deepmolecularresponseinchronicmyeloidleukemia:the new goal...
TRANSCRIPT

Review
DeepMolecular Response in ChronicMyeloid Leukemia: TheNew Goal of Therapy?
Francois-Xavier Mahon1 and Gabriel Etienne2
AbstractChronic myeloid leukemia (CML) is caused by formation of the BCR–ABL1 fusion protein. Tyrosine
kinase inhibitors (TKI) that target BCR–ABL1 are now the standard of care for patients with CML.
Molecular monitoring of residual BCR–ABL1 mRNA transcripts, typically performed using real-time
quantitative PCR, has improved treatment management, particularly for patients with CML in chronic
phase. Major molecular response (MMR; i.e., a �3-log reduction in BCR–ABL1 transcript levels) is used
in current treatment guidelines to assess prognosis. Recent evidence suggests that deeper molecular
responses (�4-log reductions in BCR–ABL1 transcript levels), particularly when attained early during
treatment, may have even better correlation with long-term outcomes, including survival and disease
progression. Furthermore, achieving deep molecular response is a requirement for entering trials
evaluating treatment-free remission (TFR). In this review, we discuss the evolving definition of minimal
residual disease and the various levels of molecular response under evaluation in current clinical studies.
In addition, the available clinical data on achieving MMR and deeper levels of molecular response with
TKI therapy, the prognostic value of deep molecular response, and factors that may predict a patient’s
ability to achieve and sustain a deep molecular response on TKI therapy are also discussed. Available
data from TFR studies are addressed. We discuss current knowledge of the ideal conditions for
attempting treatment discontinuation, factors predictive of molecular relapse, when TKI therapy should
be restarted, and which therapeutic strategies (when administered in the first-line setting and beyond)
are expected to best enable successful TFR. Clin Cancer Res; 20(2); 310–22. �2013 AACR.
IntroductionDysregulated protein tyrosine kinase (PTK) activity is
the hallmark of multiple neoplasms (1). Over the pastdecade, a broad array of drugs designed to selectively inhibitPTKs [i.e., tyrosine kinase inhibitors, (TKI)] have emerged asnovel therapies for patientswith cancer (2). Perhaps themostwell-knownPTK target todate is theBCR–ABL1oncoprotein,which is critical to the pathogenesis of chronic myeloidleukemia (CML; ref. 3). The successful treatment of patientswith CML with the BCR–ABL1 TKI imatinib has definitivelyvalidated this therapeutic strategy and established CML asa model disease for targeted cancer treatment (4).
With over a decade of imatinib use as first-line therapy inpatients withCML, surrogatemarkers that strongly correlatewith prognosis have been identified (5). The validation ofsurrogate endpoints for treatment effectiveness, such ascomplete hematologic response (CHR) and complete cyto-genetic response (CCyR), has improved treatment manage-ment (6, 7). Most patients, particularly those with CML inchronic phase (CML-CP), will achieve these endpoints on aBCR–ABL1 TKI (8–10). The progress of molecular biologyhas presented the opportunity to look beyond CHR andCCyR and monitor residual disease on a molecular level(11, 12). Current clinical practice recommendations forCML advocate monitoring patients for hematologicresponse (i.e., blood counts returning to normal values),cytogenetic response (i.e., disappearance of the Philadel-phia chromosome), andmolecular response (i.e., reductionin BCR–ABL1 gene expression; refs. 6 and 7). Molecularmonitoring is typically performed using real-time quanti-tative PCR (RQ-PCR), a simple technique that can beperformed on peripheral blood samples and is both moresensitive and more convenient than conventional cytoge-netics (13). The first level of response evaluated on themolecular scale, a major molecular response (MMR), cor-responds to a 3-log reduction in BCR–ABL1 transcript levelsfrom a standardized baseline (�0.1% BCR–ABL1 on theInternational Scale [BCR–ABL1IS]; refs. 11 and 14). MMR
Authors' Affiliations: 1Laboratoire d'H�ematologie, Centre Hospitalier Uni-versitaire de Bordeaux and Laboratoire H�ematopoï�ese Leuc�emique etCible Th�erapeutique, Bioth�erapies des maladies g�en�etiques et cancers,Inserm U1035, Universit�e Bordeaux S�egalen; and 2Centre R�egional deLutte Contre le Cancer de Bordeaux et du Sud-Ouest, Institut Bergoni�e,D�epartement d'Oncologie M�edicale, Bordeaux, France
Corresponding Author: Francois-Xavier Mahon, Laboratoire d'H�emato-logie, CHU de Bordeaux and Laboratoire H�ematopoï�ese normale et patho-logique, Universit�e Victor S�egalen Bordeaux 2, 146 rue L�eo-Saignat, InsermU1035, 33076BordeauxCedex, France. Phone: 33-5-5757-1524; Fax: 33-5-5693-8883; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-13-1988
�2013 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 20(2) January 15, 2014310
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988

hasbeen found tobe associatedwith improvedprogression-free survival (PFS; refs. 15 and 16) and event-free survival(EFS; refs. 17–19), although its prognostic value is stilldebated.The European LeukemiaNet (ELN) defines response to
TKI therapy based onmolecular and cytogenetic milestonesachieved at 3, 6, and 12 months, or beyond (6). The ELNrecommends evaluating molecular response using buffycoat from peripheral blood every 3 months until MMR isachieved, and then every 3 to 6 months. Cytogeneticresponse should be assessed using bone marrow at 3, 6,and 12 months, and then every 12 months once CCyR isachieved. Some patients (e.g., patients with monosomy 7,del[7q] or clonal chromosomal abnormalities)may requireadditional long-term bone marrow follow-up.Until recently, deepmolecular responses beyond the level
of MMR have remained largely unexplored, given a lack ofstandardized assay techniques (20). Several recent studieshave demonstrated that some patients with such responsescan achieve treatment-free remission (TFR), thereby chal-lenging the dogma that CML cannot be cured withoutallogeneic bone marrow transplantation (21, 22). Theoverall goals of therapy in CML—disease remission,reduced risk of progression, and improved overall survival(OS)—are clear; however, many questions remain aboutthe impact of molecular response on achieving these goals.Recent data, to be discussed herein, suggest that in selectpopulations, obtaining a deep molecular response shouldbe considered a primary therapeutic goal.
The Challenge of Defining Deep MolecularResponse
The development of the International Scale for BCR–ABL1 RQ-PCR assessment has enabled quantification ofmolecular response in relation to a standardized baseline(14, 23). The definition of MMR as BCR–ABL1IS �0.1%originates from the International Randomized Study ofInterferon Versus STI571 (IRIS; ref. 15). However, standard-ization of deeper levels of molecular response has provenless straightforward and is urgently needed to facilitateimproved interpretation of clinical results. Deeper levelsof molecular response may also be defined according to theInternational Scale, wherein MR4 indicates �4.0-logreduction (BCR–ABL1IS�0.01%),MR4.5 indicates�4.5-logreduction (BCR–ABL1IS �0.0032%), and MR5 indicates�5.0-log reduction (BCR–ABL1IS� 0.001%; Fig. 1; ref. 11).However, the observation of undetectable BCR–ABL1 tran-scripts is inherently linked to the sensitivity of the PCRmethod, as well as the control gene, used. An ongoingEuropean Treatment and Outcome Study (EUTOS) collab-oration aims to facilitate standardization of deepmolecularresponse across laboratories by establishing recommenda-tions for response definitions and quality control (11).
Varying definitions of complete molecular response(CMR) have been reported. For example, the NationalComprehensive Cancer Network (7) defines CMR as "nodetectable BCR–ABL1 chimeric mRNA as assessed by RQ-PCR using the International Scale with a sensitivity of 4.5-
CCR Reviews
© 2013 American Association for Cancer Research
100
10 1
2
3
4
4.5
5
6
1
0.1
0.01
0.0032
0.001
0.0001
BCR–ABL1(%IS)
Logreduction inBCR–ABL1
Reduction in BCR–ABL1
1:10
Baseline
ApproximatesMCyR
ApproximatesCCyR
MMR
Level of response
Deepmolecularresponse
MR6 (with currently available technology,this level of response cannot be assessed)
MR4
MR4.5
MR5
1:100
1:1,000
1:10,000
1:32,000
1:100,000
1:1,000,000
Figure 1. Levels of molecularresponse in CML. MCyR, majorcytogenetic response; MR,molecular response.
Deep Molecular Response in Chronic Myeloid Leukemia
www.aacrjournals.org Clin Cancer Res; 20(2) January 15, 2014 311
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988

log reduction or more from the standardized baseline,"whereas the ELN (6) recommends using the term "molec-ularly undetectable leukemia" instead of "CMR" and notesthe importance of specifying control gene copy numberwhen reporting this level of response. Undetectable mini-mal residual disease indicates a negative RQ-PCR result andmust be associated with a defined PCR assay sensitivity;however, leukemic cellsmay still be present even if RQ-PCRresults are negative (24). Notably, current RQ-PCR meth-odology is largely optimized for detection of so-called"typical" BCR–ABL1 transcripts, or those involving themajor breakpoint cluster region, and may fail to detectatypical transcripts derived from other breakpoints (25);thus, assessment of transcript type at baseline is essential toensure accurate interpretation of RQ-PCR results.
