chapter 5- stake holder analysis -...
TRANSCRIPT

123
Chapter 5- Stake holder Analysis
124
5. Stakeholder Analysis
Defining Stakeholders
The actual word ―stakeholder‖ first appeared in the management literature in an internal
memorandum at the Stanford Research Institute (now SRI International, Inc.,), in 1963.
The term ‗stakeholder‘ has numerous definitions, many of which are linked to the context
in which the term is being used. Schmeer (1999) suggested that stakeholders can include
members, employees, related organizations, potential partners, suppliers, the public,
regulatory bodies, and the government. Not-for-profit organizations and the voluntary
sector may also add clients, community groups, community leaders, volunteers and donors
to their list of stakeholders. In commercial organizations customers and owners are also
included as key stakeholders. Freeman (1984), whose work is credited for the development
of stakeholder theory and his seminal book titled ―Strategic Management- a Stakeholder
Approach‖ defines stakeholders as:
“A stakeholder in an organization is any group or individual who can affect or is affected
by the achievement of the organization‟s objectives”.
Thus, for the current study, the stakeholder is defined as:
―An individual, group or organization which has a share or interest in insurer-provider
relationship and is a party that affects or can be affected (either positively or negatively) by
the proposed strategies for synergy between provider and insurer‖36
.
The notion of ―paying attention to key stakeholder relationships‖ (Freeman, 1999) is and
has been a major theme in the strategic management literature. In fact, superior stakeholder
satisfaction is critical for successful companies in a hypercompetitive environment
(D‘Aveni, 1994). Empirical research has begun to investigate what determines the success
or failure of relationships between exchange partners. This has been accomplished by
examining both the characteristics of the organization as well as the specific stakeholder
groups and the nature of the interaction between them (Pfeffer, 1981; Jensen & Meckling,
36
Note: The definition is linked to our theoretical model, unit of study and the strategic triangle.

125
1976; Morgan & Hunt, 1994; Parsons, 2001). An assumption has been made in much of
the empirical and conceptual work is that developing and maintaining relationships are
desirable goals for both the stakeholder and the organization (Dwyer, Schurr & Oh, 1987;
Wilson, 1995). The Canadian Association (2004) informs that whether an organization is
working on a strategic plan, developing a policy or planning to implement an action, it is
essential to consult with key stakeholders as this is an important factor in achieving
ultimate success.
The stakeholder concept is deceptively simple. It is ―simple‖ because it is easy to identify
those groups and individuals who can affect, or are affected by the achievement of any
organization‘s purpose. It is ―deceptive,‖ because once stakeholders are identified; the task
of managing the relationship with them is enormous. The variety of ―stakes,‖ the necessity
of looking at multiple levels of analysis and the need to invent processes for taking
stakeholder concerns into account make a stakeholder approach to strategic management
quite complicated (Freeman, 1984).
The stakeholders Map
Figure 5.1: Potential Other Stakeholders in the Health Insurance Market
Source: Author‟s own creation

126
Table 5.1: Stakeholders - Rational for engagement and Competency (I)
Stakeholder Rationale for engagement Competency
Insured
Customers
They are the ultimate beneficiary in the health insurance
market and a common customer to both the insurers and
the providers.
Competency is low
both at treatment
and health
insurance level.
Doctors Doctors play an important role at the time of treatment of
insured patients and their decision has a direct impact on
the claim cost. They are the final decision maker when it
comes to line of treatment and their authority cannot be
easily challenged.
High competency
level w.r.t
treatment part and
Medium to low
w.r.t. health
insurance
Nursing Staff They play a major role in the delivery of health care
services. They are in direct touch with the insured patient
and spend more time with the patients than the treating
doctors. They can act as a source of control and
verification. Also, as a sharing resource.
Medium level
w.r.t. treatment
and low w.r.t
health insurance
Brokers Brokers are the intermediary between the insured and the
insurer. As per law they act on behalf of the insured
customer and get their commission from the insurance
companies. In corporate health insurance they play a major
role in decision making.
High competency
w.r.t. insurance
knowledge , less to
moderate in terms
of treatment and
healthcare
Agents and
Advisors
They act as an important intermediary at an individual
level. They are the connecting link between the customer
and the insurance companies. As per law they need to have
appropriate licensing. In retail policy, they are the
individuals who fill the proposal form for health insurance.
Moderate to high
w.r.t. insurance
and low w.r.t.
treatment and care
part
TPA They are the extended arm of the insurance company and
are regulated by the IRDA. They play an important role in
extending cashless benefit, contract negotiation with
providers, enrollment and claim administration. Off late
they have started providing services like pre-policy check-
up, underwriting, value added services like health check-up
and fraud investigation services.
High w.r.t health
insurance and
moderate to high
w.r.t. treatment
and care part
NGOs and
Community
at large
In the rural space the role played by the NGOs is quite
critical. The social health insurance schemes depend
heavily on the support of the community at large. There are
NGOs which are working in the area of microfinance and
health insurance. They can help in the implementation of
social health insurance policies and also monitoring the
delivery of health care services at the local level.
High to moderate
in their respective
areas (NGOs).
Moderate to low
(community at
large)

