who drug informationapps.who.int/medicinedocs/pdf/s4951e/s4951e.pdf · who drug information vol....
TRANSCRIPT

205
WHO Drug Information Vol. 16, No. 3, 2002
WHO Drug Information
Contents
Feature ArticleDrug and therapeutics committees:
a Swedish experience 207
Current TopicsTenth International Conference of Drug
Regulatory Authorities 214The Parenteral Society 220
Safety InformationAdverse reactions to natural health products 222Leflunomide: haematologic, hepatic and
respiratory reactions 223Herbal mixture and palpitations 224
Indapamide and hyponatraemia 225
Regulatory and Safety ActionEpoetin alfa: pure red cell aplasia 226Ergot-derived dopamine receptor agonists:
fibrotic reactions 226Buprenorphine approved for opiate
dependence 227Human tissue recalled 227Lepirudin and fatal anaphylactic reactions 227Valdecoxib: new warnings 228Parecoxib/valdecoxib: serious hypersensitivity
reactions 228Mefloquine labelling strengthened 228Glucowatch® for diabetes 229Generic omeprazole approved 229Oxaliplatin for colorectal cancer 230Ergotamine and ischaemia 230
Acetylsalicylic acid and Reye's syndrome 230Sertraline interactions 231Inhaled corticosteroids and adrenal
suppression 231Re-introduction of urokinase 232Ezetimibe approved for cholesterol-lowering 232
ATC/DDD ClassificationA historical overview of the ATC/DDD
methodology 233Drug utilization statistics and health policy 235Trends in drug utilization research in
developing countries 236Drug utilization data constraints in developing
countries 237The future of ATC/DDD and drug utilization
research 238
Recent Publications and Sources of InformationInternational Ethical Guidelines for Biomedical
Research Involving Human Subjects 241Surveying and Evaluating Ethical Review
Practices 241The importance of pharmacovigilance 241Effective drug regulation 242Dialogue in pharmacovigilance 242Good storage practices 242
Recommended International Nonproprietary Names: List 48
World Health Organization
243
206
WHO Drug Information Vol. 16, No. 3, 2002
WHO Drug Information
is now available at:
http://www.who.int/druginformation

207
WHO Drug Information Vol. 16, No. 3, 2002
Feature Article
Drug and therapeutics committees:a Swedish experienceThe development of drug and therapeutics commit-tees (DTCs) in hospitals and for primary health carevaries markedly from one country to another withinEurope (1) but has been particularly strong in theNordic countries. Since 1997, Swedish law requiresthat all twenty-one regions have a drug and thera-peutics committee. These committees have playedan increasingly important role in implementing therational use of drugs.
For 40 years, hospital drug formulary committeeshave existed in Sweden to develop guidelines forthe selection of the pharmacotherapeutic armamen-tarium. Committees were primarily established toevaluate drugs available for use in routine care andto recommend drugs of choice for common dis-eases. Selection was based on therapeutic value,therapeutic tradition, and price. The right of anindividual physician to prescribe according to hisown judgement was fully recognized as a funda-mental element of health care delivery, but thedifficulty of maintaining oversight of the increasingnumber of drugs on the market was also acknowl-edged (2). The committee's primary objective wasthus to improve rational use while decreasing thecost of drug treatment.
Four important prerequisites relating to the work ofthe committee were emphasized (2):
• Work should be a collaborative effort betweenclinicians, pharmacists and clinical pharmacolo-gists.
• Selection of recommended drugs should be basedon relevant statistics on the use of drugs in ahospital setting.
• The committee should work through “ambassa-dors” to inform prescribers about committeeevaluations and conclusions.
• The drug committee should inspire a sophisticatedand intense pharmacotherapeutic debate inhospitals.
The success of the first committees within univer-sity hospitals was instrumental in extending rationaluse throughout the country. As a result of initialwork, the number of standard solutions for infusionwas reduced from 25 to four, and the number ofpharmacotherapeutic hypnotics from 37 to six (2).During the early seventies, follow-up of the out-come of drug recommendations through drugutilization statistics was emphasized, and educa-tional initiatives were implemented when prescrib-ing was found to deviate from recommendations(3). By 1975, the concept of generic substitutionhad been successfully introduced in Stockholmhospitals. Major events in the development of drugselection are summarized in Table 1 on page 208.
In the 1980s, a special guideline focusing on drugchoices in primary health care was developed toincrease the commitment of general practitioners.In 2000, a single guideline with some 200 recom-mended first-line drugs for the most commondiseases was agreed upon for the entire populationof 1.8 million inhabitants in Stockholm. During theearly 1990s, the scope of the committees wasbroadened to include drug information and educa-tion of prescribers. The number of committees inSweden now reached almost one hundred.
In 1997, drug and therapeutics committees becameobligatory under law and instructions were issued(see Table 2 on page 208). Counties now had toprovide a budget to support committee activities.The number of coordinating DTCs was reduced to21 regional committees, performing their workthrough expert groups on different diseases andthrough local committees.
Functions of drug andtherapeutics committeesSince the 1997 Swedish Drug Reform Act, thefunction of drug and therapeutics committees has
Folke Sjöqvist , Ulf Bergman, Marja-Liisa Dahl, Lars L.Gustafsson , and Lars-Olof Hensjö , Department of Medi-cal Laboratory Sciences and Technology of the KarolinskaInstitute (Division of Clinical Pharmacology), WHO Col-laborating Center for Drug Utilization Research andClinical Pharmacological Services, Huddinge UniversityHospital, Stockholm, Sweden, and the Regional DrugCommittee (LÄKSAK), Stockholm (correspondence:[email protected])
208
WHO Drug Information Vol. 16, No. 3, 2002
been regulated by the local county councils as themain providers of public health care. As the princi-pal source of expertise, the overall aim of thecommittees is to promote the rational use of drugsat all levels of the health care system, whether atspecialized clinics or primary health care centres.The committees have become a core facility forevidence-based principles of drug therapy withinthe health care system. Clinical pharmacologists,pharmacists, and district nurses (who have re-stricted prescribing rights in Sweden) are alsorepresented. Members must declare any conflict ofinterest and acting as a consultant to industry is notallowed if this would lead to the promotion of an
individual drug product. However, scientific collabo-ration at the institutional level is acceptable andeven desirable.
Regional DTCs gather and evaluate knowledge ondrugs and drug therapies through screening ofscientific documentation systematically retrievedfrom the literature. Local networks of experts repre-sentative of the various health care levels areresponsible for implementation of the recommenda-tions. The committees are urged to improve thequality of drug therapy at all levels of health carewithin a given county, including the private sector,and collaborate with other experts from regional
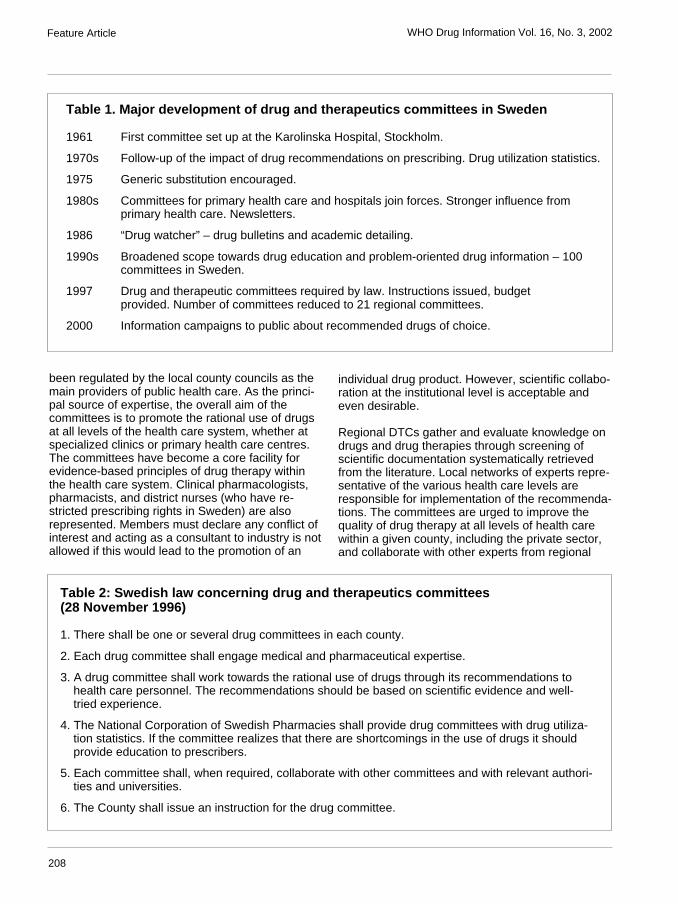
Table 1. Major development of drug and therapeutics committees in Sweden
1961 First committee set up at the Karolinska Hospital, Stockholm.
1970s Follow-up of the impact of drug recommendations on prescribing. Drug utilization statistics.
1975 Generic substitution encouraged.
1980s Committees for primary health care and hospitals join forces. Stronger influence fromprimary health care. Newsletters.
1986 “Drug watcher” – drug bulletins and academic detailing.
1990s Broadened scope towards drug education and problem-oriented drug information – 100committees in Sweden.
1997 Drug and therapeutic committees required by law. Instructions issued, budgetprovided. Number of committees reduced to 21 regional committees.
2000 Information campaigns to public about recommended drugs of choice.
Table 2: Swedish law concerning drug and therapeutics committees(28 November 1996)
1. There shall be one or several drug committees in each county.
2. Each drug committee shall engage medical and pharmaceutical expertise.
3. A drug committee shall work towards the rational use of drugs through its recommendations tohealth care personnel. The recommendations should be based on scientific evidence and well-tried experience.
4. The National Corporation of Swedish Pharmacies shall provide drug committees with drug utiliza-tion statistics. If the committee realizes that there are shortcomings in the use of drugs it shouldprovide education to prescribers.
5. Each committee shall, when required, collaborate with other committees and with relevant authori-ties and universities.
6. The County shall issue an instruction for the drug committee.
Feature Article
209
WHO Drug Information Vol. 16, No. 3, 2002
clinical pharmacology departments, telepharmaco-logical services, local pharmacies, the MedicalProducts Agency, the pharmaceutical industry, anddrug formulary committees. Other important func-tions are to provide the county council administra-tions with medical expertise in drug purchasing,develop policy documents for drug information, andprovide education and follow-up on drug utilizationand prescription patterns.
Selection of recommended drugsSelected drugs should be well documented andappropriate from the pharmaceutical, pharmacologi-cal and therapeutic point of view, and consideredessential in the treatment of common diseases.Evaluation of documentation follows the principlesof evidence-based medicine. In order to gatherexperience about the safety of the compound, anew drug should have been registered and avail-able on the market for at least two years. However,there is a trend towards quicker decisions andearlier acceptance of new drugs if they have shownpotential to improve therapy.
Treatment costs are taken into account and aneconomic evaluation is demanded both for initialdrug cost and the total treatment schedule. Recom-mended drugs should have high delivery guaran-tees from the producer/distributor, with relevant andup-to-date product information. Maintaining drugselection requires continuous follow-up of newlyregistered drugs, evaluation of the literature withrespect to new guidelines, clinical trials and reportson adverse reactions. Expert groups are expectedto stay in touch with specialist organizations prepar-ing national treatment guidelines as well as with theMedical Products Agency, which regularly initiatesand coordinates workshops.
Education and informationThe rapidly expanding number of new drugs andtreatment principles has created an increased needfor independently evaluated drug information andeducation. The drug and therapeutics committeeplays a central role here and supports a bilateralexchange of information with prescribers. Educationis mostly problem-oriented, being initiated andorganized by the medical community based on theneeds of prescribers. Different models are beingtested and an important idea is “drug education byprescribers for prescribers”. Primary health carephysicians in academic drug detailing have beenengaged at primary health care centres as “DrugWatchers” (4).
Regional drug information centres based withinclinical pharmacology departments provide inde-pendent and evaluated problem-oriented druginformation to prescribers (5) through a database —Drugline — containing more than 10 000 evaluateddocuments on drug-related issues (6).
In several counties, DTCs regularly inform thepublic of their recommendations. In Stockholm,mass media campaigns focusing on the list ofrecommended drugs have been directed at pre-scribers and their patients. The campaigns havehelped to establish the regional committee as anindependent and reliable expert organization. BothDTCs and the regional drug information centrescollaborate actively with the Medical ProductsAgency, which publishes excellent monographs onindividual drugs and reviews on the treatment ofdifferent diseases.
Electronic prescribingIn Stockholm, a computer-based prescriptionsupport system, JANUS telepharmacology, hasbeen developed (http://www.janusinfo.org) aimed atproviding all prescribers within a county with easilyaccessible, clinically relevant and updated informa-tion on drugs. The system includes (mainly inSwedish):
• information and recommendations from theregional and local drug committees in the county;
• recent guidelines from the Medical ProductsAgency;
• links to the Physicians Desk Reference (FASS)and Drugline; and
• recent drug news with comments and evaluationsby specialists.
JANUS also provides access to information on druginteractions, with evaluated literature references toeach interaction (7). The key objective is to provideappropriate information and prescribing tools tosimplify the selection and dosage of drugs.
Graphic presentations of local drug prescriptionpatterns are also included to allow quick feedbackto and between prescribers. Within the next fewyears, electronic prescribing is expected to replaceold-fashioned prescriptions, and the prescriber willthen have access to real time information whileprescribing. Integrated into the JANUS prescription
Feature Article
210
WHO Drug Information Vol. 16, No. 3, 2002
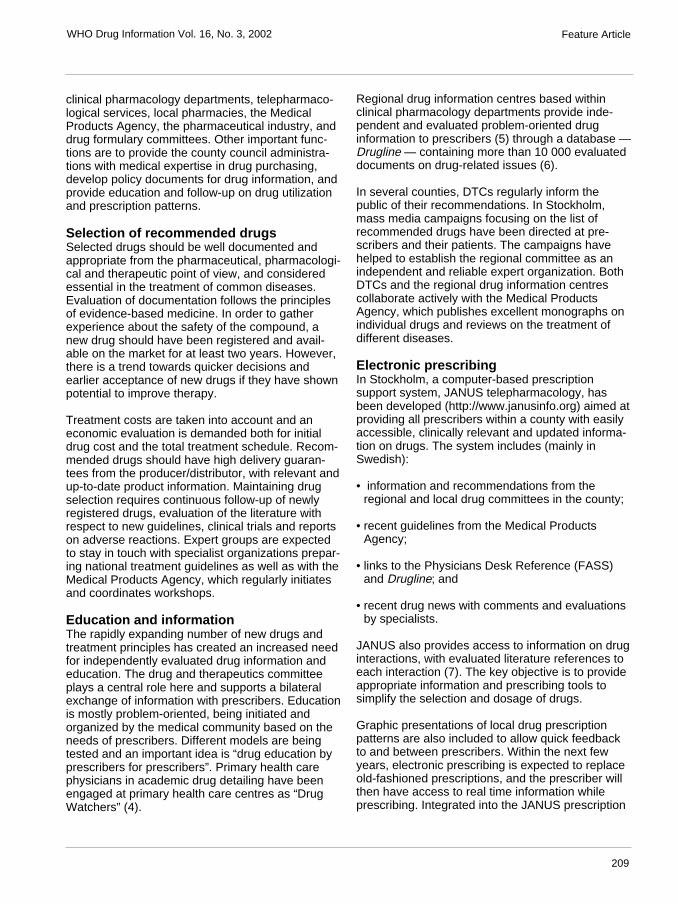
system is a website (http://www.janusinfo.org) thatserves as the electronic channel for all DTCs inStockholm. Representative examples of the sitepages in JANUS are set out in Figures 1 and 2.
Follow-up and feedback of drug utilizationIncreasing drug costs, together with the transfer ofthe drug budget from the government to the countycouncils, emphasizes the need for follow-up of druguse, prescription patterns and cost trends. Drugcommittees play a key role in developingpharmacoepidemiological tools. The 1997 DrugReform Act required bar codes for prescriptions,indicating workplace and prescriber identity. Thefeedback provided serves as an ideal self-auditsystem for primary health care centres, clinics, andindividual prescribers (10).
Local auditing of prescription patterns and costdevelopment in relation to the committee’s recom-mendations is an important strategy and stimulatesfeedback on rationality, prescribing and cost-awareness. Such data also form the basis forrevision of drug recommendations, educational andinformational activity needs, or intervention studies.Before drug reform, physicians were relativelyunaware of the costs that prescribing generated,since the government paid the bill. This will nowchange dramatically and drug costs will become anintegrated and visible part of the entire budget for aclinic or primary health care centre.
A new indicator of the quality of drug prescribinghas recently been introduced in Stockholm County(8): Drug Utilization 90% (DU90%). The term refers
Fig. 1. JANUS prescription system:
Drug statistics:Drug sales (1 million Swedish Kroner= 0.1 million Euros) by ACT class for 1st. quarter 1995–2000 inStockholm. This function is updated monthly at the webiste: http://www.janusinfo.org
Feature Article
211
WHO Drug Information Vol. 16, No. 3, 2002
to the number of drugs accounting for 90% of druguse, measured in defined daily doses (DDDs). TheSwedish Medical Quality Council (9) has suggestedusing the DU90% as a general quality indicator ofdrug prescribing, and this has also been adopted inStockholm (10). Adherence to guideline recommen-dations or other consensus documents is reflectedby the percentage of recommended drugs withinthe DU90% segment. This measure can easily beused for comparisons over time between hospitals,clinics, primary health care centers and geographi-cal regions and may identify problem areas whereeducational interventions are required. The methodcan be applied to all drugs or to different therapeu-tic classes (ATC groups). It also provides data foreconomic follow-up and analysis, as the drug costs
are also included. By sorting on “costs” the corre-sponding Drug Costs 90% – DC90% – profile isobtained.
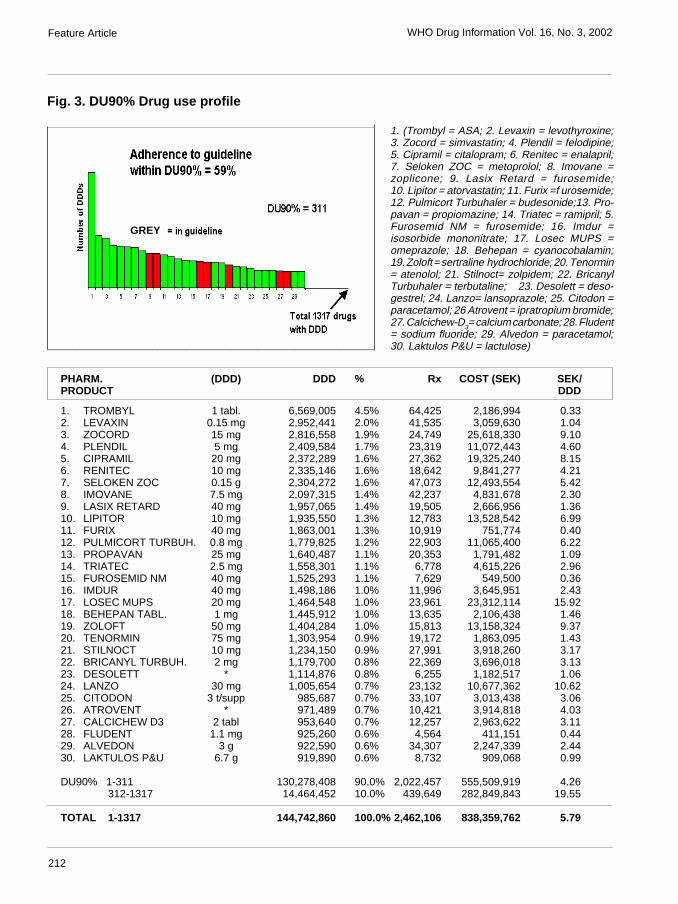
The combined DU90%/DC90% profile has turnedout to be of considerable interest to prescribers andphysicians responsible for health care costs, includ-ing drugs. Figure 3 on page 212 describes DU90%profile by brand name based on prescriptionsdispensed to the population of Stockholm duringthe three months of October–December 2000ranked by number of defined daily doses (DDD),according to the recommendations by the SwedishMedical Quality Council (9). The drug utilization90% (DU90%) segment (the area below the curve)corresponds to 311 of a total of 1,317 brand nameswith DDDs dispensed at pharmacies. Adherence to
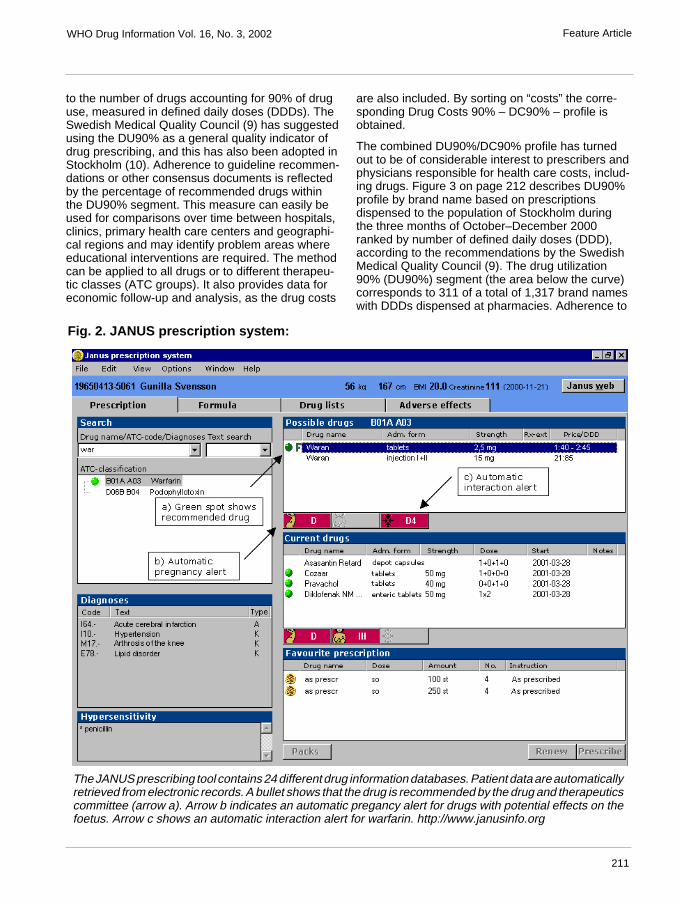
Fig. 2. JANUS prescription system:
The JANUS prescribing tool contains 24 different drug information databases. Patient data are automaticallyretrieved from electronic records. A bullet shows that the drug is recommended by the drug and therapeuticscommittee (arrow a). Arrow b indicates an automatic pregancy alert for drugs with potential effects on thefoetus. Arrow c shows an automatic interaction alert for warfarin. http://www.janusinfo.org
Feature Article
212
WHO Drug Information Vol. 16, No. 3, 2002
Fig. 3. DU90% Drug use profile
PHARM. (DDD) DDD % Rx COST (SEK) SEK/PRODUCT DDD
1. TROMBYL 1 tabl. 6,569,005 4.5% 64,425 2,186,994 0.332. LEVAXIN 0.15 mg 2,952,441 2.0% 41,535 3,059,630 1.043. ZOCORD 15 mg 2,816,558 1.9% 24,749 25,618,330 9.104. PLENDIL 5 mg 2,409,584 1.7% 23,319 11,072,443 4.605. CIPRAMIL 20 mg 2,372,289 1.6% 27,362 19,325,240 8.156. RENITEC 10 mg 2,335,146 1.6% 18,642 9,841,277 4.217. SELOKEN ZOC 0.15 g 2,304,272 1.6% 47,073 12,493,554 5.428. IMOVANE 7.5 mg 2,097,315 1.4% 42,237 4,831,678 2.309. LASIX RETARD 40 mg 1,957,065 1.4% 19,505 2,666,956 1.3610. LIPITOR 10 mg 1,935,550 1.3% 12,783 13,528,542 6.9911. FURIX 40 mg 1,863,001 1.3% 10,919 751,774 0.4012. PULMICORT TURBUH. 0.8 mg 1,779,825 1.2% 22,903 11,065,400 6.2213. PROPAVAN 25 mg 1,640,487 1.1% 20,353 1,791,482 1.0914. TRIATEC 2.5 mg 1,558,301 1.1% 6,778 4,615,226 2.9615. FUROSEMID NM 40 mg 1,525,293 1.1% 7,629 549,500 0.3616. IMDUR 40 mg 1,498,186 1.0% 11,996 3,645,951 2.4317. LOSEC MUPS 20 mg 1,464,548 1.0% 23,961 23,312,114 15.9218. BEHEPAN TABL. 1 mg 1,445,912 1.0% 13,635 2,106,438 1.4619. ZOLOFT 50 mg 1,404,284 1.0% 15,813 13,158,324 9.3720. TENORMIN 75 mg 1,303,954 0.9% 19,172 1,863,095 1.4321. STILNOCT 10 mg 1,234,150 0.9% 27,991 3,918,260 3.1722. BRICANYL TURBUH. 2 mg 1,179,700 0.8% 22,369 3,696,018 3.1323. DESOLETT * 1,114,876 0.8% 6,255 1,182,517 1.0624. LANZO 30 mg 1,005,654 0.7% 23,132 10,677,362 10.6225. CITODON 3 t/supp 985,687 0.7% 33,107 3,013,438 3.0626. ATROVENT * 971,489 0.7% 10,421 3,914,818 4.0327. CALCICHEW D3 2 tabl 953,640 0.7% 12,257 2,963,622 3.1128. FLUDENT 1.1 mg 925,260 0.6% 4,564 411,151 0.4429. ALVEDON 3 g 922,590 0.6% 34,307 2,247,339 2.4430. LAKTULOS P&U 6.7 g 919,890 0.6% 8,732 909,068 0.99
DU90% 1-311 130,278,408 90.0% 2,022,457 555,509,919 4.26 312-1317 14,464,452 10.0% 439,649 282,849,843 19.55
TOTAL 1-1317 144,742,860 100.0% 2,462,106 838,359,762 5.79
Feature Article
1. (Trombyl = ASA; 2. Levaxin = levothyroxine;3. Zocord = simvastatin; 4. Plendil = felodipine;5. Cipramil = citalopram; 6. Renitec = enalapril;7. Seloken ZOC = metoprolol; 8. Imovane =zoplicone; 9. Lasix Retard = furosemide;10. Lipitor = atorvastatin; 11. Furix =f urosemide;12. Pulmicort Turbuhaler = budesonide;13. Pro-pavan = propiomazine; 14. Triatec = ramipril; 5.Furosemid NM = furosemide; 16. Imdur =isosorbide mononitrate; 17. Losec MUPS =omeprazole; 18. Behepan = cyanocobalamin;19. Zoloft = sertraline hydrochloride; 20. Tenormin= atenolol; 21. Stilnoct= zolpidem; 22. BricanylTurbuhaler = terbutaline; 23. Desolett = deso-gestrel; 24. Lanzo= lansoprazole; 25. Citodon =paracetamol; 26 Atrovent = ipratropium bromide;27. Calcichew-D3= calcium carbonate; 28. Fludent= sodium fluoride; 29. Alvedon = paracetamol;30. Laktulos P&U = lactulose)
GREY