Deep Molecular Response in Clinical Trials ofCML-CP
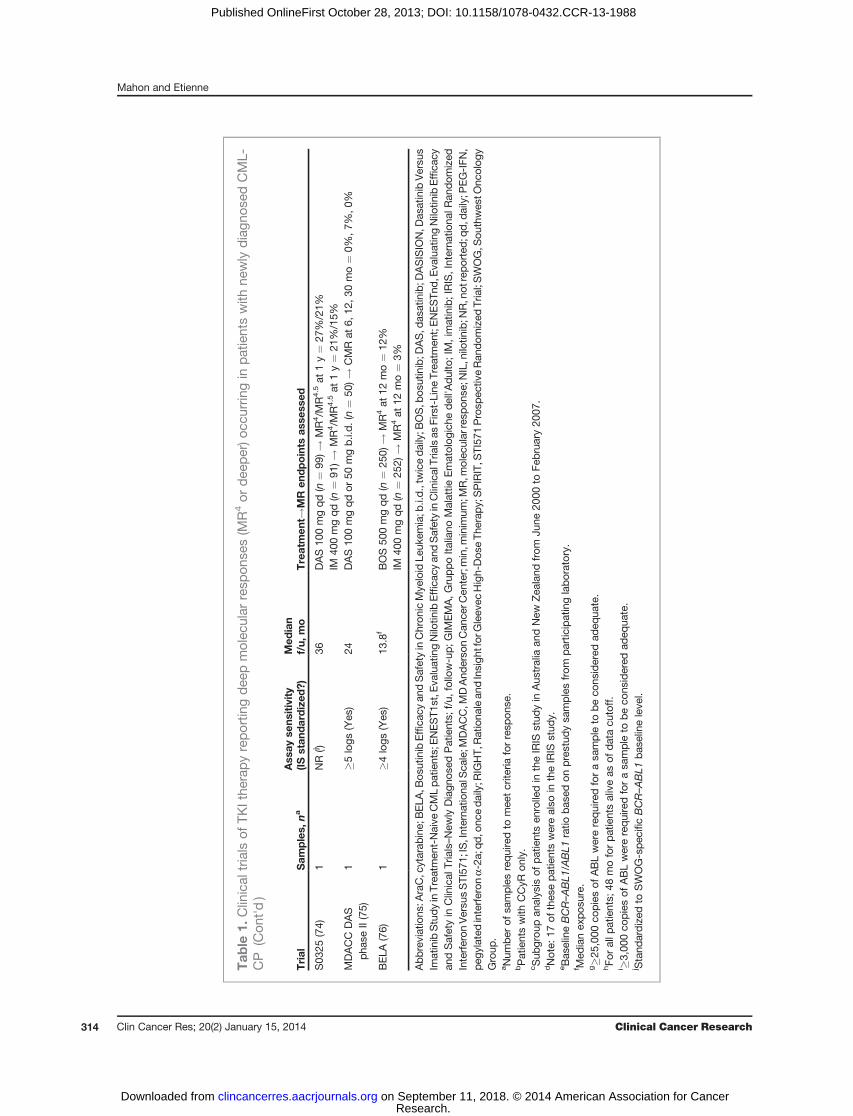
Deep molecular responses have been assessed in mul-tiple ongoing clinical trials of TKIs in patients with newlydiagnosed CML-CP (Table 1). Given the current lack ofstandardization of PCR sensitivity, rates of CMR reportedin these studies are not necessarily comparable. Discre-pancies in rates of deep molecular response may alsoresult from differences in assay techniques or studydesign. For example, PCR may be assessed using bloodor bone marrow, and response may be defined by a PCRresult at a single time point or confirmed by multiplesamples. Other variables include the study population(e.g., the proportion of high-risk patients), median fol-low-up at time of analysis, and type and dose of TKItherapy received. Although several studies have shownthat imatinib can elicit deep molecular responses in somepatients, second-generation TKIs, such as nilotinib anddasatinib, have demonstrated higher rates of deep molec-ular response attained within shorter time periods(Table 1). The combination of TKI therapy with interfer-on (IFN), which may help drive leukemic stem cells (LSC)into the cell cycle (26), thereby inducing deep molecularresponse, has also been explored. Rates of deep molecularresponse were higher with this combination versus ima-tinib alone in one study using pegylated IFN (26), butsimilar in another study using IFN-a (Table 1; ref. 27).
The Clinical Relevance of Deep MolecularResponse
Defining the value of achieving deep molecularresponse in patients with CML is an active area of ongoingresearch. There is conflicting evidence about whetherachieving an MMR provides additional benefit beyonda CCyR (20). The leukemic cell burden is similar inpatients with MMR and CCyR (only 1-log difference inBCR–ABL1 levels), and this difference may be too small toimpact long-term outcomes such as PFS and OS. Eventslike progression or death are quite infrequent with front-line TKI therapy; therefore, long-term follow-up and large
cohorts of patients would be required to definitivelydemonstrate any added benefit to achieving MMR.
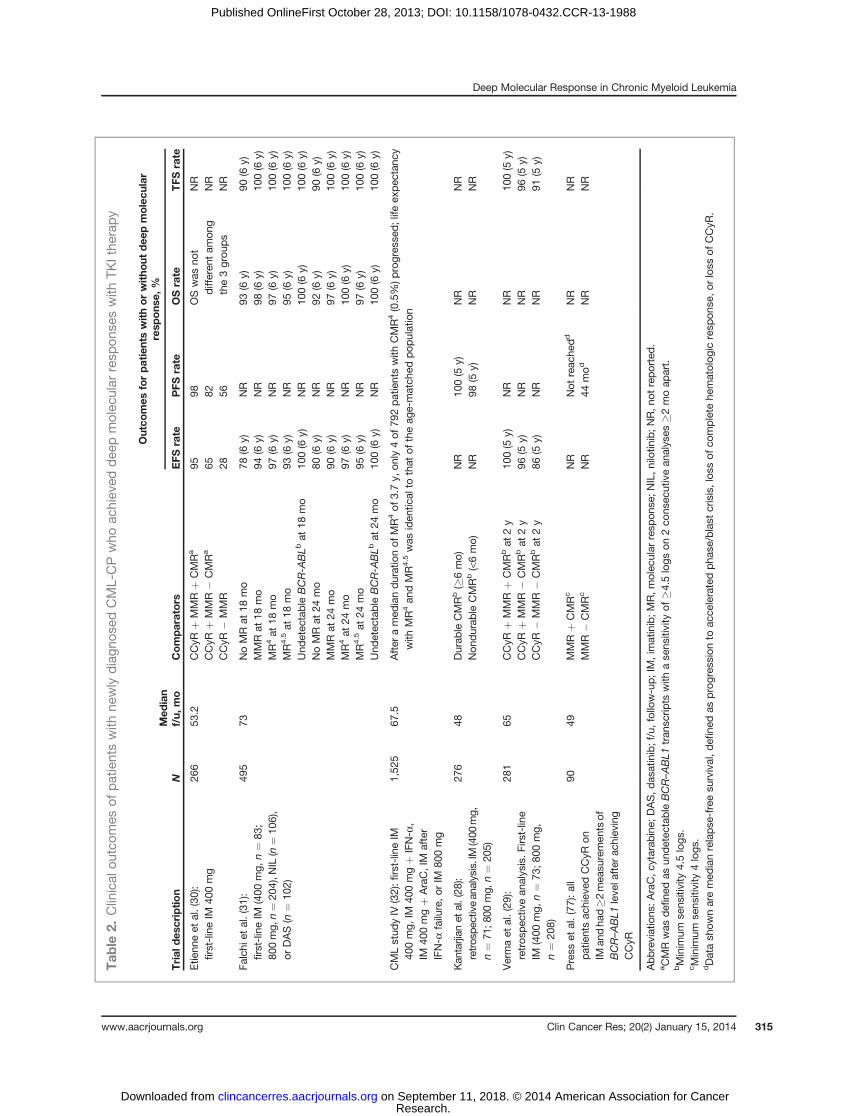
However, deeper molecular responses provide moreseparation from CCyR in terms of residual disease bur-den; therefore, it may be easier to distinguish the uniquebenefits of such responses. Patients who achieve deepmolecular response seem less likely to lose MMR, andseveral studies have shown that deep molecular responsescorrelate with better long-term clinical outcomes, such asEFS, PFS, and OS, and a low risk of progression anddisease relapse (Table 2; refs. 28 and 29). For example, astudy by Etienne and colleagues (30) found that EFS andPFS were longer in patients with CMR than those withCCyR, regardless of MMR status; OS was not significantlydifferent between these groups. Another study by Falchiand colleagues (31) showed that patients with undetect-able BCR-ABL1 levels by 18 or 24 months had 100% ratesof OS, EFS, and transformation-free survival (TFS) at 6years. In the German CML study IV, life expectancy inpatients with MR4 or MR4.5 was the same as that in an age-matched population, and only 4 of 792 patients (0.5%)who achieved MR4 had disease progression (32).
These results provide encouraging evidence that achieve-ment of deep molecular response is an important clinicalgoal and prompt the question: should patients with CCyR,who donot achieve these deep levels ofmolecular response,be switched to an alternate therapy? Theongoing EvaluatingNilotinib Efficacy and Safety in Clinical Trials–CMR(ENESTcmr) study aims to address this question by ran-domizing patients with detectable BCR–ABL1 transcriptsafter�2 years on imatinib to either continue on imatinib orswitch to nilotinib (33). After 12 and 24 months of follow-up, more patients achieved MR4.5 and undetectable BCR–ABL1 (�4.5-log RQ-PCR assay sensitivity) on nilotinibcompared with continued imatinib (33). Yet perhaps themost convincing reason to strive for sustained deep molec-ular response in patients with CML-CP is the possibility thatit may enable eventual achievement of TFR.
