dural folds and cavernous sinus
TRANSCRIPT
DURAL FOLDS AND CAVERNOUS SINUS
M.ARAVIND
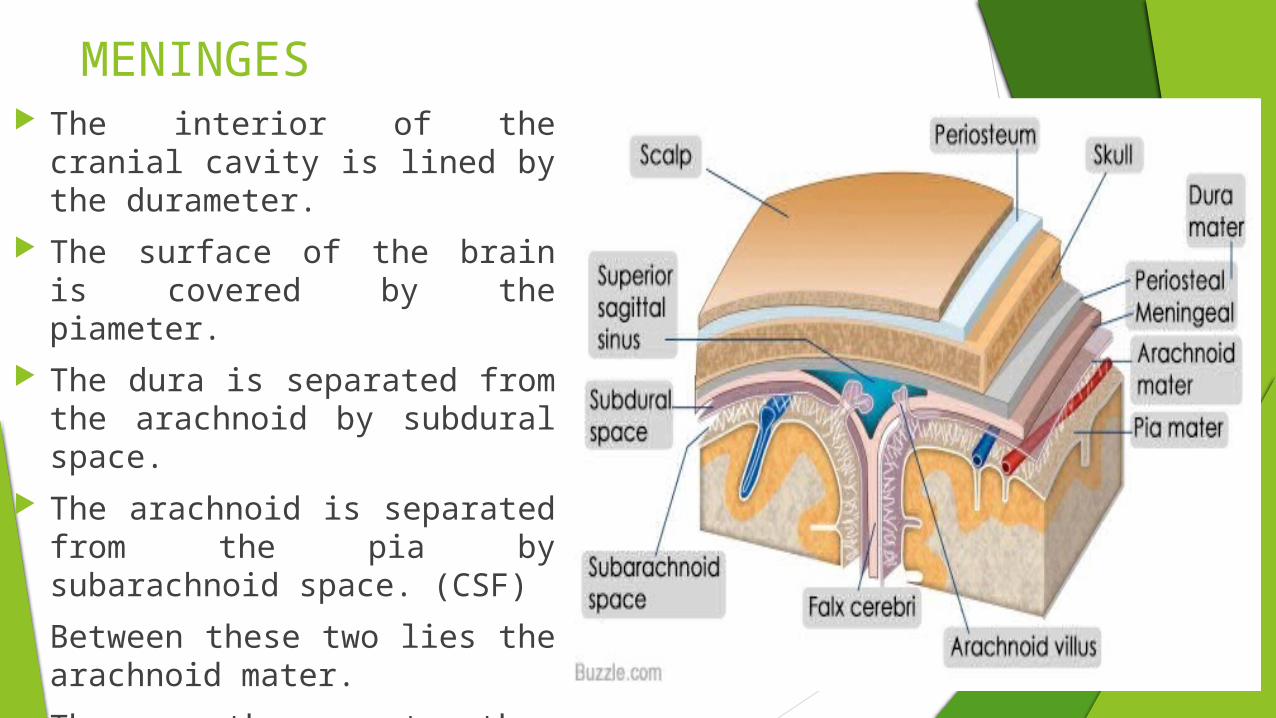
MENINGES The interior of the cranial
cavity is lined by the durameter.
The surface of the brain is covered by the piameter.
The dura is separated from the arachnoid by subdural space.
The arachnoid is separated from the pia by subarachnoid space. (CSF)
Between these two lies the arachnoid mater.
These three together constitute the meninges of the brain.
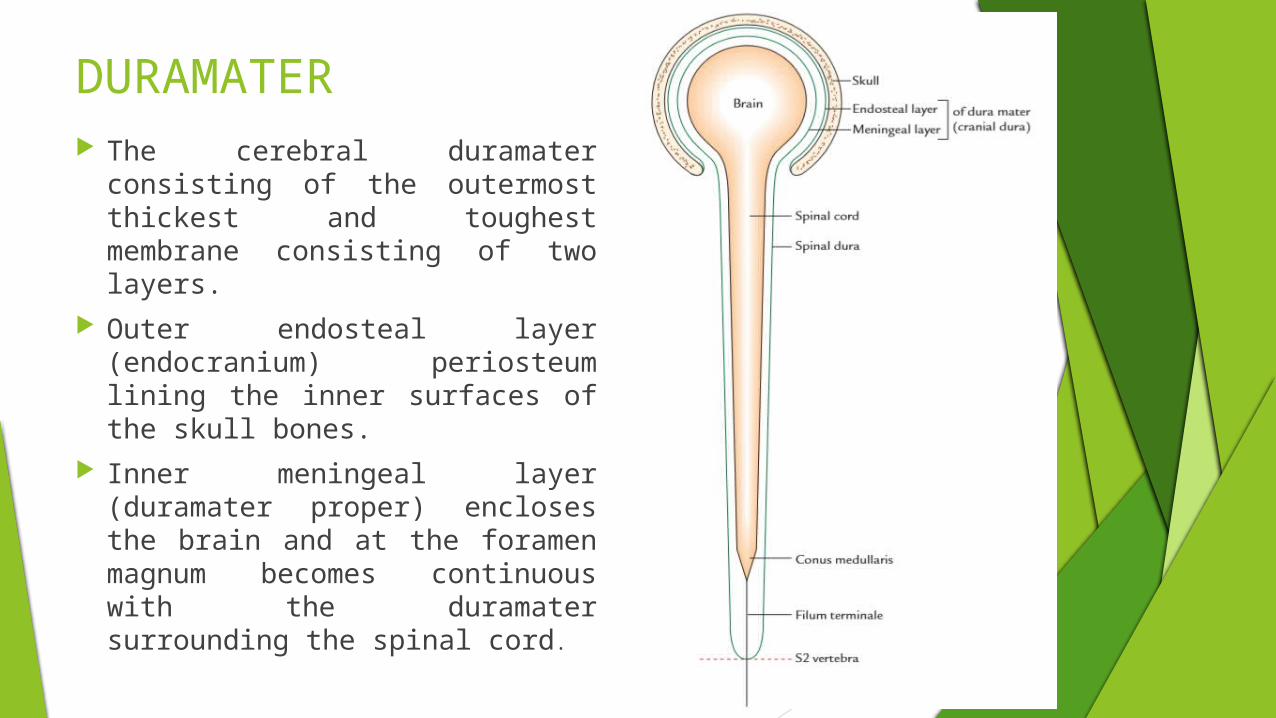
DURAMATER The cerebral duramater
consisting of the outermost thickest and toughest membrane consisting of two layers.
Outer endosteal layer (endocranium) periosteum lining the inner surfaces of the skull bones.
Inner meningeal layer (duramater proper) encloses the brain and at the foramen magnum becomes continuous with the duramater surrounding the spinal cord.