127
Table 5.2: Stakeholders - Rational for engagement and Competency (II)
Stakeholder Rationale for engagement Competency
Regulator In India insurance industry is regulated by IRDA.
They are responsible for licensing of insurance
companies, TPAs, agents and brokers and ensure
orderly growth of the insurance industry. All the
health insurance products which are launched in the
market had to be filed with the regulator. They also
play a role in handling customer grievances. As
regulators they have extreme powers to change the
growth trajectory of the health insurance industry.
High w.r.t.
insurance.
Moderate to low
w.r.t. health care
and treatment part
Govt. Bodies The ministry like Finance, Health& family welfare can
play a major role in developing and launching policies
which can have a big impact in the Indian health
insurance market (affecting both the insurers and
providers) e.g. The increasing of FDI in insurance
sector from current 26 percent to 49 percent; health
insurance portability act; clinical establishment
(registration and regulation) bill. The State bodies can
also play an important role as health is a State subject.
High in their
respective areas
Pharmaceutical&
Medical
Equipment
Industry
They play a major role in healthcare industry and are
considered to have a strong lobby at the policy level.
They have the financial strength and power to directly
affect the cost of health care. They are the major
suppliers for the providers and has the potential to
create value added services for the insurance industry
e.g. offering discounts on pharmacy and diagnostics.
Their existing relationship with providers and doctors
can act as a source for developing synergy between
insurers and providers.
High in the area of
treatment and
medical care, low
in the area of
insurance
I.T Industry They affect both the insurance and the healthcare
industry. Information technology can play an
important role in bringing in efficiency and
effectiveness. They can help built a strong
communication bridge between the insurance
companies, intermediaries and the providers. It also
has the potential to affect the cost part apart from
supplying analytical tools for better decision making.
High in their
respective areas
Education
Institutions
In health insurance industry they play a major role in
supplying quality and trained manpower across the
levels and intermediaries. They can act as a source of
center for excellence in health insurance and fulfill the
talent gap currently existing in the health insurance
industry both at the technical and managerial levels.
High in their
respective areas

128
For the purpose of the current study and based on the above definition, the following are
identified as potential stakeholders: Insured; Doctors; Nursing Staff; Brokers; Agents and
Advisors; TPA‘s; NGOs and Community at large; Regulator; Govt. Body; Pharmaceutical
and Medical Equipment Industry; I.T. Industry and Education Institutions (Figure 5.1).
If one consider health insurance companies and health care providers as organizations
aiming to bring in synergy then studying their relationship with the above listed
stakeholders becomes important. The list of stakeholders had been tabulated stating the
rationale for engagement along with their competency in the areas of insurance and
healthcare respectively. Each of the stakeholders is directly or indirectly associated with
the health insurance industry and has the potential to affect the level of synergy among
insurers and providers (see Table 5.1 and Table 5.2). The level of competencies in the
areas of insurance and healthcare differ drastically.
At one end we have stakeholder like the insured customers where the level of competency
is low; stakeholders like government bodies, IT industry, education institution where the
competencies is high (in their respective area); and finally there are stakeholders like TPAs
where the competencies are high both at the insurance and the healthcare level. As could
be seen in the rational for engagements, each stakeholder affect or has the potential to
affect the relationship between the insurers and the providers. Each one of them plays a
participatory role in either developing or destroying synergy among insurers and providers.
As had been argued earlier it is important to undertake the stakeholder‘s analysis to
understand their areas of interest, relationship, attitude and their power to influence
synergy between insurers and providers. Any strategic framework developed for synergy
between insures and providers cannot be successful if it is not acceptable by the different
stakeholders. The stakeholder analysis that includes studying their interest, attitude,
relationship and power to influence would help identify factors affecting synergy among
insurers and providers.
During our investigations and interactions with different stakeholders group different
factors were identified that could either help develop or destroy synergy among insurers

129
and providers. For better understanding, the findings of the key stakeholder groups are
clubbed under five different categories i.e. insured, government and regulatory bodies,
health care professionals (doctor and nursing staff), intermediaries (agents, brokers, TPAs)
and other (NGOs, education institutions, pharmaceutical Co., etc.). This is then followed
by summarizing the key factors identified during the stakeholder analysis.
5.1 Insured
The insured customers are one of the most important stakeholders when it comes to
identify the strategy for synergy between insurers and providers. They are the major
connecting link between the insurers and the providers. In the absence of the insured
customer, the study of relationship between insurers and provided would be of no value.
The relationship of other stakeholders with the insured customer could be seen in Figure
5.2. There are many direct linkages and a few in-direct ones. There are also cross linkages
that have the potential to affect the relationship among insurers and providers.
Figure 5.2: Stakeholder’s Interaction Network
Source: Author‟s own creation