Deep Molecular Response and TFRReports of imatinib discontinuation in patients without
sustained deep molecular responses have shown high andrapid rates of disease relapse (34–37). In contrast, a smallpilot study of imatinib discontinuation with the stringententry criteria of sustained CMR for �2 years on imatinibshowed promising results, with 6 of 12 patients remainingin molecular remission after a median 18 months of fol-low-up (38). This proof of concept inspired numerousclinical studies of imatinib discontinuation in patients withstable, deep molecular responses on TKI therapy (Table 3).In all cases, many patients were able to remain relapse-freeoff therapy.
Importantly, molecular relapse, the trigger for reintro-duction of TKI therapy in these studies, was often defineddifferently. For example, in the Stop Imatinib (STIM) study,molecular relapse was defined as positive RQ-PCR resultson 2 consecutive assessments (39, 40), whereas in the STIM
Mahon and Etienne
Clin Cancer Res; 20(2) January 15, 2014 Clinical Cancer Research312
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988

Tab
le1.
Clinicaltrialsof
TKIthe
rapyreportin
gdee
pmolec
ular
resp
onse
s(M
R4or
dee
per)o
ccurrin
ginpatientswith
newlydiagn
osed
CML-CP
Trial
Sam
ples,
na
Ass
ayse
nsitivity
(ISstan
dardized
?)Med
ian
f/u,
mo
Treatmen
t!MR
endpoints
asse
ssed
IRIS
(15,
24)
1�4
.5logs
(estab
lishe
dtheIS)
25IM
400mgqd(n
¼33
3)!
CMRat
12mo¼
4%b
81IM
400mgqd(n
¼29
c)!
MR4/M
R4.5by81
mo¼
70%
/52%
.MR4.5at
81mo¼
45%
ID-01_
151(66)
1�5
logs
(No)
15IM
400mgb.i.d.(n¼
112)
!CMR¼
28%
deLa
vallade
etal.(67
)�2
cons
ecutive
NR(Yes
)38
IM40
0mgqd(n
¼20
4d)!
CMR¼
5%
RIG
HT(68)
1�4
.5logs
(Noe)
17f
IM40
0mgb.i.d.(n¼
115)
!CMRby6,
12,1
8mo¼
39%
,44%
,55%
Verma
etal.(29
)1
�4.5
logs
(NR)
65IM
400mgqd(n
¼73
)or80
0mgqd(n
¼20
8)!
CMR¼
44%
SPIRIT
(26)
1g(Yes
)47
hIM
400mgqd(n
¼15
9)!
MR4at
12,2
4mo¼
14%
,21%
.CMRat
24mo¼
9%IM
400mgqdþ
AraC
(n¼
158)
!MR4at
12,2
4mo¼
15%
,26%
.CMRat
24mo¼
8%IM
400mgqdþPEG-IFN
(n¼15
9)!
MR4at
12,2
4mo¼30
%,3
8%.C
MRat
24mo¼16
%IM
600mgqd(n
¼16
0)!
MR4at
12,2
4mo¼
17%
,26%
.CMRat
24mo¼
8%
CMLStudyIV
(27)
1NR(Yes
)43
IM40
0mgqd(n
¼32
4)!
MR4by
12,2
4,36
mo¼
8%,3
1%,4
6%48
IM40
0mgqdþ
IFN-a
(n¼
350)
!MR4by12
,24,
36mo¼
12%
,30%
,41%
28IM
800mgqd(n
¼33
8)!
MR4by
12,2
4,36
mo¼
20%
,43%
,57%
ENESTn
d(10)
1i (Y
es)
Min
36NIL
300mgb.i.d.(n¼
282)
!MR4by1,
3y¼
20%
,50%
.MR4.5by1,
3y¼
11%
,32%
NIL
400mgb.i.d.(n¼
281)
!MR4by1,
3y¼
15%
,44%
.MR4.5by1,
3y¼
7%,2
8%IM
400mgqd(n
¼28
3)!
MR4by
1,3y¼
6%,2
6%.M
R4.5by1,
3y¼
1%,1
5%
ENEST1
st(69)
1NR(Yes
)6.5f
NIL
300mgb.i.d.(n¼
205)
!MR4by3,
6mo¼
5%,2
0%
GIM
EMA(70,
71)
1;stab
le,
3�
4moap
art
�4logs
(Yes
)48
NIL
400mgb.i.d.(n¼
73)!
MR4at
12,2
4,36
mo¼
12%
,27%
,25%
51NIL
400mgb.i.d.(n¼
73)!
Stable
MR4¼
25%
MDACC
NIL
pha
seII(72)
1�5
logs
(Yes
)17
.3NIL
400mgb.i.d.(n¼
51)!
CMRby6,
12,3
0mo¼
4%,1
1%,1
5%
Nicolini
etal.(73
)1
NR(Yes
)13
.6NIL
300mgb.i.d.þ
PEG-IFN
(n¼
40)!
MR4at
6,12
,15mo¼
23%
,57%
,80%
.MR4.5at
6,12
,15mo¼
10%
,21%
,50%
.MR5at
6,12
,15mo¼
10%
,15%
,40%
DASISION
(9)
1NR(Yes
)Min
24DAS10
0mgqd
(n¼
259)
!MR4.5by2y¼
17%
IM40
0mgqd(n
¼26
0)!
MR4.5by2y¼
8%
(Con
tinue
don
thefollo
wingpag
e)
Deep Molecular Response in Chronic Myeloid Leukemia
www.aacrjournals.org Clin Cancer Res; 20(2) January 15, 2014 313
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988
Tab
le1.
Clinical
trials
ofTK
Ithe
rapyreportin
gdee
pmolec
ular
resp
onse
s(M
R4or
dee
per)o
ccurrin
gin
patientswith
newly
diagn
osed
CML-
CP
(Con
t'd)
Trial
Sam
ples,
na
Ass
ayse
nsitivity
(ISstan
dardized
?)Med
ian
f/u,
mo
Treatmen
t!MR
endpoints
asse
ssed
S03
25(74)
1NR(j )
36DAS10
0mgqd(n
¼99
)!MR4/M
R4.5at
1y¼
27%
/21%
IM40
0mgqd
(n¼
91)!
MR4/M
R4.5at
1y¼
21%
/15%
MDACC
DAS
pha
seII(75)
1�5
logs
(Yes
)24
DAS10
0mgqdor
50mgb.i.d
.(n¼
50)!
CMRat
6,12
,30mo¼
0%,7
%,0
%
BELA
(76)
1�4
logs
(Yes
)13
.8f
BOS50
0mgqd(n
¼25
0)!
MR4at
12mo¼
12%
IM40
0mgqd
(n¼
252)
!MR4at
12mo¼
3%
Abbreviations
:AraC,c
ytarab
ine;
BELA
,Bos
utinib
Effica
cyan
dSafetyinChron
icMye
loid
Leuk
emia;b
.i.d.,tw
icedaily;B
OS,b
osutinib;D
AS,d
asatinib;D
ASISION,D
asatinib
Versu
sIm
atinibStudyinTrea
tmen
t-Naive
CMLpa
tients;ENEST1
st,E
valuatingNilo
tinibEffica
cyan
dSafetyinClinicalTrialsas
First-Line
Trea
tmen
t;ENESTn
d,E
valuatingNilo
tinibEffica
cyan
dSafetyin
Clinical
Trials–New
lyDiagn
osed
Patients;
f/u,
follo
w-up;G
IMEMA,G
ruppo
Italiano
Malattie
Ematolog
iche
dell'A
dulto;IM,imatinib;IRIS,Interna
tiona
lRan
dom
ized
Interferon
Versu
sSTI57
1;IS,Interna
tiona
lSca
le;M
DACC,M
DAnd
erso
nCan
cerC
enter;min,m
inim
um;M
R,m
olec
ular
resp
onse
;NIL,n
ilotin
ib;N
R,n
otreported;q
d,d
aily;P
EG-IFN
,pe
gylatedinterferon
a-2a
;qd,o
ncedaily;R
IGHT,
Rationa
lean
dInsigh
tfor
Gleev
ecHigh-Dos
eTh
erap
y;SPIRIT,S
TI57
1Prosp
ectiv
eRan
dom
ized
Trial;SWOG,S
outhwes
tOnc
olog
yGroup
.aNum
ber
ofsa
mplesrequiredto
mee
tcrite
riaforresp
onse
.bPatientswith
CCyR
only.
cSub
grou
pan
alys
isof
patientsen
rolledin
theIRIS
stud
yin
Aus
tralia
andNew
Zea
land
from
June
2000
toFe
bruary20
07.
dNote:
17of
thes
epatientswerealso
intheIRIS
stud
y.eBas
elineBCR–ABL1
/ABL1
ratio
bas
edon
pres
tudysa
mplesfrom
partic
ipatinglaboratory.
f Med
ianex
posu
re.
g�2
5,00
0co
piesof
ABLwererequiredforasa
mple
tobeco
nsidered
adeq
uate.
hFo
rallp
atients;
48moforpatientsaliveas
ofdatacu
toff.
i �3,00
0co
piesof
ABLwererequiredforasa
mpleto
beco
nsidered
adeq
uate.
j Stand
ardized
toSWOG-spec
ificBCR–ABL1
bas
elineleve
l.
Mahon and Etienne
Clin Cancer Res; 20(2) January 15, 2014 Clinical Cancer Research314
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988
Tab
le2.