213
WHO Drug Information Vol. 16, No. 3, 2002
Guideline 2000 issued in January 2000 was 59% inthe DU90% segment. The technical unit of compari-son (DDD) is given in mg, or number of tablets, etc.Rx = number of prescription items. Cost (SEK) inSwedish kronor. Corresponding ranking by costprovides a drug cost 90% profile – DC90%. SEK/DDD is the actual costs per DDD.
ResourcesThe drug and therapeutics committees have anannual budget which varies between the 21 re-gions. In the most progressive counties it has beenconsidered appropriate to invest a sum correspond-ing to 1% of the total drug expenditure. The annualbudget for the DTCs in Stockholm is about 4 millionEuros, with drug expenditure about 0.4 billion Eurosannually.
In Stockholm, the budget is spent on salaries andfor engaging clinical expertise. With the existingfinancial system for the health care budget it isimpossible to engage clinical experts for this intel-lectual work unless they can have leave of absencefrom their pressing daily work with patients. Much ofthe budget is spent on continuing education ofprescribers and to implement the recommendationsof the drug committee.
The committees can also use the competence ofexisting units in clinical pharmacology as well asregional and local pharmacies. The regional druginformation centres (6) offer a service to retrieve,evaluate and summarize the documentation ofdifferent drug products.
The future of drug andtherapeutics committeesA number of circumstances make it clear that theindividual prescriber will be in great need of unbi-ased, consultative support in the selection and useof drugs in the future. The aims of drug treatmentshould be that the right drug is prescribed to theright patient in the right dose with the right informa-tion and at the right (affordable) cost (11). Thisimplies competence, integrity and cost-awarenesson behalf of the prescriber.
Prescribers, then, will accept advice from theorganization paying the drug bill and not from themanufacturer alone, while providers of health carehave to take responsibility for the continued drugeducation of the prescribers. This will probably bean invaluable investment in view of the alarmingannual increase of expenditure for drugs, andadverse drug effects now reported worldwide.
For drug and therapeutics committees to be effec-tive, it is vital to broadly engage the prescribingprofessions in the work and to base the selection ofthe therapeutic choice on advice from the mostcompetent experts in pharmacotherapeutics.
References
1. Fijn, R., Brouwers, J.R., Knaap, J.R. et al. Drug andtherapeutics (D & T) committees in Dutch hospitals: anationwide survey of structure, activities, and drug selec-tion procedure. British Journal of Clinical Pharmacology,48: 239–246 (1999).
2. Barkman, R., Boréus, L.O., Böttiger, L.E. et al.Läkemedelskommittén – Service i rutinsjukvård.Läkartidningen, 26: 2491–2496 (1966).
3. Bergman, U., Christenson, I., Jansson, B. et al. Auditinghospital drug utilization by means of defined daily dosesper bed-day. A methodological study. European Journal ofClinical Pharmacology, 17:183–187 (1980).
4. Stålsby Lundborg, C., Hensjö, L-O., Gustafsson, L.L.Academic drug-detailing: from project to practice in aSwedish urban area. European Journal of Clinical Phar-macology, 52: 167–172 (1997).
5. Alván, G., Öhman, B., Sjöqvist, F. Problem-orienteddrug information: A clinical pharmacological service.Lancet, 2: 1410–1412 (1983)
6. Öhman, B., Lyrvall, H., Alván, G. Use of Drugline – Aquestion and answer database. Annals of Pharmaco-therapy, 27: 278–284 (1993).
7. Sjöqvist, F. Interaktion mellan läkemedel – systematisköversikt. In: Läkemedel i Sverige. FASS: 1583–1653(2001).
8. Bergman, U., Popa, C., Tomson, Y. et al. Drug utiliza-tion 90% – a simple method for assessing the quality ofdrug prescribing. European Journal of Clinical Pharma-cology, 54: 113–118 (1998).
9. Bergman, U., Andersson, D., Friberg, A. et al. Kvalitets-utveckling: Kvalitetsindikatorer för läkemedelsförskrivningoch–hantering. Svensk Medicin, Svenska Läkaresälls-kapet och Spri 1999. No. 66.
10. Nyman, K., Bergens, A., Björin, A.S. et al. Återföringav förskrivningsprofiler vid en vårdcentral. Viktigt inslag ikvalitetssäkringen av läkemedelsförskrivningen.Läkartidningen, 98: 160–164 (2001).
11. Sjöqvist, F. The past, present and future of clinicalpharmacology. European Journal of Clinical Pharma-cology, 55: 553–557 (1999).
Feature Article
214
WHO Drug Information Vol. 16, No. 3, 2002
Current Topics
Recommendations from the TenthInternational Conference of DrugRegulatory Authorities
Herbal medicines
1. Member States, together with WHO, shoulddefine criteria and standards for herbal medicines,health or functional foods, and dietary supplements.WHO should continue to develop guidelines on theassessment of safety, efficacy and quality control ofherbal medicinal products and herbal combinations.
2. The safe use of herbal medicines is a majorconcern for governments and consumers. WHOshould provide guidance to countries wishing toestablish safety monitoring systems or to expandexisting systems to monitor and report adversereactions to herbal medicines. Member Statesshould strengthen their post-marketing surveillance
systems for herbal medicines. Such systems shouldinvolve health care providers, consumers andmanufacturers.
3. WHO should support countries in developingsources of information on herbal medicines whilefacilitating information-sharing among countries.WHO should provide guidance to governments andnongovernmental organizations (NGOs) on how todevelop information and educational programmeson the proper use of herbal medicines for thepublic.
4. WHO should provide guidance for governmentsand NGOs on training of traditional medicine pro-viders, and promote communication with otherhealth workers.
5. Member States should seek funds to supportresearch on herbal medicines.
6. Progress should be reported back to the ICDRA.
Tenth International Conference of Drug Regulatory AuthoritiesThe Tenth International Conference of Drug Regulatory Authorities (ICDRA) took place in Hong KongSAR, People's Republic of China from 24 to 27 June 2002. Two hundred and twenty senior drugregulatory officials from over one hundred countries participated in this international forum estab-lished in 1980. The objectives of the ICDRA are to address issues of immediate concern, strengthencommunication and develop collaboration among regulatory authorities. As a platform set up todevelop international consensus, the ICDRA has been an important tool for WHO in its efforts toharmonize regulation and improve the safety, efficacy and quality of medicines. Regulatory authori-ties are continually faced with new issues brought about by globalization and development of freetrade, while increased responsibilities — such as those covering control of alternative medicines andthe introduction of innovative treatments — place heavy demands on regulatory systems and knowl-edge bases. The development of sophisticated technologies and techniques in health care andextensive use of the Internet impose new challenges.
The conference programme was developed by a planning committee of representative drug regula-tors and provided the impetus for discussion of the many current issues facing authorities. As a resultof the four days of debate, drug regulators made recommendations (as set out below) on issuescovering herbal medicines, homeopathy, regulatory reform, medicines safety, counterfeiting, accessto drugs and vaccines, regulation of clinical trials, harmonization, new technologies and e-commerce.These recommendations have been proposed to serve as a basis for future collaboration and effortsamong Member States, drug regulatory authorities, WHO, and interested agencies and institutions.
215
WHO Drug Information Vol. 16, No. 3, 2002 Current Topics
Safety of Blood-derived Products
Plasma-derived medicinal products, as well asblood and blood components, should be regulatedin the same way as other biological products andfall under the responsibility of regulatory authorities.The importance of good manufacturing practice(GMP) was emphasized. The main problem identi-fied was how best to minimize the risk of transmit-ting currently known and emerging blood-bornediseases. Developing countries in particular, haddifficult choices to make in planning balancedregulatory action.
1. WHO should promote t he regulation of bloodand plasma collection centres, with emphasis onensuring GMP compliance.
2. Regional co-operation and training should bepromoted and WHO should facilitate the develop-ment of educational programmes and trainingopportunities for staff involved in regulation andcontrol of blood products.
3. WHO should collaborate with Member States tostrengthen the technical expertise of regulatoryauthorities (especially those countries with plasmafractionation activities/facilities) to assure adequatequality, safety and efficacy of plasma products.Special emphasis should be placed on viral testing,viral inactivation procedures, and surveillance forviral and other transfusion-transmitted diseases.Special attention should be given to the possiblerisk of transmission of vCJD and appropriate valida-tion studies should be carried out.
4. In those countries where contract fractionation ofplasma is a common option, WHO should developguidance on the regulatory issues involved.
5. In order to facilitate approval by regulatory au-thorities of importation of plasma products, WHOshould promote the use of batch release certifi-cates, with a clear description of the proceduresused.
6. Progress should be reported back to the ICDRA.
Antimicrobial resistance: new initiatives
Antmicrobial resistance is a threat to effectivetreatment of infectious diseases. Since the topicwas first discussed at the ICDRA in 1996, muchhas been accomplished in this area. However, if theemergence of resistance is to be slowed, much
more needs to be done. The following are urgentrecommendations for all regulatory authorities toimplement.
1. All countries should make containment of antimi-crobial resistance a national priority by creating anintersectoral task-force to bring together all inter-ested parties and ensure collaboration among thevarious professional groups.
2. National systems should be created to monitorand analyse antimicrobial usage in food animalsand humans by collecting data from hospitals andin the community and linking these findings toresistance and disease surveillance data.
3. Efforts should continue in regulating anti-microbials, while addressing the need for availabil-ity at all levels of the health care system.
4. Promotional activities should continue to beregulated by ensuring adherence to guidelines forethical promotion of medicines.
5. Education of health professionals in rationalprescribing and of patients in compliance should beencouraged. Awareness of antimicrobial resistanceshould be raised within regulatory authorities.
6. The pharmaceutical industry should pay particu-lar attention to GMP and quality issues in relation tothe production of antimicrobials, as well as tolabelling of their products.
7. Regional and international collaboration shouldcontinue and progress reported back to the ICDRA.
Harmonization I
1. WHO should continue involvement in the ICHSteering Committee, adopting a more proactive roleby proposing topics for guideline development andexpressing opinions on the potential public healthimplications of the guidelines proposed by ICH.
2. In the light of the wide range of regulatory envi-ronments, WHO should support non-ICH MemberStates and regional harmonization initiatives byevaluating the usefulness, feasibility and impact ofimplementing ICH guidelines.
3. WHO should continue to produce briefing noteson ICH meetings for regulatory officials of non-ICHcountries and consider ways of making them widelyavailable, including use of the Internet.

216
WHO Drug Information Vol. 16, No. 3, 2002Current Topics
4. In order to improve access to essential drugs ofgood quality, especially in developing countries,WHO should assess the benefits and risks to publichealth of implementing selected ICH drug qualityguidelines on manufacturing standards for genericproducts in non-ICH countries, and intensify itsefforts to develop international standards andguidelines for the regulatory assessment of genericproducts. WHO should offer specific advice tonational authorities in non-ICH countries.
5. Progress should be reported back to the ICDRA.
Harmonization II
It was recognized that international harmonizationis characterized by a number of initiatives under-taken in different parts of the world. Such initiativesreflect specific local or regional needs and circum-stances. Although these activities and their prod-ucts may be useful examples and supply importanttechnical knowledge, no single initiative can cur-rently be considered a model for internationalapplication or implementation.
1. Countries should take into account local factors,priorities, possible implications, and implementationcapacity when evaluating harmonization initiativesand guidance materials produced elsewhere.
2. The development of international regulatoryrequirements and guidelines should be based ondemonstrated public-health needs and should notbe driven by technological progress alone.
3. WHO should continue to support regional andlocal harmonization initiatives aimed at strengthen-ing regulatory capacity and achieving public healthgoals.
4. Progress should be reported back to the ICDRA.
Protection of subjects in clinical trials
1. Drug regulatory authorities have an importantrole in protecting trial subjects. Drug regulatoryauthorities are required to keep a complete registerof trials carried out in the country and, when possi-ble, these registers should be made public (e.g.through the agency website).
2. When trials are carried out in several countries orwhere part of a study is carried out in a differentcountry, direct communication between the regula-tory authorities of the countries involved should be
established. Contact data of responsible peopleshould be available on the agency website.
3. Drug regulatory authorities should pay attentionto the informed consent procedure and ensure thatcomplete information is provided to the trial sub-jects in conformity with international guidelines, inaddition to requiring national or local ethical review.
4. WHO should develop guidelines for the effectivecontrol of trials by the regulatory authority.
5. WHO should strengthen protection of human trialsubjects by developing good clinical practices(GCP) training tools for drug regulatory authorities,promoting training of GCP inspectors, and providingassistance to Member States in setting up GCPinspectorates.
6. Progress should be reported back to the ICDRA.
Regulating biotechnology products
The need to make optimal use of the products ofnew biotechnologies in the prevention, diagnosisand treatment of diseases that are the majorcauses of morbidity and mortality throughout theworld, especially in developing countries, wasrecognized. However, it was emphasized that theseare highly complex products, often manufacturedusing novel biotechnologies, and the need forcareful evaluation and regulation was vital. Issuesrelating to the comparability of biotechnology prod-ucts, including those of scale-up, were highlightedas needing particular attention.
Rapid growth of the biotechnology industry in anumber of developing countries was noted, as wasthe science-based regulatory oversight already inplace in some instances. However, effective regula-tory oversight, as well as adequate resources todeal with biotechnology products, was still neededin the majority of developing countries. Full supportwas expressed for the application of biotechnologyto the development of vaccines, therapeutic biologi-cals and diagnostics for the prevention, treatmentor diagnosis of disease.
1. Given the rapid advances in biotechnology andthe challenge of balancing the risks and benefits,WHO, in collaboration with regulatory authorities,should monitor developments and continue toprovide clear guidelines on issues relating to qual-ity, safety and efficacy of biotechnology-derivedmedicinal products, including biocomparability.

217
WHO Drug Information Vol. 16, No. 3, 2002 Current Topics
Rapid dissemination of this advice is crucial andWHO should strive to improve awareness of avail-able guidance.
2. Regulatory authorities lacking experience in theregulation of biotechnology-derived products shouldbe strengthened through education, training andupdating, as appropriate. They should draw uponthe knowledge and skills of regulatory authoritiesalready experienced in this area, with the collabora-tion of WHO. Regulatory authorities should recog-nize the need to support the participation of officialsat scientific and related meetings dealing with theregulation of this fast-developing field.
3. Regulatory authorities with limited experienceshould identify sources of expertise within theircountries, such as in academia, to assist in thereview of applications for clinical trials and formarketing authorizations. Where these are lacking,the support of experts from more experiencedregulatory authorities should be explored, with theassistance of WHO, as a means of obtaining thenecessary skills and knowledge.
4. WHO should continue development of Interna-tional biological reference materials that can serveas reference standards for new products.
5. Progress should be reported back to the ICDRA.
Regultory challenges:health sector reformand drug regulatory capacity
Health sector reform, especially in developingcountries, has been driven more by financial con-straints than by health needs. This is an importantchallenge for drug regulatory authorities that areconfronted with reduction of public funding and theneed to develop new mechanisms to finance theiractivities.
Globalization of economies and intensification ofinternational commerce have created new chal-lenges for drug regulatory authorities. Most authori-ties, especially the less resourced ones, are con-fronted with regulatory decisions made elsewhereunder diverse circumstances.
1. It is in the paramount interest of public health thatdrug regulation remains a fundamental responsibil-ity of the public sector, is not left to market forcesalone, and is not subordinated to commercialinterests.
2. New dimensions should be considered in theregulatory assessment of drug quality, safety,efficacy, and information. This must continue to bebased on solid scientific evidence, while taking intoaccount the implications of regulatory decisions onpublic health goals and on access to medicines bythe majority of the population.
3. The resources necessary to ensure full regula-tory assessment of pharmaceuticals cannot beavailable to all countries. In order to contribute tostrengthening national regulatory capacity, WHOshould study existing experience and undertakeresearch in order to develop models for intensifiedcollaboration and, where appropriate, joint decision-making among national regulatory authorities.
4. Availability of information is a crucial tool toachieve appropriate regulatory decisions. WHOshould further support national authorities to intro-duce or improve data management systems inorder to produce and interchange information andto achieve evidence-based decision-making.
5. Progress should be reported back to the ICDRA.
Access to drugs and vaccines I
1. WHO should continue its efforts in strengtheninginternational guidelines for registration of genericdrugs.
2. In collaboration with Member States, WHOshould continue to focus on activities related togood trade and distribution practices of startingmaterials to assure the use of high quality materi-als.
3. WHO should work with other technical partners,within the concept of a global alliance, to improvethe quality of products moving in internationalcommerce.
4. WHO should establish a pre-qualification qualityassurance system for essential medicines.
5. WHO should continue its prequalification projectfor procurement of medicines for priority diseases.
6. In collaboration with Member States, WHOshould develop additional international guidance onimportant elements of combination medicinesfocusing on rational use to maximize the benefit inspecific disease treatment.

218
WHO Drug Information Vol. 16, No. 3, 2002Current Topics
7. Governments and drug regulatory authoritiesshould encourage the development of therapies forneglected diseases through incentives, co-opera-tive efforts and public/private initiatives.
8. Progress should be reported back to the ICDRA.
Access to drugs and vaccines II
1. Countries should implement programmes aimedat assuring the availability, accessibility, quality andrational use of essential medicines.
2. The Model List of Essential Medicines is a cen-tral element of national drug policies. WHO shouldcontinue to maintain the Model List and supportcountries in adapting it to their needs and nationalcontext. Selection of essential medicines should bebased on safety, quality and efficacy in addition toaccessibility.
3. Access to medicines is improved by competitionbrought about by generic products. Countriesshould take measures to foster the development ofa competitive generic market.
4. Countries and WHO should further developinitiatives aimed at expanding the implementation ofthe concept of essential medicines to encompassboth the public and private sectors.
5. Countries and WHO should intensify effortsaimed at improving access to vital medicines,particularly those used for HIV/AIDS-related careand treatment.
6. Problems of vaccine availability are becomingmore frequent. Countries and WHO should intensifytheir efforts to prevent supply shortages.
7. Countries and WHO should continue to study theimpact of international trade agreements on accessto medicines and initiatives aimed at promotingessential medicines and rational use.
8. Progress should be reported back to the ICDRA
Counterfeit pharmaceutical products:panel discussion
1. Governments should acknowledge the problemof counterfeit drugs by developing national policiesand providing a comprehensive legal framework toregulate trading of counterfeit drugs as a criminaloffence.
2. Governments should adopt WHO guidelines forthe development of measures to combat counterfeitdrugs.
3. Governments of exporting countries should havea system of control to prevent the export of counter-feit drugs.
4. Drug regulatory authorities should establish aworking relationship with national (police, customs)and international (Interpol, World Customs Organi-zation) law enforcement agencies.
5. Drug regulatory authorities should establish aneffective registration system to include the licensingof manufacturers, wholesalers, and retail outlets.
6. Drug regulatory authorities should seek to coop-erate with the drug industry in the exchange ofinformation on counterfeit drugs, and to promotereporting of counterfeit drugs to WHO.
7. WHO should strengthen the existing anti-coun-terfeit liaison officers to promote exchange ofinformation on counterfeit drugs amongst andbetween regulatory authorities and WHO.
8. WHO should encourage and support MemberStates to develop and implement national meas-ures for combating counterfeit drugs.
9. WHO should organize meetings to enhanceinternational communication on counterfeit prob-lems and encourage and assist regulatory authori-ties in the delivery of public awareness pro-grammes on the dangers of counterfeit drugs.
10. Progress should be reported back to theICDRA.
Homoeopathy
1. In collaboration with Member States, WHOshould harmonize definitions of homoeopathicproducts and practices in order to allow classifica-tion and identification of homoeopathic products atnational level.
2. WHO should cooperate with governmentalinstitutions to establish recommendations for safedegrees of dilutions of homoeopathic preparations.
3. In collaboration with Member States, WHOshould promote the exchange of information. Areference list of information resources on homoeo-

219
WHO Drug Information Vol. 16, No. 3, 2002 Current Topics
pathic medicines, including official pharmacopoeiasshould be made available. WHO should developsystems to collect and provide information to con-sumers on the safe use of homoeopathic medi-cines.
4. WHO should provide guidance to governmentsand NGOs for training of homoeopathic medicineproviders.
5. Progress should be reported back to the ICDRA.
Safety monitoring
There have been major advances in the area ofpharmacovigilance and drug monitoring since WHOestablished its Programme for International DrugMonitoring in 1968 as the global standard for drugsafety. These recommendations highlight importantissues for action by regulatory authorities andWHO.
1. Regulatory authorities should expand the scopeof their activities to include surveillance of medica-tion errors, medical devices, homeopathic products,herbal medicines, natural health products andidentify reports that may point to quality defects orto counterfeit products.
2. Regulatory authorities should improve efforts toevaluate the effectiveness of the various reportingmechanisms in operation in their countries.
3. Regulatory authorities should improve communi-cation of emerging safety concerns. To assist in thisand to ensure that confidentiality and security ofshared data is maintained, WHO should develop asecure web-based communication system.
4. Regulatory authorities should be encouraged todevelop post-marketing risk management strategiesfor products identified as posing a significant risk.
5. WHO should finalize and distribute its crisismanagement plan to Member States. This shouldbe tested periodically. WHO should provide profes-sional assistance and resources in crisis manage-ment, communications and research to MemberStates.
6. The WHO adverse reactions database utilityshould be strengthened by:
• Use of best methods to ensure timely reporting toWHO of case information, and by taking steps toincrease national reporting rates.
• Assigning unique case identification codes toavoid duplication to all case-report recipients.
• Opening access to the WHO database to allstakeholders with a genuine public health interestand the ability to evaluate such case information.
7. The current WHO Programme for InternationalDrug Monitoring should be supported by:
• Encouraging all WHO Member States includingICH member countries to participate actively in theWHO Programme, and contribute to its develop-ment.
• Periodically and regularly reviewing definitions,tools, and procedures in the light of developmentsin safety in medicine.
• Strengthening WHO’s role as the mandated globalpharmacovigilance system and recognizing WHOdefinitions, tools and practices for pharmaco-vigilance and drug monitoring as world standards.
8. WHO should convene an expert group to exam-ine the special needs for assessing the safety andrisk of medicines used in the treatment of HIV/AIDS, particularly in developing countries.
9. Progress should be reported back to the ICDRA.
E-Commerce
1. Patient/consumer protection should be the firstpriority of regulatory authorities in their approach toe-commerce. National authorities should endeavourto ensure that patients have the same level ofprotection whether they purchase pharmaceuticalsthrough legitimate Internet sites or through thetraditional channels.
2. Regulatory authorities should improve the infor-mation contents of their websites and establishappropriate programmes, including mass mediacampaigns, aimed at providing unbiased informa-tion and warn the public on the possible risks ofunregulated pharmaceutical e-commerce. Theseprogrammes must be designed in a way that en-sures that they effectively reach health profession-als and consumers.
220
WHO Drug Information Vol. 16, No. 3, 2002
3. National authorities should establish and encour-age the use of simple mechanisms for consumersand health professionals to report illegal sites andnegative experience they have had with e-com-merce.
4. WHO should establish and maintain a list ofnational focal points and circulate it to all regulatoryauthorities in order to foster international collabora-tion in combating illegal pharmaceutical e-com-merce.
5. WHO should continue to create opportunities,through international meetings of national regula-tory officials, for discussing and foster awarenesson the public-health issues related to pharmaceuti-cal e-commerce.
6. Progress should be reported back to the ICDRA.
Current topics
1. There should be only one standard of quality,safety and efficacy of medicines, whether these areproduced for local consumption or for export only.Member States should regulate drugs for export inaccordance with appropriate international stand-ards.
2. WHO should collaborate closely with the PIC/Sto enhance capacity building of nationalinspectorates. This could be undertaken within theconcept of the Global Alliance.
3. WHO should continue its efforts towards thedevelopment of international specifications andpharmacopoeial requirements and the establish-ment of international reference standards for drugsresponding to major public health needs.
4. In collaboration with Member States, WHOshould develop guidelines for the regulation ofxenotransplantation.
The Parenteral SocietyThe Parenteral Society is a non-profit organizationestablished to promote and advance the practiceand science of parenteral drug therapy in theinterests of public health and to preserve andimprove the integrity and standards of theparenteral drug industry. It was originally founded inthe United Kingdom in 1981 to serve the country'shealthcare community but has developed an inter-
national membership over the years which nowstands at over 1100 members in 29 countries.
The Parenteral Society has been developed by andfor those active in the field of injectable andimplantable drugs and devices. The Society hasmembers active in academia, hospitals, industry,health ministries and other areas. Members’ inter-ests cover research and development, manufactur-ing, quality control, engineering, medicine, nursingcare and related activities. The Parenteral Societyis a founder member of the European Sterile Prod-ucts Confederation (ESPC).
A key service provided to its members is the provi-sion of information concerning all aspects ofparenteral technology and parenteral administrationfrom basic concepts to current advanced scienceand technology. It encourages a spirit of friendlycooperation among members and promotes favour-able relations with the health care professions.The Society is committed to cultivating and main-taining cooperative relations with governments andagencies, medical, pharmaceutical and relatedhealth organizations, the academic community,compendial bodies, manufacturers, suppliers to theindustry and related organizations. It also initiatesand participates in cooperative ventures and under-takings.
The Parenteral Society is active in the educationand training of personnel in parenteral drug technol-ogy and parenteral administration. Seminars,meetings, workshops, tutorials, round table discus-sions and conferences are held regularly in theUnited Kingdom and Ireland, taking various formsand covering a range of subjects. In addition, a fiveday course “Training for Pharmaceutical ProcessOperators” is held at Bath University, United King-dom, in June and September each year.
Six specialized working groups are currently active,providing for interchange of current information andideas, leading to publication of monographs onspecialized topics. The Parenteral Society ContactScheme enables members to be placed in contactwith one another for help and advice on aspects ofparenteral drug technology. This has resulted increation of an extensive database of valuableknowledge and experience.
The Society additionally has an active publicationsprogramme. It produces the quarterly EuropeanJournal of Parenteral Sciences in association with
Current Topics