130
In the Indian context, the insured customer can be classified into three different categories.
The first category is that of the retail customers, a customer who either purchases the
insurance policy for either self or for family. The product offering are not as
comprehensive as in the other categories like group policies, but there are options
available. This section of insured population is currently low because of multiple reasons.
Some of the reasons includes: less importance given to health insurance over areas like
education, home, vehicle, children‘s marriage and alike; problems with claim processing;
limited product coverage; limited options for doctors and hospitals; agent and payment
related issues; expensive; complicated policy document and limited awareness. However,
this segment is being seen as a big opportunity by most of the upcoming health insurance
companies and there are efforts being made to lure the retail customers.
The second category is of corporate clients where the insured are the employees of
corporation or a business entity. In few cases in addition to the employees their dependents
are also covered. Here, the dependents may be defined as the immediate family (self,
spouse and children) or can include extended family (self, spouse, children and parents).
Since, this segment has been traditionally buying the health insurance cover in bulk; the
products offerings are more comprehensive. Here, additional benefits like the maternity
and outpatient are covered which are lacking in the retail segment. Because of its size this
segment is often further broken into special categories like small and medium enterprises
(SME), gold, silver and platinum clients. This categorization may not necessary be based
on the health insurance premium but could be on the overall health insurance premium
generated by the corporate clients. The corporate clients are more exposed to the concept
of health insurance and have a dedicated department responsible for managing the health
insurance piece.
The third category is of government sponsored scheme commonly termed as ―Mass‖
business. At times this category also falls under the definition of micro-insurance schemes.
The insured under this category are associated or member of a special group. This group
will have individuals of same occupation like weavers and artisan or of same socio-
economic strata like the below poverty lines.

131
Table 5.3: Stakeholder Analysis- Customer Awareness
Awareness
Potential
Customer
Insured Customer
without any Claim
Experience
Insured
Customer with
Claim
Experience
i. About Insurance Poor Poor Average
ii. Policy T&C Poor Poor Poor
iii. Cashless hospitalization Poor Poor Average
iv. TPA Poor Average Good
v. Insurance Company Poor Average Average
vi Network hospitals Poor Poor Average
Source: Summarized on the basis of Focus Group Discussions (FGD‟s) of different
categories of Insured Customers.
One of the examples of this category is the RSBY policy where the below poverty line
individuals and their family get cover for health insurance. It is only recently that the
IRDA has asked all the general insurance companies and the standalone health insurance
companies to submit the break-up health insurance data (for the year 2009-2010) for
individuals, corporate group and government sponsored schemes. For current filed study
the focused was on three types of insurance customer i.e. one who is a potential customer,
insured customer (with claim experience) and insured customer (without any claim
experience). Interestingly there were few factors which were common across all the
categories of customer like lack of awareness.
It was found that the level of awareness about insurance, policy terms and conditions,
cashless hospitalization process and details about network hospitals was poor for both
potential customer as well as customers without any claim experience. For those customers
who had experienced submitting a claim with either a TPA or an insurance company were
found to have fair idea about the TPA‘s and the cashless hospitalization process.
132
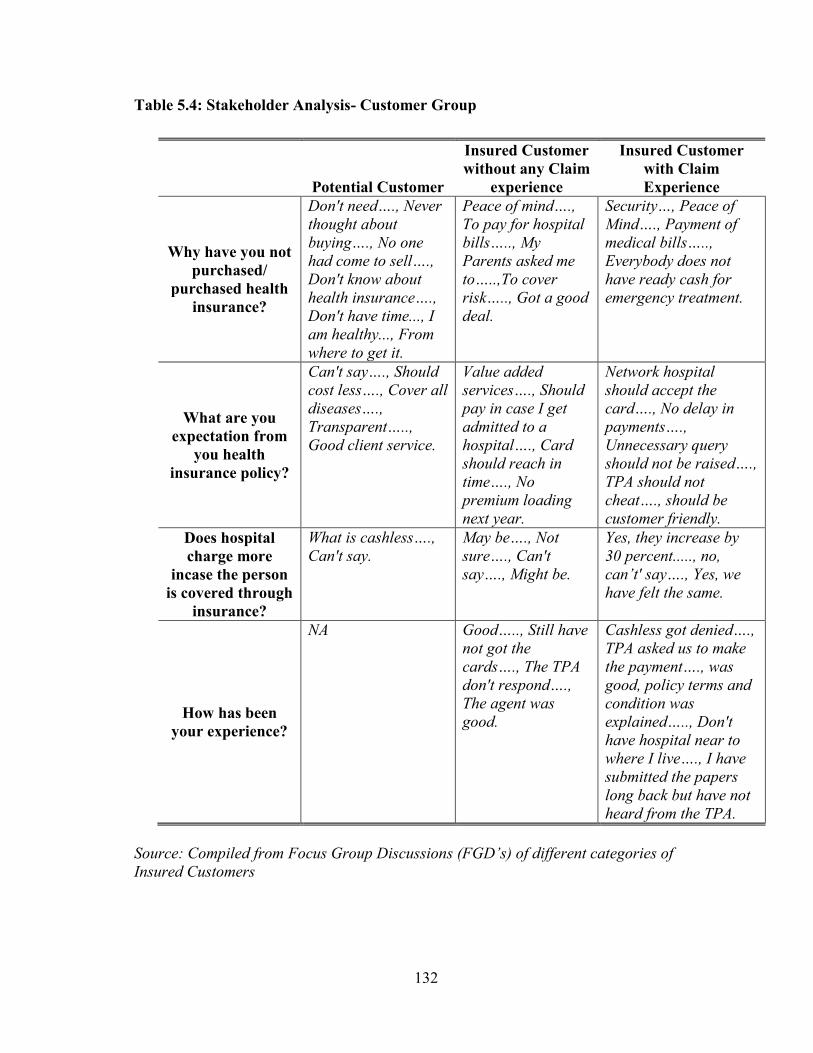
Table 5.4: Stakeholder Analysis- Customer Group
Potential Customer
Insured Customer
without any Claim
experience
Insured Customer
with Claim
Experience
Why have you not
purchased/
purchased health
insurance?
Don't need…., Never
thought about
buying…., No one
had come to sell….,
Don't know about
health insurance….,
Don't have time..., I
am healthy..., From
where to get it.
Peace of mind….,
To pay for hospital
bills….., My
Parents asked me
to…..,To cover
risk….., Got a good
deal.
Security…, Peace of
Mind…., Payment of
medical bills…..,
Everybody does not
have ready cash for
emergency treatment.
What are you
expectation from
you health
insurance policy?
Can't say…., Should
cost less…., Cover all
diseases….,
Transparent…..,
Good client service.
Value added
services…., Should
pay in case I get
admitted to a
hospital…., Card
should reach in
time…., No
premium loading
next year.
Network hospital
should accept the
card…., No delay in
payments….,
Unnecessary query
should not be raised….,
TPA should not
cheat…., should be
customer friendly.
Does hospital
charge more
incase the person
is covered through
insurance?
What is cashless….,
Can't say.
May be…., Not
sure…., Can't
say…., Might be.
Yes, they increase by
30 percent....., no,
can‟t' say…., Yes, we
have felt the same.
How has been
your experience?
NA Good….., Still have
not got the
cards…., The TPA
don't respond….,
The agent was
good.
Cashless got denied….,
TPA asked us to make
the payment…., was
good, policy terms and
condition was
explained….., Don't
have hospital near to
where I live…., I have
submitted the papers
long back but have not
heard from the TPA.
Source: Compiled from Focus Group Discussions (FGD‟s) of different categories of
Insured Customers

