e-cigarettes. legislating the conflicting interests among consumers, tobacco companies, tax...
TRANSCRIPT

Utrecht School of Economics
June 26th, 2014
“E-cigarettes: Legislating the conflicting interests among
consumers, tobacco companies, tax authorities and public health”
Tatiana Degtyareva (3755479)
Lisaima Luijten (3869202)
Supervisor: Luigi Pinna
Group supervisor: Erwin van Sas

2
Contents
Introduction ............................................................................................................................................................. 3
1. Market for tobacco .............................................................................................................................................. 4
“Big Tobacco”: Mayor Global Companies .................................................................................................... 5
Tobacco farmers: EU & US ........................................................................................................................... 6
Consumers ...................................................................................................................................................... 7
Government: Local governments, supranational EU and the US ................................................................... 8
Pharmaceutical industry ................................................................................................................................. 8
1.1 Interdependency between involved parties ................................................................................................... 9
2. Market failures .................................................................................................................................................. 11
Monopolistic (oligopoly) Power ................................................................................................................... 11
Asymmetric information .............................................................................................................................. 12
Negative externalities ................................................................................................................................... 13
“Financial” externalities ............................................................................................................................... 13
“Health” externalities ................................................................................................................................... 15
2.1 Solutions from theoretical frameworks: Coase & Hobbes .......................................................................... 17
The Coase theorem ....................................................................................................................................... 17
The Normative Coase and Hobbes theorems................................................................................................ 18
2.2 Role of taxation........................................................................................................................................... 19
3. Market for e-cigarettes ...................................................................................................................................... 21
3.1 Product and its features ............................................................................................................................... 21
3.2 Comparison with tobacco cigarettes ........................................................................................................... 22
3.3 Competition with tobacco ........................................................................................................................... 24
3.4 Regulation ................................................................................................................................................... 25
European regulation ..................................................................................................................................... 26
USA regulation ............................................................................................................................................. 27
4. “Cutting” the tobacco market – No smoke without fire .................................................................................... 29
4.1 Statistics on smoking .................................................................................................................................. 29
4.2 Conflict of Interests .................................................................................................................................... 30
4.3 Consequences of new regulations ............................................................................................................... 32
4.4 Potential complications ............................................................................................................................... 34
5. Conclusion ........................................................................................................................................................ 36
Recommendations ........................................................................................................................................ 38
Bibliography ......................................................................................................................................................... 39
Appendix A ........................................................................................................................................................... 45
Appendix B ........................................................................................................................................................... 46
Appendix C ........................................................................................................................................................... 48
Appendix D ........................................................................................................................................................... 50

3
Introduction
Originated in China, electronic cigarettes found their way to the European and American
markets in 2006 and 2007, respectively. But only recently, May 2014, has the European
Union effectuated a new Tobacco Product Directive that concerns regulation of tobacco
related products including e-cigarettes. This will imply new conditions such as constraints on
advertisement, product differentiation, adoption of regulatory rules on e-cigarettes and ban on
flavoured cigarettes. The EU claims to impose this regulation in order to protect public health
throughout the whole Union. But a question arises: why does the EU want to treat e-cigarettes
as another tobacco product that contains no tobacco, and which studies suggest is safer than
normal cigarettes (Cahn & Siegel, 2011). Therefore, our research question is whether the
motivations to regulate e-cigarettes are more concerned with public health issues or the
protection of various private interests.
In order to guide us toward answering this question, we have to define the involved
parties and their interests, whether tobacco and e-cigarettes stand in direct competition, and if
there is enough evidence to treat them equally. We also need to touch upon such issues as
taxation of both products, smoking rates among minors, externalities associated with the
tobacco industry, consequences and potential problems that may arise after the regulation is in
place.
To answer these questions, we will incorporate the qualitative research methods,
which we will do by means of analysis of statistics, documents, professional/academic
opinions and legislative acts. All drawn conclusions are supported by most recently available
research and anecdotal evidence.
In the light of the attention drawn to the topic by the media and regulatory authorities,
this paper provides a discussion relevant to various interest groups. We plan to provide one
with enough information on the existing debate around the problem and invite readers for a
further debate. This paper may also be useful for the legislative authorities faced with the
need for regulation of electronic cigarettes, as we provide our recommendations in the end of
the paper.
It is important to mention that there are certain limitations to our research, some of
which concern the biasness of the available data, as available research was often conducted
and/or funded by interested parties. Therefore, our paper takes a critical approach toward the
available data used throughout the research.

4
We start our research by outlying the involved parties along with their interest in
Section 1. Next, we address the problem of market failures on the market for ‘smoking’,
followed by the discussion on taxation. Section 3 concerns electronic cigarettes, their features
and place in the market. In Section 4 we present a critical analysis of available statistical data
and discuss the consequences of the recent regulations. The final section of the paper answers
the main question, provides drawn conclusions and several recommendations. Furthermore, at
the end of the paper we have provided four Appendices with illustrative material in order to
introduce readers to the products discussed throughout the paper, and extracts from relevant
literature.
1. Market for tobacco
As the tobacco industry is characterised by complex relations, Figure 1 below is provided to
better display the interdependency of the involved parties. First, each of the involved parties
will be discussed separately followed by an analysis of their relation.
Figure 1: Relation Diagram

5
“Big Tobacco”: Major Global Companies
Historically, the “Big Tobacco” refers to the three major tobacco corporations in the US. Here
we are to include the other global players of the industry. Here “Big Tobacco” is used as a
collective name for the biggest and most influential tobacco companies worldwide, who
consolidated themselves in five major private companies through privatization and mergers.
The big five consists of Philip Morris International, Altria/Philip Morris USA, Japan Tobacco
International, British American Tobacco, and Imperial Tobacco. However, apart from these
five private companies, there are sixteen state-owned tobacco companies that are leading
cigarette manufacturers in specific countries, which we do not include. Nevertheless, the
China National Tobacco Corporation, which produced 2.1 trillion of the 5.9 trillion cigarettes
produced worldwide in 2008, more than any other tobacco company in the world is also
included under our definition of the “Big Tobacco” (Eriksen, Mackay & Ross, 2013).
The current share of approximately 1.1 billion smokers worldwide is expected to grow
to 1.64 billion by the year 2025, mainly due to population growth. The ones to reap the
benefits from this increase will surely be the top 6 tobacco companies that together control
81% of the world tobacco market. The state-owned China National Tobacco Corporation
controls 37.1% of world’s tobacco market and has $91.7 billion annual revenue and $16
billion annual profits. Philip Morris International controls 17.4% of the global tobacco market
share and enjoys $67.7 billion annual revenue with $7.5 billion annual profits. Following
Philip Morris International is British American Tobacco, which currently holds 12.0% global
market share, has annual revenue of $58.1 billion and annual profits sum to $4.2 billion. Japan
Tobacco International has 9.6% of global market share, has $65.9 billion annual revenue and
$1.5 billion annual profits (Rehn, 2014).
Despite almost identical annual revenue as Philip Morris International, Japan Tobacco
International’s profits are just a fraction of Philip Morris’ due to the harsher regulatory
conditions in the markets they serve. The fifth largest tobacco company by market share and
world’s largest producer of rolling paper, cigars and fine-cut tobacco is Imperial Tobacco. In
2000 they dominated 0.8% of the world market but nowadays enjoy a market share of 4.9%
due to aggressive acquisitions. It has annual revenue of $38.4 billion and $2 billion annual
profits. Philip Morris U.S.A. was re-branded as 'Altria Group, Inc.'. The company controls
2.8% of global market share, $24.4 billion annual revenue and $3.9 billion in annual profits.
Philip Morris International changed strategy in 2008 to evade taxes on U.S. operations, and
now manages all overseas markets instead of the Altria Group, Inc. (Rehn, 2014).
6
Tobacco farmers: EU & US
Governments in both the European Union and the United States have always been heavily
involved with the tobacco farmers.
The main tobacco growing countries in the EU are Greece, Italy, Spain, France and
Portugal, with Greece and Italy taking up 75% of the Unions total production. Tobacco is the
most heavily subsidised crop per hectare in Europe, which creates distorted incentives and
high-levels of inefficiency (Ross, 2004).
Through the Common Agriculture Policy (CAP), approximately € 1 billion was spent
on subsidies for tobacco farmers each year throughout the EU. Only an average of € 2 million
was spent on smoking prevention programs (McKee et al., 2004).
Subsidies being heavily criticized throughout the Union, the EU has opted for a reform
of the CAP in 2001. The reform imposed that from 2001 till 2010, there will be a so called
“phasing-out” of tobacco subsidies where farmers will get fewer subsidies, and by 2010 direct
payments to these farmers would be abolished completely. Reasons for this were to depress
the supply of tobacco. The Commission justified this “phasing-out” period by referring to its
obligation under the TEC treaty to ensure a high level of health protection (Häge, 2012).
Although direct payments have been shaped to be granted only to help farmers adapt
to the temporary loss of income due to the changing demand within the market, in some cases,
like in 2007-2008, direct payments have been granted to certain farmers that would not be
justified under the reformed CAP (Burny, 2010). Furthermore, Greece is still receiving
subsidies under the 2003 CAP reform and EU farmers are still heavily subsidized through
other means of indirect subsidies. Bulgarian farmers get a one euro subsidy for every kilo of
tobacco sold whereas Greece receives a four euros per kilo subsidy (Thorpe, 2013).
In the US, as early as 1938, the Agricultural Adjustment Act regulated tobacco
farmers. Farmers were issued marketing quotas regulating supply by limiting the amount of
tobacco grown. In exchange, farmers were guaranteed a price for their product above the cost
of production. The production and location restrictions prevented growers from achieving
economies of scale and scope (Agricultural Marketing Resource Center, 2012).
In 2004, The Fair and Equitable Tobacco Reform Act (P.L. 108-357), also called the
"tobacco buy-out" or simply “TTPP” came into force. This new act helps farmers through a
system of subsidies to compete in the free market as all the quotas, location and advertisement
restrictions have been abolished. This act promised to make payments to tobacco farmers

7
from 2005 till 2014 and summing a total of approximately $10 billion (United States
department of Agriculture, 2013).
Apart from subsidies, the US government also supports tobacco farmers through the
indirect ‘Federal Crop Insurance Programme’. Private insurance companies provide the
insurance with the Federal Government subsidizing a portion of the premiums and some of
the companies’ cost related to insuring the farmers (United States Department of Agriculture,
2014).
Recently, the TTPP was heavily debated in the US and farmers were not sure if they
would receive their 2014 payment. The Obama administration was planning to only pay a
portion of the promised amount but the administration reversed its decision and payments will
be paid according to the 2004 TTPP agreements (14News, 2014, Jan 17).
Consumers
There are more than 4,000 chemicals in tobacco smoke, of which at least 250 are known to be
harmful and more than 50 are known to cause cancer. The Tobacco Atlas reports that in 2009,
the top 5 cigarette consuming countries were China, Russia, the US, Indonesia and Japan,
respectively (Eriksen, Mackay & Ross, 2013). Figure 2 presents world cigarette consumption.
Figure 2: World Cigarette Consumption
(Source: Eriksen, Mackay & Ross, 2013)
According to the World Health Organization [WHO] (2014), smoking kills more than
6 million people annually worldwide. Furthermore, statistics show that approximately 80% of
the smokers worldwide live in low- and middle-income countries. Due to poverty and harsh
economic circumstances, children are often employed on tobacco farms in these low-income

