2. vento m oxygen in delivery room and in nicu...
TRANSCRIPT

31/3/17
1
IPOKRATES SEMINAR
Neonatal Respiratory Support: State-‐of-‐the-‐art in respiratory support,
delivery room care, hemodynamic, monitoring, prevenCon and treatment of chronic lung disease.
.
La Spezia, Liguria, Italy April 2017
Máximo Vento MD PhD Spanish Maternal and Neonatal Network SAMID
InsCtute Carlos III (Ministry of Economy, Industry, CompeCCveness) Health Research Center / Division of Neonatology
University & Polytechnic Hospital La Fe Valencia (Spain)
F E D E R
How to approach oxygenaCon in the preterm infant: DR and beyond.
Schneider H Resp Physiol Neurobiol 2011
ParCal pressure of oxygen in the intervillous space
OxygenaCon in the fetal life
La Spezia 3
Embryo Placen
ta>o
n Mature placenta
Placenta 50mmHg
Exocelomic cavity (10-20mmHg)
30 Oxy
gen
part
ial p
ress
ure
(mm
Hg)
inspired air (150mmHg)
alveolar air (120mmHg)
maternal arterial blood
(90mmHg)
20
10 Embryo
(10-20mmHg)
Fetus (25-50mmHg)
NEWBORN 70-80 mmHg
40 50
60
70
80
90
100
110
120
130
140
150
Torres-‐Cuevas I et al Redox Biol 2017 La Spezia 4
OxygenaCon in the fetal life
La Spezia
• High combined Ventricular Output (400 ml x kg-‐1x min-‐1)
• High haemoglobin content (16-‐17 g/dL)
• Fetal haemoglobin (HgbF) 100%
Murphy JP Anaesth, Crit Care & Pain 2005 5 Forkner et al Anesthesiology 2007
Oxygen administraCon to the mother: fetal response
p<0.001
p<0.001
100 200 300 400 500 mmHg
Maternal arterial pO2
Fetal pO2 mmHg
60 50 40 30 20 10
Umbilical vein
Umbilical artery
La Spezia 6

31/3/17
2
Khaw KS et al BJ Anaesth 2002
MATERNAL [MDA] UMBILICAL VEIN 8-‐ISOPROSTANES
La Spezia
Oxygen administraCon to the mother: fetal response
7
META-‐TYR/PHENYL RATIO 8dG/2dG RATIO
Escobar JJ et al – Neonatology 2012 La Spezia
0
10
20
30
40
50
60
1,00 10,00 100,00 1000,00
Meta-‐tyrosine
/ Phe
nylalanine
ra>o
EPO (mU/ml)
0
10
20
30
40
50
60
70
80
90
100
1 10 100 1000 8-‐oxo-‐dihydrogua
nosine
/ 2 dihydroguan
osine
ra>o
EPO (mU/ml)
Fetal hypoxia and oxidaCve stress and maternal condiCons (pre-‐eclampsia; diabetes)
8
OxygenaCon in the fetal to neonatal transiCon and stabilizaCon
La Spezia 9
Defining the reference range for SpO2 in term and preterm infants
La Spezia 10
0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18 20 Time aaer birth (min)
Pred
uctal SpO
2 (%
)
SpO2 in ELGA neonates ≤ 28 weeks gesta>on (n=29)
La Spezia 11 Vento M et al SFNM 2010
SpO2 polynomial adjustment curve (± std) in “control” ELGA neonates (≤ 28 weeks gesta>on) (n=29).