221
WHO Drug Information Vol. 16, No. 3, 2002
other members of ESPC. A quarterly newsletter isalso published and the Society issues its ownreports, a series of technical monographs and oftutorial booklets, and other relevant literature. Eachyear, the Parenteral Society Award is open topractising scientists from all branches of parenteralscience, and is designed to encourage the further-ance of knowledge in this field. The award is basedon submission of the author’s original completedwork.
From its achievements to date, the Society hasincreased in profile and stature as an influential
body by providing a valuable discussion platform forthe legislated, legislator, public health and aca-demic communities. The Parenteral Society websiteprovides an introduction, current activities, publica-tions information and news updates on the globalregulatory scene relating to parenteral drug prod-ucts plus details of how to obtain membership.Further information is available from: http://www.parenteral.org.uk or: The Parenteral Society,Tel: +44 (0) 1793 824254 Fax: +44 (0) 1793832551 e-mail: secretary@ parenteral.demon.co.uk.
Current Topics
222
WHO Drug Information Vol. 16, No. 3, 2002
Safety Information
Adverse reactionsto natural health productsOver 50% of Canadians now use natural healthproducts in the form of traditional herbal products,vitamin and mineral supplements, traditional Chi-nese, Ayurvedic and other medicines and homeo-pathic preparations. However, there seems to be anoverall misconception that these agents are natu-rally safe because they come from 'natural’ plants(1, 2) The use of herbal products, a type of naturalhealth product, can be associated with adverseeffects attributable to factors such as inadequate orexcessive dosing, low-quality herbs or supple-ments, misidentified plant species, variability ofconstituents, contamination with heavy metals,adulteration with prescription drugs, interactionswith prescription drugs and allergic reactions (1).Also, some herbal ingredients are intrinsically toxic(2). A number of reported suspected reactions tonatural health products have been described (3–9).These factors along with the practice of usinghealth products with multiple ingredients, make theevaluation of adverse effects complex.
With the opportunity for self-selection and the wideavailability of natural health products, the publicneeds to be aware of the possible risks associatedwith these products as well as their benefits. Manyproducts contain multiple ingredients that mayprove challenging to consumers in allowing in-formed choices. Furthermore, consumers aresometimes misinformed by promotional informationabout some herbs or ingredients that may eitherobscure the risks associated with their use orexaggerate efficacy. Some examples include thepresence of ephedra in products used as diet aidsor energy boosters, and Ginkgo biloba in productspromoted as dietary supplements that enhancememory.
Health care professionals need to know whethertheir patients are using various health products,including natural health products, certain foods, andprescription and nonprescription drugs, in order toevaluate their overall therapy. Patients may bereluctant to discuss the use of natural health prod-ucts (1) and may be less likely to report adversereactions associated with their use than those
associated with conventional over-the-countermedicines (10). Health care professionals shouldask their patients if they are using complementaryor alternative therapies in order to provide adviceand to monitor for possible adverse reactions. Aswith conventional medicines, specific groups —pregnant and breastfeeding mothers, children,elderly people, patients with cardiovascular dis-ease, patients undergoing surgery and patientsusing conventional medicines where there is thepotential for interactions — may be at increasedrisk of ARs if using complementary and alternativemedicines (2).
Marielle McMorran. Canadian Adverse ReactionNewsletter. 12(4), (2002). http://www.hc-sc.gc.ca/hpb-dgps/therapeut/htmleng/publicat.html www.hc-sc.gc.ca/hpb/onhp)
References
1. Bielory, L. Adverse reactions to complementary andalternative medicine: ragweed’s cousin, the coneflower(echinacea), is “a problem more than a sneeze”. Annals ofAllergy & Asthma Immunology, 88:7–9 (2002). .
2. Barnes, J., Anderson, L.A., Phillipson, J.D. Herbalmedicines. 2nd ed. London: Pharmaceutical Press. p.1,18-21. 2002.
3. Case presentation: Kava. Canadian Adverse ReactionNewsletter, 12(3): 3 (2002).
4. Communiqué: Warfarin and glucosamine: interaction.Canadian Adverse Reaction Newsletter, 11 (2):4 (2001).
5. Communiqué: Glucosamine sulfate: hyperglycemia.Canadian Adverse Reaction Newsletter, 10 (4):4 (2000)
6. Communiqué: Gingko biloba: bleeding disorders.Canadian Adverse Reaction Newsletter, 10 (1):4 (2000)
7. Health Canada advising not to use products labelled tocontain Aristolochia [Public Advisory]. Ottawa: HealthCanada; 2001 Aug. 17. Available: www.hc-sc.gc.ca/english/protection/warnings/2001/2001_91e.htm.
8. Advisory not to use products containing Ephedra orephedrine [Public Advisory]. Ottawa: Health Canada; 2001June 14. Available: www.hc-sc.gc.ca/english/protection/warnings/2001/2001_67e.htm.
223
WHO Drug Information Vol. 16, No. 3, 2002
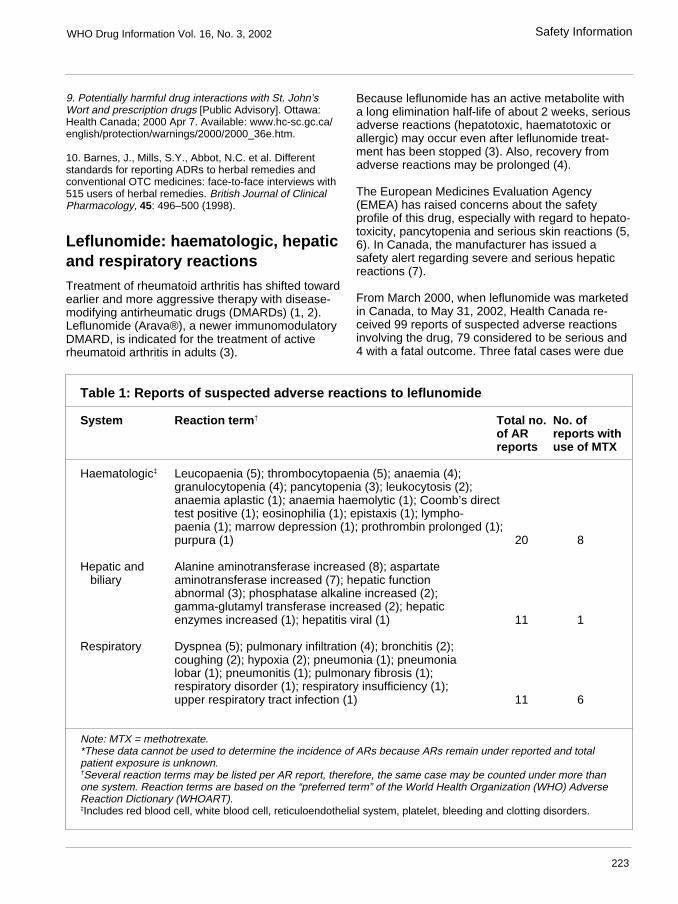
Table 1: Reports of suspected adverse reactions to leflunomide
System Reaction term † Total no. No. ofof AR reports withreports use of MTX
Haematologic‡ Leucopaenia (5); thrombocytopaenia (5); anaemia (4);granulocytopenia (4); pancytopenia (3); leukocytosis (2);anaemia aplastic (1); anaemia haemolytic (1); Coomb’s directtest positive (1); eosinophilia (1); epistaxis (1); lympho-paenia (1); marrow depression (1); prothrombin prolonged (1);purpura (1) 20 8
Hepatic and Alanine aminotransferase increased (8); aspartate biliary aminotransferase increased (7); hepatic function
abnormal (3); phosphatase alkaline increased (2);gamma-glutamyl transferase increased (2); hepaticenzymes increased (1); hepatitis viral (1) 11 1
Respiratory Dyspnea (5); pulmonary infiltration (4); bronchitis (2);coughing (2); hypoxia (2); pneumonia (1); pneumonialobar (1); pneumonitis (1); pulmonary fibrosis (1);respiratory disorder (1); respiratory insufficiency (1);upper respiratory tract infection (1) 11 6
Note: MTX = methotrexate.*These data cannot be used to determine the incidence of ARs because ARs remain under reported and totalpatient exposure is unknown.†Several reaction terms may be listed per AR report, therefore, the same case may be counted under more thanone system. Reaction terms are based on the “preferred term” of the World Health Organization (WHO) AdverseReaction Dictionary (WHOART).‡Includes red blood cell, white blood cell, reticuloendothelial system, platelet, bleeding and clotting disorders.
9. Potentially harmful drug interactions with St. John’sWort and prescription drugs [Public Advisory]. Ottawa:Health Canada; 2000 Apr 7. Available: www.hc-sc.gc.ca/english/protection/warnings/2000/2000_36e.htm.
10. Barnes, J., Mills, S.Y., Abbot, N.C. et al. Differentstandards for reporting ADRs to herbal remedies andconventional OTC medicines: face-to-face interviews with515 users of herbal remedies. British Journal of ClinicalPharmacology, 45: 496–500 (1998).
Leflunomide: haematologic, hepaticand respiratory reactionsTreatment of rheumatoid arthritis has shifted towardearlier and more aggressive therapy with disease-modifying antirheumatic drugs (DMARDs) (1, 2).Leflunomide (Arava®), a newer immunomodulatoryDMARD, is indicated for the treatment of activerheumatoid arthritis in adults (3).
Because leflunomide has an active metabolite witha long elimination half-life of about 2 weeks, seriousadverse reactions (hepatotoxic, haematotoxic orallergic) may occur even after leflunomide treat-ment has been stopped (3). Also, recovery fromadverse reactions may be prolonged (4).
The European Medicines Evaluation Agency(EMEA) has raised concerns about the safetyprofile of this drug, especially with regard to hepato-toxicity, pancytopenia and serious skin reactions (5,6). In Canada, the manufacturer has issued asafety alert regarding severe and serious hepaticreactions (7).
From March 2000, when leflunomide was marketedin Canada, to May 31, 2002, Health Canada re-ceived 99 reports of suspected adverse reactionsinvolving the drug, 79 considered to be serious and4 with a fatal outcome. Three fatal cases were due
Safety Information
224
WHO Drug Information Vol. 16, No. 3, 2002
to respiratory system disorders, with 1 case report-ing concomitant use of methotrexate. The fourthfatal case was due to a cardiac system disorder.Suspected haematologic, hepatic and respiratoryadverse reactions associated with leflunomidereported to Health Canada are summarized inTable 1. Combined use of leflunomide and meth-otrexate is associated with an increased risk oftoxicity (3) and is not approved in Canada (7).Nevertheless, a number of the AR reports receiveddescribed concomitant use.
Concomitant use of leflunomide with DMARDs toxicto liver and bone marrow is not advisable, as suchtherapy can lead to additive or even synergistictoxicity (3). Strict vigilance in monitoring liver andbone marrow function is recommended for allpatients prescribed leflunomide, particularly if usedwith other medications associated with increasedrisk of hepatic or haematologic reactions (3).
Recommended monitoring parameters are asfollows (3):
• Alanine aminotransferase and aspartate ami-notransferase levels before treatment withleflunomide and at monthly or more frequentintervals during the first 6 months, and every 8weeks thereafter.
• A complete blood count, including differentialwhite blood cell count and platelet count, beforetreatment with leflunomide and every 2 weeks forthe first 6 months, and every 8 weeks thereafter.
It is important to note that, if a severe undesirableeffect occurs during treatment with leflunomide, thewashout procedures outlined in the product mono-graph should be followed in order to clear the activemetabolite from the body. These washout proce-dures should also be followed when changingtherapy from leflunomide to another DMARD, sincethe possibility of additive risks of ARs exists for along time after switching (3).
Health care professionals are reminded that treat-ment with leflunomide may have serious hepatic,haematologic and respiratory effects (4) and thatthese risks may be increased with concomitantmethotrexate use.
Lili Loorand-Stiver, and Mano Murty, CanadianAdverse Reaction Newsletter. 12(4), (2002). http://www.hc-sc.gc.ca/hpb-dgps/therapeut/htmleng/publicat.html www.hc-sc.gc.ca/hpb/onhp)
References
1. Kremer, J. Rational use of new and existing disease-modifying agents in rheumatoid arthritis. Annals of InternalMedicine, 134(8):695–706 ( 2001).
2. Schuna, A., Megeff, C. New drugs for the treatment ofrheumatoid arthritis. American Journal of Health Systemsand Pharmacy, 57:225–237 ( 2000).
3. Arava, leflunomide tablets [product monograph]. Laval(QC): Aventis Pharma Inc. 2001.
4. Adverse Drug Reactions Advisory Committee(ADRAC). Leflunomide: serious hepatic, blood, skin andrespiratory reactions. Australian Adverse Drug ReactionsBulletin, 20(2):7 (2001). http://www.health.gov.au/tga/adr/aadrb.htm.
5. European Agency for the Evaluation of MedicinalProducts. EMEA public statement on leflunomide(Arava®): pancytopenia and serious skin reactions [docref EMEA/31637/99] (1999) http://www.emea.eu.int/htms/human/drugalert/drugalert.htm
6. European Agency for the Evaluation of MedicinalProducts. EMEA public statement on leflunomide (Arava):severe and serious hepatic reactions [doc ref EMEA/5611/01/en] (2001). http://www.emea.eu.int/htms/human/drugalert/drugalert.htm
7. Important safety information on Arava: severe andserious hepatic reactions. Laval (QC): Aventis Pharma Inc(2001). http://www.hc-sc.gc.ca/hpb-dgps/therapeut/zfiles/english/advisory/industry/leflunomide_arava_e.html
Herbal mixture and palpitationsA 30-year-old man who had taken Aphrodite®
tablets (a herbal mixture of dry extracts of Tribulusterrestris (40 mg), Cinnamomum zeylanicum (11mg), Zingiber officinal (12 mg) and Crocus sativus(3 mg)) for his impotence problem (one tablet every8 hour for 2 days) complained of rapid heartbeat.On examination, minor systolic hypertension wasobserved. The patient had no previous history ofcardiovascular problems and was not under anyother treatment. One day after stopping the use ofAphrodite®, the palpitation was fully cleared.
All components of Aphrodite® have shown benefit inthe treatment of male impotence, however theexact mechanism of this action is not known. T.terrestris as a herbal remedy that has been used intraditional medicine as a tonic with aphrodisiacactivity and C. zeylanicum has well-defined aphro-disiac properties in traditional medicine (1). C.sativum has the same properties. Z. officinal has
Safety Information

225
WHO Drug Information Vol. 16, No. 3, 2002
shown to be cardiotonic/inotropic with peripheralvasodilatory activity added to its aphrodisiac action(2) which may be the main cause of palpitationobserved in this patient. It was concluded thatAphrodite® should be used with caution in patientswith a history of cardiovascular disease.
Ebrahim Zabihi, Mohammad Abdollahi, Tehran Drug &Poison Information Center, Ministry of Health & MedicalEducation, Tehran, Iran.
References
1. Medicinal Herbal. Perham M., Sawyer K. (eds), 2nd ed.,Dorling & Kindersley, 2000, pp: 52,184,223.
2. Information and Indications of Iranian Official HerbalMedicines. Iranian Ministry of Health and Medical Educa-tion, Razi Darou Gostar Publications, 2001, Page: 17.
Indapamide and hyponatraemiaAn article recently published in the Medical Journalof Australia describes hyponatraemia in associationwith the non-thiazide diuretic, indapamide. Mar-keted in the mid-1980s in Australia, indapamide isthe most commonly reported cause of hyponatrae-mia with 164 reports.
*Spontaneous monitoring systems are useful in detecting signals of relatively rare, serious and unexpected adversedrug reactions. A signal is defined as "reported information on a possible causal relationship between an adverse eventand a drug, the relationship being unknown or incompletely documented previously. Usually, more than a single reportis required to generate a signal, depending upon the seriousness of the event and the quality of the information". Allsignals must be validated before any regulatory decision can be made.
Safety Information
Of these 164 reports, 68 also described hypokalae-mia. Over half described accompanying symptomsincuding confusion, nausea, vomiting, dizziness,anorexia, malaise, fatigue, syncope, somnolenceand convulsions. Most patients were 65 years oldor over and 82% were female. Many of the reportsdocumented a serum sodium concentration, and in75 cases the concentration was less than or equalto 120 mmol/L.
Despite the fact that hyponatraemia can complicatetreatment with any diuretic medication, the Austral-ian Drug Reactions Advisory Committee, ADRAC,continues to recieve reports of the association. Inthe first 5 months of 2002, there have been 18reports. It should also be noted that indapamide ispresent in combination with perindopril. ADRACrecommends that indapamide should be usedcautiouslz and changes in conscious or mentalstate should prompt measurement of serum sodiumconcentration.
References
1. Chapman, M.D., Hanrahan, R. McEwen, J et al. Hy-ponatraemia and hypokalaemia due to indapamide.Medical Journal of Australia, 176: 219–221 (2002).
2. Australian Adverse Drug Reaction Bulletin, August2002.

226
WHO Drug Information Vol. 16, No. 3, 2002
Regulatory and Safety Action
has been reported only after chronic use of epoetinin patients with renal failure. In a series of 82 casesreported by the FDA, PRCA developed after theuse of epoetin alfa from 1 month to 5 years.
The Australian Adverse Drug Reactions Committeehas received 12 reports of PRCA associated withepoetin alfa (Eprex®) use.
Anti-erythropoietin antibodies which develop in thiscondition cross react with other erythropoietinproducts, including darbepoetin (Aranesp®). Thisproduct has been available in Australia since No-vember 2001, experience is limited and it is notknown whether PRCA will develop.
The sponsor of Eprex ® has issued a letter recom-mending intravenous use where feasible. In pa-tients with worsening anaemia, other causes shouldbe excluded. If PRCA is suspected, it should beconfirmed with antibody testing and/or bone marrowexamination. Epoetin alfa should be discontinuedand patients should not be switched to anothererythropoietin. PRCA may respond to immunosup-pressive therapy (3).
References
1. Casadevail, N., Nataf, J., Viron, B. et al. Pure red-cellaplasia and Anti-erythropoietin antibodies in patientstreated with recombinant erythropoietin. New EnglandJournal of Medicine, 346: 469–475 (2002) .
2. Gershon, S.K., Lukshenburg, H., Coté, T.R. et al. Purered-cell aplasia and Anti-erythropoietin antibodies inpatients treated with recombinant erythropoietin. NewEngland Journal of Medicine, 346: 1584–1586 (2002) .
3. Australian Adverse Drug Reactions Bulletin, August2002.
Ergot-derived dopamine receptoragonists: fibrotic reactionsUnited Kingdom — Pergolide, bromocriptine,cabergoline, and lisuride are ergot-deriveddopamine receptor agonists indicated for the man-agement of Parkinson's disease. Fibrotic reactionsare recognized adverse events of ergot derivatives.
Epoetin alfa: pure red cell aplasiaUnited Kingdom — Epoetin alfa (Eprex®) isindicated for the treatment of anaemia associatedwith chronic renal failure, cancer chemotherapy,autologous blood donation, and during major elec-tive orthopaedic surgery.
There have been 40 cases of confirmed or sus-pected pure red cell aplasia reported worldwide inchronic renal failure patients treated with epoetinalfa. The estimated reporting rate of this suspectedadverse reaction is less than 1:10 000 patientstreated.
Patients typically present with sudden worsening ofanaemia that is unresponsive to increasing dosesof erythropoietin. Such patients have detectableantibodies to erythropoietin in serum. Many do notrespond to alternative erythropoietins and becometransfusion dependent.
In patients developing epoetin alfa failure:
• Typical causes of non-response (e.g. iron, folateand B12 deficiency, aluminium intoxication, infec-tion or inflammation, blood loss, and haemolysis)should be investigated.
• If no cause is identified, a bone marrow examina-tion should be considered.
• If pure red cell aplasia is diagnosed, therapy withepoetin alfa must be discontinued and testing forerythropoietin antibodies should be considered.
• Appropriate therapy should be initiated and suchpatients should not be switched to another eryth-ropoietin.
Reference : Current Problems in Pharmacovigilance,Volume 28, April 2002..
Australia — Pure red cell aplasia (PRCA) is a rareadverse effect of epoetin alfa which has recentlybeen highlighted in an article and subsequent letterin the literature (1, 2). The condition results from thedevelopment of anti-erythropoietin antibodies,resulting in transfusion-dependant anaemia. PRCA

227
WHO Drug Information Vol. 16, No. 3, 2002 Regulatory and Safety Action
Suspected fibrotic reactions have been reported inthe UK: many at an advanced stage. Some casesrequired surgery and 3 patients died. Before start-ing treatment it may be appropriate to performbaseline investigations and a chest X-ray. If possi-ble, lung function tests should be performed. Pre-scribers of ergot derivatives should remember thatvarious symptoms and signs could arise fromfibrotic reactions which may cause unexplained orprogressive dyspnoea, pleuritic or pericardial pain,abdominal discomfort or distention, edema andrenal insufficiency.
Prognosis of fibrosis can be prevented by earlydiagnosis and cessation of drug treatment.
Reference : Current Problems in Pharmacovigilance,Volume 28, April 2002.
Buprenorphine approvedfor opiate dependenceUnited States of America — The Food and DrugAdministration has approved buprenorphine hydro-chloride (Subutex®) and buprenorphine hydrochlo-ride and naloxone hydrochloride (Suboxone®), forthe treatment of opiate dependence. These prod-ucts treat addiction by preventing symptoms ofwithdrawal from heroin and opiates.
The first product is intended for use at the begin-ning of treatment for drug abuse, and the second isa formulation used in maintenance treatment ofopiate addiction. Naloxone has been added toguard against intravenous abuse of buprenorphine.Both drugs are supplied in 2 mg and 8 mg tablets,to be dissolved under the tongue.
These products have been studied in over 2000patients and shown to be safe and effective treat-ments for opiate dependence. Side effects mostcommonly seen include cold and flu-like symptoms,headaches, sweating, sleeping difficulties, nauseaand mood swings. These effects usually peak at thebeginning of treatment and may last a number ofweeks. Clinical data indicate that the risk of seriousdiminished breathing may be less withbuprenorphine than with other opioids when used inhigh doses or in overdose situations. Nonetheless,buprenorphine has been associated with deathsdue to diminished breathing, especially when usedin combination with alcohol or other CNS depres-sant drugs.
The sponsor, in collaboration with the FDA, hasdeveloped a comprehensive risk managementprogramme designed to deter abuse and diversionfrom legitimate use, including limits on the numberof patients individual physicians are allowed to treatand special registration for the use of the drug. Theprogramme also provides surveillance systems toidentify if drugs are being abused, including inter-views monitoring, data collection and surveillanceefforts.
Reference : FDA Talk Paper, T02–38, October 2002.
Human tissue recalledUnited States of America — The Food and DrugAdministration has ordered Cryolife Inc. to recalldistributed human tissue processed since 3 Octo-ber 2001, since the FDA has determined thatCryolife cannot ensure that the tissue is free fromfungal and bacterial contaminants.
Tissue has been associated with the death of apatient in November 2001 who received a softtissue implant during reconstructive knee surgery.During its inspection of the company, FDA foundnumerous significant violations of regulations andissued a warning letter. The company had alsodistributed tissue from a donor after the presence ofharmful microorganisms in tissue samples from thesame donor had been confirmed.
Signs and symptoms of a bacterial or fungal infec-tion following a tissue transplant would usuallyappear within days to weeks and it is thereforeunlikely that patients are at future risk.
Current federal regulations for human tissue requirefirms to prepare, validate and follow written proce-dures to prevent infectious disease contaminationor cross contamination during processing.
Reference : FDA News, P02–27 August 2002.
Lepirudin and fatalanaphylactic reactionsEuropean Union — The European MedicinesEvaluation Agency (EMEA) has been informed of 7reports of severe anaphylactic reactions in patientsreceiving lepirudin (Refludan®). In 6 of these cases,the reaction occurred after re-exposure and 5 cases