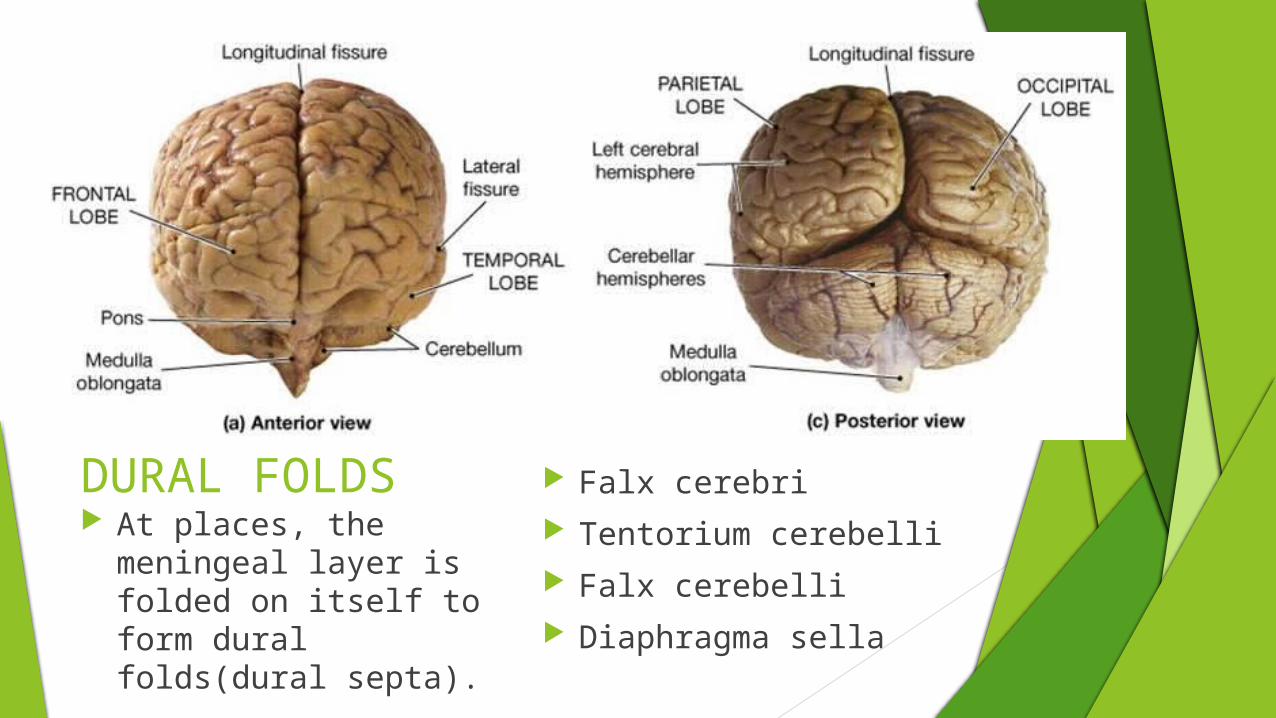
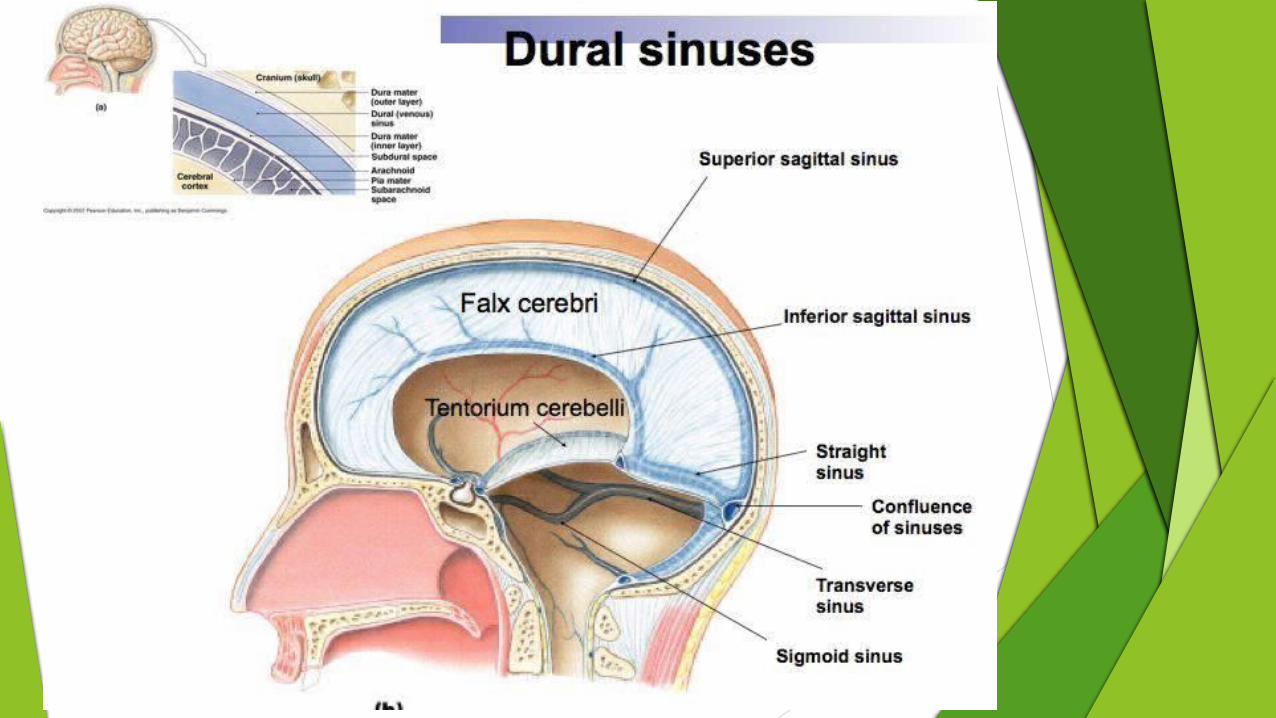
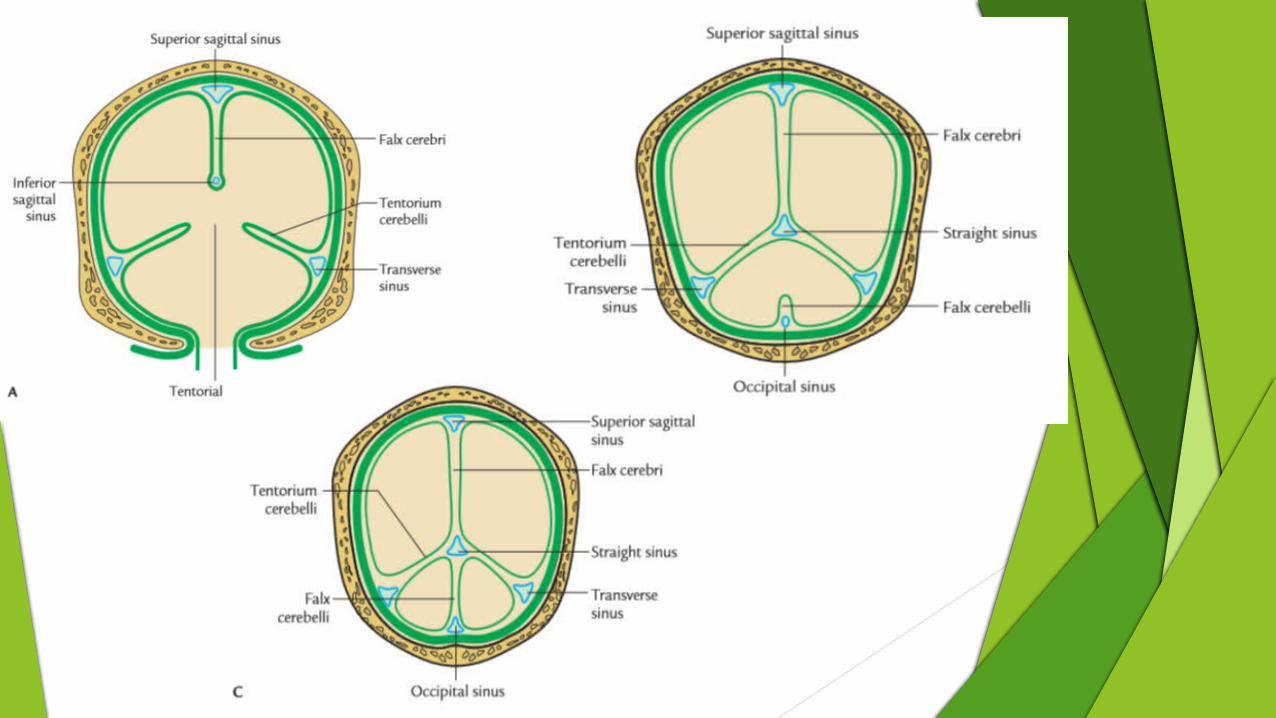
DURAL FOLDS At places, the
meningeal layer is folded on itself to form dural folds(dural septa).
