12 bppv final
TRANSCRIPT
Benign Paroxysmal Positional Vertigo
1
Topic is covered under following heads
• Brief Anatomy and Physiology• Introduction• Aetio pathogenesis• Symptoms• Types and clinical features• Differential diagnosis• Investigations• Treatment modalities
2
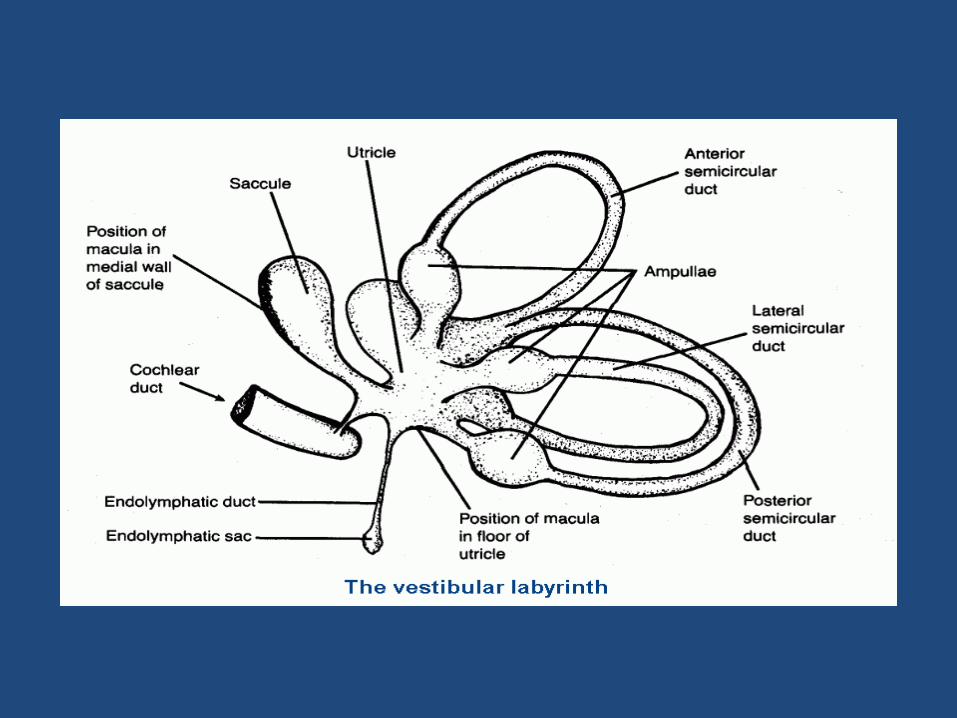
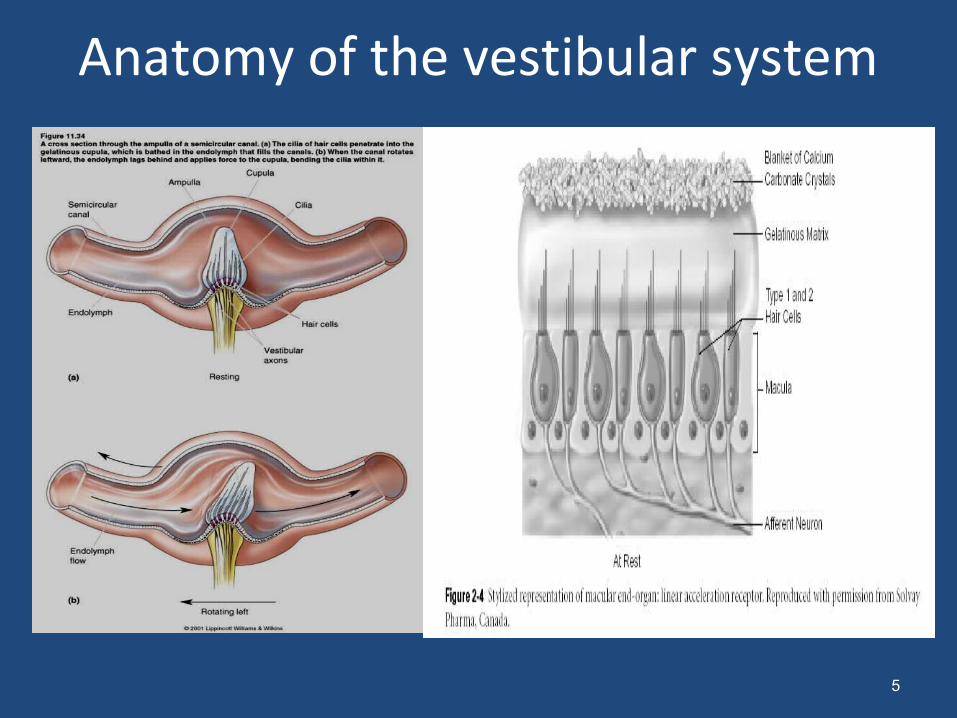
Anatomy of the vestibular system
5
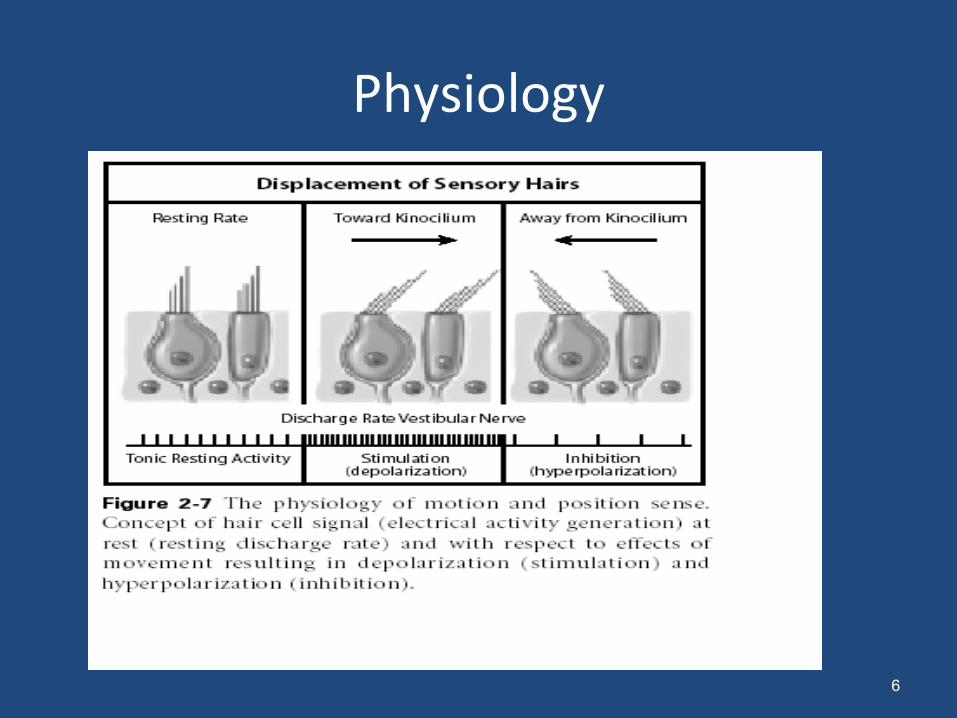
Physiology
6
Benign Paroxysmal Positional Vertigo (BPPV)
• Benign: not a very serious or progressive condition
• Paroxysmal: sudden and unpredictable in onset
• Positional: comes with a change in head position
• Vertigo: causing a sense of dizziness.