La Spezia 12 Vento M et al SFNM 2010
31/3/17
3
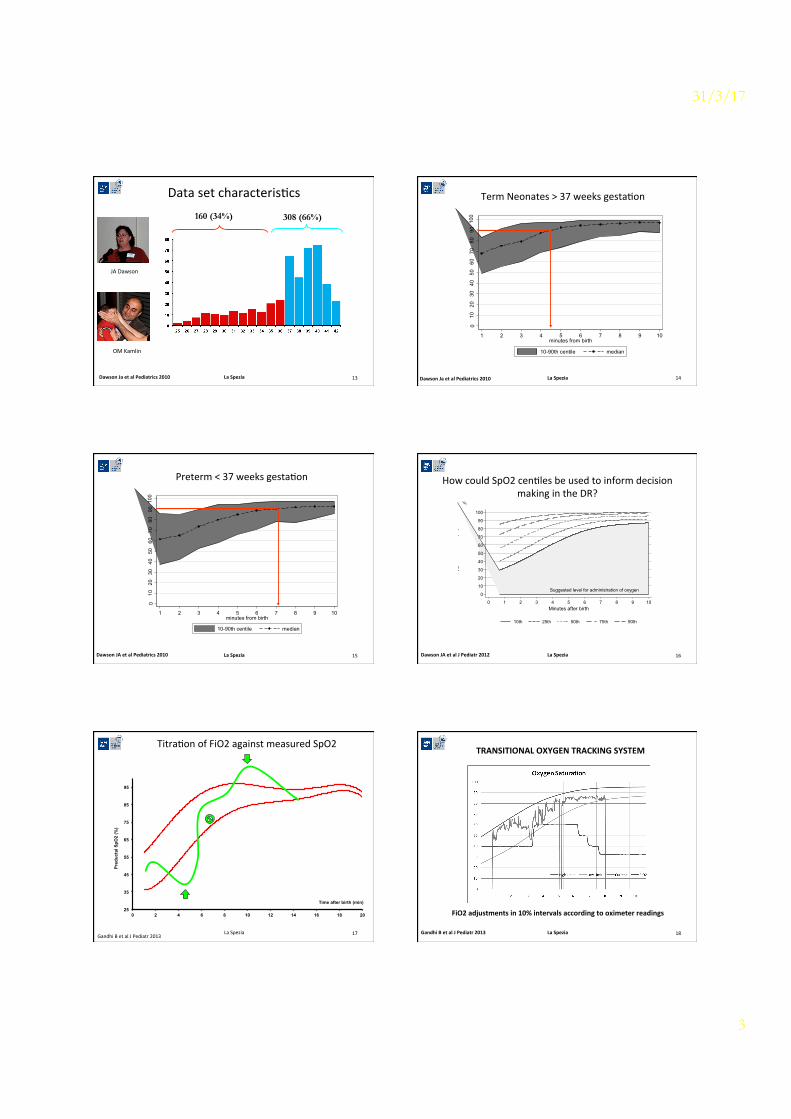
Data set characterisCcs 160 (34%) 308 (66%)
Dawson Ja et al Pediatrics 2010 La Spezia 13
JA Dawson
OM Kamlin
010
2030
4050
6070
8090
100
Oxy
gen
satu
ratio
n (%
)
1 2 3 4 5 6 7 8 9 10minutes from birth
10-90th centile median
Term Neonates > 37 weeks gestaCon
Dawson Ja et al Pediatrics 2010 La Spezia 14
010
2030
4050
6070
8090
100
Oxy
gen
satu
ratio
n (%
)
1 2 3 4 5 6 7 8 9 10minutes from birth
10-90th centile median
Preterm < 37 weeks gestaCon
Dawson JA et al Pediatrics 2010 La Spezia 15
Suggested level for administration of oxygen0
10
20
30
40
50
60
70
80
90
100
Oxy
gen
satu
ratio
n(%
)
0 1 2 3 4 5 6 7 8 9 10Minutes after birth
10th 25th 50th 75th 90th
How could SpO2 cenCles be used to inform decision making in the DR?
Suggested level for administration of oxygen0
10
20
30
40
50
60
70
80
90
100
Oxy
gen
satu
ratio
n(%
)
0 1 2 3 4 5 6 7 8 9 10Minutes after birth
10th 25th 50th 75th 90th
Suggested level for administration of oxygen0
10
20
30
40
50
60
70
80
90
100
Oxy
gen
satu
ratio
n(%
)
0 1 2 3 4 5 6 7 8 9 10Minutes after birth
10th 25th 50th 75th 90th
La Spezia 16 Dawson JA et al J Pediatr 2012
25
35
45
55
65
75
85
95
0 2 4 6 8 10 12 14 16 18 20
Pred
ucta
l SpO
2 (%
)
Time after birth (min)
TitraCon of FiO2 against measured SpO2
La Spezia 17 Gandhi B et al J Pediatr 2013
TRANSITIONAL OXYGEN TRACKING SYSTEM
FiO2 adjustments in 10% intervals according to oximeter readings
La Spezia 18 Gandhi B et al J Pediatr 2013

31/3/17
4
Oxygen supplementaCon in preterm infants during postnatal stabilizaCon
• What iniCal oxygen inspiratory fracCon (FIO2) is best?
• What SpO2 targets should be achieved upon stabilizaCon?
