis factor ligand superfamily member 4 (TNFSF4, also known as CD252 or OX40L) (270-402), produced in Chinese hamster ovary (CHO) cells, non-covalent trimer of (8-8',11-11')-bisdisulfide dimers, glycoform alfa immunomodulator, antineoplastic
éfizonérimod alfa fragment Fc modifié de l’immunoglobuline G4 humaine, fusionné au facteur associé au récepteur du facteur de nécrose tumorale TRAF2 (fragment du domaine C-C humain) et à l’antigène CD252 (fragment du domaine extracellulaire humain), héxamère, produit dans des cellules ovariennes de hamster chinois (CHO), glycoforme alfa; fragment Fc modifié de l’immunoglobuline G4 humaine (1-229) [Homo sapiens IGHG4*01 del-CH1, [10-proline (S>P)]charnière] protéine de fusion avec le facteur 2 associé au récepteur du TNF humain (TRAF2)-(310-349)-peptide (230-269) protéine de fusion avec le dès-(1-50)- membre 4 de la superfamille des ligands du facteur de nécrose tumorale humain (TNFSF4, CD252, OX40L) (270-402), produit dans des cellules ovariennes de hamster chinois (CHO), trimère non-covalent de dimères (8-8',11-11')-bisdisulfure, glycoforme alfa immunomodulateur, antinéoplasique
efizonerimod alfa fragmento Fc modificado de la inmunoglobulina G4 humana, fusionada con el factor asociado al receptor del factor de necrosis tumoral TRAF2 (fragmento del dominio C-C humano) y al antígeno CD252 (fragmento del dominio extracelular humano), hexámero, producido en las células ováricas de hámsters chinos (CHO), glicoforma alfa; fragmento Fc modificado de la inmunoglobulina G4 humana (1-229) [Homo sapiens IGHG4*01 del-CH1, [10-prolina (S>P)]bisagra] proteína de fusión con el factor 2 asociado al receptor del TNF humano (TRAF2)-(310-349)-péptido (230-269) proteína de fusión con el des-(1-50)- miembro 4 de la superfamilia de los ligandos del factor de necrosis tumoral humano (TNFSF4, CD252, OX40L) (270-402), producido en las células ováricas de hámster chino (CHO), trímero no-covalente de dímeros (8-8',11-11')-bisdisulfuro dímero, glicoforma alfa inmunomodulador, antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
273
1635395-27-5
eflenograstimum alfa # eflenograstim alfa human granulocyte-colony stimulating factor (G-CSF)
fused to a hybrid human immunoglobulin consisting of the Fc fragment of the IgG4 fused to the hinge region and amino-terminus of the IgD heavy chain isotype 2, produced in Chinese hamster ovary (CHO) cells, glycoform alfa; [human granulocyte-colony stimulating factor (G-CSF) short isoform (1-174)]-[immunoglobulin heavy chain delta (IGHD) constant region isoform 2 (133-170)-peptide (C-terminal hinge and N-terminal CH2 domains) (175-212)]-[immunoglobulin heavy chain gamma 4 (IGHG4) constant region (121-327)-peptide (CH2 and CH3 domains) (213-419)]-fusion protein, (203-203')-disulfide dimer, produced in Chinese hamster ovary (CHO) cells, glycoform alfa granulocyte colony stimulating factor
éflénograstim alfa eflenograstim alfa
facteur stimulant les colonies de granulocytes humain (G-CSF) fusionné à une immunoglobuline (Ig) humaine hybride, consistant en un fragment Fc de l'IgG4 fusionné à la région charnière et à la chaîne lourde isotoype 2 de l'IgD sur la partie N-terminale, produit par des cellules ovariennes de hamster chinois (CHO), glycoforme alfa; [facteur stimulant les colonies de granulocytes humain (G-CSF) isoforme courte (1-174)]-[région constante de la chaîne lourde delta de l'immunoglobuline (IGHD) isoforme 2 (133-170)-peptide (région charnière C-terminale et domaine CH2 N-terminal) (175-212)]-[région constante de la chaîne lourde de l'immunoglobuline gamma 4 (IGHG4) (121-327)-peptide (domaines CH2 et CH3) (213-419)]-protéine de fusion, (203-203')-disulfure dimère, produit par des cellules ovariennes de hamster chinois (CHO), glycoforme alfa facteur de stimulation des colonies de granulocytes factor estimulante de las colonias de granulocitos humanos (G-CSF) fusionado con una inmunoglobulina (Ig) humana híbrida, consistente en un fragmento Fc de la IgG4 fusionado con la región bisagra y con la cadena pesada isótopo 2 de la IgD sobre la parte N-terminal, producido por las células ováricas de hamster chino (CHO), glicoforma alfa;

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
274
[factor estimulante de las colonias de granulocitos humanos (G-CSF) isoforma corta (1-174)]-[región constante de la cadena pesada delta de la inmunoglobulina (IGHD) isoforma 2 (133-170)-péptido (región bisagra C-terminal y dominio CH2 N-terminal) (175-212)]-[región constante de la cadena pesada de la inmunoglobulina gamma 4 (IGHG4) (121-327)-péptido (dominios CH2 y CH3) (213-419)]-proteína de fusión, (203-203')-disulfuro dímero, producido por las células ováricas de hamster chino (CHO), glicoforma alfa factor estimulante de las colonias de granulocitos
1905459-83-7
elenbecestatum elenbecestat N-{3-[(4aS,5R,7aS)-2-amino-5-methyl-4a,5-dihydro-
4H-furo[3,4-d][1,3]thiazin-7a(7H)-yl]-4-fluorophenyl}- 5-(difluoromethyl)pyrazine-2-carboxamide beta-secretase inhibitor
élenbécestat N-{3-[(4aS,5R,7aS)-2-amino-5-méthyl-4a,5-dihydro- 4H-furo[3,4-d][1,3]thiazin-7a(7H)-yl]-4-fluorophényl}- 5-(difluorométhyl)pyrazine-2-carboxamide inhibiteur de la secrétase bêta
elenbecestat N-{3-[(4aS,5R,7aS)-2-amino-5-metil-4a,5-dihidro- 4H-furo[3,4-d][1,3]tiazin-7a(7H)-il]-4-fluorofenil}- 5-(difluorometil)pirazina-2-carboxamida inhibidor de la secretasa beta
C19H18F3N5O2S
1388651-30-6
Monomer sequence / Séquence du monomère / Secuencia del monómeroTPLGPASSLP QSFLLKCLEQ VRKIQGDGAA LQEKLCATYK LCHPEELVLL 50GHSLGIPWAP LSSCPSQALQ LAGCLSQLHS GLFLYQGLLQ ALEGISPELG 100PTLDTLQLDV ADFATTIWQQ MEELGMAPAL QPTQGAMPAF ASAFQRRAGG 150VLVASHLQSF LEVSYRVLRH LAQPRNTGRG GEEKKKEKEK EEQEERETKT 200PECPSHTQPL GVFLFPPKPK DTLMISRTPE VTCVVVDVSQ EDPEVQFNWY 250VDGVEVHNAK TKPREEQFNS TYRVVSVLTV LHQDWLNGKE YKCKVSNKGL 300PSSIEKTISK AKGQPREPQV YTLPPSQEEM TKNQVSLTCL VKGFYPSDIA 350VEWESNGQPE NNYKTTPPVL DSDGSFFLYS RLTVDKSRWQ EGNVFSCSVM 400HEALHNHYTQ KSLSLSLGK 419
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-chain disulfide bridges: 36-42 64-74 233-293 339-397
36'-42' 64'-74' 233'-293' 339'-397'Inter-chain disulfide bridges: 203-203'
Glycosylation sites (N) / Sites de glycosylation (N) / Posiciones de glicosilación (N)Asn-269
Glycosylation sites (O) / Sites de glycosylation (O) / Posiciones de glicosilación (O)Thr-133
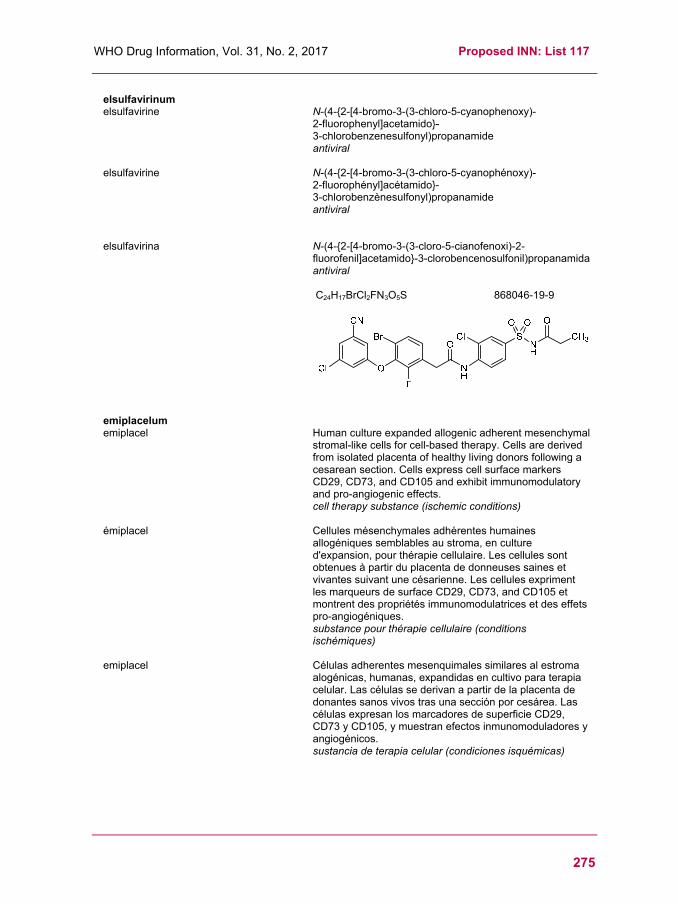
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
275
elsulfavirinum elsulfavirine N-(4-{2-[4-bromo-3-(3-chloro-5-cyanophenoxy)-
2-fluorophenyl]acetamido}- 3-chlorobenzenesulfonyl)propanamide antiviral
elsulfavirine N-(4-{2-[4-bromo-3-(3-chloro-5-cyanophénoxy)- 2-fluorophényl]acétamido}- 3-chlorobenzènesulfonyl)propanamide antiviral
elsulfavirina N-(4-{2-[4-bromo-3-(3-cloro-5-cianofenoxi)-2-fluorofenil]acetamido}-3-clorobencenosulfonil)propanamida antiviral
C24H17BrCl2FN3O5S
868046-19-9
emiplacelum emiplacel Human culture expanded allogenic adherent mesenchymal
stromal-like cells for cell-based therapy. Cells are derived from isolated placenta of healthy living donors following a cesarean section. Cells express cell surface markers CD29, CD73, and CD105 and exhibit immunomodulatory and pro-angiogenic effects. cell therapy substance (ischemic conditions)
émiplacel Cellules mésenchymales adhérentes humaines allogéniques semblables au stroma, en culture d'expansion, pour thérapie cellulaire. Les cellules sont obtenues à partir du placenta de donneuses saines et vivantes suivant une césarienne. Les cellules expriment les marqueurs de surface CD29, CD73, and CD105 et montrent des propriétés immunomodulatrices et des effets pro-angiogéniques. substance pour thérapie cellulaire (conditions ischémiques)
emiplacel Células adherentes mesenquimales similares al estroma alogénicas, humanas, expandidas en cultivo para terapia celular. Las células se derivan a partir de la placenta de donantes sanos vivos tras una sección por cesárea. Las células expresan los marcadores de superficie CD29, CD73 y CD105, y muestran efectos inmunomoduladores y angiogénicos. sustancia de terapia celular (condiciones isquémicas)

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
276
enarodustatum enarodustat N-[7-hydroxy-5-(2-phenylethyl)[1,2,4]triazolo[1,5-
a]pyridine-8-carbonyl]glycine antianaemic
énarodustat N-[7-hydroxy-5-(2-phényléthyl)[1,2,4]triazolo[1,5-a]pyridine-8-carbonyl]glycine antianémique
enarodustat N-[7-hidroxi-5-(2-feniletil)[1,2,4]triazolo[1,5-a]piridina-8-carbonil]glicina antianémico
C17H16N4O4
1262132-81-9
exebacasum # exebacase Streptococcus suis bacteriophage-derived lysin, produced
in Escherichia coli; des-Met1-phage lysin (endolysin, lysozyme, murein hydrolase, EC 3.2.1.17) of Streptococcus suis phage φ891591 (PlySs2), produced in Escherichia coli enzyme, antibacterial
exébacase lysine dérivée du bactériophage Streptococcus suis, produite par Escherichia coli; lysine du dès-Mét1-phage Streptococcus suis φ891591 (PlySs2) (endolysine, lysozyme, muréine hydrolase, EC 3.2.1.17), produite par Escherichia coli enzyme, antibactérien
exebacasa lisina derivada del bacteriófago Streptococcus suis, producido por Escherichia coli; lisina del des-Met1-fago Streptococcus suis φ891591 (PlySs2) (endolisina, lisozima, mureína hidrolasa, EC 3.2.1.17), producida por Escherichia coli enzima, antibacteriano
1404122-92-4
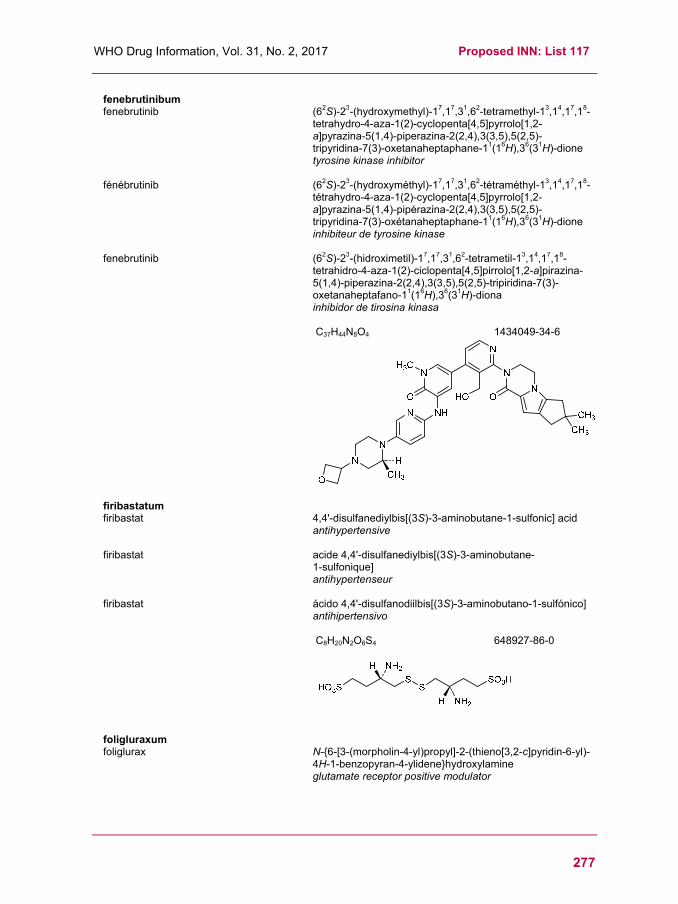
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
277
fenebrutinibum fenebrutinib (62S)-23-(hydroxymethyl)-17,17,31,62-tetramethyl-13,14,17,18-
tetrahydro-4-aza-1(2)-cyclopenta[4,5]pyrrolo[1,2-a]pyrazina-5(1,4)-piperazina-2(2,4),3(3,5),5(2,5)-tripyridina-7(3)-oxetanaheptaphane-11(16H),36(31H)-dione tyrosine kinase inhibitor
fénébrutinib (62S)-23-(hydroxyméthyl)-17,17,31,62-tétraméthyl-13,14,17,18-tétrahydro-4-aza-1(2)-cyclopenta[4,5]pyrrolo[1,2-a]pyrazina-5(1,4)-pipérazina-2(2,4),3(3,5),5(2,5)-tripyridina-7(3)-oxétanaheptaphane-11(16H),36(31H)-dione inhibiteur de tyrosine kinase
fenebrutinib (62S)-23-(hidroximetil)-17,17,31,62-tetrametil-13,14,17,18-tetrahidro-4-aza-1(2)-ciclopenta[4,5]pirrolo[1,2-a]pirazina-5(1,4)-piperazina-2(2,4),3(3,5),5(2,5)-tripiridina-7(3)-oxetanaheptafano-11(16H),36(31H)-diona inhibidor de tirosina kinasa
C37H44N8O4 1434049-34-6
firibastatum firibastat 4,4'-disulfanediylbis[(3S)-3-aminobutane-1-sulfonic] acid
antihypertensive
firibastat acide 4,4'-disulfanediylbis[(3S)-3-aminobutane- 1-sulfonique] antihypertenseur
firibastat ácido 4,4'-disulfanodiilbis[(3S)-3-aminobutano-1-sulfónico] antihipertensivo
C8H20N2O6S4
648927-86-0
foligluraxum foliglurax N-{6-[3-(morpholin-4-yl)propyl]-2-(thieno[3,2-c]pyridin-6-yl)-
4H-1-benzopyran-4-ylidene}hydroxylamine glutamate receptor positive modulator

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
278
foliglurax N-{6-[3-(morpholin-4-yl)propyl]-2-(thiéno[3,2-c]pyridin-6-yl)-4H-1-benzopyran-4-ylidène}hydroxylamine modulateur positif du récepteur glutamate
foliglurax N-{6-[3-(morfolin-4-il)propil]-2-(tieno[3,2-c]piridin-6-il)- 4H-1-benzopiran-4-ilideno}hidroxilamina modulador positivo del receptor glutamato
C23H23N3O3S
1883329-51-8
fulacimstatum fulacimstat 1-(3-methyl-2-oxo-2,3-dihydro-1,3-benzoxazol-6-yl)-
2,4-dioxo-3-[(1R)-4-(trifluoromethyl)-2,3-dihydro-1H-inden-1-yl]-1,2,3,4-tetrahydropyrimidine-5-carboxylic acid chymase inhibitor, antifibrotic
fulacimstat acide 1-(3-méthyl-2-oxo-2,3-dihydro-1,3-benzoxazol-6-yl)-2,4-dioxo-3-[(1R)-4-(trifluorométhyl)-2,3-dihydro-1H-indén-1-yl]-1,2,3,4-tétrahydropyrimidine-5-carboxylique inhibiteur de la chymase, antifibrotique
fulacimstat ácido 1-(3-metil-2-oxo-2,3-dihidro-1,3-benzoxazol-6-il)- 2,4-dioxo-3-[(1R)-4-(trifluorometil)-2,3-dihidro-1H-inden- 1-il]-1,2,3,4-tetrahidropirimidina-5-carboxílico inhibidor de la quimasa, antifibrótico
C23H16F3N3O6
1488354-15-9
garvagliptinum garvagliptin (2R,3S,5R)-2-(2,5-difluorophenyl)-5-[5-(methanesulfonyl)-
3,4,5,6-tetrahydropyrrolo[3,4-c]pyrrol-2(1H)-yl]oxan- 3-amine antidiabetic
garvagliptine (2R,3S,5R)-2-(2,5-difluorophényl)-5-[5-(méthanesulfonyl)-3,4,5,6-tétrahydropyrrolo[3,4-c]pyrrol-2(1H)-yl]oxan- 3-amine antidiabétique
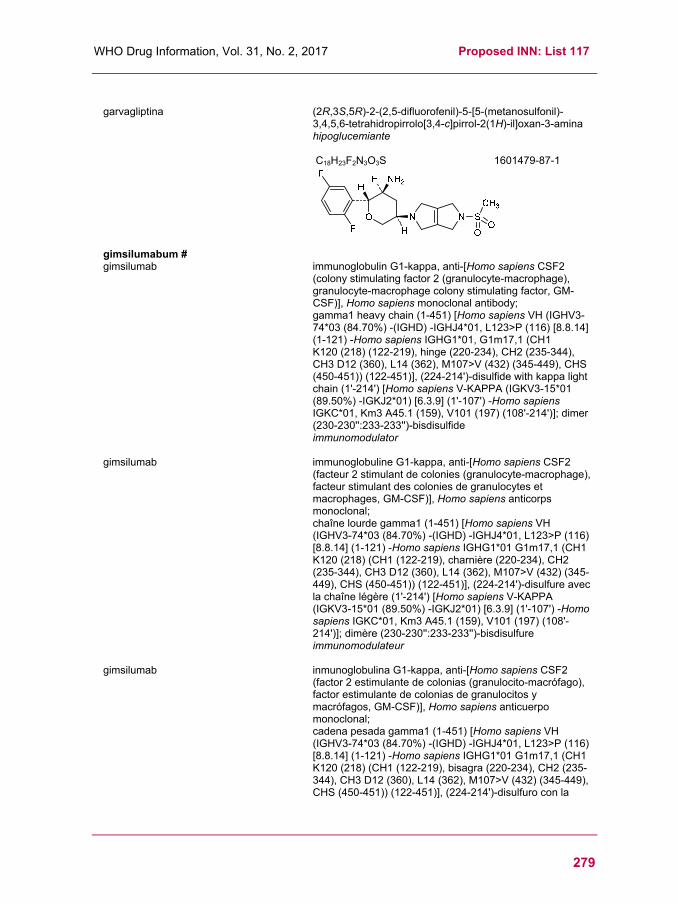
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
279
garvagliptina (2R,3S,5R)-2-(2,5-difluorofenil)-5-[5-(metanosulfonil)-
3,4,5,6-tetrahidropirrolo[3,4-c]pirrol-2(1H)-il]oxan-3-amina hipoglucemiante
C18H23F2N3O3S 1601479-87-1
gimsilumabum # gimsilumab immunoglobulin G1-kappa, anti-[Homo sapiens CSF2
(colony stimulating factor 2 (granulocyte-macrophage), granulocyte-macrophage colony stimulating factor, GM-CSF)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-451) [Homo sapiens VH (IGHV3-74*03 (84.70%) -(IGHD) -IGHJ4*01, L123>P (116) [8.8.14] (1-121) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (218) (122-219), hinge (220-234), CH2 (235-344), CH3 D12 (360), L14 (362), M107>V (432) (345-449), CHS (450-451)) (122-451)], (224-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV3-15*01 (89.50%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (108'-214')]; dimer (230-230'':233-233'')-bisdisulfide immunomodulator
gimsilumab immunoglobuline G1-kappa, anti-[Homo sapiens CSF2 (facteur 2 stimulant de colonies (granulocyte-macrophage), facteur stimulant des colonies de granulocytes et macrophages, GM-CSF)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-451) [Homo sapiens VH (IGHV3-74*03 (84.70%) -(IGHD) -IGHJ4*01, L123>P (116) [8.8.14] (1-121) -Homo sapiens IGHG1*01 G1m17,1 (CH1 K120 (218) (CH1 (122-219), charnière (220-234), CH2 (235-344), CH3 D12 (360), L14 (362), M107>V (432) (345-449), CHS (450-451)) (122-451)], (224-214')-disulfure avec la chaîne légère (1'-214') [Homo sapiens V-KAPPA (IGKV3-15*01 (89.50%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (108'-214')]; dimère (230-230'':233-233'')-bisdisulfure immunomodulateur
gimsilumab inmunoglobulina G1-kappa, anti-[Homo sapiens CSF2 (factor 2 estimulante de colonias (granulocito-macrófago), factor estimulante de colonias de granulocitos y macrófagos, GM-CSF)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-451) [Homo sapiens VH (IGHV3-74*03 (84.70%) -(IGHD) -IGHJ4*01, L123>P (116) [8.8.14] (1-121) -Homo sapiens IGHG1*01 G1m17,1 (CH1 K120 (218) (CH1 (122-219), bisagra (220-234), CH2 (235-344), CH3 D12 (360), L14 (362), M107>V (432) (345-449), CHS (450-451)) (122-451)], (224-214')-disulfuro con la

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
280
cadena ligera (1'-214') [Homo sapiens V-KAPPA (IGKV3-15*01 (89.50%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (108'-214')]; dímero (230-230'':233-233'')-bisdisulfuro inmunomodulador
1648796-29-5
ianalumabum # ianalumab immunoglobulin G1-kappa, anti-[Homo sapiens
TNFRSF13C (tumor necrosis factor receptor (TNFR) superfamily member 13C, BAFFR, BAFF-R, BR3, B cell activating factor receptor, CD268)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-454) [Homo sapiens VH (IGHV6-1*01 (96.00%) -(IGHD) -IGHJ5*01) [10.9.14] (1-124) -Homo sapiens IGHG1*03,G1m3, nG1m1 (CH1 R120 (221) (125-222), hinge (223-237), CH2 (238-347), CH3 E12 (363), M14 (365) (348-452), CHS (453-454)) (125-454)], (227-215')-disulfide with kappa light chain (1'-215') [Homo sapiens V-KAPPA (IGKV3D-11*01 (86.80%) -IGKJ1*01) [7.3.9] (1'-108') -Homo sapiens IGKC*01, Km3 A45.1 (154), V101 (192) (109'-215')]; dimer (233-233'':236-236'')-bisdisulfide immunomodulator
ianalumab immunoglobuline G1-kappa, anti-[Homo sapiens TNFRSF13C (membre 13C de la super famille du récepteur du facteur de nécrose tumorale (TNFR), BAFFR, BAFF-R, BR3, récepteur du facteur d'activation des lymphocytes B], Homo sapiens anticorps monoclonal;
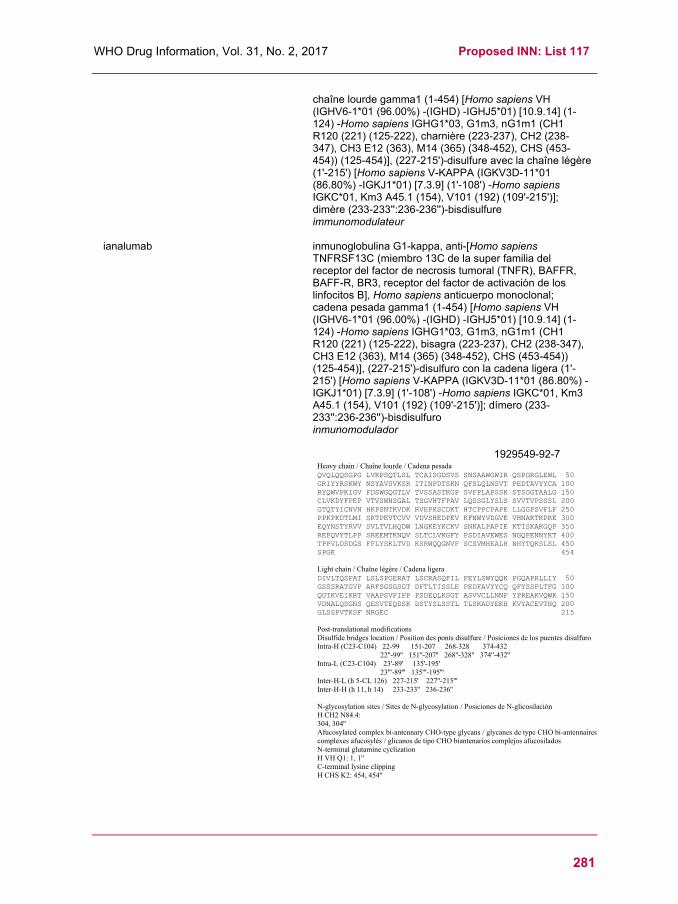
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
281
chaîne lourde gamma1 (1-454) [Homo sapiens VH (IGHV6-1*01 (96.00%) -(IGHD) -IGHJ5*01) [10.9.14] (1-124) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (221) (125-222), charnière (223-237), CH2 (238-347), CH3 E12 (363), M14 (365) (348-452), CHS (453-454)) (125-454)], (227-215')-disulfure avec la chaîne légère (1'-215') [Homo sapiens V-KAPPA (IGKV3D-11*01 (86.80%) -IGKJ1*01) [7.3.9] (1'-108') -Homo sapiens IGKC*01, Km3 A45.1 (154), V101 (192) (109'-215')]; dimère (233-233'':236-236'')-bisdisulfure immunomodulateur
ianalumab inmunoglobulina G1-kappa, anti-[Homo sapiens TNFRSF13C (miembro 13C de la super familia del receptor del factor de necrosis tumoral (TNFR), BAFFR, BAFF-R, BR3, receptor del factor de activación de los linfocitos B], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-454) [Homo sapiens VH (IGHV6-1*01 (96.00%) -(IGHD) -IGHJ5*01) [10.9.14] (1-124) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (221) (125-222), bisagra (223-237), CH2 (238-347), CH3 E12 (363), M14 (365) (348-452), CHS (453-454)) (125-454)], (227-215')-disulfuro con la cadena ligera (1'-215') [Homo sapiens V-KAPPA (IGKV3D-11*01 (86.80%) -IGKJ1*01) [7.3.9] (1'-108') -Homo sapiens IGKC*01, Km3 A45.1 (154), V101 (192) (109'-215')]; dímero (233-233'':236-236'')-bisdisulfuro inmunomodulador
1929549-92-7
Heavy chain / Chaîne lourde / Cadena pesadaQVQLQQSGPG LVKPSQTLSL TCAISGDSVS SNSAAWGWIR QSPGRGLEWL 50GRIYYRSKWY NSYAVSVKSR ITINPDTSKN QFSLQLNSVT PEDTAVYYCA 100RYQWVPKIGV FDSWGQGTLV TVSSASTKGP SVFPLAPSSK STSGGTAALG 150CLVKDYFPEP VTVSWNSGAL TSGVHTFPAV LQSSGLYSLS SVVTVPSSSL 200GTQTYICNVN HKPSNTKVDK RVEPKSCDKT HTCPPCPAPE LLGGPSVFLF 250PPKPKDTLMI SRTPEVTCVV VDVSHEDPEV KFNWYVDGVE VHNAKTKPRE 300EQYNSTYRVV SVLTVLHQDW LNGKEYKCKV SNKALPAPIE KTISKAKGQP 350REPQVYTLPP SREEMTKNQV SLTCLVKGFY PSDIAVEWES NGQPENNYKT 400TPPVLDSDGS FFLYSKLTVD KSRWQQGNVF SCSVMHEALH NHYTQKSLSL 450SPGK 454
Light chain / Chaîne légère / Cadena ligeraDIVLTQSPAT LSLSPGERAT LSCRASQFIL PEYLSWYQQK PGQAPRLLIY 50GSSSRATGVP ARFSGSGSGT DFTLTISSLE PEDFAVYYCQ QFYSSPLTFG 100QGTKVEIKRT VAAPSVFIFP PSDEQLKSGT ASVVCLLNNF YPREAKVQWK 150VDNALQSGNS QESVTEQDSK DSTYSLSSTL TLSKADYEKH KVYACEVTHQ 200GLSSPVTKSF NRGEC 215
Post-translational modificationsDisulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-99 151-207 268-328 374-432
22''-99'' 151''-207'' 268''-328'' 374''-432''Intra-L (C23-C104) 23'-89' 135'-195'
23'''-89''' 135'''-195'''Inter-H-L (h 5-CL 126) 227-215' 227''-215'''Inter-H-H (h 11, h 14) 233-233'' 236-236''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:304, 304''Afucosylated complex bi-antennary CHO-type glycans / glycanes de type CHO bi-antennairescomplexes afucosylés / glicanos de tipo CHO biantenarios complejos afucosiladosN-terminal glutamine cyclizationH VH Q1: 1, 1''C-terminal lysine clippingH CHS K2: 454, 454''
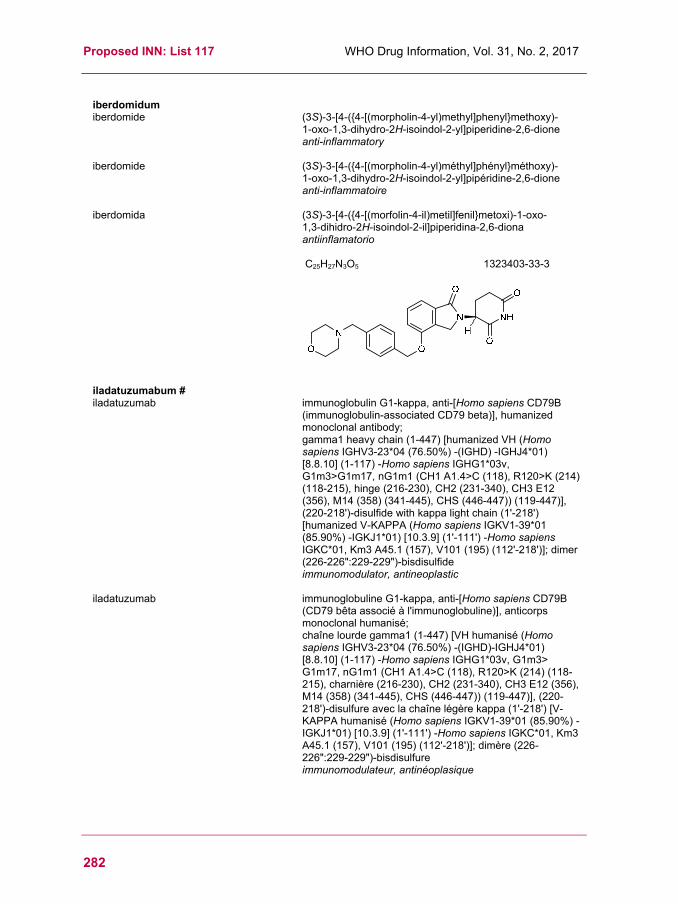
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
282
iberdomidum iberdomide (3S)-3-[4-({4-[(morpholin-4-yl)methyl]phenyl}methoxy)-
1-oxo-1,3-dihydro-2H-isoindol-2-yl]piperidine-2,6-dione anti-inflammatory
iberdomide (3S)-3-[4-({4-[(morpholin-4-yl)méthyl]phényl}méthoxy)- 1-oxo-1,3-dihydro-2H-isoindol-2-yl]pipéridine-2,6-dione anti-inflammatoire
iberdomida (3S)-3-[4-({4-[(morfolin-4-il)metil]fenil}metoxi)-1-oxo- 1,3-dihidro-2H-isoindol-2-il]piperidina-2,6-diona antiinflamatorio
C25H27N3O5
1323403-33-3
iladatuzumabum # iladatuzumab immunoglobulin G1-kappa, anti-[Homo sapiens CD79B
(immunoglobulin-associated CD79 beta)], humanized monoclonal antibody; gamma1 heavy chain (1-447) [humanized VH (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 A1.4>C (118), R120>K (214) (118-215), hinge (216-230), CH2 (231-340), CH3 E12 (356), M14 (358) (341-445), CHS (446-447)) (119-447)], (220-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dimer (226-226":229-229")-bisdisulfide immunomodulator, antineoplastic
iladatuzumab immunoglobuline G1-kappa, anti-[Homo sapiens CD79B (CD79 bêta associé à l'immunoglobuline)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-447) [VH humanisé (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD)-IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03v, G1m3> G1m17, nG1m1 (CH1 A1.4>C (118), R120>K (214) (118-215), charnière (216-230), CH2 (231-340), CH3 E12 (356), M14 (358) (341-445), CHS (446-447)) (119-447)], (220-218')-disulfure avec la chaîne légère kappa (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dimère (226-226":229-229")-bisdisulfure immunomodulateur, antinéoplasique

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
283
iladatuzumab inmunoglobulina G1-kappa, anti-[Homo sapiens CD79B (CD79 beta asociado a la inmunoglobulina)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-447) [VH humanizado (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD)-IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03v, G1m3> G1m17, nG1m1 (CH1 A1.4>C (118), R120>K (214) (118-215), bisagra (216-230), CH2 (231-340), CH3 E12 (356), M14 (358) (341-445), CHS (446-447)) (119-447)], (220-218')-disulfuro con la cadena ligera kappa (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dímero (226-226":229-229")-bisdisulfuro inmunomodulador, antineoplásico
1906205-76-2
iladatuzumabum vedotinum # iladatuzumab vedotin immunoglobulin G1-kappa, anti-[Homo sapiens CD79B
(immunoglobulin-associated CD79 beta)], humanized monoclonal antibody conjugated to auristatin E; gamma1 heavy chain (1-447) [humanized VH (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 A1.4>C (118), R120>K (214) (118-215), hinge (216-230), CH2 (231-340), CH3 E12 (356), M14 (358) (341-445), CHS (446-447)) (119-447)], (220-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dimer (226-226":229-229")-bisdisulfide; conjugated on 2 cysteinyl (at the position gamma1 CH1 1.4 (118, 118'')), to