7
Introduction
• BPPV – One of the commonest Vestibular End organ disorders
• 17-25% of all vestibular disorders
• Most common aural cause of vertigo
• Chronic, Incapacitating, Affecting day to day functioning
8
Introduction
• Hallmark of the disease is the onset of brief (seconds) spells of often severe vertigo that are experienced only with specific movements of the head with respect to gravity.
• Typical Precipitating movements- – Turning in bed,
– Getting In and Out of bed,
– Bending and straightening
– Extending the neck to look up and back• “TOP SHELF VERTIGO”
9
History
• 1921 - First described by Barany
• 1952 - Dix-Hallpike reported this entity in a large number of patients and described important features of nystagmus
• 1962, Dr Harold Schuknecht proposed the cupulolithiasis (heavy cupula) theory.
• 1980, Brandt and Daroff proposed positional exercises based on the canalolithiasis hypothesis even before the theory was described
• 1980 – Hall, Ruby and McClure described the theory of canalolithiasis
• 1991 - Free floating deposits demonstrated in Endolymph of PSSC–Parnes, McClure
10
Benign positional vertigo -epidemiology• Incidence: 1:20 in general practice
3:20 in ENT OPD• U.S. study – incidence 64 per 100,000. Av 10-64 / lakh• Incidence in general population is higher in persons older
than 40 years.• Elderly patients – incidence approximately 8%. • 20% of all falls that result in hospitalization for serious
injuries in the elderly are due to vertigo of end-organ origin (most often related to BPPV).
• Average age of onset 51 years. M=F, some studies show a slight predilection for women.
• Rarely seen in persons younger than 35 years without a history of antecedent head trauma.
11
• Idiopathic – 48%
• Head trauma
• Viral neuronitis
• Middle ear infection
• Surgical damage to the labyrinth
• Prolonged bed rest
12
BPPV- AETIOLOGY
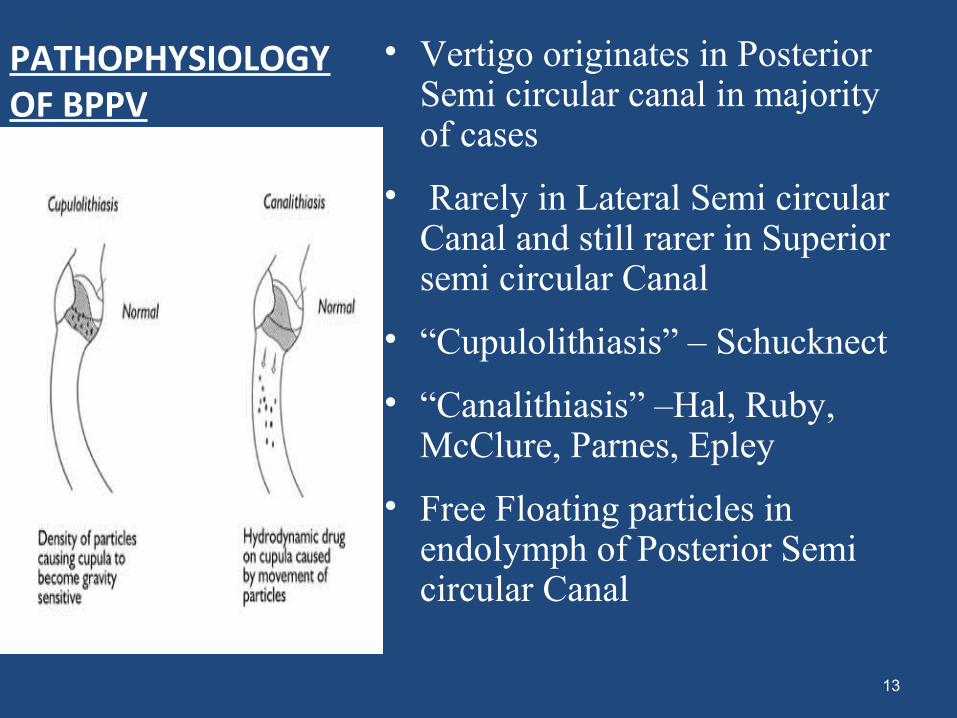
PATHOPHYSIOLOGY OF BPPV
• Vertigo originates in Posterior Semi circular canal in majority of cases
• Rarely in Lateral Semi circular Canal and still rarer in Superior semi circular Canal
• “Cupulolithiasis” – Schucknect
• “Canalithiasis” –Hal, Ruby, McClure, Parnes, Epley
• Free Floating particles in endolymph of Posterior Semi circular Canal
13
Theories of BPPV
14
Cupulolithiasis • In 1962, Dr Harold Schuknecht proposed the cupulolithiasis
(heavy cupula) theory. • Discovered basophilic particles or densities that were
adherent to the cupula.• He postulated that the PSC was rendered sensitive to gravity
by these abnormal dense particles attached to, or impinging on, the cupula.
• This produces persistent nystagmus and also explains the dizziness when a patient tilts the head backward.
• Cupulolithiasis – possible role in atypical BPPV
Theories of BPPV Canalolithiasis :
– Hall, Ruby and McClure – 1980
– Free floating deposits demonstrated in Endolymph of PSSC–Parnes, McClure-1991
• The most widely accepted theory of the pathophysiology of BPV
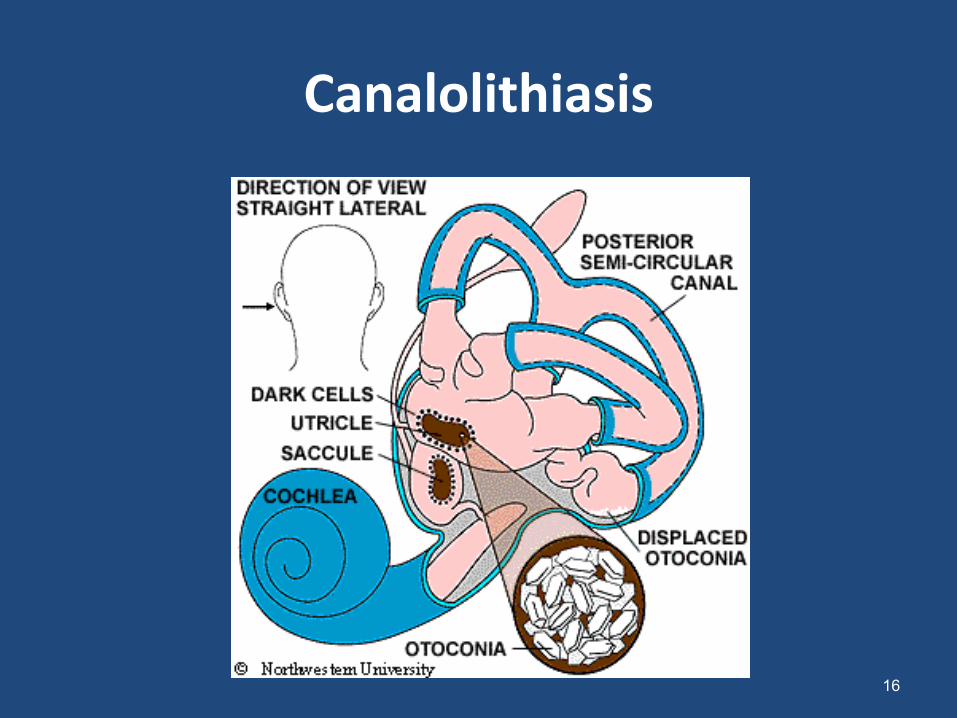
• Otoliths (calcium carbonate particles) are normally attached to a membrane inside the utricle and saccule
• Otoliths may become displaced from the utricle to enter the posterior semicircular duct since this is the most dependent of the 3 ducts
• Changing head position relative to gravity causes the free Otoliths to gravitate longitudinally through the canal.