La Spezia 19
IniCal FiO2 for preterm in the delivery room
La Spezia 20
21%
30%
60%
100%
Feasibility study in preterm with different iFiO2
La Spezia 21 Escrig R et al Pediatrics 2008 Vento M et al Pediatrics 2009 Wang CL et al Pediatrics 2009
30% vs 90%
21% vs 100%
Hydroxyl radical derived oxidaCve stress and BPD
0
5
10
15
20
BPD NO BPD
O-‐tyr/phenyl day 7 8oxodG/2dg day 7
40.0
30.0
20.0
10.0
O-‐tyr/Phe
nyl 8-‐oxodG/2dG
** **
22 Vento M et al Pediatrics 2009 La Spezia
TORPIDO 21% vs. 100% : SpO2 (95% CI) first 10 min
La Spezia 23 Oei JL al Pediatrics 2017
SpO2 ≤28 weeks gestation
TORPIDO: overall mortality
La Spezia 24
21% O2 100% O2 Rela>ve Risk (RR) [95% CI]
P
<28 weeks 10/46 (22%) 3/54 (6%) 3.9 (1.1-‐13.3) 0.03 >28 weeks 4/98 (4%) 2/89 (2%) 1.8 (0.3-‐9.6) 0.68
Oei JL al Pediatrics 2017
No paCents >29 completed weeks’ gestaCon died
31/3/17
5
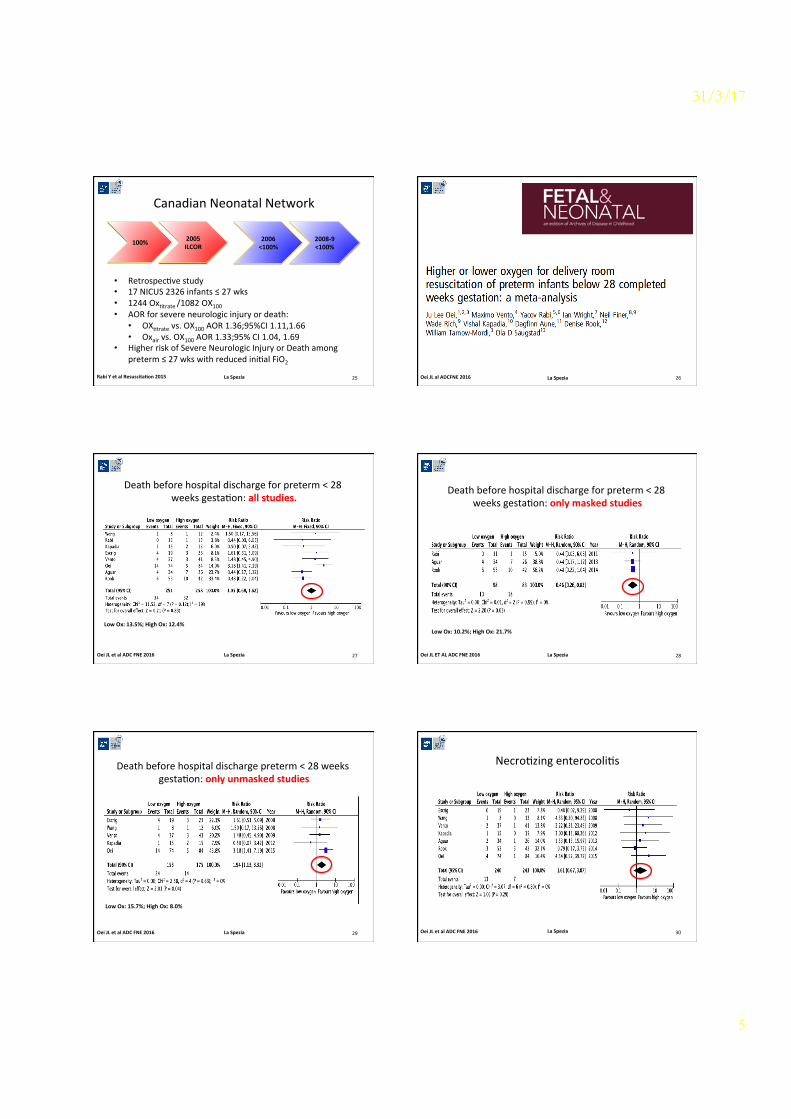
Canadian Neonatal Network
La Spezia 25
100% 2005 ILCOR
2006 <100%
2008-‐9 <100%
• RetrospecCve study • 17 NICUS 2326 infants ≤ 27 wks • 1244 OxCtrate /1082 OX100 • AOR for severe neurologic injury or death: • OXCtrate vs. OX100 AOR 1.36;95%CI 1.11,1.66 • Oxair vs. OX100 AOR 1.33;95% CI 1.04, 1.69
• Higher risk of Severe Neurologic Injury or Death among preterm ≤ 27 wks with reduced iniCal FiO2
Rabi Y et al Resuscita>on 2015 La Spezia 26 Oei JL al ADCFNE 2016
Death before hospital discharge for preterm < 28 weeks gestaCon: all studies.