228
WHO Drug Information Vol. 16, No. 3, 2002
were fatal. In several of the cases, Refludan® wasprescribed outside the approved therapeutic indica-tion.
Refludan® contains lepirudin, a recombinant hiru-din, which acts as a specific direct inhibitor of free-and clot-bound thrombin. It is indicated as ananticoagulant in adult patients suffering fromheparin-associated thrombocytopenia type II withthromboembolic disease mandating parenteralantithrombotic treatment. It was authorized in theEuropean Union in 1997 and is currently marketedin Austria, Belgium, Finland, France, Germany,Greece, Ireland, Spain, and United Kingdom.Approximately 35 000 people have been treated.
Physicians treating patients should consider care-fully the approved indications and the possibility ofallergic reactions.
Reference : EMEA Public Statement. EMEA/H/27717/02October 2002.
Valdecoxib: new warningsUnited States of America — The Food and DrugAdministration, together with the manufacturer ofvaldecoxib (Bextra®) are advising health careprofessionals about new warnings and informationin the product labelling.
Valdecoxib is a drug approved for treatment ofosteoarthritis, rheumatoid arthritis and dys-menorrhea (menstrual pain). The labelling is beingupdated with new warnings following postmarketingreports of serious adverse effects including life-threatening risks related to skin reactions — includ-ing Stevens Johnson Syndrome, and anaphylactoidreactions (serious allergic reactions). In addition,the labelling will state that the drug is contraindi-cated — not to be used — in patients allergic tosulfa containing products.
In November 2002, the manufacturer of Bextra®sent letters to health care professionals advisingthem of postmarketing reports and new warningsthat will be included in the drug label. Since the firmbegan marketing the drug in March of 2002, casesof serious skin and hypersensitivity reactions havebeen reported. These included cases of StevensJohnson syndrome, toxic epidermal necrolysis,exfoliative dermatitis and erythema multiforme.Although these adverse events are rare, some ofthese patients required hospitalization. Based on
these reports, FDA has approved labelling changesthat include a warning for serious skin reactions. Asthese reactions can be life threatening, people whoexperience a rash should discontinue the drugimmediately.
Reference : FDA Talk Paper, T02–43, 2002. http://www.fda.gov/medwatch/safety/3500.pdf
Parecoxib/valdecoxib: serioushypersensitivity reactionsEuropean Union — The European MedicinesEvaluation Agency (EMEA) has received informa-tion on reports of serious hypersensitivity reactions(anaphylaxis and angio-oedema) and serious skinreactions (Stevens-Johnson syndrome, toxic epi-dermal necrolysis, erythema multiforme and exfolia-tive dermatitis) in patients treated with valdecoxib(Bextra®, Valdyne®, Valdecoxib Pfizer andKudeq®, Valdecoxib Pharmacia Europe®) a selec-tive COX-2 inhibitor. Some of these reactions haveoccurred in patients with a history of allergic-typereactions to sulfonamides.
Valdecoxib is the active metabolite of parecoxibsodium (Dynastat®, Rayzon® and Xapit®) and it istherefore possible that such reactions may alsooccur with this substance.
As an urgent measure, prescribing and patientinformation have been modified.
Reference : EMEA Public Statement. EMEA/H/25175/02October 2002.
Mefloquine labelling strengthenedUnited States of America — Healthcare profes-sionals have been notified that mefloquine hydro-chloride (Lariam®) tablets are contraindicated inpatients with known hypersensitivity to mefloquineor related compounds. It should not be prescribedfor prophylaxis in patients with active depression, arecent history of depression, generalized anxietydisorder, psychosis, schizophrenia or other majorpsychiatric disorders or with a history of convul-sions.
Mefloquine is indicated for the treatment of mild tomoderate acute malaria caused by mefloquine-susceptible strains of Plasmodium Falciparum or P.vivax.
Regulatory and Safety Action
229
WHO Drug Information Vol. 16, No. 3, 2002
During prophylactic use, if psychiatric symptomssuch as acute anxiety, depression, restlessness orconfusion occur, these may be considered prodro-mal to a more serious event. In these cases, thedrug must be discontinued and an alternativemedication substituted.
References
1. Medwatch at http://www.fda.gov/medwatch/safetz/2002.
2. Communication from Roche Laboratories Inc., USA.September 2002
Glucowatch for diabetesUnited States of America — The Food and DrugAdministration (FDA) has approved a wrist-watch-like glucose monitoring device for use by childrenand adolescents with diabetes. The device, whichwas approved for adult use in March 2001, providesinformation that can be used to detect trends andtrack patterns in glucose levels.
The GlucoWatch G2 Biographer®, extracts fluidthrough the skin and then measures the glucose inthe fluid. Once the device has been warmed up andcalibrated through the use of a finger stick bloodglucose test, it is capable of providing up to sixpainless glucose measurements per hour for 13hours. The device sounds an alarm if the glucosereaches dangerous levels, alerting patients to apotential problem.
Although it is not a replacement for standard fingerstick blood tests, this device can help improve thequality of life of children with diabetes. These typesof products may one day completely eliminate theneed for daily finger-prick blood tests. Currently theGlucoWatch measurements must be used alongwith finger stick blood tests to ensure accurateresults.
Approval of the GlucoWatch® was based on resultsof a study that evaluated use in 66 Type-I diabeticsbetween ages 7 and 17. The study was conductedat a clinic in a home-simulated environment wherethe participants could go about various normal dailyactivities. The study showed that the product wassafe and effective for detecting trends and trackingpatterns in glucose levels in children and adoles-cents.
Although measurements are generally consistentwith those of traditional finger-stick blood glucosetests, results can differ significantly. Because thesevariations are unpredictable, individual Gluco-Watch® readings should never be used to makechanges in insulin dose. Instead, results should beinterpreted with several sequential readings overtime and then confirmed with a finger stick test.Diabetes is a chronic disease that affects thebody’s ability to produce or respond to insulin. Thiscan cause wide fluctuations in blood glucose levels,from extremely high to extremely low.
More than 150 000 children in the United Stateshave diabetes. While there is no known cure,studies have shown that patients who regularlymonitor and regulate their blood glucose levelshave a lower incidence of complications from thedisease. Uncontrolled, diabetes can result in suchserious outcomes as blindness, serious infection,amputation of limbs, coma, and death.
Reference : FDA News, P02–29 2002.
Generic omeprazole approvedUnited States of America — The Food and DrugAdministration has approved 10 and 20 mgomeprazole delayed-release capsules for thetreatment of certain gastro-intestinal conditions.The generic drug is identical to the brand namedrug in dosage form, strength, route of administra-tion and most labelled uses.
Although generic drugs are chemically identical totheir branded counterparts, they are typically sold atsubstantial discounts from the branded price. Togain FDA approval, a generic drug must:
• contain the same active ingredients as the innova-tor drug (inactive ingredients may vary)
• be identical in strength, dosage form, and route ofadministration
• have some of the same use indications
• be bioequivalent (Generic drugs use the sameactive ingredients and are shown to work thesame way in the body. Therefore they have thesame risk-benefit profile as their brand-namecounterparts.)
Regulatory and Safety Action

230
WHO Drug Information Vol. 16, No. 3, 2002
• meet the same batch requirements for identity,strength, purity, and quality
• be manufactured under the same strict standardsof FDA’s good manufacturing practice regulationsrequired for innovator products
Reference : FDA News, P02–45 2002.
Oxaliplatin for colorectal cancerUnited States of America — The Food and DrugAdministration has approved oxaliplatin injection(Eloxatin®) for use in combination with infusional 5-fluorouracil and leucovorin for the treatment ofpatients with colorectal cancer whose disease hasrecurred or become worse following initial therapywith a combination of irinotecan with bolus 5-fluorourcil and leucovorin. The combination includ-ing oxaliplatin was shown to shrink tumours insome patients and delay resumed tumour growth.There are as yet no data on the effects of thecombination on survival.
The FDA review took just seven weeks to completeunder the "rolling review" procedures of fast trackapproval. Fast track is used for drugs in develop-ment having the potential to be an advance intreatment for a serious illness and the rolling reviewprocedure allows for some components of anapplication to be presented before the remainingsections are completed. Completion of all sectionstook place in June 2002.
Oxaliplatin is intended for use by physicians experi-enced in the use of cancer agents and a black boxwarning details this use together with informationon possible anaphylactic reactions. Oxaliplatin canhave a toxic effect on nerve endings that may resultin either an acute or cumulative pattern of sideeffects. Other common side effects include vomit-ing, diarrhoea, anaemia, increased risk of bleedingor infection, or allergic reaction. Women should beadvised to avoid becoming pregnant.
Reference : FDA News, P02–25, 2002.
Ergotamine and ischaemiaUnited States of America — Recent changeshave been announced to the prescribing informa-tion for ergotamine tartrate and caffeine
Regulatory and Safety Action
(Cafergot®) suppositories and tablets, which in-clude a new warning on interactions with potentCYP 3A4 inhibitors.
Co-administration of ergotamine with potent CYP3A4 inhibitors (ritonavir, nelfinavir, indinavir, eryth-romycin, clarithromycin, and troleandomycin) hasbeen associated with acute ergot toxicity (ergotism)characterized by vasospasm and ischemia of theextremities, with some cases resulting in amputa-tion. There have been rare reports of cerebralischemia in patients on protease inhibitor therapywhen ergotamine tartrate and caffeine was co-administered, with at least one case resulting indeath. Because of the increased risk for ergotismand other serious vasospastic adverse events,ergotamine use is contraindicated with these drugsand other potent inhibitors of CYP 3A4 (e.g.,ketoconazole, itraconazole).
Reference : Communication from Novartis Pharmaceuti-cals Corporation dated October 2002, available on http://www.accessdata.FDA.gov/scripts/medwatch
Acetylsalicylic acid and Reye'ssyndromeUnited Kingdom — Reye's syndrome is a veryrare but often fatal disease characterized by en-cephalopathy and fatty degeneration of the liver. Ithas mostly affected children aged less than 5 yearsbut also occurs in older children and teenagers.The causes of Reye's syndrome are incompletelyunderstood, but an association with use of acetyl-salicylic acid in the presence of a viral infection hasbeen implicated in many cases.
Sporadic cases continue to be reported and theCommittee on Safety of Medicine now advises thatacetylsalicylic acid (Aspirin®) should not be given tochildren under 16 years of age unless specificallymedically advised.
References
1. Current Problems in Pharmacovigilance, Volume 28,April 2002.
2. Current Problems in Pharmacovigilance, Volume 28,October 2002. http://www.mca.gov.uk
231
WHO Drug Information Vol. 16, No. 3, 2002
Sertraline interactionsUnited States of America — A change in theprescribing information for sertraline hydrochloridetablets and oral concentrate (Zoloft®) has beenannounced by the manufacturer. This change wasmade at the request of the Food and Drug Adminis-tration and articulates a pimozide/sertraline interac-tion demonstrated by a phase I study. The prescrib-ing information now states that concomitant use inpatients taking monoamine oxidase inhibitors(MAOIs) or pimozide is contraindicated.
The study compared the disposition of intrave-nously administered diazepam before and after 21days of dosing with either Zoloft® (50 to 200 mg/day escalating dose) or placebo. There was a 32%decrease relative to baseline in diazepam clear-ance for the ZOLOFT group compared to a 19%decrease relative to baseline for the placebo group(p<0.03). There was a 23% increase in Tmax fordesmethyldiazepam in the Zoloft® group comparedto a 20% decrease in the placebo group (p<0.03).The clinical significance of these changes is un-known.
In a placebo-controlled trial in normal volunteers,the administration of two doses of Zoloft® did notsignificantly alter steady-state lithium levels or therenal clearance of lithium. Nonetheless, at this time,it is recommended that plasma lithium levels bemonitored following initiation of therapy with appro-priate adjustments to the lithium dose.
In a controlled study of a single dose (2 mg) ofpimozide, 200 mg sertraline (q.d.) co-administrationto steady state was associated with a mean in-crease in pimozide AUC and Cmax of about 40%,but was not associated with any changes in EKG.Since the highest recommended pimozide dose(10 mg) has not been evaluated in combination withsertraline, the effect on QT interval and PK param-eters at doses higher than 2 mg at this time are notknown. While the mechanism of this interaction isunknown due to the narrow therapeutic index ofpimozide and due to the interaction noted at a lowdose of pimozide, concomitant administration ofsertraline hydrochloride and pimozide should becontraindicated
The risk of using sertraline hydrochloride in combi-nation with other CNS active drugs has not beensystematically evaluated. Consequently, caution isadvised if concomitant administration with suchdrugs is required.
Regulatory and Safety Action
There is limited controlled experience regarding theoptimal timing of switching from other drugs effec-tive in the treatment of major depressive disorder,obsessive-compulsive disorder, panic disorder,post-traumatic stress disorder, and premenstrualdysphoric disorder to sertraline hydrochloride. Careand prudent medical judgment should be exercisedwhen switching, particularly from long-actingagents. The duration of an appropriate washoutperiod which should intervene before switchingfrom one selective serotonin re-uptake inhibitor(SSRI) to another has not been established.
Sertraline hydrochloride was launched in 1992 forthe treatment of major depressive disorder. It isalso approved for the treatment of panic disorder,obsessive-compulsive disorder (OCD), post-trau-matic stress disorder (PTSD), and premenstrualdysphoric disorder (PMDD). It has been shown tobe safe in the long-term treatment of paediatricOCD.
Sertraline hydrochloride is the only SSRI approvedfor the long-term treatment of PTSD. Over the pastdecade, sertraline hydrochloride has been used formore than 10.2 billion patient days of therapyworldwide (IMS data).
Reference : Communication from Pfizer Inc. Posted as aMedwatch Safety Alert on 19 November 2002. http://www.accessdata.FDA.gov/scripts/medwatch
Inhaled corticosteroidsand adrenal suppression
United Kingdom — The Committee on Safety ofMedicines (CSM) has reminded prescribers thatadrenal suppression is a well-established adversereaction of all inhaled corticosteroids. There havebeen rare reports of adrenal suppression leading toadrenal crisis. Symptoms and signs may be under-recognized, particularly in children receiving higherthan licensed doses of inhaled corticosteroids. TheCSM has recently reviewed evidence, includingspontaneously reported adverse drug reactions anda recent national survey of adrenal crisis due toinhaled corticiosteroids.
Presenting symptoms of adrenal suppression andcrisis are non-specific and include anorexia, ab-dominal paid, weight loss, tiredness, headache,nausea, vomiting, decreased level of conscious-ness, hypoglycaemia and seizures. Situationswhich may trigger acute adrenal crisis include
232
WHO Drug Information Vol. 16, No. 3, 2002
infection, trauma, surgery or any rapid reduction indosage. These are dose related class effects, andprescribers are strongly advised that the licenseddosages of all inhaled corticosteroids should not beexceeded in paediatric patients.
Reference : Current Problems in Pharmacovigilance,Volume 28, October 2002.
Re-introduction of urokinaseUnited States of America — The Food and DrugAdministration recently approved the re-introductionof urokinase (Abbokinase®) onto the market.Urokinase has been used for more than 20 yearsby an estimated four million patients.
As a result of a review of previous use, the productis now indicated solely for the treatment of pulmo-nary embolism; lysis of massive pulmonary emboliand pulmonary emboli accompanied by unstablehaemodynamics.
Information has been added to the labelling regard-ing post-marketing reports of anaphylaxis and otherinfusion reactions, as well as class informationregarding the potential for cholesterol embolization.
Reference : Communication from Abbott Laboratoriesdated 10 October 2002 on http://www.fda.gov/medwatch
Ezetimibe approvedfor cholesterol-loweringUnited States of America — The Food and DrugAdministration has approved ezetimibe (Zetia®), anew class of lipid-lowering compounds that selec-tively inhibits the intestinal absorption of cholesteroland related phytosterols.
Ezetimibe is effective in reducing total-C, LDL-C,Apo B and TG and increases HDL-C in patientswith hypercholesterolaemia when administered withan HMG-CoA reductase inhibitor. It reduces bloodcholesterol by inhibiting the absorption of choles-terol by the small intestine. Compared to placebo,ezetimibe had no clinically meaningful effect onplasma concentrations of the fat soluble vitamins A,D and E and did not impair adrenocortical steroidhormone production.
Ezetimibe is contraindicated in patients with activeliver disease or unexplained persistent elevations inserum transaminases. All HMG-CoA reductaseinhibitors are contraindicated in pregnancy.
Reference : Data sheet for Ezetimibe available on http://www.fda.gov
Regulatory and Safety Action
233
WHO Drug Information Vol. 16, No. 3, 2002
ATC/DDD Classification
WHO Collaborating Centre for Drug Statistics Methodology:Proceedings of the twentieth anniversry symposium:
In March 2002, the WHO Collaborating Centre for Drug Statistics Methodology celebrated its Twentiethanniversary in Oslo, Norway. The celebration was organized around a scientific symposium in parallel withthe Eleventh meeting of the WHO International Working Group for Drug Statistics Methodology.Presentations were made by members of the Working Group, the World Health Organization, Ministry ofHealth, Norway, and the Norwegian Institute of Public health. An important aim of the the symposium wasto applaud the work and achievements of the WHO Collaborating Centre in drug utilization research andrational use of drugs.
A historical overview of theATC/DDD methodology
Marit Rønning, WHO Collaborating Centre forDrug Statistics Methodology, Norway
Drug utilization research has attracted increasedattention since its early beginnings in the 1960s. Abreakthrough study on drug consumption during theperiod 1966–1967, pioneered by the WHO Re-gional Office for Europe, pointed to the differencesin drug utilization between population groups in sixEuropean countries (1). In 1969, a WHO sympo-sium declared the need for an internationally ac-ceptable classification system. It was at this timethat the Drug Utilization Research Group (DURG)was established and entrusted with development ofdrug utilization research methods. Inspired by thisinterest, a system named the Anatomical Therapeu-tic Chemical (ATC) classification was developed inNorway as a modification and extension of theEuropean Pharmaceutical Market Research Asso-ciation (EPhMRA) classification system.
In order to measure drug use, it is essential to haveboth a classification system and a unit of measure-ment. To deal with the drawbacks of traditionalunits of measurement, a technical unit of measure-ment called the Defined Daily Dose (DDD) wasdeveloped for use in drug utilization studies. Thisunit was defined as the assumed average mainte-nance dose per day for a drug when used for itsmain indication in adults.
The ATC/DDD system rapidly expanded to includemost drugs on the Nordic market. The NordicStatistics on Medicines was published using theATC/DDD methodology for the first time in 1976.Meanwhile, international interest in the ATC/DDDsystem for drug utilization research was expandingbeyond the Nordic countries, largely through activityof the DURG.
In 1981, the WHO Regional Office for Europeformally recognized the ATC/DDD system for drugutilization studies and, in 1982, the WHO Collabo-rating Centre for Drug Statistics Methodology at theNorwegian Medicinal Depot (NMD) was designatedby WHO and financed by the Norwegian Govern-ment. In 1996, WHO recognized the need tostrengthen the ATC/DDD system as an interna-tional standard and responsibility for the Centrewas transferred to WHO Headquarters in Geneva.This was seen as an important step in the linkbetween international drug utilization studies andWHO’s initiatives to promote access to essentialdrugs and the rational use of drugs. Provision ofindependent, validated information on drug use isessential to identify problems and needs for educa-tional or other interventions and before monitoringof drug utilization patterns can take place.
In January 2002, the Centre was relocated to theNorwegian Institute of Public Health. According tothe agreement between WHO and the Norwegiangovernment, the Centre’s main responsibilities arefocused around development and maintenance ofthe ATC/DDD system, including:
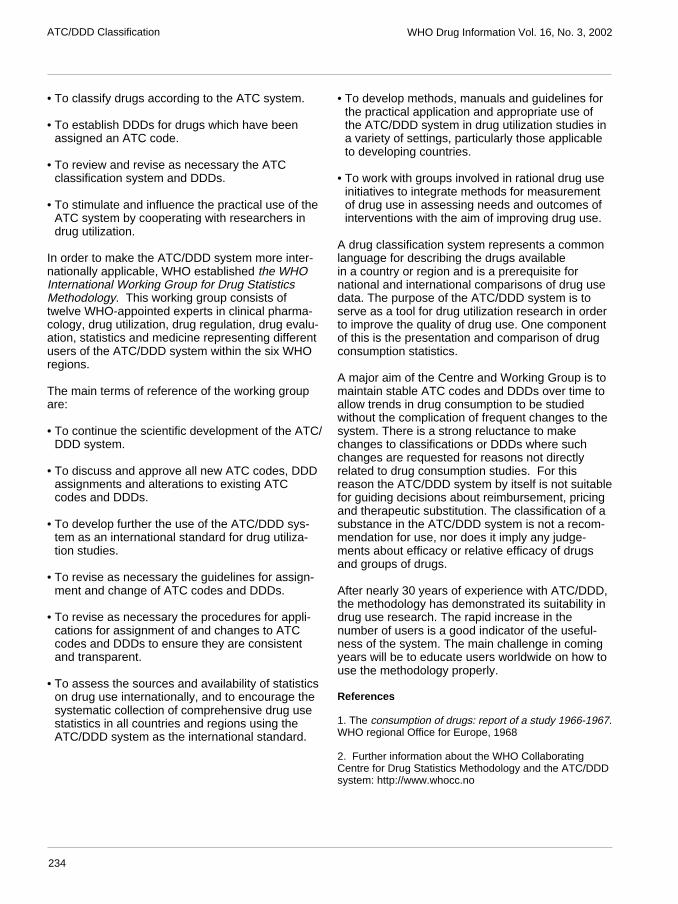
234
WHO Drug Information Vol. 16, No. 3, 2002
• To classify drugs according to the ATC system.
• To establish DDDs for drugs which have beenassigned an ATC code.
• To review and revise as necessary the ATCclassification system and DDDs.
• To stimulate and influence the practical use of theATC system by cooperating with researchers indrug utilization.
In order to make the ATC/DDD system more inter-nationally applicable, WHO established the WHOInternational Working Group for Drug StatisticsMethodology. This working group consists oftwelve WHO-appointed experts in clinical pharma-cology, drug utilization, drug regulation, drug evalu-ation, statistics and medicine representing differentusers of the ATC/DDD system within the six WHOregions.
The main terms of reference of the working groupare:
• To continue the scientific development of the ATC/DDD system.
• To discuss and approve all new ATC codes, DDDassignments and alterations to existing ATCcodes and DDDs.
• To develop further the use of the ATC/DDD sys-tem as an international standard for drug utiliza-tion studies.
• To revise as necessary the guidelines for assign-ment and change of ATC codes and DDDs.
• To revise as necessary the procedures for appli-cations for assignment of and changes to ATCcodes and DDDs to ensure they are consistentand transparent.
• To assess the sources and availability of statisticson drug use internationally, and to encourage thesystematic collection of comprehensive drug usestatistics in all countries and regions using theATC/DDD system as the international standard.
• To develop methods, manuals and guidelines forthe practical application and appropriate use ofthe ATC/DDD system in drug utilization studies ina variety of settings, particularly those applicableto developing countries.
• To work with groups involved in rational drug useinitiatives to integrate methods for measurementof drug use in assessing needs and outcomes ofinterventions with the aim of improving drug use.
A drug classification system represents a commonlanguage for describing the drugs availablein a country or region and is a prerequisite fornational and international comparisons of drug usedata. The purpose of the ATC/DDD system is toserve as a tool for drug utilization research in orderto improve the quality of drug use. One componentof this is the presentation and comparison of drugconsumption statistics.
A major aim of the Centre and Working Group is tomaintain stable ATC codes and DDDs over time toallow trends in drug consumption to be studiedwithout the complication of frequent changes to thesystem. There is a strong reluctance to makechanges to classifications or DDDs where suchchanges are requested for reasons not directlyrelated to drug consumption studies. For thisreason the ATC/DDD system by itself is not suitablefor guiding decisions about reimbursement, pricingand therapeutic substitution. The classification of asubstance in the ATC/DDD system is not a recom-mendation for use, nor does it imply any judge-ments about efficacy or relative efficacy of drugsand groups of drugs.
After nearly 30 years of experience with ATC/DDD,the methodology has demonstrated its suitability indrug use research. The rapid increase in thenumber of users is a good indicator of the useful-ness of the system. The main challenge in comingyears will be to educate users worldwide on how touse the methodology properly.
References
1. The consumption of drugs: report of a study 1966-1967.WHO regional Office for Europe, 1968
2. Further information about the WHO CollaboratingCentre for Drug Statistics Methodology and the ATC/DDDsystem: http://www.whocc.no
ATC/DDD Classification