Clinical
outcom
esof
patientswith
newly
diagn
osed
CML-CPwho
achiev
eddee
pmolec
ular
resp
onse
swith
TKIthe
rapy
Outco
mes
forpatientswithorwitho
utdee
pmolecu
lar
resp
ons
e,%
Trial
des
criptio
nN
Med
ian
f/u,
mo
Comparators
EFS
rate
PFS
rate
OSrate
TFS
rate
Etie
nneet
al.(30
):first-lineIM
400mg
266
53.2
CCyR
þMMRþ
CMRa
CCyR
þMMR�
CMRa
CCyR
�MMR
95 65 28
98 82 56
OSwas
not
differen
tam
ong
the3grou
ps
NR
NR
NR
Falchi
etal.(31
):first-lineIM
(400
mg,
n¼
83;
800mg,
n¼
204),N
IL(n
¼10
6),
orDAS(n
¼10
2)
495
73NoMRat
18mo
MMRat
18mo
MR4at
18mo
MR4.5at
18mo
Und
etec
table
BCR-A
BLb
at18
mo
NoMRat
24mo
MMRat
24mo
MR4at
24mo
MR4.5at
24mo
78(6
y)94
(6y)
97(6
y)93
(6y)
100(6
y)80
(6y)
90(6
y)97
(6y)
95(6
y)
NR
NR
NR
NR
NR
NR
NR
NR
NR
93(6
y)98
(6y)
97(6
y)95
(6y)
100(6
y)92
(6y)
97(6
y)10
0(6
y)97
(6y)
90(6
y)10
0(6
y)10
0(6
y)10
0(6
y)10
0(6
y)90
(6y)
100(6
y)10
0(6
y)10
0(6
y)Und
etec
table
BCR-A
BLb
at24
mo
100(6
y)NR
100(6
y)10
0(6
y)
CMLstud
yIV
(32):fi
rst-lineIM
400mg,
IM40
0mgþ
IFN-a
,IM
400mgþ
AraC,IM
after
IFN-a
failure,o
rIM
800mg
1,52
567
.5After
amed
iandurationof
MR4of
3.7y,
only
4of
792patientswith
CMR4(0.5%)p
rogres
sed;life
expec
tanc
ywith
MR4an
dMR4.5was
iden
tical
tothat
oftheag
e-match
edpo
pulation
Kan
tarjian
etal.(28
):retros
pectivean
alysis.IM
(400
mg,
n¼
71;8
00mg,
n¼
205)
276
48Durab
leCMRb(�
6mo)
Non
durab
leCMRb(<6mo)
NR
NR
100(5
y)98
(5y)
NR
NR
NR
NR
Vermaet
al.(29
):retros
pec
tivean
alysis.F
irst-line
IM(400
mg,
n¼
73;8
00mg,
n¼
208)
281
65CCyR
þMMRþ
CMRbat
2y
CCyR
þMMR�
CMRbat
2y
CCyR
�MMR�
CMRbat
2y
100(5
y)96
(5y)
86(5
y)
NR
NR
NR
NR
NR
NR
100(5
y)96
(5y)
91(5
y)
Press
etal.(77
):all
patientsac
hiev
edCCyR
onIM
andha
d�2
mea
suremen
tsof
BCR–ABL1
leve
lafter
achiev
ing
CCyR
9049
MMRþ
CMRc
MMR�
CMRc
NR
NR
Not
reac
hedd
44mod
NR
NR
NR
NR
Abbreviations
:AraC,c
ytarab
ine;
DAS,d
asatinib;f/u,follow-up;IM,imatinib;M
R,m
olec
ular
resp
onse
;NIL,n
ilotin
ib;N
R,n
otreported.
aCMRwas
defi
nedas
undetec
table
BCR–ABL1
tran
scrip
tswith
ase
nsitivity
of�4
.5logs
on2co
nsec
utivean
alyses
�2moap
art.
bMinim
umse
nsitivity
4.5logs
.cMinim
umse
nsitivity
4logs
.dDatash
ownaremed
ianrelapse
-freesu
rvival,d
efine
das
progres
sion
toac
celeratedph
ase/blast
crisis,los
sof
complete
hematolog
icresp
onse
,orloss
ofCCyR
.
Deep Molecular Response in Chronic Myeloid Leukemia
www.aacrjournals.org Clin Cancer Res; 20(2) January 15, 2014 315
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988
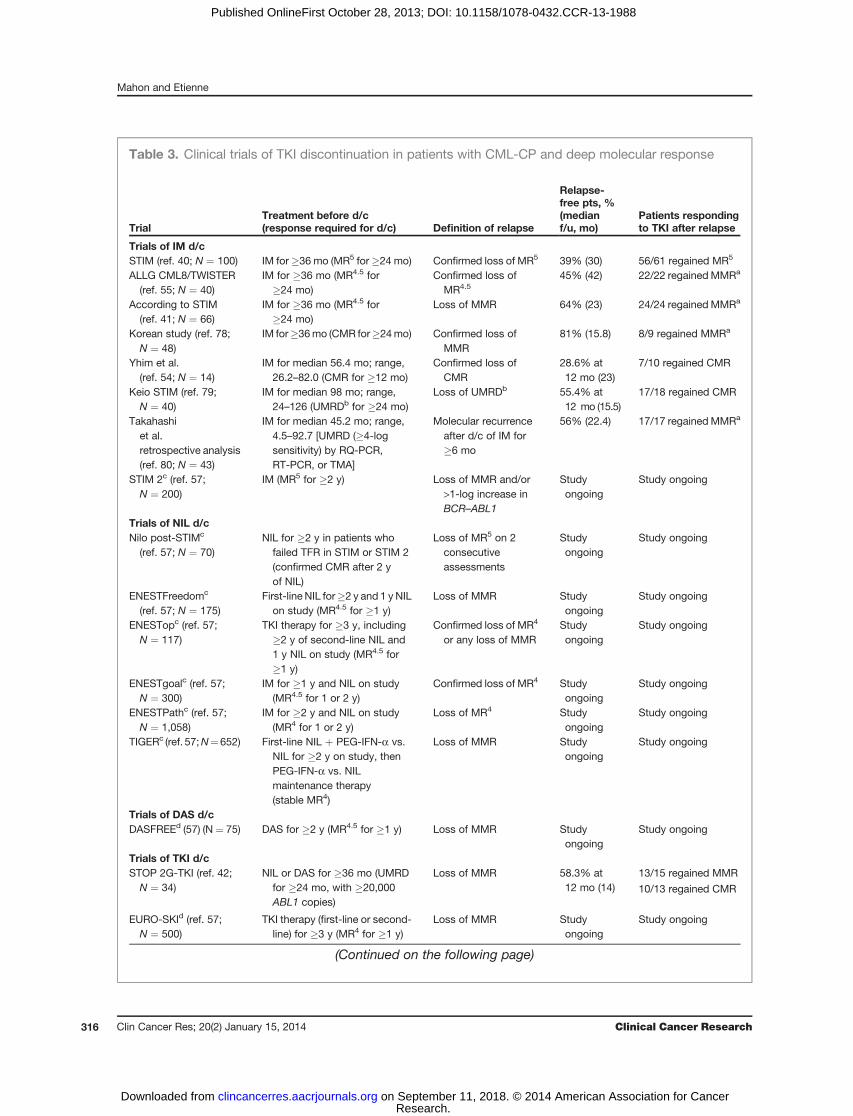
Table 3. Clinical trials of TKI discontinuation in patients with CML-CP and deep molecular response
TrialTreatment before d/c(response required for d/c) Definition of relapse
Relapse-free pts, %(medianf/u, mo)
Patients respondingto TKI after relapse
Trials of IM d/cSTIM (ref. 40; N ¼ 100) IM for�36 mo (MR5 for�24 mo) Confirmed loss of MR5 39% (30) 56/61 regained MR5
ALLG CML8/TWISTER(ref. 55; N ¼ 40)
IM for �36 mo (MR4.5 for�24 mo)
Confirmed loss ofMR4.5
45% (42) 22/22 regained MMRa
According to STIM(ref. 41; N ¼ 66)
IM for �36 mo (MR4.5 for�24 mo)
Loss of MMR 64% (23) 24/24 regained MMRa
Korean study (ref. 78;N ¼ 48)
IM for�36mo (CMR for�24mo) Confirmed loss ofMMR
81% (15.8) 8/9 regained MMRa
Yhim et al.(ref. 54; N ¼ 14)
IM for median 56.4 mo; range,26.2–82.0 (CMR for �12 mo)
Confirmed loss ofCMR
28.6% at12 mo (23)
7/10 regained CMR
Keio STIM (ref. 79;N ¼ 40)
IM for median 98 mo; range,24–126 (UMRDb for �24 mo)
Loss of UMRDb 55.4% at12 mo (15.5)
17/18 regained CMR
Takahashiet al.retrospective analysis(ref. 80; N ¼ 43)
IM for median 45.2 mo; range,4.5–92.7 [UMRD (�4-logsensitivity) by RQ-PCR,RT-PCR, or TMA]
Molecular recurrenceafter d/c of IM for�6 mo
56% (22.4) 17/17 regained MMRa
STIM 2c (ref. 57;N ¼ 200)
IM (MR5 for �2 y) Loss of MMR and/or>1-log increase inBCR–ABL1
Studyongoing
Study ongoing
Trials of NIL d/cNilo post-STIMc
(ref. 57; N ¼ 70)NIL for �2 y in patients whofailed TFR in STIM or STIM 2(confirmed CMR after 2 yof NIL)
Loss of MR5 on 2consecutiveassessments
Studyongoing
Study ongoing
ENESTFreedomc
(ref. 57; N ¼ 175)First-line NIL for�2 y and 1 y NILon study (MR4.5 for �1 y)
Loss of MMR Studyongoing
Study ongoing
ENESTopc (ref. 57;N ¼ 117)
TKI therapy for �3 y, including�2 y of second-line NIL and1 y NIL on study (MR4.5 for�1 y)
Confirmed loss of MR4
or any loss of MMRStudyongoing
Study ongoing
ENESTgoalc (ref. 57;N ¼ 300)
IM for �1 y and NIL on study(MR4.5 for 1 or 2 y)
Confirmed loss of MR4 Studyongoing
Study ongoing
ENESTPathc (ref. 57;N ¼ 1,058)
IM for �2 y and NIL on study(MR4 for 1 or 2 y)
Loss of MR4 Studyongoing
Study ongoing
TIGERc (ref. 57;N¼652) First-line NIL þ PEG-IFN-a vs.NIL for �2 y on study, thenPEG-IFN-a vs. NILmaintenance therapy(stable MR4)
Loss of MMR Studyongoing
Study ongoing
Trials of DAS d/cDASFREEd (57) (N ¼ 75) DAS for �2 y (MR4.5 for �1 y) Loss of MMR Study
ongoingStudy ongoing
Trials of TKI d/cSTOP 2G-TKI (ref. 42;N ¼ 34)
NIL or DAS for �36 mo (UMRDfor �24 mo, with �20,000ABL1 copies)
Loss of MMR 58.3% at12 mo (14)
13/15 regained MMR
10/13 regained CMR
EURO-SKId (ref. 57;N ¼ 500)
TKI therapy (first-line or second-line) for �3 y (MR4 for �1 y)
Loss of MMR Studyongoing
Study ongoing
(Continued on the following page)
Mahon and Etienne
Clin Cancer Res; 20(2) January 15, 2014 Clinical Cancer Research316
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988

study, molecular relapse was less stringently defined as lossof MMR at any time (41). In According to STIM, all 24patients who relapsed regained a response ofMMRor betteronce imatinib was reintroduced (41); therefore, waitinguntil a patient loses MMR to reinitiate TKI therapy doesnot seem to be detrimental. This suggests that BCR–ABL1positivity after TKI cessation does not necessarily equaldisease relapse (22). However, the optimal molecularresponse threshold for triggering restart of TKI therapyremains to be established.Data on discontinuation of second-generation TKIs are
limited; however, the ongoing STOP 2G-TKI study hasshown similar results to those of imatinib discontinuationtrials (Table 3; ref. 42). Thus, available results suggest thatstopping TKI therapy in patients with sustained deepmolec-ular response can be safe and associated with prolongedTFR. Given the preliminary nature of available clinical dataon TFR, both the ELN and the National ComprehensiveCancer Network currently recommend that patients remainon TKI therapy indefinitely and that TKI discontinuationonly be attempted in controlled clinical trials (6, 7).
Factors Affecting Achievement of DeepMolecular ResponseAchievement ofBCR–ABL1IS�10%at 3 or 6months after