La Spezia 27
Low Ox: 13.5%; High Ox: 12.4%
Oei JL et al ADC FNE 2016
Death before hospital discharge for preterm < 28 weeks gestaCon: only masked studies
La Spezia 28
Low Ox: 10.2%; High Ox: 21.7%
Oei JL ET AL ADC FNE 2016
Death before hospital discharge preterm < 28 weeks gestaCon: only unmasked studies
La Spezia 29
Low Ox: 15.7%; High Ox: 8.0%
Oei JL et al ADC FNE 2016
NecroCzing enterocoliCs
La Spezia 30 Oei JL et al ADC FNE 2016
31/3/17
6
La Spezia 31
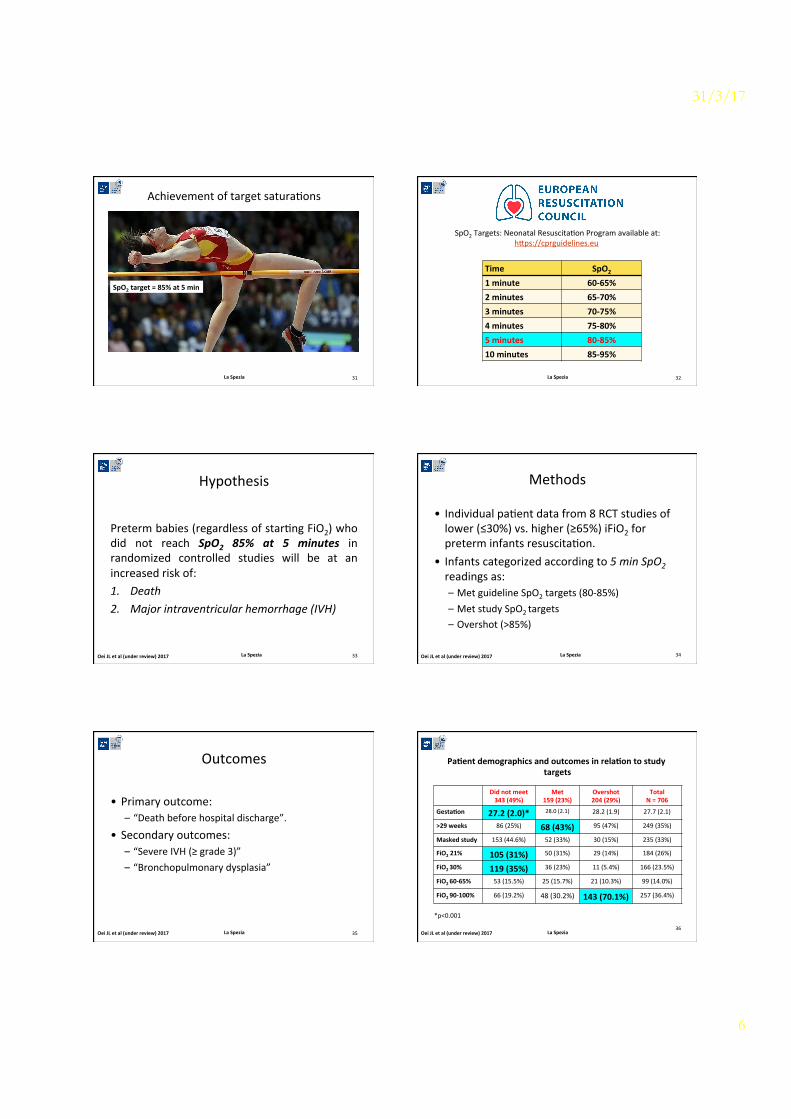
SpO2 target = 85% at 5 min
Achievement of target saturaCons
SpO2 Targets: Neonatal ResuscitaCon Program available at: hrps://cprguidelines.eu
Time SpO2 1 minute 60-‐65% 2 minutes 65-‐70% 3 minutes 70-‐75% 4 minutes 75-‐80% 5 minutes 80-‐85% 10 minutes 85-‐95%
La Spezia 32
Hypothesis
Preterm babies (regardless of starCng FiO2) who did not reach SpO2 85% at 5 minutes in randomized controlled studies will be at an increased risk of: 1. Death 2. Major intraventricular hemorrhage (IVH)
La Spezia 33 Oei JL et al (under review) 2017
Methods
• Individual paCent data from 8 RCT studies of lower (≤30%) vs. higher (≥65%) iFiO2 for preterm infants resuscitaCon.
• Infants categorized according to 5 min SpO2 readings as: – Met guideline SpO2 targets (80-‐85%) – Met study SpO2 targets – Overshot (>85%)
La Spezia 34 Oei JL et al (under review) 2017
Outcomes
• Primary outcome: – “Death before hospital discharge”.