235
WHO Drug Information Vol. 16, No. 3, 2002
Drug utilization statisticsand health policy
Anne Kari Lande Hasle, Secretary General,Norwegian Ministry of Health
Drug utilization statistics are an indispensable toolto fulfil goals outlined in health policy. Pharmaceuti-cals are recognized as playing a major role inmaintaining health. In meeting health needs, me-dicinal drug policies need to be part of healthpolicies and use of drugs in a community shouldthus be consonant with overall health goals.Achieving quality use of drugs is a priority in bothdeveloping and developed countries
It should be underlined that drug utilization statisticsare an important tool in the planning, monitoringand assessment of national drug policies. Drugsare one of the most frequently used treatments fora majority of diseases and complaints. As an exam-ple, an average 60% of all general practitionerconsultations within Norway result in delivery of aprescription.
Availability of national data on drug use representsthe first step in improving the quality of drug use inthe population. In order to measure drug use, it isimportant to have a classification system and a unitof measurement. To meet this need, the AnatomicalTherapeutic Chemical (ATC) classification systemand the Defined Daily Dose (DDD) were developedin Norway in the early 1970s.
Norway has a long tradition of accurate wholesalestatistics on drugs and was the first country toproduce public drug statistics. Since 1977, thesestatistics have been published annually. This an-nual report contains complete information aboutdrug sales in Norway and offers a rough estimate ofwhat percentage of the population is receiving acertain drug treatment. Overall sales statistics are avaluable source of time trends and regional varia-tions in drug consumption, both within the countryand in comparison with others. Staff of the WHOCollaborating Centre in Oslo have also been re-sponsible for drug use statistics at the nationallevel. The centre is therefore a user of the method-ology that it is responsible for maintaining anddeveloping at the international level.
Although highly useful, the figures based on drugsales from wholesalers to pharmacies and hospitals
have certain limitations for our use in Norway. Thedata do not reveal facts about the users or theprescribers. Thus, we still need information on:
• How many people in the population are usingdrugs.
• Which age and gender.
• For how long, and in which doses, they use drugs.
There is, therefore, a further need to establish amore comprehensive statistical base which will givedeeper insight into prescribing and utilization ofdrugs in Norwegian society. To regulate and subse-quently evaluate the impact of a country’s nationaldrug policy for a more rational use of drugs, it isvital that the system designed to collect medicineconsumption data is set up at the level of individualpatients. However, studies of how drugs are actu-ally being used, and identification of determinantsfor change in patterns of use, can only be madeafter the drug has been launched on the market.
Therefore, the Norwegian Ministry of Health isconsidering the establishment of a new nationalregister based on computerized prescriptions fromall pharmacies in Norway. The initiative to seekmore detailed drug statistics came partly in re-sponse to changes in the infrastructure of theNorwegian drug market, when Norway became amember of The European Economic Association(EEA) in 1995.
In the future, importance will focus on analysis ofthe use of medications from a public health per-spective and an evaluation of other aspects ofpublic health in relation to drug expenditure. Therecommended prescription register in Norway willcover the entire population of 4.5 million inhabit-ants, and will clearly offer unique possibilities forresearch and a better knowledge base for nationaldecision-making in drug utilization.
The work of the WHO Centre represents an impor-tant basis for all types of drug utilization statistics.From January 2002, the Centre has been formallylocated at the Norwegian Institute of Public Health.This location will hopefully provide positive synergybetween the Centre and the new Institute. TheMinistry of Health in Norway considers it importantto secure optimal continuation of the good work ofthe Centre, particularly with regard to its independ-ent status.
ATC/DDD Classification

236
WHO Drug Information Vol. 16, No. 3, 2002
Trends in drug utilization researchin developing countries
Hans V. Hogerzeil, Policy, Access and Ra-tional Use, Department of Essential Drugs andMedicines Policy, World Health Organization
The price of essential medicines is growing. Forexample, gonorrhoea is increasingly resistant topenicillin: the new-generation antibiotics nowneeded to cure the disease are 50 to 90 times moreexpensive. New arthemether-based combinationmedicines against malaria are 25 times as expen-sive as chloroquine, the standard malaria treat-ment, even at the preferential rate for developingcountries negotiated by WHO. Other malaria combi-nation therapies can cost up to 200 times as muchas chloroquine. Six months of DOTS treatment foruncomplicated tuberculosis now costs less than$10 per person; but treatment for multidrug-resist-ant tuberculosis may be 100 times as expensive.
Thirty-eight countries have an annual medicinesbudget of less than $2 per person. But many ofthese countries are heavily hit by HIV/AIDS, forwhich antiretroviral treatment costs several hundreddollars per year. In view of these huge costs, thecareful selection of a treatment of choice for publicsupply systems or reimbursement purposes re-mains extremely important, both medically andeconomically.
Within WHO, the selection of essential medicines ismoving away from experience-based towardsevidence-based selection, or, as some like to call it,“from eminence-based to evidence-based”. At thesame time, considerations of efficacy of the drugare balanced by cost-effectiveness of the treatmentas a whole and, if possible, by marginal cost-effectiveness (comparing the additional benefit ineffectiveness or safety against the additional cost).
An example of this approach is the recent review byWHO and UNAIDS health economists of the cost-effectiveness of the various interventions in theprevention and treatment of HIV/AIDS (1). Forexample, the targeted distribution of condoms isvery cost-effective — at less than one dollar per lifeyear gained. Certain methods to ensure safe bloodtransfusion, the treatment of tuberculosis and theprevention of mother-to-child transmission of HIVwith nevirapine cost less than $100 per life yeargained. On the other hand, the treatment of someHIV opportunistic infections and combination treat-ment with antiretroviral medicines may cost severalhundreds of dollars per life year gained.
Early drug utilization studies, as practised in Nordiccountries for example, were usually based onaggregated drug use data from national or provin-cial sales reports or prescription data. These stud-ies tended to be purely descriptive which limitedtheir utility and were not always easy to translateinto action. In the early 1990s, WHO and the Inter-national Network for the Rational Use of Drugs(INRUD) developed and published a simple sam-pling method and a standard set of indicators todescribe core aspects of prescribing and dispens-ing (2). These indicators have proved extremelyuseful in screening the quality of care, identifyingproblem areas, making comparisons betweencountries and over time, and in measuring theimpact of interventions. The indicators are alsodescriptive but they can be targeted to certainpopulations, they cover other aspects of the qualityof care and they add quantitative measures. Theydescribe WHAT and HOW MUCH. For example, whatproportion of prescriptions in a given province orhospital contain one or more antibiotics.
Before one can hope to change a certain pattern ofirrational drug use it is essential to know why acertain type of behaviour is occurring. This could bethrough lack of knowledge, workload, patient de-mand, commercial pressure, financial incentives orany other reason. In order to know this, qualitativestudies are needed, usually based on observations,structured interviews, peer group discussion orother techniques. They describe the WHY of drugutilization. For example, why do doctors prescribeso many antibiotics?
When it is known why a certain prescribing behav-iour occurs, a targeted intervention may be started.But does it change anything? To know this, a druguse intervention study will be needed. Most of suchstudies use the WHO indicators mentioned abovewhich adequately cover most aspects of irrationaldrug use: polypharmacy, overuse of antibiotics andinjections, lack of generic prescribing and non-adherence to national or institutional essentialmedicines lists. These studies measure the effec-tiveness of the intervention and answer the ques-tion DOES IT WORK? Did the intervention actuallyreduce the percentage of prescription with one ormore antibiotics? And did the effect last? Did theeffect occur in the control group which was notsubject to the intervention?
And even that is not enough. A small-scale inter-vention in a research setting may be effective; butthat may be due to intensive planning and supervi-
ATC/DDD Classification

237
WHO Drug Information Vol. 16, No. 3, 2002
sion, for example. So management studies areneeded with a focus on the question is the interven-tion REPRODUCIBLE and is the intervention COST EFFEC-TIVE? The selection of policy decisions and manage-ment interventions is increasingly based on evi-dence of effectiveness and, preferably, cost-effectiveness. Probably the best study in this regardwas published by Guiscafré (3) in which he provedthat scaling up of an educational intervention in thetreatment of diarrhoea and respiratory infection inMexico was very cost-effective (savings amountedto 4.4 and 21.6 times the cost of the intervention,respectively).
The first International Conference on Improving theUse of Medicines (ICIUM) held in Chiang-Mai(Thailand) in 1997, systematically reviewed theinterventions in developing countries. Considerablegaps in research were identified, especially in thefield of improving drug use in hospital settings, inthe private sector and in the community; on inter-ventions to improve the use of antibiotics andantimalarial drugs; and the impact of drugs andtherapeutic committees and of financial incentives.It is hoped that ICIUM-2, which will again be held inChiang Mai, in April 2004, will identify more effec-tive interventions in these areas. The researchmethods are available.
References
1. Creese, A., Floyd, K., Alban, A. Cost-effectiveness ofHIV/AIDS interventions in Africa: a systematic review ofthe evidence. Lancet, 359: 1635–1642 (2002).
2. World Health Organization. How to investigate drug usein health facilities. Geneva: WHO, 1993. WHO/DAP/93.11
3. Guiscafré, H., Martinez, H. et al. From research topublic health interventions. I. Impact of an educationstrategy for physicians to improve treatment practices ofcommon diseases. Archives of Medical Research, 26Spec No: S31-39 (1995).
Drug utilization data constraintsin developing countries
Tariq Iqbal Bhutta, Professor of Paediatrics,Nishtar Medical College, Pakistan
Private expenditure on pharmaceuticals in develop-ing countries typically accounts for 50–90% of allspending on drugs. Even for rural populations andthe urban poor, the most common source of drugsis out-of-pocket purchase from the private market.On the other hand, sometimes as much as 50% of
the health budget of developing countries is usedfor buying drugs. Beyond these figures, very littledata is available on how drugs are utilized.
Drug provision and distribution usually rely on a mixof public and private services to ensure the regularsupply of essential drugs. Although drugs areavailable through both the public and private healthsystems, data on their use is either unavailable ortotally inadequate in most developing countries.In addition, it is known that up to 80% of the popula-tion in developing countries also use traditionalmedicine to help meet health care needs.
In developing countries, public health is affordedlittle interest or priority by the authorities and thereexists a further divide between urban and ruralareas. Although much of the population lives in therural areas, most of the health care budget is spentin the urban areas with the result that ruralpopulations lack access to the most basic servicesand to qualified medical practitioners. The doctor-patient ratio in rural areas is extremely low, with theresult that the majority of the population will seekcare from traditional health practitioners.
A large number of factors influence drug utilizationin these countries. Firstly, much depends upon thepriority that the health sector receives in the budget.It will also depend upon the medical needs anddemands of the population. For example, if there isa high incidence of HIV/AIDS, malaria, and tubercu-losis, this will reflect in the demand for drugs totreat these diseases. None the less, introduction ofnew drugs on the market and their sometimesaggressive marketing can significantly increasetheir use irrespective of actual need.
Drug utilization also responds to regulatory effortsand national drug policies, registration policies and— at a local level — by the existence of local drugcommittees. In most developing countries, thepublic sector's role in providing health care to thepopulation is shrinking and that of the private sectoris expanding. This is particularly true for the leastdeveloped countries of Africa as well as emergingmarket economies like India, Pakistan, and China.A decreasing government role in drug control isknown to have a marked influence on drug utiliza-tion.
Health professionals and their preferences are alsoplaying an ever-increasing role in determining whatdrugs are prescribed, marketed and even regis-tered. To a certain extent, cultural preferences may
ATC/DDD Classification
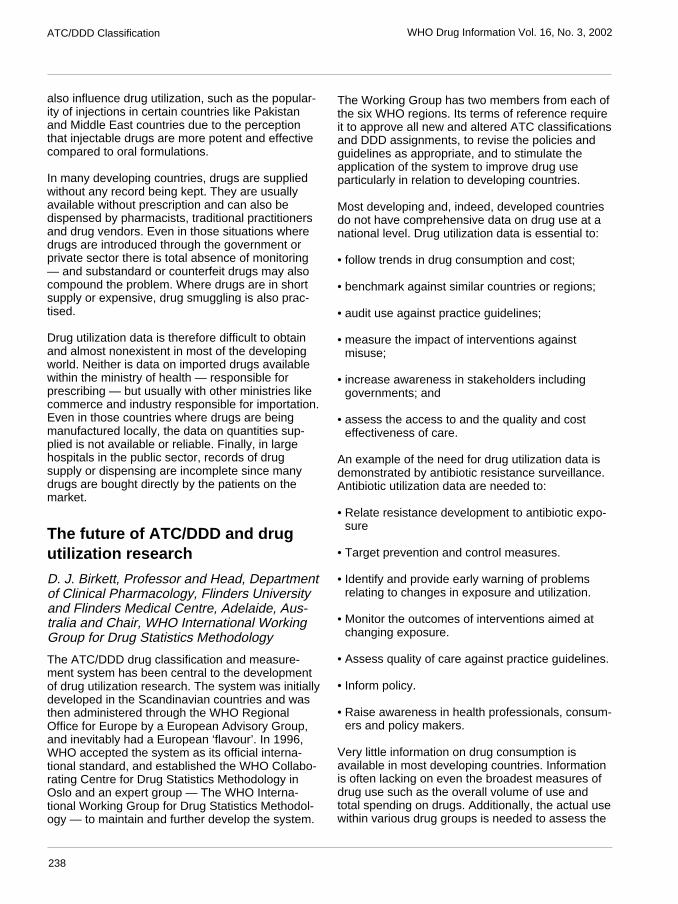
238
WHO Drug Information Vol. 16, No. 3, 2002
also influence drug utilization, such as the popular-ity of injections in certain countries like Pakistanand Middle East countries due to the perceptionthat injectable drugs are more potent and effectivecompared to oral formulations.
In many developing countries, drugs are suppliedwithout any record being kept. They are usuallyavailable without prescription and can also bedispensed by pharmacists, traditional practitionersand drug vendors. Even in those situations wheredrugs are introduced through the government orprivate sector there is total absence of monitoring— and substandard or counterfeit drugs may alsocompound the problem. Where drugs are in shortsupply or expensive, drug smuggling is also prac-tised.
Drug utilization data is therefore difficult to obtainand almost nonexistent in most of the developingworld. Neither is data on imported drugs availablewithin the ministry of health — responsible forprescribing — but usually with other ministries likecommerce and industry responsible for importation.Even in those countries where drugs are beingmanufactured locally, the data on quantities sup-plied is not available or reliable. Finally, in largehospitals in the public sector, records of drugsupply or dispensing are incomplete since manydrugs are bought directly by the patients on themarket.
The future of ATC/DDD and drugutilization research
D. J. Birkett, Professor and Head, Departmentof Clinical Pharmacology, Flinders Universityand Flinders Medical Centre, Adelaide, Aus-tralia and Chair, WHO International WorkingGroup for Drug Statistics Methodology
The ATC/DDD drug classification and measure-ment system has been central to the developmentof drug utilization research. The system was initiallydeveloped in the Scandinavian countries and wasthen administered through the WHO RegionalOffice for Europe by a European Advisory Group,and inevitably had a European ‘flavour’. In 1996,WHO accepted the system as its official interna-tional standard, and established the WHO Collabo-rating Centre for Drug Statistics Methodology inOslo and an expert group — The WHO Interna-tional Working Group for Drug Statistics Methodol-ogy — to maintain and further develop the system.
The Working Group has two members from each ofthe six WHO regions. Its terms of reference requireit to approve all new and altered ATC classificationsand DDD assignments, to revise the policies andguidelines as appropriate, and to stimulate theapplication of the system to improve drug useparticularly in relation to developing countries.
Most developing and, indeed, developed countriesdo not have comprehensive data on drug use at anational level. Drug utilization data is essential to:
• follow trends in drug consumption and cost;
• benchmark against similar countries or regions;
• audit use against practice guidelines;
• measure the impact of interventions againstmisuse;
• increase awareness in stakeholders includinggovernments; and
• assess the access to and the quality and costeffectiveness of care.
An example of the need for drug utilization data isdemonstrated by antibiotic resistance surveillance.Antibiotic utilization data are needed to:
• Relate resistance development to antibiotic expo-sure
• Target prevention and control measures.
• Identify and provide early warning of problemsrelating to changes in exposure and utilization.
• Monitor the outcomes of interventions aimed atchanging exposure.
• Assess quality of care against practice guidelines.
• Inform policy.
• Raise awareness in health professionals, consum-ers and policy makers.
Very little information on drug consumption isavailable in most developing countries. Informationis often lacking on even the broadest measures ofdrug use such as the overall volume of use andtotal spending on drugs. Additionally, the actual usewithin various drug groups is needed to assess the
ATC/DDD Classification
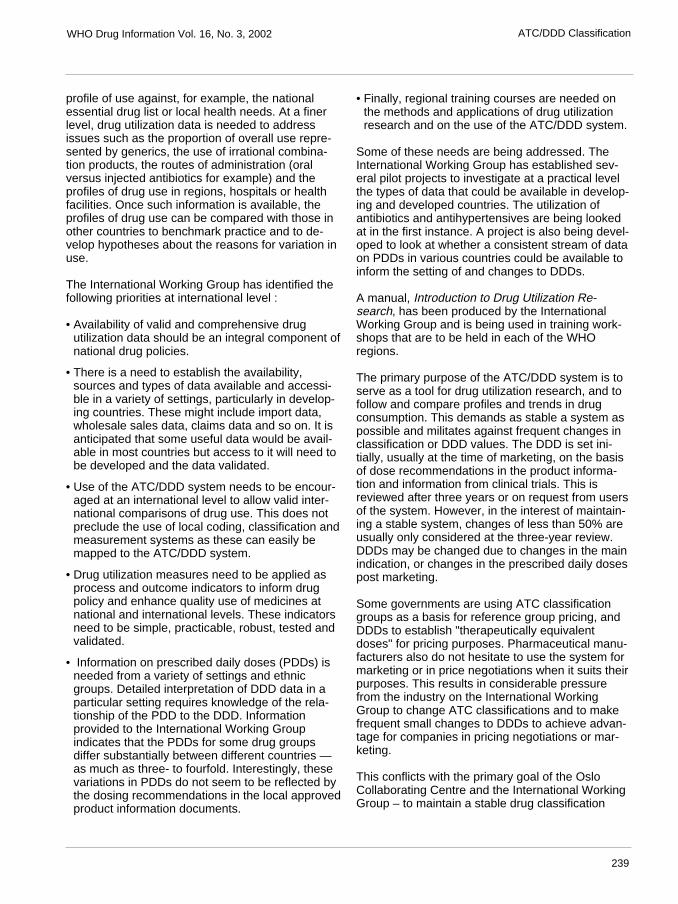
239
WHO Drug Information Vol. 16, No. 3, 2002
profile of use against, for example, the nationalessential drug list or local health needs. At a finerlevel, drug utilization data is needed to addressissues such as the proportion of overall use repre-sented by generics, the use of irrational combina-tion products, the routes of administration (oralversus injected antibiotics for example) and theprofiles of drug use in regions, hospitals or healthfacilities. Once such information is available, theprofiles of drug use can be compared with those inother countries to benchmark practice and to de-velop hypotheses about the reasons for variation inuse.
The International Working Group has identified thefollowing priorities at international level :
• Availability of valid and comprehensive drugutilization data should be an integral component ofnational drug policies.
• There is a need to establish the availability,sources and types of data available and accessi-ble in a variety of settings, particularly in develop-ing countries. These might include import data,wholesale sales data, claims data and so on. It isanticipated that some useful data would be avail-able in most countries but access to it will need tobe developed and the data validated.
• Use of the ATC/DDD system needs to be encour-aged at an international level to allow valid inter-national comparisons of drug use. This does notpreclude the use of local coding, classification andmeasurement systems as these can easily bemapped to the ATC/DDD system.
• Drug utilization measures need to be applied asprocess and outcome indicators to inform drugpolicy and enhance quality use of medicines atnational and international levels. These indicatorsneed to be simple, practicable, robust, tested andvalidated.
• Information on prescribed daily doses (PDDs) isneeded from a variety of settings and ethnicgroups. Detailed interpretation of DDD data in aparticular setting requires knowledge of the rela-tionship of the PDD to the DDD. Informationprovided to the International Working Groupindicates that the PDDs for some drug groupsdiffer substantially between different countries —as much as three- to fourfold. Interestingly, thesevariations in PDDs do not seem to be reflected bythe dosing recommendations in the local approvedproduct information documents.
• Finally, regional training courses are needed onthe methods and applications of drug utilizationresearch and on the use of the ATC/DDD system.
Some of these needs are being addressed. TheInternational Working Group has established sev-eral pilot projects to investigate at a practical levelthe types of data that could be available in develop-ing and developed countries. The utilization ofantibiotics and antihypertensives are being lookedat in the first instance. A project is also being devel-oped to look at whether a consistent stream of dataon PDDs in various countries could be available toinform the setting of and changes to DDDs.
A manual, Introduction to Drug Utilization Re-search, has been produced by the InternationalWorking Group and is being used in training work-shops that are to be held in each of the WHOregions.
The primary purpose of the ATC/DDD system is toserve as a tool for drug utilization research, and tofollow and compare profiles and trends in drugconsumption. This demands as stable a system aspossible and militates against frequent changes inclassification or DDD values. The DDD is set ini-tially, usually at the time of marketing, on the basisof dose recommendations in the product informa-tion and information from clinical trials. This isreviewed after three years or on request from usersof the system. However, in the interest of maintain-ing a stable system, changes of less than 50% areusually only considered at the three-year review.DDDs may be changed due to changes in the mainindication, or changes in the prescribed daily dosespost marketing.
Some governments are using ATC classificationgroups as a basis for reference group pricing, andDDDs to establish "therapeutically equivalentdoses" for pricing purposes. Pharmaceutical manu-facturers also do not hesitate to use the system formarketing or in price negotiations when it suits theirpurposes. This results in considerable pressurefrom the industry on the International WorkingGroup to change ATC classifications and to makefrequent small changes to DDDs to achieve advan-tage for companies in pricing negotiations or mar-keting.
This conflicts with the primary goal of the OsloCollaborating Centre and the International WorkingGroup – to maintain a stable drug classification
ATC/DDD Classification

240
WHO Drug Information Vol. 16, No. 3, 2002ATC/DDD Classification
system and utilization metric for use in studies ofdrug consumption. The system may be an accept-able starting point for drug reimbursement deci-sions but because it is established and maintainedfor a different purpose, it is not suitable as the solebasis for such decisions. Regulatory and reim-bursement decisions, even if using the ATC/DDDsystem as a starting point, have to be made at alocal level based on local regulatory and reimburse-ment policies and practices, and include considera-tions of local patterns and cultures of drug use.
Maintenance of the ATC/DDD system raises com-plex scientific and sensitive commercial issues. Theend result is not perfect, as it is inevitably a com-promise between scientific accuracy, a stablesystem and (unfortunately) commercial pressures.Nonetheless, it works well in practice, there is longexperience with its use, and it is endorsed by WHOas the international standard. Such an internationalsystem is necessary to allow valid internationalcomparisons of drug use patterns and trends tosupport quality use of medicines and better healthoutcomes. To achieve this, the challenge now is todevelop and validate sources of drug use informa-tion in a variety of settings at the international level.