Falx cerebri Tentorium cerebelli Falx cerebelli Diaphragma sella
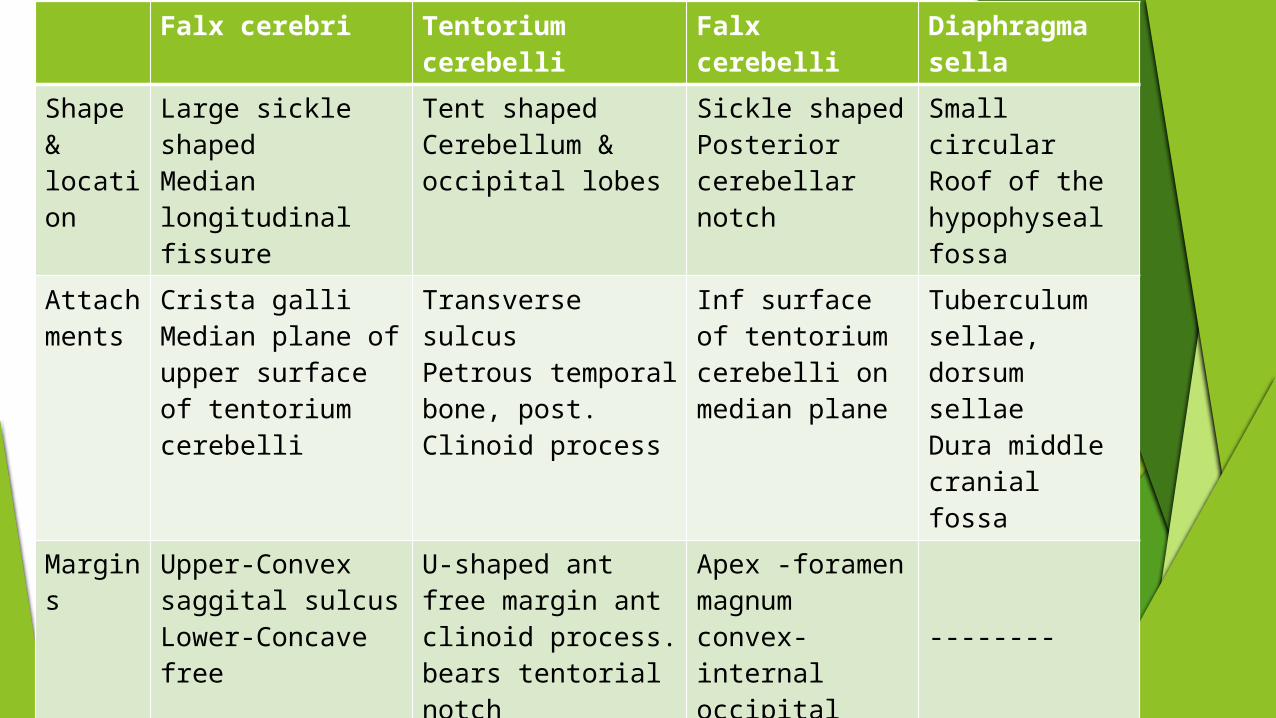
Falx cerebri Tentorium cerebelli
Falx cerebelli Diaphragma sella
Shape & location
Large sickle shapedMedian longitudinal fissure
Tent shapedCerebellum & occipital lobes
Sickle shapedPosterior cerebellar notch
Small circularRoof of the hypophyseal fossa
Attachments
Crista galliMedian plane of upper surface of tentorium cerebelli
Transverse sulcusPetrous temporal bone, post. Clinoid process
Inf surface of tentorium cerebelli on median plane
Tuberculum sellae, dorsum sellae Dura middle cranial fossa
Margins
Upper-Convex saggital sulcusLower-Concave free
U-shaped ant free margin ant clinoid process. bears tentorial notch
Apex -foramen magnumconvex-internal occipital crest
--------
Surface
Medial surface of cerebral hemisphere
Superiorly –occipital lobe of cerebrum inferiorly-superior cerebellum
------- hypophysis cerebri