• Secondary outcomes: – “Severe IVH (≥ grade 3)” – “Bronchopulmonary dysplasia”
La Spezia 35 Oei JL et al (under review) 2017
Pa>ent demographics and outcomes in rela>on to study targets
Did not meet 343 (49%)
Met 159 (23%)
Overshot 204 (29%)
Total N = 706
Gesta>on 27.2 (2.0)* 28.0 (2.1) 28.2 (1.9) 27.7 (2.1)
>29 weeks 86 (25%) 68 (43%) 95 (47%) 249 (35%)
Masked study 153 (44.6%) 52 (33%) 30 (15%) 235 (33%)
FiO2 21% 105 (31%) 50 (31%) 29 (14%) 184 (26%)
FiO2 30% 119 (35%) 36 (23%) 11 (5.4%) 166 (23.5%)
FiO2 60-‐65% 53 (15.5%) 25 (15.7%) 21 (10.3%) 99 (14.0%)
FiO2 90-‐100% 66 (19.2%) 48 (30.2%) 143 (70.1%) 257 (36.4%)
*p<0.001
La Spezia 36
Oei JL et al (under review) 2017
31/3/17
7
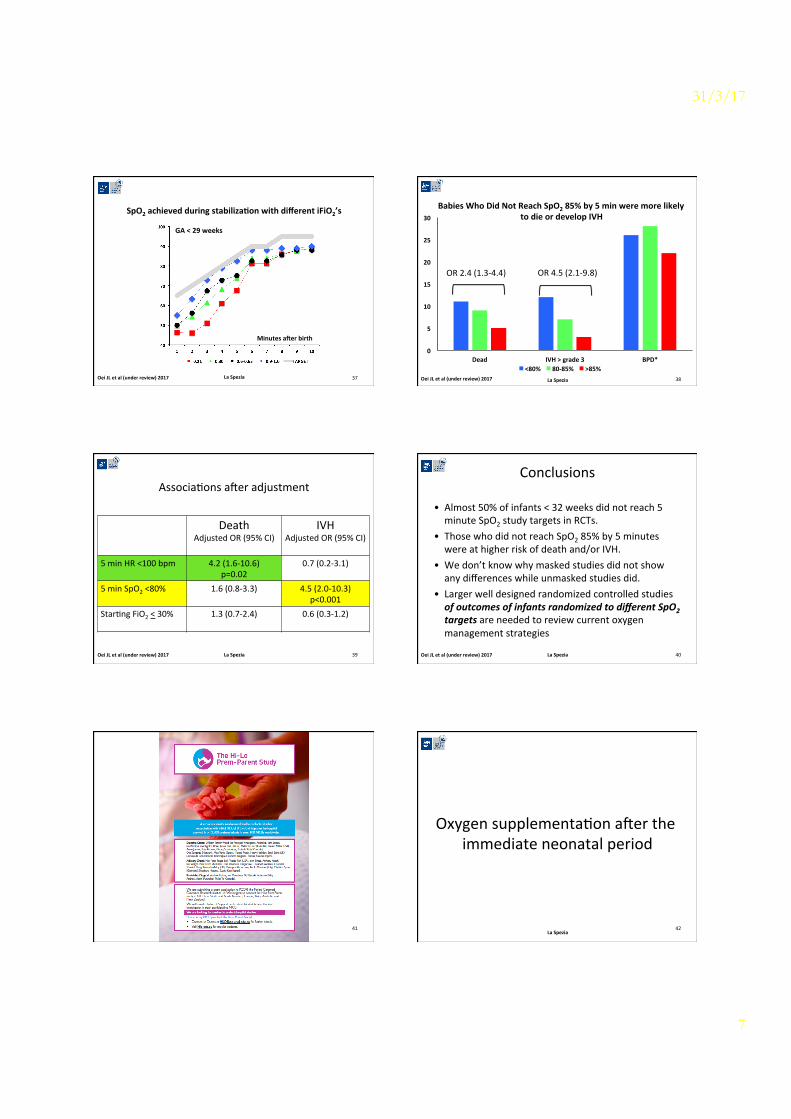
SpO2 achieved during stabiliza>on with different iFiO2’s
La Spezia 37
All gesta>onal ages
Minutes aaer birth
GA > 29 weeks
Minutes aaer birth
GA < 29 weeks
Minutes aaer birth
Oei JL et al (under review) 2017
Babies Who Did Not Reach SpO2 85% by 5 min were more likely to die or develop IVH
0"
5"
10"
15"
20"
25"
30"
Dead" IVH">"grade"3" BPD*"<80%" 80785%" >85%"
OR 4.5 (2.1-‐9.8) OR 2.4 (1.3-‐4.4)
38 La Spezia Oei JL et al (under review) 2017
AssociaCons awer adjustment
Death Adjusted OR (95% CI)
IVH Adjusted OR (95% CI)
5 min HR <100 bpm 4.2 (1.6-‐10.6)
p=0.02 0.7 (0.2-‐3.1)
5 min SpO2 <80% 1.6 (0.8-‐3.3) 4.5 (2.0-‐10.3) p<0.001
StarCng FiO2 < 30% 1.3 (0.7-‐2.4) 0.6 (0.3-‐1.2)
La Spezia 39 Oei JL et al (under review) 2017
Conclusions
• Almost 50% of infants < 32 weeks did not reach 5 minute SpO2 study targets in RCTs.