8
countries to provide an income for their families. They are especially vulnerable to "green
tobacco sickness", which is caused by the absorption of nicotine through the skin due to
contact with wet tobacco leaves (WHO, 2014).
Since it is only (relatively) recently that people became aware of the consequences of
smoking, and the lag between initial consumption of tobacco and visible signs of illnesses, the
tobacco related diseases and death causes by smoking are a fairly new phenomenon. In the
20th
century, tobacco caused 100 million deaths and that amount is expected to rise to 1
billion in the 21st century (WHO, 2014).
In Appendix A some health complications that come along with smoking are presented,
and apart from these, the overall health of the smoker is diminished.
Government: Local governments, supranational EU and the US
As research increasingly shows that smoking causes negative health effects, governments and
international organizations are increasingly involved in containing this deathly addiction from
spreading. Local governments are introducing smoking bans in a number of US states, the
European Union recently introduced a new Tobacco Product directive that would be effective
in all member states and the US is also working towards nationwide implementation of
smoking and advertisement bans with respect to cigarettes and other tobacco products.
In this paper ‘Government’ is collectively referred to the local government present in
each state in the US, the US government, governments in each member state of the EU and
the supranational decision maker, the European Union. Moreover, we include the legislative
bodies of both countries.
The Government is not only involved with regulation but also with taxation and
exchange of information with the consumers and tobacco companies to best inform, educate
and regulate the market.
Pharmaceutical industry
Throughout this paper ‘Pharmaceutical Industry’ refers to the producers, such as Pfizer and
GlaxoSmithKline, of Nicotine Replacement Therapy (NRT). The illustrative provisions for
the products can be found in the Appendix C.
The Food and Drug Administration (FDA) in the US has approved 5 types of NRT
products: patch, gum, nasal spray, inhalers and lozenges. The patches are like a plaster
(adhesive bandage), which delivers a nicotine dose through the skin. Some side effects,

9
depending on the duration and dose of the nicotine may be skin irritation, racing heartbeat and
headache (American Cancer Society, 2014).
The nicotine gum is a ‘fast-acting’ form of substitution for tobacco cigarettes in which
nicotine is absorbed through the mouth by chewing on it like a gum. Possible side effects may
be throat irritation, racing heartbeat and stomach discomfort. The nasal spray is sprayed in the
nose and nicotine is absorbed through the bloodstream. Possible side effects may be nasal
irritation, throat irritation and a danger of addiction (American Cancer Society, 2014).
The nicotine inhaler is a plastic tube with a nicotine cartridge inside. It resembles the
look of a cigarette and by inhaling; nicotine is delivered to the bloodstream. “Nicotine
inhalers are the FDA-approved nicotine replacement method that’s most like smoking a
cigarette” (American Cancer Society, 2014).
Possible side effects are upset stomach and mouth and/or throat irritation. This form
of NRT carries an additional risk to small children and pets as the used cartridges nevertheless
carry enough nicotine in them to cause harm if it gets on skin or mucous membranes.
Nicotine-containing lozenges are much like the nicotine gum and are supposed to be sucked
on until it is fully dissolved. Side effects such as nausea, heartburn and headache could arise.
Some of these products are obtained over the counter and for others; a doctor’s prescription is
needed (American Cancer Society, 2014).
A cohort study by the Harvard University and University of Massachusetts conducted
by Alpert, Connolly & Biener question the effectiveness of NRT products. They concluded
that these products are not effective in helping people stop smoking in the long run, even with
or without professional counselling. Although clinical studies show their effectiveness, real
life usage suggests otherwise (Alpert, Connolly & Biener, 2013).
1.1 Interdependency between involved parties
Before analysing the Tobacco Industry any further, it is necessary to explain the relation
between the involved parties. In Figure 1, a comprehensive scheme is presented with the
major players that are relevant to our research and their underlying dependencies and
interaction.
The Big Tobacco has a supply/demand relation with consumers and exchange
information through scientific research and findings, product information and advertisement.
Big Tobacco can be considered an oligopoly as the top 6 players control more than 80% of
worldwide market share. This makes the market very important for consumers who demand
their addictive product from the Big Tobacco and, in turn, consumers are the top priority for

10
these companies to secure their high profits. However, connection with the government is
somewhat more complex.
Big Tobacco is linked to local governments and supranational unions such as the
European Union through regulations, taxation systems and a subsidy system for tobacco
farmers. Throughout the decades, the Big Tobacco has been heavily involved in lobbying of
local governments and international organizations. Bero (2003) provides a vast amount of
examples where the Tobacco industry was involved in monetary payments to politicians in
order to influence decision making, lobbying activities with respect to local governments,
international organizations such as the WTO, United Nation and the World Bank and their
attempts to influence policy makers and their lobbying activities with the pharmaceutical
industry.
The pharmaceutical industry is the one to supply nicotine replacement therapy (NRT)
to smokers who want to quit smoking. Document analysis of leaked files done by Bero (2003)
shows that the Big Tobacco has well-hidden financial ties with the pharmaceutical companies
that promoted both collaboration and competition. “Financial ties between tobacco companies
and the chemical, pharmaceutical, and food industries gave the tobacco companies leverage to
influence policies that could affect these other industries” (p. 272). For example, the tobacco
industry has used its financial ties with pharmaceutical companies to pressure them to weaken
their marketing of nicotine replacement therapies (Bero, 2003, p. 272).
The pharmaceutical industry, in turn, stands in direct demand/supply relation with
consumers for NRT products. The industry’s relation with the government is that of taxation,
regulation and lobbying activities as described in Bero (2003). In the EU, the industry is
controlled by marketing authorisation, clinical trials, competition law and intellectual property
rights, trade, post-authorisation safety and advertisement laws (Efpia, 2014). This is much the
same in the US and is controlled by the Food and Drug Administration (FDA).
As can be observed from Figure 1, the relation between government and consumer is a
very important one. Firstly, they exchange information on products, conducted research &
findings, advertisement, public education of the consumer, etc. Second, they are linked
through the taxation system as consumers pay for cigarette consumption and raise tax revenue
for the government. Finally, the maintenance of the public health rests on the responsibility of
the Government.
With such blatant conflicts of interest, it is not at all surprising that the parties are
lining up to have an input on any impending legislation.

11
2. Market failures
As it is discussed in the context of the welfare economics, there are situations when markets
fail to allocate resources efficiently – and give rise to market failures. There are two main
reasons for market failures – market power and nonexistence of markets (Rosen & Gayer,
2010). In the market for tobacco presence of market power serves as a main reason for the rise
of market failures, of which several will be discussed further on.
In economics, demerit goods are goods that have a negative effect on, not only the
consumer, but others as well. It is perceived to be harmful and socially undesirable throughout
society (a more extensive economic discussion of demerit goods is provided in Section 2.1,
with a graphic representation in Figure 6). Some still consume them as not everyone
discounts risks equally and just like alcohol and drugs, tobacco products are considered to be
demerit goods and society would like to see their demand and supply being decreased.
Monopolistic (oligopoly) Power
Monopoly is defined as a single supplier. While pure monopoly is rare, monopoly power is
much more common and can exist even when there is more than one supplier. Markets with
only two suppliers are called duopoly; and with few firms − an oligopoly.
Monopoly is associated with entry barriers, such as predatory and limits pricing, high
set up costs, vertical integration, large-scale economies and others. Moreover, there are costs
associated with monopoly power, such as limited choice, high prices, restricted output, lower
consumer surplus, excess rents, asymmetric information, productive inefficiency, allocative
inefficiency and net welfare loss (Motta, 2004). Those associated with tobacco industry are
discussed below.
The tobacco market is very similar to the one characterised by oligopoly, as mentioned
previously, 80% of the market is under control of six players (Rhen, 2014). Due to the high
concentration of tobacco industry and addictive nature of tobacco, tobacco producers have
significant monopoly powers. An example of this was “Operation Berkshire”, where the
companies Philip Morris, R.J. Reynolds, British American Tobacco, Rothmans, Reemtsma,
and U.K. tobacco companies Gallagher and Imperia formed an international conspiracy block
in 1977 with the goal of creating controversy about the health effects of smoking (Bero, 2003,
p. 273-274).
The non-competitiveness of the industry can be seen from the increase in prices that
usually exceeds the tax increase, as under monopoly, price exceeds costs. Furthermore,

12
cigarette companies were known to distribute free cigarettes at colleges in the past, as well as
significantly lowering the price of cigarettes in order to attract more addicted consumers. On
the contrary, around 1980s, when more information about the health hazards became available
to the public, the demand for cigarettes has dropped while prices increased, which
characterises one of the features associated with the monopoly power, namely, asymmetric
information (Becker, Grossman & Murphy, 1994).
Furthermore, since the Big Tobacco “enjoys” its power, in order to make profit, the
price charged is above the competitive level and definitely above the costs, which creates the
net efficiency loss – the deadweight loss. Size of the deadweight loss depends on the elasticity
of demand. Since demand for tobacco is relatively inelastic, due to addictive nature of the
product, the deadweight loss increases, as the monopolist is able to charge a higher price; this
is known as the allocative inefficiency. Next, there is a productive inefficiency as the cost of
performing is higher under monopoly rather than under the competition, as monopolists tends
to use less efficient technology and is reluctant to innovate. This inefficiency creates
additional welfare loss (Motta, 2004).
Asymmetric information
A key market failure of the industry is that of asymmetric information, where the Big
Tobacco is better informed than the other parties (consumers & government) involved in the
transaction. “Studies show that few people understand the specific health risks of tobacco use.
For example, a 2009 survey in China revealed that only 38% of smokers knew that smoking
causes coronary heart disease and only 27% knew that it causes stroke” (WHO, 2013).
Jha et al. (2000) mention that there are two main reasons for information asymmetry to
arise in the tobacco industry. First, the industry has deliberately hid information from the
Government and consumers with respect to the true addictive nature of the product.
Consumers have also been purposefully misguided as these companies refrained from giving
information on the severe health effects of smoking despite their internal knowledge on the
matter. The industry also used advertisement to convince the public that certain variation of
cigarettes – light /mild – are “safer” than others while they knew that this was not the case.
This problem goes even further as Jha et al. (2000) and Bero (2003) discuss the fact
that tobacco companies have persuaded journalist to refrain from reporting on the health
implications of smoking, intense lobbying in international health organisations and even
funded biased scientific research to misguide consumers and governments. They would also

13
fund unrelated scientific research to mislead authorities from their activities and research. All
this would be done through industry lawyers, offshore partners and other third parties.
The second reason mentioned by Jha et al. (2000) is the fact that there is a lag (delay)
between consumption and signs from illness since the start of smoking. Since consumers
gather information from their peers and passed experiences, a good risk assessment is
hindered by the fact that the health implications only arise a few decades later. This fact is
also the reason why it is only recently that scientific researchers are able to give supported
evidence of the true malicious consequences of smoking.
Negative externalities
The second market failure is externality. By externality is meant a benefit or cost that “occurs
when the activity of one entity directly affects the welfare of another in a way that is outside
the market mechanism” (Rosen & Gayer, 2010, p. 47). Externalities concerning tobacco come
both from the producer as well as from the use of cigarettes and these are to be subdivided in
the financial and health externalities.
“Financial” externalities
In this category, we first considered the increased chance for fires due to cigarette
consumption. In 2011, the U.S. fire departments responded to an estimated 90,000 ‘cigarette
consumption caused’ fires. These resulted in an estimated 540 civilian deaths, 1,640 civilian
injuries and $621 million in direct property damage. Most of these deaths were caused by
fires that initiated in bedrooms (40%) or in living rooms, family rooms or dens (35%). The
other 72,400 ‘cigarette consumption caused’ fires were predominantly outdoor fires (Hall,
2013). In London, ‘cigarette consumption caused’ fires are the second most common cause of
fires at home and result in more deaths than any other type of fire (London Fire Brigade,
2014).
The reason for this section to be placed under externality is the fact that these
‘cigarette consumption caused’ fires could not only harm the smoker and its property but
others as well. In Hall (2013) is showed that between 2007 and 2011, only 4% of ‘cigarette
consumption caused’ fires were intentional and only 1% of associated deaths occurred in
intentional fires. Also, only 1% of home ‘cigarette consumption caused’ fires involved
someone playing with the smoking material. Furthermore, studies found that 24% of fatal
victims were not the smoker whose cigarette started the fire. From these victims, 34% were
children of the smokers, 25% were neighbours or friends of the smokers, 14% were spouses

14
or partners of the smokers, 13% were parents of the smokers and 14% had other relationships.
Secondly, the lost opportunity cost ought to be considered. Tobacco farmers could be
growing other −maybe nutritious− crops instead of tobacco plants. This will not only benefit
them and their family as they eliminate the chance of getting "green tobacco sickness", but the
population at large by increasing availability of nutritious crops. Also, the land and resources
could be put to better use.
Apart from lost opportunity costs from farmers, negative externalities around the work
place should be considered. Employees who smoke impose a significant monetary burden on
their employer and the economy as a whole. In Berman, Crane, Seiber & Munur (2013) is
found that employers face an estimated total annual excess cost of approximately $5,816 for
each employee who smokes. They found the relation between smoking and absenteeism to
cost an estimated $516 annually per smoker as employees miss on working days.
Another cost to the employer is the reduced productivity due to nicotine addiction
because of the employees lost work time due to smoking breaks. This was found to amount to
an average of 8 to 30 minutes per day per smoking employee. “Productivity loss due to
smoking breaks is by far the largest single cost that a private employer incurs from a smoking
employee. Fortunately, it is a cost that can be completely eliminated by smoking cessation”
(Berman, Crane, Seiber & Munur, 2013, p. 3).
The forth, negative “financial” externality is the increase of health care costs. Berman,
Crane, Seiber & Munur (2013) state that smoking employees lead to excess healthcare
expenses. An employer with no smoking employees is likely to obtain a discount in insurance
premiums due to the fact that its labour force is likely to have lower overall healthcare costs.
Respectively, insurance premiums are likely to be higher for employers when there are more
smokers in their labour force. This not only represents a cost to employers, but also for the
community at large as smokers can influence the cost of health care at large.
In Jha, Musgrove, Chaloupka & Yurekli (2000) is discussed that 6 to 15% of total
healthcare costs are attributed to smoking in high-income countries. In most low- and middle-
income countries, the annual costs of healthcare attributable to smoking are lower. “To the
extent that taxes, co-payments, or social insurance premiums are not differentially higher for
smokers, the higher medical costs attributable to smokers will be at least partly borne by non-
smokers” (Jha, Musgrove, Chaloupka & Yurekli, 2000, p. 160).