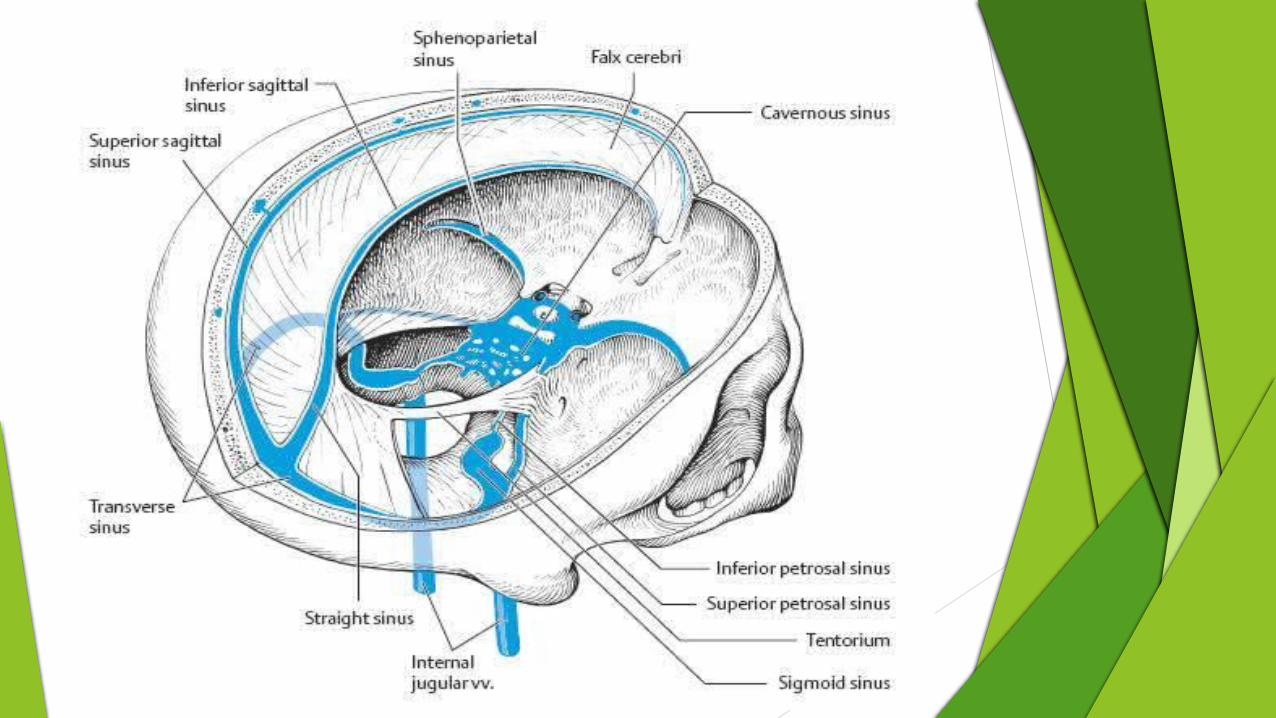
Sinus Superior & inferior saggitalStraight sinus
TransverseSuperior petrosal
Occippital ---------
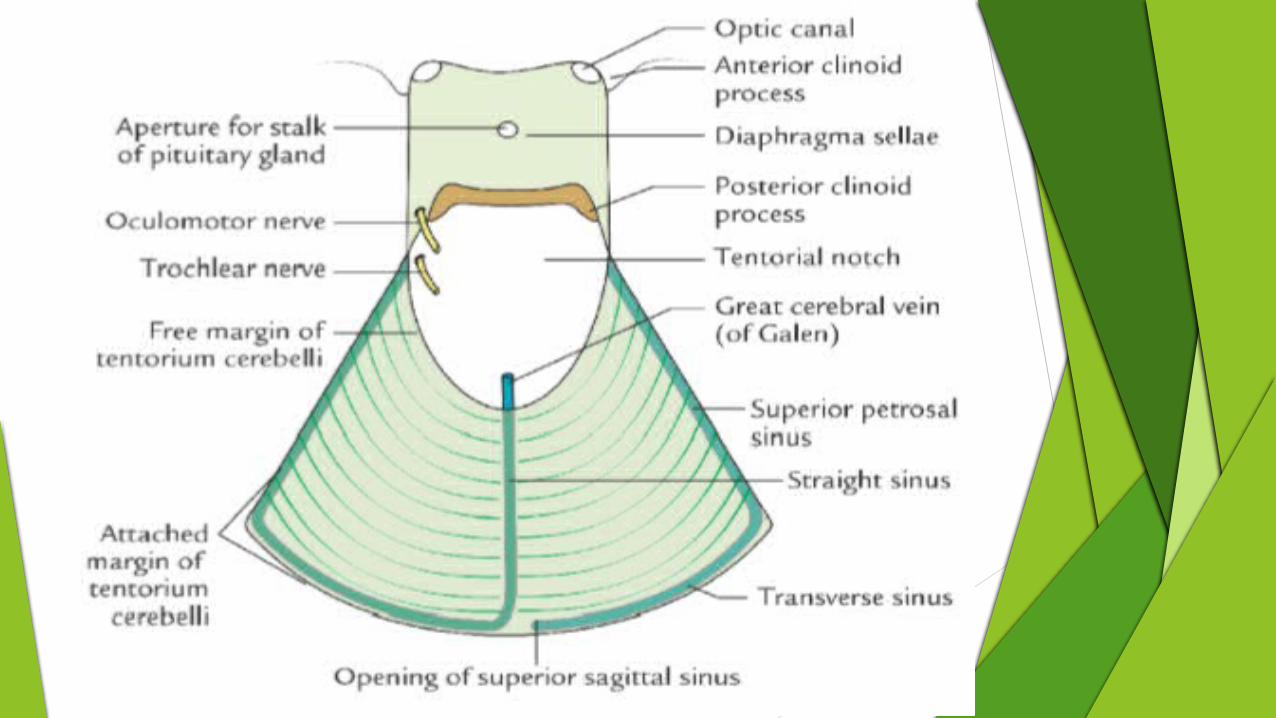

TRIGEMINAL OR MECKEL’S CAVE It is a recess of the dura
mater present in relation to the attached outer margin of the tentorium cerebelli
It is formed by the evagination of the meningeal layer of duramater by two roots of the trigeminal nerve below the superior petrosal sinus over the trigeminal impression on the anterior surface of the petrous temporal bone near its apex
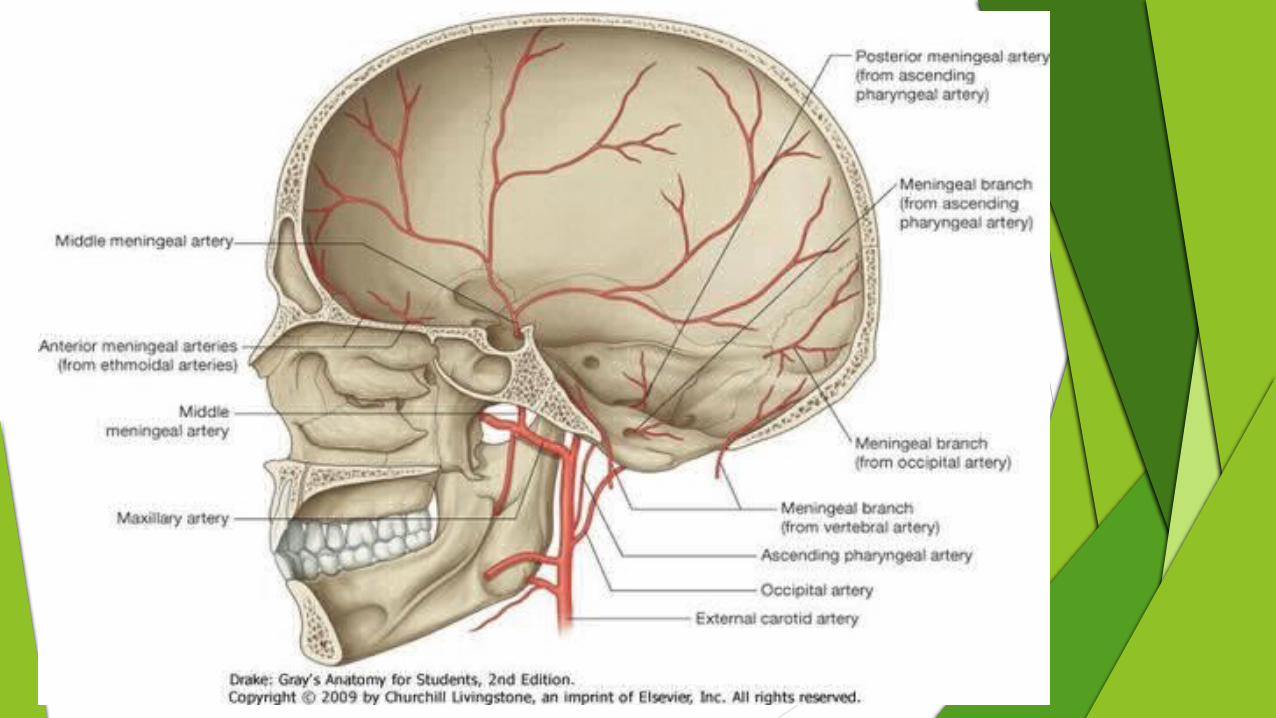
BLOOD SUPPLY OF DURA
The vault- supplied by middle meningeal artery
The anterior cranial fossa and the dural lining- supplied by anterior ethmoidal, posterior ethmoidal and ophthalmic arteries
The middle cranial fossa- supplied by middle meningeal arteries, accessory meningeal and internal carotid arteries, and meningeal branches of ascending pharyngeal artery.