241
WHO Drug Information Vol. 16, No. 3, 2002
Recent Publicationsand Sources of InformationInternational Ethical Guidelinesfor Biomedical ResearchInvolving Human SubjectsThis is the third in the series of international ethicalguidelines for biomedical research involving humansubjects issued by the Council for InternationalOrganizations of Medical Sciences (CIOMS) since1982. Its scope and preparation reflect the transfor-mation that has occurred in the field of researchethics and the changes to the Helsinki Declaration,upon which the guidelines are based. They particu-larly reflect the conditions and needs of biomedicalresearch within all countries and the implications forinternational research of both different cultures anduniversal ethical standards.
The mere formulation of ethical guidelines forbiomedical research will hardly resolve the doubtsthat can arise in the application of all research, butthe guidelines attempt to draw the attention ofsponsors, investigators and ethical review commit-tees to the need to consider carefully the ethicalimplications of research protocols and the conductof clinical trials. In this way, the highest possiblescientific and ethical standards may be achieved.
International Ethical Guidelines for Biomedical ResearchInvolving Human Subjects. Available from: Council forInternational Organizations of Medical Sciences (CIOMS),World Health Organization, Geneva. e-mail:[email protected]
Surveying and EvaluatingEthical Review PracticesEthical review provides essential guidance onconducting research and protection of trial subjects.The purpose of Surveying and Evaluating EthicalReview Practices is to facilitate and support proce-dures for quality and transparency in ethical review.The guideline is complementary to the earlierOperational Guidelines for Ethical Committees thatReview Biomedical Research, published in 2001 bythe Tropical Disease Research Programme (TDR)at the World Health Organization.
Monitoring and evaluation of ethical review prac-tices will contribute to strengthening of publicconfidence in research and clinical trial manage-ment by facilitating procedures for quality andtransparency and promoting good practices. Ethicalstandards underpinning such practices have beenestablished in international guidelines, including theHelsinki Declaration and the CIOMS InternationalEthical Guidelines for Biomedical Research Involv-ing Human Subjects.
There is growing national and international interestin ensuring that ethical review achieves the higheststandards in protecting individuals and communitiesalike and internal review of the ethical committee'soperations, such as self assessment checklists,also provides measures to evaluate performance.
Surveying and Evaluating Ethical Review Practices.Available from: Product Research and Development,TDR/CDS, World Health Organization, Geneva. e-mail:[email protected]
The Importance ofPharmacovigilanceThis document sets out to present the case for theimportance of pharmacovigilance, to record itsgrowth and potential as a discipline within medicalscience, and to describe its impact on patientwelfare and public health. It presents a criticalexamination of the strengths and weaknesses ofpresent systems of safety monitoring.
Pharmacovigilance — the detection, assessment,understanding and prevention of adverse drugreactions — involves the rapid transmission ofinformation on adverse drug reactions detected bymonitoring systems collecting international andnational data.
In order to meet the challenges of drug safetyneeds for the coming ten years, increase the impactof pharmacovigilance systems, and ensure thatthese deliver their benefits, an appraisal needs tobe made and collaboration and communication atlocal, regional and international levels strength-ened.
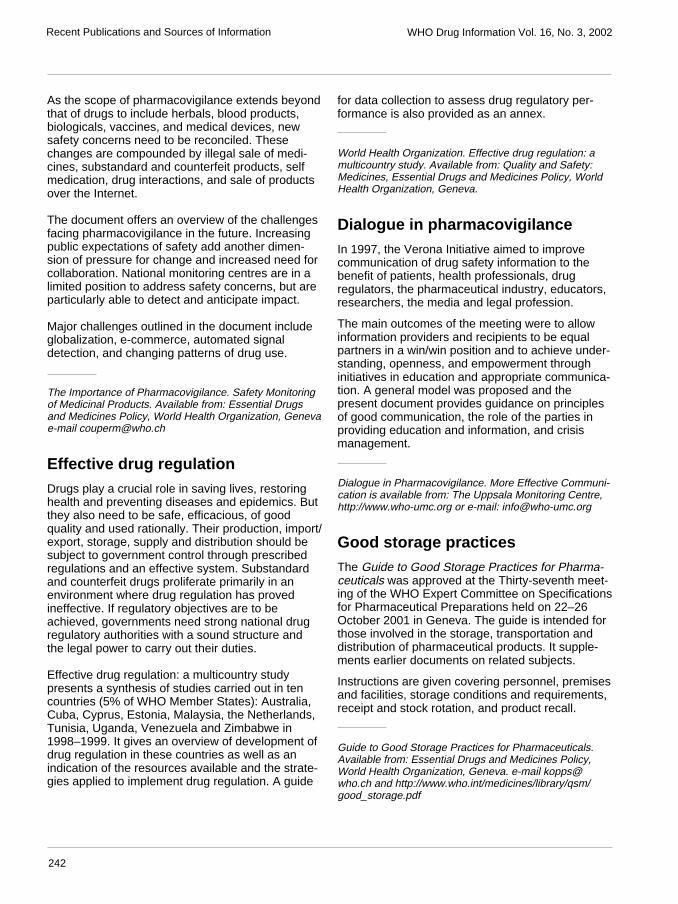
242
WHO Drug Information Vol. 16, No. 3, 2002Recent Publications and Sources of Information
As the scope of pharmacovigilance extends beyondthat of drugs to include herbals, blood products,biologicals, vaccines, and medical devices, newsafety concerns need to be reconciled. Thesechanges are compounded by illegal sale of medi-cines, substandard and counterfeit products, selfmedication, drug interactions, and sale of productsover the Internet.
The document offers an overview of the challengesfacing pharmacovigilance in the future. Increasingpublic expectations of safety add another dimen-sion of pressure for change and increased need forcollaboration. National monitoring centres are in alimited position to address safety concerns, but areparticularly able to detect and anticipate impact.
Major challenges outlined in the document includeglobalization, e-commerce, automated signaldetection, and changing patterns of drug use.
The Importance of Pharmacovigilance. Safety Monitoringof Medicinal Products. Available from: Essential Drugsand Medicines Policy, World Health Organization, Genevae-mail [email protected]
Effective drug regulationDrugs play a crucial role in saving lives, restoringhealth and preventing diseases and epidemics. Butthey also need to be safe, efficacious, of goodquality and used rationally. Their production, import/export, storage, supply and distribution should besubject to government control through prescribedregulations and an effective system. Substandardand counterfeit drugs proliferate primarily in anenvironment where drug regulation has provedineffective. If regulatory objectives are to beachieved, governments need strong national drugregulatory authorities with a sound structure andthe legal power to carry out their duties.
Effective drug regulation: a multicountry studypresents a synthesis of studies carried out in tencountries (5% of WHO Member States): Australia,Cuba, Cyprus, Estonia, Malaysia, the Netherlands,Tunisia, Uganda, Venezuela and Zimbabwe in1998–1999. It gives an overview of development ofdrug regulation in these countries as well as anindication of the resources available and the strate-gies applied to implement drug regulation. A guide
for data collection to assess drug regulatory per-formance is also provided as an annex.
World Health Organization. Effective drug regulation: amulticountry study. Available from: Quality and Safety:Medicines, Essential Drugs and Medicines Policy, WorldHealth Organization, Geneva.
Dialogue in pharmacovigilanceIn 1997, the Verona Initiative aimed to improvecommunication of drug safety information to thebenefit of patients, health professionals, drugregulators, the pharmaceutical industry, educators,researchers, the media and legal profession.
The main outcomes of the meeting were to allowinformation providers and recipients to be equalpartners in a win/win position and to achieve under-standing, openness, and empowerment throughinitiatives in education and appropriate communica-tion. A general model was proposed and thepresent document provides guidance on principlesof good communication, the role of the parties inproviding education and information, and crisismanagement.
Dialogue in Pharmacovigilance. More Effective Communi-cation is available from: The Uppsala Monitoring Centre,http://www.who-umc.org or e-mail: [email protected]
Good storage practicesThe Guide to Good Storage Practices for Pharma-ceuticals was approved at the Thirty-seventh meet-ing of the WHO Expert Committee on Specificationsfor Pharmaceutical Preparations held on 22–26October 2001 in Geneva. The guide is intended forthose involved in the storage, transportation anddistribution of pharmaceutical products. It supple-ments earlier documents on related subjects.
Instructions are given covering personnel, premisesand facilities, storage conditions and requirements,receipt and stock rotation, and product recall.
Guide to Good Storage Practices for Pharmaceuticals.Available from: Essential Drugs and Medicines Policy,World Health Organization, Geneva. e-mail [email protected] and http://www.who.int/medicines/library/qsm/good_storage.pdf

243
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
RECOMMENDED International Nonproprietary Names (Rec. INN): List 48
Notice is hereby given that, in accordance with paragraph 7 of the Procedure for the Selection of RecommendedInternational Nonproprietary Names for Pharmaceutical Substances [Off. Rec. Wld Health Org., 1955, 60, 3 (ResolutionEB15.R7); 1969, 173, 10 (Resolution EB43.R9)], the following names are selected as Recommended InternationalNonproprietary Names. The inclusion of a name in the lists of Recommended International Nonproprietary Names does notimply any recommendation of the use of the substance in medicine or pharmacy.Lists of Proposed (1–85) and Recommended (1–45) International Nonproprietary Names can be found in CumulativeList No. 10, 2002 (available in CD-ROM only).
Dénominations communes internationalesdes Substances pharmaceutiques (DCI)
Dénominations communes internationales RECOMMANDÉES (DCI Rec): Liste 48
Il est notifié que, conformément aux dispositions du paragraphe 7 de la Procédure à suivre en vue du choix de Dénominationscommunes internationales recommandées pour les Substances pharmaceutiques [Actes off. Org. mond. Santé, 1955, 60,3 (résolution EB15.R7); 1969, 173, 10 (résolution EB43.R9)] les dénominations ci-dessous sont choisises par l’Organisationmondiale de la Santé en tant que dénominations communes internationales recommandées. L’inclusion d’une dénominationdans les listes de DCI recommandées n’implique aucune recommandation en vue de l’utilisation de la substancecorrespondante en médecine ou en pharmacie.On trouvera d’autres listes de Dénominations communes internationales proposées (1–85) et recommandées (1–45)dans la Liste récapitulative No. 10, 2002 (disponible sur CD-ROM seulement).
Denominaciones Comunes Internacionalespara las Sustancias Farmacéuticas (DCI)
Denominaciones Comunes Internacionales RECOMENDADAS (DCI Rec.): Lista 48
De conformidad con lo que dispone el párrafo 7 del Procedimiento de Selección de Denominaciones ComunesInternacionales Recomendadas para las Sustancias Farmacéuticas [Act. Of. Mund. Salud, 1955, 60, 3 (ResoluciónEB15.R7); 1969, 173, 10 (Resolución EB43.R9)], se comunica por el presente anuncio que las denominaciones que acontinuación se expresan han sido seleccionadas como Denominaciones Comunes Internacionales Recomendadas. Lainclusión de una denominación en las listas de las Denominaciones Comunes Recomendadas no supone recomendaciónalguna en favor del empleo de la sustancia respectiva en medicina o en farmacia.Las listas de Denominaciones Comunes Internacionales Propuestas (1–85) y Recomendadas (1–45) se encuentranreunidas en Cumulative List No. 10, 2002 (disponible sólo en CD-ROM).
International Nonproprietary Names forPharmaceutical Substances (INN)

244
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
Latin, English, French, Spanish:Recommended INN Chemical name or description; Molecular formula; Graphic formula
DCI Recommandée Nom chimique ou description; Formule brute; Formule développée
DCI Recomendada Nombre químico o descripción; Fórmula empírica; Fórmula desarrollada
acolbifenumacolbifene (+)-(2S)-3-(4-hydroxyphenyl)-4-methyl-2-[4-[2-(piperidin-
1-yl)ethoxy]phenyl]-2H-1-benzopyran-7-ol
acolbifène (+)-(2S)-3-(4-hydroxyphényl)-4-méthyl-2-[4-[2-(pipéridin-1-yl)éthoxy]phényl]-2H-1-benzopyran-7-ol
acolbifeno (+)-(2S)-3-(4-hidroxifenil)-4-metil-2-[4-[2-(piperidin-1-il)etoxi]fenil]-2H-1-benzopiran-7-ol
C29H31NO4
O
CH3
HO
ON
OH
H
asoprisnilumasoprisnil 11β-[4-[(E)-(hydroxyimino)methyl]phenyl]-17β-methoxy-
17-(methoxymethyl)estra-4,9-dien-3-one
asoprisnil 11β-[4-[(E)-(hydroxyimino)méthyl]phényl]-17β-méthoxy-17-(méthoxyméthyl)estra-4,9-dién-3-one
asoprisnilo 11β-[4-[(E)-(hidroxiimino)metil]fenil]-17β-metoxi-17-(metoximetil)estra-4,9-dien-3-ona
C28H35NO4
OCH3
O
N
H
CH3
H
H
O CH3
HO

245
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
atomoxetinumatomoxetine (-)-(3R)-N-methyl-3-(2-methylphenoxy)-3-phenylpropan-1-amine
atomoxétine (-)-(3R)-N-méthyl-3-(2-méthylphénoxy)-3-phénylpropan-1-amine
atomoxetina (-)-(3R)-3-fenil-N-metil-3-(2-metilfenoxi)propan-1-amina
C17H21NO
O NH
H
CH3
CH3
bazedoxifenumbazedoxifene 1-[4-[2-(hexahydro-1H-azepin-1-yl)ethoxy]benzyl]-2-(4-hydroxyphenyl)-
3-methyl-1H-indol-5-ol
bazédoxifène 1-[4-[2-(hexahydro-1H-azépin-1-yl)éthoxy]benzyl]-2-(4-hydroxyphényl)-3-méthyl-1H-indol-5-ol
bazedoxifeno 1-[4-[2-(hexahidro-1H-azepin-1-il)etoxi]bencil]-2-(4-hidroxifenil)-3-metil-1H-indol-5-ol
C30
H34
N2O
3
HO
N
CH3
OH
ON
bifarceptumbifarcept interferon α/β receptor (human isoform p40 precursor)
bifarcept précurseur de la partie soluble de la chaîne 2 du récepteur humain de type Ide l’interféron α et β
bifarcept precursor de la fracción soluble de la cadena 2 del receptor humano de tipoI del interferón α y β
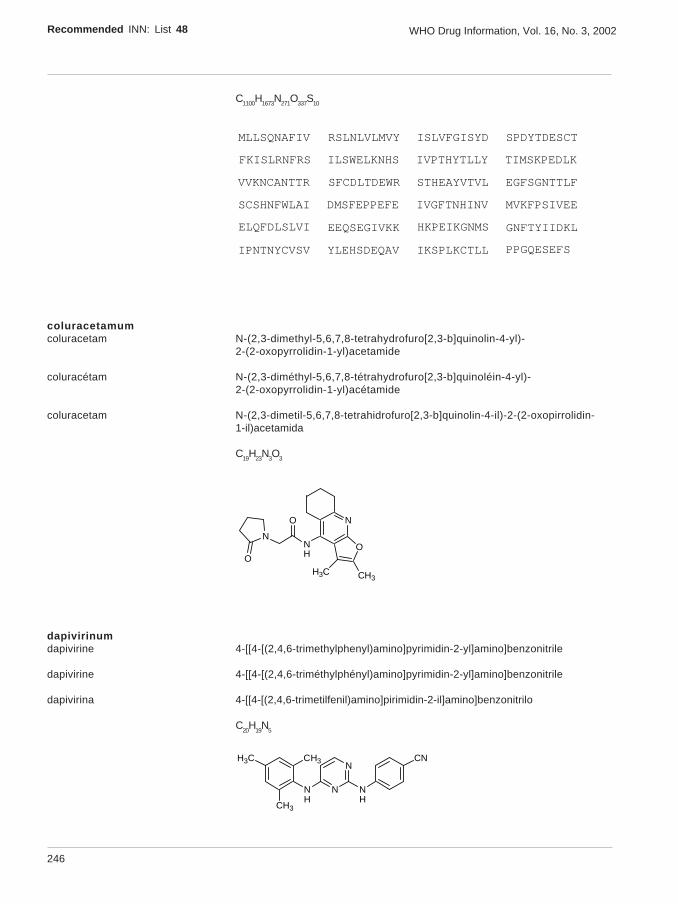
246
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
C1100H1673N271O337S10
MLLSQNAFIV
ILSWELKNHS
STHEAYVTVL
MVKFPSIVEE
IPNTNYCVSV
RSLNLVLMVY
IVPTHYTLLY
EGFSGNTTLF
ELQFDLSLVI
YLEHSDEQAV
ISLVFGISYD
TIMSKPEDLK
SCSHNFWLAI
EEQSEGIVKK
IKSPLKCTLL
SPDYTDESCT
VVKNCANTTR
DMSFEPPEFE
HKPEIKGNMS
PPGQESEFS
FKISLRNFRS
IVGFTNHINV
SFCDLTDEWR
GNFTYIIDKL
coluracetamumcoluracetam N-(2,3-dimethyl-5,6,7,8-tetrahydrofuro[2,3-b]quinolin-4-yl)-
2-(2-oxopyrrolidin-1-yl)acetamide
coluracétam N-(2,3-diméthyl-5,6,7,8-tétrahydrofuro[2,3-b]quinoléin-4-yl)-2-(2-oxopyrrolidin-1-yl)acétamide
coluracetam N-(2,3-dimetil-5,6,7,8-tetrahidrofuro[2,3-b]quinolin-4-il)-2-(2-oxopirrolidin-1-il)acetamida
C19H23N3O3
NNH
N
OO
CH3H3C
O
dapivirinumdapivirine 4-[[4-[(2,4,6-trimethylphenyl)amino]pyrimidin-2-yl]amino]benzonitrile
dapivirine 4-[[4-[(2,4,6-triméthylphényl)amino]pyrimidin-2-yl]amino]benzonitrile
dapivirina 4-[[4-[(2,4,6-trimetilfenil)amino]pirimidin-2-il]amino]benzonitrilo
C20H
19N
5
CN
NH
N
NNH
CH3
CH3
H3C
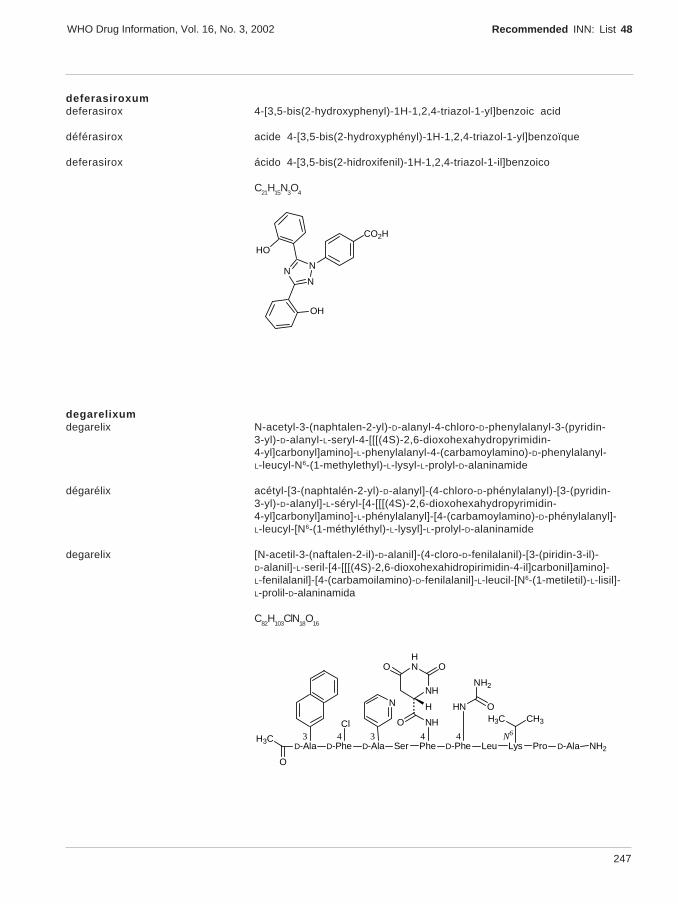
247
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
deferasiroxumdeferasirox 4-[3,5-bis(2-hydroxyphenyl)-1H-1,2,4-triazol-1-yl]benzoic acid
déférasirox acide 4-[3,5-bis(2-hydroxyphényl)-1H-1,2,4-triazol-1-yl]benzoïque
deferasirox ácido 4-[3,5-bis(2-hidroxifenil)-1H-1,2,4-triazol-1-il]benzoico
C21H15N3O4
CO2H
NN
N
HO
OH
degarelixumdegarelix N-acetyl-3-(naphtalen-2-yl)-D-alanyl-4-chloro-D-phenylalanyl-3-(pyridin-
3-yl)-D-alanyl-L-seryl-4-[[[(4S)-2,6-dioxohexahydropyrimidin-4-yl]carbonyl]amino]-L-phenylalanyl-4-(carbamoylamino)-D-phenylalanyl-L-leucyl-N6-(1-methylethyl)-L-lysyl-L-prolyl-D-alaninamide
dégarélix acétyl-[3-(naphtalén-2-yl)-D-alanyl]-(4-chloro-D-phénylalanyl)-[3-(pyridin-3-yl)-D-alanyl]-L-séryl-[4-[[[(4S)-2,6-dioxohexahydropyrimidin-4-yl]carbonyl]amino]-L-phénylalanyl]-[4-(carbamoylamino)-D-phénylalanyl]-L-leucyl-[N6-(1-méthyléthyl)-L-lysyl]-L-prolyl-D-alaninamide
degarelix [N-acetil-3-(naftalen-2-il)-D-alanil]-(4-cloro-D-fenilalanil)-[3-(piridin-3-il)-D-alanil]-L-seril-[4-[[[(4S)-2,6-dioxohexahidropirimidin-4-il]carbonil]amino]-L-fenilalanil]-[4-(carbamoilamino)-D-fenilalanil]-L-leucil-[N6-(1-metiletil)-L-lisil]-L-prolil-D-alaninamida
C82
H103
ClN18
O16
D-Ala D-Phe D-Ala Ser Phe D-Phe LeuH3C
O
Lys Pro D-Ala NH2
Cl
N
343
HNCH3H3C
N64 4
NHO
NH
HNO O
O
NH2
H
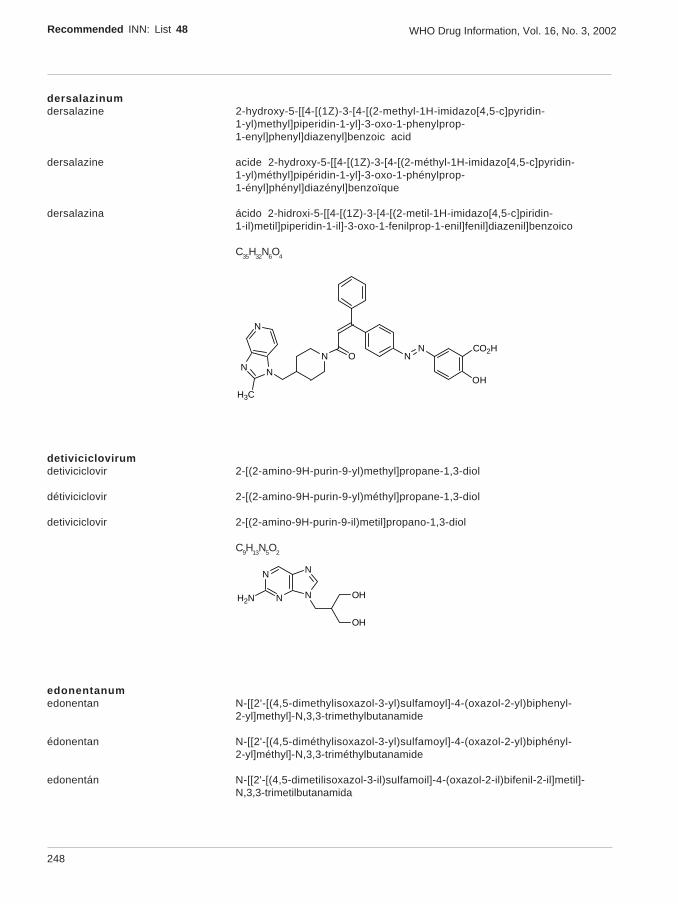
248
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
dersalazinumdersalazine 2-hydroxy-5-[[4-[(1Z)-3-[4-[(2-methyl-1H-imidazo[4,5-c]pyridin-
1-yl)methyl]piperidin-1-yl]-3-oxo-1-phenylprop-1-enyl]phenyl]diazenyl]benzoic acid
dersalazine acide 2-hydroxy-5-[[4-[(1Z)-3-[4-[(2-méthyl-1H-imidazo[4,5-c]pyridin-1-yl)méthyl]pipéridin-1-yl]-3-oxo-1-phénylprop-1-ényl]phényl]diazényl]benzoïque
dersalazina ácido 2-hidroxi-5-[[4-[(1Z)-3-[4-[(2-metil-1H-imidazo[4,5-c]piridin-1-il)metil]piperidin-1-il]-3-oxo-1-fenilprop-1-enil]fenil]diazenil]benzoico
C35H32N6O4
CO2H
OH
NNN O
NN
N
H3C
detiviciclovirumdetiviciclovir 2-[(2-amino-9H-purin-9-yl)methyl]propane-1,3-diol
détiviciclovir 2-[(2-amino-9H-purin-9-yl)méthyl]propane-1,3-diol
detiviciclovir 2-[(2-amino-9H-purin-9-il)metil]propano-1,3-diol
C9H13N5O2
N
N N
N
H2N OH
OH
edonentanumedonentan N-[[2'-[(4,5-dimethylisoxazol-3-yl)sulfamoyl]-4-(oxazol-2-yl)biphenyl-
2-yl]methyl]-N,3,3-trimethylbutanamide
édonentan N-[[2'-[(4,5-diméthylisoxazol-3-yl)sulfamoyl]-4-(oxazol-2-yl)biphényl-2-yl]méthyl]-N,3,3-triméthylbutanamide
edonentán N-[[2'-[(4,5-dimetilisoxazol-3-il)sulfamoil]-4-(oxazol-2-il)bifenil-2-il]metil]-N,3,3-trimetilbutanamida
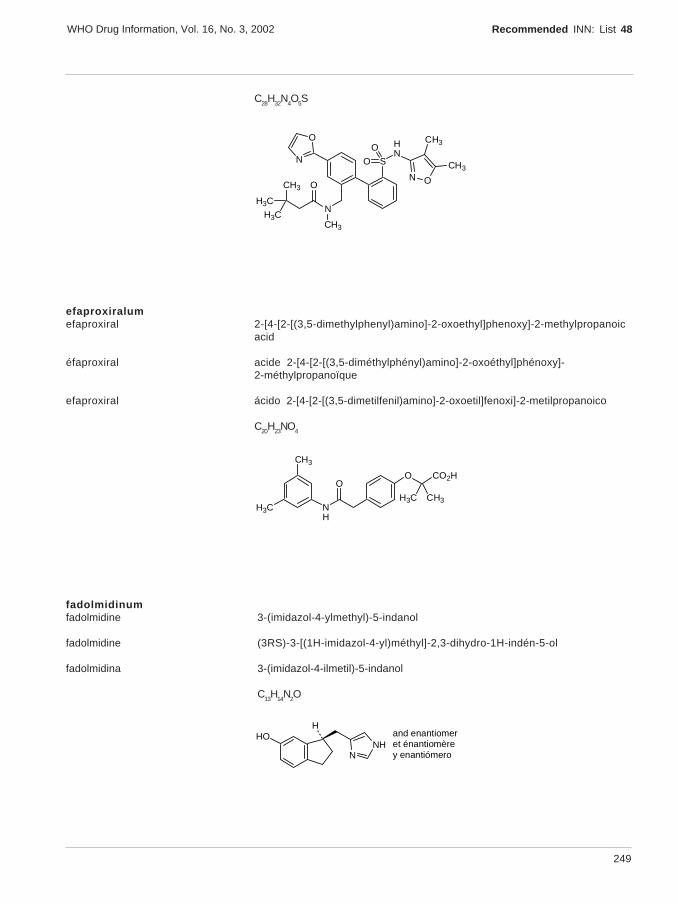
249
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
C28H32N4O5S
S
HN
N
CH3
CH3 ON O
H3C
H3C
O
NO
O
CH3
CH3
efaproxiralumefaproxiral 2-[4-[2-[(3,5-dimethylphenyl)amino]-2-oxoethyl]phenoxy]-2-methylpropanoic
acid
éfaproxiral acide 2-[4-[2-[(3,5-diméthylphényl)amino]-2-oxoéthyl]phénoxy]-2-méthylpropanoïque
efaproxiral ácido 2-[4-[2-[(3,5-dimetilfenil)amino]-2-oxoetil]fenoxi]-2-metilpropanoico
C20H23NO4
O CO2H
H3C CH3NH
H3C
CH3
O
fadolmidinumfadolmidine 3-(imidazol-4-ylmethyl)-5-indanol
fadolmidine (3RS)-3-[(1H-imidazol-4-yl)méthyl]-2,3-dihydro-1H-indén-5-ol
fadolmidina 3-(imidazol-4-ilmetil)-5-indanol
C13H14N2O
and enantiomeret énantiomèrey enantiómeroN
NHHO
H