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
284
monomethylauristatin E (MMAE), via a cleavable maleimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) type linker For the vedotin part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
immunomodulator, antineoplastic
iladatuzumab védotine immunoglobuline G1-kappa, anti-[Homo sapiens CD79B (CD79 bêta associé à l'immunoglobuline)], anticorps monoclonal humanisé conjugué à l'auristatine E; chaîne lourde gamma1 (1-447) [VH humanisé (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 A1.4>C (118), R120>K (214) (118-215), charnière (216-230), CH2 (231-340), CH3 E12 (356), M14 (358) (341-445), CHS (446-447)) (119-447)], (220-218')-disulfure avec la chaîne légère kappa (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dimère (226-226":229-229")-bisdisulfure; conjugué sur 2 cystéinyl (à la position gamma1 CH1 1.4 (118, 118'')), au monométhylauristatine E (MMAE), via un linker clivable de type maléimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) Pour la partie védotine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
immunomodulateur, antinéoplasique
iladatuzumab vedotina inmunoglobulina G1-kappa, anti-[Homo sapiens CD79B (CD79 beta asociado a la inmunoglobulina)], anticuerpo monoclonal humanizado conjugado con la auristatina E; cadena pesada gamma1 (1-447) [VH humanizado (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 A1.4>C (118), R120>K (214) (118-215), bisagra (216-230), CH2 (231-340), CH3 E12 (356), M14 (358) (341-445), CHS (446-447)) (119-447)], (220-218')-disulfuro con la cadena ligera kappa (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 A45.1 (157), V101 (195) (112'-218')]; dímero (226-226":229-229")-bisdisulfuro; conjugado con 2 restos cisteinil (en la posición gamma1 CH1 1.4 (118, 118'')), con la monometilauristatina E (MMAE), mediante el espaciador escindible de tipo maleimidocaproil-valil-citrulinil-p-aminobenciloxicarbonil (mc-val-cit-PABC) Para la fracción vedotina, pueden referirse al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
inmunomodulador, antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
285
1906205-77-3
imlifidasum # imlifidase human immunoglobulin G-degrading cysteine protease
from Streptococcus pyogenes (IdeS, residues 30-339), produced in Escherichia coli; L-methionyl-immunoglobulin G-degrading protease (Streptococcus pyogenes) (IdeS) pro-protein (30-339)-peptide, produced by Escherichia coli enzyme, immunosuppressant
imlifidase cystéine protéase de Streptococcus pyogenes dégradant l'immunoglobuline G humaine (IdeS, résidus 30-339), produite par Escherichia coli; L-méthionyl- protéase dégradant l'immunoglobuline G (Streptococcus pyogenes) (IdeS) pro-protéine (30-339)-peptide, produite par Escherichia coli enzyme, immunosuppresseur
imlifidasa cisteína proteasa de Streptococcus pyogenes que degrada a la inmunoglobulina G humana (IdeS, residuos 30-339), producido por Escherichia coli; L-metionil- proteasa que degrada la inmunoglobulina G (Streptococcus pyogenes) (IdeS) pro-proteína (30-339)-péptido, producido por Escherichia coli enzima, inmunosupresor
1947415-68-0

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
286
istiratumabum # istiratumab immunoglobulin G1-kappa anti-[Homo sapiens IGF1R
(insulin-like growth factor 1 receptor, IGF1-R, IGF-1R, CD221)], each heavy chain being fused to a scFv anti-[Homo sapiensERBB3 (receptor tyrosine-protein kinase erbB-3, HER3)], Homo sapiens monoclonal antibody, bispecific tetravalent; gamma1 heavy chain anti-IGFR1 fused to a scFv anti-ERBB3 (1-720) [Homo sapiens gamma1 heavy chain {(Homo sapiens VH (IGHV3-23*01 (90.80%) -(IGHD) -IGHJ4*01 L123>T (117))[8.8.15] (1-122) -Homo sapiens IGHG1*03v,G1m3>G1m17, nG1m1 (CH1 R120>K (219) (123-220), hinge (221-235), CH2 (236-345), CH3 E12 (361), M14 (363) (346-450), CHS K2>del (451))(123-451)}(1-451)-15-mer tris(tetraglycyl-seryl) linker (452-466) -scFv {(Homo sapiens VH (IGHV3-9*01 (92.90%) -(IGHD) -IGHJ4*01) [8.8.15] (467-588) -23-mer alanyl-seryl-threonyl-tetrakis(tetraglycyl-seryl) linker (589-611) -Homo sapiens V-LAMBDA (IGLV3-19*01 (94.80%) -IGLJ3*02 L124>V (716)) [6.3.11] (612-719) -glycyl (720)}(467-720)],(225-214')-disulfide with kappa light chain anti-IGFR1 (1'-214') [Homo sapiens V-KAPPA(IGKV1-12*01 (90.50%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (231-231'':234-234'')-bisdisulfide immunomodulator, antineoplastic
istiratumab immunoglobuline G1-kappa anti-[Homo sapiens IGF1R (récepteur du facteur de croissance 1 analogue à l'insuline, IGF1-R, IGF-1R, CD221)], chaque chaîne lourde étant fusionnée à un scFv anti-[Homo sapiens ERBB3 (récepteur à activité tyrosine kinase erbB-3, HER3)], Homo sapiens anticorps monoclonal, bispécifique tétravalent; chaîne lourde gamma1 anti-IGFR1 fusionnée à un scFv anti-ERBB3 (1-720) [chaîne lourde gamma1 Homo sapiens {(Homo sapiens VH (IGHV3-23*01 (90.80%) -(IGHD) -IGHJ4*01 L123>T (117))[8.8.15] (1-122) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (219)(123-220), charnière (221-235), CH2 (236-345), CH3 E12 (361), M14 (363) (346-450), CHS K2>del (451))(123-451)}(1-451) -15-mer tris(tétraglycyl-séryl) linker (452-466)-scFv {(Homo sapiens VH (IGHV3-9*01 (92.90%) -(IGHD) -IGHJ4-01) [8.8.15](467-588) -23-mer alanyl-séryl-thréonyl-tétrakis(tétraglycyl-séryl) linker (589-611) -Homo sapiens V-LAMBDA (IGLV3-19*01 (94.80%) -IGLJ3*02 L124>V (716)) [6.3.11] (612-719) -glycyl (720)}(467-720)], (225-214')-disulfure avec la chaîne légère kappa anti-IGFR1 (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (90.50%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (231-231'':234-234'')-bisdisulfure immunomodulateur, antinéoplasique

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
287
istiratumab inmunoglobulina G1-kappa anti-[Homo sapiens IGF1R (receptor del factor de crecimiento 1 análogo a la insulina, IGF1-R, IGF-1R, CD221)], cada cadena pesada estando fusionada con un scFv anti-[Homo sapiens ERBB3 (receptor tirosina-proteína kinasa erbB-3, HER3)], Homo sapiens anticuerpo monoclonal, biespecífico tetravalente; cadena pesada gamma1 anti-IGFR1 fusionada con un scFv anti-ERBB3 (1-720) [cadena pesada gamma1 Homo sapiens {(Homo sapiens VH (IGHV3-23*01 (90.80%) -(IGHD) -IGHJ4*01 L123>T (117))[8.8.15] (1-122) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (219)(123-220), bisagra (221-235), CH2 (236-345), CH3 E12 (361), M14 (363) (346-450), CHS K2>del (451))(123-451)}(1-451) -15-mer tris(tetraglicil-seril) espaciador (452-466)-scFv {(Homo sapiens VH (IGHV3-9*01 (92.90%) -(IGHD) -IGHJ4-01) [8.8.15](467-588) -23-mer alanil-seril-treonil-tetrakis(tetraglicil-seril) espaciador (589-611) -Homo sapiens V-LAMBDA (IGLV3-19*01 (94.80%) -IGLJ3*02 L124>V (716)) [6.3.11] (612-719) -glicil (720)}(467-720)], (225-214')-disulfuro con la cadena ligera kappa anti-IGFR1 (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (90.50%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (231-231'':234-234'')-bisdisulfuro inmunomodulador, antineoplásico
1509928-04-4

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
288
ladiratuzumabum # ladiratuzumab immunoglobulin G1-kappa, anti-[Homo sapiens SLC39A6
(solute carrier family 39 member 6, solute carrier family 39 (metal ion transporter) member 6, solute carrier family 39 (zinc transporter) member 6, LIV-1)], humanized monoclonal antibody; gamma1 heavy chain (1-450) [humanized VH (Homo sapiens IGHV1-2*02 (87.60%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (217) (121-218), hinge (219-233), CH2 (234-343), CH3 D12 (359), L14 (361) (344-448), CHS (449-450)) (121-450)], (223-219')-disulfide with kappa light chain (1'-219') [humanized V-KAPPA (Homo sapiens IGKV2-30*02 (89.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dimer (229-229":232-232")-bisdisulfide immunomodulator, antineoplastic
ladiratuzumab immunoglobuline G1-kappa, anti-[Homo sapiens SLC39A6 (membre 6 de la famille 39 des transporteurs de soluté, membre 6 de la famille 39 (transporteur d'ion métal) des transporteurs de soluté, membre 6 de la famille 39 (transporteur du zinc) des transporteurs de soluté, LIV-1)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-450) [VH humanisé (Homo sapiens IGHV1-2*02 (87.60%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (217) (121-218), charnière (219-233), CH2 (234-343), CH3 D12 (359), L14 (361) (344-448), CHS (449-450)) (121-450)], (223-219')-disulfure avec la chaîne légère kappa (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV2-30*02 (89.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dimère (229-229":232-232")-bisdisulfure immunomodulateur, antinéoplasique
ladiratuzumab inmunoglobulina G1-kappa, anti-[Homo sapiens SLC39A6 (miembro 6 de la familia 39 de los transportadores de soluto, miembro 6 de la familia 39 (transportador del ión metal) de los transportadores de soluto, miembro 6 de la familia 39 (transportador de zinc) de los transportadores de soluto, LIV-1)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-450) [VH humanizado (Homo sapiens IGHV1-2*02 (87.60%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (217) (121-218), bisagra (219-233), CH2 (234-343), CH3 D12 (359), L14 (361) (344-448), CHS (449-450)) (121-450)], (223-219')-disulfuro con la cadena ligera kappa (1'-219') [V-KAPPA humanizado (Homo sapiens IGKV2-30*02 (89.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dímero (229-229":232-232")-bisdisulfuro inmunomodulador, antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
289
1629760-28-6
ladiratuzumabum vedotinum # ladiratuzumab vedotin immunoglobulin G1-kappa, anti-[Homo sapiens SLC39A6
(solute carrier family 39 member 6, solute carrier family 39 (metal ion transporter) member 6, solute carrier family 39 (zinc transporter) member 6, LIV-1)], humanized monoclonal antibody conjugated to auristatin E; gamma1 heavy chain (1-450) [humanized VH (Homo sapiens IGHV1-2*02 (87.60%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (217) (121-218), hinge (219-233), CH2 (234-343), CH3 D12 (359), L14 (361) (344-448), CHS (449-450)) (121-450)], (223-219')-disulfide with kappa light chain (1'-219') [humanized V-KAPPA (Homo sapiens IGKV2-30*02 (89.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dimer (229-229":232-232")-bisdisulfide; conjugated, on an average of 4 cysteinyl, to monomethylauristatin E (MMAE), via a cleavable maleimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) type linker For the vedotin part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
immunomodulator, antineoplastic

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
290
ladiratuzumab védotine immunoglobuline G1-kappa, anti-[Homo sapiens SLC39A6 (membre 6 de la famille 39 des transporteurs de soluté, membre 6 de la famille 39 (transporteur d'ion métal) des transporteurs de soluté, membre 6 de la famille 39 (transporteur du zinc) des transporteurs de soluté, LIV-1)], anticorps monoclonal humanisé conjugué à l'auristatine E; chaîne lourde gamma1 (1-450) [VH humanisé (Homo sapiens IGHV1-2*02 (87.60%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (217) (121-218), charnière (219-233), CH2 (234-343), CH3 D12 (359), L14 (361) (344-448), CHS (449-450)) (121-450)], (223-219')-disulfure avec la chaîne légère kappa (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV2-30*02 (89.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dimère (229-229":232-232")-bisdisulfure; conjugué, sur 4 cystéinyl en moyenne, au monométhylauristatine E (MMAE), via un linker clivable de type maléimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) Pour la partie védotine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
immunomodulateur, antinéoplasique
ladiratuzumab vedotina inmunoglobulina G1-kappa, anti-[Homo sapiens SLC39A6 (miembro 6 de la familia 39 de los transportadores de soluto, miembro 6 de la familia 39 (transportador del ión metal) de los transportadores del soluto, miembro 6 de la familia 39 (transportador del zinc) de los transportadores del soluto, LIV-1)], anticuerpo monoclonal humanizado conjugado con la auristatina E; cadena pesada gamma1 (1-450) [VH humanizado (Homo sapiens IGHV1-2*02 (87.60%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17,1 (CH1 K120 (217) (121-218), bisagra (219-233), CH2 (234-343), CH3 D12 (359), L14 (361) (344-448), CHS (449-450)) (121-450)], (223-219')-disulfuro con la cadena ligera kappa (1'-219') [V-KAPPA humanizado (Homo sapiens IGKV2-30*02 (89.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dímero (229-229":232-232")-bisdisulfuro; conjugado, con 4 restos cisteinil, por término medio, con monometilauristatina E (MMAE), mediante un enlace de tipo maleimidocaproil-valil-citrulinil-p-aminobenziloxicarbonil (mc-val-cit-PABC) Para la fracción vedotina, pueden referirse al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
inmunomodulador, antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
291
1629760-29-7
lanacogenum vosiparvovecum # lanacogene vosiparvovec Non-replicating recombinant adeno-associated virus type 5
(AAV5) vector containing a codon-optimised of the wild type human coagulation factor IX (F9, FIX) gene under the control of the liver promoter 1 (LP1). gene therapy substance (hemophilia B)
lanacogène vosiparvovec vecteur viral adéno-associé recombinant de type 5 (AAV5) non-répliquant contenant une version avec des codons optimisés du gène du facteur IX de coagulacion de type sauvage (F9, FIX) humain sous le contrôle du promoteur LP1 des cellules hépatiques. substance pour thérapie génique (hémophilie B)
lanacogén vosiparvovec Vector del Virus Adeno-asociado de serotipo 5 (AAV5) recombinante, no replicativo, que contiene una versión con codones optimizados del gen del factor de coagulación IX humano (F9, FIX) bajo el control del promotor hepático 1 (LP1). sustancia de terapia génica (hemofilia B)
1939139-26-0
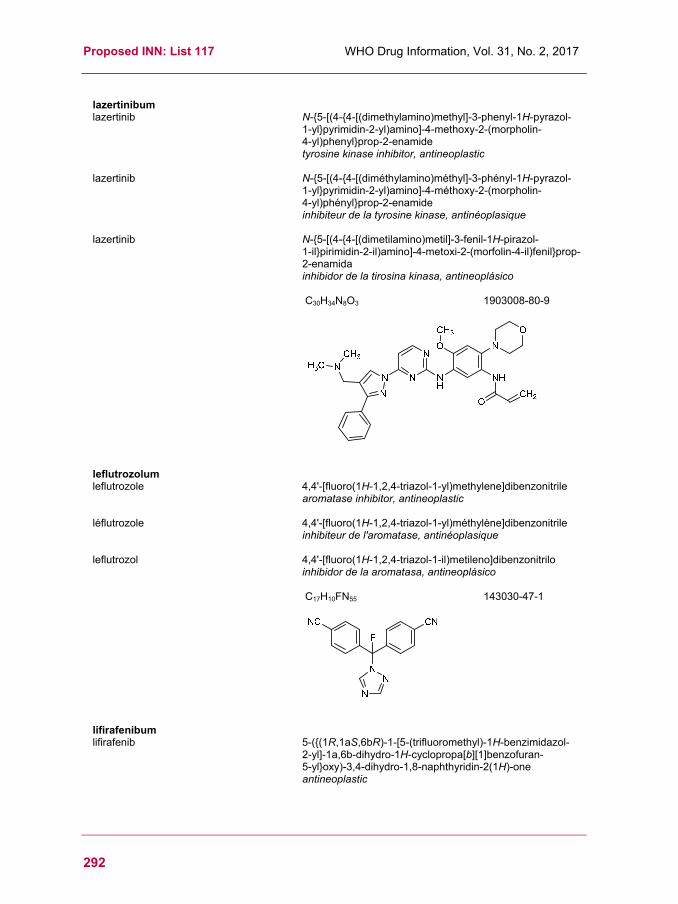
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
292
lazertinibum lazertinib N-{5-[(4-{4-[(dimethylamino)methyl]-3-phenyl-1H-pyrazol-
1-yl}pyrimidin-2-yl)amino]-4-methoxy-2-(morpholin- 4-yl)phenyl}prop-2-enamide tyrosine kinase inhibitor, antineoplastic
lazertinib N-{5-[(4-{4-[(diméthylamino)méthyl]-3-phényl-1H-pyrazol- 1-yl}pyrimidin-2-yl)amino]-4-méthoxy-2-(morpholin- 4-yl)phényl}prop-2-enamide inhibiteur de la tyrosine kinase, antinéoplasique
lazertinib N-{5-[(4-{4-[(dimetilamino)metil]-3-fenil-1H-pirazol- 1-il}pirimidin-2-il)amino]-4-metoxi-2-(morfolin-4-il)fenil}prop-2-enamida inhibidor de la tirosina kinasa, antineoplásico
C30H34N8O3
1903008-80-9
leflutrozolum leflutrozole 4,4'-[fluoro(1H-1,2,4-triazol-1-yl)methylene]dibenzonitrile
aromatase inhibitor, antineoplastic
léflutrozole 4,4'-[fluoro(1H-1,2,4-triazol-1-yl)méthylène]dibenzonitrile inhibiteur de l'aromatase, antinéoplasique
leflutrozol 4,4'-[fluoro(1H-1,2,4-triazol-1-il)metileno]dibenzonitrilo inhibidor de la aromatasa, antineoplásico
C17H10FN55
143030-47-1
lifirafenibum lifirafenib 5-({(1R,1aS,6bR)-1-[5-(trifluoromethyl)-1H-benzimidazol-
2-yl]-1a,6b-dihydro-1H-cyclopropa[b][1]benzofuran- 5-yl}oxy)-3,4-dihydro-1,8-naphthyridin-2(1H)-one antineoplastic

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
293
lifirafénib 5-({(1R,1aS,6bR)-1-[5-(trifluorométhyl)-1H-benzimidazol-
2-yl]-1a,6b-dihydro-1H-cyclopropa[b][1]benzofuran- 5-yl}oxy)-3,4-dihydro-1,8-naphthyridin-2(1H)-one antinéoplasique
lifirafenib 5-({(1R,1aS,6bR)-1-[5-(trifluorometil)-1H-benzimidazol- 2-il]-1a,6b-dihidro-1H-ciclopropa[b][1]benzofuran-5-il}oxi)-3,4-dihidro-1,8-naftiridin-2(1H)-ona antineoplásico
C25H17F3N4O3
1446090-79-4
lonapegsomatropinum # lonapegsomatropin human somatotropin (growth hormone, GH) produced in
Escherichia coli, conjugated to a multi-arm polyethylene glycol carrier molecule; somatotropin (human), produced by Escherichia coli, N6.Lys-substitued with one ({(1RS)-5-[bis(6-{[(3RS)-1-{3-[(3-{(2RS)-2,3-bis[ω-methoxypoly(oxyethylene)n-α-yl]propoxy}propyl)amino]-3-oxopropyl}-2,5-dioxopyrrolidin-3-yl]sulfanyl}hexyl)amino]-1-[4-({[3-(dimethylamino)propyl](methyl)carbamoyl}oxy)phenyl]-5-oxopentyl}oxy)carbonyl group growth hormone derivative
lonapegsomatropine somatotropine humaine (hormone de croissance, GH) produite par Escherichia coli, conjuguée à une molécule transporteur multi-bras de polyéthylène glycol; somatotropine (humaine), produite par Escherichia coli, substituée en N6.Lys par un groupe ({(1RS)-5-[bis(6-{[(3RS)-1-{3-[(3-{(2RS)-2,3-bis[ω-méthoxypoly(oxyéthylène)n-α-yl]propoxy}propyl)amino]-3-oxopropyl}-2,5-dioxopyrrolidin-3-yl]sulfanyl}hexyl)amino]-1-[4-({[3-(diméthylamino)propyl](méthyl)carbamoyl}oxy)phényl]- 5-oxopentyl}oxy)carbonyle dérivé de l'hormone de croissance
lonapegsomatropina somatotropina humana (hormona de crecimiento, GH) producida por Escherichia coli, conjugada a una molécula transportadora multi-bras de polietileno glicol; somatotropina (humana), producida por Escherichia coli, sustituida en N6.Lys por un grupo ({(1RS)-5-[bis(6-{[(3RS)-1-{3-[(3-{(2RS)-2,3-bis[ω-metoxipoli(oxietileno)n-α-il]propoxi}propil)amino]-3-oxopropil}-2,5-dioxopirrolidin-3-il]sulfanil}hexil)amino]-1-[4-({[3-(dimetilamino)propil](metil)carbamoil}oxi)fenil]- 5-oxopentil}oxi)carbonilo derivado del factor de crecimiento
O
O
N
NH
OHN
HN
F3C H
H

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
294
1934255-39-6
loncastuximabum # loncastuximab immunoglobulin G1-kappa, anti-[Homo sapiens CD19 (B
lymphocyte surface antigen B4, Leu-12)], chimeric monoclonal antibody; gamma1 heavy chain (1-449) [Mus musculus VH (IGHV1-69*02 (85.70%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (217) (121-218), hinge (219-233), CH2 (234-343), CH3 E12 (359), M14 (361) (344-448), CHS K2>del (449)) (121-449)], (223-211')-disulfide with kappa light chain (1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 (91.40%) -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01, Km3 A45.1 (150), V101 (188) (105'-211')]; dimer (229-229'':232-232'')-bisdisulfide immunomodulator, antineoplastic
loncastuximab immunoglobuline G1-kappa, anti-[Homo sapiens CD19 (antigène de surface B4 des lymphocytes B, Leu-12)], anticorps monoclonal chimérique; chaîne lourde gamma1 (1-449) [Mus musculus VH (IGHV1-69*02 (85.70%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (217) (121-218), charnière (219-233), CH2 (234-343), CH3 E12 (359), M14 (361) (344-448), CHS K2>del (449)) (121-449)], (223-211')-disulfure avec la chaîne légère kappa (1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 (91.40%) -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01, Km3 A45.1 (150), V101 (188) (105'-211')]; dimère (229-229'':232-232'')-bisdisulfure immunomodulateur, antinéoplasique
loncastuximab inmunoglobulina G1-kappa, anti-[Homo sapiens CD19 (antígeno de superficie B4 de los linfocitos B, Leu-12)], anticuerpo monoclonal quimérico;

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
295
cadena pesada gamma1 (1-449) [Mus musculus VH (IGHV1-69*02 (85.70%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (217) (121-218), bisagra (219-233), CH2 (234-343), CH3 E12 (359), M14 (361) (344-448), CHS K2>del (449)) (121-449)], (223-211')-disulfuro con la cadena ligera kappa (1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 (91.40%) -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01, Km3 A45.1 (150), V101 (188) (105'-211')]; dímero (229-229'':232-232'')-bisdisulfuro inmunomodulador, antineoplásico
1875032-68-0
loncastuximabum tesirinum # loncastuximab tesirine immunoglobulin G1-kappa, anti-[Homo sapiens CD19 (B
lymphocyte surface antigen B4, Leu-12)], chimeric monoclonal antibody conjugated to the pyrrolobenzodiazepine (PBD) dimer SCX; gamma1 heavy chain (1-449) [Mus musculus VH (IGHV1-69*02 (85.70%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (217) (121-218), hinge (219-233), CH2 (234-343), CH3 E12 (359), M14 (361) (344-448), CHS K2>del (449)) (121-449)], (223-211')-disulfide with kappa light chain

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
296
(1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 (91.40%) -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01, Km3 A45.1 (150), V101 (188) (105'-211')]; dimer (229-229'':232-232'')-bisdisulfide;conjugated, on an average of 2 cysteines, to the pyrrolobenzodiazepine (PBD) dimer SCX, via a cleavable (valine-alanine dipeptide as cathepsine B cleavage site) maleimide type linker containing a spacer PEG (n=8) For the tesirine part, please refer to the prop.INN List 113, published in the WHO Drug Information, Vol.29, No.2, 2015.
immunomodulator, antineoplastic
loncastuximab tésirine immunoglobuline G1-kappa, anti-[Homo sapiens CD19 (antigène de surface B4 des lymphocytes B, Leu-12)], anticorps monoclonal chimérique conjugué au dimère de pyrrolobenzodiazépine (PDB) SCX; chaîne lourde gamma1 (1-449) [Mus musculus VH (IGHV1-69*02 (85.70%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (217) (121-218), charnière (219-233), CH2 (234-343), CH3 E12 (359), M14 (361) (344-448), CHS K2>del (449)) (121-449)], (223-211')-disulfure avec la chaîne légère kappa (1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 (91.40%) -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01, Km3(105'-211')]; dimère (229-229'':232-232'')-bisdisulfure ; conjugué, sur 2 cystéines en moyenne, au dimère de pyrrolobenzodiazépine (PBD) SCX, via un linker clivable (dipeptide valine-alanine clivable par la cathepsine B) de type maléimide et comprenant un espaceur PEG (n=8) Pour la partie tésirine, veuillez vous référer à la Liste 113 des DCI prop, publiée dans le WHO Drug Information, Vol.29, No.2, 2015.
immunomodulateur, antinéoplasique
loncastuximab tesirina inmunoglobulina G1-kappa, anti-[Homo sapiens CD19 (antígeno de superficie B4 de los linfocitos B, Leu-12)], anticuerpo monoclonal quimérico conjugado con el dímero de pirrolobenzodiazepina (PDB) SCX; cadena pesada gamma1 (1-449) [Mus musculus VH (IGHV1-69*02 (85.70%) -(IGHD) -IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (217) (121-218), bisagra (219-233), CH2 (234-343), CH3 E12 (359), M14 (361) (344-448), CHS K2>del (449)) (121-449)], (223-211')-disulfuro con la cadena ligera kappa (1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 (91.40%) -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01, Km3(105'-211')]; dímero (229-229'':232-232'')-bisdisulfuro ; conjugado, en una media de 2 cisteinil, con el dímero de pirrolobenzodiazepina (PBD) SCX, mediante un conector escindible (dipéptido valina-alanina escindible por la catepsina B) de tipo maleimida y comprende un espaciador PEG (n=8) Para la fracción tesirina se puede referir a la Lista 113 de DCI prop., publicada en el WHO Drug Information, Vol.29, No.2, 2015. inmunomodulador, antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
297
1879918-31-6
loxicodegolum loxicodegol 4,5α-epoxy-6α-[(2,5,8,11,14,17-hexaoxanonadecan-
19-yl)oxy]-3-methoxy-17-methylmorphinan-14-ol μ-opioid receptor agonist
loxicodégol 4,5α-époxy-6α-[(2,5,8,11,14,17-hexaoxanonadécan- 19-yl)oxy]-3-méthoxy-17-méthylmorphinan-14-ol agoniste des récepteurs opioïdes μ
loxicodegol 4,5α-epoxi-6α-[(2,5,8,11,14,17-hexaoxanonadecan- 19-il)oxi]-3-metoxi-17-metilmorfinan-14-ol agonista de los receptores μ opioides
C31H49NO10
1211231-76-3

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
298
lumasiranum lumasiran {(2S,4R)-1-{1-[(2-acetamido-2-deoxy-β-D-
galactopyranosyl)oxy]-16,16-bis-({3-[(3-{5-[(2-acetamido-2-deoxy-β-D-galactopyranosyl)oxy]pentanamido}propyl)amino]-3-oxopropoxy}methyl)-5,11,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oyl}-4-hydroxypyrrolidin-2-yl}methyl hydrogen all-P-ambo-2'-O-methyl-P-thioguanylyl-(3'→5')-2'-O-methyl-P-thioadenylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-deoxy-2'-fluorocytidylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-deoxy-2'-fluorouridylyl-(3'→5')-2'-deoxy-2'-fluorocytidylyl-(3'→5')-2'-deoxy-2'-fluorocytidylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methylguanylyl-(3'→5')-2'-O-methylguanylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methyl-3'-adenylate duplex with all-P-ambo-2'-O-methyl-P-thioadenylyl-(5'→3')-2'-O-methyl-P-thiocytidylyl-(5'→3')-2'-O-methylcytidylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-O-methylguanylyl-(5'→3')-2'-O-methyladenylyl-(5'→3')-2'-O-methyladenylyl-(5'→3')-2'-deoxy-2'-fluoroadenylyl-(5'→3')-2'-O-methylguanylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-2'-O-methyladenylyl-(5'→3')-2'-O-methylguanylyl-(5'→3')-2'-O-methylguanylyl-(5'→3')-2'-O-methyladenylyl-(5'→3')-2'-deoxy-2'-fluorocytidylyl-(5'→3')-2'-deoxy-2'-fluorocytidylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-O-methyladenylyl-(5'→3')-2'-O-methyl-P-thiouridylyl-(5'→3')-2'-deoxy-2'-fluoro-P-thioadenylyl-(5'→3')-2'-O-methyluridine glycolate oxidase synthesis inhibitor
lumasiran hydrogéno-tout-P-ambo-2'-O-méthyl-P-thioguanylyl-(3'→5')-2'-O-méthyl-P-thioadénylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-désoxy-2'-fluorocytidylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-désoxy-2'-fluorouridylyl-(3'→5')-2'-désoxy-2'-fluorocytidylyl-(3'→5')-2'-désoxy-2'-fluorocytidylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthylguanylyl-(3'→5')-2'-O-méthylguanylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthyl-3'-adénylate de {(2S,4R)-1-{1-[(2-acétamido-2-désoxy-β-D-galactopyranosyl)oxy]-16,16-bis-({3-[(3-{5-[(2-acétamido-2-désoxy-β-D-galactopyranosyl)oxy]pentanamido}propyl)amino]-3-oxopropoxy}méthyl)-6,10,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oyl}-4-hydroxypyrrolidin-2-yl}méthyle
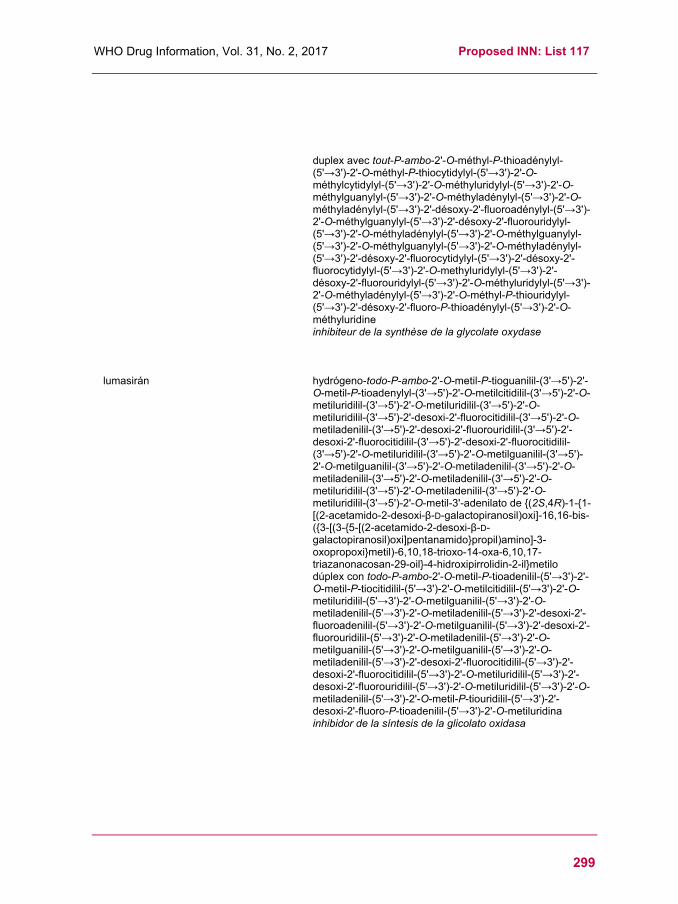
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
299
duplex avec tout-P-ambo-2'-O-méthyl-P-thioadénylyl-(5'→3')-2'-O-méthyl-P-thiocytidylyl-(5'→3')-2'-O-méthylcytidylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-2'-O-méthylguanylyl-(5'→3')-2'-O-méthyladénylyl-(5'→3')-2'-O-méthyladénylyl-(5'→3')-2'-désoxy-2'-fluoroadénylyl-(5'→3')-2'-O-méthylguanylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-2'-O-méthyladénylyl-(5'→3')-2'-O-méthylguanylyl-(5'→3')-2'-O-méthylguanylyl-(5'→3')-2'-O-méthyladénylyl-(5'→3')-2'-désoxy-2'-fluorocytidylyl-(5'→3')-2'-désoxy-2'-fluorocytidylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-2'-O-méthyladénylyl-(5'→3')-2'-O-méthyl-P-thiouridylyl-(5'→3')-2'-désoxy-2'-fluoro-P-thioadénylyl-(5'→3')-2'-O-méthyluridine inhibiteur de la synthèse de la glycolate oxydase
lumasirán hydrógeno-todo-P-ambo-2'-O-metil-P-tioguanilil-(3'→5')-2'-O-metil-P-tioadenylyl-(3'→5')-2'-O-metilcitidilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-desoxi-2'-fluorocitidilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-desoxi-2'-fluorouridilil-(3'→5')-2'-desoxi-2'-fluorocitidilil-(3'→5')-2'-desoxi-2'-fluorocitidilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metilguanilil-(3'→5')-2'-O-metilguanilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metil-3'-adenilato de {(2S,4R)-1-{1-[(2-acetamido-2-desoxi-β-D-galactopiranosil)oxi]-16,16-bis-({3-[(3-{5-[(2-acetamido-2-desoxi-β-D-galactopiranosil)oxi]pentanamido}propil)amino]-3-oxopropoxi}metil)-6,10,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oil}-4-hidroxipirrolidin-2-il}metilo dúplex con todo-P-ambo-2'-O-metil-P-tioadenilil-(5'→3')-2'-O-metil-P-tiocitidilil-(5'→3')-2'-O-metilcitidilil-(5'→3')-2'-O-metiluridilil-(5'→3')-2'-O-metilguanilil-(5'→3')-2'-O-metiladenilil-(5'→3')-2'-O-metiladenilil-(5'→3')-2'-desoxi-2'-fluoroadenilil-(5'→3')-2'-O-metilguanilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-2'-O-metiladenilil-(5'→3')-2'-O-metilguanilil-(5'→3')-2'-O-metilguanilil-(5'→3')-2'-O-metiladenilil-(5'→3')-2'-desoxi-2'-fluorocitidilil-(5'→3')-2'-desoxi-2'-fluorocitidilil-(5'→3')-2'-O-metiluridilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-2'-O-metiluridilil-(5'→3')-2'-O-metiladenilil-(5'→3')-2'-O-metil-P-tiouridilil-(5'→3')-2'-desoxi-2'-fluoro-P-tioadenilil-(5'→3')-2'-O-metiluridina inhibidor de la síntesis de la glicolato oxidasa