The posterior cranial fossa- supplied by meningeal branches of vertebral, occipital and ascending pharyngeal arteries

NERVE SUPPLY OF DURA The dura of the vault is supplied by sensory nerves
derived from ophthalmic division of trigeminal nerve The dura of the floor has rich nerve supply and is
sensitive to pain:
- anterior cranial fossa- supplied by anterior ethmoidal nerve and partly by maxillary nerve
- middle cranial fossa- supplied by maxillary nerve in the anterior part and by branches of mandibular nerve and from the trigeminal ganglion in the posterior part
- posterior cranial fossa- supplied by recurrent branches of 1st, 2nd and 3rd cervical spinal nerves and by meningeal branches of 9th and 10th cranial nerves

CLINICAL ANATOMY EXTRA DURAL AND SUBDURAL HAEMORRHAGES Common Distinguished by Extradural Haemorrhage is arterial (injury to middle
meningeal artery) Subdural Haemorrhage- venous Extradural Haemorrhage - symptoms of cerebral
compression are late Extradural Haemorrhage- paralysis appears first in
the face and then spreads to lower parts of the body. Subdural Haemorrhage - haphazard
Extradural Haemorrhage- no blood in the CSF. - Subdural Haemorrhage- it is a common feature.

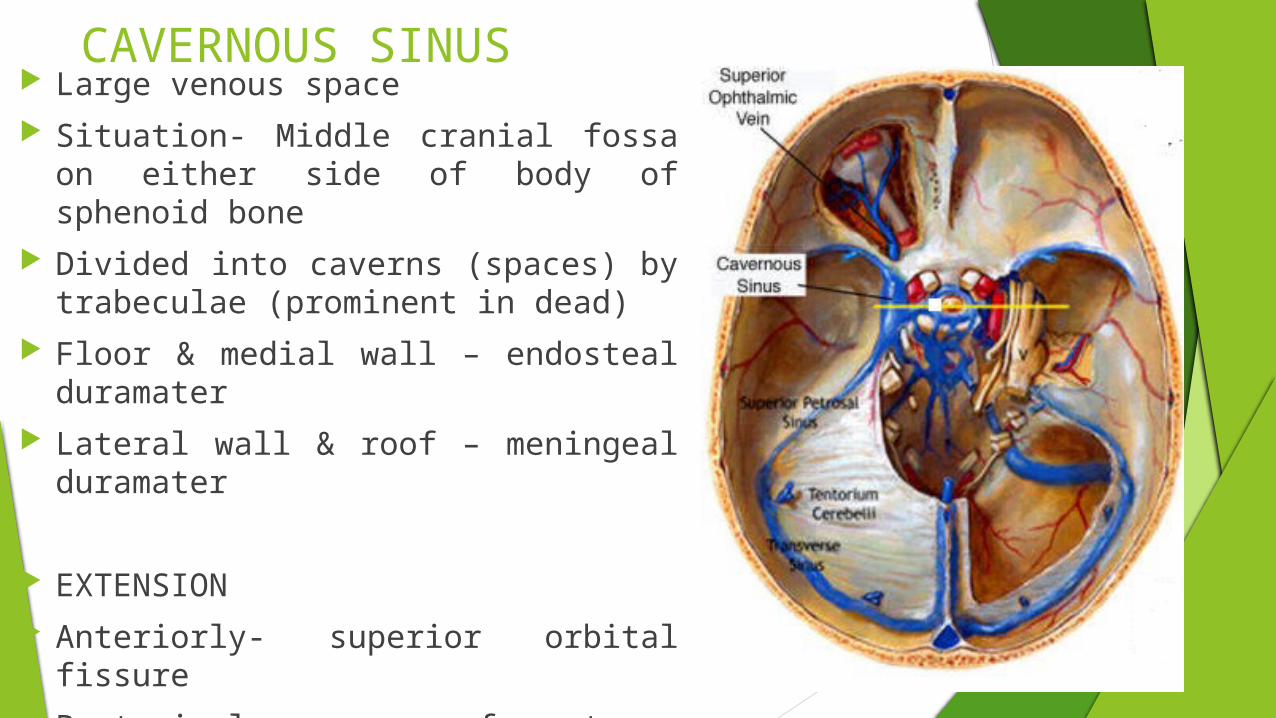
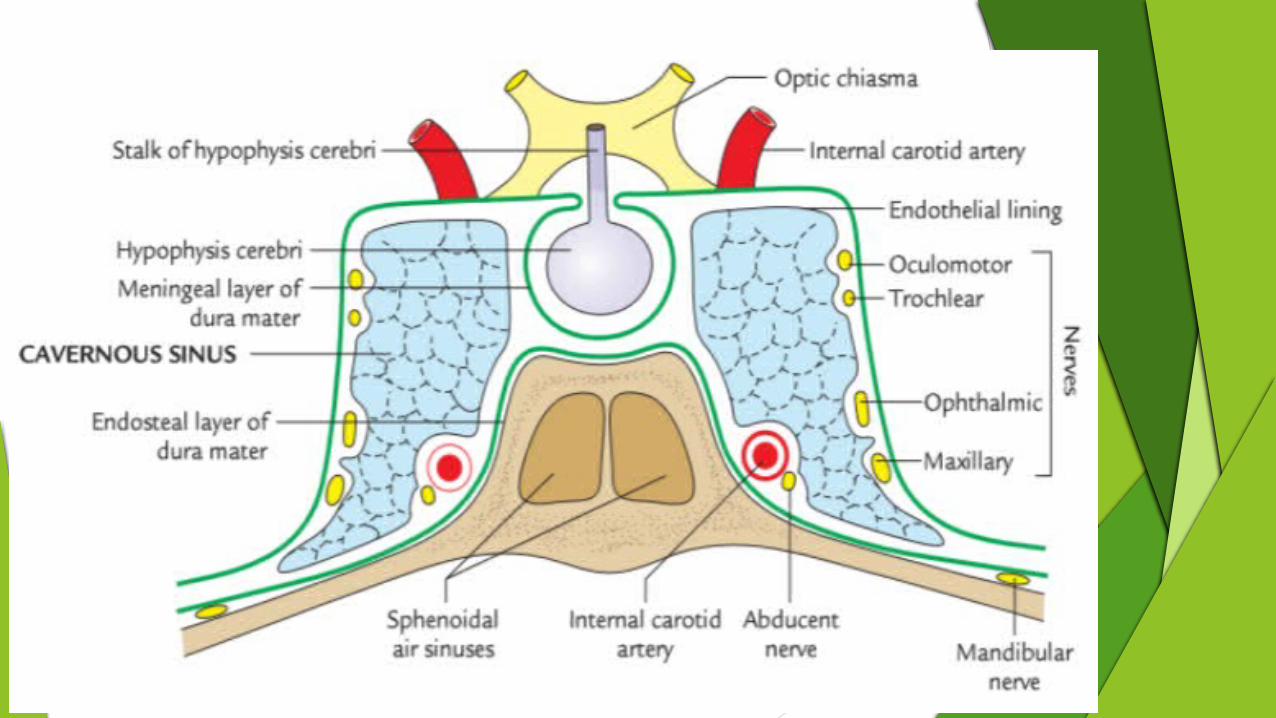
CAVERNOUS SINUS Large venous space Situation- Middle cranial fossa on
either side of body of sphenoid bone Divided into caverns (spaces) by
trabeculae (prominent in dead) Floor & medial wall – endosteal
duramater Lateral wall & roof – meningeal
duramater
EXTENSION Anteriorly- superior orbital fissure Posteriorly- apex of petrous temporal
bone 2cm long, 1cm wide
RELATIONS SUPERIORLY
Optic chiasma Optic tract Olfactory tract Internal carotid artery INFERIORLY Foramen lacerum Junction of the body and the
greater wing of sphenoid MEDIALLY Hypophysis cerebri Sphenoidal air sinus
