antimicrobial steward call august 13, 2019
TRANSCRIPT

Antimicrobial Steward CallAugust 13, 2019
Tennessee Department of HealthHealthcare Associated Infections and Antimicrobial Resistance Program

Welcome
Adobe Connect Housekeeping
• All lines have been muted• Press *6 to unmute your line• Also can use the chat box to ask questions/comment

Announcements

NHSN Antibiotic Use Reporting Implementation
• Day-long training session• October 30, 2019, 8:00 – 4:00 • Belmont University, Nashville, TN
Save the Date!!

Training Agenda
• 7:30–8:15 Registration• 8:15–8:30 Welcome and TN Progress• 8:30–8:45 NHSN AU Option Basics • 8:45–9:45 Getting Leadership on Board • 9:45–10:00 Break• 10:00–11:00 Implementation First Steps• 11:00–12:00 System Wide Implementation• 12:00–1:00 Lunch• 1:00–3:00 NHSN AU Output, Data Validation, and
Using AU Data for Action• 3:00–4:00 Overcoming Software and
Implementation Barriers Panel

Registration
• https://www.cvent.com/events/national-healthcare-safety-network-antibiotic-use-reporting-symposium/registration-4705165eaa744b1aa48be5eaefde0fa1.aspx?fqp=true

4th Annual Middle TN Symposium
January 31, 2020SAVE THE DATE!

Call for Poster Abstracts
• Due October 14, 2019• Type of Projects:
– Research Projects: Describes original research or quality improvement projects. Research projects must include Background, Methods, Results, and Conclusion.
– Best Practice Reports: Describes innovative or improved services, interventions or programmatic practices in the realm of antimicrobial stewardship. Integrative and systematic reviews are also acceptable. Best Practice Reports must include Background of Problem, Methods/Intervention, Rationale, and Implications for your facilities and other antimicrobial stewardship programs.
• Submission Guidelines: http://www.belmont.edu/pharmacy/_pdf/Poster%20Abstract%20Submission%20Guidelines%202020.pdf

2019-2020 Sepsis Surveillance Project
• CDC Hospital Toolkit for Adult Sepsis Surveillance– Modified Sepsis 3 Criteria using EHR data
• Objective– Assess feasibility of implementing the Toolkit in community and
academic medical centers
• Opportunity for facilities to pilot the toolkit and provide feedback to CDC regarding further use
If your facility is interested in participating, please e-mail [email protected]

• New requirement for Joint Commission-accredited ambulatory health care organizations that routinely prescribe antibiotics
• Effective Jan 1, 2020• Medication Management Standard MM.09.01.03 with
five new Elements of Performance:
New Antimicrobial Stewardship Requirements for Ambulatory Care

New TJC Standard MM.09.01.03

Core Element Achievement

Core Elements Statistics as of June 24, 2018
Facility Type
Total number of facilities
Number of reporters
% actually have
completed survey
5+ core elements achieved
7 core elements achieved
% of reporting achieving
all 7Acute Care Hospital (non CAH) 107 102 95 101 90 88.2Critical Access Hospital 14 14 100 14 13 92.9
LTACH 9 9 100 9 9 100
IRF 30 30 100 30 28 93.3
LTCF 320 35 11 35 28 80.0