133
However, their awareness about the policy terms and conditions were found to be poor.
For summary of the findings about the level of awareness refer to Table 5.3.
During interview different set of questions were asked and the responses were noted. There
were similarities found in the need for purchasing of health insurance by different
categories of customers. The expectations of the insured customers with past claim
experience were higher than that of a potential customer. Also, this group suggested that
the providers charges higher in-case of cashless hospitalization. The overall experience
was different for customer without any claim history with that of customers who had
lodged either a claim with the insurers or had availed the cashless services. The sample of
the interactions is presented in Table 5.4.
5.2 Government and regulatory bodies
Some critics argue that the government intervention in the market place has real social
benefits that would not have occurred without government action. For example- the health
insurance policies for the below poverty line (RSBY scheme), where the BPL family gets
covered for a sum insured of 30,000 rupees by just paying a fee of 30 rupees.
Here, the total premium paid to the insurance company per BPL family is somewhere
around 800 rupees, where the balance 760 rupees is paid by the Central and State
government (Central share is 75 percent, whereas State share is 25 percent). Had the
government not initiated this policy, the BPL families would not have got the health
insurance cover. However, just paying the major chunk of the premium does not ensure
real improvements in health of the BPL family. This could be an important area of further
research, to see if schemes like RSBY are able to improve the health status of the families
who get benefit out of such health insurance schemes.
The insurance regulator has taken multiple initiatives for the orderly growth of health
insurance industry. For example, it has form a joint working committee to look in to the
area of health insurance. It has licensed few stand alone health insurance companies and is
looking into the recommendation of reducing the working capital requirement for

134
standalone health insurance companies. The insurance regulator has done quite a fair job in
handling customer grievances. Recently, it has opened a call center, where the customer
can lodge their complaints.
Based on the current investigations, it was found that the major areas of interest for the
government are in the area of awareness, trust and transparency and to improve the health
infrastructure in the Country. The key themes and factors that emerged are discussed
below:
5.2.1 Lack of Access
One of the concerns raised was the lack of access for the insured customer when it comes
to accessing cashless benefit at hospitals. It was told that currently only the private
hospitals are included in the list of insurers and most of these providers have profit
motives. Also, in spread of these providers are primarily in the urban areas. There is a lack
of access for insured those who live in rural and semi-urban areas. If health insurance fails
to provide access to hospital care for treatment of illness covered under health insurance
then one of its key utility will be lost. The reasons which could lead to lack of access are:
unavailability of hospitals in a given geography, no network tie-up by the insurance
company in a given geography, unavailability of hospital beds in the given hospital, denial
of admission or non-acceptance of health insurance card by the provider, etc.
To make health insurance successful, it was felt that there is a need for both insurers and
providers to come together and to provide access to care and cashless benefit to all sections
of society.
5.2.2 Need to improve trust and transparency
It was suggested that there is a pressing need to develop trust and transparency within the
health insurance system. There were also comments which highlighted that at times the
parties are not fair in their approach. This observation gets validated by one such instance
where few public sector insurers stopped cashless facility in metro cities due to losses in
their health insurance portfolio without consulting the providers. It was told that both the
insurers and providers question the honesty of each other. The insurers think that the