250
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
flindokalnerumflindokalner (3S)-3-(5-chloro-2-methoxyphenyl)-3-fluoro-6-(trifluoromethyl)-1,3-dihydro-
2H-indol-2-one
flindokalner (3S)-3-(5-chloro-2-méthoxyphényl)-3-fluoro-6-(trifluorométhyl)-1,3-dihydro-2H-indol-2-one
flindokalner (3S)-3-(5-cloro-2-metoxifenil)-3-fluoro-6-(trifluorometil)-1,3-dihidro-2H-indol-2-ona
C16H10ClF4NO2
HN
F
F3C
O
OCH3
Cl
gimatecanumgimatecan (4S)-11-[(E)-[(1,1-dimethylethoxy)imino]methyl]-4-ethyl-4-hydroxy-
1,12-dihydro-14H-pyrano[3’,4’:6,7]indolizino[1,2-b]quinoline-3,14(4H)-dione
gimatécan (4S)-11-[(E)-[(1,1-diméthyléthoxy)imino]méthyl]-4-éthyl-4-hydroxy-1,12-dihydro-14H-pyrano[3’,4’:6,7]indolizino[1,2-b]quinoléine-3,14(4H)-dione
gimatecán (4S)-11-[(E)-[(1,1-dimetiletoxi)imino]metil]-4-etil-4-hidroxi-1,12-dihidro-14H-pirano[3’,4’:6,7]indolizino[1,2-b]quinolina-3,14(4H)-diona
C25H25N3O5
N O
N
O
O
HO CH3
NO
H3C
H3CCH3
icaridinumicaridin 1-methylpropyl 2-(2-hydroxyethyl)piperidine-1-carboxylate
icaridine 2-(2-hydroxyéthyl)pipéridine-1-carboxylate de 1-méthylpropyle
icaridina 2-(2-hidroxietil)piperidina-1-carboxilato de sec-butilo
C12
H23
NO3
N OCH3
OH
O CH3
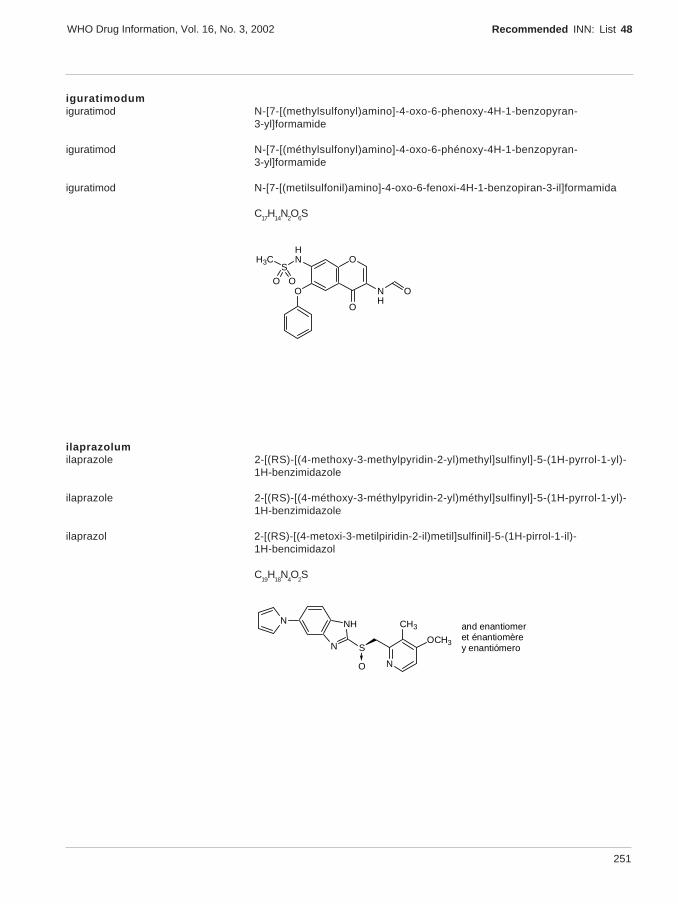
251
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
iguratimodumiguratimod N-[7-[(methylsulfonyl)amino]-4-oxo-6-phenoxy-4H-1-benzopyran-
3-yl]formamide
iguratimod N-[7-[(méthylsulfonyl)amino]-4-oxo-6-phénoxy-4H-1-benzopyran-3-yl]formamide
iguratimod N-[7-[(metilsulfonil)amino]-4-oxo-6-fenoxi-4H-1-benzopiran-3-il]formamida
C17H14N2O6S
OHN
SH3C
O NH
O
O
O O
ilaprazolumilaprazole 2-[(RS)-[(4-methoxy-3-methylpyridin-2-yl)methyl]sulfinyl]-5-(1H-pyrrol-1-yl)-
1H-benzimidazole
ilaprazole 2-[(RS)-[(4-méthoxy-3-méthylpyridin-2-yl)méthyl]sulfinyl]-5-(1H-pyrrol-1-yl)-1H-benzimidazole
ilaprazol 2-[(RS)-[(4-metoxi-3-metilpiridin-2-il)metil]sulfinil]-5-(1H-pirrol-1-il)-1H-bencimidazol
C19
H18
N4O
2S
and enantiomeret énantiomèrey enantiómeroN
NH
S
NO
CH3
OCH3
N
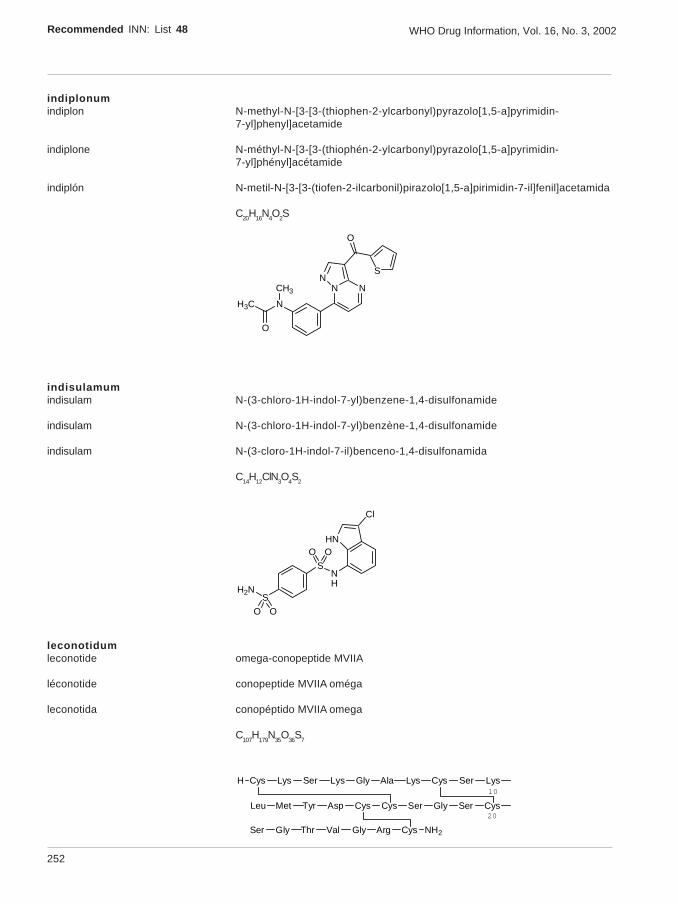
252
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
indiplonumindiplon N-methyl-N-[3-[3-(thiophen-2-ylcarbonyl)pyrazolo[1,5-a]pyrimidin-
7-yl]phenyl]acetamide
indiplone N-méthyl-N-[3-[3-(thiophén-2-ylcarbonyl)pyrazolo[1,5-a]pyrimidin-7-yl]phényl]acétamide
indiplón N-metil-N-[3-[3-(tiofen-2-ilcarbonil)pirazolo[1,5-a]pirimidin-7-il]fenil]acetamida
C20H16N4O2S
NH3C
NNN
O
CH3
O
S
indisulamumindisulam N-(3-chloro-1H-indol-7-yl)benzene-1,4-disulfonamide
indisulam N-(3-chloro-1H-indol-7-yl)benzène-1,4-disulfonamide
indisulam N-(3-cloro-1H-indol-7-il)benceno-1,4-disulfonamida
C14H12ClN3O4S2
SNH
SH2N
O O
OOHN
Cl
leconotidumleconotide omega-conopeptide MVIIA
léconotide conopeptide MVIIA oméga
leconotida conopéptido MVIIA omega
C107
H179
N35
O36
S7
H Cys Lys Ser Lys Gly Ala Lys Cys Ser Lys
Leu Met Tyr Asp Cys Cys Ser Gly Ser Cys
Ser Gly Thr Val Gly Arg Cys NH2
20
10
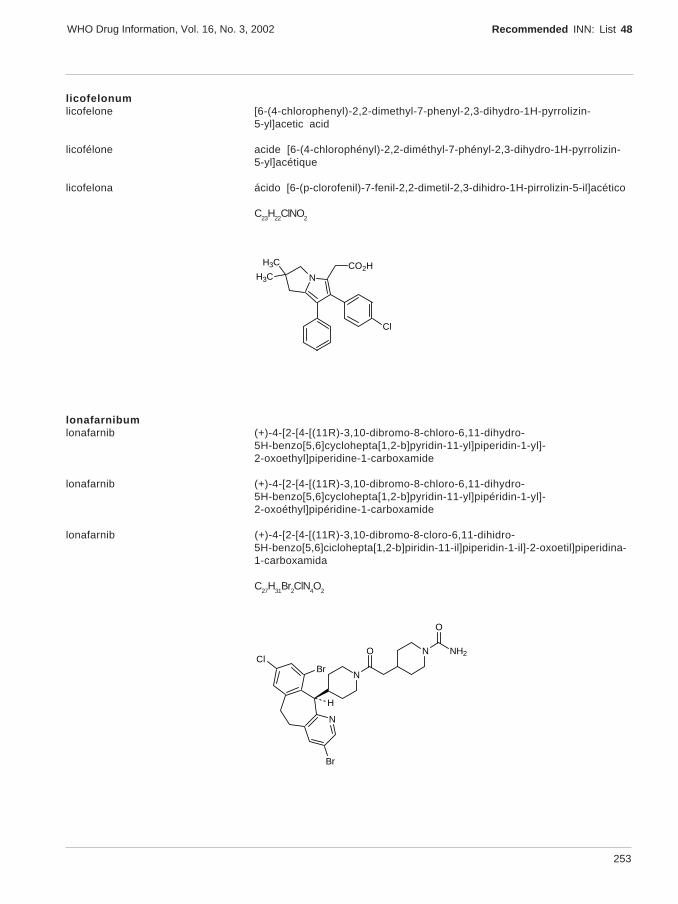
253
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
licofelonumlicofelone [6-(4-chlorophenyl)-2,2-dimethyl-7-phenyl-2,3-dihydro-1H-pyrrolizin-
5-yl]acetic acid
licofélone acide [6-(4-chlorophényl)-2,2-diméthyl-7-phényl-2,3-dihydro-1H-pyrrolizin-5-yl]acétique
licofelona ácido [6-(p-clorofenil)-7-fenil-2,2-dimetil-2,3-dihidro-1H-pirrolizin-5-il]acético
C23H22ClNO2
NCO2H
Cl
H3C
H3C
lonafarnibumlonafarnib (+)-4-[2-[4-[(11R)-3,10-dibromo-8-chloro-6,11-dihydro-
5H-benzo[5,6]cyclohepta[1,2-b]pyridin-11-yl]piperidin-1-yl]-2-oxoethyl]piperidine-1-carboxamide
lonafarnib (+)-4-[2-[4-[(11R)-3,10-dibromo-8-chloro-6,11-dihydro-5H-benzo[5,6]cyclohepta[1,2-b]pyridin-11-yl]pipéridin-1-yl]-2-oxoéthyl]pipéridine-1-carboxamide
lonafarnib (+)-4-[2-[4-[(11R)-3,10-dibromo-8-cloro-6,11-dihidro-5H-benzo[5,6]ciclohepta[1,2-b]piridin-11-il]piperidin-1-il]-2-oxoetil]piperidina-1-carboxamida
C27H31Br2ClN4O2
N
N
Br
ClBr
N NH2
O
O
H

254
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
lubazodonumlubazodone (2S)-2-[[(7-fluoro-2,3-dihydro-1H-inden-4-yl)oxy]methyl]morpholine
lubazodone (2S)-2-[[(7-fluoro-2,3-dihydro-1H-indén-4-yl)oxy]méthyl]morpholine
lubazodona (2S)-2-[[(7-fluoro-2,3-dihidro-1H-inden-4-il)oxi]metil]morfolina
C14H18FNO2
O
O
NH
F
H
luliconazolumluliconazole (-)-(E)-[(4R)-4-(2,4-dichlorophenyl)-1,3-dithiolan-2-ylidene](1H-imidazol-
1-yl)acetonitrile
luliconazole (-)-(E)-[(4R)-4-(2,4-dichlorophényl)-1,3-dithiolan-2-ylidène](1H-imidazol-1-yl)acétonitrile
luliconazol (-)-(E)-[(4R)-4-(2,4-diclorofenil)-1,3-ditiolan-2-ilideno](1H-imidazol-1-il)acetonitrilo
C14
H9Cl
2N
3S
2
N
N
NCS
S
Cl Cl
H
meldoniummeldonium 3-(2,2,2-trimethyldiazaniumyl)propanoate
meldonium 3-(2,2,2-triméthyldiazaniumyl)propanoate
meldonio 3-(2,2,2-trimetildiazanioil)propanoato
C6H14N2O2
-O2CNH
N+
CH3
CH3H3C
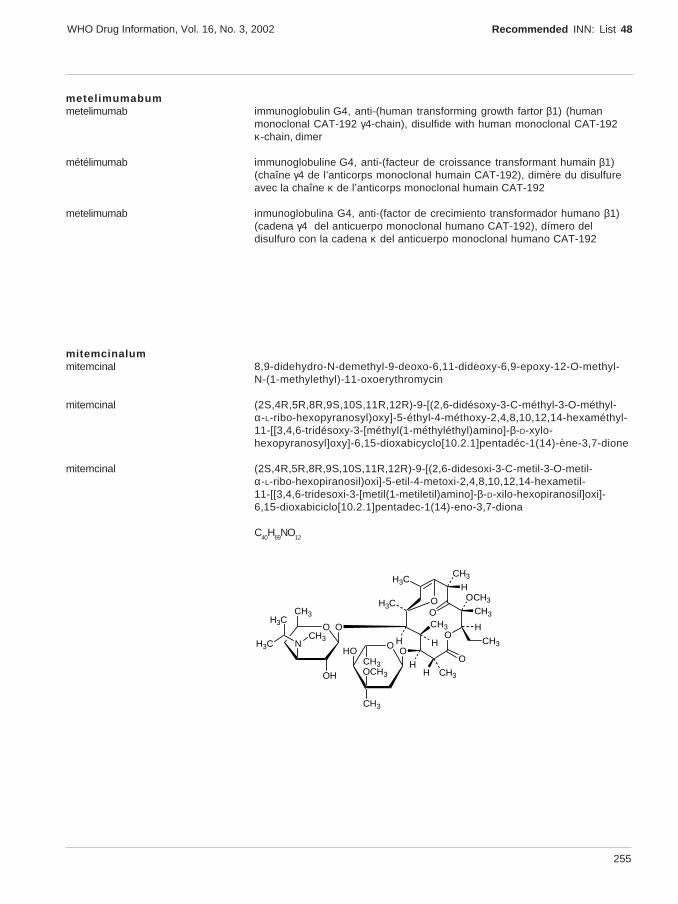
255
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
metelimumabummetelimumab immunoglobulin G4, anti-(human transforming growth fartor β1) (human
monoclonal CAT-192 γ4-chain), disulfide with human monoclonal CAT-192κ-chain, dimer
métélimumab immunoglobuline G4, anti-(facteur de croissance transformant humain β1)(chaîne γ4 de l’anticorps monoclonal humain CAT-192), dimère du disulfureavec la chaîne κ de l’anticorps monoclonal humain CAT-192
metelimumab inmunoglobulina G4, anti-(factor de crecimiento transformador humano β1)(cadena γ4 del anticuerpo monoclonal humano CAT-192), dímero deldisulfuro con la cadena κ del anticuerpo monoclonal humano CAT-192
mitemcinalummitemcinal 8,9-didehydro-N-demethyl-9-deoxo-6,11-dideoxy-6,9-epoxy-12-O-methyl-
N-(1-methylethyl)-11-oxoerythromycin
mitemcinal (2S,4R,5R,8R,9S,10S,11R,12R)-9-[(2,6-didésoxy-3-C-méthyl-3-O-méthyl-α-L-ribo-hexopyranosyl)oxy]-5-éthyl-4-méthoxy-2,4,8,10,12,14-hexaméthyl-11-[[3,4,6-tridésoxy-3-[méthyl(1-méthyléthyl)amino]-β-D-xylo-hexopyranosyl]oxy]-6,15-dioxabicyclo[10.2.1]pentadéc-1(14)-ène-3,7-dione
mitemcinal (2S,4R,5R,8R,9S,10S,11R,12R)-9-[(2,6-didesoxi-3-C-metil-3-O-metil-α-L-ribo-hexopiranosil)oxi]-5-etil-4-metoxi-2,4,8,10,12,14-hexametil-11-[[3,4,6-tridesoxi-3-[metil(1-metiletil)amino]-β-D-xilo-hexopiranosil]oxi]-6,15-dioxabiciclo[10.2.1]pentadec-1(14)-eno-3,7-diona
C40H69NO12
O
H
CH3
CH3
OCH3
H
H CH3H
H
O
CH3
CH3
H
O
N
CH3
OH
O
O
OCH3
CH3
HO
CH3
O
CH3H3C
H3C
H3C
OH3CO
256
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
naxifyllinumnaxifylline 8-[(1S,2R,4S,5S,6S)-3-oxatricyclo[3.2.1.02,4]oct-6-yl]-1,3-dipropyl-
3,7-dihydro-1H-purine-2,6-dione
naxifylline 8-[(1S,2R,4S,5S,6S)-3-oxatricyclo[3.2.1.02,4]oct-6-yl]-1,3-dipropyl-3,7-dihydro-1H-purine-2,6-dione
naxifilina 8-[(1S,2R,4S,5S,6S)-3-oxatriciclo[3.2.1.02,4]oct-6-il]-1,3-dipropil-3,7-dihidro-1H-purina-2,6-diona
C18H24N4O3
N
N N
HN
O
O
H3C
CH3
H
O
H
H
H
H
oglufanidumoglufanide L-α-glutamyl-L-tryptophan
oglufanide L-α-glutamyl-L-tryptophane
oglufanida L-α-glutamil-L-triptófano
C16
H19
N3O
5
HO2C
HN CO2H
H
HH2N
NH
O
olcegepantumolcegepant N-[(1R)-2-[[(1S)-5-amino-1-[[4-(pyridin-4-yl)piperazin-
1-yl]carbonyl]pentyl]amino]-1-(3,5-dibromo-4-hydroxybenzyl)-2-oxoethyl]-4-(2-oxo-1,4-dihydroquinazolin-3(2H)-yl)piperidine-1-carboxamide
olcégépant N-[(1R)-2-[[(1S)-5-amino-1-[[4-(pyridin-4-yl)pipérazin-1-yl]carbonyl]pentyl]amino]-1-(3,5-dibromo-4-hydroxybenzyl)-2-oxoéthyl]-4-(2-oxo-1,4-dihydroquinazolin-3(2H)-yl)pipéridine-1-carboxamide
olcegepant N-[(1R)-2-[[(1S)-5-amino-1-[[4-(piridin-4-il)piperazin-1-il]carbonil]pentil]amino]-1-(3,5-dibromo-4-hidroxibencil)-2-oxoetil]-4-(2-oxo-1,4-dihidroquinazolin-3(2H)-il)piperidina-1-carboxamida