Options for Achieving Action
0 20 40 60 80 100
Rapid diagnostics
Indication documentation
Antibiotic timeout
Audit and feedback
Automatic IV to PO conversion
Restricted antibiotics
At least 1 antibiotic guideline
% of Facilities Reporting Specific Interventions
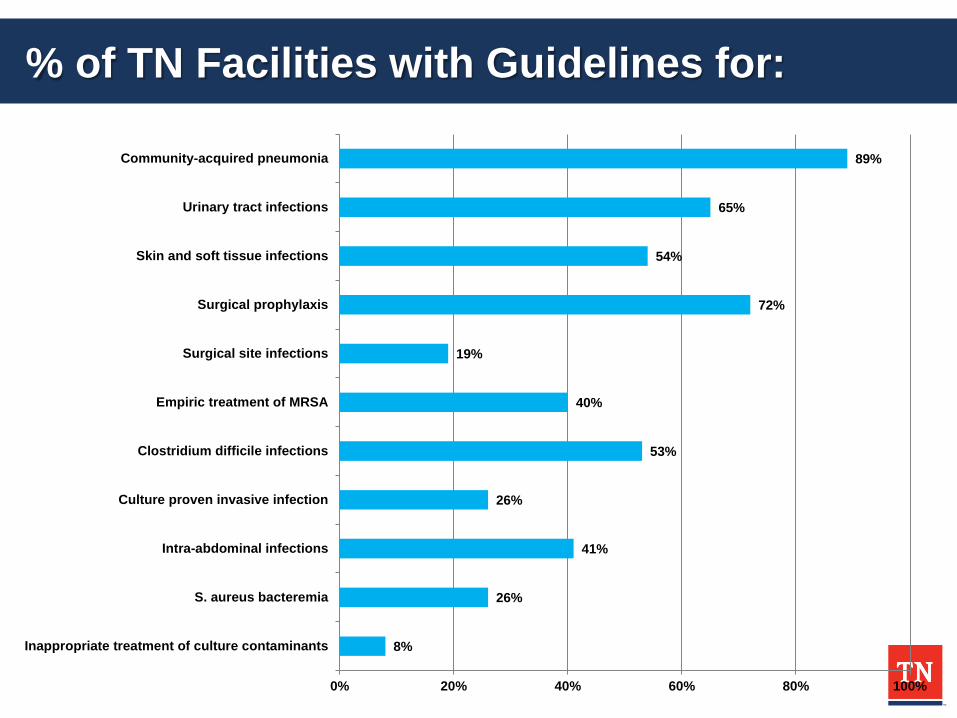
% of TN Facilities with Guidelines for:
8%
26%
41%
26%
53%
40%
19%
72%
54%
65%
89%
0% 20% 40% 60% 80% 100%
Inappropriate treatment of culture contaminants
S. aureus bacteremia
Intra-abdominal infections
Culture proven invasive infection
Clostridium difficile infections
Empiric treatment of MRSA
Surgical site infections
Surgical prophylaxis
Skin and soft tissue infections
Urinary tract infections
Community-acquired pneumonia

MRSA Guidelines
Only 40% of TN facilities have guidelines developed for (empiric
treatment of) MRSA

MRSA

Healthcare-Onset MRSA Bacteremia LabID SIR for Acute Care Hospitals, 01/01/2015–03/31/2019

NHSN: National Healthcare Safety NetworkED: Blood Culture taken in Emergency DepartmentCO: Community-Onset (day 1, 2 or 3 of admission)HO: Hospital-Onset (day 4 or later)
CDC, Vital Signs Town Hall, March 2019

ED MRSA BSI per 10,000 Encounters
2011
2014
20177.8 7.9
2.6
2.3 1.9
13.79.6
7.6
3.4
1.6
2.4
Southeast Tennessee
3.9
Northeast Tennessee
6.8Upper Cumberland
7.7West Tennessee
6.8
Mid Cumberland
4.8 East Tennessee
11.8
Memphis Delta
5.1
South Central
5.9
2018
ED MRSA Rate<= 0.8 per 10,0000.9-2 per 10,0002.1-3.2 per 10,0003.3-4.4 per 10,0004.5-5.6 per 10,0005.7-6.8 per 10,000>= 6.9 per 10,000
CDC, Vital Signs Town Hall, March 2019

TN EIP: ED MRSA Events with IDU Noted in Chart
EIP: Emerging Infections ProgramIDU: Injection Drug Use
CDC, Vital Signs Town Hall, March 2019

30 Day and 1 Year All Cause Mortality, MRSA-BSI by Class, TN, 2015-2017
18.1% 20.3%
33.5%34.9%37.4%
49.9%
0%
10%
20%
30%
40%
50%
60%
CO-ED CO-IP HO
30 Day Mortality 1 Year Mortality
CO-ED: Blood Culture taken in Emergency Department
CO-IP: Community-Onset (day 1, 2 or 3 of admission)
HO: Hospital-Onset (day 4 or later)
CDC, Vital Signs Town Hall, March 2019