15
“Health” externalities
Smoking not only causes health complications for the individual smoker, but also makes way
for heath externalities to arise. With “health” externalities we refer to the physical burden
placed on the non-smokers through second-hand smoking.
Second-hand smoke is a combination of ‘sidestream’ smoke from the burning tip of a
cigarette, cigar, or pipe, and ‘mainstream’ smoke, which smokers exhale. The Western Pacific
region had the highest rate of second-hand smoke exposure in the world, with over 50% of
men, women, and children being exposed to second-hand smoke in the year 2004. From
Figure 3 is to be seen that in 2004, Europe had the highest percentage of death attributable to
second-hand smoke.
Figure 3: Global Share of Death due to Secondhand smoke
(Source: Eriksen, Mackay & Ross, 2013)
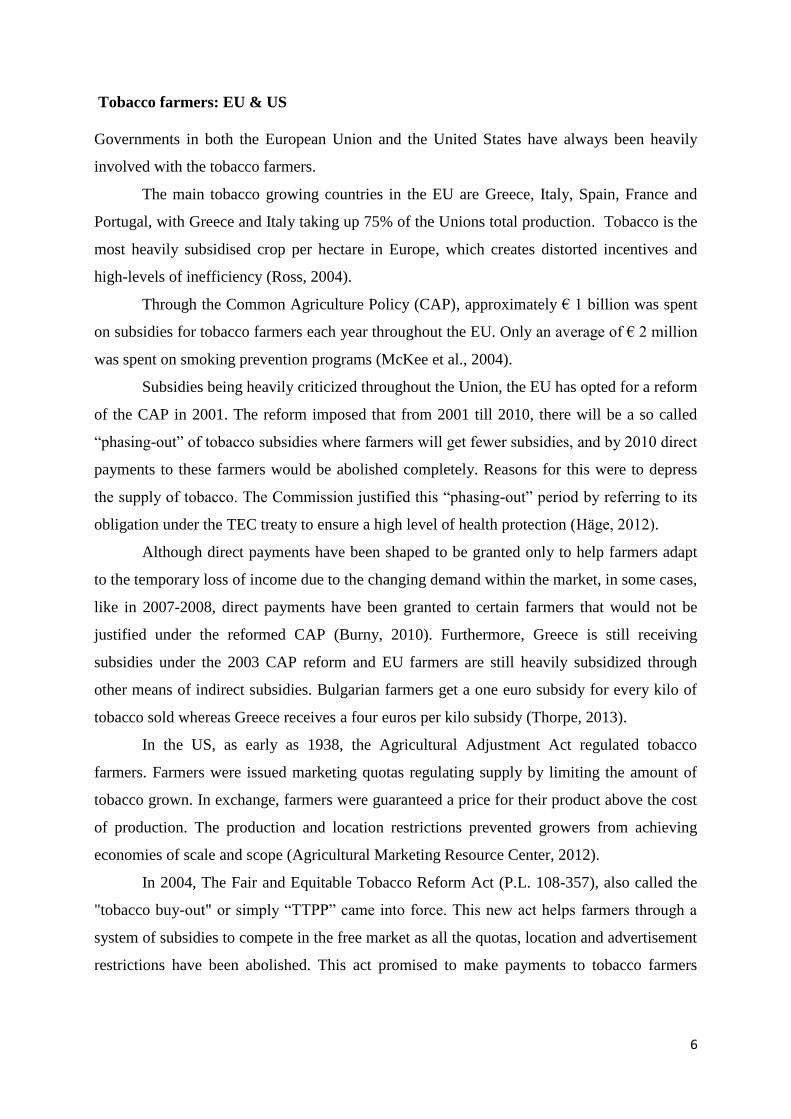
Inhaling second-hand smoke causes immediate harm to the cardiovascular and
respiratory systems. Long-term contact to second-hand smoke can also cause lung cancer.
Pregnant women, fetuses, and infants exposed to second-hand smoke are particularly at high
risk for negative health externalities as can be seen from Figure 4 (Eriksen, Mackay & Ross,
2013).
16
Figure 4: Health Externalities in Children & Adults
(Source: Eriksen, Mackay & Ross, 2013)
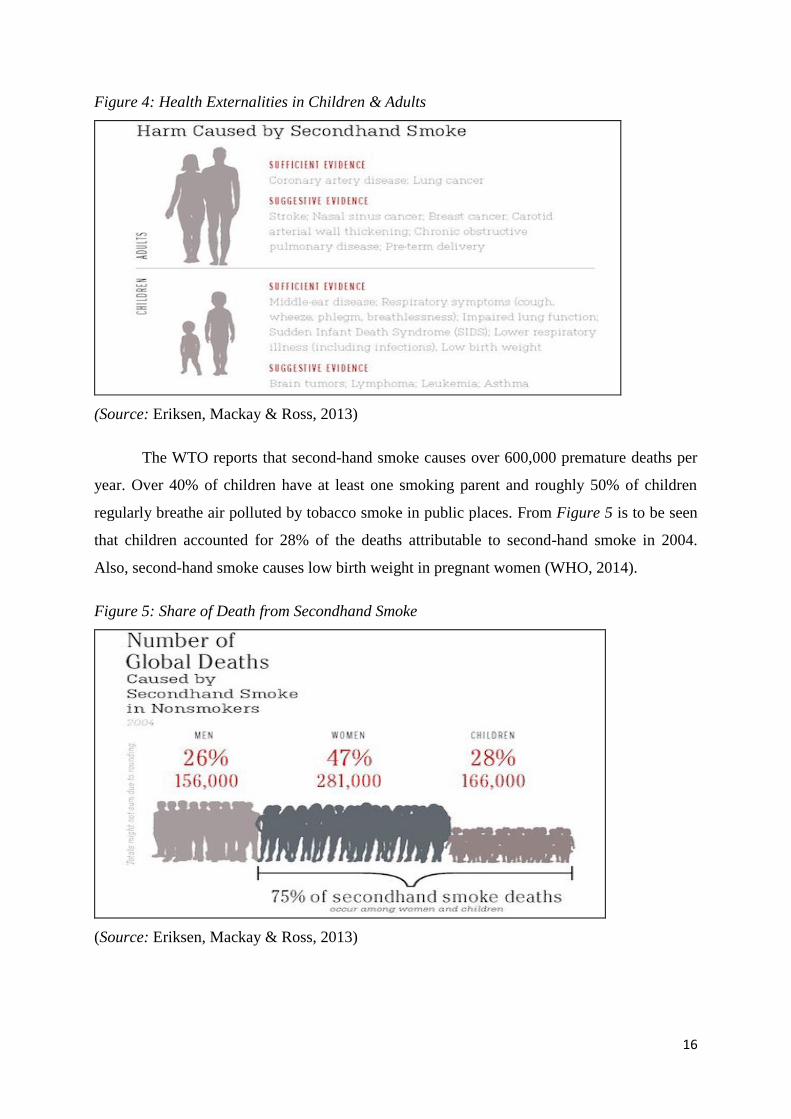
The WTO reports that second-hand smoke causes over 600,000 premature deaths per
year. Over 40% of children have at least one smoking parent and roughly 50% of children
regularly breathe air polluted by tobacco smoke in public places. From Figure 5 is to be seen
that children accounted for 28% of the deaths attributable to second-hand smoke in 2004.
Also, second-hand smoke causes low birth weight in pregnant women (WHO, 2014).
Figure 5: Share of Death from Secondhand Smoke
(Source: Eriksen, Mackay & Ross, 2013)

17
2.1 Solutions from theoretical frameworks: Coase & Hobbes
The Coase theorem
Economic theory states that in the presence of externalities, inefficiencies may rise in the
market. Economists have come up with several responses to this problem. First of all, the
Coase theorem concerning bargaining that leads to efficient allocation of resources could be
used to analyse the restraints present in order to efficiently deal and solve the externalities
arising from smoking. The theory originally deals with disputes on property matters but can
be bent to include other matters.
In Coase (1960) is said that when transaction costs are zero and rights are well defined
and tradable, an efficient use of resources could results from bargaining, regardless of the
legal assignment of property rights. In light of this paper, efficient use of resources could be
the efficient use of land, public healthcare, ‘productive’ labour force, other resources used or
destroyed by the production of tobacco products or the act of smoking or any costs imposed
on the non-smoker by the smoker. Rights stand here to mean the right to ‘clean air’. Also,
externalities arising from smoking are a public, rather than a private matter as it influences
society at large.
One can see the obvious hurdles in trying to apply these equilibrium conditions to the
subject of smoking. In order to even reach an efficient equilibrium, the involved parties
should be able to bargain with one and other. In the case of smokers, non-smokers and the big
Tobacco, this would be virtually impossible as it is extremely difficult to bargain with and
between large groups. Secondly, assessing the exact monetary harm or benefit to each party
may prove to be impossible (uncertainty) and effective bargaining is hindered. Thirdly, the
transaction costs would be enormous to rally up the involved parties (search costs), calculate
the costs and benefit of the involved parties (bargaining costs), deciding on the matter and
actually execute (enforcement costs) the bargained ‘solution’. Furthermore, the problem of
asymmetric information that dominates the tobacco industry is one that would hinder effective
bargaining as history portrays the tobacco industry as one not to be trusted. In addition, even
by including the Government as a private player in this dispute would not lead to a smoother
course of the matter, as all participants are large in number and diverse in interest.
Lee (1991) says that it is widely believed that smokers impose costs on society by
imposing disproportionate demands on the health care industry, decreasing the productivity of
the economy with excessive absenteeism, and by imposing tobacco smoke on others.
Furthermore, he argues that ‘Coasian’ conditions that would lead to the optimal