• The concurrent flow of endolymph stimulates the hair cells of the affected semicircular canal, causing vertigo.
• Explains all features of typical nystagmus
15
Symptoms
• Discrete episodes of vertigo induced by specific head motions of duration less than 1 min.
• Single bouts clustered in time with remissions lasting months or more.
• Dizziness with rapid head movements. (Cupulolithiasis)• Disequilibrium worse in the morning or after day time
naps.• Nausea and vomiting
17
NYSTAGMUS IN BPPV …
• Nystagmus : characterization and types – Rt / Lt , vertical / horizontal , changing– Tortional = Rotational – clockwise /
counterclockwise– Geotropic- toward the earth– Ageotropic – opposite
DIRECTION OF NYSTAGMUS
Destructive lesion of the vestibular end organ or the vestibular nerve will produce transient horizontal nystagmus with its quicker phase towards the opposite side.
Unilateral cerebellar lesion will produce vertigo with its quicker phase to the same side
Paretic lesion of labyrinth the nystagmus is towards healthy side
19
Nystagmus
20
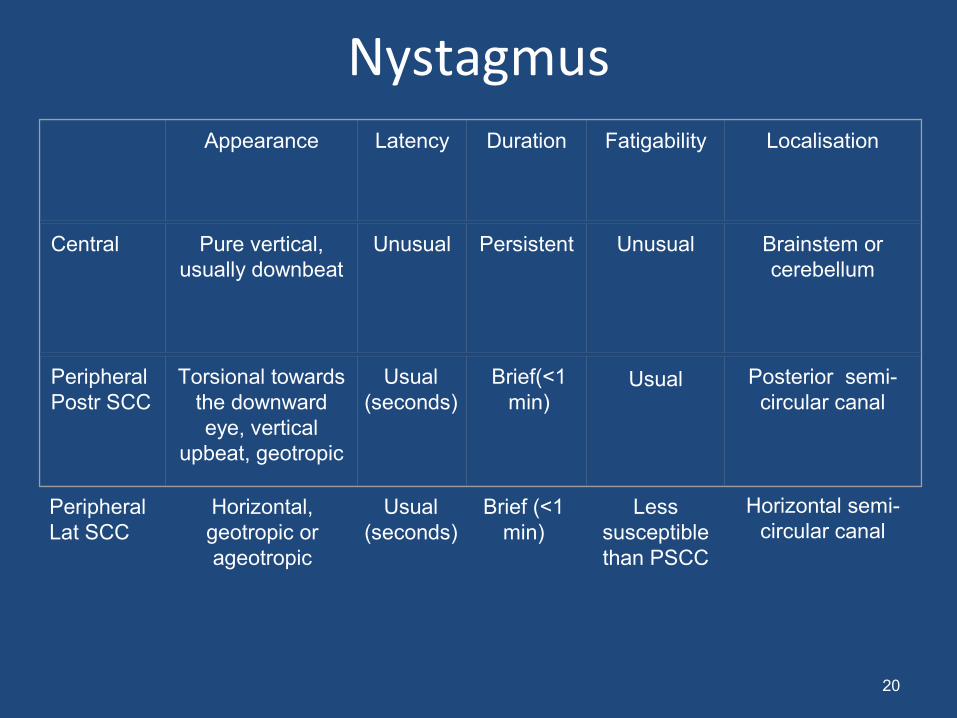
Appearance Latency Duration Fatigability Localisation
Central Pure vertical, usually downbeat
Unusual Persistent Unusual Brainstem or cerebellum
PeripheralPostr SCC
Torsional towards the downward eye, vertical
upbeat, geotropic
Usual (seconds)
Brief(<1 min)
Usual Posterior semi-circular canal
PeripheralLat SCC
Horizontal, geotropic or ageotropic
Usual (seconds)
Brief (<1 min)
Less susceptible than PSCC
Horizontal semi-circular canal
I. Classic BPPV
• Involves the Posterior SCC – Canalilithiasis of Posterior SCC – most frequent
cause– Reversal upon return to upright position– Response decline upon repetitive provocation
Types of BPPV
II. Lat. SCC BPPV
• Most common atypical BPPV• 3-9% of cases• Paroxysmal horizontal direction changing nystagmus –beats
towards ground (geotropic) when head turned to side while patient lies supine - Canalilithiasis
• Ageotropic – Nystagmus away from the dependent affected ear - Cupulolithiasis
• Nystagmus lasts 1 minute, minimal latency and no fatigability. • Occurs with head to either side but stronger on one side.
22
III. Ant. SCC BPPV
• Rare – 2%• Down-beating /torsional NG for the opposite ear
on Dix-Hallpike maneuver• Torsional downbeating nystagmus during
Hallpike test induced when the abnormal anterior canal (which lies at right angles to posterior) is uppermost.
• Repositioning maneuver starts with abnormal ear uppermost moving across to opposite head hanging position.
24
BPPV - D.D
• Meniere’s disease• Vestibular migraine• Recurrent vestibulopathy• Vestibular Labyrinthitis – Lasting days
• Inner ear fistula• Inner ear trauma• Superior SCC dehiscence syndrome• Central origin : Stroke , MS , cerebellar degeneration• Vertebral artery insufficiency• Cervical vertigo
25
Minutes to hours
Variable duration
HISTORY:
Confirmation of dizziness
Associated symptoms•Otalgia, otorrhoea, Tinnitus, headache,•Aural fullness, head injury, acoustic
trauma, ototoxic drug intake, DM, HTN, •TB, CVA, IHD•H/o Ear surgery•Difficulty in speaking/walking•Diplopia/dysarthria, loss of consciousness
points to brain stem dysfunction 26
EVALUATION AND DIAGNOSIS
Pattern Of Vertigo Onset, duration, continuous/ paroxysmalPeriod of complete reliefPostural
Preliminary tests Of Balance
Degree Of Vertigo – Is there nausea/vomiting
(I) Finger Pointing(II) Rapid Alternate Movements Of Hand(III)Gait(IV)Tandem Walk(V) Rhombergs test(VI)Unterbergers test
27
Ears-EAC-FB/WAX -TM for perforation, AOM/OME -Cholesteatoma Hearing tests -TFT -PTA -FFH -Impedance Audiometry
Otological examination
Detailed clinical examination General Systemic
28
Ocular Examination PtosisPupillary reactivityOcular alignmentEye movementsConvergence
29
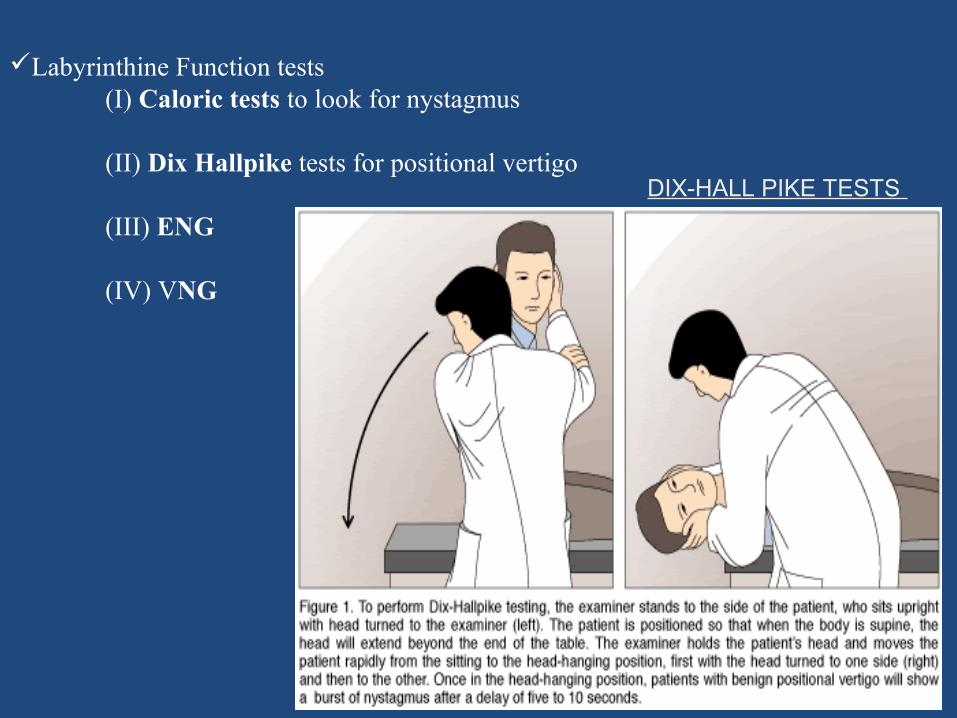
Labyrinthine Function tests (I) Caloric tests to look for nystagmus
(II) Dix Hallpike tests for positional vertigo
(III) ENG
(IV) VNG
DIX-HALL PIKE TESTS
30
RECENT ADVANCES IN EVALUATIONVIDEO NYSTAGMOGRAPHY (VNG)
•VNG – Video images of the eyes are obtained without direct contact using high resolution cameras with infrared illumination. Setup is fast & as easy using Frenzel glasses. The eyes are visualized, enabling simultaneous subjective evaluation while eye movements are analyzed by digital image processing to obtain vertical and horizontal eyeposition. Can be used for teaching purpose.