LATERALLY Temporal lobe with
uncus BELOW LATERALLY Mandibular nerve ANTERIORLY Superior orbital fissure Apex of the orbit POSTERIORLY Apex of the petrous
temporal bone Crus cerebri of mid
brain
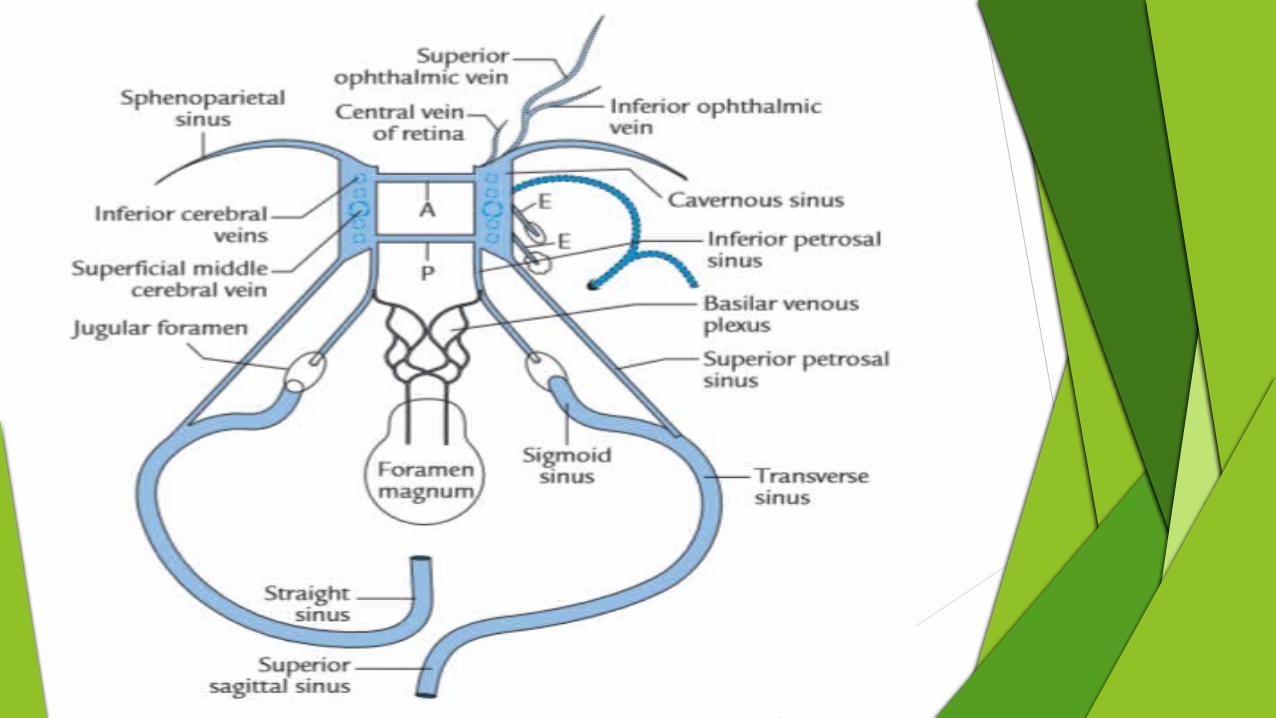
TRIBUTARIESFROM THE ORBIT Superior ophthalmic vein Inferior ophthalmic vein Central vein of retina
FROM THE BRAIN Superficial middle cerebral
vein Inferior cerebral vein
FROM THE MENINGES Sphenoparietal sinus Frontal trunk of middle
meningeal vein
STRUCTURES PASSING THROUGH
LATERAL WALL Occulomotor Trochlear Ophthalmic maxillary
MEDIAL WALL Internal carotid artery Abducent nerve
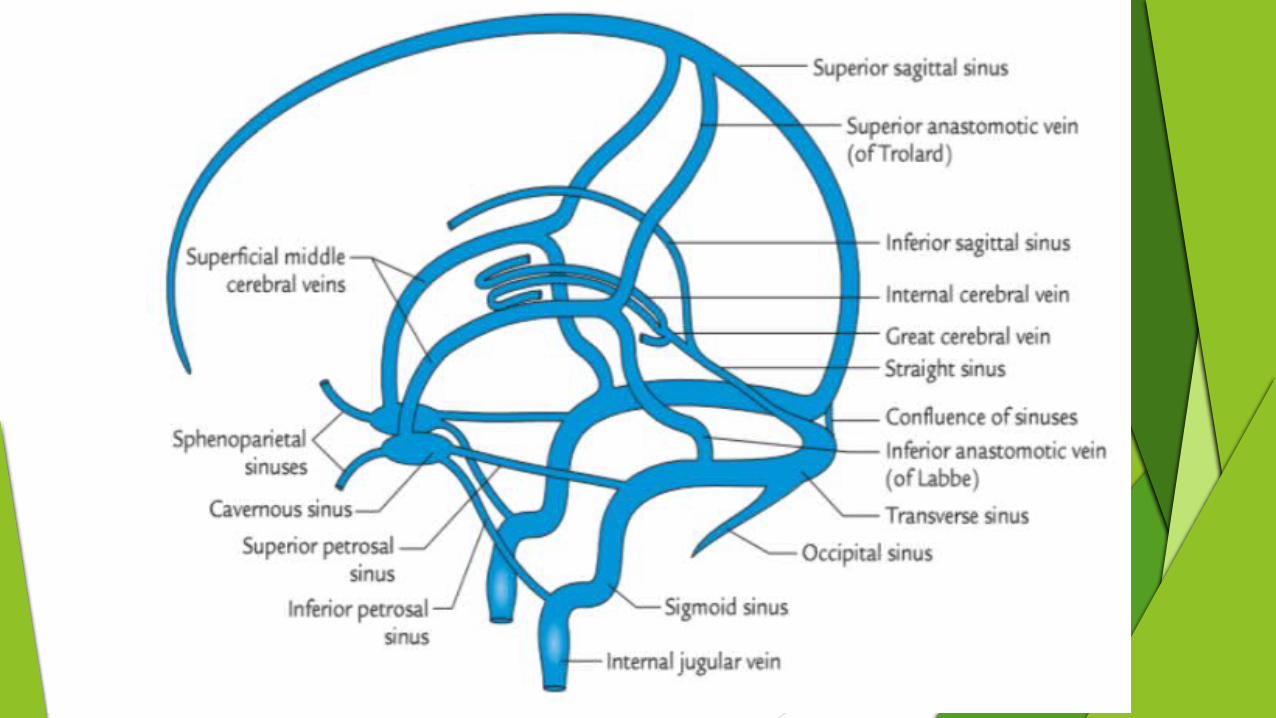
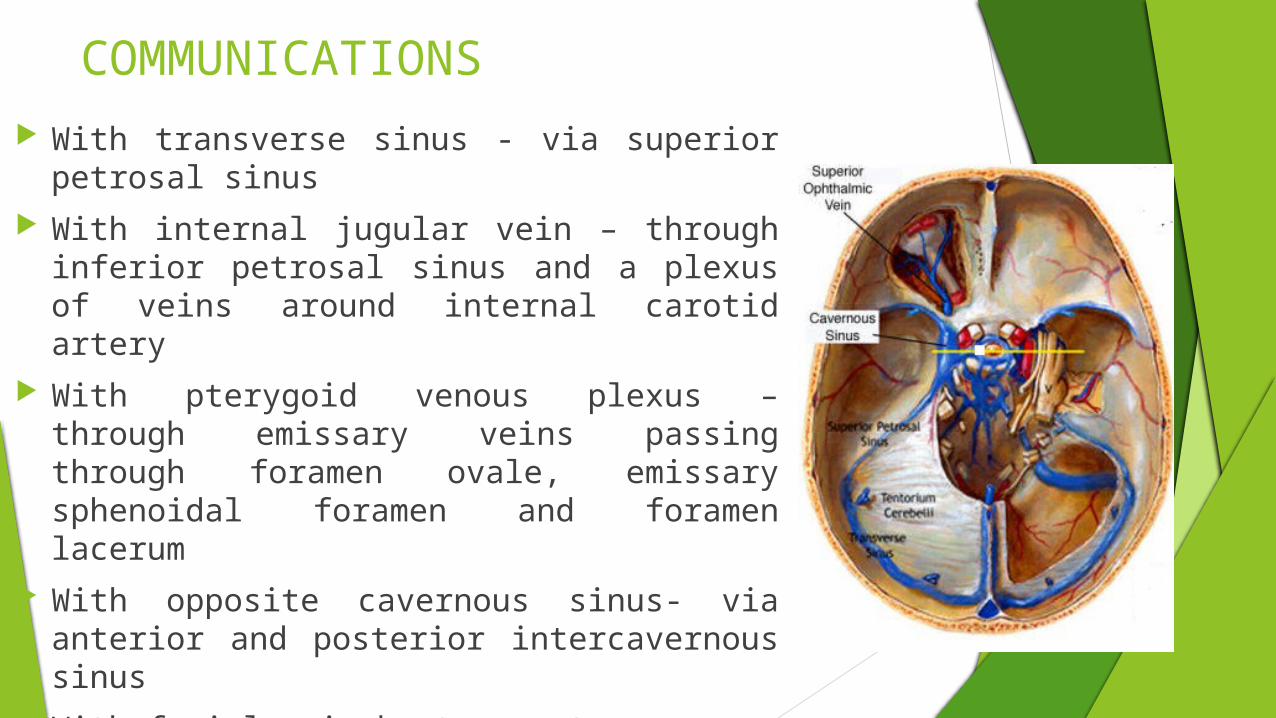
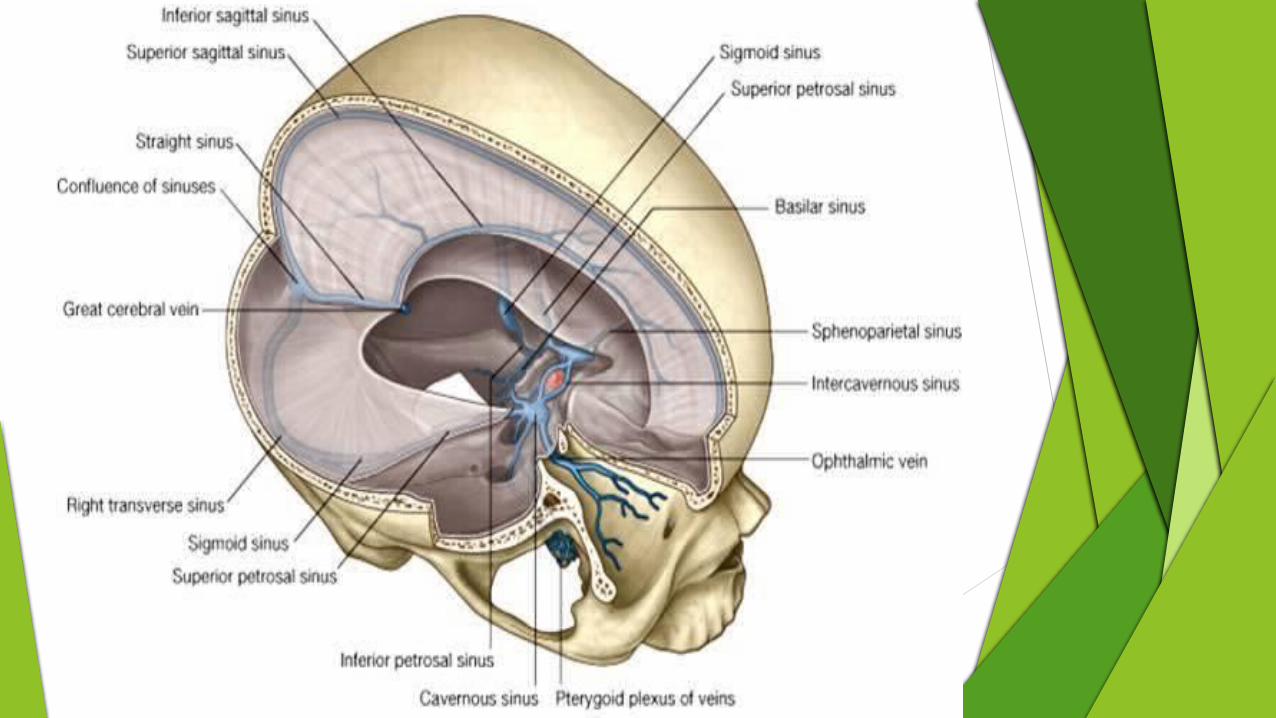
COMMUNICATIONS With transverse sinus - via superior petrosal
sinus With internal jugular vein – through inferior
petrosal sinus and a plexus of veins around internal carotid artery