18
internalization of costs are best satisfied in a private setting where personal decisions on
smoking are made, rather than in a political setting where public policy decisions on smoking
are made. We agree with his reasoning that efficiency is often better obtained when disputed
in a private setting, but in light of the difficulties preventing efficient bargaining mentioned
above, we do not think that would be the best solution and the application of the Coase
theorem is of great difficulty, if not, impossible.
The Normative Coase and Hobbes theorems
Since the conditions do not permit for a bargaining approach by the Coase theorem, we
analyse this matter of externalities in light of the Normative Coase and Hobbes theorems.
They solve the problem of externalities by “internalizing” the costs of occurred dispute.
In Cooter and Ulen (2014) we find that when the transaction costs are significant,
initial allocation of rights does matter. From here we can opt for a Normative Coase approach
where the law should be structured so to reduce transaction costs and with this, remove the
barriers to private agreements, or the Normative Hobbes approach, where the law is tailored
to minimize the failures arising in private agreements.
To start with, Lee (1991) points out that in recent years, attitudes toward public
smoking have shifted property rights away from smokers and towards non-smokers. This
means that non-smokers have the right to, let us say ‘clean air’, and it is only through consent
and compensation that the smokers can “buy the non-smoker out” of this right. If the
normative Coase approach is adopted, the law should find gateways to lower the transaction
costs. In the light of the smoking problem, we do not see a way in which the law could
achieve this efficiently giving the nature and scope of the problem. Even if the law achieves
the lowering of transaction costs, the mutual agreement between so many people will prove to
be impossible. If a Normative Hobbes approach is opted for, it will also prove extremely
difficult, if not close to impossible to achieve the lowering of harm caused in private
agreements. The reason for this is the fact that it concerns failure not only in private matters
but the smoking phenomenon harms the world population at large and cannot be left to decide
and bargained with trough private disputes. For these reasons, a different mechanism is opted
for; regulation and taxation by the Government.
In McCormick & Stone (2007) is stated that the 3 out of the 4 main reasons for
government intervention is the presence of externalities, asymmetric information and
vulnerable individuals and demerit goods. This justifies why the regulation of the tobacco
industry cannot be left in the hands of the tobacco market but is regulated by the Government

19
instead. Riley (2012) says that in the case of demerit goods, the free market may fail to take
into account the negative externalities of consumption due to the fact that the social costs
exceed the private costs. In Figure 6 is an illustrational aid provided by Riley (2012) where
the interception point Q3 is depicted as the social optimal level of consumption that takes into
account the information failure of consumers and where the negative externalities are
internalized.
Figure 6: Demerit goods
(Source: Riley, 2012)
2.2 Role of taxation
One important aspect that needs analysis is the taxation of tobacco products and the tax
revenue for governments.
Historically, the tobacco market was mostly in hands of a single firm or controlled by
local governments. Throughout the decades, it shifted to privately owned companies and
currently the industry is dominated by oligopolies (Jha & Chaloupka, 2000). Tax revenue
from the tobacco industry amounts to over € 100 billion annually throughout the European
Union and is one of the main sources of income for governments (Berger, 2013). In the US,
tax revenue summed to over $17 billion in 2012 (Bloomberg, 2012).
The “benefit principle” discussed by Jha & Chaloupka (2000) is to be the principle
where users of a particular government-provided service pay through taxation according to

20
their derived benefit from the particular consumption. With respect to taxes on tobacco
products, this implies that smokers pay for the imposed cost to the government through
private and public health care, imposed negative externalities of smoking on society and other
costs of smoking as discussed in the previous section.
According to Ramsey (1927), efficiency of taxation is when a product that is taxed
would generate a substantial level of revenue, while minimizing the welfare loss related with
the higher prices resulting from the taxes. Furthermore, the ‘Ramsey Rule’ states that the level
of taxes ought to be contrariwise related to the price-elasticity of demand, holding the supply
elasticity constant. This means that goods with relatively inelastic demand −such as tobacco
products, as proven by Jha & Chaloupka (2000) − ought to be taxed more heavily, while
relatively elastic demanded products ought to be taxed less.
As stated by Jha & Chaloupka (2000), the demand for tobacco products is fairly
inelastic in the short term in most countries. Due to the addictive nature of this product, it is
only in the long run that increases in price could affect consumption, making tobacco products
relatively inelastic in the short run. Also, studies from high-income countries show that the
youth and young adults, less educated individuals and those with lower income will be more
reactive to price increases of tobacco products. This means that increase of the tax rate will
lead to a decrease in cigarette smoking but at the same time increase tax revenue substantially.
From 3 to 5% of government revenue in high-income countries has historically been
generated through tobacco taxes and through estimations; the authors have derived that a 10%
increase in taxes would lead to an increase of approximately 7% in cigarette tax revenue. This
means that the “Ramsey Rule” checks positive as tobacco taxes generate high revenues, while
having a moderately small impact on social welfare.
The literature on externalities prescribes that individuals ought to internalize the costs
they impose on others by their actions. Pigou (1962) suggested that taxation could be an
optimal mechanism to improve economic efficiency in the presence of negative externalities.
This being said, it would seem logical to tax a product, only proportionate to its imposed
damage to society, and use these tax revenues to limit or otherwise try to counterbalance the
imposed externality in the best way possible. Although countries use these proceeds to fund
advertising campaigns against smoking, funding of health care, research on health
implications of smoking and other health related activities, they also use tobacco tax revenue
to fund other government activities and as governments have grown to be highly dependent
on these proceeds, they are of high importance for fiscal policies (Jha & Chaloupka, 2000).

21
3. Market for e-cigarettes
Before entering the discussion on the placement of the electronic cigarettes on the market and
the way they should be regulated, it is necessary to understand what electronic cigarettes are
along with their main features. Appendix B provides illustrational examples of existing e-
cigarettes. This section will address the issue of the role of e-cigarettes on the market for
“smoking” and will discuss the existing regulation debate.
3.1 Product and its features
Originated in China, electronic cigarettes found their way to the European and American
markets in 2006 and 2007, respectively. Since then they have gained considerable attention. A
lot of research has been conducted around the product, mainly on acute exposure, nicotine
delivery and consumer response, with little information available on this new, rapidly
developing industry (Noel, Rees & Connolly, 2011).
E-cigarette, also referred to as ‘vapor’ (or ‘vapour’), is a hand-held device that consists
of an atomiser that heats the liquid mixture of nicotine, flavourings and dulitans; the main
block powers the device with a battery and at the end of it there is a cap with a lamp (Jacobs
& Robinson, 2014). Nicotine is being delivered through the battery-powered vaporization of a
nicotine/propylene-glycol solution. Though ‘smoking’ electronic cigarette (called ‘vaping’)
mimics smoking, there is no combustion; therefore the user inhales vapour, not smoke.
Despite the fact that electronic cigarettes deliver nicotine, they contain no tobacco. It is
presupposed that vaping is less harmful than smoking as it does not have various toxicants
unlike tobacco smoke. Additionally, electronic cigarettes not only allow mimicking smoking
but also deliver nicotine, which basically addresses both pharmacologic and behavioural
components of the cigarette addiction (Cahn & Siegel, 2011).
Today e-cigarettes are presented in various sizes, shapes, colours, flavours and price
ranges. Various features, such as design, battery capacity and weight, are being constantly
improved, along with disposability of the device. Moreover, electronic cigarettes are
becoming more and more accessible. E-cigarettes are marketed by small distributors on
internet and in kiosks, rather than by the tobacco industry or pharmaceutical industry. One can
buy e-cigarettes in kiosks and shopping malls, as well as on the internet, where e-cigarettes
were originally marketed.

22
3.2 Comparison with tobacco cigarettes
In their research Cahn & Siegel (2011) examined various studies on the effect of electronic
cigarettes. It was found that from the estimated 10,000–100,000 chemicals in cigarette smoke
about 5,300 have ever been identified. These findings give one more comprehensive
knowledge of the chemical constituents of e-cigarettes compared to tobacco ones. Sixteen
studies have been identified that quite extensively characterize the components contained in
electronic cigarette liquid and vapour using gas chromatography mass spectrometry (GC-MS).
These studies found that the primary components of e-cigarette cartridges are nicotine,
propylene glycol (PG), and glycerine. However, many regulatory agencies focus on potential
health hazards associated with tobacco-specific nitrosamines (TSNAs) and diethylene glycol
(DEG).
TSNAs have been detected in two studies at trace levels. The maximum level of total
TSNAs reported was 8.2 ng/g. This compares with a similar level of 8.0 ng in a nicotine
patch, and it is orders of magnitude lower than TSNA levels in regular cigarettes. However, e-
cigarettes contain only 0.07–0.2 per cent of the TSNAs present in cigarettes, a 500-fold to
1400-fold reduction in concentration.
Reported presence of DEG in one of the eighteen cartridges studied by the US Food
and Drug Administration (FDA) is worrisome, yet none of the other 15 studies found any
DEG. No other chemicals apart from TSNAs and DEG, at levels detected in e-cigarettes, raise
serious health concerns. Despite the limitations of already conducted research, most of the
existing evidence justifies their higher safety compared to the tobacco cigarettes and
comparability in toxicity to conventional nicotine replacement products.
However, one cannot ignore the fact that regulating a product that does not contain
tobacco under the tobacco directive is, if not strange, than suspicious. As previously
explained, there is no evidence in support of harmfulness of the e-cigarettes found, which
proves them to be a much safer “substitute”. So what are the arguments that are being most
frequently used in support of such strict regulation?
Cahn & Siegel (2011) in their research managed to formulate five most common
arguments in support of heavy regulation of tobacco cigarettes. The first argument states that
“promotion of safer alternatives will inhibit smoking cessation/prevention efforts” (p. 24),
meaning that addiction will simply be shifted to a new product, e-cigarettes, and reduced hard
may attract new, non-smoking user.

23
A second argument concerns the combustion, as it is the combustion of tobacco that
produces inherently dangerous exposures. Therefore search for a ‘safer’ cigarette is pointless;
there cannot be a “safer” tobacco as we cannot adequately measure the actual risk.
Another argument refers to the “bad” history of tobacco, when tobacco products
promoted as “safer” were found to be not healthier or even more harmful. Misleading labels,
such as ‘light’ made consumers think that they were being exposed to lower levels of toxic
chemicals. Thus, “alternatives promoted as safer may prove more or equally dangerous,
leading to false or unsupported claims and to the misleading of the public” (Cahn & Siegel,
2011, p. 24).
The fourth argument states that nicotine replacement therapy (NRT) has not been
effective, meaning that harm reduction equals harm maintenance. NRT does not treat one
from the addiction but rather maintains it as it was found to be non-effective. Above all NRT
ensures that Big Tobacco (the large tobacco industry companies) will not lose its customers.
Finally, the fifth argument is based on the distrust to the Big Tobacco based on its
earlier history of provision of safer alternatives. Supporters of this argument say that tobacco
companies, based on their history of lies and deception, simply cannot be trusted to develop
and market a safer tobacco alternative; tobacco harm reduction will necessarily benefit the
tobacco industry regardless of what else might be achieved.
After the brief discussion of these arguments, authors put prospective on the
applicability of them to the electronic cigarettes. First of all, electronic cigarettes could entice
smokers who were not otherwise inclined, to attempt to quit. Cahn & Siegel (2011) find the
use of electronic cigarettes by non-smokers to be a theoretical concern, which has no evidence
that youths or non-smokers are using the product. Therefore, it was concluded that regulations
can address the marketing and sales of e-cigarettes to minors.
Next, as obvious as it may sound, e-cigarettes, such as NRT, are not tobacco products
and do not involve combustion, which refutes the validity of the second argument as related to
the e-cigarettes.
Argument three was found invalid as none of the chemicals present in tobacco smoke,
has been shown to be present in the cartridges or vapour of electronic cigarettes in anything
greater than trace quantities. Moreover, reported the presence of carcinogens is similar to that
in NRT products, which has not been mentioned previously. This creates no doubt that e-
cigarettes are safer.
The fourth argument does not hold, as e-cigarettes were “designed with the express
purpose of replicating the act of smoking, without using tobacco” (Cahn & Siegel, 2011, p.