31
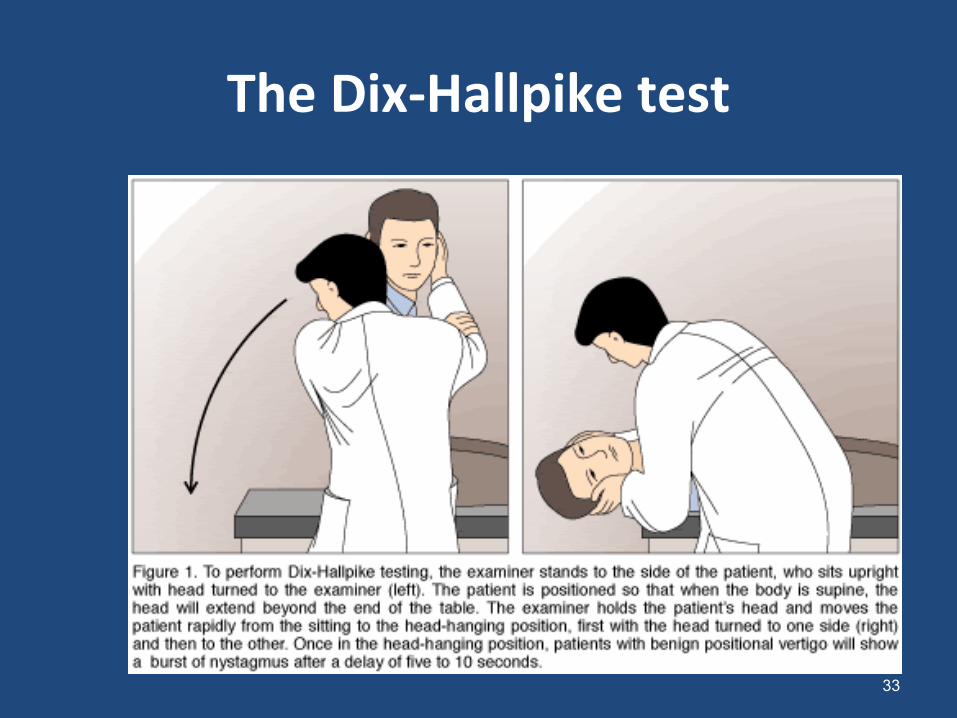
The Dix-Hallpike test
33
Laboratory testsRoutine hemogram, urine examinationBlood sugarT3, T4 ,TSHSerological tests to rule out Syphilis
Radiological investigationsX-Ray Skull-Per orbital viewX-Ray mastoidsX-Ray Cervical spineCT- Temporal bone and Brain
SPECIAL TESTS
EEGBERA
Psychological Evaluation 34
To rule out other pathologies
BPPV - Treatment
• Watchful waiting• Pharmacotherapy• Canalith repositioning procedure• Vestibular rehabilitation• Surgery care
– Singular neurectomy– Post. Canal occlusion– Vestibular nerve section
Pharmacotherapy
• Directed principally at suppressing vestibular response.
• Alleviating nausea associated with vertigo.• Does not treat underlying cause.
– Low dose diazepam – used prior to CRP– Antiemetics like phenergan– Longer acting vestibular suppressants like
clonazepam for chronic disequilibrium
36
Canalith Repositioning Procedure ( CRP )
• The treatment of choice for BPPV (Epley maneuver)
• The patient positioned in a series of steps so as to slowly move the otoconia particles from the Posterior SCC into the utricle.
• Takes approximately 5 minutes.
• The patient is instructed to wear a neck brace for 24 hours and to not bend down or lay flat for 24 hours after the procedure.
• Dix-Hallpike test is repeated soon after the CRP and after 1 week.
• If the patient does experience vertigo and nystagmus, then the CRP is repeated with a vibrator placed on the skull in order to dislodge the otoconia.