initiating first-line imatinib has been shown to be predictiveof long-term molecular response and improved outcomes(19, 43, 44), whereas delayed cytogenetic and molecularresponse on imatinib is associated with increased risk ofprogression (45). Landmark studies of second-generationTKIs have found BCR–ABL1 levels at 3 months to besimilarly predictive (46, 47). A retrospective analysis of
patients treated with second-line nilotinib, dasatinib, orbosutinib found that BCR–ABL1IS �10% at 3 months fromstart of second-line treatment was associated with signifi-cantly higher cumulative incidence of MMR and CMR andimproved OS, PFS, and EFS (48). An online database ofpatients with CML-CP treated with first-line imatinib inJapan found that patients with an MMR at 12 months weresignificantly more likely than those without to achieveundetectable BCR–ABL1 transcripts by 72 months (49).Another study found a similar association in patients trea-ted with first-line or second-line imatinib (24).
Other factors that may affect achievement of deepmolec-ular response include risk score, sex, adherence to treat-ment, and dose intensity. For example, in the EvaluatingNilotinib Efficacy and Safety in Clinical Trials–Newly Diag-nosed Patients (ENESTnd) phase III trial of first-line nilo-tinib versus imatinib, rates of deepmolecular responsewerelowest among patients with high Sokal score, althoughmore high-risk patients achieved MR4.5 by 3 years onnilotinib than imatinib (24%, 27%, and 9% in the nilotinib300 mg b.i.d., nilotinib 400 mg b.i.d., and imatinib arms,respectively; ref. 10). Univariate analysis of a study inpatients treatedwith first-line imatinib showed that femaleswere more likely than males to achieve stable undetectableBCR–ABL1 (with a RQ-PCR sensitivity of �4.5 log) by 8years (68% vs. 30%, respectively; ref. 50). Multivariateanalysis of a study in Japanese patients found adherenceto standard-dose imatinib to be predictive of CMR achieve-ment (51). Another study reported adherence to standard-dose imatinib as the only independent predictor of CMR;poor adherence and failure to achieve MMR predictedtreatment discontinuation and eventual loss of CCyR(52, 53).
Table 3.Clinical trialsof TKIdiscontinuation inpatientswithCML-CPanddeepmolecular response (Cont'd )
TrialTreatment before d/c(response required for d/c) Definition of relapse
Relapse-free pts, %(medianf/u, mo)
Patients respondingto TKI after relapse
DESTINYd (ref. 57;N ¼ 168)
IM, NIL, or DAS for �3 y andhalf-standard dose of TKI for1 y on study (MMR or MR4 for�1 y at therapeutic dose and1 y at half-standard dose)
Loss of MMR Studyongoing
Study ongoing
NCT00573378c (ref.57; N ¼ 40)
NIL or IM for �3 y, with stabledose for �1 y and sameTKI þ PEG-IFN-a for 2 y onstudy (NR)
NR Studyongoing
Study ongoing
Abbreviations: ALLG, Australasian Leukaemia and LymphomaGroup; DAS, dasatinib; d/c, discontinuation; f/u, follow-up; IM, imatinib;MR, molecular response; NIL, nilotinib; NR, not reported; PEG-IFN-a, pegylated interferon-a; RT-PCR, nested reverse transcriptasePCR; TMA, transcription-mediated amplification; UMRD, undetectable minimal residual disease.aPatients achieved this level of response or better.bUMRD defined as <100 copies by TMA; thus, loss of UMRD was >100 copies by TMA.cCurrently recruiting participants.dNot yet recruiting participants.
Deep Molecular Response in Chronic Myeloid Leukemia
www.aacrjournals.org Clin Cancer Res; 20(2) January 15, 2014 317
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988

Factors Affecting Durability of Deep MolecularResponse Off Treatment
The high rates of and rapidity of disease relapseobserved in patients who discontinue TKI therapy with-out deep molecular response (34–37) suggest that themain factor influencing relapse risk off therapy is the levelof residual molecular disease present when TKI therapy isstopped. However, even among patients with sustained,undetectable disease on TKI therapy, a significant per-centage of patients have experienced disease relapse (40),and several studies have evaluated factors potentiallycontributing to a patient’s ability to achieve successfulTFR.
Studies of imatinib discontinuation have found anassociation between Sokal score and relapse risk (39,40, 54, 55), suggesting that patients with high Sokal riskmay have inherent biologic attributes that drive develop-ment of disease relapse once BCR–ABL1 inhibition isrelieved. The duration of deep molecular response beforeTKI discontinuation and the overall duration of prior TKItreatment also seem to be important (39, 40, 56). Basedon this, the majority of ongoing studies require patientsto maintain a deep molecular response for �2 years andhave had �3 years of prior TKI treatment before attempt-ing discontinuation. More rapid achievement of deepmolecular response may also be predictive of successfulTFR (54, 55).
In the STIM study, the only factors associated withlower risk of relapse were low/intermediate Sokal scoreand duration of imatinib treatment >5 years (39, 40).Another study identified a subgroup of patients withincreased risk of molecular relapse following imatinibdiscontinuation, characterized by the following: highSokal score, >24 months to CMR, and <33 months ofimatinib after achieving CMR; patients with any of thesecharacteristics had a 0% probability of CMR persistenceat 1 year, compared with 80% probability in patientswithout these characteristics (54). Several other ongoingTKI discontinuation studies aim to determine other fac-tors that may play a role in relapse off treatment (Table3). For example, the large, phase III EURO-SKI study(NCT01596114) will explore factors associated withmolecular relapse in patients with stable MR4 who stopTKI therapy, and STIM 2 (NCT01343173) will evaluatefactors predictive of sustained deep molecular responseafter imatinib discontinuation (57). Current data suggestthat deep molecular response is heterogeneous, anddifferent patients may have differing levels of residualdisease burden despite having undetectable disease (22).
Most, if not all, patients with sustained CMR havepersistent BCR–ABL1-positive cells (based on PCR at aDNA level; ref. 55 and 58); however, this persistence doesnot necessarily lead to relapse after treatment discontinu-ation. Furthermore, the kinetics of relapse after treatmentdiscontinuation vary, with early and late molecularrelapses observed (39). This discrepancy may reflect theheterogeneity of CML at the stem cell level. The develop-
ment of highly sensitive techniques like ultra-deepsequencing (UDS) and massive parallel sequencing (MPS)may help clarify these differences. Indeed, both UDS andMPS detected more complex mutation dynamics in TKI-resistant patients than conventional Sanger sequencing(59, 60).