24
27). Nowadays there are whole online communities of ‘vapers’ who compare different
vapours. No other non-tobacco nicotine product has therefore created such dedication among
its users, “suggesting the rare promise of the electronic cigarette as a smoking cessation tool”
(Cahn & Siegel, 2011, p. 27).
Finally, electronic cigarettes are not tobacco products and are not (yet) produced by
tobacco companies. Rather than being helpful to cigarette makers, electronic cigarettes
compete directly against them. This competition is definitely worth mentioning as electronic
cigarettes are slowly overtaking the market.
3.3 Competition with tobacco
According to Jacobs and Robinson (2014) the tobacco industry “has a poor record with new
products containing the addictive nicotine but not tobacco”. The US maker of Camel
cigarettes pumped $300 million into a smokeless cigarette in the 1980s. Initial reviews were
negative as smokers complained about the taste of burning plastic. A year later the product
was canned. Therefore, sudden growth in popularity of the e-cigarettes took tobacco
multinationals by surprise.
Some analysts predicted e-cigarettes to disrupt the tobacco market and take over the
tobacco sales in the US in less than a decade. Not taking action now might mean no sales
tomorrow; that is why the industry has been forced to meet growing demand. The big four –
Philip Morris International, Imperial Tobacco, Japan Tobacco International and RJ Reynolds
– now have e-cigarettes either on the market or in development. That explains why many
small private companies, which serve as innovation providers, were acquired by tobacco
companies.
It is rather evident that electronic cigarettes are the disruptive innovation on the market
for smoking. They have started as a rather exclusive product that was imperfect, however,
now has gained considerable improvements and is already moving up the market. E-cigarettes
have a real potential to eventually displace tobacco cigarettes.
Finally, Jacobs and Robinson (2014) mention that in advanced economies, e-cigarettes
could cause the salvation of the tobacco industry (although not tobacco farmers). While in
emerging markets cigarette sales are growing, “anti-smoking policies in the developed world
mean that sales have fallen”.
In their turn Farsalinos & Stimson (2014) concluded in their research that consumers
prefer using electronic cigarettes as a guilt-free smoking due to absence of health risks
associated with tobacco smoking. In this context, e-cigarettes are in direct competition with

25
cigarettes, as nicotine in electronic cigarettes is identical to nicotine in tobacco in its
molecular structure. Moreover, most of the e-cigarettes users have been successful in giving
up smoking, which was proved in a recent study in England. Users of e-cigarettes were found
successful at giving up smoking, unlike with different NRT as nicotine patches or gum
(Brown, Beard, Kotz, Michie, & West, 2014).
As one can see, there is enough evidence in support of “guiltiness” of the electronic
cigarettes in the light of harmfulness, as opposed to the regular cigarettes. Not only do they
not contain tobacco, but also help to quit consuming it unlike any of the NRT. Promotion of
electronic cigarettes may leave the Big Tobacco insolvent as there will be no need for NRT,
which mainly consists of tobacco, but most importantly the actual cigarettes. There is a sharp
competitive edge between these two very similar, but at the same time, so different products.
3.4 Regulation
Main obstacle associated with tobacco cigarettes is creation of externalities, which calls for a
proper regulation. However, as previously discussed, second-hand smoking and cancer risks
are non-applicable to the electronic cigarettes. E-cigarettes are a relatively new product that
does not really fit into any of the existing categories. Since electronic cigarettes do contain
nicotine but no tobacco and only recreate the act of smoking, they are neither tobacco
products nor cessation devices. In this light, there are several views on how e-cigarettes
should be regulated. Some want to regulate them as medicines, others to classify them as
tobacco products with all the implied restrictions.
Crucially, regulation of e-cigarettes has an ex post character, as emergence of the
product on the market has far gone. Therefore, to prevent the use of e-cigarettes getting out of
hand, there is an option of applying existing regulation for a similar/comparable product. In
this context tobacco cigarettes are serving as a benchmark used to regulate the electronic
cigarettes due to comparability of the attributes. In the worldwide practice there are several
countries, including Australia and Brazil, which have entirely banned e-cigarettes. However,
is it the case for Europe and States?
Further on, we will discuss currently existing approaches to the regulation of
electronic cigarettes in Europe and United States. Here we are talking about different legal
systems, those of civil and common law, respectively. Despite the differences in legal systems
there is another important difference, which lies in the implementation. As implementation of
laws by Member States of the EU has a “top to the bottom” character, where EU legislation is
formulated on the supranational lever and is then implemented by Member States into the
26
National law. Whereas in the US, States formulate the legislation and later on it is being used
to provide guidance for the National law, “bottoms up” approach. We start with the regulation
of e-cigarettes in the EU and carry on with the US regulation supported by comments.
European regulation
In the European Union electronic cigarettes are covered by 17 EU directives and regulations
covering general product safety, chemical safety, electrical safety, weights and measures, etc.
Under the new legislation, e-cigarettes will be regulated under the Tobacco Products
Directive. The latest directive that came in power in May of this year restricts ingredients and
strength of the nicotine, along with advertising, as it is for tobacco products (Farsalinos &
Stimson, 2014).
Nevertheless, in the UK e-cigarette are regulated as medicine, meaning that from 2016
all e-cigarettes on sale have to be approved by the Medicines and Healthcare Products
Regulatory Agency, just as any other drug. However, this has not stopped the proposition of a
public ‘vaping’ ban in Wales (Jacobs & Robinson, 2014). Along with the UK, Sweden,
Germany and Greece have proposed e-cigarettes to be regulated as medical products and
devices. Proposed medicinal regulation was rejected by the European Parliament in favour of
a consumer model of regulation. However, there have been court cases in Europe challenging
the classification of electronic cigarettes as medicinal products and one more case in the USA.
In all of these cases, the court ruled to prohibit regulating electronic cigarettes as medications
(Farsalinos & Stimson, 2014).
Farsalinos & Stimson (2014) discussed the potential for regulating the e-cigarettes as
medicinal product, where they foresee certain challenges, as electronic cigarettes will most
probably be changed into another form of NRT, pharmaceutical nicotine inhaler, which is
currently unnecessary. Moreover, such a product will not be accepted by the public as e-
cigarettes are accepted now. Additionally, the authors find regulation of e-cigarettes as
tobacco “inappropriate, disproportionate and misleading” (p.4), as risks associated with
tobacco will be transferred upon e-cigarettes where it is not the case. Farsalinos & Stimson
(2014) suggest that the main criterion for regulation should be “to serve public health in the
most efficient way rather than to make the work of the regulators easier” (p.4). They conclude
by suggesting a development of regulation specifically designed for electronic cigarettes,
which would address the “unique aspects of the product and the way they are adopted and
used by consumers” (p.5).

27
Further we will discuss the regulation of electronic cigarettes in the USA and address
currently ongoing debate associated with this issue.
USA regulation
Regulation of e-cigarettes in the USA has merged around the Food and Drug Administration
(FDA). FDA has a regulatory jurisdiction over cigarettes and smokeless tobacco. They have
recently announced an authority over e-cigarettes, along with cigars, pipe tobacco and other
products to be given to the federal government. However, FDA’s jurisdiction over electronic
cigarettes will become formal when the rules become final, which may take months or years.
The jurisdiction has not been gained when the rules were proposed.
Currently the FDA is working on the regulation document, draft of which was
introduced to the companies, their lawyers and health experts across the country on April 24.
The proposed document contained 241 pages and included such issues as limitation of sales to
minors, but did not address the issues of marketing and regulation of flavouring. These issues
are very tricky but necessary to handle, which is being done now. It has been acknowledges
that a need of new ruling may arise (Tavernise & Meier, 2014).
There is currently a debate about the proposed regulation of the FDA, as a new
research found the e-cigarettes to be more dangerous than previously estimated. Yet, long-
term effects of vapours are unclear; nonetheless, there is no clear evidence that it causes
cancer or heart disease as cigarette smoking. “Many researchers agree that e-cigarettes will
turn out to be much safer than conventional cigarettes, an idea that e-cigarette companies have
made much of in their advertising” (The New York Times, 2014). Along with the latter, many
are in support of the view that the regulation proposed by FDA is not proportionate.
The US is currently the biggest market for vapours, where regulation varies
tremendously from State to State. While FDA is working on the regulation, on the state level
there have already been regulations in place. State legislatures have passed laws prohibiting e-
cigarette sale to minors, the new FDA regulations would extend that ban to all 50 states.
These rules are not approved yet and for now would not override state laws. In the meantime,
those state laws include other provisions — including varying definitions of e-cigarettes. Five
states — Alaska, Kentucky, Vermont, Wisconsin and Virginia — explicitly say that e-
cigarettes are not tobacco products. In at least eighteen states e-cigarettes are added to the
nontobacco category without explicit elaboration on the absence of relatedness to tobacco;
and ten states have considered e-cigarettes as tobacco products (Richtel, 2014).
28
There is an ongoing debate over the regulation of e-cigarettes in the US. Some of the
opinions presented on topic in The New York Times (2014), are more/less in support for the
proposed regulation. The former chief of the Tobacco Use Prevention Service in Oklahoma,
Doug Matheny, supports the regulation. According to him, recently three biggest companies –
Philip Morris, R.J. Reynolds and Lorillard –collaborated to promote “Trojan horse
legislation” in Oklahoma, where an e-cigarettes use rate is very high. Collectively, the
companies, by means of lobbying, were pushing a law that declared ‘vapor products’ and
‘alternative nicotine products’ to be nontobacco products. Another law would have eliminated
state excise taxes on all future non-combustible tobacco products. Therefore, D. Matheny
thinks that states need the FDA to establish strong standards for tobacco products and e-
cigarettes. New policies should recognize different degrees of risk associated with new
products, whereas community should educate youth and promote a healthy lifestyle.
Sheelah A. Feinberg, the director of the NYC Coalition for a Smoke-Free City, is also
of the opinion that e-cigarettes should be strictly marketed. She thinks that FDA should
restrict marketing and flavours, and require packaging to have warnings about the dangers of
nicotine poisoning; FDA should impose high product standards along with regulation of the
nicotine levels. Finally, Ms. Feinberg finds it urgent for FDA to review and evaluate e-
cigarettes quickly, to prevent existence and emergence of potentially dangerous products.
On the contrary, Amy L. Fairchild, a professor of sociomedical sciences at Columbia
University's Mailman School of Public Health, says that to the current smokers, teenagers or
minors, e-cigarettes seem most appealing, mainly due to the flavours. Moreover, Dr. Fairchild
finds it critical not to limit the potential of e-cigarettes as to really challenge tobacco
cigarettes. In her opinion the proposed document sets the stage “for a more tolerant approach
to tobacco control” as it leaves e-cigarettes “in a position to outstrip tobacco cigarettes in
popularity and market share” (The New York Times, 2014).
In support of the adjustment of proposed regulation, Norman Siege, civil rights and
civil liberties lawyer in New York City, mentioned the 2010 federal lawsuit, where the district
court observed that “the FDA had cited no evidence to show electronic cigarettes harmed
anyone”. Therefore, without evidence the FDA should “tread lightly” (The New York Times,
2014). Thus, FDA should not advocate media restrictions without sufficient data indicating
that e-cigarettes are harmful.

29
4. “Cutting” the tobacco market – No smoke without fire
4.1 Statistics on smoking
It is well known that tobacco is used in various ways and devices, where cigarette smoking is
the most common. Other ways include cigars, pipes, chutta, and beedis (Indian cigarettes).
There are also smokeless forms of tobacco, which include snuff, chewing tobacco, paste and
dipping (Patel, 1999).
Narayan, Chadha, Hanson, Tandon, Shekhawat, Fernandes & Gopinath (1996) found
that each year, worldwide use of tobacco resulted in approximately 3 million deaths. Nearly
one third of those deaths occurred in India. Based on those findings it was estimated that there
will be 10 million per year tobacco related deaths worldwide will by 2020; majority of these
deaths would occur in the developing countries as India and China (Patel, 1999).
More recently the World Health Organization (2014) has found that tobacco caused
100 million deaths in the 20th century; and 1 billion deaths are projected to take place in the
21st century if current tendency continues. Finally, tobacco-related deaths are approximated
to surpass 8 million per year by 2030, which is yet unchecked.
The latest statistics from the WHO (2014) also show that tobacco use kills nearly 6
million people a year from direct and second-hand smoking worldwide. Approximately half
of current smokers will eventually die of a tobacco-related disease. Moreover, it has been
highlighted that the smoking is so maleficent due to the lag of several years between the time
when one takes up tobacco use and the time when his/her health suffers.
Next important part of the smoking statistics concerns use by minors. Just as
mentioned in the previous sections, use of cigarettes by minors raises great concerns with
policymakers who are supporting the heavy regulation of e-cigarettes.
From the National Survey on Drug Use and Health in USA, Substance Abuse and
Mental Health Services Administration (SAMHSA, 2011) found that more than 80% of
regular smokers starts up before the age of 18; 90% do so before they reach their 20s, as
reported by Tobacco-Free Kids (2014). These finding could serve as a justification for the
strict regulation of the tobacco cigarettes and, thus, the electronic ones.
Despite this, it is important to mention that consumers were found to prefer using
electronic cigarettes as a guilt-free smoking due to absence of health risks associated with
tobacco smoking. In this context, e-cigarettes are in direct competition with cigarettes, as
nicotine in electronic cigarettes is identical to nicotine in tobacco in its molecular structure