37
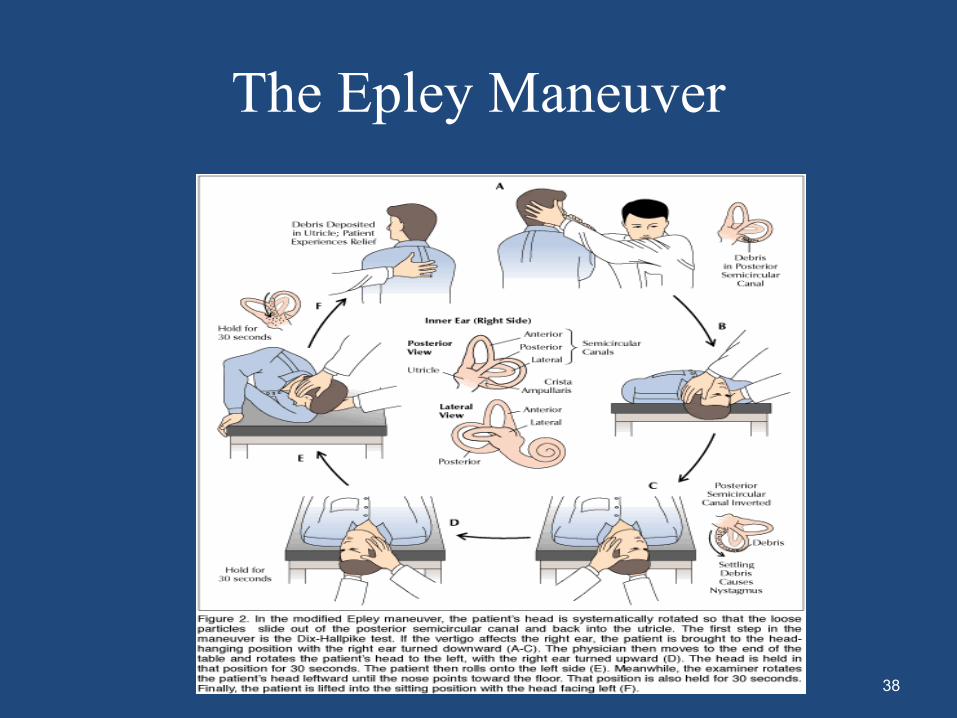
The Epley Maneuver
38

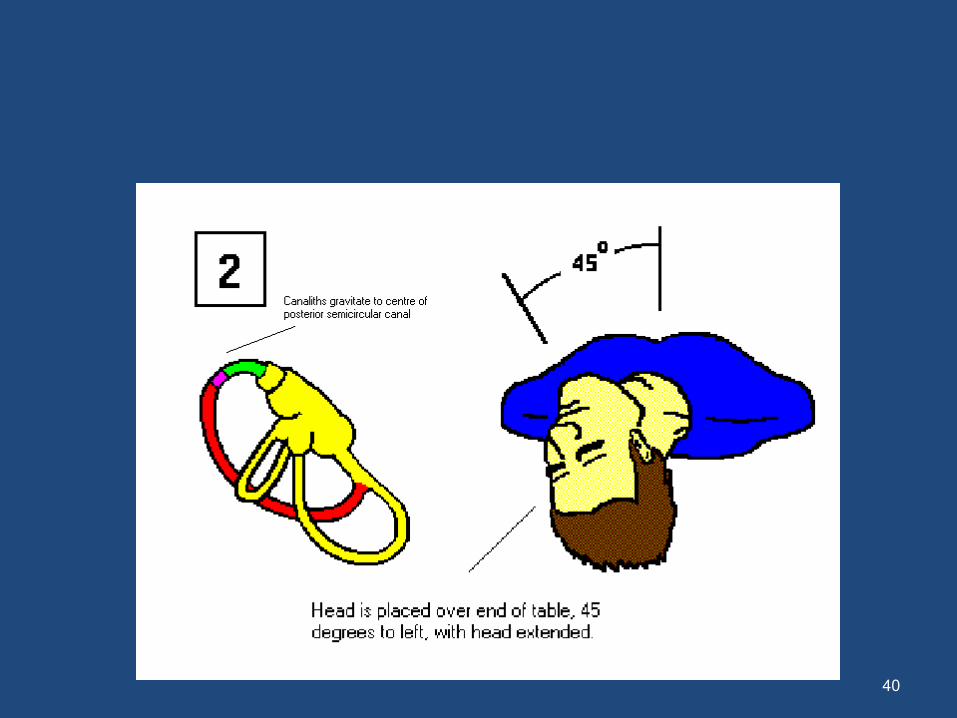
Epley manouevre
39
40
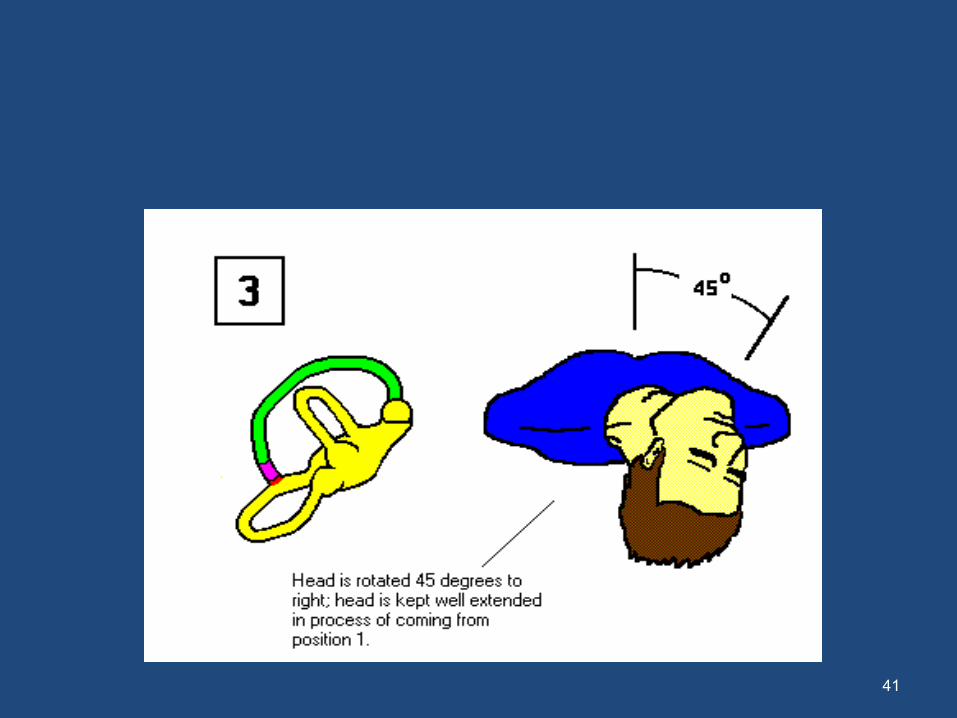
41
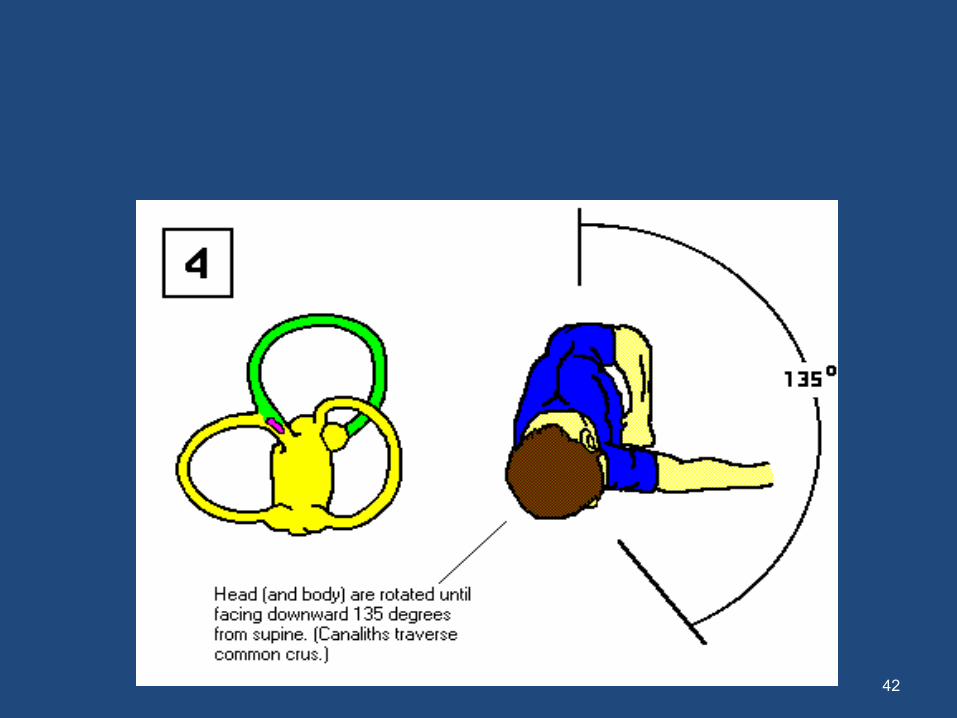
42
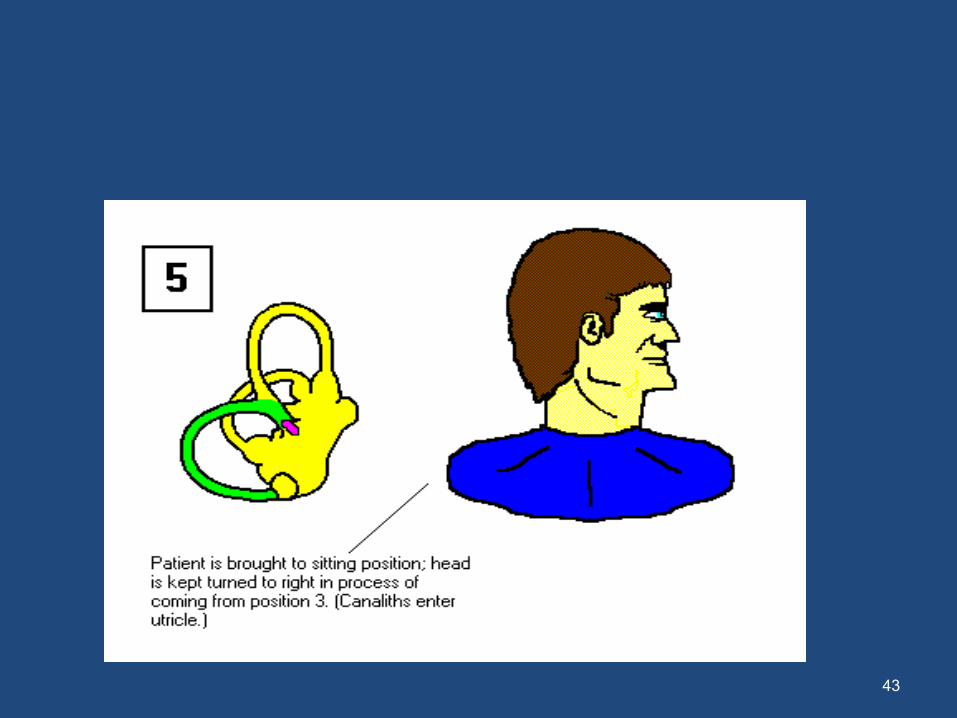
43
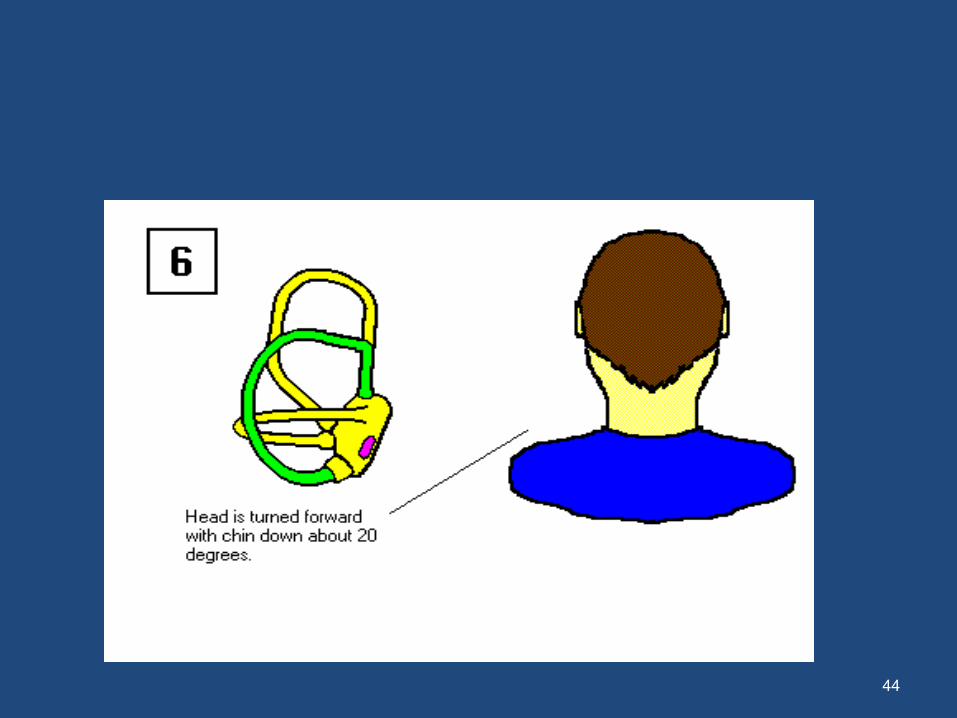
44