• Those who did not reach SpO2 85% by 5 minutes were at higher risk of death and/or IVH.
• We don’t know why masked studies did not show any differences while unmasked studies did.
• Larger well designed randomized controlled studies of outcomes of infants randomized to different SpO2 targets are needed to review current oxygen management strategies
La Spezia 40 Oei JL et al (under review) 2017
La Spezia 41
Oxygen supplementaCon awer the immediate neonatal period
La Spezia 42
31/3/17
8
ROP BPD CP NEC
M O R T A L I T Y
43 La Spezia
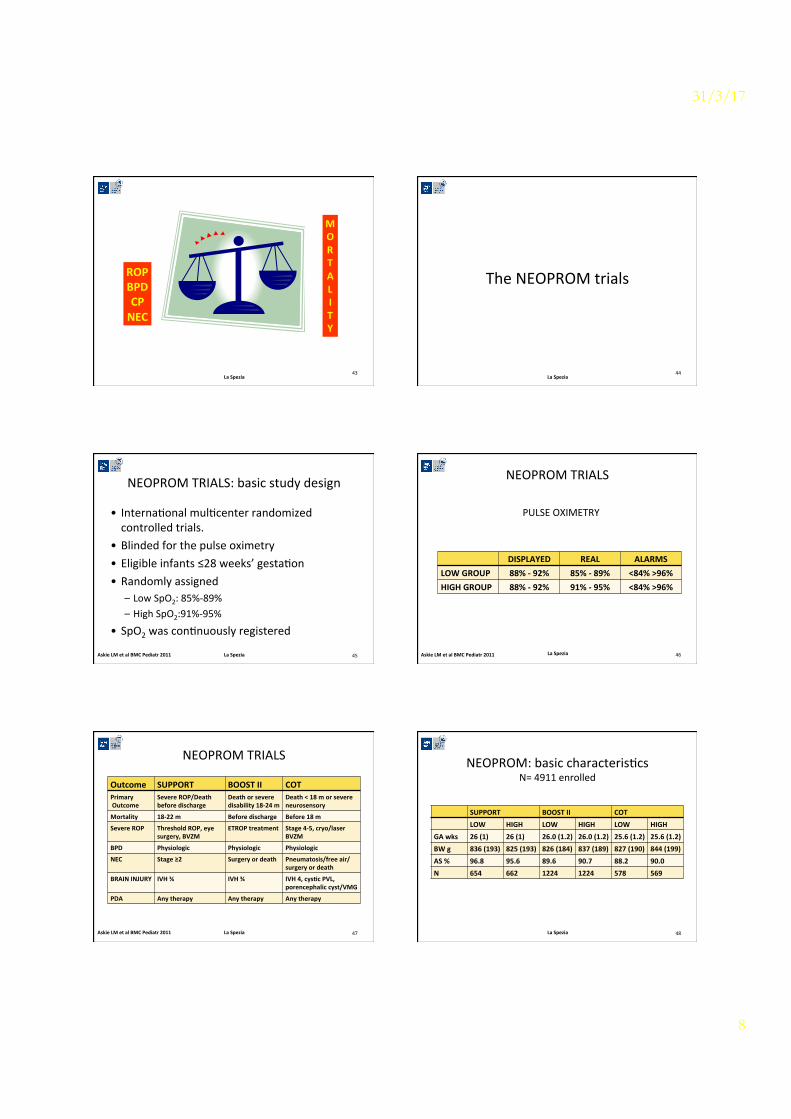
The NEOPROM trials
La Spezia 44
NEOPROM TRIALS: basic study design
• InternaConal mulCcenter randomized controlled trials.