135
providers are not honest in their dealings and charges more money from insured patients
and on the other side the providers think that insurers are here to make profit and do not
care either about them or about the poor customers. It is important that both of them work
together to develop trust and transparency. This will help in the growth of Indian health
insurance industry.
5.2.3 Improve existing health infrastructure
As per the government and regulatory bodies the level of medical infrastructure is very
poor in our country and in most of the rural areas the private facility is almost negligible. It
was thought that if insurers and providers could come together then it would help build
health infrastructure in the rural areas. The example of RSBY was given to justify the
same. It was evident that the government has the powers to influence the current
relationship between insurer and providers not merely by introducing new schemes for the
general population who can‘t afford to pay the health insurance premium but also by
bringing changes in the current regulatory regime. The insurers and providers must make
efforts to affect the public policy in a way that helps develop synergy between them.
5.3 Healthcare professionals (Doctors, Hospital Administrators and Nursing Staff)
Health professionals are one of the key stakeholders in the relationship between insurers
and providers. It is this group that delivers the actual service to the insured customer and
determines the cost of care. Without this group neither the hospitals nor the insurers
(providing health insurance benefit) can survive. The interactions with this group were the
most interesting and insightful one. This may be because they are at the center of all the
activities linked to health insurance claims. It is on the advice of the treating doctors that
the cashless benefit is triggered. It is the treating doctor who decides the line of treatment
for the insured patient and not the insurer. It is the nursing staff that provides care to the
insured patient and not the sales staff of an insurance company. Thus, it may be argued that
the power of this group to influence customer satisfaction is the highest.

136
The key themes and factors that were brought into light includes: Lack of ownership by the
insurers and TPAs; Delays in provider payments; Lack of referral system; Poor doctor and
insurer relationship; Criteria‘s for selection of providers; Lack of standardization; Training
issues, and the need to have a robust grievance handling mechanism for addressing
provider issues. All these factors are briefly discussed as under:
5.3.1 Lack of ownership
During our interaction with the healthcare professionals it was informed that both the
insurers and the TAP‘s do not own the patient at the time of need. There are situations
where the patient is asked to speak to different parties to get the cashless claim processed.
During our interview with doctors, one critical comment which came was that there is no
effort by the insurance regulator to visit and meet network providers and seek their
feedback for insurance companies and TPA‘s i.e. to understand the problems faced by the
providers and then take corrective actions. Some suggested that there is no ownership by
the TPA‘s ( the issue linked to lack of ownership is discussed separately), few of them
pointed out that they are not able to control cost, are just profit making agency without
focusing on service, have poor quality of manpower and are involved in fraudulent
practices and sharing data with competitors.
5.3.2 Delay in provider payments
The study findings suggest that the providers do not receive payment in time and that it is
perceived as a critical factor by the providers while evaluating the services of the TPAs
and insurance companies. It was observed that delays in payment to providers are at times
being used as a rationalization for charging more money from the insured patients. During
our discussion with this group it was found that if the payments to providers are made well
within the agreed timeframe then it would help built confidence in the minds of the
providers for the services promised by the insurers. This will also affect the level of
services offered to the insured patients. For example, when asked why the providers take
advance deposit from insured patients it was told that this is because there had been past
cases wherein the payments were delayed either by the insurers or the TPAs.

137
5.3.3 Lack of referral system
During our interaction with doctors and the hospital administrators it was told that in the
Indian context we don‘t follow any referral system in the private space. This has a direct
impact on the hospital occupancy rate and cost of treatment. It was informed that even for
a normal cold and fever the insured visits a super specialty hospital and get consultation
from a super specialist. It was felt that even though the percentage of business from health
insurance was low, there is an opportunity to have close network polices to control the
flow of patients to providers and also the concept of gatekeeper was thought to be a
workable solution. However, since it‘s not easy to change the behavior of customers at
least some steps may be taken to ensure that there is balance between the demand and
supply of healthcare.
5.3.4 Poor doctor-insurer relationship
It was felt that the doctor and patient relationship is quite strong in the Indian context.
However, there is hardly any relationship between the doctors and insurers. It is either the
hospitals or the TPAs those who interact at regular intervals and have some sort of on-
going relationship. The interaction between the insurers and doctors is hardly seen. It was
told that hardly anyone from the insurance companies talk with the doctors. It is either the
TPA desk or the accounts team of the hospital that interacts with the insurance companies.
Currently, there are many doctors who work on freelance basis and are not exclusively
tied-up with any specific providers. These doctors have no incentive to reduce the cost of
care for insure patients. If insurance company can initiate building relationship then it
might help manage the health insurance claims cost. For example- there are many hospitals
wherein the consultant charges are not fixed. It is up to the consultant to decide how much
will he charge and from whom. If insurance company can tie-up with these consultant and
work towards a fixed consultant charge (in lieu of patient flow) then this would help
minimize the claim cost. It was felt that building doctor and insurer relationship will help
in bringing more transparency in the system and will benefit both the providers and the
insurers.