Mathematical modeling of the kinetics of molecularrelapse in patients in the STIM study has led to a hypothesisthat selective pressure exerted by imatinib treatment resultsin an increased frequency of LSC clones with slower growthand differentiation than the predominant clone at baseline(61). Imatinib therapy may affect the ability of LSCs toproduce differentiated populations and may affect the celldivision of progenitors and differentiated leukemic cells(61). The effects of imatinib on leukemia-initiating cells(LIC) may differ from patient to patient, and these differ-ences maymanifest in varying times tomolecular relapse inpatients with deep molecular response who stop imatinibtreatment (Fig. 2).
It remains to be established whether the ultimate goalof treatment for patients with CML-CP will be a "clinicalcure" (i.e., the absence of relapse) or a "biological cure"(i.e., absence of all leukemic cells, including LSCs;refs. 22, 62, 63). Multiple strategies for specifically tar-geting the LSC reservoir in patients with CML are underinvestigation, including combination of a BCR–ABL1 TKIwith other targeted agents, such as inhibitors of theHedgehog, Wnt/B-catenin, or Notch signaling pathways,or immunomodulatory agents, such as IFN (22, 62, 63).In one study, maintenance therapy with peglyated IFNfollowing imatinib discontinuation led to retained orimproved molecular responses in the majority ofpatients, most of whom did not have deep molecularresponses (64). This may represent a viable strategy forpatients who wish to stop TKI therapy in the absence ofdeep molecular response; the ongoing TIGER study isfurther investigating this approach (Table 3). Quantifi-cation of a patient’s residual LSC reservoir and the effectof such combination treatments on LSCs remains achallenge (22, 65). Given the potential diversity in dis-ease burden and relapse risk in patients who discontinueTKI therapy, rigorous long-term follow-up is essential,and discontinuation should only be attempted in clinicaltrials.
ConclusionsMolecular monitoring affords a precise, convenient
method for monitoring residual disease burden inpatients with CML-CP. As TKIs have improved patientoutcomes, clinical trial designs have begun to evaluatedeeper levels of molecular response. Deep molecularresponses are associated with improved rates of PFS, EFS,and OS, and reduced risk of progression to advanceddisease. Furthermore, a sustained deep molecularresponse is an essential entry criterion for studies of TFR.The ability to achieve deep molecular response on ther-apy, and sustain this response off therapy, may be
Mahon and Etienne
Clin Cancer Res; 20(2) January 15, 2014 Clinical Cancer Research318
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988

affected by a variety of factors, including disease char-acteristics, risk score, and adherence to and time ontreatment. As more is learned about the optimal criteriafor successful TKI discontinuation, patients may haveincreased chances of achieving treatment-free diseasecontrol, a first step toward the elusive cure for CML.
Disclosure of Potential Conflicts of InterestF.-X. Mahon has received commercial research grants from Bristol-Myers
Squibb and Novartis Pharma. F.-X. Mahon is a consultant/advisory boardmember of Bristol-Myers Squibb,Novartis Pharma, andAriad. G. Etienne is aconsultant/advisoryboardmemberof Bristol-Myers Squibb,Novartis, Pfizer,and Ariad.
Authors' ContributionsConception and design: F.-X. Mahon, G. EtienneDevelopment of methodology: F.-X. MahonWriting, review, and/or revision of themanuscript: F.-X. Mahon, G. Etienne
AcknowledgmentsThe authors thank K. Miller-Moslin, PhD, and P. Tuttle, PhD (Articulate
Science), for medical editorial assistance.
Grant SupportFinancial support formedical editorial assistance was provided byNovar-
tis Pharmaceuticals Corporation.
Received July 19, 2013; revisedOctober 8, 2013; acceptedOctober 9, 2013;published OnlineFirst October 22, 2013.
References1. Van Etten RA, Shannon KM. Focus onmyeloproliferative diseases and
myelodysplastic syndromes. Cancer Cell 2004;6:547–52.2. Natoli C, Perrucci B, Perrotti F, Falchi L, Iacobelli S, Consorzio
Interuniversitario Nazionale per Bio-Oncologia (CINBO).
CCR Reviews
© 2013 American Association for Cancer Research
LSCs
A
B
LICs Imatinib therapySTOP
STOP
LSCs LICs Imatinib therapy
LIC with intrinsicallyfaster growth rate
Sur
viva
l with
out
mo
lecu
lar
rela
pse
Months since discontinuation of imatinib
0.00 3 6 9 12 15 18 21 24 27 30 33
Stem cell persistence butundetectable using RQ-PCR
(5-log sensitivity)
Late molecular relapse
Early molecular relapse
36 39 42 45 48 51 54 57 60
0.10.20.30.40.50.60.70.80.91.0
LIC with intrinsicallyslower growth rate
Sur
viva
l with
out
mo
lecu
lar
rela
pse
Months since discontinuation of imatinib
0.00 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60
0.10.20.30.40.50.60.70.80.91.0
Figure 2. Hypothesis for variability in duration of deepmolecular response in patientswho discontinue imatinib. Imatinib treatment has differing effects on LICsthat introduce variability in times to molecular relapse after imatinib discontinuation. A, in some patients, imatinib treatment may successfully eradicate LICs,leaving only a small population of quiescent LSCs that is undetectable by conventional RQ-PCR (�5-log sensitivity), enabling prolonged TFR. B, in otherpatients, populations of LICs with variable growth kinetics remain. Patients with faster-growing residual LICs experience more rapid molecular relapse ondiscontinuation of imatinib treatment, whereas patients with slower-growing residual LICs experience later molecular relapse. Inset graphs show the Kaplan–Meier estimate of relapse-free survival in the STIM study (relapse defined as confirmed loss of molecular response �5-log reduction) based on a medianfollow-up of 30 months (40).
Deep Molecular Response in Chronic Myeloid Leukemia
www.aacrjournals.org Clin Cancer Res; 20(2) January 15, 2014 319
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988
Tyrosine kinase inhibitors. Curr Cancer Drug Targets 2010;10:462–83.
3. DrukerBJ. Translationof thePhiladelphia chromosome into therapy forCML. Blood 2008;112:4808–17.
4. Melo JV, Barnes DJ. Chronic myeloid leukaemia as amodel of diseaseevolution in human cancer. Nat Rev Cancer 2007;7:441–53.
5. Hernandez-Boluda JC, Cervantes F. Prognostic factors inchronic myeloid leukaemia. Best Pract Res Clin Haematol 2009;22:343–53.
6. Baccarani M, Deininger MW, Rosti G, Hochhaus A, Soverini S,Apperley JF, et al. European LeukemiaNet recommendations forthe management of chronic myeloid leukemia: 2013. Blood 2013;122:872–84.
7. National Comprehensive Cancer Network. NCCN Clinical PracticeGuidelines in Oncology: Chronic Myelogenous Leukemia. Version4.2013. [cited 2013 Jul 12]. Available from: http://www.nccn.org/pro-fessionals/physician_gls/pdf/cml.pdf.
8. Deininger M, O'Brien SG, Guilhot F, Goldman JM, Hochhaus A,Hughes TP, et al. International randomized study of interferon vs.STI571 (IRIS) 8-year follow up: sustained survival and low risk forprogression or events in patients with newly diagnosed chronic mye-loid leukemia in chronic phase (CML-CP) treated with imatinib. Blood2009;114:462 (abstr 1126).
9. Kantarjian HM, Shah NP, Cortes JE, Baccarani M, Agarwal MB,Undurraga MS, et al. Dasatinib or imatinib in newly diagnosed chronicphase chronic myeloid leukemia: 2-year follow-up from a randomizedphase 3 trial (DASISION). Blood 2012;119:1123–9.
10. Larson RA, Hochhaus A, Hughes TP, Clark RE, Etienne G, Kim DW,et al. Nilotinib vs. imatinib in patients with newly diagnosed Philadel-phia chromosome-positive chronicmyeloid leukemia in chronicphase:ENESTnd 3-year follow-up. Leukemia 2012;26:2197–203.
11. Cross NCP, White H, M€uller MC, Saglio G, Hochhaus A. Standardizeddefinitions of molecular response in chronic myeloid leukemia. Leu-kemia 2012;26:2172–5.
12. Tibes R, Mesa RA. Evolution of clinical trial endpoints in chronicmyeloid leukemia: efficacious therapies require sensitive monitoringtechniques. Leuk Res 2012;36:664–71.
13. Cortes J, Quintas-Cardama A, Kantarjian HM. Monitoring molecularresponse in chronic myeloid leukemia. Cancer 2011;117:1113–22.
14. Hughes T, Deininger M, Hochhaus A, Branford S, Radich J, Kaeda J,et al. Monitoring CML patients responding to treatment with tyrosinekinase inhibitors: review and recommendations for harmonizing cur-rent methodology for detecting BCR-ABL transcripts and kinasedomain mutations and for expressing results. Blood 2006;108:28–37.
15. Hughes TP, Kaeda J, Branford S, Rudzki Z, Hochhaus A, Hensley ML,et al. Frequency ofmajormolecular responses to imatinib or interferon-aplus cytarabine in newly diagnosed chronicmyeloid leukemia. NEnglJ Med 2003;349:1423–32.