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
300
C530H712F10N173O320P43S6
1834610-13-7
mardepodectum mardepodect 2-({4-[1-methyl-4-(pyridin-4-yl)-1H-pyrazol-
3-yl]phenoxy}methyl)quinoline phosphodiesterase 10A (PDE10A) inhibitor
mardépodect 2-({4-[1-méthyl-4-(pyridin-4-yl)-1H-pyrazol- 3-yl]phénoxy}méthyl)quinoléine inhibiteur de la phosphodiestérase 10A (PDE10A)
mardepodect 2-({4-[1-metil-4-(piridin-4-il)-1H-pirazol- 3-il]fenoxi}metil)quinoleína inhibidor de la fosfodiesterasa 10A (PDE10A)
C25H20N4O
898562-94-2
milademetanum milademetan (3'R,4'S,5'R)-N-[(3R,6S)-6-carbamoyloxan-3-yl]-6''-chloro-
4'-(2-chloro-3-fluoropyridin-4-yl)-4,4-dimethyl-2''-oxo-1'',2''-dihydrodispiro[cyclohexane-1,2'-pyrrolidine-3',3''-indole]- 5'-carboxamide antineoplastic
miladémétan (3'R,4'S,5'R)-N-[(3R,6S)-6-carbamoyloxan-3-yl]-6''-chloro-4'-(2-chloro-3-fluoropyridin-4-yl)-4,4-diméthyl-2''-oxo-1'',2''-dihydrodispiro[cyclohexane-1,2'-pyrrolidine-3',3''-indole]- 5'-carboxamide antinéoplasique
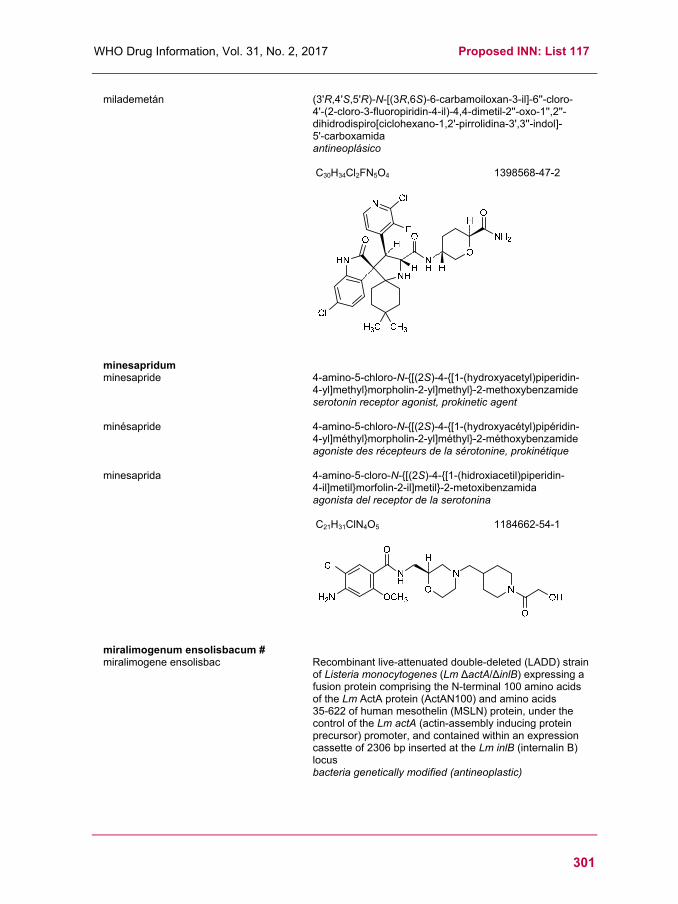
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
301
milademetán (3'R,4'S,5'R)-N-[(3R,6S)-6-carbamoiloxan-3-il]-6''-cloro- 4'-(2-cloro-3-fluoropiridin-4-il)-4,4-dimetil-2''-oxo-1'',2''-dihidrodispiro[ciclohexano-1,2'-pirrolidina-3',3''-indol]- 5'-carboxamida antineoplásico
C30H34Cl2FN5O4
1398568-47-2
minesapridum minesapride 4-amino-5-chloro-N-{[(2S)-4-{[1-(hydroxyacetyl)piperidin-
4-yl]methyl}morpholin-2-yl]methyl}-2-methoxybenzamide serotonin receptor agonist, prokinetic agent
minésapride 4-amino-5-chloro-N-{[(2S)-4-{[1-(hydroxyacétyl)pipéridin- 4-yl]méthyl}morpholin-2-yl]méthyl}-2-méthoxybenzamide agoniste des récepteurs de la sérotonine, prokinétique
minesaprida 4-amino-5-cloro-N-{[(2S)-4-{[1-(hidroxiacetil)piperidin- 4-il]metil}morfolin-2-il]metil}-2-metoxibenzamida agonista del receptor de la serotonina
C21H31ClN4O5
1184662-54-1
miralimogenum ensolisbacum # miralimogene ensolisbac Recombinant live-attenuated double-deleted (LADD) strain
of Listeria monocytogenes (Lm ∆actA/∆inlB) expressing a fusion protein comprising the N-terminal 100 amino acids of the Lm ActA protein (ActAN100) and amino acids 35-622 of human mesothelin (MSLN) protein, under the control of the Lm actA (actin-assembly inducing protein precursor) promoter, and contained within an expression cassette of 2306 bp inserted at the Lm inlB (internalin B) locus bacteria genetically modified (antineoplastic)

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
302
miralimogène ensolisbac souche vivante atténuée recombinante de Listeria monocytogenes (Lm ∆actA/∆inlB) avec double deletion, exprimant une protéine de fusion qui consiste en les 100 acides aminés à l'extrémité N-terminale de la protéine Lm ActA (ActAN100) et les acides aminés 35-622 de la mésothéline humaine (MSLN), sous le contrôle du promoteur de Lm actA (précurseur de la protéine induisant l'assemblage de l'actine), et contenu dans une cassette d'expression de 2306 paires de bases insérée sur le locus de Lm inlB (internaline B). bactérie génétiquement modifiée (antinéoplasique)
miralimogén ensolisbac Cepa viva atenuada recombinante, con doble deleción, de Listeria monocytogenes (Lm ∆actA/∆inlB) que expresa una proteína de fusión consistente en los 100 amino ácidos N-terminales de la proteína Lm ActA (ActAN100) y los amino ácidos 35-622 de la mesotelina humana (MSLN), bajo el control del promotor de Lm actA (precursor de la proteína inductora del ensamblaje de la actina), y contenido dentro de un casete de expresión de 2306 pares de bases insertado en el locus de Lm inlB (internalina B). bacteria modificada genéticamente (antineoplásico)
mirikizumabum # mirikizumab immunoglobulin G4-kappa, anti-[Homo sapiens IL23A
(interleukin 23 subunit alpha, IL-23A, IL-23 subunit p19, IL23p19)], humanized monoclonal antibody; gamma4 heavy chain (1-441) [humanized VH (Homo sapiens IGHV1-2*02 (82.70%) -(IGHD) -IGHJ6*01) [8.8.8] (1-115) -Homo sapiens IGHG4*01 (CH1 (116-213), hinge S10>P (223) (214-225), CH2 F1.3>A (229), L1.2>A (230) (226-335), CH3 (336-440), CHS K>del (441)) (116-441)], (129-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (221-221'':224-224'')-bisdisulfide immunomodulator
mirikizumab immunoglobuline G4-kappa, anti-[Homo sapiens IL23A (interleukine 23 sous-unité alpha, IL-23A, IL-23 sous-unité p19, IL23p19)], anticorps monoclonal humanisé; chaîne lourde gamma4 (1-441) [VH humanisé (Homo sapiens IGHV1-2*02 (82.70%) -(IGHD) -IGHJ6*01) [8.8.8] (1-115) -Homo sapiens IGHG4*01 (CH1 (116-213), charnière S10>P (223) (214-225), CH2 F1.3>A (229), L1.2>A (230) (226-335), CH3 (336-440), CHS K>del (441)) (116-441)], (129-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (221-221'':224-224'')-bisdisulfure immunomodulateur

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
303
mirikizumab inmunoglobulina G4-kappa, anti-[Homo sapiens IL23A (interleukina 23 subunidad alfa, IL-23A, IL-23 subunidad p19, IL23p19)], anticuerpo monoclonal humanizado; cadena pesada gamma4 (1-441) [VH humanizado (Homo sapiens IGHV1-2*02 (82.70%) -(IGHD) -IGHJ6*01) [8.8.8] (1-115) -Homo sapiens IGHG4*01 (CH1 (116-213), bisagra S10>P (223) (214-225), CH2 F1.3>A (229), L1.2>A (230) (226-335), CH3 (336-440), CHS K>del (441)) (116-441)], (129-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (221-221'':224-224'')-bisdisulfuro inmunomodulador
1884201-71-1
mosunetuzumabum # mosunetuzumab immunoglobulin G1-kappa, anti-[Homo sapiens CD3E
(CD3 epsilon) andHomo sapiens MS4A1 (membrane-spanning 4-domains subfamily A member 1, CD20)], humanized monoclonal antibody, bispecific; gamma1 heavy chain anti-CD3E (1-449) [humanized VH (Homo sapiens IGHV1-3*01 (82.70%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (216) (120-217), hinge (218-232), CH2 N84.4>G (299) (233-342), CH3 E12 (358), M14 (360), T22>S (368) / L24>A (370) / Y86>V (409) (hole) (343-447), CHS (448-449)) (120-449)], (222-219')-disulfide with kappa light chain anti-CD3E (1'-219') [humanized V-KAPPA (Homo sapiens IGKV4-1*01 (91.80%) -IGKJ1*01) [12.3.8] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')];

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
304
gamma1 heavy chain anti-MS4A1 (1-452) [humanized VH (Homo sapiens IGHV3-23*04 (81.60%) -(IGHD)-IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (219) (123-220), hinge (221-235), CH2 N84.4>G (302) (236-345), CH3 E12 (361), M14 (363), T22>W (371) (knob) (346-450), CHS (451-452)) (123-452)], (225-213')-disulfide with kappa light chain anti-MS4A1 (1'-213') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (86.50%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 A45.1 (152), V101 (190) (107'-213')]; dimer (228-231":231-234")-bisdisulfide immunomodulator, antineoplastic
mosunétuzumab immunoglobuline G1-kappa, anti-[Homo sapiens CD3E (CD3 epsilon) et Homo sapiens MS4A1 (membre 1 de la sous-famille A à 4 domaines transmembranaires, CD20)], anticorps monoclonal humanisé, bispécifique; chaîne lourde gamma1 anti-CD3E (1-449) [VH humanisé (Homo sapiens IGHV1-3*01 (82.70%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (216) (120-217), charnière (218-232), CH2 N84.4>G (299) (233-342), CH3 E12 (358), M14 (360), T22>S (368) / L24>A (370) / Y86>V (409) (hole) (343-447), CHS (448-449)) (120-449)], (222-219')-disulfure avec la chaîne légère kappa anti-CD3E (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV4-1*01 (91.80%) -IGKJ1*01) [12.3.8] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; chaîne lourde gamma1 anti-MS4A1 (1-452) [VH humanisé (Homo sapiens IGHV3-23*04 (81.60%) -(IGHD) -IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (219) (123-220), charnière (221-235), CH2 N84.4>G (302) (236-345), CH3 E12 (361), M14 (363), T22>W (371) (knob) (346-450), CHS (451-452)) (123-452)], (225-213')-disulfure avec la chaîne légère kappa anti-MS4A1 (1'-213') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (86.50%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 A45.1 (152), V101 (190) (107'-213')]; dimère (228-231":231-234")-bisdisulfure immunomodulateur, antinéoplasique
mosunetuzumab inmunoglobulina G1-kappa, anti-[Homo sapiens CD3E (CD3 epsilon) y Homo sapiens MS4A1 (miembro 1 de la subfamilia A con 4 dominios transmembranarios, CD20)], anticuerpo monoclonal humanizado, biespecífico; cadena pesada gamma1 anti-CD3E (1-449) [VH humanizado (Homo sapiens IGHV1-3*01 (82.70%) -(IGHD) -IGHJ4*01) [8.8.12] (1-119) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (216) (120-217), bisagra (218-232), CH2 N84.4>G (299) (233-342), CH3 E12 (358), M14 (360), T22>S (368) / L24>A (370) / Y86>V (409) (hole) (343-447), CHS (448-449)) (120-449)], (222-219')-disulfuro con la cadena ligera kappa anti-CD3E (1'-219') [V-KAPPA humanizado (Homo sapiens IGKV4-1*01 (91.80%) -IGKJ1*01) [12.3.8] (1'-112') -Homo sapiens IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')];

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
305
cadena pesada gamma1 anti-MS4A1 (1-452) [VH
humanizado (Homo sapiens IGHV3-23*04 (81.60%) -(IGHD) -IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (219) (123-220), bisagra (221-235), CH2 N84.4>G (302) (236-345), CH3 E12 (361), M14 (363), T22>W (371) (knob) (346-450), CHS (451-452)) (123-452)], (225-213')-disulfuro con la cadena ligera kappa anti-MS4A1 (1'-213') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (86.50%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 A45.1 (152), V101 (190) (107'-213')]; dímero (228-231":231-234")-bisdisulfuro inmunomodulador, antineoplásico
1905409-39-3
nadofaragenum firadenovecum # nadofaragene firadenovec Replication-deficient adenovirus type 5 (Ad5) vector
encoding the human interferon alpha 2 (IFNA2, interferon alpha-2b) gene under the control of the cytomegalovirus (CMV) immediate-early enhancer/promoter. gene therapy substance (antineoplastic)

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
306
nadofaragène firadénovec Vecteur adénoviral de type 5 (Ad5) à la réplication déficiente, codant pour le gène de l'interféron alpha 2 (IFNA2, interféron alpha-2b) humain sous le contrôle de l'activateur/promoteur immédiat-précoce du cytomégalovirus (CMV). substance pour thérapie génique (antinéoplasique)
nadofaragén firadenovec Vector de adenovirus tipo 5 (Ad5) deficiente de replicación, que codifica para el gen del interferón alfa 2 humano (IFNA2, inteferón alfa-2b) bajo el control del promotor/enhancer inmediato-temprano del citomegalovirus (CMV). sustancia de terapia génica (antineoplásico)
1823059-12-6
namodenosonum namodenoson 1-(2-chloro-6-{[(3-iodophenyl)methyl]amino}-9H-purin-9-yl)-
1-deoxy-N-methyl-β-D-ribofuranuronamide adenosine receptor agonist
namodénoson 1-(2-chloro-6-{[(3-iodophényl)methyl]amino}-9H-purin-9-yl)-1-désoxy-N-méthyl-β-D-ribofuranuronamide agoniste du récepteur de l'adénosine
namodenosón 1-(2-cloro-6-{[(3-iodofenil)metil]amino}-9H-purin-9-il)- 1-desoxi-N-metil-β-D-ribofuranuronamida agonista del receptor de la adenosina
C18H18ClIN6O4
163042-96-4
nangibotidum nangibotide human trem-like transcript 1 protein (TLT-1, triggering
receptor expressed on myeloid cells-like protein 1) (79-90)-peptide 12-amide: L-leucyl-L-glutaminyl-L-α-glutamyl-L-α-glutamyl- L-α-aspartyl-L-alanylglycyl-L-α-glutamyl-L-tyrosylglycyl- L-cysteinyl-L-methioninamide TREM-1 (Triggering receptor expressed on myeloid cells-1)-activation inhibitor

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
307
nangibotide protéine transcrit 1 semblable au trem humain (TLT-1, protéine 1 semblable au récepteur déclenchant exprimé par les cellules myéloïdes) (79-90)-peptide 12-amide: L-leucyl-L-glutaminyl-L-α-glutamyl-L-α-glutamyl- L-α-aspartyl-L-alanylglycyl-L-α-glutamyl-L-tyrosylglycyl- L-cystéinyl-L-méthioninamide inhibiteur de l'activation du récepteur TREM-1
nangibotida proteína transcrito 1 parecido al trem humano (TLT-1, proteína 1 parecida al receptor desencadenante expresado por las células mieloides) (79-90)-péptido 12-amida: L-leucil-L-glutaminil-L-α-glutamil-L-α-glutamil- L-α-aspartil-L-alanilglicil-L-α-glutamil-L-tirosilglicil- L-cisteinil-L-metioninamida inhibidor de la activación del receptor TREM-1
C54H82N14O22S2
2014384-91-7
olinciguatum olinciguat (2R)-3,3,3-trifluoro-2-{[(5-fluoro-2-{1-[(2-fluorophenyl)methyl]-
5-(1,2-oxazol-3-yl)-1H-pyrazol- 3-yl}pyrimidin-4-yl)amino]methyl}-2-hydroxypropanamide guanylate cyclase activator
olinciguat (2R)-3,3,3-trifluoro-2-{[(5-fluoro-2-{1-[(2-fluorophényl)méthyl]-5-(1,2-oxazol-3-yl)-1H-pyrazol- 3-yl}pyrimidin-4-yl)amino]méthyl}-2-hydroxypropanamide activateur de la guanylate cyclase
olinciguat (2R)-3,3,3-trifluoro-2-{[(5-fluoro-2-{1-[(2-fluorofenil)metil]- 5-(1,2-oxazol-3-il)-1H-pirazol-3-il}pirimidin- 4-il)amino]metil}-2-hidroxipropanamida activador de la guanilato ciclasa
C21H16F5N7O3
1628732-62-6
olorofimum olorofim 2-(1,5-dimethyl-3-phenyl-1H-pyrrol-2-yl)-N-{4-[4-(5-
fluoropyrimidin-2-yl)piperazin-1-yl]phenyl}-2-oxoacetamide antifungal
olorofim 2-(1,5-diméthyl-3-phényl-1H-pyrrol-2-yl)-N-{4-[4-(5-fluoropyrimidin-2-yl)pipérazin-1-yl]phényl}-2-oxoacétamide antifongique

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
308
olorofim 2-(1,5-dimetil-3-fenil-1H-pirrol-2-il)-N-{4-[4-(5-
fluoropirimidin-2-il)piperazin-1-il]fenil}-2-oxoacetamida antifúngico
C28H27FN6O2
1928707-56-5
omberacetamum omberacetam ethyl 1-phenylacetyl-L-prolylglycinate
nootropic
ombéracétam 1-phénylacétyl-L-prolylglycinate d'éthyle nootrope
omberacetam 1-fenilacetil-L-prolilglicinato de etilo nootropo
C17H22N2O4
157115-85-0
onasemnogenum abeparvovecum # onasemnogene abeparvovec Non-replicating recombinant self-complementary (sc)
adeno-associated virus serotype 9 (AAV9) vector containing the cDNA of the survival of motor neuron 2 (SMN2) gene under the control of the hybrid cytomegalovirus (CMV) enhancer/chicken beta-actin promoter (CBA). gene therapy substance (spinal muscular atrophy)
onasemnogène abéparvovec vecteur viral adéno-associé recombinant de sérotype 9 (rAAV9) non-répliquant et auto-complémentaire, contenant l'ADNc du gène de survie des motoneurones 2 (SMN2) sous le contrôle de l'hybride de l'activateur du cytomégalovirus (CMV) et du promoteur de l'actine bêta du poulet (ABP, CBA). substance pour thérapie génique (amyotrophie spinale)
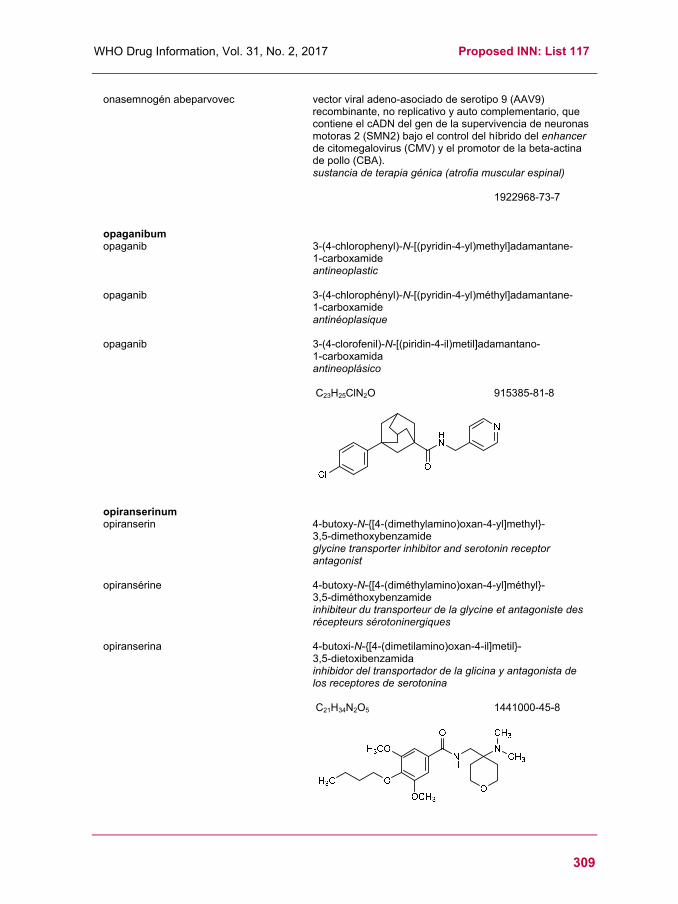
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
309
onasemnogén abeparvovec vector viral adeno-asociado de serotipo 9 (AAV9) recombinante, no replicativo y auto complementario, que contiene el cADN del gen de la supervivencia de neuronas motoras 2 (SMN2) bajo el control del híbrido del enhancer de citomegalovirus (CMV) y el promotor de la beta-actina de pollo (CBA). sustancia de terapia génica (atrofia muscular espinal)
1922968-73-7
opaganibum opaganib 3-(4-chlorophenyl)-N-[(pyridin-4-yl)methyl]adamantane-
1-carboxamide antineoplastic
opaganib 3-(4-chlorophényl)-N-[(pyridin-4-yl)méthyl]adamantane- 1-carboxamide antinéoplasique
opaganib 3-(4-clorofenil)-N-[(piridin-4-il)metil]adamantano- 1-carboxamida antineoplásico
C23H25ClN2O
915385-81-8
opiranserinum opiranserin 4-butoxy-N-{[4-(dimethylamino)oxan-4-yl]methyl}-
3,5-dimethoxybenzamide glycine transporter inhibitor and serotonin receptor antagonist
opiransérine 4-butoxy-N-{[4-(diméthylamino)oxan-4-yl]méthyl}- 3,5-diméthoxybenzamide inhibiteur du transporteur de la glycine et antagoniste des récepteurs sérotoninergiques
opiranserina 4-butoxi-N-{[4-(dimetilamino)oxan-4-il]metil}- 3,5-dietoxibenzamida inhibidor del transportador de la glicina y antagonista de los receptores de serotonina
C21H34N2O5
1441000-45-8

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
310
opolimogenum capmilisbacum # opolimogene capmilisbac Recombinant live-attenuated double-deleted (LADD) strain of Listeria
monocytogenes (Lm ∆actA/∆inlB) expressing three recombinant fusion proteins as follows: (i) the N-terminal 100 amino acids of the Lm ActA (actin-assembly inducing protein precursor) protein (ActAN100), 5 tandem copies of a 21 amino acid fragment of human epidermal growth factor receptor variant III (EGFRvIII) and human protein SSX2 (synovial sarcoma, X breakpoint 2, also known as cancer/testis antigen 5.2 (CT5.2), tumor antigen HOM-MEL-40), under the control of the Lm actA promoter, and contained within an expression cassette of 1434 bp inserted at the actA locus; (ii) the N-terminal 100 amino acids of the Lm ActA protein (ActAN100), 5 tandem copies of a 21 amino acid fragment of human epidermal growth factor receptor variant III (EGFRvIII) and amino acids 33-386 of human prostatic acid phosphatase (PAP), under the control the Lm actA promoter, and contained within an expression cassette of 2057 bp inserted at the inlB (internalin B) locus; (iii) the N-terminal 100 amino acids of the Lm ActA protein (ActAN100), 5 tandem copies of a 21 amino acid fragment of human epidermal growth factor receptor variant III (EGFRvIII) and amino acids 11-234 of human homeobox protein Nkx-3.1 (NKX3-1) plus amino acids 1-20, 44-138 and 169-750 of human glutamate carboxypeptidase 2 (also known as folate hydrolase 1 (FOLH1), prostate-specific membrane antigen (PSMA)), under the control the Lm actA promoter, and contained within an expression cassette of 4984 bp at the tRNAArg locus. bacteria genetically modified (antineoplastic)
opolimogène capmilisbac Souche vivante atténuée recombinante de Listeria monocytogenes (Lm ∆actA/∆inlB) avec double délétion, exprimant les trois protéines de fusion suivantes: (i) les 100 acides aminés à l'extrémité N-terminale de la protéine Lm actA (précurseur de la protéine induisant l'assemblage de l'actine) (ActAN100), 5 copies en tandem d'un fragment de 21 acides aminés de la variante III du récepteur du facteur de croissance épidermique humain (EGFRvIII) et la protéine humaine SSX2 (sarcome synovial, point de cassure X2, aussi connu comme antigène cancer/testicule 5.2 (CT5.2), antigène tumoral HOM-MEL-40), sous le contrôle du promoteur Lm actA, et contenu dans une cassette d'expression de 1434 paires de bases insérée sur le locus de actA; (ii) les 100 acides aminés à l'extrémité N-terminale de la protéine Lm actA (ActAN100), 5 copies en tandem d'un fragment de 21 acides aminés de la variante III du récepteur du facteur de croissance épidermique humain (EGFRvIII) et les acides aminés 33-386 de la phosphatase acide prostatique (PAP) humaine, sous le contrôle du promoteur Lm actA, contenu dans une cassette d'expression de 2057 paires de bases insérée sur le locus de inlB (internaline B); (iii) les 100 acides aminés à l'extrémité N-terminale de la protéine Lm actA (ActAN100), 5 copies en tandem d'un fragment de 21 acides aminés de la variante III du récepteur du facteur de croissance épidermique humain (EGFRvIII) et les acides aminés 11-234 de la protéine homéoboîte humaine Nkx-3.1 (NKX3-1) plus les acides aminés 1-20, 44-138, 169-750 de la glutamate caroxypeptidase 2 humaine (folate hydrolase 1, FOLH1, antigène membranaire spécifique de la prostate, PSMA) sous le contrôle du promoteur Lm actA, contenu dans une cassette d'expression de 4984 paires de bases insérée sur le locus de Lm tRNAArg. bactérie génétiquement modifiée (antinéoplasique)

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
311
opolimogén capmilisbac Cepa viva atenuada recombinante, con doble deleción, de Listeria
monocytogenes (Lm ∆actA/∆inlB) que expresa las siguientes tres proteínas recombinantes de fusión: (i) los 100 amino ácidos N-terminales de la proteína Lm ActA (precursor de la proteína inductora del ensamblaje de la actina) (ActAN100), 5 copias en tándem de un fragmento de 21 amino ácidos de la variante III del receptor para el factor de crecimiento epidérmico humano (EGFRvIII) y la proteína humana SSX2 (synovial sarcoma, X breakpoint 2, also known as cancer/testis antigen 5.2 (CT5.2), tumor antigen HOM-MEL-40), bajo el control del promotor de Lm actA, y contenido dentro de un casete de expresión de 1434 pares de bases insertado en el locus de actA; (ii) los 100 amino ácidos N-terminales de la proteína Lm ActA (ActAN100), 5 copias en tándem de un fragmento de 21 amino ácidos de la variante III del receptor para el factor de crecimiento epidérmico humano (EGFRvIII) y los amino ácidos 33-386 de la fosfatasa ácida prostática (PAP) humana, bajo el control del promotor de Lm actA, y contenido dentro de un casete de expresión de 2057 pares de bases insertado en el locus deinlB (internalina B); (iii) los 100 amino ácidos N-terminales de la proteína Lm ActA (ActAN100), 5 copias en tándem de un fragmento de 21 amino ácidos de la variante III del receptor para el factor de crecimiento epidérmico humano (EGFRvIII) y los amino ácidos 11-234 de la proteína homeobox humana Nkx-3.1 (NKX3-1) más los amino ácidos 1-20, 44-138 y 169-750 de la glutamato carboxipeptidasa 2 humana (también conocida como folato hidrolasa 1 (FOLH1), antígeno de membrana específico de próstata (PSMA)), bajo el control del promotor de Lm actA y contenido dentro de un casete de expresión de 4984 pares de bases insertado en el locus de Lm tRNAArg. bacteria modificada genéticamente (antineoplásico)
pamiparibum pamiparib (10aR)-2-fluoro-10a-methyl-5,8,9,10,10a,11-hexahydro-5,6,7a,11-
tetraazacyclohepta[def]cyclopenta[a]fluoren-4(7H)-one antineoplastic
pamiparib (10aR)-2-fluoro-10a-méthyl-5,8,9,10,10a,11-hexahydro-5,6,7a,11-tétraazacyclohepta[def]cyclopenta[a]fluorén-4(7H)-one antinéoplasique
pamiparib 10aR)-2-fluoro-10a-metil-5,8,9,10,10a,11-hexahidro-5,6,7a,11-tetraazaciclohepta[def]ciclopenta[a]fluoren-4(7H)-ona antineoplásico
C16H15FN4O
1446261-44-4
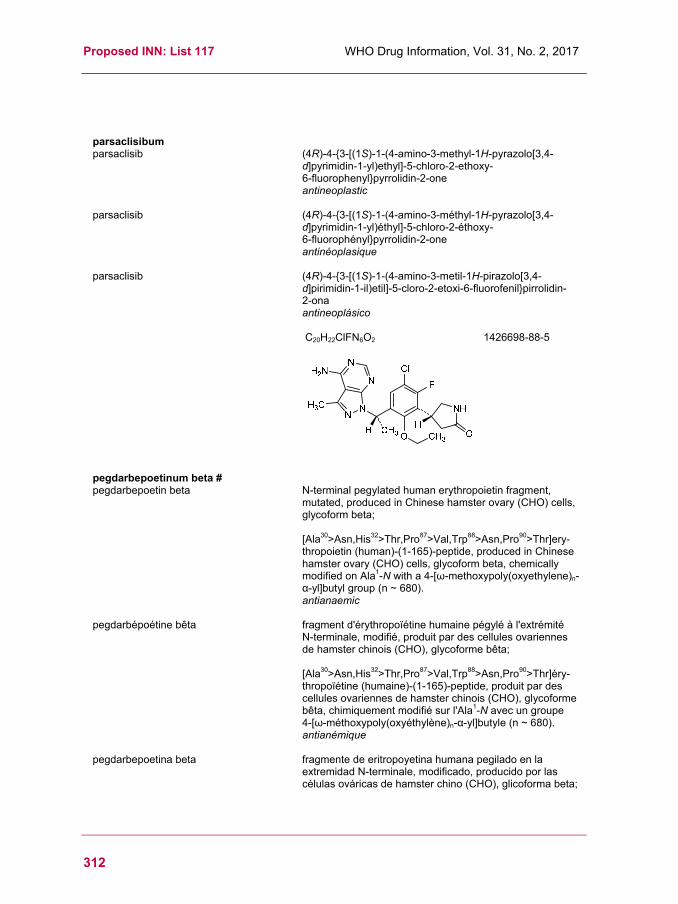
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
312
parsaclisibum parsaclisib (4R)-4-{3-[(1S)-1-(4-amino-3-methyl-1H-pyrazolo[3,4-
d]pyrimidin-1-yl)ethyl]-5-chloro-2-ethoxy- 6-fluorophenyl}pyrrolidin-2-one antineoplastic
parsaclisib (4R)-4-{3-[(1S)-1-(4-amino-3-méthyl-1H-pyrazolo[3,4-d]pyrimidin-1-yl)éthyl]-5-chloro-2-éthoxy- 6-fluorophényl}pyrrolidin-2-one antinéoplasique
parsaclisib (4R)-4-{3-[(1S)-1-(4-amino-3-metil-1H-pirazolo[3,4-d]pirimidin-1-il)etil]-5-cloro-2-etoxi-6-fluorofenil}pirrolidin- 2-ona antineoplásico
C20H22ClFN6O2
1426698-88-5
pegdarbepoetinum beta # pegdarbepoetin beta N-terminal pegylated human erythropoietin fragment,
mutated, produced in Chinese hamster ovary (CHO) cells, glycoform beta; [Ala30>Asn,His32>Thr,Pro87>Val,Trp88>Asn,Pro90>Thr]ery-thropoietin (human)-(1-165)-peptide, produced in Chinese hamster ovary (CHO) cells, glycoform beta, chemically modified on Ala1-N with a 4-[ω-methoxypoly(oxyethylene)n-α-yl]butyl group (n ~ 680). antianaemic
pegdarbépoétine bêta fragment d'érythropoïétine humaine pégylé à l'extrémité N-terminale, modifié, produit par des cellules ovariennes de hamster chinois (CHO), glycoforme bêta; [Ala30>Asn,His32>Thr,Pro87>Val,Trp88>Asn,Pro90>Thr]éry-thropoïétine (humaine)-(1-165)-peptide, produit par des cellules ovariennes de hamster chinois (CHO), glycoforme bêta, chimiquement modifié sur l'Ala1-N avec un groupe 4-[ω-méthoxypoly(oxyéthylène)n-α-yl]butyle (n ~ 680). antianémique
pegdarbepoetina beta fragmente de eritropoyetina humana pegilado en la extremidad N-terminale, modificado, producido por las células ováricas de hamster chino (CHO), glicoforma beta;

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
313
[Ala30>Asn,His32>Thr,Pro87>Val,Trp88>Asn,Pro90>Thr]eri-tropoyetina (humana)-(1-165)-péptido, producido por las células ováricas de hamster chino (CHO), glicoforma beta, químicamente modificado sobre la Ala1-N con un groupo 4-[ω-metoxipoli(oxietileno)n-α-il]butilo (n ~ 680). antianémico
C805H1310N228O245S5(C2H4O)n
1865718-54-2
pegilodecakinum # pegilodecakin N-terminal pegylated human interleukin 10 (IL10)
analogue, with an added methionine at the N-terminus, dimer, produced in recombinant Escherichia coli; N-{3-[ω-methoxypoly(oxyethylene)-α-yl]propyl}- L-methionyl-interleukin 10 (human), homodimer (non-covalent), produced in recombinant Escherichia coli interleukin derivative
pégilodécakine analogue de l’interleukine 10 humaine, pégylé en position N-terminale, avec l’ajout d’une méthionine en position N-terminale, dimère, produit par Escherichia coli; N-{3-[ω-méthoxypoly(oxyéthylène)-α-yl]propyl}- L-méthionyl-interleukine 10 (humaine), homodimère (non covalent), produit par Escherichia coli dérivé d'interleukine
pegilodecakina análogo de la interleukina 10 humano , pegilado en posición N-terminal, con la ayuda de una metionina en posición N-terminal, dímero, producido por Escherichia coli; N-{3-[ω-metoxipoli(oxietileno)-α-il]propil}- L-metionil-interleukina 10 (humano), homodímero (no covalente), producido por Escherichia coli derivado de la interleukina
1966111-35-2