138
5.3.5 Criteria for selection of providers
There was a common perception that the selection of providers is not done fairly. That, it is
the discretion of the TPAs or the insurance company and that there is no standard process
followed for undertaking this activity. It was also suggested that there are few TPA‘s
which charge kick-back from the providers for getting into their panel. There was a
pressing need to have a standard process that should be followed for selection of providers
and it should be transparent in nature, to an extent that the providers know the reasons for
not getting selected for extending cashless benefit.
5.3.6 Lack of standardization
It was felt that there is lack of standardization in both the treatment part well as the
processes followed by the insurer and TPA‘s. For example- it was told that there is no
standard treatment guideline followed by most of the providers. By implementing standard
treatment guidelines there could be more transparency in the existing system. However, it
was argued by the doctor‘s community that there are cases which are complex and involve multiple
line of treatment and one cannot have standard guidelines for the same (for example, multiple
organ failure). It is also being thought that it will restrict the freedom of the doctors in deciding the
line of treatment.
An example of lack of standardization in the processes was that most of the TPA‘s have
their own Service Level Agreement (SLA) and thus it becomes extremely difficult for
providers to measure and monitor the same. It was argued by the hospital administrators
that the benefits of standardization of SLA and inclusion of common industry benchmarks
will help bring in focus and clear expectation from the service provider, whether it is the
TPA‘s , the providers or the insurers.
5.3.7 Training issues
It was a common feedback from the healthcare professionals that there is a lack of training
given to them either by the TPA‘s or the insurance companies. On critical examination it
was found that lack of training in the area of health insurance is because of multiple
reasons, which includes: lack of funds; lack of trained manpower (trainers) and
infrastructure; focus on just selling and not focusing on quality of sale; health insurance

139
being a loss making portfolio, thus any expenses in training was never thought as an
investment; Incase of providers there is high level of attrition at the insurance desk and
also due to lack of time, given the work pressure. It was suggested that by providing
training to healthcare professional on health insurance and its processes more synergy
could be developed among insurers and providers.
5.3.8 Lack of robust grievance handling mechanism for providers
A common feedback received was that the current grievance handling mechanism of the
insurers to handle provider query and complaints are not robust. There are many instances
when the issues highlighted by the providers and or doctors are not addressed by the
providers. Also, there are delay in responses received from insurers and TPAs. There are
payment issues which had not been resolved since years. A robust grievance handling
mechanism will help build confidence in the minds of the providers and would help
develop synergy.
5.4 Intermediaries (Agents, Advisors, Brokers, TPA’s)
The intermediaries are an important stakeholder group as they not only help in sales and
distribution activity but also in the servicing of health insurance policies. The key themes
and factors highlighted by the intermediaries were in the area of provider tariff,
communication, underwriting, product innovation and health insurance fraud. The
summary of the same is presented below:
5.4.1 Dual provider tariff
There was a common complaint that most of the providers follow a dual tariff i.e. one for
patients who pays out-of-pocket and the other for insured patients. It was told that such
practices hamper the relationship among insurers and providers. It was also informed that
such practices had started with the introduction of cashless services by the insurance
companies. It is because of such instances that the TPA‘s and insurance companies are
coming up with their own package rates. Even, in the mass scheme like RSBY standard

140
package rates are followed. It was felt that such practices destroy synergy among insurers
and providers.
5.4.2 Improve communication between parties
It was commonly felt that there are opportunities to improve communication between all
parties involved in the health insurance mechanism and working on the same would help
develop synergy among insurers and providers.
5.4.3 Lack of prudent underwriting
During our interview with the intermediaries it was told that it becomes extremely difficult
for them to understand few conditions in the policy which is incorporated at the time of
underwriting. For example- if the policy document simply says that there is a room rent
capping of say 10 percent. Then, it is not clear if the hospital should ask the insured patient
to pay 10 percent of the room rent charge or all the charges which is associated with room
rent. So, at the time of underwriting adequate care should be taken while writing any
special conditions so that it is clearly understood by the providers. It was also highlighted
that the pricing of the health insurance products does not take into account medical
inflation. Prudent underwriting guidelines are hardly followed by the insurance companies
due to market pressure and lack of available data on morbidity and past claim history.
5.4.4 Inadequate cover and product innovation
The common feedback was that there is inadequate cover and product innovation in the
area of health insurance. The problem with limited cover is that it restrict the provider to
offer services and make it troublesome for the insured (as well as the provider) to
understand the If‘s and But‘s of the policy. It was also told that there is a perception among
the insured population that insurance companies want to cover only young and healthy
people so that they can make heavy profits. This gets fuelled by the fact that most of the
insurance companies don‘t extend cover if you are more than 80 yrs old. The need for
product innovation was highlighted and it impact on synergy among insurers and providers
was reflected.

141
5.4.5 Health insurance fraud
The presence of fraud in the health insurance business was acknowledged. It was informed
that there are different types of fraud prevalent in the Indian health insurance market. For
example- lodging of fraudulent reimbursement claims; mis-representation of material fact
at the time of policy issuance; manipulation of claim documents including bills and
receipts; kick-back from providers and intermediaries. There concept like ‗rent a patient‘,
‗unbundling‘, ‗up-coding‘ are becoming visible in the area of provider fraud. Few of them
told that the insured patients are made to stay more than that of patients who pay out-of-
pocket. Insured patient are prescribed high end diagnostic test like Computed Tomography
(CT scan) and Magnetic Resonance Imaging (MRI), even when the same is not linked to
the treatment. There are cases where fixed commission is being paid to the prescribing
doctors by the diagnostic centers. In case of providers, it was told that since they invest lot
of money buying the latest technology, they tend to use the technology on patients for
regular income flow and decreasing the idle time of the equipment. There was a common
feeling that the saving brought about by mitigating health insurance fraud risk will not only
benefit the insurers but all the other stakeholders in the industry.
5.5 Others (NGOs, Education institutions, Pharmaceutical Co. etc.)
The key themes those were raised by the remaining stakeholders (i.e. NGO‘s, educational
institution, etc.) were in the area of value creation, training, co-payment and deductible and
linked to insurance cover (over and under insurance). A brief summary of these are
presented below:
5.5.1 Lack of value creation: There was a common feedback that there is lack of value
creation in multiple areas. These include activities like the health insurance product
development, cashless processing and customer service (both at insurer and provider). It
was felt that the level of customer satisfaction may be increased by creating value for the
customer. For example, by reducing the premium of health insurance products and offering
care with quality of international standards.