With pterygoid venous plexus – through emissary veins passing through foramen ovale, emissary sphenoidal foramen and foramen lacerum
With opposite cavernous sinus- via anterior and posterior intercavernous sinus
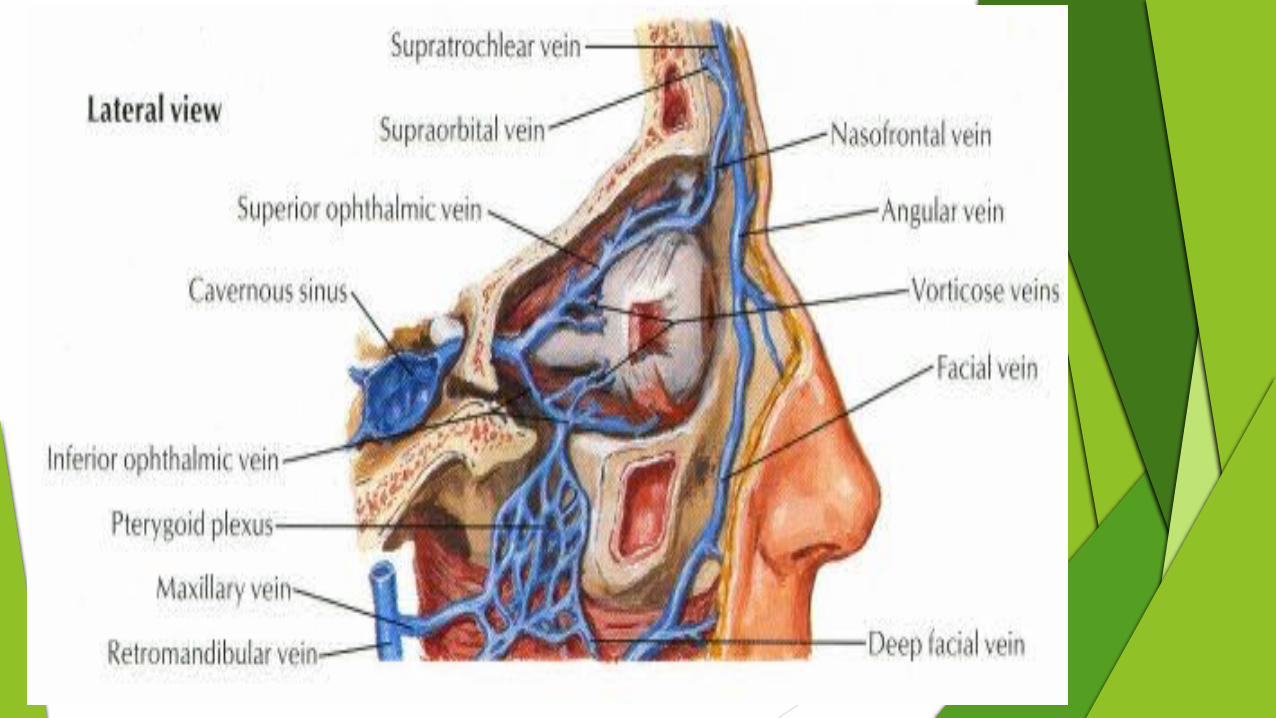
With facial vein by two routes-
- Superior ophthalmic vein and angular vein
- Pterygoid venous plexus and deep facial vein
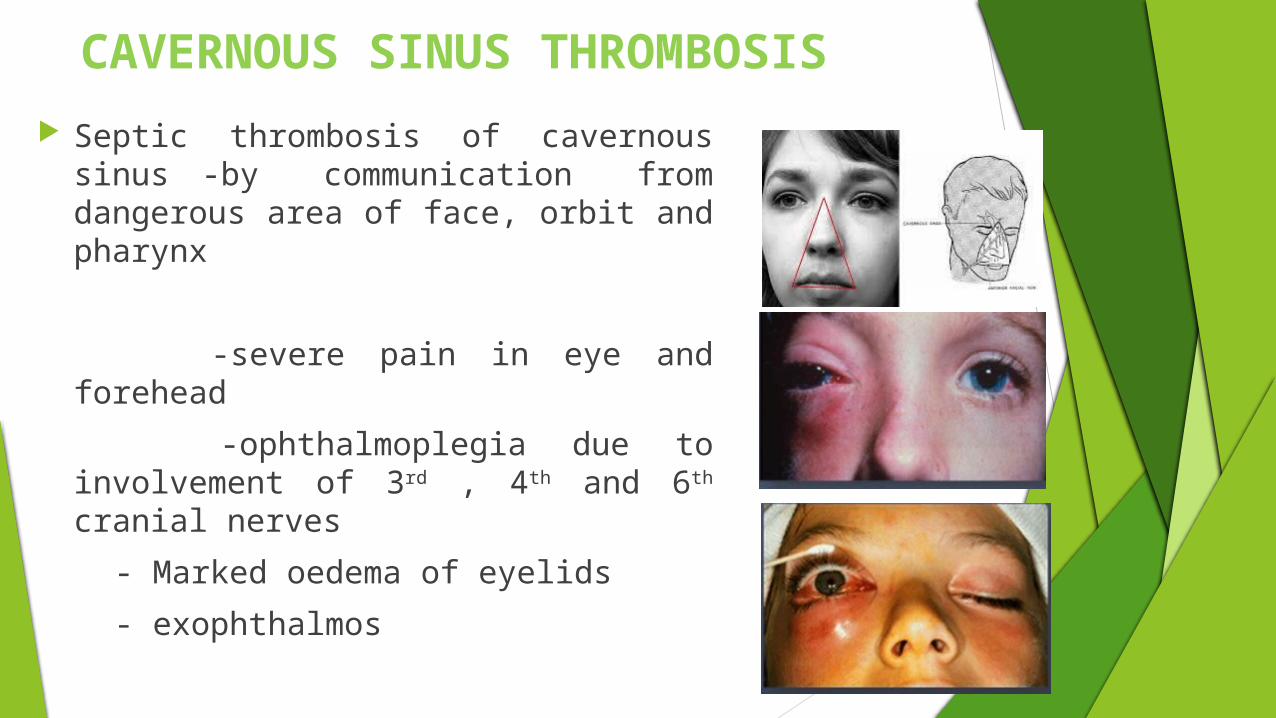
CAVERNOUS SINUS THROMBOSIS
Septic thrombosis of cavernous sinus -by communication from dangerous area of face, orbit and pharynx
-severe pain in eye and forehead
-ophthalmoplegia due to involvement of 3rd , 4th and 6th cranial nerves
- Marked oedema of eyelids
- exophthalmos
PULSATING EXOPHTHALMOS
Pulsating exophthalmos- internal carotid artery is ruptured as a result of fracture of base of skull – arterio- venous communication is established
- ligation of inernal carotid artery may be helpful, but patient may develop contralateral hemiplegia