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
314
pegzilarginasum # pegzilarginase pegylated human arginine amidinase (arginase I,
EC=3.5.3.1), mutated, cobalt ions replacing native manganese ions, trimer, produced in Escherichia coli; des-Met1-arginase-1 (human) dicobalt(II) complex, trimer, produced by Escherichia coli, substituted on an average of 8 to 16 primary amino groups of each protein monomer with [ω-methoxypoly(oxyethylene)n-α-yl]acetyl groups (n ~ 120) enzyme replacement therapy, antineoplastic
pegzilarginase arginine amidinase humaine pégylée (arginase I, EC=3.5.3.1), modifiée, dans laquelle le manganèse est remplacé par du cobalt, trimère, produit par Escherichia coli; dès-Mét1-arginase-1 (humaine) dicobalt(II) complexe, trimère, produit par Escherichia coli, substituée sur une moyenne de 8 sur 16 groupes amines primaires de chaque monomère de la protéine avec des groupes [ω-méthoxypoly(oxyéthylène)n-α-yl]acétyles (n ~ 120) traitement enzymatique substitutif, antinéoplasique
pegzilarginasa arginina amidinasa humana pegilada (arginasa I, EC=3.5.3.1), modificada, iones de cobalto que reemplazan iones de manganeso nativos, trímero, producido por Escherichia coli; des-Met1-arginasa-1 (humana) dicobalto(II) complejo, trímero, producido por Escherichia coli, sustituida por una media de 8 a 16 grupos aminas primarias de cada monómero de la proteína con los grupos [ω-metoxipoli(oxietileno)n-α-il]acetilos (n ~ 120) tratamiento enzimático de sustitución, antineoplásico
1659310-95-8
SAKSRTIGII GAPFSKGQPR GGVEEGPTVL RKAGLLEKLK EQECDVKDYG 50DLPFADIPND SPFQIVKNPR SVGKASEQLA GKVAEVKKNG RISLVLGGDH 100SLAIGSISGH ARVHPDLGVI WVDAHTDINT PLTTTSGNLH GQPVSFLLKE 150LKGKIPDVPG FSWVTPCISA KDIVYIGLRD VDPGEHYILK TLGIKYFSMT 200EVDRLGIGKV MEETLSYLLG RKKRPIHLSF DVDGLDPSFT PATGTPVVGG 250LTYREGLYIT EEIYKTGLLS GLDIMEVNPS LGKTPEEVTR TVNTAVAITL 300ACFGLAREGN HKPIDYLNPP K 321
Monomer sequence / Séquence du monomère / Secuencia del monómero
RNH
CO2H
H OHH3CO
O C
= R
n
H2N CO2H
H
NHR
S : pegylated L-serine K : pegylated L-lysines
Potential modified residues / Résidus modifiés potentiels / Restos modificados potenciales
O

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
315
pemlimogenum merolisbacum # pemlimogene merolisbac Recombinant live-attenuated double-deleted (LADD) strain
of Listeria monocytogenes (Lm ∆actA/∆inlB) expressing a fusion protein comprising the N-terminal 100 amino acids of the Lm ActA protein (ActAN100), 5 tandem copies of a 21 amino acid fragment of human epidermal growth factor receptor variant III (EGFRvIII) and amino acids 35-622 of human mesothelin (MSLN), under the control the Lm actA (actin-assembly inducing protein precursor) promoter, and contained within an expression cassette of 3874 bp inserted at the Lm tRNAArg locus. bacteria genetically modified (antineoplastic)
pemlimogène mérolisbac Souche vivante atténuée recombinante de Listeria monocytogenes (Lm ∆actA/∆inlB) avec double délétion, exprimant une protéine de fusion qui consiste en les 100 acides aminés à l'extrémité N-terminale de la protéine Lm ActA (ActAN100), 5 copies en tandem d'un fragment de 21 acides aminés de la variante III du récepteur du facteur de croissance épidermique humain (EGFRvIII) et les acides aminés 35-622 de la mésothéline humaine (MSLN), sous le contrôle du promoteur de Lm actA (précurseur de la protéine induisant l'assemblage de l'actine), et contenu dans une cassette d'expression de 3874 paires de bases insérée sur le locus de Lm tRNAArg. bactérie génétiquement modifiée (antineoplasique)
pemlimogén merolisbac Cepa viva atenuada recombinante, con doble deleción, de Listeria monocytogenes (Lm ∆actA/∆inlB) que expresa una proteína de fusión consistente en los 100 amino ácidos N-terminales de la proteína Lm ActA (ActAN100), 5 copias en tándem de un fragmento de 21 amino ácidos de la variante III del receptor para el factor de crecimiento epidérmico humano (EGFRvIII) y los amino ácidos 35-622 de la mesotelina humana (MSLN), bajo el control del promotor de Lm actA (precursor de la proteína inductora del ensamblaje de la actina), y contenido dentro de un casete de expresión de 3874 pares de bases insertado en el locus de Lm tRNAArg bacteria modificada genéticamente (antineoplásico)
petesicatibum petesicatib (2S,4R)-N-(1-cyanocyclopropyl)-4-[4-(1-methyl-1H-pyrazol-
4-yl)-2-(trifluromethyl)benzenesulfonyl]- 1-[1-(trifluoromethyl)cyclopropane-1-carbonyl]pyrrolidine- 2-carboxamide cathepsin inhibitor
pétésicatib (2S,4R)-N-(1-cyanocyclopropyl)-4-[4-(1-méthyl-1H-pyrazol-4-yl)-2-(triflurométhyl)benzènesulfonyl]- 1-[1-(trifluorométhyl)cyclopropane-1-carbonyl]pyrrolidine- 2-carboxamide inhibiteur de cathepsine

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
316
petesicatib 2S,4R)-N-(1-cianociclopropil)-4-[4-(1-metil-1H-pirazol-4-il)-2-(triflurometil)bencenosulfonil]- 1-[1-(trifluorometil)ciclopropano-1-carbonil]pirrolidina- 2-carboxamida inhibidor de catepsina
C25H23F6N5O4S
1252637-35-6
pixatimodum pixatimod 5α-cholestan-3β-yl 2,3,4,6-tetra-O-sulfo-α-D-
glucopyranosyl-(1→4)-2,3,6-tri-O-sulfo-α-D-glucopyranosyl-(1→4)-2,3,6-tri-O-sulfo-α-D-glucopyranosyl-(1→4)-2,3,6-tri-O-sulfo-β-D-glucopyranoside immunomodulator, antineoplastic
pixatimod 2,3,4,6-tétra-O-sulfo-α-D-glucopyranosyl-(1→4)-2,3,6-tri-O-sulfo-α-D-glucopyranosyl-(1→4)-2,3,6-tri-O-sulfo-α-D-glucopyranosyl-(1→4)-2,3,6-tri-O-sulfo-β-D-glucopyranoside de 5α-cholestan-3β-yle immunomodulateur, antinéoplasique
pixatimod 2,3,4,6-tetra-O-sulfo-α-D-glucopiranosil-(1→4)-2,3,6-tri-O-sulfo-α-D-glucopi-ranosil-(1→4)-2,3,6-tri-O-sulfo-α-D-glucopiranosil-(1→4)-2,3,6-tri-O-sulfo-β-D-glucopiranósida de 5α-colestan-3β-ilo inmunomodulador, antineoplásico
C51H88O60S13
1144617-49-1
plocabulinum plocabulin (1Z,4S,6Z)-1-[(2S)-2-{(2Z,4Z,6E,8S)-8-[(2S)-5-methoxy-6-
oxo-3,6-dihydro-2H-pyran-2-yl]-6-methylnona-2,4,6-trienamido}-3,3-dimethylbutanamido]octa-1,6-dien-4-yl carbamate antineoplastic
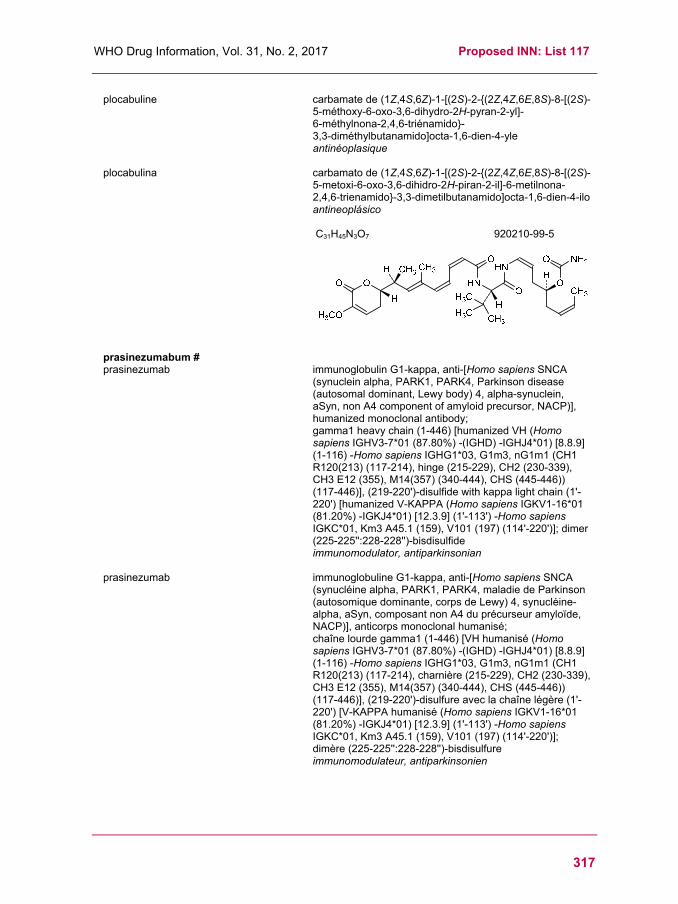
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
317
plocabuline carbamate de (1Z,4S,6Z)-1-[(2S)-2-{(2Z,4Z,6E,8S)-8-[(2S)-5-méthoxy-6-oxo-3,6-dihydro-2H-pyran-2-yl]- 6-méthylnona-2,4,6-triénamido}- 3,3-diméthylbutanamido]octa-1,6-dien-4-yle antinéoplasique
plocabulina carbamato de (1Z,4S,6Z)-1-[(2S)-2-{(2Z,4Z,6E,8S)-8-[(2S)-5-metoxi-6-oxo-3,6-dihidro-2H-piran-2-il]-6-metilnona-2,4,6-trienamido}-3,3-dimetilbutanamido]octa-1,6-dien-4-ilo antineoplásico
C31H45N3O7
920210-99-5
prasinezumabum # prasinezumab immunoglobulin G1-kappa, anti-[Homo sapiens SNCA
(synuclein alpha, PARK1, PARK4, Parkinson disease (autosomal dominant, Lewy body) 4, alpha-synuclein, aSyn, non A4 component of amyloid precursor, NACP)], humanized monoclonal antibody; gamma1 heavy chain (1-446) [humanized VH (Homo sapiens IGHV3-7*01 (87.80%) -(IGHD) -IGHJ4*01) [8.8.9] (1-116) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120(213) (117-214), hinge (215-229), CH2 (230-339), CH3 E12 (355), M14(357) (340-444), CHS (445-446)) (117-446)], (219-220')-disulfide with kappa light chain (1'-220') [humanized V-KAPPA (Homo sapiens IGKV1-16*01 (81.20%) -IGKJ4*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dimer (225-225'':228-228'')-bisdisulfide immunomodulator, antiparkinsonian
prasinezumab immunoglobuline G1-kappa, anti-[Homo sapiens SNCA (synucléine alpha, PARK1, PARK4, maladie de Parkinson (autosomique dominante, corps de Lewy) 4, synucléine-alpha, aSyn, composant non A4 du précurseur amyloïde, NACP)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-446) [VH humanisé (Homo sapiens IGHV3-7*01 (87.80%) -(IGHD) -IGHJ4*01) [8.8.9] (1-116) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120(213) (117-214), charnière (215-229), CH2 (230-339), CH3 E12 (355), M14(357) (340-444), CHS (445-446)) (117-446)], (219-220')-disulfure avec la chaîne légère (1'-220') [V-KAPPA humanisé (Homo sapiens IGKV1-16*01 (81.20%) -IGKJ4*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dimère (225-225'':228-228'')-bisdisulfure immunomodulateur, antiparkinsonien

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
318
prasinezumab inmunoglobulina G1-kappa, anti-[Homo sapiens SNCA (sinucleína alfa, PARK1, PARK4, enfermedad de Parkinson (autosómica dominante, cuerpos de Lewy) 4, sinucleína-alfa, aSyn, componente no A4 del precursor amieloide, NACP)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-446) [VH humanizado (Homo sapiens IGHV3-7*01 (87.80%) -(IGHD) -IGHJ4*01) [8.8.9] (1-116) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120(213) (117-214), bisagra (215-229), CH2 (230-339), CH3 E12 (355), M14(357) (340-444), CHS (445-446)) (117-446)], (219-220')-disulfuro con la cadena ligera (1'-220') [V-KAPPA humanizado (Homo sapiens IGKV1-16*01 (81.20%) -IGKJ4*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dímero (225-225'':228-228'')-bisdisulfuro inmunomodulador, antiparkinsoniano
1960462-19-4
ralanitenum ralaniten (2R)-3-[4-(2-{4-[(2S)-3-chloro-
2-hydroxypropoxy]phenyl}propan-2-yl)phenoxy]propane-1,2-diol antiandrogen
ralaniten (2R)-3-[4-(2-{4-[(2S)-3-chloro- 2-hydroxypropoxy]phényl}propan-2-yl)phénoxy]propane-1,2-diol antiandrogène
ralanitén (2R)-3-[4-(2-{4-[(2S)-3-cloro-2-hidroxipropoxi]fenil}propan-2-il)fenoxi]propano-1,2-diol antiandrógeno
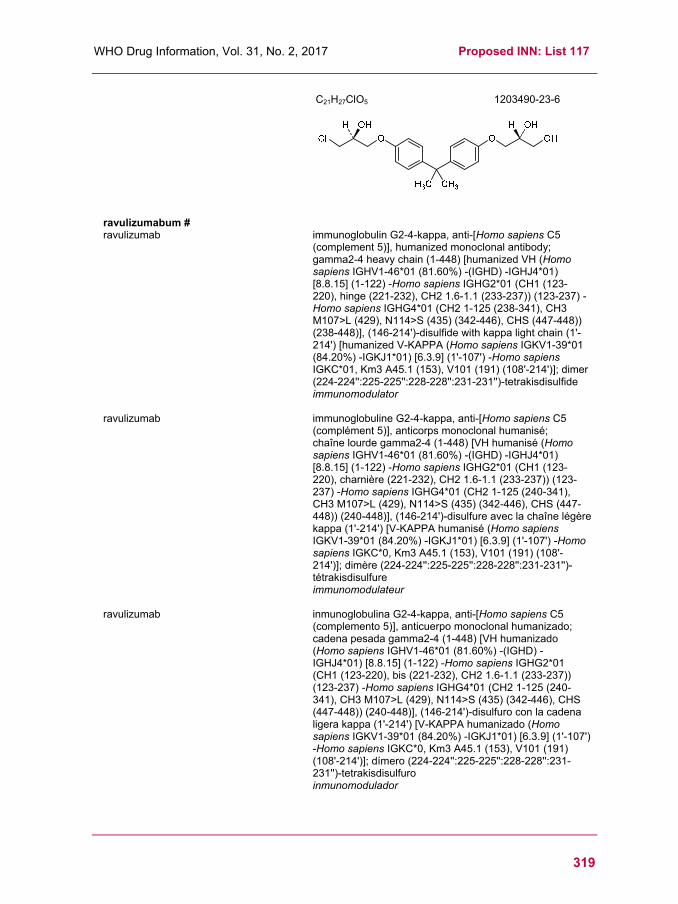
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
319
C21H27ClO5
1203490-23-6
ravulizumabum # ravulizumab immunoglobulin G2-4-kappa, anti-[Homo sapiens C5
(complement 5)], humanized monoclonal antibody; gamma2-4 heavy chain (1-448) [humanized VH (Homo sapiens IGHV1-46*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG2*01 (CH1 (123-220), hinge (221-232), CH2 1.6-1.1 (233-237)) (123-237) -Homo sapiens IGHG4*01 (CH2 1-125 (238-341), CH3 M107>L (429), N114>S (435) (342-446), CHS (447-448)) (238-448)], (146-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (84.20%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (224-224'':225-225'':228-228'':231-231'')-tetrakisdisulfide immunomodulator
ravulizumab immunoglobuline G2-4-kappa, anti-[Homo sapiens C5 (complément 5)], anticorps monoclonal humanisé; chaîne lourde gamma2-4 (1-448) [VH humanisé (Homo sapiens IGHV1-46*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG2*01 (CH1 (123-220), charnière (221-232), CH2 1.6-1.1 (233-237)) (123-237) -Homo sapiens IGHG4*01 (CH2 1-125 (240-341), CH3 M107>L (429), N114>S (435) (342-446), CHS (447-448)) (240-448)], (146-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (84.20%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*0, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (224-224'':225-225'':228-228'':231-231'')-tétrakisdisulfure immunomodulateur
ravulizumab inmunoglobulina G2-4-kappa, anti-[Homo sapiens C5 (complemento 5)], anticuerpo monoclonal humanizado; cadena pesada gamma2-4 (1-448) [VH humanizado (Homo sapiens IGHV1-46*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG2*01 (CH1 (123-220), bis (221-232), CH2 1.6-1.1 (233-237)) (123-237) -Homo sapiens IGHG4*01 (CH2 1-125 (240-341), CH3 M107>L (429), N114>S (435) (342-446), CHS (447-448)) (240-448)], (146-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (84.20%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*0, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (224-224'':225-225'':228-228'':231-231'')-tetrakisdisulfuro inmunomodulador

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
320
1803171-55-2
redasemtidum redasemtide human high mobility group protein B1 (HMG-1)-(1-44)-
peptide (including Met1), chemically synthesized (without any modified residues) high mobility group (HMG) protein B1 analogue
rédasemtide protéine B1 du groupe à haute mobilité humaine (HMGB1)-(1-44)-peptide (incluant Met1), synthétisé chimiquement (sans aucun résidu modifié) analogue de la protéine B1 du groupe à haute mobilité
redasemtida proteína B1 del grupo de alta movilidad humana (HMGB1)-(1-44)-péptido (incluyendo Met1), sintetizado químicamente (sin restos modificados) análogo de la proteína B1 del grupo de alta movilidad
C224H351N65O64S3 1606186-88-2
relmapirazinum relmapirazin N,N'-(3,6-diaminopyrazine-2,5-dicarbonyl)di-D-serine
diagnostic agent
relmapirazine N,N'-(3,6-diaminopyrazine-2,5-dicarbonyl)di-D-sérine substance à usage diagnostique
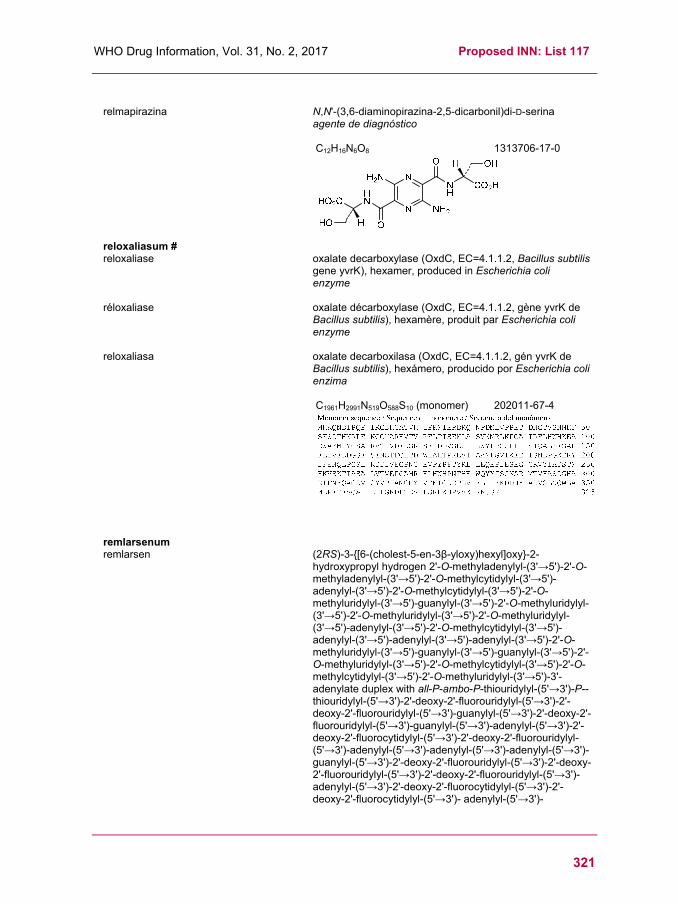
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
321
relmapirazina N,N'-(3,6-diaminopirazina-2,5-dicarbonil)di-D-serina
agente de diagnóstico
C12H16N6O8 1313706-17-0
reloxaliasum # reloxaliase oxalate decarboxylase (OxdC, EC=4.1.1.2, Bacillus subtilis
gene yvrK), hexamer, produced in Escherichia coli enzyme
réloxaliase oxalate décarboxylase (OxdC, EC=4.1.1.2, gène yvrK de Bacillus subtilis), hexamère, produit par Escherichia coli enzyme
reloxaliasa oxalate decarboxilasa (OxdC, EC=4.1.1.2, gén yvrK de Bacillus subtilis), hexámero, producido por Escherichia coli enzima
C1961H2991N519O588S10 (monomer) 202011-67-4
remlarsenum remlarsen (2RS)-3-{[6-(cholest-5-en-3β-yloxy)hexyl]oxy}-2-
hydroxypropyl hydrogen 2'-O-methyladenylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-adenylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-guanylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-adenylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-adenylyl-(3'→5')-adenylyl-(3'→5')-adenylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-guanylyl-(3'→5')-guanylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-3'-adenylate duplex with all-P-ambo-P-thiouridylyl-(5'→3')-P--thiouridylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-guanylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-guanylyl-(5'→3')-adenylyl-(5'→3')-2'-deoxy-2'-fluorocytidylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-adenylyl-(5'→3')-adenylyl-(5'→3')-adenylyl-(5'→3')-guanylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-2'-deoxy-2'-fluorouridylyl-(5'→3')-adenylyl-(5'→3')-2'-deoxy-2'-fluorocytidylyl-(5'→3')-2'-deoxy-2'-fluorocytidylyl-(5'→3')- adenylyl-(5'→3')-

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
322
2'-deoxy-2'-fluorocytidylyl-(5'→3')-guanylyl-(5'→3')-adenylyl-(5'→3')-2'-deoxy-2'-fluorouridine collagen synthesis reducer
remlarsen hydrogéno-2'-O-méthyladénylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-adénylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-guanylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-adénylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-adénylyl-(3'→5')-adénylyl-(3'→5')-adénylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-guanylyl-(3'→5')-guanylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-3'-adénylate de (2RS)-3-{[6-(cholest-5-én-3β-yloxy)hexyl]oxy}-2-hydroxypropyle duplex avec tout-P-ambo-P-thiouridylyl-(5'→3')-P-thiouridylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-guanylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-guanylyl-(5'→3')-adénylyl-(5'→3')-2'-désoxy-2'-fluorocytidylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-adénylyl-(5'→3')-adénylyl-(5'→3')-adénylyl-(5'→3')-guanylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-2'-désoxy-2'-fluorouridylyl-(5'→3')-adénylyl-(5'→3')-2'-désoxy-2'-fluorocytidylyl-(5'→3')-2'-désoxy-2'-fluorocytidylyl-(5'→3')-adénylyl-(5'→3')-2'-désoxy-2'-fluorocytidylyl-(5'→3')-guanylyl-(5'→3')-adénylyl-(5'→3')-2'-désoxy-2'-fluorouridine réducteur de synthèse du collagène
remlarsén hidrógeno-2'-O-metiladenilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-adenilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-2'-O-metiluridilil-(3'→5')-guanylyl-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metiluridilil-(3'→5')-adenilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-adenilil-(3'→5')-adenilil-(3'→5')-adenilil-(3'→5')-2'-O-metiluridilil-(3'→5')-guanilil-(3'→5')-guanilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-2'-O-metiluridilil-(3'→5')-3'-adenilato de (2RS)-3-{[6-(colest-5-en-3β-iloxi)hexil]oxi}-2-hidroxipropilo dúplex con todo-P-ambo-P-tiouridilil-(5'→3')-P-tiouridilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-guanilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-guanilil-(5'→3')-adenilil-(5'→3')-2'-desoxi-2'-fluorocitidilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-adenilil-(5'→3')-adenilil-(5'→3')-adenilil-(5'→3')-guanilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-2'-desoxi-2'-fluorouridilil-(5'→3')-adenilil-(5'→3')-2'-desoxi-2'-fluorocitidilil-(5'→3')-2'-desoxi-2'-fluorocitidilil-(5'→3')-adenilil-(5'→3')-2'-desoxi-2'-fluorocitidilil-(5'→3')-guanilil-(5'→3')-adenilil-(5'→3')-2'-desoxi-2'-fluorouridina reductor de la síntesis de colágeno
C504H640F12N171O326P47S2
1848266-71-6

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
323
renapersenum renapersen O-(2-hydroxyethyl) all-P-ambo-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-
thiocytidylyl-(3'→5')-2-O'-methyl-P-thioguanylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thiouridylyl-(3'→5')-2-O'-methyl-P-thioguanylyl-(3'→5')-2'-O-methyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O-methyl-P-thioadenylyl-(3'→5')-2'-O-methyl-P-thioadenylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thiouridylyl-(3'→5')-2-O'-methyl-P-thioguanylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O-methyl-P-thioadenylyl-(3'→5')-2'-O-methyl-P-thiouridylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(ethane-1,2-diyl)-5-methyl-P-thio-3'-cytidylate promotion of functional dystrophin synthesis
rénapersen tout-P-ambo-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2-O'-méthyl-P-thioguanylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiouridylyl-(3'→5')-2-O'-méthyl-P-thioguanylyl-(3'→5')-2'-O-méthyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O-méthyl-P-thioadenylyl-(3'→5')-2'-O-méthyl-P-thioadenylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiouridylyl-(3'→5')-2-O'-méthyl-P-thioguanylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O-méthyl-P-thioadenylyl-(3'→5')-2'-O-methyl-P-thiouridylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O,4'-C-(éthane-1,2-diyl)-5-méthyl-P-thio-3'-cytidylate de O-(2-hydroxyéthyle) stimulation de la synthèse de dystrophine fonctionnelle
renapersén todo-P-ambo-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiocitidilil-(3'→5')-2-O'-metil-P-tioguanilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiocitidilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiouridilil-(3'→5')-2-O'-metil-P-thoguanilil-(3'→5')-2'-O-metil-P-tiocitidilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiocitidilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiocitidilil-(3'→5')-2'-O-metil-P-tioadenilil-(3'→5')-2'-O-metil-P-tioadenilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiouridilil-(3'→5')-2-O'-metil-P-tioguanilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiocitidilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiocitidilil-(3'→5')-2'-O-metil-P-tioadenilil-(3'→5')-2'-O-metil-P-tiouridilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tiocitidilil-(3'→5')-2'-O,4'-C-(etano-1,2-diil)-5-metil-P-tio-3'-citidilato de O-(2-hidroxietilo) estimulación de la síntesis de distrofina funcional
C208H275N63O110P18S18
1782108-31-9
(3'-5')-(P-thio)[m5C(Et)-Gm-m5C(Et)-m5U(Et)-Gm-Cm-m5C(Et)-m5C(Et)-Am-Am-m5U(Et)-Gm
-m5C(Et)-m5C(Et)-Am-Um-m5C(Et)-m5C(Et)-(CH2-CH2-OH)]
Legend:(Et) as suffix = 2'-O,4'-C-(ethan-1,2-diyl)m as suffix = 2'-O-methylm5 as prefix = 5-methyl

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
324
rezafungini acetas rezafungin acetate N5.1,6-anhydro[(4R,5R)-4-hydroxy-2-[34-
(pentyloxy)[11,21:24,31-terphenyl]-14-carboxamido]-5-[2-(trimethylazaniumyl)ethyl]-L-ornithyl-L-threonyl-trans- 4-hydroxy-L-prolyl-(4S)-4-hydroxy-4-(4-hydroxyphenyl)- L-threonyl-L-threonyl-(3S,4S)-3-hydroxy-4-methyl-L-proline] acetate antifungal
acétate de rézafungine acétate de N5.1,6-anhydro[(4R,5R)-4-hydroxy-2-[34-(pentyloxy)[11,21:24,31-terphényl]-14-carboxamido]- 5-[2-(triméthylazaniumyl)éthyl]-L-ornithyl-L-thréonyl-trans- 4-hydroxy-L-prolyl-(4S)-4-hydroxy-4-(4-hydroxyphényl)- L-thréonyl-L-thréonyl-(3S,4S)-3-hydroxy-4-méthyl-L-proline] antifongique
acetato de rezafungina acetato de N5.1,6-anhidro[(4R,5R)-4-hidroxi-2-[34-(pentiloxi)[11,21:24,31-terfenil]-14-carboxamido]- 5-[2-(trimetilazaniumil)etil]-L-ornitil-L-treonil-trans-4-hidroxi-L-prolil-(4S)-4-hidroxi-4-(4-hidroxifenil)-L-treonil-L-treonil-(3S,4S)-3-hidroxi-4-metil-L-prolina] antifúngico
C63H85N8O17 . C2H3O2
1631754-41-0
riamilovirum riamilovir 7-(methylsulfanyl)-3-nitro[1,2,4]triazolo[5,1-c][1,2,4]triazin-
4(1H)-one antiviral
riamilovir 7-(méthylsulfanyl)-3-nitro[1,2,4]triazolo[5,1-c][1,2,4]triazin-4(1H)-one antiviral

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
325
riamilovir 7-(metilsulfanil)-3-nitro[1,2,4]triazolo[5,1-c][1,2,4]triazin-
4(1H)-ona antiviral
C5H4N6O3S
123606-06-4
rivoceranibum rivoceranib N-[4-(1-cyanocyclopentyl)phenyl]-2-{[(pyridin-
4-yl)methyl]amino}pyridine-3-carboxamide angiogenesis inhibitor, antineoplastic
rivocéranib N-[4-(1-cyanocyclopentyl)phényl]-2-{[(pyridin- 4-yl)méthyl]amino}pyridine-3-carboxamide inhibiteur de l'angiogénèse, antinéoplasique
rivoceranib N-[4-(1-cianociclopentil)fenil]-2-{[(piridin- 4-il)metil]amino}piridina-3-carboxamida inhibidor de la angiogénesis, antineoplásico
C24H23N5O
811803-05-1
rivogenlecleucelum # rivogenlecleucel Human culture expanded genetically modified allogenic T
cells for cell-based therapy. Cells are derived from isolated blood of a healthy human donor chosen by available HLA match (haploidentical up to fully matched) and are transduced with a Gibbon ape leukemia virus (GalV) pseudotyped gammaretroviral vector carrying an inducible caspase 9 suicide transgene and a truncated CD19 marker gene allowing selection, and a drug binding domain consisting of human FK506 (tacrolimus)-binding protein (FKBP12) with an F36V mutation. Cells exhibit anti-infective activity as adjunctive T-cell therapy in combination with allogenic hematopoietic stem cell transplantation, in combination with an inducible suicide mechanism in the event of donor T-cell induced graft versus host disease (GvHD). cell therapy substance (antineoplastic)

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
326
rivogenlecleucel Lymphocytes T humains allogéniques, en culture d'expansion et modifiés génétiquement en vue d'une thérapie cellulaire. Les cellules sont dérivées du sang prélevé chez un donneur sain choisi pour sa compatibilité HLA (de haploidentique à correspondant totalement) et sont transduites avec un vecteur rétroviral gamma pseudotypé virus de la leucémie du singe Gibbon (GalV) transportant un transgène suicide inductible de la caspase 9 et un gène CD19 tronqué comme marqueur permettant la sélection, ainsi qu'un domaine de liaison médicamenteuse consistant en la protéine humaine (FKBP12) se liant au tacrolimus (FK506) avec une mutation F36V. Les cellules montrent une activité anti-infectieuse comme thérapie adjuvante de lymphocytes T en association avec la transplantation de cellules souches hématopoïétiques allogéniques, en association aussi avec un mécanisme suicide inductible en cas de réaction du greffon contre l'hôte (GVH) induit par les lymphocytes T du donneur. substance de thérapie cellulaire (antinéoplasique)
rivogenlecleucel Linfocitos T alogénicos, humanos, expandidos en cultivo y modificados genéticamente para terapia celular. Las células se derivan a partir de sangre aislada de un donante humano sano elegido por su compatibilidad HLA (desde haploidéntico hasta totalmente coincidente) y están transducidas con un vector gamma-retroviral seudotipado del virus de la leucemia de monos Gibbon (GalV) que porta un transgen inducible suicida de caspasa 9 y un gen CD19 truncado como marcador que permite la selección, y un dominio de unión a drogas consistente en la proteína de unión al tacrólimus (FK506) humana (FKBP12) con una mutación F36V. Las células muestran actividad anti-infecciosa en terapia adyuvante de linfocitos T en combinación con trasplante alogénico de células madre hematopoyéticas, en combinación con un mecanismo suicida inducible en caso de enfermedad injerto contra huésped (EICH) inducida por los linfocitos T del donante. sustancia de terapia celular (antineoplásico)
rovazolacum rovazolac ethyl {5-[3'-(methanesulfonyl)[1,1'-biphenyl]-4-yl]-3-
(trifluoromethyl)-1H-pyrazol-1-yl}acetate anti-inflammatory
rovazolac {5-[3'-(méthanesulfonyl)[1,1'-biphényl]-4-yl]-3-(trifluorométhyl)-1H-pyrazol-1-yl}acétate d'éthyle anti-inflammatoire
rovazolac {5-[3'-(metanosulfonil)[1,1'-bifenil]-4-il]-3-(trifluorometil)-1H-pirazol-1-il}acetato de etilo antiinflamatorio
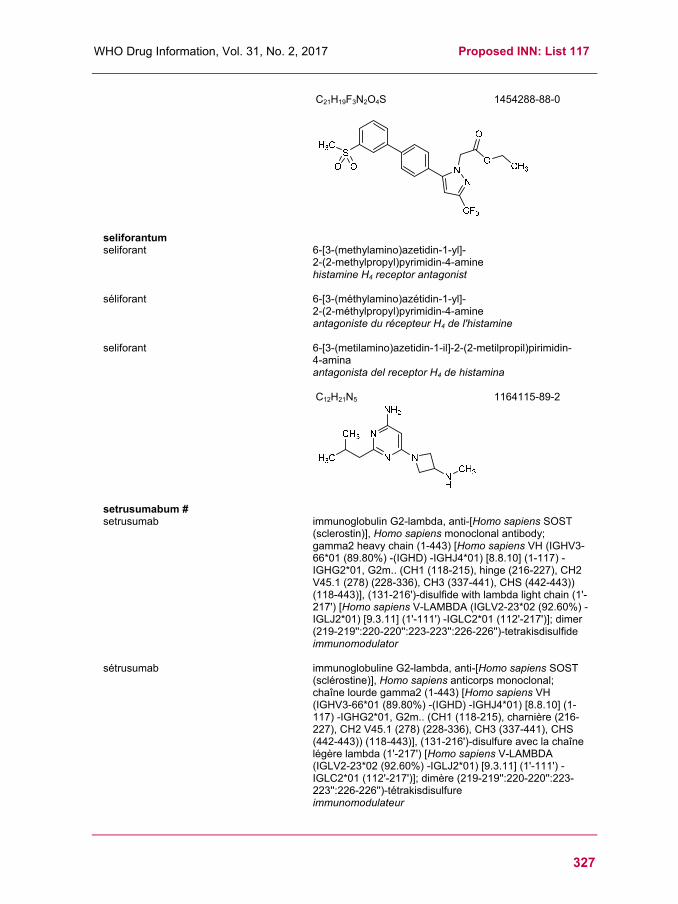
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
327
C21H19F3N2O4S
1454288-88-0
seliforantum seliforant 6-[3-(methylamino)azetidin-1-yl]-
2-(2-methylpropyl)pyrimidin-4-amine histamine H4 receptor antagonist
séliforant 6-[3-(méthylamino)azétidin-1-yl]- 2-(2-méthylpropyl)pyrimidin-4-amine antagoniste du récepteur H4 de l'histamine
seliforant 6-[3-(metilamino)azetidin-1-il]-2-(2-metilpropil)pirimidin- 4-amina antagonista del receptor H4 de histamina
C12H21N5 1164115-89-2
setrusumabum # setrusumab immunoglobulin G2-lambda, anti-[Homo sapiens SOST
(sclerostin)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-443) [Homo sapiens VH (IGHV3-66*01 (89.80%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117) -IGHG2*01, G2m.. (CH1 (118-215), hinge (216-227), CH2 V45.1 (278) (228-336), CH3 (337-441), CHS (442-443)) (118-443)], (131-216')-disulfide with lambda light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV2-23*02 (92.60%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimer (219-219'':220-220'':223-223'':226-226'')-tetrakisdisulfide immunomodulator
sétrusumab immunoglobuline G2-lambda, anti-[Homo sapiens SOST (sclérostine)], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-443) [Homo sapiens VH (IGHV3-66*01 (89.80%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117) -IGHG2*01, G2m.. (CH1 (118-215), charnière (216-227), CH2 V45.1 (278) (228-336), CH3 (337-441), CHS (442-443)) (118-443)], (131-216')-disulfure avec la chaîne légère lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV2-23*02 (92.60%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimère (219-219'':220-220'':223-223'':226-226'')-tétrakisdisulfure immunomodulateur
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
328
setrusumab inmunoglobulina G2-lambda, anti-[Homo sapiens SOST (esclerostina)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma2 (1-443) [Homo sapiens VH (IGHV3-66*01 (89.80%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117) -IGHG2*01, G2m.. (CH1 (118-215), bisagra (216-227), CH2 V45.1 (278) (228-336), CH3 (337-441), CHS (442-443)) (118-443)], (131-216')-disulfuro con la cadena ligera lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV2-23*02 (92.60%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dímero (219-219'':220-220'':223-223'':226-226'')-tetrakisdisulfuro inmunomodulador
1847394-95-9
sirtratumabum # sirtratumab immunoglobulin G2-kappa, anti-[Homo sapiens SLITRK6
(SLIT and NTRK like family member 6)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-446) [Homo sapiens VH (IGHV3-33*01 (96.90%) -(IGHD) -IGHJ6*01) [8.8.13] (1-120) -IGHG2*01, G2m.. (CH1 (121-218), hinge (219-230), CH2 V45.1 (281) (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-219')-disulfide with kappa light chain (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (93.00%) -IGKJ1*01) [11.3.9] (1'-112') -IGKC*01, Km3 A45.1 (158) V101 (196) (113'-219')]; dimer (222-222'':223-223'':226-226'':229-229'')-tetrakisdisulfide immunomodulator, antineoplastic
sirtratumab immunoglobuline G2-kappa, anti-[Homo sapiens SLITRK6 (membre 6 de la famille des analogues de SLIT et NTRK)], Homo sapiens anticorps monoclonal;