142
5.5.2 Lack of specialized training institutions and courses: One of the issues raised was
lack of specialized training institution and courses designed to address the training needs of
the Indian health insurance market. It was told that as the health portfolio was bleeding
with high claim ratio, it was never thought a good idea to spend money in training. The
NGO‘s and the educations institutions were more vocal on this issue. A pressing need to
develop course curriculum based on the needs of the health insurance industry was felt. It
is though these specialized training institutions and courses that the industry would be able
to produce trained manpower required to sustain the current growth level of health
insurance in India.
5.5.3 Co-payment and high deductibles: The NGO‘s were of the opinion that insurance
companies had started putting co-payment and deductible clauses in their products to
safeguard themselves from financial loss but such activities are completely against the
customers. It becomes very difficult for a poor patient to pay out-of-pocket when he is
covered through insurance. It was also told that such activities are not welcomed by them
and should be stopped.
5.5.4 Over and under insurance: Here again the NGO‘s were of the opinion that over and
under insurance is not customer friendly. What is the value for the customer if he is under
insured? If the sum insured is less than the treatment cost then what is the fun in buying a
health insurance cover? Over insurance is where the customer is offered higher sum-
insured but is not that prevalent in the Indian scenario due to in-capacity to pay for the cost
of higher premium. Also, it becomes difficult for the providers to process claims where the
total treatment cost is not paid by the insurers.
Thus, there are multiple factors that can affect synergy between insurers and providers.
Each stakeholder group had an interest in the relationship between insurer and provider
and can affect the implementation of potential strategies for synergy. However, if the
identified factors and issue are kept in mind while developing strategies for synergy, then
the chances of failure for implementation would be minimized.

143
5.6 Content Analysis and Competitive Diamond
5.6.1 Content Analysis
On analyzing the contents published in one of the leading national news paper of India
(Times of India) from 2007 to 2009, it was found that a total of 223 headlines were
published in the area of health insurance. These headlines contain words like health,
insurance, insurer, insured, cashless and or mediclaim and were related to the health
insurance domain. The number of headlines published in year 2007 was the highest
followed by 2009 and the least number of headlines were published in the year 2008
(Figure 5.3).
Figure 5.3: Number of Headlines on Health Insurance (TOI: 2007, 2008 and 2009)
Source: Content analysis undertaken by the author
The location source of these articles covered sixteen States. The maximum number of
headlines published on health insurance was observed in the state of Maharashtra 34
percent, followed by Delhi 31 percent. Thus, 65 percent of the articles on health insurance
were found to get reported either from the State of Maharashtra or Delhi. This may be
because of the reason that most of the insurance corporate houses are located in these two
States. Also, the number of corporate houses extending cashless benefit to its employees
would be the highest in these two states. 21 percent of the headlines were reported from
Karnataka, Tamil Nadu and Punjab. This may be because; in these three States the social
health insurance schemes are active.

144
Figure 5.4: Number of Headlines: State wise percentage distribution
Source: Content analysis undertaken by the author
Table 5.5: State wise City representation
State Name City Representation (Headlines)
Andhra Pradesh Hyderabad
Bihar Patna, Bhagalpur
Delhi New Delhi
Goa Panaji
Gujarat Ahmedabad,Vadodara, Amreli, Surat
Haryana Panipat
Himachal Pradesh Shimla
Karnataka Bangalore, Mangalore, Davanagere, Hubli
Kerala Thiruvananthapuram, Kochi
Kolkata Howrah
Madhya Pradesh Jabalpur
Maharashtra Mumbai, Pune, Nagpur
Punjab Chandigarh, Ludhiana
Rajasthan Jaipur
Tamil Nadu Chennai, Coimbatore
Uttar Pradesh Allahabad, Lucknow, Kanpur, Varanasi
Source: Content analysis undertaken by the author

145
Table 5.6: Content analysis: stakeholder wise issues and interest
Stakeholders Issues/ Interest
Community at large
Life insurance, Unique Cover, Insurance scam, Standalone
health insurance, Affordability (high premium), Access,
Differential rate, Lack of cover, New products, Growth
potential, Role of doctors, Career prospects, Tax benefits,
Commission paid to agents.
Government (Center
and State)
FDI, Insurance for Poor, Need for cover, Tax savings,
Coverage, Policy exclusions, Lack of Access and Awareness,
RSBY, Aam Adami Bima Yojana, Cashless Facility,
Divestment in PSU, Delay in processing claim and provider
payment, Forcible sale of insurance policy.
IRDA
Training of Agents, Agent Commission, Definition of Pre-
Existing disease, Cover for Sr. Citizen, De-tariff, Policy holder
Interest, Misselling, Agents recruitment exams, Premium
loading, Demand for skill set, Merger and Acquisition, Rising
number of disputes, Norms for insurance IPO, Bancassurance.
GIC Low penetration, Portability in mediclaim, Standardization,
Common definition of Pre-Existing disease
Insured Differential Premium, Poor claim processing, blacklisted
hospitals, Insurance related fraud
Insurer
TPA services, Claims & Cost, Need for Cover, Product
development, PED, lack of training and standardization, Fraud,
Huge opportunity
Insurance industry High Loss, Joint ventures, Brokerage and commission,
Uniform hospital rates
Industry (general) Competition, Investments, joint ventures
International
Community Outsourcing, Need for Care
Courts (High and
Supreme) Coverage, Health insurance Fraud
Consumer forum Deficiency in service, Policy T&C, PED, Negligence
Teaching and Training
Institution
Shortage of hospital, Lack of coordination between hospital
and insurer, Career prospects in insurance, Cover for students
Source: Content analysis undertaken by the author