16. Press RD, Love Z, Tronnes AA, Yang R, Tran T, Mongoue-Tchokote S,et al. BCR-ABL mRNA levels at and after the time of a completecytogenetic response (CCR) predict the duration of CCR in imatinibmesylate-treated patients with CML. Blood 2006;107:4250–6.
17. Cortes J, Talpaz M, O'Brien S, Jones D, Luthra R, Shan J, et al.Molecular responses in patients with chronic myelogenous leukemiain chronic phase treated with imatinib mesylate. Clin Cancer Res2005;11:3425–32.
18. Pavlovsky C, Giere I, Moiraghi B, PavlovskyMA, Aranguren PN,GarciaJ, et al. Molecular monitoring of imatinib in chronic myeloid leukemiapatients in complete cytogenetic remission: does achievement of astable major molecular response at any time point identify a privilegedgroup of patients? Amulticenter experience in Argentina andUruguay.Clin Lymphoma Myeloma Leuk 2011;11:280–5.
19. Hughes TP, Hochhaus A, Branford S, Muller MC, Kaeda JS, Foroni L,et al. Long-termprognostic significance of earlymolecular response toimatinib in newly diagnosed chronic myeloid leukemia: an analysisfrom the International Randomized Study of Interferon Versus STI571(IRIS). Blood 2010;116:3758–65.
20. Breccia M, Alimena G. The significance of early, major and stablemolecular responses in chronic myeloid leukemia in the imatinib era.Crit Rev Oncol Hematol 2011;79:135–43.
21. Mahon FX. Is going for cure in chronic myeloid leukemia possible andjustifiable? Hematology Am Soc Hematol Educ Program 2012;2012:122–8.
22. Rea D, Rousselot P, Guilhot J, Guilhot F, Mahon FX. Curing chronicmyeloid leukemia. Curr Hematol Malig Rep 2012;7:103–8.
23. Branford S, Fletcher L, Cross NC, Muller MC, Hochhaus A, Kim DW,et al. Desirable performance characteristics for BCR-ABL measure-ment on an international reporting scale to allow consistent interpre-tation of individual patient response and comparison of response ratesbetween clinical trials. Blood 2008;112:3330–8.
24. Branford S, Seymour JF, Grigg A, Arthur C, Rudzki Z, Lynch K, et al.BCR-ABL messenger RNA levels continue to decline in patients withchronic phase chronic myeloid leukemia treated with imatinib for morethan 5years and approximately half of all first-line treated patients havestable undetectable BCR-ABL using strict sensitivity criteria. ClinCancer Res 2007;13:7080–5.
25. Burmeister T, Reinhardt R. A multiplex PCR for improved detection oftypical and atypical BCR-ABL fusion transcripts. Leuk Res 2008;32:579–85.
26. PreudhommeC, Guilhot J, Nicolini FE, Guerci-Bresler A, Rigal-HuguetF, Maloisel F, et al. Imatinib plus peginterferon a-2a in chronic myeloidleukemia. N Engl J Med 2010;363:2511–21.
27. Hehlmann R, Lauseker M, Jung-Munkwitz S, Leitner A, Muller MC,PletschN, et al. Tolerability-adapted imatinib 800mg/d versus 400mg/d versus 400 mg/d plus interferon-alpha in newly diagnosed chronicmyeloid leukemia. J Clin Oncol 2011;29:1634–42.
28. Kantarjian H, O'Brien S, Shan J, Huang X, Garcia-Manero G, Faderl S,et al. Cytogenetic and molecular responses and outcome in chronicmyelogenous leukemia: need for new response definitions? Cancer2008;112:837–45.
29. Verma D, Kantarjian HM, Shan J, O'Brien S, Verma A, Jabbour E, et al.Sustained completemolecular response to imatinib in chronicmyeloidleukemia (CML): a target worth aiming and achieving? Blood 2009;114(abstr 505).
30. Etienne G, Nicolini FE, Dulucq S, Schmitt A, Hayette S, Lippert E, et al.Achieving a complete molecular remission under imatinib therapy isassociated with a better outcome in chronic phase chronic myeloidleukaemia patients on imatinib frontline therapy. Blood 2012;120 (abstr3754).
31. Falchi L, Kantarjian HM, Quintas-Cardama A, O'Brien S, Jabbour EJ,Ravandi F, et al. Clinical significance of deeper molecular responseswith four modalities of tyrosine kinase inhibitors as frontline therapy forchronic myeloid leukemia. Blood 2012;120 (abstr 164).
32. HehlmannR, LausekerM,HanfsteinB,M€ullerMC, Schreiber A, ProetelU, et al. Complete molecular remission (CMR 4.5) of CML is inducedfaster by dose—optimized imatinib predicts better survival—resultsfrom the randomized CML-study IV. Blood 2012;120 (abstr 67).
33. Hughes TP, Lipton JH, Spector N, Leher B, Pasquini R, Clementino N,et al. Switching to nilotinib is associated with continued deepermolecular responses in CML-CP patients with minimal residual dis-ease after �2 years on imatinib: ENESTcmr 2-year follow-up results.Blood 2012;120 (abstr 694).
34. Cortes J, O'Brien S, Kantarjian H. Discontinuation of imatinib therapyafter achieving a molecular response. Blood 2004;104:2204–5.
35. Mauro MJ, Druker BJ, Maziarz RT. Divergent clinical outcome in twoCML patients who discontinued imatinib therapy after achieving amolecular remission. Leuk Res 2004;28(suppl 1):S71–3.
36. Merante S, Orlandi E, Bernasconi P, Calatroni S, Boni M, Lazzarino M.Outcome of four patients with chronic myeloid leukemia after imatinibmesylate discontinuation. Haematologica 2005;90:979–81.
37. Michor F, Hughes TP, Iwasa Y, Branford S, Shah NP, Sawyers CL,et al. Dynamics of chronic myeloid leukaemia. Nature 2005;435:1267–70.
38. Rousselot P, Huguet F, Rea D, Legros L, Cayuela JM, Maarek O, et al.Imatinib mesylate discontinuation in patients with chronic myeloge-nous leukemia in complete molecular remission for more than 2 years.Blood 2007;109:58–60.
39. Mahon FX, Rea D, Guilhot J, Guilhot F, Huguet F, Nicolini F, et al.Discontinuation of imatinib in patients with chronic myeloid leukaemiawho have maintained complete molecular remission for at least 2
Mahon and Etienne
Clin Cancer Res; 20(2) January 15, 2014 Clinical Cancer Research320
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988
years: the prospective, multicentre stop imatinib (STIM) trial. LancetOncol 2010;11:1029–35.
40. Mahon F, Rea D, Guilhot J, Guilhot F, Huguet F, Nicolini FE, et al.Discontinuation of imatinib in patients with chronic myeloid leukemiawho have maintained complete molecular response: update results ofthe STIM study. Blood 2011;118 (abstr 603).
41. Rousselot P, Charbonnier A, Cony-Makhoul P, Agape P, Nicolini F,Varet B, et al. Loss of major molecular response is accurate forrestarting imatinib after imatinib discontinuation in CP-CML patientswith long lasting CMR: importance of fluctuating values of MRD andinterferon. Haematologica 2012;97(s1):77 (abstr 194).
42. Rea D, Rousselot P, Guilhot F, Tulliez M, Nicolini FE, Guerci-Bresler A,et al. Discontinuation of second generation (2G) tyrosine kinase inhi-bitors (TKI) in chronic phase (CP)-chronic myeloid leukemia (CML)patients with stable undetectable BCR-ABL transcripts. Blood2012;120 (abstr 916).
43. Marin D, Hedgley C, Clark RE, Apperley J, Foroni L, Milojkovic D, et al.Predictive value of early molecular response in patients with chronicmyeloid leukemia treated with first-line dasatinib. Blood 2012;120:291–4.
44. HanfsteinB,MullerMC,HehlmannR, ErbenP, LausekerM, FabariusA,et al. Early molecular and cytogenetic response is predictive for long-term progression-free and overall survival in chronic myeloid leukemia(CML). Leukemia 2012;26:2096–102.
45. Quintas-Cardama A, Kantarjian H, Jones D, Shan J, Borthakur G,Thomas D, et al. Delayed achievement of cytogenetic and molecularresponse is associated with increased risk of progression amongpatients with chronic myeloid leukemia in early chronic phasereceiving high-dose or standard-dose imatinib therapy. Blood 2009;113:6315–21.
46. HochhausA,Guilhot F, Haifa Al-Ali K, Rosti G,NakasekoC, Antonio DeSouzaC, et al. EarlyBCR-ABL transcript levels predict futuremolecularresponse and long-term outcomes in newly diagnosed patients withCML-CP: analysis of ENESTnd 3-year data. Haematologica 2012;97(s1):237 (abstr 0584).
47. Hochhaus A, Boque C, Bradley Garelik MB, Manos G, Steegmann JL.Molecular response kinetics and BCR-ABL reductions in patients withnewly diagnosed chronicmyeloid leukemia in chronic phase (CML-CP)receiving dasatinib versus imatinib: DASISION 3-year follow-up. Hae-matologica 2012;97(s1):609 (abstr 1537).
48. Milojkovic D, Apperley JF, Gerrard G, Ibrahim AR, Szydlo R, Bua M,et al. Responses to second-line tyrosine kinase inhibitors are durable:an intention-to-treat analysis in chronic myeloid leukemia patients.Blood 2012;119:1838–43.
49. Tauchi T, Kizaki M, Okamoto S, Tanaka H, Tanimoto M, Inokuchi K,et al. Seven-year follow-up of patients receiving imatinib for thetreatment of newly diagnosed chronic myelogenous leukemia by theTARGET system. Leuk Res 2011;35:585–90.