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
329
chaîne lourde gamma2 (1-446) [Homo sapiens VH
(IGHV3-33*01 (96.90%) -(IGHD) -IGHJ6*01) [8.8.13] (1-120) -IGHG2*01, G2m.. (CH1 (121-218), charnière (219-230), CH2 V45.1 (281) (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-219')-disulfure avec la chaîne légère (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (93.00%) -IGKJ1*01) [11.3.9] (1'-112') -IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dimère (222-222'':223-223'':226-226'':229-229'')-tétrakisdisulfure immunomodulateur, antinéoplasique
sirtratumab inmunoglobulina G2-kappa, anti-[Homo sapiens SLITRK6 (miembro 6 de la familia de los análogos de SLIT y NTRK)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma2 (1-446) [Homo sapiens VH (IGHV3-33*01 (96.90%) -(IGHD) -IGHJ6*01) [8.8.13] (1-120) -IGHG2*01, G2m.. (CH1 (121-218), bisagra (219-230), CH2 V45.1 (281) (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-219')-disulfuro con la cadena ligera (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (93.00%) -IGKJ1*01) [11.3.9] (1'-112') -IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dímero (222-222'':223-223'':226-226'':229-229'')-tetrakisdisulfuro inmunomodulador, antineoplásico
1824663-82-2
sirtratumabum vedotinum # sirtratumab vedotin immunoglobulin G2-kappa, anti-[Homo sapiens SLITRK6
(SLIT and NTRK like family member 6)], Homo sapiens monoclonal antibody conjugated to auristatin E;

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
330
gamma2 heavy chain (1-446) [Homo sapiens VH (IGHV3-33*01 (96.90%) -(IGHD) -IGHJ6*01) [8.8.13] (1-120) -IGHG2*01, G2m.. (CH1 (121-218), hinge (219-230), CH2 V45.1 (281) (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-219')-disulfide with kappa light chain (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (93.00%) -IGKJ1*01) [11.3.9] (1'-112') -IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dimer (222-222'':223-223'':226-226'':229-229'')-tetrakisdisulfide; conjugated, on an average of 4 cysteinyl, to monomethylauristatin E (MMAE), via a cleavable maleimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) type linker For the vedotin part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
immunomodulator, antineoplastic
sirtratumab védotine immunoglobuline G2-kappa, anti-[Homo sapiens SLITRK6 (membre 6 de la famille des analogues de SLIT et NTRK)], Homo sapiens anticorps monoclonal conjugué à l'auristatine E; chaîne lourde gamma2 (1-446) [Homo sapiens VH (IGHV3-33*01 (96.90%) -(IGHD) -IGHJ6*01) [8.8.13] (1-120) -IGHG2*01, G2m.. (CH1 (121-218), charnière (219-230), CH2 V45.1 (281) (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-219')-disulfure avec la chaîne légère (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (93.00%) -IGKJ1*01) [11.3.9] (1'-112') -IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dimère (222-222'':223-223'':226-226'':229-229'')-tétrakisdisulfure; conjugué, sur 4 cystéinyl en moyenne, au monométhylauristatine E (MMAE), via un linker clivable de type maléimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) Pour la partie védotine, veuillez vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
immunomodulateur, antinéoplasique
sirtratumab vedotina inmunoglobulina G2-kappa, anti-[Homo sapiens SLITRK6 (miembro 6 de la familia de los análogos de SLIT y NTRK)], Homo sapiens anticuerpo monoclonal conjugado con la auristatina E; cadena pesada gamma2 (1-446) [Homo sapiens VH (IGHV3-33*01 (96.90%) -(IGHD) -IGHJ6*01) [8.8.13] (1-120) -IGHG2*01, G2m.. (CH1 (121-218), bisagra (219-230), CH2 V45.1 (281) (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-219')-disulfuro con la cadena ligera (1'-219') [Homo sapiens V-KAPPA (IGKV2-28*01 (93.00%) -IGKJ1*01) [11.3.9] (1'-112') -IGKC*01, Km3 A45.1 (158), V101 (196) (113'-219')]; dímero (222-222'':223-223'':226-226'':229-229'')-tetrakisdisulfuro; conjugado, con 4 grupos cisteinil por término medio, con la monometilauristatina E (MMAE), mediante un enlace escindible de tipo maleimidocaproil-valil-citrulinil-p-aminobenziloxicarbonil (mc-val-cit-PABC) Para la fracción vedotina se puede referir al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
inmunomodulador, antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
331
1824663-83-3
spartalizumabum # spartalizumab immunoglobulin G4-kappa, anti-[Homo sapiens PDCD1
(programmed cell death 1, PD-1, PD1, CD279)], humanized monoclonal antibody; gamma4 heavy chain (1-443) [humanized VH (Homo sapiens IGHV1-69-2*01 (75.00%) -(IGHD) -IGHJ6*01) [8.8.10] (1-117) -Homo sapiens IGHG4*01 (CH1 (118-215), hinge S10>P (225) (216-227), CH2 (228-337), CH3 (338-442), CHS K2>del (443)) (118-443)], (131-220')-disulfide with kappa light chain (1'-220') [humanized V-KAPPA (Homo sapiens IGKV3D-11*03 (75.80%) -IGKJ1*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (114'-220')]; dimer (223-223'':226-226'')-bisdisulfide immunomodulator, antineoplastic
spartalizumab immunoglobuline G4-kappa, anti-[Homo sapiens PDCD1 (protéine 1 de mort cellulaire programmée, PD-1, PD1, CD279)], anticorps monoclonal humanisé; chaîne lourde gamma4 (1-443) [VH humanisé (Homo sapiens IGHV1-69-2*01 (75.00%) -(IGHD) -IGHJ6*01) [8.8.10] (1-117) -Homo sapiens IGHG4*01 (CH1 (118-215), charnière S10>P (225) (216-227), CH2 (228-337), CH3 (338-442), CHS K2>del (443)) (118-443)], (131-220')-disulfure avec la chaîne légère kappa (1'-220') [V-KAPPA humanisé (Homo sapiens IGKV3D-11*03 (75.80%) -IGKJ1*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (114'-220')]; dimère (223-223'':226-226'')-bisdisulfure immunomodulateur, antinéoplasique

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
332
espartalizumab inmunoglobulina G4-kappa, anti-[Homo sapiens PDCD1 (proteína 1 de muerte celular programada, PD-1, PD1, CD279)], anticuerpo monoclonal humanizado; cadena pesada gamma4 (1-443) [VH humanizado (Homo sapiens IGHV1-69-2*01 (75.00%) -(IGHD) -IGHJ6*01) [8.8.10] (1-117) -Homo sapiens IGHG4*01 (CH1 (118-215), bisagra S10>P (225) (216-227), CH2 (228-337), CH3 (338-442), CHS K2>del (443)) (118-443)], (131-220')-disulfuro con la cadena ligera kappa (1'-220') [V-KAPPA humanizado (Homo sapiens IGKV3D-11*03 (75.80%) -IGKJ1*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (114'-220')]; dímero (223-223'':226-226'')-bisdisulfuro inmunomodulador, antineoplásico
1935694-88-4
sultimotidum alfa # sultimotide alfa a fusion protein consisting of fragments of hepatitis B virus
transcription factor X, large S-protein antigen (envelope antigen), B antigen (core antigen) and of a C-terminal six-histidine tag, expressed by engineered whole heat-killed Saccharomyces cerevisiae, glycoform alfa; Met-Ala-Asp-Glu-Ala-Pro-Thr-Ser-{des-(69-83)-[P59>F]pro-tein X (hepatitis B virus)-(52-127)-peptide (9-69)}-{[M1>E,G3>Q,Q10>K,P19S,G35>R,N39>A,H51>T,P65>L,T86>Q,A91>N]large S protein (hepatitis B virus) (70-243)}-{[T4>I,V25>I,N207>S,L209>V,L213>I]small S protein (hepatitis B virus) (244-469)}-{des-Met1-[S12>T]capsid protein (hepatitis B virus) (470-651)}-His6 (652-657) fusion protein, produced in Saccharomyces cerevisiae, glycoform alfa immunological agent for active immunization (antiviral)

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
333
sultimotide alfa protéine de fusion consistant en des fragments du facteur X de transcription du virus de l’hépatite B, de l’antigène de la grande protéine S (antigène de l’enveloppe), antigène B (antigène core) et d’un fragment de 6 histidines, exprimée par une souche de Saccharomyces cerevisiae inactivée par la chaleur, glycoforme alfa: Met-Ala-Asp-Glu-Ala-Pro-Thr-Ser-{dès-(69-83)-[P59>F]pro-téine X (virus de l’hépatite B)-(52-127)-peptide (9-69)}-{[M1>E,G3>Q,Q10>K,P19S,G35>R,N39>A,H51>T,P65>L,T86>Q,A91>N]grande protéine S (virus de l’hépatite B) (70-243)}-{[T4>I,V25>I,N207>S,L209>V,L213>I]petite protéine S (virus de l’hépatite B) (244-469)}-{dès-Mét1-[S12>T]protéine de la capside (virus de l’hépatite B) (470-651)}-His6 (652-657) protéine de fusion, produite par Saccharomyces cerevisiae, glycoforme alfa agent immunologique d'immunisation active (antiviral)
sultimotida alfa proteína de fusión consistente en los fragmentos del factor X de transcripción del virus de la hepatitis B, del antígeno de la proteína S grande (antígeno de la envoltura), antígeno B (antígeno nuclear) y de un fragmento de 6 histidinas, producida por una cepa de Saccharomyces cerevisiae inactivada por el calor, glicoforma alfa: Met-Ala-Asp-Glu-Ala-Pro-Thr-Ser-{des-(69-83)-[P59>F]proteína X (virus de la hepatitis B)-(52-127)-péptido}-{[M1>E,G3>Q,Q10>K,P19S,G35>R,N39>A,H51>T,P65>L,T86>Q,A91>N]proteína S grande(virus de la hepatitis B)}-{[T4>I,V25>I,N207>S,L209>V,L213>I]proteína S pequeña (virus de la hepatitis B)}-{des-Met1-[S12>T]proteína de la cápside (virus de la hepatitis B)}-His6 proteína de fusión, producida por Saccharomyces cerevisiae, glicoforma alfa agente inmunológico para inmunización activa (antiviral)
1518923-92-6

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
334
tabelecleucelum tabelecleucel Human culture enriched allogenic Epstein-Barr virus-
specific cytotoxic T cells (EBV-CTL) for cell-based therapy. Cells are isolated from blood of EBV seropositive healthy human donors. EBV-CTLs exhibit human leukocyte antigen (HLA)-restricted cytotoxic activity against EBV+ cells in allogeneic hematopoietic cell transplant patients with EBV associated post-transplant lymphoproliferative disease. cell therapy substance (transplantation)
tabélecleucel Lymphocytes T cytotoxiques spécifiques du virus d'Epstein-Barr (EBV-CTL), allogéniques, humains, enrichis en culture pour thérapie cellulaire. Les cellules sont isolées à partir du sang de donneurs humains sains séropositifs à l'EBV. Les EBV-CTL montrent une activité cytotoxique restreinte à l'antigène leucocytaire humain (HLA) contre les cellules EBV+ chez des patients transplantés avec des cellules hématopoïétiques allogéniques souffrants d'un syndrome lymphoprolifératif associé à l'EBV post-transplantation. substance pour thérapie cellulaire (transplantation)
tabelecleucel Linfocitos T citotóxicos específicos del virus de Epstein-Barr (EBV-CTL), alogénicos, humanos, enriquecidos en cultivo para terapia celular. Las células están asiladas a partir de sangre de donantes humanos sanos seropositivo para EBV. Los EBV-CTLs muestran actividad citotóxica restringida por HLA contra células EBV+ in pacientes trasplantados con células hematopoyéticas alogénicas con enfermedad linfoproliferativa post-trasplante asociada a EBV. sustancia de terapia celular (trasplante)
talacotuzumabum # talacotuzumab immunoglobulin G1-2-kappa, anti-[Homo sapiens IL3RA
(interleukin 3 receptor subunit alpha, interleukin 3 receptor alpha (low affinity), CD123)], humanized monoclonal antibody; gamma1-2 heavy chain (1-450) [humanized VH (Homo sapiens IGHV5-51*01 (82.70%) -(IGHD) -IGHJ3*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01 (CH1 G1m17, K120 (217) (121-218) -hinge (219-233) -CH2 1.6-1.1 (234-239)) (121-239) -Homo sapiens IGHG2*01 (CH2 1-125, S3>D (242), G2m.. V45.1 (285), G110>A (330), I117>E (335) (240-343) -CH3 nG1m1 E12 (359), M14 (361) (344-448), CHS (449-450)) (240-450)], (223-220')-disulfide with kappa light chain (1'-220') [humanized V-KAPPA (Homo sapiens IGKV4-1*01 (90.10%) -IGKJ2*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dimer (229-229":232-232")-bisdisulfide immunomodulator, antineoplastic
talacotuzumab immunoglobuline G1-2-kappa, anti-[Homo sapiens IL3RA (sous-unité alpha du récepteur de l'interleukine 3, récepteur alpha (faible affinité) de l'interleukine 3, CD123)], anticorps monoclonal humanisé;

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
335
chaîne lourde gamma1-2 (1-450) [VH humanisé (Homo sapiens IGHV5-51*01 (82.70%) -(IGHD) -IGHJ3*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01 (CH1 G1m17, K120 (217) (121-218) -charnière (219-233) -CH2 1.6-1.1 (234-239))(121-239) -Homo sapiens IGHG2*01 (CH2 1-125, S3>D (242), G2m.. V45.1 (285), G110>A (330), I117>E (335) (240-343) -CH3 nG1m1 E12 (359), M14 (361) (344-448), CHS (449-450)) (240-450)], (223-220')-disulfure avec la chaîne légère kappa (1'-220') [V-KAPPA humanisé (Homo sapiens IGKV4-1*01 (90.10%) -IGKJ2*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1, V101 (114'-220')]; dimère (229-229":232-232")-bisdisulfure immunomodulateur, antinéoplasique
talacotuzumab inmunoglobulina G1-2-kappa, anti-[Homo sapiens IL3RA (subunidad alfa del receptor de la interleukina 3, receptor alfa (baja afinidad) de la interleukina 3, CD123)], anticuerpo monoclonal humanizado; cadena pesada gamma1-2 (1-450) [VH humanizado (Homo sapiens IGHV5-51*01 (82.70%) -(IGHD) -IGHJ3*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01 (CH1 G1m17, K120 (217) (121-218) -bisagra (219-233) -CH2 1.6-1.1 (234-239)) (121-239) -Homo sapiens IGHG2*01 (CH2 1-125, S3>D (242), G2m.. V45.1 (285), G110>A (330), I117>E (335) (240-343) -CH3 nG1m1 E12 (359), M14 (361) (344-448), CHS (449-450)) (240-450)], (223-220')-disulfuro con la cadena ligera kappa (1'-220') [V-KAPPA humanizado (Homo sapiens IGKV4-1*01 (90.10%) -IGKJ2*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1, V101 (114'-220')]; dímero (229-229":232-232")-bisdisulfuro inmunomodulador, antineoplásico
1826831-79-1

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
336
tasadenoturevum # tasadenoturev conditionally replicating adenovirus (CRAd) serotype 5
carrying a 24-bp deletion in early E1A gene and insertion of an integrin-binding motif (Arg-Gly-Asp) (RGD) motif into the H1 loop of the fiber knob. antineoplastic
tasadénoturev adénovirus de sérotype 5 dont la réplication est conditionnelle et portant une délétion de 24 paires de bases sur le gène précoce E1A et l'insertion d'un motif d'union à l'intégrine dans la boucle H1 du knob de la fibre antinéoplasique
tasadenoturev adenovirus de serotipo 5, con replicación condicionada, portando una deleción de 24 pares de bases en el gen temprano E1A y la inserción de un motivo de unión a integrina (Arg-Gly-Asp) (RGD) en el bucle H1 del knob de la fibra antineoplásico
1448774-00-2
tasipimidinum tasipimidine rac-2-[(1R)-5-methoxy-3,4-dihydro-1H-2-benzopyran-1-yl]-
4,5-dihydro-1H-imidazole α2 adrenoreceptor agonist (veterinary drug)
tasipimidine rac-2-[(1R)-5-méthoxy-3,4-dihydro-1H-2-benzopyran-1-yl]-4,5-dihydro-1H-imidazole agoniste des récepteurs α2-adrénergiques (usage vétérinaire)
tasipimidina rac-2-[(1R)-5-metoxi-3,4-dihidro-1H-2-benzopiran-1-il]- 4,5-dihidro-1H-imidazol agonista de los receptores α 2-adrenérgicos (uso veterinario)
C13H16N2O2
1465908-70-6
telacebecum telacebec 6-chloro-2-ethyl-N-[(4-{4-[4-
(trifluoromethoxy)phenyl]piperidin-1-yl}phenyl)methyl]imidazo[1,2-a]pyridine-3-carboxamide antituberculosis
télacébec 6-chloro-2-éthyl-N-[(4-{4-[4-(trifluorométhoxy)phényl]pipéridin-1-yl}phényl)méthyl]imidazo[1,2-a]pyridine-3-carboxamide antituberculeux

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
337
telacebec 6-cloro-2-etil-N-[(4-{4-[4-(trifluorometoxi)fenil]piperidin- 1-il}fenil)metil]imidazo[1,2-a]piridina-3-carboxamida antituberculoso
C29H28ClF3N4O2
1334719-95-7
temavirsenum temavirsen [(2S,4R)-1-{1-[(2-acetamido-2-deoxy-β-D-
galactopyranosyl)oxy]-16,16-bis({3-[(3-{5-[(2-acetamido-2-deoxy-β-D-galactopyranosyl)oxy]pentanamido}propyl)amino]-3-oxopropoxy}methyl)-5,11,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oyl}-4-hydroxypyrrolidin-2-yl]methyl hydrogen all-P-ambo-2'-O-(2-methoxyethyl)-P-thioadenylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O-(2-methoxyethyl)-P-thioadenylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O-(2-methoxyethyl)-P-thioadenylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiouridylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-P-thiouridylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-P-thiocytidylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-P-thiocytidylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]-P-thiocytidylyl-(3'→5')-2'-O,4'-C-[(1S)-ethane-1,1-diyl]cytidylyl-(3'→5')-2'-deoxy-3'-adenylate antiviral
témavirsen hydrogéno-tout-P-ambo-2'-O-(2-méthoxyéthyl)-P-thioadénylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-P-thioadénylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-P-thioadénylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiouridylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-désoxy-P-thioguanylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-P-thiouridylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-P-thiocytidylyl-(3'→5')-2'-désoxy-P-thioadénylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-P-thiocytidylyl-(3'→5')-2'-désoxy-P-thioadénylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]-P-thiocytidylyl-(3'→5')-2'-O,4'-C-[(1S)-éthane-1,1-diyl]cytidylyl-(3'→5')-2'-désoxy-3'-adénylate
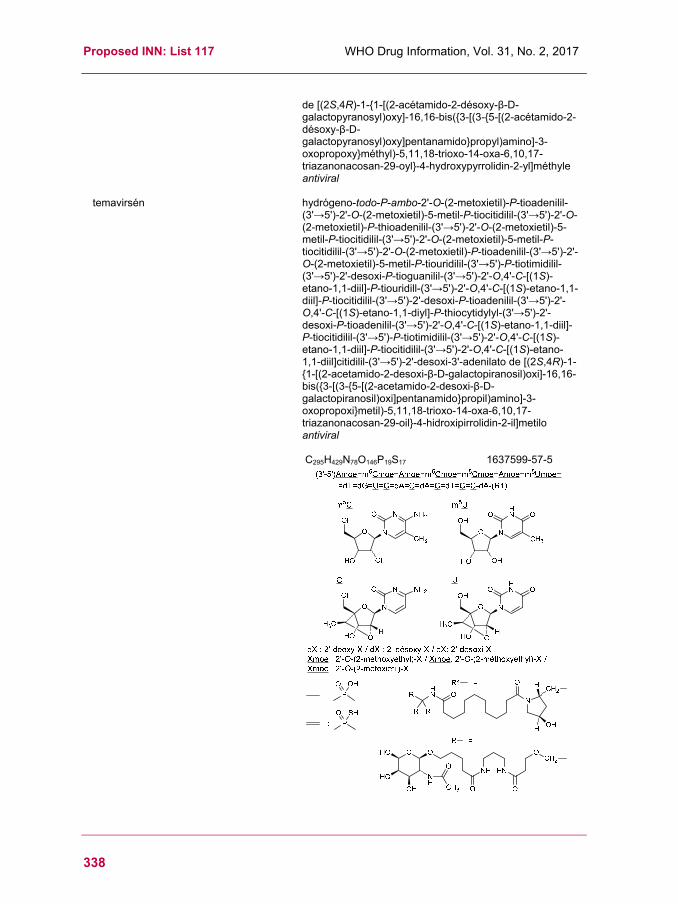
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
338
de [(2S,4R)-1-{1-[(2-acétamido-2-désoxy-β-D-galactopyranosyl)oxy]-16,16-bis({3-[(3-{5-[(2-acétamido-2-désoxy-β-D-galactopyranosyl)oxy]pentanamido}propyl)amino]-3-oxopropoxy}méthyl)-5,11,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oyl}-4-hydroxypyrrolidin-2-yl]méthyle antiviral
temavirsén hydrógeno-todo-P-ambo-2'-O-(2-metoxietil)-P-tioadenilil-(3'→5')-2'-O-(2-metoxietil)-5-metil-P-tiocitidilil-(3'→5')-2'-O-(2-metoxietil)-P-thioadenilil-(3'→5')-2'-O-(2-metoxietil)-5-metil-P-tiocitidilil-(3'→5')-2'-O-(2-metoxietil)-5-metil-P-tiocitidilil-(3'→5')-2'-O-(2-metoxietil)-P-tioadenilil-(3'→5')-2'-O-(2-metoxietil)-5-metil-P-tiouridilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-P-tiouridill-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-P-tiocitidilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diyl]-P-thiocytidylyl-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-P-tiocitidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]-P-tiocitidilil-(3'→5')-2'-O,4'-C-[(1S)-etano-1,1-diil]citidilil-(3'→5')-2'-desoxi-3'-adenilato de [(2S,4R)-1-{1-[(2-acetamido-2-desoxi-β-D-galactopiranosil)oxi]-16,16-bis({3-[(3-{5-[(2-acetamido-2-desoxi-β-D-galactopiranosil)oxi]pentanamido}propil)amino]-3-oxopropoxi}metil)-5,11,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oil}-4-hidroxipirrolidin-2-il]metilo antiviral
C295H429N78O146P19S17 1637599-57-5

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
339
tibulizumabum # tibulizumab immunoglobulin G4-kappa anti-[Homo sapiens TNFSF13B
(tumor necrosis factor (TNF) superfamily member 13B, BAFF, THANK, TALL1, TALL-1, BLYS, BLyS, B cell activating factor, B lymphocyte activator, CD257)] , each heavy chain being fused to a scFv anti-[Homo sapiens IL17A (interleukin 17A, IL-17A)], humanized monoclonal antibody, bispecific tetravalent; gamma4 heavy chain anti-TNFSF13B fused to a scFv anti-IL17A (1-714) [gamma4 heavy chain {(Homo sapiens VH (IGHV4-34*01 (100.00%) -(IGHD) -IGHJ4*01) [8.7.17] (1-123) -Homo sapiens IGHG4*01 (CH1 (124-221), hinge S10>P (231) (222-233), CH2 (234-343), CH3L125>del (344-447), CHS G1>del, K2>del) (124-447)} (1-447) -16-mer linker (448-463) -scFv {(humanized VH (Homo sapiens IGHV1-69*01 (83.70%) -(IGHD) -IGHJ4*01) [8.8.12] (464-582) -20-mer tetra(tetraglycyl-seryl) linker (583-602) -humanized V-KAPPA (Homo sapiens IGKV2D-29*02 (89.00%) -IGKJ2*02) [11.3.9] (603-714)} (464-714)], (137-214')-disulfide with kappa light chain anti-TNFSF13B (1'-214') [Homo sapiens V-KAPPA (IGKV3-11*01 (97.90%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*05, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (229-229'':232-232'')-bisdisulfide immunomodulator
tibulizumab immunoglobuline G4-kappa anti-[Homo sapiens TNFSF13B (membre 13B de la superfamille des facteurs de nécrose tumorale (TNF), BAFF, THANK, TALL1, TALL-1, BLYS, BLyS, facteur d'activation des lymphocytes B, activateur des lymphocytes B, CD257)], chaque chaîne lourde étant fusionnée à un scFv anti-[Homo sapiens IL17A (interleukine 17A, IL-17A)], anticorps monoclonal humanisé, bispécifique tétravalent; chaîne lourde gamma4 anti-TNFSF13B fusionnée à un scFv anti-IL17A (1-714) [chaîne lourde gamma4 {(Homo sapiens VH (IGHV4-34*01 (100.00%) -(IGHD) -IGHJ4*01) [8.7.17] (1-123) -Homo sapiens IGHG4*01 (CH1 (124-221), charnière S10>P (231) (222-233), CH2 (234-343), CH3 L125>del (344-447), CHS G1>del, K2>del) (124-447)} (1-447) -16-mer linker (448-463) -scFv {(VH humanisé (Homo sapiens IGHV1-69*01 (83.70%) -(IGHD) -IGHJ4*01) [8.8.12] (464-582) -20-mer tétra(tétraglycyl-séryl) linker (583-602) -V-KAPPA humanisé (Homo sapiens IGKV2D-29*02 (89.00%) -IGKJ2*02) [11.3.9] (603-714)} (464-714)], (137-214')-disulfure avec la chaîne légère anti-TNFSF13B (1'-214') [Homo sapiens V-KAPPA (IGKV3-11*01 (97.90%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*05, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (229-229'':232-232'')-bisdisulfure immunomodulateur
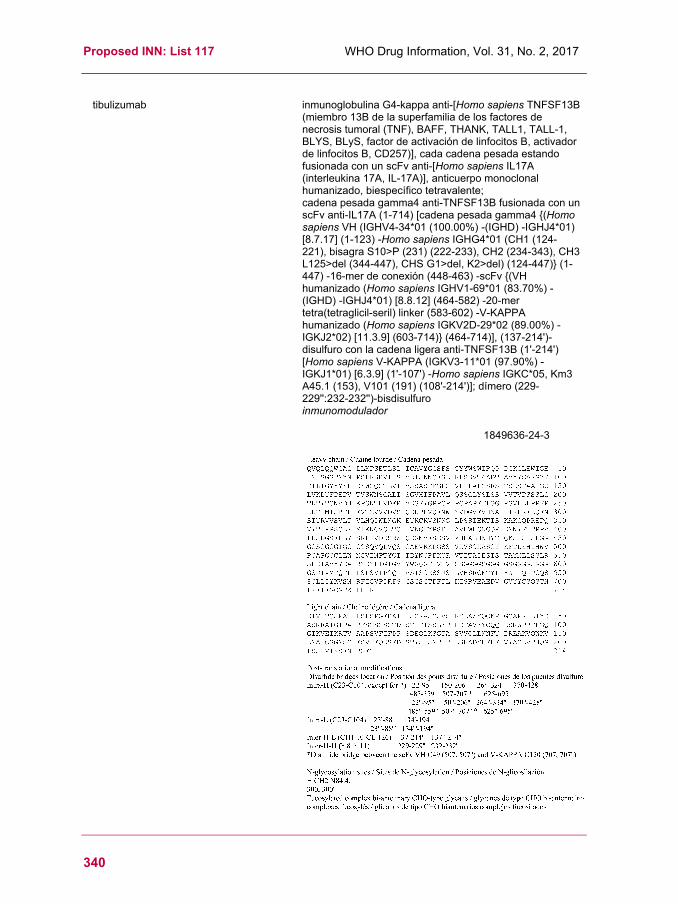
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
340
tibulizumab inmunoglobulina G4-kappa anti-[Homo sapiens TNFSF13B (miembro 13B de la superfamilia de los factores de necrosis tumoral (TNF), BAFF, THANK, TALL1, TALL-1, BLYS, BLyS, factor de activación de linfocitos B, activador de linfocitos B, CD257)], cada cadena pesada estando fusionada con un scFv anti-[Homo sapiens IL17A (interleukina 17A, IL-17A)], anticuerpo monoclonal humanizado, biespecífico tetravalente; cadena pesada gamma4 anti-TNFSF13B fusionada con un scFv anti-IL17A (1-714) [cadena pesada gamma4 {(Homo sapiens VH (IGHV4-34*01 (100.00%) -(IGHD) -IGHJ4*01) [8.7.17] (1-123) -Homo sapiens IGHG4*01 (CH1 (124-221), bisagra S10>P (231) (222-233), CH2 (234-343), CH3 L125>del (344-447), CHS G1>del, K2>del) (124-447)} (1-447) -16-mer de conexión (448-463) -scFv {(VH humanizado (Homo sapiens IGHV1-69*01 (83.70%) -(IGHD) -IGHJ4*01) [8.8.12] (464-582) -20-mer tetra(tetraglicil-seril) linker (583-602) -V-KAPPA humanizado (Homo sapiens IGKV2D-29*02 (89.00%) -IGKJ2*02) [11.3.9] (603-714)} (464-714)], (137-214')-disulfuro con la cadena ligera anti-TNFSF13B (1'-214') [Homo sapiens V-KAPPA (IGKV3-11*01 (97.90%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*05, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (229-229'':232-232'')-bisdisulfuro inmunomodulador
1849636-24-3
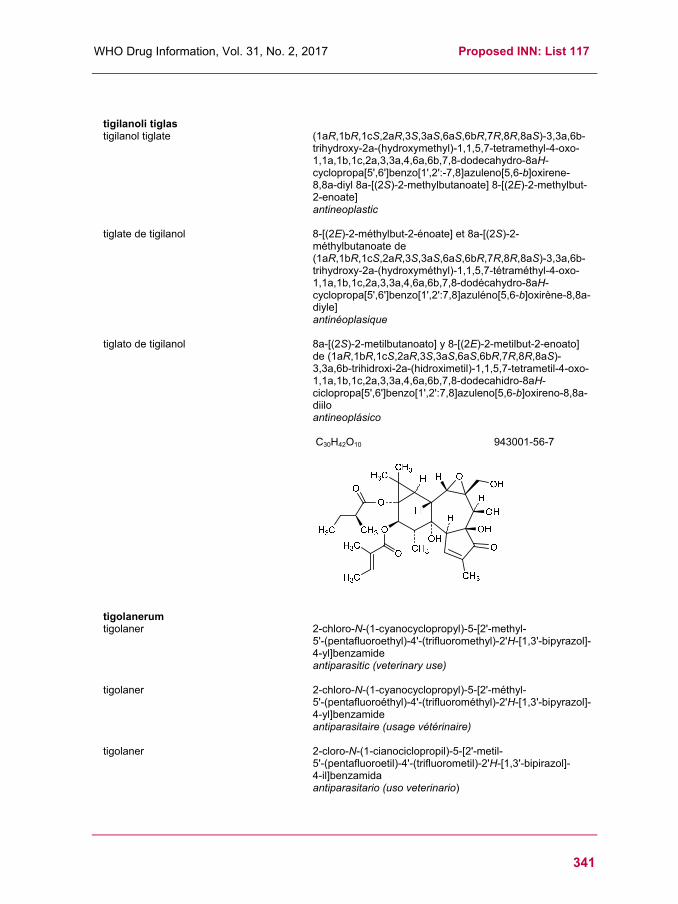
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
341
tigilanoli tiglas tigilanol tiglate (1aR,1bR,1cS,2aR,3S,3aS,6aS,6bR,7R,8R,8aS)-3,3a,6b-
trihydroxy-2a-(hydroxymethyl)-1,1,5,7-tetramethyl-4-oxo-1,1a,1b,1c,2a,3,3a,4,6a,6b,7,8-dodecahydro-8aH-cyclopropa[5',6']benzo[1',2':-7,8]azuleno[5,6-b]oxirene-8,8a-diyl 8a-[(2S)-2-methylbutanoate] 8-[(2E)-2-methylbut-2-enoate] antineoplastic
tiglate de tigilanol 8-[(2E)-2-méthylbut-2-énoate] et 8a-[(2S)-2-méthylbutanoate de (1aR,1bR,1cS,2aR,3S,3aS,6aS,6bR,7R,8R,8aS)-3,3a,6b-trihydroxy-2a-(hydroxyméthyl)-1,1,5,7-tétraméthyl-4-oxo-1,1a,1b,1c,2a,3,3a,4,6a,6b,7,8-dodécahydro-8aH-cyclopropa[5',6']benzo[1',2':7,8]azuléno[5,6-b]oxirène-8,8a-diyle] antinéoplasique
tiglato de tigilanol 8a-[(2S)-2-metilbutanoato] y 8-[(2E)-2-metilbut-2-enoato] de (1aR,1bR,1cS,2aR,3S,3aS,6aS,6bR,7R,8R,8aS)-3,3a,6b-trihidroxi-2a-(hidroximetil)-1,1,5,7-tetrametil-4-oxo-1,1a,1b,1c,2a,3,3a,4,6a,6b,7,8-dodecahidro-8aH-ciclopropa[5',6']benzo[1',2':7,8]azuleno[5,6-b]oxireno-8,8a-diilo antineoplásico
C30H42O10 943001-56-7
tigolanerum tigolaner 2-chloro-N-(1-cyanocyclopropyl)-5-[2'-methyl-
5'-(pentafluoroethyl)-4'-(trifluoromethyl)-2'H-[1,3'-bipyrazol]-4-yl]benzamide antiparasitic (veterinary use)
tigolaner 2-chloro-N-(1-cyanocyclopropyl)-5-[2'-méthyl- 5'-(pentafluoroéthyl)-4'-(trifluorométhyl)-2'H-[1,3'-bipyrazol]-4-yl]benzamide antiparasitaire (usage vétérinaire)
tigolaner 2-cloro-N-(1-cianociclopropil)-5-[2'-metil- 5'-(pentafluoroetil)-4'-(trifluorometil)-2'H-[1,3'-bipirazol]- 4-il]benzamida antiparasitario (uso veterinario)