• Blinded for the pulse oximetry • Eligible infants ≤28 weeks’ gestaCon • Randomly assigned
– Low SpO2: 85%-‐89% – High SpO2:91%-‐95%
• SpO2 was conCnuously registered
La Spezia 45 Askie LM et al BMC Pediatr 2011
NEOPROM TRIALS
DISPLAYED REAL ALARMS LOW GROUP 88% -‐ 92% 85% -‐ 89% <84% >96% HIGH GROUP 88% -‐ 92% 91% -‐ 95% <84% >96%
PULSE OXIMETRY
La Spezia 46 Askie LM et al BMC Pediatr 2011
NEOPROM TRIALS
Outcome SUPPORT BOOST II COT Primary Outcome
Severe ROP/Death before discharge
Death or severe disability 18-‐24 m
Death < 18 m or severe neurosensory
Mortality 18-‐22 m Before discharge Before 18 m
Severe ROP Threshold ROP, eye surgery, BVZM
ETROP treatment Stage 4-‐5, cryo/laser BVZM
BPD Physiologic Physiologic Physiologic
NEC Stage ≥2 Surgery or death Pneumatosis/free air/surgery or death
BRAIN INJURY IVH ¾ IVH ¾ IVH 4, cys>c PVL, porencephalic cyst/VMG
PDA Any therapy Any therapy Any therapy
La Spezia 47 Askie LM et al BMC Pediatr 2011
NEOPROM: basic characterisCcs N= 4911 enrolled
SUPPORT BOOST II COT LOW HIGH LOW HIGH LOW HIGH
GA wks 26 (1) 26 (1) 26.0 (1.2) 26.0 (1.2) 25.6 (1.2) 25.6 (1.2) BW g 836 (193) 825 (193) 826 (184) 837 (189) 827 (190) 844 (199) AS % 96.8 95.6 89.6 90.7 88.2 90.0 N 654 662 1224 1224 578 569
La Spezia 48

31/3/17
9
La Spezia
2-‐3 week
Carlo WA et al NEJM 2010
Support Trial
MORTALITY
49
NEOPROM TRIALS -‐ ALGORITHM
• New calibraCon algorithm for pulse oximeter was introduced in 2009
• In 1055 infants recruited awer 2009 mortality was significantly higher in the low SpO2 targeted group (21.8% vs. 13.3%; p<0.001)
La Spezia BOOST TRIAL II NEJM 2011 50
NEOPROM TRIALS: BOOST II
La Spezia 51
NEOPROM: Pulse oximeter algorithm modificaCon
La Spezia 52