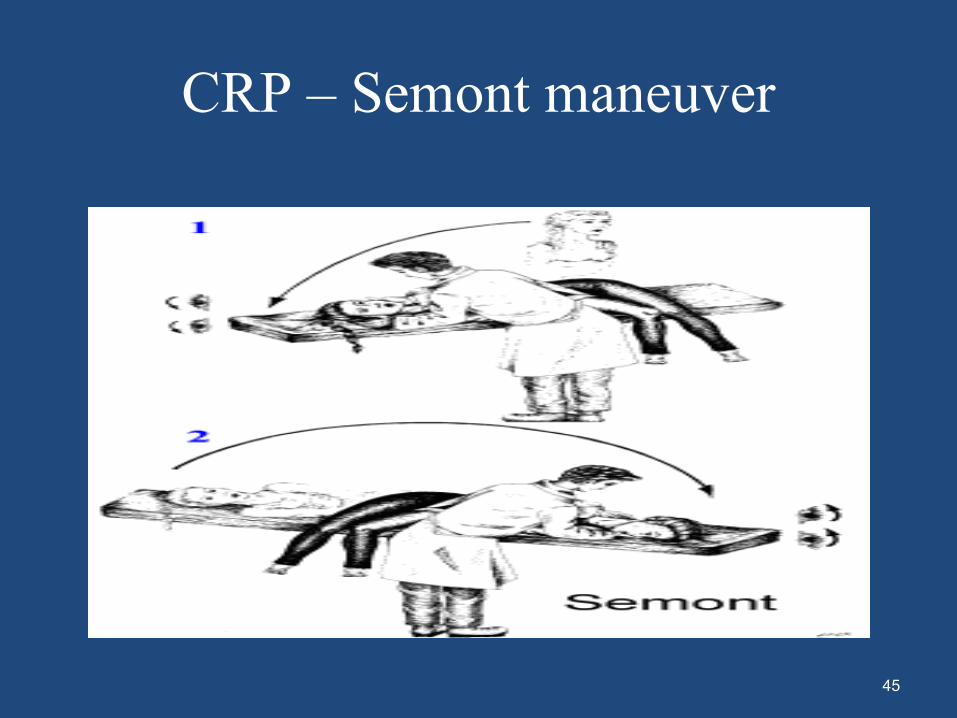
CRP – Semont maneuver
45
Brandt-Daroff Exercises
• Method of treating BPPV, usually used when the office treatment fails.
• These exercises should be performed
– For one week, three times per day
– For three weeks, twice per day.
• In each time, one performs the maneuver as shown five times.