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
342
C21H13ClF8N6O 1621436-41-6
tilsotolimodum tilsotolimod O,O'-(2-hydroxypropane-1,3-diyl) bis(hydrogen all-P-ambo-
P-thiothymidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxy-7-carba-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxy-7-carba-P-thioguanylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxy-7-carba-P-thio-3'-guanylate) immunomodulator, antineoplastic
tilsotolimod bis(hydrogéno-tout-P-ambo-P-thiothymidylyl-(3'→5')-2'-désoxy-P-thiocytidylyl-(3'→5')-2'-désoxy-7-carba-P-thioguanylyl-(3'→5')-2'-désoxy-P-thioadénylyl-(3'→5')-2'-désoxy-P-thioadénylyl-(3'→5')-2'-désoxy-P-thiocytidylyl-(3'→5')-2'-désoxy-7-carba-P-thioguanylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-désoxy-P-thiocytidylyl-(3'→5')-2'-désoxy-7-carba-P-thio-3'-guanylate) de O,O'-(2-hydroxypropane-1,3-diyle) immunomodulateur, antinéoplasique
tilsotolimod bis(hidrógeno-todo-P-ambo-P-tiotimidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxi-7-carba-P-tioguanilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxi-7-carba-P-tioguanilil-(3'→5')-P-tiotimidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxi-7-carba-P-tio-3'-guanilato) de O,O'-(2-hidroxipropano-1,3-diilo) inmunomodulador, antineoplásico
C223H284N74O115P22S22 1948266-37-2
O
HO
OH
N
NH
N O
H2Nc7G
OH
O
O
P
P
(3'-5')d(P-thio)(T-C-c7G-A-A-C-c7G-T-T-C-c7G)
(3'-5')d(P-thio)(T-C-c7G-A-A-C-c7G-T-T-C-c7G)
OHS
SOH
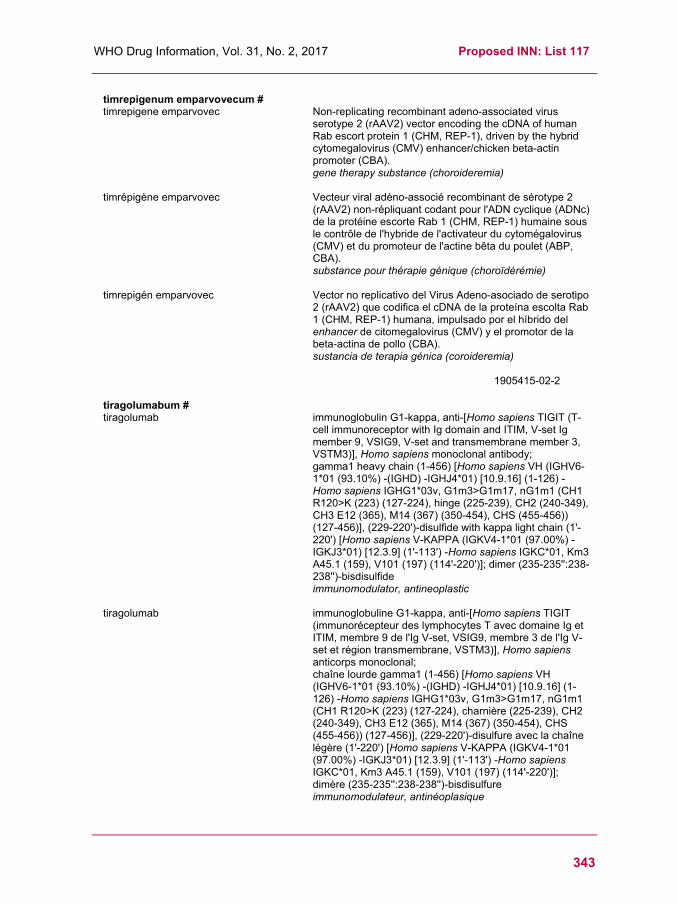
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
343
timrepigenum emparvovecum # timrepigene emparvovec Non-replicating recombinant adeno-associated virus
serotype 2 (rAAV2) vector encoding the cDNA of human Rab escort protein 1 (CHM, REP-1), driven by the hybrid cytomegalovirus (CMV) enhancer/chicken beta-actin promoter (CBA). gene therapy substance (choroideremia)
timrépigène emparvovec Vecteur viral adéno-associé recombinant de sérotype 2 (rAAV2) non-répliquant codant pour l'ADN cyclique (ADNc) de la protéine escorte Rab 1 (CHM, REP-1) humaine sous le contrôle de l'hybride de l'activateur du cytomégalovirus (CMV) et du promoteur de l'actine bêta du poulet (ABP, CBA). substance pour thérapie génique (choroïdérémie)
timrepigén emparvovec Vector no replicativo del Virus Adeno-asociado de serotipo 2 (rAAV2) que codifica el cDNA de la proteína escolta Rab 1 (CHM, REP-1) humana, impulsado por el híbrido del enhancer de citomegalovirus (CMV) y el promotor de la beta-actina de pollo (CBA). sustancia de terapia génica (coroideremia)
1905415-02-2
tiragolumabum # tiragolumab immunoglobulin G1-kappa, anti-[Homo sapiens TIGIT (T-
cell immunoreceptor with Ig domain and ITIM, V-set Ig member 9, VSIG9, V-set and transmembrane member 3, VSTM3)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-456) [Homo sapiens VH (IGHV6-1*01 (93.10%) -(IGHD) -IGHJ4*01) [10.9.16] (1-126) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (223) (127-224), hinge (225-239), CH2 (240-349), CH3 E12 (365), M14 (367) (350-454), CHS (455-456)) (127-456)], (229-220')-disulfide with kappa light chain (1'-220') [Homo sapiens V-KAPPA (IGKV4-1*01 (97.00%) -IGKJ3*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dimer (235-235'':238-238'')-bisdisulfide immunomodulator, antineoplastic
tiragolumab immunoglobuline G1-kappa, anti-[Homo sapiens TIGIT (immunorécepteur des lymphocytes T avec domaine Ig et ITIM, membre 9 de l'Ig V-set, VSIG9, membre 3 de l'Ig V-set et région transmembrane, VSTM3)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-456) [Homo sapiens VH (IGHV6-1*01 (93.10%) -(IGHD) -IGHJ4*01) [10.9.16] (1-126) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (223) (127-224), charnière (225-239), CH2 (240-349), CH3 E12 (365), M14 (367) (350-454), CHS (455-456)) (127-456)], (229-220')-disulfure avec la chaîne légère (1'-220') [Homo sapiens V-KAPPA (IGKV4-1*01 (97.00%) -IGKJ3*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dimère (235-235'':238-238'')-bisdisulfure immunomodulateur, antinéoplasique

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
344
tiragolumab inmunoglobulina G1-kappa, anti-[Homo sapiens TIGIT
(inmunoreceptor de linfocitos T con dominio Ig e ITIM, miembro 9 de la Ig V-set, VSIG9, miembro 3 de la Ig V-set y región transmembrana, VSTM3)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-456) [Homo sapiens VH (IGHV6-1*01 (93.10%) -(IGHD) -IGHJ4*01) [10.9.16] (1-126) -Homo sapiens IGHG1*03v, G1m3>G1m17, nG1m1 (CH1 R120>K (223) (127-224), bisagra (225-239), CH2 (240-349), CH3 E12 (365), M14 (367) (350-454), CHS (455-456)) (127-456)], (229-220')-disulfuro con la cadena ligera (1'-220') [Homo sapiens V-KAPPA (IGKV4-1*01 (97.00%) -IGKJ3*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dímero (235-235'':238-238'')-bisdisulfuro inmunomodulador, antineoplásico
1918185-84-8
tirvalimogenum teraplasmidum # tirvalimogene teraplasmid plasmid DNA vector encoding E6 and E7 antigens of
human papillomavirus types 16 and 18 (HPV 16/18), the extracellular domain of fms-like tyrosine kinase-3 ligand (FLT3L) and signal sequences of tissue plasminogen activator (tpa) driven by a cytomegalovirus promoter. gene therapy substance (anti-HPV)
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
345
tirvalimogène téraplasmide vecteur constitué d'ADN plasmidique codant pour les
antigènes E6 et E7 des papillomavirus humains de types 16 et 18 (VPH 16/18), le domaine extracellulaire du ligand de la tyrosine kinase 3 semblable au fms (FLT3L) et les séquences signal de l'activateur tissulaire du plasmogène (tpa) sous le contrôle d'un promoteur de cytomégalovirus. substance pour thérapie génique (anti-VPH)
tirvalimogén teraplásmido Vector de DNA plasmídico que codifica los antígenos E6 y E7 de los tipos 16 y 18 del virus del papiloma humano (VPH 16/18), el dominio extracelular del ligando de la tirosina quinasa-3 similar a fms (FLT3L) y secuencias señal del activador de plasminógeno tisular (tpa) impulsado por un promotor de citomegalovirus. sustancia de terapia génica (anti-VPH)
1905430-26-3
tisagenlecleucelum # tisagenlecleucel Human culture expanded genetically modified autologous
T cells for cell-based gene therapy. Cells are derived from isolated blood of the patient and are transduced with non-replicative lentiviral vector encoding an FMC63 anti-CD19 single chain variable fragment (scFv) 4-1BB/CD3zeta chimeric antigen receptor (CAR) under the control of the EF-1 alpha promoter. Cells exhibit anti-tumoral activity in patients with CD19-expressing B cell malignancies. cell genetically modified (antineoplastic)
tisagenlecleucel Lymphocytes T autologues humains en culture d'expansion, modifiés génétiquement en vue d'une thérapie génique avec cellules. Les cellules sont isolées à partir du sang prélevé chez le patient et sont transduites avec un veceur lentiviral non-répliquant codant pour le récepteur de l'antigène chimérique (CAR) FMC63 anti-CD-19 fragment de la chaîne simple de la région variable de l'anticorps (scFv) 4-1BB/CD3zêta (SFG-1928z CAR) sous le contrôle du promoteur EF-1 alpha. Les cellules montrent une activité anti-tumorale chez les patients présentant des lymphocytes B malins exprimant le CD19. cellule génétiquement modifiée (antinéoplasique)
tisagenlecleucel Linfocitos T autólogos, humanos, expandidos en cultivo y modificados genéticamente, para terapia génica con células. Las células se derivan a partir de sangre aislada del paciente y están transducidas con un vector lentiviral no replicativo que codifica para el receptor de antígenos quimérico (CAR) FMC63 anti-CD19 fragmento de cadena simple de la región variable del anticuerpo (scFv) 4-1BB/CD3zeta bajo el control del promotor EF-1 alfa. Las células muestran actividad anti-tumoral en pacientes con malignidades de linfocitos B que expresan CD19. célula modificada genéticamente (antineoplásico)

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
346
tislelizumabum # tislelizumab immunoglobulin G4-kappa, anti-[Homo sapiens PDCD1
(programmed cell death 1, PD-1, PD1, CD279)], humanized monoclonal antibody; gamma4 heavy chain (1-445) [humanized VH (Homo sapiens IGHV4-59*01 (88.70%) -(IGHD) -IGHJ3*01 M123>T (113)) [8.7.12] (1-118) -Homo sapiens IGHG4*01 (CH1 (119-216), hinge S10>P (226) (217-228), CH2 E1.4>P (231), F1.3>V (232), L1.2>A (233), D27>A (263) (229-338), CH3 R88>K (407) (339-443), CHS (444-445)) (119-445)], (132-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV4-1*01 (81.20%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (224-224":227-227")-bisdisulfide immunomodulator, antineoplastic
tislélizumab immunoglobuline G4-kappa, anti-[Homo sapiens PDCD1 (protéine 1 de mort cellulaire programmée, PD-1, PD1, CD279)], anticorps monoclonal humanisé; chaîne lourde gamma4 (1-445) [VH humanisé (Homo sapiens IGHV4-59*01 (88.70%) -(IGHD) -IGHJ3*01 M123>T (113)) [8.7.12] (1-118) -Homo sapiens IGHG4*01 (CH1 (119-216), charnière S10>P (226) (217-228), CH2 E1.4>P (231), F1.3>V (232), L1.2>A (233), D27>A (263) (229-338), CH3 R88>K (407) (339-443), CHS (444-445)) (119-445)], (132-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV4-1*01 (81.20%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (224-224":227-227")-bisdisulfure immunomodulateur, antinéoplasique
tislelizumab inmunoglobulina G4-kappa, anti-[Homo sapiens PDCD1 (proteína 1 de muerte celular programada, PD-1, PD1, CD279)], anticuerpo monoclonal humanizado; cadena pesada gamma4 (1-445) [VH humanizado (Homo sapiens IGHV4-59*01 (88.70%) -(IGHD) -IGHJ3*01 M123>T (113)) [8.7.12] (1-118) -Homo sapiens IGHG4*01 (CH1 (119-216), bisagra S10>P (226) (217-228), CH2 E1.4>P (231), F1.3>V (232), L1.2>A (233), D27>A (263) (229-338), CH3 R88>K (407) (339-443), CHS (444-445)) (119-445)], (132-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV4-1*01 (81.20%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (224-224":227-227")-bisdisulfuro inmunomodulador, antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
347
1858168-59-8
tralesinidasum alfa # tralesinidase alfa human α-N-acetylglucosaminidase fused to truncated
human insulin-like growth factor II (IGF2) via a peptide linker, produced in Chinese hamster ovary (CHO) cells, glycoform alfa;
human α-N-acetylglucosaminidase (NAG, EC=3.2.1.50) (1-720) fusion protein with glycyl-L-alanyl-L-prolyltriglycyl-L-seryl-bis(L-prolyl-L-alanyl-L-prolyl-L-alanyl-L-prolyl-L-threonyl)-bis(L-prolyl-L-alanyl)-triglycyl-L-prolyl-L-serylglycyl-L-alanyl-L-prolyl-[37-L-alanine(R37>A(781))]human insulin-like growth factor II (somatomedin-A, T3M-11-derived growth factor, IGF-II) (8-67)-peptide (752-811), produced in Chinese hamster ovary (CHO) cells, glycoform alfa enzyme replacement therapy
tralésinidase alfa alpha-N-acétylglucosaminidase humaine fusionnée au facteur II de croissance humain analogue à l'insuline (IGF2) tronqué, via un peptide de liaison, produit dans des cellules ovariennes de hamster chinois (CHO), glycoforme alfa;
alpha-N-acétylglucosaminidase humaine (NAG, EC=3.2.1.50) (1-720) protéine de fusion avec glycyl-L-alanyl-L-prolyltriglycyl-L-séryl-bis(L-prolyl-L-alanyl-L-prolyl-L-alanyl-L-prolyl-L-thréonyl)-bis(L-prolyl-L-alanyl)-triglycyl-L-prolyl-L-sérylglycyl-L-alanyl-L-prolyl-[37-L-alanine(R37>A(781))]facteur II de croissance analogue à l'insuline humain (somatomédine-A, T3M-11-facteur de croissance dérivé, IGF-II) (8-67)-peptide (752-811), produit dans des cellules ovariennes de hamster chinois (CHO), glycoforme alfa traitement enzymatique substitutif

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
348
tralesinidasa alfa alfa-N-acetilglucosaminidasa humana fusionada con el
factor II de crecimiento humano análogo a la insulina (IGF2) truncada, vía un péptido de unión, producida en las células ováricas de hamster chino (CHO), glicoforma alfa; alfa-N-acetilglucosaminidasa humana (NAG, EC=3.2.1.50) (1-720) proteína de fusión con glicil-L-alanil-L-proliltriglicil-L-seril-bis(L-prolil-L-alanil-L-prolil-L-alanil-L-prolil-L-treonil-bis(L-prolil-L-alanil)-triglicil-L-prolil-L-serilglicil-L-alanil-L-prolil-[37-L-alanina(R37>A(781))]factor II de crecimiento análogo a la insulina humano (somatomedina-A, T3M-11-factor de crecimiento derivado, IGF-II) (8-67)-péptido (752-811), producido en las células ováricas de hamster chino (CHO), glicoforma alfa tratamiento enzimático de sustitución
1808916-28-0
trilaciclibum trilaciclib 2'-{[5-(4-methylpiperazin-1-yl)pyridin-2-yl]amino}-
7',8'-dihydro-6'H-spiro[cyclohexane- 1,9'-pyrazino[1',2':1,5]pyrrolo[2,3-d]pyrimidin]-6'-one cyclin dependent kinase inhibitor
trilaciclib 2'-{[5-(4-méthylpipérazin-1-yl)pyridin-2-yl]amino}- 7',8'-dihydro-6'H-spiro[cyclohexane- 1,9'-pyrazino[1',2':1,5]pyrrolo[2,3-d]pyrimidin]-6'-one inhibiteur de la kinase dépendante de la cycline
trilaciclib 2'-{[5-(4-metilpiperazin-1-il)piridin-2-il]amino}-7',8'-dihidro-6'H-spiro[ciclohexano-1,9'-pirazino[1',2':1,5]pirrolo[2,3-d]pirimidin]-6'-ona inhibidor de la quínasa dependente de la ciclina

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
349
C24H30N8O 1374743-00-6
vactosertibum vactosertib 2-fluoro-N-{[4-(6-methylpyridin-2-yl)-5-([1,2,4]triazolo[1,5-
a]pyridin-6-yl)-1H-imidazol-2-yl]methyl}aniline antineoplastic
vactosertib 2-fluoro-N-{[4-(6-méthylpyridin-2-yl)-5-([1,2,4]triazolo[1,5-a]pyridin-6-yl)-1H-imidazol-2-yl]méthyl}aniline antinéoplasique
vactosertib 2-fluoro-N-{[4-(6-metilpiridin-2-il)-5-([1,2,4]triazolo[1,5-a]piridin-6-il)-1H-imidazol-2-il]metil}anilina antineoplásico
C22H18FN7 1352608-82-2
vadacabtagenum leraleucelum # vadacabtagene leraleucel Human culture expanded genetically modified autologous
T cells for cell-based gene therapy. Cells are derived from isolated blood of the patient and are transduced with non-replicative retroviral vector encoding the SJ25C1 anti-CD19 single chain variable fragment (scFv) CD28/CD3zeta chimeric antigen receptor (SFG-1928z CAR). Cells exhibit anti-tumoral activity in patients with CD19-expressing B cell malignancies. cell genetically modified (antineoplastic)
vadacabtagène léraleucel Lymphocytes T humains autologues en culture d'expansion et modifiés génétiquement pour thérapie génique avec cellules. Les cellules sont dérivées du sang prélévé chez le patient et sont transduites avec un vecteur rétroviral non-répliquant codant pour le récepteur de l'antigène chimérique SJ25C1 anti-CD-19 fragment de la chaîne simple de la région variable de l'anticorps (scFv) CD28/CD3zêta (SFG-1928z CAR). Les cellules montrent une activité anti-tumorale chez les patients présentant des lymphocytes B malins exprimant le CD19. cellule génétiquement modifiée (antinéoplasique)

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
350
vadacabtagén leraleucel Linfocitos T autólogos, humanos, expandidos en cultivo y
modificados genéticamente, para terapia génica con células. Las células se derivan a partir de sangre aislada del paciente y están transducidas con un vector retroviral no replicativo que codifica para el receptor de antígenos quimérico SJ25C1 anti-CD19 fragmento de cadena simple de la región variable del anticuerpo (scFv) CD28/CD3zeta (SFG-1928z CAR). Las células muestran actividad anti-tumoral en pacientes con malignidades de linfocitos B que expresan CD19. célula modificada genéticamente (antineoplásico)
valzifloceptum # valziflocept human immunoglobulin gamma Fc region receptor II-b
(FcγRII-b), extracellular N-terminal fragment, produced in Escherichia coli; human low affinity immunoglobulin gamma Fc region receptor II-b (IgG Fc receptor II-b, CDw32, Fc-gamma RII-b, FcRII-b, antigen CD32)-(4-179) peptide (N-terminal extracellular portion), produced in Escherichia coli immunomodulator
valziflocept récepteur II-b de la région Fc de l’immunoglobuline gamma humaine (FcγRII-b), fragment extracellulaire N-terminal, produit par Escherichia coli; récepteur II-b de faible affinité pour la région Fc de l’immunoglobuline gamma humaine (IgG Fc récepteur II-b, CDw32, Fc-gamma RII-b, FcRII-b, antigène CD32)-(4-179) peptide (partie extracellulaire immunomodulateur
valziflocept receptor II-b de la región Fc de la inmunoglobulina gamma humana (FcγRII-b), fragmento extracelular N-terminal, producido por Escherichia coli; receptor II-b de baja afinidad para la región Fc de la inmunoglobulina gamma humana (IgG Fc receptor II-b, CDw32, Fc-gamma RII-b, FcRII-b, antígeno CD32)-(4-179) péptido (parte extracelular N-terminal), producido por Escherichia coli inmunomodulador
1804910-11-9

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
351
vatinoxanum vatinoxan N-{2-[(2R,12bS)-2'-oxo-1,3,4,6,7,12b-
hexahydrospiro[[1]benzofuro[2,3-a]quinolizine- 2,4'-imidazolidin]-3'-yl]ethyl}methanesulfonamide peripheral α2 adrenoreceptor antagonist (veterinary drug)
vatinoxan N-{2-[(2R,12bS)-2'-oxo-1,3,4,6,7,12b-hexahydrospiro[[1]benzofuro[2,3-a]quinolizine- 2,4'-imidazolidin]-3'-yl]ethyl}méthanesulfonamide antagoniste des récepteurs α2 adrénergiques périphériques (usage vétérinaire)
vatinoxán N-{2-[(2R,12bS)-2'-oxo-1,3,4,6,7,12b-hexahidrospiro[[1]benzofuro[2,3-a]quinolizina- 2,4'-imidazolidin]-3'-il]etil}metanosulfonamida antagonista de los receptores α2 adrenérgicos periféricos(uso veterinario)
C20H26N4O4S 114914-42-0
vecabrutinibum vecabrutinib (3R,3'R,4'S)-1'-(6-amino-5-fluoropyrimidin-4-yl)-3-[3-chloro-
5-(trifluoromethyl)anilino]-2-oxo[1,3'-bipiperidine]- 4'-carboxamide antineoplastic
vécabrutinib (3R,3'R,4'S)-1'-(6-amino-5-fluoropyrimidin-4-yl)-3-{[3-chloro-5-(trifluorométhyl)phényl]amino}-2-oxo-[1,3'-bipipéridine]-4'-carboxamide antinéoplasique
vecabrutinib (3R,3'R,4'S)-1'-(6-amino-5-fluoropirimidin-4-il)-3-{[3-cloro-5-(trifluorometil)fenil]amino}-2-oxo-[1,3'-bipiperidina]- 4'-carboxamida antineoplásico
C22H24ClF3N7O2 1510829-06-7
N
N
N
F
NH2
HH
N
NH2
O
ONH H
Cl
CF3
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
352
veldoreotidum veldoreotide N4.1,Cα.8-anhydro[N-(2-amino-2-oxoethyl)-4-aminobutanoyl-
4-aminobutanoyl-L-phenylalanyl-L-tryptophyl-D-tryptophyl-L-lysyl-L-threonyl-L-phenylalanine] somatostatin analogue
veldoréotide N4.1,Cα.8-anhydro[N-(2-amino-2-oxoéthyl)-4-aminobutanoyl-4-aminobutanoyl-L-phénylalanyl-L-tryptophyl-D-tryptophyl-L-lysyl-L-thréonyl-L-phénylalanine] analogue de la somatostatine
veldoreotida N4.1-(2-amino-2-oxoetil)-1,8-anhidro(4-aminobutanoil- 4-aminobutanoil-L-fenilalanil-L-triptofil-D-triptofil-L-lisil- L-treonil-L-fenilalanina) análogo de la somatostatina
C60H74N12O10 252845-37-7
vorasidenibum vorasidenib 6-(6-chloropyridin-2-yl)-N2,N4-bis[(2R)-1,1,1-
trifluoropropan-2-yl]-1,3,5-triazine-2,4-diamine antineoplastic
vorasidénib 6-(6-chloropyridin-2-yl)-N2,N4-bis[(2R)-1,1,1-trifluoropropan-2-yl]-1,3,5-triazine-2,4-diamine antinéoplasique
vorasidenib 6-(6-cloropiridin-2-il)-N2,N4-bis[(2R)-1,1,1-trifluoropropan- 2-il]-1,3,5-triazina-2,4-diamina antineoplásico
C14H13ClF6N6 1644545-52-7
votrisiranum votrisiran {(2S,4R)-1-{1-[(2-acetamido-2-deoxy-β-D-
galactopyranosyl)oxy]-16,16-bis-({3-[(3-{5-[(2-acetamido-2-deoxy-β-D-galactopyranosyl)oxy]pentanamido}propyl)amino]-3-oxopropoxy}methyl)-5,11,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oyl}-4-hydroxypyrrolidin-2-yl}methyl
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
353
hydrogen all-P-ambo-2'-O-methyl-P-thiouridylyl-(3'→5')-2'-O-methyl-P-thioguanylyl-(3'→5')-2'-O-methylguanylyl-(3'→5')-2'-O-methylguanylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-deoxy-2'-fluorouridylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-deoxy-2'-fluorocytidylyl-(3'→5')-2'-deoxy-2'-fluoroadenylyl-(3'→5')-2'-deoxy-2'-fluorouridylyl-(3'→5')-2'-O-methylguanylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methyladenylyl-(3'→5')-2'-O-methylguanylyl-(3'→5')-2'-O-methyl-3'-adenylate duplex with all-P-ambo-2'-O-methyl-P-thiocytidylyl-(5'→3')-2'-O-methyl-P-thiouridylyl-(5'→3')-2'-O-methyladenylyl-(5'→3')-2'-O-methylcytidylyl-(5'→3')-2'-O-methylcytidylyl-(5'→3')-2'-O-methylcytidylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-deoxy-2'-fluoroadenylyl-(5'→3')-2'-O-methyladenylyl-(5'→3')-2'-deoxy-2'-fluoroadenylyl-(5'→3')-2'-O-methylguanylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-O-methyladenylyl-(5'→3')-2'-O-methylcytidylyl-(5'→3')-2'-deoxy-2'-fluoroadenylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-deoxy-2'-fluoroguanylyl-(5'→3')-2'-O-methylguanylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-2'-O-methyl-P-thiouridylyl-(5'→3')-2'-deoxy-2'-fluoro-P-thiocytidylyl-(5'→3')-2'-O-methyluridine transthyretin synthesis inhibitor
votrisiran hydrogéno-tout-P-ambo-2'-O-méthyl-P-thiouridylyl-(3'→5')-2'-O-méthyl-P-thioguanylyl-(3'→5')-2'-O-méthylguanylyl-(3'→5')-2'-O-méthylguanylyl-(3'→5')-2'-O-méthyladenylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-désoxy-2'-fluorouridylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-désoxy-2'-fluorocytidylyl-(3'→5')-2'-désoxy-2'-fluoroadénylyl-(3'→5')-2'-désoxy-2'-fluorouridylyl-(3'→5')-2'-O-méthylguanylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthyladenylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-O-méthyladénylyl-(3'→5')-2'-O-méthylguanylyl-(3'→5')-2'-O-méthyl-3'-adénylate de {(2S,4R)-1-{1-[(2-acétamido-2-désoxy-β-D-galactopyranosyl)oxy]-16,16-bis-({3-[(3-{5-[(2-acétamido-2-désoxy-β-D-galactopyranosyl)oxy]pentanamido}propyl)amino]-3-oxopropoxy}méthyl)-5,11,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oyl}-4-hydroxypyrrolidin-2-yl}méthyle duplex avec tout-P-ambo-2'-O-méthyl-P-thiocytidylyl-(5'→3')-2'-O-méthyl-P-thiouridylyl-(5'→3')-2'-O-méthyladénylyl-(5'→3')-2'-O-méthylcytidylyl-(5'→3')-2'-O-méthylcytidylyl-(5'→3')-2'-O-méthylcytidylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-2'-désoxy-2'-fluoroadénylyl-(5'→3')-2'-O-méthyladénylyl-(5'→3')-2'-désoxy-2'-fluoroadénylyl-(5'→3')-2'-O-méthylguanylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-2'-O-méthyladénylyl-(5'→3')-2'-O-méthylcytidylyl-(5'→3')-2'-désoxy-2'-fluoroadénylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-2'-désoxy-2'-fluoroguanylyl-(5'→3')-2'-O-méthylguanylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-2'-O-méthyl-P-thiouridylyl-(5'→3')-2'-désoxy-2'-fluoro-P-thiocytidylyl-(5'→3')-2'-O-méthyluridine inhibiteur de la synthèse de la transthyrétine
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
354
votrisirán hidrógeno-todo-P-ambo-2'-O-metil-P-tiouridilil-(3'→5')-2'-O-metil-P-tioguanilil-(3'→5')-2'-O-metilguanilil-(3'→5')-2'-O-metilguanilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-desoxi-2'-fluorouridilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-desoxi-2'-fluorocitidilil-(3'→5')-2'-desoxi-2'-fluoroadenilil-(3'→5')-2'-desoxi-2'-fluorouridilil-(3'→5')-2'-O-metilguanilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metiladenilil-(3'→5')-2'-O-metilguanilil-(3'→5')-2'-O-metil-3'-adenilato de {(2S,4R)-1-{1-[(2-acetamido-2-desoxi-β-D-galactopiranosil)oxi]-16,16-bis-({3-[(3-{5-[(2-acetamido-2-desoxi-β-D-galactopiranosil)oxi]pentanamido}propil)amino]-3-oxopropoxi}metil)-5,11,18-trioxo-14-oxa-6,10,17-triazanonacosan-29-oil}-4-hidroxipirrolidin-2-il}metilo dúplex con todo-P-ambo-2'-O-metil-P-tiocitidilil-(5'→3')-2'-O-metil-P-tiouridilil-(5'→3')-2'-O-metiladenilil-(5'→3')-2'-O-metilcitidilil-(5'→3')-2'-O-metilcitidilil-(5'→3')-2'-O-metilcitidilil-(5'→3')-2'-O-metiluridilil-(5'→3')-2'-desoxi-2'-fluoroadenylyl-(5'→3')-2'-O-metiladenilil-(5'→3')-2'-desoxi-2'-fluoroadenilil-(5'→3')-2'-O-metilguanilil-(5'→3')-2'-O-metiluridilil-(5'→3')-2'-O-metiladenilil-(5'→3')-2'-O-metilcitidilil-(5'→3')-2'-desoxi-2'-fluoroadenilil-(5'→3')-2'-O-metiluridilil-(5'→3')-2'-O-metiluridilil-(5'→3')-2'-desoxi-2'-fluoroguanilil-(5'→3')-2'-O-metilguanilil-(5'→3')-2'-O-metiluridilil-(5'→3')-2'-O-metil-P-tiouridilil-(5'→3')-2'-desoxi-2'-fluoro-P-tiocitidilil-(5'→3')-2'-O-metiluridina inhibidor de la síntesis de transtiretina
C530H715F9N171O323P43S6
1867157-35-4

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
355
zanubrutinibum zanubrutinib (7S)-2-(4-phenoxyphenyl)-7-[1-(prop-2-enoyl)piperidin-
4-yl]-4,5,6,7-tetrahydropyrazolo[1,5-a]pyrimidine- 3-carboxamide antineoplastic
zanubrutinib (7S)-2-(4-phénoxyphényl)-7-[1-(prop-2-enoyl)pipéridin- 4-yl]-4,5,6,7-tétrahydropyrazolo[1,5-a]pyrimidine- 3-carboxamide antinéoplasique
zanubrutinib (7S)-2-(4-fenoxifenil)-7-[1-(prop-2-enoil)piperidin-4-il]-4,5,6,7-tetrahidropirazolo[1,5-a]pirimidina-3-carboxamida antineoplásico
C27H29N5O3 1691249-45-2
zenocutuzumabum # zenocutuzumab immunoglobulin G1-kappa, anti-[Homo sapiens ERBB3
(receptor tyrosine-protein kinase erbB-3, HER3) and Homo sapiensERBB2 (epidermal growth factor receptor 2, receptor tyrosine-protein kinase erbB-2, EGFR2, HER2, HER-2, p185c-erbB2, NEU, CD340)], humanized monoclonal antibody, bispecific; gamma1 heavy chain anti-ERBB3 (1-453) [Homo sapiens VH (IGHV1-2*02 (100.00%) -(IGHD) -IGHJ4*01) [8.8.17] (1-124) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (221) (125-222), hinge (223-237), CH2 (238-347), CH3 L7>K (358), E12 (363), M14 (365), T22>K (373) (348-452), CHS K>del (453)) (125-453)], (227-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (100.00%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; gamma1 heavy chain anti-ERBB2 (1-450) [humanized VH (Homo sapiens IGHV1-46*01 (83.70%) -(IGHD) -IGHJ4*01) [8.8.14] (1-121) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (218) (122-219), hinge (220-234), CH2 (235-344), CH3 L7>D (355), E12 (360), M14 (362), L24>E (372) (345-449), CHS K>del (450)) (122-450)] (224-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (100.00%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimer (233-230":236-233")-bisdisulfide immunomodulator, antineoplastic

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
356
zénocutuzumab immunoglobuline G1-kappa, anti-[Homo sapiens ERBB3 (récepteur à activité tyrosine kinase erbB-3, HER3) et Homo sapiensERBB2 (récepteur 2 du facteur de croissance épidermique, récepteur tyrosine-protéine kinase erbB-2, EGFR2, HER2, HER-2, p185c-erbB2, NEU, CD340)], anticorps monoclonal humanisé, bispécifique; chaîne lourde gamma1 anti-ERBB3 (1-453) [Homo sapiens VH (IGHV1-2*02 (100.00%) -(IGHD) -IGHJ4*01) [8.8.17] (1-124) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (221) (125-222), charnière (223-237), CH2 (238-347), CH3 L7>K (358), E12 (363), M14 (365), T22>K (373) (348-452), CHS K>del (453)) (125-453)], (227-214')-disulfure avec la chaîne légère kappa (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (100.00%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; chaîne lourde gamma1 anti-ERBB2 (1-450) [VH humanisé (Homo sapiens IGHV1-46*01 (83.70%) -(IGHD) -IGHJ4*01) [8.8.14] (1-121) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (218) (122-219), charnière (220-234), CH2 (235-344), CH3 L7>D (355), E12 (360), M14 (362), L24>E (372) (345-449), CHS K>del (450)) (122-450)] (224-214')-disulfure avec la chaîne légère kappa (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (100.00%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dimère (233-230":236-233")-bisdisulfure immunomodulateur, antinéoplasique
zenocutuzumab inmunoglobulina G1-kappa, anti-[Homo sapiens ERBB3 (receptor de la actividad tirosina kinasa erbB-3, HER3) y Homo sapiensERBB2 (receptor 2 del factor de crecimiento epidérmico, receptor tirosina-proteína kinasa erbB-2, EGFR2, HER2, HER-2, p185c-erbB2, NEU, CD340)], anticuerpo monoclonal humanizado, biespecífico; cadena pesada gamma1 anti-ERBB3 (1-453) [Homo sapiens VH (IGHV1-2*02 (100.00%) -(IGHD) -IGHJ4*01) [8.8.17] (1-124) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (221) (125-222), bisagra (223-237), CH2 (238-347), CH3 L7>K (358), E12 (363), M14 (365), T22>K (373) (348-452), CHS K>del (453)) (125-453)], (227-214')-disulfuro con la cadena ligera kappa (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (100.00%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; cadena pesada gamma1 anti-ERBB2 (1-450) [VH humanizado (Homo sapiens IGHV1-46*01 (83.70%) -(IGHD) -IGHJ4*01) [8.8.14] (1-121) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (218) (122-219), bisagra (220-234), CH2 (235-344), CH3 L7>D (355), E12 (360), M14 (362), L24>E (372) (345-449), CHS K>del (450)) (122-450)] (224-214')-disulfuro con la cadena ligera kappa (1'-214') [Homo sapiens V-KAPPA (IGKV1-39*01 (100.00%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 A45.1 (153), V101 (191) (108'-214')]; dímero (233-230":236-233")-bisdisulfuro inmunomodulador, antineoplásico