146
The balance 14 percent of the headlines were reported from States like Gujarat, Uttar
Pradesh, Bihar, Kerala, Goa, Kolkata, Andhra Pradesh, Haryana, Himachal Pradesh,
Madhya Pradesh and Rajsathan (Figure 5.4). The Cities representation is given in Table
5.5. The stakeholder wise issues and interest are summarized in Table 5.6.
5.6.2 Competitive Diamond
Michael Porter introduced a model that allows analyzing why some nations are more
competitive than others are, and why some industries within nations are more competitive
than others are, in his book ―The Competitive Advantage of Nations‖. Porter‘s diamond of
national competitive advantage is a modern international trade theory (Porter, 1990). It was
derived and used to conceptualize the four conditions that are important when conducting
international business. These four factors originate from earlier country and firm-based
theories.
Figure 5.5: Competitive Diamond of Indian Health Insurance Industry
Source: Adopted from porter Competitive Diamond for Nations.
147
In simple terms, the country based theories relate to the international trade theories of
nations as a unit of business and the firm-based theories are those which relate to the firm
as a unit of business. It recognizes four pillars of research (factor conditions, demand
conditions, related and supporting industries, firm structure, strategy and rivalry) that one
must undertake in analyzing the viability of a nation competing in a particular international
market, but it also can be used as a comparative analysis tool in recognizing which country
a particular firm is suited to expanding into. The Indian health insurance industry currently
has provisions for 26 percent of FDI as per regulations. There is discussion going on to
increase this limit to 49 percent. Most of the private players have foreign partners. For
example - Max Bupa, Apollo Munich, ICICI Lombard etc., also, there are health insurance
products that compete in the international market like the international medical emergency
and travel policy (with health cover). Any foreign partner of the existing insurance
companies and those willing to enter this market would examine the above mentioned four
factors before taking the decision.
The current study attempts to examine the competitive diamond of Indian health insurance
industry. The findings and discussion are based on the desk and field research undertaken.
The Figure 5.5 depicts the competitive diamond. Under each factor the positives (+) and
opportunities for improvement (-) are listed. If Indian health insurance industry wants to
attract more foreign investment and participation then the negatives needs to be converted
into positives. The four factors are discussed briefly here under:
Factor Condition: the factor conditions are divided into basic and advanced factors. Under
the basic factors the opportunities for improvement are in the area of poor sanitation and
hygiene, poor accessibility and access of healthcare, low doctor to patient ratio and low
bed to patient ratio. The strengths are in the area of nursing education and medical
education. In the advanced category the opportunities for improvement are in the area of
poor communication between parties (insurer, provider, TPA, customer etc.), delay in
payments and funds transfer to providers, lack of trained and skill manpower and lack of
scientific research. The strengths include the technology resource available within the
country.

148
Demand Condition: the overall demand for health insurance in India is low but in the times
to come due to rising cost of healthcare and increase in disposable income this scenario
will change. The opportunities for improvement under demand condition includes lack of
awareness about the benefits of health insurance products, poor distribution strategy, lack
of value creation for the customer, need to care, need for cover and poor penetration of
health insurance. The strengths include introduction of mass policies like RSBY (the
demand is created by the government) and the rising healthcare cost (in the current
context).
Related and Supporting Industries: the opportunities for improvement include: poor re-
insurance support, medical equipments manufacturing, medical tourism, lack of ownership
by intermediaries, high level of fraud (both provider and customer related) and lack of
initiatives in the area of preventive healthcare. The strengths include support from the
banks and MFIs in serving this market segment.
Firm Strategy, Structure, and Rivalry: the opportunities for improvements include:
increasing the FDI limit from current 26 percent to 49 percent, over regulated insurance
industry, lack of specialized insurance body for health insurance, lack of standardization
and lack of trust and transparency among stakeholders. The strengths include the entry of
standalone health insurance company, de-tariffication and product innovation.
Thus, to build home based advantages and to create competitive advantage in relation to
others on a global front, the Indian health insurance industry needs to act on the
opportunities for improvements (identified above) and keep developing the strengths. On
national level, governments can (and should) consider the policies that they should follow
to establish national advantages, which enable the health insurance industry to develop a
strong competitive position globally. According to Porter, governments can foster such
advantages by ensuring high expectations of product performance, safety or environmental
standards, or encouraging vertical co-operation between suppliers and buyers on a
domestic level etc.