50. Branford S, RossD, Prime J, FieldC, AltamuraH, YeomanA, et al. Earlymolecular response and female sex strongly predict achievement ofstable undetectable BCR–ABL1, a criterion for imatinib discontinua-tion in patients with CML. Blood 2012;120 (abstr 165).
51. Yoshida C, Komeno T, Hori M, Kimura T, Fujii M, Okoshi Y, et al.Adherence to the standard dose of imatinib, rather than dose adjust-ment based on its plasma concentration, is critical to achieve a deepmolecular response in patients with chronic myeloid leukemia. Int JHematol 2011;93:618–23.
52. Marin D, Bazeos A, Mahon FX, Eliasson L, Milojkovic D, Bua M, et al.Adherence is the critical factor for achieving molecular responses inpatients with chronic myeloid leukemia who achieve complete cyto-genetic responses on imatinib. J Clin Oncol 2010;28:2381–8.
53. Ibrahim AR, Eliasson L, Apperley JF, Milojkovic D, Bua M, Szydlo R,et al. Poor adherence is the main reason for loss of CCyR and imatinibfailure for chronic myeloid leukemia patients on long term therapy.Blood 2011;117:3733–6.
54. Yhim HY, Lee NR, Song EK, Yim CY, Jeon SY, Shin S, et al. Imatinibmesylate discontinuation in patients with chronic myeloid leukemiawho have received front-line imatinib mesylate therapy and achievedcomplete molecular response. Leuk Res 2012;36:689–93.
55. Ross DM, Branford S, Seymour JF, Schwarer AP, Arthur C, Yeung DT,et al. Safety and efficacy of imatinib cessation for CML patients withstable undetectableminimal residual disease:Results from theTWIST-ER study. Blood 2013;122:515–22.
56. Lee SE, Choi SY, Bang JH, Kim SH, Jang EJ, Choi M, et al. BCR-ABLkinetics after discontinuation of imatinib in CMLpatients withMR4.5 orundetectable molecular residual disease. Haematologica 2012;97(s1):80 (abstr 200).
57. U.S. National Institutes of Health. Clinicaltrials.gov. [cited 2013 Sept12]. Available from: http://www.clinicaltrials.gov/.
58. Ross DM, Branford S, Seymour JF, Schwarer AP, Arthur C, Bartley PA,et al. Patients with chronic myeloid leukemia whomaintain a completemolecular response after stopping imatinib treatment have evidence ofpersistent leukemia by DNA PCR. Leukemia 2010;10:1719–1724.
59. Eyal E, Tohami T, Amir A, Cesarkas K, Jacob-Hirsch J, Volchek Y, et al.Detection of BCR–ABL1 mutations in chronic myeloid leukaemia bymassive parallel sequencing. Br J Haematol 2013;160:477–86.
60. Soverini S, De Benedittis C, Machova Polakova K, Brouckova A,Horner D, IaconoM, et al. Unraveling the complexity of tyrosine kinaseinhibitor-resistant populations by ultra-deep sequencing of the BCR-ABL kinase domain. Blood 2013;122:1634–48.
61. Tang M, Foo J, Gonen M, Guilhot J, Mahon FX, Michor F. Selectionpressure exerted by imatinib therapy leads to disparate outcomes ofimatinib discontinuation trials. Haematologica 2012;97:1553–61.
62. Chomel JC, Turhan AG. Chronicmyeloid leukemia stem cells in the eraof targeted therapies: resistance, persistence and long-term dorman-cy. Oncotarget 2011;2:713–27.
63. Ross DM, Hughes TP, Melo JV. Do we have to kill the last CML cell?Leukemia 2011;25:193–200.
64. Burchert A, Muller MC, Kostrewa P, Erben P, Bostel T, Liebler S, et al.Sustained molecular response with interferon alfa maintenance afterinduction therapy with imatinib plus interferon alfa in patients withchronic myeloid leukemia. J Clin Oncol 2010;28:1429–35.
65. Chu S, McDonald T, Lin A, Chakraborty S, Huang Q, Snyder DS, et al.Persistence of leukemia stem cells in chronic myelogenous leukemiapatients in prolonged remission with imatinib treatment. Blood2011;118:5565–72.
66. Kantarjian H, Talpaz M, O'Brien S, Garcia-Manero G, Verstovsek S,Giles F, et al. High-dose imatinib mesylate therapy in newly diagnosedPhiladelphia chromosome-positive chronic phase chronic myeloidleukemia. Blood 2004;103:2873–8.
67. deLavalladeH,Apperley JF,KhorashadJS,MilojkovicD,ReidAG,BuaM, et al. Imatinib for newly diagnosed patients with chronic myeloidleukemia: incidence of sustained responses in an intention-to-treatanalysis. J Clin Oncol 2008;26:3358–63.
68. Cortes JE, Kantarjian HM, Goldberg SL, Powell BL, Giles FJ, WetzlerM, et al. High-dose imatinib in newly diagnosed chronic-phase chronicmyeloid leukemia: high rates of rapid cytogenetic and molecularresponses. J Clin Oncol 2009;27:4754–9.
69. Hochhaus A, Rosti G, le Coutre PD, Ossenkoppele G, Griskevicius L,Rea D, et al. ENEST1st: nilotinib in patients with newly diagnosedchronic myeloid leukemia in chronic phase (CML-CP): a European andEUTOS clinical initiative for standardization of molecular response.Haematologica 2012;97(s1):74 (abstr 0188).
70. Gugliotta G, Castagnetti F, Breccia M, Levato L, Capucci A, Tiribelli M,et al. Early CP CML, nilotinib 400 mg twice daily frontline: beyond 3years, results remain excellent and stable (A GIMEMA CML WorkingParty trial). Blood 2011;116 (abstr 2756).
71. Rosti G, Gugliotta G, Castagnetti F, Breccia M, Levato L, Rege-Cambrin G, et al. Five-year results of nilotinib 400 mg BID in earlychronic phase chronic myeloid leukemia (CML): high rate of deepmolecular response—update of the GIMEMACMLWP trial CML0307.Blood 2012;120 (abstr 3784).
72. Cortes JE, Jones D, O'Brien S, Jabbour E, Konopleva M, Ferrajoli A,et al. Nilotinib as front-line treatment for patients with chronic myeloidleukemia in early chronic phase. J Clin Oncol 2010;28:392–7.
73. Nicolini FE, Etienne G, Dubruille V, Roy L, Huguet F, Legros L, et al.Pegylated interferon-a2a incombination to nilotinib as first line therapyin newly diagnosed chronic phase chronic myelogenous leukemia
Deep Molecular Response in Chronic Myeloid Leukemia
www.aacrjournals.org Clin Cancer Res; 20(2) January 15, 2014 321
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988

provides high rates of MR4.5. Preliminary results of a phase II study.Blood 2012;120 (suppl; abstr 166).
74. Radich JP, Kopecky KJ, Applebaum FR, Kamel-Reid S, Stock W,Malnassy G, et al. A randomized trial of dasatinib 100 mg vs imatinib400 mg in newly diagnosed chronic phase chromic myeloid leukemia.Blood 2012;120:3898–905.
75. Cortes JE, Jones D, O'Brien S, Jabbour E, Ravandi F, Koller C, et al.Results of dasatinib therapy in patients with early chronic-phasechronic myeloid leukemia. J Clin Oncol 2010;28:398–404.
76. Cortes JE, Kim DW, Kantarjian HM, Brummendorf TH, Dyagil I, Gris-kevicus L, et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: results from the BELA trial. J ClinOncol 2012;30:3486–92.
77. Press RD, Galderisi C, Yang R, Rempfer C, Willis SG, Mauro MJ,et al. A half-log increase in BCR-ABL RNA predicts a higher risk of
relapse in patients with chronic myeloid leukemia with an imatinib-induced complete cytogenetic response. Clin Cancer Res 2007;13:6136–43.
78. Lee S, Choi SY, Bang J, Kim S, Jang E, Byeun J, et al. Predictivefactors for successful imatinib cessation in chronic myeloidleukemia patients treated with imatinib. Am J Hematol 2013;88:449–54.
79. Matsuki E, Ono Y, Tonegawa K, Sakurai M, Kunimoto H, Ishizawa J,et al. Detailed investigation on characteristics of Japanese patientswith chronic phase CML who achieved a durable CMR after discon-tinuation of imatinib—an updated result of the Keio STIM study. Blood2012;120 (abstr 2788).
80. Takahashi N, Kyo T,Maeda Y, Sugihara T, Usuki K, Kawaguchi T, et al.Discontinuation of imatinib in Japanese patients with chronic myeloidleukemia. Haematologica 2012;97:903–6.
Mahon and Etienne
Clin Cancer Res; 20(2) January 15, 2014 Clinical Cancer Research322
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988
2014;20:310-322. Published OnlineFirst October 28, 2013.Clin Cancer Res François-Xavier Mahon and Gabriel Etienne Goal of Therapy?Deep Molecular Response in Chronic Myeloid Leukemia: The New
Updated version
10.1158/1078-0432.CCR-13-1988doi:
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/2/310.full#ref-list-1
This article cites 66 articles, 33 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/2/310.full#related-urls
This article has been cited by 10 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/20/2/310To request permission to re-use all or part of this article, use this link
Research. on September 11, 2018. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 28, 2013; DOI: 10.1158/1078-0432.CCR-13-1988