30
(Farsalinos & Stimson, 2014). Moreover, most of the e-cigarettes users have been successful
in giving up smoking, which was proved in a recent study in England. Users of e-cigarettes
were found successful at giving up smoking, unlike with different NRT as nicotine patches or
gum (Brown, Beard, Kotz, Michie, & West, 2014).
Finally, the online “YouGov” survey found that smokers use e-cigarettes to help them
to cut down on smoking and eventually quit. And despite the fear of many that e-cigarettes
will encourage others to take up smoking, there was no supporting evidence, as only 1% of
people who had never smoked before, have tried electronic cigarettes (Daily Mail Reporter,
2014).
These alarming statistics call for a necessary action from the policymakers. Protecting
minors against attempting to smoke, as well as the encouragement of current smokers to quit,
is necessary to eliminate the issue of second-hand smoking and to assure the health of the
population.
In Oklahoma estimated 18% of high-school students have tried vaping, which is nearly
double the national average, there was no evidence found in support of attempt to smoke
tobacco cigarettes by minors after vaping (Richtel, 2014). Despite the reasonable fears, which
are associated with the tobacco smoking, there is no evidence to assume that minors will take
up smoking due to the appearance of the flavoured vapours, which would lead them to try
tobacco cigarettes.
4.2 Conflict of Interests
As Pigou (1962) suggests that taxation could be an optimal mechanism to improve economic
efficiency in the presence of negative externalities, it would seem optimal to tax e-cigarettes
in ‘proportion’ to the externalities arising from the use of these devices. The EU and US
legislation regulates and tax electronic cigarettes equally to tobacco cigarettes despite the fact
that e-cigarettes are much healthier compared to tobacco cigarettes, more effective than other
NRT products; the lack of proof that it leads minors to start smoking and evidence that it is a
much safer product in the sense of combustion as the chance of fires is substantially
decreased. The reduced amount of both financial and health externalities by the e-cigarettes
compared to tobacco cigarettes should call for a differentiated regulation and tax mechanism
but this is not the case. This calls upon an analysis of the reasons the industry and government
might have to do so anyway.
The emergence of the electronic cigarette is highly disruptive for the Big Tobacco. As
users are seeing this as an option to decrease consumption of tobacco cigarettes or quit

31
altogether, it could shrink the market share of the Big Tobacco. The potential decease in
demand is a real threat where not only cigarette producers could be affected but also tobacco
farmers and others in the vertical chain of production. The European Commission had called
originally for a stricter regulation of electronic cigarettes, which would have categorized it as
a NRT product. 28 EU Member States supported this but the Parliament opted to keep it
regulated as a tobacco product after intense lobbying from the tobacco industry (Jolly, 2014).
The shrinkage of the Big Tobacco means shrinkage of tax revenue for governments. As
tobacco tax revenue have historically accounted for 3 to 5% of government revenue in high-
income countries (Jha & Chaloupka, 2000), this is not a number they would like to see
decreased as the authors describe how dependent governments have grown to be on these
proceeds.
As more people are using e-cigarettes to quit smoking, thus as a NRT product, it also
has the potential to decrease the market share for the pharmaceutical industry producing and
selling NRT products. Users of e-cigarettes were found successful at giving up smoking,
unlike with different NRT such as nicotine patches or gum (Brown, Beard, Kotz, Michie, &
West, 2014). Some studies showed that e-cigarettes can deliver nicotine more effectively and
considerably diminishes cravings more rapidly than a nicotine inhaler (Non-Smokers’ Rights
Association, 2013).
In the US, the threat is so real that companies such as GlaxoSmithKline and Pfizer,
which sell nicotine patches and gums that are regulated as NRT, are hoping that the FDA
regulates electronic cigarettes as another tobacco product like the European Parliament did,
rather than an NRT product like in Britain, as they see e-cigarettes as their direct competition
(McArdle, 2014).
In North Carolina a bill was passed which impose a ‘5 cents per ml of nicotine liquid’
tax on e-cigarettes, which was largely lobbied for by Reynolds American, a major producer of
both tobacco and electronic cigarettes. In Minnesota a much heftier tax was implemented;
95% of wholesale cost and other US states such as New Jersey and Ohio have pressed for
similar high rates (Drenkard, 2014).
A cigarette producer, and especially one that also produces e-cigarettes, asking for
taxes on electronic cigarettes may seem against common sense but the rationale behind it
appears to be of great strategy. By taxing electronic cigarettes as a tobacco product, e-
cigarettes become more expensive and the rate of consumers transitioning from tobacco
cigarettes to electronic cigarettes may be depressed. Companies such as Reynolds American
that are also involved in the production of e-cigarettes may push to regulate them as they try

32
to maintain their market share of the tobacco industry plus reap the proceeds of consumers
using and/or switching to e-cigarettes, therefore holding shares in both markets. With this
regulation in place the government safeguards its tax revenue by keeping the Big Tobacco ‘in
the game’. This does not seem as such an inexplicable phenomenon as “the primary historical
motivation, and still the most common rationale for tobacco taxation, is its revenue-generating
potential” (Jha & Chaloupka, 2000, p. 254); and governments will be inclined to protect that
potential. Furthermore, history proves that governments are not indifferent about inducements
and experiencing heavy lobbying activities from the Big Tobacco, as Philip Morris U.S.A.,
the second most active lobbying organization in America, spent approximately $101 million
between 1998 and 2004 in lobbying activities with the Congress alone (Rehn, 2014).
In the article of McArdle (2014), Linda McAvan, the British Labour Party member of
the European Parliament who guided the legislation through the chamber in the face of strong
opposition from the tobacco industry says that Member States have the option to adapt
national legislation to classify e-cigarettes as NRT if they choose so but would prove difficult
in practice. Furthermore, Martin Callanan, a British Conservative Party politician opposes
regulation of e-cigarettes as it helps people quit smoking and states that it is a huge loss for
public health in Europe. Drago Azinovic, president for European operations at Philip Morris
International, said that the modification of the EU Tobacco Directive “represents a worrying
departure from the E.U.’s basic standards of proportionate, evidenced-based policy making,
which will further erode intellectual property rights and undermine the EU charter where
these rights are protected”.
4.3 Consequences of new regulations
The 2014/40/EU Directive of the European Parliament and of the Council of April 3, 2014
concerns the regulation of tobacco products. Regulation is needed because “all tobacco
products have the potential to cause mortality, morbidity and disability” (p.7). Article 2 of the
directive lays down main definitions used throughout the whole legislative documents. In this
respect, there are several definitions that one must be equated with; they can be found in
Appendix D.
After one has gone through all these numerous definitions, it is crucial to mention
again that electronic cigarettes contain no tobacco and involve no combustion, which would
exclude them from the category ‘tobacco products’. For those who argue that nicotine is the
part of tobacco – nicotine can be gathered from the eggplant even if in small amounts (Cahn

33
& Siegel, 2011). Moreover, since there is no tobacco in e-cigarettes, they also do not fall
under the definition of the ‘smokeless tobacco product’.
Despite it all, the Commission gave a separate definition to electronic cigarettes,
which does not mention a single word about presence of tobacco. Article 20 of the Directive
covers the regulation of electronic cigarettes, where all the manufacturing, labelling and other
requirements are listed, except flavouring which is left to the Member States’ national
legislation. However, the labelling and marketing limitations in the concerned directive are
same for vapours as well as for tobacco products. This raises several questions; first of all,
what does a tobacco-less product do in the regulation for tobacco products (as defined
previously)? Second, if there is no tobacco in e-cigarettes why to regulate it as a tobacco
product?
As mentioned in the purpose of the Directive (2014), under number (8): “In
accordance with Article 114(3) of the Treaty of the Functioning of the European Union
(TFEU), a high level of health protection should be taken as a base for legislative proposals
and, in particular, any new developments based on scientific facts should be taken into
account. Tobacco products are not ordinary commodities and in view of the particularly
harmful effects of tobacco on human health, health protection should be given high
importance, in particular, to reduce smoking prevalence among young people” (p.2).
Further on, under number (19): “Considering this Directive's focus on young people,
tobacco products other than cigarettes and roll-your-own tobacco, should be granted an
exemption from certain requirements relating to ingredients as long as there is no substantial
change of circumstances in terms of sales volumes or consumption patterns of young people”
(p.4). Both paragraphs mention the ‘young people’; the whole directive is ‘focused’ on young
people. Further on, under numbers (21), (26) and (47), ‘young people’ are mentioned again,
mainly as a kind of benchmark reference used for exemptions or exclusion from those
exemptions. It is stated that “electronic cigarettes can develop into a gateway to nicotine
addiction and ultimately traditional tobacco consumption, as they mimic and normalize the
action of smoking” (p.7), which justifies the restrictive approach to advertising electronic
cigarettes and refill containers. Yet, there is no evidence to support the statement that young
people are lured by the electronic cigarettes to take up smoking. Could it be that US take
different approach?
First of all, the US regulation will come in place later, thus, definitely after the EU
directive which has come in power on May 19, 2014. FDA is opted for using the EU
regulation as a guideline.

34
As for now, there is no draft of the regulation available to the public, yet consecutive
summary can be obtained from the FDA website. Since FDA has authority over the tobacco
products’ regulation, they recognise a need for extension of the scope of products concerned
in the tobacco regulation. The new regulation will recognise additional tobacco product
categories, which will be a subject to general controls, as well as to the premarket review
requirements for “new tobacco products” and “modified risk tobacco products” (Deyton &
Woodcock, 2011). Those products do include electronic cigarettes. Moreover, “products made
or derived from tobacco can be regulated under the Tobacco Control Act unless they are
“marketed for therapeutic purposes”, in which case they are regulated as drugs and/or
devices” (Deyton & Woodcock, 2011).
It is not yet clear how exactly will e-cigarettes be regulated in the USA, however, the
chances are high that they would be given a separate category, that would be treated similar to
the ‘electronic cigarette’ product category in the EU directive.
4.4 Potential complications
In the report of the forum on e-cigarettes in Canada, the Non-Smokers’ Rights Association
(2013) has extensively discussed potential regulatory option for the electronic cigarettes.
Several approaches have been introduced. The first option discussed was regulation of e-
cigarettes as a drug/device. For instance, in Australia, New Zealand, Norway and Turkey e-
cigarettes have a status of drug and, therefore, are prohibited. The best part about such
approach is that goes in line with WHO recommendation and protects public from unproven
claims about the effects of e-cigarettes. Moreover, such approach would protect the regulated
NRTs from “unfair” competition but increase the manufacturing costs for e-cigarettes and
stifle competition. However, there are also downsides to this approach as it fails to address the
current situation and would lead to denied access for the smokers to e-cigarettes, which are
much safer than tobacco cigarettes. Finally, such regulation would result in making e-
cigarettes unattractive to smokers.
Another proposed approach is regulating e-cigarettes as a harm reduction aid. This
approach will possibly promote the use of safer nicotine products and will ensure that useful
information regarding the risks will be provided. However, following this path would mean
avoiding the differentiation between the proven and unproven cessation aids. Moreover, it
would provide a marketing advantage over pharmaceutical cessation aids “that have had to
undergo a higher level of scientific scrutiny and that must adhere to more legislated
restrictions” (Non-Smokers’ Rights Association, 2013, p. 7). Nonetheless, vapours are a part
35
of the “phase out” plan for cigarettes in New Zealand. Similarly, in UK, the Health and
Clinical Excellence (NICE) recommended to use safer nicotine products suggested to include
e-cigarettes to the licensed NRT in the future as some of the currently licensed NRTs provide
unclear benefits, “except that it pushes people along the continuum toward quitting” (Non-
Smokers’ Rights Association, 2013, p.8). Moreover, NICE oversees the obstacles and propose
vapour to be licensed for harm reduction, not cessation and therefore would not need to prove
their efficiency; the safety/efficacy is very similar to the nicotine inhaler, which would allow
Medicines Healthcare Regulation Authority (MHRA) to ‘cross-refer’ to the evidence on the
inhaler.
Next approach concerns regulating e-cigarettes as a consumer product, where
consumer protection laws could be used to require minimum product safety and
manufacturing standards. Current approach is very limited and has little potential; therefore, it
was not discussed in depth.
Fourth approach to regulation is regulating e-cigarettes as a tobacco product, just as in
the EU’s latest directive. The main pro of this approach is that it “ends current perverse
situation whereby the most hazardous nicotine product — cigarettes — is the least regulated”
(Non-Smokers’ Rights Association, 2013, p. 6). Furthermore, it will ensure availability of e-
cigarettes to the smokers, while undergoing the obstacles of tobacco control. Final pro is
protection of youth, which is achieved through regulating imitation products just as the actual
tobacco products, not mentioning the simplified legislation approach. Among cons there is a
need for government commitment to provide relative risks information, which is difficult to
do. Such regulation would not differentiate between tobacco products based on their level of
risk nor ensure a high standard of quality, safety and efficacy. Finally, such approach may
“undermine the promotion of e-cigarettes as a quit aid (they would be seen as tobacco
products); they would not be covered as a cessation aid by health insurance” (Non-Smokers’
Rights Association, 2013, p. 7).
Finally, the last approach used by several countries, among which are Singapore,
Seychelles and Uruguay – an effective ban. Such approach would lead to cutting people off
the cheaper and healthier alternative as mentioned in previous sections.
As with all well-intentional objectives, the real impacts are revealed once the
unexpected consequences emerge.