• 1 repetition = maneuver done to each side in turn (takes 2 minutes)
46
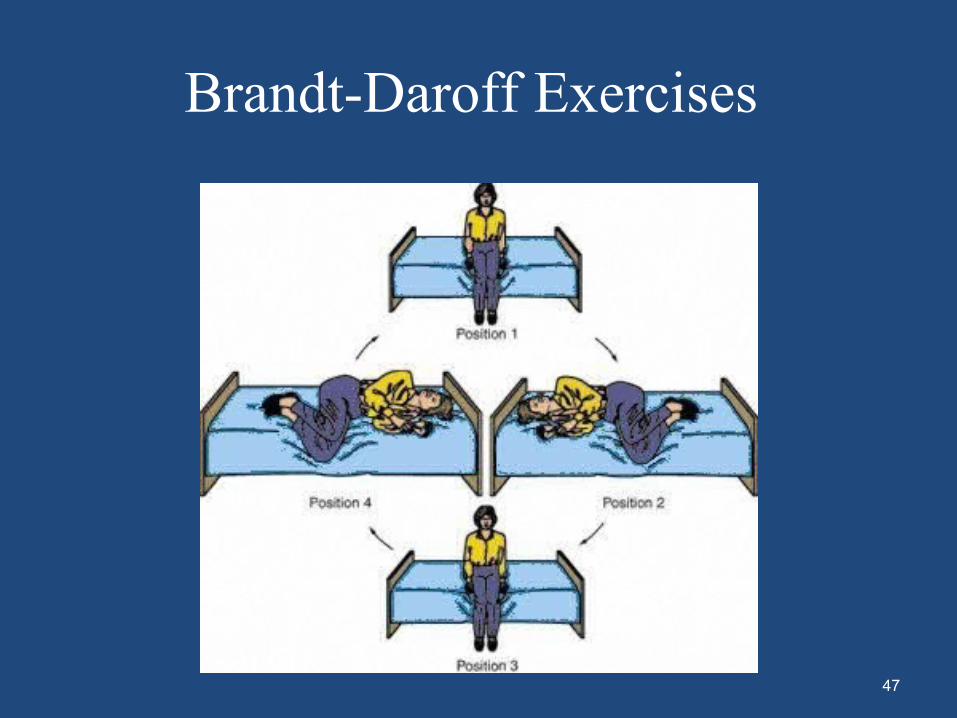
Brandt-Daroff Exercises
47
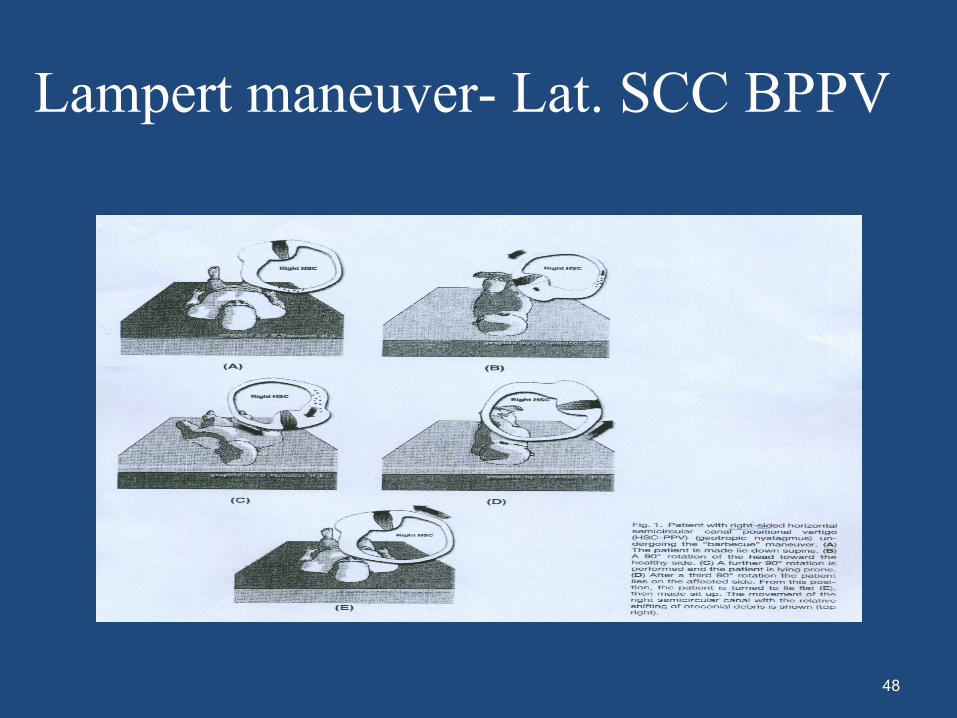
Lampert maneuver- Lat. SCC BPPV
48
Complications of CRP
• Failure – 25% (12%-56)• Recurrence – 13% in 6 months• Side effects
– Nausea ,Vomiting, Fainting, Sweating
• Worse vertigo – Lateral SCC BPPV
• “Canalith jam”
• Conversion to another canal
49
Vestibular Rehabilitation Exercises (VRE)
• Reduces symptoms, Promotes Spontaneous resolution
• Safe and effective
• Cawthorne-Cooksey Exercises
• Need to be carried out regularly
– Over 12-16 Weeks before improvement is noticed
50
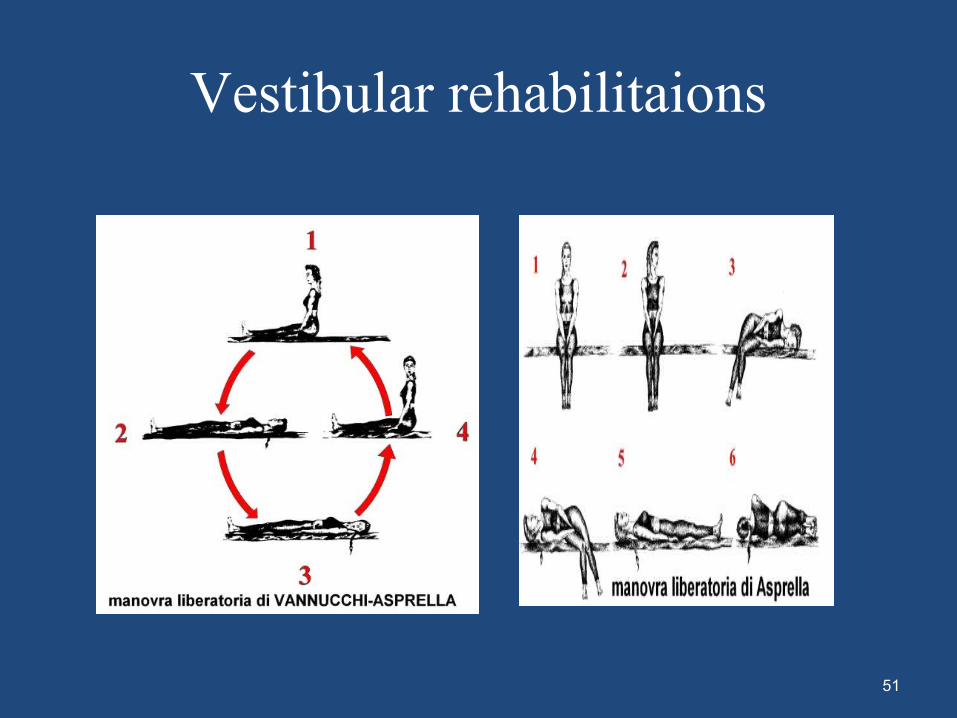
Vestibular rehabilitaions
51
Surgery• Singular neurectomy
• Posterior Canal Plugging Procedure
• Vestibular Nerve Section
52
Role of Surgery
• Very limited, < 2% may need Surgery which is rarely offered
• Highly responsive to physical therapy interventions
• Only in intractable cases affecting the life style of the patient
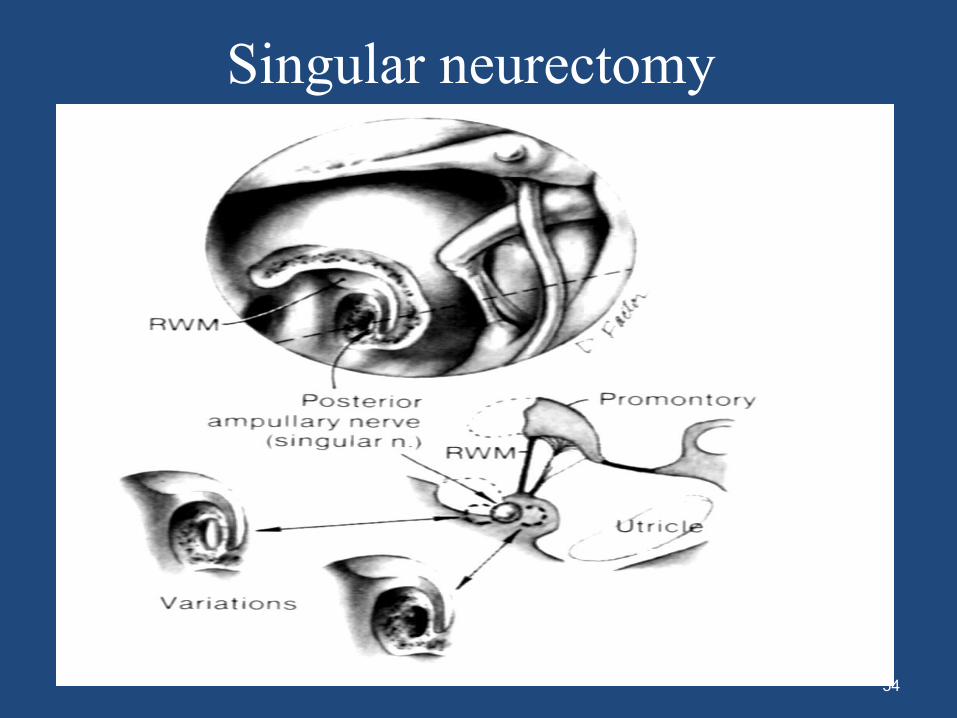
Singular neurectomy
• Evolved by Gacek
• Section the posterior ampullary nerve that transmits information from the posterior semicircular canal ampulla toward the brain.