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
357
1969309-56-5
zolbetuximabum # zolbetuximab immunoglobulin G1-kappa, anti-[Homo sapiens CLDN18
(claudin 18, claudin-18, SFTPJ, surfactant associated protein J) isoform 2, extracellular domain 1 (EC1)], chimeric monoclonal antibody; gamma1 heavy chain (1-448) [Mus musculus VH (IGHV1-61*01 (92.90%) -(IGHD) -IGHJ2*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (215) (119-216), hinge (217-231), CH2 (232-341), CH3 E12 (357), M14 (359) (342-446), CHS (447-448)) (119-448)], (221-220')-disulfide with kappa light chain (1'-220') [Mus musculus V-KAPPA (IGKV8-19*01 (100.00%) -IGKJ4*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dimer (227-227'':230-230'')-bisdisulfide immunomodulator, antineoplastic
zolbétuximab immunoglobuline G1-kappa, anti-[Homo sapiens CLDN18 (claudine 18, claudine-18, SFTPJ, surfactant associé à la protéine J) isoforme 2, domaine extracellulaire 1 (EC1)], anticorps monoclonal chimérique; chaîne lourde gamma1 (1-448) [Mus musculus VH (IGHV1-61*01 (92.90%) -(IGHD) -IGHJ2*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (215) (119-216), charnière (217-231), CH2 (232-341), CH3 E12 (357), M14 (359) (342-446), CHS (447-448)) (119-448)], (221-220')-disulfure avec la chaîne légère kappa (1'-220') [Mus musculus V-KAPPA (IGKV8-19*01 (100.00%) -IGKJ4*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dimère (227-227'':230-230'')-bisdisulfure immunomodulateur, antinéoplasique

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
358
zolbetuximab inmunoglobulina G1-kappa, anti-[Homo sapiens CLDN18
(claudina 18, claudina-18, SFTPJ, surfactante asociado a la proteína J) isoforma 2, dominio extracelular 1 (EC1)], anticuerpo monoclonal quimérico; cadena pesada gamma1 (1-448) [Mus musculus VH (IGHV1-61*01 (92.90%) -(IGHD) -IGHJ2*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3, nG1m1 (CH1 R120 (215) (119-216), bisagra (217-231), CH2 (232-341), CH3 E12 (357), M14 (359) (342-446), CHS (447-448)) (119-448)], (221-220')-disulfuro con la cadena ligera kappa (1'-220') [Mus musculus V-KAPPA (IGKV8-19*01 (100.00%) -IGKJ4*01) [12.3.9] (1'-113') -Homo sapiens IGKC*01, Km3 A45.1 (159), V101 (197) (114'-220')]; dímero (227-227'':230-230'')-bisdisulfuro inmunomodulador, antineoplásico
1496553-00-4
# Electronic structure available on Mednet: http://mednet.who.int/ # Structure électronique disponible sur Mednet: http://mednet.who.int/ # Estructura electrónica disponible en Mednet: http://mednet.who.int/ * http://www.who.int/medicines/services/inn/publication/en/

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
359
Names for Radicals and Groups Some substances for which a proposed international nonproprietary name has been established may be used in the form of salts or esters. The radicals or groups involved may be of complex composition and it is then inconvenient to refer to them in a systematic chemical nomenclature. Consequently, shorter nonproprietary names for some radicals and groups have been devised or selected, and they are suggested for use with the proposed international nonproprietary names. Dénominations applicables aux radicaux et groupes Certaines substances pour lesquelles une dénomination commune internationale proposée a été établie sont parfois utilisées sous forme de sels ou d'esters. Les radicaux ou groupes correspondants sont alors quelques fois si complexes qu'il est malcommode de les désigner conformément à la nomenclature chimique systématique. Des dénominations communes abrégées ont donc été formées ou choisies pour certains d'entre eux et il est suggéré de les employer avec les dénominations communes internationales proposées. Denominaciones para Radicales y Grupos Ciertas sustancias para las cuales hay establecidas una denominación común internacional pueden usarse en forma de sales o de ésteres. Los radicales o grupos correspondientes pueden llegar a tener una composición tan compleja que resulte incómodo referirse a ellos mediante la nomenclatura química sistemática. Las siguientes denominaciones comunes abreviadas han sido ideadas o elegidas para algunos de estos radicales y grupos y se sugiere que se empleen con las denominaciones comunes internacionales propuestas tiglas tiglate (2S)-2-methylbutanoate (ester), (2E)-2-methylbut-2-enoate (ester) tiglate (2S)-2-méthylbutanoate (ester), (2E)-2-méthylbut-2-énoate (ester) tiglato (2S)-2-metilbutanoato (éster), (2E)-2-metilbut-2-enoato (éster) C20H18O4
·
pelidotinum pelidotin (3RS)-1-(6-{[(2S)-1-({[(2S)-5-(carbamoylamino)-1-[4-({[(1-{[(2S)-1-{[(3R,4S,5S)- 3-methoxy-1-{(2S)-2-[(1R,2R)-1-methoxy-2-methyl-3-oxo-3-{[(1S)-2-phenyl-
1-(1,3-thiazol-2-yl)ethyl]amino}propyl]pyrrolidin-1-yl}-5-methyl-1-oxoheptan- 4-yl](methyl)amino}-3-methyl-1-oxobutan-2-yl]amino}-2-methyl-1-oxopropan- 2-yl)carbamoyl]oxy}methyl)anilino]-1-oxopentan-2-yl}amino)-3-methyl-1-oxobutan- 2-yl]amino}-6-oxohexyl)-2,5-dioxopyrrolidin-3-yl
pélidotine (3RS)-1-(6-{[(2S)-1-({[(2S)-5-(carbamoylamino)-1-[4-({[(1-{[(2S)-1-{[(3R,4S,5S)-3- méthoxy-1-{(2S)-2-[(1R,2R)-1-méthoxy-2-méthyl-3-oxo-3-{[(1S)-2-phényl- 1-(1,3-thiazol-2-yl)éthyl]amino}propyl]pyrrolidin-1-yl}-5-méthyl-1-oxoheptan- 4-yl](méthyl)amino}-3-méthyl-1-oxobutan-2-yl]amino}-2-méthyl-1-oxopropan- 2-il)carbamoil]oxi}méthyl)anilino]-1-oxopentan-2-yl}amino)-3-méthyl-1-oxobutan- 2-yl]amino}-6-oxohexyl)-2,5-dioxopyrrolidin-3-yle

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
360
pelidotina (3RS)-1-(6-{[(2S)-1-({[(2S)-5-(carbamoilamino)-1-[4-({[(1-{[(2S)-1-{[(3R,4S,5S)-3- metoxi-1-{(2S)-2-[(1R,2R)-1-metoxi-2-metil-3-oxo-3-{[(1S)-2-fenil- 1-(1,3-tiazol-2-il)etil]amino}propil]pirrolidin-1-il}-5-metil-1-oxoheptan- 4-il](metil)amino}-3-metil-1-oxobutan-2-il]amino}-2-metil-1-oxopropan- 2-il)carbamoil]oxi}metil)anilino]-1-oxopentan-2-il}amino)-3-metil-1-oxobutan- 2-il]amino}-6-oxohexil)-2,5-dioxopirrolidin-3-ile C69H104N12O14S
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
361
AMENDMENTS TO PREVIOUS LISTS MODIFICATIONS APPORTÉES AUX LISTES ANTÉRIEURES
MODIFICACIONES A LAS LISTAS ANTERIORES Proposed International Nonproprietary Names (Prop. INN): List 91 Dénominations communes internationales proposées (DCI Prop.): Liste 91 Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 91 (WHO Drug Information, Vol. 18, No. 2, 2004)
p. 158 alglucosidasum alfa # alglucosidase alfa replace the description and the structure by the following ones,
delete the molecular formula alglucosidase alfa remplacer la description et la structure par les suivantes,
effacer la formule moléculaire brute alglucosidasa alfa sustitúyase la descripción y la estructura por las siguientes,
suprimir la fórmula molecular
human lysosomal prepro-α-glucosidase-(57-952)-peptide 199-arginine-223-histidine-780-isoleucine variant
199-arginine-223-histidine-780-isoleucine variant du (57-952)-peptide de la prépro-α-glucosidase lysosomale humaine
199-arginina-223-histidina-780-isoleucina variante del (57-952)-péptido de la prepro-α-glucosidasa lisosomica humana

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
362
Proposed International Nonproprietary Names (Prop. INN): List 115 Dénominations communes internationales proposées (DCI Prop.): Liste 115 Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 115 (WHO Drug Information, Vol. 30, No. 2, 2016)
p. 251 atuveciclibum atuveciclib replace the chemical name and the structure by the following ones atuvéciclib remplacer le nom chimique et la structure par les suivants atuveciclib sustitúyase el nombre químico y la estructura por los siguientes
(R)-[(3-{[4-(4-fluoro-2-methoxyphenyl)-1,3,5-triazin-
2-yl]amino}phenyl)methyl](imino)(methyl)-λ6-sulfanone
(R)-[(3-{[4-(4-fluoro-2-méthoxyphényl)-1,3,5-triazin- 2-yl]amino}phényl)méthyl](imino)(méthyl)-λ6-sulfanone
(R)-[(3-{[4-(4-fluoro-2-metoxifenil)-1,3,5-triazin- 2-il]amino}fenil)metil](imino)(metil)-λ6-sulfanona
p. 257 cannabidiolum cannabidiol replace the action and use by the following one cannabinoid receptor antagonist
Proposed International Nonproprietary Names (Prop. INN): List 115 Dénominations communes internationales proposées (DCI Prop.): Liste 115 Denominaciones Comunes Internacionales Propuestas (DCI Prop.): Lista 115 (WHO Drug Information, Vol. 30, No. 2, 2016)
p. 617 brivoligidum - 618 brivoligide replace the chemical name by the following one brivoligide remplacer le nom chimique par le suivant brivoligida sustitúyase el nombre químico por el siguiente
2'-deoxycytidylyl-(3'→5')-thymidylyl-(3'→5')-2'-deoxyadenylyl-(3'→5')-
2'-deoxycytidylyl-(3'→5')-2'-deoxyguanylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyadenylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyguanylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyadenylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyguanylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyadenylyl-(3'→5')-thymidylyl-(3'→5')-2'-

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
363
deoxyadenylyl-(3'→5')-2'-deoxycytidine duplex with 2'-deoxyguanylyl-(5'→3')-2'-deoxyadenylyl-(5'→3')-thymidylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-2'-deoxycytidylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-thymidylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-2'-deoxycytidylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-thymidylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-2'-deoxycytidylyl-(5'→3')-2'-deoxyguanylyl-(5'→3')-thymidylyl-(5'→3')-2'-deoxyadenylyl-(5'→3')-thymidylyl-(5'→3')-2'-deoxyguanosine
duplex de 2'-désoxycytidylyl-(3'→5')-thymidylyl-(3'→5')-2'-désoxyadénylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxyguanylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxyadénylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxyguanylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxyadénylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxyguanylyl-(3'→5')-2'-désoxycytidylyl-(3'→5')-2'-désoxyadénylyl-(3'→5')-thymidylyl-(3'→5')-2'-désoxyadénylyl-(3'→5')-2'-désoxycytidine avec 2'-désoxyguanylyl-(5'→3')-2'-désoxyadénylyl-(5'→3')-thymidylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-2'-désoxycytidylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-thymidylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-2'-désoxycytidylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-thymidylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-2'-désoxycytidylyl-(5'→3')-2'-désoxyguanylyl-(5'→3')-thymidylyl-(5'→3')-2'-désoxyadénylyl-(5'→3')-thymidylyl-(5'→3')-2'-désoxyguanosine
dúplex de 2'-desoxicitidilil-(3'→5')-timidilil-(3'→5')-2'-desoxiadenilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiguanilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiadenilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiguanilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicytidilil-(3'→5')-2'-desoxiadenilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiguanilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiadenilil-(3'→5')-timidilil-(3'→5')-2'-desoxiadenilil-(3'→5')-2'-desoxicitidina con 2'-desoxiguanilil-(5'→3')-2'-desoxiadenilil-(5'→3')-timidilil-(5'→3')-2'-desoxiguanilil-(5'→3')-2'-desoxicitidilil-(5'→3')-2'-desoxiguanilil-(5'→3')-2'-desoxiguanilil-(5'→3')-2'-desoxiguanilil-(5'→3')-timidilil-(5'→3')-2'-desoxiguanilil-(5'→3')-2'-desoxiguanilil-(5'→3')-2'-desoxicitidilil-(5'→3')-2'-desoxiguanilil-(5'→3')-2'-desoxiguanilil-(5'→3')-2'-desoxiguanilil-(5'→3')-timidilil-(5'→3')-2'-desoxiguanilil-(5'→3')-2'-desoxicitidilil-(5'→3')-2'-desoxiguanilil-(5'→3')-timidilil-(5'→3')-2'-desoxiadenilil-(5'→3')-timidilil-(5'→3')-2'-desoxiguanosina

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
364
p. 622 dasiglucagonum dasiglucagon replace the molecular formula by the following one dasiglucagon remplacer la formule moléculaire par la suivante dasiglucagón sustitúyase la fórmula molecular por la siguiente
C152H222N38O50
p. 638 gatipotuzumabum # gatipotuzumab replace the structure by the following one gatipotuzumab remplacer la structure par la suivante gatipotuzumab sustitúyase la estructura por la siguiente
Produced in a cell line glycol-engineered from human erythroleukemia (K562) cell line. Glycans are mostly biantennary complex glycans with <30% high mannose and high degree of galactosylation. They have >5% sialylated glycans, >50% fucosylation, >10% bisecting N-acetylglucosamine bearing glycans and no N-glycolylneuraminic acid./ Produit par une lignée cellulaire modifiée au glycol issue des cellules humaines d'érythroleucémie (K562). Les glycanes sont principalement complexes bi-antennaires avec <30% de mannose de haut poinds moléculaire et de haut degré de galactosilation. Ils contiennent >5% de glycanes sialylés, >50% de fucosylation, >10% de glycanes présentant des N-acétylglucosamines bisectionnées et pas d'acide N-glycolylneuraminique./ Producido en la línea celular modificada con glicol derivada de la línea celular humana de eritroleucemia (K562). Los glicanos son principalmente glicanos complejos biantenarios con <30% de manosas de alto peso molecular y alto grado de galactosilación. Contienen >5% de glicanos sialilados, >50% de fucosilación, >10% de glicanos que llevan N-acetilglucosaminas biseccionadas y ningún ácido N-glicolilneuramínico.
Heavy chain / Chaîne lourde / Cadena pesadaEVQLVESGGG LVQPGGSMRL SCVASGFPFS NYWMNWVRQA PGKGLEWVGE 50IRLKSNNYTT HYAESVKGRF TISRDDSKNS LYLQMNSLKT EDTAVYYCTR 100HYYFDYWGQG TLVTVSSAST KGPSVFPLAP SSKSTSGGTA ALGCLVKDYF 150PEPVTVSWNS GALTSGVHTF PAVLQSSGLY SLSSVVTVPS SSLGTQTYIC 200NVNHKPSNTK VDKKVEPKSC DKTHTCPPCP APELLGGPSV FLFPPKPKDT 250LMISRTPEVT CVVVDVSHED PEVKFNWYVD GVEVHNAKTK PREEQYNSTY 300RVVSVLTVLH QDWLNGKEYK CKVSNKALPA PIEKTISKAK GQPREPQVYT 350LPPSRDELTK NQVSLTCLVK GFYPSDIAVE WESNGQPENN YKTTPPVLDS 400DGSFFLYSKL TVDKSRWQQG NVFSCSVMHE GLHNHYTQKS LSLSPGK 447
Light chain / Chaîne légère / Cadena ligeraDIVMTQSPLS NPVTPGEPAS ISCRSSKSLL HSNGITYFFW YLQKPGQSPQ 50LLIYQMSNLA SGVPDRFSGS GSGTDFTLRI SRVEAEDVGV YYCAQNLELP 100PTFGQGTKVE IKRTVAAPSV FIFPPSDEQL KSGTASVVCL LNNFYPREAK 150VQWKVDNALQ SGNSQESVTE QDSKDSTYSL SSTLTLSKAD YEKHKVYACE 200VTHQGLSSPV TKSFNRGEC 219
Post-translational modificationsDisulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-98 144-200 261-321 367-425 22''-98'' 144''-200'' 261''-321'' 367''-425''Intra-L (C23-C104) 23'-93' 139'-199' 23'''-93''' 139'''-199''' Inter-H-L (h 5-CL 126) 220-219' 220''-219''' Inter-H-H (h 11, h 14) 226-226'' 229-229''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH VH 62:57, 57''H CH2 N84.4:297, 297''
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
365
p. 638 gedivumabum # gedivumab replace the structure by the following one gédivumab remplacer la structure par la suivante gedivumab sustitúyase la estructura por la siguiente
p. 650 lesofavumabum # lesofavumab replace the structure by the following one lésofavumab remplacer la structure par la suivante lesofavumab sustitúyase la estructura por la siguiente

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
366
p. 677
timigutuzumabum #
timigutuzumab replace the structure by the following one timigutuzumab remplacer la structure par la suivante timigutuzumab sustitúyase la estructura por la siguiente
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVQPGGSLRL SCAASGFNIK DTYIHWVRQA PGKGLEWVAR 50IYPTNGYTRY ADSVKGRFTI SADTSKNTAY LQMNSLRAED TAVYYCSRWG 100GDGFYAMDYW GQGTLVTVSS ASTKGPSVFP LAPSSKSTSG GTAALGCLVK 150DYFPEPVTVS WNSGALTSGV HTFPAVLQSS GLYSLSSVVT VPSSSLGTQT 200YICNVNHKPS NTKVDKKVEP KSCDKTHTCP PCPAPELLGG PSVFLFPPKP 250KDTLMISRTP EVTCVVVDVS HEDPEVKFNW YVDGVEVHNA KTKPREEQYN 300STYRVVSVLT VLHQDWLNGK EYKCKVSNKA LPAPIEKTIS KAKGQPREPQ 350VYTLPPSRDE LTKNQVSLTC LVKGFYPSDI AVEWESNGQP ENNYKTTPPV 400LDSDGSFFLY SKLTVDKSRW QQGNVFSCSV MHEGLHNHYT QKSLSLSPGK 450
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS LSASVGDRVT ITCRASQDVN TAVAWYQQKP GKAPKLLIYS 50ASFLYSGVPS RFSGSRSGTD FTLTISSLQP EDFATYYCQQ HYTTPPTFGQ 100GTKVEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Post-translational modificationsDisulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-96 147-203 264-324 370-428 22''-96'' 147''-203'' 264''-324'' 370''-428''Intra-L (C23-C104) 23'-88' 134'-194' 23'''-88''' 134'''-194''' Inter-H-L (h 5-CL 126) 223-214' 223''-214''' Inter-H-H (h 11, h 14) 229-229'' 232-232''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:300, 300''
Produced in a cell line glycol-engineered from human erythroleukemia (K562) cell line. Glycans are mostly biantennary complex glycans with <30% high mannose and high degree of galactosylation. They have >5% sialylated glycans, >50% fucosylation, >10% bisecting N-acetylglucosamine bearing glycans and no N-glycolylneuraminic acid./ Produit par une lignée cellulaire modifiée au glycol issue des cellules humaines d'érythroleucémie (K562). Les glycanes sont principalement complexes bi-antennaires avec <30% de mannose de haut poinds moléculaire et de haut degré de galactosilation. Ils contiennent >5% de glycanes sialylés, >50% de fucosylation, >10% de glycanes présentant des N-acétylglucosamines bisectionnées et pas d'acide N-glycolylneuraminique./ Producido en la línea celular modificada con glicol derivada de la línea celular humana de eritroleucemia (K562). Los glicanos son principalmente glicanos complejos biantenarios con <30% de manosas de alto peso molecular y alto grado de galactosilación. Contienen >5% de glicanos sialilados, >50% de fucosilación, >10% de glicanos que llevan N-acetilglucosaminas biseccionadas y ningún ácido N-glicolilneuramínico.
p. 679 tivanisiranum tivanisiran replace the molecular formula by the following one tivanisiran remplacer la formule moléculaire par la suivante tivanisirán sustitúyase la fórmula molecular por la siguiente
C361H447N141O262P36

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
367
p. 680 tomuzotuximabum # tomuzotuximab replace the structure by the following one tomuzotuximab remplacer la structure par la suivante tomuzotuximab sustitúyase la estructura por la siguiente
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVQPGGSLRL SCAASGFNIK DTYIHWVRQA PGKGLEWVAR 50IYPTNGYTRY ADSVKGRFTI SADTSKNTAY LQMNSLRAED TAVYYCSRWG 100GDGFYAMDYW GQGTLVTVSS ASTKGPSVFP LAPSSKSTSG GTAALGCLVK 150DYFPEPVTVS WNSGALTSGV HTFPAVLQSS GLYSLSSVVT VPSSSLGTQT 200YICNVNHKPS NTKVDKKVEP KSCDKTHTCP PCPAPELLGG PSVFLFPPKP 250KDTLMISRTP EVTCVVVDVS HEDPEVKFNW YVDGVEVHNA KTKPREEQYN 300STYRVVSVLT VLHQDWLNGK EYKCKVSNKA LPAPIEKTIS KAKGQPREPQ 350VYTLPPSRDE LTKNQVSLTC LVKGFYPSDI AVEWESNGQP ENNYKTTPPV 400LDSDGSFFLY SKLTVDKSRW QQGNVFSCSV MHEGLHNHYT QKSLSLSPGK 450
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS LSASVGDRVT ITCRASQDVN TAVAWYQQKP GKAPKLLIYS 50ASFLYSGVPS RFSGSRSGTD FTLTISSLQP EDFATYYCQQ HYTTPPTFGQ 100GTKVEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Post-translational modificationsDisulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-96 147-203 264-324 370-428 22''-96'' 147''-203'' 264''-324'' 370''-428''Intra-L (C23-C104) 23'-88' 134'-194' 23'''-88''' 134'''-194''' Inter-H-L (h 5-CL 126) 223-214' 223''-214''' Inter-H-H (h 11, h 14) 229-229'' 232-232''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:300, 300''
Produced in a cell line glycol-engineered from human erythroleukemia (K562) cell line. Glycans are mostly biantennary complex glycans with <30% high mannose and high degree of galactosylation. They have >5% sialylated glycans, >50% fucosylation, >10% bisecting N-acetylglucosamine bearing glycans and no N-glycolylneuraminic acid./ Produit par une lignée cellulaire modifiée au glycol issue des cellules humaines d'érythroleucémie (K562). Les glycanes sont principalement complexes bi-antennaires avec <30% de mannose de haut poinds moléculaire et de haut degré de galactosilation. Ils contiennent >5% de glycanes sialylés, >50% de fucosylation, >10% de glycanes présentant des N-acétylglucosamines bisectionnées et pas d'acide N-glycolylneuraminique./ Producido en la línea celular modificada con glicol derivada de la línea celular humana de eritroleucemia (K562). Los glicanos son principalmente glicanos complejos biantenarios con <30% de manosas de alto peso molecular y alto grado de galactosilación. Contienen >5% de glicanos sialilados, >50% de fucosilación, >10% de glicanos que llevan N-acetilglucosaminas biseccionadas y ningún ácido N-glicolilneuramínico.

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
368
ANNEX 1
PROCEDURE FOR THE SELECTION OF RECOMMENDED INTERNATIONAL NONPROPRIETARY NAMES FOR PHARMACEUTICAL
SUBSTANCES1
The following procedure shall be followed by the World Health Organization (hereinafter also referred to as “WHO”) in the selection of recommended international nonproprietary names for pharmaceutical substances, in accordance with resolution WHA3.11 of the World Health Assembly, and in the substitution of such names. Article 1 - Proposals for recommended international nonproprietary names and proposals for substitution of such names shall be submitted to WHO on the form provided therefore. The consideration of such proposals shall be subject to the payment of an administrative fee designed only to cover the corresponding costs of the Secretariat of WHO (“the Secretariat”). The amount of this fee shall be determined by the Secretariat and may, from time to time, be adjusted. Article 2 - Such proposals shall be submitted by the Secretariat to the members of the Expert Advisory Panel on the International Pharmacopoeia and Pharmaceutical Preparations designated for this purpose, such designated members hereinafter referred to as “the INN Expert Group”, for consideration in accordance with the “General principles for guidance in devising International Nonproprietary Names for Pharmaceutical Substances”, annexed to this procedure2. The name used by the person discovering or first developing and marketing a pharmaceutical substance shall be accepted, unless there are compelling reasons to the contrary. Article 3 - Subsequent to the examination provided for in article 2, the Secretariat shall give notice that a proposed international nonproprietary name is being considered. a) Such notice shall be given by publication in WHO Drug Information3
and by letter to Member States and to national and regional pharmacopoeia commissions or other bodies designated by Member States.
i) Notice shall also be sent to the person who submitted the proposal (“the original applicant”) and other persons known to be concerned with a name under consideration.
b) Such notice shall:
i) set forth the name under consideration; ii) identify the person who submitted the proposal for naming the substance, if so requested by such person; iii) identify the substance for which a name is being considered; iv) set forth the time within which comments and objections will be received and the person and place to whom they should be directed; v) state the authority under which WHO is acting and refer to these rules of procedure.
1 See Annex 1 in WHO Technical Report Series, No. 581, 1975. The original text was adopted by the Executive Board in resolution
EB15.R7 and amended in resolutions EB43.R9 and EB115.R4.
2 See Annex 2.
3 Before 1987, lists of international nonproprietary names were published in the Chronicle of the World Health Organization.

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
369
c) In forwarding the notice, the Secretariat shall request that Member States take such steps as are necessary to prevent the acquisition of proprietary rights in the proposed name during the period it is under consideration by WHO.
Article 4 - Comments on the proposed name may be forwarded by any person to WHO within four months of the date of publication, under article 3, of the name in WHO Drug Information. Article 5 - A formal objection to a proposed name may be filed by any interested person within four months of the date of publication, under article 3, of the name in WHO Drug Information.
Such objection shall:
i) identify the person objecting;
ii) state his or her interest in the name; iii) set forth the reasons for his or her objection to the name proposed. Article 6 - Where there is a formal objection under article 5, WHO may either reconsider the proposed name or use its good offices to attempt to obtain withdrawal of the objection. Without prejudice to the consideration by WHO of a substitute name or names, a name shall not be selected by WHO as a recommended international nonproprietary name while there exists a formal objection thereto filed under article 5 which has not been withdrawn. Article 7 - Where no objection has been filed under article 5, or all objections previously filed have been withdrawn, the Secretariat shall give notice in accordance with subsection (a) of article 3 that the name has been selected by WHO as a recommended international nonproprietary name. Article 8 - In forwarding a recommended international nonproprietary name to Member States under article 7, the Secretariat shall: a) request that it be recognized as the nonproprietary name for the substance; and b) request that Member States take such steps as are necessary to prevent the acquisition of proprietary rights in the name and to prohibit registration of the name as a trademark or trade name. Article 9 a) In the extraordinary circumstance that a previously recommended international nonproprietary name gives rise to errors in medication, prescription or distribution, or a demonstrable risk thereof, because of similarity with another name in pharmaceutical and/or prescription practices, and it appears that such errors or potential errors cannot readily be resolved through other interventions than a possible substitution of a previously recommended international nonproprietary name, or in the event that a previously recommended international nonproprietary name differs substantially from the nonproprietary name approved in a significant number of Member States, or in other such extraordinary circumstances that justify a substitution of a recommended international nonproprietary name, proposals to that effect may be filed by any interested person. Such proposals shall be submitted on the form provided therefore and shall: i) identify the person making the proposal;
ii) state his or her interest in the proposed substitution; and iii) set forth the reasons for the proposal; and
iv) describe, and provide documentary evidence regarding the other interventions undertaken in an effort to resolve the situation, and the reasons why these other interventions were inadequate.

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
370
Such proposals may include a proposal for a new substitute international nonproprietary name, devised in accordance with the General principles, which takes into account the pharmaceutical substance for which the new substitute international nonproprietary name is being proposed. The Secretariat shall forward a copy of the proposal, for consideration in accordance with the procedure described in subsection (b) below, to the INN Expert Group and the original applicant or its successor (if different from the person bringing the proposal for substitution and provided that the original applicant or its successor is known or can be found through diligent effort, including contacts with industry associations). In addition, the Secretariat shall request comments on the proposal from:
i) Member States and national and regional pharmacopoeia commissions or other bodies designated by Member States (by including a notice to that effect in the letter referred to in article 3(a), and
ii) any other persons known to be concerned by the proposed substitution.
The request for comments shall:
i) state the recommended international nonproprietary name that is being proposed for substitution (and the proposed substitute name, if provided);
ii) identify the person who submitted the proposal for substitution (if so requested by such
person);
iii) identify the substance to which the proposed substitution relates and reasons put forward for substitution;
iv) set forth the time within which comments will be received and the person and place to whom they should be directed; and v) state the authority under which WHO is acting and refer to these rules of procedure.
Comments on the proposed substitution may be forwarded by any person to WHO within four months of the date of the request for comments. b) After the time period for comments referred to above has elapsed, the Secretariat shall forward any comments received to the INN Expert Group, the original applicant or its successor and the person bringing the proposal for substitution. If, after consideration of the proposal for substitution and the comments received, the INN Expert Group, the person bringing the proposal for substitution and the original applicant or its successor all agree that there is a need to substitute the previously recommended international nonproprietary name, the Secretariat shall submit the proposal for substitution to the INN Expert Group for further processing. Notwithstanding the foregoing, the original applicant or its successor shall not be entitled to withhold agreement to a proposal for substitution in the event the original applicant or its successor has no demonstrable continuing interest in the recommended international nonproprietary name proposed for substitution.
In the event that a proposal for substitution shall be submitted to the INN Expert Group for further processing, the INN Expert Group will select a new international nonproprietary name in accordance with the General principles referred to in article 2 and the procedure set forth in articles 3 to 8 inclusive. The notices to be given by the Secretariat under article 3 and article 7, respectively, including to the original applicant or its successor (if not the same as the person proposing the substitution, and provided that the original applicant or its successor is known or can be found through diligent effort, including contacts with industry associations), shall in such event indicate that the new name is a substitute for a previously recommended international nonproprietary name and that Member States may

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
371
wish to make transitional arrangements in order to accommodate existing products that use the previously recommended international nonproprietary name on their label in accordance with national legislation.
If, after consideration of the proposal for substitution and the comments received in accordance with the procedure described above, the INN Expert Group, the original applicant or its successor and the person bringing the proposal for substitution do not agree that there are compelling reasons for substitution of a previously recommended international nonproprietary name, this name shall be retained (provided always that the original applicant or its successor shall not be entitled to withhold agreement to a proposal for substitution in the event that the original applicant or its successor has no demonstrable continuing interest in the recommended international nonproprietary name proposed to be substituted). In such an event, the Secretariat shall advise the person having proposed the substitution, as well as the original applicant or its successor (if not the same as the person proposing the substitution, and provided that the original applicant or its successor is known or can be found through diligent effort, including contacts with industry associations), Member States, national and regional pharmacopoeia commissions, other bodies designated by Member States, and any other persons known to be concerned by the proposed substitution that, despite a proposal for substitution, it has been decided to retain the previously recommended international nonproprietary name (with a description of the reason(s) why the proposal for substitution was not considered sufficiently compelling).
ANNEX 2
GENERAL PRINCIPLES FOR GUIDANCE IN DEVISING INTERNATIONAL NONPROPRIETARY NAMES FOR PHARMACEUTICAL SUBSTANCES1
1. International Nonproprietary Names (INN) should be distinctive in sound and spelling. They should not be inconveniently long and should not be liable to confusion with names in common use. 2. The INN for a substance belonging to a group of pharmacologically related substances should, where appropriate, show this relationship. Names that are likely to convey to a patient an anatomical, physiological, pathological or therapeutic suggestion should be avoided. These primary principles are to be implemented by using the following secondary principles: 3. In devising the INN of the first substance in a new pharmacological group, consideration should be given to the possibility of devising suitable INN for related substances, belonging to the new group. 4. In devising INN for acids, one-word names are preferred; their salts should be named without modifying the acid name, e.g. “oxacillin” and “oxacillin sodium”, “ibufenac” and “ibufenac sodium”. 5. INN for substances which are used as salts should in general apply to the active base or the active acid. Names for different salts or esters of the same active substance should differ only in respect of the name of the inactive acid or the inactive base. For quaternary ammonium substances, the cation and anion should be named appropriately as separate components of a quaternary substance and not in the amine-salt style. 6. The use of an isolated letter or number should be avoided; hyphenated construction is also undesirable. 7. To facilitate the translation and pronunciation of INN, “f” should be used instead of “ph”, “t” instead of “th”, “e” instead of “ae” or “oe”, and “i” instead of “y”; the use of the letters “h” and “k” should be avoided. 1
In its Twentieth report (WHO Technical Report Series, No. 581, 1975), the WHO Expert committee on Nonproprietary Names for Pharmaceutical Substances reviewed the general principles for devising, and the procedures for selecting, INN in the light of developments in pharmaceutical compounds in recent years. The most significant change has been the extension to the naming of synthetic chemical substances of the practice previously used for substances originating in or derived from natural products. This practice involves the use of a characteristic “stem” indicative of a common property of the members of a group. The reason for, and the implications of, the change are fully discussed. The guiding principles were updated during the 13th Consultation on nonproprietary names for pharmaceutical substances (Geneva, 27-29 April 1983) (PHARM S/NOM 928 13 May 1983, revised 18 August 1983).