Despite 31% Decrease in Hospital-Onset MRSA BSI deaths*, All MRSA BSI Deaths Increase by 21%
All MRSA BSI(21% increase)
Hospital Onset MRSA BSI(31% decrease)
Deaths
• 2011 estimates based on TN’s 30 day mortality rates for 2015-2017 by class (CO-ED, CO-IP, HO)
• 2017 estimates based on applying 2017 mortality by class
• Data obtained from NHSN (MRSA LabID for TN hospitals) matched to TN Vital statistics data
13392
463
559
0
100
200
300
400
500
600
2011 2017Preliminary data
CDC, Vital Signs Town Hall, March 2019

THA MRSA Action Plan

Tennessee Center forPatient Safety
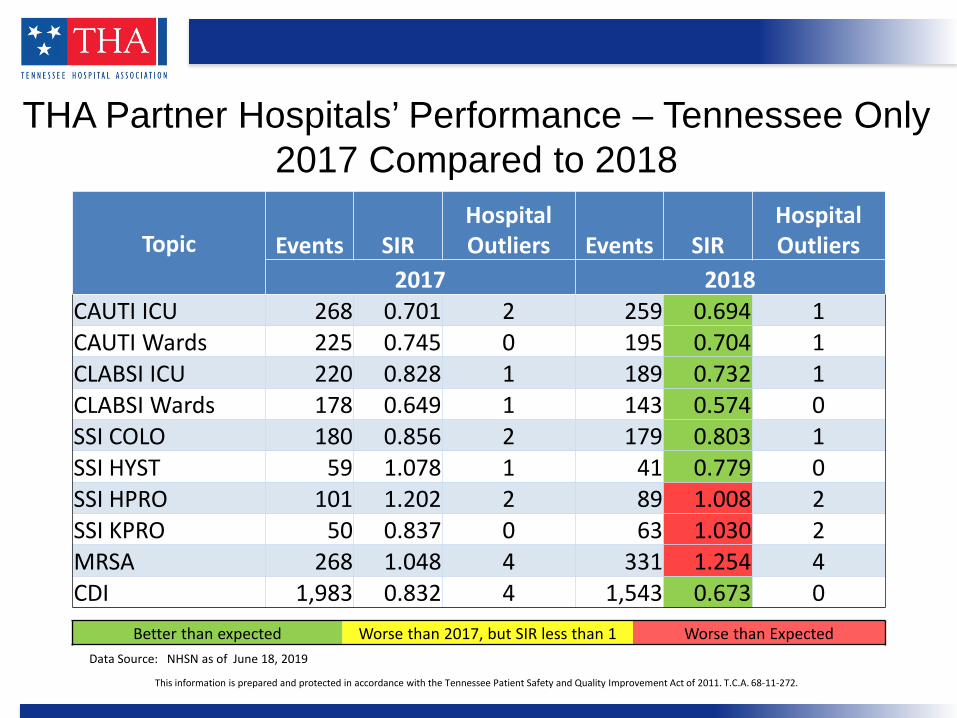
THA Partner Hospitals’ Performance – Tennessee Only2017 Compared to 2018
Data Source: NHSN as of June 18, 2019
This information is prepared and protected in accordance with the Tennessee Patient Safety and Quality Improvement Act of 2011. T.C.A. 68-11-272.
Better than expected Worse than 2017, but SIR less than 1 Worse than Expected
Topic Events SIRHospital Outliers Events SIR
Hospital Outliers
2017 2018CAUTI ICU 268 0.701 2 259 0.694 1CAUTI Wards 225 0.745 0 195 0.704 1CLABSI ICU 220 0.828 1 189 0.732 1CLABSI Wards 178 0.649 1 143 0.574 0SSI COLO 180 0.856 2 179 0.803 1SSI HYST 59 1.078 1 41 0.779 0SSI HPRO 101 1.202 2 89 1.008 2SSI KPRO 50 0.837 0 63 1.030 2MRSA 268 1.048 4 331 1.254 4CDI 1,983 0.832 4 1,543 0.673 0