257
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
C38H47Br2N9O5
N
HN
NHN
NH
N
N
N
H
H
O
O
O
O
H2N
Br
OHBr
oregovomabumoregovomab immunoglobulin G1, anti-(human CA125 (carbohydrate antigen)) (mouse
monoclonal B43.13 γ1-chain), disulfide with mouse monoclonal B43.13κ-chain, dimer
orégovomab immunoglobuline G1, anti-(antigène osidique humain CA125) (chaîne γ1 del’anticorps monoclonal de souris B43.13),dimère du disulfure avec lachaîne κ de l’anticorps monoclonal de souris B43.13
oregovomab immunoglobulina G1, anti-(antígeno osídico humano CA125) (cadena γ1 delanticuerpo monoclonal de ratón B43.13), dímero del disulfuro con lacadena κ del anticuerpo monoclonal de ratón B43.13
otamixabanumotamixaban methyl (2R,3R)-2-(3-carbamimidoylbenzyl)-3-[[4-(1-oxidopyridin-
4-yl)benzoyl]amino]butanoate
otamixaban (2R,3R)-2-(3-carbamimidoylbenzyl)-3-[[4-(1-oxydopyridin-4-yl)benzoyl]amino]butanoate de méthyle
otamixabán (2R,3R)-2-(3-carbamimidoilbencil)-3-[[4-(1-oxidopiridin-4-il)benzoil]amino]butanoato de metilo
C25H26N4O4
HN
NO
H2N
OCH3
O O
CH3
NH
H
H
258
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
paliferminumpalifermin [23-methionine]-23-163-fibroblast growth factor 7 (human clone 32/49
reduced)
palifermine [23-méthionine]-23-163-facteur 7 de croissance du fibroblaste, protéineréduite produite par le clone humain 32/49
palifermina [23-metionina]-23-163-factor 7 de crecimiento de fibroblastos, proteínareducida producida por el clon humano 32/49
C729H1156N204O207S10
MSYDYMEGGD
AVGIVAIKGV
AKWTHNGGEM
IRVRRLFCRT
ESEFYLAMNK
FVALNQKGIP
QWYLRIDKRG
EGKLYAKKEC
VRGKKTKKEQ
KVKGTQEMKN
NEDCNFKELI
KTAHFLPMAI
NYNIMEIRTV
LENHYNTYAS
T
peramivirumperamivir (1S,2S,3R,4R)-3-[(1S)-1-(acetylamino)-2-ethylbutyl]-
4-(carbamimidoylamino)-2-hydroxycyclopentanecarboxylic acid
péramivir acide (1S,2S,3R,4R)-3-[(1S)-1-(acétylamino)-2-éthylbutyl]-4-(carbamimidoylamino)-2-hydroxycyclopentanecarboxylique
peramivir ácido (1S,2S,3R,4R)-3-[(1S)-1-(acetilamino)-2-etilbutil]-4-(carbamimidoilamino)-2-hidroxiciclopentanocarboxílico
C15
H28
N4O
4
CO2H
OH
HN
NH2HN
HN
OH3C
CH3
CH3
HH
H
H
H
259
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
talibegronumtalibegron [4-[2-[[(2R)-2-hydroxy-2-phenylethyl]amino]ethoxy]phenyl]acetic acid
talibégron acide [4-[2-[[(2R)-2-hydroxy-2-phényléthyl]amino]éthoxy]phényl]acétique
talibegrón ácido [4-[2-[[(2R)-2-hidroxi-2-feniletil]amino]etoxi]fenil]acético
C18H21NO4
CO2H
O
HN
OHH
tariquidarumtariquidar N-[2-[[4-[2-(6,7-dimethoxy-3,4-dihydroisoquinolin-
2(1H)-yl)ethyl]phenyl]carbamoyl]-4,5-dimethoxyphenyl]quinoline-3-carboxamide
tariquidar N-[2-[[4-[2-(6,7-diméthoxy-3,4-dihydroisoquinoléin-2(1H)-yl)éthyl]phényl]carbamoyl]-4,5-diméthoxyphényl]quinoléine-3-carboxamide
tariquidar N-[2-[[4-[2-(6,7-dimetoxi-3,4-dihidroisoquinolin-2(1H)-il)etil]fenil]carbamoil]-4,5-dimetoxifenil]quinolina-3-carboxamida
C38H38N4O6
N
HN
OHN
N
OCH3
OCH3OCH3
OCH3O
tebaniclinumtebanicline 5-[(2R)-azetidin-2-ylmethoxy]-2-chloropyridine
tébanicline 5-[(2R)-azétidin-2-ylméthoxy]-2-chloropyridine
tebaniclina 5-[(2R)-azetidin-2-ilmetoxi]-2-cloropiridina
C9H
11ClN
2O
HN
HO
N Cl
260
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
tecastemizolumtecastemizole 1-(4-fluorobenzyl)-N-(piperidin-4-yl)-1H-benzimidazol-2-amine
técastémizole 1-(4-fluorobenzyl)-N-(pipéridin-4-yl)-1H-benzimidazol-2-amine
tecastemizol 1-(4-fluorobencil)-N-(piperidin-4-il)-1H-bencimidazol-2-amina
C19H21FN4
N
N
HN
NH
F
technetium (99mTc) fanolesomabumtechnetium (99mTc) fanolesomab immunoglobulin M, anti-(human CD15 antigen) (mouse monoclonal RB5
µ-chain), disulfide with mouse monoclonal RB5 light chain, pentamer,[99mTc]technetium salt
technétium (99mTc) fanolésomab immunoglobuline M, anti-(antigène CD15 humain) (chaîne µ de l’anticorpsmonoclonal de souris RB5), pentamère du disulfure de la chaîne légère del’anticorps monoclonal de souris RB5, sel de [99mTc]technétium
tecnecio (99mTc) fanolesomab inmunoglobulina M, anti-(antígeno CD15 humano) (cadena µ del anticuerpomonoclonal de ratón RB5), pentámero del disulfuro de la cadena ligera delanticuerpo monoclonal de ratón RB5, sal de [99mTc]tecnecio
tigecyclinumtigecycline (4S,4aS,5aR,12aS)-4,7-bis(dimethylamino)-
9-[[[(1,1-dimethylethyl)amino]acetyl]amino]-3,10,12,12a-tetrahydroxy-1,11-dioxo-1,4,4a,5,5a,6,11,12a-octahydrotetracene-2-carboxamide
tigécycline (4S,4aS,5aR,12aS)-4,7-bis(diméthylamino)-9-[[[(1,1-diméthyléthyl)amino]acétyl]amino]-3,10,12,12a-tétrahydroxy-1,11-dioxo-1,4,4a,5,5a,6,11,12a-octahydrotétracène-2-carboxamide
tigeciclina (4S,4aS,5aR,12aS)-4,7-bis(dimetilamino)-9-[[[(1,1-dimetiletil)amino]acetil]amino]-3,10,12,12a-tetrahidroxi-1,11-dioxo-1,4,4a,5,5a,6,11,12a-octahidrotetraceno-2-carboxamida
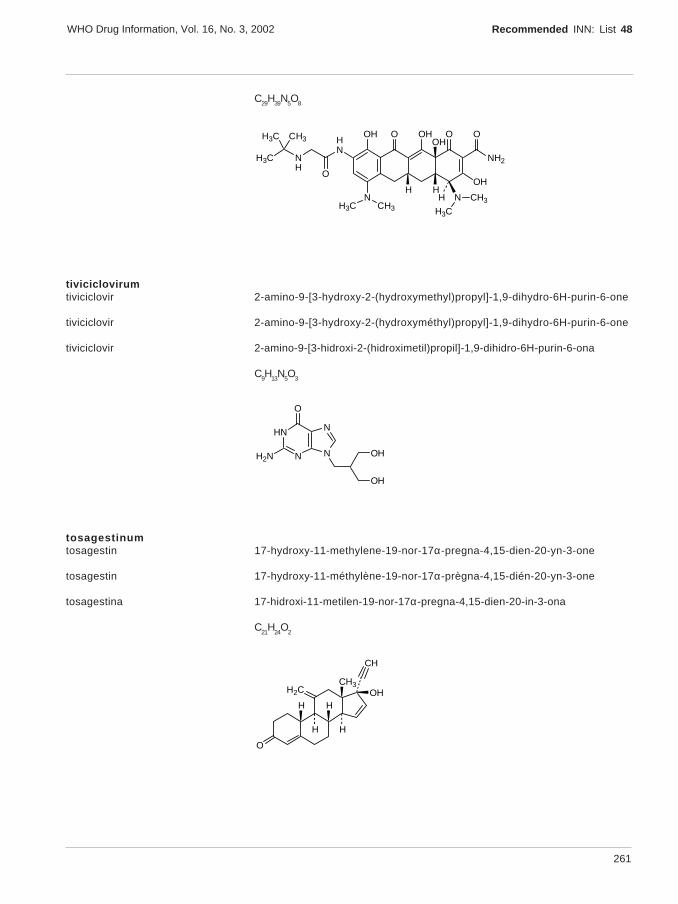
261
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
C29H39N5O8
OOH OH
NH2
H N
H3C
CH3
OOH
HH
O
OH
NH3C CH3
HN
NH
H3C
O
CH3H3C
tiviciclovirumtiviciclovir 2-amino-9-[3-hydroxy-2-(hydroxymethyl)propyl]-1,9-dihydro-6H-purin-6-one
tiviciclovir 2-amino-9-[3-hydroxy-2-(hydroxyméthyl)propyl]-1,9-dihydro-6H-purin-6-one
tiviciclovir 2-amino-9-[3-hidroxi-2-(hidroximetil)propil]-1,9-dihidro-6H-purin-6-ona
C9H13N5O3
HN
N N
N
H2N OH
OH
O
tosagestinumtosagestin 17-hydroxy-11-methylene-19-nor-17α-pregna-4,15-dien-20-yn-3-one
tosagestin 17-hydroxy-11-méthylène-19-nor-17α-prègna-4,15-dién-20-yn-3-one
tosagestina 17-hidroxi-11-metilen-19-nor-17α-pregna-4,15-dien-20-in-3-ona
C21
H24
O2
CH3
HOH
H
CH
H
H
O
H2C
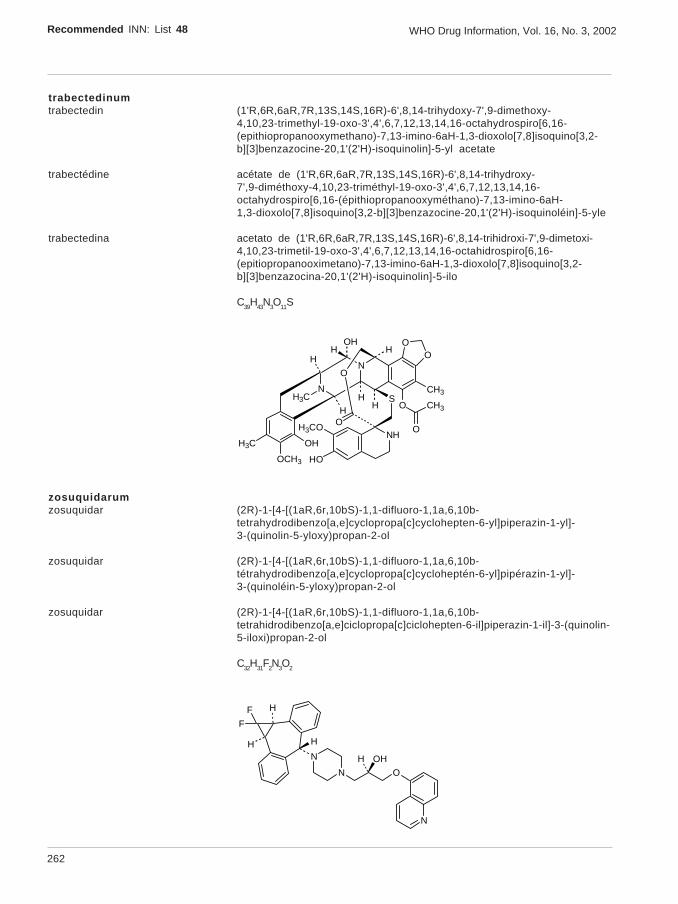
262
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
trabectedinumtrabectedin (1'R,6R,6aR,7R,13S,14S,16R)-6',8,14-trihydoxy-7',9-dimethoxy-
4,10,23-trimethyl-19-oxo-3',4',6,7,12,13,14,16-octahydrospiro[6,16-(epithiopropanooxymethano)-7,13-imino-6aH-1,3-dioxolo[7,8]isoquino[3,2-b][3]benzazocine-20,1'(2'H)-isoquinolin]-5-yl acetate
trabectédine acétate de (1'R,6R,6aR,7R,13S,14S,16R)-6',8,14-trihydroxy-7',9-diméthoxy-4,10,23-triméthyl-19-oxo-3',4',6,7,12,13,14,16-octahydrospiro[6,16-(épithiopropanooxyméthano)-7,13-imino-6aH-1,3-dioxolo[7,8]isoquino[3,2-b][3]benzazocine-20,1'(2'H)-isoquinoléin]-5-yle
trabectedina acetato de (1'R,6R,6aR,7R,13S,14S,16R)-6',8,14-trihidroxi-7',9-dimetoxi-4,10,23-trimetil-19-oxo-3',4',6,7,12,13,14,16-octahidrospiro[6,16-(epitiopropanooximetano)-7,13-imino-6aH-1,3-dioxolo[7,8]isoquino[3,2-b][3]benzazocina-20,1'(2'H)-isoquinolin]-5-ilo
C39H43N3O11S
OO
N
NH3C
OH
OCH3
H3C
O
O
CH3
CH3S
NHH3CO
HO
O
OHH
H
HO
H
HH
zosuquidarumzosuquidar (2R)-1-[4-[(1aR,6r,10bS)-1,1-difluoro-1,1a,6,10b-
tetrahydrodibenzo[a,e]cyclopropa[c]cyclohepten-6-yl]piperazin-1-yl]-3-(quinolin-5-yloxy)propan-2-ol
zosuquidar (2R)-1-[4-[(1aR,6r,10bS)-1,1-difluoro-1,1a,6,10b-tétrahydrodibenzo[a,e]cyclopropa[c]cycloheptén-6-yl]pipérazin-1-yl]-3-(quinoléin-5-yloxy)propan-2-ol
zosuquidar (2R)-1-[4-[(1aR,6r,10bS)-1,1-difluoro-1,1a,6,10b-tetrahidrodibenzo[a,e]ciclopropa[c]ciclohepten-6-il]piperazin-1-il]-3-(quinolin-5-iloxi)propan-2-ol
C32H31F2N3O2
N
N O
OHH
F
F
H
H H
N
263
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
AMENDMENTS TO PREVIOUS LISTSMODIFICATIONS APPORTÉES AUX LISTES ANTÉRIEURES
MODIFICACIONES A LAS LISTAS ANTERIORES
Recommended International Nonproprietary Names (Prop. INN): List 40Dénominations communes internationales recommendées (DCI Prop.): Liste 40Denominaciones Comunes Internacionales Recomendadas (DCI Prop.): Lista 40(WHO Drug Information, Vol. 12, No. 2, 1998)
p. 177 suprimase insérteseefavirenzo efavirenz
p. 187 suprimase insértesemoxifloxacina moxifloxacino
p. 200 technetii (99mTc) apcitidumtecnecio (99mTc) apcitida sustituyase la descripción por la siguiente:
hidrógeno [N-(mercaptoacetil)-D-tirosil-S-(3-aminopropil)-L-cisteinilglicil-L-α-aspartil-L-cisteinilglicilglicil-S-(acetamidometil)-L-cisteinilglicil-S-(acetamidometil)-L-cisteinilglicilglicil-L-cisteinamida (1→5)-sulfuro cíclico(5-)-N11,N12,N13,S13]oxo[99mTc]tecnetato(V) de sodio
p. 202 tobicillinumtobicillina sustituyase la descripción por la siguiente:
(2S,5R,6R)-3,3-dimetil-7-oxo-6-(2-fenilacetamido)-4-tia-1-azabiciclo-[3.2.0]heptano-2-carboxilato de α-hidroxi-m-tolilo, isobutirato (éster)
p. 205 suprimase insérteseclorporotixeno clorprotixeno
Recommended International Nonproprietary Names (Prop. INN): List 41Dénominations communes internationales recommendées (DCI Prop.): Liste 41Denominaciones Comunes Internacionales Recomendadas (DCI Prop.): Lista 41(WHO Drug Information, Vol. 13, No. 1, 1999)
p. 39 anatumomabum mafenatoxumanatumomab mafenatox sustituyase la descripción por la siguiente:
inmunoglobulina G1 (cadena γ1 del fragmento Fab del anticuerpomonoclonal humanizado de ratón, clon pMB125, dirigido contra laglicoproteína 72 humana asociada a tumores)-[227-alanina]enterotoxina A(Staphylococcus aureus) complejada con la cadena κ del anticuerpomonoclonal de ratón clon pMB125
p. 46 suprimase insérteseolamufloxacina olamufloxacino

264
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
p. 48 suprimase insérteseestannsoporfina estansoporfina
p. 48 stannsoporfinumestansoporfina sustituyase la descripción por la siguiente:
(OC-6-13)-dicloro[7,12-dietil-3,8,13,17-tetrametilporfirina-2,18-dipropionato(4-)-N21,N22,N23,N24]estannato(2-) de dihidrógeno
Recommended International Nonproprietary Names (Prop. INN): List 42Dénominations communes internationales recommendées (DCI Prop.): Liste 42Denominaciones Comunes Internacionales Recomendadas (DCI Prop.): Lista 42(WHO Drug Information, Vol. 13, No. 3, 1999)
p. 190 suprimase insérteseenrasentano enrasentán
p. 196 minopafantumminopafant sustituyase la descripción por la siguiente:
(+) cloruro de 1-etil-2-[[N-[[(2R)-2-metoxi-3-[[[4-[(octadecilcarbamoil)=oxi]piperidino]carbonil]oxi]propoxi]carbonil]-o-anisamido]metil]piridinio
p. 203 tabimorelinumtabimorelina sustituyase la descripción por la siguiente:
(R)-α-[(E)-5-amino-N,5-dimetil-2-hexenamido]-N-metil-N-[(R)-α-(metilcarbamoil)fenetil]-2-naftalenopropionamida
p. 212 sulesomabumsulesomab sustituyase la descripción por la siguiente:
inmunoglobulina G1, anti-(antígeno celular NCA-90 de granulocito humano)fragmento Fab’ (cadena γ1 del anticuerpo monoclonal de ratón IMMU-MN3),disulfuro con la cadena ligera del anticuerpo monoclonal de ratón IMMU-MN3
p. 212 technetium (99mTc) pintumomabumtecnecio (99mTc) pintumomab sustituyase la descripción por la siguiente:
sal de [99mTc]tecnecio de la inmunoglobulina G1 anti-(antígeno asociado alos adenocarcinomas humanos) (cadena γ1 del anticuerpo monoclonal deratón 170), dímero del disulfuro con la cadena κ del anticuerpo monoclonalde ratón 170
p. 214 igovomabumigovomab sustituyase la descripción por la siguiente:
inmunoglobulina G1, anti-[(antígeno osídico) CA 125 humano] (fragmentoF(ab’)2 (cadena γ1 del anticuerpo monoclonal de ratón OC125F(AB’)2),dímero del disulfuro con la cadena ligera del anticuerpo monoclonal de ratónOC125F(AB’)2
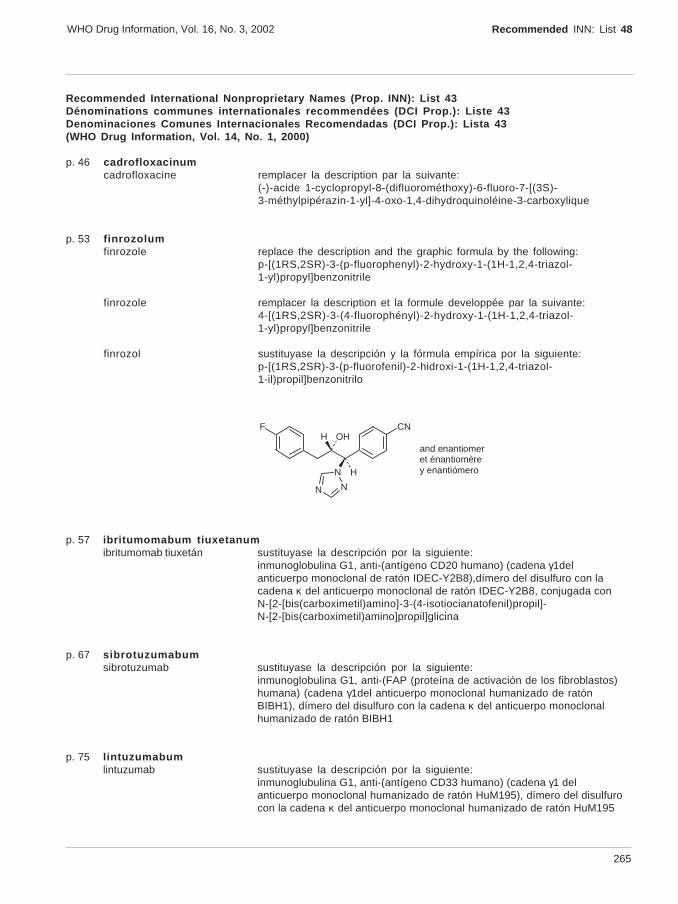
265
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
Recommended International Nonproprietary Names (Prop. INN): List 43Dénominations communes internationales recommendées (DCI Prop.): Liste 43Denominaciones Comunes Internacionales Recomendadas (DCI Prop.): Lista 43(WHO Drug Information, Vol. 14, No. 1, 2000)
p. 46 cadrofloxacinumcadrofloxacine remplacer la description par la suivante:
(-)-acide 1-cyclopropyl-8-(difluorométhoxy)-6-fluoro-7-[(3S)-3-méthylpipérazin-1-yl]-4-oxo-1,4-dihydroquinoléine-3-carboxylique
p. 53 finrozolumfinrozole replace the description and the graphic formula by the following:
p-[(1RS,2SR)-3-(p-fluorophenyl)-2-hydroxy-1-(1H-1,2,4-triazol-1-yl)propyl]benzonitrile
finrozole remplacer la description et la formule developpée par la suivante:4-[(1RS,2SR)-3-(4-fluorophényl)-2-hydroxy-1-(1H-1,2,4-triazol-1-yl)propyl]benzonitrile
finrozol sustituyase la descripción y la fórmula empírica por la siguiente:p-[(1RS,2SR)-3-(p-fluorofenil)-2-hidroxi-1-(1H-1,2,4-triazol-1-il)propil]benzonitrilo
CNF
N H
OHH
N N
and enantiomeret énantiomèrey enantiómero
p. 57 ibritumomabum tiuxetanumibritumomab tiuxetán sustituyase la descripción por la siguiente:
inmunoglobulina G1, anti-(antígeno CD20 humano) (cadena γ1delanticuerpo monoclonal de ratón IDEC-Y2B8),dímero del disulfuro con lacadena κ del anticuerpo monoclonal de ratón IDEC-Y2B8, conjugada conN-[2-[bis(carboximetil)amino]-3-(4-isotiocianatofenil)propil]-N-[2-[bis(carboximetil)amino]propil]glicina
p. 67 sibrotuzumabumsibrotuzumab sustituyase la descripción por la siguiente:
inmunoglobulina G1, anti-(FAP (proteína de activación de los fibroblastos)humana) (cadena γ1del anticuerpo monoclonal humanizado de ratónBIBH1), dímero del disulfuro con la cadena κ del anticuerpo monoclonalhumanizado de ratón BIBH1
p. 75 lintuzumabumlintuzumab sustituyase la descripción por la siguiente:
inmunoglubulina G1, anti-(antígeno CD33 humano) (cadena γ1 delanticuerpo monoclonal humanizado de ratón HuM195), dímero del disulfurocon la cadena κ del anticuerpo monoclonal humanizado de ratón HuM195
266
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
Recommended International Nonproprietary Names (Prop. INN): List 44Dénominations communes internationales recommendées (DCI Prop.): Liste 44Denominaciones Comunes Internacionales Recomendadas (DCI Prop.): Lista 44(WHO Drug Information, Vol. 14, No. 3, 2000)
p. 202 prinomastatumprinomastat replace the description by the following:
(S)-2,2-dimethyl-4-[[p-(4-pyridyloxy)phenyl]sulfonyl]-3-thiomorpholinecarbohydroxamic acid
p. 202 pumafentrinumpumafentrina sustituyase la descripción por la siguiente:
(-)-p-[(4aR*,10bS*)-9-etoxi-1,2,3,4,4a,10b-hexahidro-8-metoxi-2-metilbenzo[c][1,6]naftiridin-6-il]-N,N-diisopropilbenzamida
Recommended International Nonproprietary Names (Prop. INN): List 45Dénominations communes internationales recommendées (DCI Prop.): Liste 45Denominaciones Comunes Internacionales Recomendadas (DCI Prop.): Lista 45(WHO Drug Information, Vol. 15, No. 1, 2001)
p. 54 suprimase insérteseolmesartán medoxmilo olmesartán medoxomilo
p. 33 bevacizumabumbevacizumab sustituyase la descripción por la siguiente:
inmunoglobulina G1 anti-(factor de crecimiento del endotelio vascularhumano) (cadena γ1 del anticuerpo monoclonal humanizado de ratónrhuMab-VEGF), dímero del disulfuro con la cadena ligera del anticuerpomonoclonal humanizado de ratón rhuMab-VEGF
p. 34 bivatuzumabumbivatuzumab replace the description by the following:
immunoglobulin G1 (human-mouse monoclonal BIWA4 γ1-chain anti-humanantigen CD44v6), disulfide with human-mouse monoclonal BIWA4 κ-chain,dimer
bivatuzumab remplacer la description par la suivante:immunoglobuline G1 anti (antigène CD44v6 humain) (chaîne γ1 del’anticorps monoclonal de souris BIWA4 humanisé), dimère du disulfureavec la chaîne κ de l’anticorps monoclonal de souris BIWA4 humanisé
bivatuzumab sustituyase la descripción por la siguiente:inmunoglobulina G1 anti-(antígeno humano CD44v6) (cadena γ1 delanticuerpo monoclonal humanizado de ratón BIWA4), dímero del disulfurocon la cadena κ del anticuerpo monoclonal humanizado de ratón BIWA4
p. 40 gadofosvesetumgadofosveset sustituyase la descripción por la siguiente:
trihidrogeno[2,2’-[[(1R)-1-[[[2-[bis[(carboxi-κ-O)metil]amino-κ-N]etil][carboxi-κ-O)metil]amino-κ-N]metil]2-[[[(4,4,-difenilciclohexil)oxi]hidroxifosforil]=oxi]etil]imino-κ-N]diacetato(6-)-κ-O-κ-O’]gadolinato(3-)
267
WHO Drug Information, Vol. 16, No. 3, 2002 Recommended INN: List 48
p. 47 ozogamicinumozogamicina sustituyase la descripción por la siguiente:
(1R,4Z,8S,13E)-13-[2-[[2-[[[p-(3-carbamoilpropoxi)-α-metilbencilideno]=hidrazino]carbonil]-1,1-dimetiletil]ditio]etilideno]-8-[[4,6-didesoxi-4-[[[2,6-didesoxi-4-S-[4-[(6-desoxi-3-O-metil-α-L-manopiranosil)oxi]-3-iodo-5,6-dimetoxi-o-toluoil]-4-tio-β-D-ribo-hexopiranosil]oxi]amino]-2-O-[2,4-didesoxi-4-(N-etilacetamido)- 3-O-metil-α-L-treo-pentopiranosil]-β-D-glucopiranosil] oxi]-1-hidroxi-11-oxobiciclo[7.3.1]trideca-4,9-dieno-2,6-diino-10-carbamato de metilo
p. 48 pitavastatinumpitavastatina sustituyase la descripción por la siguiente:
ácido (3R,5S,6E)-7-[2-ciclopropil-4-(p-fluorofenil)-3-quinolil]-3,5-dihidroxi-6-heptenoico
Recommended International Nonproprietary Names (Prop. INN): List 46Dénominations communes internationales recommendées (DCI Prop.): Liste 46Denominaciones Comunes Internacionales Recomendadas (DCI Prop.): Lista 46(WHO Drug Information, Vol. 15, No. 3-4, 2001)
p. 217 supprimer insérerlérdelimumab lerdélimumab
p. 192 aviscuminumaviscumina sustituyase la descripción por la siguiente:
toxina ML-I (lectina I de muérdago) (Viscum album) obtenida por ingenieríagenética, constituida por dos cadenas peptídicas A (250 aminoácidos) y B(264 aminoácidos) unidas entre sí por un puente disulfuro
p. 201 imatinibumimatinib sustituyase la descripción por la siguiente:
α-(4-metil-1-piperazinil)-3’-[[4-(3-piridil)-2-pirimidinil]amino]-p-toluidida
p. 201 lemalesomabumlemalesomab sustituyase la descripción por la siguiente:
immunoglobulina G1, anti (antígeno celular del granulocito humano NCA 90)(cadena γ1 del anticuerpo monoclonal de ratón IMMU MN3), dímero deldisulfuro con la cadena κ del anticuerpo monoclonal de ratón IMMU MN3
p. 207 pitrakinraumpitrakinra sustituyase la descripción por la siguiente:
L-metionil-[121-ácido aspártico,124-ácido aspártico]interleukina-4
p. 208 suprimase insértesepradofloxacina pradofloxacino
268
Recommended INN: List 48 WHO Drug Information, Vol. 16, No. 3, 2002
p. 213 tipifarnibumtipifarnib sustituyase la descripción por la siguiente:
(+)-6-[(R)-amino(4-clorofenil)(1-metil-1H-imidazol-5-il)metil]-4-(3-clorofenil)-1-metilquinolin-2(1H)-ona
p. 216 zelandopamumzelandopam sustituyase la descripción por la siguiente:
(-)-(S)-4-(3,4-dihidroxifenil)-1,2,3,4-tetrahydro-7,8-isoquinolinadiol
Procedure and Guiding Principles / Procédure et Directives / Procedimientos y principios generales
The text of the Procedures for the Selection of Recommended International Nonproprietary Names for PharmaceuticalSubstances and General Principles for Guidance in Devising International Nonproprietary Names for PharmaceuticalSubstances will be reproduced in uneven numbers of proposed INN lists only.
Les textes de la Procédure à suivre en vue du choix de dénominations communes internationales recommandées pourles substances pharmaceutiques et des Directives générales pour la formation de dénominations communes internatio-nales applicables aux substances pharmaceutiques seront publiés seulement dans les numéros impaires des listesdes DCIs proposées.
El texto de los Procedimientos de selección de denominaciones comunes internacionales recomendadas para lassustancias farmacéuticas y de los Principios generales de orientación para formar denominaciones comunesinternacionales para sustancias farmacéuticas aparece solamente en los números impares de las listas de DCI propuestas.