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
372
8. Provided that the names suggested are in accordance with these principles, names proposed by the person discovering or first developing and marketing a pharmaceutical preparation, or names already officially in use in any country, should receive preferential consideration. 9. Group relationship in INN (see General principle 2) should if possible be shown by using a common stem. The following list contains examples of stems for groups of substances, particularly for new groups. There are many other stems in active use.1 Where a stem is shown without any hyphens it may be used anywhere in the name. Latin English -acum -ac anti-inflammatory agents, ibufenac derivatives -adolum -adol } analgesics -adol- -adol-} -astum -ast antiasthmatic, antiallergic substances not acting primarily
as antihistaminics -astinum -astine antihistaminics -azepamum -azepam diazepam derivatives bol bol steroids, anabolic -cain- -cain- class I antiarrhythmics, procainamide and lidocaine
derivatives -cainum -caine local anaesthetics cef- cef- antibiotics, cefalosporanic acid derivatives -cillinum -cillin antibiotics, 6-aminopenicillanic acid derivatives -conazolum -conazole systemic antifungal agents, miconazole derivatives cort cort corticosteroids, except prednisolone derivatives -coxibum -coxib selective cyclo-oxygenase inhibitors -entanum -entan endothelin receptor antagonists gab gab gabamimetic agents gado- gado- diagnostic agents, gadolinium derivatives -gatranum -gatran thrombin inhibitors, antithrombotic agents gest gest steroids, progestogens gli gli antihyperglycaemics io- io- iodine-containing contrast media -metacinum -metacin anti-inflammatory, indometacin derivatives -mycinum -mycin antibiotics, produced by Streptomyces strains -nidazolum -nidazole antiprotozoal substances, metronidazole derivatives -ololum -olol β-adrenoreceptor antagonists -oxacinum -oxacin antibacterial agents, nalidixic acid derivatives -platinum -platin antineoplastic agents, platinum derivatives -poetinum -poetin erythropoietin type blood factors -pril(at)um -pril(at) angiotensin-converting enzyme inhibitors -profenum -profen anti-inflammatory substances, ibuprofen derivatives prost prost prostaglandins -relinum -relin pituitary hormone release-stimulating peptides -sartanum -sartan angiotensin II receptor antagonists, antihypertensive (non-
peptidic) -vaptanum -vaptan vasopressin receptor antagonists vin- vin- } vinca-type alkaloids -vin- -vin-} 1 A more extensive listing of stems is contained in the working document WHO/EMP/RHT/TSN/2013.1 which is regularly updated and can be requested from the INN Programme, WHO, Geneva.
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
373
ANNEXE 1
PROCEDURE A SUIVRE EN VUE DU CHOIX DE DENOMINATIONS COMMUNES INTERNATIONALES RECOMMANDEES POUR LES
SUBSTANCES PHARMACEUTIQUES1
L’Organisation mondiale de la Santé (également désignée ci-après sous l’appellation « OMS ») observe la procédure exposée ci-dessous pour l’attribution de dénominations communes internationales recommandées pour les substances pharmaceutiques, conformément à la résolution WHA3.11 de l’Assemblée mondiale de la Santé, et pour le remplacement de telles dénominations. Article 1 - Les propositions de dénominations communes internationales recommandées et les propositions de remplacement de telles dénominations sont soumises à l’OMS sur la formule prévue à cet effet. L’examen de telles propositions est soumis au paiement d’une taxe administrative destinée uniquement à couvrir les coûts correspondants assumés par le Secrétariat de l’OMS (« le Secrétariat »). Le montant de cette taxe est déterminé par le Secrétariat et peut être modifié de temps à autre. Article 2 - Ces propositions sont soumises par le Secrétariat aux experts désignés à cette fin parmi les personnalités inscrites au Tableau d’experts de la Pharmacopée internationale et des Préparations pharmaceutiques, ci-après désignés sous l’appellation « le Groupe d’experts des DCI » ; elles sont examinées par les experts conformément aux « Directives générales pour la formation de dénominations communes internationales pour les substances pharmaceutiques » reproduites ci-après2.
La dénomination acceptée est la dénomination employée par la personne qui découvre ou qui, la première, fabrique et lance sur le marché une substance pharmaceutique, à moins que des raisons majeures n’obligent à s’écarter de cette règle. Article 3 - Après l’examen prévu à l’article 2, le Secrétariat notifie qu’un projet de dénomination commune internationale est à l’étude. a) Cette notification est faite par une insertion dans WHO Drug Information3 et par l’envoi d’une lettre aux Etats Membres et aux commissions nationales et régionales de pharmacopée ou autres organismes désignés par les Etats Membres.
i) Notification est également faite à la personne qui a soumis la proposition (« le demandeur initial ») et à d’autres personnes portant à la dénomination mise à l’étude un intérêt notoire.
b) Cette notification contient les indications suivantes :
i) dénomination mise à l’étude;
ii) nom de l’auteur de la proposition tendant à attribuer une dénomination à la substance, si cette personne le demande ;
iii) définition de la substance dont la dénomination est mise à l’étude ;
iv) délai pendant lequel seront reçues les observations et les objections à l’égard de cette dénomination ; nom et adresse de la personne habilitée à recevoir ces observations et objections ;
v) mention des pouvoirs en vertu desquels agit l’OMS et référence au présent règlement.
1 Voir annexe 1 dans OMS, Série de Rapports techniques, N° 581, 1975. Le texte original a été adopté par le Conseil exécutif dans sa résolution EB15.R7 et amendé dans ses résolutions EB43.R9 et EB115.R4.
2 Voir annexe 2. 3
Avant 1987, les listes de dénominations communes internationales étaient publiées dans la Chronique de l’Organisation mondiale de la Santé.

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
374
c) En envoyant cette notification, le Secrétariat demande aux Etats Membres de prendre les mesures nécessaires pour prévenir l’acquisition de droits de propriété sur la dénomination proposée pendant la période au cours de laquelle cette dénomination est mise à l’étude par l’OMS. Article 4 - Des observations sur la dénomination proposée peuvent être adressées à l’OMS par toute personne, dans les quatre mois qui suivent la date de publication de la dénomination dans WHO Drug Information (voir l’article 3). Article 5 - Toute personne intéressée peut formuler une objection formelle contre la dénomination proposée dans les quatre mois qui suivent la date de publication de la dénomination dans WHO Drug Information (voir l’article 3). Cette objection doit s’accompagner des indications suivantes :
i) nom de l’auteur de l’objection ; ii) intérêt qu’il ou elle porte à la dénomination en cause ; iii) raisons motivant l’objection contre la dénomination proposée. Article 6 - Lorsqu’une objection formelle est formulée en vertu de l’article 5, l’OMS peut soit soumettre la dénomination proposée à un nouvel examen, soit intervenir pour tenter d’obtenir le retrait de l’objection. Sans préjudice de l’examen par l’OMS d’une ou de plusieurs appellations de remplacement, l’OMS n’adopte pas d’appellation comme dénomination commune internationale recommandée tant qu’une objection formelle présentée conformément à l’article 5 n’est pas levée. Article 7 - Lorsqu’il n’est formulé aucune objection en vertu de l’article 5, ou que toutes les objections présentées ont été levées, le Secrétariat fait une notification conformément aux dispositions du paragraphe a) de l’article 3, en indiquant que la dénomination a été choisie par l’OMS en tant que dénomination commune internationale recommandée. Article 8 - En communiquant aux Etats Membres, conformément à l’article 7, une dénomination commune internationale recommandée, le Secrétariat : a) demande que cette dénomination soit reconnue comme dénomination commune de la substance considérée ; et b) demande aux Etats Membres de prendre les mesures nécessaires pour prévenir l’acquisition de droits de propriété sur cette dénomination et interdire le dépôt de cette dénomination comme marque ou appellation commerciale. Article 9 - a) Dans le cas exceptionnel où une dénomination commune internationale déjà recommandée donne lieu à des erreurs de médication, de prescription ou de distribution ou en comporte un risque démontrable, en raison d’une similitude avec une autre appellation dans la pratique pharmaceutique et/ou de prescription, et où il apparaît que ces erreurs ou ces risques d’erreur ne peuvent être facilement évités par d’autres interventions que le remplacement éventuel d’une dénomination commune internationale déjà recommandée, ou dans le cas où une dénomination commune internationale déjà recommandée diffère sensiblement de la dénomination commune approuvée dans un nombre important d’Etats Membres, ou dans d’autres circonstances exceptionnelles qui justifient le remplacement d’une dénomination commune internationale recommandée, toute personne intéressée peut formuler une proposition dans ce sens. Cette proposition est présentée sur la formule prévue à cet effet et doit s’accompagner des indications suivantes :
i) nom de l’auteur de la proposition ;
ii) intérêt qu’il ou elle porte au remplacement proposé ;
iii) raisons motivant la proposition ; et

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
375
iv) description, faits à l’appui, des autres interventions entreprises pour tenter de régler le problème et exposé des raisons pour lesquelles ces interventions ont échoué.
Les propositions peuvent comprendre une proposition de nouvelle dénomination commune internationale de remplacement, établie conformément aux Directives générales, compte tenu de la substance pharmaceutique pour laquelle la nouvelle dénomination commune internationale de remplacement est proposée. Le Secrétariat transmet une copie de la proposition pour examen, conformément à la procédure exposée plus loin au paragraphe b), au Groupe d’experts des DCI et au demandeur initial ou à son successeur (s’il s’agit d’une personne différente de celle qui a formulé la proposition de remplacement et pour autant que le demandeur initial ou son successeur soit connu ou puisse être retrouvé moyennant des efforts diligents, notamment des contacts avec les associations industrielles). De plus, le Secrétariat demande aux entités et personnes ci-après de formuler des observations sur la proposition :
i) les Etats Membres et les commissions nationales et régionales de pharmacopée ou d’autres organismes désignés par les Etats Membres (en insérant une note à cet effet dans la lettre mentionnée à l’article 3.a), et
ii) toutes autres personnes portant au remplacement proposé un intérêt notoire. La demande d’observations contient les indications suivantes :
i) dénomination commune internationale recommandée pour laquelle un remplacement est proposé (et la dénomination de remplacement proposée, si elle est fournie) ;
ii) nom de l’auteur de la proposition de remplacement (si cette personne le demande) ;
iii) définition de la substance faisant l’objet du remplacement proposé et raisons avancées pour le remplacement ;
iv) délai pendant lequel seront reçus les commentaires et nom et adresse de la personne habilitée à recevoir ces commentaires ; et
v) mention des pouvoirs en vertu desquels agit l’OMS et référence au présent règlement. Des observations sur la proposition de remplacement peuvent être communiquées par toute personne à l’OMS dans les quatre mois qui suivent la date de la demande d’observations. b) Une fois échu le délai prévu ci-dessus pour la communication d’observations, le Secrétariat transmet les observations reçues au Groupe d’experts des DCI, au demandeur initial ou à son successeur et à l’auteur de la proposition de remplacement. Si, après avoir examiné la proposition de remplacement et les observations reçues, le Groupe d’experts des DCI, l’auteur de la proposition de remplacement et le demandeur initial ou son successeur reconnaissent tous qu’il est nécessaire de remplacer la dénomination commune internationale déjà recommandée, le Secrétariat soumet la proposition de remplacement au Groupe d’experts des DCI pour qu’il y donne suite.
Nonobstant ce qui précède, le demandeur initial ou son successeur n’est pas habilité à refuser son accord à une proposition de remplacement au cas où il ne peut être démontré qu’il porte un intérêt durable à la dénomination commune internationale recommandée qu’il est proposé de remplacer.
Dans le cas où une proposition de remplacement est soumise au Groupe d’experts des DCI pour
qu’il y donne suite, le Groupe choisit une nouvelle dénomination commune internationale conformément aux Directives générales mentionnées à l’article 2 et selon la procédure décrite dans les articles 3 à 8 inclus. La notification faite par le Secrétariat en vertu de l’article 3 et de l’article 7, respectivement, y compris au demandeur initial ou à son successeur (si ce n’est pas la même personne que celle qui a proposé le remplacement et pour autant que le demandeur initial ou son successeur soit connu ou puisse
Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
376
être retrouvé moyennant des efforts diligents, notamment des contacts avec les associations industrielles), doit dans un tel cas indiquer que la nouvelle dénomination remplace une dénomination commune internationale déjà recommandée et que les Etats Membres peuvent souhaiter prendre des mesures transitoires pour les produits existants qui utilisent la dénomination commune internationale déjà recommandée sur leur étiquette conformément à la législation nationale.
Si, après examen de la proposition de remplacement et des observations communiquées
conformément à la procédure exposée plus haut, le Groupe d’experts des DCI, le demandeur initial ou son successeur et l’auteur de la proposition de remplacement ne s’accordent pas sur le fait qu’il y a des raisons impératives de remplacer une dénomination commune internationale déjà recommandée, cette dernière est conservée (étant entendu toujours que le demandeur initial ou son successeur n’est pas habilité à refuser son accord à une proposition de remplacement au cas où il ne peut être démontré qu’il porte un intérêt durable à la dénomination commune internationale recommandée qu’il est proposé de remplacer). Dans un tel cas, le Secrétariat informe l’auteur de la proposition de remplacement, ainsi que le demandeur initial ou son successeur (s’il s’agit d’une personne différente de celle qui a formulé la proposition de remplacement et pour autant que le demandeur initial ou son successeur soit connu ou puisse être retrouvé moyennant des efforts diligents, notamment des contacts avec les associations industrielles), les Etats Membres, les commissions nationales et régionales de pharmacopée, les autres organismes désignés par les Etats Membres et toutes autres personnes portant un intérêt notoire au remplacement proposé que, malgré une proposition de remplacement, il a été décidé de conserver la dénomination commune internationale déjà recommandée (avec une brève description de la ou des raisons pour lesquelles la proposition de remplacement n’a pas été jugée suffisamment impérative).
ANNEXE 2
DIRECTIVES GENERALES POUR LA FORMATION DE DENOMINATIONS COMMUNES INTERNATIONALES APPLICABLES AUX SUBSTANCES
PHARMACEUTIQUES1 1. Les dénominations communes internationales (DCI) devront se distinguer les unes des autres par leur consonance et leur orthographe. Elles ne devront pas être d’une longueur excessive, ni prêter à confusion avec des appellations déjà couramment employées. 2. La DCI de chaque substance devra, si possible, indiquer sa parenté pharmacologique. Les dénominations susceptibles d’évoquer pour les malades des considérations anatomiques, physiologiques, pathologiques ou thérapeutiques devront être évitées dans la mesure du possible. Outre ces deux principes fondamentaux, on respectera les principes secondaires suivants : 3. Lorsqu’on formera la DCI de la première substance d’un nouveau groupe pharmacologique, on tiendra compte de la possibilité de former ultérieurement d’autres DCI appropriées pour les substances apparentées du même groupe. 4. Pour former des DCI des acides, on utilisera de préférence un seul mot. Leurs sels devront être désignés par un terme qui ne modifie pas le nom de l’acide d’origine : par exemple «oxacilline» et «oxacilline sodique», «ibufénac» et «ibufénac sodique». 5. Les DCI pour les substances utilisées sous forme de sels devront en général s’appliquer à la base active (ou à l’acide actif). Les dénominations pour différents sels ou esters d’une même substance active ne différeront que par le nom de l’acide inactif (ou de la base inactive). 1
Dans son vingtième rapport (OMS, Série de Rapports techniques, N° 581, 1975), le Comité OMS d’experts des Dénominations communes pour les Substances pharmaceutiques a examiné les directives générales pour la formation des dénominations communes internationales et la procédure à suivre en vue de leur choix, compte tenu de l’évolution du secteur pharmaceutique au cours des dernières années. La modification la plus importante a été l’extension aux substances de synthèse de la pratique normalement suivie pour désigner les substances tirées ou dérivées de produits naturels. Cette pratique consiste à employer des syllabes communes ou groupes de syllabes communes (segments-clés) qui sont caractéristiques et indiquent une propriété commune aux membres du groupe des substances pour lequel ces segments-clés ont été retenus. Les raisons et les conséquences de cette modification ont fait l’objet de discussions approfondies. Les directives ont été mises à jour lors de la treizième consultation sur les dénominations communes pour les substances pharmaceutiques (Genève, 27-29 avril 1983) (PHARM S/NOM 928, 13 mai 1983, révision en date du 18 août 1983).

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
377
En ce qui concerne les substances à base d’ammonium quaternaire, la dénomination s’appliquera de façon appropriée au cation et à l’anion en tant qu’éléments distincts d’une substance quaternaire. On évitera de choisir une désignation évoquant un sel aminé.
6. On évitera d’ajouter une lettre ou un chiffre isolé ; en outre, on renoncera de préférence au trait d’union.
7. Pour simplifier la traduction et la prononciation des DCI, la lettre « f » sera utilisée à la place de « ph », « t » à la place de « th », « e » à la place de « ae » ou « oe », et « i » à la place de « y » ; l’usage des lettres « h » et « k » sera aussi évité.
8. On retiendra de préférence, pour autant qu’elles respectent les principes énoncés ici, les dénominations proposées par les personnes qui ont découvert ou qui, les premières, ont fabriqué et lancé sur le marché les préparations pharmaceutiques considérées, ou les dénominations déjà officiellement adoptées par un pays.
9. La parenté entre substances d’un même groupe (voir Directive générale 2) sera si possible indiquée dans les DCI par l’emploi de segments-clés communs. La liste ci-après contient des exemples de segments-clés pour des groupes de substances, surtout pour des groupes récents. Il y a beaucoup d’autres segments-clés en utilisation active. 1 Les segments-clés indiqués sans trait d’union pourront être insérés n’importe où dans une dénomination.
Latin Français
-acum -ac substances anti-inflammatoires du groupe de l’ibufénac -adolum -adol } analgésiques -adol- -adol- }
-astum -ast antiasthmatiques, antiallergiques n’agissant pas principalement en tant qu’antihistaminiques -astinum -astine antihistaminiques -azepamum -azépam substances du groupe du diazépam bol bol stéroïdes anabolisants -cain- -caïn- antiarythmiques de classe I, dérivés du procaïnamide et de la lidocaïne -cainum -caïne anesthésiques locaux cef- céf- antibiotiques, dérivés de l’acide céphalosporanique -cillinum -cilline antibiotiques, dérivés de l’acide 6-aminopénicillanique -conazolum -conazole agents antifongiques systémiques du groupe du miconazole cort cort corticostéroïdes, autres que les dérivés de la prednisolone -coxibum -coxib inhibiteurs sélectifs de la cyclo-oxygénase -entanum -entan antagonistes du récepteur de l’endothéline gab gab gabamimétiques gado- gado- agents diagnostiques, dérivés du gadolinium -gatranum -gatran antithrombines, antithrombotiques gest gest stéroïdes progestogènes gli gli antihyperglycémiants io- io- produits de contraste iodés -metacinum -métacine substances anti-inflammatoires du groupe de l’indométacine -mycinum -mycine antibiotiques produits par des souches de Streptomyces -nidazolum -nidazole substances antiprotozoaires du groupe du métronidazole -ololum -olol antagonistes des récepteurs β-adrénergiques -oxacinum -oxacine substances antibactériennes du groupe de l’acide nalidixique -platinum -platine antinéoplasiques, dérivés du platine -poetinum -poétine facteurs sanguins de type érythropoïétine -pril(at)um -pril(ate) inhibiteurs de l’enzyme de conversion de l’angiotensine -profenum -profène substances anti-inflammatoires du groupe de l’ibuprofène prost prost prostaglandines
1 Une liste plus complète de segments-clés est contenue dans le document de travail WHO/EMP/RHT/TSN/2013.1 qui est régulièrement mis
à jour et qui peut être demandé auprès du programme des DCI, OMS, Genève.

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
378
-relinum -réline peptides stimulant la libération d’hormones hypophysaires -sartanum -sartan antagonistes d’un récepteur de l’angiotensine II, antihypertenseurs (non peptidiques) -vaptanum -vaptan antagonistes du récepteur de la vasopressine vin- vin- } alcaloïdes du type vinca -vin- -vin- }
ANEXO 1
PROCEDIMIENTO DE SELECCIÓN DE DENOMINACIONES COMUNES INTERNACIONALES RECOMENDADAS PARA SUSTANCIAS FARMACÉUTICAS1
La Organización Mundial de la Salud (OMS) seguirá el procedimiento que se expone a continuación tanto para seleccionar denominaciones comunes internacionales recomendadas para las sustancias farmacéuticas, de conformidad con lo dispuesto en la resolución WHA3.11, como para sustituir esas denominaciones. Artículo 1 - Las propuestas de denominaciones comunes internacionales recomendadas y las propuestas de sustitución de esas denominaciones se presentarán a la OMS en los formularios que se proporcionen a estos efectos. El estudio de estas propuestas estará sujeto al pago de una tasa destinada a sufragar los costos de administración que ello suponga para la Secretaría de la OMS («la Secretaría»). La Secretaría establecerá la cuantía de esa tasa y podrá ajustarla periódicamente. Artículo 2 - Estas propuestas serán sometidas por la Secretaría a los miembros del Cuadro de Expertos en Farmacopea Internacional y Preparaciones Farmacéuticas encargados de su estudio, en adelante de-signados como «el Grupo de Expertos en DCI», para que las examinen de conformidad con los «Principios generales de orientación para formar denominaciones comunes internacionales para sus-tancias farmacéuticas», anexos a este procedimiento.2 A menos que haya poderosas razones en contra, la denominación aceptada será la empleada por la persona que haya descubierto o fabricado y comer-cializado por primera vez esa sustancia farmacéutica. Artículo 3 - Tras el examen al que se refiere el artículo 2, la Secretaría notificará que está en estudio un proyecto de denominación internacional. a) Esa notificación se hará mediante una publicación en Información Farmacéutica OMS3
y el envío de una carta a los Estados Miembros y a las comisiones nacionales y regionales de las farmacopeas u otros organismos designados por los Estados Miembros.
i) La notificación será enviada también a la persona que haya presentado la propuesta («el solicitante inicial») y a otras personas que tengan un interés especial en una denominación objeto de estudio.
b) En esa notificación se incluirán los siguientes datos: i) la denominación sometida a estudio; ii) la identidad de la persona que ha presentado la propuesta de denominación de la sustancia, si lo pide esa persona; iii) la identidad de la sustancia cuya denominación está en estudio;
1 Véase el anexo 1 en OMS, Serie de Informes Técnicos, Nº 581, 1975. El texto vigente fue adoptado por el Consejo Ejecutivo en su resolución EB15.R7 y modificado en las resoluciónes EB43.R9 y EB115.R4..
2 Véase el anexo 2.
3 Hasta 1987 las listas de DCI se publicaban en la Crónica de la Organización Mundial de la Salud.
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
379
iv) el plazo fijado para recibir observaciones y objeciones, así como el nombre y la dirección de la persona a quien deban dirigirse; y v) los poderes conferidos para el caso a la OMS y una referencia al presente procedimiento.
c) Al enviar esa notificación, la Secretaría solicitará de los Estados Miembros la adopción de todas las medidas necesarias para impedir la adquisición de derechos de patente sobre la denominación propuesta, durante el periodo en que la OMS la tenga en estudio. Artículo 4 - Toda persona puede formular a la OMS observaciones sobre la denominación propuesta dentro de los cuatro meses siguientes a su publicación en Información Farmacéutica OMS, conforme a lo dispuesto en el artículo 3. Artículo 5 - Toda persona interesada puede presentar una objeción formal a una denominación propuesta dentro de los cuatro meses siguientes a su publicación en Información Farmacéutica OMS, conforme a lo dispuesto en el artículo 3. Esa objeción deberá acompañarse de los siguientes datos:
i) la identidad de la persona que formula la objeción; ii) las causas que motivan su interés por la denominación; y iii) las causas que motivan su objeción a la denominación propuesta.
Artículo 6 - Cuando se haya presentado una objeción formal en la forma prevista en el artículo 5, la OMS podrá reconsiderar el nombre propuesto o utilizar sus buenos oficios para intentar lograr que se retire la objeción. La OMS no seleccionará como denominación común internacional una denominación a la que se haya hecho una objeción formal, presentada según lo previsto en el artículo 5, que no haya sido retirada, todo ello sin perjuicio de que la Organización examine otra denominación o denominaciones sustitutivas. Artículo 7 - Cuando no se haya formulado ninguna objeción en la forma prevista en el artículo 5, o cuando todas las objeciones presentadas hayan sido retiradas, la Secretaría notificará, conforme a lo dispuesto en el párrafo a) del artículo 3, que la denominación ha sido seleccionada por la OMS como denominación común internacional recomendada. Artículo 8 - Al comunicar a los Estados Miembros una denominación común internacional, conforme a lo previsto en el artículo 7, la Secretaría: a) solicitará que esta denominación sea reconocida como denominación común para la sustancia de que se trate; y b) solicitará a los Estados Miembros que adopten todas las medidas necesarias para impedir la adquisición de derechos de patente sobre la denominación, y prohíban que sea registrada como marca de fábrica o como nombre comercial. Artículo 9 a) En el caso excepcional de que, debido a su semejanza con otra denominación utilizada en las prácticas farmacéuticas y/o de prescripción, una denominación común internacional recomendada anteriormente ocasione errores de medicación, prescripción o distribución, o suponga un riesgo manifiesto de que esto ocurra, y parezca que tales errores o potenciales errores no sean fácilmente subsanables con otras medidas que no sean la posible sustitución de esa denominación común internacional recomendada anteriormente; en el caso de que una denominación común internacional recomendada anteriormente difiera considerablemente de la denominación común aprobada en un número importante de Estados Miembros, o en otras circunstancias excepcionales que justifiquen el cambio de una denominación común internacional recomendada, cualquier persona interesada puede presentar propuestas en este sentido. Esas propuestas se presentarán en los formularios que se proporcionen a estos efectos e incluirán los siguientes datos:

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
380
i) la identidad de la persona que presenta la propuesta; ii) las causas que motivan su interés en la sustitución propuesta;
iii) las causas que motivan la propuesta; y
iv) una descripción, acompañada de pruebas documentales, de las otras medidas que se hayan adoptado con el fin de resolver la situación y de los motivos por los cuales dichas medidas no han sido suficientes.
Entre esas propuestas podrá figurar una relativa a una nueva denominación común
internacional sustitutiva, formulada con arreglo a los Principios generales y que tenga en cuenta la sustancia farmacéutica para la que se proponga la nueva denominación común internacional sustitutiva.
La Secretaría enviará al Grupo de Expertos en DCI y al solicitante inicial o a su sucesor (en el caso de que sea una persona diferente de la que ha presentado la propuesta de sustitución y siempre que el solicitante inicial o su sucesor sean conocidos o puedan ser encontrados mediante esfuerzos diligentes, como el contacto con las asociaciones industriales) una copia de la propuesta, para que sea examinada de conformidad con el procedimiento descrito en el párrafo b) infra. Además, la Secretaría solicitará observaciones sobre la propuesta:
i) a los Estados Miembros y a las comisiones nacionales y regionales de las farmacopeas u otros organismos designados por los Estados Miembros (ello se hará incluyendo una notificación a tal efecto en la carta a la que se refiere el párrafo a) del artículo 3), y
ii) a cualquier persona que tenga un interés especial en la sustitución propuesta.
Al solicitar que se formulen estas observaciones se facilitarán los siguientes datos: i) la denominación común internacional recomendada que se propone sustituir (y la denominación sustitutiva propuesta, si se ha facilitado);
ii) la identidad de la persona que ha presentado la propuesta de sustitución (si lo pide esa persona); iii) la identidad de la sustancia a la que se refiere la sustitución propuesta y las razones para presentar la propuesta de sustitución; iv) el plazo fijado para recibir observaciones, así como el nombre y la dirección de la persona a quien deban dirigirse; y
v) los poderes conferidos para el caso a la OMS y una referencia al presente procedimiento.
Toda persona puede formular a la OMS observaciones sobre la sustitución propuesta dentro de los cuatro meses siguientes a la fecha en que se realizó la solicitud de observaciones. b) Una vez agotado el mencionado plazo para la formulación de observaciones, la Secretaría enviará todos los comentarios recibidos al Grupo de Expertos en DCI, al solicitante inicial o a su sucesor, y a la persona que haya presentado la propuesta de sustitución. Si después de examinar la propuesta de sustitución y las observaciones recibidas, el Grupo de Expertos en DCI, la persona que haya presentado la propuesta de sustitución y el solicitante inicial, o su sucesor, están de acuerdo en la necesidad de sustituir la denominación común internacional recomendada anteriormente, la Secretaría remitirá la propuesta de sustitución al Grupo de Expertos en DCI para que la tramite. No obstante lo anterior, el solicitante inicial o su sucesor no tendrán derecho a impedir el acuerdo sobre una propuesta de sustitución en el caso de que hayan dejado de tener un interés demostrable en la denominación común internacional cuya sustitución se propone.

WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
381
En caso de que la propuesta de sustitución sea presentada al Grupo de Expertos en DCI para que la tramite, este grupo seleccionará una nueva denominación común internacional de conformidad con los Principios generales a los que se refiere el artículo 2 y al procedimiento establecido en los artículos 3 a 8 inclusive. En ese caso, en las notificaciones que la Secretaría ha de enviar con arreglo a los artículos 3 y 7, respectivamente, incluida la notificación al solicitante inicial o a su sucesor (en el caso de que no sea la misma persona que propuso la sustitución y siempre que el solicitante inicial o su sucesor sean conocidos o puedan ser encontrados mediante esfuerzos diligentes, como el contacto con las asociaciones industriales), se indicará que la nueva denominación sustituye a una denominación común internacional recomendada anteriormente y que los Estados Miembros podrán, si lo estiman oportuno, adoptar disposiciones transitorias aplicables a los productos existentes en cuya etiqueta se utilice, con arreglo a la legislación nacional, la denominación común internacional recomendada anteriormente que se haya sustituido.
En caso de que, después de haber estudiado la propuesta de sustitución y los comentarios recibidos de conformidad con el procedimiento descrito anteriormente, el Grupo de Expertos en DCI, el solicitante inicial o su sucesor y la persona que haya presentado la propuesta de sustitución no lleguen a un acuerdo sobre la existencia de razones poderosas para sustituir una denominación común internacional recomendada anteriormente, esta denominación se mantendrá (siempre en el entendimiento de que el solicitante inicial o su sucesor no tendrán derecho a impedir el acuerdo sobre una propuesta de sustitución en el caso de que hayan dejado de tener un interés demostrable en la denominación común internacional cuya sustitución se propone). En ese caso, la Secretaría comunicará a la persona que haya propuesto la sustitución, así como al solicitante inicial o a su sucesor (en el caso de que no sea la misma persona que propuso la sustitución y siempre que el solicitante inicial o su sucesor sean conocidos o puedan ser encontrados mediante esfuerzos diligentes, como el contacto con las asociaciones industriales), a los Estados Miembros, a las comisiones nacionales y regionales de las farmacopeas o a otros organismos designados por los Estados Miembros y a cualquier otra persona que tenga interés en la sustitución propuesta, que, pese a la presentación de una propuesta de sustitución, se ha decidido mantener la denominación común internacional recomendada anteriormente (con una descripción de la o las razones por las que se ha considerado que la propuesta de sustitución no estaba respaldada por razones suficientemente poderosas).
ANEXO 2
PRINCIPIOS GENERALES DE ORIENTACIÓN PARA FORMAR DENOMINACIONES COMUNES INTERNACIONALES PARA SUSTANCIAS FARMACÉUTICAS1
1. Las denominaciones comunes internacionales (DCI) deberán diferenciarse tanto fonética como ortográficamente. No deberán ser incómodamente largas, ni dar lugar a confusión con denominaciones de uso común.
2. La DCI de una sustancia que pertenezca a un grupo de sustancias farmacológicamente emparentadas deberá mostrar apropiadamente este parentesco. Deberán evitarse las denominaciones que puedan tener connotaciones anatómicas, fisiológicas, patológicas o terapéuticas para el paciente.
Estos principios primarios se pondrán en práctica utilizando los siguientes principios secundarios:
3. Al idear la DCI de la primera sustancia de un nuevo grupo farmacológico, deberá tenerse en cuenta la posibilidad de poder formar DCI convenientes para las sustancias emparentadas que se agreguen al nuevo grupo.
4. Al idear DCI para ácidos, se preferirán las de una sola palabra; sus sales deberán denominarse sin modificar el nombre del ácido: p. ej. «oxacilina» y «oxacilina sódica», «ibufenaco» y «ibufenaco sódico». 1 En su 20º informe (OMS, Serie de Informes Técnicos, Nº 581, 1975), el Comité de Expertos de la OMS en Denominaciones Comunes para las Sustancias Farmacéuticas revisó los Principios generales para formar denominaciones comunes internacionales (DCI), y su procedimiento de selección, a la luz de las novedades registradas en los últimos años en materia de compuestos farmacéuticos. El cambio más importante había consistido en hacer extensivo a la denominación de sustancias químicas sintéticas el método utilizado hasta entonces para las sustancias originadas en productos naturales o derivadas de éstos. Dicho método conlleva la utilización de una «partícula» característica que indica una propiedad común a los miembros de un grupo. En el citado informe se examinan en detalle las razones y consecuencias de este cambio. Los Principios generales de orientación se actualizaron durante la 13ª consulta sobre denominaciones comunes para sustancias farmacéuticas (Ginebra, 27 a 29 de abril de 1983) (PHARM S/NOM 928, 13 de mayo de 1983, revisado el 18 de agosto de 1983).

Proposed INN: List 117 WHO Drug Information, Vol. 31, No. 2, 2017
382
5. Las DCI para las sustancias que se usan en forma de sal deberán en general aplicarse a la base activa o al ácido activo. Las denominaciones para diferentes sales o esteres de la misma sustancia activa solamente deberán diferir en el nombre del ácido o de la base inactivos. En los compuestos de amonio cuaternario, el catión y el anión deberán denominarse adecuadamente por separado, como componentes independientes de una sustancia cuaternaria y no como sales de una amina.
6. Deberá evitarse el empleo de letras o números aislados; también es indeseable el empleo de guiones. 7. Para facilitar la traducción y la pronunciación, se emplearán de preferencia las letras «f» en lugar de «ph», «t» en lugar de «th», «e» en lugar de «ae» u «oe», e «i» en lugar de «y»; se deberá evitar el empleo de las letras «h» y «k». 8. Siempre que las denominaciones propuestas estén de acuerdo con estos principios, recibirán una consideración preferente las denominaciones propuestas por la persona que haya descubierto las sus-tancias, o que fabrique y comercialice por primera vez una sustancia farmacéutica, así como las deno-minaciones ya adoptadas oficialmente en cualquier país. 9. El parentesco entre sustancias del mismo grupo se pondrá de manifiesto en las DCI (véase el Principio 2) utilizando una partícula común. En la lista que figura a continuación se indican ejemplos de partículas para grupos de sustancias, en particular para grupos nuevos. Existen muchas otras partículas que se usan habitualmente.1 Cuando una partícula aparece sin guión alguno, puede utilizarse en cualquier lugar de la palabra. Latin Español -acum -aco antiinflamatorios derivados del ibufenaco -adolum -adol ) analgésicos -adol- -adol- ) -astum -ast antiasmáticos, sustancias antialérgicas cuya acción principal no es la antihistamínica -astinum -astina antihistamínicos -azepamum -azepam derivados del diazepam bol bol esteroides anabolizantes -cain- -caína- antiarrítmicos de clase I, derivados de procainamida y lidocaína -cainum -caína- anestésicos locales cef- cef- antibióticos, derivados del ácido cefalosporánico -cillinum - cilina antibióticos derivados del ácido 6-aminopenicilánico -conazolum -conazol antifúngicos sistémicos derivados del miconazol cort cort corticosteroides, excepto derivados de prednisolona -coxibum -coxib inhibidores selectivos de ciclooxigenasa -entanum -entán antagonistas del receptor de endotelina gab gab gabamiméticos gado- gado- agentes para diagnóstico derivados de gadolinio -gartranum -gatrán inhibidores de la trombina antitrombóticos gest gest esteroides progestágenos gli gli hipoglucemiantes, antihiperglucémicos io- io- medios de contraste iodados -metacinum -metacina antiinflamatorios derivados de indometacina -mycinum -micina antibióticos producidos por cepas de Streptomyces -nidazolum -nidazol antiprotozoarios derivados de metronidazol -ololum -olol antagonistas de receptores -adrenérgicos -oxacinum -oxacino antibacterianos derivados del ácido nalidíxico -platinum -platino antineoplásicos derivados del platino 1 En el documento de trabajo WHO/EMP/RHT/TSN/2013.1, que se actualiza periódicamente y puede solicitarse al Programa sobre Denominaciones Comunes Internacionales, OMS, Ginebra, figura una lista más amplia de partículas.
WHO Drug Information, Vol. 31, No. 2, 2017 Proposed INN: List 117
383
-poetinum -poetina factores sanguíneos similares a la eritropoyetina -pril(at)um -pril(at) inhibidores de la enzima conversora de la angiotensina -profenum -profeno antiinflamatorios derivados del ibuprofeno prost prost prostaglandinas -relinum -relina péptidos estimulantes de la liberación de hormonas hipofisarias -sartanum -sartán antihipertensivos (no peptídicos) antagonistas del receptor de angiotensina II -vaptanum -vaptán antagonistas del receptor de vasopresina vin- vin- ) alcaloides de la vinca -vin- -vin- )