• Highly rational
• Technically difficult
• Can cause hearing loss in 7-17% of patients and fails in 8-12%.
• Anatomical abnormalities of singular canal
53
Singular neurectomy
54
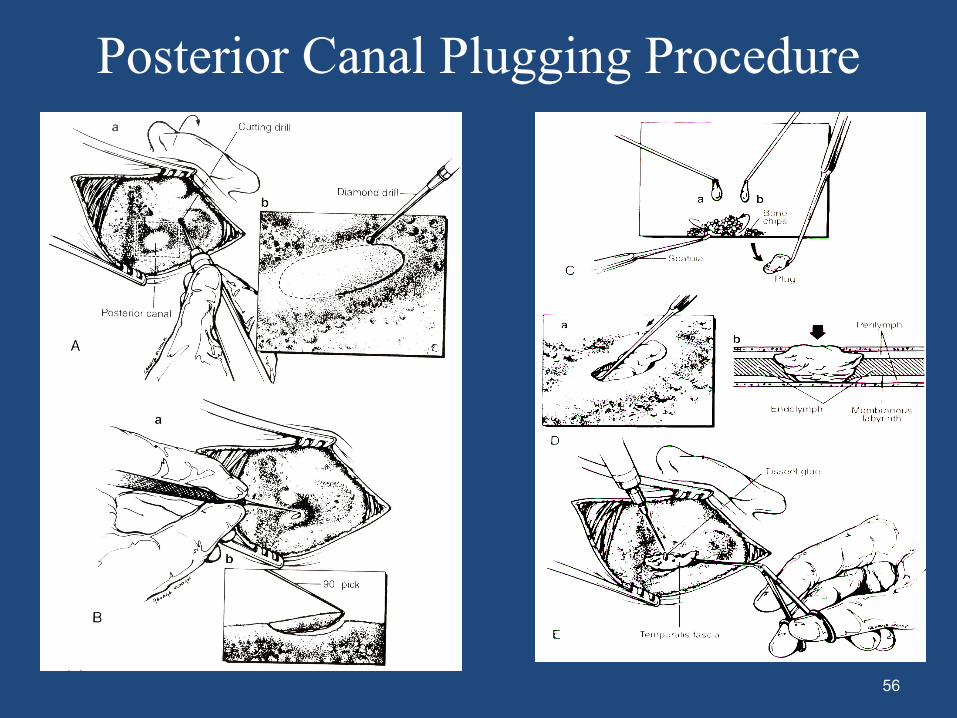
Posterior Canal Plugging Procedure
• Parnes and McLure introduced this concept.
• Prevent movement of debris towards ampulla.
• Technically simpler and safer.
• Replaced the singular neurectomy.
• Less than 20% hearing loss.
55
Posterior Canal Plugging Procedure
56
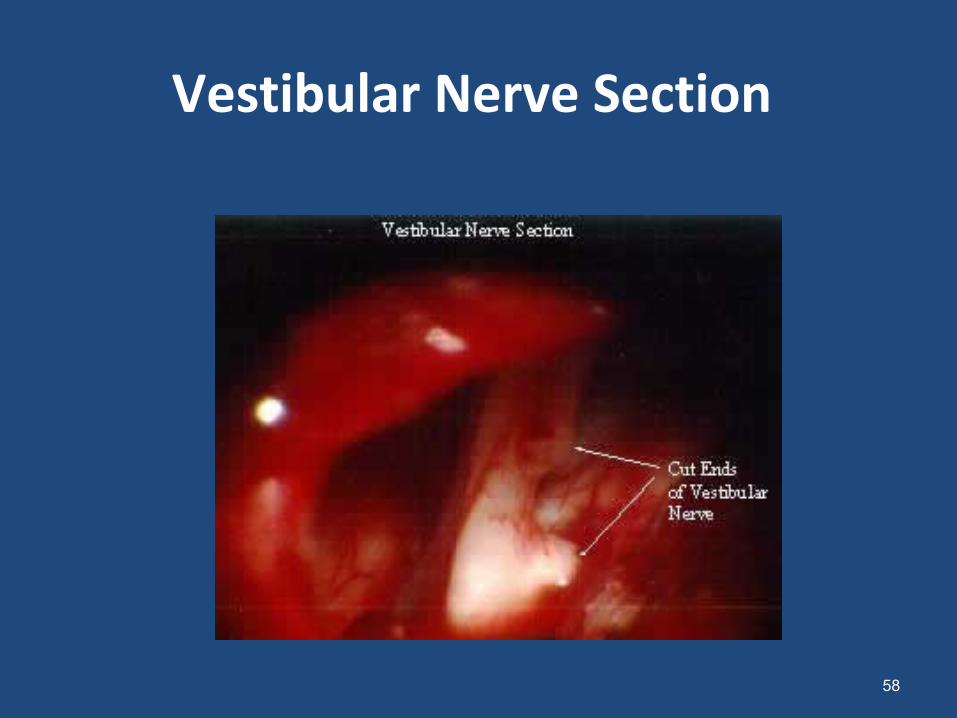
Vestibular Nerve Section
• Done when the attacks of vertigo cannot be controlled with medication. Seems unreasonably aggressive for BPPV
• Approaches – Middle fossa, retrolabyrinthine, retrosigmoid
• The vestibular part of the nerve is cut. • The operation is done with a neurosurgeon and takes
about two hours. • The success rate (no vertigo attacks) is over 90%. • The hearing is slightly affected.
57
Vestibular Nerve Section
58
Bibliography
• Scott Brown Otorhinolaryngology, Head and Neck surgery, 7th edition
• Otorhinolaryngology Head & Neck Surgery,
Ballenger (17th edition)• Galsscock – Shambaugh Surgery of the Ear 5th
edition• Cumming’s otolaryngology, head and neck surgery
4th edition59

• Thank you
60