IniCal algorithm Modified algorithm
Updated review and meta-‐analysis Acta Paediatr 2014
La Spezia 53
Saugstad OD et al Acta Paediatr 2014
Results: composite for mortality
La Spezia Saugstad OD et al Acta Paediatr 2014
Low Ox High Ox
54
31/3/17
10
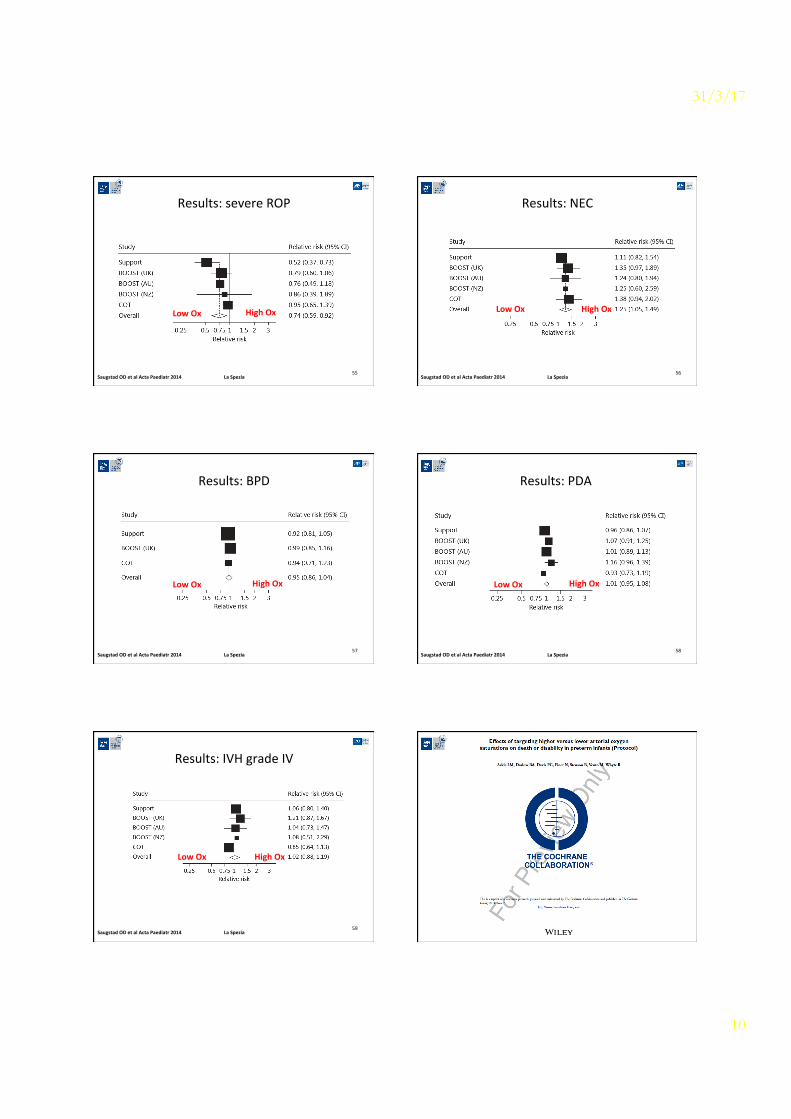
Results: severe ROP
La Spezia Saugstad OD et al Acta Paediatr 2014
Low Ox High Ox
55
Results: NEC
La Spezia Saugstad OD et al Acta Paediatr 2014
Low Ox High Ox
56
Results: BPD
La Spezia Saugstad OD et al Acta Paediatr 2014
Low Ox High Ox
57
Results: PDA
La Spezia Saugstad OD et al Acta Paediatr 2014
Low Ox High Ox
58
Results: IVH grade IV
La Spezia Saugstad OD et al Acta Paediatr 2014
Low Ox High Ox
59
31/3/17
11
La Spezia
0 10-‐15 min
55%
65%
80%
85%
90%
14-‐21 days neonatal period
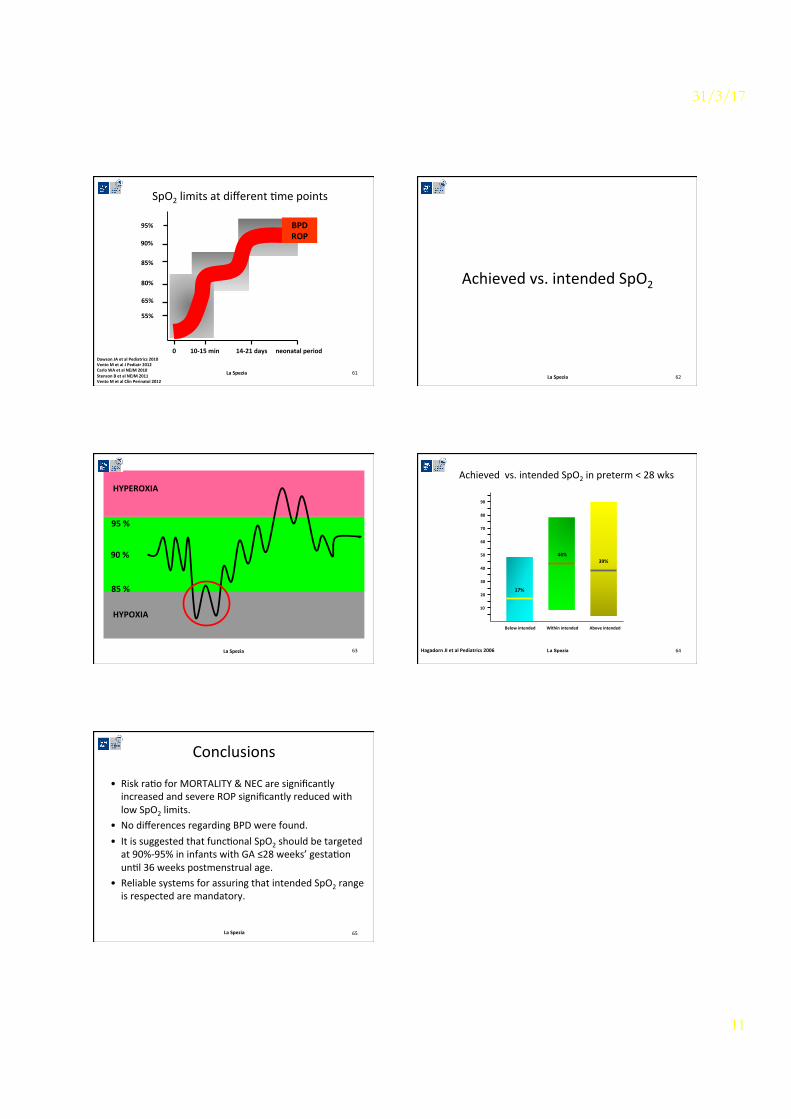
SpO2 limits at different Cme points
Dawson JA et al Pediatrics 2010 Vento M et al J Pediatr 2012 Carlo WA et al NEJM 2010 Stenson B et al NEJM 2011 Vento M et al Clin Perinatol 2012
95% BPD ROP
61
Achieved vs. intended SpO2
La Spezia 62
La Spezia
95 %
85 %
HYPEROXIA
HYPOXIA
90 %
63 La Spezia
10
20
30
40
50
60
70
80
90
Below intended Within intended Above intended
17%
44% 39%
Achieved vs. intended SpO2 in preterm < 28 wks
Hagadorn JI et al Pediatrics 2006 64
Conclusions
• Risk raCo for MORTALITY & NEC are significantly increased and severe ROP significantly reduced with low SpO2 limits.
• No differences regarding BPD were found. • It is suggested that funcConal SpO2 should be targeted at 90%-‐95% in infants with GA ≤28 weeks’ gestaCon unCl 36 weeks postmenstrual age.
• Reliable systems for assuring that intended SpO2 range is respected are mandatory.
La Spezia 65