36
5. Conclusion
Big Tobacco dominated the tobacco industry for decades with minimal disruptions from new
emerging products. In 2006/2007, a new product emerged that could potentially disrupt the
industry as a whole – electronic cigarettes. As more tobacco consumers started to switch to
these new devices, the threat of disruption became real. Surveys report on its increasing use as
tobacco smokers are opting for a ‘healthier’ way of smoking by cutting down their
consumption of normal cigarettes or quitting altogether. Reports suggest that electronic
cigarettes have proven to be much more effective in helping people to quit smoking. This will
not only lead to a decrease of the Big Tobacco’s market share but that of the NRT producers
as well.
After the emergence of this new product, regulators are trying to control and contain
its widespread use. In light of this phenomenon, the European union has adopted a new
Tobacco Product Regulation (2014/40/EU Directive) where not only tobacco products such as
cigarettes, chewing tobacco and snus are heavily regulated but electronic cigarettes as well,
despite the fact that this product contains no tobacco. In the US, the FDA has not come up
with a definite way of regulating e-cigarettes but it looks like they are going to adopt the EU’s
method and classifying it as a tobacco product.
Despite the ongoing debate concerning the safety of e-cigarettes, there is yet not
enough evidence to support the current regulation of vapours, as they have proven to help
smokers quit and to be more effective than traditional NRT products. In light of this we
question the regulatory choice of the EU and potentially the US as well. Do their motives
concern the protection of public health or are they merely protecting private interests? In
order to answer our main question, some sub-questions were to be answered in order to guide
us toward the answering of our raised questions.
We conclude that the involved parties - Big Tobacco, the Government, consumers and
the Pharmaceutical Industry - all have different, and often highly conflicting interests. Big
Tobacco is after profit maximization and the defeasance of its market share. The Government
has its responsibility to protect the public interest (public health). Since the Government has
grown to be highly dependent on the proceeds from tax revenue, the presence of conflicting
interests ought to be considered. Consumers of tobacco products, NRT and e-cigarettes are
concerned with prices and availability of the demanded products and rely on the Government
to undermine the public health. The pharmaceutical industry producing NRT products, much

37
like the Big Tobacco, wants to defend its profit and market share unobstructed by the
emergence of the electronic cigarette.
Despite the resemblance between e-cigarettes and regular tobacco cigarettes, no
evidence has been found to justify their equal regulatory or taxation treatment. The chemicals
in e-cigarettes do not exceed the permitted levels and are often less than those present in
tobacco cigarettes, and comparable to those in NRT products. Due to the similarities in
purpose, e-cigarettes stand in direct competition with the other two.
Taking into consideration the competition and conflicting interests between the
involved parties, the chosen regulation is resulting in the indirect protection of market share
for both the Big Tobacco and the Pharmaceutical Industry. Above all, it will decrease the
transitioning rate of market share from the Big Tobacco and NRT, to the market for e-
cigarettes; with this, the Government will secure its channel for tax revenue. A potential
consequence is the decreased availability of vapours to consumers. As opposed by a British
Conservative Party politician, the EU regulation of e-cigarettes prevents people from quitting
smoking and imposes a huge loss for public health in Europe.
The potential problem that could rise in the future is the re-establishment of
dominance (monopoly power) of the Big Tobacco as they are buying up startup e-cigarette
companies. The ban on advertisement of e-cigarettes could lead to a development of
asymmetric information, as the public is held fairly uninformed about these products. With
the Big tobacco’s history of inadequate supply of information and the recent development of
acquisitions of start-up companies, the problem of asymmetric information could be
worsened.
Considering the decreased health and financial externalities of electronic cigarettes,
and their potential to help smokers quit, we do not agree with the current regulation of these
products. They are distinct from normal cigarettes and are not to be treated equally. Although
further research is needed, current findings suggest their decreased toxicity and lower harm on
the smokers’ health and others as they do not produce second-hand smoke.
The final argument of the Government to regulate e-cigarettes the way they do, is the
argument of minor protection. As minors discount risk differently, they fear that e-cigarettes
leads minors to pick up the smoking of tobacco cigarettes. As studies have disproved this, it is
to be questioned what other reason the government has to heavily regulate e-cigarettes the
way they do. Our findings indicate that the Government is inclined to protect its private
interest (tax revenue) more than protecting public health.

38
Recommendations
As we do not entirely support the current regulation, we present some suggestions that could
better assess the emergence of this new product. Giving the high potential for cessation use,
we suggest regulating electronic cigarettes as NRT products for harm reduction purposes
rather than cessation, with all the implied safety and standard regulations. This classification
will exempt the vapours from proving their efficiency.
We agree with the prohibition of sales and advertisement to minors; however, we find
it necessary to provide children with a proper ‘education’ concerning the effects of smoking
in order to prevent the future consumption. Furthermore, advertisement bans should be lifted
and only permitted to advertise as an NRT product and sale ought to be accompanied by a
doctor’s prescription. The downside to the suggested approach concerns limited accessibility
and its use as a hard reduction product. But until more extensive research is conducted on its
safety and health implications, we suggest this approach to be a better alternative.

39
Bibliography
14News. (2014, Jan 17). McIntyre says Obama Administration plans to fund tobacco buyout
payments. Retrieved on May 18, 2014, from
http://www.14news.com/story/24378583/mcintyre-says-obama-administration-plans-
to-fund-tobacco-buyout-payments
Agricultural Marketing Resource Center. (2012). Tobacco Profile. Retrieved on May 18,
2014, from http://www.agmrc.org/commodities__products/specialty_crops/tobacco-
profile/
Alpert, H. R., Connolly, G. N., & Biener, L. (2013). A prospective cohort study challenging
the effectiveness of population-based medical intervention for smoking cessation.
Tobacco control, 22(1), 32-37.
American Cancer Society. (2014, June 2). What are the types of nicotine replacement
therapy?. Retrieved on June 4, 2014, from
http://www.cancer.org/healthy/stayawayfromtobacco/guidetoquittingsmoking/guide-
to-quitting-smoking-types-of-nrt
BBC News (2014, April 27). E-cigarette users in UK have 'tripled' since 2010. Retrieved on
April 28, 2014, from http://www.bbc.com/news/health-27161965
Becker, G. S., Grossman, M., & Murphy, K. M. (1994). An empirical analysis of cigarette
addiction (No. w3322). National Bureau of Economic Research.
Berger, R. (2013). The New Tobacco Products Directive – Potential Economic Impact.
Roland Berger.
Berman, M., Crane, R., Seiber, E., & Munur, M. (2013). Estimating the cost of a smoking
employee. Tobacco control. Retrieved on June 6, 2014, from
http://ucanr.edu/sites/tobaccofree/files/175136.pdf
Bero, L. (2003). Implications of the tobacco industry documents for public health and policy.
Annual Review of Public Health, 24(1), 267-288.
Bloomberg. (2012). Most tax Revenue from Alcohol, Tobacco, Betting: States. Bloomberg
Visual Data. Retrieved on May 28, 2014, from http://www.bloomberg.com/visual-
data/best-and-worst/most-tax-revenue-from-alcohol-tobacco-betting-states
Borland, R., Fong, G. T., Yong, H. H., Cummings, K. M., Hammond, D., King, B., ... &
Zanna, M. P. (2008). What happened to smokers’ beliefs about light cigarettes when
“light/mild” brand descriptors were banned in the UK? Findings from the
International Tobacco Control (ITC) Four Country Survey. Tobacco Control, 17(4),
256-262.

40
Brown, J., Beard, E., Kotz, D., Michie, S., & West, R. (2014). Real‐world effectiveness of
e‐cigarettes when used to aid smoking cessation: a cross‐sectional population study.
Addiction. Retrieved on May 25, 2014, from
http://onlinelibrary.wiley.com/journal/10.1111/%28ISSN%291360-0443/accepted
Burny, P. (2010). Reforming the Common Agricultural Policy perspective of 2013 and
beyond. Advances in Agriculture & Botanics, 2(2).
Cahn, Z., & Siegel, M. (2011). Electronic cigarettes as a harm reduction strategy for tobacco
control: A step forward or a repeat of past mistakes? Journal of public health policy,
32(1), 16-31.
Coase, R. H. (1960). Problem of social cost, the. Jl & econ., 3, 1.
Cooter, R. & Ulen, T. (2014). Law and Economics. 6th international edition. Boston: Pearson
Addison Wesley
Daily Mail Reporter. (2014, April 28). E-cigarettes AREN'T encouraging people to take up
smoking: Study finds most of those puffing on them are former tobacco smokers.
Daily Mail Online. Retrieved on May 28, 2014, from
http://www.dailymail.co.uk/health/article-2614596/Two-million-puff-e-cigarettes-
Number-using-devices-trebles-two-years.html
Deyton, L. R., & Woodcock, J. (April 25, 2011). Stakeholder Letter: Regulation of E-
Cigarettes and Other Tobacco Products. Public Health Focus. Retrieved on June 3,
2014, from http://www.fda.gov/newsevents/publichealthfocus/ucm252360.htm
Directive 2014/40/EU of the European Parliament and of the Council of 3 April 2014 on the
approximation of the laws, regulations and administrative provisions of the Member
States concerning the manufacture, presentation and sale of tobacco and related
products and repealing Directive 2001/37/EC [2014] OJ L127/1
Drenkard, S. (2014, May 27). North Carolina’s E-cigarette Tax Proposal. Tax Foundation.
Retrieved on June 2, 2014, from http://taxfoundation.org/blog/north-carolina-s-e-
cigarette-tax-proposal
Efpia. (2014). EU Legislatiion. Retrieved on May 18, 2014, from http://www.efpia.eu/eu-
legislation
Eriksen, M., Mackay, J., & Ross, H. (2013). The tobacco atlas (No. Ed. 4). American Cancer
Society.
Farsalinos, K. E., & Stimson, G. V. (2014). Is there any legal and scientific basis for
classifying electronic cigarettes as medications?. International Journal of Drug
Policy. Retrieved on May 2, 2014, from
http://dx.doi.org/10.1016/j.drugpo.2014.03.003