Methicillin-resistant Staphylococcusaureus (MRSA)
Hospital-onset Bloodstream LabIDInfections as reported to CDC
NHSN


THA Board Directive• At the Feb. meeting, the board requested TCPS develop
a targeted action plan to address MRSA with specific strategies and communication to CEOs–Share individual data with CEO, if high events. Call them and do site visits, if needed.
–Specific list of steps to address. Request to get prescriptive on what is expected and measure accountability.
–Consider a state campaign to get everyone on board like THA early elective delivery project. Get physicians/hospitals on board together to a focused goal.
Updated CDC Guidance and Recommendations
• CDC March 2019 Vital Signs report on staph infections• New Resource: Strategies to Prevent Hospital-onset
Staphylococcus aureus Bloodstream Infections in Acute Care Facilities
https://www.cdc.gov/hai/prevent/staph-prevention-strategies.html
MRSA Action Plan Goals
• Current State: TN Standardized Infection Ratio is 1.3 for CY 2018 among the Acute Care Facilities. There were 336 events in 2018.
• Desired State: Meet or exceed the HHS 2020 Goal for Hospital-Onset MRSA bloodstream infections of 0.5 SIR by December 31, 2021.
• Interim Targets for aggregate state performance proposed by THA Quality Committee:
• 10% reduction to a SIR of 1.2 by 12/31/2019• 40% reduction to a SIR of 0.8 by 12/31/2020• Achieve SIR of 0.5 by 12/31/2021• 50% overall reduction in HO MRSA events

MRSA Action Plan
Why •MRSA bacteremia has a high incidence of mortality with an estimated 23% mortality.
•Based on 2018 events, estimated 77 possibly preventable deaths.
•Cost of MRSA treatment is approximately $34,657 per case, so excess total costs of $11.64 million.

THA Baseline Survey
82%
44% 44%
84%
51%
27% 27%
65%
ICU PATIENTS CARDIOTHORACIC NEUROSURGERY ORTHOPEDIC
CHG Bathing and Nasal Decolonization
CHG Bathing Nasal Decolonization
60 total responses - 50 responses on CHG baths;37 responses on nasal decolonization

THA Baseline SurveyVariability in Practice
90%
59%
93%
27%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Contact Precautions for MRSA Infection
Contact Precautions for MRSA colonization
Audit for Completion of Practices
Audit for Competency of Practices
Other MRSA Prevention Practices

THA Action Plan Recommendations• Adoption of CDC Guidance Core Strategies focused on
MRSA transmission among high-risk patients during high-risk periods–ICU patients-CHG daily bathing while in ICU with nasal
decolonization–High-risk surgeries (cardiothoracic, orthopedic and neurological
surgeries) -Preoperative CHG bathing with nasal decolonization–Supplemental strategies based on performance and risk
assessment• All hospitals conduct a risk assessment and gap analysis
to address the CDC recommendations for overall infection prevention practices and adopt supplemental strategies as needed to address individual facility risks

THA Action Plan• Education Plans
– Established an advisory committee of local infection prevention experts
–August 20 – Workshop to launch efforts–Webinar/Collaborative series to support implementation with national experts and local success sharing
–Campaign approach–Enlist support and partnerships with key stakeholder groups
• Education materials for hospitals, including toolkit of resources
• Public outward-facing campaign after implementation begins

THA Action Plan• Letter of commitment from hospital/system leadership
–Sign commitment to participate by Aug. 30–Begin implementation into practice by Sept. 30
• Endorsement of THA Action Plan by the THA Quality Committee and CMO Society for adoption of CDC MRSA updated guidance with emphasis on core strategies for high-risk populations during high-risk times
• Approved by THA Board July 10th

We Need You!!!• Support plan implementation
– Some hospitals may include product for decolonization in the pharmacy• May be engaged as part of the multi-disciplinary team for
implementation• Watch and report trends

Next Steps
• Next Call– October 8 at 2pm Eastern/1pm Central Time
• Opportunities for involvement– THA MRSA Workshop – August 20 – AU Reporting Symposium – October 30– Belmont Symposium – January 31, 2020 – Speaker or Topic for future call
• Feedback always appreciated– [email protected]