41
Guindon, G. E., Tobin, S., & Yach, D. (2002). Trends and affordability of cigarette prices:
ample room for tax increases and related health gains. Tobacco control, 11(1), 35-43.
Hall, J. R. Jr. (2013, July). The Smoking-Material Fire Problem. National Fire Protection
Association: Fire Analysis and Research Division. Retrieved on June 6, 2014, from
http://www.nfpa.org/~/media/Files/Research/NFPA%20reports/Major%20Causes/os
smoking.pdf
Häge, F. M. (2012). Bureaucrats as Law-makers: Committee Decision-making in the EU
Council of Ministers (Vol. 21). Routledge.
HowStuffWorks. (2011). How Electronic Cigarettes Work. Retrieved on June 9, 2014, from
http://science.howstuffworks.com/innovation/everyday-innovations/electronic-
cigarette1.htm
Jacobs, E., & Robins, D. (2014, April 17). E-cigarettes: no smoke without fear. Financial
Times Magazine. Retrieved on April 20, 2014, from
http://www.ft.com/intl/cms/s/2/ed185b54-c5e0-11e3-a7d4-
00144feabdc0.html#axzz2zakjNBqd
Lee, D. R. (1991). Government v. Coase: the case of smoking. Cato J., 11, 151.
Jha, P., & Chaloupka, F. J. (2000). Tobacco control in developing countries. In Chaloupka, F.
J., Hu, T., Warner, K. E., Jacobs, R. & Yurekli. A., The taxation of tobacco products.
(pp. 237-272). Oxford University Press.
Jha, P., Musgrove, P., Chaloupka, F. J., & Yurekli, A. (2000). The economic rationale for
intervention in the tobacco market. Tobacco control in developing countries, (pp.
153-174). Oxford University Press.
Jolly, D. (2014, February 26). European Parliament Approves Tough Rules on Electronic
Cigarettes. New York Times. Retrieved on June 2, 2014, from
http://www.nytimes.com/2014/02/27/business/european-union-approves-tough-rules-
on-electronic-cigarettes.html?_r=0
London Fire Brigade. (2014). Smoking. Retrieved on June 6, 2014, from http://www.london-
fire.gov.uk/smoking.asp
McArdle, M. (2014, February 6). E-Cigarettes: A $1.5 Billion Industry Braces for FDA
Regulation. Bloomberg BusinessWeek. Retrieved on June 2, 2014, from
http://www.businessweek.com/articles/2014-02-06/e-cigarettes-fda-regulation-
looms-for-1-dot-5-billion-industry
McCormick, B., & Stone, I. (2007). Economic costs of obesity and the case for government
intervention. Obesity Reviews, 8(s1), 161-164.

42
McKee, M., MacLehose, L., & Nolte, E. (2004). Health policy and European Union
enlargement. McGraw-Hill International.
Mincer, J. (2014, May 25). Quality issues push e-cigarette production to U.S. from China.
Reuters. Retrieved on May 27, 2014, from
http://www.reuters.com/article/2014/05/25/us-usa-tobacco-ecigarettes-
idUSBREA4O06420140525
Motta, M. (2004). Competition policy: theory and practice. Cambridge University Press.
MSN Healthy Living. (2014). Day 2: Slap on the patch. Retrieved on June 9, 2014, from
http://healthyliving.msn.com/health-wellness/healthy-habits/21-days-to-a-new-you-
stop-smoking?pagebr=2#3
Narayan, K. V., Chadha, S. L., Hanson, R. L., Tandon, R., Shekhawat, S., Fernandes, R. J., &
Gopinath, N. (1996). Prevalence and patterns of smoking in Delhi: cross sectional
study. BMJ: British Medical Journal, 1576-1579.
Noel, J. K., Rees, V. W., & Connolly, G. N. (2011). Electronic cigarettes: a new ‘tobacco’
industry?. Tobacco Control, 20(1), 81-81.
Non-Smokers’ Rights Association (January 30, 2013). Report of the Forum on E-cigarettes.
Retrieved on June 1, 2014, from http://www.nsra-adnf.ca/cms/file/files/SHAF_E-
cig_Forum_Report_Feb_2013-FINAL.pdf
Patel, D. R. (1999). Smoking and children. The Indian Journal of Pediatrics, 66(6), 817-824.
Phizer. (n.d.). Dosage and Administration. Retrieved on June 9, 2014, from
https://www.pfizerpro.com/hcp/nicotrol/dosage
Pigou, A. C. (1962). A Study in Public Finance, 3rd revised edn. London: Macmillan and Co.
Ramsey, F. P. (1927). A Contribution to the Theory of Taxation. The Economic Journal,
37(145), 47-61.
Rehn, A. (2014, Feb 12). 6 Mega Corporations Control Almost the Entire Global Cigarette
Industry. PolicyMic. Retrieved May 18, 2014, from
http://www.policymic.com/articles/81365/6-mega-corporations-control-almost-the-
entire-global-cigarette-industry
Richtel, M. (2014, April 26). Where Vapor Comes Sweeping Down the Plain. E-Cigarettes
Take Hold in Oklahoma. The New York Times. Retrieved April 28, 2014, from
http://www.nytimes.com/2014/04/27/business/e-cigarettes-take-hold-in-
oklahoma.html
Riley, G. (2012). Demerit goods. Tutor2u. Retrieved on June 14, from
http://tutor2u.net/economics/revision-notes/as-marketfailure-demerit-goods.html

43
Rosen, H.S. and T. Gayer (2010), Public Finance, 9th edition, New York: McGraw-Hill/Irwin
Ross, H. (2004). The economics of tobacco and tobacco control. European Union ASPECT
Consortium. Tobacco or health in the European Union: past, present and future.
Luxembourg, Office for Official Publications of the European Communities, 69-98.
SMOCARE. (2014). Washable Clearomizer EGO CE4 Electronic Cigarette. Retrieved on
June 9, 2014, from http://www.egoelectronic-cigarettes.com/quality-1559561-
washable_clearomizer_ego_ce4_electronic_cigarette.html
Soap. (2014). Nicorette OTC Stop Smoking Nicotine Gum, 4mg-Fruit Chill-100 ct. retrieved
on June 10, 2014, from http://www.soap.com/p/nicorette-otc-stop-smoking-nicotine-
gum-4mg-fruit-chill-49019
Tavernise, S. & Meier, B. (2014, April 24). For E-Cigarettes, the Regulatory Battle Now
Begins. The New York Times. Retrieved April 28, 2014, from
http://www.nytimes.com/2014/04/25/business/for-e-cigarettes-the-regulatory-battle-
now-begins.html?_r=0
The New York Times. (2014, May 4). How Should E-Cigarettes Be Regulated? The opinion
pages. Retrieved on May 5, 2014, from
http://www.nytimes.com/roomfordebate/2014/05/04/how-should-electronic-
cigarretes-be-regulated
Thorpe, N. (2013, May 17). Bulgaria tobacco growers hope for EU cash. BBC News.
Retrieved May 17, 2014, from http://www.bbc.com/news/world-europe-22544741
Tobacco-Free Kids. (March 27, 2014). The Path to Smoking Addiction Starts at Very Young
Age. Fact Sheet. Retrieved on May 28, 2014, from
http://www.tobaccofreekids.org/research/factsheets/pdf/0127.pdf
United Medical Blog. (2013). Electronic Cigarette. Retrieved on June 10, 2014, from
http://umd0.info/electronic-cigarette.html
United States department of Agriculture. (2013). Tobacco Transition Payment Program.
Retrieved may 18, 2014, from
http://www.fsa.usda.gov/FSA/webapp?area=home&subject=toba&topic=landing
United States Department of Agriculture. (2014). Government payments and the Farm Sector.
Retrieved on May 18, 2014, from http://ers.usda.gov/topics/farm-economy/farm-
commodity-policy/government-payments-the-farm-sector.aspx#.U3iYfscwi3U
U.S. Department of Health and Human Services. (2014). The Health Consequences of
Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: U.S.
Department of Health and Human Services, Centers for Disease Control and
Prevention, National Center for Chronic Disease Prevention and Health Promotion,
Office on Smoking and Health, 2014.

44
World Health Organization. (2014). Tobacco. Fact sheet №339. Retrieved on May 20, 2014,
from http://www.who.int/mediacentre/factsheets/fs339/en/
World Press. (n.d.) Tools to Help You Quit. Retreieved on June 10, 2014, from
http://icanquit.wordpress.com/tools-to-help-you-quit/

45
Appendix A
Health complications of smoking
(Source: U.S. Department of Health and Human Services, 2014)

46
Appendix B
B1) Electronic cigarettes. Inside an E-cigarette
(Source: HowStuffWorks, 2011)
B2) Flavoured E-cigarettes
(Source: SMOCARE, 2014)

47
B3) Researchable E-cigarette
(Source: United Medical Blog, 2013)

48
Appendix C
C1) Inhaler (NRT)
(Source: Pfizer, n.d.)
C2) Nicotine Patch (NRT)
(Source: MSN Healthy Living, 2014)
C3) Nicotine Gum (NRT)
(Source: Soap, 2014)

49
C4) Nasal Spray (NRT)
(Source: World Press, n.d.)
C5) Lozenges (NRT)
(Source: World Press, n.d.)

50
Appendix D
Article 2 of the Directive 2014/40/EU (2014, p. 10-12) uses the following definitions:
(1) ‘tobacco’ means leaves and other natural processed or unprocessed parts of tobacco plants,
including expanded and reconstituted tobacco;
(4) ‘tobacco products’ means products that can be consumed and consist, even partly, of
tobacco, whether genetically modified or not;
(5) ‘smokeless tobacco product’ means a tobacco product not involving a combustion process,
including chewing tobacco, nasal tobacco and tobacco for oral use;
(9) ‘tobacco products for smoking’ means tobacco products other than a smokeless tobacco
product;
(10) ‘cigarette’ means a roll of tobacco that can be consumed via a combustion process and is
further defined in Article 3(1) of Council Directive 2011/64/EU;
(14) ‘novel tobacco product’ means a tobacco product which:
(a) does not fall into any of the following categories: cigarettes, roll-your-own
tobacco, pipe tobacco, waterpipe tobacco, cigars, cigarillos, chewing tobacco, nasal tobacco
or tobacco for oral use; and
(b) is placed on the market after 19 May 2014;
(16) ‘electronic cigarette’ means a product that can be used for consumption of nicotine-
containing vapour via a mouth piece, or any component of that product, including a cartridge,
a tank and the device without cartridge or tank. Electronic cigarettes can be disposable or
refillable by means of a refill container and a tank, or rechargeable with single use cartridges;
(17) ‘refill container’ means a receptacle that contains a nicotine-containing liquid, which can
be used to refill an electronic cigarette;
(18) ‘ingredient’ means tobacco, an additive, as well as any substance or element present in a
finished tobacco product or related products, including paper, filter, ink, capsules and
adhesives;
(19) ‘nicotine’ means nicotinic alkaloids;
(20) ‘tar’ means the raw anhydrous nicotine-free condensate of smoke;

51
(21) ‘emissions’ means substances that are released when a tobacco or related product is
consumed as intended, such as substances found in smoke, or substances released during the
process of using smokeless tobacco products;
(22) ‘maximum level’ or ‘maximum emission level’ means the maximum content or emission,
including zero, of a substance in a tobacco product measured in milligrams;
(23) ‘additive’ means a substance, other than tobacco, that is added to a tobacco product, a
unit packet or to any outside packaging;
(24) ‘flavouring’ means an additive that imparts smell and/or taste;
(25) ‘characterising flavour’ means a clearly noticeable smell or taste other than one of
tobacco, resulting from an additive or a combination of additives, including, but not limited
to, fruit, spice, herbs, alcohol, candy, menthol or vanilla, which is noticeable before or during
the consumption of the tobacco product;
(26) ‘addictiveness’ means the pharmacological potential of a substance to cause addiction, a
state which affects an individual's ability to control his or her behaviour, typically by instilling
a reward or a relief from withdrawal symptoms, or both;
(27) ‘toxicity’ means the degree to which a substance can cause harmful effects in the human
organism, including effects occurring over time, usually through repeated or continuous
consumption or exposure;
(28) ‘substantial change of circumstances’ means an increase of the sales volumes by product
category by at least 10% in at least five Member States based on sales data transmitted in
accordance with Article 5(6) or an increase of the level of prevalence of use in the under 25
years of age consumer group by at least five percentage points in at least five Member States
for the respective product category based on the Special Eurobarometer 385 report of May
2012 or equivalent prevalence studies; in any case, a substantial change of circumstances is
deemed not to have occurred if the sales volume of the product category at retail level does
not exceed 2,5 % of total sales of tobacco products at Union level;